Embed Size (px)
Citation preview

Validation of the Immunoscore Prognostic Value in Stage III Colon Cancer Patients treated with Oxaliplatin
in the prospective IDEA France cohort study (PRODIGE-GERCOR).
ASCO 2019
Abstract #3513
copies of this poster obtained through Quick Response (QR) Code
are for personal use only and may not be reproduced without permission
from ASCO® and the author of this poster
Introduction
Methods
Results
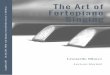
Prognostic value of IS in stage III patients
(A) IS 2 groups (Low, Int+High) (B) IS 3 groups (Low, Int, High) (C) Low-risk / High-risk (IS 2 groups)
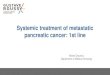
-> T stage, N stage, gender, MSI status and IS are independent parameters (all p < 0.05)
Multivariable analyses
Multivariate analysis for DFS
combining IS and Histopathological classifications
Conclusion
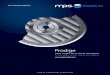
IS (Int + High)
IS Low
(B) Low risk (T1-T3, N1) (C) High risk (T4 and/or N2) (A) All patients
The efficacy of 3 vs 6 months of mFOLFOX6 therapy according to IS status
- The Immunoscore in 2 categories (Low, Int +High), 3 categories (Low, Int, High) and as a continuous variable is confirmed as a prognostic factor for DFS in stage III CC patients in the prospective IDEA France cohort study. - Only patients with IS Intermediate or High did benefit from 6 months of mFOLFOX6 treatment compared with 3 months, both in low (T1-T3, N1) and high-risk (T4 and/or N2) stage III groups - These results need to be confirmed on another patients’ population included in the IDEA international study, to evaluate the IS impact on the efficacy of 3 vs 6 months of CAPOX treatment, and to validate its use to guide the choice of oxaliplatin-based adjuvant chemotherapy duration in stage III CC.
Franck Pagès1,2,4,17, Thierry André6, Julien Taieb2,3,4, Dewi Vernerey7,8, Julie Henriques7,8, Florence Marliot1,2,4,17, Rim Ben Jannet9,10, Christophe Louvet11, Laurent Mineur12, Jaafar Bennouna13, Jérôme Desrame14, Roger Faroux15, Alex Duval5, Pierre Laurent-Puig2,4, Magali Svrcek3,6, Fabienne Hermitte16, Aurélie Catteau16, Jérôme
Galon1,3,4,5,17, Jean-François Emile9,10
1- INSERM, Laboratory of Integrative Cancer Immunology, Equipe Labellisée Ligue Contre le Cancer, Paris, France; 2- Européen Georges Pompidou Hospital, Paris, France; 3- Université Sorbonne Paris Cité, Paris, France; 4- Université Paris Descartes, Paris, France; 5- Université Paris Diderot, Paris, France; 6- Saint-Antoine Hospital,
Paris, France; 7- Methodology and Quality of Life in Oncology Unit, Besançon University Hospital, Besançon, France; 8- Bourgogne Franche-Comté University, INSERM, Etablissement Français du Sang Bourgogne Franche-Comté, UMR1098, Interactions Hôte-Greffon-Tumeur/Ingénierie Cellulaire et Génique, Besançon, France; 9-
EA4340-BECCOH, Versailles University, Boulogne, France; 10- Ambroise Paré Hospital, AP-HP, Boulogne, France; 11- Institut Mutualiste Montsouris, Paris, France ; 12- Institut Sainte Catherine, Avignon, France; 13- University Hospital of Nantes, Nantes, France; 14- Private Hospital Jean Mermoz, Lyon, France; 15- CHD Vendée, La
Roche sur Yon, France; 16- HalioDx, Marseille, France; 17- Centre de Recherche des Cordeliers, Paris, France
- Immunoscore@ (IS) is an IVD assay, which provides an individualized risk of relapse in early-stage colon cancer (CC) patients
by measuring the host adaptive immune response in the tumor core and its invasive margin.1
- It has been repeatedly shown to provide a prognostic factor independent and more accurate than the AJCC-UICC TNM
classification.2, 3
- Its robustness and prognostic performance has been consolidated through an international validation study of 3 539 patients’
stage I-III CCs from 13 countries led by the Society for Immunotherapy of Cancer (SITC).4
- IS was assessed in the IDEA France cohort study,5 evaluating 3 vs 6 months of oxaliplatin-based adjuvant chemotherapy in
stage III CC patients.
The primary objective was to validate whether the Immunoscore test is able to identify patients with high risk of
relapse or death whichever occurs first among stage III patients under oxaliplatin-based adjuvant therapy
IDEA France Cohort
- Phase III randomized study of stage III CC patients (IDEA France part [n=2010] of the IDEA international collaboration
[n=12834]).6
- 3 vs 6 months of chemotherapy with mFOLFOX6 or CAPOX.
- Randomization stratified by center, T stage, N stage, ECOG PS, and age.
- mFOLFOX6 or CAPOX left to the patient and investigator decision; 90% of patients were treated with mFOLFOX6, 10% with
CAPOX.
Immunoscore Methodology
- Densities of CD3+ and cytotoxic CD8+ T cells in the core tumor (CT)
and invasive margin (IM) of each patient were quantified by digital
pathology and converted to IS using pre-defined published cut-offs.4
- IS was classified into 2-groups (Low, Int+High); in 3-groups (Low, Int, High),
and as a continuous score.
Statistics
- The performance of IS to predict disease-free survival (DFS) was assessed in the modified intention-to-treat population, in
each study arm and was adjusted with clinical features in multivariable Cox models. Harrell’s C-statistics was used to
investigate the IS performance.
- The study design is registered on ClinicalTrials.gov (#NCT03422601).
Patients Characteristics and IS Determination
- 1 322 patients with available tumor sample. A lower proportion of low-risk patients (T1-T3/N1), especially with T1 tumors was
observed in those with sample available for the IS characterization.
- 82 samples were excluded due to pre-analytical non-conformity; 1 062 patients (85.6%) reached the IS quality control, 973
treated with mFOLFOX6 and 89 by CAPOX.
- 463 (43.6%) IS Low; 20 MSI (4.6%), 414 MSS (95.4%), 29 missing data
- 499 (47.0%) IS Intermediate; 34 MSI (7.2%), 439 MSS (92.8%), 26 missing data
- 100 (9.4%) IS High; 22 MSI (23.7%), 71 MSS (76.3%), 7 missing data
(A) Among patients’ groups stratified by IS in 2 categories (Low vs Int+High), the 3-year DFS rates were 66.80% [95%CI 62.23-
70.95] and 77.14% [95%CI 73.50-80.35] for IS Low and IS Int+High, respectively (p=0.0001).
(B) With IS in 3 categories, the 3-year DFS rate of 85% was observed in patients with IS High, vs 67% in patients with IS Low
(p=0.0001) NB: IS as continuous variable was also significantly associated with 3-year DFS (p<0.001).
(C) The deleterious effect of IS Low in terms of DFS was higher in patients with T1-3 than in patients with T4 tumors (p=0.0212).
(A) The beneficial effect of the 6 months vs 3 months FOLFOX regimen was observed in patients with IS (Int+High).
(B, C) This benefit was retained in the low-risk (T1-T3 and N1) and in the high-risk tumors (T4 and/or N2). In contrast, no
significant benefit of the 6-month FOLFOX regimen was observed for patients with IS Low. A moderate benefit of the
6-month FOLFOX regimen was observed in the first 3 years and was nullified thereafter.
References 1 Galon J et al. J Pathol 2014; 2 Mlecnik B et al. J Immunity 2016; 3 Sinicrope F et al. J Clin Oncol 2018;4 Pagès F et al. The Lancet 2018; 5 André T et
al. J Clin Oncol 2018; 6 Grothey A et al. NEJM 2018