Embed Size (px)
Citation preview

WHO/BS/09.2116
ENGLISH ONLY
EXPERT COMMITTEE ON BIOLOGICAL STANDARDIZATION
Geneva, 19 to 23 October 2009
Value Assignment of the Proposed 6th
International Standard for
Blood Coagulation Factor VIII and von Willebrand Factor in
Plasma, Human (07/316)
Anthony R. Hubbard
1,3, Michelle Hamill
2, Malinee Beeharry
1, Sally Bevan
1 &
Alan B. Heath
1 Haemostasis Section, Biotherapeutics Group, and
2 Biostatistics Section,
National Institute for Biological Standards and Control,
Blanche Lane, South Mimms,
Potters Bar, Herts EN6 3QG, UK
3Principal Investigator
© World Health Organization 2009
All rights reserved. Publications of the World Health Organization can be obtained from WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; e-mail: [email protected]). Requests for permission to reproduce or translate WHO publications – whether for sale or for noncommercial distribution – should be addressed to WHO Press, at the above address (fax: +41 22 791 4806; e-mail: [email protected]).
The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters. All reasonable precautions have been taken by the World Health Organization to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall the World Health Organization be liable for damages arising from its use. The named authors [or editors as appropriate] alone are responsible for the views expressed in this publication.

WHO/BS/09.2116
Page 2
Summary
Background and aim The current WHO 5
th International Standard (5
th IS) Factor VIII/von Willebrand factor, plasma
(02/150) is used for the potency estimation of 5 analytes in plasma (Factor VIII:coagulant
activity; Factor VIII:antigen, VWF:antigen, VWF:ristocetin cofactor, VWF:collagen binding).
The 5th
IS provides a common traceable source of calibration to promote harmonisation between
secondary working plasma standards and is primarily used for the estimation of these analytes in
relation to the diagnosis of disease (eg. haemophilia A and von Willebrand disease). Stocks of
the WHO 5th
IS are extremely low and a replacement preparation is required. This report
describes the value assignment of the proposed WHO 6th
IS by assay relative to the WHO 5th
IS
and locally collected normal plasma pools.
Methods and Results Value assignment of the replacement WHO IS has been achieved through an international multi-
centre study involving 44 laboratories from 14 countries.
Estimates for FVIII:C, relative to the 5th
IS, by all three methods (one-stage clotting, two-stage
clotting, chromogenic), showed good inter-laboratory agreement with overall geometric
coefficient of variation (GCV) of 4.06% and a combined mean value of 0.68 IU per ml (n=52).
A significant difference was found between estimates relative to the fresh (mean 0.57 IU/ml) and
the frozen normal pools (mean 0.72 IU/ml). Estimates relative to the fresh normal plasma pools
were significantly lower (p<0.0001) and more variable (GCV 13.9%) than estimates relative to
the 5th
IS (GCV 4.06 %). In consideration of the known stability of the 5th
IS, the variability of
estimates relative to the fresh normal pools, and in order to maintain continuity between the 5th
and 6th
IS it is proposed that the 6th
IS be assigned the mean value obtained relative to the 5th
IS
of 0.68 IU per ampoule.
Estimates for FVIII:antigen, relative to the 5th
IS, showed good agreement between laboratories
with GCV of 4.24% and an overall mean of 1.04 IU per ml (n=10). These estimates were
significantly different from the estimates obtained relative to the normal plasma pools (mean
0.93 IU per ml) which were also more variable (inter-laboratory GCV 10.5 %). In the interest of
continuity it is proposed that the 6th
IS be assigned the mean value obtained relative to the 5th
IS
of 1.04 IU per ampoule.
Estimates for VWF:antigen, relative to the 5th
IS, showed excellent agreement between the
ELISA and immuno-turbidimetric methods and produced an overall mean of 1.00 IU/ml (n=31)
with low inter-laboratory variability (GCV 4.29%). Estimates relative to the normal pools were
significantly lower (mean 0.89 IU/ml) and more variable (GCV 12.92%). In consideration of the
variability of the estimates relative to the normal pools and in order to maintain continuity of the
IU it is proposed that the 6th
IS be assigned the mean value obtained relative to the 5th
IS of 1.00
IU per ampoule.
Estimates for VWF:RCo relative to the 5th
IS by the aggregometric methods were less variable
(GCV 6.52%) but not significantly different to estimates by visual agglutination (GCV 12.0%).
Combination of all estimates relative to the 5th
IS produced a mean of 0.87 IU/ml (n=28) with
acceptable inter-laboratory variability (GCV) of 8.13 %. In contrast the estimates relative to the
normal pools were much more variable between laboratories with GCVs from 10 – 28% and this
hindered meaningful statistical analysis comparing fresh and frozen pools. There was no
significant difference between the overall combined estimates relative to the 5th
IS (0.87 IU/ml,

WHO/BS/09.2116
Page 3
n=28) and the normal pools (0.90 IU/ml, n=28). It is proposed that the 6th
IS be assigned the
mean value obtained relative to the 5th
IS of 0.87 IU per ampoule.
Estimates for VWF:collagen binding, relative to the 5th
IS were associated with very good
agreement between estimates obtained using type III and type I/III mix collagen reagents and
produced an overall mean of 1.03 IU/ml (n=21) with inter-laboratory variability (GCV) of 5.80
%. Estimates relative to the normal plasma pools were associated with greater inter-laboratory
variability (GCV 12.24%, mean 0.99 IU/ml, n=20) but were not significantly different to
estimates vs the 5th
IS. It is proposed that the 6th
IS be assigned the mean value obtained relative
to the 5th
IS of 1.03 IU per ampoule.
Estimates for VWF:collagen binding in the 1st IS VWF Concentrate relative to the 5
th IS
indicated no significant difference between the use of type III and type I/III mix collagen
reagents. The overall combination of estimates produced a mean value of 10.74 IU/ml with
inter-laboratory variability (GCV) of 19.5%. These results indicate improved harmonisation
between laboratories compared to the original attempt to assign a value to the 1st IS VWF
Concentrate in 2000 and may be an indication that it will be possible to assign a value for
VWF:CB to the proposed 2nd
IS VWF Concentrate in 2010.
Stability of the proposed 6th
IS has been assessed through an accelerated degradation study after
storage of ampoules at elevated temperatures (+4, +20, +37, +45 °C) for up to 9 months. The
results from the initial testing are very encouraging and indicate that all analytes in the proposed
6th
IS are extremely stable when stored at the bulk storage temperature of -20 oC with the mean
predicted losses per year of 0.074% for FVIII:C 1-stage, 0.146% for FVIII:C chromogenic,
0.049% for FVIII:antigen, 0.00% for VWF:antigen, 0.022% for VWF:ristocetin cofactor and
0.002% for VWF:collagen binding.
Proposal It is proposed that the preparation coded 07/316 be accepted as the WHO 6
th International
Standard Factor VIII/von Willebrand Factor, Plasma with the following assigned values
estimated relative to the 5th
IS FVIII/VWF Plasma (02/150):
Factor VIII:C 0.68 IU per ampoule
Factor VIII:Antigen 1.04 IU per ampoule
VWF:Antigen 1.00 IU per ampoule
VWF:Ristocetin cofactor 0.87 IU per ampoule
VWF:Collagen binding 1.03 IU per ampoule
Responses from study participants and SSC/ISTH sub-committees
on Factor VIII/IX and von Willebrand factor Responses have been obtained from all of the 44 participants and all have approved of the
proposed value assignments for the 5 analytes. Additional comments were received relating to
errors or omissions in the description of methodologies (Appendix 3) or the names of
participants (Appendix 2) and these have been corrected. Several participants commented on the
limited value of including local normal pools and questioned if this comparison could be
excluded from future studies. One participant commented on the proposed value for FVIII:C
(0.68 IU per ampoule) and indicated they would have preferred a value around 1.00 IU per
ampoule. The participant was informed that the processing of the lyophilised standard together
with the use of citrate-based anticoagulant were the main reasons for the lower FVIII:C value;
similar values have been found for previous standards and have not affected their validity for

WHO/BS/09.2116
Page 4
FVIII:C estimation. One participant emphasised the need to exclude estimates for VWF:RCo
obtained using an immuno-turbidimetric method since this method is based on antigen
determination rather than platelet agglutination; results from this method have not been included
in the combined mean values for value assignment.
Responses have also been sought from experts associated with the Factor VIII/Factor IX and von
Willebrand factor sub-committees of SSC/ISTH. All responses were in favour of the proposal
and the following comments were also noted:
1) One comment suggested the number of laboratories using the immuno-turbidimetric method
for VWF:RCo should be increased in future studies, however, this is not in agreement with
current opinion (or the participant comment above) which does not support the inclusion of
surrogate measurements of VWF function based on antibodies directed against the Glycoprotein
1b binding site on VWF.
2) A comment expressed concern over the comparison of lyophilised and fresh plasma, in the
estimation of VWF:RCo, due to the increased opacity of lyophilised plasma which made it
difficult to “set up” aggregometers. The response to this comment attempted to provide
reassurance that the design of the study, which required the testing of 3 dilutions of all samples,
would allow the detection of such an effect by non-parallelism of the dose-response relationships.
Since no significant non-parallelism was detected between lyophilised plasma and fresh plasma
samples it was concluded that the comparisons were valid. Any such effect would have no
impact on comparisons of the 5th
IS and the proposed 6th
IS which are both lyophilised.
3) One comment recommended that normal plasma pools should be retained in future
collaborative studies as a “reality check” to provide contact with the “real world”.
The proposal to accept the preparation coded 07/316 as the 6th
IS Factor VIII/VWF Plasma with
values assigned relative to the 5th
IS was discussed at the WHO-ISTH Liaison Group Meeting
on 12 July 2009 and subsequently endorsed at the SSC Business Meeting, held in Boston MA,
on 15 July 2009.
Introduction and objectives of the study Stocks of the current WHO 5
th IS Factor VIII/VWF Plasma (02/150) will be exhausted by the
end of 2009 and the primary objective of this study is the assignment of values to the
replacement preparation, the proposed WHO 6th
IS Factor VIII/VWF Plasma (07/316). Values
will be assigned for the same five analytes attached to the 5th
IS, namely, factor VIII coagulant
activity (FVIII:C), factor VIII antigen (FVIII:Ag), von Willebrand factor antigen (VWF:Ag),
von Willebrand factor Ristocetin Cofactor activity (VWF:RCo) and von Willebrand factor
collagen binding (VWF:CB). Value assignment is achieved by the assay of the proposed WHO
6th
IS relative to the current WHO 5th
IS and locally collected normal plasma pools. The former
comparison provides continuity of the value of the International Unit (IU) between successive
standards and the latter comparison provides a check on the value of the IU relative to the
original definition of the “plasma unit” as the amount of analyte in 1 ml of pooled normal plasma.
In accordance with WHO principles the objective is to assign a single value for each analyte
which is valid for use with all current methodologies. This standard is intended to be used in the
in vitro diagnostics field and relates to category 4 of the principles set out in ISO 17511.
A secondary objective is to obtain further data on the inter-laboratory variability of VWF:CB
estimates for the WHO 1st IS VWF Concentrate (00/514) relative to the WHO 5
th IS plasma. A
previous attempt to assign a value for VWF:CB to the WHO 1st Concentrate, in 2000, was
unsuccessful due to extremely large variability between laboratories and methods. The
information obtained in the present study will indicate the current status of VWF:CB testing and

WHO/BS/09.2116
Page 5
will help in formulating the strategy for replacement of the WHO 1st IS VWF Concentrate which
is scheduled for 2010.
Samples included in the collaborative study
Sample A: WHO 5th
IS Factor VIII/VWF Plasma (02/150) The WHO 5
th IS was established in 2003 with assigned values for FVIII:C (0.68 IU/ampoule),
FVIII:Ag (0.94 IU/ampoule), VWF:Ag (0.91 IU/ampoule), VWF:RCo (0.78 IU/ampoule) and
VWF:CB (0.94 IU/ampoule) (Hubbard and Heath, 2004).
Sample B: Proposed WHO 6th
IS Factor VIII/VWF Plasma (07/316) The proposed WHO 6
th IS was prepared from a pool of 80 donations from normal healthy donors
(UK National Blood Service) collected by conventional venepuncture into citrate-phosphate-
dextrose-adenine anticoagulant. Each donation was checked and found negative for HBsAg,
anti-HIV-1 and -2, anti-HCV, HCV-RNA (mini-pool testing) and syphilis. Each donation
underwent leuco-filtration before being centrifuged twice to remove all cellular components.
The units were then frozen and stored at -70oC. Plasma was thawed on the day of filling, pooled
and then buffered by the addition of HEPES (N-[2-Hydroxyethyl]piperazine-N'-[2-
ethanesulfonic acid]) to a final concentration of 40 mmol/l. One ml of the pooled plasma was
dispensed into each of approximately 20,000 ampoules. Freeze-drying was performed in
accordance with the conditions required for International standards (Campbell 1974). Details of
the filling procedure and the characteristics of the lyophilised preparation are given in the table
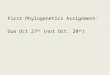
below. A comparison of the multimeric profile of von Willebrand factor in the proposed 6th
IS,
the current 5th
IS and frozen normal plasma has revealed a similar distribution for all three
preparations (Figure 1).

WHO/BS/09.2116
Page 6
DETAILS OF CANDIDATE FILL (07/316)
Presentation
sealed glass DIN ampoules
Excipients/additives
Recovered normal human plasma with additive HEPES (N-[2-
Hydroxyethyl]piperazine-N'-[2-ethanesulfonic acid]) to final
concentration of 0.04 mol/l
Liquid filling weight (g)
Mean 1.1056 g
(range 1.1010 g – 1.1095 g)
Coefficient of variation of the
liquid fill (%)
0.118 % based on 786 check-weight ampoules
Residual moisture after
lyophilisation (%)
Mean 0.30%, CV 11.8% (n = 12)
Dry weight (mg)
Mean 93.4 mg, CV 0.39% (n = 6)
Headspace oxygen (%)
Mean 0.13%, CV 57.4% (n = 12)
Reconstitution volume and fluid
1.0 ml distilled water
Number of ampoules in stock
19,300
Manufacturing site
NIBSC, Potters Bar, UK
Custodian
NIBSC, Potters Bar, UK
Storage temperature
-20 °C
Sample C: WHO 1st IS von Willebrand Factor Concentrate (00/514)
This standard was established in 2001 and was included only in the VWF:CB assays. This
standard has no assigned value for VWF:CB (Hubbard et al, 2002).
Sample N: Locally collected normal plasma pools Participants were requested to prepare two fresh normal plasma pools N1 and N2 using at least 16
different donors in total according to the instructions given in the study protocol (Appendix 1).
Fresh normal pools were preferred for the estimation of FVIII:C and VWF:RCo whereas frozen
pools were acceptable for the testing of other analytes. For FVIII:C estimates 11 laboratories
prepared fresh pools (total 227 donors), 16 laboratories prepared frozen pools (total exceeding
4,700 donors), 2 laboratories used a mixture of fresh and frozen pools (analysed as frozen pools)
(total 28 donors) and one laboratory used a commercial lyophilised normal plasma pool. For the
VWF:RCo estimates 9 laboratories prepared fresh pools (total 146 donors), 21 laboratories
prepared frozen pools (total exceeding 4,400 donors), 2 laboratories used a mixture of fresh and

WHO/BS/09.2116
Page 7
frozen pools (analysed as frozen pools) (total 26 donors) and one laboratory used a commercial
lyophilised normal plasma pool.
Participants Samples were despatched in September 2008 to 44 laboratories in 14 different countries. The
participants comprised 20 clinical laboratories, 21 manufacturers’ laboratories and 3 regulators
(Appendix 2). Results were received from all laboratories. Participating laboratories have been
assigned code numbers to retain confidentiality in the report.
Assay methods and study design Participants were asked to follow their routine assay methodology as far as possible within the
specified assay design. Most laboratories assayed more then one analyte in the study. A
summary of the assay methods used in the study and the number of estimates is given in the
following table: Analyte Total
data sets
Methods
VIII:C
53
1-stage clotting (31), 2-stage clotting (1), chromogenic (21)
VIII:Ag
11
ELISA
VWF:Ag
31
ELISA (21), immuno-turbidimetric (10)
VWF:RCo
29
aggregometry (21), visual agglutination (7), immuno-turbidimetric (1)
VWF:CB
21
ELISA-type with detection using anti-VWF conjugate
Details of the methods used by the individual laboratories are given in Appendix 3.
Participants were requested to carry out four assays for each analyte using fresh ampoules of A
and B for each assay (and fresh ampoules of sample C for each VWF:CB assay) (Appendix 1).
The four assays were split into two sessions of two assays each. It was requested that a different
normal plasma pool (N1, N2) was included in each session if possible. Participants were
requested to follow a balanced assay design in which three different dilutions of each assay
material were tested in replicate wherever possible. Since most laboratories performed more
than one assay method on the same ampoules it was specified that assays of FVIII:C and
VWF:RCo must be carried out on freshly reconstituted ampoules whereas assays for FVIII:Ag,
VWF:Ag and VWF:CB could be carried out on frozen aliquots if this was unavoidable.
Statistical analysis All assays were analysed as multiple parallel line bioassays comparing response to log
concentration (Finney 1978). Linear and parallel response lines are required for this type of
analysis. If necessary, the responses were log transformed to achieve this. The parallelism of
the assays was assessed by comparing the slopes of the dose-responses across the assays.
For each assay the following potency estimates were calculated:
• proposed 6th
IS FVIII/VWF Plasma (B) vs 5th
IS FVIII/VWF Plasma (A) using the
assigned values for the 5th
IS FVIII/VWF Plasma
• proposed 6th
IS FVIII/VWF Plasma (B) vs local normal plasma pools (N) using an
arbitrary value of 1.0 unit per ml for the local normal plasma pools.

WHO/BS/09.2116
Page 8
• 1st IS VWF Concentrate (C) vs 5
th IS FVIII/VWF Plasma (A) and vs local normal plasma
pools (N) (VWF:CB assays only).
Estimates of FVIII:C and VWF:RCo were also sub-divided into groups using fresh or frozen
normal plasma pools. This is particularly important for FVIII:C estimates where levels can be
affected by freeze-thawing. No sub-division was made for FVIII:Ag, VWF:Ag and VWF:CB.
Estimates for any analyte, where the normal pool was a lyophilised preparation (Laboratory 10)
were not included in the calculation of means.
Combined potency estimates for each laboratory were obtained by taking unweighted geometric
means of results from all assays. Overall combined estimates were obtained by taking
unweighted geometric means of the mean results from the different laboratories. Where a
laboratory performed more than one assay method, the results for each method were analysed as
if from separate laboratories. Differences in potency estimates between laboratories (outlier
detection) were assessed using a Duncan's multiple range test (Duncan 1975). Intra- and inter-
laboratory variability is expressed as the geometric coefficient of variation (GCV%) (Kirkwood
1979).
Some estimates of VWF:RCo by visual agglutination methods (titres) were not suitable for
parallel line analysis. The results returned by the participants have been included in the tables
with an indication that raw data analysis was not carried out by NIBSC.
Results and conclusions
General comments on statistical analysis The parallelism of the proposed 6
th IS FVIII/VWF Plasma and the 1
st IS VWF Concentrate
against the 5th
IS and the normal plasma pools was assessed by calculating the ratio of the slopes
of the dose-response relationships and by visual inspection of all individual assays. The overall
mean ratios of slopes for all assay methods ranged from 96.5% - 100% for estimates against the
5th
IS and from 97.3% - 105.7% for estimates against the normal plasma pools. All assays were
considered valid for inclusion in the analysis except for the exclusions detailed below. In some
cases it was necessary to exclude single data points at the extreme ends of the dose-response
relationships in order to achieve linearity. The following sets of data were excluded from the
study:
- VWF:CB estimates of the 1st IS VWF Concentrate: exclusion of 4 assays by laboratories 3, 20
and 32 due to poor dose-response and non-parallelism of the 1st IS VWF Concentrate with the 5
th
IS; exclusion of single assays by laboratories 15, 30, 44 due to possible dilution errors causing
either non-parallelism and/or non-linearity.
- VWF:Ristocetin Cofactor: exclusion of two assays for the proposed 6th
IS vs the normal pools
by laboratory 28c due to lack of dose-response of the normal pools.
- VWF:Antigen: exclusion of two assays for the proposed 6th
IS vs the normal pools by
laboratory 38 due to lack of dose-response of the normal pools.
The following estimates were identified as “outlying" results and excluded from the calculation
of the overall mean values:
- FVIII chromogenic Lab 22 for the proposed 6th
IS vs the 5th
IS
- FVIII antigen Lab 27 for the proposed 6th
IS vs the 5th
IS
- VWF collagen binding Lab 24 for the proposed 6th
IS vs the normal pools

WHO/BS/09.2116
Page 9
Intra- and Inter-laboratory variability of estimates A summary of intra-laboratory variability for estimates of the proposed 6
th IS by all methods is
given in Table 1. For all methods there was a higher percentage of laboratories with GCVs
below 5% for estimates relative to the 5th
IS than for estimates relative to the normal pools.
Similarly there were a higher percentage of laboratories with GCVs greater than 10% for
estimates relative to the normal pools. The larger intra-laboratory variability for estimates
relative to the normal pools is not surprising when we consider that most of the laboratories used
two different normal pools for their assays. Considering the intra-laboratory variability for
estimates relative to the 5th
IS it is apparent that the lowest variability (eg. most labs with GCVs
<5%) is associated with the estimates of FVIII:C, VWF:Ag and FVIII:Ag whereas the highest
variability was associated with estimates of VWF:CB. The GCVs for most of the VWF:CB
estimates (53%) fell in the range of 5 – 10%. The VWF:RCo method is generally regarded as
one of the most variable and this is supported by the finding that the GCV exceeded 10% in 29%
of laboratories.
A summary of inter-laboratory variability for estimates of the proposed 6th
IS by all methods is
given in Table 2. It is not surprising that the variability relative to the normal pools is greater
than the variability relative to the 5th
IS, for all methods, considering that each laboratory used a
different normal pool. Estimates of inter-laboratory variability based on assays relative to the 5th
IS indicated very good agreement with GCVs around 6% and below for sub-set methods and
overall combinations for FVIII:C, FVIII:antigen, VWF:antigen and VWF:CB. VWF:RCo
estimates by aggregometry also displayed low inter-laboratory variability (GCV 6.52%) whereas
the semi-quantitative estimates by visual agglutination were associated with the largest
variability (GCV 12.00%) and this has influenced the estimation of overall variability for
VWF:RCo of 8.13%.
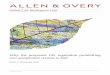
Factor VIII:C in the proposed 6th
IS FVIII/VWF Plasma (Sample B) The mean results from the individual laboratories together with the means from each method are
given in Table 3 and Figures 2a and 2b.
a) estimates vs the 5th
IS FVIII/VWF Plasma (A) One estimate was identified as an outlier (chromogenic estimate from Lab 22) and this was
excluded from the calculation of overall mean values. There was very good inter-laboratory
agreement within the 1-stage and chromogenic methods with GCVs of 2.80% (n=31) and 3.57%
(n=20) respectively. The mean values from each method were also very similar at 0.67 IU/ml
(1-stage), 0.72 IU/ampoule (2-stage) and 0.70 IU/ampoule (chromogenic), however, there was a
significant difference between the estimates for the 1-stage and chromogenic methods
(p<0.0001). Combination of potencies from all three methods (52 estimates) gave an overall
mean of 0.68 IU per ml with low inter-laboratory variability (GCV 4.06%).
b) estimates vs the normal plasma pools (N) Inter-laboratory variability (GCV) exceeded 10% within the 1-stage and chromogenic methods
for estimates relative to both fresh and frozen plasma pools. There was good agreement between
the mean values calculated relative to the fresh normal plasma pools for the 1-stage (0.56 IU/ml,
n=11) and chromogenic methods (0.61 IU/ml, n=5). Estimates calculated relative to the frozen
pools were greater for the 1-stage (0.70 IU/ml, n=19) and chromogenic methods (0.76 IU/m,
n=12) and there was a highly significant difference (p<0.0001) between all estimates calculated
relative to the fresh (mean 0.57 IU/m, n=16) and frozen pools (mean 0.72 IU/ml, n=31).

WHO/BS/09.2116
Page 10
c) comparison of estimates vs 5th
IS and fresh normal pools Comparing estimates from all laboratories and methods, relative to the 5
th IS (mean 0.68 IU/ml,
n=52), with estimates from all methods, relative to the fresh normal pools (mean 0.57 IU/ml,
n=16) indicated a highly significant difference (p<0.0001). Comparison of estimates from only
those laboratories which used both fresh normal plasma pools and the 5th
IS in the same assays
(paired t test, n=16) also indicated a highly significant difference (p<0.0001).
FVIII:C value assignment: Estimates for FVIII:C relative to the 5th
IS showed good
overall agreement both within and between the three different methods producing an overall
combined mean of 0.68 IU per ml with inter-laboratory variability (GCV) of 4.06%. Although
the mean estimates by the one-stage and chromogenic methods were similar (0.67 and 0.70
IU/ml respectively) there was a significant difference between these estimates and this reflects
the extremely good agreement between laboratories within each method (GCVs 2.80% and
3.57%). In practice the small difference between the mean values supports the calculation of a
valid overall mean value from all estimates from the 3 methods.
Estimates relative to the normal plasma pools were associated with greater inter-laboratory
variability (GCV >10%) as might be expected considering that all laboratories used different
normal pools. Moreover there was a clear and highly significant difference (p<0.0001) between
all estimates calculated relative to the fresh pools (0.57 IU/ml) and the frozen pools (0.72 IU/ml).
This was also observed in the calibration of the 5th
IS and probably reflects the lability of
FVIII:C and loss of activity following freezing and thawing. This finding invalidates the
combination of estimates calculated relative to fresh and frozen pools and limits the calculation
of the overall mean to 16 laboratories which used fresh normal pools and gives a mean value of
0.57 IU per ml (GCV 13.90 %). Comparison of estimates from those laboratories (n=16) which
included both fresh normal pools and the 5th IS in the same assays indicated a highly significant
difference (p<0.0001) with means of 0.68 and 0.57 IU per ml relative to the 5th
IS and the fresh
normal pools respectively.
Assignment of a value for FVIII:C has to reconcile the need for continuity of the unitage
between the 5th
IS and the 6th
IS and also to recognise possible drift of the IU away from the
original "plasma unit". Previously, in the calibration of the 4th
IS there was a 15% discrepancy
between the estimates relative to the 3rd IS (0.60 IU per ml) and the fresh normal pools (0.52 IU
per ml) and an attempt was made to partially rectify the difference by assigning a mean value of
0.57 IU per ampoule to the 4th IS (Hubbard et al, 2001). This correction resulted in a change in
value of the IU for FVIII:C of around 7 – 8% and was a cause of confusion for several years
until it had been assimilated by manufacturers of secondary standards. Despite this correction
the subsequent calibration of the 5th
IS revealed a discrepancy of 11% between estimates relative
to the 4th
IS and the fresh normal pools. In consideration of the extremely good stability for
FVIII:C in the 4th
IS it was accepted that the varying discrepancy was caused by “oscillation” of
the mean FVIII:C in the normal pools between studies rather than by instability of FVIII:C in the
freeze-dried 4th
IS. It was therefore agreed that the 5th
IS should be assigned the consensus mean
value from estimates against the 4th
IS (Hubbard and Heath, 2004). The results in the present
study have presented a similar scenario with the mean value for the proposed 6th
IS relative to the
fresh normal pools (0.57 IU/ml) approximately 16% lower than the mean relative to the 5th
IS
(0.68 IU/ml). This is unlikely to have been caused by instability of the 5th
IS since stability
studies have indicated that no detectable loss of FVIII:C has occurred during its lifetime
(Appendix 4). Based on previous experience with the correction applied to the 4th
IS it is
unlikely that a further re-valuation of the IU would provide a permanent “fix” to reconcile the IU
and the “fresh plasma unit”. It is therefore proposed that continuity of the IU should take

WHO/BS/09.2116
Page 11
precedence and that the 6th
IS should be assigned the mean value calculated relative to the 5th
IS
of 0.68 IU/ml.
Factor VIII: antigen in the proposed 6th
IS FVIII/VWF Plasma (Sample B) All 11 laboratories used ELISA methods to estimate FVIII:Ag (Table 4 and Figures 3a and 3b).
Estimates calculated relative to the 5th
IS showed good inter-laboratory agreement when an
outlying result (Lab 27) was excluded to give a GCV of 4.24% and an overall mean value of
1.04 IU/ml (n=10). Estimates calculated relative to the normal pools were more variable with
inter-laboratory variability (GCV) of 10.53% and an overall mean value of 0.93 IU/ml (n=11).
Estimates calculated relative to the 5th
IS were significantly different to estimates relative to the
normal pools when analysed by unpaired “t” test (p<0.01, n=10 vs n=11) and paired “t” test
(p<0.05, n=10 vs n=10).
FVIII:antigen value assignment: There was very good agreement between laboratories
for estimates relative to the 5th
IS (GCV 4.24%) and a mean value of 1.04 IU/ml was obtained.
Estimates relative to the normal plasma pools were more variable (GCV 10.5%) as expected
from the use of different pools in each laboratory and a mean of 0.93 IU/ml was obtained. The
discrepancy between estimates relative to the 5th
IS and the normal pools in the present study
(11%) is slightly larger than that found in the previous calibration of the 5th
IS (8%) and
probably reflects variability in the normal plasma pools between the two studies. In the interests
of continuity it is proposed that the 6th
IS is assigned the overall mean estimate relative to the 5th
IS of 1.04 IU/ml.
von Willebrand Factor: antigen in the proposed 6th
IS FVIII/VWF Plasma
(Sample B) Twenty-one estimates were obtained using ELISA methods and 10 using immuno-turbidimetric
methods to estimate VWF:Ag (Table 5 and Figures 4a and 4b). There were no significant
differences between the two methods for estimates calculated relative to either the 5th
IS or the
normal plasma pools. Estimates calculated relative to the 5th
IS showed excellent inter-
laboratory agreement within both methods with inter-laboratory variability (GCV) of 5.17% and
1.46 % for the ELISA and immuno-turbidimetric methods respectively. Combining all estimates
relative to the 5th
IS gave an overall mean of 1.00 IU/ml (n=31) with inter-laboratory variability
of 4.29%. Estimates relative to the normal pools showed increased inter-laboratory variability
(overall GCV 12.92%) with an overall mean of 0.89 IU/ml (n=30). There was a highly
significant difference (p<0.0001) between the estimates calculated relative to the 5th
IS and the
normal plasma pools.
VWF:Antigen value assignment: Good agreement was found between the two methods
for estimates of the proposed 6th
IS vs the 5th
IS and for the proposed 6th
IS vs the normal pools.
However, there was a significant difference between estimates of the proposed 6th
IS vs the 5th
IS
(mean 1.00 IU/ml) and the normal pools (mean 0.89 IU/ml). This represents an 11%
discrepancy between the IU and the “plasma unit” and is much larger than that found in the
calibration of the previous 5th
IS where there was only a 2% difference, however in the earlier
calibration of the 4th
IS there was a 12% difference (Hubbard, 2006). Considering the good
stability of VWF:antigen in the lyophilised standards it is once again most likely that the
discrepancies are caused by variability in the normal pools between studies and decisions to
adjust the value of the IU should be undertaken with caution. It is proposed that continuity of the
IU should once again take precedence and it is recommended that the 6th
IS is assigned the mean
value relative to the 5th
IS of 1.00 IU per ml.

WHO/BS/09.2116
Page 12
von Willebrand Factor: Ristocetin Cofactor in the proposed 6th
IS FVIII/VWF
Plasma (Sample B) Twenty-one estimates were obtained using aggregometric methods and 7 estimates were
obtained using visual agglutination methods (Table 6 and Figures 5a and 5b). One laboratory
used an immuno-turbidimetric method for VWF activity and this result was not included in the
calculation of overall means. Estimates calculated relative to the 5th
IS using the aggregometric
methods gave a mean value of 0.86 IU/ml (n=21) and good agreement between laboratories
(GCV 6.52%); these estimates were not significantly different to the estimates obtained relative
to the 5th
IS using visual agglutination methods (mean 0.90 IU/ml, n=7). Estimates calculated
relative to the normal pools were much more variable with inter-laboratory GCVs ranging from
10 to 28%. There was no significant difference between the use of fresh and frozen pools for
estimates obtained using aggregometric methods, however, there was a significant difference
(p<0.05) between fresh (mean 0.80 IU/ml, n=8) and frozen pools (mean 0.94 IU/ml, n=20) when
estimates from all methods where included (excluding the immuno-turbidimetric method).
There was no significant difference between all estimates relative to the 5th
IS (mean 0.87 IU/ml,
n=28) and all estimates relative to the normal pools (mean 0.90 IU/ml, n=28).
VWF:Ristocetin cofactor value assignment: Estimates calculated relative to the 5th
IS
using aggregometric methods showed low inter-laboratory variability (GCV 6.52%) whereas
there was larger variability for the estimates based on visual agglutination (GCV 12.0%). This is
not surprising since the visual agglutination method is a semi-quantitative procedure with a
subjective aspect to end-point detection. However, combination of all estimates relative to the
5th
IS provided a valid mean of 0.87 IU/ml with acceptable overall inter-laboratory variability
(GCV) of 8.13 %. In contrast the estimates relative to the normal pools were much more
variable between laboratories (GCVs 10 – 28%) and this has compromised the conclusions from
statistical analysis. The variability of the method coupled with the variability between the
different normal pools has obscured any meaningful conclusions regarding the use of fresh or
frozen pools or agreement between methods relative to the normal pools. It is therefore not
possible to consider the estimates relative to the normal pools in the proposed assigned value for
the 6th
IS, except to note that the combined estimates relative to the normal pools (mean 0.90
IU/ml) are not significantly different to the combined estimates relative to the 5th
IS (mean 0.87
IU/ml). It is proposed that the 6th
IS is assigned the mean value relative to the 5th
IS of 0.87
IU/ml.
von Willebrand Factor: collagen binding in the proposed 6th
IS FVIII/VWF
Plasma (Sample B) Twenty one estimates were obtained using a range of different collagen reagents (Table 7 and
Figures 6a and 6b). There were no significant differences between estimates obtained with the
type III collagen reagents and those using type I and type I/III mix reagents when calculated
relative to the 5th
IS or the normal plasma pools. Estimates calculated relative to the 5th
IS, were
associated with very good inter-laboratory agreement (GCV 5.8%) with an overall mean of 1.03
IU per ml (n=21). Analysis of estimates calculated relative to the normal plasma pools revealed
one outlier (Lab 24) which was not included in the calculation of the overall means. Estimates
relative to the normal pools were more variable (GCV 12.24%, n=20) with an overall mean of
0.99 IU per ml, however, these estimates were not significantly different to the estimates
calculated relative to the 5th
IS.
VWF:collagen binding value assignment: There was good agreement between the use
of different collagen reagents and between the estimates relative to both the 5th
IS (mean 1.03

WHO/BS/09.2116
Page 13
IU/ml, GCV 5.80 %) and the normal pools (mean 0.99 IU/ml, GCV 12.24%). These results
provide a robust basis for the proposal that the 6th
IS is assigned the mean value relative to the 5th
IS of 1.03 IU/ml.
von Willebrand Factor: collagen binding in the 1st IS VWF Concentrate (C)
Eighteen estimates were obtained using a range of different collagen reagents (Table 8 and
Figures 7a and 7b). There were no significant differences between estimates obtained with the
type III collagen reagents and those using type I and type I/III mix reagents when calculated
relative to the 5th IS or the normal plasma pools. Estimates calculated relative to the 5th
IS, were
slightly less variable between laboratories (GCV 19.51%, mean 10.74 IU/ml, n=18) and not
significantly different to estimates relative to the normal pools (GCV 25.39%, mean 10.75 IU/ml,
n=18).
Comments on VWF:collagen binding estimates for the 1st IS VWF Concentrate:
The 1st IS VWF Concentrate was included in the present study to provide further information on
the inter-laboratory variability associated with the comparison of concentrate vs plasma samples
prior to the collaborative study to calibrate the proposed 2nd
IS VWF Concentrate which is
scheduled for Autumn 2009. As expected the inter-laboratory variability for estimates of the 1st
IS Conc vs the 5th
IS Plasma (GCV 19.5%) was greater than estimates of the proposed 6th
IS
Plasma vs the 5th
IS Plasma (GCV 5.8%). These data support the “like vs like” principle in that
a plasma standard is not ideal for the estimation of VWF:CB in concentrates. The previous
attempt to assign a value to the 1st IS Conc by assay relative to the 4
th IS Plasma in 2000 was
unsuccessful due to the extremely large variability between laboratories (GCV 40%) and a
marked difference between estimates obtained using type III and type I/III mix collagen reagents
(Hubbard et al, 2002). In contrast the results from the present study indicated much better
agreement between the use of different collagen types and improved overall inter-laboratory
variability relative to the 5th
IS (GCV 19.5%). These results are very encouraging and, if
reproducible, they show promise for the value assignment of the proposed 2nd
IS VWF
Concentrate for VWF:CB in 2010.
Stability of the proposed WHO 6th
IS FVIII/VWF Plasma
Accelerated degradation study Stability of the proposed 6
th IS has been assessed in an accelerated degradation study which
allows the estimation of predicted loss per year based on the observed loss occurring in ampoules
stored at elevated temperatures (Kirkwood and Tydeman 1984). The study involved 8
laboratories and the testing of 6 analytes (FVIII:C 1-stage, FVIII:C chromogenic, FVIII:antigen,
VWF:antigen, VWF:RCo, VWF:CB). Results were obtained from 2 different laboratories for
each analyte. The residual potencies of ampoules stored at 4, 20, 37 and 45 oC after storage for 7
or 9 months are given in Table 9 expressed as a % relative to ampoules stored at -20oC. Some
laboratories reported problems in the reconstitution and testing of the ampoules stored at +45 °C.
The results from this initial testing are very encouraging and indicate that all analytes in the
proposed 6th
IS are extremely stable when stored at the bulk storage temperature of -20oC with
the mean predicted losses per year of 0.074% for FVIII:C 1-stage, 0.146% for FVIII:C
chromogenic, 0.049% for FVIII:antigen, 0.00% for VWF:antigen, 0.022% for VWF:ristocetin
cofactor and 0.002% for VWF:collagen binding.
Stability after reconstitution Although the Instructions for Use will recommend that assays are performed as soon as possible
after reconstitution it is useful to indicate a suitable period of use. In common with previous

WHO/BS/09.2116
Page 14
WHO Plasma Standards for blood coagulation factors it is recommended that the standard is
transferred, after reconstitution, to a plastic tube in order to prevent activation by the glass
surface of the ampoule. Recommendations for the storage after reconstitution have been limited
to the period of storage on melting ice since local ambient temperature can vary considerably.
Results from two separate tests on the most labile analyte (FVIII:C), performed at NIBSC,
indicated that 99% and 101% respectively, of the starting concentration of FVIII:C was retained
after 3 hours for the freshly reconstituted standard when stored in melting ice in plastic tubes.
This period is sufficient for numerous assays to be performed. The use of frozen aliquots of the
proposed 6th
IS for the estimation of FVIII:C, VWF:RCo and VWF:CB is not recommended.
The use of frozen aliquots for the estimation of FVIII:antigen and VWF:antigen requires local
validation.
References Campbell PJ (1974) International biological standards and reference preparations. 1. Preparation
and presentation of materials to serve as standards and reference preparations. J Biol
Standardisation 2; 249-67
Duncan DB (1975) T-tests and intervals for comparisons suggested by the data. Biometrics 31;
339-359
Finney DJ (1978) Statistical methods in biological assay. 3rd
edition Charles Griffin. London.
Hubbard AR, Rigsby P & Barrowcliffe TW (2001) Standardisation of Factor VIII and von
Willebrand Factor in plasma: calibration of the 4th International Standard. Thrombosis and
Haemostasis 85; 634-638
Hubbard AR, Sands D, Chang AC & Mazurier C (2002) Standardisation of von Willebrand
Factor in therapeutic concentrates: calibration of the 1st International Standard for von
Willebrand Factor Concentrate (00/514). Thrombosis and Haemostasis 88; 380-386
Hubbard AR and Heath AB (2004) Standardization of factor VIII and von Willebrand factor in
plasma: calibration of the WHO 5th International Standard (02/150). Journal of Thrombosis and
Haemostasis 2, 1380-4
Hubbard AR (2006) von Willebrand Factor standards for plasma and concentrate testing. Semin
Thromb Hemost 32; 522-528
Kirkwood TBL (1979) Geometric means and measures of dispersion. Biometrics 35; 908-9
Kirkwood TBL & Tydeman MS (1984) Design and analysis of accelerated degradation tests for
the stability of biological standards II. A flexible computer program for data analysis. J Biol
Standardisation 12; 207-14
Acknowledgements We are very grateful to the participants in this calibration exercise for their considerable efforts
in performing the assays; to Prof Dr Ulrich Budde for the VWF multimer gel electrophoresis; to
the Standards Processing Division (NIBSC) for preparing the ampouled materials and despatch
of samples, and finally to the chairs and members of the ISTH/SSC sub-committees for
FVIII/FIX and von Willebrand Factor for their support.

WHO/BS/09.2116
Page 15
Instructions for Use The draft Instructions for Use for the proposed WHO 6
th IS Factor VIII / von Willebrand factor,
plasma are found in Appendix 5.
Table 1: Intra-laboratory variability for estimates of the proposed 6th
IS by all methods
assays vs 5th
IS
assays vs normal pools Analyte
GCV < 5% GCV > 10%
GCV < 5% GCV > 10%
Factor VIII: C
41/53 (77%) 3/53 (6%) 21/49 (43%) 10/49 (20%)
Factor VIII: Ag
7/11 (64%) 2/11 (18%) 2/11 (18%) 2/11 (18%)
VWF: Ag
21/31 (68%) 4/31 (13%) 11/31 (35%) 9/31 (29%)
VWF: RCo
13/28 (46%) 8/28 (29%) 10/28 (36%) 9/28 (32%)
VWF: CB
6/21 (29%) 3/21 (14%) 3/21 (14%) 9/21 (43%)
Figures indicate numbers of laboratories with GCV <5% or >10%
Table 2: Summary of inter-laboratory variability (GCV%) for estimates of the proposed 6
th IS by
all methods
Analyte and method
assays vs 5th IS assays vs normal pools
Factor VIII:C
1-stage clotting
Chromogenic
Overall
2.80%
3.57 % (ex lab 22)
4.06% (ex lab 22)
fresh 10.29%; frozen 14.16%
fresh 20.28%; frozen 11.04%
fresh 13.90%; frozen 13.54%
Factor VIII: antigen
4.24% (ex lab 27) 10.53%
VWF: antigen
ELISA
Immuno-turbidimetric
Overall
5.17%
1.46%
4.29%
13.14%
12.51%
12.92%
VWF: ristocetin cofactor
Aggregometry
Visual agglutination
Overall
6.52%
12.00%
8.13%
fresh 10.42%; frozen 30.60%
fresh* ----; frozen 24.16%
fresh 9.62%; frozen 28.26%
VWF: collagen binding
Type I/III mix collagen
Type III collagen
Overall
5.09%
6.37%
5.80%
15.58% (ex lab 24)
11.77%
12.24% (ex lab 24)
* - estimates from only 1 laboratory

WHO/BS/09.2116
Page 16
Table 3: Estimates for FVIII:C (IU per ml) in the Proposed 6th IS FVIII/VWF Plasma (07/316)
relative to the 5th IS FVIII/VWF Plasma (02/150) and the normal plasma pools Method Laboratory vs 5th IS (A)
n mean GCV%
vs normal pools (N)
n mean GCV%
2
3
4
5
6
7
10
11 12
13
16 17
18
19 20
21 23
24
25 27
29
30
32
33
34
35
36
37 38
43
44
4 0.68 3.28
4 0.65 3.47
4 0.66 3.41
4 0.68 2.09
4 0.67 2.06
4 0.67 2.24
4 0.64 7.98
4 0.65 4.69 4 0.67 2.00
4 0.67 5.62
4 0.67 7.83 4 0.70 3.50
4 0.68 4.11
4 0.64 11.91 4 0.66 0.26
4 0.69 3.46 4 0.65 5.79
4 0.66 0.62
4 0.64 4.22 4 0.68 4.33
4 0.66 2.01
4 0.63 1.77
4 0.69 3.35
4 0.67 2.19
4 0.66 1.09
4 0.67 2.19
5 0.69 4.20
4 0.69 3.12 4 0.67 6.29
4 0.70 3.35
4 0.69 3.07
4 0.70 12.09*
4 0.88 8.45†
4 0.86 2.97†
4 0.59 4.91*
4 0.65 6.66†
4 0.62 7.07†
4 0.79 1.81‡
4 0.64 6.23† 4 0.63 2.88†
3 0.74 12.04†
4 0.64 4.35† 4 0.72 3.63†
4 0.71 13.14†
4 0.50 20.31* 4 0.64 4.34†
4 0.55 9.14* 4 0.90 12.06†
4 0.67 1.50†
4 0.65 5.19† 4 0.68 22.61†
4 0.57 5.59*
4 0.55 5.54†
4 0.65 8.11†
4 0.49 5.38*
4 0.57 4.46*
4 0.60 4.93*
5 0.52 42.71*
4 0.54 7.43* 4 0.80 12.32†
4 0.75 3.48†
4 0.57 6.22*
1-stage clotting
Mean 31 0.67 2.80 Fresh 11 0.56 10.29
Frozen 19 0.70 14.16
26
4 0.72 2.86
no pool
2-stage clotting
Mean 1 0.72 ------ -- ----- -----
3
5
8
10
13
14
16 18
21
22 23
24
28 29
34
39
41
42
43a
43b
44
4 0.73 3.81
4 0.70 2.18
4 0.71 6.51
4 0.70 2.45
4 0.71 0.89
4 0.69 7.39
4 0.72 5.83 4 0.74 4.63
4 0.68 2.70
4 1.14 12.46 4 0.66 10.10
4 0.71 1.33
4 0.71 2.26 4 0.77 2.20
4 0.68 1.38
4 0.71 3.04
4 0.72 0.66
4 0.69 3.08
4 0.67 2.40
4 0.70 4.56
4 0.69 8.32
4 0.89 8.36†
4 0.57 5.94*
4 0.74 2.14†
4 0.76 1.00‡
4 0.76 3.86†
no pool
4 0.67 3.84† 4 0.76 21.31†
4 0.59 9.11*
4 0.73 17.48† 4 0.96 6.79†
4 0.70 1.80†
4 0.77 10.73† 4 0.82 7.33*
4 0.59 3.18*
no pool
no pool
4 0.67 2.76†
4 0.74 2.10†
4 0.73 3.83†
4 0.50 3.28*
Chromogenic
Mean
Exc Lab 22
21 0.72 11.75
20 0.70 3.57
Fresh 5 0.61 20.28
Frozen 12 0.76 11.04
Overall mean estimate
Exc Lab 22
52 0.68 4.06
Fresh 16 0.57 13.90
Frozen 31 0.72 13.54
* - fresh normal pools, † - frozen normal pools, ‡ - lyophilised pools
NOTES: GCV – geometric coefficient of variation for intra-laboratory variability (individual laboratories) and inter-laboratory
variability (combined mean values). Labs 17 and 38 used a mixture of fresh and frozen pools – the laboratory mean values have
been included as frozen pools in the calculation of overall mean values. Lab 10 used a lyophilised pool – this result has not been
included in the combined results.

WHO/BS/09.2116
Page 17
Table 4: Estimates for FVIII:antigen (IU per ml) in the Proposed 6
th IS FVIII/VWF Plasma
(07/316) relative to the 5th
IS FVIII/VWF Plasma (02/150) and the normal plasma pools Method Laboratory vs 5
th IS
n mean GCV%
vs normal pools
n mean GCV%
ELISA
3
9
11
15
17
22
24
27
28
29
40
4 1.01 1.98
4 1.06 4.33
4 1.02 1.45
4 1.10 4.05
4 0.99 7.67
4 1.11 13.57
4 1.01 2.39
4 1.26 21.46
3 1.05 4.64
4 0.99 3.46
4 1.06 12.82
4 0.93 8.41
4 0.94 7.81
4 0.80 5.52
4 0.79 33.36
4 1.01 5.63
4 1.03 6.60
4 0.85 1.83
4 0.99 24.99
3 0.90 4.26
4 1.06 5.24
4 0.99 9.28
Overall mean estimate
Excluding Lab 27
11 1.06 7.35
10 1.04 4.24
11 0.93 10.53
GCV – geometric coefficient of variation for intra-laboratory variability (individual laboratories) and inter-laboratory variability
(combined mean values).

WHO/BS/09.2116
Page 18
Table 5: Estimates for VWF:antigen (IU per ml) in the Proposed 6th
IS FVIII/VWF Plasma
(07/316) relative to the 5th
IS FVIII/VWF Plasma (02/150) and the normal plasma pools Method Laboratory vs 5
th IS
n mean GCV%
vs normal pools
n mean GCV%
3
8
9
11
12
13
16
18
19
22
23
26
27
28
30
31
35
36b
37
42
43
4 0.94 4.08
4 0.94 1.09
4 0.99 2.51
4 0.99 3.52
4 0.93 23.07
4 0.98 4.86
8 1.01 5.26
4 1.06 15.58
4 0.93 8.58
4 1.02 7.72
4 1.13 3.87
4 1.02 5.54
4 1.05 3.14
4 1.01 4.71
4 0.92 16.32
4 1.06 12.78
4 1.00 1.67
5 1.01 5.78
4 1.01 1.59
4 1.02 3.17
4 1.00 5.25
4 0.95 7.05
4 0.89 1.62
4 1.01 3.82
4 0.90 7.63
4 0.99 31.86
4 0.76 2.16
8 0.83 21.48
4 0.79 14.90
4 0.89 20.25
4 1.10 3.75
4 0.95 8.49
2 0.70 6.06
4 0.98 24.73
4 0.88 21.89
4 0.83 7.31
4 1.11 8.79
4 0.92 9.89
5 0.79 37.27
4 0.78 3.19
4 0.81 3.23
4 0.76 3.01
ELISA
Mean 21 1.00 5.17 21 0.88 13.14
2
4
6
7
10
33
34
36a
38
44
4 1.00 1.37
4 1.00 3.10
4 1.00 2.60
4 0.99 1.04
4 0.98 1.78
4 0.99 2.88
2 0.98 1.07
5 1.01 2.67
4 1.03 2.96
4 1.00 1.37
4 0.90 5.36
4 1.09 5.42
4 0.85 9.02
4 1.04 2.85
4 0.89 1.93
4 0.90 3.33
2 0.81 12.41
5 0.80 34.69
2 1.06 0.51
4 0.90 5.36
Immuno-
turbidimetric
Mean 10 1.00 1.46 9 0.92 12.51
Overall mean estimate
31 1.00 4.29
30 0.89 12.92
GCV – geometric coefficient of variation for intra-laboratory variability (individual laboratories) and inter-laboratory variability
(combined mean values). Lab 10 used a lyophilised pool – this result has not been included in the combined result for estimates vs the normal pools.

WHO/BS/09.2116
Page 19
Table 6: Estimates for VWF:ristocetin cofactor (IU per ml) in the Proposed 6th
IS FVIII/VWF
Plasma (07/316) relative to the 5th
IS FVIII/VWF Plasma (02/150) and the normal plasma pools
Method Laboratory vs 5th IS
n mean GCV%
vs normal pools
n mean GCV%
1
2
3
4
5
12
18
19
20
21
25
28b
28c
29
30
31
33
34
37
38
42
4 0.90 5.69
4 0.80 2.22
4 0.87 1.50
4 0.83 15.01
4 0.82 12.10
4 0.81 1.34
4 0.92 1.60
4 0.85 5.68
4 0.81 27.66
4 0.90 4.90
4 0.85 4.62
4 0.88 1.24
4 0.90 6.55
4 0.88 1.32
4 0.90 13.15
4 0.99 5.62
4 0.74 23.55
2 0.92 4.56
4 0.88 2.49
4 0.89 8.50
4 0.83 12.21
4 1.05 4.34†
4 0.88 11.05*
4 1.13 6.09†
4 1.03 4.95†
4 0.55 25.76†
4 0.81 5.39†
4 0.91 7.43†
4 0.82 13.86*
4 0.86 20.92†
4 0.84 16.84*
4 1.13 4.57†
4 1.30 0.83†
2 1.36 3.51†
4 0.90 9.29*
4 0.59 16.41†
4 0.80 11.35†
4 0.69 26.17*
2 0.79 2.09*
4 0.72 1.56*
4 1.00 5.62†
4 0.77 12.70†
aggregometry
Mean 21 0.86 6.52 Fresh 7 0.80 10.42
Frozen 14 0.92 30.60
All 21 0.88 26.08
7+
8+
22
26
28a+
43+
44+
4 0.78 2.70
4 0.78 0.00
4 0.87 8.51
4 0.92 12.80
4 0.92 4.55
4 1.03 7.28
4 1.02 42.57
4 0.84 1.38†
4 0.99 0.00†
4 0.95 5.69†
4 0.72 7.93†
4 1.15 5.71†
4 1.32 7.63†
4 0.80 3.84*
visual
agglutination
Mean 7 0.90 12.00 Fresh 1 0.80 -----
Frozen 6 0.98 24.16
All 7 0.95 23.53
immuno-
turbidimetric
10 4 0.85 5.14 4 0.99 2.69‡
Overall mean estimate
(excluding Lab 10)
28 0.87 8.13
Fresh 8 0.80 9.62
Frozen 20 0.94 28.26
All 28 0.90 25.29
* - fresh normal pools, † - frozen normal pools, ‡ - lyophilised pools + - laboratory's own analysis
NOTES: GCV – geometric coefficient of variation for intra-laboratory variability (individual laboratories) and inter-laboratory
variability (combined mean values). Lab 38 used a mixture of fresh and frozen pools – the laboratory mean value has been
included as a frozen pool in the calculation of overall mean values. Lab 10 used an immuno-turbidimetric method and a
lyophilised pool – these results have not been included in the combined results.

WHO/BS/09.2116
Page 20
Table 7: Estimates for VWF:collagen binding (IU per ml) in the Proposed 6th
IS FVIII/VWF
Plasma (07/316) relative to the 5th
IS FVIII/VWF Plasma (02/150) and the normal plasma pools
Collagen Reagent Laboratory vs 5th IS (A)
n mean GCV%
vs normal pools (N)
n mean GCV%
5
15
18
24
28a
31
44
4 0.98 5.70
4 1.11 6.89
4 1.03 9.65
4 1.00 11.28
4 1.06 5.33
4 0.96 10.11
4 1.00 3.63
4 1.01 4.37
4 0.91 40.10
4 0.87 17.79
4 1.70 60.64
4 1.28 6.77
4 1.02 9.14
4 0.88 14.16
Type I and Type
I/III mix
Mean 7 1.02 5.09 7 1.07 27.72
6* 0.99 15.58 *exc Lab 24
1
3
11
20
23
25
28b
30
32
34
37
40
43
4 1.09 5.21
4 1.16 6.48
4 1.03 4.59
4 1.06 2.02
4 1.10 1.60
4 1.02 9.14
4 1.01 6.62
4 0.91 9.68
4 1.06 4.45
4 1.12 2.16
4 1.01 3.40
4 1.01 13.27
4 1.00 6.74
4 1.04 7.33
4 1.10 30.33
4 0.94 16.28
4 1.02 9.95
4 0.96 5.96
4 1.15 5.05
4 1.12 5.47
4 0.90 20.08
4 0.88 3.01
4 0.89 9.95
4 0.79 1.06
4 1.01 17.32
4 1.08 6.62
Type III
Mean 13 1.04 6.37 13 0.99 11.77
Not specified 27 4 1.01 6.62 4 0.99 14.78
Overall mean estimate
21 1.03 5.80
21 1.01 17.79
20* 0.99 12.24 *exc Lab 24
GCV – geometric coefficient of variation for intra-laboratory variability (individual laboratories) and inter-laboratory variability
(combined mean values).

WHO/BS/09.2116
Page 21
Table 8: Estimates for VWF:collagen binding (IU per ml) in the 1st IS VWF Concentrate (00/514)
relative to the 5th
IS FVIII/VWF Plasma (02/150) and the normal plasma pools
Collagen Reagent Laboratory vs 5th IS (A)
n mean GCV%
vs normal pools (N)
n mean GCV%
5
15
18
24
28a
31
44
4 11.16 8.04
4 11.75 32.32
4 10.69 12.49
4 8.08 19.55
4 11.97 6.12
4 9.67 11.35
4 7.10 4.60
4 11.52 12.52
4 10.28 35.92
4 9.02 10.26
4 14.83 22.96
4 14.24 8.22
4 10.25 11.15
4 6.43 22.91
Type I and Type
I/III mix
Mean 7 9.90 22.04 7 10.58 32.88
1
11
23
25
28b
30
34
37
40
43
4 13.26 4.48
4 11.18 2.57
4 13.22 8.94
4 12.96 5.56
4 12.02 6.23
4 8.93 4.96
4 13.09 1.84
4 9.70 2.66
4 10.16 14.15
4 11.87 9.93
4 12.69 3.86
4 10.23 12.82
4 11.56 5.68
4 14.61 7.55
4 13.28 5.88
4 9.28 7.75
4 10.37 9.87
4 7.58 2.02
4 10.08 15.05
4 12.82 3.53
Type III
Mean 10 11.54 15.31 10 11.06 21.66
Not specified 27 4 9.28 5.04 4 9.05 20.40
Overall mean estimate
18 10.74 19.51
18 10.75 25.39
GCV – geometric coefficient of variation for intra-laboratory variability (individual laboratories) and inter-laboratory variability
(combined mean values).
Table 9: Results from the accelerated degradation study on the proposed WHO 6th
IS
Residual potencies after storage
(% vs -20 °C ampoules)
Analyte Lab ID
+4°C +20°C +37°C +45°C
Mean predicted % loss per
year at -20 °C (and 95 %
upper conf limit of loss)
FVIII:C
1-stage clotting
A†
B*
98
97
90
90
36
43
17
18
0.074% (0.179%)
FVIII:C
chromogenic
A†
B*
100
104
88
91
32
41
26
33
0.146% (0.546%)
FVIII:Antigen
A*
B*
94
96
89
93
33
49
----
----
0.049% (0.403%)
VWF:Antigen
A†
B*
97
103
97
101
42
38
2
----
0.000% (0.000%)
VWF:RCo
A*
B*
101
96
102
76
30
----
----
----
0.022% (0.516%)
VWF:CB
A†
B*
102
98
105
97
69
47
76
----
0.002% (0.021%)
† - tested after storage for 7 months; * - tested after storage for 9 months;
Results are the mean values from 3 independent assays

WHO/BS/09.2116
Page 22
Figure 1: Von Willebrand factor multimer profile for the proposed WHO 6th
IS, the
current WHO 5th
IS and frozen normal plasma (agarose gel medium resolution)
1 Frozen normal plasma
2 Proposed WHO 6th
IS (07/316)
3 WHO 5th
IS (02/150)

WHO/BS/09.2116
Page 23
Figure 2a: Factor VIII:C in the proposed 6th
IS relative to the 5th
IS
0
2
4
6
8
10
12
14
16
18
20
22
24
% of Overall Mean
50 55 60 65 70 75 80 85 90 95 100 105 110 115 120 125 130 135 140 145 150
03
04
10
11
19
20
23
23
24
25
29
30
34
02
05
06
07
12
13
14
16
18
21
21
27
32
33
34
35
36
37
38
42
43.1
44
44
03
05
08
10
13
16
17
24
26
28
39
41
43
43.2
18 29
Figure 2b: Factor VIII:C in the proposed 6th
IS relative to the normal pools
0
1
2
3
4
5
6
7
8
9
10
% of Overall Mean
50 55 60 65 70 75 80 85 90 95 100 105 110 115 120 125 130 135 140 145 150
19*
33*
36*
44*
21*
37*
05*
29*
30
34*
44*
05*
07
21*
34*
35*
06
11
12
16
20
25
32
16
24
27
42
02*
18
24
08
13
17
22
43
43.1
43.2
10‡
13
18
28
10‡
38
29* 03
04
03
23
23
* - fresh pools ‡ - lyophilised pool
*

WHO/BS/09.2116
Page 24
Figure 3a: Factor VIII:antigen in the proposed 6th
IS relative to the 5th
IS
0
1
2
3
4
5
6
7
8
9
10
% of Overall Mean
50 55 60 65 70 75 80 85 90 95 100 105 110 115 120 125 130 135 140 145 150 155
03
17
24
29
09
11
28
40
15
22
27
Figure 3b: Factor VIII antigen in the proposed 6th
IS relative to the normal pools
0
1
2
3
4
5
6
7
8
9
10
% of Overall Mean
50 55 60 65 70 75 80 85 90 95 100 105 110 115 120 125 130 135 140 145 150
11
15
24 28 03
09
27
40
17
22
29

WHO/BS/09.2116
Page 25
Figure 4a: VWF:antigen in the proposed 6th
IS relative to the 5th
IS
0
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
% of Overall Mean
50 55 60 65 70 75 80 85 90 95 100 105 110 115 120 125 130 135 140 145 150
30 03
08
12
19
02
04
06
07
09
10
11
13
16
22
26
28
33
34
35
36a
36b
37
42
43
44
18
27
31
38
23
Figure 4b: VWF:antigen in the proposed 6th
IS relative to the normal pools
0
1
2
3
4
5
6
7
8
9
10
% of Overall Mean
50 55 60 65 70 75 80 85 90 95 100 105 110 115 120 125 130 135 140 145 150
26 13
43
18
34
36a
36b
37
42
06
16
30
02
08
10‡
11
19
28
33
44
03
23
35
12
27
07
09
38 04
22
31

WHO/BS/09.2116
Page 26
Figure 5a: VWF:Ristocetin Cofactor in the proposed 6th
IS relative to the 5th
IS
0
1
2
3
4
5
6
7
8
9
10
% of Overall Mean
50 55 60 65 70 75 80 85 90 95 100 105 110 115 120 125 130 135 140 145 150
33 02
07
08
04
05
12
20
42
03
10
19
22
25
28b
29
37
38
01
18
21
26
28a
28c
30
34
31
44
43
Figure 5b: VWF:Ristocetin Cofactor in the proposed 6th
IS relative to the normal pools
0
1
2
3
4
5
6
7
8
9
10
% of Overall Mean
50 55 60 65 70 75 80 85 90 95 100 105 110 115 120 125 130 135 140 145 150 155
05* 30 26
33*
37*
42 12
19*
31
34*
44*
07
20
21*
02*
29*
18
22
08
10‡
04
38
01 03
25
28a 28b 28c
43

WHO/BS/09.2116
Page 27
Figure 6a: VWF:Collagen Binding in the proposed 6th
IS relative to the 5th
IS
0
1
2
3
4
5
6
7
8
9
10
% of Overall Mean
50 55 60 65 70 75 80 85 90 95 100 105 110 115 120 125 130 135 140 145 150
30
32
05
24
31
43
44
11
18
25
27
28B
37
40
01
20
23
28A
15
34
03
Figure 6b: VWF:Collagen Binding in the proposed 6th
IS relative to the normal pools
0
1
2
3
4
5
6
7
8
9
10
% of Overall Mean
50 55 60 65 70 75 80 85 90 95 100 105 110 115 120 125 130 135 140 145 150
37 15
18
30
32
34
44
11
23
05
27
40
01
20
31
03
43
25
28B
28A

WHO/BS/09.2116
Page 28
Figure 7a: VWF:Collagen Binding in the 1st IS VWF Concentrate relative to the 5
th IS
0
1
2
3
4
5
6
7
8
9
10
% of Overall Mean
50 55 60 65 70 75 80 85 90 95 100 105 110 115 120 125 130 135 140 145 150
44 24 27
30
31
37
40 18 05
11
15
28A
28B
43
25
34
01
23
Figure 7b: VWF:Collagen Binding in the 1st IS VWF Concentrate relative to the normal
pools
0
1
2
3
4
5
6
7
8
9
10
% of Overall Mean
50 55 60 65 70 75 80 85 90 95 100 105 110 115 120 125 130 135 140 145 150
44 37 18
27
30
11
15
31
34
40
05 23 01
43
28B 28A 25 24

WHO/BS/09.2116
Page 29
Appendix 1: Study protocol provided to participants
1 SAMPLES INCLUDED IN THE ASSAYS
A - 5
th International Standard Factor VIII/VWF Plasma (02/150)
B - Proposed 6th
International Standard Factor VIII/VWF Plasma (07/316)
C - 1st International Standard VWF Concentrate (00/514) (VWF:CB assays only)
N1, N2 - fresh normal plasma pools prepared locally by participants (see section 5)
Samples A and B are pooled normal plasmas. Sample C is a purified concentrate for inclusion
only in VWF:CB assays – it has a nominal VWF:CB content of 8 – 10 IU/ampoule. All plasma
donations used to prepare samples A, B and C have been tested and found negative for HBsAg,
antibodies to HIV-1 and -2, antibodies to HCV and for the presence of HCV RNA (mini-pools).
2 STORAGE AND RECONSTITUTION OF SAMPLES A, B AND C
Store the unopened ampoules of A, B and C at -20
oC or below. Allow the ampoules to warm to
room temperature before reconstitution. Tap ampoules gently to ensure that all of the contents
are in the lower part of the ampoules. Reconstitute by adding 1.0 ml of distilled water at room
temperature. Dissolve the contents with gentle agitation at room temperature. When
reconstitution is complete transfer the entire contents to stoppered plastic tubes and store at 4oC
during the assay period.
3 GENERAL PLAN OF THE STUDY
You are requested to carry out 4 assays by each method using fresh ampoules for each assay. If
you are measuring 1 or 2 different analytes only 4 ampoules of A, B (and C where applicable)
are provided (plus 1 spare ampoule of each) and it will therefore be necessary to carry out more
than one assay method on each ampoule (where applicable). If you are measuring 3 or more
analytes then extra ampoules of A, B and C will be supplied. Please ensure that sufficient
volume is available for all of the assay methods you are using. Please let me know if you require
more ampoules.
Assays for FVIII:C and VWF:RCo must be carried out on freshly reconstituted ampoules of A
and B and fresh normal pools (N1, N2). If both of these methods are being carried out they
should ideally be performed at the same time. If this is not possible please carry out the assays
of FVIII:C first followed by assays for VWF:RCo.
Assays for FVIII:Ag and VWF:Ag should preferably be carried out on fresh samples but may
be carried out on frozen aliquots where unavoidable.
Assays for VWF:CB should preferably be carried out on fresh samples but may be carried out
on frozen aliquots where unavoidable. Sample C should be included only in VWF:CB assays.
The 4 assays should be spread over 2 separate days/sessions as follows:
Assay session
Normal pool Ampoules of A and B
(and C where applic)
Assay number
1 1 Day 1 N1
2 2
3 3 Day 2 N2
4 4

WHO/BS/09.2116
Page 30
If you are unable to prepare the two fresh local pools (N1, N2) you may alternatively include
the same local frozen plasma pool in all four assays.
4 ASSAY DESIGN
All three preparations (A, B, N) are included in each of the 4 assays. (Sample C is also included
in the VWF:CB assays). A minimum of 3 dilutions of each preparation should be tested, in
replicate, within each assay. Please follow a balanced assay design such as the optimal 18-place
assay described in Design 1 below. If an 18-place assay is not possible please use an alternative
design such as Design 2 (15-place assay). Please contact me if you need help with the assay
design. A separate design is given below for the VWF:CB assays.
In the following designs, each letter refers to a separate set of three or more dilutions and A, A'
and B, B' etc. refer to fresh sets of dilutions (replicates) made from the same ampoule.
Design 1 (18-place assay)
Assay 1 A B N1 N1' B' A'
Assay 2 B N1 A A' N1' B'
Assay 3 B A N2 N2' A' B'
Assay 4 N2 B A A' B' N2'
Design 2 (15-place assay)
Assay 1 A B N1 N1' B'
Assay 2 N1 A B B' A'
Assay 3 B N2 A A' N2'
Assay 4 N2 B A A' B'
Design for VWF:CB assays (24-place assay)
Assay 1 A B C N1 N1' C’ B' A'
Assay 2 B C N1 A A' N1' C’ B'
Assay 3 C N2 A B B’ A’ N2' C'
Assay 4 N2 A B C C’ B’ A' N2'
5 COLLECTION OF FRESH NORMAL PLASMA
Collect fresh normal plasma on two separate days to prepare pools N1 and N2. The method of
collection for the fresh normal plasma is an important part of the study and should be
standardised as far as possible according to the following protocol.
Donors Normal healthy volunteers, excluding women taking oral contraceptives or pregnant.
Take blood from as many different individuals as possible, on two separate days. If possible, use
a minimum of 8 different donors for each pool; if this is not possible, some of the same
individuals can be used again, but the aim is to have as many different donors as possible from
each laboratory.

WHO/BS/09.2116
Page 31
Anticoagulant 0.109 mol/L tri-sodium citrate or a mixture of tri-sodium citrate and citric acid
with a total citrate concentration of 0.109 mol/L. Add 9 volumes of blood to 1 volume of
anticoagulant.
Centrifugation Blood should be centrifuged at 4oC as soon as possible after collection either at
50,000 g for 5 minutes or at 2,000 g for 20 minutes.
Storage Keep plasma pool in a plastic stoppered tube at 4oC during the assay session. Freeze
aliquots of each pool (N1, N2) for subsequent assays where applicable.
6 RESULTS
Please return the raw data from your assays and the methodology questionnaire, by e-mail to
[email protected], using the Excel results sheets by 28 November 2008. Please ensure
that your results are presented as true raw data (eg. clotting time, optical density) rather than as
% or units relative to an in house standard. You are also invited to calculate your own estimates
for B relative to A and for B relative to to N1 and N2 if you wish (see Excel results sheets). If
you are unable to use the Excel sheets please use the results sheets which are attached to this
document. Results returned by post should be addressed to:
Dr A R Hubbard, Haemostasis Section, NIBSC, Blanche Lane, South Mimms, Potters Bar,
Hertfordshire. EN6 3QG United Kingdom
Fax: International +44 1707 641050 UK 01707 641050 E-mail: [email protected]

WHO/BS/09.2116
Page 32
Appendix 2: List of participants
Dr M Shima
Nara Medical University
Kashihara City, Japan
Mr K Sukhu/Dr P Giangrande
Oxford Haemophilia & Thrombosis Centre
Churchill Hospital
Oxford, United Kingdom
Dr R Bader
Centro Emofilia e Trombosi "A Bianchi
Bonomi"
Milan, Italy
Ms E Duncan
Division of Haematology
Institute of Medical & Veterinary Science
Adelaide, Australia
Dr K Friedman / Ms J Endres
Blood Center of SE Wisconsin
Milwaukee, WI
United States of America
Dr C Eby
Washington University School of Medicine
Saint Louis, MO
United States of America
Dr B Woodhams
Diagnostica Stago R&D
Gennevilliers
France
Dr A Lichte/Dr J Patzke/Mr M Timme
Siemens Healthcare Diagnostics
Products GmbH, Marburg
Germany
Dr C Andreini
Instrumentation Laboratory
Milan
Italy
Dr S Rosén
Rossix
Molndal
Sweden
Dr S Duff/Dr M Boylan
Precision Biologic Inc
Dartmouth, Nova Scotia
Canada
Dr S Cinotti
Centro Emofilia
Azienda Ospedaliera Careggi
Florence, Italy
Mr C Watson
Haemostasis Lab, Royal Infirmary
Leicester, United Kingdom
Dr B Kerbl
Technoclone GmbH
Vienna, Austria
Dr M G Riera
Instituto Grifols S.A.
Barcelona, Spain
Dr F Rodeghiero/Dr A Tosetto
San Bortolo Hospital
Vicenza, Italy
Dr M Chitlur / Dr J M Lusher
Children's Hospital of Michigan
Detroit, MI
United States of America
Dr M Wolf
Hôpital Antoine-Béclère
Clamart, France
Dr P Turecek / Dr H Gritsch
Baxter Innovations GmbH
Vienna, Austria
Dr E J Favaloro
Institute of Clinical Pathology & Medical
Research
Westmead Hospital
Westmead, Australia

WHO/BS/09.2116
Page 33
Dr A Hunfeld/Ms J Fötisch
Ms A Schroda/Ms R Nawroth
Dept Haematology &Transfusion Medicine
Paul-Ehrlich-Institut, Langen, Germany
Dr K Trumbull
Instrumentation Laboratory
Lexington, MA
United States of America
Dr B Samor
LFB Biotechnologies
Lille, France
Ms S Bevan/ Ms M Beeharry
Haemostasis Section
NIBSC
Potters Bar, United Kingdom
Prof C A Ludlam/Ms L Germain
Dept of Haematology
Royal Infirmary
Edinburgh, United Kingdom
Dr S Kitchen / Ms K Goodfellow
Dept of Coagulation
Royal Hallamshire Hospital
Sheffield, United Kingdom
Ms A Riddell
Haemophilia Centre & Thrombosis Unit
Royal Free Hospital
London, United Kingdom
Dr S Berrier
Diagnostica Stago QC
Franconville, France
Mme C Caron
Laboratoire d'Hématologie
Centre de Biologique Pathologie
Lille, France
Dr C M Eckmann
Sanquin Plasma Supply Foundation
Amsterdam, The Netherlands
Dr P Gärtner
Baxter AG
Vienna, Austria
Dr D Elmlinger
Octapharma SA QC
Lingolsheim, France
M Blum
Baxter AG
Orth/Donau, Austria
Dr J Amiral
Hyphen Biomed SAS
Neuville-sur-Oise
France
Dr M Bono
Haemostasis Dept.
Diagnostic Grifols
Barcelona, Spain
Dr J C J Eikenboom
Leiden University Medical Center
Dept Thrombosis and Hemostasis
Leiden, The Netherlands
Dr K Pock
Octapharma R & D
Vienna, Austria
Prof A Federici/Dr M T Canciani
Dept. Internal Medicine
A Bianchi Bonomi Hemophilia &
Thrombosis Centre
Milan, Italy
Dr J Conkie / Ms G Hickman
Dept Haematology
Royal Infirmary
Glasgow, United Kingdom
Dr M Telesca
Presbyterian Hospital
New York, NY
United States of America
Mr G Longin
CAF-DCF Red Cross
Neder-Over-Heembeek (Brussels)
Belgium
Dr G Rautmann / Ms C Raphalen
EDQM, Council of Europe
Strasbourg, France

WHO/BS/09.2116
Page 34
Dr D Krause
QC Method Validation
Octapharma Prod. GmbH
Vienna, Austria
Dr A Blande
Bio Products Laboratory
Elstree, United Kingdom

WHO/BS/09.2116
Page 35
Appendix 3: Details of methodology
Factor VIII: Clotting activity
Method Laboratory APTT reagent Substrate plasma Instrument
1-stage clotting
2
3
4
5
6
7
10
11
12
13
16
17
18
19
20
21
23
24
25
27
29
30
32
33
34
35
36
37
43
44
Hemosil/IL APTT-SP
DAPTTIN (Baxter)
Stago CK Prest
Biomerieux Auto APTT
IL Synthasil
Biomerieux
Hemosil/IL APTT Synthasil
Stago CK Prest
IL Synthasil
Hyphen Cephen LR
DG-APTT
IL Synthasil
Platelin LS
Biomerieux Auto APTT
STA Cepascreen
Actin FS
DAPTTIN (Baxter)
Triniclot APTT
Silica
Hemosil/IL APTT-SP
Actin FSL
Hemosil APTT
Hemosil APTT
Stago STA-PTTA
Actin FSL
Hemosil/IL APTT Synthasil
Stago PTTA /CK Prest
Actin FS
Hemosil/IL APTT-SP
Hemosil/IL APTT-SP
immuno-depleted
immuno-depleted
Severe Haem Plasma
immuno-depleted
immuno-depleted
immuno-depleted
immuno-depleted
immuno-depleted
immuno-depleted
immuno-depleted
Immuno-depleted
Severe Haem Plasma
ng
immuno-depleted
immuno-depleted
immuno-depleted
Severe Haem Plasma
immuno-depleted
Immuno-depleted
immuno-depleted
immuno-depleted
Severe Haem Plasma
Severe Haem Plasma
immuno-depleted
immuno-depleted
immuno-depleted
immuno-depleted
Severe Haem Plasma
immuno-depleted
immuno-depleted
IL ACL 9000
KC4A
STA-R Evolution
STA-R Evolution
ACL TOP
STA-R
ACL TOP
STA-R
ACL TOP
STA-R
Amax mechanical
ACL TOP
Behring BCS
STA-R
STA-R Evolution
BCS-XP
KC10
Sysmex CA 1500
BCT Dade Behring
STA Compact
Sysmex CA 7000
ACL 3000
ACL 10000
STA-R
Sysmex CA 1500
ACL TOP
STA-R
BCS
STA-R
ACL TOP 500
Method Laboratory Reagents Samples adsorbed Instrument
2-stage clotting 26
Diagnostic Reagents
Yes
Sysmex CA 7000
Method Laboratory Kit Rate or end-point Instrument
Chromogenic
3
5
8
10
13
14
16
18
21
22
23
24
28
29
34
39
41
42
43
44
Baxter Immunochrom
Hyphen Biophen
Chromogenix Coamatic
Chromogenix Coamatic
Hyphen Biophen
Chromogenix Coatest SP4
DG-Chrom FVIII
Hyphen Biophen
Chromogenix Coamatic
Chromogenix Coatest SP4
Technochrom
Hyphen Biophen
Chromogenix Coamatic
Chromogenix Coatest SP4
Siemens FVIII Chromogenic
Chromogenix Coamatic
Chromogenix Coatest SP4
Chromogenix Coamatic
Chromogenix Coamatic
Chromogenix Coatest SP4
Rate
Rate
End-point
Rate
Rate
End-point
Rate
End-point
Rate
End point
Rate
Rate
End-point
End-point
Rate
End-point
End-point
Rate
End-point
Rate
Powerwave 340
STA-R Evolution
Versamax
ACL TOP
STA-R
T-Max microplate reader
Amax optical
Bio Tek plate reader
ACL Advance
Multiskan JX
Microplate reader
STA-R
Spectramax Plus
Biomek 2000
Sysmex CA-1500
iEMS
Spectramax
ACL 200/3000 plus
STA-R/MTP-Reader
ACL TOP 500
ng - details not given

WHO/BS/09.2116
Page 36
Factor VIII: Antigen
Method Laboratory Method/Kit Capture antibody
ELISA
3
9
11
15
22
24
27
28
29
40
Asserachrom FVIII:Ag
Asserachrom FVIII:Ag
Asserachrom FVIII:Ag
VisuLize FVIII:Ag (Affinity Biologicals)
In house
Asserachrom FVIII:Ag
Haematologic Technologies
Asserachrom FVIII:Ag
In-House
Asserachrom FVIII:Ag
Mouse monoclonal
Mouse monoclonal
Mouse monoclonal
Sheep polyclonal
Human allo-antibodies
Mouse monoclonal
Sheep polyclonal
Mouse monoclonal
Mouse monoclonal
Mouse monoclonal
von Willebrand Factor: Antigen Method Laboratory Method/Kit Antibodies
ELISA
3
8
9
11
12
13
16
17
18
19
22
23
26
27
28
30
31
35
36b
37
42
43
In house
Asserachrom VWF:Ag
In house
Asserachrom VWF:Ag
In house
Hyphen Zymutest
DG-EIA VWF kit
Asserachrom VWF:Ag
In house
In house
In house
Technozym VWF:AG
In house
In house
Asserachrom VWF:Ag
In house
In house
In house
Asserachrom VWF:Ag
In house
In house
Asserachrom VWF:Ag
Dako Rabbit polyclonal
Rabbit polyclonal
Dako Rabbit polyclonal
Rabbit polyclonal
Dako Rabbit polyclonal
Rabbit polyclonal
Rabbit polyclonal
Rabbit polyclonal
Dako Rabbit polyclonal
Dako Rabbit polyclonal
Dako Rabbit polyclonal
Dako rabbit anti-human
Dako Rabbit polyclonal
PBI/HTI antibodies
Rabbit polyclonal
Dako Rabbit polyclonal
Rabbit polyclonal
Dako Rabbit polyclonal
Rabbit polyclonal
Dako Rabbit polyclonal
Dako Rabbit polyclonal
Rabbit polyclonal
Immuno-
turbidimetric
2
4
6
7
10
33
34
36a
38
44
Hemosil/IL VWF Antigen
Stago Liatest
Hemosil/IL VWF Antigen Stago
Liatest
Hemosil/IL VWF Antigen
Stago Liatest
Siemens VWF Ag
Stago Liatest
Stago Liatest
Hemosil/IL VWF Antigen
Rabbit polyclonal
Rabbit polyclonal
Rabbit polyclonal
Rabbit polyclonal
Rabbit polyclonal
Rabbit polyclonal
Rabbit polyclonal
Rabbit polyclonal
Rabbit polyclonal
Rabbit polyclonal

WHO/BS/09.2116
Page 37
von Willebrand Factor: Ristocetin cofactor
Method Laboratory Platelets Reagents Instrument
aggregometry
1
2
3
4
5
12
18
19
20
21
25
28b
28c
29
30
31
33
34
37
38
42
Fixed
Fixed
Fixed
Fixed
Fixed
Fixed
Fixed
Fixed
Fixed
Fixed
Fixed
Fixed
Fixed
Fixed
Fixed
Fixed
Fixed
Fixed
Fixed
Fixed
Fixed
Dade Behring/Siemens
Mascia Brunelli Ristocetin
Dade Behring/Siemens
ABP Ristocetin
Helena Ristocetin
American BP Ristocetin
Dade Behring/Siemens
Hart Biologicals
ABP Ristocetin
Dade Behring/Siemens
Dade Behring/Siemens
Dade Behring + Ristocetin A
(Mascia Brunelli S.P.A)
Dade Behring + Ristocetin A
(Mascia Brunelli S.P.A)
Dade Behring/Siemens
Dade Behring/Siemens
ng
Bio-Data
Siemens BC von Willebrand
Dade Behring/Siemens
Dade Behring/Siemens
Helena Biosciences
BCS
Chronolog
BCS
STA-R Evolution
Helena Pack-S 4
Bio Data PAP-4
BCS
Chronolog
Helena AggRam
BCS-XP
BCS
BCS-XP
ACL 10000
BCS
ACL 9000
Aggregometer
Bio-Data PAP-4D
BCS XP
BCS
BCS
Helena Pack-S 4
visual
agglutination
7
8
22
26
28
43
44
Fixed
Fixed
Fixed
Fixed
Fixed
Fixed
Fixed
Dade Behring/Siemens
Dade Behring/Siemens
Dade Behring/Siemens
In house
Dade Behring/Siemens
Dade Behring/Siemens
Dade Behring/Siemens
--------------
--------------
--------------
--------------
--------------
--------------
--------------
immuno-
turbidimetric
10 Not applicable Hemosil/IL VWF activity ACL TOP
ng - details not given
von Willebrand Factor: Collagen binding
Method Laboratory Kit or in house collagen anti-VWF antibody
ELISA-type
1
3
5
11
15
18
20
23
24
25
27
28a
28b
30
31
32
34
37
40
43
44
In house
Technozym VWF:CBA
In house
Asserachrom VWF:CB
Technozym VWF:CBA
In house
Corgenix Kit
Technozym VWF:CBA
In house
In house
In- house
Technozym VWF:CBA
Technozym VWF:CBA
In-House
In-House
Technozym VWF:CBA
Technozym VWF:CBA
In-house
In house
Technozym VWF:CBA
In-House
Human type III
Human type III
Bovine type I/III mix
Human type III
Type I
Bovine type I/III mix
Equine type III
Human type III
Equine type I/III mix
Human type III
Proprietary
Human type I
Human type III
Human type III
Type I
Human type III
Human type III
Human type III
Human type III
Human type III
Equine type I/III mix
HRP conjugate
polyclonal HRP conjugate
polyclonal HRP conjugate
polyclonal HRP conjugate
polyclonal HRP conjugate
polyclonal HRP conjugate
polyclonal HRP conjugate
polyclonal HRP conjugate
polyclonal HRP conjugate
polyclonal HRP conjugate
polyclonal HRP conjugate
polyclonal HRP conjugate
polyclonal HRP conjugate
polyclonal HRP conjugate
polyclonal HRP conjugate
polyclonal HRP conjugate
polyclonal HRP conjugate
polyclonal HRP conjugate
polyclonal HRP conjugate
polyclonal HRP conjugate
polyclonal HRP conjugate

WHO/BS/09.2116
Page 38
Appendix 4: Real-time stability data for the 5th
IS FVIII/VWF
Plasma (02/150) Ampoules of the 5
th IS were stored for 6.67 years at -150, -70 and -20 °C. Factor VIII:C was
estimated by both 1-stage clotting and chromogenic methods and the potency of -70 and -20
°C ampoules has been expressed as a percentage of the vials stored at -150 °C.
Estimates of Factor VIII:C in ampoules stored for 6.67 years at -20oC and -
70°C relative to ampoules stored at -150oC (assigned 100%).
Chromogenic
One-stage clotting
Ampoule/Assay
number
-20 °C storage -70 °C storage -20 °C storage -70 °C storage
1
2
3
4
5
6
100.45
97.97
101.58
98.75
106.05
96.89
101.25
99.88
104.14
99.05
103.19
97.56
100.17
99.83
100.24
102.71
96.21
99.02
100.67
94.44
96.05
102.71
99.05
102.27
Mean
100.24 %
100.82 %
99.68 %
99.15 %
There was no significant difference between estimates for ampoules stored at -150, -70 and -20 °C.

WHO/BS/09.2116
Page 39
Appendix 5: Draft Instructions for Use for the proposed WHO 6th
International Standard Factor VIII and von Willebrand factor in
plasma (07/316)

WHO/BS/09.2116
Page 40

WHO/BS/09.2116
Page 41