Embed Size (px)
Citation preview

NATURE REVIEWS | RHEUMATOLOGY VOLUME 10 | AUGUST 2014 | 463
Department of Pathology and Laboratory Medicine, School of Medicine, University of North Carolina at Chapel Hill, 308 Brinkhous-Bullitt Building, CB#7525, Chapel Hill, NC 27599-7525, USA (J.C.J., R.J.F.).
Correspondence to: J.C.J. [email protected]
Pathogenesis of antineutrophil cytoplasmic autoantibody-mediated diseaseJ. Charles Jennette and Ronald J. Falk
Abstract | Antineutrophil cytoplasmic autoantibodies (ANCAs) are the probable cause of a distinct form of vasculitis that can be accompanied by necrotizing granulomatosis. Clinical and experimental evidence supports a pathogenesis that is driven by ANCA-induced activation of neutrophils and monocytes, producing destructive necrotizing vascular and extravascular inflammation. Pathogenic ANCAs can originate from precursor natural autoantibodies. Pathogenic transformation might be initiated by commensal or pathogenic microbes, legal or illegal drugs, exogenous or endogenous autoantigen complementary peptides, or dysregulated autoantigen expression. The ANCA autoimmune response is facilitated by insufficient T-cell and B-cell regulation. A putative pathogenic mechanism for vascular inflammation begins with ANCA-induced activation of primed neutrophils and monocytes leading to activation of the alternative complement pathway, which sets in motion an inflammatory amplification loop in the vessel wall that attracts and activates neutrophils with resultant respiratory burst, degranulation, extrusion of neutrophil extracellular traps, apoptosis and necrosis. The pathogenesis of extravascular granulomatosis is less clear, but a feasible scenario proposes that a prodromal infectious or allergic condition positions primed neutrophils in extravascular tissue in which they can be activated by ANCAs in interstitial fluid to produce extravascular necrotizing injury that would initiate an innate granulomatous inflammatory response to wall off the necrotic debris.
Jennette, J. C. & Falk, R. J. Nat. Rev. Rheumatol. 10, 463–473 (2014); published online 8 July 2014; doi:10.1038/nrrheum.2014.103
IntroductionAntineutrophil cytoplasmic autoantibodies (ANCAs) are associated with, and are the probable cause of, a distinct form of vasculitis that can affect any organ in the body. Although small vessels are the predominant target, ANCA-associated vasculitis (AAV) can affect many different types of vessels including ar teries, arterioles, capillaries, venules and veins (Figure 1).1 Immuno pathologically, AAV has an absence or paucity of immunoglobulin deposition in injured vessels (pauci-immune vasculitis), compared with the more extensive deposition of immunoglobulin in immune-complex-mediated small-vessel vasculitis.1 AAV can be limited to one organ at the time of presentation (for example, lung-limited disease or renal-limited disease) or involve multiple organs. Frequent target tissues are the upper and lower respiratory tract, kidneys, skin and periph-eral nerves. Onset and exacerbations induce signs and symptoms of high levels of circulating inflammatory cytokines, such as fever, arthralgia and myalgia. In addi-tion to these nonspecific systemic inflammatory mani-festations, inflammation of vessel walls causes more specific signs and symptoms of vasculitis depending on which vessels and which organs are affected, for example purpura caused by dermal venulitis; pulmonary
haemorrhage caused by alveolar capillaritis; glomerulo-nephritis caused by glomerular capillaritis; peripheral neuropathy caused by epineural arteritis; and ocular inflammation caused by vasculitis in small vessels in the eye and orbit. In addition to vasculitis, some variants of ANCA-associated disease have extravascular necrotiz-ing granulomatous inflammation (granulomatosis)— seemingly not arising from vascular inflammation—that most often affects the upper and lower respiratory tracts but can affect any organ.
On the basis of the distribution of vascular inflam-mation and the presence or absence of granulomatosis and asthma, systemic AAV is categorized as microscopic polyangiitis (MPA) if there is vasculitis but no evidence of granulomatosis or asthma, granulomatosis with poly-angiitis (GPA) if there is granulomatosis but no asthma, and eosinophilic granulomatosis with poly angiitis (EGPA; also known as Churg–Strauss syndrome) if there is granulomatosis, asthma and blood eosinophilia.1 Organ-limited disease, including isolated pauci-immune necrotizing and crescentic glomerulonephritis, can be considered limited variants of MPA. Limited variants of GPA and EGPA can be confined to the respiratory tract.
AAV can also be classified on the basis of auto-antigen specificity. In patients with vasculitis, the two best- documented autoantigen targets of ANCA are myelo peroxidase (MPO)2 and proteinase 3 (PR3).3–5 Classification of AAV by antigen specificity clearly shows differences in clinical presentations and outcomes,
Competing interestsJ.C.J. has acted as a consultant for Amicus Therapeutics, Genentech, GlaxoSmithKline and Protalix BioTherapeutics, and has undertaken research in collaboration with ChemoCentryx. R.J.F. declares no competing interests.
FOCUS ON VASCULITIS
© 2014 Macmillan Publishers Limited. All rights reserved

464 | AUGUST 2014 | VOLUME 10 www.nature.com/nrrheum
organ system involvement, patterns of extravascular inflammation, and genetic associations including HLA associ ations.6,7 The most informative AAV classifica-tion scheme includes both the ANCA antigen specifi-city and the clinicopathological phenotype, for example MPO-ANCA MPA or PR3-ANCA MPA.1
MPO and PR3 are not the only autoantigens recog-nized by ANCAs. For instance, ANCAs specific for elastase occur, and are most often identified, in patients with drug-induced ANCA-associated disease, including disease induced by cocaine adulterated with leva misole.8,9 A controversial autoantigen specificity is for lysosomal-associated membrane protein 2 (LAMP-2). Kain et al.10 reported finding LAMP-2-ANCA in ~90% of patients
Key points
■ Antineutrophil cytoplasmic autoantibodies (ANCAs) are associated with and probably cause pauci-immune systemic necrotizing small-vessel vasculitis and glomerulonephritis
■ ANCAs specific for proteinase 3 or myeloperoxidase occur with organ- limited disease, microscopic polyangiitis, granulomatosis with polyangiitis or eosinophilic granulomatosis with polyangiitis
■ ANCAs seem to cause vasculitis by activating circulating primed neutrophils and causing them to attach to, penetrate and damage vessel walls by undergoing respiratory burst, degranulation, NETosis, apoptosis and necrosis
■ ANCA-induced neutrophil activation also releases factors that activate the alternative complement pathway, which establishes a destructive inflammatory amplification loop that attracts and activates more neutrophils that, in turn, further activates the complement system
■ ANCA-associated granulomatosis might result from the same pathogenic sequence of events involving extravascular primed neutrophils and interstitial-fluid ANCAs, followed by a granulomatous reaction to wall off the resulting extravascular necrosis
with pauci-immune necrotizing glomerulonephritis, including patients who were positive for MPO-ANCA or PR3-ANCA and others who were negative for both. However, Roth et al.11 were unable to confirm this high frequency of LAMP-2-ANCA in these patients. Similarly, Kawakami et al. did not detect LAMP-2-ANCA in patients with MPA, although they did report evidence for LAMP-2-ANCA in some patients with cutaneous poly-arteritis nodosa12 and IgA vasculitis (formerly known as Henoch–Schönlein purpura).13 ANCAs also occur in patients with inflammatory bowel disease, and are detected by indirect immunofluorescence assay in ~60% of patients with ulcerative colitis and ~20% of those with Crohn disease.14–16 In this setting, ANCAs only rarely have specificity for PR3, MPO or elastase: the major autoantigens are catalase, α-enolase, lacto transferrin and bactericidal permeability-increasing protein.14–16 ANCA, usually MPO-ANCA, occurs in a small minor-ity of patients with systemic lupus erythe matosus who seem to to have vasculitic features of ANCA-associated disease.17 Approximately 30% of patients with anti-glomerular basement membrane disease have ANCA, usually MPO-ANCA.18
An important role for ANCAs in the pathogenesis of vasculitis and glomerulonephritis is supported by clinical evidence and by in vitro and in vivo experimental data (summarized in Box 1). The leading theory proposes that circulating neutrophils and monocytes that have been primed by inflammatory stimuli display ANCA antigens at or near the cell surface, and that interaction of these antigens with ANCAs results in neutrophil activation and initiation of vascular inflammation. An extension of this theory proposes that primed extravascular neutro-phils interact with interstitial ANCAs, causing necrotiz-ing inflammation and resultant reactive granulomatous inflammation. This Review summarizes observations that support these pathogenic theories as well as puta-tive mechanisms for the origin of the pathogenic ANCA autoimmune response.
Pathology of ANCA-associated diseaseAny valid theories about pathogenic mechanisms in ANCA-associated disease must explain the development of the observed pathologic lesions. The acute and chronic lesions described in this section provide guidance in formulating pathogenic theories.
Vasculitis and glomerulonephritisIn patients19–21 and experimental animal models,22 the acute vascular and extravascular lesions of ANCA-associated disease begin as neutrophil-rich necrotizing inflammation. In vessels, the earliest lesions have mar-gination and diapedesis of predominantly neutrophils with admixed monocytes (Figure 2a,b). Areas of segmen-tal vascular necrosis also develop perivascular infiltrates that initially have numerous neutrophils.
Within hours, neutrophils undergo apoptosis and necrosis (Figure 2a,b). The early destruction of neutro-phils by apoptosis and necrosis during ANCA-associated glomerulonephritis and vasculitis is supported by the
Medium-vessel vasculitisPolyarteritis nodosaKawasaki disease
Immune complex small-vessel vasculitisCryoglobulinemic vasculitis
IgA vasculitis (Henoch–Schönlein)Hypocomplementemic urticarial vasculitis
(Anti-C1q vasculitis)
ANCA-associated small-vessel vasculitisMicroscopic polyangiitis
Granulomatosis with polyangiitis (Wegener)Eosinophilic granulomatosis with polyangiitis (Churg–Strauss)
Large-vessel vasculitisTakayasu arteritisGiant cell arteritis
Anti-GBM disease
Figure 1 | Diagram depicting the predominant types of vessels affected by major categories of systemic vasculitis. Note that vasculitis that is associated with ANCAs can target a broad range of vessel types including medium and small arteries, arterioles, capillaries, venules and veins. Large arteries, such as main visceral arteries, are rarely affected by AAV. Thus, the types of vessels affected by AAV overlap with other variants of systemic vasculitis, which results in many overlapping clinical signs and symptoms of disease. Abbreviations: AAV, ANCA-associated vasculitis; ANCA, antineutrophil cytoplasmic antibody; GBM, glomerular basement membrane. Reproduced with permission from John Wiley & Sons, Inc. © Jennette, J. C. et al. Arthritis Rheum. 65, 1–11 (2013).
REVIEWS
© 2014 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | RHEUMATOLOGY VOLUME 10 | AUGUST 2014 | 465
frequent observation of leukocytoclasia (fragmentation of nuclei) at sites of acute fibrinoid necrosis (Figure 2d). Conspicuous leukocytoclasia with numerous nuclear fragments could result from the intensity of neutrophil infiltration or reduced clearance of neutrophil fragments, or both. Neutrophil cytoplasmic and nuclear constitu-ents, including neutrophil extracellular traps (NETs), are present at sites of inflammation and acute necro-sis.26–28 NETs comprise extracellular fibrillary material containing chromatin and granule proteins extruded by activated neutrophils.
Necrotizing injury to vessel walls results in haemor-rhage and release of plasma proteins into the vessel walls and adjacent extravascular tissue. These proteins include coagulation factors, which are activated by thrombogenic cellular and tissue debris, and tissue factor, which results in the formation of fibrin within areas of fibrinoid necro-sis (Figure 2c,d). Fibrin formation also might be facili-tated by tissue factor present in NETs.29 In glo meruli, foci of segmental fibroid necrosis develop adjacent cel-lular reactions (crescents) composed predominantly of monocytes, macrophages and activated epithelial cells (Figure 2d).
Within days, the initial acute neutrophil-rich inflam-mation and necrosis is replaced by inflammation with a predominance of monocytes and macrophages and, eventually, T cells (Figure 2c). Vascular and extravascu-lar inflammatory infiltrates also often contain eosino-phils, which are most numerous in EGPA. In glomerular lesions of ANCA-associated glomerulonephritis, at the time of biopsy, leukocytes are predominantly mono-cytes and macrophages with admixed T cells and usually only scant neutrophils.23–25 Within glomeruli in animal models of ANCA-associated disease, the neutrophils that are predominant during the first several days of
necrotizing inflammation are subsequently replaced by monocytes and macrophages.22
Within 1–2 weeks, vascular segments transition through the monocyte and/or macrophage-rich phase of inflammation to a phase of scarring that involves inter-stitial deposition of collagen. The extent of scarring, and the likelihood of return to normal structure and func-tion, depends on the severity and duration of the inflam-matory injury. Areas of mild segmental vascular injury can undergo complete remodelling to restore normal architecture, whereas severe vascular injury could result in irreversible total vascular occlusion.
GranulomatosisPatients with GPA and EGPA have nodular extra-vascu lar inflammatory lesions that contain numerous macro phages, often including multinucleated giant cells (Figure 3).19–21 In an early granulomatous pulmonary lesion, the centre is in essence a microabscess contain-ing neutrophils in varying stages of necrosis and apop-tosis, and the margin has a thin band of macrophages that are responding to the necrosis (Figure 3a). In a later stage of granulomatosis, the centre of the lesion contains amorphous necrotic debris that is walled off from the adjacent lung parenchyma by a well-defined band of epithelioid macrophages (macrophages with elongated nuclei and abundant acidophilic cytoplasm, resembling epithelial cells) (Figure 3b). At this stage, neutrophils are no longer conspicuous, and the granulomatous inflammation contains progressively more lymphoid cells including effector T cells, memory T cells, B cells, dendritic cells, macrophages and plasma cells.30 At a still-later stage, the necrotic debris is replaced by scar tissue, and lymphocytes, including organized lymphoid folli-cles, become components of the chronic granulo matous inflammation. End-stage lesions are predominantly scar tissue, often with no definitive histological features of the earlier granulomatous inflammation.
Genesis of the ANCA autoimmune responseThe evidence suggests that multiple genetic and environ-mental factors converge to induce the onset of ANCA-associated disease, and these factors have modulatory effects on the clinical and pathological phenotype of disease. These factors differ among patients; for example, in a given patient the pivotal aetiological event could be an infection, a drug, impaired immune regulation or dysregulation of genomic expression of autoantigens, or combinations of these and other factors.
Natural ANCAsAlthough Ehrlich described the horror of autotoxicus and Burnet theorized the elimination of ‘forbidden clones’, all healthy individuals seem to have numerous circulating autoantibodies with beneficial homeostatic functions.31 Thus, pathogenic autoimmunity might arise from dysregulation of homeostatic autoimmunity.
Healthy individuals have circulating autoantibodies against MPO and PR3.32–36 In asymptomatic indi viduals, such autoantibodies are often designated ‘natural’ or
Box 1 | Evidence that ANCAs are pathogenic
Clinical evidence ■ Strong association with ANCA (MPA >90%, GPA >90%, EGPA >40%*) ■ Partial correlation of ANCA titre with disease activity ■ Correlation of ANCA epitope specificity with disease activity (MPO-ANCA only) ■ Disease induction by transplacental transfer of ANCA (one MPO-ANCA case report) ■ Similar disease associated with drug-induced ANCA ■ HLA genetic associations with MPO-ANCA and PR3-ANCA-associated disease ■ Response to immunosuppressive therapy that targets B cells
In vitro evidence ■ Activation of cytokine-primed neutrophils by ANCA IgG ■ Endothelial injury by ANCA-activated neutrophils ■ Alternative complement pathway activation by ANCA-activated neutrophils
Evidence from animal models‡
■ Induction of pauci-immune vasculitis, glomerulonephritis and granulomatosis in mice and rats by anti-MPO IgG
■ Prevention of murine anti-MPO IgG-induced disease by deficiency of neutrophils ■ Prevention of murine anti-MPO IgG-induced disease by blockade of alternative
complement pathway activation or blockade of C5a receptors*More than 75% of patients with EGPA and glomerulonephritis have ANCA. ‡Convincing animal models of MPO-ANCA-associated disease have been described, but only less-convincing animal models of PR3-ANCA-associated disease have been described. Abbreviations: ANCA, antineutrophil cytoplasmic autoantibody; EGPA, eosinophilic granulomatosis with polyangiitis; GPA, granulomatosis with polyangiitis; MPA, microscopic polyangiitis; MPO, myeloperoxidase; PR3, proteinase 3.
FOCUS ON VASCULITIS
© 2014 Macmillan Publishers Limited. All rights reserved

466 | AUGUST 2014 | VOLUME 10 www.nature.com/nrrheum
nonpathogenic autoantibodies. Presumably, quanti-tative or qualitative differences determine autoantibody pathogenicity. Compared with pathogenic MPO-ANCA, natural MPO-ANCA has lower titres, lower avidity, less subclass diversity and less capability to activate neutro-phils in vitro.34 In autoimmune diseases that have auto-antigens with multiple epitope specificities, the epitope specificity of natural autoantibodies can differ from that of pathogenic autoantibodies. Roth et al.35 identified more than 20 MPO epitopes that can be recognized by MPO-ANCA in patients with ANCA-associated dis-ease. MPO-ANCA IgG from patients with active disease recognized the largest number of epitopes, including epitopes that were never recognized by MPO-ANCA IgG from patients with ANCA-associated disease in
remission or from healthy individuals. Healthy indi-viduals had very low titres of MPO-ANCA that recog-nized only a few MPO epitopes. Some patients with clinical and pathological features of ANCA-associated disease who were determined to be ANCA-negative using conventional clinical assays reacted with a specific MPO epitope when a highly sensitive epitope-excision method was used; this epitope was blocked from reacting with ANCA IgG in serum because of competitive binding by a fragment of ceruloplasmin, which is a natural inhibi-tor of MPO.35 Modulation of epitope specificity (epitope spreading) can be influenced by endogenous or exo-genous stimuli, causing nonpathogenic autoantibodies to become pathogenic.
The detection and characteristics of autoantibodies in asymptomatic individuals might be a predictor of sub-sequent development of disease. This predictive value has been evaluated using the US Department of Defense serum repository, which contains thousands of serum samples taken from healthy military service members at the time of enlistment as well as during their subsequent time in the military.36 When compared with indi viduals who did not develop GPA, a greater percentage of those with GPA had at least one elevated PR3-ANCA titre before diagnosis (63% versus 0%) and a greater rate of increase in titre (62% versus 0%). The rises in PR3-ANCA titre typically occurred before the onset of elevations in serum C-reactive protein level or signs and symptoms of GPA. These findings are consistent with the concept that endogenous or exogenous influences might modify quan-titative or qualitative characteristics of natural ANCAs to render them pathogenic.
Pathogenic ANCAsFactors that could induce the development of patho-genic ANCAs include exposure to exogenous anti-gens that influence ANCA epitope specificity (such as drugs or microbes), newly expressed or modified ANCA autoantigens (such as alternatively spliced tran-scripts or antisense transcripts), immunogenic display of ANCA autoantigens (for example, on apoptotic cells or NETs), or loss of effective suppression of the ANCA autoimmune response (for example, because of defec-tive T cells, B cells or myeloid-derived suppressor cells). This pathogenic transformation could be multifactorial, with genetic, environmental and immunological events conspiring to break autoimmune homeostasis.
Mapping of epitopes that are the targets of natural and pathogenic MPO-ANCAs has demonstrated that these two classes of epitopes occur in close proximity on the 3D structure of MPO.35 This finding suggests that epitope spreading of ANCA specificity, from nonpathogenic to pathogenic epitopes, occurs as disease develops.
Modulation of existing epitope specificities is known to occur during immune responses to infectious patho-gens, and several microorganisms have been implicated in the induction and modulation of ANCA-associated disease, such as Staphylococcus aureus37,38 and Ross River virus.39 A novel model for induction of the ANCA autoimmune response theorizes that the initial immune
a
c d
b
E L
A
A
N
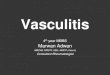
Figure 2 | Vascular and glomerular pathology of AAV. a | Leukocytoclastic venulitis in the nasal septal mucosa of a patient with PR3-ANCA-associated disease (magnification ×400, H&E staining) demonstrates features of early AAV lesions: numerous neutrophils (arrows) are marginating along and penetrating the wall of a venule, and accumulating in the perivascular interstitium, with some undergoing apoptosis and karyorrhexis (leukocytoclasia). b | Another venule from the same specimen demonstrates neutrophils in the lumen, marginating neutrophils, endothelial cells and apoptotic bodies derived from neutrophils (magnification ×1,000, H&E staining). c | Necrotizing arteritis of a small artery in the kidney of a patient with microscopic polyangiitis involves a circumferential zone of fibrinoid necrosis (arrow) and perivascular leukocytes that, at this phase, contain predominantly mononuclear leukocytes (magnification ×400, H&E staining). d | A glomerulus from a patient with ANCA-associated glomerulonephritis shows segmental fibrinoid necrosis (lower arrow) and an adjacent cellular crescent composed of mononuclear leukocytes and epithelial cells (upper arrow) (magnification ×400, H&E staining). Abbreviations: A, apoptotic bodies; AAV, ANCA-associated vasculitis; ANCA, antineutrophil cytoplasmic antibody; E, endothelial cells; H&E, haematoxylin and eosin; L, lumen; N, marginating neutrophils; PR3, proteinase 3.
REVIEWS
© 2014 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | RHEUMATOLOGY VOLUME 10 | AUGUST 2014 | 467
response is not against the autoantigen but rather a peptide that has a complementary structure relative to the auto antigen, and that the anti-idiotypic response to this initial immune response results in antibodies that recognize the autoantigen (Figure 4).40,41 Complementary
peptides have structures and physicochemical character-istics that give them affinity to bind together. A classic complementary peptide pair comprises the sense and antisense transcripts of a gene; however, peptide mimics of an antisense peptide are similarly complementary to the sense peptide. Codon-directed amino acids in sense peptides have specific pairwise interactions with the corresponding complementary amino acids in complementary peptides.42
An immune response to one complementary protein can result in the production of an immune response to the paired complementary protein; thus, immunization with an antisense complementary peptide can induce an antibody response to the sense peptide.42,43 Patients positive for PR3-ANCA have circulating antibodies reactive not only to PR3 sense peptides but also to PR3 complementary antisense peptides.40,41 In addition to antibodies that recognize complementary PR3 antigens, Yang et al.44 detected anticomplementary PR3-specific memory T cells—directed against a PR3 complementary peptide—in patients with PR3-ANCA. The stimulus for the antibodies to complementary PR3 could have been endogenous PR3 antisense peptides45 or exogenous pep-tides that mimic the antisense peptides, such as peptides brought in by commensal or pathogenic microbes.40 Interestingly, the bioinformatics software tool BLAST (basic local alignment search tool) identifies multiple microbial peptide homologues of complementary PR3, including peptides from microbes that are known to be associated with PR3-ANCAs such as Ross River virus and S. aureus.40,41
A genome-wide association study has indicated that different HLA specificities correlate with MPO-ANCA and PR3-ANCA, and a gene encoding PR3 was associ-ated with PR3-ANCA but not MPO-ANCA.7 These findings suggest that antigen-recognition capabilities are important in ANCA-associated disease, and that the initial antigen recognized by antigen-presenting cells is different in PR3-ANCA-associated disease as opposed to MPO-ANCA-associated disease. HLA specifi cities seemed to be involved in the ability of ANCA to recog-nize both sense and antisense antigen peptides.46 The HLA DRB1*15 allele is over-represented in African American patients with PR3-ANCA-associated disease (odds ratio 73.3).46 The DRB1*1501 protein binds with high affinity to both sense-PR3 peptide as well as the complementary antisense-PR3 peptide.46 This finding suggests that one factor in the induction of ANCA-associated disease could be the presence of HLA antigen- binding sites that recognize the autoantigen and a complementary protein.
Thus, the theory of autoantigen complementarity sug-gests that a patient with a genetically determined pre-disposing antigen-recognition capability could produce pathogenic ANCA as a result of an initial appropriate immune response against a microbial mimic of a com-plementary peptide, or against an endogenously pro-duced antisense transcript, that would be transformed into an autoimmune response by an anti-idiotypic res-ponse (Figure 4). In support of this theory, anti-idiotypic
a b
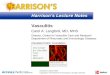
Figure 3 | Pathology of ANCA-associated necrotizing granulomatosis. a | The edge of an early acute pulmonary lesion in a patient with PR3-ANCA-positive GPA is characterized by a central zone of necrosis containing numerous neutrophils in varying stages of leukocytoclasia, and by an adjacent band of monocytes and macrophages (arrows) (magnification ×400, H&E staining). b | A later stage of granulomatous inflammation in the same pulmonary lesion specimen demonstrates a central zone of amorphous necrotic debris containing a few pyknotic leukocytes, and an adjacent marginal zone of epithelioid macrophages (arrows) (magnification ×400, H&E staining). Abbreviations: ANCA, antineutrophil cytoplasmic antibody; GPA, granulomatosis with polyangiitis; H&E, haematoxylin and eosin; PR3, proteinase 3.
Endogenous source
Exogenous source
Microbes
Neutrophil
Anti-idiotypicantibody
(autoantibody)
Mimic ofantisense peptide
Antisensetranscription
Sensetranscription
Sense DNAstrand
AntisenseDNA strand
ANCA antigenpeptide
Antisensepeptide
T cell
Idiotypicantibody
Idiotopemimicking theautoantigen
Figure 4 | Diagram of the induction of an ANCA-mediated autoimmune response by an initial immune response to a peptide that is complementary to an autoantigen peptide. This complementary peptide immunogen could arise from antisense transcription of the antisense strand of the autoantigen gene, or could be a mimic of an antisense peptide that is produced by a symbiotic or pathogenic microbe. The anticomplementary peptide antibody idiotopes would engender an anti-idiotypic antibody response that crossreacts with the autoantigen epitopes that are complementary to the initial immunogenic peptide. Abbreviation: ANCA, antineutrophil cytoplasmic antibody.
FOCUS ON VASCULITIS
© 2014 Macmillan Publishers Limited. All rights reserved

468 | AUGUST 2014 | VOLUME 10 www.nature.com/nrrheum
antibodies raised against autoantibodies have been shown in multiple animal models to induce anti- anti-idiotypic antibodies that possess characteristics of the initial autoantibodies and cause autoimmune disease.47
Induction of pathogenic ANCAs by microbial molecu-lar mimicry of autoantigens has been proposed as a cause for ANCAs with specificity for LAMP-2.10 The human LAMP-2 epitope has complete homology with the bacte-rial adhesin FimH, and human LAMP-2-ANCA cross-reacts with this microbial protein. Kain et al.10 reported that rats immunized with FimH develop antibodies to rat and human LAMP-2, and develop pauci-immune necrotizing glomerulonephritis that resembles human ANCA-associated glomerulonephritis. This study pro-poses that infection with fimbriated bac teria can cause an immune response against FimH that crossreacts with human LAMP-2 and mediates ANCA-associated disease. However, Roth et al.11 were not able to reproduce the findings from this experimental animal model.
Another exogenous stimulus that can induce a patho genic ANCA immune response is drugs, includ-ing hydralazine, minocycline, propylthiouracil and levamisole- adulterated cocaine.8,9 The mecha nisms by which drugs induce ANCAs could shed light on patho-genic mechanisms that do not involve drugs. Hydralazine-induced ANCA-associated disease is ac companied by dysregulation of ANCA-antigen expression by neutro-phils.8 Hydralazine is a DNA methylation inhibi tor that might reverse epigenetic silencing of PR3 and MPO, resulting in increased expression of both autoantigens in neutrophils. This increased autoantigen expression in drug-induced disease is similar to a phenomenon observed in patients with ANCA-associated disease who have abnormal epigenetically deregulated overexpres-sion of MPO and PR3 in neutrophils.48,49 Increased auto-antigen expression in neutrophils could either facilitate a loss of tolerance to these proteins, or enhance the activa-tion of neutrophils by ANCAs, or both. Organized lym-phoid configuration in areas of granulomatosis that bring together antigen-presenting cells with T cells and B cells,30 as well as effective presentation of neutrophil antigens on apoptotic neutrophils50,51 and NETs,27 could also augment ANCA autoimmune responses.
Regulation of the ANCA immune responseThe pathogenic ANCA autoimmune response seems to be enabled by impaired T-cell and B-cell suppression, and possibly by enhanced B-cell stimulation by ANCA-activated neutrophils. Patients with ANCA-associated disease have dysfunction of regulatory T (TREG) cells that could contribute to loss of tolerance and emergence of a pathogenic ANCA response.52–54 TREG cells are charac-terized by high expression of CD25 and FOXP3. Even though patients with active GPA have increased numbers of CD4+ CD25+ T cells, the numbers of FOXP3+ cells are decreased.52 The suppressive function of TREG cells from patients with ANCA-associated disease has been reported to be markedly decreased in active disease and more normal during remission.53 Free et al.54 described an increase in a proinflammatory suppression- resistant
effector CD4+ T-cell subset in patients with active ANCA-associated disease, in comparison with patients in remission and with healthy individuals. Although circulating TREG cell numbers were increased in active dis ease, these cells had decreased suppressive function because of expression of a FOXP3 isoform that lacks exon 2.54 A study by Wilde et al.55 showed that increased expression of the negative co-stimulator programmed cell death protein 1 (PD-1) on circulating T cells in patients with GPA might oppose T-cell activation; how-ever, T cells in renal lesions in these patients mostly lacked PD-1 expression.
B-cell regulation might also influence production of pathogenic ANCAs.56,57 B cells that have high expression of CD5 and produce IL-10 have regulatory capabilities. Patients with active ANCA-associated disease have a reduced percentage of circulating CD5+ B cells whereas most patients in remission have a normal percentage.52 In addition, the degree of normalization of circulating CD5+ B cells after therapy with rituximab correlates with more-persistent remission.56
ANCA-activated neutrophils might augment the production of ANCAs by stimulating B cells. Acti-vated neutrophils release ligands for B-cell-activating fac tor (BAFF; also known as TNF ligand superfamily mem ber 13B or B lymphocyte stimulator), which stimu-lates B-cell proliferation and inhibits apoptosis.58 Patients with ANCA-associated disease have serum levels of BAFF that are elevated during active disease and decline during remission.59–62
Thus, B-cell-stimulating factors released by ANCA-activated neutrophils along with permissive T-cell and B-cell regulation seem to facilitate the production of pathogenic ANCAs.
Pathogenesis of vascular inflammationNeutrophil and monocyte activation by ANCAsIn vitro studies have shown that both MPO-ANCA and PR3-ANCA IgG can activate neutrophils that have been primed by proinflammatory stimuli, such as TNF,63 bac-terial lipopolysaccharide64 or the complement anaphyla-toxin C5a.65 Priming causes neutrophils to release ANCA target antigens (for example, MPO and PR3) at the cell surface and into the microenvironment that can then interact with ANCAs. Full neutrophil activation results from engagement of constitutively expressed Fcγ recep-tors (FcγRs) by immune complexes containing ANCA and antigen66,67 and from binding of F(ab')2 fragments of ANCA to antigen expressed on neutrophil surfaces.68,69 Phosphorylation of p38 mitogen-activated protein kinase (p38 MAPK) and the extracellular signal-regulated kinase (ERK) are involved in neutrophil priming and activation, and blockade of MAPK prevents this priming and activation.70–72
ANCA-activated neutrophils generate a respiratory burst with production of toxic oxygen radicals, release des tructive enzymes through degranulation, and extrude NETs that have proinflammatory properties.27,28,63–74 These ANCA-activated cells have been shown to cause injury to and death of cultured monolayers of endo thelial
REVIEWS
© 2014 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | RHEUMATOLOGY VOLUME 10 | AUGUST 2014 | 469
cells.75–78 Release of NETs (a process referred to as NETosis) by ANCA-activated neutrophils27,28 contributes to endothelial injury and death.79
In considering pathogenic pathways in ANCA-associated disease, it is important to note that monocytes as well as neutrophils contain ANCA antigens (including PR3 and MPO) and can be activated in vitro by engage-ment of FcγRs by ANCA IgG.80,81 ANCA-activated monocytes release proinflammatory cytokines, includ-ing monocyte chemoattractant protein-1 (MCP-1, also known as CCL2)80 and IL-8.81 IL-8 attracts and activates neutrophils and thus could amplify neutrophil- mediated injury. MCP-1 attracts monocytes and macrophages and could participate in the transition of ANCA-induced vascular injury from predominantly neutrophil-rich inflammation to predominantly monocyte and/or macrophage-rich inflammation, including granulo-matous inflammation. Monocytes are conspicuous at sites of ANCA vascular inflammation,24 especially
after the first day or two, and there is evidence for sys-temic activation of monocytes in patients with active ANCA-associated disease.82
Induction of necrotizing vascular inflammationPathogenic mechanisms of ANCA-induced vascular inflammation must be in accord with observed lesions in tissue specimens from patients with ANCA-associated disease or in animal models. Earlier in this Review, we described the pathological features of AAV. The histo-pathology of the earliest acute vascular lesions reveals a very destructive localized neutrophil-rich necrotizing inflammation that quickly transforms into monocyte/macrophage-rich inflammation. Immunohistology reveals a paucity, but usually not an absence, of immuno-globulin at sites of inflammation. Small amounts of ANCA and ANCA-antigen are found at sites of vascular inflammation, including glomerulonephritis, in patients’ biopsies15,26,83 and in experimental animal models of ANCA-associated disease.84 In vitro studies have dem-onstrated that ANCA-induced neutrophil activation releases into the microenvironment ANCA-antigens that can bind to nearby structures to act as targets for in situ immune-complex formation.76 However, the amount of immunoglobulin deposited at sites of inflammation in ANCA-associated disease typically is far less than is seen with conventional forms of immune-complex-mediated vascular inflammation.1 This observation supports the concept that the vascular inflammation of ANCA-associated disease is caused primarily by direct activation of neutrophils and monocytes by ANCA, with somewhat incidental deposition of immune complexes containing ANCA and ANCA antigen at the sites of injury.
The most compelling evidence that ANCAs are pathogenic and the most informative experiments that elucidate the underlying pathogenic mechanisms come from animal models of ANCA-associated disease.85–87 Multiple convincing models of MPO-ANCA-associated dis ease have been described and confirmed.84–87 How-ever, no convincing models of PR3-ANCA-associated disease have been widely accepted, although several have been proposed.88–91
Mouse models of AAV and ANCA-associated glo-merulonephritis induced by anti-MPO antibodies have been used most extensively to elucidate pathogenic mechanisms.64,65,71,84,92–98 Disease can be induced by injecting mouse anti-MPO IgG into immunocompetent or immunodeficient mice,84 injecting splenocytes con-taining anti-MPO B cells into immunodeficient mice,84 or transplanting bone marrow that contains MPO-positive myeloid cells into MPO-knockout mice.93 In these models, a pathogenic level of anti-MPO antibodies induces necrotizing and crescentic glomerulonephritis in all mice of susceptible strains, and systemic necrotiz-ing small-vessel vasculitis and granulomatous inflam-mation in some, but not all, animals. The inflammatory lesions in these mouse models closely mimic human ANCA-associated disease.
Several conclusions can be drawn from experiments using mouse models of MPO-ANCA-associated disease:
C5aC5a receptorCytokineCytokinereceptor
Neutrophil
Apoptotic body
Macrophage
Monocyte
Unprimedneutrophil
Priming
Activation
Alternativepathway
activation
NETosis
Acutein�ammation
Chronic in�ammationand scarring
ANCA antigen
ANCA
Fc receptor
T cell
Fibroblast
Fibrin
Collagen
Epithelial cell
Figure 5 | Putative sequence of pathogenic events in ANCA-mediated vasculitis. Circulating neutrophils are primed for activation by ANCA by inflammatory cytokines or C5a derived from complement activation (note that monocytes can be similarly primed and activated but are not illustrated). Primed neutrophils release ANCA antigens at the cell surface and into the microenvironment, where they interact with ANCA. Fc receptor engagement by ANCA bound to ANCA antigens as well as F(ab')2 binding to ANCA antigens on neutrophil surfaces cause neutrophil activation. ANCA-activated neutrophils release factors that activate the alternative complement pathway, generating C5a. C5a and ANCA create an inflammatory amplification loop, with C5a attracting and priming more neutrophils for activation by ANCA, which causes, in turn, further activation of the alternative complement pathway and production of more C5a. ANCA-activated neutrophils marginate and penetrate vessel walls and undergo respiratory burst, degranulation, NETosis, apoptosis and necrosis. Disruption of endothelium allows plasma to spill into vascular and perivascular tissue where activation of the coagulation cascade produces the fibrin strands of fibroid necrosis. The innate inflammatory response orchestrates the conversion of the initial acute neutrophil-rich inflammation into mononuclear leukocyte-rich inflammation and subsequent collagen deposition and fibrosis. Abbreviation: ANCA, antineutrophil cytoplasmic antibody.
FOCUS ON VASCULITIS
© 2014 Macmillan Publishers Limited. All rights reserved

470 | AUGUST 2014 | VOLUME 10 www.nature.com/nrrheum
antibody to MPO alone (in the absence of functional T cells) is sufficient to cause acute disease;84 bone- marrow-derived cells are sufficient and necessary to induce disease;92 neutrophils are required;92 genetic back-ground determines the susceptibility to and severity of dis ease;94 circulating proinflammatory factors exacer bate dis ease;64 and activation of the alternative complement path way is required to induce vascular inflammation.96 Studies of these mouse models also showed that disease can be prevented or ameliorated by hydrolysis of anti-MPO IgG glycans, which affects FcγR–antibody inter-actions;95 by inhibition of p38 MAPK, which prevents priming of neutrophils by inflammatory stimuli;71 and by blockade of C597 or C5a receptor,65,98 which prevents activation of the alternative complement pathway.
Evidence from animal models of the involvement of alternative complement pathway activation in the patho-genesis of ANCA-associated disease prompted studies to
identify supportive evidence in human disease. Exami-nation of glomerular and vascular inflammatory lesions in biopsy specimens from patients with ANCA-associated dis ease revealed markers of alternative complement path-way activation including factor B and properdin, as well as factors shared by the classical and alternative path-ways including C3d and membrane attack complex, but the absence of components of the classical and lectin path ways such as C4d and mannose-binding lectin.99 Although not yet substantiated by other investigators, one research group has reported evidence of alternative complement pathway activation in patients with active ANCA-associated disease, including elevated plasma levels of C3a, C5a, soluble C5b-9, and Bb; reduced levels of properdin; and normal levels of C4d.100,101
On the basis of observations in experimental animal models and supportive findings in patients, a pathogenic scenario can be proposed for the interaction of patho-genic ANCAs with neutrophils that have been primed by a synergistic proinflammatory condition (Figure 5). Circulating neutrophils are primed by, for example, inflammatory cytokines or C5a derived from com-plement activation. Primed neutrophils release small amounts of ANCA antigens at the cell surface and in the micro environ ment, where these antigens can inter-act with ANCAs. FcγR engagement by ANCAs bound to ANCA antigens as well as F(ab')2 binding to ANCA antigens expressed on neutrophil surfaces cause neu-trophil activation. ANCA-activated neutrophils release factors that activate the alternative complement pathway with generation of C5a. Neutrophils, C5a and ANCAs create an inflammatory amplification loop, with C5a attracting and priming more neutrophils for activation by ANCAs, which in turn causes further activation of the alternative complement pathway and consequent production of more C5a. ANCA-activated neutrophils marginate and penetrate vessel walls, and undergo res-piratory burst, degranulation, NETosis, apoptosis and necrosis. Disruption of endo thelium enables plasma to spill into vascular and perivascular tissue where acti-vation of the coagulation cascade produces the fibrin strands of fibroid necrosis. Modulated by the severity and reversibility of the acute injury, the innate inflammatory response orchestrates the conversion of the acute inflam-mation into mononuclear-leukocyte-rich inflammation and subsequent fibrosis.
Pathogenesis of granulomatosisThere has been substantial controversy over the nature of the granulomatosis seen in GPA and EGPA. The term ‘granulomatosis’ has been used to describe the multiple foci of extravascular inflammation that were described initially by Klinger102 and Wegener103,104 in GPA, and by Churg and Strauss in EGPA.105 Controversy over the pathogenesis of this granulomatous inflammation derives from the fact that it can arise from at least two distinct pathways—one initiated by a T-cell mediated (type IV) immune response specific for PR3 or MPO, and another by an antigen-independent innate response of macro-phages to something in the tissue that needs to be
Unprimedneutrophils
Activation
Microabscessformation
Granulomatosis
Priming
C5aC5a receptorCytokineCytokinereceptor
Neutrophil
Macrophage
Monocyte
ANCA antigen
ANCA
Fc receptor
T cell
Multinucleatedgiant cell
Fibrin
Figure 6 | Putative sequence of pathogenic events in ANCA-mediated necrotizing granulomatosis. An inflammatory prodrome, such as an infectious or allergic inflammatory respiratory tract disease, positions increased numbers of primed neutrophils in extravascular interstitial tissue. ANCA immunoglobulin in the interstitial fluid would activate primed neutrophils and initiate an inflammatory amplification loop that would attract and activate more neutrophils, resulting in the formation of a necrotizing microabscess. This acute inflammation and necrosis would initiate an innate inflammatory response that would wall off the necrotic zone with granulomatous inflammation containing a predominance of monocytes and macrophages with admixed lymphocytes. Abbreviation: ANCA, antineutrophil cytoplasmic antibody.
REVIEWS
© 2014 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | RHEUMATOLOGY VOLUME 10 | AUGUST 2014 | 471
walled off.106 The latter pathway is an exaggerated version of the innate monocyte and macrophage response that closely follows any acute inflammatory event. Although many investigators have proposed that ANCA-associated granulomatosis is caused by an antigen-specific type IV adaptive immune response, we favour the theory that the granulomatosis is an innate inflammatory response to acute extravascular inflammation that is initiated by ANCA-induced neutrophil activation.
The concept that the granulomatosis of GPA is a res ponse to acute neutrophil-mediated necrosis is not new. For example, based on careful histopathological examination of lesions in patients with GPA and EGPA, Fienberg and his associates concluded that “micro-necrosis, usually with neutrophils (microabscesses), constitutes the early phase in the development of the pathognomonic organized palisading granuloma”.21 Lungs of patients with active GPA and EGPA often have a range of granulomatous lesions, from acute lesions with central microabscesses (Figure 3a) or subacute lesions with central necrosis (Figure 3b) to chronic lesions with a central zone of scarring and chronic inflammation.20 Chronic lesions contain substantial accumulations of lymphocytes and dendritic cells, including T cells and B cells with specificity for ANCA antigens that could be a source for autoantibody production.108
On the basis of this apparent sequence of pathologi-cal events, and the knowledge that ANCA IgG activates primed neutrophils, even in vitro, a reasonable hypothesis is that if an inflammatory condition (perhaps infection in GPA and allergy in EGPA) positions primed neutrophils in the extravascular tissue (for example, the submucosa of the respiratory tract), these primed neutrophils would be activated by ANCA IgG in the interstitial fluid of a
patient with circulating ANCAs. ANCA-induced neutro-phil activation, possibly fuelled by activation of the alter-native complement path way, would induce microabscess formation that, in turn, would engender a granulomatous reaction to wall off the zone of necrosis (Figure 6).
ConclusionsPauci-immune necrotizing small-vessel vasculitis and extra vascular granulomatosis are associated with, and might be caused by, ANCAs. The distinctive, extremely des tructive necrotizing vascular inflammation of AAV seems to be fuelled by an amplification loop in which ANCA-activated neutrophils activate the alterna-tive complement pathway, which, in turn, leads to the attraction and activation of more neutrophils. Promising therapies are those that can target one or multiple com-ponents of this vicious cycle (for example ANCAs, ANCA antigens, neutrophil activation and complement activation). The pathogenesis of ANCA-associated necrotizing extra vascular granulomatous inflammation is not known, but might be fuelled by the same inflam-matory amplification loop occurring in the extravas-cular compartment, in volving primed neutrophils and interstitial ANCAs.
Review criteria
This Review is based primarily on full-text, peer-reviewed, English-language medical literature from the 1980s into 2014 reporting on vasculitis and glomerulonephritis caused by antineutrophil cytoplasmic autoantibodies, as well as the authors’ knowledge of the field acquired over more than 30 years of involvement in research on glomerulonephritis and vasculitis.
1. Jennette, J. C. et al. Revised International Chapel Hill Consensus Conference nomenclature of vasculitides. Arthritis Rheum. 65, 1–11 (2013).
2. Falk, R. J. & Jennette, J. C. Anti-neutrophil cytoplasmic autoantibodies with specificity for myeloperoxidase in patients with systemic vasculitis and idiopathic necrotizing and crescentic glomerulonephritis. N. Engl. J. Med. 318, 1651–1657 (1988).
3. Goldschmeding, R. et al. Wegener’s granulomatosis autoantibodies identify a novel diisopropylfluorophosphate-binding protein in the lysosomes of normal human neutrophils. J. Clin. Invest. 4, 1577–1579 (1988).
4. Niles, J. L., McCluskey, T., Ahmad, M. F. & Amin Arnaout, M. A. Wegener’s granulomatosis autoantigen is a novel neutrophil serine proteinase. Blood 74, 1888–1893 (1989).
5. Jennette, J. C., Hoidal, J. H. & Falk, R. J. Specificity of anti-neutrophil cytoplasmic autoantibodies for proteinase 3. Blood 75, 2263–2264 (1990).
6. Lionaki, S. et al. Classification of antineutrophil cytoplasmic autoantibody vasculitides: the role of antineutrophil cytoplasmic autoantibody specificity for myeloperoxidase or proteinase 3 in disease recognition and prognosis. Arthritis Rheum. 64, 3452–3462 (2012).
7. Lyons, P. A. et al. Genetically distinct subsets within ANCA-associated vasculitis. N. Engl. J. Med. 367, 214–223 (2012).
8. Pendergraft, W. F. 3rd & Niles, J. L. Trojan horses: drug culprits associated with antineutrophil cytoplasmic autoantibody (ANCA) vasculitis. Curr. Opin. Rheumatol. 26, 42–49 (2014).
9. Graf, J. Rheumatic manifestations of cocaine use. Curr. Opin. Rheumatol. 25, 50–55 (2013).
10. Kain, R. et al. Molecular mimicry in pauci-immune focal necrotizing glomerulonephritis. Nat. Med. 14, 1088–1096 (2008).
11. Roth, A. J. et al. Anti-LAMP-2 antibodies are not prevalent in patients with antineutrophil cytoplasmic autoantibody glomerulonephritis. J. Am. Soc. Nephrol. 23, 545–555 (2012).
12. Kawakami, T., Ishizu, A., Arimura,Y. & Soma, Y. Serum anti-lysosomal-associated membrane protein-2 antibody levels in cutaneous polyarteritis nodosa. Acta Derm. Venereol. 93, 70–73 (2013).
13. Kawakami, T., Takeuchi, S., Arimura, Y. & Soma, Y. Elevated antilysosomal-associated membrane protein-2 antibody levels in patients with adult Henoch-Schönlein purpura. Br. J. Dermatol. 166, 1206–1212 (2012).
14. Roozendaal, C. et al. Does analysis of the antigenic specificities of anti-neutrophil cytoplasmic antibodies contribute to their clinical significance in the inflammatory bowel diseases? Scand. J. Gastroenterol. 34, 1123–1131 (1999).
15. Ooi, C. J., Lim, B. L., Cheong, W. K., Ling, A. E. & Ng, H. S. Antineutrophil cytoplasmic antibodies
(ANCAs) in patients with inflammatory bowel disease show no correlation with proteinase 3, lactoferrin, myeloperoxidase, elastase, cathepsin G and lysozyme: a Singapore study. Ann. Acad. Med. Singapore 29, 704–707 (2000).
16. Mahler, M. et al. PR3-ANCA: a promising biomarker for ulcerative colitis with extensive disease. Clin. Chim. Acta. 424, 267–273 (2013).
17. Hervier, B. et al. Systemic lupus erythematosus associated with ANCA-associated vasculitis: an overlapping syndrome? Rheumatol. Int. 32, 3285–3290 (2012).
18. Levy, J. B., Hammad, T., Coulthart, A., Dougan, T. & Pusey, C. D. Clinical features and outcome of patients with both ANCA and anti-GBM antibodies. Kidney Int. 66, 1535–1540 (2004).
19. Jennette, J. C. & Thomas, D. B. in Heptinstall’s Pathology of the Kidney 6th edn (eds Jennette, J. C. et al.) 643–674 (Lippincott Williams & Wilkins, 2007).
20. Jennette, J. C. Nomenclature and classification of vasculitis: lessons learned from granulomatosis with polyangiitis (Wegner’s granulomatosis). Clin. Exp. Immunol. 164 (Suppl. 1), 7–10 (2011).
21. Mark, E. J., Matsubara, O., Tan-Liu, N. S. & Fienberg, R. The pulmonary biopsy in the early diagnosis of Wegener’s (pathergic) granulomatosis: a study based on 35 open lung biopsies. Hum. Pathol. 19, 1065–1071 (1988).
22. Jennette, J. C., Xiao, H., Falk, R. & Gasim, A. M. Experimental models of vasculitis and
FOCUS ON VASCULITIS
© 2014 Macmillan Publishers Limited. All rights reserved

472 | AUGUST 2014 | VOLUME 10 www.nature.com/nrrheum
glomerulonephritis induced by antineutrophil cytoplasmic autoantibodies. Contrib. Nephrol. 169, 211–220 (2011).
23. Rastaldi, M. P. et al. Glomerular monocyte-macrophage features in ANCA-positive renal vasculitis and cryoglobulinemic nephritis. J. Am. Soc. Nephrol. 11, 2036–2043 (2000).
24. Weidner, S., Carl, M., Riess, R. & Rupprecht, H. D. Histologic analysis of renal leukocyte infiltration in antineutrophil cytoplasmic antibody-associated vasculitis: importance of monocyte and neutrophil infiltration in tissue damage. Arthritis Rheum. 50, 3651–3657 (2004).
25. Cunningham, M. A. et al. Prominence of cell-mediated immunity effectors in “pauci-immune” glomerulonephritis. J. Am. Soc. Nephrol. 10, 499–506 (1999).
26. Bajema, I. M., Hagen, E. C., de Heer, E., van der Woude, F. J. & Bruijn, J. A. Colocalization of ANCA-antigens and fibrinoid necrosis in ANCA-associated vasculitis. Kidney Int. 60, 2025–2030 (2001).
27. Kessenbrock, K. et al. Netting neutrophils in autoimmune small-vessel vasculitis. Nat. Med. 15, 623–625 (2009).
28. Abreu-Velez, A. M., Smith, J. G. Jr & Howard, M. S. Presence of neutrophil extracellular traps and antineutrophil cytoplasmic antibodies associated with vasculitides. North Am. J. Med. Sci. 1, 309–313 (2009).
29. Kambas, K. et al. Tissue factor expression in neutrophil extracellular traps and neutrophil derived microparticles in antineutrophil cytoplasmic antibody associated vasculitis may promote thromboinflammation and the thrombophilic state associated with the disease. Ann. Rheum. Dis. http://dx.doi.org/10.1136/annrheumdis-2013-203430 (2013).
30. Lamprecht, P. & Gross, W. L. Current knowledge on cellular interactions in the WG-granuloma. Clin. Exp. Rheumatol. 25 (Suppl. 44), S49–S51 (2007).
31. Jennette, J. C. & Falk, R. J. The rise and fall of horror autotoxicus and forbidden clones. Kidney Int. 78, 533–535 (2010).
32. Cui, Z., Zhao, M. H., Segelmark, M. & Hellmark, T. Natural autoantibodies to myeloperoxidase, proteinase 3, and the glomerular basement membrane are present in normal individuals. Kidney Int. 78, 590–597 (2010).
33. Olson, S. W. et al. Asymptomatic autoantibodies associate with future anti-glomerular basement membrane disease. J. Am. Soc. Nephrol. 22, 1946–1952 (2011).
34. Xu, P. C., Cui, Z., Chen, M., Hellmark, T. & Zhao, M. H. Comparison of characteristics of natural autoantibodies against myeloperoxidase and anti-myeloperoxidase autoantibodies from patients with microscopic polyangiitis. Rheumatology (Oxford) 50, 1236–1243 (2011).
35. Roth, A. J. et al. ANCA epitope specificity determines pathogenicity, detectability and clinical predictive value. J. Clin. Invest. 123, 1773–1783 (2013).
36. Olson, S. W. et al. Relation between asymptomatic proteinase 3 antibodies and future granulomatosis with polyangiitis. Clin. J. Am. Soc. Nephrol. 8, 1312–1318 (2013).
37. Popa, E. R., Stegeman, C. A., Kallenberg, C. G. & Tervaert, J. W. Staphylococcus aureus and Wegener’s granulomatosis. Arthritis Res. 4, 77–79 (2002).
38. Laudien, M. et al. Nasal carriage of Staphylococcus aureus and endonasal activity in Wegener’s granulomatosis as compared to rheumatoid arthritis and chronic rhinosinusitis
with nasal polyps. Clin. Exp. Rheumatol. 28 (Suppl. 57), 51–55 (2010).
39. Davies, D. J., Moran, J. E., Niall, J. F. & Ryan, G. B. Segmental necrotizing glomerulonephritis with antineutrophil antibody: possible arbovirus aetiology? Br. Med. J. (Clin. Res. Ed.) 285, 606 (1982).
40. Pendergraft, W. F. et al. Autoimmunity is triggered by cPR-3(105–201), a protein complementary to the autoantigen proteinase 3. Nat. Med. 10, 72–79 (2004).
41. Preston, G. A., Pendergraft, W. F. 3rd & Falk, R. J. New insights that link microbes with the generation of antineutrophil cytoplasmic autoantibodies: the theory of autoantigen complementarity. Curr. Opin. Nephrol. Hypertens. 14, 217–222 (2005).
42. Heal, J. R., Roberts, G. W., Raynes, J. G., Bhakoo, A. & Miller, A. D. Specific interactions between sense and complementary peptides: the basis for the proteomic code. Chembiochem. 3, 136–151 (2002).
43. Mekler, L. B. On the specific mutual interaction of amino acid residues of polypeptide chains and amino acid residues with codons. Oncology 27, 286–288 (1973).
44. Yang, J. J. et al. ANCA patients have T cells responsive to complementary PR-3 autoantigen. Kidney Int. 74, 1159–1169 (2008).
45. Badhwar, A. K., Simmons, J., Jennette, J. C., Falk, R. J. & Preston, G. A. Characterization of an antisense transcript from the proteinase-3 gene locus in patients with ANCA-vasculitis utilizing strand-specific RT-PCR and 5'RACE [abstract]. J. Am. Soc. Nephrol. 19, 188A (2008).
46. Cao, Y. et al. DRB1*15 allele is a risk factor for PR3-ANCA disease in African Americans. J. Am. Soc. Nephrol. 22, 1161–1167 (2011).
47. Shoenfeld, Y. Idiotypic induction of autoimmunity: a new aspect of the idiotypic network. FASEB J. 8, 1296–1301 (1994).
48. Yang, J. J. et al. Circumvention of normal constraints on granule protein gene expression in peripheral blood neutrophils and monocytes of patients with antineutrophil cytoplasmic autoantibody-associated glomerulonephritis. J. Am. Soc. Nephrol. 15, 2103–2114 (2004).
49. Ciavatta, D. J. et al. Epigenetic basis for aberrant upregulation of autoantigen genes in humans with ANCA vasculitis. J. Clin. Invest. 120, 3209–3219 (2010).
50. Durant, S. et al. Apoptosis-induced proteinase 3 membrane expression is independent from degranulation. J. Leukoc. Biol. 75, 87–98 (2004).
51. Kantari, C. et al. Proteinase 3, the Wegener autoantigen, is externalized during neutrophil apoptosis: evidence for a functional association with phospholipid scramblase 1 and interference with macrophage phagocytosis. Blood 110, 4086–4095 (2007).
52. Morgan, M. D. et al. Patients with Wegener’s granulomatosis demonstrate a relative deficiency and functional impairment of T-regulatory cells. Immunology 130, 64–73 (2010).
53. Rimbert, M. et al. Decreased numbers of blood dendritic cells and defective function of regulatory T cells in antineutrophil cytoplasmic antibody-associated vasculitis. PLoS ONE 6, e18734 (2011).
54. Free, M. E. et al. Patients with antineutrophil cytoplasmic antibody-associated vasculitis have defective TREG cell function exacerbated by the presence of a suppression-resistant effector cell population. Arthritis Rheum. 65, 1922–1933 (2013).
55. Wilde, B et al. Aberrant expression of the negative costimulator PD-1 on T cells in granulomatosis with polyangiitis. Rheumatology (Oxford) 7, 1188–1197 (2012).
56. Bunch, D. O. et al. Decreased CD5+ B cells in active ANCA vasculitis and relapse after rituximab. Clin. J. Am. Soc. Nephrol. 8, 382–391 (2013).
57. Wilde B. et al. Regulatory B cells in ANCA-associated vasculitis. Ann. Rheum. Dis. 72, 1416–1419 (2013).
58. Scapini, P., Bazzoni, F. & Cassatella, M. A. Regulation of B-cell-activating factor (BAFF)/B lymphocyte stimulator (BLyS) expression in human neutrophils. Immunol. Letters 116, 1–6 (2008).
59. Krumbholz, M. et al. BAFF is elevated in serum of patients with Wegener’s granulomatosis. J. Autoimmun. 25, 298–302 (2005).
60. Sanders, J. S., Huitma, M. G., Kallenberg, C. G. & Stegeman, C. A. Plasma levels of soluble interleukin 2 receptor, soluble CD30, interleukin 10 and B cell activator of the tumour necrosis factor family during follow-up in vasculitis associated with proteinase 3-antineutrophil cytoplasmic antibodies: associations with disease activity and relapse. Ann. Rheum. Dis. 65, 1484–1489 (2006).
61. Nagai, M. et al. Serum levels of BAFF and APRIL in myeloperoxidase anti-neutrophil cytoplasmic autoantibody-associated renal vasculitis: association with disease activity. Nephron Clin. Pract. 118, c339–c345 (2011).
62. Bader, L., Koldingsnes, W. & Nossent, J. B-lymphocyte activating factor levels are increased in patients with Wegener’s granulomatosis and inversely correlated with ANCA titer. Clin. Rheumatol. 29, 1031–1035 (2010).
63. Falk, R. J., Terrell, R. S., Charles, L. A. & Jennette, J. C. Anti-neutrophil cytoplasmic autoantibodies induce neutrophils to degranulate and produce oxygen radicals in vitro. Proc. Natl Acad. Sci. USA 87, 4115–4119 (1990).
64. Huugen, D. et al. Aggravation of anti-myeloperoxidase antibody induced glomerulonephritis by bacterial lipopolysaccharide: role of tumor necrosis factor α. Am. J. Pathol. 167, 47–58 (2005).
65. Schreiber, A. et al. C5a receptor mediates neutrophil activation and ANCA-induced glomerulonephritis. J. Am. Soc. Nephrol. 20, 289–298 (2009).
66. Porges, A. J. et al. Anti-neutrophil cytoplasmic antibodies engage and activate human neutrophils via Fcγ RIIa. J. Immunol. 153, 1271–1280 (1994).
67. Kocher, M., Siegel, M. E., Edberg, J. C. & Kimberly, R. P. Cross-linking of Fcγ receptor IIa and Fcγ receptor IIIb induces different proadhesive phenotypes on human neutrophils. J. Immunol. 159, 3940–3948 (1997).
68. Kettritz, R., Jennette, J. C. & Falk, R. J. Cross-linking of ANCA-antigens stimulates superoxide release by human neutrophils. J. Am. Soc. Nephrol. 8, 386–394 (1997).
69. Williams, J. M. et al. Activation of the Gi heterotrimeric G protein by ANCA IgG F(ab')2 fragments is necessary but not sufficient to stimulate the recruitment of those downstream mediators used by intact ANCA IgG. J. Am. Soc. Nephrol. 14, 661–669 (2003).
70. Kettritz, R., Schreiber, A., Luft, F. C. & Haller, H. Role of mitogen-activated protein kinases in activation of human neutrophils by antineutrophil cytoplasmic antibodies. J. Am. Soc. Nephrol. 12, 37–46 (2001).
REVIEWS
© 2014 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | RHEUMATOLOGY VOLUME 10 | AUGUST 2014 | 473
71. van der Veen, B. S. et al. Effects of p38 mitogen-activated protein kinase inhibition on anti-neutrophil cytoplasmic autoantibody pathogenicity in vitro and in vivo. Ann. Rheum. Dis. 70, 356–365 (2011).
72. Hao, J., Meng, L. Q., Xu, P. C., Chen, M. & Zhao, M. H. p38MAPK, ERK and PI3K signaling pathways are involved in C5a-primed neutrophils for ANCA-mediated activation. PLoS ONE 7, e38317 (2012).
73. Charles, L. A., Caldas, M. L., Falk, R. J., Terrell, R. S. & Jennette, J. C. Antibodies against granule proteins activate neutrophils in vitro. J. Leukoc. Biol. 50, 539–546 (1991).
74. Csernok, E., Ernst, M., Schmitt, W., Bainton, D. F. & Gross, W. L. Activated neutrophils express proteinase 3 on their plasma membrane in vitro and in vivo. Clin. Exp. Immunol. 95, 244–250 (1994).
75. Ewert, B. H., Jennette, J. C. & Falk, R. J. Anti-myeloperoxidase antibodies stimulate neutrophils to damage human endothelial cells. Kidney Int. 41, 375–383 (1992).
76. Savage, C. O., Gaskin, G., Pusey, C. D. & Pearson, J. D. Myeloperoxidase binds to vascular endothelial cells, is recognized by ANCA and can enhance complement dependent cytotoxicity. Adv. Exp. Med. Biol. 336, 121–123 (1993).
77. Ewert, B. H., Becker, M. E., Jennette, J. C. & Falk, R. J. Antimyeloperoxidase antibodies induce neutrophil adherence to cultured human endothelial cells. Ren. Fail. 17, 125–133 (1995).
78. Lu, X., Garfield, A., Rainger, G. E., Savage, C. O. & Nash, G. B. Mediation of endothelial cell damage by serine proteases, but not superoxide released from antineutrophil cytoplasmic antibody-stimulated neutrophils. Arthritis Rheum. 54, 1619–1628 (2006).
79. Gupta, A. K. et al. Activated endothelial cells induce neutrophil extracellular traps and are susceptible to NETosis-mediated cell death. FEBS Letters 584, 3193–3197 (2010).
80. Casselman, B. L., Kilgore, K. S., Miller, B. F. & Warren, J. S. Antibodies to neutrophil cytoplasmic antigens induce monocyte chemoattractant protein-1 secretion from human monocytes. J. Lab. Clin. Med. 126, 495–502 (1995).
81. Ralston, D. R., Marsh, C. B., Lowe, M. P. & Wewers, M. D. Antineutrophil cytoplasmic antibodies induce monocyte IL-8 release. Role of surface proteinase-3, α1-antitrypsin, and Fcγ receptors. J. Clin. Invest. 100, 1416–1424 (1997).
82. Muller Kobold, A. C., Kallenberg, C. G. & Tervaert, J. W. Monocyte activation in patients
with Wegener’s granulomatosis. Ann. Rheum. Dis. 58, 237–245 (1999).
83. Arimura, Y. et al. The role of myeloperoxidase and myeloperoxidase-antineutrophil cytoplasmic antibodies (MPO-ANCAs) in the pathogenesis of human MPO-ANCA-associated glomerulonephritis. Clin. Exp. Nephrol. 17, 634–637 (2013).
84. Xiao, H. et al. Antineutrophil cytoplasmic autoantibodies specific for myeloperoxidase cause glomerulonephritis and vasculitis in mice. J. Clin. Invest. 110, 955–963 (2002).
85. Jennette, J. C., Xiao, H., Falk, R. & Gasim, A. M. Experimental models of vasculitis and glomerulonephritis induced by antineutrophil cytoplasmic autoantibodies. Contrib. Nephrol. 169, 211–220 (2011).
86. van Timmeren, M. M. & Heeringa, P. Pathogenesis of ANCA-associated vasculitis: recent insights from animal models. Curr. Opin. Rheumatol. 24, 8–14 (2012).
87. Salama, A. D. & Little, M. A. Animal models of antineutrophil cytoplasm antibody-associated vasculitis. Curr. Opin. Rheumatol. 24, 1–7 (2012).
88. van der Geld, Y. M. et al. Rats and mice immunized with chimeric human/mouse proteinase 3 produce autoantibodies to mouse Pr3 and rat granulocytes. Ann. Rheum. Dis. 66, 1679–1682 (2007).
89. Pfister, H. et al. Antineutrophil cytoplasmic autoantibodies against the murine homolog of proteinase 3 (Wegener autoantigen) are pathogenic in vivo. Blood 104, 1411–1418 (2004).
90. Primo, V. C. et al. Anti-PR3 immune responses induce segmental and necrotizing glomerulonephritis. Clin. Exp. Immunol. 159, 327–337 (2010).
91. Little, M. A. et al. Anti-proteinase 3 anti-neutrophil cytoplasm autoantibodies recapitulate systemic vasculitis in mice with a humanized immune system. PLoS ONE 7, e28626 (2012).
92. Xiao, H. et al. The role of neutrophils in the induction of glomerulonephritis by anti-myeloperoxidase antibodies. Am. J. Pathol. 167, 39–45 (2005).
93. Schreiber, A., Xiao, H., Falk, R. J. & Jennette, J. C. Bone marrow-derived cells are sufficient and necessary targets to mediate glomerulonephritis and vasculitis induced by anti-myeloperoxidase antibodies. J. Am. Soc. Nephrol. 17, 3355–3364 (2006).
94. Xiao, H. et al. Genetically determined severity of anti-myeloperoxidase glomerulonephritis. Am. J. Pathol. 8, 139–160 (2013).
95. van Timmeren, M. M. et al. IgG glycan hydrolysis attenuates ANCA-mediated glomerulonephritis. J. Am. Soc. Nephrol. 21, 1103–1114 (2010).
96. Xiao, H., Schreiber, A., Heeringa, P., Falk, R. J. & Jennette, J. C. Alternative complement pathway in the pathogenesis of disease mediated by antineutrophil cytoplasmic autoantibodies. Am. J. Pathol. 170, 52–64 (2007).
97. Huugen, D. et al. Inhibition of complement factor C5 protects against anti-myeloperoxidase antibody-mediated glomerulonephritis in mice. Kidney Int. 71, 646–654 (2007).
98. Xiao, H. et al. C5a receptor (CD88) blockade protects against MPO-ANCA glomerulonephritis. J. Am. Soc. Nephrol. 25, 225–231 (2014).
99. Xing, G. Q. et al. Complement activation is involved in renal damage in human antineutrophil cytoplasmic autoantibody associated pauci-immune vasculitis. J. Clin. Immunol. 29, 282–291 (2009).
100. Yuan, J. et al. C5a and its receptors in human anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis. Arthritis Res. Ther. 14, R140 (2012).
101. Gou, S. J., Yuan, J., Chen, M., Yu, F. & Zhao, M. H. Circulating complement activation in patients with anti-neutrophil cytoplasmic antibody-associated vasculitis. Kidney Int. 83, 129–137 (2012).
102. Klinger, H. Grenzformen der periarteriitis nodosa [German]. Frankf. Z. Pathol. 42, 455–480 (1931).
103. Wegener, F. Über generalisierte septische Gefässerkrankungen [German]. Verh. Deut. Pathol. Ges. 29, 202–210 (1936).
104. Wegener, F. Über eine eigenartige rhinogene Granulomatose mit besonderer Beteiligung des Arteriensystems und der Nieren [German]. Beitr. Pathol. Anat. 102, 30–68 (1939).
105. Churg, J. & Strauss, L. Allergic granulomatosis, allergic antiitis, and periarteritis nodosa. Am. J. Pathol. 27, 277–294 (1951).
106. Petersen, H. J. & Smith, A. M. The role of the innate immune system in granulomatous disorders. Front. Immunol. 4, 120 (2013).
107. Voswinkel, J., Müller, A. & Lamprecht, P. Is PR3-ANCA formation initiated in Wegener’s granulomatosis lesions? Granulomas as potential lymphoid tissue maintaining autoantibody production. Ann. NY Acad. Sci. 1051, 12–19 (2005).
AcknowledgementsThe authors are supported by a grant from the NIH National Institute of Diabetes and Digestive and Kidney Diseases (P01-DK058335-11).
Author contributionsJ.C.J. researched data for the article, and both authors contributed equally to discussions of content, writing and review/editing of the manuscript before submission.
FOCUS ON VASCULITIS
© 2014 Macmillan Publishers Limited. All rights reserved