Embed Size (px)
Citation preview

VALUE OF DIALYSIS IN OBSTRUCTIVELESIONS OF THE UPPER URINARY TRACT
By MILES Fox, M.D., Ch.M., F.R.C.S.,' and F. M. PARSONS, B.Sc., M.D., F.R.C.P.E.
Renal Research Unit and Department of Uvology, General Infirmary at Leeds
MANAGEMENT of urinary tract obstruction presents no difficulty in most cases. If the obstruction is severe however, and particularly when prolonged, problems may arise. A proportion of these patients arrive in hospital in advanced renal failure and in poor general condition. Prompt relief of the obstruction, hydration and correction of electrolyte abnormalities is sufficient in some to begin and to maintain the road to recovery, but in other cases renal function, at least in the immediate period, may be inadequate or so marginal that without dialysis deterioration will continue.
The cause of the obstruction may not be clear on admission and must be established as soon as possible in uraemic patients. Cystoscopy and retrograde catheterisation can be performed under local anaesthesia but adequate assessment by bimanual examination of the pelvic contents and biopsy is not possible without general anaesthesia which may be hazardous to life in advanced urzmia. Blind preliminary diversion of the urine by nephrostomy or ureterostomy is not to be advocated without adequate assessment, Only then can a firm decision be made regarding operative intervention and complete restorative surgery may be possible in one stage once the urzmia has been corrected by dialysis.
Material and Methods.-Indications for dialysis in advanced uraemia from prostatic obstruction have been described previously (Fox and Parsons, 1964). The present report deals with the management of 33 patients with severe uraemic obstruction of the upper urinary tract referred to and treated in the Artificial Kidney Unit in Leeds over a 10-year period, 1957 to 1966. Twenty-one of the patients were referred from centres outside Leeds. The blood urea levels on admission ranged from 220 mg./100 ml. to 600 mg./100 ml. with a mean of 368 mg./100 ml., and the ages from 27 to 82 years (mean 52 years). The majority of patients were treated by hzmodialysis with a Kolff rotating drum machine (Parsons et al., 1961), but in the last two years peritoneal dialysis was used in most cases.
The following causes of obstruction were encountered : Renal stone . . 7 Ureteric stone . 3 Pelviureteric obstruction . . 1 Periureteric fibrosis . . 2 Retroperitoneal sarcoma . . 1 Tuberculosis . . 2 Bladder lymphosarcoma . . 1 Bladder carcinoma . . 5 Cervical carcinoma . . 4 Uterine carcinoma . . 1 Rectal carcinoma . . 4 Prostatic carcinoma . 1 Operative trauma . . I 1 Present address : Department of Urology, Royal Hospital, Sheffield.
197

No.
-
I 2 3 4 5 6 7 8 9 10
II
12
13
Age
58
30
-
64
27
65
55
41
34
59
33
46
66
65
Sex -
M
M
M
M
M
F F F M
M
F M
F M
F M
M
Dia
gnos
is
Stag
horn
sto
ne s
olita
ry
kidn
ey
Ston
es s
olita
ry k
idne
y
Bila
t. re
nal
ston
es a
nd
hydr
onep
hros
es
3ila
t. re
nal
ston
es.
Neu
roge
nic
blad
der
iton
e so
litar
y ki
dney
Mat
. ren
al s
tone
s
iena
l st
ones
and
hy
dron
ephr
osis
iton
e ur
eter
of
solit
ary
func
tioni
ng k
idne
y
itone
ure
ter
of s
olita
ry
kidn
ey
itone
ure
ter
of s
olita
ry
func
tioni
ng k
idne
y
'elv
i-ure
teric
ohs
truc
-
3ydr
onep
hros
is
'eriu
rete
ric
fibr
osis
tion.
'eriu
rete
ric
fibr
osis
tetr
oper
iton
eal
lipo-
sa
rcom
a
rube
rcul
ous
urel
eric
ob
stru
ctio
n
rube
rcul
ous u
rete
ric
Iarc
inom
a bl
adde
r
obst
ruct
ion
Blo
od U
rea
on
Adm
issi
on
(mg.
/IOO
ml
220
334
292
433
336
219
300
468
309
333
405
360
290
390
595
600
510
TA
BL
E
Dia
lysi
s
Day
s af
ter
Ref
erra
l
14+2
1
1 1
0+
2
0, 4
+10
I, 2,
4+ I
1
2 1 0
2+
5
0, 5
, 13
+
21
0 13 1
1+15
1
0+7
1
H-h
zmo
P-pe
riton
ea
H
H
H
H
H
H
P H
H
H
P H
H
H
H
H
H
Ope
ratio
n
-I N
ephr
olit
hoto
my
1
Cys
tosc
opy + r
etro
grad
e.
Nep
hros
tom
y.
Cys
tosc
opy
+ret
rogr
ade.
Py
elol
ithot
omy
Cys
tosc
opy + r
etro
grad
e.
Pyel
olith
otom
y an
d ne
phro
stom
y.
...
Nep
hrol
itho
tom
y.
Cys
tosc
opy + r
etro
grad
e.
Ure
tero
litho
tom
y.
Nep
hros
tom
y.
Ure
tero
litho
tom
y.
Cys
tosc
opy
+ret
rogr
ade
Exp
lora
tion
ure
ter
shel
l onl
y.
Cys
tosc
opy + r
etro
grad
e.
Ure
tero
lysi
s.
Nep
hros
tom
y.
Cys
tosc
opy + r
etro
grad
e (o
bstr
uctio
n re
lieve
d).
Lap
arot
omy.
Cys
tosc
opy + r
etro
grad
e.
Ure
teri
c m
eato
tom
y.
Nep
hrec
torn
y (o
ppos
ite).
Ure
tero
stom
y.
Cys
tosc
opy
+nep
hros
-
Ure
tero
colo
stom
y.
tom
y.
23
1 3 0 2 1 3 0 1 ...
6 1 3 I 25
1 6 ... 2 ... 1 4 14 3 5 2
125
153 3 2 14
Peri
od i
n H
ospi
tal
(wee
ks)
6t
6f
Die
d
I (tr
ansf
erre
d:
Die
d
Die
d 5 4 5+
6t 4
Die
d
Die
d
7 6 + 6t
Die
d
7
Blo
od U
rea
on
Dis
char
ge
mg.
/l00
ml.
I38 73
...
...
...
...
55
30
61
37
300 ...
...
28
141 + 184 ... 12
Surv
ival
6 m
onth
s *
7 ye
ars
*
5 da
ys
4 m
onth
s
13 d
ays
15 d
ays
8 m
onth
s *
4+ y
ears
*
7 ye
ars *
5 ye
ars*
50 d
ays
1 da
y
33 d
ays
3 m
onth
s
7 m
onth
s
11 d
ays
5 m
onth
s
Com
men
ts
t
Pulm
onar
y in
fect
ion
and
edem
a.
Acu
te o
n ch
roni
c su
ppur
ativ
e py
elo-
ne
phri
tis.
Pneu
mon
ia,
ente
ritis
, su
ppur
ativ
e py
elo-
ne
phri
tis.?
Nev
er f
it fo
r op
erat
ion.
...
...
Seve
re, i
rrec
over
able
re
nal
dam
age.
Rap
idly
det
erio
rate
d.
Dia
lysi
s to
o la
te.
Uri
nary
re
trog
rade
. dr
aina
ge a
fter
Die
d of
sup
pura
tive
py
elon
ephr
itis.
t Ir
radi
atio
n gi
ven.
Thr
ee m
onth
s in
san
a-
tori
um b
etw
een
peri
ods
in h
ospi
tal.?
Sept
icae
mia
.
Palli
ativ
e ur
eter
o-
colo
stom
y.

I 1s
50
day
s
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
Pneu
mon
ia a
nd p
yelo
- 1
neph
ritl
. 70
63
60
82
31
41
56
53
50
66
57
43
57
63
62
60
M
M
M
M
M
F F
F
F
F
M
M
M
M
M
F
-
Cnr
rino
ma
hlad
der
Car
cino
ma
blad
der
Car
cino
ma
blad
der
Car
cino
ma
blad
der
Lym
phos
arco
ma
blad
de
Car
cino
ma
cerv
ix
Car
cino
ma
cerv
ix
Car
cino
ma
cerv
ix
Car
cino
ma
cerv
ix
Car
cino
ma
uter
us
Car
cino
ma
rect
um
Car
cino
ma
rect
um
Car
cino
ma
rect
um
Car
cino
ma
rect
um
Car
cino
ma
pros
tate
Ope
rativ
e tr
aum
a of
ur
eter
dur
ing
rem
oval
of
ova
rian
car
cino
ma
309
438
23 1
73-2
40
489
47 I
400
255
249
428
25
h3
81
415
6b
34
0
258
600
300
6 I I 8 I 0
1 +
5 0 1 I 12 I 13
6 1 1
H
H
H
H
H
H
H
H
P H
H
H
H
H
P H
Cys
tosc
opy
biop
sy.
T.G
.R.
t~ii
iclu
i.
Cys
tosc
opy
fnep
hros
-
Ure
tero
stom
y.
Tot
al c
yste
ctom
y.
i to
my.
Cys
tosc
opy + b
iops
y.
Cys
tosc
opy
+ret
rogr
ade.
Cys
tosc
opy + r
etro
grad
e.
Lap
arot
omy+
bio
psy.
Cys
tosc
opy
fatt
empt
ed
Ure
tero
colo
stom
y.
Cys
tosc
opy + E
.U.A
.
retr
ogra
de.
Cys
tosc
opy f E
.U.A
. an
d bi
opsy
.
Cys
tosc
opy +
biop
sy
Cys
tosc
opy
+ret
rogr
ade.
C
ysto
scop
y +r
etro
grad
e.
Lap
arot
omy,
bio
psy
and
Cys
tosc
opy + r
etro
grad
e.
Lap
arot
omy.
uret
erol
ysis
.
...
...
1 2 2 I2
10
11 2 6
0+
3
3 4 2 9 15 2 12
15 4 7 ...
...
Die
d
Die
d
Die
d
Die
d
Die
d
Die
d
Die
d
3 3
Die
d
Die
d
Die
d 5
Die
d
Die
d
Die
d
...
...
...
...
...
...
...
60
30
...
...
...
73
...
...
...
~
50 d
ays
19 d
ays
20 d
ays
13 d
ays
8 da
ys
II d
ays
3 m
onth
s
4 m
onth
s *
21 d
ays
26 d
ays
Not
10
day
s kn
own
14 d
ays
I da
ys
5 da
ys
Ver
y ad
vanc
ed t
umou
r.
Acu
te p
yelo
neph
ritis
.
Ana
plas
tic w
ides
prea
d tu
mou
r.
Adv
ance
d tu
mou
r.
Vag
ino-
peri
tone
al
fistu
la.
Peri
toni
tis.
Palli
ativ
e di
vers
ion.
Fo
llow
ing
star
t of
radi
othe
rapy
for
ex-
tens
ive
tum
our
deve
lope
d an
uria
w
hich
lat
er c
lear
ed.?
Lar
ge tu
mou
r.
Exte
nsiv
e tu
mou
r.
Inop
erab
le tu
mou
r.
Inop
erab
le tu
mou
r.i
Inop
erab
le tu
mou
r.
Palli
ativ
e ur
eter
olys
is
Live
r se
cond
arie
s.
Bro
ncho
-pne
umon
ia.
Peri
toni
tis.
Pyel
o-
neph
ritis
.
* Aliv
e.
t See
text
.

200 BRITISH J O U R N A L OF UROLOGY
Clinical Course.-Clinical details, treatment and results are summarised in the Table. Six cases are described in greater detail.
Case 2.-L. L., male, aged 30 years, was admitted because of 36 hours’ anuria and several days’ prior oliguria. Twelve years previously left nephrectomy had been carried out for renal stones. Blood urea on admission was 334 mg./100 ml.
Cystoscopy was performed the morning after admission under local anesthesia and a right ureteric catheter was passed. The presence of an obstructing stone at the pelviureteric junction was confirmed by X-ray. Several
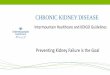
PYELOLITHOTOMY
d L.L.
3Oyrs
5
i
m
6 J.S
65yrs
I ENTERITIS - PNEUMONIA -
I I I j 10 20
0 0 10 20
DAYS
FIG. 1 DAYS
FIG. 2
other calculi were present in the calyces. As the ureteric catheter did not relieve the obstruction, a six-hour hsmodialysis was carried out the same day, the blood urea falling to 103 mg./100 ml. (Fig. 1). Two days later the kidney was explored. The renal substance was found to be diminished and the urine in the collecting system was purulent. The stones were removed and a nephrostomy was established. After several days’ oliguria and a rise of the blood urea to 218 mg./100 ml., satisfactory recovery occurred and the patient was discharged home (without nephrostomy) with normal micturition six and a half weeks from admission. He remains well seven years later with a blood urea in the region of 70 mg./100 ml.
Comment.-The sequence and timing of the management provided the patient with optimum chance of recovery. The definitive operation was made possible by dialysis and was carried out within four days of admission. Nephrostomy was performed because of the severe infection in the kidney.
Case 5.-J. S., male, aged 65 years, was referred because of five days’ history of left renal pain associated with oliguria and then anuria. Right nephrectomy had been performed 28 years previously for multiple renal stones. He was drowsy on admission (blood urea 336 mg./100 ml., Na 117 mEq./litre, K 7.7 mEq./litre and CO2 combining power 10 mEq./litre). His general condition improved following correction of the electrolyte imbalance with parenteral molar sodium lactate, dextrose and insulin and oral ‘‘ Resonium A ”. A left ureteric catheter was passed under local anesthesia and the presence of an obstructing stone in the renal pelvis was confirmed by X-ray. A four-hour hernodialysis was performed the next day (Fig. 2) and pyelolithotomy the day after that. The urine was heavily infected with B. proteeus. Urine output was poor and further hemodialyses were performed three days and nine days after operation. The patient developed a Staphylococcus aweus enteritis and a staphylococcal and pyocyaneus chest infection which did not respond to treatment and from which he died on the eleventh post-operative day.
Comment.-The patient was treated expeditiously and the obstructing stone was removed following dialysis. The poor resistance to infection of the chronic uremic subject is demonstrated, against which antibiotics had but little effect. Catabolism was increased by the infection with rapid progression of the urazmic condition.
Case 13.-G. B., female, aged 65 years, was admitted because of vomiting, drowsiness, and a two weeks’ history of oliguria. The blood urea was 290 mg./100 ml. No abnormality was found on abdominal examination.

D I A L Y S I S I N O B S T R U C T I V E LESIONS O F U P P E R U R I N A R Y T R A C T 20 1
The bladder was normal on cystoscopy. The right ureter was obstructed 10 cm. from the bladder. The left ureter was catheterised, urine escaped under pressure and continued to drain when the catheter was withdrawn. Dilated pelvis, calyces and upper ureter were seen on retrograde pyelography. The blood urea fell to 85 mg./100 ml. and laparotomy was carried out four days after admission. .The ureters were found to be involved in periureteric fibrosis and were freed. Following operation urine output diminished and the blood urea rose, fmally reaching 446 mg./100 ml. Hsmodialysis was performed nine days post-operatively but had to be discontinued because of deterioration of general condition and hypotension. Nephrostomy was carried out the following day, but urinary output did not increase. The urine became infected with P.pyocyaneus and the patient died 33 days after admission with broncho-pneumonia. The kidneys showed acute pyelonephritis.
Comment.-Sufficient renal tissue for survival was present as shown by the initial rapid recovery from renal failure. Urinary drainage was probably impaired by ureteric cedema following the operation and renal failure was further aggravated by post-operative increase of catabolism. Dialysis was too long delayed and once infection developed a rapid downhill course resulted.
600
o x
E P
a 400 w K 3
0 0
m s
200
0
DIALYSIS 1
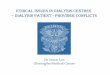
7 A S
37 y r s
NE PHR ECTOMY
‘ I 1
I I 1 I 2 4 6 ‘12 16 18
WEEKS
FIG. 3
Case 15.-A. S., female, aged 37 years, was admitted in a semi-comatose condition. Her general health had gradually deteriorated over eight months. She had had frequency of micturition for several months. Blood urea was 595 mg./lOO ml., Na 113 mEq./litre, K 7.0 mEq./litre. Her general condition improved slightly following hydration and electrolyte correction. Urine output rose to approximately 500 ml. per 24 hours, but the blood urea did not fall. Cystoscopy was performed two days after admission. The bladder was mildly inflamed. The right ureter was catheterised but the left ureter was blocked. X-ray examination showed extensive calcification in the left renal area and a right hydronephrosis and hydroureter extending to the bladder. Tubercle bacilli were found and subsequently cultured in the urine. A five-hour hzmodialysis was carried out three days later (Fig. 3) and anti-tuberculous therapy (PAS and INAH) was commenced. Her general condition improved and the urine output increased to 3 to 4 litres per day. Following four months’ sanatorium treatment the patient was readmitted. Thc blood urea was then 200 to 250 mg./100 ml. A right ureteric meatotomy was performed endoscopically because of distal ureteric narrowing. A second hcmodialysis was carried out one month later and a large left tuberculous pyonephrosis was removed two days afterwards. The patient was discharged home two and a half wecks post-operatively with a blood urea of 130 rns.il00 ml. She finally died in renal failure eight months after the original admission.
Comment.-A high blood urea which could not be reduced by correction of electrolyte imbalances and adequate hydration was lowered by dialysis without subsequent rise, for at least a period of time, and with associated improvement in general condition. The value of pre-operative dialysis in a subject with a moderately raised blood urea is shown. It anticipates increased protein catabolism which follows operative intervention and

202 BRITISH J O U R N A L OF UROLOGY
by lowering the baseline of excretory metabolites in the blood it often avoids dialysis in the immediate post- operative period with its attendant dangers.
Case 26.-M. E. M., female, aged 50 years, while undergoing treatment with supervoltage X-ray therapy for Stage 3 carcinoma of the cervix developed oliguria and finally anuria. She was admitted with a blood urea of 249 nig./100 ml., Na 118 mEq./litre, K 7.4 mEq./litre, CI 90 mEq./litre and CO2 combining power 11 mEq./litre. Electrolyte imbalances were corrected with molar sodium chloride and bicarbonate and “ Resonium A ” and the following day peritoneal dialysis was commenced. Twenty-seven exchanges were employed over two days and the blood urea was reduced to 95 mg./100 ml. Cystoscopy was performed four days after admission under general anresthesia. Neither ureteric orifice could be seen owing to distortion and adema of the posterior wall of the bladder. A large fixed pelvic mass was felt on bimanual examination. In view of the advanced nature of the provcd tumour it was decided not to perform exploratory laparotomy or urinary diversion. She remained anuric for SIX days, but then started to pass large amounts of urine and was discharged 23 days after admission, with a normal blood urea, to complete the course of radiotherapy. She was alive and well four months later.
Comment.-Ureteric obstruction was produced, probably by initial reaction from irradiation in the region of the tumour. As it subsided, the obstruction was relieved.
Case 29.-A. C., male, aged 43 years, was admitted because of low abdominal pain, vomiting, drowsiness and oliguna. Blood urea was 415 mg./100 ml., and K was 9.2 mEq./litre. Four months previously an abdomino- perineal resection had been performed for rectal carcinoma. Intravenous glucose and insulin were administered and haemodialysis was started twelve hours later. The blood urea was reduced to 124 mg./100 ml. and the potassium to normal levels after four hours’ dialysis. Cystoscopy and retrograde catheterisation were performed under general anasthesia the next day. The left ureter was completely obstructed 3 cm. from the bladder. After advancing the catheter on the right side to between 5 and 10 cm. from the bladder, marked efflux of urine occurred. Urine continued to drain after withdrawal of the catheter. A pelvic mass was felt. Four days later laparotomy was 13erformed and a large, fixed recurrent neoplasm was found in the pelvis. No further treatment was given and {he patient died in urzmia five days after the operation.
Comment.-Dialysis allowed a firm diagnosis to be established without delay and a course of action to be laken accordingly in a patient with recurrent advanced inoperable tumour.
DISCUSSlON
Urinary obstruction requires prompt relief if the only functioning renal tissue is involved. Endoscopic procedures are sufficient in some cases as a temporary measure. Opera- tive intervention is required in others and may carry considerable risk. Patients with urzmia, particularly if chronic, are undernourished, have diminished resistance to infection (Balch et al., 1955; Parsons and McCracken, 1959), wound healing is delayed (Stein and Wiersum, 1959) and electrolyte imbalances, anamia and cardiac insufficiency increase the immediate hazards still further.
Immediate dialysis was required as a life-saving measure in some cases. Subsequently, indications for dialysis fell into three broad categories :
1. To establish a Diagnosis.-Retrograde pyelography may be inconclusive or not possible under local anasthesia. Adequate palpation, laparotomy and biopsy require relaxation and usually general anasthesia.
Dialysis was performed in all but two patients with this end in view. Treatment was not continued in 11 when it became obvious that other factors such as advanced inoperable malig- nancy or irreversible renal damage would otherwise rapidly terminate life.
2. To prepare the Patient for Definite Operation.-Preliminary diversion of the urine by nept-trostomy has been considered the safest and most expeditious method of improving renal function and the patient’s general condition in upper urinary tract obstruction (Cabot and Holland, 1931 ; Boyd, 1932; Graves and Buddington, 1939; Kimbrough, 1940; Lowsley and Kirwin, 1940; Livermore, 1947; Miller, 1949), and definitive surgery has been postponed to some later date. Nephrostomy in itself carries an immediate risk to life in these very ill patients and subsequent infection in the presence of diminished resistance (Parsons and McCracken, 1959) is a further serious hazard. Advanced urremia may cause an increase in protein catabolism with overloading of the already diminished renal reserve (Parsons, 1960), which nephrostomy in iiself will not reverse.

D I A L Y S I S I N O B S T R U C T I V E L E S I O N S OF U P P E R U R I N A R Y T R A C T 203
Dialysis corrects most of the abnormalities encountered in renal failure and marked im- provement can be expected within 48 hours. If a diagnosis has been made, corrective surgery may be performed at this stage or following a Second dialysis two to three days later. This is advisable in chronic uramia particularly if hcemodialysis is being used (Merrill, 1952, 1957; Fox and Parsons, 1964).
Eighteen patients underwent elective surgery without previous urinary diversion. Nephro- stomy was established at the same time in three because of severe infection and the possibility of inadequate drainage from reaction and edema at the site of operation. Diversion after dialysis and before considering further surgery was performed in five to try to improve general condition (nephrostomy 3, ureterostomy 2) and as a palliative procedure in one. Two died before further operative intervention was possible. Palliative uretero-colostomy was carried out in two patients.
A moderately raised blood urea is no contra-indication to operation, bbt the additional stress of an increase in protein catabolism in the immediate post-operative period may overload damaged renal tissue and produce a dangerous uraemic state. Pre-operative dialysis, anticipating these sequels, is preferable to dialysis in the early post-operative period. An example was seen in Case 15.
3. Dialysis in the Post-operative Period.-Three patients were dialysed post-operatively. They had been urcemic for some time prior to surgery and urinary infection and pyelonephritis had set in. The infection progressed rapidly in spite of antibiotic therapy and death occurred from septicsmia, peritonitis or broncho-pneumonia. The poor resistance to infection in this type of patient was once again demonstrated.
The blood urea rose post-operatively in most cases but with careful regulation of fluid intake and electrolyte replacement, particularly of sodium (Lapides, 1953 ; Parsons, 1954), a satisfactory stable balance was achieved. Regional heparinisation (Nakamoto and Holmes, 1958 ; Anderson and Kolff, 1959) was not employed during dialysis and bleeding from the operation site was not encountered.
Ureteric obstruction resolved spontaneously in one patient undergoing radiotherapy for cervical carcinoma, in whom anuria developed during treatment. The obstruction was probably caused by early hypercemia and cedema from the effects of irradiation and resolved subsequently. Lee and Brooks (1965) recorded a somewhat similar case of ureteric obstruction from carcinoma of the prostate which resolved with estrogen therapy. Dialysis maintained life in the interim period. The final outcome and the possible response to therapy of even an advanced tumour must therefore be assessed carefully before the situation is rejected as hopeless and further dialysis discontinued. Sitprija, Nakamoto and Kolff (1963) performed dialysis and nephrostomy in patients with even the most advanced tumours.
Peritoneal versus Ha?modialysis.--In patients who have urinary tract obstruction that cannot be relieved by simple means such as the passage of a ureteric catheter, drainage should be established by operative means as soon as possible. For this purpose the more rapid correction of the biochemical abnormalities achieved by hsmodialysis would make this the method of choice rather than the slower procedure of peritoneal dialysis. When infection of the renal tract accompanies the obstruction, rapid relief of the obstruction is imperative and haemodialysis again is the initial treatment of choice.
For pre-operative preparation in a patient with a normal catabolic rate and where time is of less importance, peritoneal dialysis appears the more suitable, easier and often more con- venient method. In severe chronic uraemia a slower reduction of the metabolic abnormalities is to be preferred to avoid the dangers of a disequilibrium syndrome (Kennedy et al., 1963; Rosen, O’Connor and Shaldon, 1964). The method has been used more and more frequently with experience gained.
The results in this series of cases may appear disappointing at first sight. Only 13 patients

204 BRITISH J O U R N A L OF U R O L O G Y
survived three months or longer, and four over one year with probably another two if followed up longer. It must be remembered, however, that all were in severe renal failure on admission, 18 had wide-spread inoperable tumours and two had advanced tuberculosis of the renal tract. The diagnosis was established and no further treatment was possible in 13. The best prognosis occurred in 10 patients with a stone obstructing the upper urinary tract. The majority of long- term survivors were in this group. Dialysis enabled definitive surgery to be performed with little delay, in relative safety, and with satisfactory results.
SUMMARY
Thirty-three patients with severe ursemic upper urinary tract obstruction were treated in Leeds over the past 10 years with the aid of dialysis. The value and indications for dialysis and results are described and discussed.
We wish to thank Professor L. N. Pyrah and the late Mr F. P. Raper for permission to publish the case histories of patients who were admitted under their care.
REFERENCES
ANDERSON, A., and KOLFF, W. J. (1959). Ann. intern. Med., 51, 476. BALCH, H. H., MERONE, W. H., and SAKO, Y. (1955). Surgery Gynec. Obstet., 100,439. BOYD, M. L. (1932). J . Am. med. Ass., 99, 1226. CABOT, H., and HOLLAND, H. W. (1931). Trans. Am. Ass. gen. urin. Surg. 24, 95. Fox, M., and PARSONS, F. M. (1964). Br. J. Urol., 36, 487. GRAVES, R. C., and BUDDINGTON ,W. T. (1939). J. Urol., 41, 265. KENNEDY, A. C., LINTON, A. L., LUKE R. G. and RENFREW, S. (1963). Lancet, 1,408. KIMBROUGH, J. C. (1940). Urol. cutan. Rev., 44, 296. LAPIDES, J. (1953). J. Urol., 70, 74. LEE, H. A., and BROOKS, P. L. (1965). Bv. J . Surg., 52, 151. LIVERMORE, G. R. (1947). J. Urol., 57, 213. LOWSLEY, 0. S., and KIRWIN, T. J. (1940). “ Clinical Urology.” Baltimore: Williams and Wilkins
co. MERRILL, J. P. (1952). New Engl. J . Med., 246, 17. __ (1957). J. chron. Dis., 5, 138. MILLER, A. (1949). Proc. R . SOC. Med., 42, 801. NAKAMOTO, S., and HOLMES, J. H. (1958). Trans. Am. SOC. arrif. intern. Org., 4, 36. PARSONS, F. M. (1954). Br. J . Urol., 26, 7. __ (1960). In “ Modern Trends in Urology ”, ed. Riches, Sir Eric. London: Butterworths. PARSONS, F. M., HOBSON, S. M., BLAGG, C. R., and MCCRACKEN, B. H. (1961). Lancet, 1, 129. PARSONS, F. M., and MCCRACKEN, B. H. (1959). Br. med. J., 1, 740. ROSEN, S. M., O’CONNOR, K., and SHALDON, S. (1964). Br. med. J . , 2, 672. SITPRIJA, V., NAKAMOTO, S., and KOLFF, W. J. (1963). J. Urol., 89, 149. STEIN, A. A., and WIERSUM, J. (1959). J. Urol., 82, 271.

![Case Report Bilateral Obstructive Uropathy Secondary to ...syndrome [ ], subacute intestinal obstruction [ , ], recur-rent acute urinary retention [ ], or exceptionally bilateral hydronephrosis](https://img.pdfslide.us/doc/110x75/60f789064e4fc37e631734b3/case-report-bilateral-obstructive-uropathy-secondary-to-syndrome-subacute.jpg)