Embed Size (px)
Citation preview

Validation of the Functional Assessment of CancerTherapy Esophageal Cancer Subscale
Gail Darling, MD1
David T. Eton, PhD2
Joanne Sulman, MSW3
Alan G. Casson, MB, ChB4
David Cella, PhD2
1 Division of Thoracic Surgery, Toronto GeneralHospital, University of Toronto, Toronto, Ontario,Canada.
2 Center on Outcomes, Research and Education,Evanston Northwestern Healthcare and Northwes-tern University Feinberg School of Medicine,Evanston, Illinois.
3 Department of Social Work, Mount Sinai Hospi-tal, Toronto, Ontario, Canada.
4 Division of Thoracic Surgery, Dalhousie Univer-sity, Halifax, Nova Scotia, Canada.
BACKGROUND. To develop and validate a quality of life subscale for patients with
esophageal cancer to be used with the Functional Assessment of Cancer Ther-
apy—General (FACT-G).
METHODS. Prospective cohort study of patients with esophageal cancer treated
with surgery alone or neoadjuvant chemoradiotherapy and surgery evaluating the
validity, internal consistency, and responsiveness to change of the FACT-Esopha-
geal (FACT-E) when comparing it with the European Organization for the
Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ
30) and esophageal (OES 24) as well as clinical factors.
RESULTS. The FACT-E demonstrated very good convergent and divergent valid-
ity when compared with the EORTC QLQ30 and OES 24 and clinical variables.
Internal consistency was also good with coefficient a >0.70 for all subscales
and individual items. Stability coefficients were >0.80. Changes in clinical status
were reflected in changes in FACT-E scores demonstrating responsiveness to
change, particularly in patients receiving neoadjuvant chemoradiotherapy before
surgery.
CONCLUSIONS. The FACT-E met or exceeded all standards for validity, providing
an option to measure health-related quality of life for different treatment strate-
gies for esophageal cancer. Cancer 2006;107:854–63.
� 2006 American Cancer Society.
KEYWORDS: esophageal neoplasm, quality of life, health-related quality of life,cancer treatment.
E sophageal cancer has the sixth highest mortality rate of all can-
cers.1 Overall survival is <10% although 5-year survival for
resected patients is 20%–40%.2–5 Phase III trials of neoadjuvant che-
moradiotherapy before surgery have been disappointing, but meta-
analyses have shown some survival benefit.6 However, the time
required for such regimens represents 20% of the estimated median
survival of 16.3 months for patients with resected esophageal can-
cer.7 Relief of the dysphagia experienced by patients with esopha-
geal cancer is also a very important outcome not only because
of resulting weight loss but also because of the loss of enjoyment of
eating with friends or family and social isolation. Hence, quality of
life is an important consideration when making treatment decisions.
To evaluate the effect of treatment on quality of life, an esophageal
cancer subscale (ECS) to be used with the Functional Assessment of
Cancer Therapy—General (FACT-G) quality of life measure was
developed. The FACT-Esophageal (FACT-E) is the complete measure
(FACT-G and ECS). The objective of this study was to validate the
FACT-E in patients with esophageal cancer.
Address for reprints: Gail Darling, MD, Division ofThoracic Surgery, University of Toronto, TorontoGeneral Hospital 9N-955, 200 Elizabeth Street,Toronto, Ontario M5G 2C4, Canada; Fax: (416)340-3660; E-mail: [email protected]
We acknowledge the contributions of Lynn Coul-ter, Jennifer Hornby, and Debbie Murnaghan incompleting this research.
Received December 8, 2005; revision receivedMarch 24, 2006; accepted March 31, 2006.
ª 2006 American Cancer SocietyDOI 10.1002/cncr.22055Published online 6 July 2006 in Wiley InterScience (www.interscience.wiley.com).
854

METHODSDevelopment of the FACT Esophageal Cancer SubscaleThe ECS was developed using an iterative process of
item generation, item reduction, scale construction,
and initial psychometric evaluation.
Item generationThe initial items for the esophageal subscale were
adapted from a disease-specific instrument for head
and neck cancer and the initial questionnaire devel-
oped in collaboration with Cella et al.8,9
Item reduction and further item generationThrough qualitative analysis based on feedback from
11 patients, the initial 57-item disease-specific ques-
tionnaire generated several symptom themes: cough-
ing, pain, lack of energy/fatigue, digestion/elimination,
swallowing, eating including social aspects, and voice
quality. Items that did not fall into these themes as
well as redundant items were eliminated.
After field testing, new items were generated: dry
mouth, breathing, communication, sleep disturbance,
and weight loss. The final list of 17 esophageal-speci-
fic items was appended to the FACT-G and then
evaluated by 7 patients. Feedback confirmed the ap-
propriateness of the changes and ease of completion
of the questionnaire.
Scale constructionThe esophageal subscale was revised to be consistent
with the existing FACT subscales and then reviewed
by an expert panel, and field-tested with 38 patients
who reported that the FACT-E questions were easy to
understand and answer.
Initial psychometric evaluationBased on initial results demonstrating good internal
consistency (Cronbach’s a ¼ 0.86; SPSS 10.0), a for-
mal validation study was initiated.
Validation of the FACT-EThe following steps were completed:
1. Determine the convergent and divergent validity
of the FACT-E against an established standard,
European Organization for the Research and Treat-
ment of Cancer Quality of Life Questionnaire(EORTC core QLQ-C30) and OES 24.
2. Determine the internal consistency and stability
of the FACT-E and its subscales in comparison
with an established standard.
3. Determine the concurrent validity of the FACT-E
by comparing scores across clinical risk factors.
4. Determine the responsiveness to change of the
FACT-E over time and with changes in clinicalcondition.
The 2 parts of the study included the initial vali-
dation in a group of surgical patients (Cohort A) and
then further evaluation of responsiveness to change
in patients receiving induction chemoradiotherapy
before surgery (Cohort B). The study was approved
by the institutional research ethics boards and
informed consent was obtained from all patients.
Study MeasuresFACT-EThe FACT-G consists of 27 items divided among
4 subscales: physical well-being (PWB), functional
well-being (FWB), social/family well-being (SWB), and
emotional well-being (EWB). The sum of these sub-
scales forms the total FACT-G score. The FACT-G
has been well studied and previously validated.9 The
ECS addresses concerns specific to patients with
esophageal cancer such as eating, appetite, swallow-
ing, pain, talking/communicating, mouth dryness,
breathing difficulty, coughing, and weight loss. The
total FACT-E score is the sum of the ECS and the
FACT-G scores. A trial outcome index (TOI) score,
useful where the physical domains are of interest,
was computed by adding the PWB and FWB scores
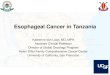
to the ECS score (See Fig. 1).
Swallowing and eating indexesSwallowing and eating indexes were created a priori
from the ECS items. The swallowing index consists of
5 items (items hn7, e1, e2, e3, and e5 in Fig. 1), and
the eating index consists of 3 items (items hn1, hn5,
and e6 in Fig. 1).
All FACT-E items are rated on a 5-point Likert-
type scale ranging from 0 ¼ ‘‘not at all’’ to 4 ¼ ‘‘very
much’’. Negatively-worded items are reverse scored
so that higher scores always represent better quality
of life (QOL) or less severe symptoms. Possible score
ranges are PWB (0–28), FWB (0–28), SWB (0–28),
EWB (0–24), ECS (0–68), TOI (0–124), swallowing
index (0–20), eating index (0–12), FACT-G (0–108),
and FACT-E (0–176).
QLQ-C30 and OES 24The EORTC core QLQ-C3010 can be used across can-
cer types and consists of 5 functional scales (physi-
cal, role, emotional, cognitive, and social), a global
QOL scale, 8 symptom scales, and 5 single items.
QLQ functional and global QOL scores are trans-
formed to a linear 0–100 scale, with higher scores
indicating better function and QOL. Higher scores on
Validation of the FACT-E/Darling et al. 855

the symptom scales indicate greater symptomatology.
The esophageal cancer-specific module (OES 24) is
designed for use with esophageal cancer patients of
any stage or treatment. It consists of 6 scales and 5
single items (mouth dryness, taste sensation, cough-
ing, talking, and hair loss). All scale and single-item
scores are transformed to a 0–100 scale, with higher
scores indicating greater symptomatology.11
PatientsCohort A included 54 surgical patients with histologi-
cally proven resectable squamous or adenocarci-
noma of the esophagus or gastroesophageal junction,
18 years of age or older, competent to provide in-
formed consent, English-speaking, and with an esti-
mated survival of >3 months.
Cohort B included 29 patients scheduled for
neoadjuvant chemoradiation before surgery. Eligibil-
ity criteria were the same as for Cohort A, specifying
clinical stages T1N1M0, T2-3N0-1M0, T1-3N0-1M1a,
performance status Eastern Cooperative Oncology
Group 0–2, and were medically fit for chemora-
diotherapy.
Data CollectionCohort A patients completed the FACT-E and EORTC
QLQ C30 þ OES 24 modules before surgery (base-
line) and 3–4 months after surgery. At baseline
assessment, alcohol use, weight loss, pain, stage,
treatment, and performance status were noted. The
ECS was administered 3–7 days after the baseline
assessment to determine test–retest reliability.
Cohort B patients completed the FACT-E at base-
line (pretreatment), week 7 (near the end of neoadju-
vant therapy), and week 12–14 (4–6 weeks after
neoadjuvant therapy, but before surgery).
Data AnalysesSpearman correlations (r) were used to determine
the convergent and divergent validity of the FACT-E
including the overall scale, subscales, and aggregate
scores. Spearman correlations were also used to
determine test–retest reliability of the ECS. Coeffi-
cient a was used to determine internal reliability of
the FACT-E. Independent sample t tests were used to
determine whether FACT-E scores can discriminate
across clinical risk factors and symptoms (concurrent
FIGURE 1. Esophageal cancer sub-scale to be used with the FACT-G.
856 CANCER August 15, 2006 / Volume 107 / Number 4

validity). Because of the number of analyses, a was
set at 0.01 (2-tailed) for all significance tests. How-
ever, given the modest number of patients available
for each analysis, effect sizes (ESs) associated with
each mean difference were also computed. The ES
for cross-sectional analyses equals the group mean
difference divided by the pooled within group stan-
dard deviation.
Paired sample t test and repeated measures ana-
lyses of variance (ANOVAs) were used to determine
responsiveness to change in the FACT-E over time. awas again set at 0.01 (2-tailed) for all significance tests.
The ES for prospective analyses equals the difference
between means at 2 time points divided by the sample
standard deviation at the earlier time point.
RESULTSValidation Study, Cohort AIn Cohort A, the average age was 62 years (SD ¼ 11)
and 70% were ECOG 0. Locally advanced disease was
present in 58%: 17% Stage I, and 23% M1A. Patients
were treated with surgery alone (Ivor Lewison, 33%),
left thoracoabdominal with a cervical anastomosis
(29%), transhiatal (19%), or McKeown approaches
(19%).
Convergent and divergent validity of the FACT-EThere was good correlation between the PWB, FWB,
EWB subscales of the FACT-E and the corresponding
physical function, role function, and emotional func-
tion scales of the QLQ (Table 1), demonstrating con-
vergent validity. The PWB subscale showed good
correlations with QLQ symptom scales, including fati-
gue, nausea/vomiting, pain, and appetite loss, whereas
the FWB showed good correlations with fatigue, pain,
sleep, and appetite loss.
Demonstrating divergent validity, there was lower
correlation between EWB and the physical and role
function scales of the QLQ as well as many of the phy-
sical symptoms scales of the QLQ (i.e., fatigue, nau-
sea/vomiting, sleep, and constipation). Similarly, there
was lower correlation between the PWB and the QLQ
30 role function scale and between the FWB subscale
and the EORTC QLQ 30 physical function scale.
There was moderate correlation between the
SWB scale and the QLQ social function scale, but
these 2 scales focus on different issues. The former
focuses on sociability and social support, whereas
the latter taps social activity limitations. The SWB
also correlated with the QLQ’s fatigue and physical
function scale.
As expected, the FACT-G total score, an overall
assessment of health status/QOL, correlates highly
with most of the scales of the QLQ.
Esophageal cancer subscaleThe overall ECS score of the FACT-E correlated highly
with all of the multi-item scales of the OES 24 (Table
2). Most importantly, there were especially high cor-
relations between the overall ECS score, the TOI
score, and the eating and swallowing indexes with
the dysphagia and eating items from the OES 24.
These indexes were also highly correlated with the
emotional problems scale of the OES, a scale that
taps perceptions of worry and burden of the illness
and its treatment. There was also good correlation
between overall ECS and TOI with deglutition, gas-
tro-intestinal symptoms, and pain (Table 2). Weak
correlations with the single items, hair loss and dry
mouth, are likely related to the small number of sur-
gical patients who experienced these items.
Reliability of FACT-EInternal consistency of all FACT-E scales was excel-
lent (Table 3). Coefficient a for all FACT-E subscales,
total, and aggregate scores were >0.70 at both base-
TABLE 1Baseline Convergent and Divergent Validity Coefficients (Spearman Correlations)
FACT score
EORTC QLQ C30 scale
PF RF EF CF SF QOL FT NV PN DYS SL AL CO
PWB 0.53 0.47 0.33 0.46 0.55 0.56 �0.58 �0.52 �0.63 �0.13 �0.37 �0.57 �0.34
SWB 0.43 0.37 0.28 0.04 0.47 0.30 �0.60 �0.15 �0.39 �0.02 �0.30 �0.41 �0.23
EWB 0.22 0.17 0.67 0.42 0.36 0.33 �0.22 �0.24 �0.55 �0.04 �0.29 �0.42 0.02
FWB 0.48 0.58 0.58 0.49 0.68 0.63 �0.64 �0.19 �0.54 �0.06 �0.61 �0.39 �0.33
FACT-G 0.50 0.48 0.64 0.47 0.69 0.58 �0.62 �0.28 �0.63 �0.04 �0.49 �0.49 �0.22
EORTC QLQ scales: PF, physical function; RF, role function; EF, emotional function; CF, cognitive function; SF, social function; QOL, global quality of life; FT, fatigue; NV, nausea/vomiting; PN, pain; DYS, dyspnea;
SL, sleep; AL, appetite loss; CO, constipation.
FACT scales: PWB, physical well-being; SWB, social/family well-being; EWB, emotional well-being; FWB, functional well-being; FACT-G, FACT-general.
Validation of the FACT-E/Darling et al. 857

line and follow-up. Both aggregate indexes derived
from eating and swallowing items from the ECS had
very good to excellent internal consistency (a > 0.80).
Test–retest reliability for the FACT-G has been pre-
viously shown to be quite good,9 and therefore, test–
retest reliability for the ECS alone was determined in
this study (3–7-day interval after baseline). Stability
coefficients were excellent for the ECS (0.89), eating
index (0.80), and swallowing index (0.87).
Correlation of FACT-E scores with clinical factorsBaseline FACT-E scale, subscale, and aggregate index
scores were compared across 3 clinical factors: alco-
hol use, weight loss, and pain (Tables 4–6). Patients
with worse baseline clinical features tended to report
worse QOL and more symptoms.
Responsiveness to change of FACT-E in surgical patientsResponsiveness to change was evaluated in Cohort A
by comparing baseline to 3–4 months FACT-E sub-
scale scores. As Table 7 shows, PWB decreased signif-
icantly over the study time interval, a result
consistent with the expectations after major surgery,
whereas EWB scores significantly improved. The
overall ECS score showed very little change over
time, as many patients had almost regained their
baseline level of well-being by 3–4 months after sur-
gery. However, after surgery, patients did report sig-
nificantly more mouth dryness and significantly less
chest pain. Increases in breathing difficulty and
declines in ability to communicate with others,
though not statistically significant, were moderate in
size (ESs � 0.50).
Changes in esophageal-specific concerns asso-
ciated with overall QOL were explored by creating
change scores for the swallowing index, eating index,
and all other ECS items by subtracting baseline score
from follow-up score (Table 8). These were then cor-
related with the follow-up FACT-G total score, con-
trolling for baseline FACT-G total score. As Table 8
shows, in Cohort A, 3 changes in esophageal con-
cerns were significantly associated with overall QOL.
Improvements in eating behavior, communication
with others, and appetite from baseline to follow-up
were associated with better follow-up QOL. Though
not statistically significant, increased mouth dryness
from baseline to follow-up was moderately asso-
ciated with worse follow-up QOL.
TABLE 3Internal Reliabilities at Baseline and 3–4-Month Follow-Up
a at Baseline a at Follow-up
FACT-E scale or subscale
Physical well-being 0.72 0.79
Social well-being 0.83 0.75
Emotional well-being 0.88 0.82
Functional well-being 0.90 0.89
FACT-G total 0.85 0.91
Esophageal Ca subscale 0.89 0.86
Eating index 0.88 0.84
Swallowing index 0.86 0.82
Trial outcomes index 0.91 0.92
FACT-E total 0.87 0.92
QLQ-C30 scale
Physical function 0.70 0.86
Role function 0.90 0.96
Emotional function 0.91 0.84
Cognitive function 0.59 0.53
Social function 0.75 0.91
General health/QOL 0.89 0.92
Fatigue 0.84 0.84
Nausea/vomiting 0.66 0.70
Pain 0.83 0.86
OES-24 scale
Dysphagia 0.80 0.70
Deglutition 0.78 0.13
Eating 0.88 0.88
GI symptoms 0.50 0.64
Esophageal pain 0.66 0.60
Emotional problems 0.71 0.81
TABLE 2Spearman Correlations of FACT-E Esophageal-Specific Scores and EORTC OES 24 Scales at Baseline
FACT score
EORTC OES 24 scale
DYSP DEG EAT GIsx ESPain Emot DM TS CGH TK HL
ECS �0.87 �0.42 �0.84 �0.46 �0.49 �0.65 �0.14 �0.38 �0.33 �0.22 0.06
TOI �0.80 �0.35 �0.76 �0.48 �0.53 �0.78 �0.13 �0.44 �0.35 �0.29 �0.18
Eating �0.80 �0.33 �0.82 �0.45 �0.40 �0.64 .00 �0.44 �0.35 �0.29 �0.18
Swallowing �0.83 �0.52 �0.72 �0.40 �0.38 �0.47 �0.14 �0.31 �0.33 �0.16 0.50
FACT-E �0.71 �0.28 �0.68 �0.41 �0.52 �0.84 �0.07 �0.44 �0.32 �0.59 �0.42
EORTC OES scales: DYSP, dysphagia; DEG, deglutition; EAT, eating; GIsx, gastro-intestinal symptoms; ESPain, esophageal-specific pain; Emot, emotional problems; DM, dry mouth; TS, taste sensation; CHG,
coughing; TK, talking; HL, hair loss.
FACT scale: ECS, esophageal cancer scale; TOI, trial outcome index; eating, eating index; swallowing, swallowing index; FACT-E, FACT-esophageal.
858 CANCER August 15, 2006 / Volume 107 / Number 4

Responsiveness to change in patients having neoadjuvantchemoradiotherapy, Cohort BCohort B consisted of 29 patients (22 male), average
age 58 years, (SD ¼ 11) with clinically staged locally
advanced disease (18 stage III, 9 with M1A disease
and 2 with stage II), treated with neoadjuvant che-
moradiotherapy before surgery. All patients were
ECOG 0-1. The baseline scores before the start of
therapy were compared with the follow-up FACT-E
subscale scores at 7 weeks and 12–14 weeks.
TABLE 4Baseline FACT-E Comparisons: Alcohol Use
Alcohol (Yes/No) n Mean ± SD T(df ) P Effect size
PWB No 23 24.57 6 3.10 2.82(51) 0.007 0.73
Yes 30 20.93 6 5.55
SWB No 23 25.21 6 3.28 1.91(51) 0.061 0.52
Yes 30 22.91 6 5.00
EWB No 23 16.72 6 6.36 1.47(51) 0.147 0.40
Yes 30 14.38 6 5.22
FWB No 23 20.57 6 7.18 1.83(51) 0.073 0.50
Yes 30 17.00 6 6.91
FACT-G No 23 87.06 6 17.19 2.56(50) 0.013 0.68
Yes 29 74.49 6 17.87
ECS No 23 51.85 6 10.36 2.01(50) 0.050 0.55
Yes 29 44.72 6 14.28
TOI No 23 96.98 6 17.68 2.39(50) 0.021 0.64
Yes 29 82.71 6 23.85
Eat. Index No 23 6.65 6 3.81 1.21(50) 0.232 0.34
Yes 29 5.24 6 4.44
Swal. Index No 23 14.86 6 4.21 1.92(50) 0.061 0.53
Yes 29 12.14 6 5.69
FACT-E No 23 138.91 6 24.45 2.70(49) 0.009 0.72
Yes 28 118.52 6 28.55
For abbreviation used, see footnotes to Tables 1 and 2.
TABLE 5Baseline FACT-E Comparisons: Weight Loss
Weight loss n Mean ± SD T(df ) P Effect size
PWB None 15 24.66 6 3.54 2.35(47) 0.023 0.71
Some 34 21.15 6 5.26
SWB None 15 24.53 6 4.55 0.69(47) 0.491 0.22
Some 34 23.54 6 4.62
EWB None 15 17.60 6 4.75 1.93(47) 0.060 0.58
Some 34 14.15 6 6.16
FWB None 15 21.67 6 6.28 2.20(47) 0.033 0.68
Some 34 16.82 6 7.43
FACT-G None 15 88.46 6 16.25 2.37(46) 0.022 0.73
Some 33 75.04 6 19.02
ECS None 15 53.71 6 13.72 2.41(46) 0.020 0.72
Some 33 44.35 6 11.85
TOI None 15 100.03 6 22.07 2.68(46) 0.010 0.80
Some 33 82.38 6 20.78
Eat. Index None 15 8.13 6 3.81 2.84(46) 0.007 0.83
Some 33 4.64 6 4.01
Swal. Index None 15 14.90 6 5.07 1.74(46) 0.089 0.53
Some 33 12.16 6 5.06
FACT-E None 15 142.16 6 28.46 2.76(45) 0.008 0.83
Some 32 118.80 6 26.48
For abbreviation used, see footnotes to Tables 1 and 2.
Validation of the FACT-E/Darling et al. 859

TABLE 6Baseline FACT-E Comparisons: Pain
Pain (Yes/No) n Mean ± SD t(df) P Effect size
PWB No 13 25.60 6 2.87 2.84(52) 0.007 0.85
Yes 41 21.39 6 5.09
SWB No 13 25.23 6 3.26 1.23(52) 0.226 0.39
Yes 41 23.51 6 4.68
EWB No 13 16.43 6 6.86 0.86(52) 0.396 0.27
Yes 41 14.81 6 5.63
FWB No 13 22.69 6 5.22 2.51(52) 0.015 0.76
Yes 41 17.27 6 7.20
FACT-G No 13 89.95 6 14.27 2.39(51) 0.021 0.73
Yes 40 76.50 6 18.55
ECS No 13 56.63 6 10.63 3.05(51) 0.004 0.91
Yes 40 44.88 6 12.45
TOI No 13 104.92 6 15.44 3.29(51) 0.002 0.96
Yes 40 83.60 6 21.59
Eat. Index No 13 7.69 6 4.42 1.93(51) 0.059 0.60
Yes 40 5.18 6 3.97
Swal. Index No 13 16.71 6 4.15 2.91(51) 0.005 0.87
Yes 40 12.21 6 5.03
FACT-E No 39 146.58 6 21.74 3.05(50) 0.004 0.91
Yes 120.95 6 27.47
For abbreviation used, see footnotes to Tables 1 and 2.
TABLE 7FACT-E Scores at Baseline and 3–4-Month Follow-up (Surgery Group—Cohort A)
FACT-E scale, subscale, or item Time point Mean ± SD t(df) P Effect size
Physical well-being Baseline 22.3 6 5.0 t(52) ¼ 2.87 0.006 0.40
3–4 mo 20.3 6 6.0
Functional well-being Baseline 18.5 6 7.2 t(52) ¼ 1.80 0.079 0.29
3–4 mo 16.4 6 7.3
Social well-being Baseline 23.8 6 4.4 t(52) ¼ 1.51 0.136 0.23
3–4 mo 22.8 6 4.9
Emotional well-being Baseline 15.2 6 6.0 t(52) ¼ 3.55 0.001 0.35
3–4 mo 17.3 6 4.8
Esophageal Ca subscale Baseline 47.6 6 13.1 t(51) ¼ 0.07 0.944 0.01
3–4 mo 47.5 6 11.8
Eating index Baseline 5.8 6 4.2 t(51) ¼ 0.46 0.646 0.07
3–4 mo 6.1 6 3.5
Swallowing index Baseline 13.3 6 5.2 t(51) ¼ 1.62 0.111 0.23
3–4 mo 14.5 6 4.5
Dry mouth Baseline 0.6 6 0.9 t(50) ¼ 2.71 0.009 0.56
3–4 mo 1.1 6 1.4
Trouble breathing Baseline 0.3 6 0.6 t(50) ¼ 2.59 0.012 0.67
3–4 mo 0.7 6 1.1
Voice quality Baseline 2.9 6 1.5 t(50) ¼ 0.59 0.556 0.13
3–4 mo 2.7 6 1.4
Communication with others Baseline 3.7 6 0.5 t(51) ¼ 2.30 0.026 0.80
3–4 mo 3.3 6 1.1
Pain in chest Baseline 0.9 6 1.0 t(50) ¼ 4.17 0.000 0.70
3–4 mo 0.2 6 0.6
Good appetite Baseline 2.4 6 1.6 t(51) ¼ 1.50 0.141 0.19
3–4 mo 2.1 6 1.5
Coughing at night Baseline 0.5 6 1.1 t(51) ¼ 1.36 0.180 0.27
3–4 mo 0.8 6 1.1
Pain in stomach Baseline 0.8 6 1.2 t(51) ¼ 2.47 0.017 0.42
3–4 mo 1.3 6 1.4
Weight loss Baseline 1.3 6 1.4 t(49) ¼ 0.97 0.339 0.21
3–4 mo 1.0 6 1.3
860 CANCER August 15, 2006 / Volume 107 / Number 4

As Table 9 shows, PWB and FWB scores declined
significantly from baseline to Week 7, but improved
significantly by Week 12–14. There were no changes
over time in the SWB and EWB scores.
There was a significant improvement in overall
ECS score from Week 7 to Week 12–14 (Table 9).
Swallowing index scores also improved from Week 7
to Week 12–14 after completion of chemoradiother-
apy. Scores for voice quality and appetite substan-
tially declined from baseline to Week 7, but improved
significantly by Week 12–14.
DISCUSSIONThis analysis of the psychometric properties of the
FACT-E supports its use as a patient-reported out-
come measure in esophageal cancer. The FACT-E has
good construct validity (convergence and divergence)
when compared with the EORTC QLQ 30 and OES
24. It has very good to excellent internal consistency
and stability (test–retest) reliability. FACT-E scores
correlated well with several important clinical factors
and were found to be responsive to change in pa-
tients treated with surgery alone and in those treated
with neoadjuvant chemoradiotherapy.
Although health-related quality of life (HRQOL)
has been identified as an important outcome mea-
sure in cancer and other disease states,12 most stu-
dies of esophageal cancer therapy have not evaluated
the effect of treatment on HRQOL. Neoadjuvant che-
moradiotherapy is used frequently, but when the
toxicity, duration, and limited efficacy of neoadjuvant
therapy is considered, its value over esophagectomy
alone has been questioned.11,13–16 The availability of
a valid, self-administered QOL questionnaire for eso-
phageal cancer will allow comparison of the effect of
different treatments on HRQOL as well as survival
and treatment-related toxicities.
The ECS is similar in length (17 items) to the
OES-18, which was developed as a 24-item scale
(OES 24), and subsequently revised to 18 items by
Blazeby.11,17 The ECS is designed to be used with the
FACT-G, which has been validated previously.9 The
FACT-E can generate a summary or individual com-
ponent scores: (e.g., FACT-G total, FACT-E total) and
individual item or subscale scores (e.g., PWB, ECS,
swallowing index). The 4 primary QOL domains of
the FACT-G provide excellent information on the
common elements that comprise QOL, and allows
for domain comparisons across sites.
On the basis of clinical experience and previous
work by Blazeby et al.,18 patients 3–4 months after
esophagectomy have poorer QOL when compared
with baseline. Similarly, Brooks, using the FACT-E,
reported that QOL did not return to baseline until
9 months after esophagectomy. Furthermore, patients
who had preoperative chemoradiotherapy did not
achieve their baseline QOL, even at 9 months.19 In
contrast, our patients in Cohort A, who had surgery
alone had almost fully recovered by 3–4 months
postoperatively, based on both clinical parameters
and overall FACT-E score. Although there was no sig-
nificant change in the overall ECS score, there were
significant changes in individual items, which em-
phasize the importance of considering individual item
data, the eating and swallowing indexes, in addition
to the total ECS score, to maximize the clinical utility
of the FACT-E. If only the overall score is considered,
important information on the individual factors, such
as communication with others, affecting HRQOL will
be missed.
The second phase of the study (Cohort B), which
evaluated the FACT-E in a group of patients having
preoperative chemoradiotherapy wherein data were
collected at more frequent time points, clearly
demonstrates the responsiveness of the FACT-E to
significant clinical changes.
CONCLUSIONSThis prospective, observational cohort study demon-
strates that the FACT-E is a psychometrically sound
instrument. The scale shows good construct validity
when compared with another validated measure of
esophageal cancer. It also has very good to excellent
reliability (internal consistency and stability) and can
differentiate clinically distinct groups of patients. The
FACT-E is responsive to changes in patient status
over the course of standard therapies for esophageal
cancer. These characteristics make the FACT-E an
excellent choice for use in clinical trials of esopha-
geal cancer.
TABLE 8Partial Correlations of ECS Item and Index Change Scores (Baselineto Follow-up) with Follow-up FACT-G Score Controlling forBaseline FACT-G Score (Cohort A)
ECS index or item Correlation P
Swallowing index 0.02 0.901
Eating index 0.42 0.003
Mouth dryness �0.35 0.013
Trouble breathing �0.27 0.060
Strength of voice quality �0.07 0.629
Communication with others 0.53 0.000
Pain in chest on swallowing 0.10 0.476
Good appetite 0.47 0.001
Coughing at night �0.03 0.816
Pain in stomach 0.01 0.926
Weight loss �0.26 0.071
Validation of the FACT-E/Darling et al. 861

REFERENCES1. Parkin DM, Bray FI, Devesa SS. Cancer burden in the year
2000. The global picture. Eur J Cancer. 2001;37:S4–S66.
2. LeRut T, Coosemans W, Decker G, De Leyn P, Nafteux P,
Van Raemdonck D. Cancer of the esophagus and gastro-
esophageal junction: Potentially curative therapies. Surg
Onc. 2001;10:113–122.
3. Visbal Al, Allen MS, Miller DL, Deshcamps C, Trastek VF,
Pairolero PC. Ivor Lewis esophagogastrectomy for esopha-
geal cancer. Ann Thorac Surg. 2001;71:1803–1808.
TABLE 9FACT-E Scores at Baseline, Week 7 and Week 12–14 (Neo-adjuvant Group—Cohort B)
FACT-E scale, subscale, or item Time Point Mean ± SD F(df) P
Effect sizes of
adjacent means
Physical well-being Baseline 23.7 6 4.4 F(2,44) ¼ 21.01* 0.000 0.72, 1.75
7 wk 16.0 6 6.7
12–14 wk 20.8 6 5.3
Functional well-being Baseline 20.0 6 6.0 F(2,44) ¼ 11.25* 0.000 0.31, 0.77
7 wk 15.4 6 5.8
12–14 wk 17.2 6 4.5
Social well-being Baseline 25.4 6 2.4 F(2,44) ¼ 1.15 0.327 0.17, 0.42
7 wk 24.4 6 2.4
12–14 wk 24.8 6 2.3
Emotional well-being Baseline 15.7 6 4.4 F(2,44) ¼ 0.60 0.555 0.09, 0.16
7 wk 16.4 6 4.6
12–14 wk 16.0 6 4.8
Esophageal Ca subscale Baseline 47.1 6 12.3 F(2,44) ¼ 6.36y
0.004 0.20, 0.78
7 wk 44.7 6 10.0
12–14 wk 52.5 6 11.2
Eat. index Baseline 6.1 6 4.1 F(2,44) ¼ 3.57 0.037 0.10, 0.54
7 wk 5.7 6 3.5
12–14 wk 7.6 6 3.7
Swal. index Baseline 11.8 6 4.4 F(2,44) ¼ 11.35y
0.000 0.20, 0.71
7 wk 12.7 6 4.5
12–14 wk 15.9 6 3.4
Dry mouth Baseline 0.9 6 1.1 F(2,42) ¼ 0.12 0.887 0.09, 0.10
7 wk 1.0 6 1.0
12–14 wk 0.9 6 1.0
Trouble breathing Baseline 0.4 6 0.7 F(2,42) ¼ 0.09 0.914 0.13, 0.14
7 wk 0.3 6 0.8
12–14 wk 0.4 6 0.9
Voice quality Baseline 3.4 6 1.0 F(2,44) ¼ 7.61{ 0.001 0.67, 1.10
7 wk 2.3 6 1.2
12–14 wk 3.1 6 1.1
Communication with others Baseline 3.7 6 0.5 F(2,44) ¼ 3.08 0.056 0.25, 0.60
7 wk 3.4 6 0.8
12–14 wk 3.6 6 0.7
Pain in chest Baseline 1.3 6 1.2 F(2,44) ¼ 2.53 0.091 0.00, 0.50
7 wk 1.3 6 1.0
12–14 wk 0.8 6 1.0
Good appetite Baseline 2.8 6 1.2 F(2,44) ¼ 5.41{ 0.008 0.46, 0.75
7 wk 1.9 6 1.3
12–14 wk 2.5 6 1.2
Coughing at night Baseline 0.2 6 0.6 F(2,44) ¼ 0.78 0.463 0.13, 0.33
7 wk 0.4 6 0.8
12–14 wk 0.3 6 0.6
Pain in stomach Baseline 1.0 6 1.3 F(2,44) ¼ 0.69 0.508 0.08, 0.25
7 wk 1.1 6 1.2
12–14 wk 0.8 6 1.2
Weight loss Baseline 1.2 6 1.2 F(2,42) ¼ 0.30 0.745 0.08, 0.08
7 wk 1.1 6 1.2
12–14 wk 1.0 6 1.3
* Baseline > 12–14 wk > 7 wk.y12–14 wk > Baseline, 7 wk.
{ Baseline, 12–14 wk > 7 wk.
862 CANCER August 15, 2006 / Volume 107 / Number 4

4. Swanson SJ, Batirel HF, Bueno R, et al. Transthoracic esopha-
gectomy with radical mediastinal and abdominal lymph
node dissection and cervical esophagsogastrostomy for eso-
phageal carcinoma. Ann Thorac Surg. 2001;72:1918–1925.
5. Hulscher JBF, van Sandick JW, DeBoer AGEM, et al.
Extended transthoracic resection compared with limited
transhiatal resection for adenocarcinoma of the esophagus.
N Engl J Med. 2002;347:1662–1669.
6. Urschel JD, Vasan H, Blewett CJ. A meta-analysis of rando-
mized controlled trials that compared neoadjuvant che-
motherapy and surgery to surgery alone for resectable
esophageal cancer. Am J Surg. 2002;183:274–279.
7. Tamim WZ, Davidson RS, Quinlan RM, O’ Shea MA, Orr RK,
Swanson RS. Neoadjuvant chemoradiotherapy for esopha-
geal cancer: Is it worthwhile? Arch Surg. 1998;133:722–726.
8. Morton RP, Witterick IJ. Rationale and development of a
quality-of-life instrument for head and neck cancer
patients. Am J Otolaryngol. 1995;16:284–293.
9. Cella DF, Tulsky DS, Gray G, et al. The functional assess-
ment of cancer therapy scale: Development and validation
of the general measure. J Clin Oncol. 1993;11:570–579.
10. Aaronson NK, Ahmedzai S, Bergman B, et al. The European
Organization for Research and Treatment of Cancer QLQ-
C30: A quality-of-life instrument for use in international cli-
nical trials in oncology. J Natl Cancer Inst. 1993;85:365–376.
11. Blazeby JM, Alderson D, Winstone K, et al. Development of
an EORTC questionnaire module to be used in quality of
life assessment for patients with oesophageal cancer. Eur J
Cancer. 1996;32A:1912–1917.
12. Kreder HJ, Wright JG, McLeod R. Outcomes studies in sur-
gical research. Surgery. 1997;121:223–225.
13. Orringer MB, Marshall B, Iannettoni MD. Transhiatal eso-
phagectomy: Clinical experience and refinements. Ann
Surg. 1999;230:392–400.
14. van Sandick JW, van Lanschot JJB, ten Kate FJ, Tijssen JG,
Obertop H. Indicators of prognosis after transhiatal eso-
phageal resection without thoracotomy for cancer. J Am
Coll Surg. 2002;194:28–36.
15. Nigro JJ, DeMeester SR, Hagen JA, et al. Node status in
transmural esophageal adenocarcinoma and outcome after
en bloc esophagectomy. J Thorac Cardiovasc Surg. 1999;117:
960–968.
16. Dimick JB, Wainess RM, Upchurch GR Jr, Iannettoni MD,
Orringer MB. National trends in outcomes for esophageal
resection. Ann Thorac Surg. 2005;79:212–216.
17. Blazeby JM, Conroy T, Hammerlid E, et al. Clinical and
psychometric validation of an EORTC questionnaire mod-
ule, the EORTC QLQ-OES18, to assess quality of life in
patients with oesophageal cancer. Eur J Cancer. 2003;39:
1384–1394.
18. Blazeby JM, Farndon JR, Donovan J, Alderson D. A pro-
spective longitudinal study examining the quality of life of
patients with esophageal carcinoma. Cancer. 2000;88:1781–
1787.
19. Brooks JA, Kesler KA, Johnson CS, Ciatta D, Brown JW. Pro-
spective analysis of quality of life after surgical resection
for esophageal cancer: Preliminary results. J Surg Oncol.
2002;81:185–194.
Validation of the FACT-E/Darling et al. 863



















![[Ghiduri][Cancer]Esophageal Cancer](https://img.pdfslide.us/doc/110x75/577cc7761a28aba711a10585/ghiduricanceresophageal-cancer.jpg)