-
8/12/2019 Vago Thomas
1/29
VagotomyThomas Kristianto
-
8/12/2019 Vago Thomas
2/29
Background
Vagotomy is the surgical cuttingfrom the vagus nerve to lessen
acid
secretion within the stomach.
Vagotomy is an essential component of
surgical management of peptic (duodenal
and gastric) ulcer disease (PUD)
-
8/12/2019 Vago Thomas
3/29
The basic types of vagotomy are as follows:
Truncal vagotomy(TV)
Selective vagotomy(SV)
Highly selective vagotomy(HSV)
All types of vagotomy can be performed at
open surgery (laparotomy) or using minimally
invasive surgery (laparoscopy). A vagotomy isconducted under
general anesthesia.
-
8/12/2019 Vago Thomas
4/29
-
8/12/2019 Vago Thomas
5/29
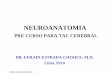
Zeman, M. et al., Speciln chirurgie, ISBN 80-7262-260-9,
2004
Vagotomy
-
8/12/2019 Vago Thomas
6/29
Truncal vagotomy (TV):
This procedure includes
division of the main trunk
of the vagus (including itsceliac/hepatic branch) and
denervation of the
pylorus;therefore, a
pyloric drainageprocedure, such as pyloric
dilatation or disruption
(pyloromyotomy or
pyloroplasty) or
gastrojejunostomy (GJ), is
needed. This procedure
also denervates the liver,
biliary tree, pancreas, and
small and large bowel.
Selective vagotomy (SV):
This procedure includes
division of the anterior and
posterior gastric nerves ofLatarjet only (after
celiac/hepatic branches have
been given off). It also
denervates the pylorus and,therefore, a pyloric drainage
procedure is needed. It does
not denervate the liver,
biliary tree, pancreas, or
small and large bowel. This
procedure is rarely
performed.
-
8/12/2019 Vago Thomas
7/29
Highly selective vagotomy (HSV):
This procedure includes denervation of only the
fundus and body (parietal cell containing areas) of
the stomach (also called parietal cell vagotomy[PCV]). It
preserves the nerve supply of the
antrum and pylorus; a pyloric drainage procedure
is not needed. It does not denervate the liver,
biliary tree, pancreas, or small and large bowel.
This procedure is also called proximal gastric
vagotomy (PGV).
-
8/12/2019 Vago Thomas
8/29
-
8/12/2019 Vago Thomas
9/29
Indication
Vagotomy is indicated as management of peptic ulcerdisease (PUD)
in the following cases:
Elective - Failure of medical treatment (with the availability
of
effective acid suppression with H2-receptor antagonists
andproton pump inhibitors, however, this indication has
virtually
become nonexistent
Semi-elective- Pyloric stenosis (obstruction) due to PUD
Emergency - Upper GI bleeding due to PUD or stress gastriculcers
(erosive gastric mucosal disease) or perforated PUD that is
causing peritonitis
Incidental vagotomy - An inadvertent vagotomy performed
during esophagectomy
-
8/12/2019 Vago Thomas
10/29
Anatomy Arterial blood supply
Lymphatic drainage Nerve supply
-
8/12/2019 Vago Thomas
11/29
Anatomy and physiology
The duodenum connects the stomach to the
jejunum, which is the second part of the
small bowel
-
8/12/2019 Vago Thomas
12/29
It is 20 cm (8 inches) in length and divided into four parts
The duodenum is retroperitoneal (has peritoneum, the thin
layerof tissue that lines the abdominal cavity) only on the
anterior
(front) side; fixed in location; wraps around the head, neck
and
body of the pancreas; and the superior mesenteric artery and
vein
(major blood vessels for the bowel) pass anterior to the 3rd
portion
The ampulla of Vater (entrance site into duodenum of joined
common bile duct and pancreatic duct) enters the medial
(towards the midline) side of the 2nd portion of the
duodenum
The accessory pancreatic duct enters slightly higher in the
medial
wall of the duodenum
-
8/12/2019 Vago Thomas
13/29
The ligament of Treitz (a supporting band
of peritoneum and muscle fibers) marks the
point between the duodenum and jejunumThe wall of the small
bowel (Figure 2) is
made up of four layers:
-
8/12/2019 Vago Thomas
14/29
The mucosa is the inner most layer and composed of
small fingerlike projections (villi) covered with a single
layer of cells (epithelium). Beneath the epithelium is athin
layer of connective tissue (lamina propria) and
muscle (muscularis mucosa)
The submucosa is a thin strong layer containing
connective tissue, vessels, nerves and lymphatics
The muscularis propria is composed of smooth muscle
that has a thicker circular inner layer and thin outer
layer that runs lengthwise
The serosa is the single cell thick outer layer similar to
the peritoneum (visceral peritoneum)
-
8/12/2019 Vago Thomas
15/29
The duodenum produces many hormones that help
regulate digestion. Liver bile and pancreaticsecretions are
added to the bowel through the
ampulla of Vater. The actual passage and presence
of food in the duodenum starts the flow of
hormones, bile and pancreatic secretions. By thetime food leaves
the duodenum most of the
ingredients necessary for digestion have been
added. Little digestion and absorption (passage of
nutrients from the bowel into the blood) take place
in the duodenum.
-
8/12/2019 Vago Thomas
16/29
Preparation
A blood transfusion may be needed for patients with ableeding
peptic ulcer.
Resuscitation, fluid and electrolyte imbalance correction,
and antibiotics should be administered, as needed, in
patients with perforated peptic ulcer. Patients with pyloric
stenosis due to peptic ulcer have
dehydration, alkalosis, and hypokalemia, which need
correction with normal saline and potassium chloride.
Gastric aspiration and lavage is required to decompress the
dilated stomach.
A nasogastric tube allows easier intraoperative
identification (palpation) of the esophagus.
-
8/12/2019 Vago Thomas
17/29
potitioning
The patient is placed in the supine position;
a slight reverse Trendelenburg (head up)
may be used in order to displace theintestines caudad.
The patient is placed in a right lateral (left
up) for the thoracic approach.
-
8/12/2019 Vago Thomas
18/29
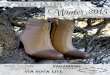
Highly selective vagotomy
Highly selective parietal cell vagotomy (division of the
fibers of the vagus nerve that go to the body of the
stomach) This interrupts acid secretion of the stomach.
The anterior and posterior
vagus nerves are seen lying
on the stomach
The branches of the vagus
nerves going to the
stomach are cut to givethe selective vagotomy
-
8/12/2019 Vago Thomas
19/29
The main vagal trunks are dissected and looped as
described above.
The hepatic branch of the anterior vagus and celiac branch
of the posterior vagus are identified and carefully
preserved; the anterior and posterior gastric nerves ofLatarjet
(which lie about 1-2 cm from the lesser curve) are
also identified and carefully preserved.
The greater curvature of the stomach is retracted
downward and to the left. The anterior layer of the lesser
(gastrohepatic) omentum is
incised close to the lesser curve, taking care not to injure
the vascular arcade formed by the left and right gastric
vessels and the anterior gastric nerve of Latarjet.
-
8/12/2019 Vago Thomas
20/29
Branches of nerves and vessels (which travel together) going
toward
the stomach wall are ligated and divided in bits and pieces
proximal
to the cardia to the incisura angularis (which lies on the
lesser curve
about 6-7 cm proximal to the pylorus), taking care to identify
andpreserve at least 3 terminal branches (crow foot) of the
anterior
gastric nerve of Latarjet, which supply the antrum and the
pylorus.
This dissection is kept as close to the stomach as possible.
The greater (gastrocolic) omentum is divided 1-2 cm from the
greater curve, taking care not to injure the vascular arcade
formedby the left and right gastroepiploic vessels, and the lesser
sac
(behind the stomach and in front of the pancreas) is
entered.
The stomach is turned upward and to the right, and its
posterior
surface is exposed.
The posterior layer of the lesser (gastrohepatic) omentum is
incised
close to the lesser curve, taking care not to injure the
vascular arcade
formed by the left and right gastric vessels and the posterior
gastric
nerve of Latarjet.
-
8/12/2019 Vago Thomas
21/29
Branches of nerves and vessels (which travel together) going
toward the stomach wall are ligated and divided in bits and
pieces from the cardia to the incisura angularis (which lies
on
the lesser curve about 6-7 cm proximal to the pylorus),
takingcare to identify and preserve at least 3 terminal branches
(crow
foot) of posterior gastric nerve of Latarjet, which supply
the
antrum and the pylorus. This dissection is kept as close to
the
stomach as possible. The lower 6-7 cm of esophagus is cleared of
all nerve
branches. A posterior gastric branch of the right vagus,
called
the criminal nerve of Grassi (which traverses to the left
and
supplies the cardia and the fundus of the stomach) is looked
for
and divided. The main vagal trunks that had been looped
earlier are carefully preserved.
-
8/12/2019 Vago Thomas
22/29
In HSV, the main (right and left) vagal trunks, anterior and
posterior gastric nerves of Latarjet (which lie at a
distance
of about 1-2 cm from the lesser curve), and at least 3
terminal branches (crow foot) of the anterior and
posteriorgastric nerves of Latarjet, which supply the antrum and
the
pylorus, are preserved. Only nerve branches to the
esophagus, cardia, fundus, and body are divided.
The bared lesser curve may be reperitonealized by closingthe
anterior and posterior layers of the lesser omentum.
Alternatively, it can be covered with omentum. Some
surgeons, however, leave it bare as it is.
-
8/12/2019 Vago Thomas
23/29
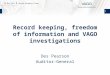
Vagotomy and Antrectomy
The lines of incision to
remove the lower portion
of the stomach (antrum),
pylorus, and a small
amount of duodenum. The
vagus nerves are also cut(truncal vagotomy)
The bowel is reconstructed by
closing the end of the duodenum
and bringing up a loop of
jejunum to anastomose to the
stomach. This is called a Billroth
II reconstruction.
-
8/12/2019 Vago Thomas
24/29
Vagotomy and Antrectomy
Keuntungan dari vagotomy dan antrektomi
adalah risiko rendah terjadinya kekambuhan
ulkus dan penerapan operasi pada pasiendengan ulkus peptikum
dengan komplikasi
(perdarahan duodenum dan ulkus gaster,
obstruksi ulkus peptikum, ulkus gaster yangtidak sembuh, dan
ulkus rekuren)
-
8/12/2019 Vago Thomas
25/29
Vagotomy and Antrectomy
Kerugian dari operasi ini adalah memiliki
mortalitas yang tinggi dibanding dengan
Highly Selective Vagotomy atauVagotomy+Drainase.
Setelah antrktmy, gastrointestinal
disambung kembali, baik melalui billroth Igastroduodenostomi
atau bilroth II loop
gastrojejunostomi
-
8/12/2019 Vago Thomas
26/29
Post Vagotomy syndrome
Highly selective vagotomy aims to maintain the nerves of
Latarjet(branches of the vagus nerve which supply the
pyloric
sphincter) and obviate the need for an accompanying drainage
procedure (usually pyloroplasty).
Complications afterwards include:
Steatorrhoea and diarrhoea, which are common after vagotomy
(although this is less of a problem after highly selective
vagotomy).
Often such symptoms are transient or episodic. However, in
about2% of cases symptoms are severe or persistent.
Stomal ulceration, which can occur particularly if the vagotomy
is
incomplete.
-
8/12/2019 Vago Thomas
27/29
Komplikasi
Perforasi
Penetrasi tukak yang mengenai pankrreas
Obstruksi outlet
Intraktibilitas
Keganasan dalam duodenum
-
8/12/2019 Vago Thomas
28/29
Prognosis
Prognosis tergantung dari perjalanan
penyakit dan komplikasi yang terjadi.
Kebanyakan pasien berhasil diobati denganeradikasi infeksi
H.pylori, menghindari
NSAID, dan penggunaan yang tepat
antisekresi
-
8/12/2019 Vago Thomas
29/29
TERIMA KASIH