Embed Size (px)
Citation preview

VL
La
b
c
d
e
a
AA
KCERRA
1
ioioeitipt22
UT
(s(
1d
Respiratory Physiology & Neurobiology 167 (2009) 162–167
Contents lists available at ScienceDirect
Respiratory Physiology & Neurobiology
journa l homepage: www.e lsev ier .com/ locate / resphys io l
alidity and reliability of cardiorespiratory measurements recorded by theifeShirt during exercise tests
isa Kenta, Brenda O’Neill a, Gareth Davisonb, Alan Nevill c, J. Stuart Elbornd,e, Judy M. Bradleya,e,∗
Health and Rehabilitation Sciences Research Institute, University of Ulster, Jordanstown, BT37 0QB, UKSport and Exercise Sciences Research Institute, University of Ulster, Jordanstown, BT37 0QB, UKSchool of Sport, Performing Arts and Leisure, University of Wolverhampton, WS1 3BD, UKRespiratory Medicine Group, Centre for Infection and Immunology, Queens University Belfast, BT7 1NN, UKRespiratory Medicine, Belfast Health and Social Care Trust, BT9 7AB, UK
r t i c l e i n f o
rticle history:ccepted 27 March 2009
eywords:alibrationxercise
a b s t r a c t
The LifeShirt is a novel ambulatory monitoring system that records cardiorespiratory measurements out-side the laboratory. Validity and reliability of cardiorespiratory measurements recorded by the LifeShirtwere assessed and two methods of calibrating the LifeShirt were compared. Participants performed anincremental treadmill test and a constant work rate test (65% peak oxygen uptake) on four occasions (>48 hapart) and wore the LifeShirt, COSMED system and Polar Sport Tester simultaneously. The LifeShirt was
espiratory inductive plethysmographyespiratory physiologymbulatory monitoring
calibrated using two methods: comparison to a spirometer; and 800 ml fixed-volume bag. Ventilation,respiratory rate, expiratory time and heart rate recorded by the LifeShirt were compared to measurementsrecorded by laboratory equipment. Sixteen adults participated (6M:10F); mean (SD) age 23.1 (2.9) years.Agreement between the LifeShirt and laboratory equipment was acceptable. Agreement for ventilationwas improved by calibrating the LifeShirt using a spirometer. Reliability was similar for the LifeShirt andthe laboratory equipment. This study suggests that the LifeShirt provides a valid and reliable method of
ambulatory monitoring.. Introduction
Exercise testing and physical activity monitoring are importantn many areas such as health promotion in the general populationr assessing patients with chronic disease. In terms of exercise test-ng the gold standard is cardiopulmonary exercise testing carriedut in a laboratory. In-depth analysis of gas exchange, ventilation,lectrocardiogram and blood pressure allows clinicians to elicit andnterpret abnormalities in the cardiovascular and pulmonary sys-ems (Porszasz et al., 2007). These measures have been shown to bemportant for diagnosis and prognosis, assessment of severity and
rogression of disease, understanding the physiological response toherapies and as an endpoint in clinical trials (Bradley and O’Neill,005; Bradley and Moran, 2008; McKone et al., 2002; Ram et al.,005). Despite the extensive data gained, cardiopulmonary exer-∗ Corresponding author at: Health and Rehabilitation Sciences Research Institute,niversity of Ulster, Jordanstown, Newtownabbey, BT37 0QB, UK.el.: +44 0 28 9036 8991; fax: +44 0 28 9036 8068.
E-mail addresses: [email protected] (L. Kent), [email protected]. O’Neill), [email protected] (G. Davison), [email protected] (A. Nevill),[email protected] (J. Stuart Elborn), [email protected]. Bradley).
569-9048/$ – see front matter © 2009 Elsevier B.V. All rights reserved.oi:10.1016/j.resp.2009.03.013
© 2009 Elsevier B.V. All rights reserved.
cise testing is time and labour intensive and requires expensiveequipment. Field tests such as shuttle walk/run tests provide a lessexpensive alternative which are easier to carry out in large groupsof subjects or for repeated testing. Field tests are often used in largeepidemiological studies (e.g. Northern Ireland Young Hearts Project,Boreham et al., 1993) however results are based on performance(e.g. distance run) and information on physiological response islimited.
Physical activity monitoring is becoming recognised as animportant tool for both promoting physical activity and assess-ing the outcome of interventions. Methods used to date includeself-reported recall questionnaires (e.g. Baecke Physical ActivityQuestionnaire (Baecke et al., 1982)), activity diaries (e.g. BouchardActivity Diary (Bouchard et al., 1983)) and objective movement sen-sors such as pedometers and accelerometers. Although objectivemeasures of activity may be more reliable they do not provide dataon physiological response to activity.
The LifeShirt® (Vivometrics, Inc., Ventura, CA, U.S.A.) is a novelmulti-function ambulatory device and consists of a Lycra® garment,
data recorder, and computer-based analysis software (VivoLogic)(Grossman, 2004; Wilhelm et al., 2003). Respiratory inductiveplethysmography is the core technology which has been shownto provide accurate non-invasive assessment of respiratory pattern(Carry et al., 1997). The basic system also incorporates a three-lead
gy & N
Emtft
ifti(pHmeptmec
scaurhr
2
2
t(cw
2
vtiiwPmamp(S(rhwi
2
mi
L. Kent et al. / Respiratory Physiolo
CG and a tri-axial accelerometer. As the LifeShirt simultaneouslyonitors physiological measurements such as ventilation, respira-
ory rate and heart rate as well as activity, it provides an opportunityor monitoring response to exercise and physical activity outside ofhe laboratory.
The LifeShirt has been successfully used to measure key phys-ological measurements during activities of daily living in heartailure which were important in predicting mortality and tailoringherapy (Brack et al., 2007). To date three small studies have exam-ned the validity of the LifeShirt and involved healthy volunteersn = 45) and a small number of patients with cardiac (n = 5) and res-iratory disease (n = 6) (Clarenbach et al., 2005; Witt et al., 2006;eilman and Porges, 2007). However in these studies measure-ents were only examined at one time point. No study to date has
xamined validity and reliability of the LifeShirt over multiple timeoints. This is important as many areas of research involve repeatedesting, including assessing treatment efficacy and training effects,
onitoring physical activity, and collection of physiological data inpidemiological studies. Repeated testing is also important clini-ally in monitoring patients over the lifetime of their disease.
The hypotheses for this study were that cardiorespiratory mea-urements recorded by the LifeShirt during exercise would beomparable to measurements recorded by laboratory equipmentnd reliable over four occasions, and that calibration of the LifeShirtsing a spirometer would improve the agreement in ventilationecorded by the LifeShirt and laboratory equipment. A furtherypothesis was that activity measured by the LifeShirt would beeliable over four occasions.
. Methods
.1. Subjects
Sixteen individuals aged 18–30 were recruited via email adver-isement within the University of Ulster. Participants were healthyno known respiratory or cardiac disease) Caucasians. The proto-ol was approved by the University of Ulster ethics procedures andritten informed consent obtained.
.2. Procedure
Participants attended the Human Performance Laboratory (Uni-ersity of Ulster) on four occasions separated by at least 48 h. Visitsook place at the same time of day with the same assessor andnvolved a period of familiarisation with equipment (performedn sitting). Height (nearest 1.0 cm) and weight (nearest 0.1 kg)
ere measured. Physical activity was scored using the Baeckehysical Activity Questionnaire and categorized into low (3–7),oderate (7–11) and high (11–15) levels of activity (Baecke et
l., 1982). At each visit subjects completed an incremental tread-ill test and a constant work rate treadmill test. Cardiopulmonary
arameters were recorded simultaneously by the LifeShirt systemVivometrics, Inc., Ventura, CA, U.S.A.), heart rate monitor (Polarport Tester, RS600i, Kempele, Finland) and pneumotachographCOSMED quarkB2, Rome, Italy). Cardiorespiratory measurementsecorded were: ventilation; respiratory rate; expiratory time; andeart rate. Activity during the walking stages of the incremental testas recorded by the LifeShirt accelerometer (summation of motion
n 3 axis).
.3. Calibration of LifeShirt
Ventilation recorded by the LifeShirt was calibrated using twoethods. For the spirometer calibration a set of 20 breaths were
dentified and visually inspected for uniformity using VivoLogic
eurobiology 167 (2009) 162–167 163
software and matched to twenty breaths recorded by the spirome-ter. A mean value of the 20 breaths recorded by the spirometer wasinputted when using the fixed-volume calibration option withinthe VivoLogic software. Fixed-volume calibration required subjectsto repeatedly inflate and deflate a fixed-volume 800 ml bag whilstwearing nose clips performed in standing.
2.4. Calibration of the COSMED system
The pneumotachograph was calibrated using a 3 l calibrationsyringe (Hans Rudolph, Kansas City, MO). The fast respondinginfrared CO2 and Zirconium O2 analysers were calibrated using thefollowing BOC gas concentrations: reference gas = 21% O2; calibra-tion gas = 5.19% CO2, 16.43% O2, balanced N2.
2.5. Test protocols
2.5.1. Incremental testThe 15 stage standardised exponential exercise protocol was
used which starts at a low work load and increases exponen-tially involving changes in speed and gradient at 1 min intervals(Northridge et al., 1990). All participants started at level 3 (3 METs;10.3 ml kg−1 min−1) and continued until volitional fatigue. An addi-tional level (9.0 km h−1, 16% gradient) was completed if participantsdid not reach volitional fatigue by the final stage of the originalprotocol.
2.5.2. Constant work rate testFollowing the maximal test subjects rested for a period of at least
30 min and until heart rate returned to 10 beats min−1 above thepre-recorded resting heart rate before they performed the constantwork rate test. From the linear relationship between oxygen uptakeand heart rate, a target heart rate equivalent to 65% peak oxygenuptake (V̇O2peak
) was estimated from peak heart rate recorded dur-ing the incremental test on the first visit. A 5 min recording beganonce the target heart rate was achieved and maintained for 1 min.
2.6. Statistics
Cardiorespiratory data were matched on a breath-by-breathbasis between the LifeShirt and COSMED. Preliminary breath-by-breath analysis of incremental test data showed large amounts ofvariability for both validity (co-efficient of variation (CV): 17.9%)and reliability analyses for the LifeShirt (CV: 18.9%) and COSMED(CV: 17.5%). To control for this breath-by-breath variation thatis unlikely to reflect the more stable underlying cardiorespira-tory response to exercise, mean values of the final 30 s of eachstage were used as is recommended and has been used in previ-ous investigations (ATS/ACCP Statement, 2003; Benoit et al., 1997;Young et al., 1985). Only the stages that all participants com-pleted were included in the analyses. Mean values for activity wereextracted for the last 30 s of stages during which all subjects main-tained a walking pace. Exploratory assessment of constant workrate test data (using repeated measures ANOVA) revealed that asteady state work rate was achieved by the third minute there-fore the final 2 min were analysed. Reliability of activity was notassessed for the constant work rate test as a target heart ratewas used to guide work rate, therefore treadmill speed may nothave been consistent over the four occasions. When the two sys-tems were compared, differences (residual errors) were found to
be associated with the size of the measurements (heteroscedas-ticity) (Figs. E1 and E2 in the online supplement) and as such, alldata were log transformed (Atkinson and Nevill, 1998). Validity(between systems) and reliability (between days but within sys-tems) was assessed using repeated-measures ANOVA performed in
1 gy & Neurobiology 167 (2009) 162–167
Mnirfb1
3
ywu1m
3
3
semidmbLboeicmc
3
wcdC
FLb
64 L. Kent et al. / Respiratory Physiolo
initab (Minitab Ltd., Coventry, UK). Results are reported as sig-ificance of bias (systematic differences between measurements
n a particular direction) and within-subject mean-square errorseported as coefficients of variation (CV%) (unexplained error dif-erences between measurements). The research team consideredias to be significant at p < 0.05 level and a CV acceptable below0%.
. Results
16 young adults participated (6M:10F); mean (SD) age 23.1 (2.9)ears, height 169.7 (9.1) cm and weight 67.3 (8.6) kg. Participantsere moderately active, mean (SD) physical activity score 7.2 (1.1)nits. In the incremental test all participants reached at least stage1 (mean (SD): V̇O2 kg−1: 29 (3.2) ml min−1 kg−1, R: 1.02 (0.1)). Theean speed during the constant work rate test was 6.3 km h−1.
.1. Incremental test
.1.1. VentilationThe bias (p = 0.055) and CV (3.8%) for ventilation between the
pirometer calibrated LifeShirt and COSMED was acceptable, how-ver there was an interaction due to exercise intensity (p < 0.001)eaning that the difference between the systems became signif-
cant at stage 7 and progressively increased. The greatest meanifference was observed at stage 11 (9.5%; 4.6 l min−1). Ventilationeasured by fixed-volume bag calibrated LifeShirt showed greater
ias (p = 0.002) and CV (11.0%) compared to the COSMED, withifeShirt underestimating values (Fig. 1). There was no significantias over days for the LifeShirt (using either calibration method)r COSMED. However there was an interaction over days due toxercise intensity when measured by COSMED (p = 0.033) and annteraction approaching significance when measured by spirometeralibrated LifeShirt (p = 0.06). CVs were smaller over four assess-ents for spirometer calibrated LifeShirt (6.4%) and COSMED (6.6%)
ompared to fixed-volume calibrated LifeShirt (15.8%).
.1.2. Respiratory rateThere was no significant bias (p = 0.895) and CV was well
ithin the acceptable threshold (1.4%) when the two systems wereompared (Fig. 2). Both systems showed no significant bias overays with CVs just outside the acceptable range (LifeShirt 10.2%;OSMED 10.3%).
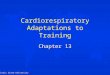
ig. 1. Mean ln[ventilation] at each stage of incremental test for COSMED (diamond),ifeShirt calibrated by spirometer (square) and LifeShirt calibrated by fixed-volumeag (triangle). Error bars represent standard deviation.
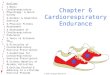
Fig. 2. Mean ln[respiratory rate] at each stage of incremental test for COSMED (dia-mond) and LifeShirt (square). Error bars represent standard deviation.
3.1.3. Expiratory timeThere was significant bias between the LifeShirt and COSMED
(p = 0.007) (LifeShirt slightly underestimating) and also an effectdue to exercise intensity (p = 0.008); as intensity increased the dif-ference between systems became smaller (contrary to the effectof intensity on ventilation) (Fig. 3). The CV between systems waswithin the acceptable threshold (2.2%) and the greatest mean differ-ence was observed at stage 3 (2.5%; 0.04 s). Expiratory time showedno significant bias over days for either the LifeShirt or COSMEDand CVs were just outside the acceptable range (LifeShirt 10.8%;COSMED 10.6%).
3.1.4. Heart rateThere was a significant bias between the LifeShirt and COSMED
(p = 0.005) and a significant effect due to exercise intensity(p = 0.018) however the CV was within acceptable limits (3.6%).The greatest mean difference was observed at stage 4 (3.5%;2.8 beats min−1) and is unlikely to be important (Fig. 4). TheLifeShirt showed no significant bias over days (p = 0.092), whereasthe Polar Sport Tester showed no bias over days (p = 0.145) but
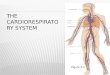
did show a significant effect over days due to exercise intensity(p = 0.03). Both systems had acceptable CV over the four occasions(LifeShirt 5.5%; Polar Sport Tester 2.3%).Fig. 3. Mean ln[expiratory time] at each stage of incremental test for COSMED (dia-mond) and LifeShirt (square). Error bars represent standard deviation.

L. Kent et al. / Respiratory Physiology & N
Fig. 4. Mean ln[heart rate] at each stage of incremental test for Polar Sport Tester(diamond) and LifeShirt (square). Error bars represent standard deviation.
Fmd
3
(
3
3
vwi
TA
S(
33444444
ig. 5. Mean ln[activity] at each walking stage of the incremental test for Day 1 (dia-ond), Day 2 (square), Day 3 (triangle), Day 4 (circle). Error bars represent standard
eviation.
.1.5. ActivityThere was a significant bias (p = 0.009) but an acceptable CV
4.9%) over days in the values for activity (Fig. 5; Table 1).
.2. Constant work rate test
.2.1. Ventilation
The spirometer calibrated LifeShirt marginally underestimatedentilation compared to the COSMED (5.8%; 1.8 l min−1) and CV wasithin the acceptable threshold (9.7%), however the bias was signif-
cant (p = 0.032). The fixed-volume bag calibrated LifeShirt greatly
able 1ctivity measured by the LifeShirt accelerometer over four incremental tests.
peed (km h−1)/slope%)
Activity (digital units) mean (SD)
Day 1 Day 2 Day 3 Day 4
.2/1.5 6.7 (0.889) 7.1 (0.942) 6.9 (1.146) 7.0 (1.065)
.2/3.0 6.9 (1.021) 7.3 (1.054) 7.2 (0.932) 7.4 (1.404)
.0/3.0 8.4 (1.159) 8.8 (1.142) 8.7 (1.283) 9.0 (1.334)
.0/5.0 8.9 (1.442) 9.0 (1.387) 9.3 (1.494) 9.2 (1.496)
.0/7.0 9.4 (1.608) 9.5 (1.816) 9.7 (1.734) 9.6 (1.603)
.8/7.0 11.3 (2.115) 11.2 (2.449) 11.8 (2.212) 11.6 (2.070)
.8/9.0 12.0 (2.293) 12.1 (2.448) 12.5 (2.587) 12.2 (2.375)
.8/11.0 12.7 (2.529) 12.9 (2.673) 13.3 (2.616) 13.1 (2.451)
eurobiology 167 (2009) 162–167 165
underestimated ventilation (28.4%; 6.67 l min−1) and showed sig-nificant bias (0 = 0.001) and greater CV 16.7%. The LifeShirt (usingeither calibration method) and COSMED showed no significant biasover days (LifeShirt-spirometer p = 0.425; LifeShirt-fixed-volumep = 0.114; COSMED p = 0.834) however CV was outside the accept-able threshold for all three systems (LifeShirt-spirometer 12.7%;LifeShirt-fixed-volume 19.1%; COSMED 17.2%).
3.2.2. Respiratory rateThere was a significant bias between the LifeShirt and COSMED
(p = 0.031) however CV was within the acceptable threshold (0.4%)and mean difference negligible (0.2%; 0.06 breaths min−1). Biasover days for both systems was not significant (LifeShirt p = 0.268;COSMED p = 0.311) however CVs were just outside the acceptablethreshold (LifeShirt 10.5%; COSMED 10.6%).
3.2.3. Expiratory timeThere was a significant bias between the LifeShirt and COSMED
in measurement of expiratory time (p = 0.008) however CV (1.4%)and mean difference (1.2%; 0.015 s) between systems were small.There was no significant bias over days (LifeShirt p = 0.485; COSMEDp = 0.387) and CV were just outside the acceptable threshold forboth systems (LifeShirt 10.6%; COSMED 10.5%).
3.2.4. Heart rateThere was significant bias between the LifeShirt and Polar Sport
Tester in heart rate (p = 0.011) however CV was well within theacceptable threshold (0.7%) and mean difference between systemswas small (0.8%; 1.0 beat min−1). Reliability of heart rate mea-sured by either system was good with no significant bias (LifeShirtp = 0.553; COSMED p = 0.731) and CV well within the acceptablethreshold (LifeShirt 1.9%; COSMED 2.1%).
4. Discussion
This is the first study to assess validity and reliability of theLifeShirt in comparison to laboratory systems across multiple timepoints (four occasions). Validity and reliability over multiple timepoints is important as monitoring patients over the lifetime of theirdisease and assessing treatment efficacy involves repeated test-ing. Breath-by-breath analysis is fundamentally open to variationand exploratory analysis using individual breaths revealed a greatamount of error variation. As is recommended by the ATS/ACCPstatement on cardiopulmonary exercise testing (2003) we obtaineda more stable measure of response during both the incremental test(mean of final 30 s of each stage) and the constant work rate test(final 2 min of test). This was a crucial step in being able to explorethe agreement between the two systems. Agreement between theLifeShirt and laboratory equipment were within acceptable rangesfor both incremental and constant work rate exercise (Figs. 1–4).The LifeShirt and COSMED both showed no significant bias overdays for any measurement. CVs over days for the incremental testwere within acceptable limits and for the constant work rate testwere mainly just over 10%. Most importantly the results for relia-bility were similar for the LifeShirt and the laboratory equipment.The LifeShirt is therefore suitable for field monitoring when use oflaboratory equipment is not feasible.
The results of this study are in agreement with results of thevalidation study by Clarenbach et al. (2005) which compared theLifeShirt to laboratory equipment at one time point only. The
present study is the first to look at the validity and also reliabilityof LifeShirt measurements over multiple time points. Results fromthis study for reliability of ventilation and heart rate measured bythe LifeShirt and COSMED are similar to previous data on reliabilityof laboratory systems (Nordrehaug et al., 1991).
1 gy & N
e(utaetsvlcdoat
ibodbmte
ssmsaevaitimgtatcatl
ttaaaapr
twphr(amcs
66 L. Kent et al. / Respiratory Physiolo
This is also the first study to show the benefits of using a spirom-ter for calibrating the LifeShirt over using a fixed-volume bagFig. 1). Accuracy of the fixed-volume bag procedure, which is thesual method of calibrating the LifeShirt, is affected by different pat-erns of respiratory muscle recruitment, air leaks (insufficient sealt mouthpiece or puffing of cheeks), gas compression (continuedxpiration when bag is filled), gas expansion (continued inspira-ion when bag is empty). Calibration by spirometer requires lesskill on the part of the subject. The lower levels of within-subjectariation detected for the spirometer-calibrated ventilation wouldower the sample size required in studies that use the LifeShirt as alinical endpoint. Spirometer calibration would also improve confi-ence in results when the LifeShirt is used clinically to assess effectsf therapies in individual patients. In view of this new informationspirometer should be used to calibrate the LifeShirt to improve
he accuracy of volume components of breathing.Although activity measured by the LifeShirt during the walk-
ng stages of the incremental test were found to have significantias over days there is no published data to facilitate judgmentn whether this represents a clinically important difference. Theifferences over days however appear to be small and unlikely toe clinically important. As with other activity monitoring devicesore research is needed to guide the interpretation of the output of
he LifeShirt accelerometer in relation to activity level and energyxpenditure.
The choice of system used for recording cardiorespiratory mea-urements depends on the purpose of the test. Metabolic cartsuch as the COSMED quarkB2 are considered the gold standard inonitoring respiratory gas exchange and cardiopulmonary mea-
urements during exercise tests and are useful for diagnosis ofbnormalities in the cardiopulmonary response to exercise. How-ver they are mainly confined to the laboratory and ambulatoryersions such as COSMED K4b2 still require the individual to wearfacemask/mouthpiece which is known to alter breathing pattern,
s cumbersome and intrusive and not feasible for extended moni-oring. As the LifeShirt is a light-weight 24 h ambulatory device its suitable for extended monitoring of cardiopulmonary measure-
ents during activities of daily living and sleep when respiratoryas exchange measurements are not required. Therefore in contrasto the artificial environment of a laboratory, the LifeShirt could givebetter insight into the daily function of different patient popula-
ions in their own environment. For example patients with chroniconditions that alter the response to activity such as respiratorynd cardiac patients. Indeed a recent study in cystic fibrosis usedhe LifeShirt to detect a response to a new therapy for CF relatedung disease (Wilschanski et al., 2008).
The level of structure during the monitoring period depends onhe information required. For example set tasks such as a shuttleest or 6 min walk test may be used to elicit abnormal responses toctivity. Alternatively an unstructured or free living protocol mayllow assessment of physiological responses to patient’s normalctivities of daily living. Furthermore the LifeShirt diary functionllows patients to record symptoms at the time of the event and sohysiological measurements are available to supplement subjectiveeports.
This study was conducted in healthy individuals and consideringhe demanding nature and number of study visits for reliability itas considered unreasonable for the purpose of the study to involveatients. Therefore a limitation of this study is that measurementsave not been examined for validity and reliability throughoutanges typical of responses to exercise in some patient populations
i.e. low exercise capacity or high ventilatory response). There arefew limitations to the LifeShirt. Volume components of breathingay be less useful at high intensity activity (e.g. ventilation) andonversely timing components may be less useful at lower inten-ity activity (e.g. expiratory time); however in the present study
eurobiology 167 (2009) 162–167
differences between systems remained within clinically acceptablelimits. Further research should focus on validity and reliability ofperipheral devices available with the LifeShirt such as pulse oxime-ter, blood pressure monitor and cough monitor (Grossman, 2004;Wilhelm et al., 2003; Coyle et al., 2005).
In conclusion when assessment of cardiopulmonary measure-ments is required the LifeShirt can provide valid and reliablerespiratory data across multiple assessments. Calibration of theLifeShirt using a spirometer improves the accuracy of volumecomponents compared to fixed volume bag calibration. When cal-ibrated appropriately, the LifeShirt is likely to be a useful tool tomonitor cardiorespiratory response to exercise and activity out-side of the laboratory, or as an outcome measure in trials of newinterventions.
Acknowledgements
The authors would like to acknowledge Dr. John Brown and RoyCrowe in the Human Performance Laboratory, University of Ulsterfor assistance with exercise testing.
Appendix A. Supplementary data
Supplementary data associated with this article can be found, inthe online version, at doi:10.1016/j.resp.2009.03.013.
References
Atkinson, G., Nevill, A.M., 1998. Statistical methods for assessing measurement error(reliability) in variables relevant to sports medicine. Sports Med. 26 (4), 217–238.
American Thoracic Society and American College of Chest Physicians, 2003.ATS/ACCP statement: cardiopulmonary exercise testing (corrected version). Am.J. Respir. Crit. Care Med. 167, 1451–1452.
Baecke, J.A.H., Burema, J., Frijters, J.E.R., 1982. A short questionnaire for the measure-ment of habitual physical activity in epidemiological studies. Am. J. Clin. Nutr.36, 936–942.
Benoit, H., Busso, T., Prieur, F., Castells, J., Freyssenet, D., Lacour, J.R., Denis, C.,Geyssant, A., 1997. Oxygen uptake during submaximal incremental and constantwork load exercises in hypoxia. Int. J. Sports Med. 18 (2), 101–105.
Boreham, C., Savage, J.M., Primrose, D., Cran, G., Strain, J., 1993. Coronary risk factorsin schoolchildren. Arch. Dis. Child. 68, 182–186.
Bouchard, C., Tremblay, A., Leblanc, C., Lortie, G., Savard, R., Thériault, G., 1983. Amethod to assess energy expenditure in children and adults. Am. J. Clin. Nutr. 37,461–467.
Brack, T., Thüer, I., Clarenbach, C.F., Senn, O., Noll, G., Russi, E.W., Bloch, K.E., 2007.Daytime Cheyne–Stokes respiration in ambulatory patients with severe con-gestive heart failure is associated with increased mortality. Chest 132, 1463–1471.
Bradley, J.M., Moran, F., 2008. Physical training for cystic fibrosis. Cochrane Databaseof Syst. Rev. Issue 1. Art. No.: CD002768. doi:10.1002/14651858.CD002768.pub2.
Bradley, J.M., O’Neill, B., 2005. Short-term ambulatory oxygen for chronic obstructivepulmonary disease. Cochrane Database of Syst. Rev. Issue 4. Art. No.: CD004356.doi:10.1002/14651858.CD004356.pub3.
Carry, P.-Y., Baconnier, P., Eberhard, A., Cotte, P., Benchetrit, G., 1997. Evaluation ofrespiratory inductance plethysmography. Chest 111 (4), 910–915.
Clarenbach, C.F., Senn, O., Brack, T., Kohler, M., Bloch, K.E., 2005. Monitoring of venti-lation during exercise by a portable respiratory inductive plethysmograph. Chest128 (3), 1282–1290.
Coyle, M.A., Keenan, D.B., Henderson, L.S., Watkins, M.L., Haumann, B.K., Mayleben,D.W., Wilson, M.G., 2005. Evaluation of an ambulatory system for the quantifica-tion of cough frequency in patients with chronic obstructive pulmonary disease.Cough. 1:3. Available from http://www.coughjournal.com/content/1/1/3.
Grossman, P., 2004. The LifeShirt: a multi-function ambulatory system monitoringhealth, disease, and medical intervention in the real world. Stud. Health Technol.Inform. 108, 133–141.
Heilman, K.J., Porges, S.W., 2007. Accuracy of the LifeShirt (VivoMetrics) in the detec-tion of cardiac rhythms. Biol. Psychol. 75, 300–305.
McKone, E.F., Barry, S.C., Fitzgerald, M.X., Gallagher, C.G., 2002. The role of supple-mental oxygen during submaximal exercise in patients with cystic fibrosis. Eur.Respir. J. 20, 134–142.
Nordrehaug, J.E., Danielsen, R., Stangeland, L., Rosland, G.A., Vik-Mo, H., 1991. Res-piratory gas exchange during treadmill testing: reproducibility and comparisonof different exercise protocols. Scand. J. Clin. Lab. Invest. 51, 655–658.
Northridge, D.B., Grant, S., Ford, I., Christie, J., McLenachan, J., Connelly, D., McMurray,J., Ray, S., Henderson, E., Dargie, H.J., 1990. Novel exercise protocol suitable foruse on a treadmill or a bicycle ergometer. Br. Heart J. 64 (5), 313–316.

gy & N
P
R
W
L. Kent et al. / Respiratory Physiolo
orszasz, J., Stringer, W., Casaburi, R., 2007. Equipment measurements and qual-ity control in clinical exercise testing. In: Ward, S.A., Palange, P. (Eds.), ClinicalExercise Testing. European Respiratory Society Journals Ltd., Sheffield, UK, pp.108–128.
am, F.S.F., Robinson, S.M., Black, P.N., Picot, J., 2005. Physical training for asthma.Cochrane Database of Syst Rev. Issue 4. Art. No.: CD001116. doi:10.1002/14651858.CD001116.pub2.
ilhelm, F.H., Roth, W.T., Sackner, M.A., 2003. The LifeShirt: an advanced system forambulatory measurement of respiratory and cardiac function. Behav. Modif. 27(5), 671–691.
eurobiology 167 (2009) 162–167 167
Wilschanski, M., Armoni, S., Yaakov, Y., Blau, H., Shoseyov, D., Cohen, M., Hirawat,S., Elfring, G.L., Reha, A., Miller, L.L., Kerem, E., 2008. PTC124 treatment over 3months improves pharmacodynamic and clinical parameters in patients withnonsense-mutation-mediated CF. J. Cyst. Fibros. 7 (Suppl. 2), S22 [abstract].
Witt, J.D., Fisher, J.R.K.O., Guenette, J.A., Cheong, K.A., Wilson, B.J., Sheel, A.W., 2006.Measurement of exercise ventilation by a portable respiratory inductive plethys-mograph. Respir. Physiol. Neurobiol. 154 (3), 389–395.
Young, A.J., Cymerman, A., Burse, R.L., 1985. The influence of cardiopulmonary fitnesson the decrement in maximal aerobic power at high altitude. Eur. J. Appl. Physiol.54, 12–15.