Embed Size (px)
Citation preview
American Journal of Transplantation 2012; 12: 2974–2985Wiley Periodicals Inc.
C© Copyright 2012 The American Society of Transplantationand the American Society of Transplant Surgeons
doi: 10.1111/j.1600-6143.2012.04273.x
Varicella-Zoster Immunization in Pediatric LiverTransplant Recipients: Safe and Immunogenic
K. M. Posfay-Barbea,*, L. F. Pitteta,b, C. Sottasa,b,
S. Grilletb, B. E. Wildhaberc, M. Rodrigueza,
L. Kaiserd, D. C. Bellie, V. A. McLine
and C. A. Siegrista,b
aDepartment of Pediatrics, Division of General Pediatrics,Children’s Hospital of Geneva, University Hospitals ofGeneva, SwitzerlandbDepartments of Pathology-Immunology and Pediatrics,Centre for Vaccinology and Neonatal Immunology,University of Geneva, SwitzerlandcDepartment of Pediatrics, Division of Pediatric Surgery,Children’s Hospital of Geneva, University Hospitals ofGeneva, SwitzerlanddLaboratory of Virology, Department of Genetics andLaboratory Medicine and Department of MedicalSpecialities, University Hospitals of Geneva & Faculty ofMedicine, University of Geneva, SwitzerlandeDepartment of Pediatrics, Division of PediatricGastroenterology and Transplantation, Children’s Hospitalof Geneva, University Hospitals of Geneva, Switzerland*Corresponding author: Klara M. Posfay-Barbe,[email protected]
Varicella can have a severe course in immunosup-pressed patients. Although prevention is fundamen-tal, live-attenuated varicella-zoster (VZV) vaccine isnot currently recommended in transplant recipients.Our aims were to (1) evaluate VZV immunity in pe-diatric liver transplant (LT) recipients; (2) immunize(two doses) seronegative patients post-LT; (3) moni-tor vaccine safety, (4) assess B and T cell vaccine re-sponses. All patients followed at the Swiss NationalPediatric LT Center were approached and 77/79 (97.5%)were enrolled (median age 7.8 years). Vaccine safetywas monitored by standardized diary cards and phonecalls. VZV-specific serology and CD4+ T cells were as-sessed before and after immunization. Thirty-nine pa-tients (51.1%) were seronegative including 14 childrenimmunized pre-LT. Thirty-six of 39 seronegative pa-tients were immunized post-LT (median 3.0 years postLT). Local (54.8%) and systemic (64.5%) reactions weremild and transient. The frequency of VZV-specific CD4+T cells and antibody titers increased significantly (re-spectively from 0.085% to 0.16%, p = 0.04 and 21.0to 1134.5 IU/L, p < 0.001). All children reached sero-protective titers and 31/32 (97%) patients assessed re-mained seroprotected at follow-up (median 1.7 years).No breakthrough disease was reported during follow-up (median 4.1 years). Thereby, VZV vaccine appears to
be safe, immunogenic and provide protection againstdisease in pediatric LT patients.
Key words: Child, enzyme-linked immunosorbent as-say, humoral, immunity, immunosuppression, livertransplantation, T-lymphocytes, Varicella zoster virus,vaccination
Abbreviations: CNS, central nervous system; ELISA,enzyme-linked immunosorbent assay; HIV, human im-munodeficiency virus; IFN-gamma, interferon-gamma;IQR, interquartile range; LT, liver transplant; VZV,varicella-zoster virus; VZV-gp, varicella-zoster viruslectin affinity purified glycoprotein.
Received 12 March 2012, revised 05 July 2012 andaccepted for publication 08 July 2012
Introduction
Varicella is a common acute disease caused by varicella-zoster virus (VZV) (1–2). It is highly contagious with sec-ondary attack rates greater than 85% among susceptiblesubjects (3–4). The clinical course of disease is generallymild in previously healthy children (2). The course of dis-ease is more severe, prolonged and with higher complica-tion rates in immunosuppressed patients with leukemia,human immunodeficiency virus (HIV), or transplant recip-ients (2,5–6). The most feared complications include sec-ondary bacterial infections of skin lesions, severe dehy-dration, pneumonia, hepatitis and central nervous system(CNS) involvement. Untreated varicella in immunocompro-mised persons could lead to death in up to 7% of patients(5). In many centers, aggressive prophylaxis and treatmentare used to prevent complications and deaths in seronega-tive transplant recipients exposed to VZV in the community(7–8). These patients thus require hospital admission, di-agnostic testing and costly medical interventions.
Varicella can be prevented by vaccination, and hence israrer in countries where VZV immunization is part of theroutine immunization program. However, even in theselower risk countries, exposure to VZV happens: preven-tion is still essential for individuals at high risk for se-vere disease. In healthy children, vaccine efficacy is about70–90% against chickenpox and 95–100% against se-vere disease (2,9–10). VZV vaccine triggers both humoraland cell-mediated responses, which both contribute to
2974

VZV Vaccination in Pediatric LT Recipients
protection (11). Correlations have been established be-tween vaccine-induced antibody responses and protection(12–15). Healthy individuals however usually resist infec-tion after vaccine-induced antibodies have become unde-tectable, suggesting a protective function for CD4+ T cellresponses. Positive anti-VZV antibodies may thus essen-tially be a surrogate of a protective cellular immunity (16).
The VZV vaccine is a live-attenuated vaccine currently con-traindicated in immunosuppressed patients because of thefear that immunosuppression may result into enhancedviral replication and severe disease, and the belief thatimmunosuppressed patients would fail to mount protec-tive responses (17). The recommendation to elicit VZV im-munity prior to the onset of immunosuppression (18) ishowever not always possible, e.g. when organ transplan-tation is required in early infancy. In countries without awell-implemented routine VZV immunization policy, manychildren are seronegative at time of organ transplant (19).They are exposed to natural disease in the community,and recall of their VZV history for a better risk estimationis often difficult. Finally, it is observed that recipients mayhave waning immunity to vaccines both before and aftersolid-organ transplantation (18).
This observational prospective cohort study’s aims wereto evaluate the VZV immunity of pediatric orthotopic livertransplant (LT) recipients, to immunize seronegative pa-tients regardless of their past VZV history, to monitor vac-cine safety and to assess B and T cell immunogenicity inthis population at risk of VZV complication.
Materials and Methods
Patients
All pediatric LT recipients who were at least 1 year after transplantation,at least 2 months after an episode of acute rejection, and followed at theSwiss National Reference LT Center (University Hospitals of Geneva) wereapproached to participate in the study. After obtaining written consent fromthe parents and the patient when possible, medical records were reviewedto retrieve all significant medical history and varicella-related events. Vacci-nation records were obtained, and parents and physicians were interviewedfor varicella-related history (exposure, past disease, complications, treat-ment and vaccination). Recent (<6 months) screening VZV serologies wereused to identify seronegative children, to whom VZV immunization wasrecommended at the next medical visit, regardless of their VZV disease orimmunization history.
VZV vaccination
LT recipients, ≥12 months old, with anti-VZV gp antibodies <50 IU/L wereoffered two standard intramuscular doses of a live attenuated VZV vac-cine (Varilrix R©, GlaxoSmithKline Biologicals SA, Rixensart, Belgium) given2 months apart. Inclusion criteria for immunization included (1) to be on lowimmunosuppressive therapy, defined as <2 mg/kg/day of steroids and <0.3mg/kg/day of tacrolimus (with levels <8 ng/mL for more than 1 month), and(2) to have a total lymphocyte count ≥750 cells/lL at time of immuniza-tion. Temporary exclusion criteria for vaccination were (1) known recent(4 weeks) exposure to wild type varicella; (2) intravenous polyclonal im-munoglobulins in the last 5 months; (3) antiviral agents during the preced-
ing 4 weeks; (4) febrile illness (>38.5◦C) in the preceding 72 h; (5) aspirintherapy; (6) any other live vaccinations in the last 4 weeks; (7) pregnancy.
Safety and immunological monitoring
Parents evaluated—using a standardized diary card—local and systemic re-actions to the vaccines at weeks 1, 2, 4, 6 and 8 after each immunization.Parents were contacted by phone weekly for 2 weeks and subsequentlyevery other week until week 8 after each vaccination to identify poten-tial adverse events. Physicians in charge of these children outside of ourinstitution were informed of the study and received instructions on surveil-lance and treatment options in the case of adverse events or breakthroughvaricella. The safety primary outcome was the nonoccurrence of seriousadverse events between enrollment and 12 months after the last vaccinedose.
The effectiveness outcome was the duration of the disease-free period fromimmunization to onset of breakthrough VZV-related disease. VZV-specificantibody and interferon-gamma (IFN-gamma) production by VZV-specific Tcells were measured before and after the second vaccine dose. A third vac-cine dose was offered if anti-VZV antibodies remained < 50 IU/L, the puta-tive protective threshold (see below), followed by repeat serology. Anti-VZVtiters were subsequently quantified at each medical visit to our referencecenter. The primary immunogenicity endpoints were defined as reachingthe putative protection (antibodies) or detection (T cells) thresholds afterimmunization.
VZV serology
To detect even low anti-VZV IgG titers, we used an enzyme-linked im-munosorbent assay (ELISA)-based assay using the lectin affinity-purifiedglycoprotein (VZV-gp) from normal human dermal fibroblasts (EastCoastBio R©, North Berwick, Maine) (12). A low initial serum dilution (1:4) wasused to further improve assay sensitivity. Our adapted in-house assay wasvalidated using sera from immune and nonimmune (12-month-old infantswith no VZV history) individuals tested in our routine laboratory, and accred-ited according to Good Laboratory Practice guidelines. Intraassay variabilitywas 4.5% and interassay variability was 7.9%. Overall variability was 12%,yielding satisfactory results (20). A standard serum generated by Merck R©(Whitehouse Station, NJ, USA) during vaccine efficacy studies and corre-lating with protection at a level of 5 gp U/mL (12) (generous gift of FlorianSchroedel, Merck R©) was used to define the corresponding threshold of theWorld Health Organization (WHO) international standard (W1044, NIBSC,Potters Bar, UK). A value of 50 IU/L, correlating with 5 gp U/mL of theMerck R© serum, was set as a marker for vaccine-induced protective effi-cacy. Analyses were performed sequentially.
VZV-specific CD4+ T cells
To detect the production of IFN-gamma by CD4+ T cells, we used a modi-fied Miltenyi’s Interferon-gamma (IFN-gamma) secretion assay R© (MiltenyiBiotec GmbH, Bergisch Gladbach, Germany) relying on a dual antibody con-struct. Fresh, heparinized whole-blood samples (1 mL) were diluted 1/4in RPMI 5% AB serum and incubated for 24 h with VZV-gp (10 lg/mL).CD28 and CD49d antibodies (BD Biosciences, Erembodegem, Belgium)(0.5 lg/mL each) were added to provide costimulation signals, as de-scribed (20). Negative (CD28/CD49d antibodies without VZV-gp) and posi-tive (tetanus toxoid (TT) antigen) controls were included in each assay (21–22). Cells were stained with anti-CD4+ (BD Biosciences, Erembodegem,Belgium) monoclonal antibodies prior to analysis with fluorescent-activatedcell sorting (BD FACSArray Bioanalyzer System R©, BD Biosciences, Erem-bodegem, Belgium) and the Flowjo R© (Tree Star Inc., Ashland, OR, USA)flow cytometry analysis software. Intraassay variability was 12% for VZVand 18% for TT. Analyses were performed sequentially. The cut-off valueof VZV-specific IFN-gamma secreting cells was experimentally set at 0.1%based on the mean of negative controls (<0.05%).
American Journal of Transplantation 2012; 12: 2974–2985 2975
Posfay-Barbe et al.
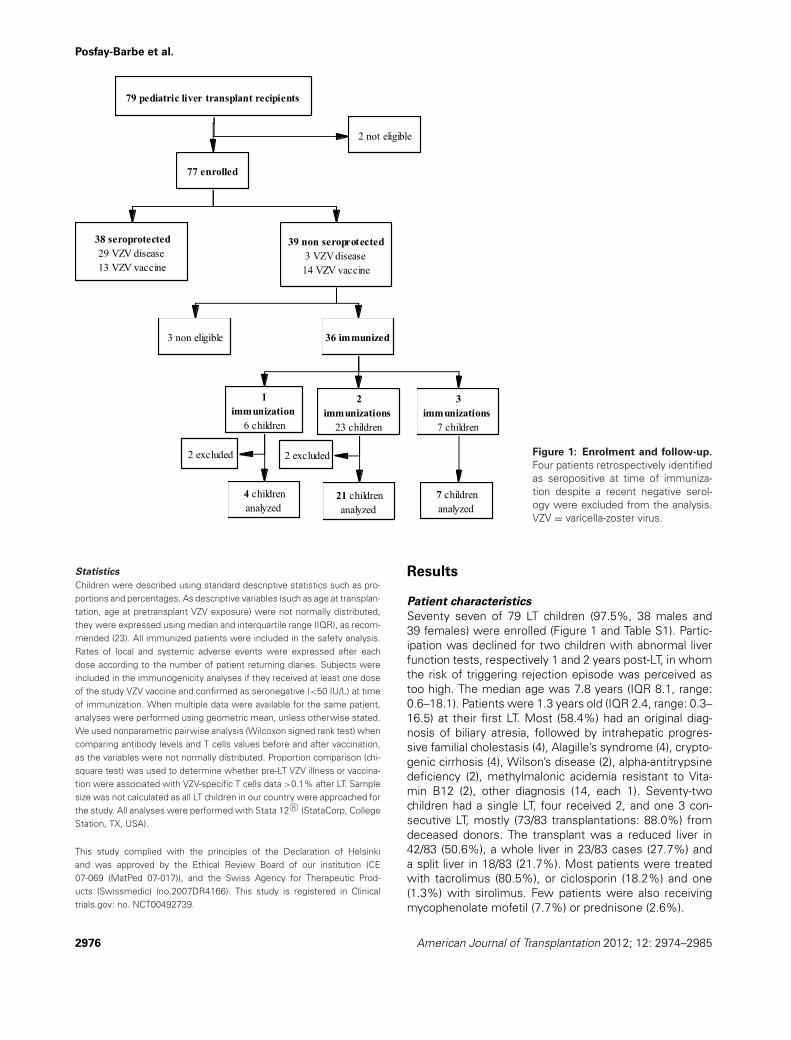
Figure 1: Enrolment and follow-up.
Four patients retrospectively identifiedas seropositive at time of immuniza-tion despite a recent negative serol-ogy were excluded from the analysis.VZV = varicella-zoster virus.
Statistics
Children were described using standard descriptive statistics such as pro-portions and percentages. As descriptive variables (such as age at transplan-tation, age at pretransplant VZV exposure) were not normally distributed,they were expressed using median and interquartile range (IQR), as recom-mended (23). All immunized patients were included in the safety analysis.Rates of local and systemic adverse events were expressed after eachdose according to the number of patient returning diaries. Subjects wereincluded in the immunogenicity analyses if they received at least one doseof the study VZV vaccine and confirmed as seronegative (<50 IU/L) at timeof immunization. When multiple data were available for the same patient,analyses were performed using geometric mean, unless otherwise stated.We used nonparametric pairwise analysis (Wilcoxon signed rank test) whencomparing antibody levels and T cells values before and after vaccination,as the variables were not normally distributed. Proportion comparison (chi-square test) was used to determine whether pre-LT VZV illness or vaccina-tion were associated with VZV-specific T cells data >0.1% after LT. Samplesize was not calculated as all LT children in our country were approached forthe study. All analyses were performed with Stata 12 R© (StataCorp, CollegeStation, TX, USA).
This study complied with the principles of the Declaration of Helsinkiand was approved by the Ethical Review Board of our institution (CE07-069 (MatPed 07-017)), and the Swiss Agency for Therapeutic Prod-ucts (Swissmedic) (no.2007DR4166). This study is registered in Clinicaltrials.gov: no. NCT00492739.
Results
Patient characteristics
Seventy seven of 79 LT children (97.5%, 38 males and39 females) were enrolled (Figure 1 and Table S1). Partic-ipation was declined for two children with abnormal liverfunction tests, respectively 1 and 2 years post-LT, in whomthe risk of triggering rejection episode was perceived astoo high. The median age was 7.8 years (IQR 8.1, range:0.6–18.1). Patients were 1.3 years old (IQR 2.4, range: 0.3–16.5) at their first LT. Most (58.4%) had an original diag-nosis of biliary atresia, followed by intrahepatic progres-sive familial cholestasis (4), Alagille’s syndrome (4), crypto-genic cirrhosis (4), Wilson’s disease (2), alpha-antitrypsinedeficiency (2), methylmalonic acidemia resistant to Vita-min B12 (2), other diagnosis (14, each 1). Seventy-twochildren had a single LT, four received 2, and one 3 con-secutive LT, mostly (73/83 transplantations: 88.0%) fromdeceased donors. The transplant was a reduced liver in42/83 (50.6%), a whole liver in 23/83 cases (27.7%) anda split liver in 18/83 (21.7%). Most patients were treatedwith tacrolimus (80.5%), or ciclosporin (18.2%) and one(1.3%) with sirolimus. Few patients were also receivingmycophenolate mofetil (7.7%) or prednisone (2.6%).
2976 American Journal of Transplantation 2012; 12: 2974–2985

VZV Vaccination in Pediatric LT Recipients
Baseline anti-VZV antibodies were >50 IU/L in 38/77(49.4%) patients and <50 IU/L in 39 (50.6%) (Figure 1).Among the 38 seropositive patients, 29 (76%) had a pos-itive history of chickenpox before and/or after transplantat a median age of 5.5 years (IQR 4.3), one patient hadtwo zoster episodes and 13 had been immunized prior toLT (median interval since immunization: 9.5 years). Sevenchildren out of 27 immunized before LT (25.9%) reported ahistory of VZV disease despite immunization. Two patientsdid not know if they had chickenpox or not. Among chil-dren with anti-VZV < 50 IU/L, three had a positive historyof chickenpox at a median age of 5.5 years (IQR 5.9) and14 had been immunized prior to LT (median interval sinceimmunization 2.95 years).
Safety of VZV immunization in LT children
A total of 36/39 (92.3%) seronegative children, of whom13 had been immunized prior to LT and 3 had a positiveVZV history, were eligible for immunization and vaccinatedagainst VZV (Figure 1): at the time of this report, 6 childrenhad received one dose (median age 9.8 years, IQR 8.5),23 children two doses (median age 4.8 years, IQR 7) and7 children three doses (median age 3.5 years IQR 5.2). Attheir first dose of VZV vaccine, children were at a medianof 3.1 years after their first LT (IQR 7.7, range: 1–13.4).
Diary cards were returned by 31/36 (86.1%) patients atweeks 1, 2, 4 after the first dose, and by 29/36 (80.6%)patients at weeks 6 and 8. For the second dose, diarycards were returned by 24/30 (80.0%) patients at week1, 22/30 (73.3%) patients at weeks 2 and 4 and 21/30(70.0%) patients at weeks 6 and 8. For the third dose,5/7 (71.4%) patients returned the dairy cards at weeks1, 2, and 4 and 3/7 (42.9%) patients at weeks 6 and 8.The reported adverse events are shown in Table 1. Half ofthe patients (17/31 = 54.8%) reported a localized adversereaction and 20/31 (64.5%) experienced at least once asystemic reaction to VZV vaccination. The rate of adversereactions decreased with the second and third dose. Fivechildren had ‘vesicles’ within 8 weeks after vaccination:these could have been VZV-related according to their pri-mary care physician. In the absence of systemic disease,these children were not treated with antivirals and all le-sions disappeared spontaneously in less than 48 h. Viralanalysis was not performed to distinguish vaccine-strainor wild-type VZV virus acquired through natural exposure(24). Three patients experienced a transient generalizednonvesicular rash, within 1 week (2 patients) or 2 weeks(1 patient) of immunization. The ones occurring in the firstweek were considered as unlikely related to immunization,given that most vaccine-associated rashes are vesicularand occur between 1 and 6 weeks after immunization. Asthe three children were otherwise symptomless, no inves-tigation or treatment was initiated and the rashes quicklyresolved uneventfully. Liver enzyme (AST, ALT, gamma-GTand bilirubin) values remained unaffected by immunization(data not shown). A single rejection episode was identi-fied more than 1 year after vaccination and considered as
unrelated to immunization. All parents were successfullyreached by phone and the orally provided information didnot retrieve additional adverse events.
Antibody responses to VZV immunization
A summary of VZV serology is shown in Tables 2 and 3,and Figure 2. Four patients were retrospectively identifiedas seropositive (>50 IU/L) at time of immunization, de-spite a recent seronegative serology, and were excludedfrom the analysis of vaccine responses. Two patients ofthese patients had received one dose, and the two oth-ers two doses. The median baseline titer for the remaining32 patients was 21.0 IU/L (IQR 18.0). Ten patients hadan optional additional VZV serology measured after onevaccine dose during a routine medical visit, at a mediantime of 5.1 weeks after vaccination (IQR 13.6). Their an-tibody titers had increased from a median of 17.5 IU/L(IQR 32.0) to 413.0 IU/L (IQR 1371.0) (p = 0.005). Fourof these postdose 1 seroprotected patients did not subse-quently receive the planned second dose. All four remainedseropositive at follow-up. The 28 remaining patients weretested per protocol at a median of 5.4 weeks after theirsecond vaccination (IQR 3.1). Their antibody titers had in-creased from a median of 21.0 IU/L (IQR 17.0) prior toimmunization, to 657.0 IU/L (IQR 1242.5) after their sec-ond dose (p < 0.001), with no detectable influence of timeinterval after immunization. Seven children initially reachedbut rapidly returned below the seroprotective titer of 50IU/L after two doses and received a third dose. Their me-dian anti-VZV titer increased from 25.0 IU/L (IQR 26.0) afterdose 2 to 2004.0 IU/L (IQR 4871.0, p = 0.018) after dose3. Thus, all children reached seroprotection after 1, 2 or 3vaccinations (Figures 2 and 3). There were no statisticallysignificant differences in vaccine titers between previouslyunexposed (1473.0, IQR 1731.5) and patients exposed toVZV through infection and/or vaccination prior LT (727.5,IQR 871.5; p = 0.23). VZV serology was subsequentlymeasured at each routine medical visit. At a median of89.9 weeks (IQR 146.6) after the last vaccine dose (range:4.0–201.1 weeks), 31/32 (97%) children remained sero-protected, with high-median antibody titers (Table 2 andFigure 3). The only patient whose VZV titer waned belowthe 50 IU/L threshold still had detectable immunoglobu-lins (25 IU/L) 9.8 months after immunization. This 8-year-old child was transplanted at 7.3 months of age for intra-hepatic progressive familial cholestasis, had multiple mor-bidities and required three immunizations to reach a titer>100 IU/L. Overall, the peak of vaccine-induced antibodieswas indeed strongly associated to the persistence of highantibody titers at follow-up (p < 0.001, R2 = 81.7%).
T cell responses to VZV immunization
At baseline, IFN-gamma+ VZV-specific T cells were as-sessed in 73 patients (four missing samples). VZV-specificCD4+ T cells were present above the cut-off of 0.1% in45/73 (61.6%) patients, at a median frequency of 0.13%(IQR 0.13) (Figure 4 and Table S1). A significantly higherproportion of children with a known history of VZV illness
American Journal of Transplantation 2012; 12: 2974–2985 2977
Posfay-Barbe et al.
Table 1: Adverse events related to VZV vaccination reported by 31 liver-transplanted children
Total After dose After dose After dosen = 59 doses no. 1 no. 2 no. 3
Adverse event (%) (n = 31) (n = 23) (n = 5)
Pain at injection site 8 6 1 1(15.3%)
Redness at injection site 7 5 2 0(11.9%)
Induration at injection site 5 3 2 0(8.5%)
Cutaneous rash at injection site 5 3 2 0(8.5%)
Generalized rash 3 3 0 0(5.1%)
Vesicles 5 3 2 0(8.5%)
Number of vesicles<5 2 (3.4%) 0 2 05–50 2 (3.4%) 2 0 0>50 1 (1.7%) 1 0 0
Fever ≥ 38◦C 14 10 4 0(23.7%)
Decreased appetite 11 6 5 0(18.6%)
Muscle/articular pain 3 0 3 0(5.1%)
Irritability 9 7 2 0(15.3%)
Fatigue 14 9 5 0(23.7%)
Nausea/vomiting 7 5 2 0(11.9%)
Chills 7 4 3 0(11.9%)
Headache 10 6 4 0(16.9%)
n = number of patient returning the diary side effects’ card.
(27/32 = 84.4%) had IFN-gamma+ VZV-specific CD4+ Tcells above 0.1% than patient who did not report chicken-pox (16/39 = 41%), whether or not they had previouslybeen immunized (p < 0.001). IFN-gamma+ VZV-specificCD4+ T cells >0.1% were observed in 78.6% (33/42) ofchildren with anti-VZV titers > 50 IU/L compared to 38.7%(12/31, p < 0.001) of children <50 IU/L, in whom the fre-
quency of VZV-specific T cells was also lower (0.17 vs.0.08, p < 0.001). Overall, higher baseline antibody titerswere correlated with higher frequencies of VZV-specificT cells (R2 = 20%, p < 0.001).
Comparing baseline and postimmunization in 20 patientswith paired samples indicated a significant increase of
Table 2: VZV antibody responses in IU/L to vaccination in children after liver transplantation
Timing of the serology Before immunization After dose 2 After dose 3 Peak1 Follow-up2
n tested patients 323 284 7 32 32Median; IQR 21; 18 360.7; 567 459.2; 1269.7 1134.5; 1766 464; 669Range 2–50 45–2755 86–3238.8 86 – 7500 25 – 5000Difference between before
and after immunization(p values)
- <0.001 0.018 <0.001 <0.001
VZV = varicella-zoster virus; n = number; In patients for whom multiple data were available, analyses were performed using geometricmean.1Median 8.07 weeks (IQR 49.29) after last dose of VZV vaccine (range: 3.0–177.71 weeks).2Median 89.93 weeks (IQR 146.57) after last dose of VZV vaccine (range: 4.0–201.1 weeks)3Thirty-six patients were vaccinated; four were excluded from the analysis because of baseline seropositivity4Four patients analyzed only received one dose.
2978 American Journal of Transplantation 2012; 12: 2974–2985
VZV Vaccination in Pediatric LT Recipients
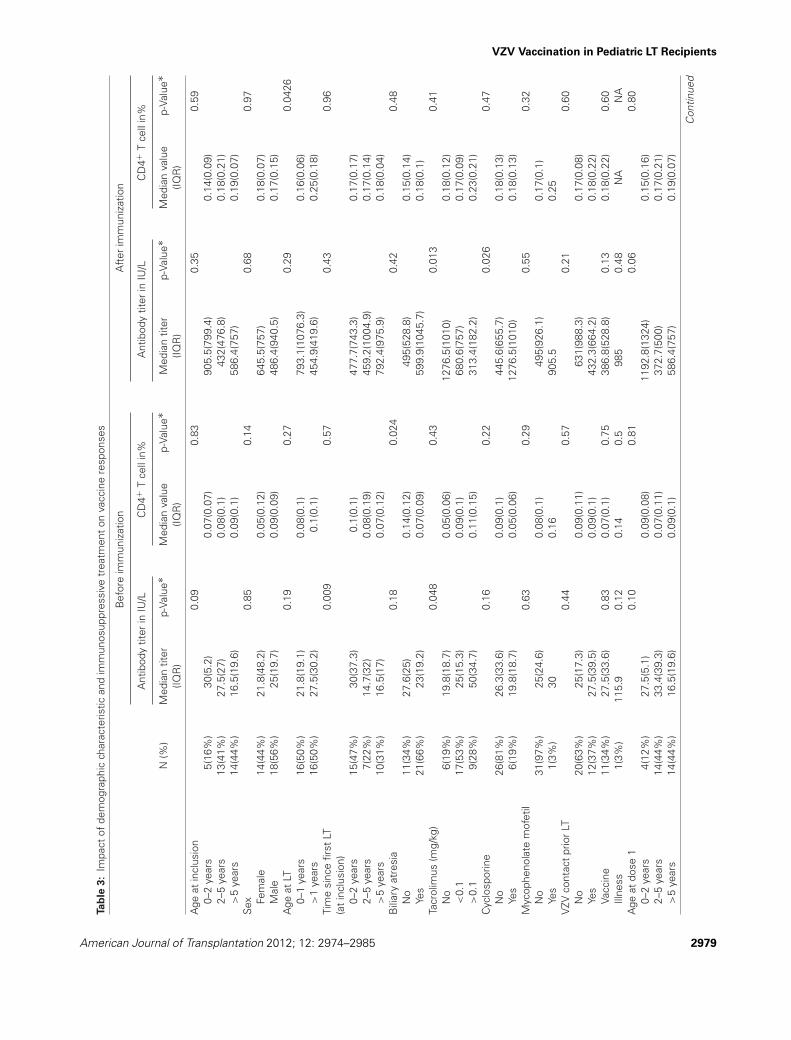
Tab
le3:
Impa
ctof
dem
ogra
phic
char
acte
ristic
and
imm
unos
uppr
essi
vetr
eatm
ent
onva
ccin
ere
spon
ses
Bef
ore
imm
uniz
atio
nA
fter
imm
uniz
atio
n
Ant
ibod
ytit
erin
IU/L
CD
4+T
cell
in%
Ant
ibod
ytit
erin
IU/L
CD
4+T
cell
in%
N(%
)M
edia
ntit
erp-
Valu
e∗M
edia
nva
lue
p-Va
lue∗
Med
ian
titer
p-Va
lue∗
Med
ian
valu
ep-
Valu
e∗(IQ
R)
(IQR
)(IQ
R)
(IQR
)
Age
atin
clus
ion
0.09
0.83
0.35
0.59
0–2
year
s5(
16%
)30
(5.2
)0.
07(0
.07)
905.
5(79
9.4)
0.14
(0.0
9)2–
5ye
ars
13(4
1%)
27.5
(27)
0.08
(0.1
)43
2(47
6.8)
0.18
(0.2
1)>
5ye
ars
14(4
4%)
16.5
(19.
6)0.
09(0
.1)
586.
4(75
7)0.
19(0
.07)
Sex
0.85
0.14
0.68
0.97
Fem
ale
14(4
4%)
21.8
(48.
2)0.
05(0
.12)
645.
5(75
7)0.
18(0
.07)
Mal
e18
(56%
)25
(19.
7)0.
09(0
.09)
486.
4(94
0.5)
0.17
(0.1
5)A
geat
LT0.
190.
270.
290.
0426
0–1
year
s16
(50%
)21
.8(1
9.1)
0.08
(0.1
)79
3.1(
1076
.3)
0.16
(0.0
6)>
1ye
ars
16(5
0%)
27.5
(30.
2)0.
1(0.
1)45
4.9(
419.
6)0.
25(0
.18)
Tim
esi
nce
first
LT0.
009
0.57
0.43
0.96
(at
incl
usio
n)0–
2ye
ars
15(4
7%)
30(3
7.3)
0.1(
0.1)
477.
7(74
3.3)
0.17
(0.1
7)2–
5ye
ars
7(22
%)
14.7
(32)
0.08
(0.1
9)45
9.2(
1004
.9)
0.17
(0.1
4)>
5ye
ars
10(3
1%)
16.5
(17)
0.07
(0.1
2)79
2.4(
975.
9)0.
18(0
.04)
Bili
ary
atre
sia
0.18
0.02
40.
420.
48N
o11
(34%
)27
.6(2
5)0.
14(0
.12)
495(
528.
8)0.
15(0
.14)
Yes
21(6
6%)
23(1
9.2)
0.07
(0.0
9)59
9.9(
1045
.7)
0.18
(0.1
)Ta
crol
imus
(mg/
kg)
0.04
80.
430.
013
0.41
No
6(19
%)
19.8
(18.
7)0.
05(0
.06)
1276
.5(1
010)
0.18
(0.1
2)<
0.1
17(5
3%)
25(1
5.3)
0.09
(0.1
)68
0.6(
757)
0.17
(0.0
9)>
0.1
9(28
%)
50(3
4.7)
0.11
(0.1
5)31
3.4(
182.
2)0.
23(0
.21)
Cyc
losp
orin
e0.
160.
220.
026
0.47
No
26(8
1%)
26.3
(33.
6)0.
09(0
.1)
445.
6(65
5 .7)
0.18
(0.1
3)Ye
s6(
19%
)19
.8(1
8.7)
0.05
(0.0
6)12
76.5
(101
0)0.
18(0
.13)
Myc
ophe
nola
tem
ofet
il0.
630.
290.
550.
32N
o31
(97%
)25
(24.
6)0.
08(0
.1)
495(
926.
1)0.
17(0
.1)
Yes
1(3%
)30
0.16
905.
50.
25V
ZVco
ntac
tpr
ior
LT0.
440.
570.
210.
60N
o20
(63%
)25
(17.
3)0.
09(0
.11)
631(
988.
3)0.
17(0
.08)
Yes
12(3
7%)
27.5
(39.
5)0.
09(0
.1)
432.
3(66
4.2)
0.18
(0.2
2)Va
ccin
e11
(34%
)27
.5(3
3.6)
0.83
0.07
(0.1
)0.
7538
6.8(
528.
8)0.
130.
18(0
.22)
0.60
Illne
ss1(
3%)
115.
90.
120.
140.
598
50.
48N
AN
AA
geat
dose
10.
100.
810.
060.
800–
2ye
ars
4(12
%)
27.5
(5.1
)0.
09(0
.08)
1192
.8(1
324)
0.15
(0.1
6)2–
5ye
ars
14(4
4%)
33.4
(39.
3)0.
07(0
.11)
372.
7(50
0)0.
17(0
.21)
>5
year
s14
(44%
)16
.5(1
9.6)
0.09
(0.1
)58
6.4(
757)
0.19
(0.0
7)
Con
tinue
d
American Journal of Transplantation 2012; 12: 2974–2985 2979
Posfay-Barbe et al.
Tab
le3:
Con
tinue
d
Bef
ore
imm
uniz
atio
nA
fter
imm
uniz
atio
n
Ant
ibod
ytit
erin
IU/L
CD
4+T
cell
in%
Ant
ibod
ytit
erin
IU/L
CD
4+T
cell
in%
N(%
)M
edia
ntit
erp-
Valu
e∗M
edia
nva
lue
p-Va
lue∗
Med
ian
titer
p-Va
lue∗
Med
ian
valu
ep-
Valu
e∗D
elay
betw
een
first
LTan
ddo
se1
0.00
90.
670.
660.
800–
2ye
ars
15(4
7%)
30(3
7.3)
0.1(
0.1)
477.
7(74
3.3)
0.17
(0.1
7)2–
5ye
ars
6(19
%)
14.7
(32)
0.08
(0.1
9)57
5.1(
940.
5)0.
18(0
.07)
>5
year
s11
(34%
)16
.4(1
7)0.
08(0
.12)
599.
9(10
28.1
)0.
17(0
.07)
Loca
ladv
erse
even
t(a
ny)
0.50
0.70
0.98
0.06
No
13(4
6%)
25(1
6.9)
0.07
(0.1
9)45
9.2(
282.
9)0.
2(0.
07)
Yes
15(5
4%)
25(3
5.3)
0.09
(0.0
7)90
5.5(
1200
.5)
0.14
(0.0
9)Pa
inat
inje
ctio
nsi
te0.
960.
180.
590 .
40N
o22
(79%
)25
(20.
2)0.
07(0
.11)
445.
6(41
2.4)
0.18
(0.1
1)Ye
s6(
21%
)24
.3(3
3)0.
11(0
.07)
1038
.3(2
84.8
)0.
16(0
.03)
Red
ness
atin
ject
ion
site
0.30
00.
610.
611
No
22(7
9%)
25(2
2.5)
0.09
(0.1
1)48
6.4(
774.
6)0.
18(0
.07)
Yes
6(21
%)
27.5
(55.
3)0.
07(0
.05)
506.
2(13
90.4
)0.
18(0
.19)
Indu
ratio
nat
inje
ctio
nsi
te0.
200.
550.
430.
63N
o24
(86%
)25
(20.
6)0.
08(0
.11)
468.
4(76
6.3)
0.18
(0.1
1)Ye
s4(
14%
)51
.7(7
5.3)
0.14
(0.0
7)10
38.3
(750
.3)
0.16
Cut
aneo
usra
shat
inje
ctio
nsi
te0.
130.
610.
230.
0506
No
23(8
2%)
25(1
9.2)
0.07
(0.1
1)49
5(10
49.3
)0.
18(0
.12)
Yes
5(18
%)
39.3
(25)
0.14
(0.0
5)43
2(79
9.6)
0.09
(0.0
7)G
ener
aliz
edra
sh0.
500.
250.
650.
10N
o26
(93%
)25
(22.
9)0.
07(0
.11)
534(
876.
9)0.
18(0
.10)
Yes
2(7%
)19
.9(1
0.3)
0.09
(0.0
02)
269.
4(32
5.1)
0.09
Vesi
cles
0.69
0.51
0.50
0.06
6N
o24
(86%
)25
(21.
5)0.
07(0
.11)
525.
4(82
5.8)
0 .18
(0.1
2)Ye
s4(
14%
)21
.1(2
7.4)
0.09
(0.0
4)32
8.6(
831.
9)0.
09(0
.09)
Syst
emic
adve
rse
even
t(a
ny)
0.33
0.89
0.54
0.22
No
10(3
6%)
20.8
(23.
7)0.
06(0
.12)
468.
4(58
8.5)
0.2(
0.09
)Ye
s18
(64%
)25
(33.
1)0.
09(0
.07)
534(
1177
.3)
0.16
(0.1
)Fe
ver≥
38◦ C
0.05
120.
250.
890.
56N
o16
(57%
)17
.7(1
3.1)
0.09
(0.1
2)44
5.6(
469.
3)0.
18(0
.07)
Yes
12(4
3%)
36.3
(40.
2)0.
07(0
.1)
823.
6(12
09.5
)0.
13(0
.25)
Dec
reas
edap
petit
e0.
710.
470.
500.
009
No
21(7
5%)
25(1
6.9)
0.09
(0.1
2)49
5(65
0.4)
0.2(
0.07
)Ye
s7(
25%
)25
(63.
6)0.
07(0
.06)
313.
4(12
55.8
)0.
1(0.
04)
Mus
cle/
artic
ular
pain
0.68
0.58
0.65
0.12
No
25(8
9%)
25(2
2.9)
0.08
(0.1
1)47
7.7(
671.
6)0.
18(0
.11)
Yes
3(11
%)
18.6
(18.
6)0.
09(0
.07)
1091
.6(1
503)
0.12
(0.0
7)Irr
itabi
lity
0.85
0.65
0.98
0.29
No
21(7
5%)
25(3
5.9)
0.09
(0.1
4)47
7.7(
671.
6)0.
18(0
.1)
Yes
7(25
%)
25(8
.9)
0.07
(0.0
2)49
5(12
94.6
)0.
13(0
.16)
Con
tinue
d
2980 American Journal of Transplantation 2012; 12: 2974–2985
VZV Vaccination in Pediatric LT Recipients
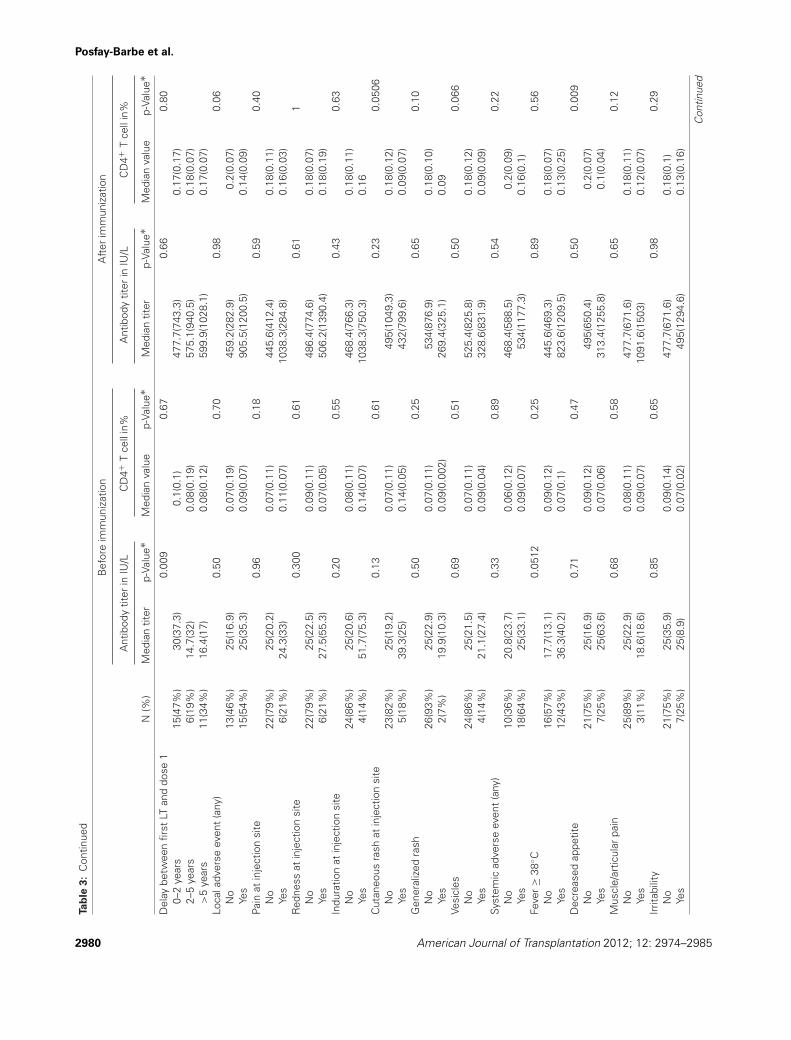
Tab
le3:
Con
tinue
d
Bef
ore
imm
uniz
atio
nA
fter
imm
uniz
atio
n
Ant
ibod
ytit
erin
IU/L
CD
4+T
cell
in%
Ant
ibod
ytit
erin
IU/L
CD
4+T
cell
in%
N(%
)M
edia
ntit
erp-
Valu
e∗M
edia
nva
lue
p-Va
lue∗
Med
ian
titer
p-Va
lue∗
Med
ian
valu
ep-
Valu
e∗Fa
tigue
0.52
0.61
0.58
0.01
6N
o19
(68%
)25
(19.
2)0.
09(0
.12)
495(
650.
4)0.
2(0.
07)
Yes
9(32
%)
25(3
1.4)
0.07
(0.0
8)31
3.4(
1200
.5)
0.1(
0.07
)N
ause
a/vo
miti
ng0.
770.
200.
460.
11N
o24
(86%
)25
(28.
1)0.
08(0
.11)
534(
815.
2)0.
18(0
.12)
Yes
4(14
%)
21(1
6.4)
0.08
(0.0
9)14
6.2(
732.
8)0.
09(0
.09)
Chi
lls0.
910.
740.
700.
46N
o22
(79%
)25
(16.
8)0.
08(0
.1)
486.
4(87
6.9)
0.18
(0.0
7)Ye
s6(
21%
)27
(35.
9)0 .
08(0
.12)
498.
4(19
9.6)
0.13
(0.1
)H
eada
che
0.37
0.88
0.56
0.02
6N
o23
(82%
)25
(33.
6)0.
08(0
.1)
477.
7(87
6.9)
0.19
(0.0
9)Ye
s5(
18%
)18
.6(1
0.3)
0.09
(0.0
7)57
3(90
6.1)
0.11
(0.0
5)∗ A
naly
sis
usin
gK
rusk
al–W
allis
one-
way
anal
ysis
ofva
rianc
eby
rank
s(n
onpa
ram
etric
test
).N
=nu
mbe
r;V
ZV=
varic
ella
zost
ervi
rus;
LT=
liver
tran
spla
ntat
ion.
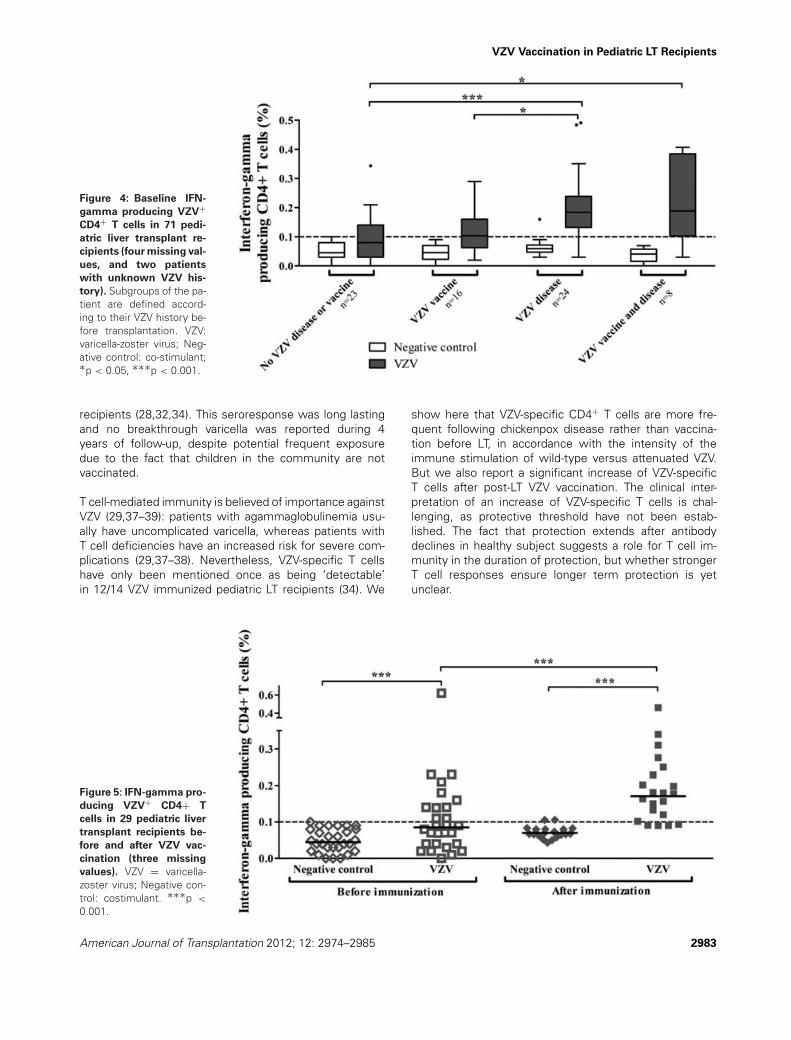
IFN-gamma+ VZV-specific CD4+ T cells, from 0.085% (IQR0.125) at baseline to 0.16% (IQR 0.175, p = 0.04) (Table3 and Figure 5). No correlation was observed betweenvaccine-induced antibody titers and T cell responses.
Despite active follow-up, no breakthrough VZV-related dis-ease was reported during the follow-up period (median4.14 years, IQR 0.90).
Discussion
VZV is a significant threat for pediatric LT patients, giventheir high risk of serious VZV-associated complications andfrequent exposure to the virus—especially in countrieswithout universal vaccination recommendations (25). Ide-ally, immunization should be implemented before trans-plant, but pediatric LT candidates are often too young tobe vaccinated during this period (26–28). In our cohort,seven children transplanted after the age of 1 year (me-dian age 1.3 years, range: 1.1–2.5) could/should have beenimmunized prior to LT (missed opportunities). However,pretransplant-induced immunity may wane as a result ofimmunosuppression (29). Indeed, 25.9% of our patientsimmunized before LT reported VZV disease despite immu-nization. After solid-organ transplantation, live-attenuatedVZV vaccine is currently officially contraindicated (30–33).Although some centers have sporadically vaccinated pedi-atric LT recipients (28,34), to our knowledge large prospec-tive cohorts of systematic VZV vaccination have not beenpublished in solid-organ recipients (18,28,34). We show inthis observational prospective cohort study that VZV vacci-nation is safe and immunogenic in pediatric LT recipients,including in seronegative children with no prior history ofdisease or vaccination.
A primary endpoint of this study was to monitor vaccinesafety. Immunization did not trigger clinical or biologicalepisodes of graft rejection. Approximately half of the chil-dren reported local reactions and two-thirds had systemicreactions, which appears similar as in healthy children (35).Among the three generalized skin rash reported, only onemay have been associated to the vaccine. It is likely thatthe five children with vesicles within 8 weeks had an at-tenuated form of varicella infection, but these remainedisolated and all lesions spontaneously disappeared within48 h, without any antiviral treatment.
Two doses of varicella vaccine are recommended to VZV-naive patients to ensure sustained seroresponses andprotection (35–36). In this study, 7/32 (21.9%) children re-quired an additional third dose. The impact of this third doseon VZV immunity was reflected by a significant increaseof anti-VZV titers. This proportion of nonserorespondersafter two vaccine doses is higher than in healthy children(35). Although anti-VZV titers may not directly correlatewith vaccine-induced protection given the role of CD4+ Tcells, they are a marker of VZV-induced immunity (16). The
American Journal of Transplantation 2012; 12: 2974–2985 2981
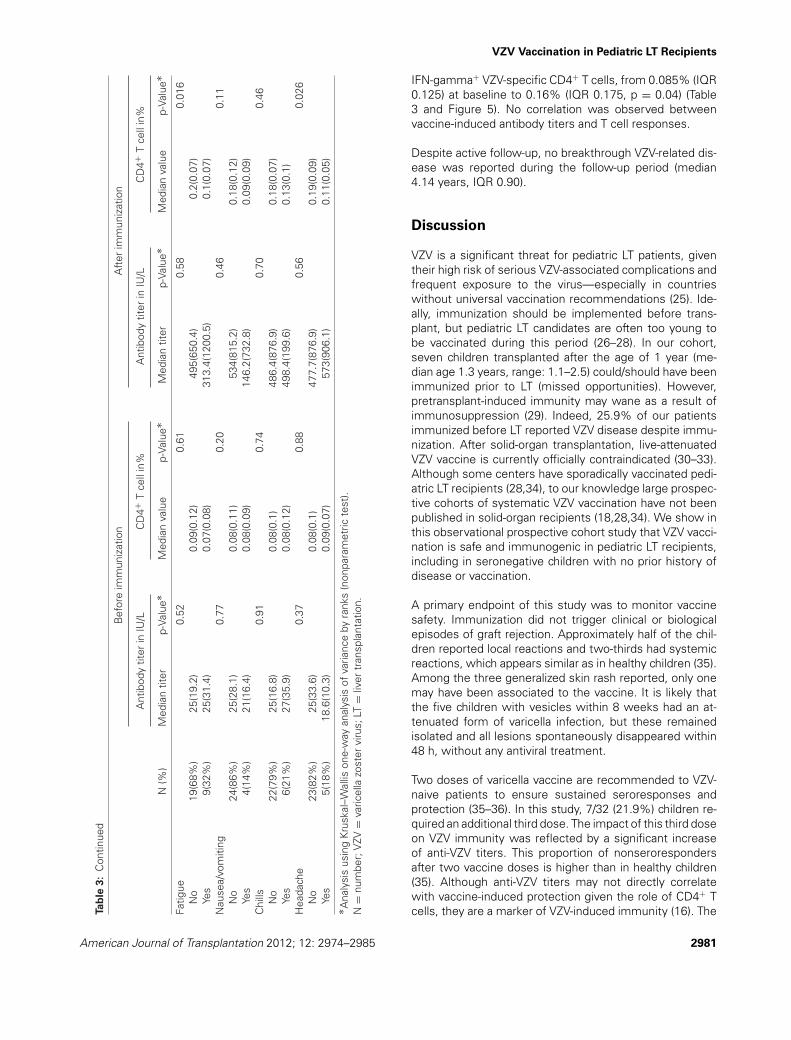
Posfay-Barbe et al.
Figure 2: VZV antibody titers following vaccination in 32 pediatric liver transplant recipients before or after the indicated dose.
Follow-up: last available sample. Time in weeks between dose and serology (median [interquartile range]): a 11.93 [24.29]; b 72.07 [98.43];c 5.29 [3.14]; d 87.71 [152.71]; e 4.14 [6.71]; f 131.0 [133.57]. VZV: varicella-zoster virus.
number of patients requiring a third dose of vaccine wassmall. This precluded further exploration into predictive pa-rameters for the need for a third dose of VZV vaccine, andjustified a routine serological evaluation after two doses.
Following a maximum of three doses, all children reachedantibody levels defined as protective (12–15). This 100%seroconversion rate is higher than reported in the literatureafter two vaccine doses given to solid-organ transplant
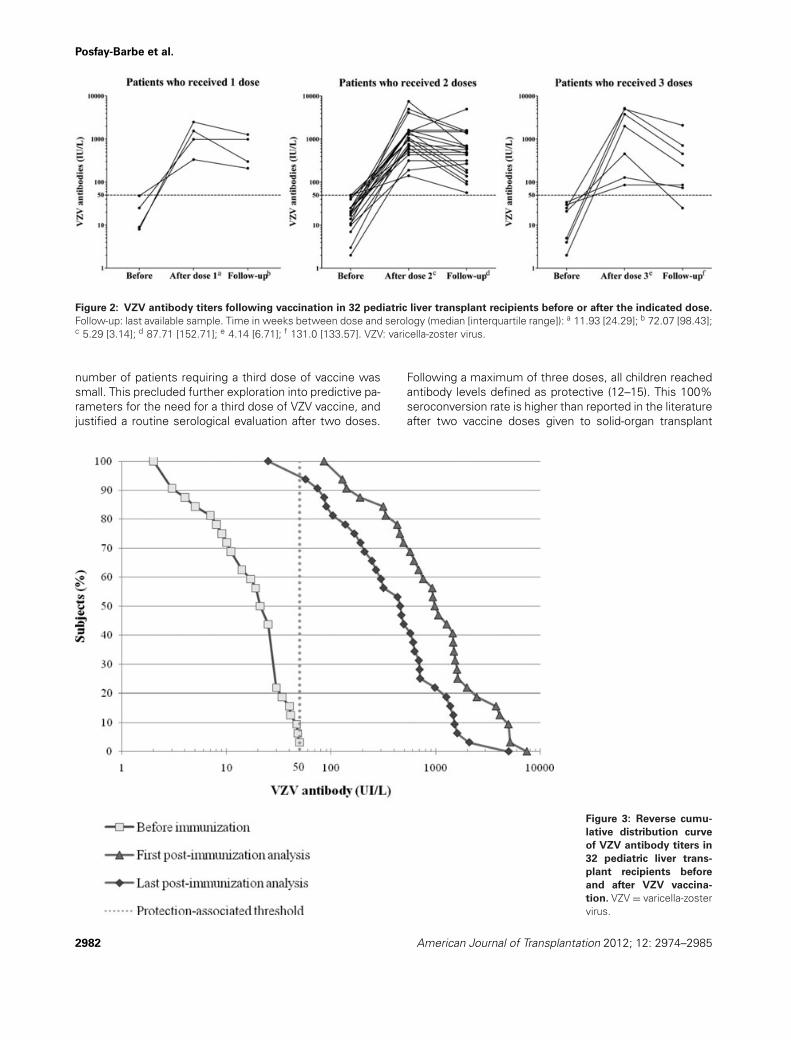
Figure 3: Reverse cumu-
lative distribution curve
of VZV antibody titers in
32 pediatric liver trans-
plant recipients before
and after VZV vaccina-
tion. VZV = varicella-zostervirus.
2982 American Journal of Transplantation 2012; 12: 2974–2985
VZV Vaccination in Pediatric LT Recipients
Figure 4: Baseline IFN-
gamma producing VZV+CD4+ T cells in 71 pedi-
atric liver transplant re-
cipients (four missing val-
ues, and two patients
with unknown VZV his-
tory). Subgroups of the pa-tient are defined accord-ing to their VZV history be-fore transplantation. VZV:varicella-zoster virus; Neg-ative control: co-stimulant;∗p < 0.05, ∗∗∗p < 0.001.
recipients (28,32,34). This seroresponse was long lastingand no breakthrough varicella was reported during 4years of follow-up, despite potential frequent exposuredue to the fact that children in the community are notvaccinated.
T cell-mediated immunity is believed of importance againstVZV (29,37–39): patients with agammaglobulinemia usu-ally have uncomplicated varicella, whereas patients withT cell deficiencies have an increased risk for severe com-plications (29,37–38). Nevertheless, VZV-specific T cellshave only been mentioned once as being ‘detectable’in 12/14 VZV immunized pediatric LT recipients (34). We
show here that VZV-specific CD4+ T cells are more fre-quent following chickenpox disease rather than vaccina-tion before LT, in accordance with the intensity of theimmune stimulation of wild-type versus attenuated VZV.But we also report a significant increase of VZV-specificT cells after post-LT VZV vaccination. The clinical inter-pretation of an increase of VZV-specific T cells is chal-lenging, as protective threshold have not been estab-lished. The fact that protection extends after antibodydeclines in healthy subject suggests a role for T cell im-munity in the duration of protection, but whether strongerT cell responses ensure longer term protection is yetunclear.
Figure 5: IFN-gamma pro-
ducing VZV+ CD4+ T
cells in 29 pediatric liver
transplant recipients be-
fore and after VZV vac-
cination (three missing
values). VZV = varicella-zoster virus; Negative con-trol: costimulant. ∗∗∗p <
0.001.
American Journal of Transplantation 2012; 12: 2974–2985 2983

Posfay-Barbe et al.
VZV vaccination has been previously shown to be safelyadministered to children with leukemia in remission, HIVinfection, or, in some specific cases, organ transplanta-tion (40–41). To our knowledge this is the largest prospec-tive pediatric transplant cohort vaccinated against VZV. Weshould highlight that there was heterogeneity in the timingof sample collection and missing samples for T cell anal-yses: this is mostly due to children living away from thehospital, and medical appointments being planned accord-ing to parents’ and attending physicians’ availabilities ratherthan according to the study protocol. We used convention-ally accepted antibody thresholds for the interpretation ofthe results, but correlates of protection against VZV havenot been firmly established (29) and could differ in trans-plant recipients.
However, our results show that VZV immunity could beelicited in all tested LT recipients, including those with nohistory of prior disease or immunization and who wereseronegative at study inclusion. Adverse reactions wereonly mild and transient; breakthrough disease was notidentified despite monitoring and presumed exposure,as VZV is endemic in the Swiss schools and communi-ties attended by our patients. These vaccine responseswere elicited later than 1 year after LT. Whether theycould have been induced earlier is an interesting ques-tion: for this first study, we had elected to immunizechildren on lower immunosuppressive regimen and ina steady state regarding the risk of triggering rejectionepisodes (42). Another open question is whether thesepatients will require/would benefit from subsequent boost-ers: this will require longer follow-up and monitoring ofbreakthrough disease. Although vaccinating children priorto LT is preferable, VZV immunity may not last and pri-mary or booster VZV immunization appears safe, immuno-genic and efficient in pediatric LT patients. Based on ourexperience, that of other centers (28, 34), and our anal-ysis of the risk–benefit ratio, we recommend that VZVserology be assessed 1 year after LT in all patients (re-gardless of pretransplant VZV exposure or immunization)and that VZV (re-)immunization be considered for seroneg-ative patients fulfilling specific criteria (such as the onesused in this or other studies [28,34]), with confirmation ofseroconversion.
Acknowledgments
We thank the participating children and their family, their physicians, as wellas the Plateforme de Recherche Clinique en Pediatrie’s staff and SimonaKorff for their help in this study. This study was possible thanks to an internalresearch grant of the University Hospitals of Geneva (Fonds de Rechercheet Developpement).
Funding sources: Research grants from the University Hospitalsof Geneva and from the Center for Vaccinology and NeonatalImmunology
Disclosure
The authors of this manuscript have no conflicts of inter-est to disclose as described by the American Journal ofTransplantation.
Author contributions
Conceived and designed the study: K.M.P.B., C.A.S. Col-lected the clinical data: M.R., K.M.P.B., B.W., D.C.B., V.A.M.Conceived and designed the experiments: C.S., S.G., L.K.,K.M.P.B. Performed the experiments: C.S., S.G. Analyzedthe data: K.M.P.B., L.F.P. Wrote the paper: K.M.B.P., L.F.P.,C.A.S. Reviewed critically the manuscript: K.M.P.B., L.F.P.,S.G., C.S., M.R., L.K., B.W., D.C.B., V.A.M., C.A.S.
References
1. Davison AJ, Scott JE. The complete DNA sequence of varicella-zoster virus. J Gen Virol 1986; 67: 1759–1816.
2. Heininger U, Seward JF. Varicella. Lancet 2006; 368: 1365–1376.3. Ross AH. Modification of chicken pox in family contacts by admin-
istration of gamma globulin. N Engl J Med 1962; 267: 369–376.4. Izurieta HS, Strebel PM, Blake PA. Postlicensure effectiveness of
varicella vaccine during an outbreak in a child care center. JAMA1997; 278: 1495–1499.
5. Feldhoff CM, Balfour HH, Jr., Simmons RL, Najarian JS, MauerSM. Varicella in children with renal transplants. J Pediatr 1981; 98:25–31.
6. Levitsky J, Kalil AC, Meza JL, Hurst GE, Freifeld A. Chicken pox af-ter pediatric liver transplantation. Liver Transplant 2005; 11: 1563–1566.
7. McGregor RS, Zitelli BJ, Urbach AH, Malatack JJ, Gartner JC, Jr.Varicella in pediatric orthotopic liver transplant recipients. Pedi-atrics 1989; 83: 256–261.
8. Weinstock DM, Boeckh M, Boulad F, et al. Postexposure pro-phylaxis against varicella-zoster virus infection among recipientsof hematopoietic stem cell transplant: Unresolved issues. InfectControl Hosp Epidemiol 2004; 25: 603–608.
9. Vazquez M, LaRussa PS, Gershon AA, Steinberg SP, FreudigmanK, Shapiro ED. The effectiveness of the varicella vaccine in clinicalpractice. N Engl J Med 2001; 344: 955–960.
10. Skull SA, Wang EE. Varicella vaccination—a critical review of theevidence. Arch Dis Child 2001; 85: 83–90.
11. Ludwig B, Kraus FB, Allwinn R, Keim S, Doerr HW, BuxbaumS. Loss of varicella zoster virus antibodies despite detectable cellmediated immunity after vaccination. Infection 2006; 34: 222–226.
12. Li S, Chan IS, Matthews H, et al. Inverse relationship between sixweek postvaccination varicella antibody response to vaccine andlikelihood of long term breakthrough infection. Pediatr Infect Dis J2002; 21: 337–342.
13. Clements DA, Armstrong CB, Ursano AM, Moggio MM, WalterEB, Wilfert CM. Over five-year follow-up of Oka/Merck varicellavaccine recipients in 465 infants and adolescents. Pediatr InfectDis J 1995; 14: 874–879.
14. Johnson CE, Stancin T, Fattlar D, Rome LP, Kumar ML. A long-term prospective study of varicella vaccine in healthy children.Pediatrics 1997; 100: 761–766.
15. Michalik DE, Steinberg SP, Larussa PS, et al. Primary vaccine fail-ure after 1 dose of varicella vaccine in healthy children. J Infect Dis2008; 197: 944–949.
2984 American Journal of Transplantation 2012; 12: 2974–2985

VZV Vaccination in Pediatric LT Recipients
16. Plotkin SA. Correlates of protection induced by vaccination. ClinVaccine Immunol 2010; 17: 1055–1065.
17. Donati M, Zuckerman M, Dhawan A, et al. Response to varicellaimmunization in pediatric liver transplant recipients. Transplanta-tion 2000; 70: 1401–1404.
18. Abuali MM, Arnon R, Posada R. An update on immunizations be-fore and after transplantation in the pediatric solid organ transplantrecipient. Pediatr Transplant 2011; 15: 770–777.
19. Diana A, Posfay-Barbe KM, Belli DC, Siegrist CA. Vaccine-inducedimmunity in children after orthotopic liver transplantation: A 12-year review of the Swiss national reference center. Pediatr Trans-plant 2007; 11: 31–37.
20. Sottas C. Developpement de nouveaux tests quantifiantl’immunite face a la varicelle et application a une popula-tion immunosupprimee: les enfants receveurs de transplantationhepatique. [Medicine]. Geneva: University of Geneva; 2009.
21. Brosterhus H, Brings S, Leyendeckers H et al. Enrichment anddetection of live antigen-specific CD4(+) and CD8(+) T cells basedon cytokine secretion. Eur J Immunol. 1999; 29: 4053–4059.
22. Desombere I, Meuleman P, Rigole H, Willems A, Irsch J, Leroux-Roels G. The interferon gamma secretion assay: A reliable toolto study interferon gamma production at the single cell level. JImmunol Methods 2004; 286: 167–185.
23. Altman DG, Gore SM, Gardner MJ, Pocock SJ. Statistical guide-lines for contributors to medical journals. Br Med J (Clin Res Ed)1983; 286: 1489–1493.
24. Leung J, Harpaz R, Baughman AL, et al. Evaluation of laboratorymethods for diagnosis of varicella. Clin Infect Dis 2010; 51: 23–32.
25. Other herpesviruses: HHV-6, HHV-7, HHV-8, HSV-1 and -2, VZV.Am J Transplant 2004 Nov; 4(Suppl 10): 66–71.
26. Furth SL, Fivush BA. Varicella vaccination in pediatric kidney trans-plant candidates. Pediatr Transplant 2002; 6: 97–100.
27. Geel A, Zuidema W, van Gelder T, van Doornum G, Weimar W.Successful vaccination against varicella zoster virus prior to kidneytransplantation. Transplant Proc 2005; 37: 952–953.
28. Khan S, Erlichman J, Rand EB. Live virus immunization after ortho-topic liver transplantation. Pediatr Transplant 2006; 10: 78–82.
29. Prelog M, Zimmerhackl LB. Varicella vaccination in pediatric kidneyand liver transplantation. Pediatr Transplant 2010; 14: 41–47.
30. Pergam SA, Limaye AP. Varicella zoster virus (VZV) in solid organtransplant recipients. Am J Transplant 2009; 9(Suppl 4): S108–S115.
31. Gershon AA. Immunizations for pediatric transplant patients. Kid-ney Int Suppl 1993; 43: S87–S90.
32. Avery RK, Michaels M. Update on immunizations in solid organtransplant recipients: What clinicians need to know. Am J Trans-plant 2008; 8: 9–14.
33. Danzinger-Isakov L, Kumar D. Guidelines for vaccination of solidorgan transplant candidates and recipients. Am J Transplant 2009;9(Suppl 4): S258–S262.
34. Weinberg A, Horslen SP, Kaufman SS, et al. Safety and im-munogenicity of varicella-zoster virus vaccine in pediatric liverand intestine transplant recipients. Am J Transplant 2006; 6: 565–568.
35. Marin M, Guris D, Chaves SS, Schmid S, Seward JF. Prevention ofvaricella: Recommendations of the Advisory Committee on Immu-nization Practices (ACIP). MMWR Recomm Rep 2007; 56: 1–40.
36. Chaves SS, Gargiullo P, Zhang JX, et al. Loss of vaccine-inducedimmunity to varicella over time. N Engl J Med. 2007; 356: 1121–1129.
37. Haberthur K, Engelmann F, Park B, et al. CD4 T cell immunityis critical for the control of simian varicella virus infection in anonhuman primate model of VZV infection. PLoS Pathog 2011; 7:e1002367.
38. Arvin AM. Humoral and cellular immunity to varicella-zoster virus:An overview. J Infect Dis 2008; 197(Suppl 2): S58–S60.
39. Arvin A, Abendroth A. VZV: Immunobiology and host response.In: Arvin A, Campadelli-Fiume G, Mocarski E, eds. Human Her-pesviruses: Biology, Therapy, and Immunoprophylaxis. Cambridge:Cambridge University Press, 2007: 700–712.
40. Sartori AM. A review of the varicella vaccine in immunocompro-mised individuals. Int J Infect Dis 2004; 8: 259–270.
41. Levin MJ. Varicella vaccination of immunocompromised children.J Infect Dis 2008; 197(Suppl 2): S200–S206.
42. Duchini A, Goss JA, Karpen S, Pockros PJ. Vaccinations for adultsolid-organ transplant recipients: Current recommendations andprotocols. Clin Microbiol Rev 2003; 16: 357–364.
Supporting Information
Additional Supporting Information may be found in the on-line version of this article:
Table S1: Impact of demographic characteristic and im-munosuppressive treatment on baseline VZV-specific anti-body titer and CD4+ T cell
Please note: Wiley-Blackwell is not responsible for the con-tent or functionality of any supporting materials suppliedby the authors. Any queries (other than missing material)should be directed to the corresponding author for thearticle.
American Journal of Transplantation 2012; 12: 2974–2985 2985