Embed Size (px)
Citation preview
Vector-Borne Diseases of Interest in Ontario
2
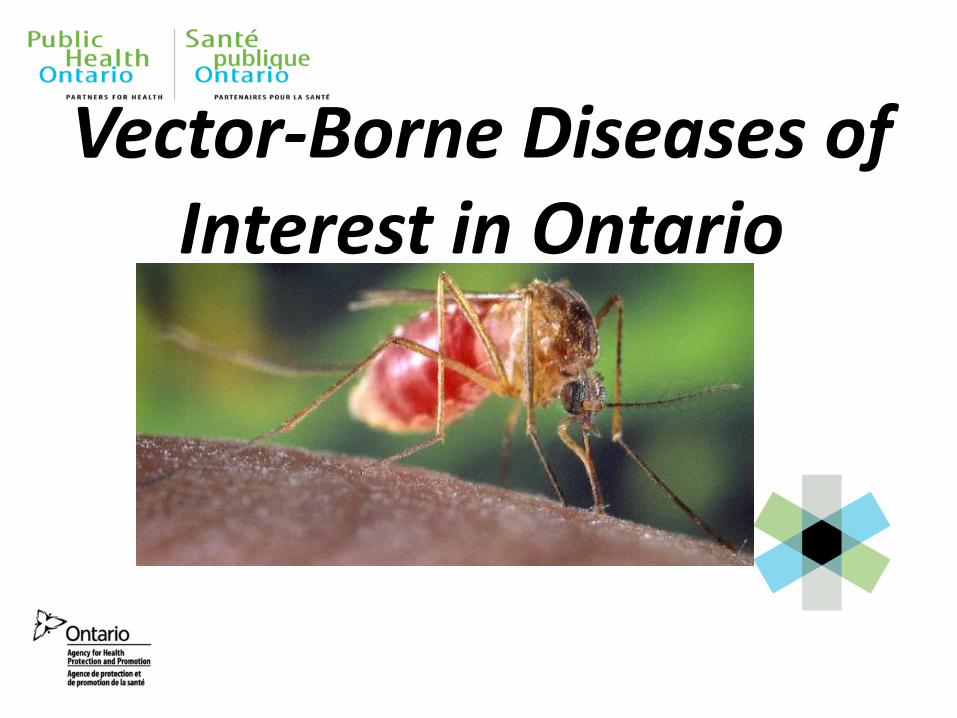
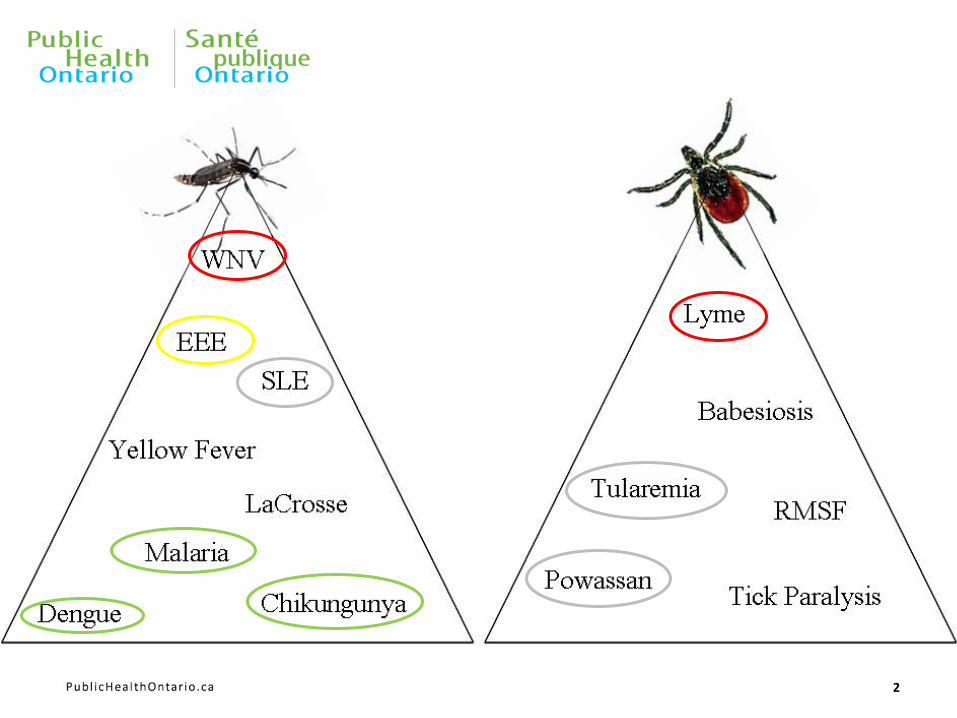
Ontario’s Vector-Borne Diseases • Reportable vector-borne diseases in Ontario are:
• West Nile Virus (WNV)
• Lyme disease (LD)
• Eastern Equine Encephalitis (reported under encephalitis)
• Malaria
• Yellow Fever
• Dengue (reported under hemorrhagic fever)
Vector-Borne Disease Program
Ontario’s program consists of the following:
• Human surveillance
• Vector surveillance
• Vector control
• Public education
Roles of Public Health Units
• To conduct vector surveillance in an effort to assess the risk of vector-borne diseases to humans.
• To conduct local risk assessments based on surveillance data and local ecological factors.
• Create local programs based on the results of the risk assessments.
• Coordinate the provincial program
• Provide expert consultation, create guidelines, best practices, and data analysis
• To ensure that health units are able to conduct local risk assessments properly
EZVBD Unit Activities
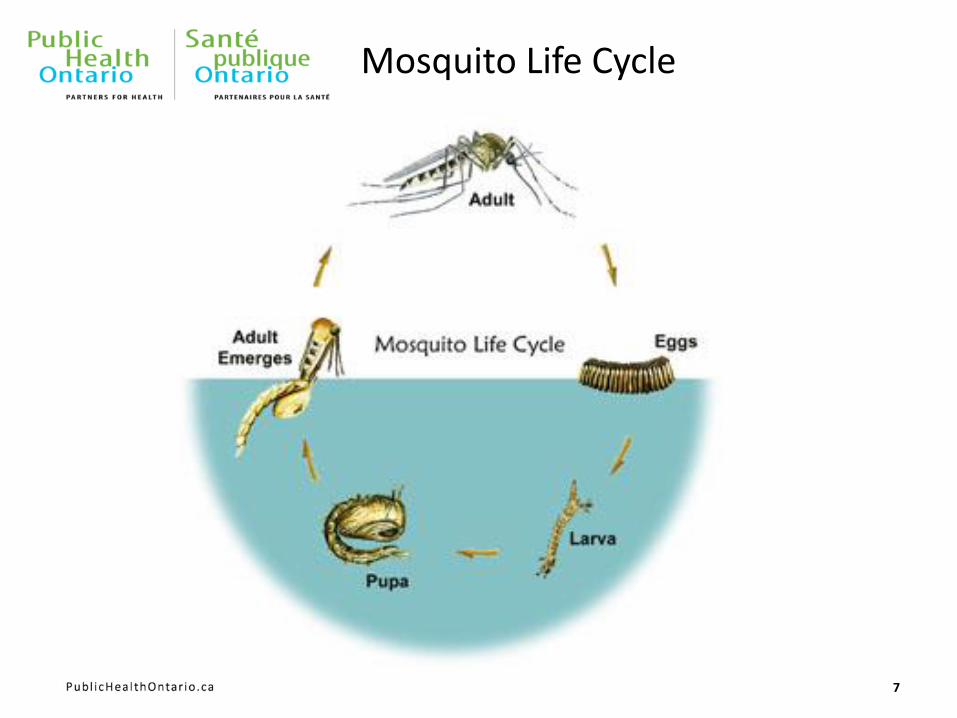
Mosquito Life Cycle
7
Objectives of Mosquito Surveillance
• To determine the location and infection rate of mosquito vectors.
• Mosquito surveillance is one of the most effective tools in assessing the risk of mosquito-borne diseases to the public.
• Mosquito surveillance is conducted by all health units in Ontario.
• This surveillance also gives Ontario the opportunity to monitor for invasive species and other mosquito-borne diseases such as Eastern Equine Encephalitis
How Mosquito Surveillance is Conducted
• Health units set up mosquito traps on a weekly basis.
• The traps are set in the same place from year to year.
• Each health unit is allotted a certain number of traps per week depending on risk, geographical size and population.
• Trapped mosquitoes are sent to qualified service providers for speciation and viral testing
• The service providers report the data to the health units and ministry on a weekly basis
• EZVBDU staff create a weekly vector surveillance report that is distributed to the health units

Mosquito Surveillance (Trapping)
CDC Miniature Light Trap
• Attracts host-seeking adult mosquitoes.
Larval Dipping
• Looking for larvae in their aquatic habitat.
http://www.johnwhock.com/images/512.jpg
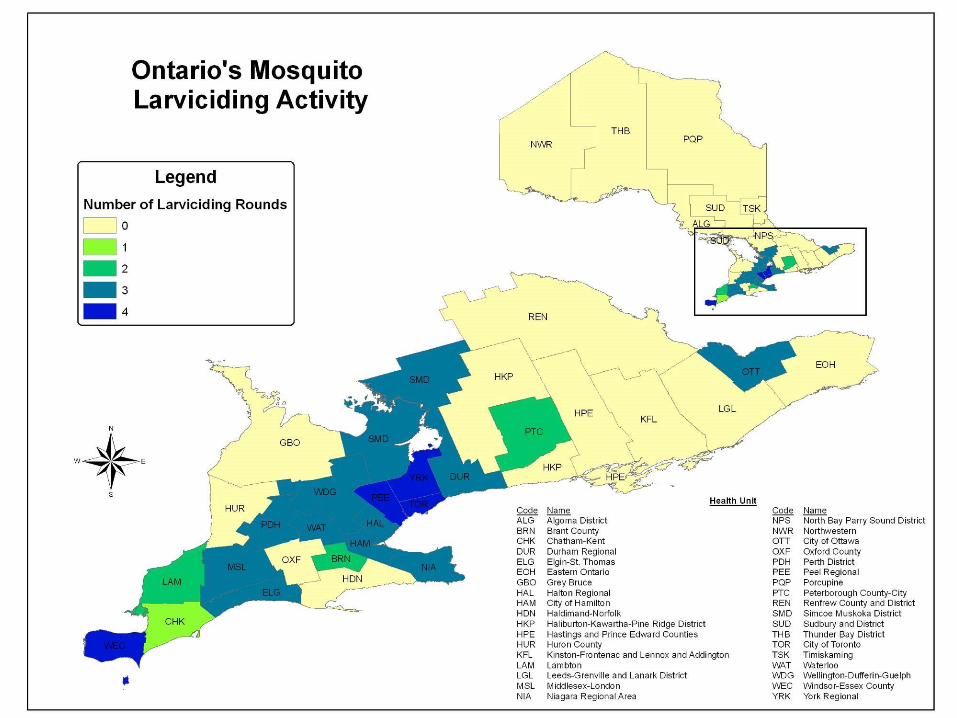
Mosquito Control in Ontario
• There are three larvicides currently approved for WNV control in Ontario:
1. Bacillus thuringiensis israelensis (Bti) 2. Bacillus sphaericus (B. sphaericus) 3. Methoprene
The only adulticide product currently approved for use in Ontario is malathion.
12 CDC/ James D. Gathany
Malaria
13
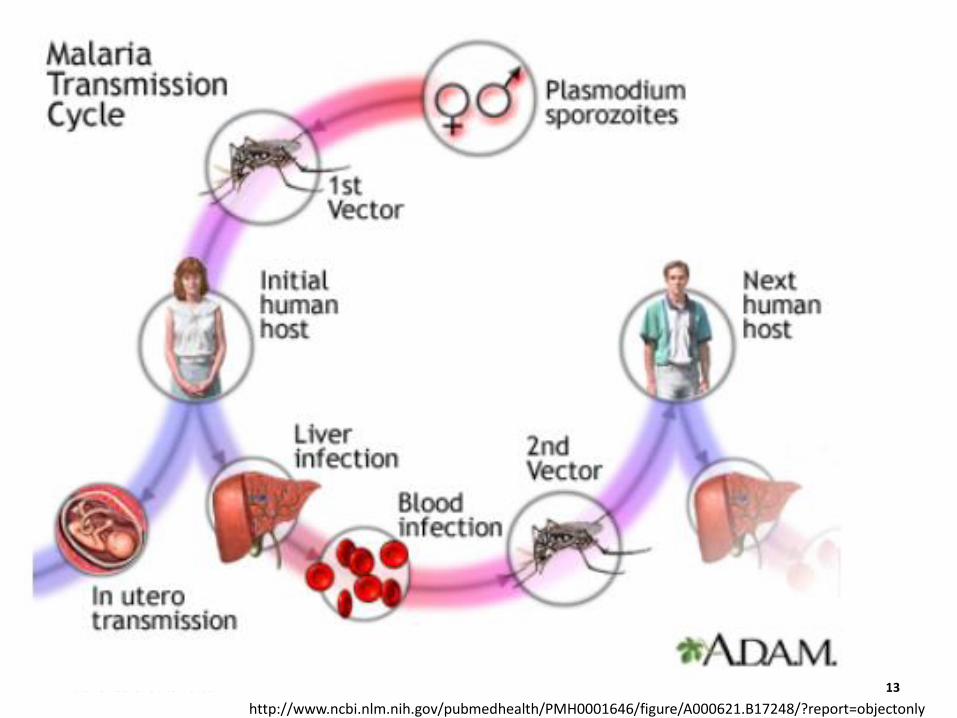
http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0001646/figure/A000621.B17248/?report=objectonly
Malaria
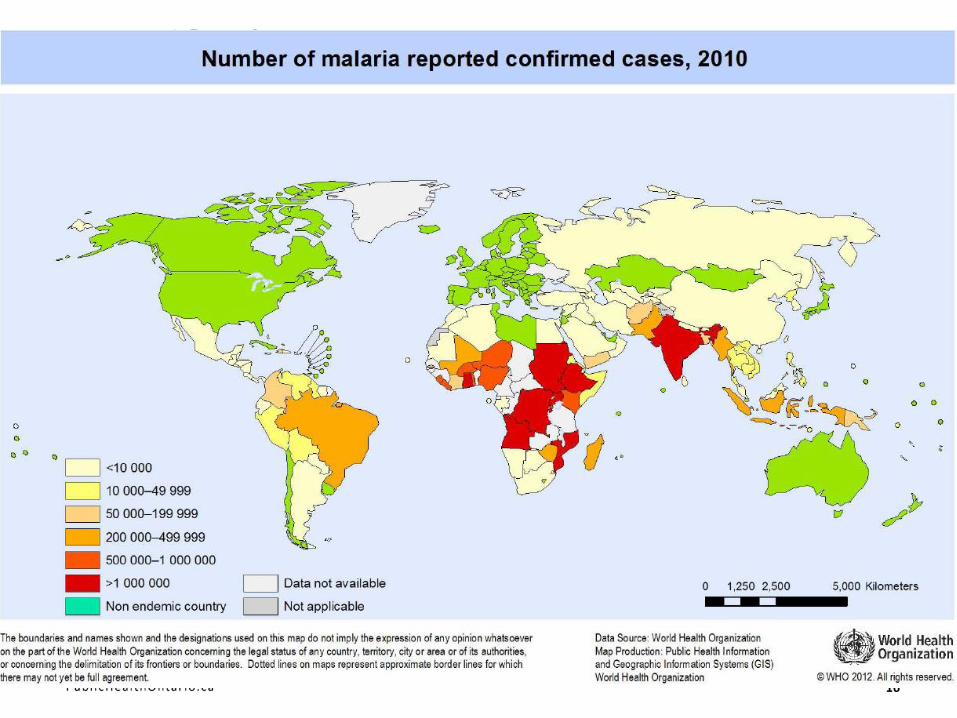
• In 2010, malaria caused about 219 million cases (with an uncertainty range of 154-289 million) and an estimated 660 000 deaths (with an uncertainty range of 610 000 to 971 000), mostly among African children.
• Malaria mortality rates have fallen by more than 25% globally since 2000, and by 33% in the WHO African Region.
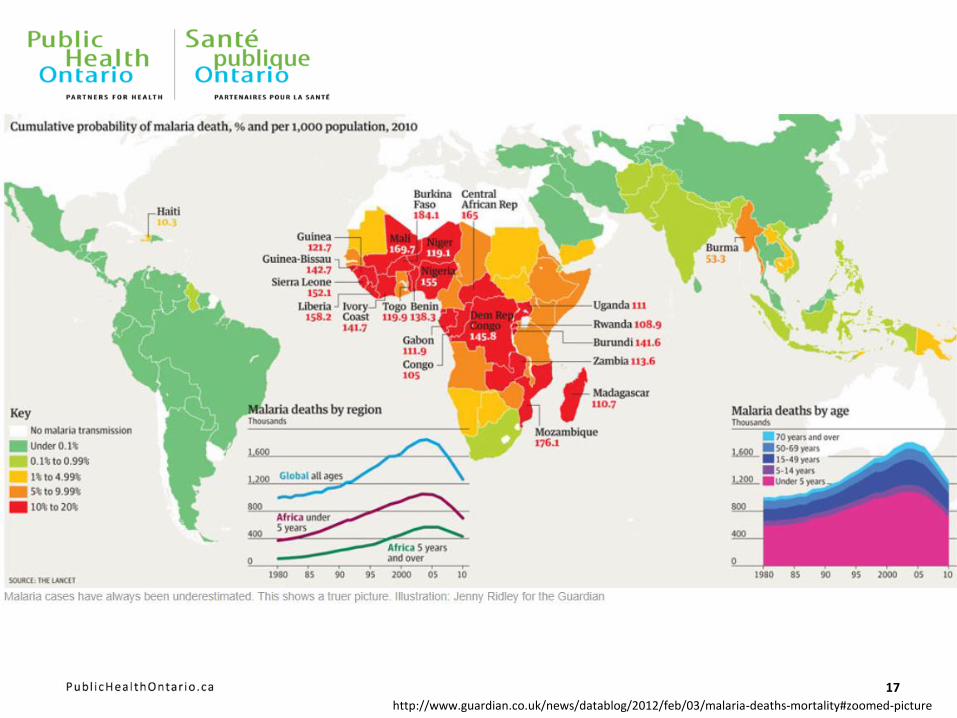
• The Democratic Republic of the Congo and Nigeria account for over 40% of the estimated total of malaria deaths globally
• There are four parasite species that cause malaria in humans: Plasmodium falciparum, P. vivax, P. malariae, P. ovale • P. falciparum and P. vivax are the most common
• P. falciparum is the most deadly.
14
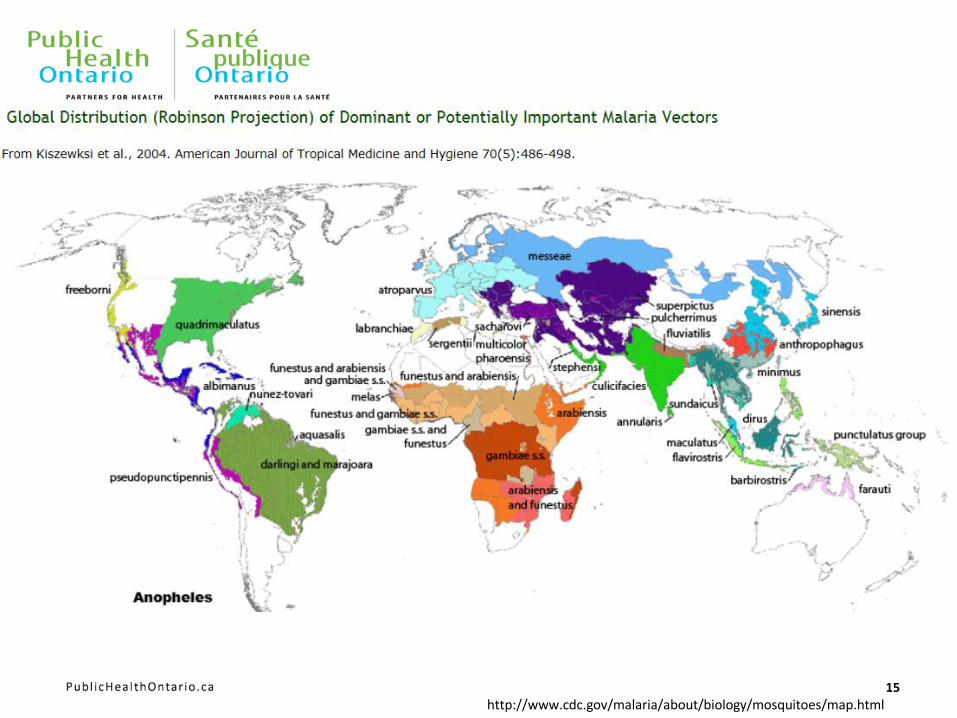
15 http://www.cdc.gov/malaria/about/biology/mosquitoes/map.html
16
17
http://www.guardian.co.uk/news/datablog/2012/feb/03/malaria-deaths-mortality#zoomed-picture
Symptoms
• Can take from one week to several months to occur (depending on the type of malaria parasite).
• Are often flu-like, including: fever, sweats, chills, headache, abdominal pain, muscle and joint pain, nausea and vomiting, diarrhea and feeling generally unwell.
• In more severe cases may include seizures, coma, kidney and respiratory failure, and shock which may lead to death.
Treatment
• Specific treatment options depend on the species of malaria, the likelihood of drug resistance (based on where the infection was acquired), the age of the patient, pregnancy status, and the severity of infection.
18
19
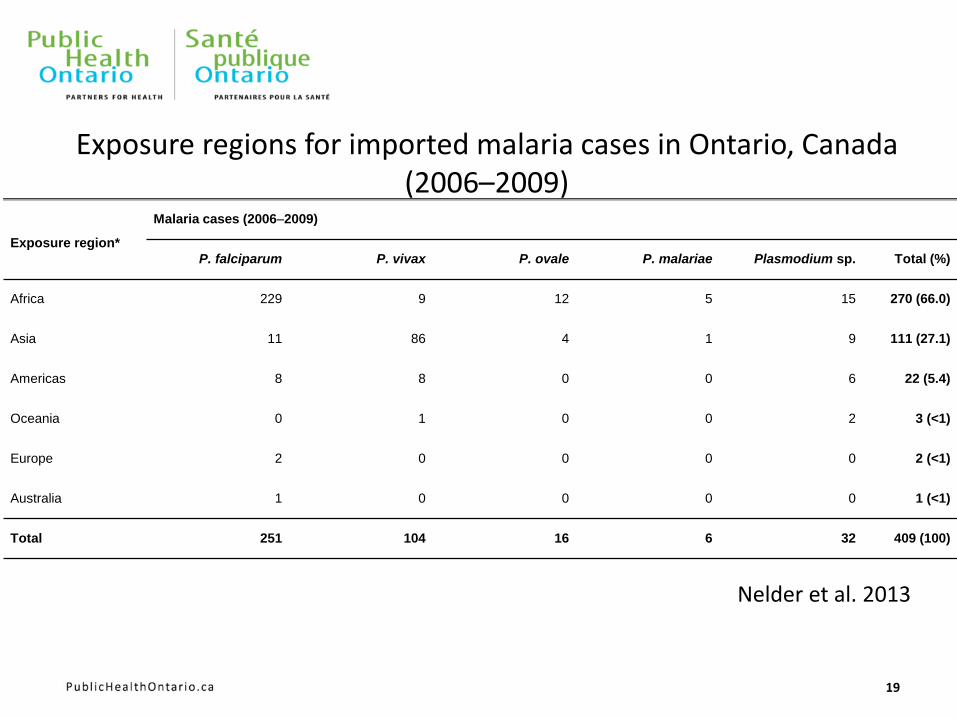
Exposure region*
Malaria cases (2006–2009)
P. falciparum P. vivax P. ovale P. malariae Plasmodium sp. Total (%)
Africa 229 9 12 5 15 270 (66.0)
Asia 11 86 4 1 9 111 (27.1)
Americas 8 8 0 0 6 22 (5.4)
Oceania 0 1 0 0 2 3 (<1)
Europe 2 0 0 0 0 2 (<1)
Australia 1 0 0 0 0 1 (<1)
Total 251 104 16 6 32 409 (100)
Exposure regions for imported malaria cases in Ontario, Canada (2006–2009)
Nelder et al. 2013
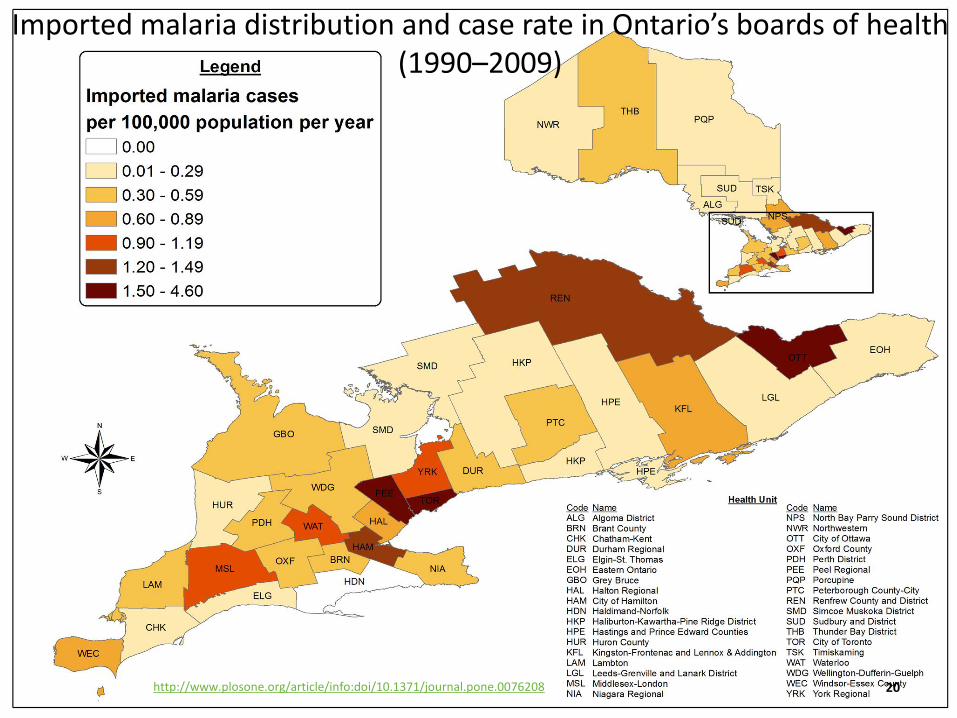
20
Imported malaria distribution and case rate in Ontario’s boards of health (1990–2009)
http://www.plosone.org/article/info:doi/10.1371/journal.pone.0076208
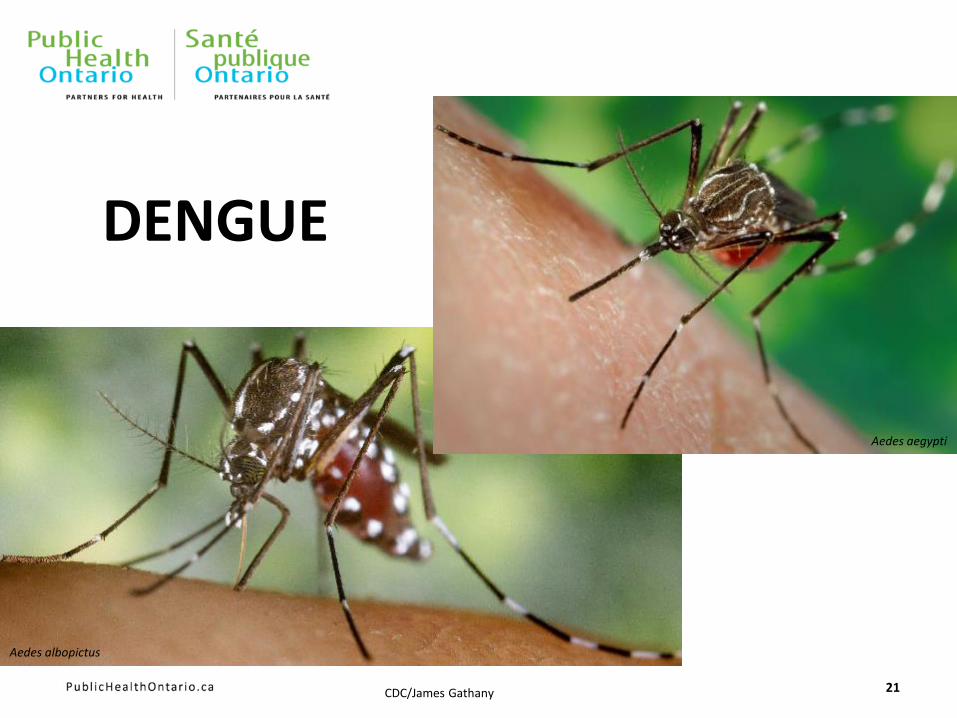
DENGUE
21 CDC/James Gathany
Aedes aegypti
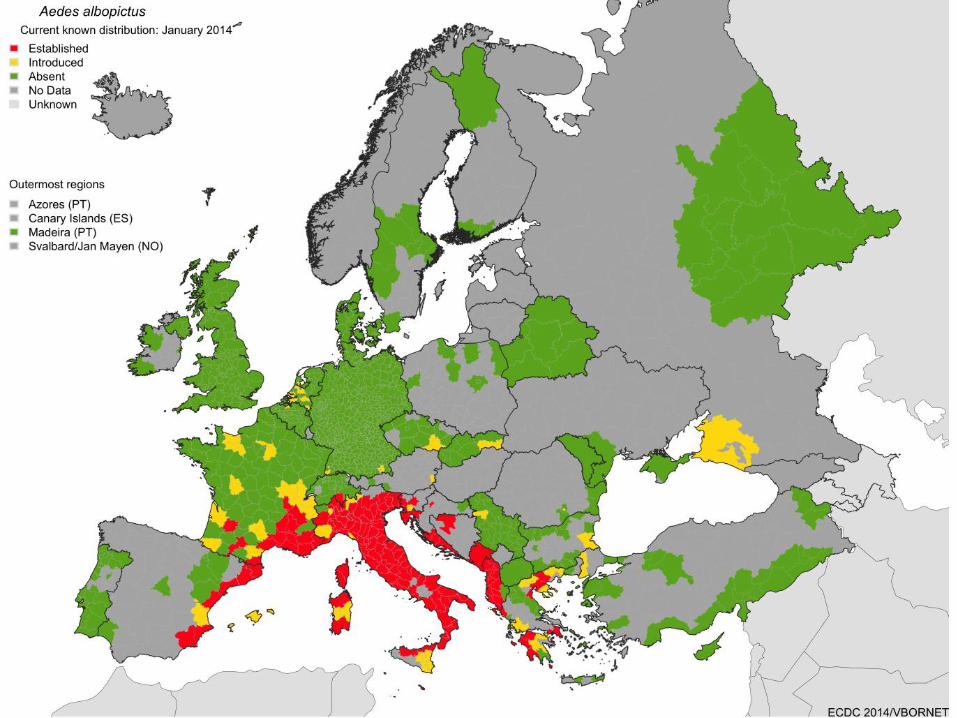
Aedes albopictus
22
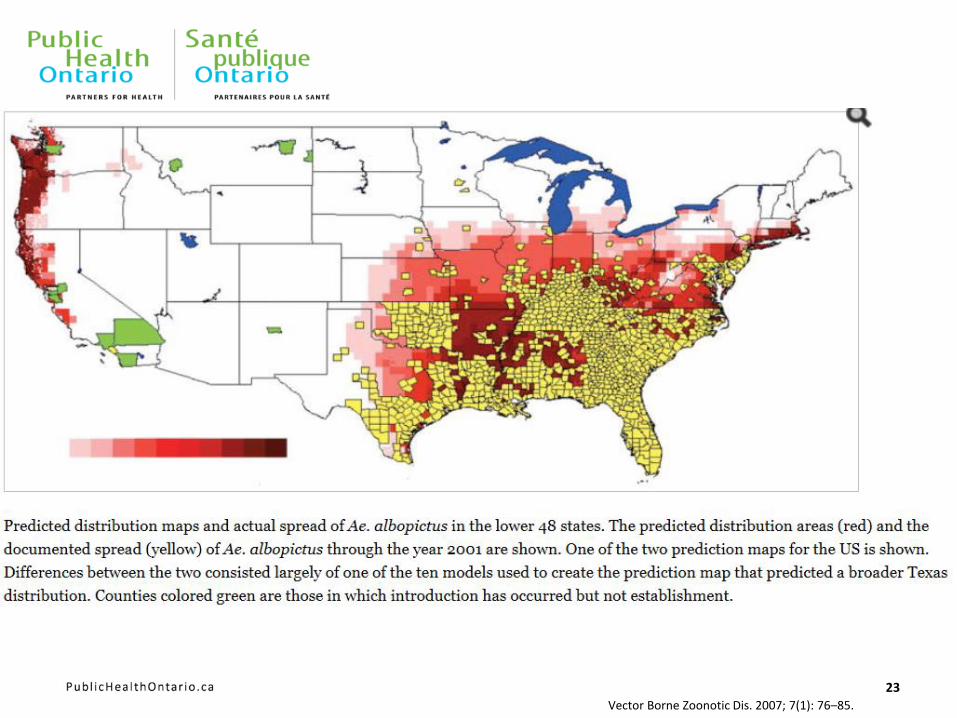
23
Vector Borne Zoonotic Dis. 2007; 7(1): 76–85.
Dengue
• Flavivuris: similar to Yellow Fever, WNV, St. Louis Encephalitis
• 40% of world’s population at risk of dengue with ~50-100 million infection every year
• Four different serotypes with lifelong immunity after recovery
• Subsequent infection with another serotype increases the risk of severe dengue (i.e. dengue hemorrhagic fever)
• DHF is the leading cause of hospitalization and death in Asian and Latin American children
24
http://www.who.int/mediacentre/factsheets/fs117/en/index.html
Symptoms
• Severe headache
• Pain behind the eyes
• Nausea, Vomiting
• Swollen glands
• Muscle and joint pains
• Rash
Severe Dengue
• Persistent vomiting
• Rapid breathing
• Bleeding gums
• Blood in vomit
• Fatigue, restlessness
• The next 24-48 hours of the critical stage can be lethal; proper medical care is needed to avoid complications and risk of death.
25
http://www.who.int/denguecontrol/human/en/index.htm
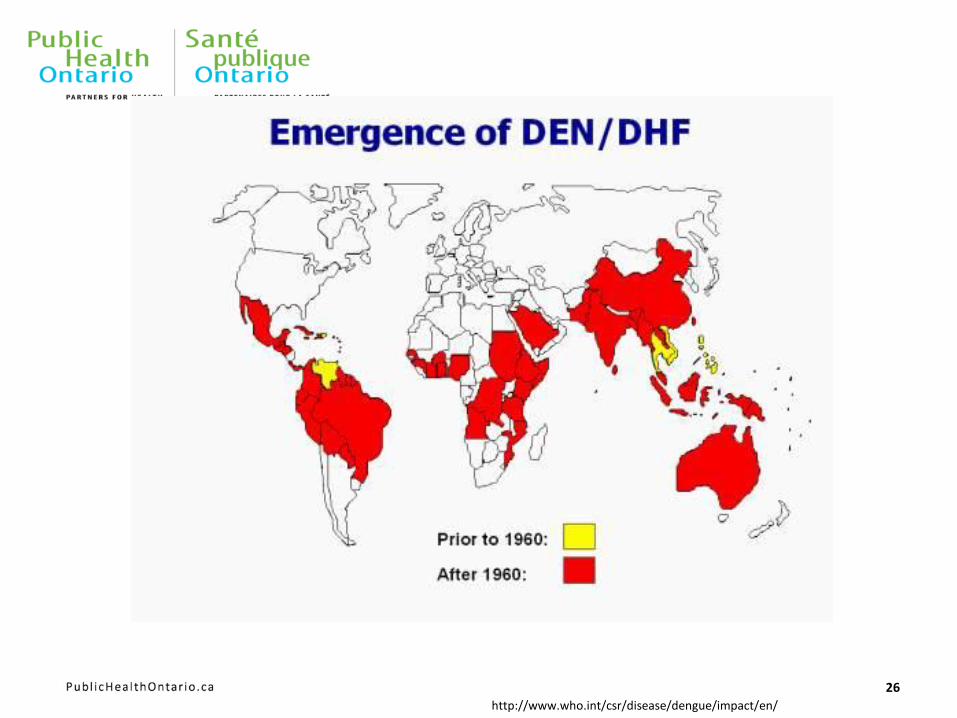
26
http://www.who.int/csr/disease/dengue/impact/en/
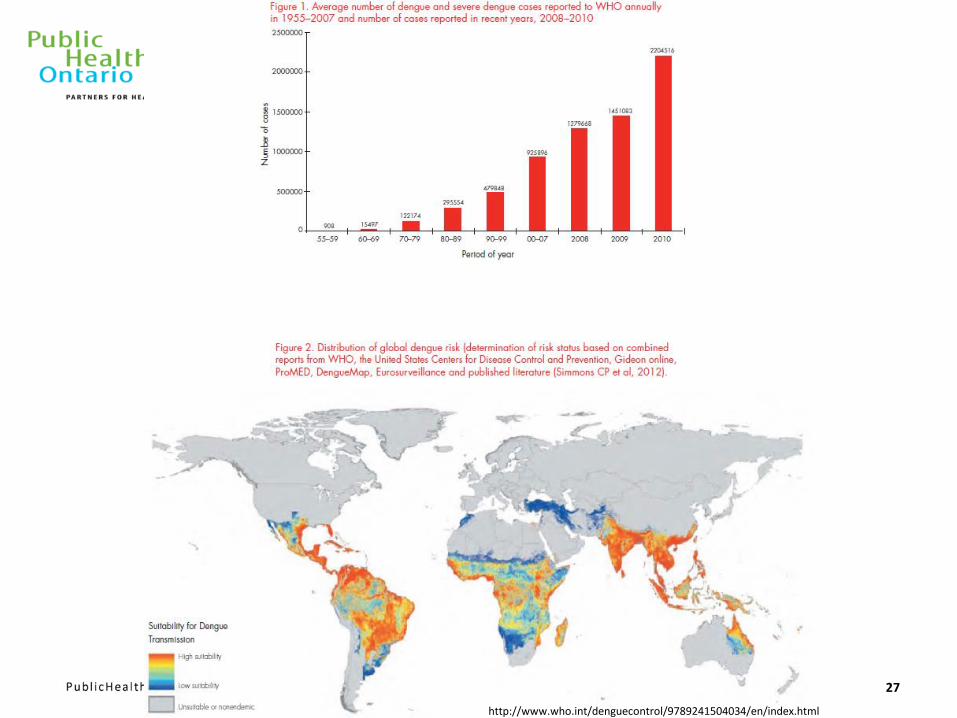
27
http://www.who.int/denguecontrol/9789241504034/en/index.html
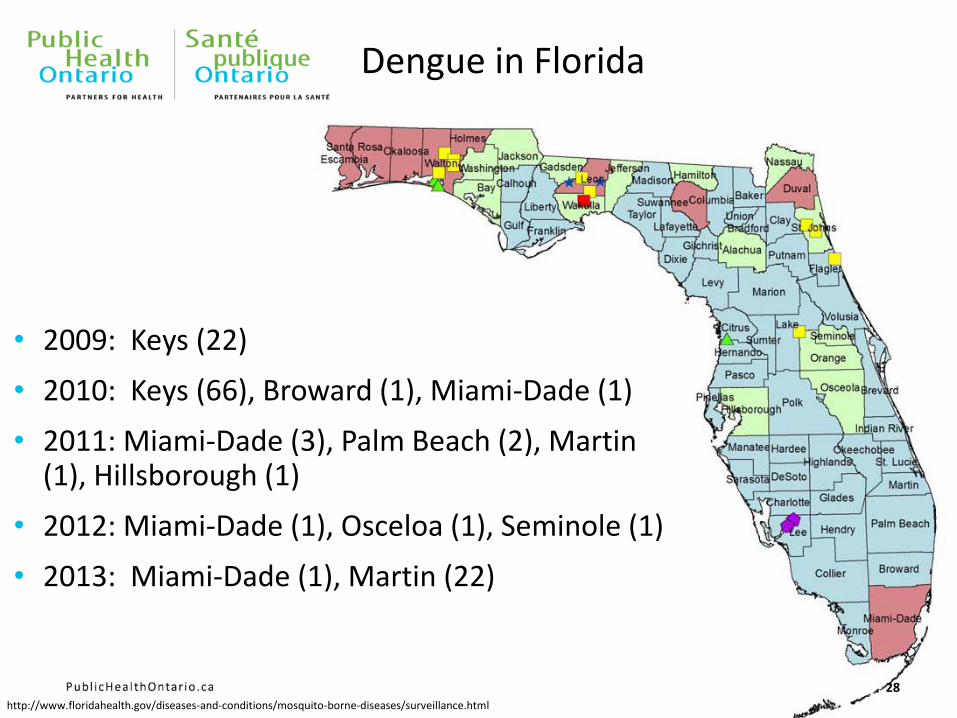
Dengue in Florida
28
• 2009: Keys (22)
• 2010: Keys (66), Broward (1), Miami-Dade (1)
• 2011: Miami-Dade (3), Palm Beach (2), Martin (1), Hillsborough (1)
• 2012: Miami-Dade (1), Osceloa (1), Seminole (1)
• 2013: Miami-Dade (1), Martin (22)
http://www.floridahealth.gov/diseases-and-conditions/mosquito-borne-diseases/surveillance.html
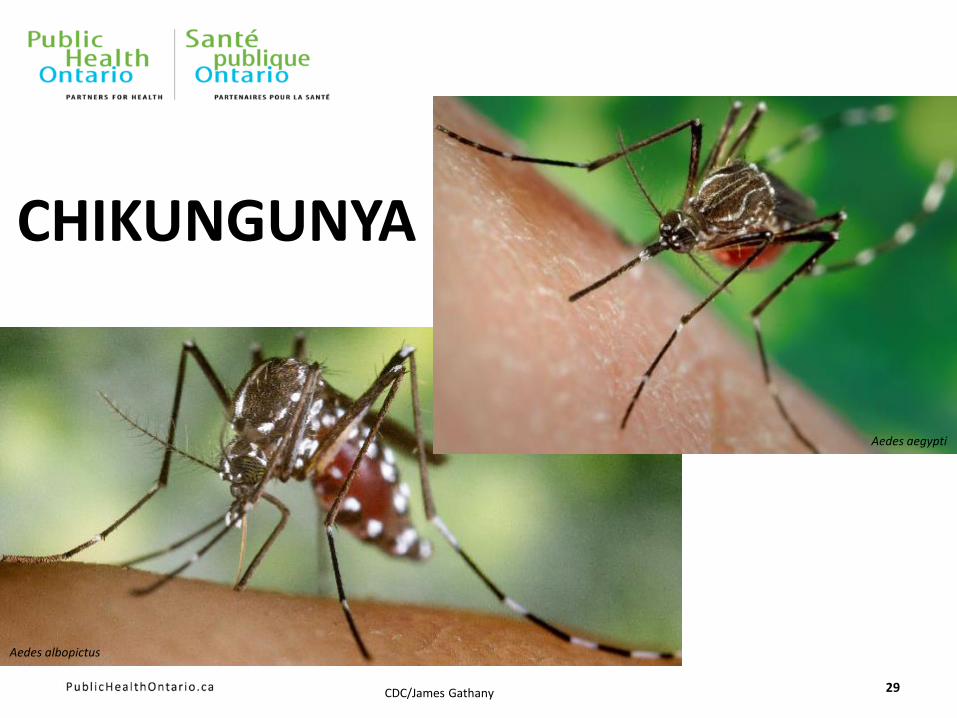
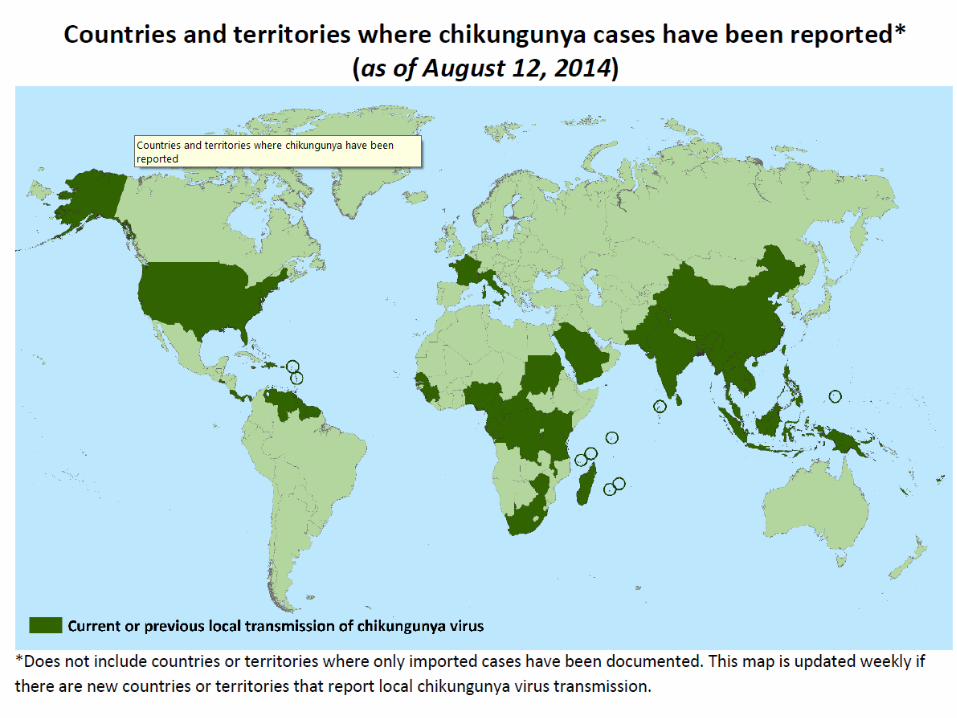
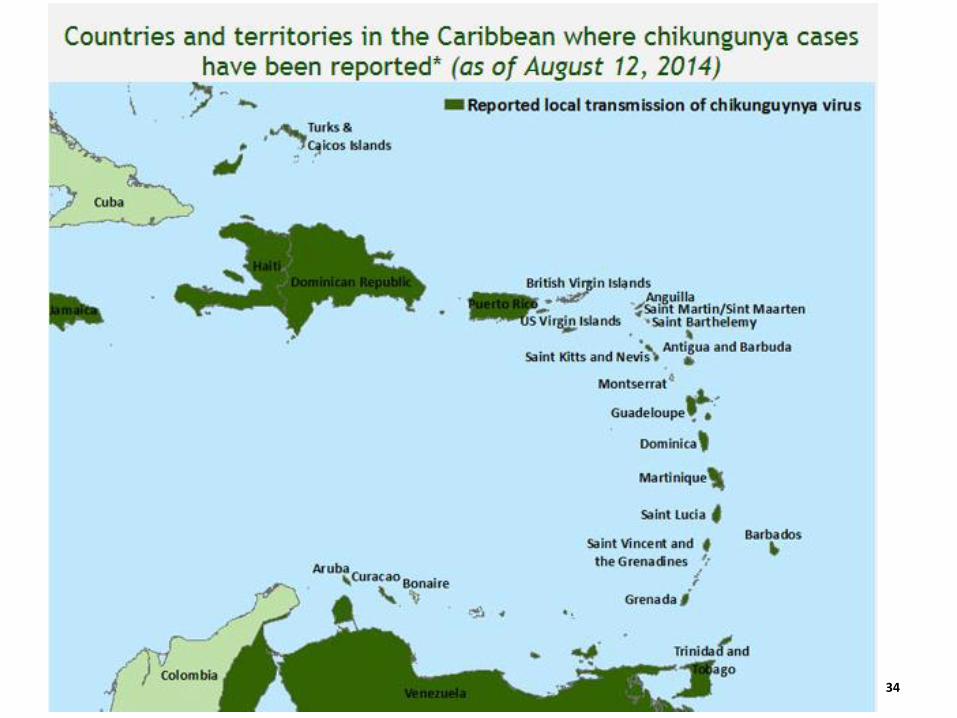
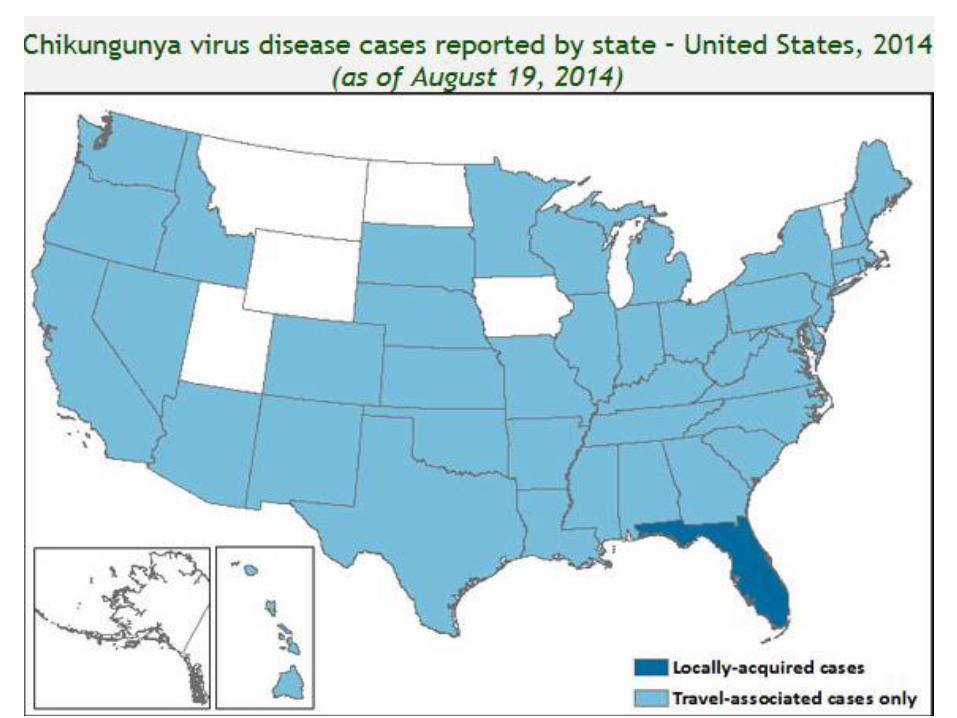
CHIKUNGUNYA
29 CDC/James Gathany
Aedes aegypti
Aedes albopictus
Chikungunya
• Alphavirus from the Togaviridae family
• Transmitted by Aedes mosquitoes to vertebrates.
• The word ‘chikungunya’ comes from the Makonde dialect in Tanzania, and means 'which bends up', related to the posture of the suffering patients
30
Symptoms • Fever
• Joint pain
• Headache
• Muscle pain
• Rash
• Joint swelling
Treatment
• Supportive care
• Pain releavers-
31
http://www.cdc.gov/chikungunya/symptoms/index.html
32
33
34
35
WEST NILE VIRUS
36

37
www.cdc.gov
www.haliburton.ca
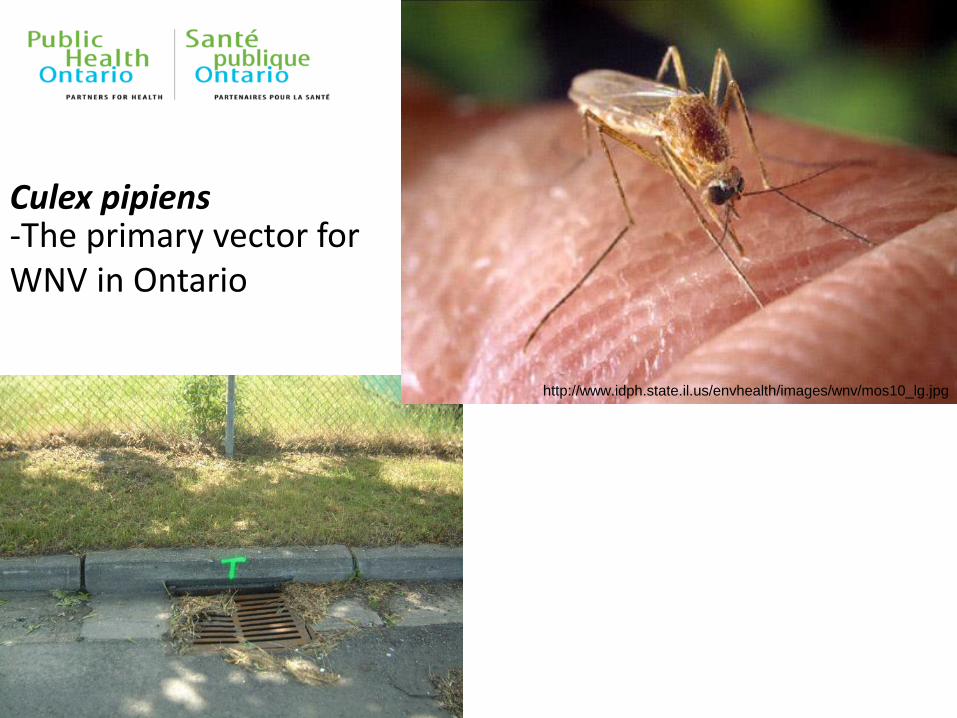
Culex pipiens -The primary vector for WNV in Ontario
http://www.idph.state.il.us/envhealth/images/wnv/mos10_lg.jpg
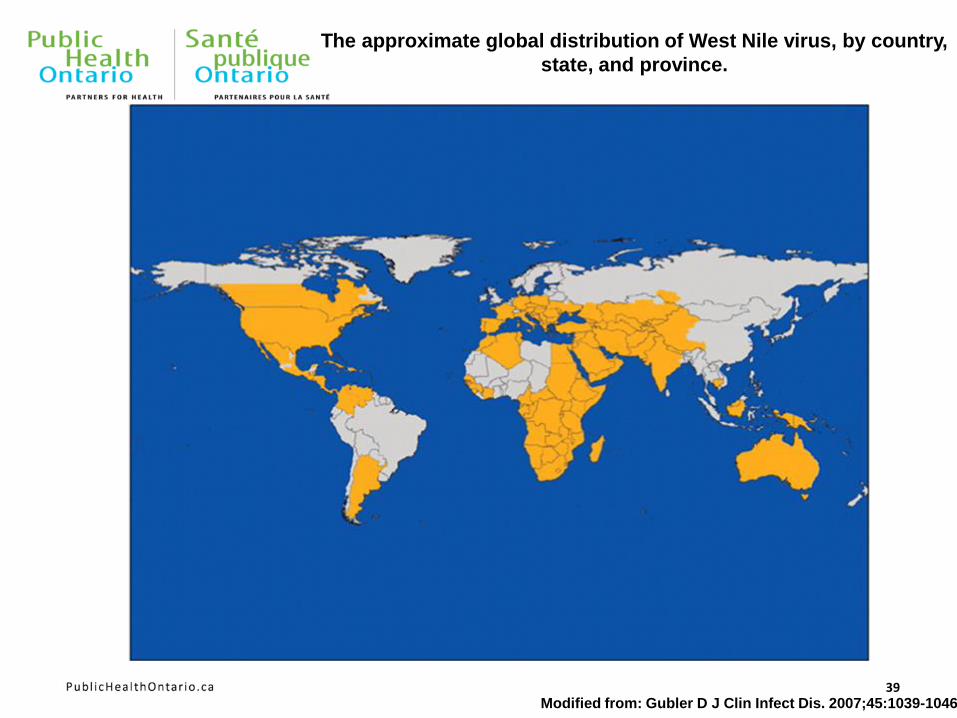
39 Modified from: Gubler D J Clin Infect Dis. 2007;45:1039-1046
The approximate global distribution of West Nile virus, by country,
state, and province.
Culex pipiens

CDC Miniature Light Trap
• Attracts host-seeking mosquitoes
• Uses light and CO2 (Dry Ice) as bait
• Mosquitoes are sucked into the trap via a fan
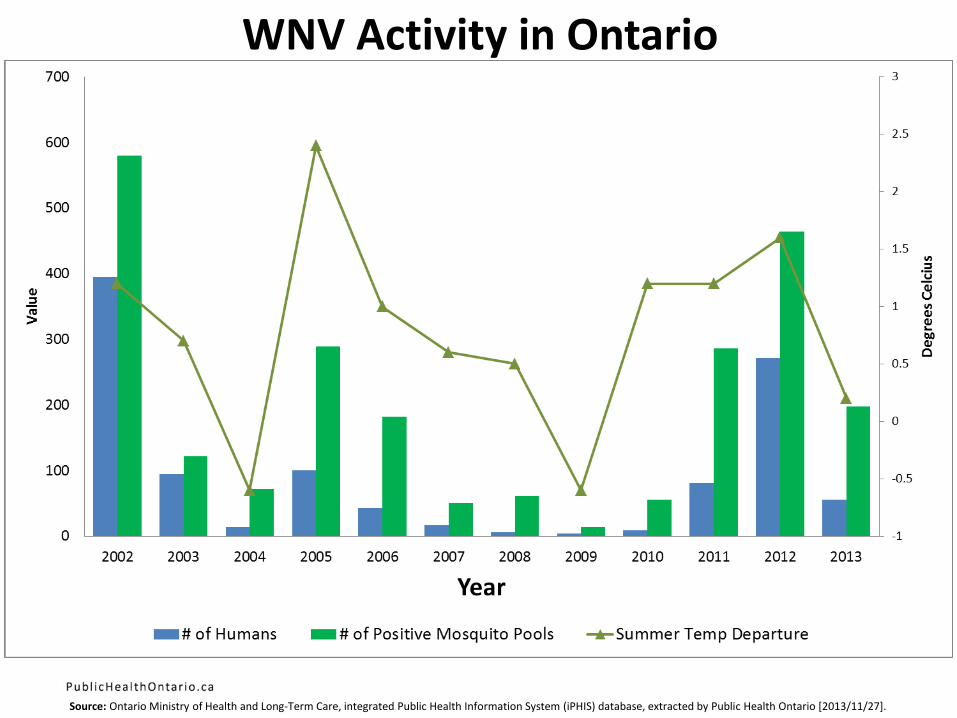
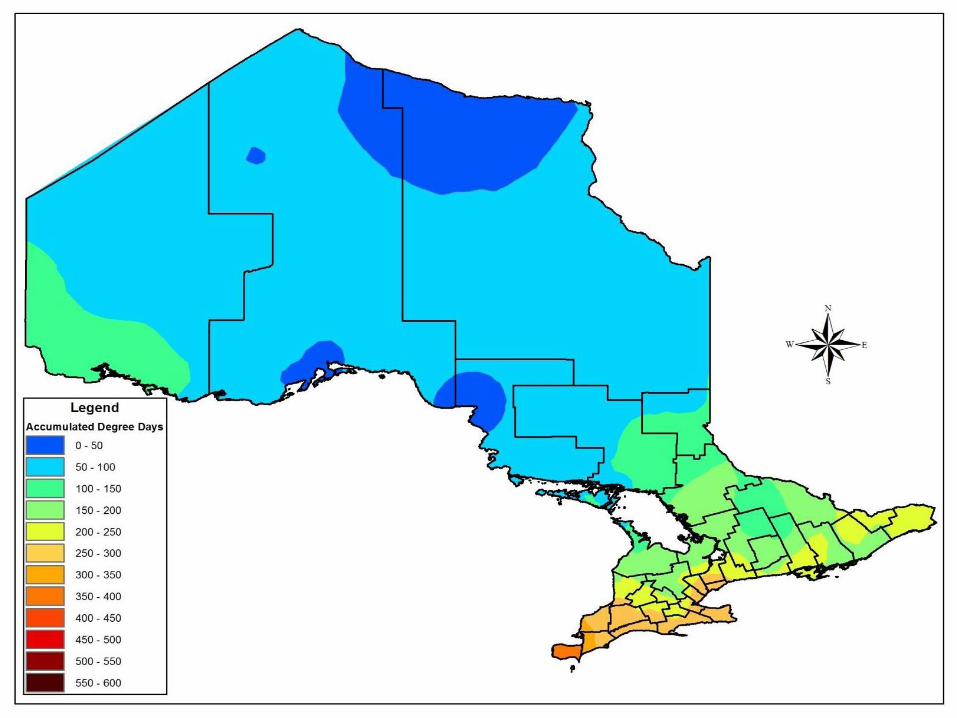
WNV Activity in Ontario
Source: Ontario Ministry of Health and Long-Term Care, integrated Public Health Information System (iPHIS) database, extracted by Public Health Ontario [2013/11/27].
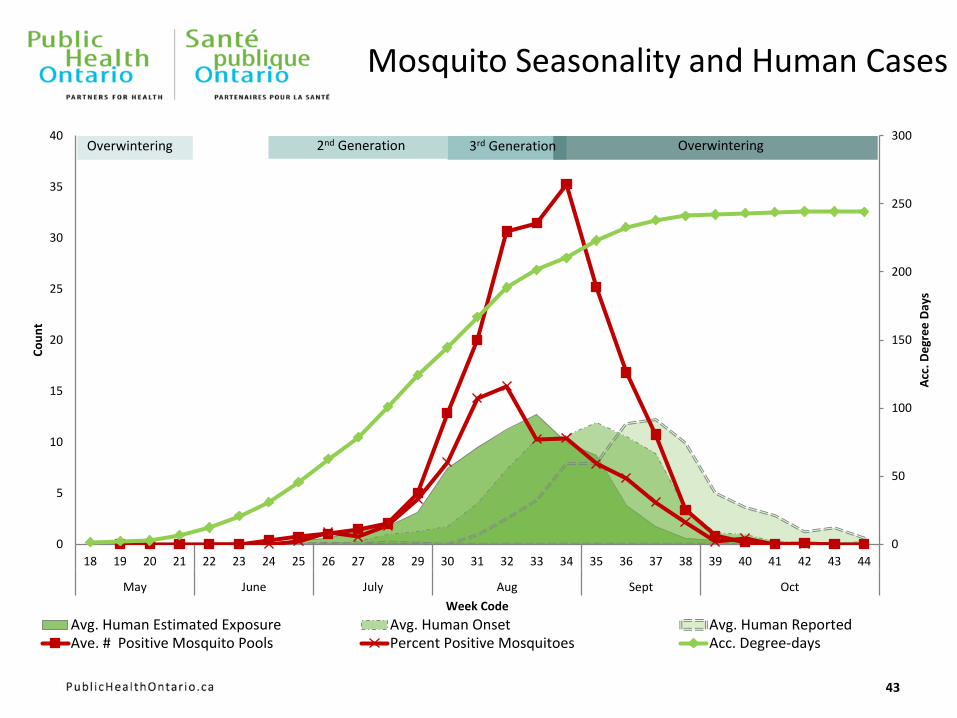
Mosquito Seasonality and Human Cases
43
0
50
100
150
200
250
300
0
5
10
15
20
25
30
35
40
18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44
May June July Aug Sept Oct
Acc
. De
gre
e D
ays
Co
un
t
Week Code
Avg. Human Estimated Exposure Avg. Human Onset Avg. Human ReportedAve. # Positive Mosquito Pools Percent Positive Mosquitoes Acc. Degree-days
Overwintering Overwintering 2nd Generation 3rd Generation
Source: Ontario Ministry of Health and Long-Term Care, integrated Public Health Information System (iPHIS) database, extracted by Public Health Ontario [2012/10/09].
45
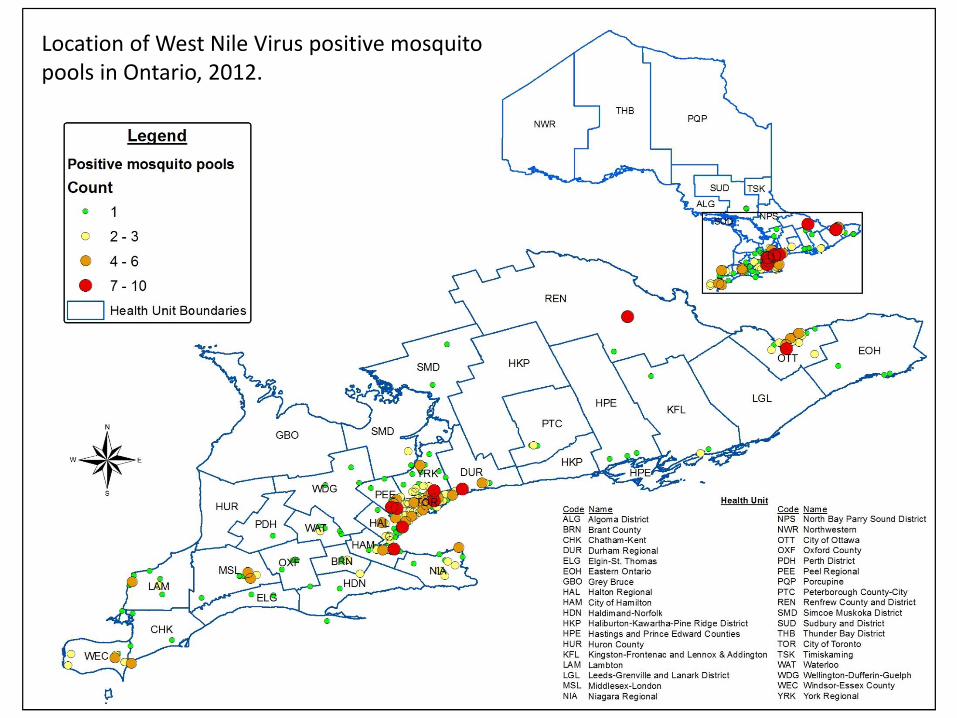
Location of West Nile Virus positive mosquito pools in Ontario, 2012.
Clinical Manifestations of WNV Non-Neurological Syndrome • Abrupt onset of fever
• Headache
• Sudden sensitivity to light
• Myalgia
• Weakness
• Abdominal pain
• Maculopapular rash (often transient)

Gorsche, R. et al. CMAJ 2005;172:1440
Outcome of WNV Non-Neurological Syndrome • Acute phase of illness lasts several days
• Fatigue and weakness can last for weeks
Clinical Manifestations of WNV Neurological Syndrome • Neck stiffness
• Headache typical of aseptic meningitis
• Mental status changes indicating encephalitis (i.e. confusion)
• Movement disorders (i.e. tremors, Parkinsonism)
• Seizures
• Acute flaccid paralysis
52
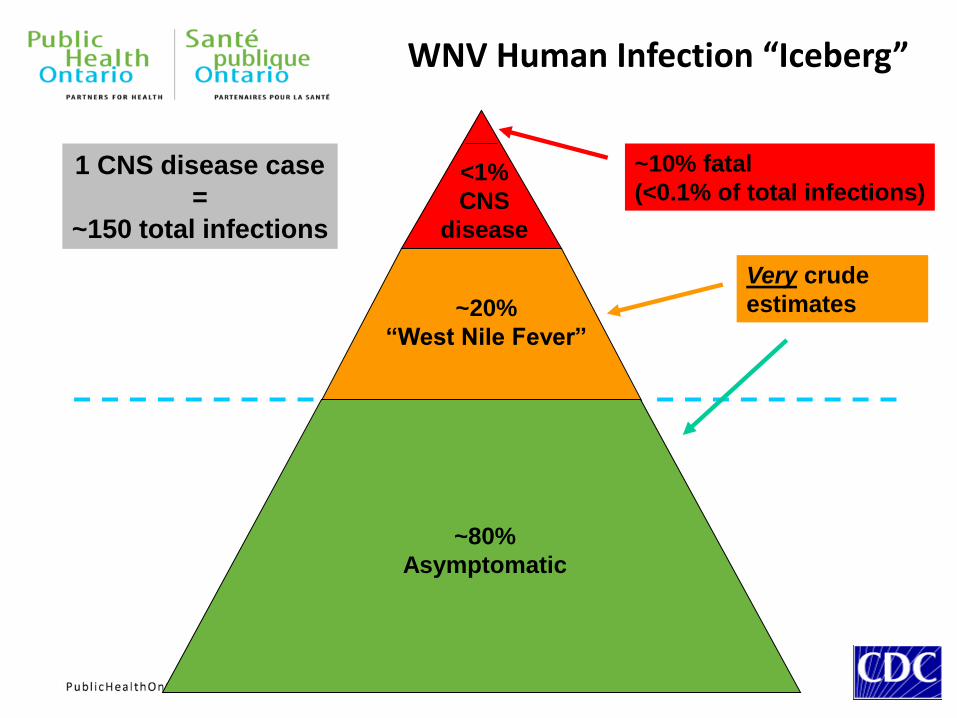
~80%
Asymptomatic
~20%
“West Nile Fever”
<1%
CNS
disease
~10% fatal
(<0.1% of total infections)
WNV Human Infection “Iceberg”
1 CNS disease case
=
~150 total infections
Very crude
estimates
Treatment of WNV • Treatment of WNV is supportive
• No specific therapy has been proven effective
• Control research trials with interferon, Immune Globulin with WNV-specific antibodies and RNA translation inhibitors is underway
EASTERN EQUINE ENCEPHALITIS
54
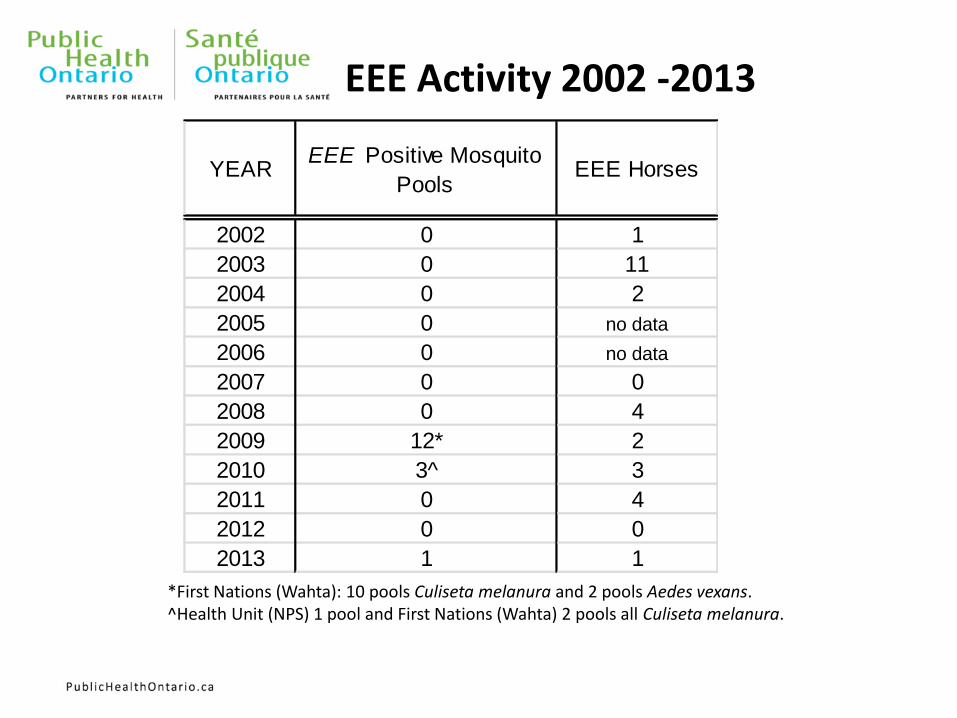
EEE Activity 2002 -2013
*First Nations (Wahta): 10 pools Culiseta melanura and 2 pools Aedes vexans. ^Health Unit (NPS) 1 pool and First Nations (Wahta) 2 pools all Culiseta melanura.
YEAREEE Positive Mosquito
PoolsEEE Horses
2002 0 1
2003 0 11
2004 0 2
2005 0 no data
2006 0 no data
2007 0 0
2008 0 4
2009 12* 2
2010 3^ 3
2011 0 4
2012 0 0
2013 1 1
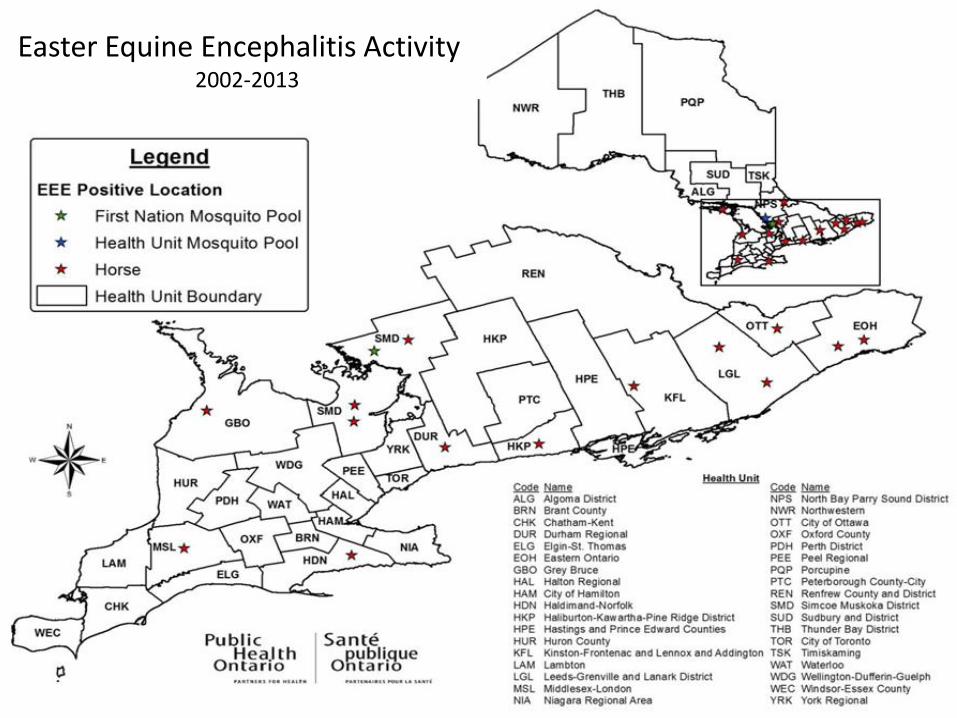
Easter Equine Encephalitis Activity 2002-2013
57
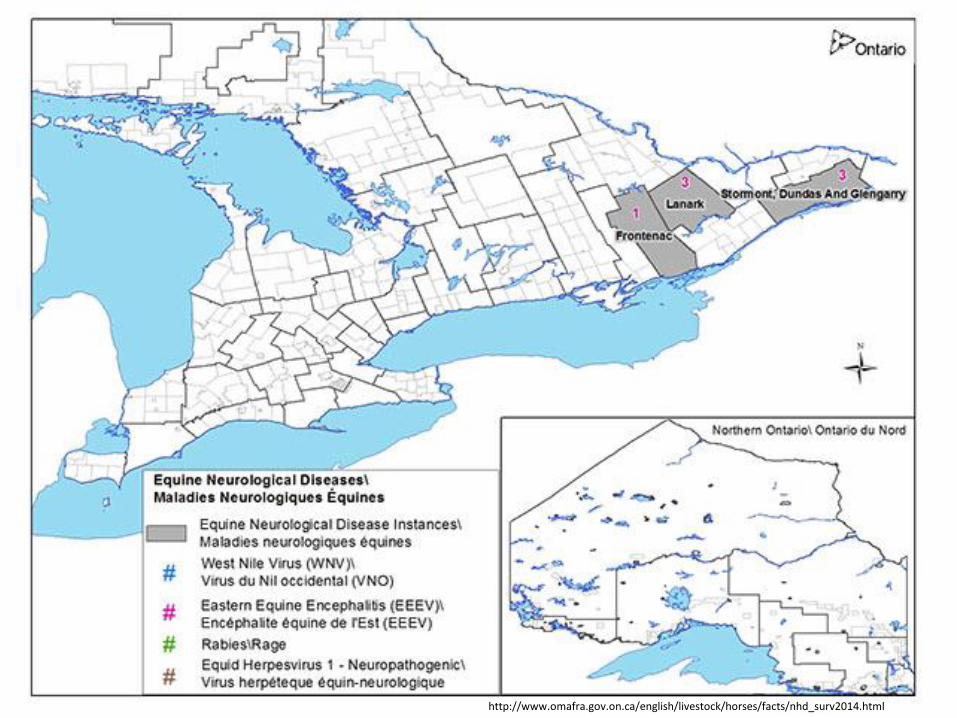
http://www.omafra.gov.on.ca/english/livestock/horses/facts/nhd_surv2014.html
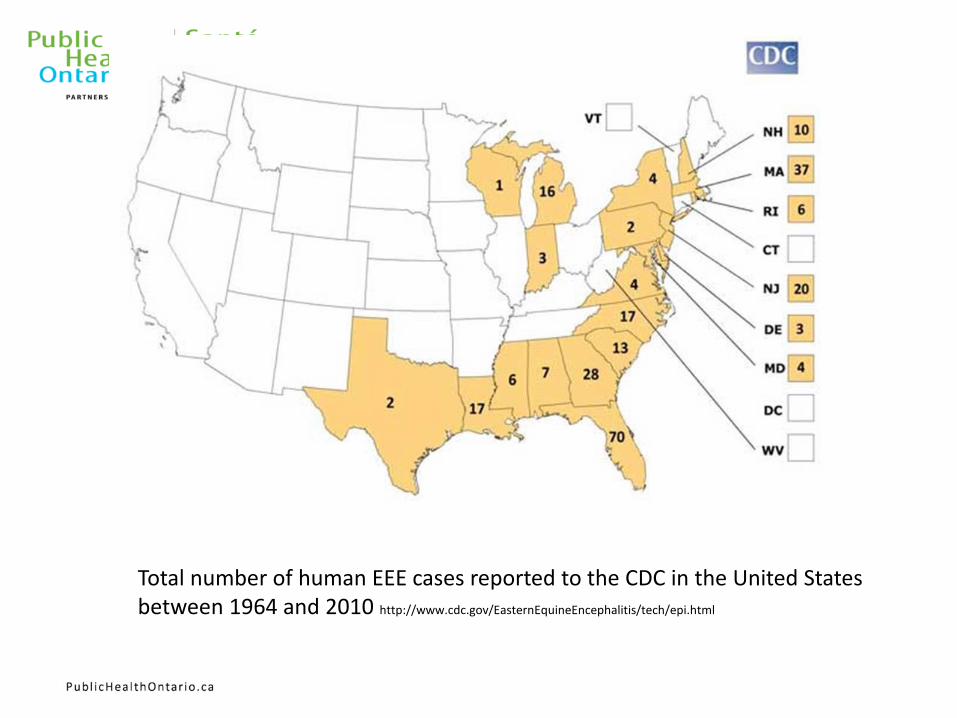
Total number of human EEE cases reported to the CDC in the United States between 1964 and 2010 http://www.cdc.gov/EasternEquineEncephalitis/tech/epi.html
59
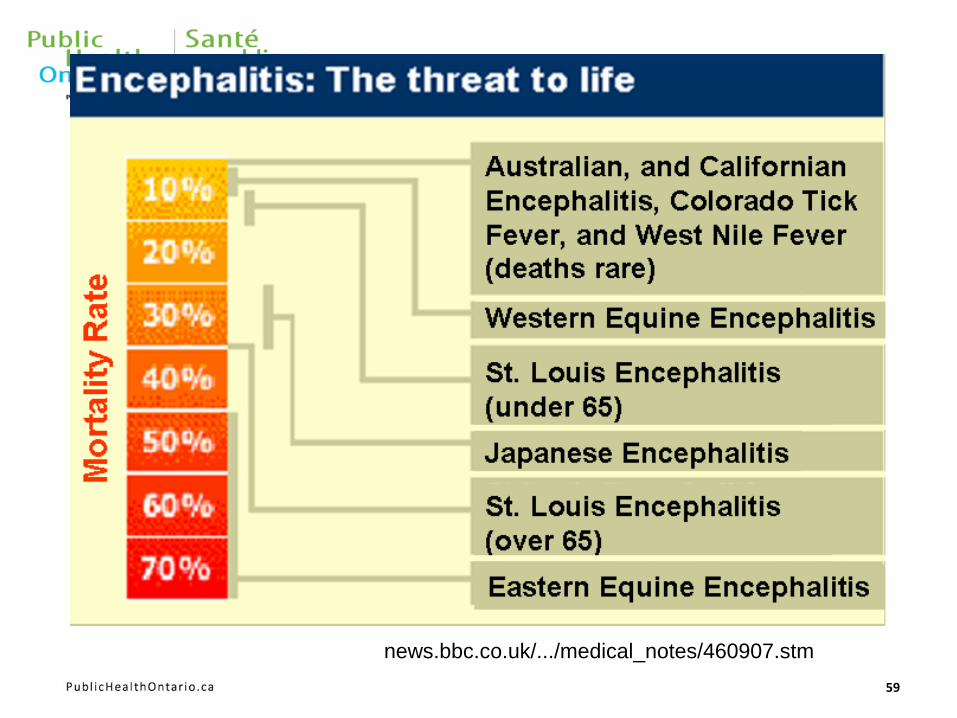
news.bbc.co.uk/.../medical_notes/460907.stm
Ticks & Lyme disease in Ontario
Curtis Russell Program Consultant
https://www.msu.edu/course/isb/202/ebertmay/images/Deertick%20Female.jpg
Lyme disease History
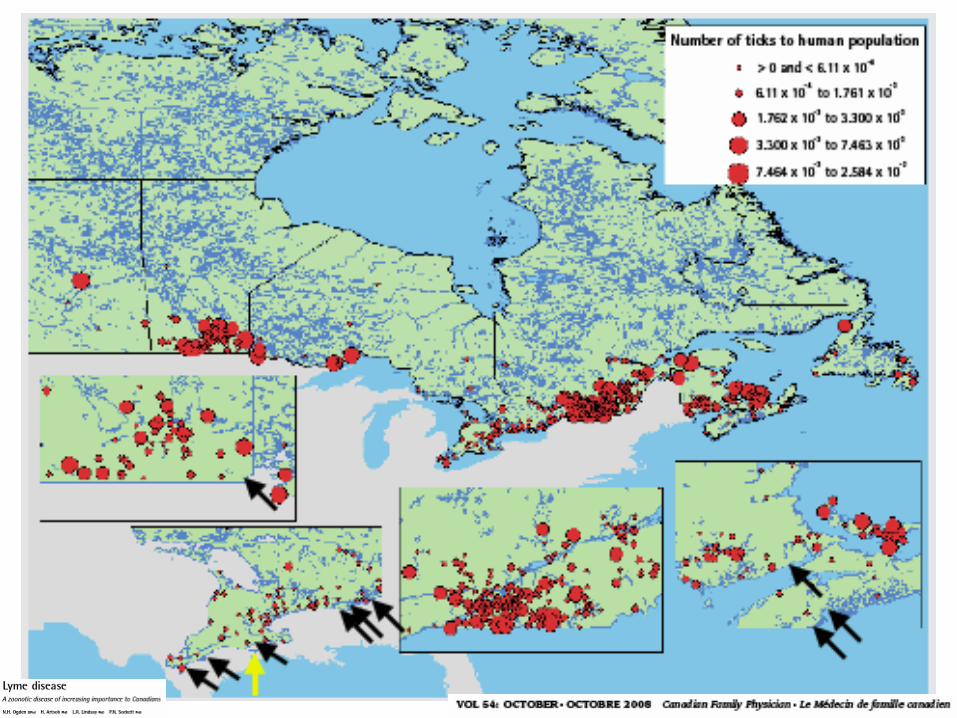
• In 1991 only one population of ticks that carry Lyme disease (LD) was known in Canada located in Ontario at Long Point Provincial Park.
• After that the following areas were identified:
• Turkey Point Provincial Park
• Rondeau Provincial Park
• Point Pelee National Park
• Prince Edward Point National Wildlife Area
• In 2006 the Ministry participated in tick surveillance studies with the Public Health Agency of Canada and discovered an new endemic area in St. Lawrence Islands National Park area
• The Ministry started to active tick surveillance in 2007.
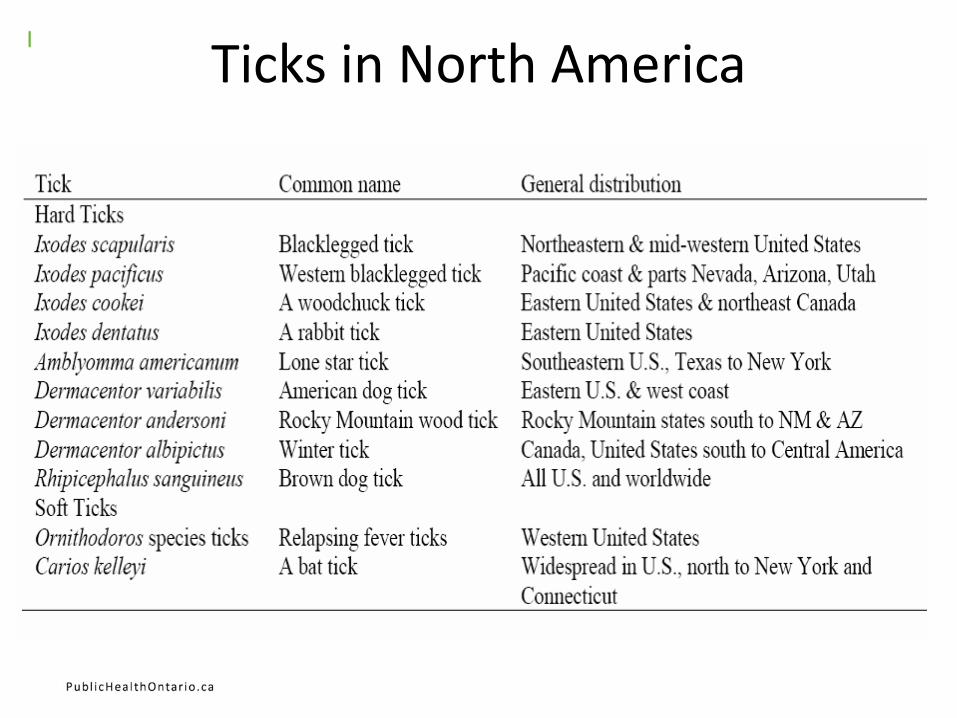
Ticks in North America
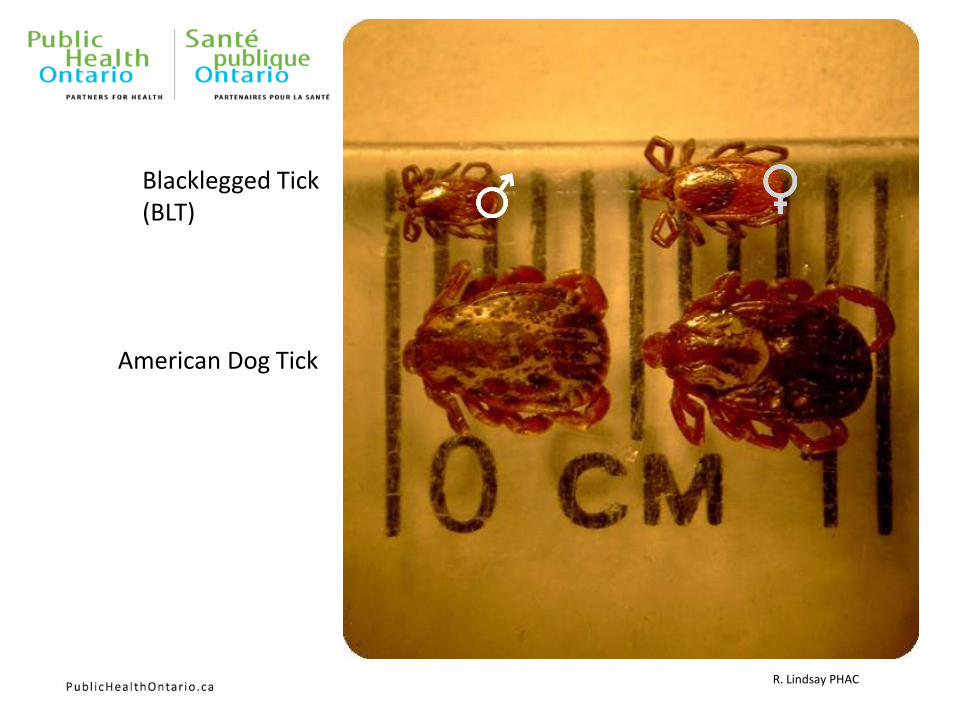
Blacklegged Tick (BLT)
American Dog Tick
R. Lindsay PHAC
0
200
400
600
800
1000
1200
Co
un
t
Month
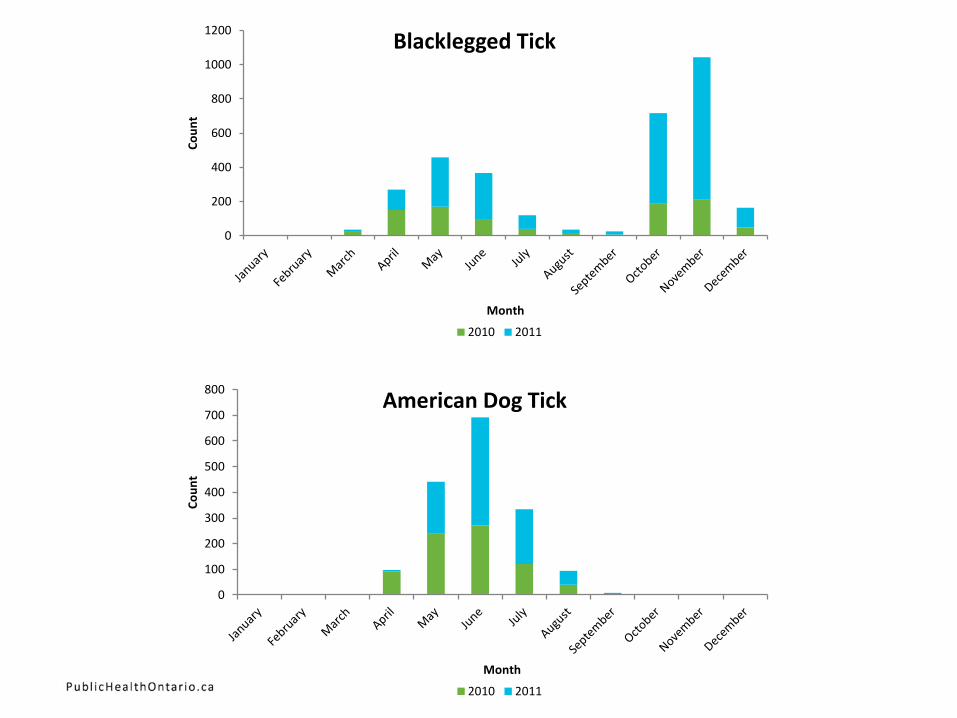
Blacklegged Tick
2010 2011
0
100
200
300
400
500
600
700
800
Co
un
t
Month
American Dog Tick
2010 2011
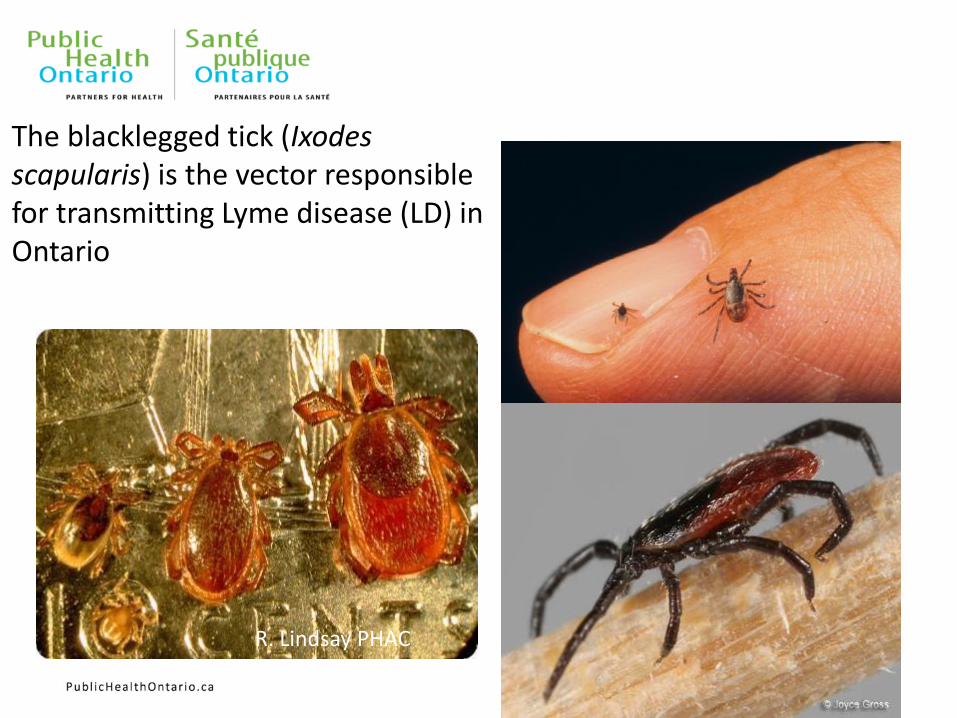
The blacklegged tick (Ixodes scapularis) is the vector responsible for transmitting Lyme disease (LD) in Ontario
R. Lindsay PHAC
66
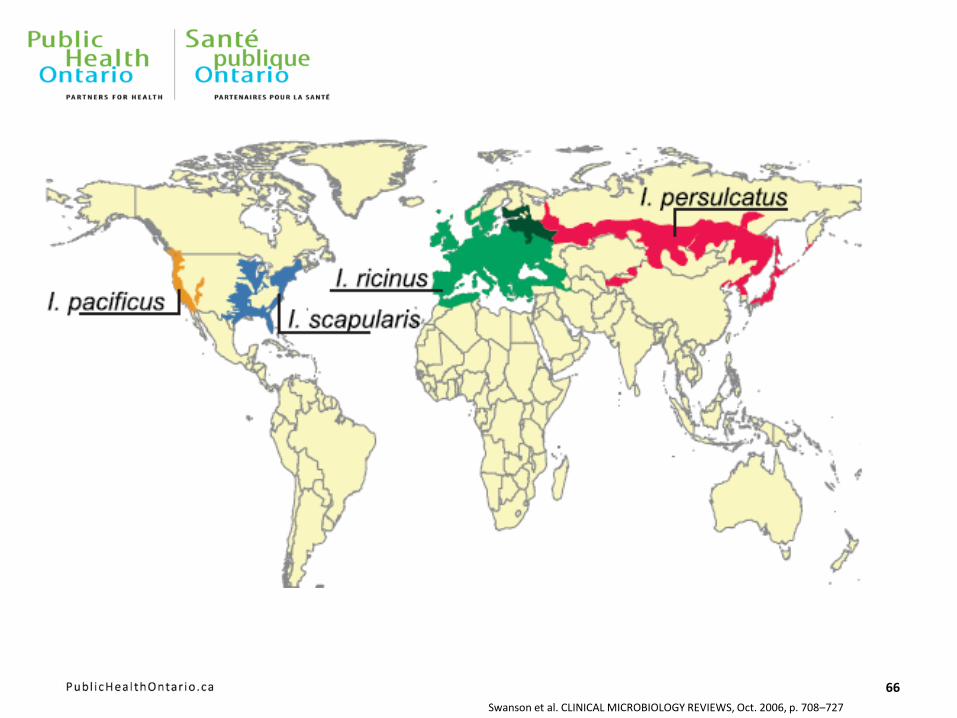
Swanson et al. CLINICAL MICROBIOLOGY REVIEWS, Oct. 2006, p. 708–727
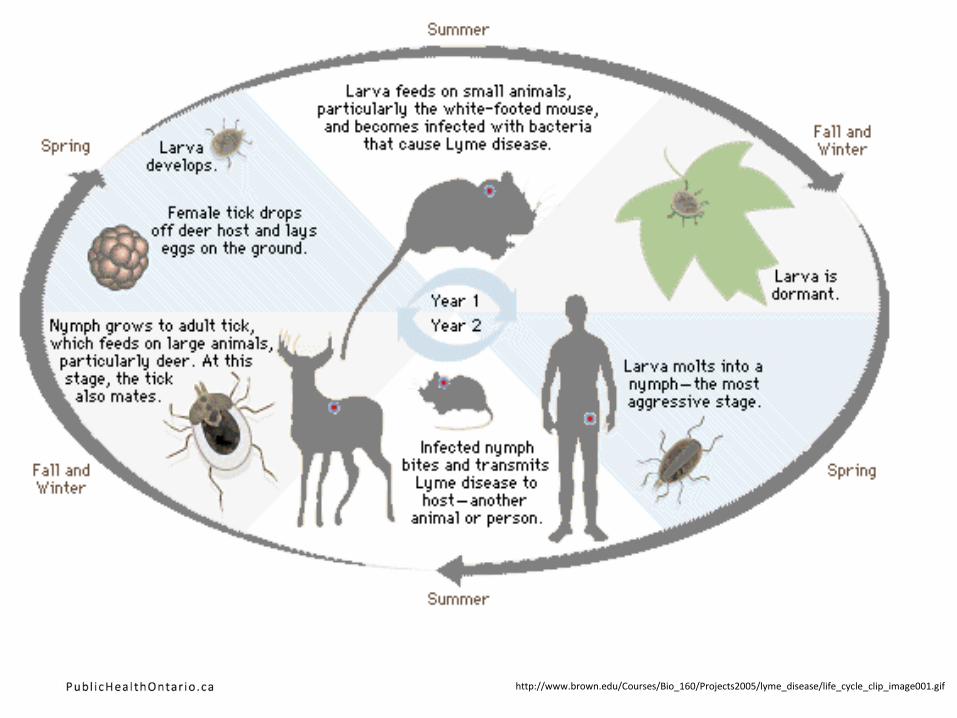
http://www.brown.edu/Courses/Bio_160/Projects2005/lyme_disease/life_cycle_clip_image001.gif
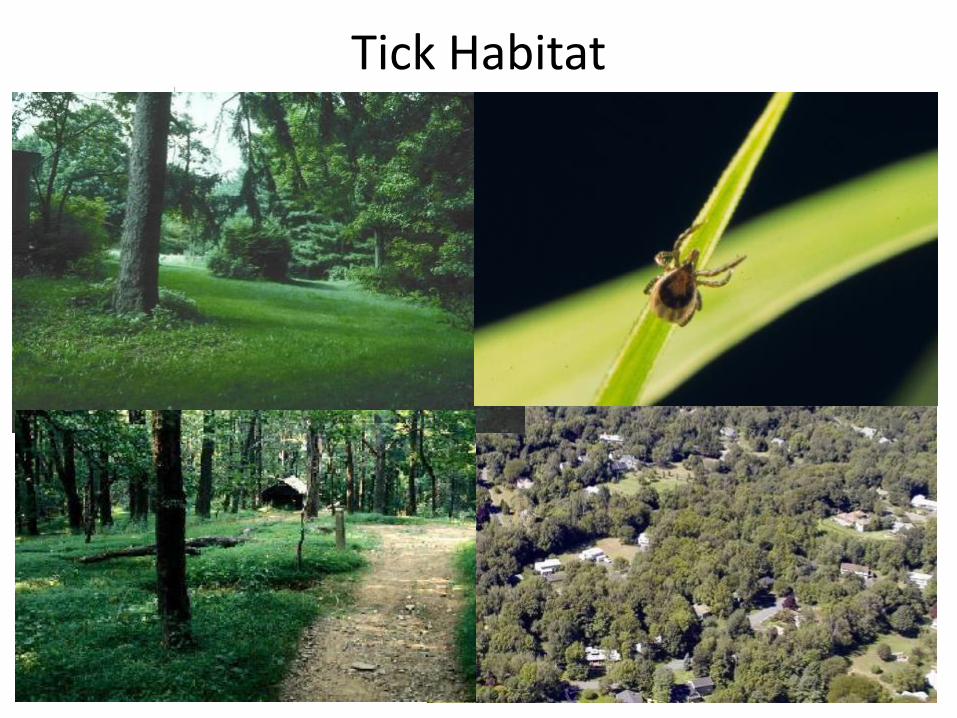
Tick Habitat
www.scienceclarified.com
www.zectect.de
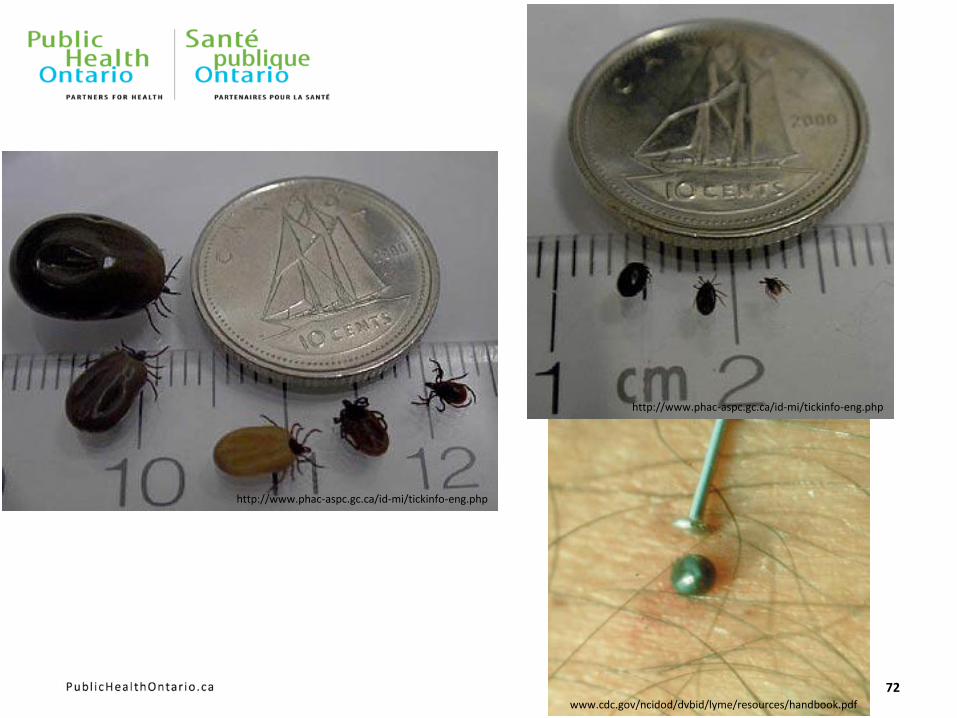
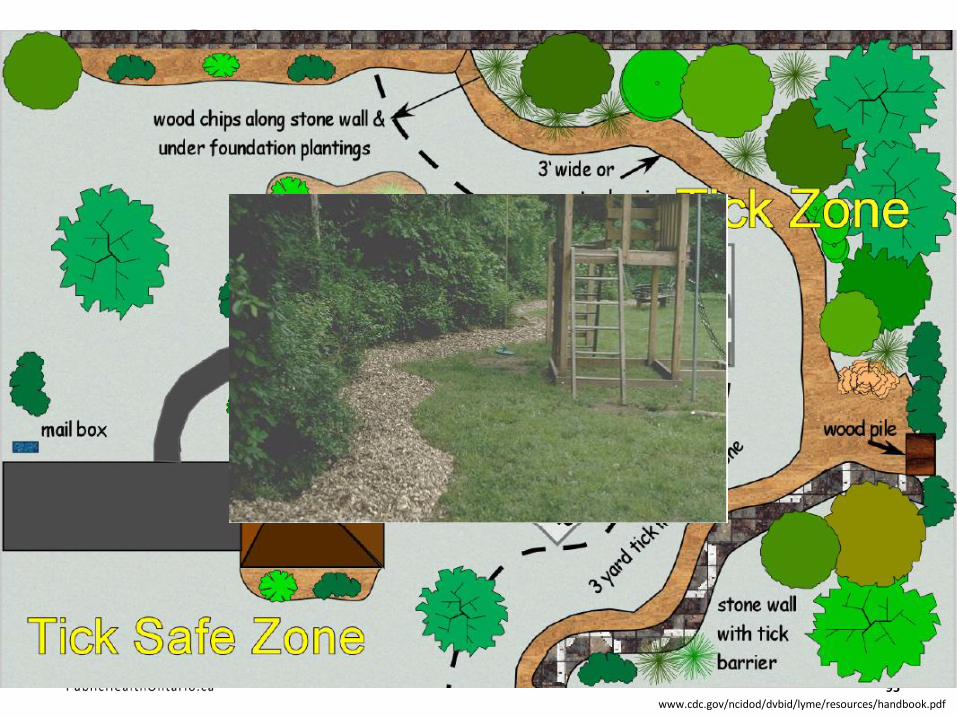
http://www.cdc.gov/ncidod/dvbid/lyme/resources/handbook.pdf
71
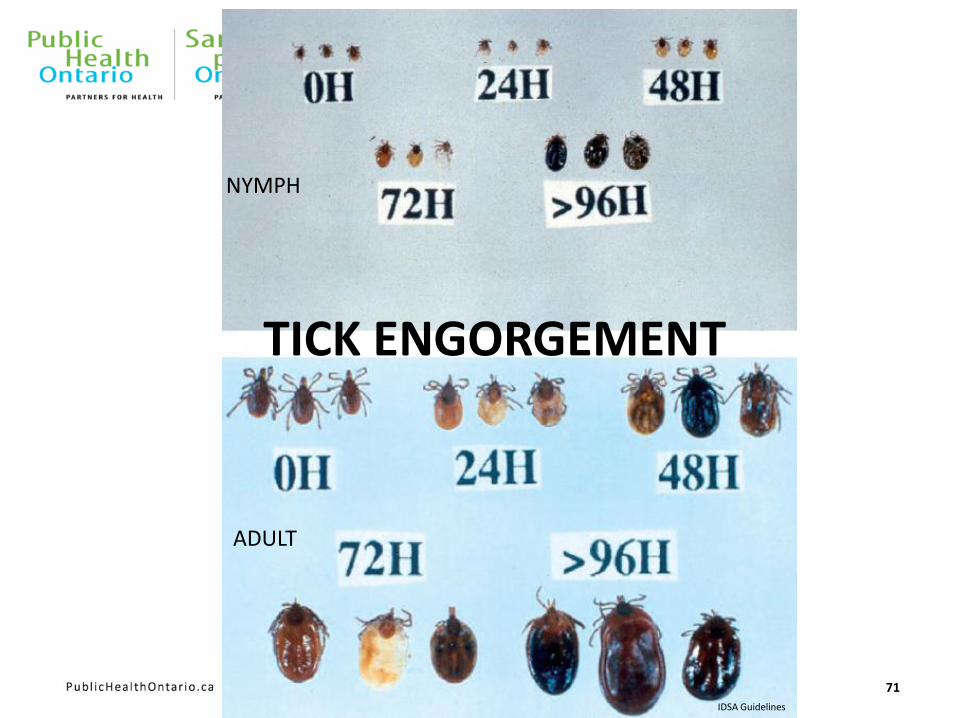
TICK ENGORGEMENT
ADULT
NYMPH
IDSA Guidelines
72
http://www.phac-aspc.gc.ca/id-mi/tickinfo-eng.php
http://www.phac-aspc.gc.ca/id-mi/tickinfo-eng.php
www.cdc.gov/ncidod/dvbid/lyme/resources/handbook.pdf
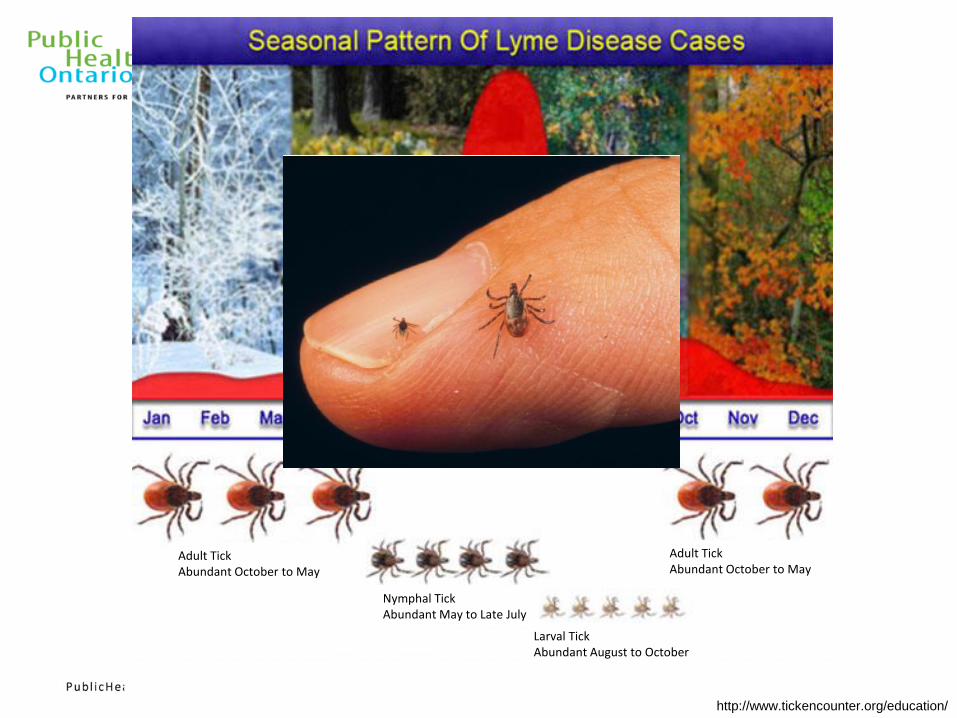
Adult Tick Abundant October to May
Nymphal Tick Abundant May to Late July
Larval Tick Abundant August to October
Adult Tick Abundant October to May
http://www.tickencounter.org/education/
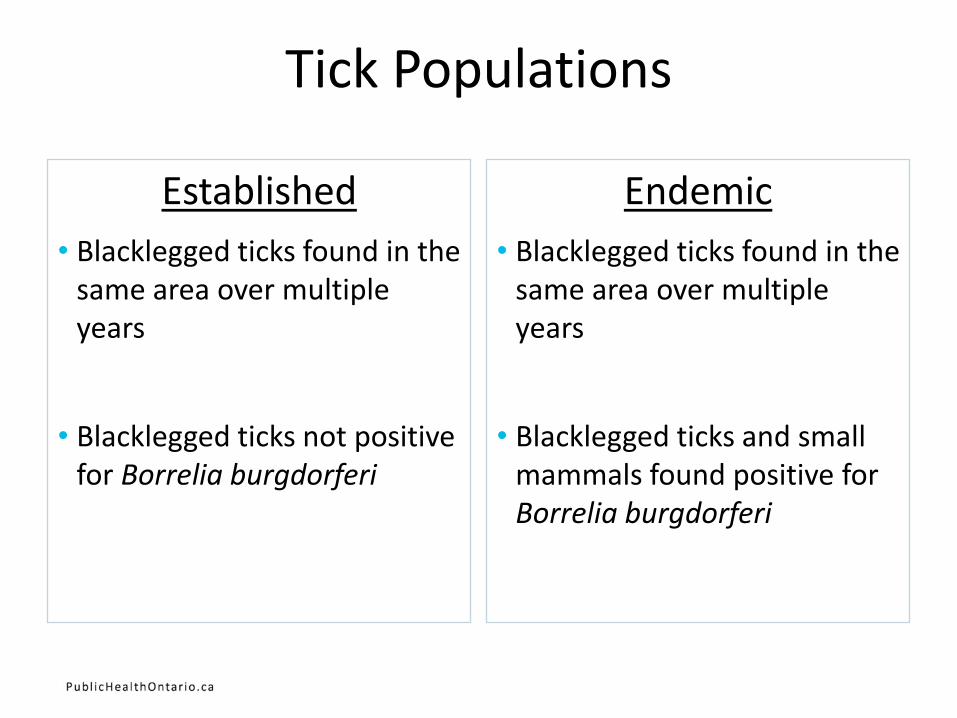
Tick Populations
Established
• Blacklegged ticks found in the same area over multiple years
• Blacklegged ticks not positive for Borrelia burgdorferi
Endemic
• Blacklegged ticks found in the same area over multiple years
• Blacklegged ticks and small mammals found positive for Borrelia burgdorferi
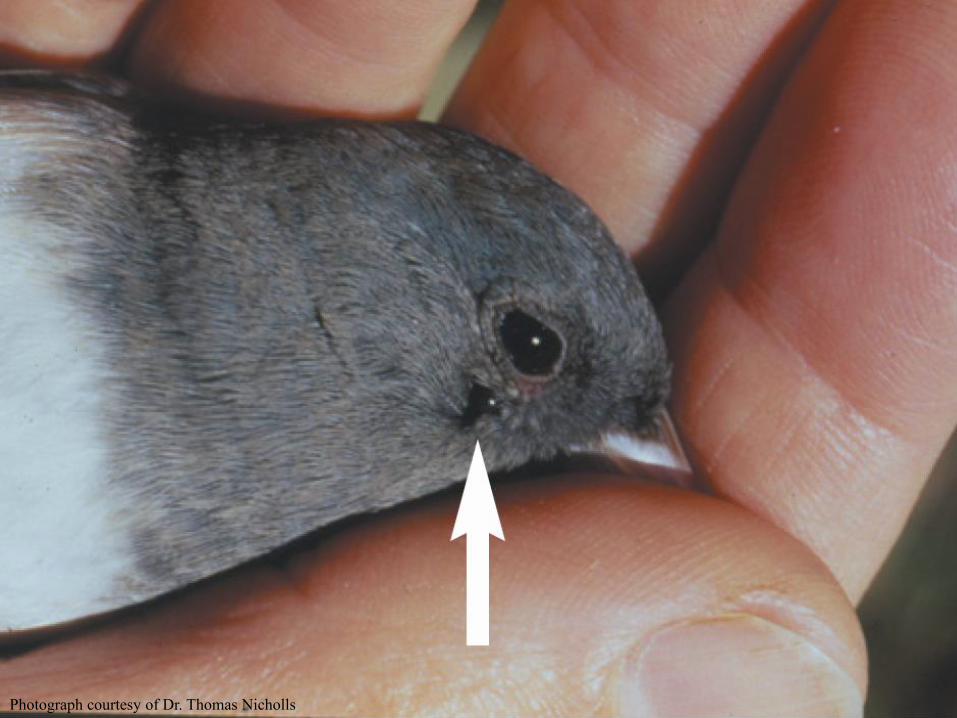
Photograph courtesy of Dr. Thomas Nicholls
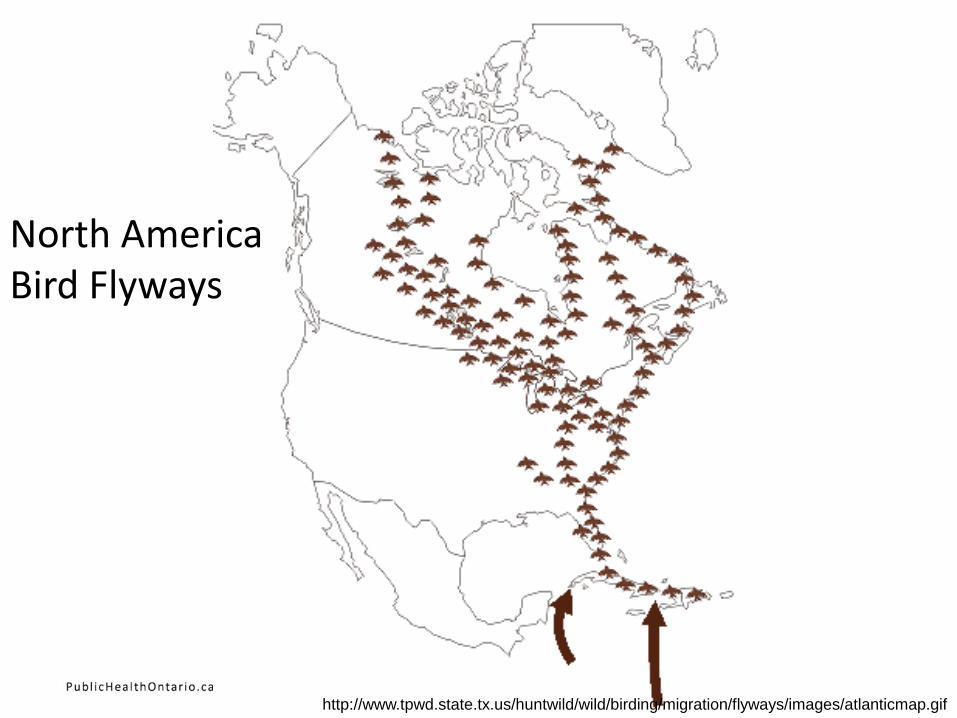
North America Bird Flyways
http://www.tpwd.state.tx.us/huntwild/wild/birding/migration/flyways/images/atlanticmap.gif
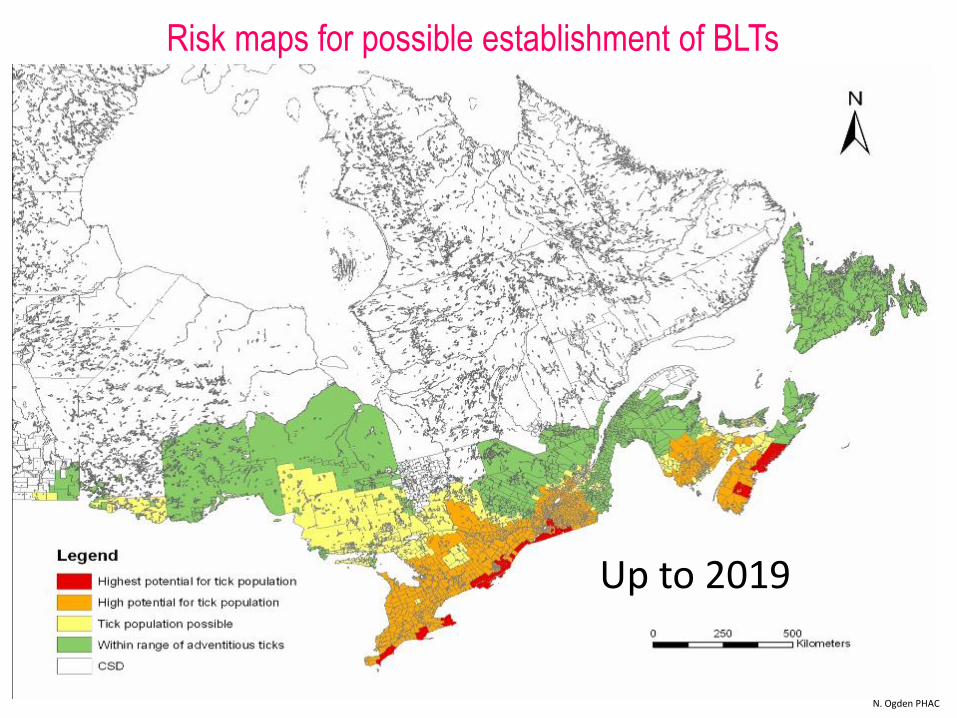
Up to 2019
Risk maps for possible establishment of BLTs
N. Ogden PHAC
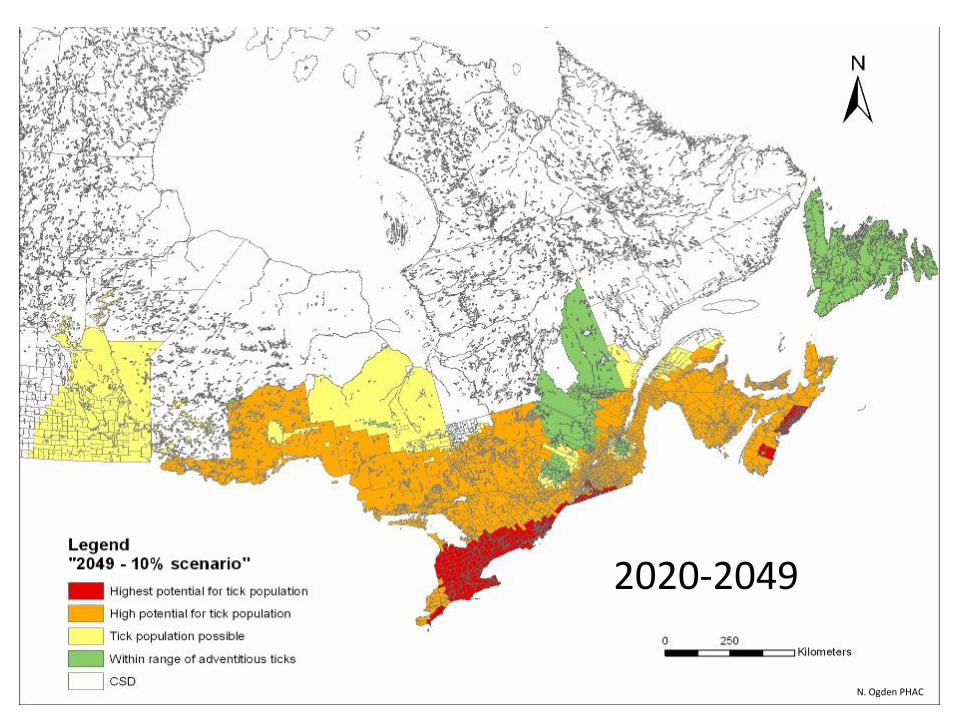
2020-2049
N. Ogden PHAC
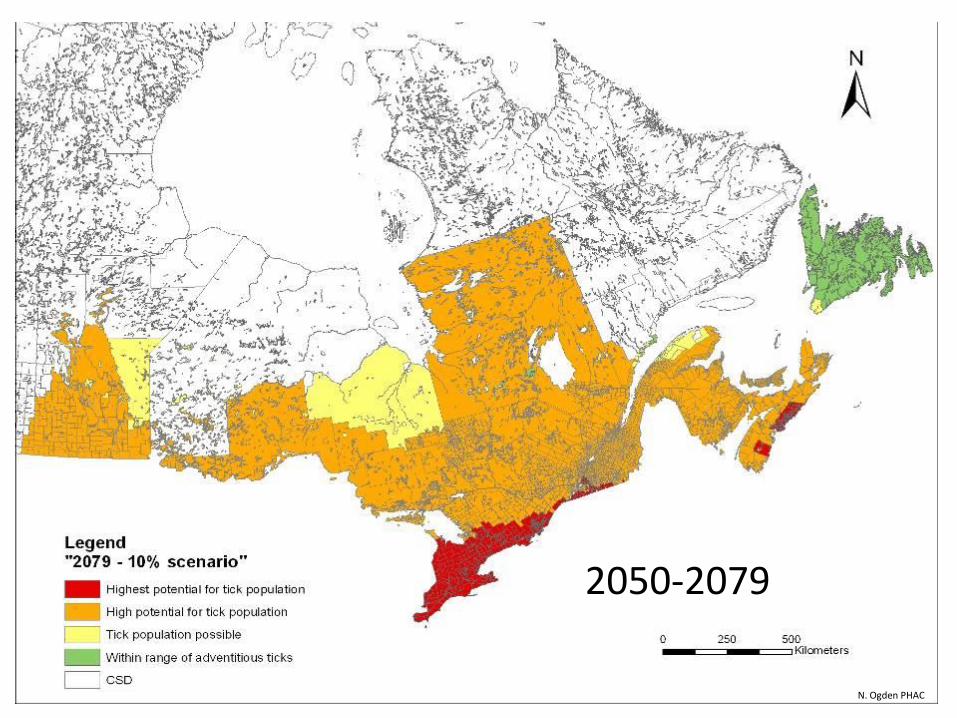
2050-2079
N. Ogden PHAC
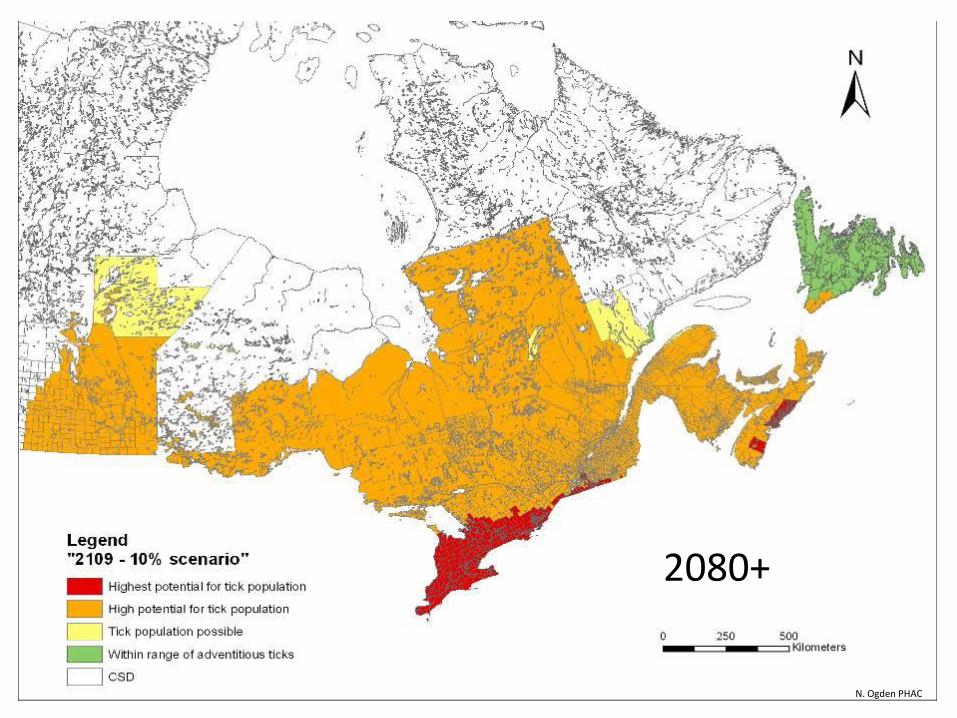
2080+
N. Ogden PHAC
Passive Surveillance • Ticks are submitted to the health unit
• Physicians, veterinarians, public
Active Surveillance • Go out into the environment to look for the ticks
• Tick dragging
• Small mammal trapping
Lyme Disease Surveillance in Ontario
Objectives of Tick Surveillance
• Establish presence/geographic distribution of LD vector.
• Adventitious ticks vs. established populations.
• Size/density of vector populations.
• Prevalence of B. burgdorferi infection.
• Infer risk of exposure based on the above factors and intensity of human use of habitat/opportunity for exposure to infected vectors.
• Implement measures to mitigate risk of exposure & subsequent infection and disease.
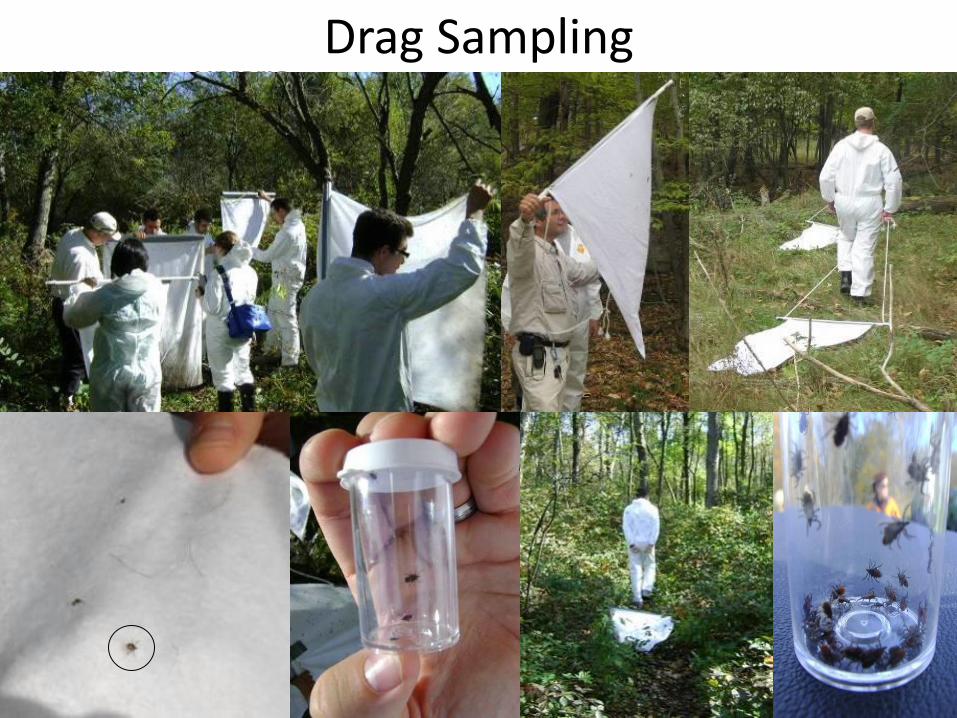
Drag Sampling

Small Mammal Trapping
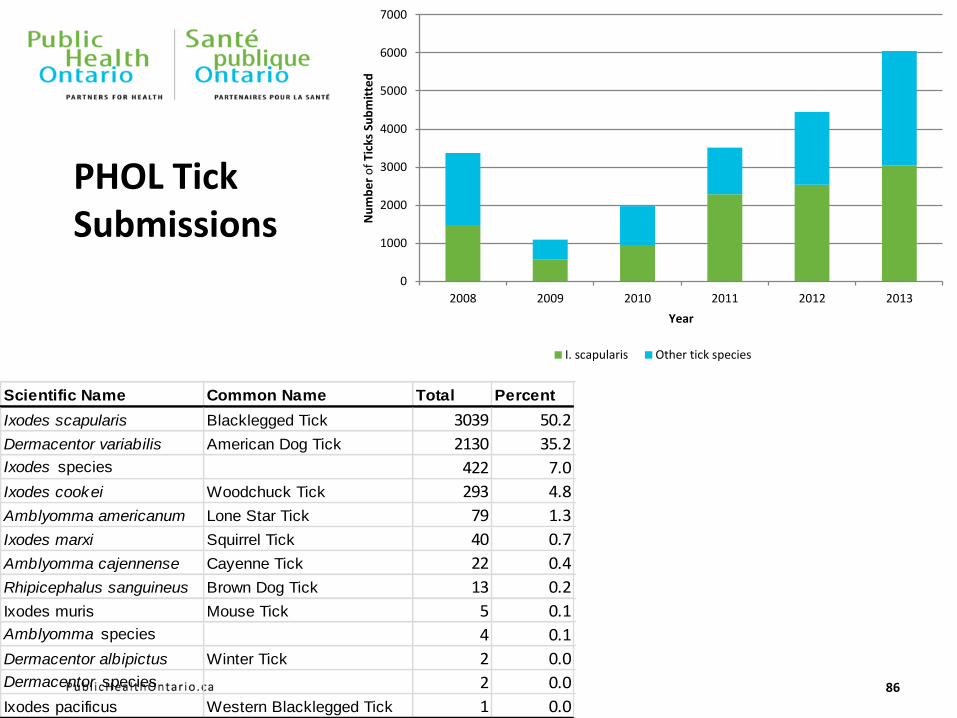
PHOL Tick Submissions
Scientific Name Common Name Total Percent
Ixodes scapularis Blacklegged Tick 3039 50.2
Dermacentor variabilis American Dog Tick 2130 35.2
Ixodes species 422 7.0
Ixodes cookei Woodchuck Tick 293 4.8
Amblyomma americanum Lone Star Tick 79 1.3
Ixodes marxi Squirrel Tick 40 0.7
Amblyomma cajennense Cayenne Tick 22 0.4
Rhipicephalus sanguineus Brown Dog Tick 13 0.2
Ixodes muris Mouse Tick 5 0.1
Amblyomma species 4 0.1
Dermacentor albipictus Winter Tick 2 0.0
Dermacentor species 2 0.0
Ixodes pacificus Western Blacklegged Tick 1 0.0
0
1000
2000
3000
4000
5000
6000
7000
2008 2009 2010 2011 2012 2013
Nu
mb
er
of
Tick
s Su
bm
itte
d
Year
I. scapularis Other tick species
86
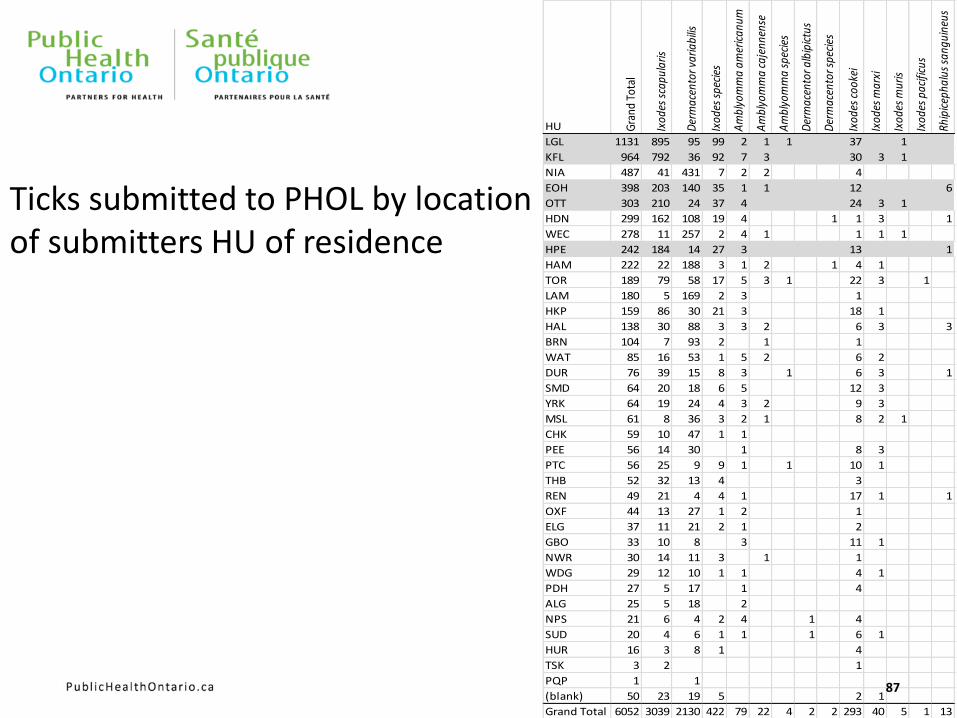
Ticks submitted to PHOL by location of submitters HU of residence
HU Gra
nd T
otal
Ixod
es s
capu
laris
Der
mac
ento
r var
iabi
lis
Ixod
es s
peci
es
Am
blyo
mm
a am
eric
anum
Am
blyo
mm
a ca
jenn
ense
Am
blyo
mm
a sp
ecie
s
Der
mac
ento
r alb
ipic
tus
Der
mac
ento
r spe
cies
Ixod
es c
ooke
i
Ixod
es m
arxi
Ixod
es m
uris
Ixod
es p
acifi
cus
Rhip
icep
halu
s sa
ngui
neus
LGL 1131 895 95 99 2 1 1 37 1
KFL 964 792 36 92 7 3 30 3 1
NIA 487 41 431 7 2 2 4
EOH 398 203 140 35 1 1 12 6
OTT 303 210 24 37 4 24 3 1
HDN 299 162 108 19 4 1 1 3 1
WEC 278 11 257 2 4 1 1 1 1
HPE 242 184 14 27 3 13 1
HAM 222 22 188 3 1 2 1 4 1
TOR 189 79 58 17 5 3 1 22 3 1
LAM 180 5 169 2 3 1
HKP 159 86 30 21 3 18 1
HAL 138 30 88 3 3 2 6 3 3
BRN 104 7 93 2 1 1
WAT 85 16 53 1 5 2 6 2
DUR 76 39 15 8 3 1 6 3 1
SMD 64 20 18 6 5 12 3
YRK 64 19 24 4 3 2 9 3
MSL 61 8 36 3 2 1 8 2 1
CHK 59 10 47 1 1
PEE 56 14 30 1 8 3
PTC 56 25 9 9 1 1 10 1
THB 52 32 13 4 3
REN 49 21 4 4 1 17 1 1
OXF 44 13 27 1 2 1
ELG 37 11 21 2 1 2
GBO 33 10 8 3 11 1
NWR 30 14 11 3 1 1
WDG 29 12 10 1 1 4 1
PDH 27 5 17 1 4
ALG 25 5 18 2
NPS 21 6 4 2 4 1 4
SUD 20 4 6 1 1 1 6 1
HUR 16 3 8 1 4
TSK 3 2 1
PQP 1 1
(blank) 50 23 19 5 2 1
Grand Total 6052 3039 2130 422 79 22 4 2 2 293 40 5 1 13
87
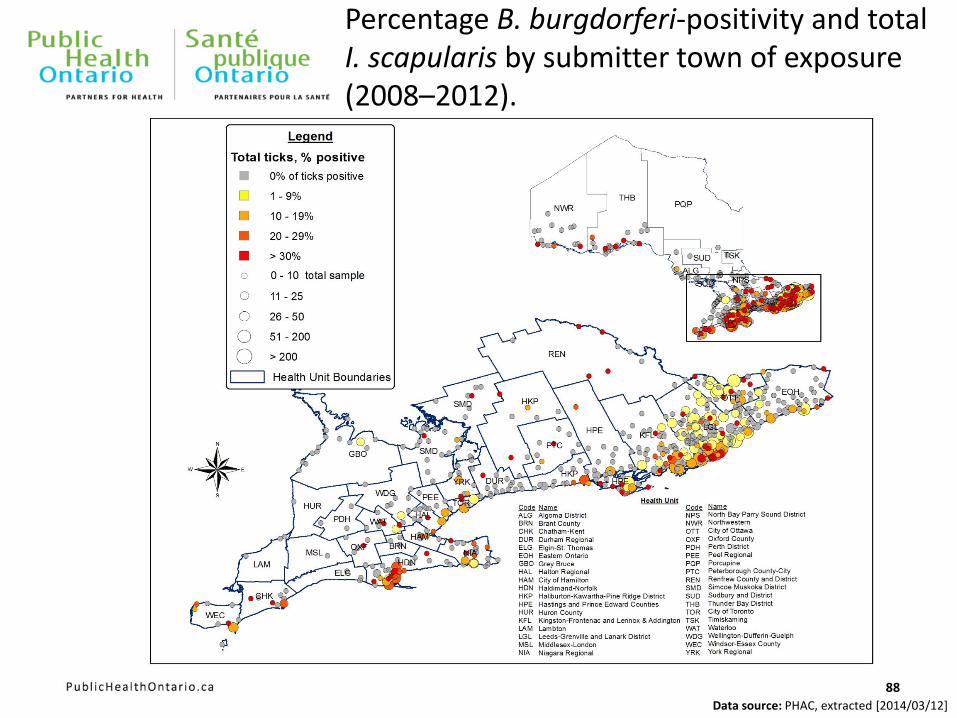
Percentage B. burgdorferi-positivity and total I. scapularis by submitter town of exposure (2008–2012).
Data source: PHAC, extracted [2014/03/12]
88
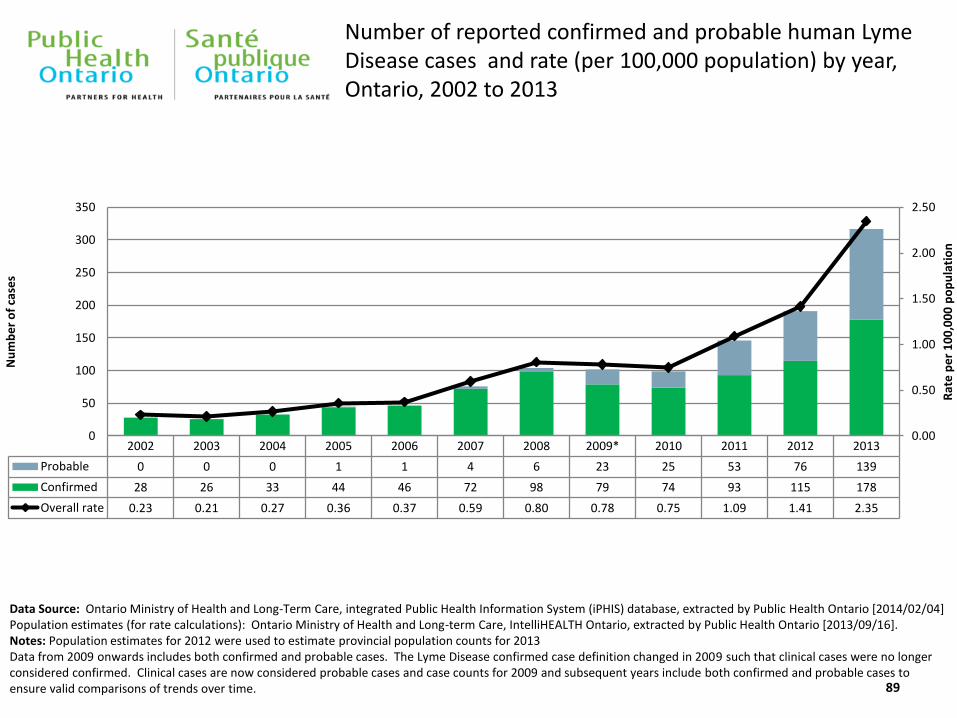
2002 2003 2004 2005 2006 2007 2008 2009* 2010 2011 2012 2013
Probable 0 0 0 1 1 4 6 23 25 53 76 139
Confirmed 28 26 33 44 46 72 98 79 74 93 115 178
Overall rate 0.23 0.21 0.27 0.36 0.37 0.59 0.80 0.78 0.75 1.09 1.41 2.35
0.00
0.50
1.00
1.50
2.00
2.50
0
50
100
150
200
250
300
350
Rat
e p
er
10
0,0
00
po
pu
lati
on
Nu
mb
er
of
case
s
Data Source: Ontario Ministry of Health and Long-Term Care, integrated Public Health Information System (iPHIS) database, extracted by Public Health Ontario [2014/02/04] Population estimates (for rate calculations): Ontario Ministry of Health and Long-term Care, IntelliHEALTH Ontario, extracted by Public Health Ontario [2013/09/16]. Notes: Population estimates for 2012 were used to estimate provincial population counts for 2013 Data from 2009 onwards includes both confirmed and probable cases. The Lyme Disease confirmed case definition changed in 2009 such that clinical cases were no longer considered confirmed. Clinical cases are now considered probable cases and case counts for 2009 and subsequent years include both confirmed and probable cases to ensure valid comparisons of trends over time.
Number of reported confirmed and probable human Lyme Disease cases and rate (per 100,000 population) by year, Ontario, 2002 to 2013
89
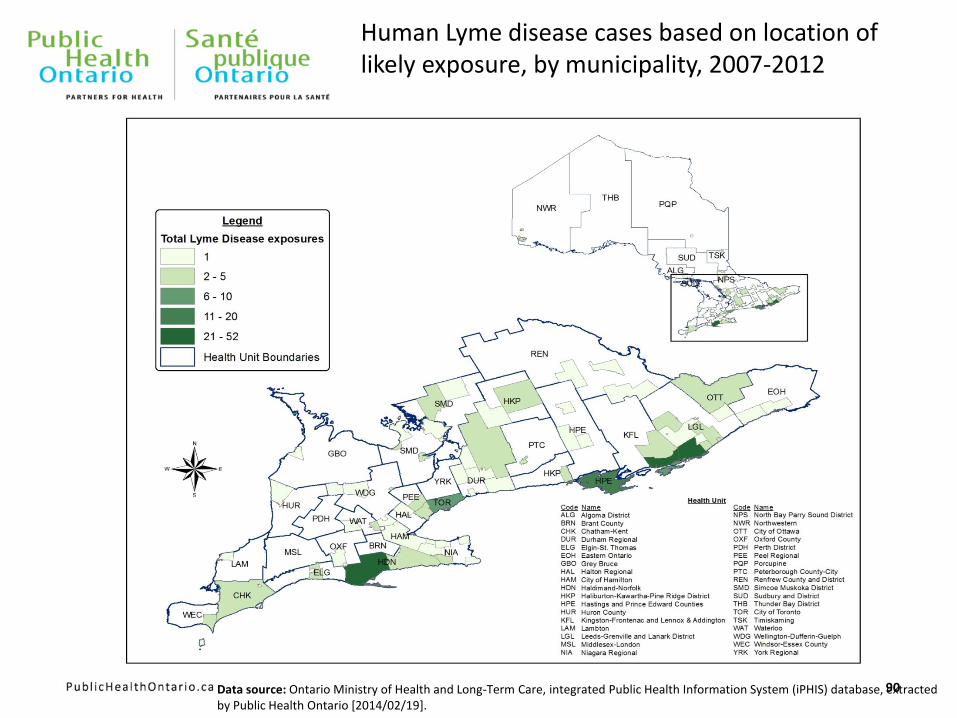
Human Lyme disease cases based on location of likely exposure, by municipality, 2007-2012
Data source: Ontario Ministry of Health and Long-Term Care, integrated Public Health Information System (iPHIS) database, extracted by Public Health Ontario [2014/02/19].
90
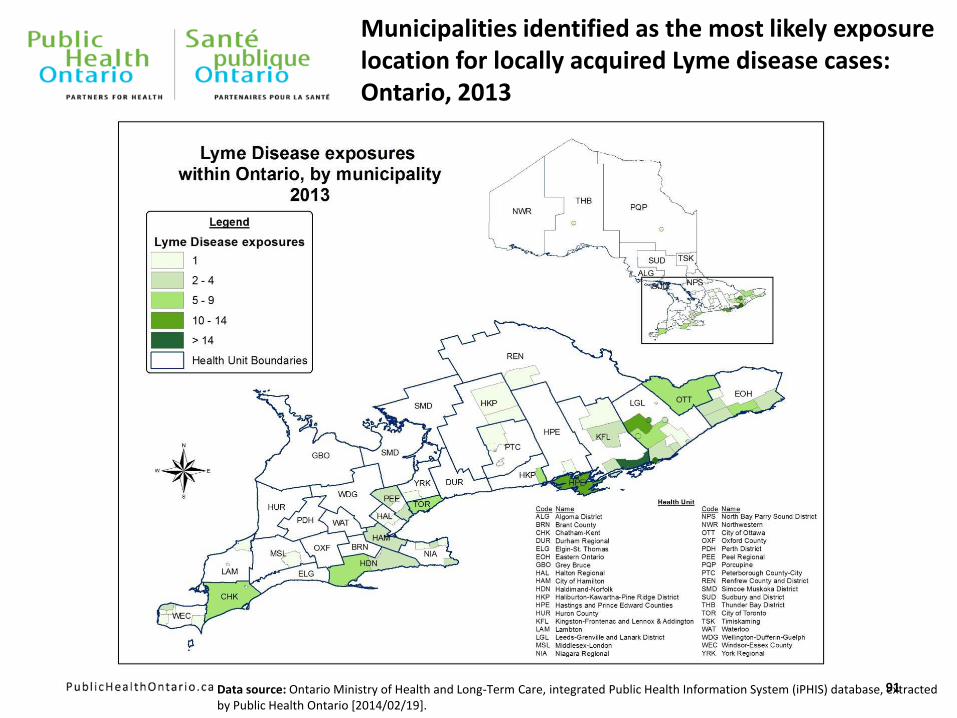
Municipalities identified as the most likely exposure location for locally acquired Lyme disease cases: Ontario, 2013
Data source: Ontario Ministry of Health and Long-Term Care, integrated Public Health Information System (iPHIS) database, extracted by Public Health Ontario [2014/02/19].
91
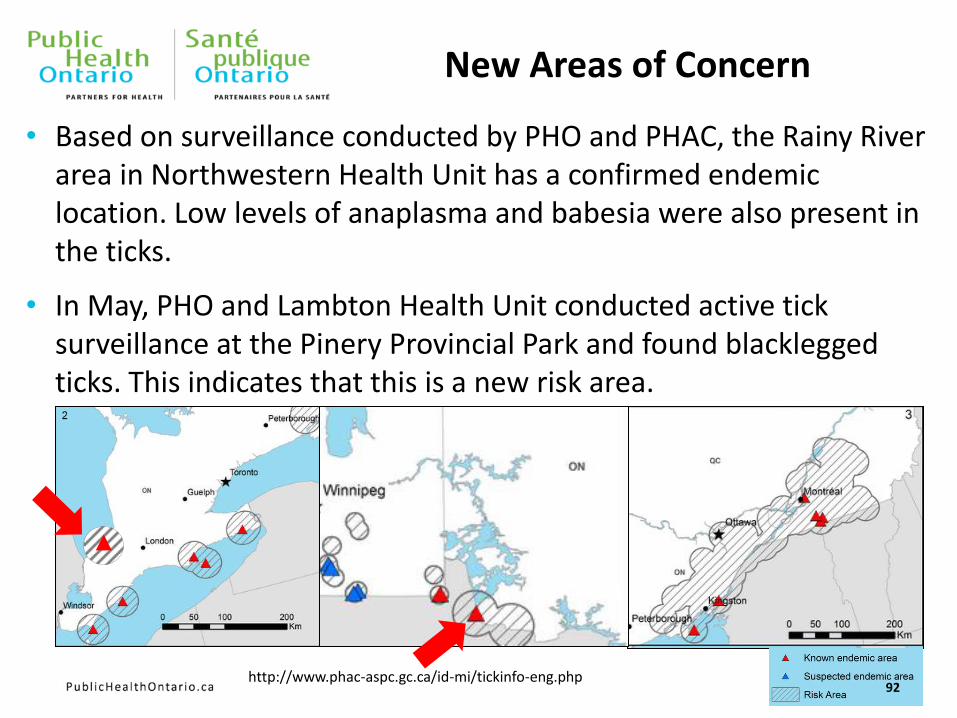
New Areas of Concern
• Based on surveillance conducted by PHO and PHAC, the Rainy River area in Northwestern Health Unit has a confirmed endemic location. Low levels of anaplasma and babesia were also present in the ticks.
• In May, PHO and Lambton Health Unit conducted active tick surveillance at the Pinery Provincial Park and found blacklegged ticks. This indicates that this is a new risk area.
http://www.phac-aspc.gc.ca/id-mi/tickinfo-eng.php 92
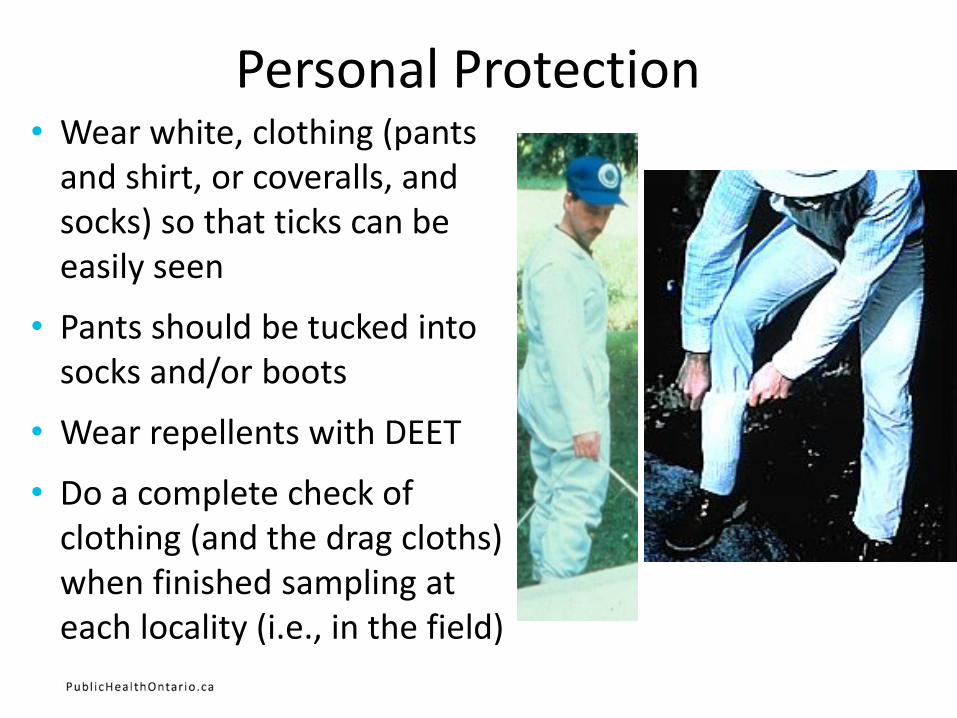
Personal Protection • Wear white, clothing (pants
and shirt, or coveralls, and socks) so that ticks can be easily seen
• Pants should be tucked into socks and/or boots
• Wear repellents with DEET
• Do a complete check of clothing (and the drag cloths) when finished sampling at each locality (i.e., in the field)
Personal Protection continued • At home, carefully recheck your clothing and boots; and
thoroughly check your skin for attached ticks
• Use the “Buddy” system
• Bite sites should be monitored and any attached ticks should be preserved (frozen) for identification and possible testing should symptoms develop
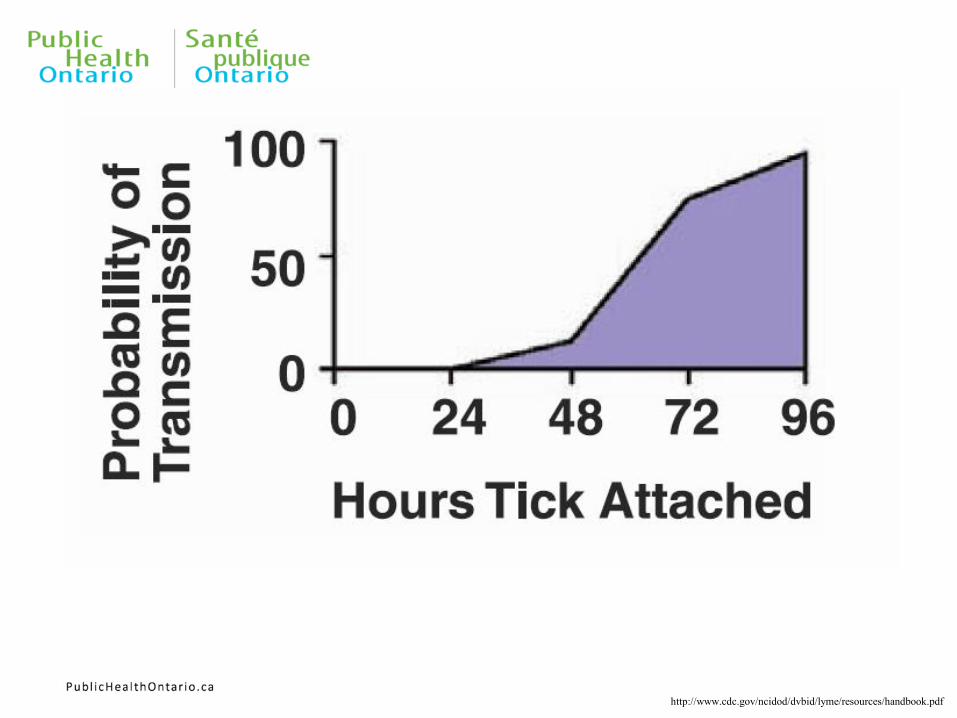
• It is important to remember that attached ticks do not immediately start to transmit the agent of LD but rather it takes 24 to 48 hours of attachment before the bacteria is transferred
95 www.cdc.gov/ncidod/dvbid/lyme/resources/handbook.pdf
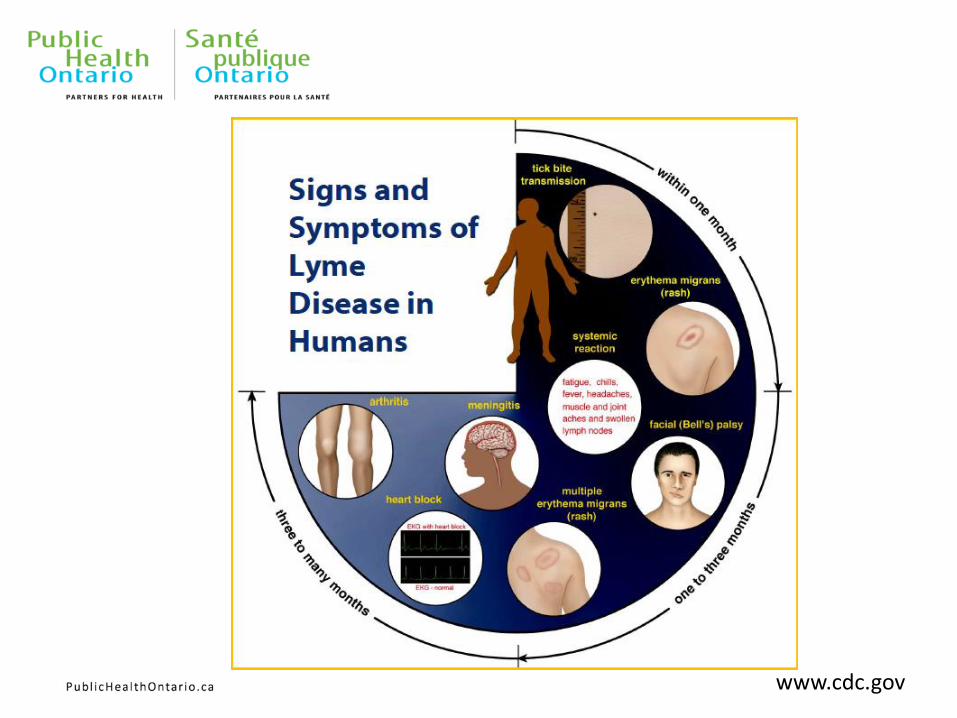
www.cdc.gov


From: IDSA Guidelines – CID 2006:43 (1 November)
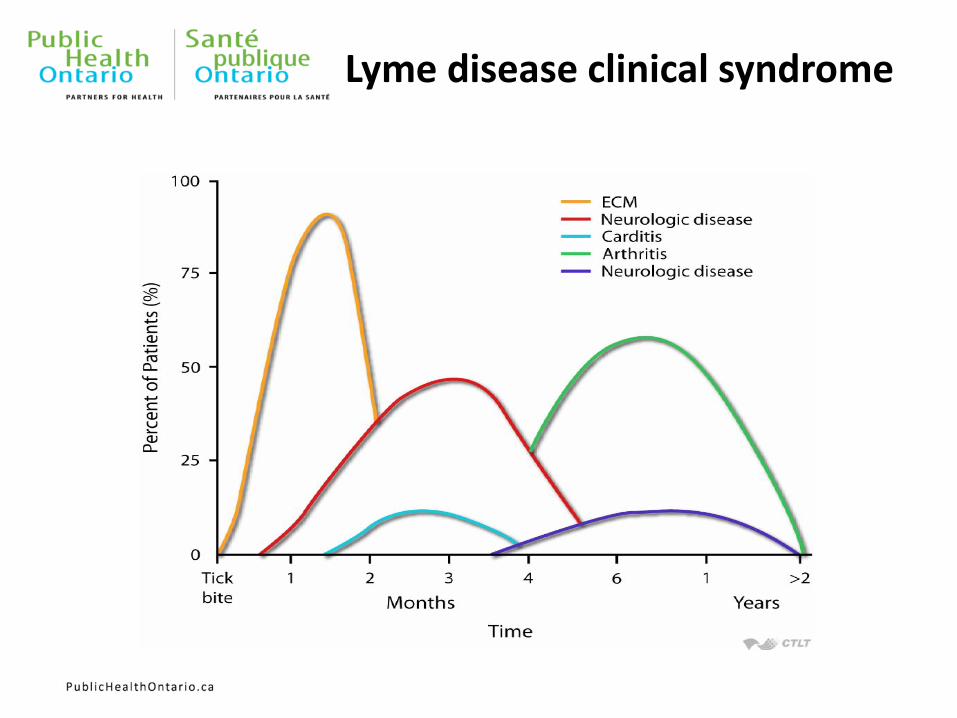
Lyme disease clinical syndrome
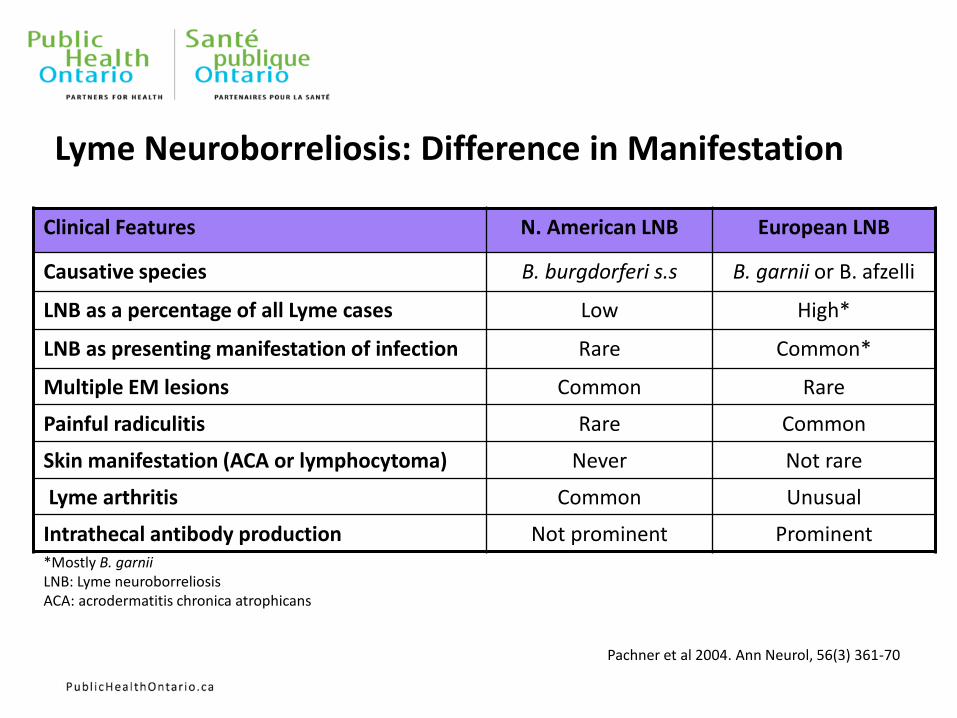
Lyme Neuroborreliosis: Difference in Manifestation
Clinical Features N. American LNB European LNB
Causative species B. burgdorferi s.s B. garnii or B. afzelli
LNB as a percentage of all Lyme cases Low High*
LNB as presenting manifestation of infection Rare Common*
Multiple EM lesions Common Rare
Painful radiculitis Rare Common
Skin manifestation (ACA or lymphocytoma) Never Not rare
Lyme arthritis Common Unusual
Intrathecal antibody production Not prominent Prominent *Mostly B. garnii LNB: Lyme neuroborreliosis ACA: acrodermatitis chronica atrophicans
Pachner et al 2004. Ann Neurol, 56(3) 361-70
Laboratory Tests for Lyme disease • Serologic testing
• Serum IgM ELISA
• Peaks at 3 – 6 weeks after onset of infection
• Serum IgG ELISA
• Usually increases slowly and is highest weeks to months later
• Western Blot testing
• Done on all ELISA positive samples for confirmation
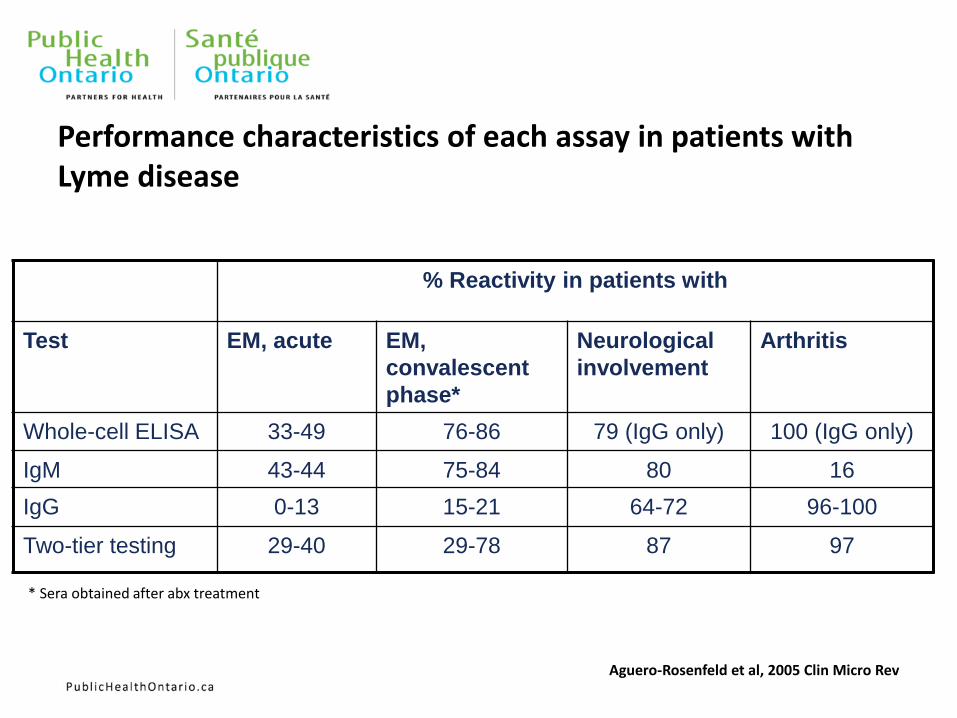
Performance characteristics of each assay in patients with Lyme disease
% Reactivity in patients with
Test EM, acute EM,
convalescent
phase*
Neurological
involvement
Arthritis
Whole-cell ELISA 33-49 76-86 79 (IgG only) 100 (IgG only)
IgM 43-44 75-84 80 16
IgG 0-13 15-21 64-72 96-100
Two-tier testing 29-40 29-78 87 97
* Sera obtained after abx treatment
Aguero-Rosenfeld et al, 2005 Clin Micro Rev
Challenges posed by private laboratories in USA
• Private labs uses variety of different assays to diagnose Lyme disease
• None of them are scientifically validated
• In 2005 the CDC placed a notice in their Morbidity and Mortality Weekly Report (MMWR) cautioning about using these private laboratories: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5405a6.htm
103
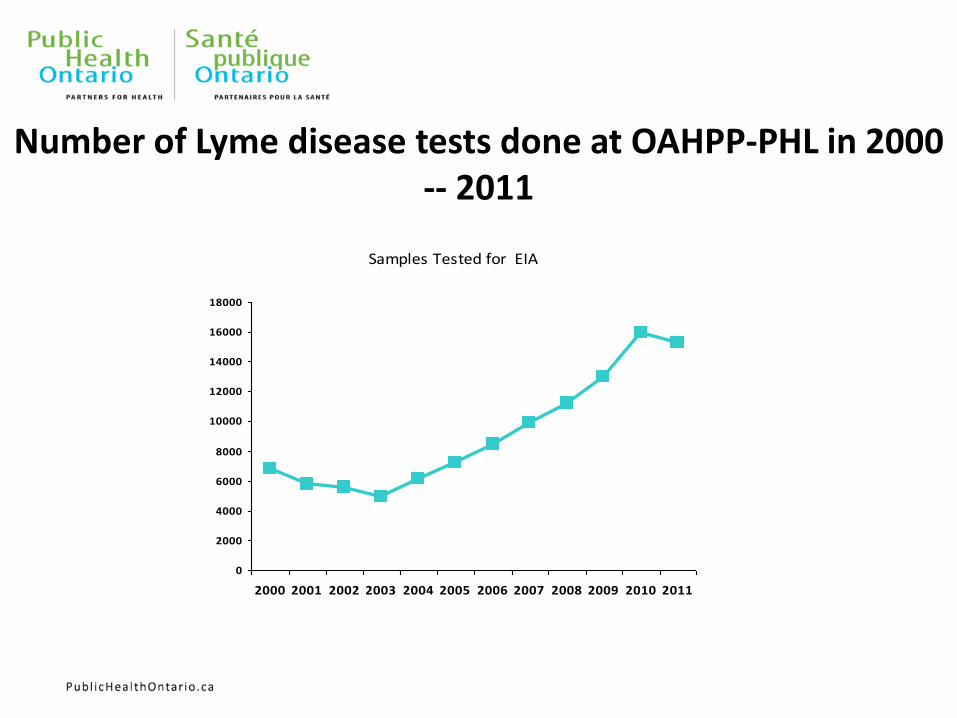
Number of Lyme disease tests done at OAHPP-PHL in 2000 -- 2011
Samples Tested for EIA
0
2000
4000
6000
8000
10000
12000
14000
16000
18000
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011
Post Lyme Disease Treatment Syndrome (PLDS)
• Often called “chronic Lyme disease,” this condition is properly known as “Post-treatment Lyme disease Syndrome” (PTLDS)
• Can be divided into 2 groups: sero-positive or sero-negative group
• Some evidence that show that delay in treatment of Lyme disease may result in longer PLDTS
• The exact cause of PTLDS is not yet known. Most medical experts believe that lingering symptoms are due to residual damage to the tissues and the immune system that occurred during the infection. Similar complications and auto-immune responses are known to occur following other infectious diseases. CDC
• There is no credible scientific evidence that PTLDS is caused by persistent infection. CDC
105
Long-Term Antibiotic Treatment
• The National Institute of Allergy and Infectious Diseases (NIAID) has funded three placebo-controlled clinical trials on the efficacy of prolonged antibiotic therapy for treating PLDS.
• “Carefully designed, placebo-controlled studies have failed to demonstrate that prolonged antibiotic therapy is beneficial.” NIAID
• http://www.niaid.nih.gov/topics/lymeDisease/understanding/Pages/chronic.aspx
106

Questions?
107