Embed Size (px)
Citation preview

3 The abbreviations used are: BCPT. Breast Cancer Prevention Trial: ERT,
estrogen replacement therapy.
Vol. 7, 591-595, Jul��� 1998 Cancer Epidemiology, Biomarkers & Prevention 591
Validation of a Model Predicting Enrollment Status in a
Chemoprevention Trial for Breast Cancer’
Anita Yeomans Kinney,2 Sally W. Vernon, Wen Shui,Diane V. Weber, Michael Schell, and Victor G. Vogel
The University of North Carolina Lineberger Comprehensive Cancer Center
IA. Y. K.. M. 5.1 and Department of Epidemiology, The University of NorthCarolina School of Public Health IA. Y. K.l, Chapel Hill, North Carolina
27599: Departments of Behavioral Science and Epidemiology. The University
of Texas Health Science Center, Houston. School of Public Health [S. W. VI,
and Departments of Gastrointestinal Oncology [W. S.l and Clinical Cancer
Prevention [D. V. WI, The University of Texas M. D. Anderson Cancer
Center, Houston, Texas 77030; and The University of Pittsburgh Cancer
Institute, Pittsburgh. Pennsylvania 15213 IV. G. V.1
Abstract
We evaluated the performance of a regression model inpredicting enrollment status in a chemoprevention trialfor breast cancer using a population independent of thatfrom which the model was derived. In years 1 and 2 ofrecruitment, questionnaires were completed by eligibleparticipants following attendance at informationalmeetings about the Breast Cancer Prevention Trial. Thevariables in the original model, based on womenrecruited in year 1, included not being able to takeestrogen replacement therapy (ERT), concern about theside effects of tamoxifen, the possibility of getting aplacebo, the out-of-pocket expenses associated with thetrial, and disagreement with the statement “significantothers would be reassured if the respondent was taking
tamoxifen.” These variables were used to predictenrollment status of women newly recruited to the trial inyear 2. Among the 89 women in the study populationwho responded to the questionnaire, 66% did not enrollin the trial. By applying the original logistic regressionmodel, enrollment status in the trial was correctlypredicted for 72% of year 2 questionnaire respondents.Age and risk scores, as binary variables, were used in aderived logistic model to determine whether theyprovided additional predictive information on enrollmentstatus. The resulting four-factor model, which predictednonenroliment, included: age of �50 years, not being ableto take ERT, expressed concern that significant otherswould not be reassured if the respondent was taking
tamoxifen, and concern about out-of-pocket expensesassociated with the trial. This model correctly classified76% of the respondents. The logistic regression models
Received 7/14/97; revised 3/1 2/98; accepted 4/7/98.
I This research was supported. in part, by an American Cancer Society doctoralscholarship (to A. Y. K.) and a National Cancer Institute postdoctoral fellowship
in cancer prevention and control at the University of North Carolina Lineberger
Comprehensive Cancer Center and the Department of Epidemiology. University
of North Carolina School of Public Health, Chapel Hill. NC (CA 57726; to
A. Y. K.).
2 To whom requests for reprints should be addressed. at University of Utah,
College of Nursing, 10 South 2000 East Front. Salt Lake City. UT 841 12-5880.
performed reasonably well in predicting enrollmentstatus. Not being able to take ERT remained thestrongest factor predicting nonenrollment. More researchis needed to evaluate factors that motivate persons toseek participation in primary chemoprevention trials inculturally diverse populations.
Introduction
The importance of the recruitment phase in clinical trials is
widely recognized ( I,2). Recruitment is critical to the validity
of a trial’s results. Participation in chemoprevention trials is arelatively new area of research that warrants additional atten-
tion and much additional data (3). Chemoprevention trials mustenlist large numbers of participants. Recruitment to chemopre-vention trials may be particularly difficult because subjects are
often healthy and may be required to participate for many years.Failure to recruit a sufficient number of individuals can corn-promise statistical power, and biased recruitment may jeopard-
ize the generalizability of a trial’s results. Investigation offactors influencing trial participation may be used to designinterventions to enhance recruitment, evaluate the effects ofselection biases on the generalizability of the trial’s results, anddesign future trials that are acceptable to the target population.
To our knowledge, there is only one prospective report offactors related to enrollment in a breast cancer chemopreven-
tion trial (4). We recently performed a multivariate analysisusing data from one comprehensive cancer center to predict
enrollment in the BCPT3 at that site (4). The BCPT is alarge-scale randomized primary chemoprevention trial de-
signed to evaluate the efficacy of tamoxifen for prevention ofbreast cancer in women who have not yet developed the disease
(5, 6). Healthy women 60 years of age and older are eligible toparticipate in the trial. Women between 35 and 59 years areeligible if their 5-year risk of breast cancer, based on the modeldescribed by Gail et a!. (7-9), is equivalent to or greater than
that of a typical 60-year old woman. Reasons for exclusion are
pregnancy or intent to become pregnant, use of exogenousestrogen, past use of tamoxifen, a history of ductal carcinomain situ, and a history of invasive breast cancer.
A model for predicting enrollment status was developedusing women recruited to the BCPT at a large comprehensive
cancer center during year 1 of the trial (4). Five factors pre-dicted nonenrollment: concern about not being able to takeERT, concern about the side effects of tamoxifen, the possibil-ity of getting a placebo, the out-of-pocket expenses associatedwith trial participation, and significant others not being reas-sured if the respondent was taking tamoxifen. The derivedlogistic regression model correctly classified 79% of the non-participants and 78% of the participants. Assuming, as was
on April 3, 2019. © 1998 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

592 Validation of a Model Predicting Enrollment Status in the BCPT
observed, that approximately half of all eligible subjects will
not enroll in the BCPT, the positive predictive value of themodel is 75%. These estimates, however, may be optimisticbecause they were based on the same data that were used to fitthe model. In the current study, we validated this model usingan independent data set.
Materials and Methods
One hundred seventy-five women completed risk assessmentforms at our BCPT site and were considered potentially eligiblefor the BCPT at the beginning of year 2; 148 women attended
an informational meeting. The study population consisted ofwomen who attended an informational meeting during recruit-ment in year 2 and who completed a psychosocial questionnairewith questions based on the Health Belief Model (10) and theTheory of Reasoned Action (I I). Briefly, the questionnaire
assessed respondents’ beliefs about breast cancer, perceivedsusceptibility to breast cancer, barriers and benefits related to
the BCPT, normative influences, and health behaviors. A moredetailed description of the 90-item questionnaire and format ofthe informational meetings has been published previously (4,I 2). All women were asked to complete the questionnaire after
the meeting and to return it in a prepaid envelope. Women who
did not return the questionnaire within 8-10 weeks were sentanother copy, a prepaid envelope, and a cover letter from theprincipal investigator requesting their cooperation. One hun-dred seventeen women completed and returned the question-naire; 89 were white, 12 were African-American, 10 were
Hispanic, I was Asian or Pacific Islander, 3 were NativeAmerican or Alaskan Islander, and 2 were “other” racial/ethnic
origin. The analysis was restricted to 89 white women becausethe original model included only white women.
Data were analyzed using the Statistical Program for theSocial Sciences (13) and STATA (14). Standard x� and Fisher
exact tests were used for the binary and categorical variables,and Student’s t test was used for the continuous variables in the
univariate analysis. Here, the variables identified as importantpredictors of nonenrollment in year 1 were included in thelogistic regression procedures to predict nonenrollment in year2. Because women recruited in year 2 were significantly older
and had higher Gail risk scores (7) than women recruited inyear I and because age and risk factor profile might affect thedecision-making process, a second model was computed usingyear 2 data, incorporating age (<50 years versus �50 years)and Gail risk score (<4.0 versus �4.0) as binary variables.Factors that did not contribute significantly to the classificationof enrollment status in the presence of other factors were
eliminated from the model by means of backward stepwisevariable selection using likelihood ratio tests (15). The resulting
logistic regression model was then used to classify respondents
according to their enrollment status.Here, prediction and classification are distinguished by the
data set on which the model is applied. Prediction refers to theapplication of the model derived in year 1 (model I) to anindependent data set (year 2 enrollment data) that was not usedfor model derivation. Classification refers to use of the model
to partition women from the same data set from which themodel was derived (model II). The number of correct predic-
tions or classifications for respondents with a particular riskfactor configuration (i.e. , a set of numerical values for the fivevariables in the model) was calculated and is the number ofagreements between the observed outcomes and the model-expected outcomes. The number of correct predictions or clas-sifications was obtained by summing the number of agreements
over all risk factor configurations. Regression diagnostics (16)were performed for both models to test for potential outliers orinfluential observations. Because there were no highly influen-
tial observations, the analyses for model I, year 2 and model II
were performed using all of the respondents.
Results
Comparison of Year 1 and Year 2 Study Populations.Among the 89 women in the study population, 66% did not
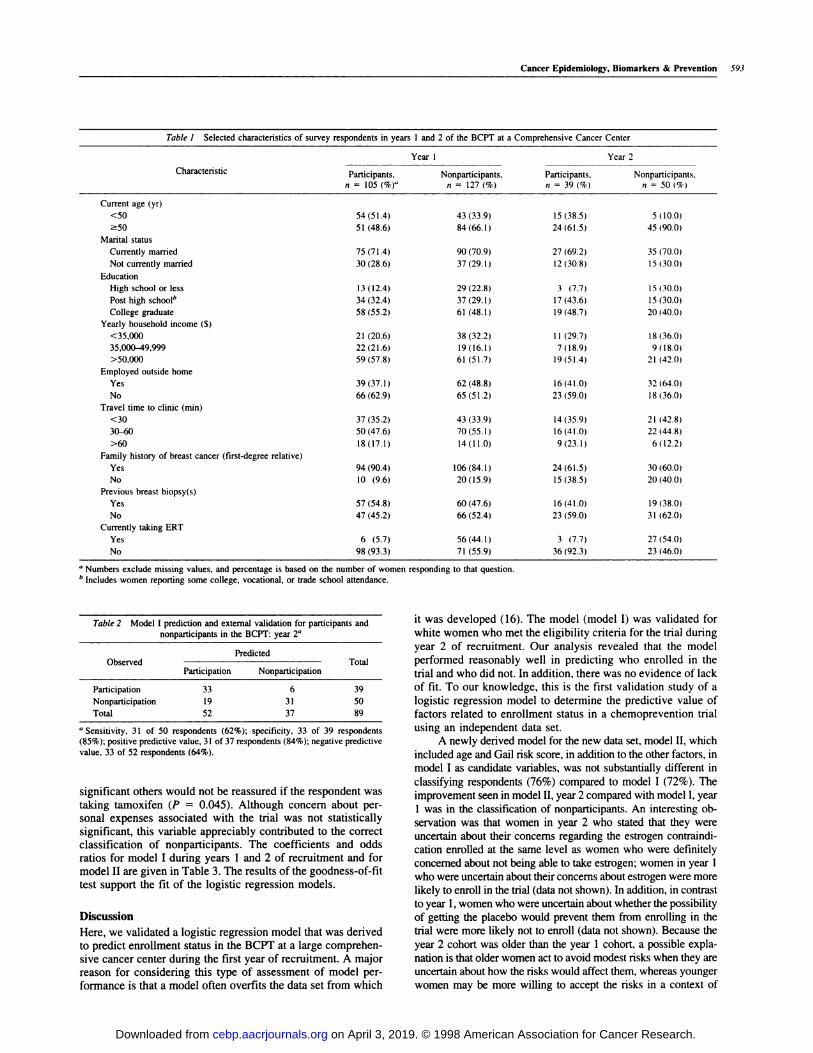
enroll in the trial, compared with 55% in year 1. Table 1compares selected characteristics of women who did and didnot enroll in the trial in year 1 compared with year 2. In general,
the characteristics of women who enrolled in the trial weresimilar in years I and 2. The respondents in year 2 were similar
to the respondents in year 1 with respect to their responses toquestions about their perceived benefits, perceived barriers,
perceived breast cancer risk, normative influences, and self-reported health and cancer-screening behaviors. For example,-90% of the women recruited in both years 1 and 2 reportedthat they were somewhat or very likely to develop breastcancer. Similarly, -90% of women recruited in years 1 and 2reported that tamoxifen was somewhat or very likely to reduce
their breast cancer risk. Women recruited in year 2 were older
than women recruited in year 1 (mean ages = 59 versus 53years, respectively; P < 0.001). The average Gail model breastcancer risk score (7) was 14 during year 1 but only 4 duringyear 2 (P < 0.001). Additionally, fewer women recruited inyear 2 reported ever having a breast biopsy (39%) than womenrecruited in year 1 (50%). Furthermore, 86% of the womenrecruited in year 1 had at least one first-degree relative with
breast cancer, compared to 61 % of the women recruited in year2. As in year 1, more participants than nonparticipants in year2 reported that their concern about perceived barriers would
prevent them from enrolling in the trial. In both years 1 and 2,
participants were more likely to express concern that significantothers would not be reassured if the respondent was takingtamoxifen, compared with nonparticipants.
Model Validation. Application of model I to the participantswho responded to the questionnaire in year 2 resulted in correctprediction of 64 of 89 respondents (72%). The results of modelI prediction and external validation are given in Table 2. Thelogistic model correctly predicted 62% of the nonparticipants
and 85% of the participants. The positive predictive value of themodel was 84%. The range of values of the confidence intervals
for the variables used in the model derived in year 1 areconsistent with the point estimates in the validation model
(model I, year 2), with the exception of the variable tamoxifenside effects (Table 3).
The variables that were considered for a derived maineffects model (model II) included the five variables in model Iplus age and Gail model risk score (Table 3). For this model,the ERT barrier was dichotomized as no concern versus definiteor uncertain concern because of similar effects on outcome andsmall cell size. Overall, model II correctly classified 76% of thewomen, including 72% of the nonparticipants and 82% of theparticipants (Table 4). Only four of the seven factors considered
for model II substantially contributed to the classification en-rollment status. The possibility of getting a placebo and concernabout the side effects of tamoxifen did not substantially con-tribute to the classification of enrollment status; therefore, thevariables were not included in the derived model (model II).Three of the variables in model II were significantly associatedwith nonenrollment: concern about not being able to take ERT
(P = 0.001), age of �50 years (P = 0.014), and concern that
on April 3, 2019. © 1998 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Cancer Epidemiology, Biomarkers & Prevention 593
Table 1 Selected characteristics of surve y respondents in year s I and 2 of the BCPT at a Co mprehensive Cance r Center
Characteristic
Yearl Year2
Participants, Nonparticipants, Participants. Nonparticipants.n 105 (%)“ n 127 (%) n = 39 (%) n 50 (%)
Current age (yr)
<50 54(51.4) 43 (33.9) 15 (38.5) 5 (10.0)
�50 51 (48.6) 84(66.1) 24 (61.5) 45 (90.0)
Marital status
Currently married 75 (71.4) 90(70.9) 27 (69.2) 35 (70.0)
Not currently married 30 (28.6) 37 (29.1) 12 (30.8) 15 (30.0)
Education
High school or less 13 (12.4) 29 (22.8) 3 (7.7 15 (30.0)
Post high school” 34 (32.4) 37 (29.1) 17 (43.6) 15 (30.0)
College graduate 58 (55.2) 61 (48.1) 19 (48.7) 20(40.0)
Yearly household income ($)
<35,000 21 (20.6) 38 (32.2) 1 1 (29.7) 18 (36.0)
35,000-49,999 22(21.6) 19(16.1) 7(18.9) 9(18.0)
>50,000 59(57.8) 61 (51.7) 19(51.4) 21 (42.0)
Employed outside home
Yes 39 (37.1) 62 (48.8) 16 (41.0) 32 (64.0)
No 66 (62.9) 65 (51.2) 23 (59.0) 18 (36.0)
Travel time to clinic (mm)
<30 37 (35.2) 43 (33.9) 14 (35.9) 21 (42.8)
30-60 50(47.6) 70(55.1) 16(41.0) 22(44.8)
>60 18(17.1) 14(11.0) 9(23.1) 6(12.2)
Family history of breast cancer (first-degree relative)
Yes 94(90.4) 106(84.1) 24(61.5) 30 (60.0)
No 10 (9.6) 20(15.9) 15(38.5) 20(40.0)
Previous breast biopsy(s)
Yes 57(54.8) 60(47.6) 16(41.0) 19(38.0)
No 47 (45.2) 66 (52.4) 23 (59.0) 31 (62.0)
Currently taking ERT
Yes 6 (5.7) 56 (44.1) 3 (7.7) 27 (54.0)
No 98 (93.3) 71 (55.9) 36 (92.3) 23 (46.0)
“ Numbers exclude missing values, and percentage is based on the number of women responding to that question.b Includes women reporting some college, vocational, or trade school attendance.
Table 2 Model I p
no
rediction and external validation for particip
nparticipants in the BCPT: year 2#{176}
ants and
ObservedPredicted
TotalParticipation Nonparticipation
Participation
Nonparticipation
Total
33 6
19 31
52 37
39
50
89
#{176}Sensitivity, 31 of 50 respondents (62%); specificity, 33 of 39 respondents
(85%); positive predictive value, 3 1 of 37 respondents (84%); negative predictive
value, 33 of 52 respondents (64%).
significant others would not be reassured if the respondent wastaking tamoxifen (P = 0.045). Although concern about per-sonal expenses associated with the trial was not statistically
significant, this variable appreciably contributed to the correctclassification of nonparticipants. The coefficients and oddsratios for model I during years 1 and 2 of recruitment and formodel II are given in Table 3. The results of the goodness-of-fit
test support the fit of the logistic regression models.
Discussion
Here, we validated a logistic regression model that was derivedto predict enrollment status in the BCPT at a large comprehen-
sive cancer center during the first year of recruitment. A majorreason for considering this type of assessment of model per-formance is that a model often overfits the data set from which
it was developed (16). The model (model I) was validated for
white women who met the eligibility criteria for the trial during
year 2 of recruitment. Our analysis revealed that the model
performed reasonably well in predicting who enrolled in the
trial and who did not. In addition, there was no evidence of lack
of fit. To our knowledge, this is the first validation study of a
logistic regression model to determine the predictive value of
factors related to enrollment status in a chemoprevention trialusing an independent data set.
A newly derived model for the new data set, model II, whichincluded age and Gail risk score, in addition to the other factors, inmodel I as candidate variables, was not substantially different in
classifying respondents (76%) compared to model I (72%). The
improvement seen in model II, year 2 compared with model I, year1 was in the classification of nonparticipants. An interesting ob-
servation was that women in year 2 who stated that they wereuncertain about their concerns regarding the estrogen contraindi-
cation enrolled at the same level as women who were definitely
concerned about not being able to take estrogen; women in year 1who were uncertain about their concerns about estrogen were more
likely to enroll in the trial (data not shown). In addition, in contrastto year 1, women who were uncertain about whether the possibilityof getting the placebo would prevent them from enrolling in thetrial were more likely not to enroll (data not shown). Because the
year 2 cohort was older than the year 1 cohort, a possible expla-
nation is that older women act to avoid modest risks when they areuncertain about how the risks would affect them, whereas younger
women may be more willing to accept the risks in a context of
on April 3, 2019. © 1998 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

594 Validation of a Model Predicting Enrollment Status in the BCPT
4 J. Costantino, personal communication.
Table 3 Cocfficient s and statistical tests for the two 1ogistic regression models”
VariableModel I, year 1 (n = 232) Model I. year 2 (n = 89) Model II, year 2 (n = 89)
Odds ratio 95% Cl5 Odds ratio 95% CI Odds ratio 95% CI
ERT contraindicated
No concem 1.0
Uncertain or no concem 1.0 1.0
Definite concern 12.1 3.6-40.6 7.5 0.7-82.1
Uncertain or definite concern 14.9 2.9-75.3
Tamoxifen side effects
Uncertain or no concern 1 .0 1.0
Definite concern 5.1 2.4-10.8 1.6 0.2-11.3
Possibility of placebo
No concern 1 .0 1.0
Uncertain concern 1.1 0.4-3.4 1.9 0.3-12.7
Definite concern 7.8 1.5-39.7 3.8 0.3-44.1
Personal expenses
No concern 1.0 1.0 1.0
Uncertain concem 0.9 0.3-2.6 2.4 0.5-I 1.8 2.9 0.6-15.5
Definite concern 3.2 1.1-9.2 1.4 0.4-4.7 2.3 0.6-9.0
Significant others not reassured if respondent on tamoxifen
Uncertain or no concem 1.0 1.0 1.0 1.0 1.0
Definite concern 2.6 1.0-6.4 3.0 0.5-17.7 8.9 1.1-75.1
Age (yr)
<50 1.0
�50 6.3 1.5-27.0Tests of lit’
�2 4.07 5.99 9.34
Degrees of freedom 8 8 8
P 0.85 0.64 0.31
“ Dependent variable was coded 0 for enrollment and 1 for nonenrollment.
S CI. confidence interval.‘ Hosmer-Lemeshow goodness-of-fit statistic; P > 0.05 indicates that the model fits the data.
Table 4 Model II cI assification of BCPT participants and nonp
year 2”articipants:
ObservedClassified
TotalParticipation Nonparticipation
Participation 32 7 39
Nonparticipation 14 36 50
Total 46 43 89
‘, Sensitivity. 36 of 50 respondents (72%); specificity, 32 of 39 (82%); positivepredictive value, 36 of43 respondents (84%); negative predictive value, 32 of 46
respondents (70%).
uncertainty. It would have been informative to evaluate model Ivariables in younger women (<50 years) and older women (�50
years) separately to obtain an adequate estimate of the effects of
the interaction of age; however, the sample size was a limitingfactor.
The average age of respondents in year 2 was greater thanthat in year 1 . The respondents recruited in years 1 and 2 also
differed with respect to risk score, which is partly due todifferences in family history of breast cancer and to ever having
had a breast biopsy. Nationally, 69% of the women who sub-mitted risk assessment forms to the trial were eligible to enroll,and their average relative risk assessed by the Gail model was
4.2 during year I of the BCPT. During the last year of enroll-ment the proportion eligible had fallen to 50%, and their aver-age relative risk had fallen to 34,4 No information has been
published about the variability of specific risk factors among
participants enrolled during different time periods in the trial. Itis possible that women who had more anxiety about their
perceived risk of breast cancer (i.e. ,especially younger womenwith more affected first-degree relatives) self-selected them-selves during the early enrollment period. Women who soughtinformation about the trial during year 2 at our cancer center
had only moderately elevated risks, on average, compared towomen who sought information about the trial in year 1 . Theymay have had lower levels of anxiety about their chances of
developing breast cancer. If the pool of potential individualsconsidering enrollment changes over the course of a prevention
trial, models established for early candidates may not apply tolater candidates. At our cancer center, however, although therespondents in year 1 and year 2 differed somewhat, we wereable to validate the logistic regression model.
Our previous finding that the ERT contraindication wasthe most important predictor of nonparticipation was supported
in this study (4). This finding is critical because it may help in
the design of future chemoprevention trials and programs forbreast cancer, especially because, in general: older women areat higher risk for the disease than are younger women, andestrogen replacement may be important to some postmeno-
pausal women for a variety of reasons. It is important tounderstand the major reasons why women take ERT andwhether or not these reasons affect the decision to participate in
a chemoprevention trial for breast cancer in which ERT iscontraindicated. Previous research has shown that a majority ofwomen decide to take ERT because they place greater weight
on the quality of life benefits (e.g., reduction of hot flashes,
vaginal dryness, and dyspareunia and improvement in mood
state) and place less weight on the longer-term benefits (reduc-
on April 3, 2019. © 1998 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

Cancer Epidemiology, Biomarkers & Prevention 595
tion in mortality; Ref. 17). The results of our study suggest that,for the majority of women who were taking or planning to take
estrogen in the near future, the perceived benefits of estrogen
outweighed the perceived benefits of enrolling in a breast
cancer prevention trial that precludes the use of estrogen. Fur-thermore, there is some support for the observation that havinga 50% probability of getting a placebo may be a negative factorin the decision to enroll on the BCPT among estrogen users.However, for some women, the perceived benefits of taking
tamoxifen may outweigh the benefits of taking ERT, but other
barriers to participation (e.g., lack of support of significantothers, the possibility of getting a placebo, and concern about
side effects or personal expenses) tilts the scale in favor oftaking estrogen. Research that is designed to identify and sys-
tematically assess the factors that affect these judgments is
needed.Bias affecting the generalizability of the study population
of a chemoprevention trial can occur at multiple phases of thetrial. Research is needed of sources of bias that may occurduring recruitment, enrollment, run-in periods, and postran-
domization (e.g., differential attrition and pill adherence rates).This study has several limitations. The generalizability is
limited by the exclusion of nonwhite women and by the un-
derrepresentation of women from lower socioeconomic groups.In addition, our study population consisted of women at oneBCPT site, a large comprehensive cancer center, thereby lim-
iting the generalizability of the findings. Moreover, there is a
possibility that women who did not attend one of the informa-
tion sessions or did not respond to the questionnaire weredifferent from those who attended one of the meetings or who
completed the questionnaire.
Conclusion. Our model performed well in predicting enroll-ment status in a chemoprevention trial for breast cancer. We
observed that application of the original logistic regressionmodel to an independent data set was predictive of enrollment
status in the trial, although the characteristics of the studypopulations differed somewhat. Not being able to take estrogenwas the dominant predictor of nonparticipation in all of the
analyses. Following an information session about the trial,
younger women were more likely to enroll in the trial than older
women. The influential role of significant others in motivatingwomen to participate in cancer prevention trials was supported.Effective recruitment strategies may differ, depending on the
characteristics of the people being targeted for recruitment.Future research should explore the effects of age and othersociodemographic variables on behavioral factors influencingthe decision to enroll in chemoprevention trials. In addition, we
suggest that measures of anxiety about breast cancer risk andpersonality characteristics be studied in relation to enrollment
in chemoprevention trials. More in-depth studies are needed to
increase our understanding of the complexities of recruiting
individuals to chemoprevention trials.
References
1. Spilker. B. C., and Cramer, J. A. Patient Recruitment in Clinical Trials. New
York: Raven Press, 1992.
2. Hunninghake, D. B., Darby, C. A., and Probstfield, J. L. Recruitment expc-
rience in clinical trials: literature summary and annotated bibliography. Con-
trolled Clin. Trials, 8 (Suppl.): 6S-30S. 1987.
3. Office of Research on Women’s Health, In Recruitment, and Retention of
Women in Clinical Studies, NIH PubI. No. 95-3756. Bethesda, MD: NIH. 1995.
4. Yeomans-Kinney. A., Vernon, S. W., Frankowski, R. F., Weher. D. M.,
Bitsura, J. M., and Vogel, V. G. Factors related to enrollment in the breast cancer
prevention trial at a comprehensive cancer center during the first year of recruit-
ment. Cancer (Phila.), 76: 46-56, 1995.
5. Bush, T. L.. and Helzlsouer. K. J. Tamoxifen for the primary prevention of
breast cancer: a review and critique of the concept and trial. Epidemiol. Rev., 15:
233-243, 1993.
6. Love, R. R. The National Surgical Adjuvant Breast Project (NSABP) Breast
Cancer Prevention Trial revisited. Cancer Epidemiol. Biomark. Prey.. 2: 403-407, 1993.
7. Gail, M. H., Brinton, L. A., Byar, D. P., Corle, D. K., Green, S. B., Schairer,
C., and Mulvihill, J. J. Projected individual probabilities of developing breastcancer for white females who are being examined annually. J. NatI. Cancer Inst.
(Bethesda), 8/: 1879-1886, 1989.
8. Spiegelman, D., Colditz, G. A., Hunter, D., and Hert.zmark, E. Validation of
the Gail et al. model for predicting individual breast cancer risk. J. NatI. Cancer
Inst. (Bethesda), 86: 600-607, 1994.
9. Bondy, M. L., Lustbader, E. D., Halabi, S., Ross, E., and Vogel. V. G.
Validation of a breast cancer risk assessment model in women with a positive
family history. J. NatI. Cancer Inst. (Bethesda), 86: 620-625, 1994.
10. Rosenstock, I. M., Strecher, V. J., and Becker, M. H. Social learning theoryand the Health Belief Model. Health Educ. Q.. 15: 175-183, 1988.
1 1 . Fishbein, M., and Ajzen, I. Belief, Attitude, Intention, and Behavior. Boston:
Addison-Welsey, 1975.
12. Hudmon, K. S., and Kinney, A. Y. Issues of enrollment bias in cancer
chemoprevention trials. Cancer Bull.. 47: 339-342, 1995.
I 3. SPSS Inc. SPSS for Windows: Advanced Statistics, Release No. 6. 1. Chi-
cago: SPSS Inc., 1994.
14. StataCorp. Stata Statistical Software, Release 4.0. College Station, TX:
StataCorp., 1995.
15. Kleinbaum, D. G., Kupper, L. L., and Morgenstern, H. Epidemiologic Re-
search: Principles and Quantitative Methods. New York: Van Nostrand Reinh-
hold, 1987.
16. Hosmer, D. W.. and Lemeshow, S. Applied Logistic Regression. New York:
John Wiley & Sons, 1989.
17. Rothert, M., Rovner, D. Holmes, M., Schmitt, N., Talarczyk, G.. Kroll, J., and
Gogate, J. Women’s use of information regarding hormone replacement therapy.
Res. Nurs. Health, 13: 355-366, 1990.
on April 3, 2019. © 1998 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

1998;7:591-595. Cancer Epidemiol Biomarkers Prev A Yeomans Kinney, S W Vernon, W Shui, et al. chemoprevention trial for breast cancer.Validation of a model predicting enrollment status in a
Updated version
http://cebp.aacrjournals.org/content/7/7/591
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cebp.aacrjournals.org/content/7/7/591To request permission to re-use all or part of this article, use this link
on April 3, 2019. © 1998 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from





























