Embed Size (px)
Citation preview
Case Report
Vascular access for chronic hemodialysisin a patient with epidermolysis bullosa
dystrophica Hallopeau-Siemens
Sanja SAKAN,1 Nikolina BASIC-JUKIC,2 Boris TOMASEVIC,1 Petar KES,2
Daniela BANDIC PAVLOVIC,1 Mladen PERIC1
1Department of Anesthesiology, Reanimatology and Intensive Care, University Hospital Center, Zagreb,Croatia; 2Department of Nephrology, Arterial Hypertension and Dialysis, University Hospital Center
Zagreb, Zagreb, Croatia
AbstractEpidermolysis bullosa is a rare genetic hereditary disease characterized with mechanobullousdermatosis. Except cutaneous, these patients have various extracutaneous manifestations andsome types of epidermolysis bullosa comprise almost all organ systems. Because of prolonged lifespan, chronic renal insufficiency has become an important cause of morbidity and death in thesepatients. Establishment of functional vascular dialysis access is a great challenge for both thedoctors and the patients. Multidisciplinary approach is essential. We present a case of successfulestablishment of dialysis access via Tesio catheter in a young woman suffering from epidermolysisbullosa dystrophica Hallopeau-Siemens and end-stage renal disease. Since then, the Tesio catheterinserted via the right internal jugular vein has been the functional mean of dialysis. The patient wasgiven the opportunity to lead a quality and active life in spite of disabling disease. Several cases ofsuccessful dialysis access establishment with dialysis catheters via central veins have beenreported. We report the successful establishment of long-term dialysis access via Tesio catheter andsuggest this approach as ideal for these patients. This is the first report dealing with vascular accessin this group of patients.
Key words: Catheter, end-stage renal disease, epidermolysis bullosa dystrophica, renal dialysis
INTRODUCTION
Epidermolysis bullosa dystrophica Hallopeau-Siemens(EBDHS) is an autosomal recessive inherited type ofmechanobullous dermatosis which is caused by mutationsof the gene COL7A1.1 Recently, according to the revised
classification system, EBDHS has changed the name tosevere generalized recessive dystrophic epidermolysisbullosa to emphasize the clinical picture of the subtype.2
The consequence of mutations is lack or dysfunctionalstructure of collagen type VII which is anchoring fibrilsbetween lamina lucida of the basement membraneand upper papillary layer of dermis. The result isdermal blistering.2–6 Epidermolysis bullosa dystrophicaHallopeau-Siemens is the most severe, generalized type ofdystrophic epidermolysis bullosa group which begins atbirth with spontaneous generalized blistering of the skinand mucosa.2,3,6 The blisters and vesicles heal with atro-phic scars and milia formation. Possible extracutaneous
Correspondence to: S. Sakan, MD, Department ofAnesthesiology, Reanimatology and Intensive Care,University Hospital Center Zagreb, Kišpaticeva 12, 10000Zagreb, Croatia. E-mail: [email protected]: None.Financial disclosure: None.
Hemodialysis International 2012; ••:••–••
© 2012 The AuthorsHemodialysis International © 2012 International Society for HemodialysisDOI:10.1111/j.1542-4758.2012.00699.x 1
manifestations are dystrophic or absent nails, sparse scalphair or alopecia, excessive dental caries, microstomia, oralcavity ulcers, fixation of the tongue to the floor of the oralcavity, pseudosyndactylia, syndactylia, and deformities ofthe hands and feet.2,3 The epithelial surface of respiratory,gastrointestinal, genitourinary, and ocular system is alsoaffected with blistering.3 Bleeding from lesions of the skinand mucosa happens frequently. These patients areusually anemic, cahectic, and growth retarded with diffi-culty moving, in contractures. Epidermolysis bullosa dys-trophica Hallopeau-Siemens is often complicated withdevelopment of chronic renal insufficiency which is one ofthe important causes of early death of these patients.7 Themain problem is establishment of vascular access for dialy-sis. To the best of our knowledge, we present a first case ofTesio catheter for permanent dialysis vascular access inpatient with EBDHS.
CASE REPORT
A 32-year-old Caucasian woman suffering from EBDHSwas urgently admitted to the Department of Dialysis dueto deterioration of chronic renal insufficiency associatedwith threatening hyperkalemia (7,4 mEq/L), nausea, vom-iting, hypervolemia, and febrility. She was diagnosed withEBDHS at birth, and has been under regular dermatologyfollow-up due to extensive lesions of the skin and mucosa.Owing to frequent skin infections, she was treated empiri-cally with gentamycin and azithromycin. Dysphagiacaused by stenotic esophageal lesions demanded frequentendoscopic balloon dilatations. Also, she underwent sur-gical excision of the squamous cell carcinoma from thesacral area 3 years ago and from the left foot 2 years ago.She suffered from osteopenia, anemia, adrenal glandinsufficiency, hypothyreosis, and hemorrhagic diathesiswith frequent epistaxis and bleeding from the skin ero-sions. Her drug therapy included hydrocortisone, levothy-roxine, pantoprazole, sodium bicarbonate, calcitriol,calcium carbonate, and furosemide.
Five years ago, she was diagnosed with chronic renalinsufficiency. She was under the regular nephrologicalfollow-up. One year ago, she reached the end-stage renaldisease. Peritoneal dialysis was excluded because of ahigh risk for development of the catheter exit-site infec-tion with subsequent peritonitis, while there was nohealthy part of skin on the abdominal wall for catheterinsertion. Another contraindication was poor patientcompliance due to deformities of the hands. Hemodialy-sis had been chosen for replacement of renal functiondespite difficult venous access, patient skin changes,and contractures. Hickman catheter was inserted via the
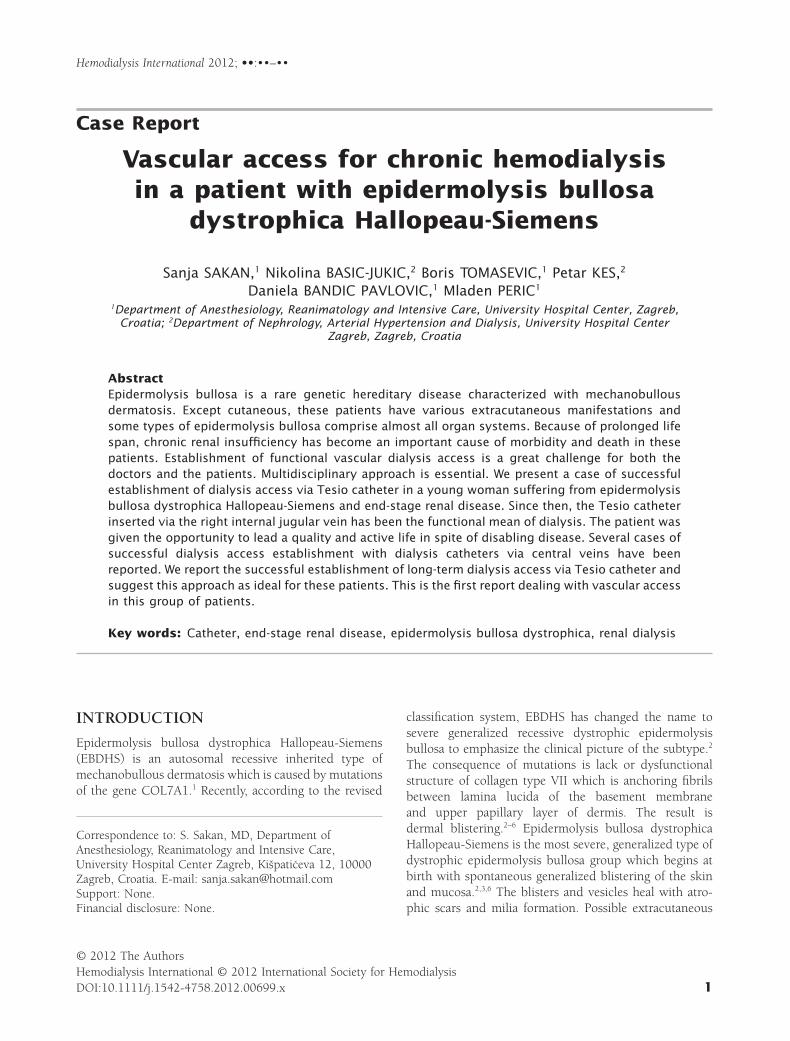
left subclavian vein. Regular hemodialysis three timesa week was started. From that point, she was constantlysubfebrile with slightly elevated inflammation parame-ters and skin infection around the Hickman catheterexit site (Figure 1). From the swab of the intravascularHickman catheter Staphylococcus aureus sensitive to van-comycin was isolated. The antibiotic therapy was started,and, thence, she was on continuous antibiotic therapywith vancomycin once a week. Two months ago, theHickman catheter in the left subclavian vein becameafunctional due to thrombosis, and was replaced with thenew one. She complained of discomfort in the left shoul-der and impaired motility of the arm due to the Hickmancatheter.
At admission in the hospital, she was in verbal contact,conscious, cahectic, with pale skin and mucosa, in con-tractures, and febrile with axillary temperature 38.6°C.Almost all skin was erythematous with hemorrhagiccrusts, blisters, and erosions except the small sternal skinarea. She had microstomia, upper teeth were missing, andher tongue was fixated to the floor of the oral cavity. Scalphair was sparse. Deformities and syndactylia of the fistsand feet with amputated fingers were seen. Muscles wereatrophic and extremities were slightly edematous. Liverand spleen border was palpable. She was hemodyna-mically and respiratory stable. Blood pressure was 120/80 mmHg, pulse 100/min. Heart and lungs auscultatoryshowed no pathological findings. Her electrocardio-gram demonstrated tachycardia, irregular heartbeats,and pointed T waves in all precordial leads. Laboratoryresults revealed anemia (E 2.9 ¥ 106/mL [2.9 ¥ 109/L],
Figure 1 Afunctional Hickman catheter inserted via the leftsubclavian vein with the exit site skin infection around thecatheter.
Sakan et al.
Hemodialysis International 2012; ••:••–••2

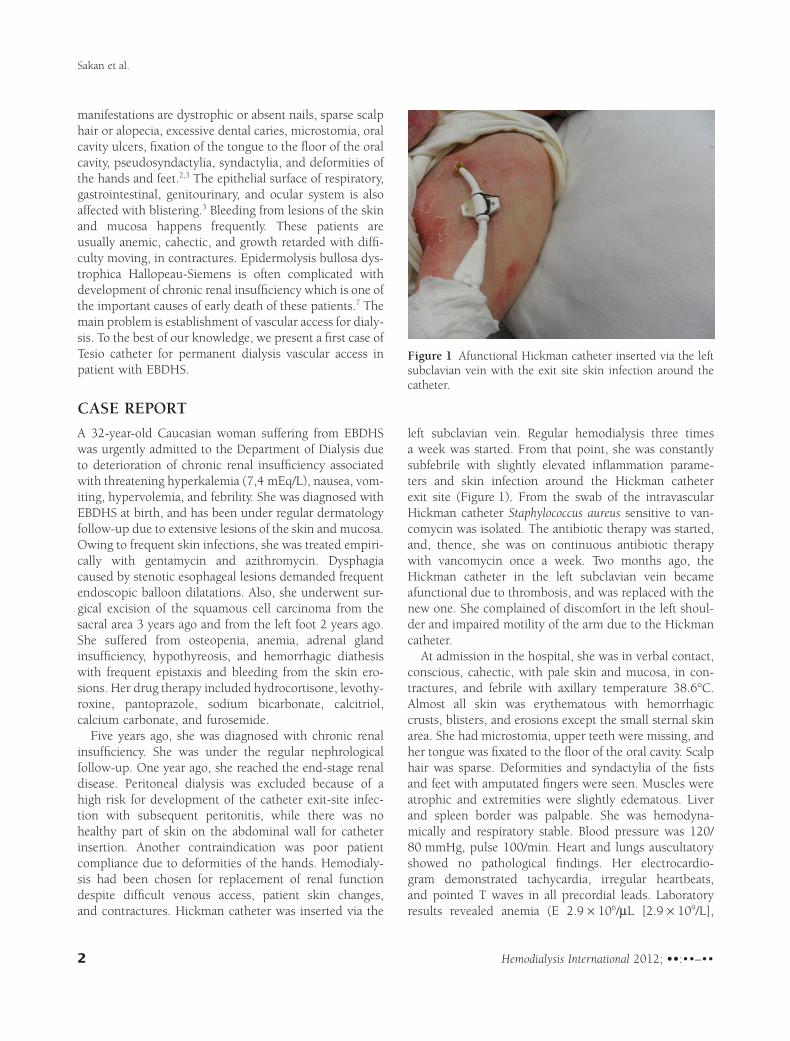
Hb 8.3 g/dL [83 g/L], Hct 26%), elevated inflammatoryparameters (L 13.1 ¥ 103/mL [13.1 ¥ 109 L], C-reactiveprotein 10.3 mg/dL [103 mg/L], ESR 105 mm/h), pro-longed activated partial thromboplastin time (43.2 s), andelevated fibrinogen (790 mg/dL (23.2 mmol/L)), elevatedserum urea nitrogen (68.9 mg/dL (24.6 mmol/L)), andcreatinine (8.2 mg/dL (628 mmol/L)). Hyperkalemia (K7.4 mEq/L), hyperphosphatemia (P 36 mg/dL [2.0 mmol/L]), hypocalcemia (Ca2++ 1.48 mEq/L [0.74 mmol/L]),sideropenia (Fe 27.9 mg/dL [5 mmol/L]), and hyper-ferritinemia (ferritin 1404 ng/mL [1404 mg/L]) wererecorded. Because of the threatening hyperkalemiaand hypervolemia, urgent hemodialysis was essential.However, the replaced 2 months ago Hickman catheter viathe left subclavian vein again became afunctional probablydue to thrombosis. Meantime, the staff was educatedand skilled for Tesio catheter insertion. Due to patient’sanxiety and discomfort, procedure was done in intrave-nous sedation with propofol and sufentanyl and localinfiltration of 1% lidocaine in the area of the right jugularfossa. The patient was spontaneously breathing during theprocedure. The intravenous line used for anesthetic appli-cation was placed on the left forearm and fixated with thespecial self-adherent soft silicone foam dressing (MepilexBoreder Lite with Safetac Technology, Moelnlycke HealthCare AB, Goetborg, Sweden). During the procedure,pulse oximetry on the ear lobe, electrocardiogram, andnoninvasive blood pressure monitoring were performed.Owing to skin fragility, applied monitoring requiredspecial precautions to avoid any skin trauma. Alreadymentioned special self-adherent soft silicone foam dress-ing was interposed between the electrocardiogram elec-trodes and pulse oximetry probe, and the skin.Importantly, soft gauze was wrapped around the limbbeneath the blood pressure cuff. Also, while the patientwas lying on the operating table, pressure points wereprotected with the soft gauze. Tesio catheter was insertedvia the right internal jugular vein uneventfully. Theexternal part of the Tesio catheter was subcutaneouslytunneled to the normal sternal skin area to reduce infec-tious complications, and the catheter was also securedwith special self-adherent soft silicone foam dressing(Figure 2). The Hickman catheter was removed. Theempiric antibiotic therapy with vancomycin was started.From the tip of the Hickman catheter, S. aureus was iso-lated sensitive to vancomycin. Hemocultures were sterile.Gradually, her clinical condition improved, and inflam-matory and other laboratory parameters normalized. Shewas discharged from the hospital after 10 days, and, sincethat time, the Tesio catheter has still been her functionalvascular access for dialysis.
DISCUSSION
Epidermolysis bullosa dystrophica Hallopeau-Siemens isan autosomal recessive hereditary dermatosis which com-prises almost all organ systems since birth. Chronic renalinsufficiency according to studies is the second cause ofdeath in these patients after squamous cell carcinoma.7
The cumulative risk of death is about 12.3% until the ageof 35.7 Also, it is relevant to emphasize that many patientsdie from dilatative cardiomyopathy.8 Chronic renal insuf-ficiency is usually a consequence of secondary amyloido-sis, IgA nephropathy, postinfectious glomerulonephritis,and obstructive uropathy.7–9 Chronic inflammatory syn-drome because of recurrent skin, respiratory and geni-tourinary infections, mechanical obstructive uropathy,and permanent intravascular hypovolemia owing todehydration, dysphagia, vomiting, and hypoalbumine-mia are probably responsible mechanisms for renalimpairment.9–11 Patient in this case also had the men-tioned mechanisms. However, when the chronic renalinsufficiency was diagnosed, our patient, even after broadexplanation of the procedure, refused to do renal biopsyto exclude the cause. Moreover, diuretic therapy and fre-quent use of aminoglycoside antibiotics due to skin infec-tions contributed to renal impairment. Dialysis access inthese patients with the end-stage renal disease is the mainproblem. Skin lesions and their predisposition to infec-tions are major limitation factors especially for implanta-tion of peritoneal dialysis catheter. Another limitationfactor is difficult intravenous access due to skin changesand contractures which makes arteriovenous fistulaestablishment and its future use impossible.12 Presently,
Figure 2 The external part of the Tesio catheter inserted viathe right internal jugular vein subcutaneously tunneled to thenormal sternal skin area.
Hemodialysis in epidermolysis bullosa
Hemodialysis International 2012; ••:••–•• 3

hemodialysis via tunneled dialysis catheter inserted in oneof the central veins is the best solution.13 Nevertheless,to prevent many complications, we should always lookfor the clear skin area for the external part of the Tesiocatheter as it was sternal skin area in our case. Moreover,due to extreme skin and mucosa fragility, these patientsusually require anesthesia for almost every procedurewhich is painful for them. However, special precautionsmust be taken to avoid new blisters formation when usingmonitoring and securing devices.14,15 Self-adherent softsilicone foam dressing products are preferred for fixationof the catheters and other devices to minimize the skintrauma.16 To conclude, every decision about these patientsshould be multidisciplinary. Chronic renal insufficiencymay have greater incidence than squamous cell carcinomain these patients, but they probably do not live longenough to develop it. In addition, patients suffering fromepidermolysis bullosa should be treated in specializedcenters. In respect this incapacitating disease they shouldhave opportunity to lead quality and active life.
Manuscript received January 2012; revised March 2012.
REFERENCES1 Varki R, Sadowski S, Uitto J, Pfendner E. Epidermolysis
bullosa. II. Type VII collagen mutations and phenotype/genotype correlations in the dystrophic subtypes. J MedGenet. 2007; 44:181–192.
2 Fine JD, Eady RAJ, Bauer EA, et al. The classification ofinherited epidermolysis bullosa (EB): Report of the ThirdInternational Consensus Meeting on Diagnosis and Clas-sification of EB. J Am Acad Dermatol. 2008; 58:931–950.
3 Fine JD, Mellerio JE. Extracutaneous manifestations andcomplications of inherited epidermolysis bullosa. Part I.Epithelial associated tissues. J Am Acad Dermatol. 2009;61:367–384.
4 Ducret F, Pointet P, Turc-Baron C, Vernin G. Kidneydisease in dystrophic epidermolysis bullosa: Case report.Nephrol Ther. 2008; 4:187–195.
5 Varki R, Sadowski S, Pfendner E, Uitto J. Epidermolysisbullosa. I. Molecular genetics of the junctional and
hemidesmosomal variants. J Med Genet. 2006; 43:641–652.
6 Kihiczak NI, Papadopoulos AJ, Schwartz RA, JannigerCK. Epidermolysis bullosa hereditaria simplex. Casereport. Acta Dermatovenerol Alp Panonica Adriat. 2001;10:24–29.
7 Fine JD, Johnson LB, Weiner M, et al. National epider-molysis bullosa registry. Inherited epidermolysis bullosaand the risk of death from renal disease: Experience ofthe national epidermolysis bullosa registry. Am J KidneyDis. 2004; 44:651–660.
8 Sidwell RV, Yates R, Atherton D. Dilated cardiomyopathyin dystrophic epidermolysis bullosa. Arch Dis Child.2000; 83:59–63.
9 Kawasaki Y, Isome M, Takamo K, et al. IgA nephropathyin a patient with dominant dystrophic epidermolysisbullosa. Tohoku J Exp Med. 2008; 214:297–301.
10 Farhi D, Ingen-Housz-Oro S, Ducret F, et al. Recessivedystrophic epidermolysis bullosa (Hallopeau-Siemens)with IgA nephropathy: 4 cases. Ann Dermatol Venereol.2004; 131:963–967.
11 Mann JF, Zeier M, Zilow E, et al. The spectrum of renalinvolvement in epidermolysis bullosa dystrophicahereditaria: Report of two cases. Am J Kidney Dis. 1988;11:437–441.
12 Baloch MS, Fitzwilliams B, Mellerio J, et al. Anaesthesticmanagement of two different modes of delivery inpatients with dystrophic epidermolysis bullosa. IntJ Obstet Anesth. 2008; 17:153–158.
13 Tammaro F, Calabrese R, Aceto G, et al. End-stage renaldisease secondary to IgA nephropathy in recessive dys-trophic epidermolysis bullosa: A case report. PediatrNephrol. 2008; 23:141–144.
14 Ames WA, Mayou BJ, Williams K. Anaesthetic manage-ment of epidermolysis bullosa. Br J Anaesth. 1999;82:746–751.
15 Gottschalk A, Venherm S, Vowinkel T. Anesthesia forballoon dilatation of esophageal strictures in childrenwith epidermolysis bullosa dystrophica: From intubationto sedation. Curr Opin Anaesthesiol. 2010; 23:518–522.
16 Meola S, Olivieri M, Mirabile C, Mastrandrea P.Anesthetic management for right upper extremityamputation due to recidivans cutaneous carcinomaand acute postoperative pain control in patients affectedby epidermolysis bullosa. Minerva Anestesiol. 2010;76:144–147.
Sakan et al.
Hemodialysis International 2012; ••:••–••4





























