Embed Size (px)
Citation preview

VCUDEATH AND COMPLICATIONS CONFERENCE03/22/2012

Brief Overview of Case
Multiple gunshot wounds with pulselessness
Emergency room thoracotomy Death

Introduction for Every Case Complication
Death Procedure
Emergency room thoracotomy Primary Diagnosis
Multiple gunshot wounds

Clinical History HPI:
27 yo male arrived in the trauma bay as a delta trauma team alert following report of multiple gunshot wounds
Per EMS they were unable to obtain IV access en route and his initial GCS was 15 although just prior to arrival he deteriorated to 5
Intubation had not been attempted prior to arrival
PMH/PSHx: suspected multiple abdominal surgeries with large ventral hernia with skin graft
Meds/Allergies: unknown Presentation:
Agonal respirations, GCS 5, initial HR 50s, unable to obtain BP with cuff
PE: 13 GSWs counted 2 to head, 2 to chest, bilateral upper extremities, abdomen
Femoral pulse present as patient was getting intubated, lost during intubation
WBC: 8.7x10 ^3, Hgb 13.9 Plt 293 x10^3 Na 153, K 5.4, Cl 105, Co2 11, Glc 186, BUN 12, Cr 1.84, Ca 10.4

Clinical History
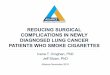
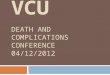
Immediate ED thoracotomy was commenced by performing a left anterolateral incision.
The heart was not empty, no sustained meaningful cardiac movements, no wounds noted to the heart, or lungs. Pericardium was opened with clear fluid noted within the sac
The aorta was palpated along the spine and noted to be flat, this was clamped by the attending surgeon
Immediately upon arrival right femoral venous access had been obtained and the patient was getting resuscitation with normal saline and 2PRBC
Based on the findings during the thoracotomy right subclavian venous line was placed and subsequent resuscitative fluids given via that access
2 rounds of intracardiac epinephrine were administered while performing direct cardiac massage
Bicarbonate was given IV Following 19 minutes of ACLS-ATLS protocol he never regained vital
signs Time of death was 02:39

Analysis of Complication
• Was the complication potentially avoidable?– No
• Would avoiding the complication change the outcome for the patient?– No
• What factors contributed the complication?– The complication was a result of his extensive
wounds.– Possible devastating head injury– Possible infradiaphragmatic vessel injury – Cardiac arrest

FIGURE 6-5 Anterolateral thoracotomy/emergency room thoracotomy. (Adapted from Ivatury, R.R. In: Feliciano, D.V.; Moore, E.E.; Mattox, K.L. (eds.). Trauma, 3rd ed. Stamford, CT, Appleton & Lange, 1996.)

Johnson et. Al. Chapter 49, thoracic trauma. Mastery of Surgery. Lippincott Williams and Wlilkins. 2009

Selke et,a l. Sabiston and Spencer’s Surgery of the Chest. 8th ed. Saunders. 2009 Chapter 7: Thoracic Trauma
Box 7– Indications and Contraindications for Emergency Room Thoracotomy Accepted Indications
• Unresponsive hypotension (systolic blood pressure [SBP] < 60 mm Hg)
• Rapid exsanguination from indwelling chest tube (>1500 mL)
• Traumatic arrest with previously witnessed cardiac activity (before or after hospital admission) after penetrating thoracic injuries
• Persistent hypotension (SBP < 60 mm Hg) with diagnosed cardiac tamponade, air embolism
Relative Indications
• Traumatic arrest with previously witnessed cardiac activity (before or after hospital admission) after blunt trauma
• Traumatic arrest without previously witnessed cardiac activity (before or after hospital admission) after penetrating chest injuries
• Prehospital cardiopulmonary resuscitation: <10 minutes in intubated patient, <5 minutes in nonintubated patient
Contraindications
• Blunt thoracic injuries with no previously witnessed cardiac activity
• Multiple blunt trauma
• Severe head injury

Cothren and Moore. Emergency department thoracotomy for the critically injured patient: Objectives, indications, and outcomes. World J Emerg Surg. 2006; 1:4

Cothren and Moore. Emergency department thoracotomy for the critically injured patient: Objectives, indications, and outcomes. World J Emerg Surg. 2006; 1:4
The summarized data confirms EDT has the highest survival rate following isolated cardiac injury; ~35% of adult patients presenting in shock, and ~20% without vital signs, were salvaged after isolated penetrating injury to the heart if EDT was performed.
Following penetrating torso injuries, ~14% of patients requiring EDT are salvaged if they are hypotensive with detectable vital signs, whereas 8% of those who have no vital signs but have signs of life at presentation, and 1% of those without signs of life are salvaged.
Survival rates by mechanism in descending order are 19.4% for isolated cardiac wounds, 16.8% for stab wounds, 4.3% for gunshot wounds, and 1% for blunt trauma.

Ivatury RR, Kazigo J, Rohman M, Gaudino J, Simon R, Stahl WM. "Directed" emergency room thoracotomy: a prognostic prerequisite for survival. J Trauma. 1991 Aug;31(8):1076-81; discussion 1081-2. Department of Surgery, New York Medical College, Bronx.
AbstractThe results of 163 patients (49 SWs, 85 GSWs, 29 blunt trauma) who had resuscitative thoracotomy in the emergency room (ERT) were reviewed to reassess the indications for the procedure. The Revised Trauma Score (RTS) of the patients ranged from 0 to 3 in 138, 4 to 8 in 21, and greater than 8 in four. No patient with blunt trauma survived. Sixteen patients [12 (24.5%) with stab wounds and 4 (4.7%) with gunshot wounds] were eventually discharged, an overall survival of 9.8%. Eight of the survivors were without vital signs on arrival at the emergency center and one of them had only signs of life at the scene. Survival was best when the site of penetration was thoracic (n = 84) and the ERT was "directed" at potential cardiac injury. Fifty-six of these patients (66.6%) did have cardiac wounds with tamponade and 12 of them survived (21.4%). Two of the remaining 28 patients, both with pulmonary injury, were salvaged. This was significantly (p less than 0.001) higher than in patients with head and neck (n = 4), abdominal (n = 19), or multiple site (n = 40) injury when the ERT was nondirected. Two of the five patients (40%) with extremity vascular injuries survived after ERT was successful in restoring a cardiac rhythm. These data suggest that in patients without vital signs, ERT "directed" at potential cardiac injury based on thoracic penetration is an important prognostic prerequisite for survival. Emergency room thoracotomy is not beneficial in blunt trauma and its role in penetrating abdominal injuries remains unproven.

P.M. Rhee, J. Acosta Survival after emergency department thoracotomy: review of published data from the last 25 years. J Am Coll Surg, 190 (2000), pp. 288–299
AbstractBACKGROUND: Emergency department thoracotomy (EDT) has become standard therapy for patients who acutely arrest after injury. Patient selection is vitally important to achieve optimal outcomes without wasting valuable resources. The aim of this study was to determine the main factors that most influence survival after EDT.STUDY DESIGN: Twenty-four studies that included 4,620 cases from institutions that reported EDT for both blunt and penetrating trauma during the past 25 years were reviewed. The primary outcomes analyzed were in-hospital survival rates.RESULTS: EDT had an overall survival rate of 7.4%. Normal neurologic outcomes were noted in 92.4% of surviving patients. Factors reported as influencing outcomes were the mechanism of injury (MOI), location of major injury (LOMI), and signs of life (SOL). Survival rates for MOI were 8.8% for penetrating injuries and 1.4% for blunt injuries. When penetrating injuries were further separated, the survival rates were 16.8% for stab wounds and 4.3% for gunshot wounds. For the LOMI, survival rates were 10.7% for thoracic injuries, 4.5% for abdominal injuries, and 0.7% for multiple injuries. If the LOMI was the heart, the survival rate was the highest at 19.4%. The third factor influencing outcomes was SOL. If SOL were present on arrival at the hospital, survival rate was 11.5% in contrast to 2.6% if none were present. SOL present during transport resulted in a survival rate of 8.9%. Absence of SOL in the field yielded a survival rate of 1.2%. There was no clear single independent preoperative factor that could uniformly predict death.CONCLUSIONS: The best survival results are seen in patients who undergo EDT for thoracic stab injuries and who arrive with SOL in the emergency department. All three factors-MOI, LOMI, and SOL-should be taken into account when deciding whether to perform EDT. Uniform reporting guidelines are needed to further elucidate the role of EDT taking into account the combination of MOI, LOMI, and SOL.

Take Home Points
ABCs can be assessed concurrently to expedite appropriate care in the trauma setting
Indications for emergency room thoracotomy
Very low survival rate associated with penetrating trauma with multiple injuries
The utility of reassessing the mode of providing care when appropriate

References
Rhee PM, Acosta J, Bridgeman A, Wang D, Jordan M, Rich N. "Survival after emergency department thoracotomy: Review of published data from the past 25 years". JACS. 2000;190:288.