Embed Size (px)
Citation preview

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 1/66
C HAPTER 4
104
C HAPTER 4
Vascular Diseasesof the Brain
Imaging is an essential component of the workup of patients present-ing with symptoms of stroke. Stroke is a nonspecific term denoting asudden loss of neurologic function by any cause (e.g., ischemic infarc-tion, spontaneous hemorrhage, postictal state). Although this termhas little clinical value, it is useful because it is familiar to the publicand the lay press. In our information age, where diseases compete forattention and dollars, it is a widely recognized trademark for a mostimportant category of diseases. Over the past two decades, a host ofnew and evolving imaging techniques have been developed, allow-ing for ever more accurate and timely detection and characteriza-tion of strokes. The development and utilization of these techniqueshave been spurred by therapeutic advances, most notably the 1996approval by the U.S. Food and Drug Administration of thrombolytictherapy with tissue plasminogen activator (tPA) for intravenous use aswell as the positive results reported from intra-arterial thrombolysis.The imaging techniques available for the assessment of stroke includecomputed tomography (CT), magnetic resonance imaging (MRI),noninvasive angiography (CTA and MRA), catheter angiography, andCT and magnetic resonance (MR) perfusion imaging. In this chapterwe discuss primary ischemic abnormalities and then turn to the hem-orrhagic causes of stroke. Our goal is to provide a foundation to under-stand the diseases and problems that exist under the gamut of stroke.
ISCHEMIC CEREBROVASCULARDISEASE (STROKE)
Clinical FeaturesIschemic stroke has been recognized since the work of Hippocrates.Its etiology has been aggressively debated and remains as controver-sial as its recognition is old. Thromboembolic disease consequentto atherosclerosis is the principal cause of ischemic cerebrovasculardisease. Ischemic stroke has been classified by subtypes (Box 4-1)based on a multicenter clinical trial, TOAST, or Trial of ORG 10172in Acute Stroke Treatment. The most common causes of infarctioninclude large-artery atherosclerosis, cardioembolism, and lacunes.This widely accepted classification scheme allows for assessmentof etiology, prognosis, and treatment options. Outcomes differdepending on subtype. Large artery lesions have a higher mortal-ity than lacunes. Recurrent strokes are most common in patientswith cardioembolic stroke and have the highest 1-month mortal-ity. Using the TOAST classification, treatment decisions and the
outcomes of these treatments can be measured, allowing for bodocumentation of individual clinical competency and evidencbased assessment of therapeutic efficacy of different treatmenand devices. For instance, carotid endarterectomy or stenting is ttreatment of choice for large-vessel disease, whereas anticoagution therapy is most useful in patients with small-vessel diseaTerms such as significant stenosis become rigorous when explicitlydefined as greater than 50% to 70%, in particular when this defition has proven prognostic value.
Nonatherosclerotic causes of ischemic stroke include vasclopathies, migraine headache, and systemic/metabolic even(e.g., anoxia/profound hypoxia). They make up a small proption of strokes in patients over age 50 years. In younger patienthese nonatherosclerotic causes of ischemic stroke are mocommon, in particular in the absence of cardiovascular risk ftors (i.e., hypertension, diabetes, smoking, and hyperlipidemia
Thromboembolic events are the principal causes of ischemstroke. Emboli can arise from arterial stenosis and occlusionatherosclerotic debris and ulceration—in the extremities wicoexistent right-to-left shunts, or cardiac sources (a cardiac souof emboli is responsible for 15% to 20% of ischemic strokes). Textent to which narrowing of the arterial lumen contributes stroke is complex. Even in the absence of severe stenosis threduction in flow may decrease the ability to “wash out” disemboli before they produce ischemia (Box 4-2).
Robert D. Zimmerman
B OX 4-1. TOAST Classification of Subtypesof Acute Ischemic Stroke
Large-artery atherosclerosis (embolus/thrombosis)Cardioembolism (high-risk/medium-risk)Small-vessel occlusion (lacune)Stroke of other determined etiologyStroke of undetermined etiology
Two or more causes identifiedNegative evaluationIncomplete evaluation
B OX 4-2. Risk of Cardioembolism
HIGH-RISK SOURCESMechanical prosthetic valveMitral stenosis with atrial fibrillationAtrial fibrillationLeft atrial/atrial appendage thrombusSick sinus syndromeRecent myocardial infarction (<4 weeks)Left ventricular thrombusDilated cardiomyopathyAkinetic left ventricular segmentAtrial myxomaInfective endocarditisMEDIUM-RISK SOURCESMitral valve prolapseMitral annulus calcificationMitral stenosis without atrial fibrillationLeft atrial turbulenceAtrial septal aneurysmPatent foramen ovaleAtrial flutterLone atrial fibrillationBioprosthetic cardiac valveNonbacterial thrombotic endocarditisCongestive heart failureHypokinetic left ventricular segmentMyocardial infarction (>4 weeks, <6 months)
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 2/66
V ASCULAR D ISEASES OF THE B RAIN 105
Extracranial/proximal intracranial large-vessel atherosclerosisleads to infarction when there is “hemodynamically significantnarrowing”; that is, when the diameter of the vessel is decreasedby 50% to 70% or the vessel lumen is reduced to less than1.5 mm. Hemodynamically significant lesions are manifested bya pressure gradient across the stenosis, but cerebral blood flow(CBF) reduction does not occur until the diameter is decreasedby approximately 90% as a result of autoregulation in the brain,where flow is maintained by decreasing cerebrovascular resis-tance. Blood flow may be preserved and infarction may even beprevented with complete occlusion of the vessel because of col-lateral circulation (circle of Willis and leptomeningeal vessels).Conversely, patients with complete internal carotid artery occlu-sions in the neck may still have cerebral infarctions from emboli.Emboli may be multiple and simultaneous, or a single embolusmay break up and produce multiple infarctions.
Atherosclerosis is common and typically affects multipleextracranial and proximal intracranial vessels or multiple regionswithin the same vessel. Thirty-five percent of patients over age50 years have atherosclerotic changes in cervical cerebral arteries,but only one third of these individuals have symptoms of vas-cular disease. Primary stenosis/occlusion most often results ininfarction when there is a preexistent stenosis with either newocclusion or a period of systemic hypotension. Acute extracranial
carotid occlusion may produce large areas of infarction involvingthe deep (ganglionic) and superficial (cortical) middle cerebralartery (MCA) distribution (Fig. 4-1A). In these cases the infarctsare likely the result of large distal emboli associated with theproximal occlusion. The anterior cerebral artery (ACA) territoryis typically spared because of collateral supply from the contra-
lateral ACA via the anterior communicating artery (ACoAcircle of Willis. Isolated ACA and combined MCA/ACAhemispheric”) (seeFig. 4-1B) infarcts are rare; holohemisphinfarcts are usually fatal. They most often occur in patienacute myocardial infarction and atrial fibrillation due to thbination of large emboli and poor cardiac output. Alterncarotid stenosis or occlusion may occur without markedembolization, producing “watershed” or border-zone infaVascular watersheds are the distal arterial territories oftenders between two vascular distributions (see Chapter 2).border zones are found between the anterior and middlebral arteries and the middle and posterior cerebral artReduction in flow affects these zones to the greatest ebecause they are furthest from the heart. Borderzone inoccur in the posterior parietal region (MCA/PCA borderthe frontal lobes (ACA/MCA border zone), and the basal (Fig. 4-2). These infarcts are often small and may be conwith lacunar infarcts. The key to diagnosis is the presence otiple infarcts at the interface between different vascular tries and evidence of carotid occlusion or slow flow. Othin the brain are selectively jeopardized by hypoxia or hysion due to increased susceptibility to ischemia from incmetabolic rate and a lack of redundancy of blood supply. include the hippocampus (Ammon’s horn), globus pallidu
amygdala (anterior choroidal-posterior cerebral watersheebellum, and occipital lobes, in that order.Interest in the detection and treatment of extracranial c
artery disease has been heightened by the results of two laals for the treatment of symptomatic and asymptomatic paThe North American Symptomatic Carotid Endarterec
A B C
D E
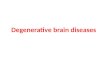
F IGURE 4-1.Thromboembolic stroke. A, Middle cerebral artery (MCA).
Computed tomography scan at level oflateral ventricles reveals a large area ofhypodensity in the right MCA distribution.B, Anterior cerebral artery. Diffusion-weighted image reveals hyperintensity inthe medial (parasagittal) portions of theleft frontal lobe.C, Cerebellar infarct.FLAIR reveals inferior medial cerebellarhemisphere infarct.D and E, Basilar tipocclusion. FLAIR reveals bilateral upperbrain stem, right hippocampal, left occipi-tal, and bilateral thalamic infarcts indica-tive of occlusion of distal branches of thebasilar artery.
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 3/66

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 4/66
V ASCULAR D ISEASES OF THE B RAIN 107
unilateral, and tubular in appearance on axial imaging, reflectingthe location and course of the pontine perforating arteries (seeFig. 4-4C). Although these infarcts were originally thought toarise from small-vessel atherosclerosis and lipohyalinosis associ-ated with hypertension, many other causes have been proposed,including emboli, hypercoagulable states, vasospasm, and smallintracerebral hemorrhages.
Transient ischemic attack (TIA) is a sudden functional neu-rologic disturbance limited to a vascular territory that usuallypersists for less than 15 minutes, with complete resolution by24 hours. The diagnosis of TIA is difficult because it is by defi-nition retrospective. In approximately 25% of cases the clinicaldiagnosis of TIA is incorrect. The event is either a completedinfarct or has another etiology (e.g., intracranial hemorrhage,migraine or seizure). Although TIAs have a variety of causes,
the common pathway is temporarily inadequate blood supplyto a focal brain region. TIAs are not benign events. Almost onethird of patients will eventually have cerebral infarction (20%within 1 month of the initial TIA) or, despite resolution of symp-toms, have a diffusion-positive event on MRI. Quantitative mea-surement of apparent diffusion coefficients (ADC) from MRdiffusion-weighted images (DWI) may reveal mild decreased dif-fusion (<25%) in symptomatic areas without signal abnormalityon DWI, indicating that although there is no permanent func-tional deficit, neurons have been lost (25% in some animal stud-ies). Thus, proceeding with the workup after the TIA is urgent.A reversible ischemic neurologic deficit lasts less than 7 days andsymptoms should resolve. Again, DWI is positive in about 50% ofthese cases, even with symptom resolution. So are these entitiestruly reversible/transient or just compensated?
PATHOLOGY OF ATHEROSCLEROSISThe process begins in the first decade of life in the aorta withsubendothelial fatty deposition (fatty streak) consisting ofsmooth muscle cells, foam cells, T lymphocytes, and an extra-cellular matrix of lipid and collagen. Fat is discharged into theextracellular space, precipitating intimal thickening, prolifera-tion of smooth muscle cells, and inflammatory changes, eventu-ally resulting in fibrosis and scarring. A fibrous plaque consistsof collagen, lipid, smooth muscle cells, and fibroblasts. Theendothelial surface of the plaque may degenerate with ulcerationand discharge of lipid or calcified debris into the vessel lumen.Platelets may accumulate on the ulcerated intimal surface andbecome exposed to collagen, leading to thrombus formation and
platelet emboli. Arterial bifurcations are subject to the gmechanical stress and are especially prone to atheroscleroscomposition of plaques is variable, with some becoming lafibrotic, producing luminal narrowing, whereas others aclate lipid and cholesterol. The composition of the plaquehave significant prognostic and therapeutic implications. Pwith thick fibrous caps may be stable and asymptomaticwhile producing significant stenosis. These lesions may rno therapeutic intervention. Plaques with a thin or absen(unstable plaque) with exposed lipid or hemorrhage are prdevelopment of thrombus and embolization. Aggressive tmay be warranted regardless of the degree of stenosis. Imacarotid plaques with MR and CT is an area of active resemay be that by the time of the next edition of this book pimaging will be a standard diagnostic tool. Surface coil
plaque imaging readily identifies enhancement of fibrouand plaque hemorrhage (blood intensity) and calcificationon all sequences). Platelet accumulation at the site of plaqruption through a thin fibrous cap (nodules interrupting ening cap) can now be readily identified with surface coil plaque imaging.
IMAGING TOOLS
BrainComputed tomography has been the mainstay of stroke ing since its inception in the mid-1970s. Unenhanced CTare fast and readily available. They are excellent for ding large ischemic infarcts of more than 6 to 8 hours’ duNonischemic causes of stroke, including hemorrhage, tion, and tumor, are easily detected although often poorlyacterized. There are, however, significant limitations to does not reliably detect infarcts of less than 4 hours’ duand the extent of the infarct is often difficult to charactAcute lacunar infarcts often go undetected and are typimpossible to distinguish from chronic lacunar infarcts. detection rates for acute infarction are approximately 5the first 24 hours. Detection of hyperacute infarction (<6 on unenhanced CT is a skill that requires expertise and rience. Initial results from the European Cooperative Stroke trial of intravenous tPA indicated that the drug weffective. Review of the imaging studies by expert neurorgists revealed that the lack of efficacy was the result of pviolations caused by incorrect interpretations of CT scanMassachusetts General Hospital group recommends usin
A B C
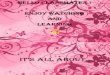
F IGURE 4-4. Lacunar infarcts. A, Diffusion-weighted image reveals a round focus of hyperintensity in the left periventricular white matter inacute lacunar infarct.B, FLAIR image reveals central fluid intensity with peripheral T2 hyperintensity indicative of a chronic lacunar infaC, Braistem infarct. Sagitally oriented T2 hyperintense lesion in the right pons with sharp medial border at the midline indicative of acute infarct on bilateral chronic ischemic change.
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 5/66
108 Neuroradiology: The Requisites
narrow CT window widths and levels to spot subtle low-densitychanges that portend infarct. Unfortunately, patients with acuteinfarction do not have the option of having their scans read byexperts. The introduction of low-dose algorithms to limit radi-ation exposure may be necessary from the perspective of theoverall population safety, but the increased noise inherent inthese scans makes detection of subtle infarct changes more dif-ficult. Unenhanced CT can provide limited information aboutthe intracranial vessels (the dense vessel sign of acute embolicocclusion) and no information on the status of the brain that sur-rounds the already infarcted tissue. Perfusion CT shows promisein identifying strokes that may develop and are inapparent onenhanced CT.
MRI is much more sensitive than CT in the detection of hyper-acute infarction. T2-weighted FLAIR scans have a sensitivity of85% within the first 24 hours. Hemorrhage (either within theinfarct or as an independent cause of stroke) is readily seen and,in contradistinction to early opinions, MR is more sensitive thanCT, even in the hyperacute phase. Detection of hemorrhage hasbeen greatly facilitated by the routine use of gradient echo andmore recently susceptibility-weighted (SWI) sequences. Othercauses of stroke, including venous thrombosis, vascular mal-formations, infections, and tumors, are detected and character-ized with greater accuracy than is possible with CT. Arterial and
venous occlusion or slow flow can be detected on MRI, in par-ticular with the use of gradient echo scans and FLAIR. Focalacute embolus in a major vessel (the corollary of the dense ves-sel sign on CT) is best detected on gradient echo scans, and slowflow can be seen on FLAIR and enhanced T1-weighted images(T1WI).
Of course, the advent of DWI has greatly enhanced our abil-ity to detect hyperacute infarction and to characterize all infarc-tion. Whereas “routine” MRI has an 85% sensitivity for infarctionwithin 24 hours, MR with DWI has a sensitivity of approximately95% in this period, including the first 3 hours after infarction,when CT typically does not demonstrate any parenchymal abnor-mality. The dramatic hyperintensity seen in acute infarction (the“light bulb sign”) also makes detection easier, especially for theinexperienced observer. CT is easy to do and hard to interpret.MRI is hard to do but easy to interpret.
So how does DWI work? Diffusion imaging is a technique that issensitive to the movement of water molecules (Brownian motion).In pure water, protons move about and jostle each other. Manyof us remember high school science class experiments where wetrained low-tech light microscopes on small pools of water andwatched as particles of dust wobbled around under the influenceof unseen water molecules. Fewer of us are aware that the math-ematical proof of Brownian motion published by Albert Einsteinin 1905 confirmed once and for all the existence of molecules. Inpure water, the extent of water molecule motion (self-diffusion)will be determined by temperature. The higher the temperature,the more energy the protons possess and the farther they willmove. Biologic tissues are more complex. The water moleculeencounters various barriers and impediments to motion, includ-ing cell membranes, intracellular organelles, and extracellular pro-teins. The termapparent is applied to modify the worddiffusion,connoting the uncertainty of the water motion in biologic samplescaused by these barriers. In gray matter these structures are rela-tively randomly arrayed so diffusion is the same in all directions(isotropic). In white matter diffusion is constrained by the orien-tation of the white matter tracts. Water will diffuse preferentiallyalong rather than across these tracts and is therefore anisotropic.The distance traveled by a particular proton will depend on thenumber of impediments it encounters and the period of time dur-ing which the molecule is “observed” during the MR sequence.If the observation time is too short, the paths of most moleculeswill not be differentially affected by cellular barriers (i.e., mem-branes, proteins); however, when the observation time is longenough encounters with barriers will restrict diffusion. Thus DWI
is unique among all imaging techniques in that it is a direct widow into the spatial scale of molecules and cells. The effect of tdiffusion can be measured as a change in signal intensity on MThis measurement can be made by applying two gradient pulsto dephase and rephase the water molecules during the imagacquisition. Those molecules that diffuse the greatest distanc(i.e., subject to the greatest gradient strength difference) wibe unable to rephase completely and will lose signal. The signloss depends on the diffusion coefficient of the molecule and thstrength and duration of the gradient pulses. This can be definemathematically by the following equation:
S(b) = S0 • e −bD
where D is the diffusion coefficient, S 0 is the signal intensity ofthe unweighted image, S(b) is the signal intensity of the imagesfor variousb values, and theb value is specific for the particularpulse sequence used to measure diffusion.b is a function of thediffusion gradient strength, the duration of the diffusion gradiepulse, and the time of the diffusion measurement. Theb valuedetermines the degree to which an image is sensitive to diffusi(the higher theb value the more diffusion weighted an imagebecomes). The ADC can be calculated by using images with vied gradient strengths (differentb values). At a minimum ADC
can be calculated if there are at least twob values, one of whichmust be set to approximately 0; that is, with no diffusion weiging. In clinical practice twob values are generally used; however,four or moreb values can be measured to improve accuracy omeasurement. Commonly used values include ab value of 800 to1,200 sec/mm2, with time to echo (TE) of 90 to 120 msec.
Diffusion images can be created to be (1) directionallsensitive (with a T2 component); (2) directionally insenstive (the cube root of the product of three directions—withT2 component); or (3) directly correlated to ADC values (T2 component). In clinical practice, DWI sequences includapproximately 30 slices, with individual images obtained approximately 20 msec. Four acquisitions are obtained at ealocation (total acquisition time for the brain < 1 min). Onacquisition is acquired with no diffusion gradients (the b0 image—a T2- and susceptibility-weighted image) and thresets of orthogonal (anteroposterior, superoinferior and righleft) images are acquired with ab value of ~1000. The threeorthogonal images are averaged to produce a “trace” imathat is insensitive to the anisotropy created by the orientatioof white matter tracts. For instance, on a DWI acquired witthe diffusion gradients applied in the anteroposterior directiothe corpus callosum will appear bright because there is almono anteroposterior motion of water molecules in the highorganized right-to-left–oriented callosal fibers. On the othhand, on images where the diffusion gradients are applied a right-left–orientation the vertically oriented white mattof the corticospinal tract will appear bright. The trace imais the average of these three acquisitions that eliminates theffects of fiber tract orientation on signal intensity. In clinicpractice only the trace image is viewed because in processlike infarction and other diseases it is the magnititude, not thdirectionality, of diffusion that is important. However, informtion on the direction of diffusion and the degree of anisotropare obtained and can be used to create images that record thdirection and integrity of white matter tracts. This techniquecalleddiffusion tensor imaging , requires image acquisition in atleast six planes rather than the three planes used in clinicaDWI to completely describe the diffusion tensor. (A tensor any measurement with at least three components.) The diffusion data can be used to generate ADC maps by performingvoxel-by-voxel calculation of ADC using the trace diffusion ab0 image. Subtractions of the diffusion and b0 data can also beused to generate “exponential” diffusion images. Generation these maps is fast and simple. In clinical practice it is comm
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 6/66
V ASCULAR D ISEASES OF THE B RAIN 109
to generate and view DWI, ADC, and exponential images.ADC maps and exponential maps eliminate the T2 componentof intensity (T2 shine-through) on diffusion sequences (seebelow). All DWI start life as T2WI, from which signal is sub-tracted based on the extent of diffusion; therefore, with routineDWI there is always a contribution of T2 to signal intensity.It is also helpful to have the b0 images available for viewing.Because of speed, these images are rarely motion degraded;therefore, in uncooperative patients or in patients having veryrapid MR studies, the b0 can serve as a “poor man’s” T2WI orSWI.
On diffusion-weighted imaging, tissues that most nearly approx-imate water will have the highest rates of diffusion (high ADC)and will lose signal more rapidly than those with low ADC. Thus,cerebrospinal fluid (CSF) appears dark on DWI as the water mole-cules can freely diffuse for relatively large distances, whereas graymatter is light gray and white matter slightly darker gray. On ADCmaps contrast is reversed. Increased diffusion is bright; thereforeCSF is bright while brain tissue is dark. Some clinicians preferexponential diffusion images to ADC maps because the relativesignal intensities are the same as with DWI (high diffusion suchas CSF is bright). In reality the reversal of signal between DWIand ADC maps is not a problem if one simply remembers thatCSF has the highest diffusion and that lesions with low diffusion
will look the opposite of CSF. In tissues where diffusion is morerestricted than in normal brain (e.g., hyperacute infarction) therewill be less water molecule motion than in normal tissue and there-fore less signal loss during the diffusion acquisition. These regionswill appear dark on ADC maps. When water motion is increasedin tissue due to vasogenic edema (increased extracellular water)or gliosis (decreased cellularity), tissue will appear isointense onDWI and hyperintense on ADC maps. Tissues with increased dif-fusion are typically isointense rather than hypointense on DWIbecause of T2 effects. Increased tissue water (vasogenic edema)increases the T2 of the tissue; therefore, the effects of increasedT2 (increased signal) and increased diffusion (decreased signal)tend to cancel each other out. In circumstances when diffusion isequal to normal brain but T2 is increased (subacute infarction),the tissue will look bright on DWI and isointense on ADC maps,a phenomenon known asT2 shine-through.
VesselsIt is obviously important to have knowledge of the arteriesand veins in assessing individuals presenting with “stroke.”Identification of occlusion or stenosis of extracranial and intra-cranial arteries can confirm the ischemic nature of a lesion andhelp to determine whether an infarct is due to slow flow, proximal(e.g., MCA) embolic occlusion, or small-vessel disease. Directvisualization of the dural venous sinuses and cortical veins isoften critical to the correct diagnosis of venous thrombosis in par-ticular, given the protean clinical manifestations, etiologies, andimaging findings in this disorder. In the past, assessment of vas-cular structures required invasive catheter angiography, but thereare now multiple noninvasive ways of assessing the cervicocer-ebral vessels, including CTA, MRA, and ultrasound. Each ofthese techniques has its advantages and limitations; the choiceof the technique or combination of techniques to be utilized willdepend on the circumstances and diagnostic questions in eachcase. Catheter angiography is reserved for those cases in whichnoninvasive studies do not provide a definitive diagnosis and,most importantly, when endovascular intervention (e.g., angio-plasty, stenting, aneurysm coiling) is performed.
Carotid Ultrasound/Transcranial Doppler Ultrasound uses sound waves to image structures or measure thevelocity and direction of blood flow. Color-coded Doppler ultra-sound can depict the residual lumen of the extracranial carotidartery more accurately than conventional duplex Doppler.However, the results from color-coded Doppler ultrasound
examination are operator dependent and controversial. Proinclude distinguishing high-grade stenosis from occlusionfied plaques interfering with visualization of the vascular inability to show lesions of the carotid near the skull baseculty with tandem lesions, and inability to image the origincarotid or the vertebral arteries. In the NASCET study, Domeasurements were 59.3% sensitive and 80.4% specific detection of stenosis greater than 70%. A battery of sonononinvasive carotid studies, including indirect tests monthe superficial and deep orbital circulations and direct susing imaging and function, has been advocated to increaaccuracy, particularly in significant vascular disease.
Transcranial Doppler ultrasound is a noninvasive meanto evaluate the basal cerebral arteries through the infratemfossa. It evaluates the flow velocity spectrum of the cerebsels and can provide information regarding the direction othe patency of vessels, focal narrowing from atheroscleroease or spasm, and cerebrovascular reactivity. It can detadequacy of MCA flow in patients with carotid stenosis adence of embolus within the proximal MCA. It is very usthe detection of cerebrovascular spasm after subarachnoid rhage (SAH) or surgery, and can rapidly assess the results oranial angioplasty or papaverine infusions to treat vasospa
AngiographyMRA is a critical and important tool for assessing the extrand intracranial vascular system. The technique is noninand does not involve use of ionizing radiation. (The effradiation exposure from CT scanning on population canchave recently become of concern; therefore, use of MRbe preferred, in particular in younger patients.) In many MRA does require an injection of contrast material. Threeent techniques are used to generate MRA: time-of-flight (phase contrast (PC), and contrast-enhanced MRA (CEMOnce the imaging data is gathered, it may be processed beral display techniques. The one most commonly used is tmaximal intensity projection (MIP), which finds the brightest pialong a ray and projects them along any viewing angle. MIand insensitive to low-level variations in background inten
In TOF MRA (the most commonly used technique) prnot immediately exposed to a radiofrequency (RF) pulse (urated spins) flow into the imaging volume and have highethan the partially saturated stationary tissue (which has lonal secondary to the RF pulse). This is a T1 effect and hastermed flow-related enhancement . The images can be acquiredindividual slices (2D) or as a volume (3D) acquisition. In 3MRA the volume of tissue to be imaged is limited becausetons “flow” through the volume they are exposed to RF and become saturated. To cover large areas, (e.g., the ccavity) 2 to 3 volumes are acquired with overlap between umes. In either case flowing blood will appear bright. Toalize the arteries without interference from the veins, an superior nonspatially localized saturation pulse is appliedblood flowing inferiorly in the venous system will be saand will not be visible on the MRA. With TOF MR venog(MRV) the saturation pulse is applied inferiorly to saturaarterial blood. The 2D TOF techniques are very sensitive toor moderate flow (as flow-related enhancement is maximwhereas 3D techniques are better than 2D MRA for rapid flhave higher resolution. They are also less likely to be deby patient motion. In the evaluation of cervical vasculatucommon to perform a 2D sequence of the entire cervical and a small-volume 3D sequence centered on the carotid btion. Intracranial arterial evaluation is performed with 3DA pitfall in the evaluation of TOF MRA can occur when thT1 hyperintense lesions or structures within the tissues. Tareas of T1 hyperintensity will be visible on the MRA ibecause the MIP images will include all regions with an inabove a predefined threshold. Thus, subacute hematoma
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 7/66
110 Neuroradiology: The Requisites
fat-containing lesions will appear bright. Subacute intramural clotin dissections and venous sinus thrombosis will also appear brightand may be mistaken for flow.
The advent of 3 Tesla (3T) MR scanners has produced a dra-matic improvement in TOF MRA (Fig. 4-5). This is related inpart to increased signal-to-noise ratio; however, a more impor-tant cause is increased T1 of normal tissues when imaged at 3T.Because the T1 is longer it is easier to suppress background sig-nal at 3T, resulting in a marked improvement in visualizationof flowing intravascular protons. This effect is most notable onintracranial MRA. At 1.5T visualization of second-order intracra-nial branches (e.g., intrasylvian MCA branches) is limited; there-fore, detection of distal occlusions, vasculopathy, and arterialspasm is not reliable. At 3T these vessels and even smaller arter-ies (e.g., lenticulostriate arteries) are well visualized in almost allcases (seeFig. 4-5). Therefore, it is preferable to perform MRAstudies on 3T scanners.
In phase-contrast MRA, bipolar flow-sensitizing gradients ofopposite polarity are used to “tag” moving spins (protons) that arethen identified owing to their position change at the time of eachgradient application. The operator chooses the flow velocities thatthe angiogram will be sensitive to, termed theVENC , which varyin neuroradiology from 30 cm/sec for arterial flow to 15 cm/sec forvenous flow. (At lower VENC levels phase-contrast techniques
can be used to assess spinal fluid flow.) Complex subtraction ofdata from the two acquisitions (one of which inverts the polarityof the bipolar gradient) will cancel all phase shifts except thosedue to flow. This technique provides excellent background sup-pression to differentiate flow from other causes of T1-shortening,such as subacute hemorrhage or fat. In the “early” days of MR,phase-contrast was an alternative to TOF for the routine assess-ment of arterial disease but TOF proved superior for this task.Phase-contrast MRV is, however, routinely used for suspectedvenous thrombosis because of its ability to differentiate betweenflow and subacute (bright) thrombus that obfuscates TOF MRV.
Contrast-enhanced MRA uses paramagnetic contrast enhance-ment in association with 3D TOF imaging. This method hasmany advantages over the noncontrast approach. Like CTA (seebelow) the technique visualizes contrast within vessels and isnot dependent on flow. The result is a rapidly acquired (<30 sec)high-resolution image of the extracranial and proximal intracra-nial vessels with typical coverage from the aortic arch to the circleof Willis (Fig. 4-6). Timing is critical because enhancement ofveins confounds the ability to demonstrate arterial anatomy andthe sequence is typically triggered with MR fluoroscopic tech-niques. This technique offers excellent visualization of the aorticarch and proximal cervical vessels. These structures are not seenon routine TOF MRA and may be difficult to visualize on CTA.Because it is not dependent on flow and not affected by turbu-
lence it is superior to noncontrast MRA for evaluation of carobifurcations and cervical and intracranial vertebrobasilar systemIt also can decrease ambiguity in cases with flow reversal suchsubclavian steal (Fig. 4-7). CEMRA is not used for the routineassessment of intracranial vessels because of problems producby venous contamination and enhancing normal (sinus mucosand pathologic tissues (e.g., brain tumors).
MRA is a good tool for the noninvasive evaluation of textracranial vasculature for the presence of a hemodynamicasignificant lesion of the carotid arteries, dissection of the verbral and carotid arteries, extracranial traumatic fistula, extracranvasculitis such as giant cell arteritis, or congenital abnormalitof the vessels such as fibromuscular disease. Because it is noinvasive and does not utilize ionizing radiation, it is an excellscreening test for cervical vascular disease. Although noncontMRA is simple to perform, in clinical practice CEMRA is nroutinely used in the outpatient assessment of the cervical vaculature. In the evaluation of acute infarction it is more commto perform noncontrast MRA of the extracranial and intracranvessels. This allows for a good global assessment of the vascuture. Limitations of MRA in assessment of patients presentinwith “stroke” include motion degradation in ill or uncooperatipatients, limited ability to differentiate extremely slow flow (ethe “string sign” of long segment internal carotid narrowing due
tandem lesions) from occlusion, and susceptibility artifacts cauby atherosclerotic calcification (typically at the cervical carobifurcation and within the cavernous carotid artery) and air-bointerfaces (in the petrous segments of the internal carotid arteies). Cervical MRA tends to overestimate moderate stenosis, particular if only unenhanced 2D TOF methods are used. Thuapparent severe stenosis (>85%) may actually be moderate (~50The limitations of noncontrast MRA can be overcome in most caby careful assessment of MRA source images and routine MRI.
Intracranial MRA can be used to reliably detect proximstenosis and occlusion as well as vasculopathy (at 3T). MRhas been shown to accurately detect aneurysms (90% accurafor aneurysms >3 mm). It is therefore useful as a screening tofor asymptomatic patients with a risk of intracranial aneury(e.g., patients with polycystic kidney disease or individuals wa first-degree relative with a history of ruptured aneurysm). It calso be used to follow patients with known nonruptured anerysms and patients who have undergone endovascular coilinganeurysms. In the workup of patients with known or suspectSAH, CTA is preferred. CTA acquisition is faster and providmore precise anatomic detail on aneurysm morphology and retionship to parent vessels. Although MRA may easily detearteriovenous malformations (AVM), the superimposition of feing arteries and draining veins makes assessment of this lesionlimited value. 4D CTA and MRA, in which a time element i
A B C
F IGURE 4-5. Magnetic resonance angiography (MRA) 1.5-Tesla (1.5T) versus 3T. Comparison of 1.5T ( A ) and 3T (B ) collapsed images from cranialMRA reveals improved visualization of small and peripheral vessels at 3T (arrows inB ).C, Focal atherosclerotic irregularity of the right middle cerebrartery is visible at 3T (arrow ).
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 8/66
V ASCULAR D ISEASES OF THE B RAIN 111
A B C
F IGURE 4-7. Subclavian steal. A, Time of flight MRA fails to adequately demonstrate the proximal left vertebral artery. You can just make oof the vessel (arrows ).B, Gadolinium enhanced MRA now shoes the left vertebral artery, the victim of slow flow. The cause is a stenosis of left subclavian artery (arrowhead ), which is hard to believe on this projection, but much more plausible (arrowhead ) on the oblique view (C ).
A
B C
D
F IGURE 4-6. Contrast-enhanced magnetic resonance angiography (CEMRA). A , CEMRwith coned down views reveals excellent visualization of the aortic arch and itsbranches.B and C , CEMRA demonstrates good visualization of vessels from tharch to the circle of Willis. Note left middle cerebral artery occlusion (arrow inB ) and lecavernous aneurysm (arrow in C ). D , Selected image of the left cerebral artery reatherosclerotic tortuosity and irregularity of the internal and external carotid arte
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 9/66
112 Neuroradiology: The Requisites
superimposed to show inflow and outflow, may solve some of theambiguities around AVMs and fistulas.
MRA images, particularly the extracranial portion of theexamination, are challenging to interpret. Source image shouldalways be evaluated with care. The cross-sectional area of thecommon carotid bifurcation and proximal internal carotid arter-ies should be determined (in particular on 3D images) becausethis can provide the most accurate assessment of presence anddegree of stenosis. The intracranial circulation should be lookedat on source images as well. Source images allow for detection ofsusceptibility artifacts (see above) and for assessment of cross-sectional luminal narrowing. Dissections are best demonstratedon these images (in combination with T1- and T2-weighted brainor neck images) because of the ability to differentiate the luminalnarrowing from the vessel wall thickening and for the detectionof false lumens and webs. Careful evaluation of the common loca-tions of aneurysms (e.g., anterior communicating artery, posteriorcommunicating origin from the internal carotid artery, MCA tri-furcation) is highly recommended in all cases. Isolated MIPs ofeach vessel should be performed and evaluated in multiple pro- jections to eliminate the effects of arterial overlap. MRA (and forthat matter CTA) interpretation has been markedly facilitated bythe interpretation of images on PACS workstations.
Computed tomographic angiography (Fig. 4-8) has emerged
as an alternative to MRA for imaging both the extracranial andintracranial blood vessels with the development of multirowdetector scanners. Current 16- to 64-row scanners can provideexcellent visualization of extracranial and intracranial vesselswithout venous contamination (assuming accurate timing of con-trast bolus injection, which is frequently a BIG assumption).New 320-row detector scanners can acquire data from the entirebrain simultaneously and therefore, with multiple acquisitions,produce time-resolved angiographic studies that mimic catheterangiography in their appearance. CTA requires the placement ofa catheter, usually in the antecubital vein, with rapid injection ofapproximately 50 to 125 mL of iodinated contrast material. Aftera short delay following contrast injection, imaging commencesand a 3D data set is acquired. CT advances have resulted in thin-ner images, improving resolution. Computer postprocessing isnecessary for MIP images and for excluding the bony base of theskull structures. In the past postprocessing was a relatively time-consuming, labor-intensive task requiring knowledge of anat-omy and the ability to use 3D workstations. As 3D workstationshave been improved, the task of reconstructing CTA studies hasbecome easier and can now be done (at least preliminarily) bytechnologists at the CT scanner. It has gained immense popular-ity in the workup of hyperacute infarction when used in combina-tion with CT and CT perfusion because of availability and easeand speed of data acquisition. It is superior to MRA for detect-ing and characterizing smaller aneurysms at the cost of radiationand iodinated contrast dye. CT and CTA are typically performedat initial presentation of suspected aneurysmal SAH (aSAH) onthe ED scanner because all data can be collected in less than 2minutes.
Computed tomography angiography has several advantageswhen compared to MRA. Because the images are not motion- sensitive, CTA allows for accurate assessment of extracranialstenosis (seeFig. 4-8C and D). Workstations often have softwarethat allows for measurement of cross-sectional areas at multiplesites. Calcification does not cause the same artifacts that are seenon MR, and extremely slow flow and tandem lesions are morereliably detected on CTA than MRA. Intracranial embolic occlu-sion is more easily seen, and focal clot within proximal intracranialvessels may be directly visualized (seeFig. 4-8E). CTA has betterspatial resolution than MRA; therefore, identification of aneurysmmorphology (including overall size and neck morphology) and rela-tionship to adjacent and parent vessels is better (seeFig. 4-8F).The superb quality of CTA has prompted many neurosurgeons to
operate directly on the basis of CTA findings, reserving cathetangiography for those cases where CTA findings are inconclusor when endovascular treatment is to be performed. Interestingover the past few years there has been a movement back tperforming catheter angiography even when surgery is the trement of choice. This may reflect improvements in digital sutraction conventional angiography equipment with ability to pform rotational (3D) images during arterial contrast injectioAlthough MRA is more accurate for the assessment of aneurystreated with endovascular coils, CTA has proven to be moaccurate for the assessment of aneurysms treated with surgicclipping.
The limitations of CTA include: (1) risks of intravenous iodnated contrast injection; (2) exposure to radiation; (3) obscution of vessels at the base of the skull due to bone and contrain the cavernous sinus; (5) obscuration of aneurysms by extensSAH; (6) extensive atherosclerotic calcifications in the wallsthe vessels; (7) atherosclerotic calcifications and normal ossestructures, such as the anterior clinoid process, obscuring tunderlying vessel and less frequently mimicking the appearanof an aneurysm on CTA surface renditions (seeFig. 4-8G andH); (8) the operator-dependent nature of the 3D reconstructioprocess. Calcification can be a problem with CTA, MRA, aeven catheter angiography. With moderate calcification CTA
superior to MRA for assessing degree of stenosis, but with hecalcification the lumen may be obscured on CTA but visible oMRA.
Detection of aneurysms near the skull base (e.g., cavernous aneurysms) is limited by bony artifact. Although workstions have improved the ability to detect aneurysms near the skubase, in particular within and adjacent to the cavernous sinus, skat image manipulation is often required to make aneurysms this region visible. Depending on how one “windows and levethe source images, small aneurysms may be missed or infunbular widening of the origins of small vessels may be mistaken aneurysms.
Arterial catheter angiography (Fig. 4-9) is the definitive imagingmodality for vascular lesions of the brain and great vessels of neck but has been relegated to a secondary role in the diagnosof stroke. Patients are referred for angiography for the followreasons: (1) if the MRA, CTA, or carotid ultrasound are equivcal; (2) if MRA is contraindicated (e.g., in patients with pacemers); (3) if cardiac output is too low to produce a diagnostic CT(4) to evaluate complex aneurysms or vascular malformatiresponsible for an intracranial hemorrhage; and (5) for the evaltion of vasculitis. The advent of rotational 3D digital subtractiangiography has made it possible to combine the advantagesselective arterial injection of contrast with the 3D imaging intrsic to CTA.
For assessment of AVMs and fistulas selective catheter angioraphy is necessary to obtain time-resolved images that separaarterial and venous components of the malformations. Althouhigh-field MRA and CTA may suggest the correct diagnoof vasculitis, the absence of evidence of vasculopathy does nexclude this diagnosis. Because the treatment of this disordis not without risk, catheter angiography may be performed confirm or exclude the diagnosis and may be used to determithe best site for biopsy if necessary. Angiography is a safe (but harmless) study and in many situations provides crucial informtion. The incidence of all complications for femoral artery caeterizations is approximately 8.5% with the range of permanecomplications (the most significant of which is stroke) from 0.to 0.33%, a 2.6% incidence of transient complications, and a 4incidence of local complications.
In individuals with acute or chronic ischemic disease angiogphy is used in selective cases, in particular if endovascular intvention is contemplated. It is an excellent albeit invasive methfor determining whether a lesion is hemodynamically signific
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 10/66
V ASCULAR D ISEASES OF THE B RAIN 113
H
A B
Left
E
D
C
F
G
F IGURE 4-8. CT angiography (CTA). A , Lateral image of the normal cervical common internal and external carotid arteries.B , Lateral image of linternal carotid artery occlusion (arrow ). C andD , Fifty percent internal carotid stenosis viewed with surface rendered (arrow in C ) and sagittal refmation (D ). Note absence of calcification and low density (lipid) within plaque (arrows in D ). E , Proximal right severe middle cerebral artery steclearly visible (arrow ) in patient with border zone infarcts.F , Aneurysm arising from the left internal carotid artery terminus. Note well-formedbilobed appearance (arrow ). G andH , CTA pitfall: Apparent aneurysm of the left anterior cerebral anterior communicating artery junction (arrow ) on surface-rendered image (G ) is identified as a calcification on CTA source image (arrow in H ).
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 11/66
114 Neuroradiology: The Requisites
in the carotid circulation (Box 4-3). Assessment of collateralcirculation distal to a stenosis or occlusion is most easily deter-mined with catheter angiography, where serial images showthe presence, source, and extent of collateral supply to thebrain.
Detection of ulcerated plaques is more accurate with cath-eter than noninvasive angiography. However, on all types ofangiographic examinations it is difficult to distinguish ulcerationfrom irregularity. The most reliable angiographic sign is the pen-etrating niche, but depression between adjacent plaques and
intraplaque hemorrhage may produce a similar appearance (sFig. 4-9). Luminal bulging secondary to destruction of the medwith an intact intima can also appear as an ulcer. One shouappreciate that the association of ulcer and stroke is also cotroversial. Many asymptomatic plaques are ulcerated and masymptomatic plaques are not. Generally, however, ulcerationfrequently found on the symptomatic side in association wisignificant stenosis. High-resolution surface coil-enhanced Mimaging is an excellent way to evaluate ulcerated plaque brequires hands-on study to optimize planes of section and flosuppression. The best approach presently is for the radiologistdescribe the plaque as smooth or irregular, and if an underminniche is present, the termulceration can be used. It is in the prov-ince of the physician caring for the patient to base therapy on tseverity of findings and on the patient’s symptoms. No studihave documented any greater risk of angiography during an acstroke. The vascular supply to the symptomatic region should the first order of business. What is the current role of angiogphy in hyperacute stroke? It is primarily used in an interventionmode for thrombolysis and stenting.
PerfusionPerfusion imaging aims to characterize microscopic flow at capillary level. The key concept to remember in perfusion imaing is the central volume principle:
A B
F IGURE 4-9. A, Common carotid angiogram showing high-grade stenosis of the left internal carotid artery. Notice the ulceration in a distal(arrow ). B, The patient underwent an angioplasty and stenting procedure. Observe the improved flow and the obliteration of the ulcer by the st(Courtesy of P. Kim Nelson, MD.)
B OX 4-3. Angiographic Findings in Hemodynamically
Significant Lesions of the Extracranial Carotid ArteriesLesions with 50% to 70% reduction of vesel lumen diameter<2 mm residual lumen corrected for angiographic magni-
ficationExternal carotid artery opacification leads internal carotid
artery opacificationDelayed ocular choroidal bluch (>5.6 sec for patients age
>30 yr) with injection of contralateral carotid or vertebralarteries, angiographic filling of ipsilateral carotidcirculation
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 12/66
V ASCULAR D ISEASES OF THE B RAIN 115
CBF = CBV/MTT
Cerebral blood flow is determined by the ratio of cerebral bloodvolume (CBV) divided by the mean transit time (MTT). TheCBF of the normal brain ranges between 45 and 110 mL/100 gof tissue/min. Cerebral oligemia (about 20 to 40 mL/100 g/min) isdefined as underperfused asymptomatic region of brain that willrecover spontaneously, whereas an ischemic hypoperfused brainis symptomatic and at risk to develop irreversible infarct withoutrevascularization. The ischemic threshold identified in animalexperiments when there is cessation of action potential genera-tion occurs around 20 mL/100 g/min and the infarction threshold,associated with irreversible neuronal damage, is at approximately10 mL/100 g/min. Therefore, ultimately, it is CBF that deter-mines whether tissue will live or die, but changes in MTT andCBV reflect the pathophysiologic processes that precede and thendetermine when CBF decreases to nonviable levels. The initialevent is an increase in MTT due to an occlusion or stenosis. MTTwill be determined by the site of occlusion or stenosis and thepresence and type of collateral supply to the affected brain. Theautoregulatory response of the brain is vasodilation of the vascu-lar bed distal to the occlusion or stenosis and increased oxygenextraction from the blood. Vasodilation increases CBV; therefore,initially CBF is maintained or at least does not decrease to thelevel where neuronal death occurs. However, once maximal vaso-dilation is achieved any further increases in MTT (due to progres-sive occlusion, new embolization, or decrease in systemic bloodpressure) will result in decrease in central perfusion pressure, col-lapse of the vascular bed, and decrease in CBV and consequentdecrease in CBF.
Perfusion imaging can be performed in a number of ways, butby far the most common technique in clinical practice involvesan intravenous injection of contrast material that does not tra-verse the blood-brain barrier. Rapid sequential imaging (imagesevery 15 sec) of all or part of the brain allows the visualizationof the effect of the contrast agent as it traverses the vascularsystem. This “bolus tracking” technique is used for both MRperfusion (MRP) and CT perfusion (CTP). In CTP the den-
sity of the brain increases while the iodinated contrast agentpasses the vascular supply; with MRP the intensity of the braindecreases because the paramagnetic gadolinium agent causesT2-shortening (dynamic susceptibility imaging). In both casesone obtains direct measurement of CBV (it is the area underthe curve of the density/intensity change). The time that ittakes the contrast to traverse the brain is the MTT; therefore,the CBF can be calculated using the central volume principle.However, to precisely measure CBV and MTT it is necessaryto eliminate the contribution of contrast within small arteriolesand venules. This requires mathematical “deconvolution” ofthe data. This is easy with CTA, where data from the arterialinput and venous output (obtained by measuring the changesin density within large arteries such as the anterior cerebralarteries and large veins such as the superior sagittal sinus)can be obtained. With MR, this is more difficult because ofthe contribution of flow effects within large vessels. Therefore,the values obtained from CTA are precise mathematical mea-sures of the three perfusion parameters, whereas those obtainedwith MR perfusion are relative values (e.g., rCBV, rCBF,rMTT). With both CTA and MRA parametric MTT, CBV,and CBF maps are generated and evaluated qualitatively.Measurement of absolute values is only possible with CTP.The parametric maps provide somewhat different informa-tion, and each has its advantages and limitations. Becausethe initial event in an infarct is increase in MTT, the MTTmaps are the most sensitive to early ischemic changes, but
because not all areas of elevated MTT go on to infaMTT maps tend to overestimate final infarct volume. measure best correlates with the size of the final infadepends on many factors, including what literature youCBV maps appear to have the best correlation with thmate infarct volume. However, this is controversial, witreports indicating that rCBV underestimated final infarume whereas rCBF overestimates it. Such differences mpart, be related to when the measurement is made (12 versus 24 hours). Perfusion imaging is critical to deting whether or not there is salvageable brain that can btected by use of intravenous or intra-arterial thrombtherapy (tPA), medical therapy, or mechanical clot redevices (MERCI and Penumbra). All of these treatmenassociated with an increased risk of intracranial hemorrhagtherefore, treatment should be reserved for individualcan benefit from recanalization. Individuals in whom thof infarction corresponds to the area of abnormal pershould not be treated regardless of other factors (timeonset of symptoms, extent of infarcted brain) since therebrain to protect. On the other hand in patients where brrisk is greater than the already infarcted brain by more20%, treatment is likely to result in improved outcomebrain at risk is described as the ischemic penumbra. On
the penumbra is the brain tissue surrounding the core sion-“positive” (hyperintense) infarcted brain that has ndiffusion but abnormal relative perfusion (diffusion/permismatch). On CT there is no easy direct way to measuextent of the already infarcted brain; therefore, it is necto use quantitative measures of perfusion to define thedicted infarcted brain (<10 mL/100 g/min) and the penu(10–30 mL/100 g/min) (Figs. 4-10 and 4-11).
Other methods of measuring brain perfusion deserveattention. Nuclear medicine studies, including positron son tomography and single photon emission computed traphy, can be used to generate perfusion maps but haveutility in the workup of acute infarction. Xenon CT cperformed quickly but is not readily available in mosters. Arterial spin labeling (ASL) is an MR perfusion tecthat requires no exogenous contrast agent. In this techthe protons in arteries at the base of the brain are subjto an MR pulse that inverts their spins. The tagged prcan then be measured as they pass through the brain. Inxenon CT and arterial spin labeling the perfusion agent (and tagged water molecules, respectively) freely diffusethe blood-brain barrier; therefore, it is possible to directlsure CBF. However, although CBF is the critical determof brain tissue viability, knowledge of MTT and CBV for understanding of the status of the vascular system just the brain. Arterial spin labeling is currently techncally demanding and not in common use. The amount ofthat can be imaged is small. On the other hand, becaucontrast injection is necessary arterial spin labeling perstudies can be repeated as often as necessary. With technadvances, ASL may become a tool for the routine assesof brain perfusion.
IMAGING OF INFARCTION CT and MR findings change rapidly in the initial week afinfarct, reflecting underlying relatively stereotypically pathiologic changes. In this section we describe each phase batime from infarction, predominant underlying event, and CMR imaging findings (Table 4-1).
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 13/66
116 Neuroradiology: The Requisites
A B C
D E F
G H
F IGURE 4-10. Perfusion imaging. A, Computed tomography (CT) scan 3 hours after onset of left hemiplegia reveals loss of normal gray matter din the right insula (arrows ). CT perfusion parametric maps. Cerebral blood volume (B ), mean transit time (MTT) (C ), and cerebral blood flow (CBF)(D ) reveal decreased perfusion that exceeds the extent of CT hypodensity. MTT map (C ) shows the most dramatic change. The extent of perfusionabnormality exceeds core infarct by more than 20% and therefore the patient is a candidate for thrombolytic therapy assuming other inclusioare met.E, DW image in a different patient reveals a large T2 infarct in the left middle cerebral artery distribution.F–H, Magnetic resonance perfusionmaps.F, Negative enhancement interval, a surrogate for CBV;G , mean time to enhance, a surrogate for MTT;H , Maximum slope of decrease, a CBFsurrogate. All maps reveal decreased perfusion in the left hemisphere that extends beyond the abnormality on DW image, but changes are mosive on the mean time to enhance map (G ). Extent of perfusion abnormality exceeds core infarct by more than 20%; therefore, the patient is a candfor thrombolytic therapy assuming other inclusion criteria are met.
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 14/66
B978-0-323-04521-6.00004-8, 00004
V ASCULAR D ISEASES OF THE B RAIN 117
Hyperacute Infarction (0–6 Hours)Vascular Insufficiency and Cytotoxic EdemaThe initial event that leads to infarction is vascular insuffi-ciency due to focal proximal or distal occlusion or stenosis. Inmost instances routine imaging will not demonstrate the occlu-sion except when there is embolic occlusion of large vessels (e.g.,MCA or basilar artery). Vascular occlusion leads to decreased per-
fusion, which when sufficiently severe or prolonged initiates the“ischemic cascade.” Within 5 minutes of hypoxia, the membranepumps that maintain the disparity between the normal high con-centration of extracellular sodium and the lower intracellularsodium fail. Sodium enters the cell, and the influx of sodium pro-duces an osmotic gradient. Water passively enters the cell, creat-ing “cytotoxic” edema. In addition, calcium enters the cell, whichin turn activates intracellular enzymes that begin to lyse intracel-lular organelles and precipitates proteins. This produces cell lysisand the release of excitatory amino acids (glutamine and gluta-mate) and vasoactive substances, which further compromise themetabolic status of adjacent cells.
During the hyperacute phase, CT may be normal ordemonstrate the “dense vessel” sign when there is an emocclusion of a proximal vessel (Fig. 4-12). The initial parenchmal finding is loss of normal gray matter density withoueffect. The gray matter becomes isodense to adjacent matter, leading to loss of the normal “cortical ribbon”Fig
4-13) or loss of the ability to differentiate the basal ganthalamus from the internal capsule (Fig. 4-14). Loss of cortidensity may occur as early as 3 hours but more typically to 6 hours to develop. This finding is subtle and is often mby inexperienced observers. The advent of PACS readintions has facilitated detection of hyperacute infarctioncan improve detection of loss of gray matter density by ning the window on CT images, thus accentuating gray-density differences (Fig. 4-15). In addition it is helpful to vmultiple slices simultaneously (“tile” rather than “stack” and defocus slightly. Detectable hyperacute infarcts are urelatively large, and viewing multiple images simultan
Ischemic penumbraBrain at risk
DWI normalCBF 10–20 mL/100 g/min
Core infarctIrreversible infarct
DWI + orCBF <10 mL/100 g/min
Normal brainCBF 50 mL/100 g/min
Oligemic regionBrain not at acute risk
CBF 30–50 mL/100 g/min
NO MISMATCH
Don’t treatTreat
>20% mismatch
A B
PERFUSION/DIFFUSION MISMATCH
DWI–CBF 10–30 mL/100 g/min
DWI+CBF <10 mL/100 g/minCore irreversible infarct
DWI+
Core infarct
F IGURE 4-11. Ischemic penumbra. A, Core infarct defined as diffusion-weighted image (DWI)-positive region (area of irreversible infarctinetic resonance or cerebral blood flow (CBF) <10 mL/100 g/min on CT. Ischemic penumbra is region that is DWI normal with CBF of 10 to 2There may be a region of relative oligemia (CBF >30 mL/100 g/min that is not at risk for acute infarction but that might be at risk if there promise of arterial supply).B, Thrombolytic therapy is indicated when the mismatch between core infarct and penumbra is >20% if all othecriteria are met (<4.5 hr duration, no hemorrhage, infarct <30% of the vascular distribution). If mismatch is less than 20%, thrombolyticnot be undertaken because there is insufficient target brain at risk to warrant treatment.
T ABLE 4-1. Ischemic Stroke: MR Intensity, DWI, ADC
Stage T1WI T2WI DWI ADC
Hyperacute (0–6 hrs) Isointense; may be some loss of sulci Isointense Bright LowAcute (6 hrs–4 days) Low intensity; mass effect High intensity Bright LowSubacute (4–14 days) Low intensity High intensity High intensity secondary to T2
shine-throughPseudonormalizatio
Chronic Smaller area of low intensity;encephalomalacia
High intensity High intensity secondary to T2shine-through
High
ADC, apparent diffusion coefficient; DWI, diffusion-weighted imaging; MR, magnetic resonance; T1WI, T2WI, T1-, T2-weighted imaging.
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 15/66
118 Neuroradiology: The Requisites
C
A
B
D
F IGURE 4-12. Hyperacute infarct CT—dense vessel sign. A , Axial image at the level of the circle of Willis at 3 hours reveals hyperdensity in the pmal left middle cerebral artery, indicative of proximal embolic occlusion (arrow ). B , Focal hyperdensity in the left sylvian fissure is indicative of distembolus (arrow ). C , Focal hyperdensity in the basilar tip is present at 4 hours without other evidence of infarction (arrow ). D , Repeat examination at24 hours reveals persistent basilar hyperdensity with new edema of the brain stem and left superior cerebellum, indicative of acute infarctihydrocephalus with dilated temporal horns (arrows ) secondary to acute cerebellar infarct.
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 16/66
V ASCULAR D ISEASES OF THE B RAIN 119
A B C
F IGURE 4-13. Hyperacute–subacute infarct CT. A , Initial scan at 4 hours reveals subtle loss of normal cortical density along the insula (“ibon sign”) and the convexity gyri (arrows ). Note that sulci are visible since there is no mass effect.B , Repeat examination at 36 hours reveals absuniform hypodensity of gray and white matter of the right middle cerebral artery distribution. Mass effect is present with sulcal obliteratiinfarct are discrete and straight (arrows ). C , Repeat examination at 4 days reveals marked increase in mass effect with transfalcian herniatiohyperdensity within the infarct represents reperfusion hemorrhage (arrows ).
A B
F IGURE 4-14. Acute ganglionic infarct. A , CT scan at approximately 4 hours reveals relative hypodensity in the right basal ganglia comparedlonarrow ). The normally hypodense internal capsule visible on the left ( short arrow ) cannot be differentiated from adjacent basal ganglia becausehypodensity.B , Diffusion-weighted MR approximately 1 hour after CT reveals obvious hyperintensity.
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 17/66
120 Neuroradiology: The Requisites
increases the chances of detection. Another “trick” is to reviewthe source images from CTA examinations done as part ofmultimodal CT imaging for acute infarction. The normal brainwill become hyperdense because of the intravascular contrast,whereas the infarcted brain will not change in density, makingthe infarct more apparent (Fig. 14-16). Loss of cortical densityis typically described as cytotoxic edema. Although it is truethat cytotoxic edema is occurring, it is likely that the loss ofnormal gray matter density is not a direct result of this process.
We think of edema as hypodense because the most commoncause of brain edema is disruption of the blood-brain barrier(vasogenic edema) leading to increased tissue water, which inturn produces hypodensity. In cytotoxic edema there is shift
of water from the extracellular space to the intracellular spawithout an increase in the total amount of tissue water. In addtion, at this stage of infarction there is often little or no hypeintensity on FLAIR and T2WI (Fig. 4-17). Because T2WI aremuch more sensitive than CT to changes in tissue water, it unlikely that subtle changes in water would be detected oCT and not MR. A more likely cause of the initial changes CT is decreased CBV. Gray matter is denser than white mattein large part because it has a higher blood volume. Decrease
blood volume renders gray matter isodense to white matteThis concept helps to explain several observations concering acute infarction. For instance, it typically takes approxmately 24 hours for ganglionic hypodensity to be seen in acu
A B
F IGURE 4-15. Use of narrow stroke windows. A, A CT scan at approximately 5 hours reveals loss of normal gray matter density in the left insulacortical gyri, and lateral basal ganglia (note the inability to identify left internal and external capsule white matter).B, The same section with narrowwindows improves visualization of loss of normal gray matter density.
BA
F IGURE 4-16. Computed tomog-raphy angiography (CTA) sourceimages in the detection of hyper-acute infarction. A, Unenhancedscan reveals subtle loss of normalgray matter density in the left mid-dle cerebral artery (MCA) distribu-tion. B, Source image from CTAreveals obvious relative hypoden-sity in the left MCA and anteriorcerebral artery distributions. Lesionis more conspicuous and extensivethan on unenhanced scan.
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 18/66
V ASCULAR D ISEASES OF THE B RAIN 121
anoxic injury (e.g., smoke inhalation and near-drowning). This
relative delay in development of hypodensity likely reflectsthe fact that in anoxic injury there is no decrease in bloodflow but rather a decrease in blood oxygen level. It has beenobserved that infarcts that become apparent on CT within4 hours of symptom onset have a worse prognosis than similar-sized infarcts that do not become apparent until 6 to 12 hours.This most likely is the result of the more profound perfusiondeficit that must be necessary for these infarcts to becomeapparent in the first few hours. One way to improve infarctdetection is to evaluate CTA “source” images. The normallyperfused gray matter becomes hyperdense compared to theunderperfused infarcted brain.
Although large infarcts in the MCA distribution can bedetected within 6 hours in about 75% of cases (at least by expertreaders), the overall sensitivity for detection of all infarcts on CTis only 45% in the first 24 hours. The low rate occurs because ofthe poor performance of CT in detecting small cortical infarcts,cerebellar infarcts, and white matter infarcts. In addition evenwhen an infarct is detected its true extent is difficult to deter-mine. One of the major contraindications to use of intravenoustPA is large infarct size (infarcts that involve more than one thirdof the MCA distribution). Therefore, noncontrast CT is not inand of itself a good tool for assessment of infarction, in partic-ular if intravenous or intra-arterial therapy is contemplated. Itsmajor role is to identify hemorrhagic infarctions and to excludeprocesses such as nonischemic hemorrhage (e.g., hypertensivehemorrhage), masses, or infections presenting as stroke. Notethat the vast majority of infarcts in the first 24 hours are nothemorrhagic.
Because of these limitations, the CT evaluation of infarction inthe hyperacute phase should be performed in conjunction withCTA and CTP (multimodal CT). CTA can demonstrate the pres-ence and location of stenosis or occlusion, and CTP can deter-mine if there is viable brain that can be saved by thrombolytictherapies (Fig. 4-18).
Several MR findings are indicative of vascular insufficiency(Fig. 4-19). It is important to remember that the typical intralu-minal hypointensity is a result of flow effects rather than theintrinsic signal of blood. Blood is a proteinaceous fluid that isrelatively T1 isointense and T2 hyperintense. After contrastadministration blood becomes T1 hyperintense. When flow isslow the intrinsic signal of blood can be “captured.” The MRfeatures of vascular insufficiency include the following: The MRcorrelate of the CT dense vessel sign of acute embolic occlusionis intraluminal hypointensity without associated flow-related
hyperintensity on gradient-echo images. Normally, larg
sels are centrally hypointense on gradient echo with assohyperintensity adjacent to the vessel. The hyperintensityresents signal from the blood that has been spatially disalong the phase-encoding direction due to flow effects. presence of acute clot there is marked hypointensity thatextends beyond the lumen of the vessel (“blooming”) andis no associated flow-related hyperintensity. Chronic occor extremely slow flow in large vessels (e.g., cavernousartery) is manifested by isointensity to hyperintensity on and hyperintensity on T2WI. In the presence of proximal sion or severe stenosis, intraluminal hyperintensity is presFLAIR images due to slow flow. If contrast is given, intralhyperintensity will be more extensive distal to an occlusioin normal circulation.
Hyperacute infarction is T1 isointense and T2 isointenmildly hyperintense. T2 hyperintensity is best appreciatFLAIR (sometimes only in retrospect) and is typically coto the gray matter in thromboembolic infarction. In th24 hours FLAIR hyperintensity is seen in approximatelof cases, but it is seen in less than two thirds of cases swithin 6 hours.
Diffusion-weighted imaging increases the sensitivitdetection of acute infarction to greater than 90% in the hacute period (Fig. 4-20; see alsoFig. 4-17). DWI hyperintesity with ADC map hypointensity can be seen within mof the onset of ischemia in animal models and in clinicawhere patients have the misfortune of developing an infaring or just before the MR examination. These early changthe result of cytotoxic edema. So why should the shift offrom the extracellular to the intracellular space cause resdiffusion? As previously described, diffusion will be rewhen there are cellular and molecular barriers to proton ment. Simply put, there are more barriers within the cellin the extracellular spaces, so the shift of water from thdiffusing extracellular space to the slow-diffusing intraccompartment will restrict diffusion in the volume of brainbeing imaged. However, this is probably not the major carestricted diffusion because the intracellular compartment mally much larger than the extracellular compartment. Choccurring within the cells are the likely source of restrictfusion. With failure of the membrane pump and damagdestruction of intracellular structures, the intracellular enment becomes more viscous, and this produces restrictedsion. Thus, in the vast majority of cases the restricted difis an indicator of irreversible neuronal damage and death.
A B C D
F IGURE 4-17. Hyperacute infarction. Computed tomography (CT) better than FLAIR. A, CT scan at 3 hours reveals loss of normal gray matter din the left basal ganglia insula and frontal and parietal cortex without mass effect.B, FLAIR image obtained at 4 hours reveals no hyperintensityaffected area.C, Diffusion-weighted image reveals extensive ganglionic and cortical hyperintensity indicative of hyperacute infarction.D, Apparendiffusion coefficient map reveals diffuse hypointensity indicative of restricted diffusion.
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 19/66
122 Neuroradiology: The Requisites
than 5% of cases diffusion changes are reversible. In most ofthese instances there is early (<3 hours) spontaneous or thera-peutic recanalization of the occluded vessels. The initial ADCreduction is often less than that seen in most infarcts (~25% ascompared to >75%). It should be noted that in some of thesecases subsequent examinations reveal return of restricted dif-fusion and DWI hyperintensity. These unusual cases probablyrepresent examples of borderline ischemia. If flow is rapidlyreestablished, damaged cells may return to normal metabolicfunction, at least transiently. These cells may fully recover, butmany will go on to cell death (with return of DWI hyperinten-sity) due to continued ischemia or apoptosis (programmed celldeath). In 5% to 10% of cases, the initial DWI study is normalwhen an infarct is present (as confirmed by clinical findings orsubsequent imaging studies). Most of these cases are small infe-rior brain stem or cerebellar infarcts that are obscured by suscep-tibility artifact from the skull base (Fig. 4-21). In some cases, thenormal initial DWI study may be due to pseudonormalization.DWI sensitivity seems to drop in the 8- to 16-hour range, a time
period in which partial recovery of cellular function may resultransient resolution of DWI and ADC abnormalities.
As opposed to CT, unenhanced MR is sufficient to detect essentially all hyperacute infarcts. Therefore multimodal MR (MRMRA, and MRP) is of value only when thrombolytic therapyother aggressive interventions are contemplated. CraniocerviMRA allows for detection of stenosis, occlusion, and dissectiMRP allows for identification of areas of hypoperfusion thmight be the target of thrombolytic therapy.
To appreciate how multimodal CT and MR are used in treatment decisions, it is necessary to understand the risks and benefof those options. It has been shown that intravenous (IV) admistration of tPA improves outcomes (e.g., residual disability) stroke patients in the following circumstances: (1) treatment mubegin within 4.5 hours of symptom onset, (2) no CT evidencehemorrhage, and (3) infarct not exceeding 33% of the distributof the MCA territory. With multimodal imaging, additional criria have been established, including (1) no evidence of occlusof the distal internal carotid artery and proximal MCA and A
A B C
DD E F
F IGURE 4-18. Multimodal computed tomography (CT) in assessment of acute infarction. A, Unenhanced CT scan at approximately 4 hours revealhypodensity in the right posterior lateral basal ganglia and insula (arrows ). B, Source image from CT angiography (CTA) reveals focal filling defectright middle cerebral artery (MCA) just proximal to bifurcation (arrow ).C, CTA image reveals occlusion of a proximal MCA branch (arrow ). Note: CTAimage right-left reversed.D, CT perfusion (CTP) cerebral blood volume (CBV) map reveals focal decreased volume in the region of the brainhypodense on CT. Cerebral blood flow (CBF) map (E ) and mean transit time (MTT) (F ) maps reveal core of infarcted brain surrounded by a large regiof decreased perfusion (brain at risk—penumbra).
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 20/66
V ASCULAR D ISEASES OF THE B RAIN 123
(T occlusion) and (2) the presence of a penumbra of salvageablebrain that represents at least 20% of the overall region of abnormalperfusion (seeFigs 4-10 and 4-17). Application of these criteriaeliminates more than 90% of patients presenting to emergencydepartments with signs of acute infarction (Fig. 4-22). These cri-teria are strict because IV tPA treatment is not benign. The riskof intracerebral hemorrhage, often massive, is high in particular inpatients treated too late or in whom an infarct is too large. IV tPAis ineffective if there is no salvageable brain or there is a proximalocclusion that is unlikely to lyse with IV treatment. Intra-arterialtreatment can extend the therapeutic window to up to 8 hours inthe anterior circulation and up to 24 hours in the vertebrobasilarcirculation. In addition to extending the time window for treat-ment intra-arterial therapy can be used to eliminate proximal clotsthat are unlikely to lyse with IV tPA. Intra-arterial treatmentsinclude direct injection of tPA into the clot via superselectivecatheter placement, manual clot disruption, and removal of theclot with a mechanical device (e.g., MERCI and Penumbra).
Acute Infarction (6 Hours–3 Days)Cytotoxic and Vasogenic EdemaWith continued ischemia, neuronal damage and death toxic edema) increases. Endovascular cells are damaged,ing in opening of the blood-brain barrier and leakage ointo the extravascular space. With increased tissue watebrain swelling occurs. Red cell extravasation may alsoalthough hemorrhage is usually absent or mild. Clot proximal vessels may persist or dissolve and wash “stream” into distal vessels. Leptomeningeal collateral vcan dilate to provide some perfusion to affected brainextent and rate at which vasogenic edema develops deon the blood flow to the affected brain. If there is no fusion, edema is mild and takes longer to develop. If frapidly reestablished (spontaneously or due to treatmenthe vascular bed is damaged, edema will develop rapidhemorrhage may occur.
B CA
D E F
F IGURE 4-19. Vascular insufficiency MR. A , A gradient echo MR image reveals adjacent hyperintensity and hypointensity in the region of the dnal carotid arteries and middle cerebral arteries. Hyperintensity is the spatially misregistered signal from flowing blood, and the hypointention of the artery (arrows ). B , A CT scan reveals hyperdensity in the horizontal segment of the right middle cerebral artery (MCA) (arrow ).C , A gradieecho scan in the same patient reveals corresponding hypointensity with “bloom” effect and absence of hyperintensity of flowing blood whethe left MCA (arrow ).D, Anteroposterior catheter angiogram of the right carotid artery demonstrates complete occlusion of the right internal cat its origin.E , A gradient echo MR image reveals a focus of marked hypointensity, indicative of acute clot (arrow ).F, A FLAIR image reveals intralumhyperintensity distal to the clot, indicative of slow flow (arrows ).
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 21/66
124 Neuroradiology: The Requisites
E
A B
D
C
F
F IGURE 4-20. Hyperacute embolic infarct: CT at 3 hours, MRI at 3 hours 30 minutes. A , CT reveals loss of gray-white differentiation in the righoccipital lobe (arrow ).B , FLAIR image reveals subtle T2 hyperintensity in the temporal and occipital gyri (arrows ).C , Diffusion-weighted image revealshyperintensity in the affected gyri.D, ADC map reveals obvious hypointensity, indicative of restricted diffusion.E , A gradient echo scan reveals focus ofsusceptibility hypointensity in the region of the posterior cerebral artery branch, indicative of intraluminal clot.F , Follow-up CT scan at 30 hours revealsabsolute hypodensity and sulcal effacement.
A B
F IGURE 4-21. Diffusion-weighted image (DWI) of negative acute infarct. A , Initial DWI in a patient with lateral medullary syndrome at 8 houB , Repeat exam at 24 hours reveals subtle DWI hyperintensity in the right posterior lateral medulla (arrow ).
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 22/66
V ASCULAR D ISEASES OF THE B RAIN 125
Vasogenic edema produces absolute hypodensity in the affectedbrain. In thromboembolic infarcts, the gray matter becomeshypodense and swollen (gyral effacement) (seeFigs. 4-13B and4-20A and G). It is homogeneous and has well-defined smoothto convex borders. Lacunar infarcts are visible as discrete roundto oval foci of hypodensity without mass effect. It is difficult todistinguish between acute and chronic lacunar infarcts on thebasis of a single CT study, although the presence of distinct con-vex margins are suggestive of acute disease. Hemorrhage is typi-cally not present unless there is spontaneous or therapeutic clotlysis. Clot within a proximal vessel will still be visible. There isno parenchymal enhancement at this stage of infarct evolution.
T1 isointensity and T2 hyperintensity (best appreciated onFLAIR) are present in the infarcted brain. In thromboembo-lic infarcts the T2 hyperintensity is confined to the gray matter(Fig. 4-23). Focal swelling and sulcal effacement are present.
The infarct is DWI hyperintense and there is ADC hypoisity indicative of restricted diffusion. Although the extedegree of T2 hyperintensity increases during the acute phinfarction, the extent of DWI abnormality remains relativeble unless there is actual progression of the infarct. DWIvolume measured within 48 hours has been suggested treasonable predictor of outcome in stroke. Lacunar infarcent as foci of T1 isointensity and T2 hyperintensity. As iwith CT it is difficult to distinguish acute from chronic inon T2WI, in particular when there are multiple foci of T2 intensity in the white matter. Finding an acute lacunar inon FLAIR in elderly patients is like trying to find “WaDWI makes detection of acute lacunar infarcts simple sinacute lesions are hyperintense while chronic white mattenar infarction and ischemic change is DWI isointense (Fig. 4-24)Hypointensity on susceptibility-weighted sequences (gradien
A B
C D
F IGURE 4-22. Acute infarct without mismatch. A, Diffusion-weighted image reveals hyperintensity throughout much of the left middle cerebterritory.B, Apparent diffusion coefficient maps reveal hypointensity indicative of restricted diffusion.C, Magnetic resonance perfusion time to enh(MTT) andD, maximum slope of decrease (CBF) reveal perfusion deficit that is the same size as the infarct.
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 23/66
A B C
D E F
F IGURE 4-23. Acute (24-hour) infarct magnetic resonance scan. FLAIR ( A andB ) and diffusion-weighted (C andD ) images reveal hyperintensity inthe left basal ganglia insula and with apparent sparing of the subjacent white matter (arrows in A andC ). E andF, Apparent diffusion coefficient mapsreveal hypointensity indicative of restricted diffusion.
F IGURE 4-24. Acutewhite matter infarct.
A, FLAIR image revealsextensive confluent andmultifocal T2 hyperin-tensity. B, Diffusion-weighted image revealsfocal hyperintense acuteinfarct (“Waldo”) in theright frontal subcorticalwhite matter (arrow ).
A B
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 24/66
V ASCULAR D ISEASES OF THE B RAIN 127
and SWI) may be present, indicative of hemorrhage. Severalstudies have shown that susceptibility-weighted sequences aremore sensitive than CT in detecting subtle hemorrhagic trans-formation of infarction (Fig. 4-25). In addition, these sequencesallow for detection of chronic petechial hemorrhages (microb-leeds), typically the result of hypertension or cerebral amyloidangiopathy (CAA). The presence of microbleeds implies vascu-lar fragility and carries an increased risk of hemorrhagic transfor-mation of infarction and an increased risk of future infarction.Evidence of proximal intraluminal clot or slow flow (see above)can be seen at this stage of infarction, although with slightly lowerfrequency than in the hyperacute phase due to clot resolution.If contrast is given, slow flow within vessels distal to a clot maybe present and sulcal enhancement may be seen as a result ofleptomeningeal collaterals.
Multimodal CT and MR continue to demonstrate the presenceof stenosis or occlusion. Perfusion studies may show persistence
of the penumbra of brain at risk for infarction, but in manthe penumbra will decrease in size as the infarct enlarges inareas of hypoperfusion.
Early Subacute Infarction (36 Hours–5 Days)
ReperfusionBlood flow to the affected portion of the brain is typicalltablished 24 to 72 hours after infarction. Proximal and disare lysed or break up and move downstream. Leptomencollaterals become prominent during this phase. By day ingrowth of new vessels into the area of infarction commThese immature vessels have “leaky” blood-brain barrierresult of these changes, vasogenic edema increases with psive mass effect that typically peaks at around 5 days. Ininfarcts, mass effect can lead to transfalcine or transteherniation. Hemorrhagic transformation most commonly
AB
C D
F IGURE 4-25. Acute infarct with hemorrhagic transformation. A, Computed tomography (CT) scan at 36 hours reveals a discrete hypodense rigtal middle cerebral artery acute infarct with sulcal effacement. Mild central heterogeneous density is present, but there is no definite evidorrhage.B, FLAIR reveals heterogeneous hyperintensity with relative isointensity of gyri.C, B0 image demonstrates T2 hyperintensity surrounrelatively isointense gyri.D, Gradient-echo image demonstrates obvious hypointensity indicative of hemorrhage.
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 25/66
128 Neuroradiology: The Requisites
during this phase of infarction (Fig. 4-26). While vasogenic edemais increasing, cytotoxic edema may actually decrease as neuronaldeath leads to cell lysis. Of course if there is ongoing ischemia,new areas of infarction with cytotoxic edema may develop.
The infarct is hypodense on CT (Fig. 4-27). In thromboembolicinfarcts, hypodensity involves both the gray matter and adjacentwhite matter. Density is more heterogeneous than in the acutephase with streaky mild “gyral” hyperdensity representing eitherreperfused cortex or hemorrhagic transformation (seeFig. 4-13C).Frank hyperdense gyriform hemorrhage may occur. The marginsof the infarct are less distinct. Mass effect increases. The degreeof edema and mass effect is determined by the size of infarctionand the extent of arterial recanalization. In severe cases (“malig-nant infarct”), there may be transfalcine or transtentorial hernia-tion (seeFig. 4-27). Intraluminal clot (dense vessel) is no longervisible. Contrast-enhanced scans may demonstrate parenchymal
enhancement. In cortical infarction, the enhancement is typicalgyriform. In deep gray matter (ganglionic and thalamic) enhancemis often peripheral and may mimic that seen in necrotic masses.
The infarcted brain is mildly T1 hypointense and marked Thyperintense (Fig. 4-28A and B). The T2 hyperintensity involvesboth gray and white matter and the margins are ill-defineIntraluminal clot and distal slow flow are not present. Differentiatbetween bland reperfused gray matter and hemorrhagic transfmation is straightforward on MR. Hemorrhagic transformatproduces mild to moderate T2 hypointensity and marked hypoitensity on susceptibility-weighted sequences. Intensity on DWand ADC maps is variable at this stage, reflecting the extent cytotoxic edema (decreased ADC) and vasogenic edema (increaADC). In most cases, DWI hyperintensity persists (seeFig. 4-28C),but ADC hypointensity becomes less apparent or resolves if cytoxic edema decreases or there is extensive vasogenic edem
A B
F IGURE 4-26. Acute infarct. Hemorrhagic conversion. A, Computed tomography (CT) scan 3 hours after onset of symptoms reveals loss of normalmatter density in right temporal parietal cortex (arrow ). Patient treated with intravenous tissue plasminogen activator.B, CT scan at 18 hours revealshemorrhagic conversion of infarction.
F IGURE 4-27. Subacute “malignant infarct.”Computed tomography scan 40 hours afteronset of symptoms with progressive obtun-dation. A, Scan at level of suprasellar cisternreveals marked hypodensity in right middlecerebral artery (MCA) distribution. The supra-sellar cistern is obliterated (long arrow ), theright temporal horn ( short arrow ) is mediallydisplaced, and the left temporal horn is dilated,indicative of transtentorial herniation.B, Scanat level of lateral ventricles reveals hypoden-sity throughout the right MCA territory withsomewhat ill-defined anterior and posteriormargins (arrows ) and marked mass effect withtransfalcine herniation.
A B
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 26/66
V ASCULAR D ISEASES OF THE B RAIN 129
(Fig. 4-29). In some cases, DWI hyperintensity may decrease orcompletely resolve during this phase. If contrast is administered,parenchymal enhancement may be encountered that is similarto that seen on CT. Leptomeningeal enhancement becomes lessapparent or resolves. When the infarct involves the corticospinaltract (e.g., posterior limb of internal capsule) wallerian degenera-tion occurs, resulting in mild T2 hyperintensity, and mass effectmay be seen in the ipsilateral cerebral peduncle and pons thatshould not be mistaken for an additional area of infarction.
Multimodal CT and MR at this stage of infarction offervery little value in the absence of new clinical abnormalities.Perfusion imaging will demonstrate expansion of the CBF defectto “fill in” the penumbra and decrease in the MTT defect withrevascularization.
Late Subacute (5–14 Days)Resolving Edema and Early HealingOver time, edema is resorbed with resultant decreasedeffect. Macrophages and glial cells enter the area of infand begin to remove dead neuronal tissue. Cytotoxic eresolves. Blood flow is reestablished. Mild reperfusion rhage can occur, but symptomatic hemorrhagic transforis rare.
Density becomes more heterogeneous. The infarct cally remains hypodense; however, as edema resolves antical density is at least partially reestablished, there maytransient period when the infarct is isodense to normal(fog effect) (Fig. 4-30). Mass effect resolves and there be early evidence of focal atrophy. If significant hemo
F IGURE 4-28. Early subacute to chronic infarct magnetic resonance imaging. T1-weighted image (T1WI) ( A ), FLAIR (B ), and diffusion-weighimage (DWI) (C ) at 36 hours reveal mild gyral swelling and mild hypointensity on T1WI (arrow ) ( A ) and cortical hyperintensity on FLAIR (B ) (arrowsand DWI (C ). T1WI, (D ) FLAIR (E ), and DWI (F ) at 1 month reveal focal atrophy and hypointensity on T1WI (D ). On FLAIR (E ) T2 hyperintensiis present in the subcortical white matter. The overlying cortex, which was previously hyperintense, is now isointense (arrows ). On DWI (F ), the chroninfarct is mildly hypointense.
A B C
E FD
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 27/66
130 Neuroradiology: The Requisites
transformation has occurred, the hemorrhage will undergo typi-cal evolutionary changes. Lacunar infarcts appear as nonspecificfoci of hypodensity in the deep gray matter or periventricularwhite matter. If contrast is administered parenchymal enhance-ment often occurs and is increased in extent compared to thatseen in the early subacute phase. The presence of enhancementin isodense regions of subacute infarction improves detectionbut may create a diagnostic dilemma because it may be mis-taken for neoplastic or inflammatory disease. As always, clinicalinformation is critical in differentiating between disease pro-cesses, in particular if the initial imaging occurs during the latesubacute phase of infarction.
T1 hypointensity and T2 hyperintensity persist. Thereis no MR equivalent with the “fog effect” seen on CT. Inthromboembolic infarcts, these intensity changes are mostmarked in the subcortical white matter beneath the infarctedcortex. The overlying infarcted gray matter may be nearly
isointense to normal cortex on T1- and T2-weighted sequenceDWI reveals isointensity to mild hyperintensity. ADC mapdemonstrate hyperintensity indicative of increased diffusion. Therefore, residual DWI hyperintensity is the result oT2 shine-through (seeFig. 4-30D). Susceptibility-weightedsequences may reveal hypointensity due to subacute to chronhemorrhage. Because pathologic studies reveal small amounof hemorrhage in most infarcts, improvements in detection susceptibility effects (e.g., high-field MR, SWI) will inevitablead to increased detection of small amounts of hemorrhage thare not clinically significant. Lacunar infarcts are T1 hypoitense and T2 hyperintense. DWI hyperintensity has typicallresolved, although mild residual hyperintensity due to T2 shinthrough may be present. ADC maps reveal increased intensitEnhancement frequency and pattern are similar to that seen oCT with the same caveats about differentiation between subacuinfarction and other disease processes.
A
D E F
B C
F IGURE 4-29. Early subacute infarct magnetic resonance imaging. A, Hyperacute infarct (4 hours) reveals subtle hyperintensity in the insular cort(long arrow ) and intravascular hyperintensity ( short arrow ) on FLAIR. Diffusion-weighted image (DWI) hyperintensity (B ) and apparent diffusion coef-ficient (ADC) hypointensity (C ) present in the insula and right frontal cortex.D, At 3 days the infarct is hyperintense on FLAIR with involvement both gray and white matter.E, Infarct is markedly hyperintense on DWI.F, ADC map hypointensity is relatively mild compared to prior examinatiindicative of resolving restricted diffusion.
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 28/66
V ASCULAR D ISEASES OF THE B RAIN 131
Chronic Infarction (>2 Weeks) HealingEdema has completed resolved. Dead neuronal tissue is removedand replaced by gliosis and cystic degeneration (cystic encepha-lomalacia). Infarcted cortex demonstrates pseudolaminar necrosis(pseudolaminar because it is not confined to a specific corti-cal layer). Lacunar infarcts are typically small fluid-filled cavi-ties surrounded by zones of gliosis (a “true” pathologic lacune).There is focal volume loss. Depending on the size and location ofthe infarct, this results in focal cortical atrophy or focal dilatationof the adjacent ventricle (Fig. 4-31). If the infarct involves thecorticospinal tract, there will be wallerian degeneration, produc-ing atrophy of the ipsilateral cerebral peduncle and ventral pons(Fig. 4-32).
Hypodensity is present in the infarcted brain. With thrombbolic infarction, this is most marked in the subcortical whiter with portions of the overlying gray matter appearing nomildly hyperdense. It is important to note that although thelying cortex may be normal in density it is not functional. CCT hypodensity that is present in the hyperacute and acute of infarction evolves into subcortical hypodensity with rcortical hyperdensity. Lacunar infarcts appear as discrete hypodensity that are difficult to differentiate from acute linfarcts and chronic ischemic white matter disease. Focal aleads to sulcal enlargement or local ventricular dilatationenhancement may persist for up to 2 months but more oftresolved by the end of 3 weeks. Wallerian degeneration isfested by focal atrophy of the ipsilateral cerebral peduncventral pons (seeFig. 4-31).
A
D E F
B C
F IGURE 4-30. Late subacute infarct computed tomography (CT) and magnetic resonance (MR) imaging. A, CT scan 3 days after onset of symptreveals focal hypodensity in the left frontal lobe and caudate nucleus with mild mass effect.B, Repeat CT at 11 days reveals near-complete resolof hypodensity. Isodense infarct not visible. FLAIR (C ) and diffusion-weighted image (D ) on same day asB reveals obvious T2 hyperintensity withe infarct (C ) with mild residual DWI hyperintensity (D ) due to T2 shine-through.E, MR at 25 days reveals little apparent change on FLAIR.F, Notmarked T1 cortical hyperintensity within infarct on T1-weighted image due to laminar necrosis, not hemorrhage
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 29/66

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 30/66
V ASCULAR D ISEASES OF THE B RAIN 133
herniation. The superior vermis can herniate upward throughthe tentorium, whereas the tonsils and inferior vermis may her-niate downward into the foramen magnum. Treatment of acutecerebellar infarction producing such mass effect involves ven-tricular drainage and cerebellar/posterior fossa decompression,often with bilateral occipital bone craniectomy or resection ofinfarcted brain.
ANOXIA, HYPOXIA, AND BRAIN DEATHAnoxic and hypoxic injuries to the brain occur when there isdecreased oxygen content of the blood. Anoxic injuries occurwhen there is near-complete absence of oxygen in the bloodfor more than 5 minutes, whereas hypoxia occurs when there
is partial but more prolonged hypoxemia. Clear separation ofthese entities can be somewhat difficult because a short periodof anoxia can give way to hypoxia and both conditions can becomplicated by hypotension (either as a cause or an effect).Anoxia can be seen in cardiac arrest, prolonged seizures, stran-gulation/hanging, near-drowning, and smoke/carbon monoxideinhalation.
In anoxic injuries, the metabolically active areas of the brainare most severely affected, including the basal ganglia andAmmon’s horns (dentate nucleus and hippocampus). The ear-liest CT finding is loss of the ability to differentiate the basalganglia and thalami from the internal capsules due to subtleloss of normal gray matter hyperdensity. With time, obvioushypodensity and mass effect become apparent. It is importantto stress that CT abnormalities take at least 12 and more com-monly 24 hours to become manifest. Thus, a normal CT scanobtained on admission or after a cardiac arrest does not implya good prognosis (Fig. 4-34A and B). The delayed appearance(as opposed to that seen in hyperacute infarction) probablyresults from the fact that CBV is maintained (in hyperacuteinfarction it is diminished); therefore, CT changes are not vis-ible until vasogenic edema has developed. On MR, anoxicinjuries are visualized much earlier (3 hours) due to cytotoxicedema and cell death resulting in DWI hyperintensity andrestricted diffusion on ADC maps (seeFig. 4-34C–F). If thepatient survives, chronic anoxic injury results in basal gangliaand hippocampal atrophy with secondary dilation of the tem-poral and frontal horns of the lateral ventricles. The frontalhorns lose their normally concave contour and become flat-tened or convex.
Carbon monoxide toxicity produces anoxic injury by ping the binding of oxygen to hemoglobin. Changes are simthose seen in anoxia but are most marked in the bilateral pallidus. A delayed encephalopathy begins 2 to 3 weekrecovery and occurs in 3% of patients, resulting in additionings of high intensity on T2WI in the corpus callosum, subU fibers, and internal and external capsules associated wiintensity on T2WI in the thalamus and putamen (see Charegarding postanoxic encephalopathy).
Prolonged hypoxia results in damage to those portiothe brain that are farthest from the heart. The basal glia and hippocampi are relatively spared. Edema devat the gray-white junctions similar in location to that swatershed infarction; however, in hypoxia changes a
fuse rather than multifocal. CT will initially be normathere is subsequent development of diffuse cerebral ewith loss of definition of gray-white junctions. MR reveand DWI hyperintensity with restricted diffusion at thewhite junctions bilaterally. Because the process is diffis possible to overlook the changes on DWI, in particuinfants.
In severe cases, anoxia or hypoxia progress to thewhere there is diffuse edema with sulcal and cisternal eration. The increased intracranial pressure produces cand tonsillar herniation with complete cessation of CBFdeath). On CT, the brain is diffusely hypodense with nowhite matter differentiation and is nearly completely feless. The ventricles are small, and the sulci and cisternnot visible. The vessels around the circle of Willis and thand tent remain relatively hyperdense and may be misfor SAH.
VASCULOPATHIES (TABLE 4-2 )The vasculopathies are an interesting and heterogeneous of diseases. Vasculopathy is preferred to the traditional tervas-culitis because some of these diseases do not have an inmatory component. Vessel changes may be due to endodamage and thrombosis produced by circulating anantibody complex (systemic lupus), mural edema, or Inflammation, when present, may be the cause of the vaprocess or a late phenomena occurring as a result of the vinsult. Prolonged insults may result in fibrosis and fixed ning regardless of the initial insult. Many of these diseases h
A B C
F IGURE 4-33. Acute cerebellar infarction. A, Computed tomography scan demonstrating an acute cerebellar infarct having a variegated anteand producing significant mass effect with compression of the pons and fourth ventricle.B, Higher section revealing acute hydrocephalus from comsion of the fourth ventricle by the cerebellar mass effect. The superior vermis is also involved (arrows ) and the swollen cerebellum compresses the supvermian cistern (not visualized).C, Enhancement on T1 in the infarcted cerebellum is seen.
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 31/66
134 Neuroradiology: The Requisites
immunologic basis, resulting in vascular injury. In other cases theinflammation may be extravascular (e.g., brain parenchyma orleptomeninges) with compression of the vessel leading to spasmand then mural inflammation. Catheter angiography remains theimaging “gold standard” for detection and characterization ofvasculopathy. CTA and MRA are capable of documenting proxi-mal occlusion and stenosis but do not provide sufficient detail forreliable detection or exclusion of vasculopathic changes in sec-ondary or tertiary intracranial vessels (e.g., sylvian and convex-ity MCA branches). 3T MRA allows for routine visualization ofthe secondary and tertiary vessels as well as the lenticulostriatearteries and it is therefore the preferrednoninvasive angiographicexamination for the workup of vasculopathy. Often, however,final diagnosis requires biopsy to see meningeal or parenchymalsmall-vessel inflammatory changes. While the primary diseaseoccurs within the vessel wall or lumen, catheter angiographicstudies are often normal (10% of patients undergoing catheterangiography for vasculitis actually have it angiographically doc-umented) because many of these diseases affect small arteries
and arterioles that are too small to be detected even with hig resolution catheter angiography. Hence, biopsies of meningevessels, and parenchyma are often still required to diagnosome vasculitides.
Brain imaging features depend on the location and extent of thvascular pathology as well as systemic abnormalities. “Territor(e.g., MCA, ACA) infarcts are seen with proximal vessel invoment, and small deep white matter and ganglionic infarcts aencountered when there is involvement of deep perforating arteies. Parenchymal and superficial SAH may occur because of diarterial disease. Associated abnormalities can be seen secondto nonvascular involvement by the disease process (e.g., hydcephalus in tuberculosis, enhancing meninges in sarcoidosiMany of the vasculopathies are systemic diseases; therefore laoratory, clinical, and imaging evidence of involvement of othorgans provide important clues as to correct diagnosis.
Because of the large number of causes of vasculopathy and tsimilarity of the appearances of many of these diseases, it is easto discuss these processes based on the location of the abnormali
BA C
ED F
F IGURE 4-34. Anoxic injury. A, Computed tomography (CT) scan obtained 8 hours after cardiac arrest reveals normal density of basal ganglia thand cortex with good visualization of the normal hypodense internal capsules (arrows ). B, Repeat examination at 36 hours reveals hypodensity in thbasal ganglia and thalami (note inability to identify the internal capsule). Diffuse brain edema is present with early loss of gray matter densityobliteration (arrows ). C–F, Magnetic resonance (MR) scan at 6 hours in a different patient. CT scan 1 hour prior to MR was normal. Mild T2 htensity (C ) is present in the basal and ganglia bilaterally. Diffusion-weighted image (DWI) hyperintensity (D ) and restricted diffusion (E ) is present.Hippocampal DWI hyperintensity is also present (arrows ) (F ).
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 32/66
V ASCULAR D ISEASES OF THE B RAIN 135
T ABLE 4-2. Vasculopathy
Disease Age (yr) Sex Etiology Special Features
ExtracranialFibromuscular dysplasia >50 F > M Unknown Extracranial internal
artery (C2) and vertebralarteries; multiple vessels
Giant Cell Arteritis 70 F > M Associated with polymyalgia
rheumatica
Extracranial vessels in
particular superficialtemporal arterySkull Base—Circle of WillisMoyamoya disease 10–30 M = F q25.3, on chomosome17 Childhood and adu
variantsSickle cell disease 10–20 M = F Sickle cell More common in chi
transfusions reduce risk;may mimic moyamoyadisease
Basal meningitis 5–15 M = F Tuberculosis and fungaldisease
Also affects basilar arterydeep collaterals lesscommon
Cocaine abuse 20–40 M = F Chronic vasospasm leadsto fibrosis
Rare
Secondary and Tertiary VesselsInflammatory Granulomatous1) Primary angitis of the central
nervous System (PACNS)2) Polyarteritis nodosum3) Wegner’s granulomatosis4) Sarcoidosis5) Behçet’s disease
5030–5020–6020–4020–30
F = MM > FM > FF > MM > F
AutoimmuneAutoimmuneUnknownUnknownAutoimmune—HLA-B51?
Middle Eastern descent,brain stem involvement
Infectious 1) Herpes zoster2) Tuberculosis and fungal3) Neurosyphilis
>5020–40 >50
F = MM = FM > F
Spread along fifth nerve fromfacial zoster infection
Often in association with basalmeningeal disease
Late tertiary phase of disease
Often immunecompromised (e.g. HIV)
Noninflammatory 1) Drug related2) Pregnancy, puerperium, birth
control pills
20–5020–40
M > FF (duh)
Vasospasm and mural edema;inflammation late, Vasospasm
edema, eclampsia
Acute hypertension mayproduce PRES
Cocaine, amphetamines,Sympathomimetic amin(e.g. Ephedrine )
Lymphomatoid Granulomatosis >50 M > F Epstein Barr –inducedlymphoma
Small Vessel
Collagen Vascular Diseases 1) Systemic lupus erythematosus
(SLE)2) Anti-cardiolipin and
anti-phosolipid antibodysyndrome
3) Sjögren syndrome
20–50
20–50
40–60
F > M
F > M
F > M
Autoimmune
With or without SLE
Autoimmune
Relative sparing ofperiventricular whitematter
Cortical infarcts due toemboli (Libman-Sacksendocarditis)
4) Radiation change Any M = F Fibrinoid necrosis Confluent white matdisease; months to yearsafter treatment; focal ma
like lesions less common5) Migraine headache 20–50 F > M Vasospasm Few lesions, subcortfrontal lobes
6) HIV encephalitis <15 M = F Inflammatory Vasculitis Deep gray; basal gacalcification in children
7) Susac’s syndrome 20–40 F > M Idiopathic Corpus callosuminvolvement frequent;lesions smaller than in MMicro-infarcts in cortex
Cerebral Autosomal DominantArteriopathy with SubcorticalInfarcts and Leukoencephalopathy(CADASIL)
30–50 M = F NOTCH 3 Gene onChromosome 19
Predilection for the anterifrontal and temporal lob(60%–100%)
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 33/66
136 Neuroradiology: The Requisites
rather than the etiology. Broadly the vasculopathies can be said toaffect (1) extracranial and extradural arteries; (2) arteries at the skullbase at or near the circle of Willis; (3) secondary and tertiary branchesof the carotid or basilar arteries (e.g., sylvian and convexity branchesof the MCA); and (4) small perforating arteries (e.g., lenticulostri-ate arteries). Table 4-2 contains an extensive list of disease processesand potential patterns of involvement.
Extracranial and Extradural ArteriesFibromuscular DysplasiaFibromuscular dysplasia (FMD) produces nonatheromatousfibrous and muscular thickening alternating with dilation of thearterial wall, producing an appearance characterized as a “stringof beads” (Type 1 FMD) (Fig. 4-35). Less common appearancesinclude unifocal or multifocal tubular stenosis (Type 2) or lesionsconfined to only a portion of the arterial wall (Type 3). Althoughall layers of the artery may be involved, the media is most com-monly affected, with hyperplasia producing arterial narrowingand thinning associated with disruption of the internal elasticlamina, producing saccular dilations (pseudoaneurysm picture).FMD involves the cervicocephalic arteries in 30% of cases withthe most common the internal carotid artery, approximately 2 cmfrom the bifurcation (around C2) in 90% of cases. The vertebralartery is involved in approximately 12% of FMD. Multiple vesselinvolvement is common (bilateral carotid involvement occurs in60% of cases), whereas intracranial FMD is rare. Dilated regionsare always wider than the normal lumen, and narrowing is usuallyless than 40% diameter stenosis. Complications of FMD includedissection (which may be difficult to differentiate from FMDalone) and cavernous carotid fistulae. A higher rate of intracranialaneurysms may be due in part to pseudoaneurysm formation.
The etiology of FMD is unknown. The condition has a markefemale predominance (4 to 1) with a mean age of 50 yeaSymptoms and findings, such as headache, TIAs, stroke, vascudissection, or SAH, have been reported. The differential diagnoof FMD includes atherosclerotic disease, vascular spasm seconary to the catheter, and (on catheter angiography) standing wavAtherosclerotic disease is usually asymmetric and has a propenfor the bifurcation. Catheter spasm can be identified at the tiof the catheter, and standing waves do not usually have the costrictive picture characteristic of FMD. Dilatation of the vesselnot seen with catheter spasm. When diagnosis is in doubt, evalution of systemic vessels, including the renal arteries, may confidiagnosis.
Giant Cell Arteritis (Temporal Arteritis)This disorder tends to involve the media of systemic vesseThe temporal artery is usually affected. Most patients are ovage 70 years, and females outnumber males. Polymyalgia rhematica occurs in approximately 40% of patients with giant carteritis. Patients are seen most commonly with visual loss aheadache, usually with tenderness, swelling, and nodularity ovtheir temporal arteries. The lesions tend to be scattered along thartery so that angiography may be useful in demonstrating vculitic changes in the temporal artery and in guiding the biops
Intracranial arterial involvement is rare but has been reported.Skull Base/Circle of Willis
Moyamoya Disease ( Fig. 4-36 )In this disease, there is progressive stenosis and then occlusion of distal internal carotid arteries and their proximal first-order branc(the circle of Willis). Because the process develops over a long peof time and occurs in young patients, extensive collaterals deveto supply the brain distal to the circle of Willis. These collaterinclude dural vessels (e.g., external carotid artery to orbital brancof the internal maxillary artery to transethmoid collaterals to tinferior frontal ACA branches), leptomeningeal collaterals from theposterior cerebral arteries (splenial branch to pericallosal arterydistal ACA and MCA territory), and deep perforating lenticulostrarteries. These collateral vessels produce an appearance on anggraphy termedmoyamoya, which in Japanese translates to “hazy likea puff of cigarette smoke.” Moyamoya disease was first reporin and most commonly encountered in Japanese patients, but it not restricted to this population. It is now believed to be linked tospecific genetic defect (q25.3, on chomosome 17). The disease mbe divided into pediatric and adult subgroups on the basis of clincal course and disease features. In children, moyamoya has a mprogressive course, presenting with symptoms of cerebral ischemincluding TIAs and stroke, whereas in adults intraparenchymal asubarachnoid hemorrhages are the most common presentationOver time dementia develops due to progressive compromise of vascular system and chronic hypoxia.
Moyamoya may be an epiphenomenon of numerous vasclopathies that may lead to proximal artery stenoses, includineurofibromatosis with internal carotid artery stenoses, radiatvasculopathy, severe atherosclerosis, and sickle cell vasculopatComputed tomography angiography and MRA are capabledemonstrating the stenotic or occluded arteries at the base othe brain and information about collateral supply (see Fig. 4-36Eand F), but these studies cannot provide the necessary detail antime-resolved images for full evaluation of the collateral supplythe brain, in particular if revascularization procedures are conteplated. Catheter angiography (see Fig. 4-36G) demonstrates distalinternal carotid artery and proximal first-order branch stenosocclusions with the extensive collaterals from the vertebral aexternal carotid arteries. The lenticulostriate and other perforaing arteries are dilated and irregular, producing the characterismoyamoya appearance. On CT, mottled hyperdensity may be visibin the basal ganglia. On axial MR, foci of T1 and T2 hypointens
F IGURE 4-35. Fibromuscular disease. “String of beads” appearance ofboth the carotid (open arrows ) and vertebral (closed arrows ) arteries onthis lateral right common arteriogram with reflux up the right vertebralartery.
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 34/66
V ASCULAR D ISEASES OF THE B RAIN 137
are seen in the basal ganglia. Sagittal and coronal images revealthese foci to be curvilinear hypointensity indicative of the exten-sive basal ganglionic vascular collateral network that is virtuallypathognomonic of this entity. Slow-flow luminal hyperintensitymay be visible on FLAIR in the deep and superficial arteries (seeFig. 4-36B). There is absence of normal flow voids within the
distal internal carotid arteries and proximal MCA and ACenhanced T1WI slow flow within collateral vessels at the the brain and leptomeninges may be seen (seeFig. 4-36C and D)Brain parenchymal changes include deep ganglionic and csubcortical infarcts, ganglionic hemorrhages, and superficiSerial studies demonstrate development of atrophy.
BA C
ED F
G
F IGURE 4-36. Moyamoya disease. A, Axial T2-weighted image (T2WI) at the level of the suprasellar cistern reveals absence of normal flothe distal internal carotid arteries. Small arterial branches along the sylvian fissures represent middle cerebral artery (MCA) branches (arrows ). B, AxiFLAIR image at the level of the basal ganglia demonstrates multiple T2 hyperintense foci within the basal ganglia, representing slow flowlenticulostriate arteries (arrows ). Axial (C ) and coronal (D ) contrast-enhanced T1WI demonstrate multiple small vascular structures along the the bilateral proximal MCAs. Small serpentine enhancing vessels along the gyrus rectus and dilated lenticular arteries are present ( small arrows inC anD ). Leptomeningeal enhancement is present in the occipital lobes (long arrows inD ). Frontal (E ) and lateral (F ) magnetic resonance angiography imof the right carotid artery demonstrate occlusion of the supraclinoid internal carotid artery ( short arrows ) with numerous small collateral branches iregion of the M1 segment of the MCA (long arrows , E ). Note enlarged ophthalmic artery (long arrow in F ) and poor filling of distal MCA brancheGCatheter angiogram confirms occlusion of the distal internal carotid artery ( short arrow ) with filling of the right posterior cerebral artery (PCA) angrade filling of the pericallosal artery via leptomeningeal collaterals (long arrow ). Note acute right MCA infarct in A andC .
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 35/66
138 Neuroradiology: The Requisites
Sickle Cell DiseasePatients with sickle cell disease have an incidence of cerebrovascu-lar occlusive disease ranging from 5% to 17%. Children are at higherrisk than adults. A common misconception is that occlusion of thecapillaries, small venules, and arterioles by sickled red blood cells(RBCs) is responsible for the infarction in these patients. Althoughthis may happen, it is not the most important pathophysiologic ele-ment in the vast majority of cases. Rather, infarction is most likelyrelated to stasis and ischemia in the vasa vasorum, leading to inti-mal and medial hyperplasia with eventual significant narrowing orocclusion of the internal carotid artery or the proximal ACA andMCA. The process occurs over time and collateral vessels develop.Thus, findings are identical to those seen in moyamoya disease.The posterior circulation is usually spared. In U.S. urban centers,sickle cell anemia is a more common cause of moyamoya patternthan moyamoya disease. Its incidence is decreasing with effectivetreatment with blood transfusions to suppress the level of hemo-globin S to less than 30%, producing a decrease in the occurrenceof stroke within 3 years from 67% to 10% or less.
Angiography reveals large-vessel disease in up to 87% ofcases with CNS presentations. At the time of initial infarction,the angiographic manifestations in some cases may be minorwith only mild luminal irregularity and slight arterial narrowing.Angiographic contrast media may precipitate a sickle cell crisis;
therefore, protective measures such as exchange transfusions(decreasing the percentage of hemoglobin S to <20%), volumeexpansion before angiography, supplemental oxygen, and awarming blanket are useful in minimizing angiographic risks.
Brain MR and CT examinations demonstrate findings similar tothose seen in moyamoya disease. In addition foci of T2 hyperinten-sity may be seen. Their appearance is indistinguishable from that ofmultiple sclerosis, but the clinical presentation is different. Theselesions likely result from small-vessel sludging and occlusion.
Granulomatous Meningitis (e.g., Tuberculosis)Patients with severe basal cisternal meningeal inflammationmay develop proximal stenoses and occlusion due to arterialconstriction and spasm. In acute bacterial meningitis this isuncommon; when it occurs it typically leads to massive cata-
strophic infarction. In chronic granulomatous meningitis, stenosisand occlusion may develop slowly and persist for long periods oftime, leading to moyamoya pattern. However, in these diseases,involvement of the basilar artery and its branches is common;therefore, posterior circulation changes occur as well. In manycases of granulomatous meningitis the disease affects the smallperforating arteries that arise within the leptomeninges, leadingto deep gray matter (basal ganglia and thalamus) infarcts. Thecombination of communicating hydrocephalus and deep infarc-tion is highly suggestive of granulomatous meningitis.
Secondary and Tertiary Carotidand Basilar Branch VesselsA large number of disease processes can produce the classicfindings of “cerebral vasculitis.” Long segments of vessels areinvolved circumferentially. Circumferential tapered stenosis ofarteries alternate with regions of normal to enlarged vessel cali-ber. Multiple short segments of narrowing may produce a “stringof beads” appearance. Typically vessels in multiple vascular ter-ritories are involved. Focal occlusion may lead to leptomeningealcollateral filling of portions of vascular territory distal to the occlu-sion. Atherosclerosis (in particular in diabetic or hypertensivepatients) can also produce narrowing of these arteries, but thestenosis is typically asymmetric and irregular. Vasospasm associ-ated with SAH produces more diffuse narrowing with no inter-vening regions of normal vessel caliber, often centered at arterialbifurcations.
The imaging workup begins with a CT or MR scan. Presentingsymptoms are quite variable and often nonspecific. Patients may
present with nonfocal findings such as headache or seizures. Fodeficits occur when there is secondary infarction or hemorrhaand depend on the location of these lesions (Fig. 4-37). Thesestudies may reveal one or more cortical infarcts (often hemrhagic), typically within the distal portions of a vascular territFocal parenchymal hemorrhage or superficial SAH may occDeep structures (basal ganglia, thalami, brain stem) are less comonly involved. When there are no focal findings, CT and tolesser extent MR may be normal. On MR intra-arterial hyperitensity on FLAIR and extensive heterogeneous arterial enhancment on enhanced T1WI may indicate the presence of slow floGradient-echo or SWI may reveal microbleeds. CTA and MRmay be normal. 3T MRA will typically reveal involvement secondary arterial vessels (e.g., intrasylvian MCA branches). Mor CT perfusion studies can reveal microcirculatory abnormaties, but more importantly can provide evidence that there is nperfusion abnormality, thus effectively eliminating the diagnsis of vasculitis. Nonetheless, catheter angiography is the gostandard for detecting and characterizing the extent of “vasclitis.”
Noninfectious VasculitisThe angiographic imaging and clinical finding of vasculitis cbe seen in isolation or in association with diseases that produ
systemic vasculitis.Primary angiitis of the central nervous system (PACNS, or gralomatous angiitis of the nervous system) affects parenchymal aleptomeningeal arteries, with a predilection for small arteries aarterioles (200 to 500mm in diameter). This can be a rapidly progressive, frequently fatal disease. The erythrocyte sedimentation rateelevated in more than two thirds of patients, and CSF demonstratelevated protein and pleocytosis in more than 80% of cases.
Wegener granulomatosis (see Chapter 10) is a necrotizing stemic vasculitis that affects the kidneys and upper and lowrespiratory tracts. It can affect the brain, producing stroke, visuloss, and other cranial nerve problems. The peak incidence is the fourth to fifth decade with a slight male predominance. Higintensity abnormalities on T2WI occur in about 28% of casHistory plus positive c-ANCA (antineutrophil cytoplasmic an
body) tests help make the diagnosis.Polyarteritis nodosa is a multisystem disease characterized necrotizing inflammation of the small and medium-sized arterwith CNS involvement occurring late in the disease in more th45% of cases. It is an immune-mediated disease with about 30%patients having hepatitis B surface antigen. Polyarteritis is closrelated to allergic angiitis and granulomatosis (Churg-Strausyndrome). Aneurysms, which are common in the renal asplanchnic vessels, are unusual in the CNS.
Neurosarcoidosis can rarely produce a CNS vasculitis characized by frank granulomatous invasion of the walls of the arterwith or without ischemic changes in the supplied brain parechyma. The angiographic picture is similar to that of PACNThese patients usually have a history of systemic sarcoialthough sarcoid can rarely affect only the CNS (see Chapter Sarcoidosis may also cause inflammation of the small veins lead to microinfarcts from the venous side. The veins are oftinflamed in the meningeal form of sarcoidosis.
Infectious VasculitisTuberculosis and Haemophilus influenzae infections may on occa-sion affect secondary and tertiary arteries. Meningovascular syphaffects both arteries and veins, particularly in the MCA distributiHerpes zoster infections may spread to the cavernous sinus frothe face along the trigeminal nerve branches and then produce aextensive vasculitis with multiple areas of infarction, mimickPACNS. Fungal sinusitis from aggressive Mucor or aspergillosis mayalso affect cavernous sinus vessels. Other inflammatory lesions tcan produce arterial or venous abnormalities (e.g., Behçet diseahuman immunodeficiency virus) are discussed in Chapter 6.
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 36/66
V ASCULAR D ISEASES OF THE B RAIN 139
VasculopathiesThe “vasculitis” pattern may also be seen in conditions in whichinflammation of the vessel wall is not present (based on postmortemstudies). Women who are pregnant, peripartum, or taking birth con-trol pills can develop changes that have traditionally been thought tobe inflammatory but are now believed to be primarily the result ofedema or spasm. The risk of stroke is increased 13 times in pregnancyor the puerperium. Conditions responsible for this increase includehypercoagulability, embolism, migraine, vasculitis, and vasospasm,which result in arterial occlusion or venous thrombosis. The same istrue for drug-related (e.g., amphetamines and cocaine) “vasculitis.”Proposed mechanisms for cocaine-induced strokes include increasedplatelet aggregation with thrombosis, hypertension, direct or indirectarterial constriction, or migraine phenomena induced by the drug.
Cocaine-induced hypertensive episodes have been thoughtresponsible for preexisting aneurysmal rupture and bleedinAVMs. The use of cocaine has been implicated specifically intion of the spinal cord and retina, and in intraparenchymalventricular, and subarachnoid hemorrhage. In all of these conrapid development of systemic hypertension may lead to theopment of posterior reversible encephalopathy syndrome.
Lymphomatoid Granulomatosis(Neoplastic Angioendotheliosis)This malignant lymphoma is restricted to the intracranial vIt presents with recurrent strokes or strokelike symptoms, ealopathy, and seizures. There are multiple high-intensity lon T2WI in the cerebral white matter, often extending alo
BA C
D F
G H
E
F IGURE 4-37. Case 1: Secondary and tertiary arvasculopathy in a 24-year-old patient with coabuse. A, Computed tomography scan revearight subfrontal subcortical hematoma.B, Lateramagnetic resonance angiography (MRA) revedefinite abnormality given the limitations oftechnique.C, Lateral carotid catheter angiogreveals focal areas of narrowing ( short arrows ) andfocal dilatation (long arrows ), indicative of acu“arteritis” or focal arterial wall edema. Casea 39-year-old woman with elevated erythrosedimentation rate, FLAIR images (D–F ) reveaT2 hyperintensity in the right occipital cortex nium of the corpus callosum and parietal sutical white matter.G, Lesions are hyperintenon diffusion-weighted imaging.H, MRA at 3reveals marked irregularity of right posterior bral artery branches.
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 37/66
140 Neuroradiology: The Requisites
perivascular spaces, with associated enhancement. Angiographyshows evidence of medium-sized vascular occlusions. Brain biopsyis needed to establish the diagnosis.
Small-vessel DiseasesInvolvement of small perforating arteries and arterioles character-izes several disease processes. Because of the small caliber of thevessels involved, angiographic studies are virtually always nor-mal. Imaging features consist of deep gray matter, white matter,and subcortical infarcts. Lesions tend to have a different shape(irregular-parallel) along the periventricular white matter, help-ing to differentiate this process from multiple sclerosis (flameshaped-perpendicular). Parenchymal hemorrhage is less com-mon than in other forms of vasculopathy. Earlier age of onset,rapid progression, and more extensive subcortical involvementare clues to correct diagnosis.
Collagen Vascular Diseases (Systemic Lupus Erythematosus, Anticardiolipin, and Antiphospholipid Antibodies Syndromes)Cerebral vasculitis is rarely associated with collagen vascular dis-ease. The primary CNS lesion seen at autopsy in patients withCNS systemic lupus erythematosus is perivascular inflammationor endothelial cell proliferation (similar to pathologic changesin chronic hypertension). True vasculitis is rarely if ever pres-ent (7%) and may be related to infection. The causes of strokein patients with collagen vascular diseases include cardiac val-vular disease (Libman-Sacks endocarditis), an increased ten-dency toward thrombosis (or reduced thrombolysis) related toantiphospholipid antibodies such as lupus anticoagulant or anti-cardiolipin antibodies, and atherosclerosis accelerated by hyper-tension or long-term steroid use. Venous thrombosis is also a risk.Atrophy is commonly found in these patients, related either tothe encephalopathy itself or to the effect of steroid treatment.
Sjögren SyndromeThis autoimmune disease is characterized by focal or confluentlymphocytic infiltrates in the exocrine glands producing clini-cal features of dry eyes and dry mouth; however, 25% of thesepatients have CNS complications, including infarction. The eti-ology of the stroke may be a small-vessel vasculitis; however,these patients also have antiphospholipid antibodies (another
risk factor). Cerebral angiography has been reported as positiveapproximately 20% of cases.
Radiation Vasculopathy ( Fig. 4-38 )Radiation can induce structural damage to arteries, incluing endothelial degeneration, intimal fibrosis, and fibroblasproliferation of the media. Radiation vascular injury should considered as a cause of stroke months to years after therapVascular occlusion of the extracranial portion of the internal carartery rarely occurs after neck irradiation. Intracranial involvemtypically affects small arteries and is therefore angiographicaoccult, but in severe cases there can be diffuse narrowing of sondary and tertiary arteries. Nonetheless, radiation vasculitis the skull base may result in moyamoya phenomenon. MR anCT reveal diffuse white matter abnormality (T2 hyperintensitand CT hypodensity) (seeFig. 4-38). Less commonly, focal radia-tion necrosis will occur at the site of the original neoplasm. Thefoci mimic recurrent neoplasm with progressive heterogeneointensity, central necrosis, irregular enhancement, and peripheral edema. They can be distinguished from neoplasm becauthey are hypometabolic rather than hypermetabolic. Thus, postron emission tomography scans reveal the lesions to be “coland MRS reveals lipid/lactate peaks without N-acetyl aspartaTelangiectasias and cavernous malformations have been asso
ated with radiation therapy (see Chapters 3, 6, and 7). MigraineWhite matter T2 hyperintensity can be seen in 10% to 25% patients with migraine headaches. Lesions are typically few number and have a predilection for the subcortical white mater of the frontal lobes. These lesions are felt to be the result spasm in small arteries associated with migraine attacks. Theresignificant controversy concerning the frequency of this phenoenon. Migraine is often invoked as a cause of white matter lesiowhen these are encountered in healthy young individuals undegoing MR scans for a variety of clinical findings. Other cauof a few “incidental” white matter lesions in this populatioinclude prior minor head trauma and prior infection (e.g., Lymdisease meningitis in childhood). Rarely, patients with migraiwill present with evidence of infarction (hemiplegic migrainusually in the ACA or MCA distribution. Migraines occur wgreater frequency in patients with CADASIL (see below), an
BA
F IGURE 4-38. Radiation change.
A, Magnetic resonance scan beforewhole brain radiation for brain metas-tases. Mild age-related periventricularwhite matter T2 hyperintensity.B, Follow-up examination at 8 monthsafter whole brain radiation reveals dif-fuse periventricular T2 hyperintensityindicative of radiation change.
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 38/66
V ASCULAR D ISEASES OF THE B RAIN 141
women with migrainous auras are at highest risk for subsequentdevelopment of migraine-associated strokes.
Cerebral Autosomal Dominant Arteriopathywith Subcortical Infarcts and
LeukoencephalopathyCerebral autosomal dominant arteriopathy with subcorticalinfarcts and leukoencephalopathy (CADASIL) is a rare diseasethat has received much attention because of its direct geneticcausation. The disease presents between age 30 and 50 yearswith variable findings, including multiple infarcts, migraineheadaches with aura, depression, and dementia. Imaging featuresat least early in the disease are rather characteristic. Focal or con-fluent subcortial white matter involvement in the superior fron-tal lobes, external capsule, and anterior temporal lobes is presentin more than 75% of cases. Lacunar infarcts in these regions arecommon (80% of cases) and microbleeds are present in the major-ity of patients on gradient-echo and SWI MR sequences. As thedisease progresses involvement becomes more widespread andlesions become confluent.
INTRACRANIAL HEMORRHAGEIntracranial hemorrhage is the primary event in 15% to 20% of strokes.We now consider CT and MR characteristics of hemorrhage andattempt to explain why we see what we do with these modalities.
Computed Tomography The x-ray attenuation values of a substance or a structure deter-mine its visibility on CT. With hemorrhage, there is a linear rela-tionship between CT attenuation (density) and hematocrit. Theattenuation of whole blood with a hematocrit of 45% is approx-imately 56 Hounsfield units (HU). Normal gray matter rangesfrom 37 to 41 HU, and normal white matter from 30 to 34 HU.Thus, freshly extravasated blood in a patient with a normal he-maocrit can immediately be demonstrated on CT. The increasedattenuation of whole blood is based primarily on its protein con-
centration (mostly hemoglobin) rather than iron. In seanemic patients, there is a small possibility that the acute hrhage will be isodense to brain because of low hematocrit (Conversely, in infants with high hematocrit or patients witcythemia the dural sinuses, large veins, and proximal arteriappear extremely dense (mimicking thrombosis).
After the extravasation, density progressively increases proximately 72 hours (Figs. 4-39 and 4-40). This is caused increasing hemoglobin concentration due to clot formatioretraction. The presence of fluid-fluid levels within a hematomgests active bleeding or absence of coagulation, often due tocation effects of heparin or warfarin. Swirling, whirling appalso are present with actively bleeding hematomas. After thday, the attenuation values of the clot begin to decrease, aning the next 2 weeks, the hemorrhage fades to isodensity (sFig4-40). The clot loses density from the periphery inward, proa “melting ice cube” (seeFig. 4-40C) appearance. Loss of dsity is the result of several factors. The protein structure hemoglobin molecule changes, resulting in decreased capaabsorb x-rays. The RBCs undergo lysis, with dilution, andquent digestion of the blood products by peripheral macropEventually (rarely more than 1 month), no high density can bfrom a single intraparenchymal hemorrhage, but ring enment may be seen on CECT. Factors affecting evolution of d
include (1) size of initial hematoma (the larger the hematolonger it takes to become isodense); (2) recurrent hemorrhagticularly common in subdural hemorrhage); (3) mixture oand fluid (e.g., subdural and subarachnoid hemorrhage); (4hematocrit; (5) location of hemorrhage; (6) cause of hem(tumor, AVM, cavernoma, aneurysm); and (7) rate of resorpremoval of blood (e.g., subarachnoid blood is rapidly removthe CNS due to resorption with spinal fluid by the pacchgranulations). Each of these factors is more or less involvhemorrhage in different intracranial compartments, accoundifferences seen in parenchymal, subarachnoid, subdural, adural hemorrhage.
To best understand these changes, it is helpful to use pchymal hemorrhage as the “index” condition. A thin zone
A B
F IGURE 4-39. Hyperacute intracerebral hemorrhage. A , Hyperacute (3 hours) right lateral ganglionic hypertensive hemorrhage. Note the lacrounding edema and paucity of mass effect.B , CT angiography source image reveals focal enhancement (arrow ) within the anterior portion of the hetoma, indicative of acute extravasation and active hemorrhage.
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 39/66
142 Neuroradiology: The Requisites
attenuation surrounding the high-density hyperacute intraparen-chymal hemorrhage develops within the first 6 hours due to serumthat is “extruded” from the retracted clot. Extensive edema aroundan acute clot (<12 hours) should raise suspicion for an underlyingpreexistent process (tumor, infection, or prior hemorrhage). Thecircumferential hypodensity increases and reaches a maximum atapproximately 5 days because of vasogenic edema (blood productsand the inflammatory reaction they incite are cytotoxic). Focal paren-chymal hematomas result in less atrophy than hemorrhagic infarctsor contusions because the hematoma tends to displace rather thandestroy brain tissue. After approximately 2 months, a small hema-toma may be completely invisible or there may be a hypodense cleftrepresenting the residua of the hemorrhagic event. Subtle marginalhyperdensity is occasionally seen, likely due to hemosiderin deposi-tion or minimal dystrophic calcification. Large chronic hematomasproduce nonspecific regions of hypodensity with focal volume loss.
Hyperacute, acute, and subacute hemorrhage is reliablydetected on CT (seeFigs. 4-39 and 4-40). CT is fast, avail-able, easily performed, and accurate. Interpretation is relativelyuncomplicated. It is therefore an excellent tool for evaluation ofpatients suspected of having acute hemorrhage. However, there
are limitations to CT. Small hemorrhages in the posterior fosthe anterior inferior frontal and temporal lobes (the most common locations for traumatic contusions), and adjacent to the cvarium are difficult to detect because of artifact from adjacebone or partial volume effects (the hematoma must be twice thwidth of the slice thickness to be unaffected by partial volumaveraging). In cases where hemorrhage is suspected but not cofirmed, coronal and sagittal reformations of the initial data (submillimeter) can help to confirm or exclude hemorrhage problematic locations. Of course, MR can also be performedprovide more definitive information on the presence, extent, ancause of hemorrhage.
The use of intravenous iodinated contrast in patients with hemorrhage is unnecessary in most situations. Identification of undlying mass lesions is best done with enhanced MR (see belofor discussion of enhancement patterns of hemorrhagic masseContrast is routinely utilized in CTA and CT venography (CTVto evaluate for vascular anomalies (aneurysms and AVMs) athrombosis (arterial or venous). In these circumstances evaluatof CTA source images should be performed to assess for undlying masses. Focal extravasation of contrast (the “dot sign
E
A B C
D
F IGURE 4-40. CT of hematoma evolution. A , CT scan 6 hours after onset of symptoms in a patient with chronic hypertension reveals a large lenlar nucleus homogeneous hyperdense hematoma with mild surrounding edema and relatively little mass effect.B , Follow-up exam at 6 days revealsdecreased density at the margin of the hematoma. There is increased mass effect on the right lateral ventricle.C , Examination at 3 weeks revealsdecreased central hyperdensity that fades gradually at the periphery of the hematoma (arrows ), where hematoma is now hypodense.D, A CT scan in adifferent hypertensive patient at 18 hours reveals discrete hyperdense left thalamic hemorrhage with surrounding edema and mass effect on tventricle.E , Follow-up exam at 2 weeks reveals complete resolution of hyperdensity. Hypodense hematoma still has mass effect on the third v
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 40/66
V ASCULAR D ISEASES OF THE B RAIN 143
into a portion of a hematoma on source images is a sign of activehemorrhage and is often associated with continued growth of thehematoma (seeFig. 4-39). If contrast is given, intraparenchymalhemorrhage is often associated with a peripheral rim of enhance-ment from approximately 6 days to 6 weeks after the initial event.This enhancement is the result of breakdown of the blood-brainbarrier at the margin of the hematoma due to toxic/inflammatoryeffects of blood products. The rim is relatively smooth and fol-lows the contour of the original hematoma. Rim enhancementcan give rise to diagnostic dilemmas. In patients scanned acutely,rim enhancement suggestive of a preexisting mass may occur ifthere has been prior subclinical hemorrhage (e.g., cerebral amy-loid angiopathy). In patients initially scanned weeks after hem-orrhage the absence of central hematoma hyperdensity may leadto the erroneous diagnosis of tumor or infection. Similar diagnos-tic dilemmas may occur with enhanced MR but are more easilysorted out.
Magnetic Resonance ImagingMRI has dramatically improved our diagnostic prowess in the assess-ment of hemorrhagic conditions. MRI is more sensitive than CT inthe detection of hemorrhage at all stages of parenchymal hematomaevolution. Detection of associated and underlying lesions is facili-
tated, and the intensity pattern on multiple sequences allows foraccurate “aging” of the hematoma. These gifts do not come withouta cost (there is no free lunch). The MRI features and their underly-ing causes are complex when compared to CT. Understanding thesecomplex MR characteristics is, however, essential to our ability totake advantage of MRI in the evaluation of hemorrhagic lesions.The progression of imaging hallmarks is well understood, althoughthe specific time intervals for these changes are variable. Temporalvariation is the result of the same factors described above for CT.MRI of hemorrhage is more than “dark, bright; bright, dark.” Let usnow briefly consider some of the biophysical mechanisms necessaryto understand the MR appearance of blood.
Structure of HemoglobinHemoglobin, the primary oxygen carrier in the bloodstream, is com-
posed of four protein subunits. Each subunit contains one hememolecule, consisting of a porphyrin ring and an iron atom, whichprovides the binding site for oxygen. Binding of oxygen to the hememolecule of an individual subunit produces a conformational changein that and adjacent subunits. The iron atom (Fe2+ ) sits near the cen-ter of the porphyrin ring and binds to oxygen (O2). Oxyhemoglobinfunctionally has no unpaired electrons and is diamagnetic.
When a hemoglobin subunit loses its O2 to form deoxyhemo-globin, the protein undergoes a small but significant change inits tertiary structure. The Fe2+ is pulled out of the plane of theporphyrin ring, causing the porphyrin to dome. Because of thedoming, water molecules are effectively prevented from approach-ing close enough (3 Å) to the paramagnetic iron to undergo pro-ton-electron dipole-dipole interactions (PEDDI). The watermolecules around deoxyhemoglobin are unable to bind to theheme iron as they do in methemoglobin (see next section).
Deoxyhemoglobin (which has four unpaired electrons) can beoxidized to methemoglobin via several different mechanisms.Normally an enzyme system within the red blood cell rapidlyreduces methemoglobin back to deoxyhemoglobin, but in hem-orrhage, this mechanism deteriorates and irreversible oxidationto methemoglobin takes place. The iron atom (in methemoglo-bin) is closer to the plane of the porphyrin ring than the iron atomof deoxyhemoglobin, allowing a water molecule to bind to theheme iron. The iron atom of methemoglobin has five unpairedelectrons.
Susceptibility EffectsWhen placed in a magnetic field, certain substances generate anadditional smaller magnetic field, which either adds to or subtracts
from the externally applied field. The proportionality cobetween the strength of the external field and the indfield is a measure of the “susceptibility” of the subsDiamagnetic substances have no unpaired electrons and gevery weak fields that subtract from the externally applied Paramagnetic materials such as deoxyhemoglobin and meglobin have unpaired electrons that generate much largefields surrounding the paramagnetic molecule that add externally applied field.
When deoxyhemoglobin or methemoglobin is encapswithin RBCs, the effective local field is greater within ththan outside the cell because of the greater susceptibility intracellular paramagnetic hemoglobin solution compareextracellular plasma. Protons precess at a rate proportithe strength of the local magnetic field. Therefore, the pwithin the RBC precess faster than those outside because increased effective field. Thus, after a 90-degree pulse theof the transverse magnetization accumulates faster for spinthe RBC than outside. In addition water protons move (dthrough these locally varying gradients during the time t(TE). Each proton charts a unique course through the tissutherefore “experiences” a magnetic field of unique streEach accumulates a different amount of phase change, deing on the time spent at different effective field strengths. T
phase dispersions produce signal loss on T2WI (proton relenhancement). Imagine placing microscopic iron filingthe sample. The “artifact” generated by the iron would dphase coherence between precessing protons even if theythe same T2. This phase dispersion leads to loss of signaeffect hypointensity). Extrinsic factors determine the extwhich T2* effects are visible on an image. Susceptibility for imaging magnets are roughly proportional to the squarmain magnetic field. The longer the TE the longer the timdiffusion of water protons, leading to greater phase incohand hence the greater the signal loss. It should be noted thatnificant signal loss results from a very large susceptibilityhypointensity will occur at short TEs (PDWI and T1WI) ather incremental signal loss may not be detectable on incrTE. Gradient-refocused echo images (check Chapter 1 tothat there is no 180-degree refocusing pulse) are more seto susceptibility changes, because the resultant local fieldients are superimposed on the applied phasing and rephgradients. Echo planar sequences (such as used in DWI) ala refocusing echo and therefore also demonstrate suscepeffects. (These techniques may therefore be termed generasT2* or susceptibility weighted ). Hence, signal loss on T2WI fdeoxyhemoglobin, intracellular methemoglobin, and hemoserin can be attributed to susceptibility effects and proton ation enhancement.
Proton-electron Dipole-dipole InteractionThe paramagnetic iron atom in methemoglobin generates field approximately 1,000 times greater than the local fieerated by the proton nucleus. If a proton moves close enothis field (within 3 Å), a spin transition can be induced. binding to the heme is required to have a significant PEBoth T1 and T2 are shortened by PEDDI. However, wadded to the smaller relaxation rate (1/T1), the PEDDI econtributes proportionally more to the observed relaxatiothan it would if added to the larger (1/T2). Therefore, PEare best observed on T1WI, where T1-shortening producesignal intensity. Although the iron atom of deoxyhemoglogenerates a local magnetic field, no significant PEDDI efobserved because the heme iron moves out of the plane porphyrin ring, limiting binding of the water molecules.
In summary, two key effects are created by the hemoglobiecule: (1) the paramagnetic effect, secondary to the iron witheme molecule, which can produce susceptibility effects/protorelaxation enhancement in the case of intracellular deoxyhem
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 41/66
144 Neuroradiology: The Requisites
and methemoglobin and hemosiderin, leading to T2-shortening,and (2) PEDDIs with methemoglobin (both intracellular andextracellular), leading to T1 shortening. Susceptibility effects arefield strength-dependent but PEDDI is not.
Caveat: Care must be exercised in interpreting hematomas onDWI. Both restricted and increased diffusion occurs within andadjacent to hematomas of various etiologies at different stages ofevolution. Susceptibility effects are present and can obscure orchange the intensity on these sequences. Rely more heavily onT1WI, T2WI, and gradient echo scans.
Temporal Changes in Intensity ( Table 4-3 )Hyperacute Hemorrhage (0–6 Hours) ( Figs. 4-41
and 4-42 ): T1 Mildly Hyperintense, T2 Hyperintense,T2* Peripherally HypointenseIn the first 3 to 6 hours after extravasation the intact red cellscontain mostly diamagnetic oxyhemoglobin. There is early clotformation without clot retraction. Hyperacute hemorrhage is,in essence, a highly proteinaceous cellular fluid and like othersuch fluids (e.g., the contents of a craniopharyngioma) it is mildlyT1 hyperintense (because protein decreases T1 but edema/water increases T1) and T2 hyperintense (T2WI and FLAIR).The periphery of the hematoma contains RBCs containing hemo-globin that has started to desaturate (deoxyhemoglobin). Thisproduces hypointensity, in particular on susceptibility-weightedsequences (gradient-echo and echo planar sequences) and athigher field strength. The presence of marginal hypointensity on
gradient-echo scans is key to differentiating hyperacute hemorhage from other mass lesions; therefore, gradient echo or newSWI sequences should be included in any protocol used to deteor exclude acute hemorrhage. If no gradient-echo sequence performed, it is helpful to evaluate the b0 image from a DWIsequence for evidence of peripheral hypointensity. Although nas sensitive as gradient echo images, the b0 image does allow forconfirmation of hemorrhage in the majority of cases. At this stT2 hyperintense peripheral vasogenic edema is mild.
Acute Hemorrhage (6–72 Hours) ( Fig. 4-43 ; seealso Fig. 4-42 ): T1 Hypointense, T2 Hypointense,T2* HypointenseDuring this period there is progressive conversion of oxyhmoglobin to deoxyhemoglobin due to local hypoxia and adosis. Clot formation and retraction leads to decreased wacontent. T2 shortening due to proton relaxation enhancemenof intracellular deoxyhemoglobin abounds. These effects prduce profound T2 (or more accurately T2*) hypointensity thbegins at the periphery and extends to the center of the hematoma. Hypointensity is more marked and appears earlier on T2(susceptibility-weighted) sequences and on high–field-strengmagnets. At this stage hematomas are mildly hypointenson T1 images due to the susceptibility effects and increasewater content of edema. Because water molecules are unable approach close enough to the iron atom of deoxyhemoglobin, T1-shortening is caused by PEDDI. There is an increase in T
T ABLE 4-3. Stages of Hemorrhage
Stage CT T1WI T2WI Mass Effect Time Course Explanation
Hyperacute High density Mildhyperintensity
High intensitywithperipherallow intensity
+++ <6 hours CT: High proteinT1WI, T2WI: Central oxyhemoglobinin with peripheral deoxyhemoglobin(deoxy-Hb)
Acute High density Isointense to lowintensity
Low intensity +++ <6 to 72 hours T1WI: High protein,susceptibility(deoxy-Hb)
T2WI: Susceptibility (deoxy-Hb)CT: High protein
Early subacute High density High intensity Low intensity +++/++ <3 days to 1week
T1WI: PEDDI (intracellularmethemoglobin [met-Hb]), highprotein
T2WI: Susceptibility (intracellularmet-Hb), high protein
CT: High proteinLate subacute Isodense High intensity High intensity
with rim oflow intensity
± 1 to 2 weeks tomonths
T1WI: PEDDI (free met-Hb),absence of susceptibility effects(from intracellular met-Hb), dilutionof high protein
T2WI: PEDDI (free met-Hb),absence of susceptibilityeffects, dilution of high protein,susceptibility effects fromhemosiderin and ferritin inperipheral rim
CT: Absorption of high proteinChronic Low density Low intensity Low intensity − 2 weeks to years T1WI: Susceptibility effects from
hemosiderin and ferritin (T2 effecton T1WI)
T2WI: Susceptibility effects fromhemosiderin and ferritin
CT: Atrophy
*This appearance is classic at 1.5T; however, with decreasing field strength the susceptibility effects are diminished.CT, computed tomography; Hb, Hemoglobin; PEDDI, proton-electron dipole-dipole interaction; T1WI, T2WI, T1-, T2-weighted imageNote that time course is variable, but progression usually follows the stages.Range of mass effect: − (mass effect absent) to +++ (greatest amount of mass effect).
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 42/66
V ASCULAR D ISEASES OF THE B RAIN 145
hyperintense peripheral vasogenic edema, with a concomitantincrease in mass effect.
Early Subacute Hemorrhage (3–7 days)(Fig. 4-44 ): T1 Hyperintense, T2 ModeratelyHypointense, T2* Markedly HypointenseDuring this period, there is oxidation of the deoxyhemoglo-bin to methemoglobin inside the RBC. Unlike deoxyhemoglo-bin, water molecules are able to approach within 3 Å of theparamagnetic heme of methemoglobin, permitting PEDDIsthat shorten T1. This effect gives subacute hematomas theircharacteristic hyperintensity on T1WI. Oxidation of deoxy-hemoglobin to methemoglobin proceeds from the peripheryto the center of the clot during the first week after the ictus;therefore T1 hyperintensity is initially seen at the edge of thehematoma (2 to 3 days) with progressive “filling in” of the cen-ter of the hematoma (7 to 10 days). Because the paramagneticmethemoglobin remains encapsulated within the RBC, markedhypointensity is present on the T2WI and in particular gradient-echo images due to the susceptibility mechanism describedfor deoxyhemoglobin from iron-producing proton relaxation
enhancement. Toward the end of the early subacute phashypointensity decreases due to cell lysis. Once paramamethemoglobin is no longer sequestered within the redlocal field inhomogeneity begins to decrease and susceity-induced T2* hypointensity begins to resolve. In effe“true” prolonged T2 of the hematoma and edema reaitself in the late subacute phase. Peripheral edema and
effect continue to increase during this period.Late Subacute Hemorrhage (7–14 Days)(Fig. 4-45 ): T1 Hyperintense, T2 Isointenseto Hyperintense with Hypointense Rim, T2*Moderately Hypointense with Hypointense RimDuring this period RBC and clot lysis occur. Methemoglless stable than deoxyhemoglobin, and the heme group cantaneously be lost from the protein molecule. This free heother exogenous compounds promote RBC lysis. Concomthere is protein breakdown and dilution of the remainingcellular methemoglobin. Hyperintensity persists on because of the T1-shortening effects of intracellular and exlular methemoglobin even at relatively low concentration
B C
E
A
D
F IGURE 4-41. Magnetic resonance study of hyperacute hemorrhage. A, Computed tomography (CT) scan at the level of the foramen of Monro 2 ho
ictus reveals a large right parasylvian hematoma.B, T1-weighted image 1 hour 30 minutes after CT reveals mildly hyperintense mass in the right pregion. Small subdural hematoma is also hyperintense (arrow ).C, T2WI reveals hematoma is mildly hyperintense to normal cortex. Note fluid level inportion of the hematoma. Subdural hematoma is hyperintense (arrow ).D, Gradient-echo scan reveals marked peripheral hypointensity and mild centratensity pathognomic of hyperacute intracranial hemorrhage. Subdural hematoma is hyperintense with a hypointense rim (arrow ).E, FLAIR reveals hematoto be minimally hyperintense to gray matter. Note extensive sulcal hyperintensity (arrows ) indicative of subarachnoid hemorrhage not apparent on CT.
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 43/66

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 44/66
V ASCULAR D ISEASES OF THE B RAIN 147
B
D
A
C
F IGURE 4-43. Magnetic resonance study of acute intracranial hemorrhage. A, Computed tomography scan 4 hours after onset of symptoms in hypertensive patient reveals right pontine hematoma. T1-weighted image (T1WI) (B ) and T2WI (C ) at 36 hours reveals large focus of hypointeD, On gradient-echo scan hypointensity is increased.
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 45/66
148 Neuroradiology: The Requisites
hematoma intensity progressively increases on T2WI, approach-ing that of CSF, because of a loss of local field inhomogeneityand reduction in proton relaxation enhancement that results fromRBC lysis and a decrease in the protein concentration. Parallelingthe breakdown of the methemoglobin is an accumulation of theiron molecules hemosiderin and ferritin within macrophages atthe periphery of the lesion. The iron cores of hemosiderin andferritin contain approximately 2000 iron molecules ferromagneti-cally coupled to produce a “superparamagnetic” substance thatexhibits a very large T2-shortening susceptibility effect. Theresult is a hypointense rim at the margin of the lesion, variablyvisible on T1WI but increasingly prominent on T2WI, GrE, andSWI. In addition peripheral edema and mass effect decrease.
Chronic Hemorrhage (>2 Weeks) ( Figs. 4-46 and 4-47 ): T1 and T2 Hyperintense with MildlyHypointense Rim, T2* Markedly Hypointense RimThe hematoma becomes progressively smaller. The centralT1 and T2 hyperintensity and peripheral T2/T2* hypointensity
persist, but peripheral edema and mass effect completely resolvAfter months there is nearly complete breakdown and resortion of the fluid and protein within the clot such that the brighsignal on T1WI and T2WI resolves. The iron atoms from thmetabolized hemoglobin molecules are deposited in hemosierin and ferritin molecules that are trapped permanently withthe brain parenchyma because of restoration of the blood-brabarrier. The susceptibility effects of the superparamagnetiiron cores of hemosiderin produce permanent hypointension all sequences, but are most prominent on the gradient-echand SWI sequences where “blooming” of the hypointensity observed. Therefore, chronic hemorrhage is directly visible MR as opposed to CT, where only the sequelae of the hemorrhage (lacunes, hypodensity, volume loss) are apparent (sFig. 4-47). The pattern of hemosiderin “scarring” dependson the size, location, and etiology of the original hemorrhaSmall hematomas and deep gray matter bleeds produce peripheral hypointense cleft (hemosiderin slit), whereas larghematomas, hemorrhagic infarcts, and contusions produ
B
D
A
C
F IGURE 4-44. Subacute hematoma in a 76-year-old man. A, Computed tomography scan at 1 day reveals a large irregular hyperdense left parieto-occipitalhematoma with intraventricular hemorrhage. Magnetic resonance imaging performed at 3 days.B, T1-weighted image (T1WI) reveals hyperintensityat the margin of the lesion and within the anterior and posterior portions of the hematoma.C, T2WI reveals homogeneous marked central hypointen-sity with mild surrounding T2 hyperintense edema.D, Gradient-echo scan reveals diffuse hypointensity with a more hypointense rim. Findings mcompatible with cerebral amyloid angiopathy.
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 46/66
V ASCULAR D ISEASES OF THE B RAIN 149
areas of encephalomalacia with marginal or gyral hypointensity.Small petechial hemorrhages (microbleeds) produce foci of T2*hypointensity that cannot be detected on CT or other MR fast–spin echo sequences. Microbleeds typically occur in hyperten-sive cerebrovascular disease, amyloid angiopathy, and as resultof head trauma with axonal injury (Fig. 4-48). They may alsobe seen with multiple cavernous malformations and capillarytelangiectasias, and after radiation therapy. When there is recur-rent hemorrhage that leaks into the subarachnoid spaces, hemo-siderin staining of the leptomeninges may occur, producingsuperficial siderosis. This may be seen in recurrent hemorrhagefrom brain tumors, trauma, weepy granulation tissue, or amyloidangiopathy (see Fig. 4-48). It is rare after a single event of aneu-rysmal SAH, presumably because the blood is adequately andrapidly cleared from the spinal fluid.
ETIOLOGIES OF INTRACRANIALHEMORRHAGEIntraparenchymal Hemorrhage (Box 4-4)Spontaneous (nontraumatic, nonischemic) parenchymal hemor-rhage accounts for approximately 10% of “strokes.” The mostcommon causes of spontaneous (nontraumatic) parenchymal hem-
orrhage in patients older than 60 years are hypertension, hrhagic infarction, and cerebral amyloid angiopathy. In ypatients, parenchymal hemorrhages are more commonly than underlying vascular anomaly (AVM or cavernous anvenous thrombosis, or vasculopathy. Parenchymal hemocan occur in association with intracranial neoplasms at any may be the presenting finding for a previously undiagnosedAcute hematomas are most often diagnosed with CT in thegency department or unenhanced MR in short-term folloThe subsequent workup is dependent on clinical factors (page, presence of underlying diseases such as hypertension,ated imaging findings on initial examination). For instanceelderly hypertensive patient the presence of a ganglionic toma does not require further workup, in particular if theother CT or MR findings indicative of hypertensive cevascular disease (ischemic white matter change, chronic infarcts, chronic hemorrhage). The same ganglionic hemoin a young patient without hypertension will require furtheing, including contrast-enhanced MR scans, and, if an undvascular lesion is suspected, angiographic studies (MRA, Ccatheter angiography). Bleeding diatheses (spontaneous orelated) increase both the risk and severity of parenchymal rhage with or without an underlying cause.
A B C
D E
F IGURE 4-45. Late subacute hematomComputed tomography scans at 24 h( A ) and 14 days (B ) reveal evolution right ganglionic hematoma. Magnresonance scan also performed at 14 reveals peripheral hyperintensity and tral isointensity on T1-weighted im(T1WI) (C ); marked peripheral hypertensity, central mild hyperintensity, ansubtle hypointense margin on T2WI (D )and central hyperintensity with a pereral hypointense margin on gradient-eimage (E ). Note that size of hematommore easily appreciated on MR thanat this stage. Hematoma is approximathe same size on MR as it was at timinitial CT.
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 47/66
150 Neuroradiology: The Requisites
HypertensionIn hypertensive cerebrovascular disease, damage to small perfo-rating arteries arising from proximal vessels (e.g., MCA and basilararteries) leads to fibrinoid necrosis. In the past it was thoughtthat hypertensive hemorrhages arose from microscopic (Charcot-Bouchard) aneurysms on small arteries (100 to 300mm in diam-eter). However, modern histologic techniques have revealedthat most of these “aneurysms” were due to fixation artifacts.Hemorrhages occur most frequently in the basal ganglia followedby the thalamus, brain stem, and cerebellum (seeFigs. 4-39, 4-40,4-43, 4-45, and4-47). Approximately 10% of hypertensive hem-orrhages may be lobar, but the incidence of lobar hemorrhage iscontroversial because older hypertensive patients may also havecerebral amyloid angiopathy (see below). Initially hypertensivehemorrhages may have very little mass effect (seeFigs. 4-39 and4-40). Over the first 24 to 36 hours the hemorrhages often enlargeand always develop vasogenic edema and increasing mass effect.
These changes account for the clinical observation that patienwith hypertensive hemorrhage typically deteriorate over thfirst few days. Imaging studies typically reveal other eviden
of hypertensive cerebrovascular disease. Chronic lacunar infar(seeFig. 4-47) or hemorrhages and extensive microvascular whimatter disease are typically present. On gradient-echo and SWMR sequences, microbleeds (punctate foci of T2* hypointensitare encountered in the deep gray matter, posterior fossa, and sucortical regions (seeFig. 4-48A–D). Although chronic hyperten-sion alone can lead to parenchymal hemorrhage, rapid episodincrease in blood pressure, such as may occur with cocaine udialysis, or fluid overload, can also lead to parenchymal hemrhage and brain damage.
Cerebral Amyloid Angiopathy CAA results from deposition of amyloid (an eosinophilic, insuble extracellular protein) in the media and adventitia of sma
A B C
D E F
F IGURE 4-46. Magnetic resonance study of chronic hematoma. Right temporal hematoma examined 4 days after ictus reveals typical featuressubacute hematoma with peripheral hyperintensity on T1-weighted image (T1WI) ( A ), diffuse hypointensity on T2WI with surrounding edema anmass effect (B ), and marked hypointensity on gradient echo (C ). D–F, Repeat examination at 2 months reveals marked contraction of clot with fovolume loss and no edema. Residual central T1 (D ) and T2 (E ) hyperintensity is present. There is extensive T2 and susceptibility hypointensity in tadjacent tissue, and there is mild sulcal hemosiderin deposition in the leptomeninges (siderosis) adjacent on the gradient-echo scan (F ).
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 48/66
V ASCULAR D ISEASES OF THE B RAIN 151
B
D
A
C
F IGURE 4-47. Chronic hypertensive hemorrhage. A, Computed tomography scan reveals a focus of hypodensity in the left lateral posterior nucleus. Findings consistent with chronic lacunar infarct hemorrhage or dilated Virchow-Robin space.B, T1-weighted image (T1WI) reveals the leto be isointense to spinal fluid.C, T2WI reveals that the center of the lesion is hyperintense but that the rim is hypointense.D, Gradient-echo screveals more conspicuous hypointense rim. Findings on T2WI and gradient-echo scans are specific for chronic hemorrhage.
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 49/66
152 Neuroradiology: The Requisites
A B C
D E
G H
F
F IGURE 4-48. Microbleeds and superficial siderosis.Case 1: Patient with chronic hypertension. T2-weighted images (T2WI) at the level of the brstem ( A ) and basal ganglia (B ) reveal a few subtle foci of hypointensity. Ganglionic hyperintensities are dilated perivascular spaces.C andD, Gradient-echo scans at the same levels reveal numerous foci of T2* hypointensity in the brain stem, cerebellum, basal ganglia, and subcortical whiindicative of microbleeds.Case 2: Patient with history of subacute parenchymal hemorrhage and presumed diagnosis of cerebral amyloid angiE, FLAIR reveals a chronic left occipital hematoma (central hyperintensity with peripheral hypointensity and no edema).F, Gradient-echo scan revealschronic hematoma with hypointense rim and numerous additional foci of T2* hypointensity indicative of chronic microbleeds.G, T2WI near vertexdoes not demonstrate hemorrhage.H, T2* hypointensity is present within the sulci near the vertex, indicative of superficial siderosis.
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 50/66
V ASCULAR D ISEASES OF THE B RAIN 153
and medium-sized vessels of the superficial layers of the cere-bral cortex and leptomeninges, with sparing of the deep graynuclei. Amyloid deposition increases with age but does notcorrelate with hypertension or the presence or absence of sys-temic amyloidosis. (It does correlate with brain parenchy-mal amyloid deposition, so is more common in patients withAlzheimer disease.) Amyloid accumulates Congo red dye andexhibits yellow-green birefringence when examined with polar-izing light. Amyloid protein replaces the normal constituentsof the vessel wall, in particular the elastic lamina, leading tomicroaneurysm formation and fibrinoid degeneration. Thesechanges produce marked vascular fragility. Hemorrhages areusually lobar, involving the frontal and parietal lobes, includingthe subjacent white matter. CAA is rarely found in the cerebel-lum, white matter, basal ganglia, or brain stem. Subarachnoidand subdural hemorrhages have also been reported as a resultof the superficial vessels involved in CAA. There is a propen-sity for recurrent hemorrhage in the same location or multiplesimultaneous hemorrhages. The presence of multiple simul-taneous lobar hemorrhages in an elderly patient is highly sus-picious for CAA, although multiple hemorrhagic metastasesmust always be considered. Because CAA may produce recur-rent hemorrhage in a single location, hematomas are often com-plex in appearance on both CT and MR. Variable CT densityand MR intensity within the same lesion reflect hemorrhage
of different ages. Extensive edema and enhancement aro“hyperacute” hematoma (the result of an earlier clinicallybleed) and lesion growth may be suggestive of underlyinplasm. In some instances the only way to differentiate beCAA and neoplasm is the performance of serial examiover a several-week period or observing enhancing nodmetastases. One finding that can help to establish the disis of CAA is presence of cortical or subcortical microblT2*-weighted imaging. In virtually all cases, CAA is acnied by extensive microvascular white matter ischemic cwith sparing of subcorticalU fibers. It may be responsibleup to 10% of nontraumatic intraparenchymal hemorrhagFig. 4-40). It is important to note that in the past CAA herhages were rarely encountered in patients under age 70Using newer susceptibility-weighted scan techniques, homay push this age differential earlier. Another pattern nowcommonly seen with SWI is multiple superficial corticachial hemorrhages. In addition to Alzheimer disease, amdeposition has been seen in association with Down syndchronic traumatic encephalopathy (dementia pugilisticapostirradiation necrosis, and Creutzfeldt-Jakob disease.
Venous Thrombosis (Box 4-5)
Venous thrombosis is an often challenging diagnosis (Fig. 4-49)Symptoms and signs are nonspecific, variable, and protean, ding on the location of the clot and the acuity of the process. occur secondary to a large number of conditions. Imaging finroutine CT may be subtle and overlooked if clinical suspicionFortunately, the advent of MR and the development of CTAniques have dramatically improved our ability to make this dia
Venous thrombosis is the great mimicker of other diseaoccurs in the setting of dehydration (e.g., infants with syinfection, severe nausea and vomiting), hypercoagulationimmune diseases, collagen vascular disease, inflammatorydisease, pregnancy, puerperium, and use of birth controlacute bacterial infection, and hereditary conditions. Calvdural tumors (e.g., meningiomas) may cause venous thromand it may be seen in association with skull fractures that tdural sinuses. In a significant number of cases an etiologydiscovered. Venous thrombosis and/or stenoses have alsimplicated as the cause of dural AV fistulas and of pseudocerebri (benign idiopathic intracranial hypertension).
The disease is most commonly encountered in young wand children because they are more likely to have the condthat predispose to venous thrombosis. Clinical findings arnonspecific and include headache and seizures. Signs on nation may be nonspecific or may indicate increased intrapressure with papilledema. Localizing neurologic finding
B OX 4-4. Hemorrhagic Causes of Stroke
PRIMARY INTRACEREBRAL HEMORRHAGEAneurysm (mycotic, congenital)Hemorrhagic infarction (arterial, venous)Hypertensive, arteriosclerotic hemorrhageNeoplasms (primary or metastases)Trauma
VasculitisVascular malformationsAmyloid angiopathyDrugs
CocaineAmphetaminePhenylpropranolaminel-asparaginase
Hematologic causesAntithrombin III deficiencyProtein C+ S deficiencyAntiphospholipid antibodiesFactor VII deficiencyFactor IX deficiencyFactor VIII deficiency
von Willebrand factor deficiencyAcquired coagulopathiesThrombocytopenia and platelet dysfunctionDisseminated intravascular coagulopathyUremiaMultiple myelomaMyeloproliferative disordersLymphoproliferative disordersLeukemia
SUBARACHNOID HEMORRHAGEAneurysmAVM, nonaneurysmal perimesencephalic hemorrhageDural malformationHemorrhagic tumorTrauma
Vascular dissection
B OX 4-5. Causes of Venous Thrombosis
Acute dehydration (diarrhea)Chemotherapeutic agents (l-asparaginase)Cyanotic congenital heart diseaseHypercoagulable states and coagulopathies: sickle cell
ease, hemolytic anemia, polycythemia, use of oral contratives, inflammatory bowel disease, nephritic syndrometein S and protein C deficiencies, antithrombin III deciency
Iatrogenic (indwelling venous catheters)Infection involving sinuses, mastoids, and leptomeningeMalignancy, including leukemia (also associated with cg-
ulopathies)MalnutritionPregnancyTrauma
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 51/66
154 Neuroradiology: The Requisites
B C
E F
G H
A
D
F IGURE 4-49. Venous thrombosis. Computed tomography (CT) and magnetic resonance (MR) imaging 1 day postpartum with seizure. CT scalevel of the transverse sinus ( A ) and superior sagittal sinus near the vertex (B ) reveal mild hyperdensity within the transverse and superior sagittal asuperficial cortical veins (arrow in B ). C, T2-weighted image (T2WI) reveals hypointensity within the transverse sinus. Findings may representmal flow or acute thrombus. Gradient-echo scans reveal marked hypointensity and “bloom” artifact in the transverse sinus (D ), superior sagittal sinus(E ), and superficial cortical veins (arrows ).F, Contrast-enhanced T1WI at the vertex (same level asE ) reveals filling defect in the superior sagittal sinuand adjacent cortical veins (arrows ). Frontal (G ) and lateral (H ) time-of-flight MR venograms reveal absence of flow in the superior sagittal sinusright transverse sinus.
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 52/66
V ASCULAR D ISEASES OF THE B RAIN 155
from regional venous infarcts and parenchymal hemorrhage. Insevere cases, venous thrombosis can lead to intracranial hyper-tension, coma, and death. The temporal pattern of the disease isalso variable and depends on the cause of the thrombosis, loca-tion and extent of initial thrombosis, rate of progression or spon-taneous regression, and the pattern of collateral venous drainage.Some patients present with an acute ictus and rapid deteriora-tion suggestive of infarction. In most cases, clinical onset is lessabrupt and progression occurs over days, mimicking the timecourse of intracranial infection. In rare cases the onset is insidi-ous with patients presenting with slowly progressive symptoms(months to years), including dementia mimicking neurodegen-erative processes.
Venous thrombosis typically begins in a dural venous sinus(superior sagittal sinus or transverse sinus). The thrombosis mayprogress to involve other portions of the dural venous system orextend into adjacent cortical veins. Isolated cortical vein throm-bosis is rare, but thrombosis of the deep venous system (e.g.,internal cerebral veins and vein of Galen) can occur in children.
Spontaneous resolution of venous thrombosis can lead torapid resolution of symptoms. Use of intravenous or intra-arterialmedications to dissolve venous clots or endovascular treatmentto remove clot often results in dramatic improvement in clini-cal outcome even in the presence of parenchymal hemorrhage or
long-standing symptoms.Because treatment can dramatically improve outcome anunderstanding of the imaging diagnosis of venous thrombosisis extremely important. Imaging findings can be divided intothree categories: (1) direct identification of clot in a dural sinusor vein, (2) identification of collateral venous channels, and (3)identification of the complications of venous thrombosis. Clotidentification is complicated by the fact that, like all hemato-mas, clots within the venous system undergo time-dependentCT and MR intensity changes and therefore look different atdifferent times.
On unenhanced CT acute dural sinus clot appears hyperdenseand the sinus itself is often enlarged (seeFig. 4-49A-B). If theclot is located in a portion of the superior sagittal sinus that is per-pendicular to the axial plane (e.g., posteriorly), the clot may bedetected with relative ease. However, when the superior sagittalsinus is occluded superiorly or there is clot within the transversesinus (both parallel to the axial imaging plane), detection of clotis more difficult. Careful attention must be paid to the densityof the transverse sinuses, and it is important to carefully evalu-ate the most superior slices. The diagnosis of transverse sinusthrombosis is complicated by the fact that the transverse sinusesare often asymmetric. One sinus (more typically the left) may besmall or absent. In patients with asymmetric sinuses, flow in thelarger sinus may appear abnormally dense and be mistaken forthrombosis. It is also important to remember that in newbornswith expected normal polycythemia leading to increased vascu-lar density, the relative hypodensity of the brain, and the fre-quent occurrence of minimal perinatal paratentorial hemorrhagecan mimic the appearance of transverse sinus thrombosis.
Cortical vein thrombosis can produce a dense superficialstructure on CT that extends along the convexity surface ofthe brain in the region of the dural venous sinus (cord sign;see Fig. 4-49B). Dilated superficial veins indicative of collat-eral drainage rather than thrombosis are occasionally visible onunenhanced CT. Within a week, clot in a dural sinus becomesisodense to hypodense and sinus expansion resolves. Therefore,direct identification of sinus thrombosis on unenhanced CTbecomes impossible. CT detection of sinus thrombosis is facil-itated on contrast-enhanced studies. Nonenhancing clot withinthe superior sagittal sinus (empty delta sign) is a well-known signof venous thrombosis. Detection of in plane intrasinus clot onroutine contrast-enhanced CT can be problematic for the samereasons that detection of hyperdense clot is problematic onunenhanced CT. Use of dynamic thin-section CTA protocols
with multiplanar reconstruction has made the diagnovenous thrombosis straightforward. In addition to acidentification of thrombus, the source images allow for tion of ancillary findings, including dilated cortical venolateral vessels and thick enhancement of the tentorium o
Identification of the complications of sinus thromboCT is more problematic. Focal subcortical hemorrhage nethrombosed sinus is easily detected, as is SAH and suhematoma. Focal and diffuse edema (hypodensity) are moficult to detect and characterize with CT. The brain may aswollen or “tight,” but this is difficult to differentiate fromal, particularly in young women. Narrowing or obliterabasal cisterns (e.g., suprasellar, prepontine) helps to distinormal from abnormal studies. It is not possible on CT ferentiate between reversible edema and irreversible vinfarction.
Although the diagnosis of venous thrombosis can be mCT, particularly if the level of clinical suspicion is high ocontrast CT findings prompt performance of a CTV examithe diagnosis is made more readily with MR (seeFig. 4-49C–F)Detection of clot within a dural sinus or vein is dependeunderstanding of two factors: (1) the normal appearancedural venous sinuses on different pulse sequences and (2) kedge that intraluminal clots have some of the same intensi
temporal changes in intensity as parenchymal hematomthings evolve more slowly and hemosiderin is absent.Signal within the dural sinuses is similar to that seen in
arteries. On most images the sinuses will be hypointenboth T1- and T2-weighted sequences. However, since vflow is slower than arterial flow, flow-related hyperintensbe encountered more often, particularly in flow that is npendicular to the plane of section. Therefore, T1 hyperintand less extensive T2 hyperintensity can be seen in portithe patent dural sinuses and within cortical veins, particuthe vessel is obliquely oriented to the section of acquisitiogradient-echo scans flow-related hyperintensity is routinewithin or adjacent to the transverse and superior sagittalThese flow phenomena are inconsistent from image to imafrom plane to plane. Acute sinus clot is T1 isointense to hyperintense and T2 hypointense and thus similar in appeato flowing blood. The key finding at this stage is marked htensity with blooming on gradient-echo scans. A sinus thahypointense and gradient-echo hyperintense cannot be occWith thrombosis, the dural sinuses are typically expandecross-sectional images their lateral walls are convex. Throcortical veins are also markedly hypointense with bloomifact on gradient echo. Detection of isolated cortical vein bosis can be made in most cases. In addition dilated colcortical veins are readily visible on unenhanced T2WItherefore possible to make the diagnosis of venous thrombroutine noncontrast MR scans even in the absence of clinicpicion of the correct diagnosis. Diagnosis on MR is facilitperformance of MRV using phase-contrast or enhanced orhanced time-of-flight (TOF) techniques. As previously sphase-contrast MRA can be made sensitive to slow flow ratherefore can be performed such that only the patent veivisualized. 2D phase-contrast MRV images in the sagittal aonal planes can be obtained in less than 1 minute and allassessment of dural venous sinuses. TOF techniques take lbut provide greater detail about both the dural sinuses ancortical veins. One potential limitation of TOF MRV is thaacute T1 hyperintense intrasinus clot will appear hyperinand mimic flow. It is therefore helpful to perform both contrast and TOF MRV. By adding an enhanced TOF sequone can often sort out the slow flow or turbulent flow aremimic sinus thrombosis or sinus stenosis. Coronal acquto put the sagittal sinus and deep veins in cross-section oittal acquisitions to put those pesky transverse sinuses insection may help to reduce confusion about patency of tur
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 53/66
156 Neuroradiology: The Requisites
or hypoplastic sinuses. Sometimes pacchionian granulations mayappear as filling defects in normal sinuses on enhanced CT andMR scans, but these same filling defects can be due to focalthrombi. Fortunately the arachnoid granulations have CSF signaland are typically very bright on T2WI.
MR is superior to CT in detecting the complications of sinusthrombosis. Detection of hemorrhage is equal to or superior to thatseen with CT. A general rule of thumb is that the parenchymalhematoma clot will look “younger”—more acute—than theintraluminal clot because it develops at some point after thethrombus forms. Detection of focal and diffuse T2 hyperintenseedema is much easier on MR than CT, and use of DWI allowsfor differentiation between irreversible venous infarction (DWIhyperintense with restricted diffusion) and reversible venousedema (DWI isointense with increased diffusion). However, DWIand venous infarction is trickier than arterial stroke. SometimesDWI-positive venous strokes reverse. Potential pitfall here.
After approximately 3 to 5 days, the sinus clot becomes T1hyperintense and after 7 to 10 days T2 hyperintense. Diffusesinus T1 hyperintensity is virtually pathognomonic of subacutesinus thrombosis and renders TOF MRV tricky also because thebright clot simulates flow. Chronic sinus thrombosis is usuallyT1 hypointense and T2 and gradient echo isointense to hyperin-tense. Chronically occluded sinuses are small in caliber. In many
cases there is at least partial recanalization of dural sinuses. Mand CTV studies reveal irregular areas of narrowing or focal ocsion in the chronic phase.
Arterial DissectionDissection occurs when an intimal tear allows blood to enter tarterial wall (Fig. 4-50). The blood divides the layers of the wallproducing stenosis, occlusion, or pseudoaneurysm formatioThe blood can extend within the wall for several centimeteand then re-enter the true lumen. Clot within the dissection cathen be evacuated, leading to the development of a false lumeDissection usually affects the extracranial vessels but can occurintracranial vessels as well. One or more vessels may be involvIt is most often the result of neck injury. The injury is often miand symptoms may take hours to days to develop, so the associatbetween the injury and the dissection may be clinically obscurBlunt and penetrating trauma are obvious causes of dissectiobut in many cases the initial insult is the result of rapid neck turing (e.g., in chiropractic manipulation or motor vehicle accidenor hyperextension. Dissection can occur spontaneously in assciation with hypertension, FMD, and connective tissue diseas(e.g., Ehlers-Danlos syndrome type IV, Marfan syndrome). Othreported circumstances include migraine headache, coughin
B C
E
A
D
F IGURE 4-50. Bilateral carotid artery dissec-tion. On T1-weighted image (T1WI) ( A ), fat-suppressed T1WI (B ), and T2WI (C ), there ishyperintensity within the walls of both internalcarotid arteries, indicative of mural thrombus surrounding the hypointense narrowed lumens. Themural thrombi are seen to advantage on fat-sat-urated images.D, Source image from magneticresonance angiography (MRA) reveals the moderately hyperintense mural hematoma (arrows ) sur-rounding the more hyperintense lumen.E, MRAimage of the right internal carotid artery revealshyperintense narrowed lumen surrounded bymildly hyperintense intramural hematoma.
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 54/66
V ASCULAR D ISEASES OF THE B RAIN 157
violent sneezing, vomiting, intubation/ventilation associatedwith resuscitation or anesthesia, and respiratory tract infection.Dissection of the carotid or vertebral artery should always be con-sidered as a cause of stroke in young otherwise healthy patients.Symptoms result from the primary cervical vascular injury andsecondary ischemia, but pain in the neck may also accompany theevent. Extracranial carotid dissection can present with neck andface pain, headache, ptosis, and myosis (Horner syndrome) due toexpanding intramural hematoma and compression of sympatheticnerves adjacent to the internal carotid artery. Ischemic infarctionis usually the result of distal embolization from the cervical dis-section rather than occlusion. Embolic infarction typically occursseveral hours to days after the onset of the dissection but may bedelayed for several weeks. Intracranial dissections can occur as aresult of skull base or penetrating injuries. Idiopathic intracranialdissection can produce fusiform aneurysms with heterogeneousintramural clot. It should also be considered when there is iso-lated stenosis of a proximal intracranial vessel without other clini-cal or imaging evidence of atherosclerosis. Whiplash injuries mayalso cause intracranial dissections.
Traditionally, dissections are detected by angiographic studies.In the extracranial internal carotid artery four patterns of lumi-nal abnormality can be detected with catheter and noninvasivetechniques: (1) smooth tapering to a pointed occlusion; (2) long
segment asymmetric narrowing (occasionally spiraling around thelumen); (3) double lumen with an intimal flap (the true lumenis typically smaller than the false lumen); and (4) pseudoaneu-rysm formation. In the vertebral arteries luminal patterns are lessspecific. Occlusion or stenosis of the midsection of the vertebralartery within the foramen transversarium (often around C5 whererotation tends to be maximal) or presence of a false lumen inthe distal vertebral artery is most frequently observed. Luminalchanges are well seen with both catheter angiography and CTA.Source images from CTA allow for detection of intimal flaps anddouble lumens and are particularly valuable in assessing the smallvertebral arteries. MR/MRA is excellent for carotid dissection butcan be more problematic with vertebral dissections because ofthe artifact from the vertebral bodies and in-plane flow aroundthe skull base. Intraluminal intensity changes secondary to tur-bulent and in-plane flow artifacts may be difficult to differentiatefrom flaps and false lumens. The mural hematoma is commonlyT1 hyperintense and T2 hypointense to hyperintense (patientswith dissections are most often imaged 3 to 7 days after the ini-tial event). Within the expanded T1 hyperintense artery wall thesmall hypointense residual lumen is often present (target sign).Fat-suppressed T1-weighted sequences may be useful to distin-guish periarterial fat from intramural subacute hemorrhage, par-ticularly in the neck. Because the mural hematoma is typicallyhyperintense, care must be taken in evaluating MRA sequencesto ensure that hyperintense mural clot is not mistaken for hyper-intense normal flow. The mural clot is typically less hyperin-tense than the lumen and it has an amorphous appearance. Muralclot is less often visualized in vertebral artery dissections. MRis also useful for following the dissection to visualize when thehemorrhage is reabsorbed, when the normal lumen dimensionsare reestablished, and if there is progression to pseudoaneurysm.The principal complications of extracranial vascular dissec-tion—infarcts and TIAs—result from luminal compromise and,more commonly, embolic phenomena. Treatment (anticoagula-tion) is directed toward preventing recurrent emboli. Most dissec-tions of the neck heal spontaneously. The treatment for dissectinganeurysms in the cervical region is stenting, whereas intracranialdissecting aneurysms associated with SAH are usually treated byoccluding the vessel to prevent initial or recurrent hemorrhage.
Intratumoral HemorrhageBrain tumors associated with hemorrhage are usually malig-nant primary astrocytoma (WHO grade III [anaplastic astrocy-toma] and grade IV [glioblastoma multiforme]) and metastases.
In the general population, the most common hemorrhagic encountered on imaging include, in order of decreasing freqgrade IV astrocytomas (glioblastoma), lung and breast me(very common lesions that bleed occasionally), melanomatases (rather common lesions that bleed in most cases), renthyroid metastases (uncommon lesions that bleed in many and choriocarcinoma metastases (rare lesions that bleed icases). Other tumors associated with hemorrhage include padenomas, hemangioblastomas, dysembryoblastic neuroeptumors, ependymomas, and craniopharyngiomas.Hemorrhage into neoplasm is often recurrent and takesover days to weeks. Therefore, hemorrhagic tumors typroduce more heterogeneous CT density and MR intethan “simple” parenchymal hematomas, and they do notthe same temporal progression. With tumoral hemorrhagdeoxyhemoglobin state may be prolonged with central htensity existing for more than a week. A complete rim ofsiderin-induced T2 hypointensity is usually absent. Thgenerally more edema and mass effect than are consistena simple hematoma. Edema is present at the time of the ictus and does not resolve over time. Enhancement withadjacent to the hematoma should always raise the suspicunderlying neoplasm, in particular when encountered wifew days of ictus. Hemorrhagic gliomas are typically la
hemorrhage is intratumoral. Therefore, most often theperipheral neoplastic components that can be detected, iticular on enhanced scans where irregular enhancement ioften encountered. As previously stated, hemorrhage assowith CAA may mimic findings in hemorrhagic gliomas (aversa). Hemorrhagic metastases are often smaller and hemocan be extratumoral. In these cases, the tumor is detectedall) as a small enhancing nodule at the margin of a largetoma. Diagnosis of hemorrhagic metastases is usually simby the presence of additional nonhemorrhagic lesions (sfully evaluate the remainder of the examination). In some clarge acute hematoma will completely obscure an underlyinplasm, making correct diagnosis impossible until the true of the lesions becomes apparent after hemorrhage resolve
Siderosis of the CNS (see Fig. 4-48H )Hemosiderin deposition on the surface of the brain (leeningeal and subpial) and cranial nerves can occur as theof chronic recurrent SAH. It is typically not seen withgle aneurysmal SAH (aSAH) no matter how severe becablood is cleared from the spinal fluid before it can be conto hemosiderin. Recurrent bleeding occurs with condsuch as postoperative granulation tissue, chronic lowneoplasms, vascular malformations, CAA, and recurrent and is more common when patients have bleeding dses. Hemosiderin is neurotoxic; therefore, when it invthe cranial nerves patients may develop specific neurosymptoms. Siderosis cannot be diagnosed readily on CMR, hypointensity coating the surface of the brain annial nerves is visible on T2-weighted and more extensivT2*-weighted images. Hemosiderin deposition has alsonoted on the ventricular ependyma after neonatal intraveular hemorrhage.
Subarachnoid HemorrhageImaging CharacteristicsSAH has different CT and MR imaging features than otherof hemorrhage because the blood mixes with CSF. Spinadilutes the blood (hematocrit is typically <5%) and antifibelements in CSF prevent or inhibit clot formation. The uted blood is rapidly cleared from the subarachnoid space pacchionian granulations. Finally, the subarachnoid CSa relatively high oxygen tension (43 mm Hg) and therefdeoxyhemoglobin concentration is low (28%).
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 55/66
158 Neuroradiology: The Requisites
On CT SAH produces hyperdensity in the affected sulci, cis-terns, and fissures (Fig. 4-51). The hyperdensity changes quicklyover the first week with complete resolution within 2 days forsmall amounts of isolated superficial SAH and within 5 to 7 daysfor most aSAH. When hemorrhage is brisk the anticlotting mecha-nisms of the CSF may be overcome and focal clot will form at thesite of bleeding, producing an expanded hyperdense subarach-noid space with local mass effect and edema in the adjacent brain(Fig. 4-52A). Density will persist more than 1 week in focal suba-rachnoid clot or large-volume bleeds. Depending on the sourceand extent of SAH, intraventricular hemorrhage may coexist.
Historically, MR was felt to be insensitive to SAH. On rou-tine T1WI, SAH produces only subtle T1 hyperintensity (“dirty”
CSF) and normal intensity on T2WI. Rapid dilution and removof blood, absence of clot formation, and presence of high O2 con-centration (which limits the amount of deoxyhemoglobin) prevethe development of T2 and T2* hypointensity and subacutT1 hyperintensity. Although MR still has a “bad reputation” fdetecting SAH, the advent of FLAIR has markedly improved thsensitivity of MR to SAH (seeFig. 4-52). Blood in the subarach-noid space changes the T1 of the CSF sufficiently to prevent supression of signal by the 180-degree inversion pulse. Because Csignal is not suppressed, T2 effects are visible and the bloody Cis bright on FLAIR. In fact, for any given concentration of bloFLAIR is much more sensitive than CT. Ironically, while sensitivis high, specificity is low. Subarachnoid FLAIR hyperintensity m
B
D
A
C
F IGURE 4-51. Aneurysmal subarachnoid hemorrhage. A and B, Computed tomography scans at the level of the suprasellar cistern and inferior thventricle reveal diffuse hyperdensity in the suprasellar cistern sylvian fissures and anterior interhemispheric fissure. Intraventricular hemorrhydrocephalus are present.C, CT angiography source image reveals left anterior communicating aneurysm (arrow ).D, 3D reconstruction from catheterangiogram reveals relationship between aneurysm neck (arrows ) and adjacent anterior cerebral artery and anterior communicating artery.
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 56/66
V ASCULAR D ISEASES OF THE B RAIN 159
be seen in inflammatory and neoplastic leptomeningeal disease.Artifactual FLAIR hyperintensity occurs when metal is pres-ent (e.g., shunt valves, dental appliances) and when patients arebreathing pure oxygen (anesthesia) during the examination. (O2 is paramagnetic and its presence within the subarachnoid CSFshortens T1 sufficiently to prevent suppression of signal.) Themost common artifactual cause of FLAIR CSF hyperintensity ispulsation artifact at the skull base. This limits the utility of FLAIRin the region of the basal cisterns where aSAH is most common.In reality SAH that is detectable on CT is easily detected andcharacterized on MR; therefore, there is no danger of failing todetect unexpected SAH if MR rather than CT is performed as theinitial examination. When focal clot does form the MR intensi-ties encountered are similar to those seen in parenchymal hemor-rhage but without hemosiderin deposition. Acute clot is T2 andT2* hypointense and subacute clot is T1 hyperintense. Becauseacute clot is T2 hypointense it is isointense (not visible) to CSF onFLAIR but readily apparent on T2WI.
Causes of Subarachnoid Hemorrhage ( Box 4-6 )SAH may result from a variety of circumstances, includingtrauma, ruptured aneurysm, AVM, vasculopathy, venous throm-bosis, and extension of parenchymal hemorrhage into the suba-rachnoid space. The two most common causes of SAH are traumaand ruptured aneurysm. The pattern/location of SAH in theseentities is typically different (see Chapter 5).
Trauma There are four patterns of traumatic SAH. In most cases ofsevere head trauma SAH accompanies and is adjacent to paren-chymal or extra-axial hematomas. Isolated SAH overlying thecerebral hemispheres is relatively common in mild and moderatehead trauma. The small amount of sulcal hemorrhage will oftenresolve quickly (within 24 hours) and may be seen to migratetoward the vertex on serial examinations. It may be difficult oninitial examinations to differentiate between focal SAH and smallcortical contusions, and serial examinations may reveal evolutionof parenchymal contusions at the site of focal SAH. Extensivebasal SAH without parenchymal or extra-axial hemorrhage is
uncommon. It is typically a result of a traumatic dissectparticular of a vertebral artery. Basal skull fractures can rdissection of the carotid and proximal middle cerebral awith secondary SAH. Even when there is a history of trais necessary to exclude the possibility of an underlying anbecause spontaneous SAH may be the precipitating event
BA
F IGURE 4-52. Subarachnoid hemorrhage (SAH) on FLAIR. A, Computed tomography scan at the level of the suprasellar cistern reveals acusylvian fissure hematoma secondary to rupture of middle cerebral aneurysm hematoma. No other areas of SAH are visible (arrow , suprasellar cisterB, FLAIR image on same day reveals hyperintensity in the suprasellar cistern (long arrow ) and superficial sulci ( short arrows ) indicative of SAH visible on CT. Hyperacute right sylvian fissure hematoma is isointense.
B OX 4-6. Disorders Associated with IntracranialAneurysms
3M syndromeAlkaptonuriaAnderson-Fabry diseaseAutosomal dominant polycystic kidney disease (10% of
asymptomatic patients)Behçet diseaseCoarctation of the aortaCollagen vascular diseaseEhlers-Danlos syndrome type IVFamilial idiopathic nonarteriosclerotic cerebral calcific
syndromeFibromuscular dysplasiaHereditary hemorrhagic telangiectasiaHomocystinuriaMarfan syndromeMoyamoya diseaseNeurofibromatosis type 1Noonan syndromePseudoxanthoma elasticumSickle cell diseaseSystemic lupus erythematosusTakayasu diseaseTuberous sclerosisWermer syndromeα -Glucosidase deficiencyα 1-Antitrypsin deficiency
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 57/66
160 Neuroradiology: The Requisites
episode of head trauma. In these cases it is necessary to excludethe possibility of underlying aneurysm that may have precededand caused head trauma. Finally, a small amount of SAH is oftenseen in the interpeduncular cistern. This is a benign processwith no significant clinical sequelae.
Aneurysmal Subarachnoid Hemorrhage(see Figs. 4-51 and 4-52 )Aneurysmal SAH is typically centered around the base of the
brain, in particular within the suprasellar cistern (90% of aneu-rysms occur in the region of the circle of Willis). Although hemor-rhage is typically diffuse, the region with the most accumulationof blood is likely adjacent to the source of hemorrhage. Sensitivityof CT in the first 48 hours after aSAH approaches 95%. Sensitivitydecreases to about 50% by postictal day 5 as blood is resorbed.False-negative CT scans occur when the initial hemorrhage ismild, when it results from posterior fossa aneurysms, or whenthe initial CT is obtained several days after ictus. Recognition ofsubtle signs of aSAH is of paramount importance. Subtle SAH isrelatively isodense to adjacent brain and therefore the basal cis-terns are not visible (seeFig. 4-53). The hypodense CSF withinthe anterior third ventricle and temporal horns of the lateral ven-tricles, and sometimes the aneurysm itself, stands out becausenormal cisternal CSF density is not present. Careful inspection ofthe sylvian fissures and the anterior interhemispheric fissure willtypically reveal mild hyperdensity or at the least no hypodensity.In normal individuals these cisternal spaces may be small, butcareful inspection should reveal some normal hypodense CSF.Posterior fossa SAH (e.g., from posterior inferior cerebellar arteryaneurysms) is also difficult to detect because the cisterns are com-monly small and beam-hardening artifact from the skull base mayobscure the CSF spaces. When subtle SAH is suspected, alwayscheck the occipital horns of the lateral ventricles and the fourthventricle for hyperdensity (seeFig. 4-53B). Extension of hemor-rhage into the ventricular system is common. The intraventricu-lar hemorrhage layers and becomes relatively hemoconcentratedin the dependent portions of the ventricles. Presence of intraven-tricular hemorrhage therefore helps to confirm the diagnosis ofSAH in cases with subtle findings.
VASCULAR ABNORMALITIESCerebral Aneurysms ( Fig. 4-54 ; Box 4-7 )An aneurysm is a focal dilatation of an artery. Many differetypes of aneurysms involve the CNS. The most frequent aneurysm encountered in the CNS is the saccular (berry) aneurysA fusiform aneurysm is a diffuse long segment enlargement a vessel, most commonly the distal vertebral, basilar, or promal MCA (seeFig. 4-54F and G). Fusiform aneurysms are mostoften the result of severe atherosclerosis but may also be se
in traumatic and spontaneous arterial dissection, in associatiwith vasculopathies and congenital conditions, including colgen disorders and neurofibromatosis type 1. Septic emboli mlead to development of mycotic aneurysms, which are typicasmall and arise from distal vessels, most frequently in the MCdistribution. Aneurysms may be seen on feeding vessels or withthe nidus of high-flow AVMs. Neoplastic aneurysms result frotumor emboli and subsequent growth of the neoplasm througthe vessel wall.
Saccular (seeFigs. 4-51 and 4-54A–E) aneurysms are out-pouchings from a parent vessel, most often at a point of vesbranching. They form as a result of damage to the endotheliumthinning of the tunica media, and fragmentation of the intenal elastica, likely the result of shear forces, where a formestraight vessel curves and gives off branches. The etiology aneurysms remains controversial. The advent of noninvasivascular imaging has made it clear that saccular aneurysms rarely seen in children or young adults unless there is a prdisposing factor (see above). They are acquired, not congeital, lesions that typically develop after the fourth decade life. Although not congenital, there are clearly genetic forcat work. Multiple aneurysms are present in approximately 20of patients presenting with aSAH, and there is a higher thaexpected incidence of aneurysms (7% to 20%) in individuawith first-degree relatives who have suffered aSAH. Patholoevaluation of vessel wall histology in patients who have haSAH reveals no differences from normal vessels. Conditiothat are believed to increase the incidence of aSAH include ciarette smoking, rapid increase in blood pressure (e.g., cocaiuse), and binge drinking.
F IGURE 4-53.Isodense subarachnoid hemorrhage. Three-day history of severe headache. A, Scan at the level of the suprasellar cistern reveals that onlthe anterior third ventricle and temporal horns are hypodense. The basal cisterns (arrows ) are isodense.B, Scan at the level of foramen of Monro reveals
no visualization of normal fluid density in the sylvian fissures, interhemispheric fissures, and superficial sulci. Hyperdensity in the occipital hlateral ventricles (arrows ) confirms the presence of intracranial hemorrhage.
BA
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 58/66
V ASCULAR D ISEASES OF THE B RAIN 161
The reported frequency of aneurysms in different locdepends on whether one includes ruptured aneurysms orruptured and unruptured aneurysms. From the InternatCooperative Study on the Timing of Aneurysm Surgerylished in 1990, the frequency of ruptured aneurysms wfollows: anterior communicating/ACA, 39%; supraclinonal carotid artery (posterior communicating, anterior choophthalmic segment origins, and carotid terminus), 30%;22%; and vertebrobasilar circulation (basilar tip, origin terior inferior cerebellar artery and superior cerebellar ar
F IGURE 4-54. Aneurysms. Catheter angiography of an anterior communicating artery aneurysm. A, Oblique view of a left internal carotid angioreveals aneurysm of the anterior communicating artery.B, 3D reconstruction from rotational angiogram provides more detail of the aneurysm,the presence of luminal irregularity and small outpouching as well as the relationship between the aneurysm and the A2 segment of the bral artery.C andD, Computed tomography angiogram (CTA) of left posterior communicating artery (PCoA) origin aneurysm. Source ima(C ) reveals aneurysm extending posteriorly from the carotid artery. Note that the large PCoA takes origin from the medial wall of the anthan the internal carotid artery. CTA 3D image (D ) confirms origin of the PCoA rather than the carotid artery. Aneurysm has a well-defined nrelatively smooth.E, Catheter angiogram of a giant internal carotid artery aneurysm that had recently bled. Coronal (F ) and sagittal (G ) maximal intesity projection views from a CTA reveal large irregular fusiform aneurysm of sylvian branch of the middle cerebral artery. Aneurysm m
or the result of dissection.
C
E F G
BA
D
B OX 4-7. Aneurysms
DissectingFusiform or atheroscleroticMycoticNeoplasticPseudoaneurysmSaccular or berryTraumatic
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 59/66
162 Neuroradiology: The Requisites
8%. The remaining aneurysms were unclassified but includeaneurysms on more distal branches, such as the pericallosalartery and posterior cerebral artery. The incidence of unrupturedaneurysms based on angiographic and autopsy studies is approx-imately 5%. When unruptured aneurysms are included, thefrequency of MCA aneurysms and ophthalmic artery originaneurysm increases.
Incidentally discovered unruptured aneurysms that are smallerthan 5 mm are unlikely to bleed, and the incidence of hemorrhageincreases with aneurysm size. This fact leads to an apparent par-adox because many ruptured aneurysms are smaller than 5 mm(some as small as 1 to 2 mm). The paradox is solved if one con-siders the natural history of aneurysms. An aneurysm forms andgrows acutely. During the acute stage the aneurysm may bleed(even when small) or stabilize. Aneurysms that stabilize at smallerthan 5 mm are less likely to grow and are unlikely to bleed.Aneurysms that stabilize at more than 5 mm are likely to grow andmany may eventually hemorrhage. There are no clear guidelineson the appropriate treatment (surgical excision or endovascularablation or even watchful waiting) for small unruptured aneu-rysms. Although size matters, it is not the sole determining fac-tor. Aneurysm morphology, patient age, patient comorbidity, theskill/experience of the particular treating neurosurgeon or inter-ventional neuroradiologist, and most importantly the patient’s
wishes must all be factored into the therapeutic plan. If a decisionis made to not treat an aneurysm, serial noninvasive studies (CTAor MRA) should be performed because an increase in aneurysmsize or change in morphology are indications of instability and pos-sible future hemorrhage.
The average age of patients with aSAH is 50 years. Before age50, men have a higher incidence, but postmenopausal womenhave a higher incidence than men. Whereas the treatment (ornot) of unruptured aneurysms remains controversial, the treat-ment of ruptured aneurysms is not. Aneurysmal SAH is a dev-astating and often fatal disease. Approximately 12% of patientswith aSAH die before reaching the hospital. Forty percent of hos-pitalized patients die within 1 month of ictus and one third of thesurvivors have major neurologic deficits. Rebleeding occurs in20% of untreated patients within 2 weeks of initial hemorrhage,in 30% by 1 month, and in 40% by 6 months. Rebleeding is asso-ciated with a mortality rate in excess of 40%. Even after 1 yearthe rebleeding rate is 2% per year. New aneurysms have beenreported to develop in at least 2% of patients with previously rup-tured aneurysm. The incidence of SAH in the United States isabout 1 in 10,000, but is 6 to 10 times higher in patients withprevious SAH who have a new aneurysm.
Because of this grave prognosis, especially for untreated rup-tured aneurysm, correct diagnosis at time of presentation andappropriate treatment are mandatory if there is to be any hope ofgood recovery. Although the sensitivity of CT is high, the penaltyof failing to diagnose aSAH is so severe that a normal CT scanshould not be taken as a reason to stop further workup if there isa clinical suspicion of SAH. Lumbar puncture, MR, CTA/MRA,and even catheter angiography may be undertaken when there isevidence of aSAH.
Workup of Aneurysmal Subarachnoid HemorrhageThe workup of aSAH has evolved over the past few years underthe influence of rapidly advancing technology (CTA) and newtreatment options (endovascular versus open surgical). The ini-tial imaging examination remains a CT scan. In addition to doc-umenting the presence of SAH, the pattern of hemorrhage willtypically be a good indicator of the site of hemorrhage if multipleaneurysms are present. ACoA aneurysms produce symmetric SAH(seeFig. 4-51) centered on the suprasellar cistern, anterior inter-hemispheric fissure, and cistern of the lamina terminalis (the CSFspace below the frontal horns of the lateral ventricles). Extensioninto the lateral ventricles from the cistern of the lamina terminalis
is common. When hemorrhage is brisk focal clot may developthe inferior medial frontal lobe. Posterior communicating (PCoanterior choroidal and carotid terminus aneurysms produce heorrhage centered on the suprasellar cistern, often with extensiinto the ipsilateral sylvian fissure and anterior portion of the pimesencephalic cistern. MCA aneurysms typically arise from lateral portion of the horizontal segment of the MCA where tvessel divides (M1-M2 junction) into its sylvian branches. SAfrom MCA aneurysms has a similar pattern to that seen with PCaneurysms, but SAH is most marked near the root of the sylvifissure rather than in the suprasellar cistern. Brisk hemorrhafrom an MCA aneurysm may produce thick clot that expands tsylvian fissure and mimics a parenchymal hematoma (seeFig. 4-52). Basilar tip aneurysms produce SAH centered in the interpduncular cistern with extension into the suprasellar cistern and tanterior and posterior perimesencephalic and prepontine cisternPosterior inferior cerebellar artery aneurysms produce SAH thaconfined to the posterior fossa and upper cervical region and therefore often difficult to detect. Presence of apparently isolatintraventricular hemorrhage in the fourth ventricle should raisuspicion of a ruptured posterior inferior cerebellar artery anerysm. At the time of the initial examination some degree of hydcephalus is virtually always present due to partial obstructionCSF outflow. Presence of severe hydrocephalus requires emerge
placement of a ventricular drain and therefore should be reportto the referring physician. Sometimes the offending aneurysm wbe outlined as a “filling defect” by salt in the cisterns. Look for tfinding. In addition to providing information on the likely site hemorrhage, the initial CT also provides prognostic informatioPoor outcome is associated with “thick” SAH (due to the likedevelopment of vasospasm) and extensive intraventricular hemrhage. The Fisher grade of SAH reflects the risk from SAH siand spread to the parenchyma: Grade 1 has no SAH present, Gra2 is less than 1 mm thick on CT, Grade 3 is more than 1 mm thion CT, and Grade 4 shows intraventricular hemorrhage or parechymal blood. The higher the grade, the worse the prognosis.
The Hunt and Hess classification scheme may suggest lonterm prognosis (Table 4-4).
In most institutions, the noncontrast CT is followed immedately by a CTA. With modern multidetector (16 row or greateCT scanners these examinations can be completed in less tha2 minutes as long as there is good venous access. If the patieis deemed to be a surgical candidate the anatomic informatioprovided by the CTA is often sufficient to proceed to surgereliminating the need for catheter angiography in unstable oldpatients. If the patient is deemed to be a candidate for endovascular treatment (as more and more patients are), diagnosangiography and endovascular intervention are performed in tsame sitting. In all cases of confirmed or strongly suspected aSa negative CTA should not be considered sufficient for exclsion of aneurysm. Catheter angiography with visualization ofintracranial vessels should be performed in these cases.
T ABLE 4-4. Hunt and Hess Grading System
Grade Signs and Symptoms Survival
1 Asymptomatic or minimal headache andslight neck stiffness
70%
2 Moderate to severe headache; neckstiffness; no neurologic deficit exceptcranial nerve palsy
60%
3 Drowsy; minimal neurologic deficit 50%4 Stuporous; moderate to severe hemiparesis;
possibly early decerebrate rigidity andvegetative disturbances
20%
5 Deep coma; decerebrate rigidity; moribund 10%
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 60/66
V ASCULAR D ISEASES OF THE B RAIN 163
The goal of angiography (however performed) is to character-ize the aneurysm and its relationship to adjacent vessels so thatappropriate therapy can be planned (seeFig. 4-54). Advances insurgical techniques, aneurysm clips, endovascular coils, and stentsprovide the treating physician with many more therapeutic optionsthan were available even a short time ago. Angiographic studies areused to choose among these options before starting the interven-tion. Key findings that need to be recognized and reported includeaneurysm size, including maximum diameter and width, and aneu-rysm neck morphology. The neck may be narrow or broad based,and it may be incorporated into the wall of the parent vessel orthe origin of the branching vessel (e.g., PCoA aneurysms), requir-ing vascular reconstruction at the time of intervention (e.g., stentplacement). In addition, the shape and contour of the aneurysm areimportant findings. Multilobed aneurysms, irregular aneurysms,and aneurysms with focal outpouchings at the dome (“Murphy’stit”) are indicators of prior hemorrhage or propensity for futurehemorrhage. A filling defect within the aneurysm is indicative ofacute clots that carry an increased risk for embolization. Anotherimportant factor is wall thickness. Thick-walled aneurysms arelikely chronic with episodes of prior intraluminal or intramuralhemorrhage. The precise relationship to adjacent vessels that maybe closely applied to aneurysms and the normal anatomic variationsof the circle of Willis and vertebral basilar system should be noted
because they have a significant effect on treatment choices. Duringtreatment, extra care must be taken when an aneurysm arises nearthe origin of a “dominant” PCoA that provides all or most of thearterial supply to the posterior cerebral artery or when there is anACoA aneurysm in an individual with a hypoplastic A1 segmentof ACA. The presence of focal or diffuse spasm, and aneurysmwall and neck calcification, which will make successful clippingmore difficult because the “squeeze” cannot be applied with such“hard” calcified walls, should be noted, as should the presence ofadditional aneurysms. When multiple aneurysms are present, thelikely source of SAH must be determined. Indicators of source ofhemorrhage include pattern of SAH on CT (see above), size andshape of aneurysm (the largest or most irregular is most likely tohave ruptured), and location of vasospasm if present. If the site ofhemorrhage cannot be determined on the basis of CT and angio-graphy, MR can be performed. Focal clot is more readily identifiedon MR than CT (see above), and the location of clot is an excellentindicator of site of hemorrhage.
Aneurysms larger than 3 mm rarely present diagnostic diffi-culty; however, small aneurysms may be difficult to diagnose.A small looping arterial branch may be mistaken for an aneu-rysm on a single angiographic view. 3D CTA and 3D catheterangiographic capacity have made it relatively easy to differen-tiate loops from small aneurysms. Some vessels, in particularthe PCoAs, may have a somewhat dilated origin (infundibulum)that may mimic an aneurysm. Typically the branch vessel isseen to “arise” from the apex of the conical vessel origin. Whenthe branch vessel is small it may be difficult to visualize on CTAimages; therefore, careful evaluation of source images is nec-essary to differentiate between infundibulae and aneurysms. Itis of course imperative to evaluate the entire vascular system.Aneurysms in unusual locations can be overlooked unless a sys-tematic search of the angiographic examination is undertaken,in particular on CTA.
In the week after initial diagnosis and treatment, clinical dete-rioration may occur for a number of reasons: (1) recurrent hem-orrhage, in particular if exclusion of the aneurysm cannot beachieved; this will often extend into the brain parenchymabecause the aneurysm has become adherent to the adjacent brain;(2) possible progression of hydrocephalus if a ventricular cathe-ter is not in place or is not functioning; (3) vasospasm as a resultof chemical irritation to the arterial wall (the most common andserious cause of deterioration); or (4) stroke. Spasm usually beginsapproximately 3 days after the initial bleed and can persist orworsen over the next 2 weeks if not treated. It may be focal or dif-
fuse. If unchecked, spasm can lead to infarction distal to throwing. Medical treatment includes hypertension, hypervoand hemodilution (“Triple H” therapy). Endovascular treatmincluding angioplasty and stenting, may be performed whenical therapy is ineffective. The diagnosis of vasospasm (inular before it leads to permanent infarction) is difficult. Ovascular distribution, hypodensity is visualized only aftertion has occurred. Transcranial Doppler ultrasound and CTdemonstrate luminal narrowing and decreased flow beforetion occurs, but many patients have “clinical vasospasm” wangiographic abnormality. CT perfusion can be performed junction with CTA (as it is in acute stroke) to assess blooand to guide treatment.
Assuming that the patient survives the initial postictal pserial CT scans will show resolution of hemorrhage and edmost individuals hydrocephalus will also resolve. Less thof patients with aSAH require permanent shunting. Residuosis and volume loss will be present at sites of prior parenhemorrhage or severe vasospasm. Aneurysm clips and coiartifacts on both CT and MR that obscure the brain adjacthe treated aneurysm. Whatever the treatment, it is impto assess for aneurysm regrowth. Even minimal residualof an aneurysm can lead to progressive enlargement of therysm with peripheral displacement of the clips or coils. Cu
follow-up aneurysm checks are performed with MRA foraneurysms and CTA for clipped aneurysms because coils pmore artifacts on CT and clips produce more artifacts oCatheter angiography is performed only when suspectedrysm regrowth is sufficient to warrant evaluation for retre
Angiographically negative spontaneous SAH occurs in amately 10% of cases. It may be seen when there is severspasm or when the aneurysm has filled with clot, when theof hemorrhage is within the spinal canal, or when hemoarises from the venous plexus posterior to the clivus. Spontthrombosis of an aneurysm may seem like a good thinunfortunately these aneurysms virtually always recur andquently bleed. Therefore, when the initial angiographic sare negative or reveal only vasospasm but the pattern of SCT or MRI (e.g., focal clot at a common location for aSsuggestive of aneurysmal hemorrhage, repeat angiography1 week of the initial bleed is necessary. This is a truly pous situation because recanalization can occur at any timhemorrhage (often massive) often follows shortly thereafrare occasions, intracranial SAH occurs secondary to a vanomaly in the cervical spine, such as an AVM or AV fistustudies of the cervical spine can be performed to excludpossibility, in particular if large amounts of SAH are idearound the foramen magnum or in the upper cervical sproutine head CT scans.
The most common cause of angiographically negativeis benign nonaneurysmal perimesencephalic SAH (Fig. 4-55)The clinical presentation is similar to that seen in mild except patients are typically younger and there is a maldominance. These cases have an uncomplicated clinical (hydrocephalus and vasospasm may develop but are tymild) and rehemorrhage does not occur (hence the namebenign)Current opinion is that hemorrhage arises from the richclival venous plexus, and anecdotal evidence suggests may be associated with coitus. Before a diagnosis of norysmal perimesencephalic SAH can be made, vertebral aneurysmal subarachnoid hemorrhage must be excludedafter a negative angiogram and a characteristic appearathe site of hemorrhage adjacent to the basilar tip or in thepeduncular cistern can one begin to raise the presumptioit is nonaneurysmal. At least one follow-up angiographi(CTA or catheter angiogram) should be performed to cthat no aneurysm is present. MR is also a useful adjunctT1 hyperintense clot surrounding the distal basilar artery ally seen from 3 to 10 days after SAH.
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 61/66

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 62/66
V ASCULAR D ISEASES OF THE B RAIN 165
large, draining most of a cerebral hemisphere. These lesions arevisible on unenhanced MR scans. One important aspect of thislesion is that the DVA is a compensatory drainage route for normalbrain. Sacrifice of this pathway can produce venous infarction oftissue being drained. Therefore, these lesions are not amenableto surgical or endovascular treatment unless hemorrhage is life-threatening or resection of the adjacent brain will not cause majordeficit. DVAs and cavernomas often coexist.
Arteriovenous Malformations ( Fig. 4-57 )True AVMs contain one or more enlarged feeding arteries and anidus and have enlarged early draining veins. They are consideredcongenital anomalies of blood vessels that arise in fetal life but
usually become symptomatic in the third or fourth decalife. They have a tendency to hemorrhage at a rate that haestimated in a study from Finland to be 4% annually (3% in the United States) with an annual mortality rate and a mean interval between hemorrhagic events of 7.7Steal phenomenon is a recognized complication of AVwhich blood preferentially seeks the AVM and normalparenchyma is hypoperfused. Steal can produce focal logic symptoms, seizures, and ultimately parenchymal the affected part of the brain without hemorrhage. Highaneurysms can be detected on feeding arteries or draining(varicosities) and may be a source of hemorrhage rather thAVM proper. The AVM consists of a feeding artery or awhich are usually dilated, and a cluster of entangled va
B
D
A
C
F IGURE 4-56. Cavernous malformation and developmental venous anomaly (DVA). A, T1-weighted image (T1WI) reveals a mixed-intensity with small foci of hyperintensity and mild peripheral hypointensity.B, T2WI reveals a peripheral hypointense margin with central foci of both tensity and hyperintensity.C, Gradient-echo scan reveals marked peripheral hypointensity that extends into and “stains” the adjacent paD, Enhanced T1WI reveals linear enhancing DVA that surrounds the cavernous malformation and drains into the subependymal venou
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 63/66
166 Neuroradiology: The Requisites
loops (the core or nidus) connected to abundant vascular chan-nels where the arterial blood is shunted, finally terminating inenlarged draining veins. The draining veins are typically muchlarger than the feeding arteries. Intranidal aneurysms can bedetected in more than 50% of AVMs. In unruptured AVMs, thepresence of nidal aneurysms and relative small size and numberof draining veins have been associated with an increased risk ofhemorrhage. AVMs can be supplied by a single or multiple vas-cular systems (e.g., anterior and middle cerebral arteries). Duralarteries can be recruited to supply superficial AVMs, in particu-lar in the posterior fossa. It is important to map completely the
anatomy of these lesions. AVMs have been classified accordito their size, location, and venous drainage (Table 4-5). Thehigher the score, the worse the surgical outcome.
The diagnosis of AVM without associated hemorrhage can made in most cases on routine CT or MR. On CT, the dilatevessels (mostly the draining veins) in or adjacent to the braparenchyma are mildly hyperdense without contrast (blood poeffect) and have a serpentine, punctate, or an irregular mélanconfiguration (seeFig. 4-55). Curvilinear or speckled calcificationmay be present. Surrounding hypodensity indicative of gliofrom chronic ischemia or prior hemorrhage may be present. T
I
B C
D
A
E
G H I
F
F IGURE 4-57. Arteriovenous malformation (AVM). Sagittal T1-weighted image (T1WI) ( A ) and coronal T2WI (B ) reveal dilated right middle cerebralartery (MCA) branches ( short arrow in A ) and draining veins (long arrow ). Nidus of malformation ( short arrow inB ) and aneurysmal venous dilation (longarrow inB ) are visible as well.C, Noncontrast computed tomography (CT) reveals hyperdense material in the right parietal lobe without edema oeffect.D, On source images from CT angiography (CTA) dilated pericallosal artery ( short arrow ), nidus (medium arrow ), and markedly dilated drainingveins (long arrows ) are visible.E , Coronal maximal intensity projection image from CTA reveals dilated MCA branches ( short arrow ), the nidus (mediumarrow ),and dilated draining veins (long arrows ) as well.F, CTA 3D image reveals all components of the AVM. Catheter angiogram reveals sequentiaing of all components of the AVM during early (G ), mid (H ), and late phases (I ).
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 64/66
V ASCULAR D ISEASES OF THE B RAIN 167
vascular nature of these lesions is apparent on enhanced scanswhere the intensely enhancing curvilinear structures are visible.On MR curvilinear flow voids in dilated veins are observed, andmodestly dilated proximal arteries can also be noted. AVMs are
visible on routine MRA and CTA, but these studies do not yetprovide much useful temporal information because the feedingarteries and draining veins are visualized simultaneously. Theintroduction of time-resolved enhanced MRA and CTA has dra-matically improved the utility of these techniques in assessmentand treatment planning.
AVMs are common causes of spontaneous parenchymalhemorrhage in adults (age 20 to 50 years). Hemorrhage mayoccur in any portion of the brain. Careful evaluation of non-contrast CT scans may reveal evidence of dilated drainingveins. On MR, draining veins and enlarged feeding arteriesare more readily apparent. In approximately 30% of patientswith parenchymal hemorrhage secondary to AVMs the abnor-mal vessels cannot be detected on routine CT or MR. Be sureto carefully observe the enhanced MR scans because the AVM
may be apparent on careful scrutiny of these images as a smalltuft where veins drain. Missing the AVM occurs most oftenwith small AVMs and when the AVM is located near a majordural venous sinus. In these cases, the draining veins need totravel only a short distance and may not be apparent on routineimaging. Less commonly, the hemorrhage or compression fromthe hematoma will temporarily obscure the underlying AVM.Therefore a normal CT, MR, CTA, or MRA does not “ruleout” an underlying AVM.
The definitive study for detection and characterization ofAVMs is catheter angiography. The diagnosis is made by dem-onstrating enlarged feeding arteries, the core or nidus, and theenlarged draining veins. If the initial angiogram is negative butother causes of hemorrhage have been excluded, repeat angiog-raphy is warranted because small AVMs may be temporarilyobscured by mass effect from acute hemorrhage.
Vein of Galen malformations are a special type of AVM.These malformations often present in infancy with signs ofhydrocephalus (rapidly enlarging head, seizures) or high-out-put cardiac failure. Imaging reveals a markedly enlarged veinof Galen or basal vein of Rosenthal. (Technically the enlargedvein is not the vein of Galen but rather an enlarged medianprosencephalic vein.) The dural sinuses are also enlarged,and there is often a persistent falcine sinus draining superi-orly into the superior sagittal sinus. These malformations arethe result of direct fistulae from choroidal arteries arising fromthalamoperforate branches of the basilar and proximal poste-rior cerebral arteries into the deep venous system. On CT andMR, the dilated veins and enlarged feeding arteries are easilyvisualized. Hydrocephalus is virtually always present. Common
complications include intraventricular hemorrhage anddural sinus thrombosis. The brain may be atrophic or adelayed in development due to in utero ischemia as a of chronic steal phenomena. Prognosis is poor withoutment and as a rule of thumb the earlier the presentationworse the outcome. Treatment is endovascular occlusiondiagnostic and therapeutic catheter angiography is challbecause flow is very high and total allowable contrast limited by the small size and often tenuous cardiac stathe infant. In many cases, treatment must be staged to sreduce flow through the malformation. Dilation of the vGalen may occur with pial AVMs as well; however, patieolder (children or adults), the vein of Galen is less dilatehydrocephalus is not present.
A few genetic syndromes are associated with vasculaformations. Wyburn-Mason syndrome is a disorder of cutaneous, mandibular, and brain stem vascular malftions. Klippel-Trenaunay-Weber syndrome is a hemihtrophy syndrome with angiomatosis of the extremitthe brain. It may be part of the Sturge-Weber spectHereditary hemorrhagic telangiectasia (HHT), (Osler-WeberRendu disease) is an autosomal dominant (endoglin [ ENGgene on chromosome 9 and activin receptor-like kinaseon chromosome 12) vascular disorder with mucocut
telangiectasias and visceral AVMs. Two percent of ceAVMs have been reported to be associated with HHT, anto 10% of patients with HHT have cerebral AVMs (muin 50% of cases). These lesions tend to be small and cin location.
Treatment of AVMs depends on size, location, and aarchitecture. It consists of endovascular therapy, surgeryation therapy, or combinations thereof. In cases of AVthan 3 cm in diameter, stereotactic radiotherapy is the ment of choice (depending on location), with cure ra80% to 90% within 2 to 3 years. An immediate complassociated with surgical or endovascular treatment of with extensive steal is brain swelling (sometimes resultrapid herniation and death) or hemorrhage. This is secoto perfusion pressure breakthrough related to marked hdynamic changes after obliteration of the AVM. The ccally hypoperfused brain is unable to autoregulate becalong-standing ischemia and the abrupt change in hemodyics after obliteration of the AVM. Staged treatment is theadvocated to prevent perfusion breakthrough from occThe rate of cure for endovascular treatment alone is apmately 20%.
Dural Arteriovenous Fistula Dural arteriovenous fistula (DAVF) are acquired lesionare the consequence of dural sinus thrombosis with quent often sudden recanalization of the sinus resultidirect communication between the small dilated arteries sinus wall and the sinus lumen. This results in increasedsure within the sinus and impaired outflow from the adbrain. Development of “downstream” stenosis due to turbhigh flow may further compromise venous drainage and ivenous back-pressure. As a result cortical veins may dilatemay in turn result in parenchymal hemorrhage, SAH, vinfarction, and elevated intracranial pressure. Increased neurologic deficits is associated with dural fistulae that (1) deep venous system, (2) have associated retrograde venou(3) have venous aneurysms, (4) have stenotic channels twhich they must drain, and (5) are complex.
Symptoms depend on the location, size of the malformand venous drainage pattern. Parasellar malformations ing into the cavernous sinus with retrograde flow in the sophthalmic vein (supplied from the meningohypophysealaccessory meningeal artery, middle meningeal artery, br
T ABLE 4-5. AVM Classification
Feature Score
Size<3 cm 13–6 cm 2>6 cm 3
EloquentNo 0Yes 1
Venous DrainageSuperficial only 0Any deep 1
From Spetzler RF, Martin NA: A proposed grading system for arteriovenous malfor-mations. J Neurosurg 65:476–483, 1986.
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 65/66
168 Neuroradiology: The Requisites
of the ascending pharyngeal artery, and other vessels) create alow-flow nontraumatic carotid-cavernous fistula. CT and MRreveal enlargement of the cavernous sinus and superior ophthal-mic vein, as well as stranding of intraorbital fat, enlargement ofextraocular muscles, and proptosis. Patients present with propto-sis, visual loss due to glaucoma, and ophthalmoplegia. Slow-flowcarotid-cavernous fistulae can spontaneously resolve (sometimesaided by intermittent ipsilateral carotid artery compression) orcan improve after incomplete embolization or even after diag-nostic angiography. Endovascular particulate occlusion of feed-ing arteries can be performed when less invasive measures fail.Fistulae arising from the sigmoid sinus can present with tinni-tus and bruit over the temporal bone and are the most commonlocation for dural AVFs. Transverse sinuses and superior sagittalsinus fistulae and/or sinus stenoses may present with parenchy-mal hemorrhage and increased intracranial pressure (pseudo-tumor cerebri, idiopathic intracranial hypertension). Rarely,patients may present with progressive dementia due to chronichypoperfusion. Even patients who have been symptomatic foryears may demonstrate resolution of dementia after treatmentof the fistula.
Dural fistulas associated with the superior sagittal sinus, trans-verse sinuses, and sigmoid sinuses are often difficult to diagnose.Routine CT and MR may be normal or demonstrate a “tight”
brain with small ventricles and sulci. Subtle enlargement ofcortical veins and dural sinus enlargement may be present butis easily overlooked. In other cases CT and MR may demon-strate prominent vessels associated with a parenchymal hema-toma, mimicking an AVM. Chronic fistulae may produce dilatedvessels throughout the cranial cavity with little hint as to theactual location of the malformation. CTA and MRA may appearnormal or may demonstrate dilated middle meningeal or pos-terior fossa arteries. MRV and CTV may document regions ofvenous sinus stenosis or focal occlusion. Catheter angiography isthe key to the diagnosis of this lesion. The initial internal carotidor vertebral artery injections may reveal little or no abnormality(often a surprise in patients with parenchymal hemorrhages asso-ciated with dilated vessels). Injections into the common carotidarteries or selective injection of the external carotid arterieswill demonstrate the dilated meningeal arteries, the site of thefistulae, and delayed filling of cortical veins. Dural malforma-tions can be treated with success by embolization using liquidagents (e.g., Onyx, n=BCA glue). These agents, however, areassociated with increased risk of complications, including skinnecrosis, cranial nerve palsies (Onyx), and visual loss. Anotherapproach to reduce venous hypertension is to reopen by stent-ing the previously thrombosed sinus with restoration of normalflow patterns.
S UGGESTED R EADINGS
Adams HJ, Bendixen B, Kappelle LJ, et al: Classification of subtype of acuteischemic stroke. Definitions for use in a multicenter clinical trial. TOAST: Trialof Org 10172 in Acute Stroke Treatment, Stroke 24(1):35–41, 1993.
Alhalabi M, Moore P: Serial angiography in isolated angiitis of the central nervoussystem, Neurology 44(7):1221–1226, 1994.
Anderson SC, Shah CP, Murtagh FR: Congested deep subcortical veins as a signof dural venous thrombosis: MR and CT correlations, J Comput Assist Tomogr 11:1059–1061, 1987.
Anderson G, Ashforth R, Steinke DE, et al: CT angiography for the detection ofcerebral vasospasm in patients with acute subarachnoid hemorrhage, AJNR Am J
Neuroradiol 21(6):1011–1015, 2000.Atlas S, DuBois P, Singer MB, et al: Diffusion measurements in intracranial
hematomas: implications for MR imaging of acute stroke, AJNR Am J Neuroradiol 21(7):1190–1194, 2000.
Atlas SW, Mark AS, Grossman RI, et al: Intracranial hemorrhage: gradient-echo MR imaging at 1.5T: comparison with spin-echo imaging and clinicalapplications, Radiology 168:803–807, 1988.
Atlas S, Thulborn K: MR detection of hyperacute parenchymal hemorrhage of thebrain, AJNR Am J Neuroradiol 19(8):1471–1477, 1998.
Baird A, Loveblad K, Schlaug R, et al: Multiple acute stroke syndrome: marker ofembolic disease, Neurology 54(3):674–678, 2000.
Baird A, Warach S: Magnetic resonance imaging of acute stroke, J Cereb Blood Flow Metab 18(6):583–609, 1998.
Bizzi A, Brooks RA, Brunetti A, et al: Role of iron and ferritin in MR imaging othe brain: a study in primates at different field strengths, Radiology 177:59–65,1990.
Bradley WG, Schmidt PG: Effect of methemoglobin formation on the MRappearance of subarachnoid hemorrhage, Radiology 156:99–103, 1985.
Bragoni M, Di Piero V, Priori R, et al: Sjögren’s syndrome presenting as ischemstroke, Stroke 25(11):2276–2279, 1994.
Broderick JP, Brott TG, Tomsick T, et al: Ultra-early evaluation of intracerebralhemorrhage, J Neurosurg 72:195–199, 1990.
Brooks RA, Di Chiro G, Patronas N: MR imaging of cerebral hematomas atdifferent field strengths: theory and applications, J Comput Assi st Tomogr
13:194–206, 1989.Bruggen NV, Syha J, Busza AL, et al: Identification of tumor hemorrhage in an animodel using spin echoes and gradient echoes, Magn Res Med 15:121–127, 1990.
Chalela J, Alsop D, Gonzalez-Atavales JB, et al: Magnetic resonance perfusionimaging in acute ischemic stroke using continuous arterial spin labeling, Stroke 31(3):680–687, 2000.
Chimowitz MI, Awad IA, Furlan AJ: Periventricular lesions on MR: facts andtheories, Stroke 20:963–967, 1989.
Clark RA, Watanabe AT, Bradley WG, et al: Acute hematomas: effects ofdeoxygenation, hematocrit, and fibrin-clot formation and retraction on T2shortening, Radiology 175:201–206, 1990.
Crain MR, Yuh WTC, Greene GM, et al: Cerebral ischemia: evaluation withcontrast-enhanced MR imaging, AJNR Am J Neuroradiol 12:631–639, 1991.
Di Chiro G, Brooks RA, Girton ME, et al: Sequential MR studies of intracerebrhematomas in monkeys, AJNR Am J Neuroradiol 7:193–199, 1986.
Ebisu T, Tanaka C, Umeda M, et al: Hemorrhagic and nonhemorrhagic stroke:diagnosis with diffusion-weighted and T2-weighted echo-planar MR imaging
Radiology 203(3):823–828, 1997.Edelman RR, Johnson K, Buxton R, et al: MR of hemorrhage: a new approach,
AJNR Am J Neuroradiol 7:751–756, 1986.Essig M, von Kummer R, Egelhof T, et al: Vascular MR contrast enhancement in
cerebrovascular disease, AJNR Am J Neuroradiol 17(5):887–894, 1996.Forbes K, Pipe J, et al: Evidence for cytotoxic edema in the pathogenesis of
cerebral venous infarction, AJNR Am J Neuroradiol 22(3):450–455, 2001.Futrell N, Millikan C: Frequency, etiology, and prevention of stroke in patients
with systemic lupus erythematosus, Stroke 20:583–591, 1989.Gammal TE, Adams RJ, Nichols FT, et al: MR and CT investigation of cerebrovascu
disease in sickle cell patients, AJNR Am J Neuroradiol 7:1043–1049, 1986.Giang D: Central nervous system vasculitis secondary to infections, toxins, and
neoplasms, Semin Neurol 14(4):313–319, 1994.Gillard J, Barker P, van Zijl PC, et al: Proton MR spectroscopy in acute middle
cerebral artery stroke, AJNR Am J Neuroradiol 17(5):873–886, 1996.Goldberg HI, Grossman RI, Gomori JM, et al: MR diagnosis of cervical interna
carotid artery dissecting hemorrhage, Radiology 158:157–161, 1986.Gomori JM, Grossman RI: Mechanisms responsible for the MR appearance and
evolution of intracranial hemorrhage, Radiographics 8:427–439, 1988.Gomori JM, Grossman RI, Bilaniuk LT, et al: High-field MR imaging of superfic
siderosis of the central nervous system, J Comput Assist Tomogr 9(5):972–975,1985.
Gomori JM, Grossman RI, Goldberg HI, et al: Occult cerebrovascularmalformations: high-field MR imaging, Radiology 158:707–713, 1986.
Gomori JM, Grossman RI, Hackney DB, et al: Variable appearances of subacuteintracranial hematomas on high-field spin-echo MR, AJNR Am J Neuroradiol 8:1019–1026, 1987.
Gomori JM, Grossman RI, Yu-Ip C, et al: NMR relaxation times of blood:dependence on field strength, oxidation state, and cell integrity, J Comput AssistTomogr 11:684–690, 1987.
Gonzalez R, Schaefer P, Buonanno FS, et al: Diffusion-weighted MR imaging:diagnostic accuracy in patients imaged within 6 hours of stroke symptom,
Radiology 210(1):155–162, 1999.Grossman RI, Gomori JM, Goldberg HI, et al: MR imaging of hemorrhagic
conditions of the head and neck, Radiographics 8:441–453, 1988.Grossman RI, Kemp SS, Ip CY, et al: Importance of oxygenation in the appeara
of acute subarachnoid hemorrhage on high field magnetic resonance imaging, Acta Radiol 139:56–58, 1988.
Hackney DB, Atlas SW, Grossman RI, et al: Subacute intracranial hemorrhage:contribution of spin density to appearance on spin-echo MR images, Radiology 165:199–202, 1987.
Haley EC Jr, Kassell NF, Torner JC: The International Cooperative Study on theTiming of Aneurysm Surgery: the North American experience, Stroke 23:205–214,1992.
Hart RG, Easton DJ: Dissections, Stroke 16:925–927, 1985.Hecht-Leavitt C, Gomori JM, Grossman RI, et al: High field MRI of hemorrhag
cortical infarction, AJNR Am J Neuroradiol 7:581–586, 1986. Jacobs K, Moulin T, Bogousslavsky J, et al: The stroke syndrome of cortical ve
thrombosis, Neurology 47(2):376–382, 1996. Johnston S, Selvin S, Gress DR, et al: The burden, trends, and demographics of
mortality from subarachnoid hemorrhage, Neurology 50(5):1413–1418, 1998. Johnston S, Wilson C, Halbach VV, et al: Endovascular and surgical treatment of
unruptured cerebral aneurysms: comparison of risks, Ann Neurol 48(1):11–19, 2000. Joshi V, Pawel B, Connor E, et al: Arteriopathy in children with acquired immu
deficiency syndrome, Pediatr Pathol 7(3):261–275, 1987.Kassell NF, Torner JC, Haley EC Jr, et al: The International Cooperative Study on
the Timing of Aneurysm Surgery: part 1—overall management results, J Neurosurg 73:18–36, 1990.
Downloaded from ClinicalKey.com at Univ Gr T Popa Med & Pharmacy on February 28, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

8/18/2019 Vascular Diseases of the Brain
http://slidepdf.com/reader/full/vascular-diseases-of-the-brain 66/66
V ASCULAR D ISEASES OF THE B RAIN 169
Kassell NF, Torner JC, Jane JA, et al: The International Cooperative Study on theTiming of Aneurysm Surgery: part 2—surgical results, J Neurosurg 73:37–47,1990.
Koc Y, Gullu I, et al: Vascular involvement in Behçet’s disease, J Rheumatol 19(3):402–410, 1992.
Koeppen AH, Dentiger MP: Brain hemosiderin and superficial siderosis of thecentral nervous system, J Neuropathol Exp Neurol 47:249–270, 1988.
Kushner JM, Bressnman SB: The clinical manifestations of pontine hemorrhage, Neurology 35:637–643, 1985.
Lev M, Farkas J, Gemmete JJ, et al: Acute stroke: improved nonenhanced CTdetection—benefits of soft-copy interpretation by using variable window width
and center level settings, Radiology 213(1):150–155, 1999.Liem M, Gzesh D, Flanders AE, et al: MRI and angiographic diagnosis of lupuscerebral vasculitis, Neuroradiology 38(2):134–136, 1996.
Macchi PJ, Grossman RI, Gomori JM, et al: High field MR imaging of cerebralvenous thromboisis, J Comput Assist Tomogr 10:10–15, 1986.
Maldjian J, Listerud J, Moonis G, et al: Computing diffusion rates in T2-darkhematomas and areas of low T2 signal, AJNR Am J Neuroradiol 22(1):112–118,2001.
Marks MP, Lane B, Steinberg GK, et al: Hemorrhage in intracerebral arteriovenousmalformations: angiographic determinants, Radiology 176:807–813, 1990.
Mason WG, Latchaw RE, Yock DH: Spontaneous hemorrhage during cranialcomputed tomography, AJNR Am J Neuroradiol 1:266–268, 1980.
Matias-Guiu X, Alejo M, Sole T, et al: Cavernous angiomas of the cranial nerves, J Neurosurg 73:620–622, 1990.
Matsubara S, Manzia J, ter Brugge K, et al: Angiographic and clinicalcharacteristics of patients with cerebral arteriovenous malformations associatedwith hereditary hemorrhagic telangiectasia, AJNR Am J Neuroradiol 21(6):1016–1020, 2000.
Miyazawa N, Hashizume K, Uchida M, et al: Long-term followup of asymptomaticpatients with major artery occlusion: rate of symptomatic change and evaluationof cerebral hemodynamics, AJNR Am J Neuroradiol 22(2):243–247, 2001.
Morgenstern L, Hankins L, Grotta JC, et al: Anterior choroidal artery aneurysmand stroke, Neurology 47(4):1090–1092, 1996.
Norman D, Price D, Boyd D, et al: Quantitative aspects of computed tomographyof the blood and cerebrospinal fluid, Radiology 123:335–338, 1977.
North American Symptomatic Carotid Endarterectomy Trial Collaborators: Beneficialeffect of carotid endarterectomy in symptomatic patients with high-grade carotidstenosis, N Engl J Med 325:445–453, 1991.
Ostergaard L, Sorensen A, Chesler DA, et al: Combined diffusion-weighted andperfusion-weighted flow heterogeneity magnetic resonance imaging in acutestroke, Stroke 31(5):1097–1103, 2000.
Osumi A, Tien R, Felsberg GJ, et al: Cerebral amyloid angiopathy presenting as abrain mass, AJNR Am J Neuroradiol 16(4 Suppl):911–915, 1995.
Pantano P, Toni D, Caramia F, et al: Relationship between vascular enhancement,cerebral hemodynamics, and MR angiography in cases of acute s troke, AJNR Am
J Neuroradiol 22(2):255–260, 2001.Perl JN, Tkach J, Porras-Jimenez M, et al: Hemorrhage detected using MR
imaging in the setting of acute stroke: an in vivo model, AJNR Am J Neuroradiol 20(10):1863–1870, 1999.
Petty G, Engel A, Younge BR, et al: Retinocochleocerebral vasculopathy, Medicine 77(1):12–40, 1998.
Pomper M, Miller T, Stone JH, et al: CNS vasculitis in autoimmune disease: MRimaging findings and correlation with angiography, AJNR Am J Neuroradiol 20(1):75–85, 1999.
Provenzale J, Allen N: Neuroradiologic findings in polyareritis nodosa, AJNR Am J Neuroradiol 17(6):1119–1126, 1996.
Provenzale J, Sorensen A: Diffusion-weighted MR imaging in acute stroke:theoretic considerations and clinical applications, AJR Am J Roentgenol 173(6):1459–1467, 1999.
Reneman L, Habraken J, Majoie CBL, et al: MDMA (Ecstasy) and its associationwith cerebrovascular accidents: preliminary findings, AJNR Am J Neuroradiol 21(6):1001–1007, 2000.
Requena I, Arias M, Lopez-Ibor L, et al: Cavernomas of the central nervoussystem: clinical and neuroimaging manifestations in 47 patients, J Neurol
Neurosurg Psychiatry 54:590–594, 1991.Rigamonti D, Spetzler RF, Medina J, et al: Cerebral venous malformations, J Neurosurg
73:560–564, 1990.
Rinne J, Hernesniemi J, Puranen M, et al: Multiple intracranial aneurysmsdefined population: prospective angiographic and clinical study, Neurosurgery 35(5):803–808, 1994.
Rippe DJ, Boyko OB, Spritzer CE, et al: Demonstration of dural sinus occthe use of NM angiography, AJNR Am J Neuroradiol 11:199–201, 1990.
Roda JM, Alvarez F, Isla A, et al: Thalamic cavernous malformation, J Neurosurg 72:647–649, 1990.
Salgado AV, Furlan AJ, Keys TF: Mycotic aneurysm, subarachnoid hemorand indications for cerebral angiography in infective endocarditis, Stroke 18:1057–1060, 1987.
Schievink W: Spontaneous dissection of the carotid and verebral arteries N Engl
J Med 22:898–906, 2001.Schievink W, Wijdicks E, Parisi JE, et al: Sudden death from aneurysmalsubarachnoid hemorrhage, Neurology 45(5):871–874, 1995.
Scott WR, New PFJ, Davis KR, et al: Computerized axial tomography ofintracerebral and intraventricular hemorrhage, Radiology 112:73–80, 1974.
Seeger JF, Gabrielsen TO, Giannotta SL, et al: Carotid-cavernous sinus fisand venous thrombosis, AJNR Am J Neuroradiol 1:141–148, 1980.
Shrier D, Tanaka H, Numaguchi Y, et al: CT angiography in the evaluationacute stroke, AJNR Am J Neuroradiol 18(6):1011–1020, 1997.
Sigal R, Krief O, Houtteville JP, et al: Occult cerebrovascular malformatiofollow-up with MR imaging, Radiology 176:815–819, 1990.
Singer M, Chong J, et al: Diffusion-weighted MRI in acute subcortical inf Stroke 29(1):133–136, 1998.
Som PM, Patel S, Nakagawa H, et al: The iron rim sign, J Comput Assist Tomogr 3:109–112, 1979.
Sorensen A, Copen W, Østergaard L, et al: Hyperacute stroke: simultaneoumeasurement of relative cerebral blood volume, relative cerebral blood fmean tissue transit time, Radiology 210(2):519–527, 1999.
Spetzler RF, Martin NA: A proposed grading system for arteriovenousmalformations, J Neurosurg 65:476–483, 1986.
Storen E, Wijdicks E, Crum BA, et al: Moyamoya-like vasculopathy fromdependency, AJNR Am J Neuroradiol 21(6):1008–1010, 2000.
Suzuki S, Inoue T, Haga S, et al: Stroke due to a fusiform aneurysm of thevertebral artery: case report, Neuroradiology 40(1):19–22, 1998.
Thijs V, Lansberg M, Beaulieu C, et al: Is early ischemic lesion volumdiffusion-weighted imaging an independent predictor of stroke outcA multivariable analysis, Stroke 31(11):2597–2602, 2000.
Thulborn KR, Brady TJ: Iron in magnetic resonance imaging of cerebralhemorrhage, Magn Res Q 5:23–38, 1989.
Thulborn KR, Sorensen AG, Kowall NW, et al: The role of ferritin andhemosiderin in the MR appearance of cerebral hemorrhage: a histopathobiochemical study in rats, AJNR Am J Neuroradiol 11:291–297, 1990.
Thulborn KR, Waterton JC, Matthews PM, et al: Oxygenation dependencetransverse relaxation time of water protons in whole blood at high field, Biochem
Biophys Acta 714:265–270, 1982.Tsuruda JS, Shimakawa A, Pelc NJ, et al: Dural sinus occlusion: evaluation w
phase-sensitive gradient-echo MR imaging, AJNR Am J Neuroradiol 12:481–488,1991.
Ulmer JL, Elster AD: Physiologic mechanisms underlying the delayed del AJNR Am J Neuroradiol 12:647–650, 1991.
Wang P, Barker P, Wityk RJ, et al: Diffusion-negative stroke: a report of tw AJNR Am J Neuroradiol 20(10):1876–1880, 1999.
Weingarted K, Zimmerman RD, Deo-Narine V, et al: MR imaging of acuteintracranial hemorrhage: findings on sequential spin-echo and gradient-eimages in a dog model, AJNR Am J Neuroradiol 12:457–467, 1991.
White P, Wardlaw J, Easton V, et al: Can noninvasive imaging accurately dintracranial aneurysms? A systematic review, Radiology 217(2):361–370, 2000
Yousem DM, Balakrishnan J, Debrun GM, et al: Hyperintense thrombus on GRimages: potential pitfall in flow evaluation, AJNR Am J Neuroradiol 11:51–58, 1990.
Yuh WTC, Crain MR, Loes DJ, et al: Cerebral ischemia: evaluation with cenhanced MR imaging, AJNR Am J Neuroradiol 12:631–639, 1991.
Yuh W, Ueda T, Maley JE, et al: Diagnosis of microvasculopathy in CNS vasvalue of perfusion and diffusion imaging, J Magn Reson Imaging 10(3):310–313, 1
Zimmerman RD, Leeds NE, Naidich TP: Ring blush associated with intrachematoma, Radiology 122:707–711, 1977.
Zimmerman RS, Spetzler RF, Lee SK, et al: Cavernous malformations of tstem, J Neurosurg 75:32–39, 1991.