Embed Size (px)
Citation preview
Valvular Flow Abnormalities Are Often Identifiedby a Resting Focused Doppler Examination
Performed at the Time of Stress Echocardiography
Abhishek Gaur, MD, Susan B. Yeon, MD, Christopher W. Lewis, MD, Warren J. Manning, MD
BACKGROUND: Patients are usually referred for stress echo-cardiography to assess whether there is inducible myocardialischemia. At some centers, a focused Doppler examination isalso performed. We sought to determine the clinical value ofthis additional study by examining how often valvular flow ab-normalities were identified that might affect clinical care.METHODS: We reviewed 1272 consecutive stress echocardio-gram reports from a 1-year period, including 1223 tests thatcontained focused Doppler data. Important Doppler findingswere defined as at least moderate mitral regurgitation, at leastmild aortic regurgitation, any aortic or mitral valve stenosis, orany resting left ventricular outflow tract gradient.RESULTS: Overall, focused Doppler identified an importantDoppler abnormality in 214 patients (17%). At least moderatemitral regurgitation was identified in 67 patients (5%) and atleast mild aortic regurgitation was identified in 163 patients(13%). In addition, aortic stenosis (n � 14; 1%), mitral stenosis
(n � 5; 0.4%), and resting outflow tract gradient (n � 2; 0.2%)were noted. A prior echocardiogram had been performed at ourinstitution in 317 patients (26%). For this subset, a new impor-tant Doppler finding, a two-step change in regurgitant grade, ora one-step change in stenosis severity was noted in 28 patients(9%). Among patients who had a previous study, the prevalenceof new findings was the same (9%) in those who had been stud-ied within the previous year as in those whose previous studyhad been performed more than 2 years before.CONCLUSION: Focused Doppler documents valvular flowabnormalities in 17% of patients referred for stress echocardi-ography, thereby enhancing the potential overall value of thetest. The frequency of new findings was independent of the timeinterval from the previous Doppler study. These data should beconsidered when clinicians choose a stress imagingmodality. Am J Med. 2003;114:20 –24. ©2003 by ExcerptaMedica Inc.
Surface echocardiography is the most common im-aging procedure used in clinical cardiology (1). Ex-ercise or dobutamine stress echocardiography is
performed commonly in the noninvasive evaluation ofpatients with suspected coronary artery disease (2,3). Al-though coronary artery disease may explain symptoms ofchest pain or dyspnea, other cardiovascular conditions,such as valvular dysfunction or an obstructive cardiomy-opathy, may coexist (4) or be the primary disease process.Echocardiographic data are also a determinant for theneed for antibiotic prophylaxis (5).
Resting and postexercise regional and global myocar-dial contractility are assessed routinely during a conven-tional stress echocardiogram. Doppler examination is notrecommended specifically (6), nor is its value empha-sized, when considering stress echocardiography or nu-clear imaging (7). At our center, a resting focused Dopp-ler examination is performed routinely at the time ofstress echocardiography. We sought to examine the po-tential clinical value of the additional study by determin-
ing the frequency of new Doppler findings that mightaffect clinical care.
METHODS
Focused Doppler ExaminationAt our institution, the focused Doppler examination con-sists of brief (5 to 10 seconds per view) color flow Dopplerinterrogations of mitral and aortic valve flow in theparasternal long axis, and in the apical four-chamber,five-chamber, and three-chamber long-axis views. In ad-dition, pulsed Doppler is performed along the interven-tricular septum and into the left ventricular outflow tractto look for a resting outflow tract gradient, and again atthe tips of the mitral leaflets. Continuous wave Doppler isperformed in the apical five-chamber view across the aor-tic valve. All studies were performed on Sonos 2500, 5000,or 5500 units (Philips Medical Systems, Andover, Massa-chusetts). Data were recorded on videotape and reviewedby clinical staff, all of whom have passed the AmericanSociety of Echocardiography Special Competency Exam-ination in Echocardiography.
Study DesignStress echocardiography reports from all 1272 patients atour institution who underwent physiologic or pharma-cologic examinations from December 1, 1999, to Novem-ber 30, 2000, were reviewed. Patient characteristics, aswell as clinical indications for the stress test, were re-
From the Harvard-Thorndike Laboratory of the Department of Medi-cine, Cardiovascular Division, Beth Israel Deaconess Medical Center,Harvard Medical School, Boston, Massachusetts.
Requests for reprints should be addressed to Warren J. Manning,MD, Beth Israel Deaconess Medical Center, 330 Brookline Avenue, Bos-ton, Massachusetts 02215, or [email protected].
Manuscript submitted December 31, 2001, and accepted in revisedform August 5, 2002.
20 ©2003 by Excerpta Medica Inc. 0002-9343/03/$–see front matterAll rights reserved. doi: 10.1016/S0002-9343(02)01381-5
corded. Severity of mitral regurgitation and aortic regur-gitation were reported as none, trace, mild (1�), mild tomoderate (1 to 2�), moderate (2�), moderate to severe(3�), or severe (4�). Aortic stenosis was diagnosed as apeak transaortic gradient �2 m/s. The presence of a leftventricular outflow tract gradient �2 m/s or mitral ste-nosis (valve area �2.0 cm2) was also recorded.
The resting left ventricular systolic function was esti-mated visually and categorized as normal (ejection frac-tion �55%), mildly depressed (ejection fraction, 40% to54%), moderately depressed (ejection fraction, 30% to39%), or severely depressed (ejection fraction �30%).Left ventricular systolic dysfunction was defined as anejection fraction �55%, or if regional dysfunction wasnoted, as an ejection fraction �55%. The presence of in-ducible ischemia was also recorded.
All inpatient and outpatient echocardiographic studiesfor the past 14 years are recorded in an electronic data-base. If the patient had a prior study at our institution, theDoppler findings were compared with the index study.An “important change” in the severity of valvular regur-gitation was defined as a new diagnosis of at least moder-ate mitral regurgitation or at least mild aortic regurgita-tion, or a two-step change in regurgitant severity. An “im-portant change” in the severity of aortic or mitral stenosiswas defined as a new diagnosis or a one-step change instenosis severity. The study was approved by the hospitalCommittee on Clinical Investigation, which waived therequirement for informed consent.
StatisticsComparisons of proportions were made using chi-squared statistics, or tests for trend. Statistical signifi-cance was set at P �0.05.
RESULTS
Of the 1272 patients who underwent stress echocardiog-raphy, 1223 (96%) had Doppler data reported (Table 1).This included 1108 patients (91%) who underwent exer-cise stress testing and 115 (9%) who underwent dobut-amine stress testing. Resting left ventricular systolic dys-function was present in 209 patients (17%). Chest pain orevaluation for coronary artery disease was the predomi-nant (71%) indication for stress testing. Stress echocardi-ography demonstrated inducible ischemia in 89 patients(8%).
Mitral and Aortic RegurgitationValvular regurgitation was the most common Dopplerabnormality, with at least moderate mitral regurgitationor at least mild aortic regurgitation noted in 204 patients(17%) (Table 2). At least moderate mitral regurgitationand at least mild aortic regurgitation was present in 26
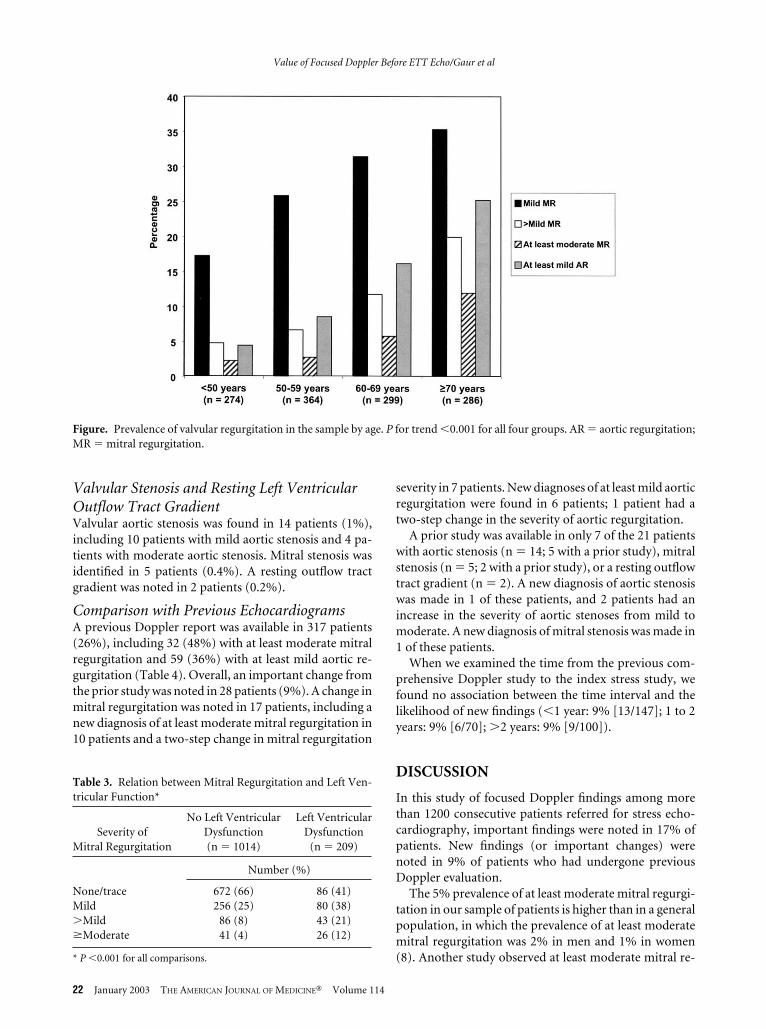
patients (2%). The prevalence of mitral regurgitation in-creased progressively with age (P �0.001; Figure).Among patients older than 50 years, 61 (5%) had at leastmoderate mitral regurgitation. At least moderate mitralregurgitation was almost three times more common(12% vs. 4%) than among those with normal function(Table 3).
Focused Doppler demonstrated at least mild aortic re-gurgitation in 163 patients (13%) (Table 2), with 28 (2%)having greater than mild aortic regurgitation. The preva-lence of aortic regurgitation also increased with age (Fig-ure; P �0.001). The prevalence of at least mild aorticregurgitation was four times higher (16% [151/949] vs.4% [12/274], P �0.001) among those 50 years of age orolder than among younger patients.
Table 1. Characteristics of the 1223 Patients Who UnderwentStress Echocardiography with Focused Doppler Examinations
CharacteristicNumber (%) or
Mean � SD
Age (years) 59 � 13Female sex 619 (51)Resting left ventricular function
Normal (ejection fraction �55%) 1014 (84)Mildly depressed (ejection fraction, 40%
to 54%)142 (12)
Moderately depressed (ejection fraction,30% to 39%)
40 (3)
Severely depressed (ejection fraction�30%)
27 (2)
Indications for stress testChest pain/coronary artery disease 866 (71)Dyspnea 122 (10)Syncope/presyncope 34 (3)Arrhythmia 74 (6)Others 127 (10)
Table 2. Severity of Valvular Regurgitation in the 1223 Patients
SeverityMitral
RegurgitationAortic
Regurgitation
Number (%)
None/trace 758 (62) 1060 (87)Mild 336 (28) 135 (11)Mild-moderate 62 (5) 16 (1)Moderate 50 (4) 11 (1)Moderate-severe 15 (1) 0Severe 2 (0.2) 1 (0.1)
�Mild 465 (38) 163 (13)�Mild 129 (11) 28 (2)�Moderate 67 (5) 12 (1)
Value of Focused Doppler Before ETT Echo/Gaur et al
January 2003 THE AMERICAN JOURNAL OF MEDICINE� Volume 114 21
Valvular Stenosis and Resting Left VentricularOutflow Tract GradientValvular aortic stenosis was found in 14 patients (1%),including 10 patients with mild aortic stenosis and 4 pa-tients with moderate aortic stenosis. Mitral stenosis wasidentified in 5 patients (0.4%). A resting outflow tractgradient was noted in 2 patients (0.2%).
Comparison with Previous EchocardiogramsA previous Doppler report was available in 317 patients(26%), including 32 (48%) with at least moderate mitralregurgitation and 59 (36%) with at least mild aortic re-gurgitation (Table 4). Overall, an important change fromthe prior study was noted in 28 patients (9%). A change inmitral regurgitation was noted in 17 patients, including anew diagnosis of at least moderate mitral regurgitation in10 patients and a two-step change in mitral regurgitation
severity in 7 patients. New diagnoses of at least mild aorticregurgitation were found in 6 patients; 1 patient had atwo-step change in the severity of aortic regurgitation.
A prior study was available in only 7 of the 21 patientswith aortic stenosis (n � 14; 5 with a prior study), mitralstenosis (n � 5; 2 with a prior study), or a resting outflowtract gradient (n � 2). A new diagnosis of aortic stenosiswas made in 1 of these patients, and 2 patients had anincrease in the severity of aortic stenoses from mild tomoderate. A new diagnosis of mitral stenosis was made in1 of these patients.
When we examined the time from the previous com-prehensive Doppler study to the index stress study, wefound no association between the time interval and thelikelihood of new findings (�1 year: 9% [13/147]; 1 to 2years: 9% [6/70]; �2 years: 9% [9/100]).
DISCUSSION
In this study of focused Doppler findings among morethan 1200 consecutive patients referred for stress echo-cardiography, important findings were noted in 17% ofpatients. New findings (or important changes) werenoted in 9% of patients who had undergone previousDoppler evaluation.
The 5% prevalence of at least moderate mitral regurgi-tation in our sample of patients is higher than in a generalpopulation, in which the prevalence of at least moderatemitral regurgitation was 2% in men and 1% in women(8). Another study observed at least moderate mitral re-
Table 3. Relation between Mitral Regurgitation and Left Ven-tricular Function*
Severity ofMitral Regurgitation
No Left VentricularDysfunction(n � 1014)
Left VentricularDysfunction
(n � 209)
Number (%)
None/trace 672 (66) 86 (41)Mild 256 (25) 80 (38)�Mild 86 (8) 43 (21)�Moderate 41 (4) 26 (12)
* P �0.001 for all comparisons.
Figure. Prevalence of valvular regurgitation in the sample by age. P for trend �0.001 for all four groups. AR � aortic regurgitation;MR � mitral regurgitation.
Value of Focused Doppler Before ETT Echo/Gaur et al
22 January 2003 THE AMERICAN JOURNAL OF MEDICINE� Volume 114

gurgitation in 2.1% of subjects (9). Our finding likelyreflects referral bias among patients who undergo stressechocardiography, as left ventricular dysfunction is morecommon in these patients. Our data are consistent with asmaller study among patients referred for exercise echo-cardiography, in which 27% had mild regurgitation, 5%had moderate regurgitation, and 1% had severe regurgi-tation at rest (10). Among patients referred for nonemer-gent transthoracic echocardiography, Krumholtz andcolleagues (11) reported that 18% of patients had at leastmoderate mitral regurgitation. In that study, however,the two most common indications for the study wereevaluation of valve dysfunction and left ventricular sys-tolic function. In our study, 17% of patients had left ven-tricular systolic dysfunction, and mitral regurgitation wasmore common in these patients, consistent with previousresults (9).
Fleischmann and coworkers (12,13) evaluated the roleof Doppler echocardiography among patients presentingwith chest pain. Mitral regurgitation and moderate-to-severe left ventricular systolic dysfunction were indepen-dent predictors of subsequent mortality. In another studyof patients with coronary artery disease and pulmonaryedema (14), about two thirds had at least mild-moderateregurgitation. Thus, mitral regurgitation detected by fo-cused Doppler examination may provide additionalprognostic information in patients with coronary arterydisease and left ventricular systolic dysfunction.
We found aortic regurgitation (mild or greater) in 13%of the patients, similar to the 10% prevalence in theStrong Heart Study (15) and the 11% prevalence of atleast trace aortic regurgitation in the Framingham off-spring study (8). Unlike mitral regurgitation, we foundno association between aortic regurgitation and left ven-tricular systolic dysfunction. Both mitral and aortic re-gurgitation were more common with advancing age(8,9,15,16). The prevalence of hypertrophic cardiomyop-athy in the general population is about 0.2% (17), similarto our findings. In these patients, caution is needed dur-ing exercise or dobutamine infusion, as worsening ob-struction and exercise-induced hypotension may de-velop.
The concept of limited echocardiographic imaging hasbeen applied to screening for left ventricular hypertrophyin hypertension (18), mitral valve prolapse (19), pericar-
dial effusion (20), and suspected cardiac embolism (20).Using this strategy, most major cardiac disorders can beexcluded. If an important finding is seen, a comprehen-sive examination can be performed expeditiously (21). Ina busy laboratory, with patients scheduled every 45 to 60minutes, it is not usually possible to alter the schedule tocomplete the stress echocardiogram and perform a com-prehensive resting Doppler and two-dimensional exam-ination. A focused Doppler study to screen for valvulardysfunction can be completed in only 2 to 3 minutes.After the introduction of this strategy at our institution 2years ago, we continued to schedule patients for stressechocardiography at similar (45-minute) time intervals.As implemented at our institution, the focused Dopplerexamination does not include M-mode or detailed two-dimensional assessment of valvular morphology, nordoes it include all the views obtained during a compre-hensive evaluation (e.g., parasternal short-axis views ofthe aortic and mitral valves; magnified/zoom two-dimen-sional imaging of the aortic and mitral valves in theparasternal long axis).
Our study has several limitations. It was a retrospectiveanalysis of a selected sample from an academic institu-tion, and may not be applicable to other situations. Wedid not have medical history or physical examination in-formation in our database, and cannot conclude whichvalvular flow abnormalities may have been recognized bythe referring physician or if any specific therapies (e.g.,afterload reduction, antibiotic prophylaxis) were initi-ated based on the focused Doppler data. Thus, the poten-tial clinical effects of the focused Doppler study on pa-tient care can only be inferred from our findings. Al-though our study does not address the issue of when amore comprehensive echocardiographic study should berequested by the referring physician, this would seem rea-sonable in patients who have moderate or severe valvularregurgitation. Finally, the focused Doppler examinationat our hospital does not include assessment of the pulmo-nary artery pressure or change in regurgitant severity withexercise.
We observed important resting Doppler abnormalitiesin 17% of patients, compared with an 8% prevalence ofischemic wall motion changes. Yet, when comparing theclinical value of stress echocardiography and radionu-clide imaging—tests that have a similar sensitivity and
Table 4. Comparison of Doppler Findings with Previous Comprehensive Echocardiogram
Group (n)
Number (%)with Prior
Echocardiogram
Number (%) with PriorEchocardiogram
Who Had Important Changes
Total sample (1223) 317 (26) 28 (9)�Moderate mitral regurgitation (67) 32 (48) 17 (53)�Mild aortic regurgitation (163) 59 (36) 7 (12)
Value of Focused Doppler Before ETT Echo/Gaur et al
January 2003 THE AMERICAN JOURNAL OF MEDICINE� Volume 114 23

specificity for the detection of coronary artery disease—the potential benefit of resting Doppler data is not usuallyconsidered (7,22). The high prevalence of new Dopplerfindings suggests that these data should be consideredwhen choosing among stress imaging studies.
ACKNOWLEDGMENTThe authors would like to thank Ms. Janet Lee and Ms. IrisWasserman for their administrative assistance.
REFERENCES1. Popp RL, Winters WL Jr. Clinical competence in adult echocardi-
ography. A statement for physicians from the ACP/ACC/AHA TaskForce on Clinical Privileges in Cardiology. J Am Coll Cardiol. 1990;15:1465–1468.
2. Roger VL, Pellikka PA, Oh JK, et al. Stress echocardiography. Part I.Exercise echocardiography: techniques, implementation, clinicalapplications and correlations. Mayo Clin Proc. 1995;70:5–15.
3. Pellikka PA, Roger VL, Oh JK, et al. Stress echocardiography. PartII. Dobutamine stress echocardiography: techniques, implementa-tion, clinical applications and correlations. Mayo Clin Proc. 1995;70:16 –27.
4. Lung B. Interface between valve disease and ischaemic heart dis-ease. Heart. 2000;84:347–352.
5. Dajani AS, Taubert KA, Wilson W, et al. Prevention of bacterialendocarditis. Recommendations by the American Heart Associa-tion. JAMA. 1997;277:1794 –1801.
6. Armstrong WF, Pellikka PA, Ryan T, et al. Stress echocardiography:recommendations for performance and interpretation of stressechocardiography. Stress echocardiography task force of the no-menclature and standards committee of the American Society ofEchocardiography. J Am Soc Echocardiogr. 1998;11:97–104.
7. Fleischmann KE, Hunink MG, Kuntz KM, Douglas PS. Exerciseechocardiography or exercise SPECT imaging? A meta-analysis ofdiagnostic test performance. JAMA. 1998;280:913–920.
8. Singh JP, Evans JC, Levy D, et al. Prevalence and clinical determi-nants of mitral, tricuspid and aortic regurgitation in a population-based cohort. Am J Cardiol. 1999;83:897–902.
9. Jones EC, Devereux RB, Roman MJ, et al. Prevalence and correlatesof mitral regurgitation in a population-based sample (Strong HeartStudy). Am J Cardiol. 2001;87:298 –304.
10. Peteiro J, Freire E, Montserrat L, Castro-Beiras A. The effect ofexercise on ischemic mitral regurgitation. Chest. 1998;114:1075–1082.
11. Krumholz HM, Douglas PS, Goldman L, Waksmonski C. Clinicalutility of transthoracic two dimensional and Doppler echocardiog-raphy. J Am Coll Cardiol. 1994;24:125–131.
12. Fleischmann KE, Lee RT, Come PC, et al. Impact of valvular regur-gitation and ventricular dysfunction on long-term survival in pa-tients with chest pain. Am J Cardiol. 1997;80:1266 –1272.
13. Fleischmann KE, Goldman L, Robiolio PA, et al. Echocardio-graphic correlates of survival in patients with chest pain. J Am CollCardiol. 1994;23:1390 –1396.
14. Stone GW, Griffin B, Shah PK, et al. Prevalence of unsuspectedmitral regurgitation and left ventricular dysfunction in patientswith coronary artery disease and acute pulmonary edema associ-ated with normal or depressed left ventricular systolic dysfunction.Am J Cardiol. 1991;67:37–41.
15. Lebowitz NE, Bella JN, Roman MJ, et al. Prevalence and correlatesof aortic regurgitation in American Indians: the Strong HeartStudy. J Am Coll Cardiol. 2000;36:461–467.
16. Klein AL, Burstow DJ, Tajik AJ, et al. Age related prevalence ofvalvular regurgitation in normal subjects: a comprehensive colorflow examination of 118 volunteers. J Am Soc Echocardiogr. 1990;3:54 –63.
17. Maron BJ. Hypertrophic cardiomyopathy. Lancet. 1997;350:127–133.
18. Sheps SG, Frohlich ED. Limited echocardiography for hypertensiveleft ventricular hypertrophy. Hypertension. 1997;29:560 –563.
19. Kimura BJ, Scott R, Willis CL, DeMaria AN. Diagnostic accuracyand cost-effective implications of an ultrasound screening strategyin suspected mitral valve prolapse. Am J Med. 2000;108:331–333.
20. Kimura BJ, Pezeshki B, Frack AS, DeMaria AN. Feasibility of “lim-ited” echo imaging: characterization of incidental findings. J AmSoc Echocardiogr. 1998;11:746 –750.
21. Kimura BJ, DeMaria AN. Indications for limited echocardio-graphic imaging: a mathematical model. J Am Soc Echocardiogr.2000;13:855–861.
22. Kuntz KM, Fleischmann KE, Hunink MG, Douglas PS. Cost-effec-tiveness of diagnostic strategies for patients with chest pain. AnnIntern Med. 1999;130:709 –718.
Value of Focused Doppler Before ETT Echo/Gaur et al
24 January 2003 THE AMERICAN JOURNAL OF MEDICINE� Volume 114







![Pitfall in Echocardiography: infective endocarditis or …...genesis is believed to be related to endocardial lesions in areas of high stress (valvular closure lines) [2]. In this](https://img.pdfslide.us/doc/110x75/5ea0b050586e033ab63d438c/pitfall-in-echocardiography-infective-endocarditis-or-genesis-is-believed-to.jpg)