-
8/2/2019 Vagnoni Grant Proposal Submission 2 Full Word07
1/19
Fusion: Integrating heterogeneous EHR data from diverse
sources.A. Specific AimsThe Institute of Medicine (IOM) reported in
2000 that as many as 98,000 people die annually as a result
ofmedical errors [16]. Several years later, a more comprehensive
study found that the number was more than195,000 patients dying
each year from preventable in-hospital medical errors. This is
equivalent to more thanone 747 jumbo jet full of patients crashing
everyday. The Center for Disease Control's annual list of
leadingcauses of death does not include medical errors. If the list
did, preventable medical errors would show up as3rd behind heart
disease and cancer [36]. Additionally, hospital-acquired infections
account for more than90,000 deaths each year and are largely
preventable [7][10]. Few individuals now doubt that
preventablemedical injuries are a serious problem. However, there
is still uncertainty among medical professionals as tothe best
means to combat this epidemic [17].
Many high-hazard industries begin combating preventable mistakes
by focusing on the flaws within the systemand not by blaming and
shaming the people in those systems [17]. For this reason, interest
in technologies tosupport safer care by assisting in reducing the
complexity and problem areas within the health care system
hasincreased. Studies report that Electronic Health Record (EHR)
systems could obviate many of the preventabledeaths while saving 81
billion dollars annually [14]. While EHR systems are a step in the
right directioncomputerized assistance can help even further. One
key assistive technology has been the computer-assistedphysician
order entry systems (CPOE). In one experiment, implementation of a
CPOE application leveragingan existing EHR system decreasedserious
medication errors by 55%[4].
CPOE systems aid in solving the problem, but they are not a
complete solution. These systems are only asgood as the data they
have access to. The current data landscape makes access to all the
timely, relevaninformation incredibly challenging. At least 35
different laboratory information systems are used in the U.S.
[2]Adding to the complexity, between 200 and 350 vendors offer EHR
products in the U.S. that interact with anynumber of the lab
systems[31][22][9]. These are just the publically sold systems;
many more hospitals havedeveloped their own in-house, custom EHR
systems. Thus it is no surprise today that a patients data can
beeasily lost during a migration from one hospital to the next or
when a hospital switches from one vendor to thenext.
Without access to all the relevant data, these systems will
never be able to prevent the crashing jumbo jetsfrom killing all
the patients within. Not only does the right data need to be
present at the right time, but whathe computerized systems really
need is information and not data to act upon. Artifacts from
different EHRsystems often distort the information and hamper more
advanced systems like CPOEs from working to their fullpotential. We
seek to address these short comings by integrating all the data a
Decision Support or CPOEsystem needs when it is needed by
transforming and integrating all of a patients EHR data into the
requisiteinformation.
While some have proposed standardization as a means of solving
the integration problem, such approacheshave suffered from many
hurdles. A standard has to be created (there are many competing
standards today)Even if one was settled on (for instance Health
Level Sevens, HL7), it would only be effective once all
vendorssupported the standard. This would involve significant work
and money, and currently few EHR companiescomply with the
accreditations available [40]. Finally, even if all the problems
were overcome, the data wouldbe syntactically integrated but not
semantically integrated. That is, the representation of a concept
such asfemale could be handled by designating a 2 in one hospital
while as an F at another. A CPOE will not know
that they are the same without being told.
The other possibility is to implement a semi-autonomous
algorithm to not only integrate the data from disparatesources, but
to integrate the meaning or semantics of the data across
organizations into a common informationand knowledge
representation. Some algorithms have been created to do exactly
this, the best known isBioStorm. BioStorm is an integrated
knowledge representation system aimed primarily at the
bio-surveillancedomain. Its chief problem is the overly simplistic
and brittle assumptions made in its architecture [21]Regardless, an
integration and knowledge creation algorithm will have to undergo
rigorous testing beforemedical organizations will trust it with
their data and put their faith in the results. Unfortunately, there
has beena complete lack of validation and systematic verification
of medical data integration algorithms. A goldstandard to compare
against is sorely needed for the field to progress and gain
credibility.
-
8/2/2019 Vagnoni Grant Proposal Submission 2 Full Word07
2/19
Specific Aims:
1. To produce an algorithm that semantically integrates
heterogeneous data from diverse sources. Thisalgorithm will not
only integrate the data but use the extracted knowledge to further
augment those sub-systems that provide it with data and/or
information. This will be a top-down and simultaneouslybottom-up
process. This enables preexisting knowledge and recently
encountered experiences totransform into something better than the
sum of its parts. Further, we contend that existing,
commonrepresentations from relational databases to textual
repositories occlude all the information that ispresent in the data
from outside extraction and use.
2. To generate a gold standard to serve as evaluation criterion
to be used to judge integration algorithmsagainst medical doctors,
serving as domain experts. This is a very successful strategy that
has as aresult of providing an objective fitness function spurred
areas from natural language processing (NLP)to decision support to
flourish. For the class of heterogeneous integration algorithms,
particularly withinthe medical community, no such gold standard
exists. The inability to objectively compareimplementations of
disparate, medical data integration is a real rate limiting factor
and one pointed oncommonly in the literature.
-
8/2/2019 Vagnoni Grant Proposal Submission 2 Full Word07
3/19
B. Background and SignificanceMerriam-Webster defines a mistake
as: to blunder in the choice of, to misunderstand the meaning or
intentionof, and to identify wrongly. When a physician prescribes
the wrong medicine for a patient, a blunder has beenmade that often
is catastrophic. When a surgeon misunderstands the orders, the
wrong body part is operatedon. When a patient is misdiagnosed, the
consequences can be fatal. So fatal, that it is estimated that
morethan 195,000 patients die each year from preventable
in-hospital, medical errors. This is equivalent to morethan one 747
jumbo jet full of patients crashing everyday. Indeed the safety
record of the health system in theUnited States lags far behind the
similarly complex aviation industry. A person would have to fly
nonstop fo438 years before expecting to be involved in a deadly
airplane crash [19]. These numbers dont encompassthe whole problem,
because in-hospital patients are a small fraction of the total
patient population. Retaipharmacies fill countless prescriptions
each year, nursing homes watch over the elderly and infirm,
anddoctors offices met out care in an out-patient setting. The
195,000 patients dying each year are in-hospitapatients, the tip of
the iceberg. No one knows how deep the iceberg extends beneath the
United Statestroubled waters.
B.1 Medical ErrorsThe American Hospital Association (AHA) lists
the following items as common types of errors: incompletepatient
information, unavailable drug information, and miscommunication of
drug orders [19]. Patieninformation is incomplete and not
accessible in its entirety at the point of care. A patients
allergies or all themedications being taken might hide in the
pharmacys database. Previous diagnosis for past illnesses o
additional current ailments might reside in another doctors
electronic health record (EHR). Pending lab resultsmight be tucked
away in a third-partys laboratory information management system
(LIMS). At least 35different LIMS are used in the United States and
20,580 labshave been certified by the U.S Department oHealth and
Human Services. It is common for practices to receive results for a
patient from multiplelaboratories. What makes matters worse is that
between 200 to 300 vendors offer ambulatory EHR productsinthe U.S.
[28], on top of the number of custom, in-house EHR systems that
exist.
Another problem area is the current disconnect between warnings
that are released by the FDA orpharmaceutical companies and the
patients taking the drug. Doctors arguably are supposed to be that
linkbut they can be caught unaware for many reasons. Time is a
scare resource, and the doctors and their stafare often overworked.
The method of dissemination can introduce difficulties. Paper
notices can get lostemails can get put in a spam folder, or
websites can go down. Even if time and dissemination dont fail,
a
doctor must remember all the drugs from all of the patients
under their care, which is simply not possiblewithout using an
electronic system more specialized than the EHR, called the
computer physician order entrysystem (CPOE). The CPOE allows
medical staff to electronically order drugs and automatically check
fointeractions, complications, and warnings. However, a CPOE system
is only as good as the information it hasto work on.
Finally, the orders for drugs themselves can be mistakenly
communicated. Name confusion is the mosheinous example, says Peter
Honig, M.D. and FDA expert on drug risk-assessment [19]. Take the
sound-alikenames of Lamictal, an antiepileptic drug, with Lamisil,
the antifungal drug. The volume of dispensing errors othese two
drugs was so vast that campaigns to warn physicians and pharmacists
of the potential confusion hadto be waged. It still hasnt stopped
epileptic patients from dying when they are erroneously given the
antifungal drug Lamisil instead of Lamictal. The FDA has clamped
down on sound-alike names of drugs, but the
problem is far from eradicated. A CPOE system can only go so far
in assisting to increase the specificity of thedrug ordered. Sloppy
handwriting and miss dosing might disappear, but until the CPOE
system canunderstand the semantics of a patients condition and the
drugs that should be used to treat will there be anytrue progress
in eliminating these types of mistakes. After all, a CPOE system
would not prevent a doctor fromtreating an epileptic seizure with
antifungal medicine, because a patient might have both conditions.
If a CPOEsystem had access to all the information relevant to a
patient, unlike the current state, it could realize thepatient is
in the hospital for a seizure episode based on the chief compliant
entered during the patientsadmittance, and further know that fungal
drugs are not ordered to be used by nurses in hospitals but rather
asan outpatient treatment.
B.2 Perspectives of Error
-
8/2/2019 Vagnoni Grant Proposal Submission 2 Full Word07
4/19
While many errors are being committed everyday, who is to blame?
The state of malpractice suits might arguethat the doctors and
staff are at blame. However in reality, medicine is practiced
within a very complex systemThis complexity coupled with the
limitations of humans make avoiding mistakes an extremely demanding
task.
In its landmark report, To Err is Human, the Institute of
Medicine (IOM) suggested moving from the traditionaculture of
picking out an individuals failings then blaming and shaming them
[17][19]. The IOM asserts thasystems failures are at the heart of
the problem rather than bad physicians. This is a crucial
scientificfoundation for improvement of safety found in all
successful high-hazard industries. Errors are seen asconsequences
rather than causes, having their origins in upstream systematic
factors. The central idea is tha
of system defense within the complex environment of health care.
In aviation maintenance an activity whosecomplexity is close to
that found in medical practice, 90% of mistakes were judged to be
blameless[23]. Ovethe past decade, research into error management
determined two essential components for managing unsafeacts:
limiting the incidence of them and creating systems that are better
able to tolerate occurrences of errorsand contain their damaging
effects. As a result, interest in technological solutions to manage
the complexity othe health care system have surged [19].
B3. ComplexityHealthcare is more complex than any other industry
in terms of relationships. There are over 50 different typesof
medical specialties which then have further subspecialties
interacting with each other and with an equallylarge array of
allied health professionals. The more complex a system is the more
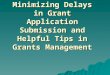
chances it has to failFigure 1 demonstrates the complexity of one
routine activity at a pediatric cardiovascular surgical care unit
in ahospital.
Medical care today depends on the interactions between many
different individuals and parts of the healthcaresystem. As complex
as health care is today, it is just as fragmented. There is an over
emphasis on focusing
Figure 1: Process map in Healthcare and Between Healthcare and
Secondary [3]. Pediatric cardiothoracic surgical teammembers
at two large urban medical centers delineated the steps of
care from the patients perspective, starting with
the
referral for surgery until the childs first post -discharge
follow up visit. Notice that different groups of individuals
withdifferent backgrounds and levels of experience are involved and
this process crosses multiple organizational boundaries.
-
8/2/2019 Vagnoni Grant Proposal Submission 2 Full Word07
5/19
and acting on the parts without looking at relationships to the
whole: the patients and their health [25].However, complex systems
are more than the sum of their parts [34][18]. Unfortunately,
specialization with itscommensurate focus on only a narrow portion
of a patients medical history has exploded without acomparable
growth in the ability to integrate the information surrounding a
patient. As a result, our ability toturn data into information and
information into knowledge has diminished [25]. Thus while the US
continues tomake advances technologically, its healthcare system
remains fragmented, ranking 37th in performance toother systems in
the world[35]. Current information technology systems focus
narrowly on care of individuadiseases, rather than higher level
integration of care for prevention, mental health, multimorbid
conditionsand acute concerns [12][26][27]. Knowledge generation is
narrowly partitioned in disease-specific institutes
and initiatives without sufficient balancing research that
transcends these boundaries.
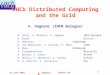
B4. Data the Rate LimiterHealthcare suffers from data explosion
[1,2]. US Government Census, [6,7], indicated that in 2002 there
were6,541 hospitals and in 2005 there were 7,569. There were 33.7
million hospital inpatient discharges in 2002on any given day,
there are 539,000 hospital inpatients, nationwide, excluding
newborns. Each patientgenerates a multitude of structured lab
reports and unstructured summary notes by ER, nurses, and
doctors.There are one or more EHR systems for a patient at each of
the different hospitals a patient might have visitedduring the
course of his or her life.
Figure 2: Different types of datain a Hospitals Clinical Data
Center
[1] illustrates the diverseecology of todays clinicaldata
center. It is commonfor departments to generatethe same type of
data buthave it provided by differentvendors or custom systems.
B5. Standards arent thesolution
Standards have been
around for more than a 100of years. These earlystandards were
for singleand simple things like thewattages of a light bulb orthe
spacing of threads on ascrew. The complexity ofsystems and
industriesrequiring standards hasgrown significantly sincethen. An
EHR, for example, is so complex it cannot be described in a single
standard, but will requirehundreds of new and existing
standards[32][33]. Furthermore there are many competing
standards
organizations that need to be involved such as: The
International Standards Organization (ISO), Clinical
DataInterchange Standards Consortium (CDISC), International
Healthcare Terminology Standards DevelopmenOrganization (IHTSDO),
the World Health Organization (WHO), National Council for
Prescription DrugPrograms (NCPDP), Health Level Seven (HL7), Health
Information Technology Standards Panel (HITSP), theEuropean
Committee for Standardization (CEN), and ASTM International. Each
of these organizations hastheir own working groups on different
aspects of the EHR such as CENs: Data Structure, Messaging
andCommunications, Health Concept Representation, Security, Health
Cards, Pharmacy and Medication, Devicesand Business Requirements
for EHRs. Indeed, Charles Jaffe, M.D. the CEO of HL7 is quoted as
sayingThere is not a lack of standards, there are, in fact, too
many standards and too many organizations writingthem[15]. Sam
Karp, Vice President of Programs, California Healthcare Foundation
testified to the Institute ofMedicine as follows, Our experience
with the current national data standards effort is that it is too
slow, toocumbersome, too political and too heavily influenced by
large IT vendors and other large institutions The
Figure 2: Different types of data in a Hospitals Clinical Data
Center [1]. Analog datafrom ECG Waveforms and sound, binary data
from images and videos, structured datafrom the EHR systems from
various departments, and free-text from notes and reviewsare all
present for each patient seen at each hospital a patient has been
to. Differentdepartments have different types, formats, and intent
behind their data. These oftenform silos that must be breached to
allow for true integration of the patients medicalhistor .
http://www.cdisc.org/http://www.cdisc.org/http://www.cdisc.org/http://www.cdisc.org/
-
8/2/2019 Vagnoni Grant Proposal Submission 2 Full Word07
6/19
current approach to standards development is too complex and too
general to effectively support widespreadimplementation.
Assuming at some point in the next five years a national EHR
standard is reached, then the task of compliancemust be surmounted.
This is a rather daunting task, because of the sheer size of the
Healthcare Industry inthe United States. There are at least 50
different medical specialties and subspecialties at more than
7,569hospitals being served by over 300 private EHR vendors and/or
custom built EHR system [28][5]. Thesehospitals are served by the
20,580 laboratories each using a version of a LIMS from the over 35
differentvendors. Then there are the varied pharmacists using their
own systems. Vendors must be convinced toimplement the new
standards with little benefit. The additional cost is not
compensated for directly. Adoptionis a significant hurdle in and of
itself [32][33].
When all of this has been accomplished, data interoperability
will finally be realized. However, the integrationof this data will
only be superficial. While the structure of the data might be
dictated by the standards, thecontent of the data or the
information within the data remains isolated. One vendor might
represent theconcept of human female by the numeral 2 while another
represents it as the letter F and a third as areference to another
location (demographics table for instance). Even higher level
concepts like the history oall medications taken by a patient can
be represented in an uncountable number of ways while still
complyingwith the letter of the standard. Worse, a standard cannot
account for all data a vendor might have, so oftenthere are
locations within the standard for optional data. All of these
factors make true interoperabilityextremely difficult, even when
all parties comply with all the diverse standards that exist.
B6. Grid-based approach
The Novo Grid uses an agents as distributed software entities to
exchange information between people andapplications. Agents are
task-specific software programs that can be installed in any
location. The idea behindthe concept is to create small, modular
programs interacting through a workflow activity. This both
encouragesefficient composition and reduces design time. Once
installed, agents could theoretically interact with theilocal
environment to extract and insert information and exchange the
information with other agents to automateworkflow tasks. However,
the agents are still specific instantiations of domain knowledge
towards a specificdata source at a specific location. Even though
the agents are small and light-weight pieces of code, this is
stilno guarantee on their efficiency and usefulness. The most
important thing from a data integration stand poinis what data they
were created to interact with.
For example, an agent installed on a server in a hospitals data
center can listen for HL7 result messages fromthe hospitals
interface engine. Without a mechanism of formalized representation
of knowledge about whatdata is, what the formats for the data are,
what the domains constraints are, and what the
environmentsspecifics are it is difficult to make this process
efficient. Its programming will be overly specific to a
narrowlydefined input and transformed output, and not allow for the
degree of generalizability necessary to overcomethe exponential
combinatoric problem that exists within the health care system.
Namely any party can wandata from any other party and any time.
Finally for inter-agent communication a blackboard or post
office metaphor is implemented. The Novo Gridprovides a messaging
post office that allows agents to send information from one to
another. However, therestill must be a common mechanism for
communication, which for the Novo Grid is a vendor specific
standard
That is, the agents communicate through message passing that
they have been pre-programmed tounderstand. There is however an
alternative. Knowledge about the system could be explicitly
represented sothat it is comprehensible to both humans and
machines.
B7. The Semantic Web
The semantic web is an explicit, graph-based representation of
knowledge that is both human and machinecomprehensible and
computable. This framework is designed to enable data to be shared,
federated, andenhanced regardless of system boundaries. The
semantic web was designed around the Open WorldAssumption that
truth is independent of whether it is known by any single entity.
That is, the graph-basedknowledge formalized into an ontology can
be extended by another entity. The language used to
represenknowledge is called the Resource Description Framework
(RDF). Its basic representation of a statement o
-
8/2/2019 Vagnoni Grant Proposal Submission 2 Full Word07
7/19
knowledge is the triple: a subject, predicate, and object.
Subjects and predicates are resources that refer toconcepts that
via the Open World Assumption can be extended or changed at any
time. Objects can either beresources or literal values (text,
numbers, dates, etc.). Resources are both unique and globally
identifiable byusing a Universal Resource Identifier (URI), of
which a Universal Record Locator (URL) from the internet is
asubset.
B8. BioSTORM (Biological Spatio-Temporal Outbreak Reasoning
Module)One of the most well known attempts at semantic integration
of disparate date is BioSTORM, a system forautomated surveillance
of diverse data sources. The system is agent-based, like the Novo
Grid, with a three
layered architecture consisting of a Knowledge Layer, an Agent
Platform, and a Data Source Layer. TheKnowledge Layer is composed
of a library of problem solving methods and a collection of
ontologies definingthe system components. The problem solving
methods are implemented either by BioSTORM or domainexperts
according to an Application Programming Interface (API). The
ontologies in this layer describe systemvariables, the problem
domain, and deployment configurations. The Agent Platform is the
middle layer, and iprimarily deploys agents based upon the
specifications in the Knowledge Layer. The agents act according
tothe knowledge describing the tasks and problem domain. The Data
Source Layer describes the environmenthrough an ontology. This
provides a binding between the tasks the agents are to undertake
and the actuaphysical resource [21].
However, BioSTORM has several shortcomings. It is focused on the
Bio-Surveillance area within publichealth. Their data broker
component is concerned with mapping from the raw data to the needs
of a particular
problem solving method from the Knowledge Layer. This does not
scale, because a particular method mighrequire any given subset of
data within the cloud of all patient EHR data. There are simply too
many vendorssupplying EHR systems to a vast array of different
users who have any number of different data sources andtypes. Then
couple this with all the possible uses the patient, the doctors,
the researchers, the governmentetc. might have for the data.
Furthermore, this methodology requires a priori knowledge of the
data sourcesThe implementer of an agent using the data broker must
know what they are looking for and where it islocated. It does not
allow for exploration and change of the data present.
-
8/2/2019 Vagnoni Grant Proposal Submission 2 Full Word07
8/19
C. Preliminary Studies
C.1 Modeling DataThe semantic web will be used to enable
extensions and enhancements to the data. An ontology is a
formaspecification of a conceptualization. It describes kinds of
entities and how they are related verses a dataschema which speaks
more to message formats (syntax) than knowledge representation.
Ontologies alsoprovide generic support for a machine to reason on
by making data machine understandable (historically it hasbeen only
human comprehensible). It defines individuals, classes, and
properties within a domain, formally
organizing knowledge and terms. Ontology Web Language, OWL, is
the mechanism for doing just this.Statements are asserted about a
particular subject in the form of a triple composed of a subject, a
predicateand an object. From these triples or statements, logical
consequences and facts entailed by the semantics canbe derived.
Universal Resource Identifier, URI, (University Resource Location,
URL, is a sub-type of URI) isused to specify unique ids for a
subject, its properties, and in some cases an object of the
statement. It is theuse of URIs that makes it easy to extend
ontologies by uniquely identifying a concept, taking into
consideration
what others have asserted about the same URIIt is precisely
these features that we leverage inthe proposed Fusion System.
C.2 Integrated Department InformationService (IDIS)The mechanism
of integration was used toaugment the extraction of information
fromdifferent data sources. The Intra-DepartmentaIntegrated Search
(IDIS) project integratedhierarchical (database) and textual (web
pages)search results, mutually reinforcing each otherThe goal was
to process a domain(www.cs.uiuc.edu) and enable better
searchresults by leveraging all the data within thatdomain from its
relational databases (RDBS) tothe textual data. We placed the RDBS
datawithin an Oracle database, which comprisedthings like faculty
information and student rostersKnowledge about the database was
extractedfrom metadata (i.e. the schema) and insighprovided by the
textual processing. The textuaprocessing began as an automated
crawling ofthe www.cs.uiuc.edu domain. Once all the htmpages were
collected, an open source text searchengine was employed to extract
phrases. Theresults were integrated via a web-based GUI.
IDIS integrated across three different dimensionsFirstly, it not
only combined results from both arelational and a text database, it
was able toleverage the results from one to get higher
qualityinformation from the other. After the usersKeyword Query was
transformed by the SQLQuery Composer into an appropriate query to
therelational database, these results were utilized toprovide the
context upon which textual resultswere extracted from the large
corpus ofdepartmental web pages. Then the textuaresults drove how
the structured results from thedatabase were presented inside of
thePresentation Layer. This synchronicity was one
Figure 3: The IDIS System received queries from theinternet,
which were processed into SQL Queries. Theresults of the SQL
Queries were then used to extractcontextualized and relevant
results from the textdatabase, which contains all the department s
internetpages. Some of the data is injected into the
relationaldatabase, while the majority remains in the textdatabase.
Most of the data from the relational databasecame from the
departments structured data. Thepresentation layer not only
displays the results butassists in future querying by providing
context to boththe user and the system.
-
8/2/2019 Vagnoni Grant Proposal Submission 2 Full Word07
9/19
of the key components we are going to utilize in the currently
proposed research. There is information that isuniquely embodied in
the textual data that simply cannot be conveyed in the structured,
relational databaserepository. For example, RDBMS traditionally do
a poor job efficiently storing the often sparse structure of
textwhich makes it extremely difficult to interact with. Likewise,
the relational database has information explicitlyrepresented in
its structure (particularly its schema) that cannot be represented
in the typical webpage.However, both of these hurdles are solved in
xml for humans and made machine understandable in thesemantic webs
RDF/OWL ontologies.
Another very relevant area of integration was across time. IDIS
used past context to enhance current search
The history of a users search and interact ion with the site
provided a trajectory through which current needswere channeled.
For instance while trying to prioritize a users query results, past
activity within the area ofcourses offered by the college would
cause professors related to those past searches to be ranked higher
anddisplayed more prominently. Finally, search was integrated with
navigation. Indeed, how the user interactedwith the results
provided useful information for current and future searchingas
well. A user might drill down ona professors research interests to
then find classes related to those interests. These two cases
areparticularly interesting, because bothcan be conceived as
trajectories or graphs of a users behavior. In bothcases, the users
current actions extend the graph representing all past interactions
with the informationcontained across textual and relational
databases. This is one of the reasons why using the semantic web,
agraph-based representation of data, should be so powerful in our
proposed project. Many of these synergiesare easier and/or
augmented by using a representation that more closely approximated
the phenomenon weare trying to elicit.
From the users perspective, the IDIS system completely
abstracted the representation of the data from usersinteraction.
The users of the system did not need to know the structure of the
databases nor even how tointeract with them (i.e. SQL Querying
Language). Rather the user interacted with the system and
requestedadditional information from the system by navigating
through the relationships between the information. Insome cases
that information was present in the users head (via keyword
queries), but in other cases it waspresent in the representation of
the information to the user by the system.
C.3 Computerized Medical SystemsWhile at Computerized Medical
Systems, I was responsible for creating a new system of integrating
medicaand health data from within the company and across its
partners. This project differed from IDIS in that it dealwith a
wide assortment of medical data from digital images to demographic
information to medical records.
Each application had its own particular means of representing
the data. Much of the companys future hingedon being able to access
data uniformly from anywhere, because of the exponential growth of
complexity asnew applications were introduced that then needed to
interact with existing applications. When everyapplication needs to
potentially interact with every other, typical methods using
standards and messagepassing just did not scale. This burden was
threatening to halt future application development. Worse thehurdle
for a collaborator to work with our products was even more
insurmountable, because at leastdevelopers within the company had a
familiarity with internal standards. However, giving away
proprietaryformats represented a problem in both intellectual
property and time. Even if there was no concern oinadvertently
giving away a secret, collaborators would be burdened with spending
the time to understand longspecifications about each products data
requirements.
C.4 XML-to-Ontology (X2O)
My work at the School of Health Information Sciences (SHIS) has
given me over 18 months of experience withall the technologies
needed to complete the Fusion Algorithm. I will be presenting the
work I have done whileat SHIS at the upcoming SemTech 2009
conference titled, What is in XML: Automated Ontology Learning
andInformation Transformation from Continuously Varying Clinical
Data.
-
8/2/2019 Vagnoni Grant Proposal Submission 2 Full Word07
10/19
C.4.1 Raw DataAt SHIS, I have been researchingand improving upon
existingalgorithms to integrate theElectronic Medical Records(EMRs)
from 7 local hospitalsEach hospitals data is differen
from each others and representsinformation from its
emergencydepartment and patient physicianvisits. The data are
received inunstructured XML (see figure4)The schema for the XML
isunknown and the structure canchange without notice. Data
arereceived as a stream from eachhospital, with a packerepresenting
a snapshot of whaoccurred in the previous ten
minutes. Over 4 millionmessages have been receivedduring the
past 4 years.
It is important to note that sincethere exists a
triviatransformation of a database intoxml, X2O can operate on
bothXML and Relational DatabasesRelational Databases are
actuallyeasier than XML, because with adatabase structure is
necessitated and a great amount of latent information resides
within its required schema. Comma delineatedlists, another common
file format, can also be trivially converted into an XML document.
Outside of binary fileformats, starting with XML has proved to be
the most comprehensive starting point for most of the
common,structured data formats. Further, X2O does not need a XML
Schema Definition (XSD) for the XML iprocesses. Again, the mining
of relevant information from such supplied structure, should it be
available, ispotentially very exciting; however, it isn't
necessary, because we perform well without it. There is no real
needto "standardize" the input data, because the ontologies
describing the data present in X2O serve as adistributed mechanism
for translating the data from machine incoherence into machine
comprehension.Increased human readability and understandability is
also a by-product of the X2O process.
C.4.2 The MappingAs discussed during the introduction, the
mappings are done through ontologies. The inherent, open-world
assumption around the Semantic Web means that adding further
semantics, statements about concepts, is atrivial matter. The
technology has such expectations built into it at every point, so
when there is an updated oreplacement to a medical ontology (UMLS
for instance) there is only a growth in understanding by
themachines that process the concepts and no additional work on a
humans part to update anything.
There are four levels of ontologies in X2O. The first level
defines at its most atomic what it means to be datasuch as concepts
and descriptions of those concepts. It is called the Core Data
Model, and it is the foundationupon which the next level resides.
For each type of data from XML to databases, there exists a model
thaexpresses all the nuances of that particular medium, Data
Specific Model. The third layer is the DomainSpecific Model. It
creates a mapping from within the domain leveraging what the system
explicitly knows fromthe previous levels to enable semi-autonomous
mapping. A domain expert describes the elements and
Figure 4: Sample of the XML data received every 10 minutes.
Thecontents of the XML are subject to change without
notification.
-
8/2/2019 Vagnoni Grant Proposal Submission 2 Full Word07
11/19
attributes from the perspective of the XML ontology. The
important distinction, however, from other efforts isthat an
exhaustive mapping of every possible value is not necessary.
Rather, patterns are described within thedata based upon location
within a snippet relative to other elements and attributes. This
flexibility captures alof the mappings traditionally found, but
does so more elegantly and extensibility. If a new value appears
withinthe XML, because of this feature, usually it is still
captured.
The fourth and final ontology level could be expressed in the
Semantic Web languages, but for efficiency it wasexpressed in the
programming code. This is called the Action Model, and it provides
the intentionality uponwhich the XML model, in this case, is
operationalized. This is beyond just the programming necessary
to
control a computer's manipulation of the data. Within the code,
lies a model that expresses the statementsand meaning behind each
element and attributes encountered within the hospital data
streamed through oursystem. Answering what can be said about a
fundamental class located within the data that will be
describedwithin the TBox verse the ABox.
C.4.3 PreprocessingAs the raw data is received, it isn't
automatically processed into its final form. Rather, there exists
anintermediary format that is quite novel. For each XML element,
including all attendant attributes, a node iscreated. At the end of
this pass, a hierarchical tree structure has emerged that has
indexed and re-groupedthe entire message. Because an xml element
might not actually be meaningful but rather some attribute
withinthe element is, this preprocessing essentially allows for a
transformation of the message into the conceptualrepresentation
that X2O will explicitly construct.
C.4.4 Construction of TBox and ABoxThe final stage of processing
actually sees the data bifurcated into a TBox and an ABox. One
particularlyinteresting property of X2O is that regardless of
whether the XML possess any metadata, the system does abeautiful
job of elegantly creating a TBox for it. The TBox is compact but as
demonstrated in priorexperiments, domain experts agree it
accurately describes the concepts present. The ABox generated is
arepository of the instances already present within the XML, and as
such is a more meaningful form of that datathan when it resided
within the XML. This is because the ABox has further meaning
applied to it through thegenerated TBox and the other models like
the core data model and any potential outside knowledge
sourcesimported.
C.5 BLUEText
BLUEText addresses the problem of extracting information from
clinical text found within EHRs, which includestriage notes,
physician and nurse notes, and chief complaints. Unfortunately,
this text is often written in shorhand: lacking proper grammatical
structure, prone to using abbreviations, and possessing
misspellings. Thishinders performance of traditional natural
language processing technologies that rely heavily on the syntax
oflanguage and the grammatical structure of the text. Figure 5
illustrates the architecture of BLUEText.
It has superior results on clinical text, which is often not
only unstructured but unconstrained. That is it often
isgrammatically incorrect, misspelling are rampant, and
abbreviations of concepts frequently occurs. Theinformation is
often compressed, and so the deviation from proper structure
contains more information than ifthe sentence had be properly
written. One such example is: Pt a 76 yrs old Af/Am fem. w/ bp
50/120, Hx oHA x 3 years. The sentence could be properly written
as: The patient is 76 years and an African-Americanfemale. She has
an initial diastolic blood pressure of 50 beats per minute and a
systolic blood pressure of 120
beats per minute. She has had three heart attacks that we are
aware of.
-
8/2/2019 Vagnoni Grant Proposal Submission 2 Full Word07
12/19
Figure 5: Schematic depiction of the BLUE-Text processes and
ontologies. Existing knowledge sources such as UMLS is
leveraged by the Semantic Knowledge of the system. Additionally,
the Syntactic and Domain Knowledge are all used
when generating the Conceptual Graph. After a preliminary text
preparation phase, the Minimal Syntactic Parser first
parses the text and then analyzes the syntax. The results of the
syntactic analysis forms a parse graph that is comprised of
tokens of text mapped to the Syntactic Knowledge. The Semantic
Interpreter performs automated ontology mapping:
using the parse graph to map from the tokens derived from the
original text to the concepts from the domain knowledge.
Also, a separate algorithm indexes these tokens semantically.
The interpreter uses this knowledge and the parse graph to
construct a conceptual graph that represents the content of the
input text. The Conceptual Graph is an intermediary and
generic output that builds on the parse graph and maps it to the
appropriate concepts from the domain knowledge. All
nodes in the conceptual graph have both a positional and a
semantic index that will be used by the Output Constructors
toextract different formats of outputs defined by user and/or task
based queries. The Semantic Interpreter uses this
information to im rove the conce tual ra h throu h a
normalization and disambi uation rocess.
-
8/2/2019 Vagnoni Grant Proposal Submission 2 Full Word07
13/19
D. Research Design and MethodsThe overall research plan is
summarized in the flowchart in Figure 6. Tasks on the flowchart are
numbered asx.y, where x corresponds to the Specific Aim associated
with the task, while y represents the specific taskitself. The same
numbering scheme is used in the text of this section, for easy
reference to the figure.
D.0 Choose 100 Records:The same corpus of data from our prior
work (C.4.1) will be leveraged for thisexperiment as well. As a
result of our need to validate our results and create a gold
standard, it wasimportant to devise a suitable number of patient
records to provide generalizability while not overwhelmingthe human
medical experts. The records will come equally from both the Cerner
systems and the
Allscripts data. We will attempt to keep an even distribution
across age, race, gender, and primarydiagnosis (ICD9 code).
D.1 To produce an algorithm that semantically integrates
heterogeneous data sources.D.1.1 XML-to-Ontology (X2O): Thissystem
will be used with little modification. The system
architecture currently fits into conceived architecture of the
Fusion Algorithm. The Fusion Algorithmtakes as input the resultant
TBox and ABox generated after X2O completes its processing of
theraw XML messages.
i. Results: Ontologies that can serve as input for the Fusion
Algorithm. Also this portion of thesystem controls what data the
BLUEText (BLU) sub-system processes. In that context, thecorpus of
text resides solely in free-text portions present within an XML
message. The X2Owill determine when a section of XML is suitable to
be processed by BLU based on someheuristics such as size of the
value and prior information contained within the ontologies.
Figure 6: Flowchart of activities in project. Number in boxes
corresponds to task numbers used in the textin Section D.
-
8/2/2019 Vagnoni Grant Proposal Submission 2 Full Word07
14/19
ii. Problems: One problem is that X2O might fail to provide BLU
all the text that BLU couldprocess, thereby missing information
that could have been extracted. Work and especiallyvalidation will
need to be done to ensure that X2O is filtering the data BLU
processesaccurately.
iii. Alternate Approaches: There are alternatives to X2O,
BioStorm is one such example. In theworst case, BioStorm could be
used, but it is very unlikely that contingency would beneeded.
Further, we have already discussed in section B.6 the short comings
of BioStorm,and why X2O is a superior choice.
iv. Transition: As a result of most of the work for this
component already being in a complete
state, any modifications that need to do be done can occur
concurrently with modificationsof BLU and creation of Fusion. That
is, only minor adjustments should be necessary, andtherefore should
not exist as an obstruction to timely progression.
v. Expertise: X2O was designed by the PI andother investigators
on the grant.
D.1.2 BLUEText (BLU): Currently BLUETextprocesses text into
ontologies, but not in the formatrequired by the Fusion Algorithm
(TBox and ABox).The refactoring to accomplish this will be
significantbut well-known and straight-forward. There are
noexpected difficulties in this rework. Fortunately aswith the
XML-to-Ontology algorithm, we were the
creators of BLU, so we are confident of ourassessment of the
scope of the modificationsrequired.
i. Results: Some rather significant workremains until BLU will
be in a state tocontribute to Fusion.
ii. Problems: The major concern is that thescope of the changes
necessary for BLU tocomply with the input expected by the
FusionAlgorithm is not accurate. This seemsunlikely based upon our
extensiveexperience with the system, plus in the worst
case the output of BLU could be treated asXML by X2O. As such,
X2O could transformthe output of BLU into the output expected
byFusion.
iii. Alternate Approaches: There are many NLPsolutions and some
of them specific to themedical domain that could be used.However,
most medical NLP solutions areproprietary and therefore expensive.
Themost well-known open solution is the NLMsSPECIALIST NLP Suite of
Tools developedby the The Lexical Systems Group of The
Lister Hill National Center for BiomedicalCommunications to
investigate thecontributions that natural languageprocessing
techniques can make to the taskof mediating between the language of
usersand the language of online biomedicalinformation
resources.
iv. Transition: As explained in D.1.1v. Expertise: We designed
the algorithm.
D.1.3 Outside Ontologies: BLU makes use of various outside
ontologies to provide much of theknowledge base upon which is
operates. More importantly, the Fusion Algorithm will rely upon
Figure 7: Overview of the system architecture
of the Fusion System. Structured data is
handled by the XML-to-Ontology sub-system
through XML messages. The NLP algorithm,
BLUEText, will process unconstrained text
within the XML messages sent to the XML-to-Ontology algorithm.
The output of both sub-
systems is integrated within the Fusion
Component. Finally, the results of the
integration is used to enable both of the
upstream algorithms to process further, while
simultaneously enabling downstream
applications like EHR CPOE Decision
Support systems to function.
-
8/2/2019 Vagnoni Grant Proposal Submission 2 Full Word07
15/19
Outside Ontologies to increase its knowledge of the corpus of
medical data to further augment theaccuracy of the Fusion
Algorithm. Furthermore, it is very important the Fusion is able to
takeadvantage of outside augmentations to its knowledge source in
much the same way it is able toprocess the input from X2O and
BLU.
i. Results: This is a significant demonstration of the viability
of extensibility promised by theSemantic Webs design and the
conceived goals of the Fusion Project. As weve illustratedearlier
in sections B7 and C4, semantic federation of knowledge is itself
an unsolved butvitally important area of research. It is the only
way we can hope to manage the onslaughtof exponentially increasing
data generated all across society, but particularly within the
medical domain as it relates to patient health and safety.ii.
Problems: Access to useful Outside Ontologies is perhaps the
biggest problem. However
the NLM publishes taxonomies (like UMLS, SnoMedCT, etc), which
weve previously beenable to successfully translate into a true
ontology. Additionally, there are many usefulontologies about
location, demographics, measurements, drugs, etc that we would like
toleverage. Weve had some past successes incorporating a
measurement ontologydeveloped by NASA into BLU. We will have to
analyze how far these transformedtaxonomies and outside ontologies
are from the desired input of Fusion.
iii. Alternate Approaches: We can abandon the use of Outside
Ontologies without jeopardizingthe core aim of integrating
heterogeneous data from multiple sources.
iv. Transition: As explained in D.1.1D.1.4 Fusion Algorithm: At
the core of the proposed architecture, resides the Fusion
Algorithm. Its
purpose is to take in the pre-processed data from several
algorithms that have been previouslydesigned (D.1.1 and D.1.2) to
translate a specific format of data into an ontological
representation.Fusion then takes these ontological representations
and integrates them into a unified knowledgebase of (all) patients
information. Then an EHR, CPOE, Decision Support, etc system can
build ontop of the unified view of the patients information.
i. Results: Providing a single unified and well defined
knowledge base will enable existingsolutions and research into the
next generation of solutions to increase their
accuracy.Additionally, production times, maintenance, and other
issues typically encountered whenneeding to cope with a diverse
ecology of data islands should disappear.
ii. Problems: The core problems that Fusion needs to solve is
referred to as semanticfederation or ontology integration. It is
our belief that the diverse ontologies provided bytrusted, outside
sources and those created by sub-systems (X2O and BLU in this case)
can
be integrated by analyzing the graph-based representation of the
data. Graph analysis isimportant in a whole host of areas; one of
the most well-known examples is internet search(i.e. Googles
PageRank). It is our intent to use PageRank and K-Nearest
NeighborsAlgorithms to analyze the graph structure that comprises
the ontologies that Fusion receivesand determine a measure of
similarity between the different ontologies based on both
theinformation or semantics within the ontologies and the structure
of the graph representingthe connection between the atomic units of
information inside the ontology. It is unlikely thatan entire
automated algorithm will ever exist, nor that it would be
advantageous. As a resultof the catastrophic risks (patient death
or serious injury), medical experts will always berequired to
provide their consent to the results. However, medical experts are
both rare andtheir time extremely valuable. To this end, the aim of
Fusion is to vastly augment theproductivity of the doctors and
medical staff involved. This is also another reason for the
necessity of a gold standard. We will be augmenting what a human
could do if they hadsufficient time to do so, so we want to ensure
that we are at least as good as what a doctoror nurse might arrive
at. Without a human medical expert performing the same task
asFusion, it will be impossible to verify the success or accuracy
of Fusion.
iii. Alternate Approaches: Fortunately the space of graph
algorithms is ripe with research.While the field of ontology
integration is still very young, there are methods in the
literatureof graph algorithms (particularly in the area of webpage
analysis and searching) that couldbe applied to this task. One such
interesting method has just recently been applied to thearea of web
search that uses Level Statistics from a field called random matrix
theory originallydesigned to analyze quantum systems [6]. The new
method gauges the importance of words in
-
8/2/2019 Vagnoni Grant Proposal Submission 2 Full Word07
16/19
a document based on where they appear (pattern of locality),
rather than simply on howoften they occur. This is precisely what
is needed when integrating ontologies as well.
iv. Transition: This aim partially relies upon the completion of
the D.2 aim, however, this is whywe have medical experts
(physicians) assisting with early verification testing of the
results ofthe Fusion System.
v. Expertise: Several medical experts will be collaborating to
help verify the results, in additionto the gold standard generated
as a result of D.2. We have demonstrated, we hope, ourexpertise in
the areas of data integration, ontologies, and data modeling.
Summary: The successful completion of this aim will result in a
novel mechanism for solving the problemsof data explosion both in
quantity and representation. This is a real rate limiter that is
stifling realization oftechnologies like EHR and CPOE systems from
realizing their full potential to eliminate the vast majority
ofpreventable medical errors, which are currently the number 3
killer of Americans if it was on the CDCsannual list of leading
causes of death.
D.2 To generate a gold standard, evaluation criterion for
judging the success not only to evaluate ourperformance, but the
many other current and future attempted solutions.
D.2.1 Choose Experts: The initial choice of 3 experts to
integrate 100 records was chosen partially inaccording with choices
made in related areas of Health Informatics. Studies on the
inter-rateragreement of Mesh Tagging by pubmed editors for
instance.
i. Problems: Recruiting medical experts is a notoriously
difficult task, further getting experts
interested in spending the amount of time necessary to integrate
100 patient records will bea challenge. Fortunately, we are located
in Houston Texas medical center, where there is alarge pool of
medical experts present.
ii. Alternate Approaches: Unfortunately there are not good
alternatives to using medicalexperts as our gold standard. It is a
commonly held belief that medical experts such asdoctors, nurses,
and health informaticians are what a computerized implementation
shouldbe held to. Clinical Decision Support is a particularly
salient example where this occurs.There are, however, alternatives
to creating a gold standard to evaluate our algorithm.Some of these
statistics we would use anyway during analysis of aim 1. For
instance, oneof the central hypothesis is that the Fusion will
augment the information providing by thecomponent pieces (X2O and
BLU). Therefore, it is posited that more knowledge would
bediscovered on a second pass of the initial patient data by
incorporating the results from
Fusion. Analyzing how much new knowledge (if any) is discovered
could be one metric.iii. Transition: Much of the transition from
choosing and recruiting to actually having the experts
perform D.2.2 will be educating them on the task and what is
required of them.iv. Expertise: Medical experts will be used to
help select an appropriate cohort. Proposed
members of the team have experience recruiting experts from past
experiments.D.2.2 Integrate and Extract: Fundamentally, the experts
will be performing the same task as Fusion
but in their own way. They are free to integrate and extract
concepts as they see fit. Their timespent at the computer
integrating the EHR data will be recorded by video camera and also
trackedwithin the program they will be using called TopBraid
Composer. We have already written a pluginto the application that
allows us to do this.
i. Results: Indeed, much like a psychologist gains insight into
human behavior throughobservation, it is possible that we can glean
important and useful algorithmic information
from analyzing howthe experts integrate. This should be a
significant contribution beyondsimply providing the gold standard.
That is, little research has been done on how a humanmedical expert
might integrate disparate medical data. We hope to gain both a
goldstandard and an insight into human algorithms being employed by
medical experts tointegrate the data.
ii. Problems: Actually performing the task will rely upon our
training and the expertsexperience. If the experts lack sufficient
medical experience to comprehend the underlininginformation in the
data and transform the data into comprehensible knowledge, they
couldskew the results in favor of our algorithm by brining human
performance artificially down.Likewise if we fail to properly
educate the experts on their task, a similar result would be
-
8/2/2019 Vagnoni Grant Proposal Submission 2 Full Word07
17/19
observed. Partially, we hope that D.2.3 will help us discover
problems with individuals, but itcannot uncover cross cutting bias
or problems.
iii. Alternate Approaches: There is really no alternative to
using human medical experts, savefor comparing the performance of
Fusion against existing systems. However, most dataintegration
systems are propriety and uninterested in being declared inferior
to another(rival) system. Therefore getting access to another
system would be difficult. BioStorm isperhaps one of the few
examples of a fairly successful and open sourced system that
wecould use. This is another reason why having an independent gold
standard backed byhuman experts can help put pressure on existing
solutions. Purchasers and users of such
existing solutions can assess them prior to competing, which
currently is not possible in anyrigorous way.
iv. Transition: After this phase, a number of transition points
exist. If D.2.3 asserts theexpected amount of inter-rater agreement
and our own experts concur, there will be no needto repeat this
phase. However, if there is some sort of systematic bias that has
skewed theresults, it would be necessary to repeat either D.2.2 or
both D.2.1. and D.2.2. This woulddepend upon our analysis and our
assessment of where the bias is originating.
v. Expertise: As explained in D.2.1.D.2.3 Assess Inter-rater
reliability: At this point, our statistician will analyze the
agreement of the
experts attempts to integrate the patients data. Additionally,
our medical domain experts willassess how reasonable the results
are.
i. Results: A measure of confidence both objective and
subjective of the proposed gold
standard.ii. Problems: As explained in D.2.2.iii. Alternate
Approaches: Two approaches are being used, both with their own
strengths and
weaknesses.iv. Transition: As explained in D.2.2v. Expertise:
Our statistician has over 20 years experience, while our medical
experts each
have over 10 years.D.2.4 Compare Experts to the Fusion
Algorithm: This final portion will entail utilizing two
measures
of similarity. The first is our data modelers assessment of both
results. They both have extensiveexperience modeling data and
analyzing ontologies. Secondly, the similarity methods developedfor
D.1.4 will be re-employed here. Not only will this provide a means
of validation (because oursimilarity methods can be compared
against human data modelers) but it will assist in
systematically and objectively analyzing the results.i.
Problems: Discrepancies between the methods will help us to analyze
where the failures
are.ii. Alternate Approaches: We will be using two different
methods, it should not be necessary to
use alternative approaches.Summary: The successful completion of
this aim will not only provide a gold standard for any medical
dataintegration algorithm to use, but validate the novel Fusion,
the heterogeneous data from disparate sourcesintegration algorithm.
Even in the unlikely event that we do not succeed in all of our
aims, a great deal willbe learned by this experiment. We will be
collecting and analyzing how human experts integrate data,which
could yield an interesting direction to explore future integration
research. Further, simply having agold standard to compare existing
and future algorithms is a worthy aim in itself. One such benefit
isholding accountable those companies who sell their medical
integration software to the claims they make.
Additionally, enabling true competition by enabling consumers to
objectively compare competition and newsolutions should exert its
own evolutionary pressures. Even in failure, important lessons can
be gleanedabout how to approach future attempts at heterogeneous
data integration. Most existing research does notengage the very
diverse and often unharmonious ecology of realistic data. It would
be surprising if allexisting successful research in this area could
withstand the amount of rigorous testing we will haveemployed. If
Fusion fails, how it fails might be as interesting as how well it
succeeds.
-
8/2/2019 Vagnoni Grant Proposal Submission 2 Full Word07
18/19
D.3 Research Work Plan and Timeline
TimelineYear 1 year 2
Complete Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4IRB Submission & Review XD.0
Choose Representative Records XD.1.1 XML-to-Ontology XX XXD.1.2
BLUEText XX XX
D.1.3 Outside Ontologies XD.1.4 Fusion Algorithm XX XX XXD.1.5
Recurrent Data to D.1.1 & D.1.2 XX XD.2.1 Choose Experts XX
XXD.2.2 Integrate and Extract XX XX XX XXD.2.3 Assess Interrater
Reliability XX XXD.2.4 Compare Experts to Algorithm XX
Human Subjects Protection: IRB approval will be required for the
secondary data use and will be obtained fromthe University of Texas
at Houstons Medical CenterIRB.
-
8/2/2019 Vagnoni Grant Proposal Submission 2 Full Word07
19/19
Y. Collaborators
Principal Investigator: Matthew Vagnoni, MS brings an expertise
in data integration, ontologies, andunderlying technologies such as
programming, system architecture, etc.
Investigators:
Parsa Mirhaji, MD brings an expertise in NLP (BLUEText),
ontologies, data modeling, and medicaldomain.
James Turley, RN, PhD brings an expertise in statistics, system
evaluation, and the medical domain. Jorge Herskovic, M.D.,
Ph.D.brings an expertise in information retrieval, clinical
decision support, and
the medical domain.
Min Zu, MD, MS brings experience in both the medical domain and
as a data modeler.