Embed Size (px)
Citation preview

HE extreme-lateral craniocervical approach is the ap-proach preferred by several neurosurgeons to reachthe ventral surface of the spinomedullary junction
and the lower clivus.5,8,22–24 By drilling various bony struc-tures in that region, including the occipital condyle, jugulartubercle, and articular facets of C-1 and C-2, access to thenormal anatomical structures and the pathological lesions is provided.3,6–8,15,18 Whether or not occipitocervical fusionbecomes necessary depends on the type of approach that is performed. The need for this procedure has been ques-tioned, especially as it applies to treating certain types oflesions in the region.2 By understanding the anatomy ofspecific components of the approach, the surgeon can tailorthe technique to different lesions, providing the requiredexposure, without unnecessary surgical steps. In this reportwe present an anatomical study and clinical experiencebased on performing six variations of the extreme-lateral
craniocervical approach.
Clinical Material and Methods
Surgery was performed in 69 patients in whom one of sixvariations on the extreme-lateral craniocervical approachwas performed; all surgeries were performed by two sur-geons (L.N.S. and D.C.W.) at The George Washington Uni-versity Medical Center during a more than 4-year period.Fifty-one patients harbored neoplastic lesions: there were 24 meningiomas, 10 chordomas, seven paragangliomas,three schwannomas, two chondrosarcomas, two neurofi-bromas, and one each of hemangiopericytoma, osteochond-roma, and metastatic carcinoma. Twelve patients had ver-tebral artery (VA) or vertebrobasilar (VB) aneurysms. Sixpatients had different cystic, inflammatory, and other vas-cular lesions (Table 1).
J Neurosurg (Spine 2) 90:206–219, 1999
206
Variations of the extreme-lateral craniocervical approach:anatomical study and clinical analysis of 69 patients
EDUARDO SALAS, M.D., LALIGAM N. SEKHAR, M.D., IBRAHIM M. ZIYAL, M.D., ANTHONY J. CAPUTY, M.D., AND DONALD C. WRIGHT, M.D.
Department of Neurosurgery, The George Washington University Medical Center, Washington, D.C.
Object. The aim of this study was to describe six variations of the extreme-lateral craniocervical approach, theirapplication, and treatment results.
Methods. During a 4-year period 69 patients underwent surgery in which six variations of the extreme-lateral cra-niocervical approach were performed. The variations included: the transfacetal approach (TFA), performed to treat fourlesions in the upper cervical spine anterior or anterolateral to the spinal cord; the retrocondylar approach, to treat fiveintradural lesions located anterolateral to the medulla oblongata and six vascular lesions to expose the extradural seg-ment of the vertebral artery (VA); the partial transcondylar approach (PTCA), to treat 18 intradural lesions located ante-rior to the medulla oblongata; the complete transcondylar approach (CTCA), to treat 13 extradural lesions that involvedthe lower clivus and anterior upper cervical spine; the extreme-lateral transjugular approach, to treat 14 jugular foramentumors; and the transtubercular approach with or without division of the sigmoid sinus, to treat complex VA and ver-tebrobasilar junction aneurysms. An anatomical prosection was performed to study the surgical exposure of each of thesix variations of the extreme-lateral craniocervical approach.
Total removal was achieved in 35 (69%) of the patients with tumor; subtotal resection was achieved in 16 (31%) ofthose patients. In the 12 patients with VA aneurysms, seven underwent clipping, three underwent trapping and a vein graftbypass procedure, and two underwent trapping without the use of a bypass procedure. In five other patients, different cys-tic, inflammatory, and other vascular lesions were successfully treated. Fifty percent of the patients who underwent surgeryvia the TFA, 83% via the of the CTCA, and 11% via the PTCA required an occipitocervical fusion procedure. The meanKarnofsky Performance Scale score was 74.7 preoperatively and 76.4 postoperatively. Major complications were hydro-cephalus (nine patients), cerebrospinal fluid leakage (seven patients), worsened cranial nerve function (seven patients), ver-tebrobasilar vasospasm (one patient), and sigmoid sinus thrombosis (one patient).
Conclusions. To treat lesions in the region of the foramen magnum and surrounding areas, the approach should betailored to each specific lesion to provide the needed exposure without unnecessary operative steps.
KEY WORDS • chordoma • craniocervical junction • jugular foramen tumor •meningioma • neurinoma • posterior circulation aneurysm
T
J. Neurosurg: Spine / Volume 90 / April, 1999

At presentation the most frequent symptoms were gaitdisturbance (49%), headache (40%), and swallowing diffi-culty (40%) (Table 2). The ninth to 11th (37%), the 12th(21%), and the eighth (29%) cranial nerves were more fre-quently affected in patients with tumors. Nearly 29% (13patients) had undergone at least one previous surgery. Eightpatients, four of whom harbored chordomas, three menin-giomas, and one of whom harbored a hemangiopericytoma,had undergone preoperative radiotherapy. Vertebral arteryencasement was observed in 22 patients (43%) with tu-mors. The tumor dimension was expressed as the tumorequivalent diameter (TED) = 3√D1 � D2 � D3, where D1,D2, and D3 represent the tumor diameter in all three planes.The mean TED of the surgically treated tumors was 3.5 cm(range 1–5.6 cm). Most of the tumors surgically treated viathe complete transcondylar approach (CTCA) were large(mean TED 4.15 cm).
Anatomical Studies
Twelve cadaver heads were embalmed with glutaralde-hyde solution. The arteries and veins were injected withred- and blue-colored latex (Microfil; Flow Tech, Inc., Car-ver, MA), respectively. Dissections were performed via allsix types of the extreme-lateral craniocervical approach,and photographs were obtained to illustrate the stages andfinal exposures.
Preoperative Studies
The neoplastic lesions were evaluated preoperativelywith magnetic resonance (MR) imaging, computerized to-mography (CT), and angiography. For vascular lesions thepreoperative studies included angiography, MR angiogra-phy, and/or three-dimensional CT scanning. The three-di-
J. Neurosurg: Spine / Volume 90 / April, 1999
Variations of the extreme-lateral craniocervical approach
207
TABLE 1Lesions and variation on the extreme-lateral craniocervical approach in patients undergoing surgical treatment
TFA RCA PTCA CTCA ETJA TTA TotalType of Lesion (4 pts) (11 pts) (18 pts) (13 pts) (14 pts) (9 pts) (69 pts)
meningioma 1 5 14 0 4 0 24chordoma & chondrosarcoma 0 0 0 12 0 0 12neurofibroma 1 0 0 0 1 0 2schwannoma 1 0 0 0 2 0 3paraganglioma 0 0 0 0 7 0 7osteochondroma 1 0 0 0 0 0 1metastatic carcinoma 0 0 0 1 0 0 1hemangiopericytoma 0 0 1 0 0 0 1granuloma 0 0 1 0 0 0 1cystic lesion* 0 0 2 0 0 0 2VA–VB junction aneurysms 0 3 0 0 0 9 12condylar vein varix 0 1 0 0 0 0 1VA kinking by bone 0 1 0 0 0 0 1dural fistula† 0 1 0 0 0 0 1
* Cystic lesions included one neurenteric cyst and one epidermoid cyst.† Dural fistula = meningeal branch of the VA to sigmoid sinus.
TABLE 2Preoperative signs and symptoms in 69 patients
Extreme-Lateral Craniocervical Approach
TFA RCA PTCA CTCA ETJA TTA TotalPreop Symptoms (4 pts) (11 pts) (18 pts) (13 pts) (14 pts) (9 pts) (%)
headache 1 5 9 6 2 5 40gait disturbance 3 4 11 6 6 4 49dysarthria 0 0 3 5 4 0 17motor deficit* 1 3 5 1 1 3 20dysmetria 1 2 3 1 3 0 14sensory 2 1 3 0 2 0 11urinary incontinence 0 1 0 0 1 2 6cognitive symptoms 0 2 0 0 0 4 9endocrine dysfunction 0 1 1 0 2 0 6swallowing difficulty 0 1 5 9 12 1 407th CN† 0 0 3 0 2 0 78th CN† 0 2 7 5 6 0 299th–11th CN† 0 1 5 7 12 1 3712th CN† 0 2 3 9 6 1 21
* Includes hemiparesis, monoparesis, or quadriparesis. † Either paresis or paralysis.

mensional CT scanning was very useful in establishing therelationship of aneurysms to bony structures and in plan-ning the appropriate approach.
Selection of Different Types of the Extreme-LateralCraniocervical Approach
The transfacetal approach (TFA) was performed to reachthe four lesions found in the upper cervical spine, anterioror anterolateral to the spinal cord. The retrocondylar ap-proach (RCA) was performed to reach 11 intradural lesionslocated anterolateral to the spinomedullary area or to ex-pose the extradural segment of the VA for proximal control.Via the partial transcondylar approach (PTCA) 18 intradur-al lesions located anterior to the spinomedullary area weretreated. Thirteen extradural tumors involving the lower clivus and anterior upper cervical spine were surgicallytreated via the CTCA. The extreme-lateral transjugular ap-proach (ETJA) was performed to treat 18 paragangliomasand other jugular foramen tumors. Nine complex VA andVB aneurysms were surgically treated via the transtubercu-lar approach (TTA), with or without division of the sigmoidsinus (Fig. 1).
Anesthesia and Monitoring
A standard neuroanesthetic technique was used in all pa-tients. Somatosensory evoked potentials and, when indicat-ed, brainstem auditory evoked responses were monitoredthroughout the operations. Prophylactic intravenous antibi-otic agents were administered.
Operative Techniques
The patient was usually placed in a lateral position. Thelower arm was supported below the upper end of the table,and the axilla and other structures were well padded (Fig.2). When a patient is placed supine, with the head rotatedmore than 60˚, the transverse process and foramen of C-1move medial and inferior to the mastoid tip, making expo-sure of the VA in the C-1 transverse foramen more difficult.However, if the extreme-lateral craniocervical approachis combined with the presigmoid petrosal approach, or ifintraoperative angiography is planned, it is much easier toplace the patient supine with the head turned away from thesurgeon.
A C-shaped incision was used in most of the patients.When an occipitocervical fusion procedure was planned,an inverted U-shaped incision was preferred because betterexposure of the upper cervical spine could be obtained.
Next, the superficial, middle, and deep muscle layerswere dissected. All of the muscles were reflected medially,except the sternocleidomastoid muscle, which was reflect-ed inferiorly after being separated from the skin flap, or lat-erally with the skin flap. The extradural VA was exposedfrom the C-2 transverse foramen (or from the C-3 foramen,if necessary) to its dural entrance point. A partial mas-toidectomy and unroofing of the sigmoid sinus was per-formed; this was followed by a small craniotomy approxi-mately 3 cm posterior to the sigmoid sinus, except insurgeries via the TFA. After this initial approach, the expo-sure is continued by performing one of the six variations ofthe extreme-lateral craniocervical approach depending onthe location and the type of the lesion (Fig. 1).
Transfacetal Approach. The TFA was used to treat extra-and intradural lesions anterior to the upper cervical spinalcord (Fig. 3). The VA was exposed and mobilized medial-ly. A C1–2 hemilaminectomy was performed. The posteri-or half of the C-1 and C-2 facet joints and the occipitalcondyle were drilled away until the dural exits of the rootsof C1–2 were exposed. Mastoidectomy and craniotomywere not performed in these patients. The dura was openedin a linear fashion, anterior to the cervical roots (Fig. 4A).The dura, the dentate ligament, and the C1–2 roots wereretracted posteriorly. The anterior aspect of the spinal cordwas exposed (Fig. 4B). An occipitocervical fusion proce-dure was required following this technique.
When the lesion was anterolateral to the spinal cord, it was not necessary to drill the facets extensively, and the craniocervical junction was stable after the procedure.When the lesion involved osseous elements, bone removaldepended on the extent of the lesion.
Retrocondylar Approach. The RCA was performed totreat intradural lesions that were located predominantly lat-eral or anterolateral to the spinomedullary area or to exposethe extradural portion of the VA (Fig. 5). In this approachthe general principles of the operative technique are fol-lowed, but it does not require removal of the occipital con-dyle (Fig. 6).
Partial Transcondylar Approach. The PTCA was per-formed to treat lesions that were located predominantlyanterior to the spinomedullary junction (Fig. 7). The VAwas mobilized medially after opening the C-1 foramen(Fig. 8A). The posterior one third of the occipital condyleand superior facet of C-1 were drilled away. The hypoglos-sal canal was the anterior limit of condylar resection. Thedura was opened, leaving a cuff around the VA (Fig. 8B).Intradural management of the lesion was performed as pre-viously reported (Fig. 8C–D).3
Complete Transcondylar Approach. The CTCA was per-formed to treat extradural lesions (Fig. 9), and occipito-cervical fusion was necessary after this procedure.1,13 Af-ter medial mobilization of the VA, the initial removal of the posterior one half of the occipital condyle exposed thehypoglossal canal. By working superior and inferior to thiscanal, most of the jugular tubercle and the entire condylewere removed, thus achieving exposure of the midclivalarea (Fig. 10A). The removal of the lateral mass and later-al portion of the anterior arch of C-1 provided access to thelower clivus and to the odontoid process (Fig. 10B).
Extreme-Lateral Transjugular Approach. The ETJA wasperformed to supplement the traditional lateral transtempo-ral approach for the treatment of jugular foramen lesions(Fig. 11). A complete mastoidectomy procedure was per-formed initially with anterior mobilization of the mastoidsegment of the facial nerve along with the digastric muscleto expose the jugular bulb and jugular vein (Fig. 12A). TheVA was mobilized medially after unroofing the C-1 trans-verse foramen, and the transverse process of C-1 was resect-ed. The posterolateral one third of the occipital condyle wasremoved in such a way that the entire hypoglossal canal wasexposed. By drilling the lateral portion of the jugular tuber-cle, the medial wall of the jugular bulb and the ninth through11th cranial nerves were exposed (Fig. 12B). A linear duralincision was made approximately 1 cm posterior to the sig-moid sinus for the removal of the intradural portion of the
E. Salas, et al.
208 J. Neurosurg: Spine / Volume 90 / April, 1999

lesion. Removal of a lesion such as a paraganglioma re-quired ligation of the sigmoid sinus, whereas lesions such asschwannomas in the lower cranial nerves were removed byworking medial, inferior, and anterior to the jugular bulb.
The ETJA adds an inferomedial exposure to the jugular
foramen, in addition to other approaches previously de-scribed.14,15
Transtubercular Approach. The key element of the TTA isto remove the jugular tubercle that, intradurally, obstructsthe view of the VA or VB junction. The TTA was performed
J. Neurosurg: Spine / Volume 90 / April, 1999
Variations of the extreme-lateral craniocervical approach
209
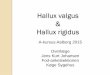
FIG. 1. Schematic drawings illustrating the relationship between the lesion and the bone removed in each type of extreme-lateral craniocervical approach. A: The TFA; B: The RCA; C: The PTCA; D: The CTCA; E: The ETJA; and F: The TTA.

to treat complex aneurysms in this location (Fig. 13). Theposteromedial one third of the occipital condyle and the C-1 lateral mass were drilled away. The jugular tubercleabove the hypoglossal canal was removed extradurally tothe extent possible. However, complete removal was usual-ly not achieved in this manner (Fig. 14A). The retrosigmoiddura was opened, and if the sigmoid sinus was shown to be nondominant and well collateralized on preoperativeangiography, it was divided after measuring the intrasinuspressure by using temporary occlusion.20,25 The two ends ofthe sinus were occluded with temporary clips and were resu-tured using No. 6-0 prolene at the end of the operation. Thedeepest part of the jugular tubercle (Fig. 14B) was thendrilled away intradurally by working superiorly and medial-ly to the ninth cranial nerve or inferolaterally to the 11th cranial nerve as it approaches the jugular foramen. The re-moval of the jugular tubercle was performed even when thesigmoid sinus was not divided; the procedure was aided bythe anterior mobilization of the sigmoid sinus.
The TTA resulted in better exposure of the distal ipsilat-
eral VA, the contralateral VA, and the VB junction (Fig.14C) compared with a very lateral retrosigmoid approachand even to the RCA. Both steps of the operation (sigmoidsinus division whenever possible and jugular tubercle re-section) enhanced the exposure of the deep operative field.
Management of the Vertebral Artery
To drill the occipital condyle safely, the extradural seg-ment of the VA was reflected medially, away from the C-1foramen. After completing the appropriate bone removalfor each approach, the dura was opened, leaving a smalldural cuff around the VA, except in the TFA and the RCA.In those cases the dural entrance of the VA was not ex-posed. In the CTCA, the dura was not opened. This incisionavoids injuring the VA branches that arise extradurally ornear the dural entrance.16,21 It also facilitates the dural clo-sure at the end of the surgery.3
The spinal root of the spinal accessory nerve coursesposterior to the VA. Thus, the posterior transposition of theintradural segment of the VA also mobilizes its branches(posterior inferior cerebellar, anterior spinal, and perforat-ing arteries) and the 11th cranial nerve. This creates a largeworking window to the lower clivus between the 11th cra-nial nerve and C-2 (C-1 was cut) for the removal of thelesion. This window easily exposes the contralateral VA to its dural entrance point and the contralateral 12th cra-nial nerve and C-1 rootlets (Fig. 8D). The VB junction isexposed without perforatoring arteries interposed if thejunction is low or normal in position (Fig. 14C).
Management of the 12th Cranial Nerve
During surgery via the CTCA and ETJA, the 12th crani-al nerve is exposed in the hypoglossal canal and tracedforward for identification and preservation. This techniquealso allowed us, whenever possible, to work around the
E. Salas, et al.
210 J. Neurosurg: Spine / Volume 90 / April, 1999
FIG. 2. Drawing depicting the patient in the lateral position. Thelower arm is supported below the upper end of the table, and theaxilla and other structures are well padded. The dashed line indi-cates a C-shaped incision.
FIG. 3. Imaging studies in a 47-year-old man who had a history of headache, numbness, tingling in his left hand andfingertips, and gait ataxia due to progressive compression of C1–2 spinal cord levels and who underwent surgery via theTFA. He had previously undergone surgery to resect an osteochondroma located in the articular processes of C-1 and C-2 and the body of C-2. Left: Magnetic resonance image and three-dimensional computerized tomography scans. AC1–2 laminectomy had been performed and a biopsy sample had been obtained, but the tumor was not removed. Right:Computerized tomography scan. In our institution, a right TFA (C1–2) was performed, and the tumor was totallyremoved. On the following day, the patient underwent an occipitocervical fusion procedure. At 16 months postopera-

nerve and to visualize the clivus in the midline.During surgery to remove intradural tumors that encase
the 12th cranial nerve, the nerve can be identified distally,in the hypoglossal canal, and traced proximally. When thetumor is placed in, or lateral to, the hypoglossal canal, therootlets of the nerve are identified at their exit from themedulla in the preolivary sulcus and traced distally. Intra-operative monitoring of electromyographic activity fromthe tongue can be useful in identifying and preserving thehypoglossal nerve.
Occipitocervical Fusion
The major factors involved in maintaining the stabil-
ity of the occipitocervical junction are the preservation of the occipital condyle and the C-1 lateral mass, as well aspreservation of the attachments of the alar and transverseligaments to the anterior one third of the occipital condyleand the anterior one third of the C-1 lateral mass. In casesin which the integrity of these structures has been com-promised, as it is via the CTCA and TFA or by tumor de-struction of these areas, an occipitocervical fusion proce-dure becomes necessary.
Fusion is performed as a second-stage operation 1 to 3 days after the initial procedure via the CTCA or TFA,provided there is no cerebrospinal fluid (CSF) effusion. IfCSF effusion is present, then the procedure is delayed for2 to 4 weeks to avoid the risk of a CSF leak or infection.
The fusion procedure is performed with the patient proneand the head is held in pins in a neutral position; this is con-firmed radiographically. Somatosensory evoked potentialmonitoring is maintained throughout the procedure. Thehead, neck, and the posterior iliac crest region are preparedand draped. A midline incision is made from the inion tothe level of C-6. A subperiosteal exposure of the occiputand the upper cervical laminae is obtained. To prepare forfusion, the interspinous ligaments and the flavum ligament
J. Neurosurg: Spine / Volume 90 / April, 1999
Variations of the extreme-lateral craniocervical approach
211
FIG. 4. Photographs of cadaveric specimens on the left side(position as shown in Fig. 2) illustrating aspects of the TFA. A:The opening of the transverse foramina and a C1–2 hemilaminec-tomy have been performed on the left side. The VA has been trans-posed posteriorly and medially, and the posterior one third of thefacets of C-1 and C-2 have been drilled away. The ventral branchof C-2 has been divided to mobilize the VA inferiorly to the levelof C-3 (it is reconstructed at the end of the surgery). An extensionof the drilling to the occipital condyle and superior facet of C-1exposes the foramen magnum. The dura is opened anterior to thecervical roots (dashed line). B: The anterior aspect of the spinalcord is exposed without the interposition of the cervical root, acces-sory nerve, or dentate ligament. C1 = lateral mass of the atlas; C2 =lateral mass of the axis.
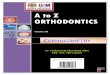
FIG. 5. Magnetic resonance imaging studies in a 39-year-oldman who presented with a 2-year history of numbness and clumsi-ness and who underwent surgery via the RCA. The symptoms be-gan in the right upper extremity and progressed to involve all ex-tremities. Upper: Magnetic resonance imaging revealed a largemass compatible with a meningioma at the anterolateral wall of thelower clivus and foramen magnum; it was shown to encase the leftVA and displace the medulla and the upper cervical spinal cord.Lower: Surgery was performed via a left extreme-lateral RCA, andthe tumor was completely removed. Postoperatively, the patientexperienced 12th cranial nerve paresis, but he recovered complete-ly. At follow-up review, he was doing well, working, and free ofdisease 36 months after the operation.

are removed from the laminae that will be used in the fu-sion. A pneumatic drill is used to place four burr holes inthe suboccipital portion of the skull, which are used for bi-lateral fixation. The laminae, facet joints, and suboccipitalarea are decorticated. Autologous corticocancellous bonegraft is taken from the posterior iliac crest.
A rod-wire construct is used to provide internal fixation.A 3/16-in titanium alloy rod (Sofamor Danek, Memphis,TN) is configured into a U-shaped curve and then bent to conform to the angle of the occipitocervical junction. Titanium cables with an integral crimp (Atlas cable sys-tem; Sofamor Danek) are passed in a sublaminar fashionthrough the levels to be incorporated into the fusion, usual-ly C2–3. The cables are then passed between the burr holesin the suboccipital region bilaterally. The 3/16-in titaniumalloy rod construct is secured with titanium cables into po-sition against the suboccipital bone and the laminae. Afterthe facet joints are packed with cancellous bone graft thecables are tightened to a maximum tension of 30 ft/lb and
crimped. The cancellous bone graft is then placed over the facets, laminae, and suboccipital bone, with the corticalgraft placed more superficially.
Dural Closure
Primary watertight dural closure is essential. However,a fascia lata graft is often required because some shrink-age of the dura occurs during operation. If the dura aroundthe VA entrance was excised because of the tumor inva-sion, the fascial graft is loosely sutured to the adventitia orto the periadventitial tissues of the VA. Fibrin glue is alsoused to achieve a seal. The exposed air cells in the mastoidbone are waxed, and a fat graft is used to fill up the mastoid cavity. The muscle layers are approximated asanatomically correctly as possible. An excessive amountof fat can compress the VA, and this should be avoided. Alumbar drainage catheter placed postoperatively is usefulto allow sealing of the wound without pseudomeningoceleformation if the dural closure is not watertight.
E. Salas, et al.
212 J. Neurosurg: Spine / Volume 90 / April, 1999
FIG. 6. Photographs showing anatomical dissection of the leftsuboccipital region (position as shown in Fig. 2). A: The RCA hasbeen performed. The occipital condyle and atlantooccipital joint (*)have been preserved. The dura is opened in a linear fashion posteri-or to the sigmoid sinus and VA (dashed line). Lesions that are locat-ed in the anterolateral aspect of the foramen magnum displace thebrainstem medially and can be exposed by this approach. B: Thedentate ligament and the C1–2 roots are retracted medially.
FIG. 7. Imaging studies in a 49-year-old woman who had a histo-ry of numbness and tingling involving the upper and lower extremi-ties as well as progressive gait ataxia. Upper: Magnetic resonanceimage leading to the diagnosis of a very large foramen magnummeningioma, slightly more toward the right side, with severe brain-stem compression and right VA encasement and narrowing (upper).The tumor was extremely vascular but could be embolized preop-eratively. The patient underwent surgery via an extreme-lateralapproach with partial drilling of the occipital condyle. The tumorwas completely removed. Lower: Postoperative computerized to-mography scans demonstrated the absence of tumor. The patientmade a complete recovery of her preoperative symptoms, and shewas free of disease 14 months postoperatively. She had returned toher prior occupation as an at-home mother.

Postoperative Care
Patients were observed postoperatively particularly forlower cranial nerve problems, respiratory difficulties, andCSF leakage or effusion. Swallowing and coughing dif-ficulty may be present because of ninth and 10th cranialnerve paresis. This condition can be aggravated by 12th cra-nial nerve palsy. Unilateral ninth and 10th cranial nervepalsy can be managed by performing an arytenoid adduc-tion procedure and a percutaneous gastrostomy or jejunos-tomy, if necessary. Bilateral palsy of ninth and 10th cranialnerves will require a tracheostomy and jejunostomy. Be-cause the brainstem may be dysfunctional postoperatively,patients are carefully monitored for sleep apnea or hypo-ventilation. If a ventriculostomy was performed preopera-tively, a permanent postoperative shunt may eventually berequired.
Results
Gross-total removal was achieved in 35 (69%) and subto-
tal removal in 16 (31%) of the 51 patients who harboredtumors. Gross-total removal of the lesions was achieved in100% of patients undergoing the TFA, 80% undergoing theRCA, and 78% undergoing the ETJA. In patients in whomsurgery was performed via PTCA and CTCA, total removalwas accomplished in 66% and 46%, respectively. However,these groups contained a higher percentage of patients whohad undergone previous treatment.
Gross-total removal was achieved in 16 (66%) of the 24patients with meningioma, four (40%) of the 10 patientswith chordoma, seven (100%) of the patients with paragan-glioma, two (66%) of the three patients with schwannoma,and one (50%) of the two patients with chondrosarcoma.Subtotal removal was achieved in eight (33%) of thepatients with meningioma, six (60%) of the patients withchordoma, one patient with chondrosarcoma, and one pa-tient with schwannoma. Gross-total removal was achievedin the eight remaining patients who harbored differenttypes of neoplastic lesions (Table 3). Four patients in whom
J. Neurosurg: Spine / Volume 90 / April, 1999
Variations of the extreme-lateral craniocervical approach
213
FIG. 8. Photographs illustrating aspects of the PTCA. A: During surgery via the PTCA the mastoid process is removed, the sigmoid sinusunroofed, and the VA transposed medially. The atlantooccipital joint is exposed (left side, same position as in Fig. 2). B: The posterior onethird of the C-1 lateral mass and occipital condyle was drilled until the intracranial opening of the hypoglossal canal was exposed. The duralincision, with a cuff around the VA entrance point, is indicated by the dashed line. C: Intradural view before VA mobilization. The VA,PICA, and perforating branches to the brainstem as well as the 10th and 11th cranial nerve, and C-1 and C-2 roots are exposed. D: The VAand its branches have been transposed posteriorly. The opposite VA and the anterior aspect of the spinomedullary junction and foramen magnum have been exposed without neural retraction. Ant. = anterior; CN = cranial nerve; IJV = internal jugular vein; opp. = opposite side;SCM m. = sternocleidomastoid muscle.

subtotal tumor resection was achieved underwent postoper-ative gamma knife therapy, and two patients received che-motherapy.
The TTA was performed only in those patients with VAand VB junction aneurysms. In seven patients, the aneurysmswere successfully clipped. Three of the remaining five pa-tients with fusiform or dissecting aneurysms underwent avein graft bypass procedure from the extradural to the in-tradural VA because of the dominance of the affected VA andbecause the parent artery could not be preserved.19 The othertwo patients, in whom the contralateral VA was larger orequal in size, underwent trapping of the aneurysm without abypass procedure and the reimplantation of the posterior infe-rior cerebellar artery (PICA) (Table 4).
Occipitocervical Fusion
Fifteen patients underwent occipitocervical fusion, 11(85%) of them after the CTCA, two (50%) after the TFA,and two (11%) after the PTCA. All patients who harboredchordomas and chondrosarcomas underwent an occipito-cervical fusion (Table 5).
In our series drilling of the posterior one third or one halfof the occipital condyle did not cause spinal instability. Ofthe two patients who required an occipitocervical fusion af-ter surgery via the PTCA, one also had preoperative C1–2subluxation and the other, who harbored a hemangiopericy-toma, had extensive weakening of the condyle secondary tobone invasion by tumor.
Treatment Complications
The most frequent complications were hydrocephalus innine patients (in eight patients a ventriculoperitoneal shuntwas placed and in one patient the hydrocephalus resolvedwithout treatment) and CSF leakage in seven patients (fivewere treated with lumbar drainage, and two required re-vision and duraplasty with pericranial or fascia lata graft).The highest incidence of cranial nerve morbidity was inpatients with lesions that required the PTCA. Seven pa-tients sustained a cranial nerve deficit; four experienced12th cranial nerve palsy and three had ninth to 11th cranial
E. Salas, et al.
214 J. Neurosurg: Spine / Volume 90 / April, 1999
FIG. 9. Magnetic resonance imaging studies in a 19-year-old woman who presented with a 1-year history of neck painand who underwent sugery via a CTCA. Left: Imaging revealed a large clival mass that involved the right occipitalcondyle, both intra- and extradural, producing significant mass effect and displacement of the medulla and cervical cord.Right: Postoperative images. She underwent surgery via an extreme-lateral approach with complete removal of the boneinfiltrated by the tumor (occipital condyle, clivus, and lateral mass). The diagnosis was chordoma, and there was no duralinvasion by the tumor. An occiput/C2–3 fusion was performed the next day. After 2 months of follow up she was doing welland had returned to her college studies.
TABLE 3Results of surgery in 51 patients who harbored various tumors
Total Subtotal Follow-upNo. of Removal Removal Period
Type of Lesion Patients (%) (%) (mos)
meningioma 24 66 33 14.8chordoma 10 40 60 23.7chondrosarcoma 2 50 50 15neurofibroma 2 100 0 10.2schwannoma 3 66 33 12.5paraganglioma 7 100 0 38hemangiopericytoma 1 100 0 14osteochondroma 1 100 0 16metastatic carcinoma* 1 100 0 9.5
* Patient died of multiple metastases in other locations.

palsy. However, in all of these patients, arytenoid adductionand thyroplasty allowed them to overcome their swallow-ing and coughing difficulties.
Two patients suffered serious complications, which couldnot be adequately treated. One patient, who harbored a re-current foramen magnum meningioma and who had under-gone three previous operations, underwent resection of herrecurrent tumor; there was initial improvement of her dis-abled condition. On postoperative Day 3, she suffered a cli-val epidural hemorrhage that was successfully evacuated.However, 5 days postoperatively she suffered severe neu-rological deterioration due to cerebellar infarction caused by severe vasospasm of the VB arteries, requiring angio-plasty and hypertensive, hypervolemic, and hemodilutionaltherapy. Because of delayed recognition and treatment ofthe vasospasm, her condition did not improve, and she re-mained severely disabled. Another patient, who harboredan extensive chordoma and who had previously undergoneboth surgery and proton-beam radiotherapy, suffered sig-moid sinus thrombosis with severe cerebellar and brainstemedema on the 1st postoperative day; she became comatose.The sinus could not be reopened despite attempted intravas-
cular thrombolysis, and this patient died (Table 6).
Outcome Results
The mean preoperative Karnofsky Performance Scale11
(KPS) score was 74.7 (standard deviation � 4.64), and post-operatively, considering the last follow up, it was 76.4 (�4.33). The mean follow-up period was 18.2 months (range1–50 months). The mean KPS score in TTA- and RCA-treated patients significantly improved. In CTCA- andETJA-treated patients, the mean KPS score decreasedslightly (Table 7).
Discussion
Hammon and colleagues9 in 1972 and Heros10 in 1986described a lateral suboccipital approach that was used as aninitial attempt to perform a more lateral suboccipital expo-sure for VA and VB aneurysms.9,10 Since then the extreme-lateral craniocervical approach has been progressively de-veloped as a more and more lateral approach to provide
J. Neurosurg: Spine / Volume 90 / April, 1999
Variations of the extreme-lateral craniocervical approach
215
FIG. 11. Magnetic resonance (upper) and computerized tomog-raphy studies (lower) obtained in a 56-year-old man who sufferedfor several months from right-sided tongue paralysis and a morerecent onset of vocal cord paresis, manifested by a hoarse voice; he underwent surgery via the ETJA. Preoperative imaging studiesrevealed a very large tumor extending from the right jugular fora-men inferiorly into the parapharyngeal space (upper). The lesionwas exposed via the ETJA. A schwannoma originating from thehypoglossal nerve was completely removed (lower). The patientrequired postoperative thyroplasty and arytenoid adduction to reha-bilitate his vocal cord palsy. He returned to work and was free ofdisease after 26 months of follow up.
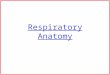
FIG. 10. Photographs of a cadaveric dissection on the left side(position as shown in Fig. 2) illustating several aspects of theCTCA. A: The hypoglossal canal has been exposed and skele-tonized. The drilling of the jugular tubercle and the occipital con-dyle exposes the middle clivus. B: Removal of the C-1 lateralmass exposes the lower clivus and the odontoid process of C-2.

access to lesions in the midline on the anterior aspect of theforamen magnum.3,4,6,15,18,22–24 However, it has been pointedout that the surgeon should be judicious in choosing an ap-proach to cranial base lesions to avoid unnecessary surgery(M Samii, personal communication, 1997).
The anatomy of bony structures, the VA, sigmoid sinus,jugular bulb, the ninth through 12th cranial nerves, and the C1–2 level determine the access gained through lateralapproaches to the medulla, upper cervical spinal cord, andthe craniocervical bony structures.
With regard to the neural structures, the C-1 root can becut without apparent adverse effects. Lateral approaches to intradural structures are performed through windows be-tween the exit points of ninth and 12th cranial nerves andC-2. The surgeon may also work between rootlets of the10th and 11th cranial nerve. Because the 12th cranial nerveis located more medially, in practice a large window existsbetween the 11th cranial nerve and C-2. However, the VAcrosses from lateral to medial in this space.
Some authors report the partial drilling of the occipitalcondyle and jugular tubercle for VA and VB aneurysmswithout medial mobilization of the intradural VA.5,12 Thedura is reflected laterally, carrying with it the inferior por-tion of the sigmoid sinus and achieving a parallel sight tothe intracranial course of the VA without brainstem retrac-tion.5 Nevertheless, to reach the VB junction and the areadirectly anterior to the spinomedullary junction, it is neces-sary to work between the 11th and 12th cranial nerves andthe VA. This technique is associated with a higher inci-dence of injury to the lower cranial nerves as well as therisk of injury to the VA or its branches.5,12 Therefore, in ourseries, mobilizing the VA medially from approximately C-2 to the VB junction created a larger exposure. This tech-nique allowed us to use this window to visualize the VBjunction and to work anterior to the ninth through 12th cra-nial nerves.3,26 On the other hand, in patients with tumors lo-cated lateral, or anterolateral, to the spinomedullary areas,much more mobilization is unnecessary.
The bony structures that lie directly lateral to the clivusand the anterior aspect of C-1 and C-2 include the mastoidprocess, jugular tubercle, the occipital condyle, the lateralmass of C-1, and the facets and lateral masses of C-2 andC-3 vertebrae. More direct lateral approaches to this area
E. Salas, et al.
216 J. Neurosurg: Spine / Volume 90 / April, 1999
FIG. 12. Photographs of an anatomical dissection on the left side(position as shown in Fig. 2) illustrating aspects of the ETJA. A:During the approach, the mastoidectomy has been extended to thejugular bulb, exposing its lateral aspect. B: The lateral mass of C-1 has been removed and the VA has been transposed medially. Theoccipital condyle has been drilled away until the entire hypoglos-sal canal is exposed. An approach to the jugular foramen is nowpossible from a lateral and posteroinferior direction. The additionof the subtemporal–infratemporal approach will facilitate an ante-rior approach as well, if needed. ICA = internal carotid artery.
FIG. 13. Imaging studies performed in a 61-year-old man whohad a history of sudden onset of multiple VB transient ischemicattacks approximately 1 year previously and who underwent surgery via a TCA. The diagnosis was that of a large fusiform aneurysm of the dominant left VA. Upper: Three-dimensionalcomputerized tomography scan and angiogram. The left PICA wasarising from the aneurysm, but the PICA on the right side wasmarkedly dominant. A left extreme-lateral TCA was combinedwith a pre- and retrosigmoid craniotomy and transsigmoid sinusapproach. Lower: Three-dimensional computerized tomographyscan and angiogram. The aneurysm was resected, and a vein graftprocedure was performed from the extra- to intradural VA. Thepatient experienced swallowing difficulty postoperatively becauseof ninth and 10th cranial nerve paresis, and an arytenoid adductionprocedure and a percutaneous jejunostomy were performed. Thepercutaneous jejunostomy was removed after 2 months. At follow-up review 10 months postoperatively, the patient had returned towork and had no neurological deficits.

require the removal of these bony elements and judgmentmust be balanced against the extent of surgery and the needfor fusion because bony elements critical for spinal stabili-ty are removed. A partial mastoidectomy exposes the sig-moid sinus and makes possible its mobilization. In many
reports this step has not been taken.4,24 The sigmoid sinusinitially lies posterior to the anterior surface of the pons andmedulla, but it moves more anteriorly as it travels inferior-ly in such a way that the jugular bulb is slightly anterior tothe anterior surface of the medulla. Thus, approaches to theupper cervical cord and the craniocervical junction do notrequire the mobilization of the jugular bulb; however, inapproaches to the anterior surface of the upper medulla orthe pontomedullary junction area, sigmoid sinus manage-ment becomes an important factor. Pre- and retrosigmoidsinus approaches with mobilization of the sinus or its divi-sion (whenever possible) are useful.
Other surgeons who perform lateral approaches to thecraniocervical junction area have recognized the value ofclassifying the approaches according to the respective dis-ease process. In one report Babu and colleagues3 discuss thenecessity and disadvantages of the transcondylar approach,pointing out that the extent of occipital condyle resectioncan be varied according to the specific needs of the case.3Samii, et al.,17 in a series of 38 patients with 40 meningi-
J. Neurosurg: Spine / Volume 90 / April, 1999
Variations of the extreme-lateral craniocervical approach
217
FIG. 14. Photographs demonstrating aspects of surgery via thePTA. A: During the transtubercular approach, drilling of the pos-terior one third of the occipital condyle (left side, same position asin Fig. 2) has exposed the intracranial opening of the hypoglossalcanal. The jugular tubercle (arrow) has been removed extradurallyas much as possible. B: The retrosigmoid dura has been opened.The remaining part of the jugular tubercle impedes the view of theclivus and VB junction. C: The remaining jugular tubercle hasbeen drilled away intradurally. The distal VA and the VB junction
TABLE 4Location and treatment of aneurysms in 12 patients who
underwent surgery*
Treatment
Trapping Trapping Case No. Location Clipping w/ Graft w/o Graft
1† VB junction(fenestrated BA) +
2† VB junction +3‡ VB junction +4 VA-saccular +5 VA-saccular +6† VA-saccular +7 VA-saccular +8 VA-saccular +9† VA-fusiform +
10 VA-fusiform +11§ VA-dissecting +12§ VA-dissecting +
* BA = basilar artery; + = procedure performed.† The sigmoid sinus was divided and reconstructured at the end of the
operation. ‡ This patient was described in a case report published by Sekhar, et al.§ In these cases the posterior inferior cerebellar artery was reimplant-
ed to VA.
TABLE 5Number of patients undergoing surgery via an extreme-lateral
craniocervical approach who also underwent an occipitocervical fusion procedure
No. of No. of FusionApproach Patients Procedures (%)
TFA 4 2 (50)RCA 11 0PTCA 18 2 (11)CTCA 13 11 (85)ETJA 14 0TTA 9 0total 69 15 (22)

omas of the craniocervical junction, performed a partialdrilling of the occipital condyle in only seven patients andan RCA in 33 patients. They achieved total removal of tu-mors in 63% of the patients. George and Lot7 performed sur-geries via three different approaches to C-1 and C-2 neu-rinomas. They described the posterior, the posterolateral, and the anterolateral approaches, according to the extent ofbone removal needed. In a detailed anatomical study, Wenand colleagues26 have described the trans-, supra-, and para-condylar extensions of the far-lateral approach.
Occipitocervical Fusion
The extreme-lateral craniocervical approach may requirean occipitocervical fusion procedure depending on the ex-tent of bone removal.1,4,23 In our experience in performing the CTCA, postoperative fusion was needed. Patients under-going the TFA require fusion only when removal of the pos-terior half or more of the facets is performed.
During the CTCA, if both condyles are invaded by thetumor, a fusion procedure is performed during the firststage. A few months later, after the fusion has matured, thecontralateral side can be surgically treated.21
Conclusions
Six variations of the extreme-lateral craniocervical ap-proach are described. The tailoring of the approach to eachspecific lesion avoids unnecessary surgery while providingthe needed exposure. Anteriorly and anterolaterally locatedlesions in the craniocervical area can be better exposed viathese approaches, resulting in positive outcomes and mini-mal complications. An occipitocervical fusion is requiredwhen the entire occipital condyle, C-1 lateral mass, or cer-vical facets are removed or when the lesion has destroyedthe contralateral condyle.
Acknowledgments
The authors wish to thank Jennifer Pryll for her talented workwith the illustrations and Amal Nadel and James Agee for their con-stant technical support.
References
1. Al-Mefty O, Borba LA, Aoky N, et al: The transcondylar ap-proach to extradural nonneoplastic lesions of the cranioverte-bral junction. J Neurosurg 84:1–6, 1996
2. Arnold H, Sepehrnia A: Extreme lateral transcondylar ap-proach. J Neurosurg 82:313–314, 1995 (Letter)
3. Babu RP, Sekhar LN, Wright DC: Extreme lateral transcondy-lar approach: technical improvements and lessons learned. JNeurosurg 81:49–59, 1994
4. Bertalanffy H, Seeger W: The dorsolateral, suboccipital, trans-condylar approach to the lower clivus and anterior portion ofthe craniocervical junction. Neurosurgery 29:815–821, 1991
5. Day JD, Fukushima T, Giannotta SL: Cranial base approaches toposterior circulation aneurysms. J Neurosurg 87:544–554, 1997
6. George B, Dematons C, Cophignon J: Lateral approach to theanterior portion of the foramen magnum. Application to surgi-cal removal of 14 benign tumors: technical note. Surg Neurol29:484–490, 1988
7. George B, Lot G: Neurinomas of the first two cervical nerveroots: a series of 42 cases. J Neurosurg 82:917–923, 1995
8. George B, Lot G, Tran Ba Huy P: The juxtacondylar approachto the jugular foramen (without petrous bone drilling). SurgNeurol 44:279–284, 1995
9. Hammon WM, Col MC, Kempe LG: The posterior fossa ap-proach to aneurysms of the vertebral and basilar arteries. J Neu-
E. Salas, et al.
218 J. Neurosurg: Spine / Volume 90 / April, 1999
TABLE 6Postoperative Complications*
Extreme-Lateral Craniocervical Approach
TFA RCA PTCA CTCA ETJA TTA TotalComplication (4 pts) (11 pts) (18 pts) (13 pts) (14 pts) (9 pts) (%)
CSF leak 0 0 4 2 1 0 10CNS infection 0 0 2 1 2 0 7hematoma 0 1 0 0 1 0 3contusion
(cerebellar) 0 0 0 1 0 0 1brain swelling 0 1 0 0 0 1 3vasospasm 0 0 0 0 1 0 1SS thrombosis & death 0 0 0 1 0 0 1hydrocephalus 0 1 4 1 3 0 13cranial nerve worsening 0 0 3 1 3 0 10
* One patient had a suboccipital epidural and one patient a temporal lobe hematoma. Abbreviations: CNS = central nervous system;SS = sigmoid sinus.
TABLE 7Outcome based on Karnofsky Performance Scale score*
KPS ScoreNo. of
Approach Patients Preop Postop
TFA 4 85 85RCA 11 70 82PTCA 18 75.2 76.2CTCA 13 79 72ELTJA 14 76 72TTA 9 67 80overall mean score 74.7 � 4.64 76.4 � 4.33
* Value is expressed as the mean � standard deviation. Abbreviation:KPS = Karnofsky Performance Scale.

rosurg 37:339–347, 197210. Heros RC: Lateral suboccipital approach for vertebral and ver-
tebrobasilar artery lesions. J Neurosurg 64:559–562, 198611. Karnofsky DA, Burchenal JH: The clinical evaluation of che-
motherapeutic agents in cancer, in MacLeod CM (ed): Eval-uation of Chemotherapeutic Agents. New York: ColumbiaUniversity Press, 1949, pp 191–205
12. Kawase T, Bertalanffy H, Otani M, et al: Surgical approachesfor vertebro-basilar trunk aneurysms located in the midline. Ac-ta Neurochir 138:402–410, 1996
13. Lanzino G, Sekhar LN, Hirsch WL, et al: Chordomas and chon-drosarcomas involving the cavernous sinus: review of surgi-cal treatment and outcome in 31 patients. Surg Neurol 40:359–371, 1993
14. Patel SJ, Sekhar LN, Cass SP, et al: Combined approaches forresection of extensive glomus jugulare tumors: a review of 12cases. J Neurosurg 80:1026–1038, 1994
15. Perneczky A: The posterolateral approach to the foramen mag-num, in Samii M (ed): Surgery in and Around the BrainStem and the Third Ventricle. Berlin: Springer-Verlag, 1986,pp 460–466
16. Salas E, Ziyal IM, Bank WO, et al: Extradural origin of the posteroinferior cerebellar artery: an anatomical study withhistological and radiographic correlation. Neurosurgery 42:1326–1331, 1998
17. Samii M, Klekamp J, Carvalho G: Surgical results for me-ningiomas of the craniocervical junction. Neurosurgery 39:1086–1095, 1996
18. Seeger W: Atlas of Topographical Anatomy of the Brain and Surrounding Structures. Wien: Springer-Verlag, 1978,pp 486–489
19. Sekhar LN, Chandler JP, Alyono D: Saphenous vein graft re-construction of an unclippable giant basilar artery aneurysmperformed with the patient under deep hypothermic circulatoryarrest: technical case report. Neurosurgery 42:667–673, 1998
20. Sekhar LN, Tzortzidis FN, Bejjani GK, et al: Saphenous veingraft bypass of the sigmoid sinus and jugular bulb during theremoval of glomus jugulare tumors: report of two cases. JNeurosurg 86:1036–1041, 1997
21. Sekhar LN, Tzortzidis F, Salas E: Extreme lateral retrocondy-lar and transcondylar approaches and combined approaches, in Sekhar LN, de Oliveira E (eds): Cranial Microsurgery—Approaches and Technique. New York: Thieme, 1998, pp464–481
22. Sen CN, Sekhar LN: An extreme lateral approach to intradurallesions of the cervical spine and foramen magnum. Neuro-surgery 27:197–204, 1990
23. Sen CN, Sekhar LN: Surgical management of anteriorly placedlesions at the craniocervical junction—an alternative approach.Acta Neurochir 108:70–77, 1991
24. Spetzler RF, Grahm TW: The far-lateral approach to the inferi-or clivus and the upper cervical region: technical note. BNIQuart 6:35–38, 1990
25. Spetzler RF, Daspit CP, Pappas CTE: The combined supra- andinfratentorial approach for lesions of the petrous and clivalregions: experience with 46 cases. J Neurosurg 76:588–599,
J. Neurosurg: Spine / Volume 90 / April, 1999
Variations of the extreme-lateral craniocervical approach
219