Embed Size (px)
Citation preview

VASCULAR SURGERY

Assessment of arterial circulation in limp.
• Inspect: 1. Color: marble white, blue hue, cyanosed 2. Vascular angle- Burger's angle: lift leg to white look at
what angle the leg is. 3. Capillary filling time: after lifting the leg but it over the
bed and see how long it takes for skin to turn pink. 4. Venous filling: look for guttering, and angle of venous
loss. 5. Pressure areas: look particularly closely at these, as
changes will be first apparent here, trophic, ulceration, gangrenous changes-heel, malleoli, head of 5th metatarsal, tips of toes, between toes, ball of foot.

Assessment of arterial circulation in limp
• Palpation: – Temperature: after 5 min exposure to ambiant temp.
– Capillary refilling: press tip of toe.
– Pulses: fem, dorsalis pedis, posterial tibial artery (medial malleoli), popliteal.
– Test muscles/nerves- may be affected by ischaemia.
• Auscultation:– over all major arteries
– Blood pressure in both armes.

ISCHEMIA
It the condition of inadequate blood supply to an area of tissue producing harmful effect to its function &nutrition

Acute Ischemia
It the condition of inadequate blood supply to an area of tissue producing harmful effect to its function &nutrition of less than 2 weeks duration

Acute Ischemia ( etiology)
1. Embolism2. Thrombosis3. Others
– Acute arterial trauma– Dissecting aortic aneurysm– Compartmental syndrome– External compression– Poploteal entrapment– Cystic adventational disease

Acute Ischemia
I viableI viable
DescriptionDescriptionNot threatenedNot threatened
Muscle Muscle weaknessweakness
NoNo
Sensory lossSensory lossNoNo
Arterial on Arterial on DopplerDoppler
AudibleAudible
>30 mmHg>30 mmHg
Venous on Venous on DopplerDoppler
AudibleAudible
IIa
Marginally
Salvagable
With Tr
No
No
Inaudible
Audible
IIb
ImmediatelySalvagable with
re vascularization
Mild to moderate
Rest pain
Inaudible
Audible
III
Irreversable
Major loss & permanent
damage
Profound paralysis
anesthesia
Inaudible
Inaudible

Acute Ischemia
I viableI viable
DescriptionDescriptionNot threatenedNot threatened
ClinicallyClinicallyNormalNormal
IIa
Marginally
Salvagable
With Tr
Less sever
ischemia
IIb
Immediately
Salvagable with re
vascularization
Sever ischemia
III
Irreversable
Major loss & permanent
damage
Gangrenous

Acute Ischemialess sever ischemiaSever ischemia
onsetGradual over few daysSudden within hours
HistoryChronic ischemia with previous claudication or rest pain
Normal limb but with cardiac problem as a source of emboli
1. PainSever then decreaseSever resistant to analgesia
2. ParesisFoot drop & tender calf are bad signs
Unable to move
3. Par aesthesia
presentEven anesthesia due to nerve
ischemia
4. Perishing cold
Colder than other limbColder than other limb
5. PallorLimb dusky color
Sever pallor then marble due to purple batches then fixed
blue
6. Pulseabsentabsent

Acute Ischemialess sever ischemiaSever ischemia
Contra-lateral limb examination
May detect absent pulse due to
atherosclerosisUsually normal
Ipsi-lateral limb
examination
may detect poploteal aneurysm as a
source of emboli

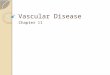
Acute ischemia with Gangrene

ARTERIAL EMBOLISM (Sever Ischemia)1. PainSever resistant to analgesia
2. ParesisUnable to move
3. Par aesthesiaEven anesthesia due to nerve ischemia
4. Perishing coldColder than other limb
5. PallorSever pallor then marble due to purple batches then fixed blue
6. Pulseabsent

Less sever Ischemia1. PainSever then decrease
2. ParesisFoot drop & tender calf are bad signs
3. Par aesthesiapresent
4. Perishing coldColder than other limb
5. PallorLimb dusky color
6. Pulseabsent

Less sever Ischemia

Less sever Ischemia

Management of acute ischemia
• Investigations– Urea, electrolytes, BSL– ECG, chest x ray
• Initial treatment– Rehydration– I V analgesia– Heparinization

Acute IschemiaIIa
Marginally
Salvagable
With Tr
Less sever ischemia
Angiography
Then
Thrombo-lysis
Then
bypass
IIb
Immediately
Salvagable with re vascularization
Sever ischemia
Embolectomy
III
Irreversable
Major loss & permanent damage
Gangrenous
Amputation or
terminal care

Acute LL ischemiaAcute LL ischemia
Sever LL ischemiaSever LL ischemia(previously normal limb)(previously normal limb)
Less sever LL ischemiaLess sever LL ischemia(previously ischemic limb)(previously ischemic limb)
Fogarty embolectomyFogarty embolectomyArterio-graphy must be Arterio-graphy must be
done to determine done to determine site, size& extent of site, size& extent of thrombus occlusionthrombus occlusion

Sever LL ischemiaSever LL ischemia(previously normal limb)(previously normal limb)
Femoral embolectomyFemoral embolectomy(assess degree of inflow)(assess degree of inflow)
Poor inflowGood inflow
Perform proximal Iliac embolectomy
Distal embolectomy
Perform intra-operative arteriogram To assess efficiency
No occlusionResidual thrombus
Close arteiotomy&Perform fasciotomy Thrombolysis
Poor inflow
Proximal vascularreconstruction

Less sever LL ischemiaLess sever LL ischemia(previously ischemic limb)(previously ischemic limb)
Arterio-graphyArterio-graphy
Thrombolysis
By pass procedure to site of occlusion or
angioplasty
If thrombo-lysis are contraindicated
After the underlying Cause is detected

Thrombo-lysis• This depend on per-
cutaneous delivery of thrombo-lytic drugs within the thrombus
• to dissolve it by intra-arterial catheter placed within the thrombus
• Most centers in UK have limited the technique for thrombus less than 30 days

Thrombo-lysis• Drugs
– Streptokinase– Urokinase– Recombinant TPA
• Technique– Local low dose– Pulse spray technique– High dose bolus technique
• Check angio-graphy is done every 8-9 hous and catheter tip repositioned as necessary
• Success is 60- 70 % with careful selection

Thrombo-lysis• Complications
– Mortality 1-2 %
– Major bleeding 10 %
– Minor bleeding 25 %
– Stroke
– Embolization
• Contraindications– Bleeding diathesis
– Long term anticoagulant
– Stroke
– Old age > 75 Y
– Peptic ulcer

Chronic LL ischemia (Risk factors)
Risk factors of LL ischemia
Age & sex
Diabetes
Smoking Hypertension
Hyper-lipidaemia
Obesity
Sedentary life

Chronic LL ischemia (Etiology)
Age above 45 Y Age below 45 years
Atherosclerosis Atherosclerosis is the commonest is the commonest
causecause
Diabetics Non Diabetics
Pre-senile atherosclerosis
In malessmokers In femaleIn both
Burger’s disease
Raynaud’sdiseaseArteritis

Chronic LL ischemia (Clinically)
Press & See How Color Fade (pre-gangrene) & (gangrene)
Pain Sensation Hotness Color Function
Pre-gangrene(Nutritional) Gangrene

Chronic LL ischemia (DD)
• Nerve compression (Sciatica)
• Veins ( CVI and DVT)
• Joints (arthropathy)
• Muscle ( myopathy)
• Bone pains
• Superficial lesions in skin& Sc tissue


Aortoiliac pattern
Femoropopliteal pattern
Distal circulation pattern
Inguinal ligament
Adductor hiatus
1. Claudication gluteal region
2. Wasting of thigh muscles
3. Lost or weak femoral pulses
4. Impotence if bilateral
1. Claudication calf2. Lost or weak popliteal pulse3. Beurger’s sign (pallor on
elevation and rubor on dependency)
Where is the site of occlusion ?

Chronic LL ischemia(thrombosis)
Le Riche syndrome• Claudication in gluteal
region • Wasting of thigh
muscles • Lost or weak femoral
pulses• Impotence

Aortoiliac pattern
Femoropopliteal pattern
Distal circulation pattern
Inguinal ligament
Adductor hiatus
1. Claudication foot2. Lost or weak dorsalis pedis and
or posterior tibial3. Beuger’s sign4. Nutritional changes (10 items)
1. Skin, 2. skin appendages, 3. subcutaneous fat, 4. muscles, 5. ulcers, 6. gangrene, 7. delayed venous filling,8. coldness, 9. motor and 10. sensory changes

Chronic LL ischemia

Chronic LL ischemia

Chronic LL ischemia

Chronic LL ischemia

Vascular lab1. Segmental limb
pressure
2. Ankle- Brachial Index
– Normal > 1
– Intermittent claudication 0.5- 0.9
– No healing < 0.5
– Rest pain 0.4

Vascular lab
1. Toe- brachial Index– Normal 0.8- 0.9
– Caludicate 0.35
– Rest pain 0.1
2. Toe pressures– Normal 90 – 100
mmHg
– CLI < 30 mmHg
3. Exercise tests

Non Invasive
• Doppler U/S
• Duplex U/S
• Plethysmography
• Isotope blood flow
• Trans-cutaneous oxygen tension

Invasive (Arteriography)It is the gold stander of
arterial tree
Methods
1. Directly trans-femoral if pulse is palpable
2. Seldinger approach
3. Digital sub-straction angiography contrast material injected I.V in large volumes or IA. In small tiny volumes

Invasive (Aorto-graphy)
»Translumbar if both F pulses are not felt
»Transfemoral aortography if one F pulse is felt
»Transbrachial if the entire distal aorta is occluded
»Digital sub-straction angiography

Invasive (Arteriography)Potential complications include • Contrast-related
– Anaphylactic reaction – Toxic reactions – Deterioration in renal function
• Technique-related – Haematoma – Arterial spasm – Sub-intimal dissection – False aneurysm – Arteriovenous fistula – Embolisation – Infection

New imaging modalites
• MR angiography (is now providing the most sensitive test for identifying tibial vessels)
• CT angiography which is articularly useful for the assessment of aneurysmal disease
• Angioscopy• Intravascular ultrasonography

Treatment of chronic LL ischemia
I - Risk factor reduction – Stop smoking - arrests disease progression– Lipid-lowering drugs – Anti-platelet medication – Good diabetic control if appropriate
II- Regular exercise – as part of supervised exercise program – Lose weight

Treatment of chronic LL ischemia
III – Pharmaco-therapy• Vasodilator drugs with small benefits
– Naftidrofyl oxalate, Praxiline – Pentoxyifyllin, Trental 400– Prostacyclin
• Vasodilator drugs with minimal benefits– Antiplatlets ( aspirin)– Prostaglandins– Ca channel blockers

Endo vascular surgery
Basic principles• The symptoms should be life-style limiting• Co-management of underlying conditions
likely to limit safety or success (smoking, heart failure etc)
• Proximal disease should be managed before distal ones
• Localized (<10 cm) non-ulcerating lesion is an ideal lesion

Endo vascular surgery
Basic techniques
• Balloon dilatation
• Stents
• Atherectomy devices
• Lasers
• Vibrating and rotating wires

Percutaneous transluminal angioplasty
• Angioplasty of the aorto-iliac segment has a 90% 5 year patency
• Angioplasty of the infra-inguinal vessels has a 70% 5 year patency
• Best results seen with short segment stenoses less than 2 cm long
Complications occur in less than 2% of patients o Wound haematoma o Acute thrombosis o Distal embolisation o Arterial wall rupture

Percutaneous transluminal angioplasty with stents
Use of stents • Most are used to correct inadequacies or
complications of PTA• To avoid re-stenosis which occurs within 90
days of PTA• When there is significant residual gradient or
stenosis following PTA• When there is acute occlusions during PTA• When there is dissection longer than PTA site

Surgical treatment of claudication and rest pain
• Indications for surgery:Indications for surgery: 1. claudication is a relative indication. 2. rest pain if fit for operation. 3. Ischaemic ulceration that does not respone
to conservative management. 4. acute occlusion.
• After decision on surgery is done do arteriography: site, type of operation and if technically possible

Surgical treatment
Direct arterial surgery Indirect arterial surgery
BypassThromb
endarterectomySympathectomy Amputation

Thrombendarterectomy

Bypass ReconstructionSupra inguinal bypass
Anatomical reconstruction Aortobifemoral bypass with 90 % success
Extra anatomical reconstructionAxillobifemoral 33- 85 % successFemorofemoral 80 % success
Infra-inguinal bypass (Femoro-poploteal bypass graft)Reversed saphenousIn situo saphenousSynthetic Gortex

Bypass Reconstruction
• Femoro-poploteal Bypass graft– Supra-genicular
• Synthetic 80 % patency
• Vein 90 % patency
– Infra-genicular• Armed Gortex 50 %
patency
• Vein 75 % patency

Bypass Reconstruction
• Graft failure• < 30 day
– techniqual
• < 1 Y – neo-intimal hyper-
plasia or graft stenosis
• > 1 Y – progresion of distal
disease

Sympathectomy
Not very effective for claudication.
Works especially on skin and subcutaneous tissues. so may help ulceration and rest pain.
Chemical sympathectomy is an alternative to surgical but not if anticoagulants are used.

Sympathectomy (Indications)
1. In combination with major arterial surgery with poor run off
2. In combination with minor amputation to decrease major
3. Burger’s disease4. Resistant ischemic ulcer5. Other indications
– Vasospastic disoders– Hyperhydrosis– Dysmenorrhea– Cancer bladder

Critical limb ischemia (CLI)Defined as • Persistent rest pain for >2 weeks.Rest pain
is usually nocturnal at first due to 1. relative decrease in cardiac output at night,2. recumbancy makes the leg relatively elevated,
and3. warmth increase the metabolic rate of tissues of
the foot.
• Ankle systolic <50 mmHg and/or toe systolic <30mm Hg
• Ulceration or gangrene of feet or any degree of tissue loss of the feet.

Critical limb ischemia (CLI)On the basis of the workup, a preoperative plan
composed of 5 items should be considered
1. Severity of ischemia • Rest pain without tissue loss can be
treated only with proximal lesion correction,
• while foot tissue loss necessitates restoration of pulsatile flow to the foot
2. The inflow (The aortoiliac disease if present should be corrected first)

Critical limb ischemia (CLI)3. The outflow
• (Duplex, or arteriography or even MR should be used to demonstrate possible patent tibial vessels)
• ideally, a vessel with runoff into the foot should be chosen.
• If the patient has a non-healing foot wound, the ultimate goal is to restore pulsatile flow to the appropriate part of the foot
• (anterior tibial for toe ulcers, and posterior tibial for heal ulcers)
4. Choice of graft • The epsilateral or contralateral greater saphenous is the best
5. Configuration of the graft

Critical limb ischemia (CLI)
Limb Not Salvageable Limb Salvageable
Fitpatient
Unfitpatient
Amputation Terminalcare
Rest pain Without
Tissueloss
Rest pain With Tissueloss
Correct Proximal Lesion by
Endovascular or Bypass
Must pulsatile
Flow in thefoot
•Endovascular• Bypass
•Sequential surgery