Embed Size (px)
Citation preview

From the Vascular and Endovascular Surgery Society2014 Norman M. Rich Military Vascular Award
FromAPa
AuthDiscan
PresMw
PresMPlC
Repteda
Thetom
0741Pubhttp
162
Validation of the Short Musculoskeletal FunctionAssessment in patients with battlefield-relatedextremity vascular injuriesDaniel J. Scott, MD,a,b J. Devin B. Watson, MD,a,b Thomas A. Heafner, MD,a,b Michael S. Clemens, MD,b
Brandon W. Propper, MD,a,b and Zachary M. Arthurs, MD,b San Antonio and Fort Sam Houston, Tex
Objective: Vascular extremity injuries can be a significant burden on a patient’s long-term quality of life. Currently, nolimb-specific surveys have been used to quantify the relation between injury pattern and the resultant physical or psy-chological impact. The objective of this study was to validate the use of the Short Musculoskeletal Function Assessment(SMFA) in the setting of extremity vascular injury.Methods: The Joint Theater Trauma Registry was queried and filtered for U.S. troops with an extremity vascular injuryisolated to a single limb. Injury andmanagement data were obtained, and the SMFAwas administered after patient contactand consent. Validity was analyzed by characterization of SMFA score distribution, correlation with 36-Item Short FormHealth Survey (SF-36) scores, and assessment of its discriminative capability to external measures of injury severity (ie,Injury Severity Score [ISS], Mangled Extremity Severity Score [MESS], and Medicare Part A disability qualification).Results: At mean follow-up of 5 years, 164 patients (median age, 25 years; interquartile range, 22-31 years) completedboth surveys. The overall SMFA Dysfunction Index was 24.8 6 15.2 (range, 0-78; skewness, 0.60; floor/ceiling effect,0%-1.2%; and nonresponse, 0%), and the overall Bother Index was 29.46 20.2 (range, 0-96; skewness, 0.58; floor/ceilingeffect, 0%-4.3%; and nonresponse, 0.6%). SF-36 physical component summary scores correlated inversely with theDysfunction Index (r [ L0.64; P < .01), whereas mental component summary scores correlated inversely with theBother Index (r[L0.59; P < .01). No difference was found in reported scores between those considered severely injured(ISS > 15) and those not severely injured (ISS # 15). However, those with mangled extremities (MESS $ 7) reportedhigher Dysfunction and Bother indices than those with lower scores (P < .05). In addition, patients considered disabled(per Medicare Part A qualifications) reported higher Dysfunction and Bother indices compared with those not considereddisabled (P < .05).Conclusions: Use of the SMFA is validated in those with extremity vascular injuries, and it should be considered anadjunctive tool in evaluating long-term patient outcomes. (J Vasc Surg 2014;60:1620-6.)
Battlefield-related injuries are associated with high ratesof extremity vascular injuries.With specific rates of extremityvascular injuries accounting for 10% of all wartime trauma,this injury pattern can be a major source of morbidity andmortality.1 Modern management practices in warfare (ie,
the 59th Clinical Research Division, Lackland Air Force Base, Sanntonioa; and the U.S. Army Institute of Surgical Research, Chambersss, Fort Sam Houston.b
or conflict of interest: none.laimer: The viewpoints expressed in this article are those of the authorsd do not reflect the official position of the U.S. Department of Defense.ented at the Vascular and Endovascular Surgery Society Springeeting, Hynes Convention Center, Boston Mass, June 4, 2014 andinner of the Dr Norman M. Rich Award.ented at the Vascular and Endovascular Surgery Society Wintereeting/Society for Military Vascular Surgery Scientific Program,enary Presentation (M2), Steamboat Grand Hotel, Steamboat Springs,olo, January 29-February 2, 2014.rint requests: Daniel J. Scott, MD, San Antonio Military Medical Cen-r, 3851 Roger Brooke Dr, Fort Sam Houston, TX 78234 (e-mail:[email protected]).editors and reviewers of this article have no relevant financial relationshipsdisclose per the JVS policy that requires reviewers to decline review of anyanuscript for which they may have a conflict of interest.-5214
lished by Elsevier Inc. on behalf of the Society for Vascular Surgery.://dx.doi.org/10.1016/j.jvs.2014.08.060
0
predeployment training, early tourniquet use, rapid trans-port, and structured levels/echelons of care) have temperedthe mortality associated with this pattern of injury; however,the long-term morbidity is still under investigation.2-7
To date, patient-based outcomes related to peripheralvascular injuries have been limited to the use of genericquality of life surveys, such as the Medical Outcomes Study36-Item Short Form (SF-36).8,9 Whereas these surveysoffer insight into a patient’s global well-being, factors unre-lated to a patient’s injured limb (ie, socioeconomic status,education level, age, psychiatric disorders) can heavily in-fluence outcomes.9 As a result, the addition of a disease-specific quality of life survey can be helpful in determiningthe impact of a patient’s injury on quality of life. This, inturn, may allow further investigation of limb-specific modi-fiable factors to improve a patient’s quality of limb and life.
Currently, no disease-specific quality of life surveystarget extremity vascular injuries. The Short Musculoskel-etal Function Assessment (SMFA) is a limb-specific qualityof life survey developed for musculoskeletal disease andpostinjury states and has potential translational value in pa-tients with combat-related extremity vascular injuries. Theobjective of this study was to validate the use of the SMFAin a cohort of patients with battlefield-related extremityvascular injuries.

JOURNAL OF VASCULAR SURGERYVolume 60, Number 6 Scott et al 1621
METHODS
Patient selection and data acquisition
This study was conducted under approval from theU.S. Army Medical Research and Material CommandInstitutional Review Board. The Joint Theater TraumaRegistry (JTTR) and associated Vascular Injury Initiative(JTTR-VII) database were used.10 A query of the JTTRwas performed, identifying U.S. troops who sustained ex-tremity vascular injury in either Operation Iraqi Freedom(Iraq, 2003-2011) or Operation Enduring Freedom(Afghanistan, 2001 to present). To limit potential con-founding variables influencing recovery from extremityvascular injury, patients who sustained concomitant headinjuries (blunt or penetrating) with severe traumatic braininjury and ongoing neurologic and cognitive sequelaewere excluded. In addition, patients who sustained multi-ple limb injuries, including associated primary or traumaticamputations (nonindex limb), were also excluded. Further,patients who had undergone initial attempts at limbsalvage, followed by secondary or delayed amputation,were also excluded.
All patients underwent chart review for collection ofpertinent demographic and injury-specific information toinclude point-of-contact assessments of injury severity:the Injury Severity Score (ISS, 2005 revision) and theMangled Extremity Severity Score (MESS). Patients werethen contacted by a team of research nurse coordinators,and informed consent was obtained. Patients consentingto the study were administered the SF-36 and SMFAsurveys.
Survey selection
SF-36. The SF-36 generic quality of life survey con-sists of 36 multiple-choice questions and seeks to evaluatethe overall quality of life of a patient in a wide variety ofdisease and injury states.8,11,12 The SF-36 targets eightspecific scales of well-being, each with its own score. Fourscales (vitality, social functioning, role emotional, andmental health) contribute to an encompassing mentalcomponent summary score, and four scales (physicalfunctioning, role physical, bodily pain, and general health)contribute to an overall physical component summaryscore. Each raw score is scaled from 0 to 100, with higherscores denoting better health.13
SMFA. Developed from the longer MusculoskeletalFunction Assessment, the SMFA is a limb-specific, two-part, 46-item questionnaire designed to evaluate patients’perceived physical and emotional difficulty related to theirinjured or dysfunctional limb.14 Thirty-four questions aregrouped into four categories that evaluate a patient’sdysfunction related to daily activities, emotional status,upper extremity function, and mobility. These componentscontribute to an overall Dysfunction Index (SMFA-DI).The remaining 12 items assess how much patients arebothered by problems across four categoriesdrecreation/leisure, sleep/rest, work, and familydall of whichcontribute to an overall Bother Index (SMFA-BI). The
survey uses a 5-point Likert-type response system that isfurther transformed into a score ranging from 0 to 100,with higher scores indicative of poorer function.14
Statistical analysis
Content validity was evaluated by score distributionanalysis and was described in terms of range, kurtosis,and skew. Skew values of less than 1.0 were indicative ofa normal distribution. Floor and ceiling effects (percentageof scores at minimum or maximum values, respectively)were evaluated with acceptable proportions of <5%.Nonresponse rates were also evaluated, with values <5%as acceptable.
Construct validity was assessed by means of evaluatingrelationship to other health status questionnaires (ie, theSF-36). Survey comparisons were conducted withSpearman r, with r $ 60.5 considered to be of moderateclinical correlation.
Criterion validity was evaluated by the ability of theSMFA to predictively discriminate between groups on thebasis of external measures of dysfunction. Variablesanalyzed included disability qualifications and injuryseverity. Dichotomous delineations were based on previ-ously reported standards. Those qualifying for MedicarePart A disability were considered disabled and were ulti-mately determined by Social Security Administration fieldoffice eligibility (ie, those with described injuries resultingin disability of at least 12 months’ duration, prohibitingfull-time employment). Those remaining on full active mil-itary duty were considered nondisabled. Those with ISS>15 were considered severely injured, and those withMESS $7 were considered to have severely injured ex-tremities.15-17 Parametric continuous variables were sum-marized by mean and standard deviation and werecompared by unpaired, two-tailed t-test.
All statistical testing was two sided, with a significancelevel of P < .05. SPSS version 20 software (IBM, Armonk,NY) was employed for statistical analysis.
RESULTS
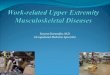
Demographic data. Query of the JTTR-VII resultedin 1018 service members with extremity vascular injuries(Fig 1). Successful contact was made in the majority ofpatients (n ¼ 891; 88%). At the time of analysis, 214 pa-tients (24%) completed both surveys. Exclusion of patientswith multiple limb injuries (including those with associatedprimary amputations, n ¼ 22) and those who eventuallyunderwent secondary amputation (n ¼ 28) resulted in acohort of 164 patients with a mean follow-up of 62.4 623.7 months. Patients were predominantly young (medianage, 25 years; 25th-75th interquartile range, 22-31 years),male (97.6%), and moderately to severely injured withmean ISS of 13.7 6 7.8 and MESS of 5.4 6 1.2. Addi-tional injury characteristics are detailed in Table I. Nodifferences in scores (SMFA or SF-36) were found incomparing patients with proximal vs distal injuries, arterialvs venous vs combined injuries, proximal vs distal injuries,upper vs lower injuries, injuries resulting from blast vs blunt

Table I. Injury characteristics
Extremity injuredUpper (%) 45.1Lower (%) 54.9
Mechanism of injuryBlast (%) 64.0Blunt (%) 2.4Penetrating (%) 33.5
Vessel injuredArterial (%) 70.1Venous (%) 9.8Combined (%) 20.1
Vessel locationProximal (%) 60.3Distal (%) 39.6
Associated injuriesSoft tissue (%) 85.4Bone (%) 45.7Nerve (%) 59.1
Fig 1. Consolidated Standards of Reporting Trials (CONSORT)diagram detailing number of combat-related extremity vascularinjuries on initial Joint Theater Trauma Registry (JTTR) query andfinal cohort after exclusion criteria.
Table II. Inverse correlation coefficients between ShortMusculoskeletal Function Assessment (SMFA) indicesand 36-Item Short Form Health Survey (SF-36) scales(all P < .001)
Dysfunction index vsPCS BP GH PF RP.636 .607 .524 .665 .563MCS VT RE MH SF.475 .550 .541 .477 .585
Bother index vsPCS BP GH PF RP.561 .603 .549 .541 .590MCS VT RE MH SF.589 .602 .620 .569 .642
BP, Body physical; GH, general health; MCS, mental component summary;MH, mental health; PCS, physical component summary; PF, physicalfunctioning; RE, role emotional; RP, role physical; SF, social functioning;VT, vitality.
JOURNAL OF VASCULAR SURGERY1622 Scott et al December 2014
vs penetrating, and presence of associated bone or softtissue injuries (all P > .05). There was a trend toward worsescores in the presence of nerve injury in both Dysfunctionand Bother indices (P ¼ .075 and .076, respectively).
Content validity. The mean SMFA-DI was 24.8 615.2. Scores ranged from 0 to 78 with a kurtosis and skewof 0.42 and 0.60, respectively. The floor and ceiling effectswere 1.2% and 0%, respectively. In comparison, the meanSMFA-BI was 29.4 6 20.2. Scores ranged from 0 to 96,with kurtosis and skewness values of 0.58 and �0.15,respectively. The respective floor and ceiling effects were4.3% and 0%. Whereas one subject (0.6%) did not respondwith answers to the SMFA-BI portion of the survey, therewas a 0% nonresponse for the SMFA-DI portion.
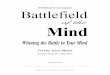
Construct validity. Correlations between reportedSMFA-DI and SMFA-BI scores and the SF-36 scales aredetailed in Table II. The SMFA-DI score inversely corre-lated most with the physical scales and associated compo-nent summary score. Represented graphically in Fig 2, A,an r value of �0.636 was indicative of a moderate inversecorrelation. Conversely, the SMFA-BI score inverselycorrelated most with the mental scales and componentsummary score. Similarly, a correlation coefficientof �0.589 was also considered a moderate inverse linearcorrelation (Fig 2, B).
Criterion validity. Of patients considered disabled,per Medicare Part A qualifications, both the SF-36component scores and SMFA indices demonstratedpoorer outcomes compared with those not qualifying fordisability (Table III, A). The SMFA-DI demonstrated thelargest disparity, with average scores of 33.3 6 16.2 vs22.3 6 14.2 in those considered disabled and nondisabled,respectively (P < .001).
Comparison of scores between those nonseverelyinjured and those considered major traumas/severelyinjured on the basis of overall ISS (score # 15 vs > 15)demonstrated no significant differences between eitherSF-36 component scores or SMFA indices (Table III, B).However, as demonstrated in Table III, C, on comparisonof patients without and with severe limb-specific injuryscores (MESS < 7 vs $ 7, respectively), only the SMFA
indices demonstrated significant differences in scores,each indicative of poorer outcomes (SMFA-DI: 31.5 615.7 vs 23.8 6 14.9, and SMFA-BI: 38.0 6 20.2 vs28.0 6 19.8; both P < .05).
DISCUSSION
SMFA. The SMFA, initially developed by Swiontkow-ski et al in 1999, has since been implemented in a widerange of musculoskeletal disease and pathologic states andhas undergone multiple cross-cultural adaptations.14,18-21
Whereas the initial target population of the SMFAincluded those with extremity musculoskeletal disease,there is clear theoretical translational potential in patientswith extremity vascular injuries. There exists a unique op-portunity in military medicine to evaluate this uniquecohort of patients. The validation and use of a limb-specificquality of life survey can help study and guide managementof this traditionally morbid injury pattern. Validity, orthe “degree to which a health-related patient-reported

Fig 2. A, Scatter plot and linear correlation of 36-Item Short Form Health Survey (SF-36) physical componentsummary vs Short Musculoskeletal Function Assessment Dysfunction Index (SMFA-DI) (r ¼ �0.636; P < .001). B,Scatter plot and linear correlation of SF-36 mental component summary vs Short Musculoskeletal Function AssessmentBother Index (SMFA-BI) (r ¼ �0.589; P < .001).
Table III. A, Score comparisons between disabled and nondisabled patients (as defined by Medicare Part A qualification)
Survey Disabled (n ¼ 38) Nondisabled (n ¼ 119) Mean difference (95% CI) P value
SF-36 PCS 40.9 6 7.9 44.2 6 9.7 3.4 (0.3-6.5) .034SF-36 MCS 41.8 6 13.3 48.0 6 12.0 6.2 (1.4-11.1) .012SMFA-DI 33.3 6 16.2 22.3 6 14.2 �11.0 (�16.8 to �5.1) <.001SMFA-BI 37.2 6 18.9 26.6 6 20.0 �10.6 (�17.7 to �3.4) .004
CI, Confidence interval; MCS, mental component summary; PCS, physical component summary; SF-36, 36-Item Short Form Health Survey; SMFA-BI, ShortMusculoskeletal Function Assessment Bother Index; SMFA-DI, Short Musculoskeletal Function Assessment Dysfunction Index.
Table III. B, Score comparisons between severe (ISS > 15) and nonsevere (ISS # 15) overall injury scores
Survey Severely injured (ISS > 15; n ¼ 46) Nonseverely injured (ISS # 15; n ¼ 117) Mean difference (95% CI) P value
SF-36 PCS 43.0 6 8.4 43.7 6 9.5 0.7 (�2.3 to 3.7) .663SF-36 MCS 46.7 6 11.4 46.0 6 13.3 �0.6 (�4.8 to 3.5) .767SMFA-DI 24.2 6 13.7 25.0 6 15.8 0.8 (�4.1 to 5.8) .742SMFA-BI 27.5 6 17.2 29.9 6 21.1 2.4 (�4.0 to 8.7) .461
CI, Confidence interval; ISS, Injury Severity Score; MCS, mental component summary; PCS, physical component summary; SF-36, 36-Item Short FormHealth Survey; SMFA-BI, Short Musculoskeletal Function Assessment Bother Index; SMFA-DI, Short Musculoskeletal Function Assessment DysfunctionIndex.
Table III. C, Score comparisons between severe (MESS $ 7) and nonsevere (MESS < 7) limb injury scores
Survey Mangled extremity (MESS $ 7; n ¼ 24) Nonmangled extremity (MESS < 7; n ¼ 140) Mean difference (95% CI) P value
SF-36 PCS 41.1 6 8.9 43.8 6 9.3 2.7 (�1.3 to 6.7) .180SF-36 MCS 45.0 6 12.4 46.5 6 12.9 1.5 (�4.1 to 7.1) .583SMFA-DI 31.5 6 15.7 23.8 6 14.9 �7.8 (�14.8 to �0.8) .031SMFA-BI 38.0 6 20.2 28.0 6 19.8 �10.0 (�19.1 to �0.9) .032
CI, Confidence interval; MCS, mental component summary; MESS, Mangled Extremity Severity Score; PCS, physical component summary; SF-36, 36-ItemShort Form Health Survey; SMFA-BI, Short Musculoskeletal Function Assessment Bother Index; SMFA-DI, Short Musculoskeletal Function AssessmentDysfunction Index.
JOURNAL OF VASCULAR SURGERYVolume 60, Number 6 Scott et al 1623
outcome instrument measures the construct it purports tomeasure,” in this cohort has been assessed across itsfundamental properties of content, construct, and criterionvalidity.22
Content validity. Content validity is the “degree towhich a health-related patient-reported outcome instru-ment is an adequate reflection of the construct to bemeasured.”21 The most important aspect contributing to
the content validity is the degree to which the measure-ment instrument matches the target population.23 Allquestions of the SMFA are demographically and clinicallyrelevant to patients with extremity vascular injuries.Expectedly, relying on face validity in this manner is oftenpurely a subjective measure of content. Therefore, scoredistribution characteristics can be employed as surrogatesto evaluate the appropriateness of survey items.14,23 As

JOURNAL OF VASCULAR SURGERY1624 Scott et al December 2014
such, a normal curve distribution of reported scores is ex-pected with limited floor/ceiling effects and nonresponserates. Whereas a floor/ceiling effect is typically defined as15% of highest and lowest possible scores, respectively,values of <5% are considered favorable.14,24,25 Asdemonstrated, content validity of the SMFA was present inthis cohort of patients with extremity vascular injuries. TheSMFA-DI encompassed a wide range of scores with littleskew, limited ceiling and floor effects, and 0% nonresponserates. The SMFA-BI demonstrated similar results, althoughwith slightly higher but acceptable floor effects andbroadened kurtosis value.
Construct validity. Construct validity is the “degreeto which the scores of a health-related patient-reportedoutcome instrument are consistent with other hypotheses(ie, relationship to scores of other [established] in-struments) based on the assumption that the instrumentvalidly measures the construct to be measured.”22
Convergent construct validity was evaluated by compari-son of the SMFA to an established generic quality of lifesurvey (ie, SF-36). The SF-36 has been validated in a widerange of disease and postinjury states and has also beendescribed previously in this particular patient cohort toeffectively distinguish between those with favorable andunfavorable outcomes.9 In comparing the SMFA indices tothe SF-36 subscale scores, there were predominantlymoderate correlations (defined as 50%-75% correlation).23
This correlation was most pronounced between the phys-ical component summary score of the SF-36 and theDysfunction Index of the SMFA (r ¼ �0.636) and themental component summary score of the SF-36 and theBother Index of the SMFA (r ¼ �0.589). Previous studies,including the initial validation of the SMFA, have evaluatedthe relationship between the SMFA and SF-36 in a widerange of orthopedic and rheumatologic pathologic states,all demonstrating similarly moderate to strong correlationcoefficients ranging from �0.47 to �0.81.14,26
Criterion validity. Criterion validity is the “degree towhich the scores of a health-related patient-reportedoutcome instrument are an adequate reflection of a “goldstandard” [as measured by concurrent or predictive val-idity].”22 Whereas there exists no current gold standard ofevaluating a patient’s perceived limb dysfunction, clinicallyrelevant substitutes include objective injury severity scoring(concurrent) and disability qualifications (predictive).Comparison between those who were considered to havesevere or mangled extremities and those with less severeinjuries (MESS $7 and <7, respectively), the SMFA-DIand SMFA-BI demonstrated improved discriminativecapability compared with the SF-36. Similar findings weredemonstrated in comparison between those patients whoqualified for disability (as determined by Medicare Part Aeligibility) and those who did not.
As demonstrated, neither the SMFA nor the SF-36 wasable to demonstrate significant score differences betweenthose who were considered to have severe overall injuries(ISS > 15) and those who were not (ISS # 15). Onemay infer that a higher global injury severity would
translate into poorer outcomes. Whereas the ISS may beuseful in evaluating a patient’s initial mortality associatedwith a particular injury pattern, consideration of potentialconfounding variables should be made in applying any pre-dictive value to long-term morbidity. First, the ISS con-siders multiple organ systems in computing a final ISSscore. Severe injuries, although conferring similar effectson initial survival, often have different long-term sequelaeaffecting a patient’s long-term quality of life. For example,splenic lacerations and severely mangled extremities,although both life-threatening on initial presentation,have significantly different long-term outcomes. Second,the ISS is a compounded calculation from multiple abbre-viated injury scores. As such, recording errors becomecompounded as well. Last, the conventional ISS cutoffscore of 15 may be overly sensitive, capturing patientswith more moderate injuries and improved recovery andlong-term outcomes. These confounders may result inthe inability of the SMFA or SF-36 to delineate thosewith truly severe and morbid injuries based on an ISS scoreof 16 or more.
Limitations. Several limitations of this study warrantmention. There is significant heterogeneity within thecohort of patients examined. Whereas all patients incurredsignificant extremity vascular injuries, all requiring surgicalintervention (ie, operative exploration with ligation orrepair), certain injury patterns have differing potential forlong-term dysfunction or disability. Nevertheless, hetero-geneity limits the purity of application to specific injurypatterns. Possible type II errors may exist, particularly inevaluating the criterion validity of the SMFA. Inclusion ofall extremity vascular injuries into a single cohort allowssubsequent broader application.
Primary and secondary/delayed amputees wereexcluded from analysis. The military experience with ampu-tation and limb salvage (in the setting of severe orthopedicinjuries) has been described elsewhere.27 Inherently, thereexist many complex and potentially confounding variableswithin this demographic that can significantly affect out-comes and analysis when considered as a total group.Conceivably, quality of life scores can be influenced by fac-tors such as time to secondary amputation, level of ampu-tation, type/capability of prosthesis, ancillary support(professional and family), and other factors. As demon-strated by Doukas et al, patients undergoing amputationappeared to even have less dysfunction compared withlimb salvage, although the authors do acknowledge a largepotential selection bias.27 Additional and directed investi-gation in the outcomes of this unique patient populationis warranted once patient accrual has been accomplished.
Whereas these results help validate the use of theSMFA in the setting of extremity vascular injuries, nodata currently exist to examine the reliability or responsive-ness of the SMFA. The trauma population has several prac-tical limitations in the ability to assess a patient’s well-beingand limb functionality in a preinjury state. In addition,long-term evaluation of this injury pattern by objectiveclinical tests of limb dysfunction is often logistically

JOURNAL OF VASCULAR SURGERYVolume 60, Number 6 Scott et al 1625
difficult. Clinical efforts are being made to improve long-term clinical surveillance of extremity vascular injuries.
This study is also survey based and has additionallimitations to be considered. As with many studies ofthis nature, there was significant overall nonresponse.Whereas effort was made to limit this by offering multi-ple modalities of survey fulfillment, scheduled reminders,and available staff for questions and concerns, the studyexperienced approximately 76% nonresponse rate. Under-standably, this lends results to a possible selection bias asmany nonresponders may also be outliers, thus influ-encing both ceiling and floor effects. Although otherstudies cross-validating the SMFA quote higher returnrates, they are often smaller or with significantly shorterfollow-up.14,18-21,26,28-31
CONCLUSIONS
Use of the SMFA is valid in those with extremityvascular injuries. Across all facets of survey validity, theSMFA-DI in particular was best able to describe all aspectsof a patient’s limb dysfunction and to correlate with estab-lished quality of life surveys, and it was better able todiscriminate patients by means of external indicators oflimb injury severity. The SMFA should be considered anadjunctive tool in evaluating patient-based outcomes aftercombat-related extremity vascular injuries.
The authors acknowledge Joint Theater Trauma Reg-istry (JTTR) and Patient Administration Systems andBiostatistics Activity (PASBA) for providing data for thisstudy.
AUTHOR CONTRIBUTIONS
Conception and design: DS, ZAAnalysis and interpretation: DS, BP, ZAData collection: DS, JW, TH, MCWriting the article: DS, JW, TH, MCCritical revision of the article: DS, BP, ZAFinal approval of the article: DS, JW, TH, MC, BP, ZAStatistical analysis: DS, ZAObtained funding: BP, ZAOverall responsibility: ZA
REFERENCES
1. White JM, Stannard A, Burkhardt GE, Eastridge BJ, Blackbourne LH,Rasmussen TE. The epidemiology of vascular injury in the wars in Iraqand Afghanistan. Ann Surg 2011;253:1184-9.
2. Gifford SM, Aidinian G, Clouse WD, Fox CJ, Porras CA, Jones WT,et al. Effect of temporary shunting on extremity vascular injury: anoutcome analysis from the Global War on Terror vascular injuryinitiative. J Vasc Surg 2009;50:549-55; discussion: 555-6.
3. Markov NP, DuBose JJ, Scott D, Propper BW, Clouse WD,Thompson B, et al. Anatomic distribution and mortality of arterialinjury in the wars in Afghanistan and Iraq with comparison to a civilianbenchmark. J Vasc Surg 2012;56:728-36.
4. Rasmussen TE, Clouse WD, Jenkins DH, Peck MA, Eliason JL,Smith DL. The use of temporary vascular shunts as a damage controladjunct in the management of wartime vascular injury. J Trauma2006;61:8-12; discussion: 12-5.
5. Rasmussen TE, Clouse WD, Jenkins DH, Peck MA, Eliason JL,Smith DL. Echelons of care and the management of wartimevascular injury: a report from the 332nd EMDG/Air Force TheaterHospital, Balad Air Base, Iraq. Perspect Vasc Surg Endovasc Ther2006;18:91-9.
6. Woodward EB, Clouse WD, Eliason JL, Peck MA, Bowser AN,Cox MW, et al. Penetrating femoropopliteal injury during modernwarfare: experience of the Balad Vascular Registry. J Vasc Surg2008;47:1259-64; discussion: 1264-5.
7. Kragh JF Jr, Littrel LM, Jones JA, Walters TJ, Baer DG, Wade CE,et al. Battle casualty survival with emergency tourniquet use to stoplimb bleeding. J Emerg Med 2011;41:590-7.
8. Ware JE Jr, Sherbourne CD. The MOS 36-item short-form healthsurvey (SF-36). I. Conceptual framework and item selection. Med Care1992;30:473-83.
9. Scott DJ, Arthurs ZM, Stannard A, Monroe HM, Clouse WD,Rasmussen TE. Patient-based outcomes and quality of life aftersalvageable wartime extremity vascular injury. J Vasc Surg 2014;59:173-9.
10. Stannard A, Scott DJ, Ivatury RA, Miller DL, Ames-Chase AC,Feider LL, et al. A collaborative research system for functional out-comes following wartime extremity vascular injury. J Trauma AcuteCare Surg 2012;73(Suppl 1):S7-12.
11. McHorney CA, Ware JE Jr, Lu JF, Sherbourne CD. The MOS 36-itemShort-Form Health Survey (SF-36): III. Tests of data quality, scalingassumptions, and reliability across diverse patient groups. Med Care1994;32:40-66.
12. McHorney CA, Ware JE Jr, Raczek AE. The MOS 36-Item Short-Form Health Survey (SF-36): II. Psychometric and clinical tests ofvalidity in measuring physical and mental health constructs. Med Care1993;31:247-63.
13. SF-36 [Internet]. Version v2. Available at: http://www.sf-36.org.Accessed July 2012.
14. Swiontkowski MF, Engelberg R, Martin DP, Agel J. Short musculo-skeletal function assessment questionnaire: validity, reliability, andresponsiveness. J Bone Joint Surg Am 1999;81:1245-60.
15. Salottolo K, Settell A, Uribe P, Akin S, Slone DS, O’Neal E, et al. Theimpact of the AIS 2005 revision on injury severity scores and clinicaloutcome measures. Injury 2009;40:999-1003.
16. Johansen K, Daines M, Howey T, Helfet D, Hansen ST Jr. Objectivecriteria accurately predict amputation following lower extremitytrauma. J Trauma 1990;30:568-72; discussion: 572-3.
17. Prichayudh S, Verananvattna A, Sriussadaporn S, Sriussadaporn S,Kritayakirana K, Pakart R, et al. Management of upper extremityvascular injury: outcome related to the Mangled Extremity SeverityScore. World J Surg 2009;33:857-63.
18. Bohm TD, Kirschner S, Kohler M, Wollmerstedt N, Walther M,Matzer M, et al. The German Short Musculoskeletal FunctionAssessment questionnaire: reliability, validity, responsiveness, andcomparison with the Short Form 36 and Constant scoreda prospectiveevaluation of patients undergoing repair for rotator cuff tear. Rheu-matol Int 2005;25:86-93.
19. Taylor MK, Pietrobon R, Menezes A, Olson SA, Pan D, Bathia N, et al.Cross-cultural adaptation and validation of the Brazilian Portugueseversion of the short musculoskeletal function assessment questionnaire:the SMFA-BR. J Bone Joint Surg Am 2005;87:788-94.
20. Reininga IH, el Moumni M, Bulstra SK, Olthof MG, Wendt KW,Stevens M. Cross-cultural adaptation of the Dutch Short Musculo-skeletal Function Assessment questionnaire (SMFA-NL): internalconsistency, validity, repeatability and responsiveness. Injury 2012;43:726-33.
21. Ponzer S, Skoog A, Bergstrom G. The Short Musculoskeletal FunctionAssessment Questionnaire (SMFA): cross-cultural adaptation, validity,reliability and responsiveness of the Swedish SMFA (SMFA-Swe). ActaOrthop Scand 2003;74:756-63.
22. Mokkink LB, Terwee CB, Patrick DL, Alonso J, Stratford PW,Knol DL, et al. The COSMIN study reached international consensuson taxonomy, terminology, and definitions of measurement propertiesfor health-related patient-reported outcomes. J Clin Epidemiol2010;63:737-45.

JOURNAL OF VASCULAR SURGERY1626 Scott et al December 2014
23. Scholtes VA, Terwee CB, Poolman RW. What makes a measurementinstrument valid and reliable? Injury 2011;42:236-40.
24. McHorney CA, Tarlov AR. Individual-patient monitoring in clinicalpractice: are available health status surveys adequate? Qual Life Res1995;4:293-307.
25. Terwee CB, Bot SD, de Boer MR, van der Windt DA, Knol DL,Dekker J, et al. Quality criteria were proposed for measurementproperties of health status questionnaires. J Clin Epidemiol 2007;60:34-42.
26. Busse JW, Bhandari M, Guyatt GH, Heels-Ansdell D, Mandel S,Sanders D, et al; SPRINT Investigators. Use of both Short Musculo-skeletal Function Assessment questionnaire and Short Form-36 amongtibial-fracture patients was redundant. J Clin Epidemiol 2009;62:1210-7.
27. Doukas WC, Hayda RA, Frisch HM, Andersen RC, Mazurek MT,Ficke JR, et al. The Military Extremity Trauma Amputation/LimbSalvage (METALS) study: outcomes of amputation versus limb salvagefollowing major lower-extremity trauma. J Bone Joint Surg Am2013;95:138-45.
28. Van Son MA, Den Oudsten BL, Roukema JA, Gosens T,Verhofstad MH, De Vries J. Psychometric properties of the Dutch
Short Musculoskeletal Function Assessment (SMFA) questionnaire inpatients with a fracture of the upper or lower extremity. Qual Life Res2014;23:917-26.
29. Kirschner S, Walther M, Bohm D, Matzer M, Heesen T, Faller H, et al.German short musculoskeletal function assessment questionnaire(SMFA-D): comparison with the SF-36 and WOMAC in a prospectiveevaluation in patients with primary osteoarthritis undergoing total kneearthroplasty. Rheumatol Int 2003;23:15-20.
30. Dattani R, Slobogean GP, O’Brien PJ, Broekhuyse HM, Blachut PA,Guy P, et al. Psychometric analysis of measuring functional outcomes intibial plateau fractures using the Short Form 36 (SF-36), ShortMusculoskeletal Function Assessment (SMFA) and the WesternOntario McMaster Osteoarthritis (WOMAC) questionnaires. Injury2013;44:825-9.
31. Hedbeck CJ, Tidermark J, Ponzer S, Blomfeldt R, Bergstrom G.Responsiveness of the Short Musculoskeletal Function Assessment(SMFA) in patients with femoral neck fractures. Qual Life Res2011;20:513-21.
Submitted Jun 8, 2014; accepted Aug 6, 2014.
![Musculoskeletal Soft Tissue Clinic...the patient has a mangled extremity [ 1,2]. Achieving the best outcome in patients with severe extremity injuries requires a multidisciplinary](https://img.pdfslide.us/doc/110x75/5ee0b2eaad6a402d666bd6e4/musculoskeletal-soft-tissue-the-patient-has-a-mangled-extremity-12-achieving.jpg)


















![Musculoskeletal Soft Tissue Clinic · the patient has a “mangled extremity” [1,2]. Achieving the best outcome in patients with severe extremity injuries requires a multidisciplinary](https://img.pdfslide.us/doc/110x75/5ee0b2c9ad6a402d666bd6d2/musculoskeletal-soft-tissue-the-patient-has-a-aoemangled-extremitya-12-achieving.jpg)