-
8/9/2019 Vacuna VHE 3ra fase
1/10
Articles
www.thelancet.com Published online August 23, 2010
DOI:10.1016/S0140-6736(10)61030-6 1
Published Online
August 23, 2010
DOI:10.1016/S0140-
6736(10)61030-6
See Online/Comment
DOI:10.1016/S0140-
6736(10)61260-3
Jiangsu Provincial Centre for
Disease Control and
Prevention, Nanjing, Jiangsu
Province, China (F-C Zhu MSc,
X-F Zhang MSc, H Wang MD,
X Ai MSc, Y-M Hu MD,
Q Tang MD); National Institute
of Diagnostics and Vaccine
Development in Infectious
Diseases, The Key Laboratory of
the Ministry of Education for
Cell Biology and Tumour Cell
Engineering, Xiamen
University, Xiamen, China
(Prof J Zhang MD, S-J Huang MD,Q Yan MSc, Prof T Wu PhD,
Prof J Miao PhD,
Prof M-H Ng PhD,
Prof J W-K Shih PhD,
Prof N-S Xia MD); National
Institute for the Control of
Pharmaceuticals and Biological
Products, Beijing, China
(C Zhou MD, X Yao MSc);
Dongtai Centre for Disease
Control and Prevention,
Dongtai, Jiangsu Province,
China (Z-Z Wang MD,
C-L Yang BSc, H-M Jiang BSc,
J-P Cai BSc, Y-J Wang BSc); and
Xiamen Innovax Biotech,
Xiamen, China (Y-L Xian BSc,Y-M Li MD)
Correspondence to:
Dr Ning-Shao Xia, National
Institute of Diagnostics and
Vaccine Development in
Infectious Diseases, The Key
Laboratory of the Ministry of
Education for Cell Biology and
Tumour Cell Engineering,
Xiamen University, 422nd
Siming South Road, Xiamen,
361005, China
[email protected]
Ecacy and saety o a recombinant hepatitis E vaccine in
healthy adults: a large-scale, randomised,
double-blindplacebo-controlled, phase 3 trial
Feng-Cai Zhu, Jun Zhang, Xue-Feng Zhang, Cheng Zhou, Zhong-Ze
Wang, Shou-Jie Huang, Hua Wang, Chang-Lin Yang, Han-Min Ji ang,
Jia-Ping Cai, Yi-Jun Wang, Xing Ai, Yue-Mei Hu, Quan Tang, Xin
Yao, Qiang Yan, Yang-Ling Xian, Ting Wu, Yi-Min Li, Ji Miao,
Mun-Hon Ng,
James Wai-Kuo Shih, Ning-Shao Xia
SummaryBackground Seroprevalence data suggest that a third o the
worlds population has been inected with the hepatitis Evirus. Our
aim was to assess ecacy and saety o a recombinant hepatitis E
vaccine, HEV 239 (Hecolin; XiamenInnovax Biotech, Xiamen, China) in
a randomised, double-blind, placebo-controlled, phase 3 trial.
Methods Healthy adults aged 1665 years in, Jiangsu Province,
China were randomly assigned in a 1:1 ratio to receivethree doses o
HEV 239 (30 g o puried recombinant hepatitis E antigen adsorbed to
08 mg aluminium hydroxidesuspended in 05 mL bufered saline) or
placebo (hepatitis B vaccine) given intramuscularly at 0, 1, and 6
months.Randomisation was done by computer-generated permuted blocks
and stratied by age and sex. Participants wereollowed up or 19
months. The primary endpoint was prevention o hepatitis E during 12
months rom the 31st dayater the third dose. Analysis was based on
participants who received all three doses per protocol. Study
participants,care givers, and investigators were all masked to
group and vaccine assignments. This trial is registered
withClinicalTrials.gov, number NCT01014845.
Findings 11 165 o the trial participants were tested or
hepatitis E virus IgG, o which 5285 (47%) were seropositive
orhepatitis E virus. Participants were randomly assigned to vaccine
(n=56 302) or placebo (n=56 302). 48 693 (86%)participants in the
vaccine group and 48 663 participants (86%) in the placebo group
received three vaccine doses andwere included in the primary ecacy
analysis. During the 12 months ater 30 days rom receipt o the third
dose
15 per-protocol participants in the placebo group developed
hepatitis E compared with none in the vaccine group.Vaccine ecacy
ater three doses was 1000% (95% CI 7211000). Adverse efects
attributable to the vaccine wereew and mild. No vaccination-related
serious adverse event was noted.
Interpretation HEV 239 is well tolerated and efective in the
prevention o hepatitis E in the general population inChina,
including both men and women age 1665 years.
Funding Chinese National High-tech R&D Programme (863
programme), Chinese National Key Technologies R&DProgramme,
Chinese National Science Fund or Distinguished Young Scholars,
Fujian Provincial Department oSciences and Technology, Xiamen
Science and Technology Bureau, and Fujian Provincial Science Fund
orDistinguished Young Scholars.
IntroductionHepatitis E virus is a major cause o sporadic
and
epidemic hepatitis.1 Seroprevalence data suggest that athird o
the worlds population has been inected withthe virus.2 Although
most cases are in developingcountries, hepatitis E is no longer
rare and it might bethe most common type o acute viral hepatitis
inindustrialised countries.3
Clinically indistinguishable rom other types o acuteviral
hepatitis, hepatitis E tends to be sel-limited andusually does not
become chronic.4The severity o illnessincreases with age; the
overall case atality ratio isestimated to be 13%.5 Hepatitis E has
a poor prognosisin pregnant women: mortality is 525%, and
survivorshave high rates o spontaneous abortion and
stillbirth.6,7In patients with chronic liver disease,
superinectionwith hepatitis E virus oten leads to a poor
outcome.8,9
Every year, 13 00026 000 deaths are estimated inpatients with
chronic liver disease in industrialised
countries.10 In a continuing hepatitis E epidemic inUganda that
has caused illness in more than 10 196people and 160 deaths,
mortality was 13% in children.11
At least our genotypes o hepatitis E viruses havebeen
identied.12 Genotypes 1 and 2 were isolated romhuman beings and are
mainly seen in developingcountries. Genotypes 3 and 4 are zoonotic,
with pigsbeing the principal reservoir; they have been identiedin
many sporadic cases and limited oodborne outbreaksmainly aecting
middle-aged and elderly men. 1315Nevertheless, all hepatitis E
virus associated withhuman diseases can be considered as belonging
toone serotype.16
Two recombinant vaccines have undergone phase 2clinical trials.
One o the vaccines was produced in
-
8/9/2019 Vacuna VHE 3ra fase
2/10
Articles
2 www.thelancet.com Published online August 23, 2010
DOI:10.1016/S0140-6736(10)61030-6
insect cells and was sae and immunogenic in youngmen (mean age
252 years; SD 625), providing 95%protection against hepatitis E in
Nepal, where onlygenotype 1 hepatitis E virus had been isolated.17
Theresults were encouraging but two questions remainedto be
answered. The rst related to the saety and ecacyo the vaccine in
the general population, especially in
women and elderly people. The second related to theecacy o a
vaccine originally derived rom hepatitis Evirus genotype 1 against
disease caused by heterogenichepatitis E virus. The other candidate
vaccine, HEV 239(Hecolin; Xiamen Innovax Biotech, Xiamen,
China),was produced in bacterial cells and was sae andecacious
against inection with hepatitis E virus inseronegative participants
in a phase 2 trial.18
We undertook a randomised, double-blind, placebo-controlled,
phase 3 trial to assess the ecacy and saetyo HEV 239 in the general
population. The trial includedmen and women rom age 16 to 65 years,
with or withoutantibodies against hepatitis E, rom a region where
bothgenotypes 1 and 4 cocirculate with the zoonoticgenotype 4
predominating.
Methods
Study design and participantsThis double-blind, randomised,
placebo-controlled trialwas done between August, 2007, and June,
2009, inDongtai County, Jiangsu Province, China. On October,2007,
ater enrolment in one township (Quindong), andbeore enrolment in
ten other townships, the protocol wasmodied so that each o the 10
000 participants in one othe ten townships (Aneng) had serum
samples collectedon day 0 and month 7 to assess the level o
antibodyprotection through long-term ollow-up. Independentethics
committee approval was obtained rom the EthicsCommittee o the
Jiangsu Provincial Centre or DiseaseControl and Prevention (JSCDC),
and the study was donein accordance with the principles o the
Declaration o
Helsinki, the standards o Good Clinical Practice, andChinese
regulatory requirements as stipulated by theChinese Food and Drug
Administration.
The study was designed by JSCDC and XiamenUniversity. Study sta
at JSCDC were responsible or datacollection. A sentinel hepatitis
surveillance system wasset up to identiy incident hepatitis cases
as they presented.Serial serum samples obtained rom study
participantswere independently tested by the Chinese
NationalInstitute or the Control o Pharmaceuticals and
BiologicalProducts (NICPBP). A contract research
organisation(PPD-Excel PharmaStudies, Beijing, China) monitoredand
ensured that the trial was done in compliance withthe protocol,
evaluated progress, veried that the rights othe participants were
protected, and ensured that datawere complete, accurate, and
veriable rom source data.An independent data and saety monitoring
board(DSMB) was set up to oversee the trial and ensure thesaety o
participants and the integrity o the data. TheDSMB reviewed the
clinical and laboratory data to conrmthe diagnosis o hepatitis E
beore the group assignment(ie, vaccine vs placebo) o trial
participants was broken.
Men and women were eligible or enrolment i theywere healthy,
aged 1665 years, and understood the studyprocedures (detailed
eligibility criteria are described inwebappendix pp 23). Written
inormed consent wasobtained rom all participants.
VaccinationThe preparation o HEV 239 vaccine is
describedelsewhere.19 The vaccine contains 30 g o the puriedantigen
adsorbed to 08 mg aluminium hydroxidesuspended in 05 mL buered
saline. A licensedhepatitis B vaccine (Beijing Tiantan Biologic,
Beijing,China) containing hepatitis B virus surace antigen in05 mL
aluminium hydroxide, was given as placebo.Vaccine doses and placebo
doses were repackaged byInnovax under Good Manuacturing Practice
conditionsor identical appearance, but labelled with two
letterseach according to a random assignment. Three doses ovaccine
or placebo were given intramuscularly at 0, 1,and 6 months.
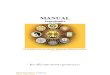
122179 individuals screened
112604 randomly assigned
56302 assigned to vaccine group
7609 did not receive three doses3817 received one dose3792
received two doses
3542 received doses one and two250 received doses one and
three
48693 participants were included inprimary efficacy analysis5567
included in immunogenicity subset1316 included in reactogenicity
subset
48663 participants were included inprimary efficacy analysis5598
included in immunogenicity subset1329 included in reactogenicity
subset
7639 did not receive three doses3874 received one dose3765
received two doses
3504 received doses one and two261 received doses one and
three
56302 assigned to placebo group
9575 excluded9263 excluded before vaccination
3652 did not meet inclusion criteria
5611 met exclusion criteria312 excluded before the codes
were broken146 did not meet inclusion criteria
(did not live in the study region)52 did not meet inclusion
criteria
(age 65 years)95 received wrong vaccine for
at least one dose19 were not given second dose
at the specified time
Figure 1: Trial prole
The webappendix lists reasons or exclusion (p 30) and or
non-completion (p 31).
For the protocol see http://
nidvd.xmu.edu.cn/HEV/
protocol/Protocol_
phase_3_100509.pdf
See Online for webappendix
-
8/9/2019 Vacuna VHE 3ra fase
3/10
Articles
www.thelancet.com Published online August 23, 2010
DOI:10.1016/S0140-6736(10)61030-6 3
Randomisation and masking
Trained local health-care workers enrolled theparticipants, and
some o these health-care workersinterviewed participants to assess
adverse events andpossible acute hepatitis later in the trial. An
independentstatistician prepared a permuted-block
1:1:1:1randomisation list (with 20 codes to a block) using
SASsotware. The randomisation list was concealed andtranserred into
an immunisation managementcomputer program through which
participants werestratied by age and sex, and assigned vaccine
codes.The study-group and vaccine code assignments weremasked rom
all participants, carers, and investigators(or monitors). The
integrity o the masking process wasconrmed by the investigators and
DSMB beore the
assignment o study group and vaccine codes was nallyrevealed.
Health-care workers rom JSCDC assignedparticipants to the study
groups; they did not have anyurther involvement in the trial.
A subset o participants rom one township wasselected or active
surveillance o adverse events(reactogenicity subset). Serum samples
beoreimmunisation were obtained rom these participants andthose rom
another township to establish the baselineconcentration o hepatitis
E virus IgG and or assessmento immunogenicity (immunogenicity
subset). Fingerprintscanners and digital photographs were used to
identiyand track participants throughout immunisation,
bloodcollection, and ollow-up.
Hepatitis surveillanceParticipants with suspected hepatitis were
identiedthrough an established active hepatitis surveillancesystem
comprising 205 sentinels, including162 community clinics, 30
private clinics, 11 centralhospitals located in the townships, and
two centralhospitals in the city o Dongtai (webappendix p 32).
Acase o hepatitis was dened as a patient presentingwith
constitutional symptoms such as atigue, loss oappetite, or both or
longer than 3 days with alanineaminotranserase (ALT) exceeding
25-times the upperlimit o normal range. Patients with abnormal
concentrations o ALT were tested at rst presentationby JSCDC or
hepatitis A virus IgM, surace antigen ohepatitis B virus, hepatitis
B virus core protein IgM,hepatitis C virus immunoglobulin, and
hepatitis E virusIgM. Paired serum samples were obtained rom
thesepatients at the t ime o presentation and 26 weeks later.Serial
samples were sent to the NICPBP to test orhepatitis E virus IgM and
IgG, hepatitis E virus RNA,and hepatitis A virus IgM. The DSMB
reviewed theclinical and laboratory results and conrmed
thediagnoses o hepatitis E beore unblinding. To bedened as an acute
hepatitis E patient, a participantneeded to ull three conditions:
acute illness lastingor at least 3 days; abnormal serum ALT
concentration25-times the upper limit o normal range or
greater;
and positive hepatitis E virus IgM and RNA, 4-timesincrease in
hepatitis E virus IgG, or both.
Laboratory measurementsThe tests or hepatitis E virus IgM were
done by use o twocommercial assays in parallel (Beijing Wantai,
Beijing,China; MP Biomedicals, Singapore).11,2025 The assay
orhepatitis E virus IgG used antigen more truncated thanthat in the
vaccine antigen (Beijing Wantai, China).20,21Hepatitis E virus IgGs
were urther quantied andexpressed in WHO units per mL(Wu/mL;
webappendix p 2).The lower limit o hepatitis E virus IgG
quantication was
0077 Wu/mL.26 For the analysis, the antibody concentrationin
samples negative or hepatitis E virus IgG were arbitrarilyset at
00385 Wu/mL. Serum samples o patients withdetectable hepatitis E
virus IgM or a two times or greaterrise o hepatitis E virus IgG
concentration in paired sampleswere tested or hepatitis E virus
RNA.27 Serum sampleswere taken beore the rst vaccine dose and 1
month aterthe third dose rom participants in the
immunogenicitysubset to establish concentration o hepatitis E virus
IgG.Antibody concentration o 0077 Wu/mL or greater wasdeemed to be
a positive nding. Antibody response wasdened as a greater than
our-times increase o hepatitis Evirus IgG in an individuals paired
sera. All reagents weresupplied by Beijing Wantai Biological
Pharmacy Enterprise,Beijing, China.
Vaccine group Placebo group
Randomised participants* 56 302 56 302
Men 24 511 (435%) 24 567 (436%)
Age (years) 4414 (1140) 4413 (1140)
Age group (years)
1620 2520 (4%) 2480 (4%)
2130 4598 (8%) 4653 (8%)
3140 12 684 (23%) 12 688 (23%)
4150 18 292 (32%) 18 310 (33%)
5160 14 644 (26%) 14 657 (26%)
6165 3564 (6%) 3514 (6%)
Per-protocol population (three doses) 48 693 48 663
Male to emale ratio 074 074
Mean age (years) 4472, SD 1109 4468, SD 1110
Immunogenicity subset 5567 5598
Male to emale ratio 064 065
Mean age (years) 4522 (1075) 4525 (1082)
Anti-HEV prevalence 4776% (46444909) 4691% (45604823)
GMC (Wu/mL) 014 (013014) 013 (013014)
Reactogenicity subset 1316 1329
Men 524 (398%) 561 (422%)
Age (years) 4470, SD 1123 4493, SD 1110
Data are number (%), mean (SD), or mean (95% CI). HEV=hepatitis
E virus. GMC=geometric mean concentration. *All
randomised participants who received at least one dose o vaccine
or placebo. Per-protocol population denotes all
randomised participants who received three doses o vaccine or
placebo. Participants in the immunogenicity subset
were rom two townships additionally investigated or antibody
response to vaccination. Participants in the
reactogenicity subset were rom one township visited regularly at
home by investigators to assess adverse events.
Table 1: Baseline characteristics o participants
-
8/9/2019 Vacuna VHE 3ra fase
4/10
Articles
4 www.thelancet.com Published online August 23, 2010
DOI:10.1016/S0140-6736(10)61030-6
Adverse eventsAter each dose, participants were observed or 30
min orimmediate adverse reactions. Participants in
thereactogenicity subset were visited at home by investigatorsat 6
h, 24 h, 48 h, 72 h, 7 days, 14 days, and 28 days atereach dose,
and observed or reported adverse eects, iany, were recorded on
saety diary cards. Other participants
were asked to report any adverse events to nearby clinics
within 1 month ater each dose. Additionally,
investigatorsreviewed all records o admission to hospital and death
toidentiy trial participants. Any serious adverse eventswere
recorded throughout the study by use o the MedicalDictionary or
Regulatory Activities (version 12.0).
Statistical analysisWe estimated that the incidence o hepatitis
E or adultsaged 1665 years would be about our cases per10 000
person-years (webappendix p 1). On the assumptiono a vaccine ecacy
o 70%, a two-group continuity-corrected test with a one-sided
signicance level o005 would have a power o 80% to detect a dierence
inincidence with 41 277 participants per group. To
compensate or dropouts, 50 000 participants per groupwere
needed.
Prespecied outcome analyses were done in eligibleparticipants
who had received at least one dose o eithervaccine, and in those
who received all o the three doseso the vaccines. The primary
endpoint was prevention ohepatitis E in participants who received
three doses ovaccine (ie, the per-protocol population) during the12
months rom the 31st day ater receipt o the thirddose. Vaccine ecacy
and 95% CIs were calculated onthe basis o the identied dierence
between the vaccinegroup and the placebo group and the accrued
person-time. An exact conditional procedure was used to
evaluatevaccine ecacy under the assumption that the numberso
patients with hepatitis E in the vaccine and placebogroups were
independent Poisson random variables.28For robustness, ecacy was
also assessed by use o a Coxproportional hazard model, and a
log-rank test was usedto compare the cumulative incidence o
hepatitis Ebetween the study groups.
Adverse events were summarised or all vaccinationvisits as
requencies and percentages according to studygroup. Proportions o
events and 95% CIs (unadjustedor multiplicity) were compared
between the groups byuse o two-sided Fishers exact test.
Data analysis was done with SAS sotware version 9.1.All reported
p values are two-sided with an value
o 005.
Role o the unding sourceThe sponsor o the study had no role in
study design,data collection, data analysis, data interpretation,
orwriting o the report. The corresponding author had ullaccess to
all the data in the study and had nalresponsibility or the decision
to submit or publication.
Results122 179 people rom 11 townships attended the
enrolmentvisit between August and October, 2007. 112
604participants ullled the eligibility requirements, wererandomly
assigned to the study group, and received atleast one dose o
vaccine or placebo. 97 356 participants
For more on the Medical
Dictionary for Regulatory
Activities see http://www.
meddramsso.com/
9812 fatigue or loss of appetite 3 days
4931 vaccine group4881 placebo group
Determined by DSMB
23 confirmed hepatitis E1 vaccine group, onset 719 months
22 placebo group (one onset 015months, five onset 156 months,and
16 onset 719 months)
200 not hepatitis E103 vaccine group
97 placebo group
223 ALT 25 ULN104 vaccine group119 placebo group
15 hepatitis E in per-protocol cohort0 vaccine group
15 placebo group
55 had at least one of three acuteHEV infectious markers:
HEV-IgM,
rising HEV-IgG, or HEV-RNA28 vaccine group27 placebo group
145 had none of three acuteHEV infectious markers:HEV-IgM,
rising HEV-IgG,or HEV-RNA75 vaccine group70 placebo group
46 did not meet with the definitionof hepatitis E25 vaccine
group
5 with rising IgG only20 with IgM only
21 placebo group3 with rising IgG only
18 with IgM only
9 met the definition of hepatitis E,
but were excluded from theconfirmed hepatitis E by the
DSMBbefore unblinding according to theirclinical and laboratory
profiles3 vaccine group
1 in per-protocol group2 received one dose
6 placebo group
3 in per-protocol group1 received two doses
2 received three doses but onsetbefore the third dose
34 non-E viral hepatitis16 hepatitis A
9 vaccine group7 placebo group
16 acute hepatitis B8 vaccine group8 placebo group
2 hepatitis C1 vaccine group1 placebo group
166 without acute viral hepatitismarkers85 vaccine group81
placebo group
Figure 2: Flowchart o surveillance and certication o acute
hepatitis E
Sentinel hepatitis surveillance system was set up to monitor
study participants or development o acute hepatitis
(webappendix p 32). A case o acute hepatitis was dened as a
participant who presented with constitutional
signs, such as atigue, nausea or at least 3 days, and alanine
aminotranserase (ALT) exceeding 25-times the
upper limit o normal range (ULN). Clinical and laboratory ndings
were assessed by an independent data and
saety monitoring board (DSMB). The DSMB reviewed clinical and
laboratory data to conrm the diagnosis o
hepatitis E beore the group assignment o trial participants was
broken. HEV=hepatitis E virus.
-
8/9/2019 Vacuna VHE 3ra fase
5/10
Articles
www.thelancet.com Published online August 23, 2010
DOI:10.1016/S0140-6736(10)61030-6 5
received all three doses o vaccine or placebo and wereincluded
in the analysis o the primary endpoint(gure 1). Table 1 shows the
baseline characteristics ostudy participants.
The DSMB conrmed 23 cases o hepatitis E beoreunblinding (gure
2); details o each case are listed inwebappendix pp 424. Compared
with the general studypopulation, patients with hepatitis E were
older (mean513 years, SD 82; median 53, range 3663) and morelikely
to be men (male-to-emale ratio 23). The meanmaximum serum ALT
concentration o patients withhepatitis E was 308-times upper limit
o normal range(SD 293; 181, 25969), and the mean duration oillness
was 571 days (SD 398; 41, 9175). 15 patientswere admitted to
hospital or a mean o 244 days(SD 145; 20, 966). All 23 patients
tested positive or
hepatitis E virus IgM, 22 were positive or hepatitis Evirus RNA,
and 14 had a 4-times or greater increase inhepatitis E virus IgG. O
the 13 patients whose viruseswere isolated or sequencing, 12 had
genotype 4 and onehad genotype 1. O the eight patients who received
allthree doses and whose viruses underwent sequencing,all had
genotype 4.
In the primary analysis population 15 participantsdeveloped
hepatitis E during the 12 months rom the 31stday ater receipt o the
third dose; all 15 were in theplacebo group (table 2). Vaccine
ecacy againsthepatitis E was 1000% (95% CI 7211000), andprotection
extended to all participants throughout the12 months. Five
participants developed hepatitis E duringthe 14 days ater the
second dose and beore the third
dose; all were in the placebo group. Vaccine ecacy atertwo doses
was 1000% (911000).
Most randomised participants who received at least onedose o
vaccine or placebo were ollowed up or 19 monthsrom the beginning o
the study, and a small proportion oparticipants were ollowed up rom
month 7 o the study.There were 23 cases o hepatitis E during the
ollow-up,one in the vaccine group (the participant received one
Follow-up
(month ostudy)
Vaccine group Placebo group Vaccine ecacy
(95% CI)
p value
Number o
participants/
person-years at risk
Number
o cases
Incidence
(per 10 000
person-years)
Number o
participants/
person-years at risk
Number
o cases
Incidence
(per 10 000
person-years)
Per-protocol
Whole group (three doses) 719 48 693/48 5946 0 00 48 663/48 5551
15 31 1000% (7211000)
-
8/9/2019 Vacuna VHE 3ra fase
6/10
Articles
6 www.thelancet.com Published online August 23, 2010
DOI:10.1016/S0140-6736(10)61030-6
dose o the vaccine) and 22 in the placebo group (table
2).Vaccine ecacy or participants who received at least onedose was
955% (95% CI 663994). There were 17 caseso hepatitis E during the
12 months rom the 31st day aterthe receipt o the nal dose (which
could be the rst,second, or third dose), one in the vaccine group,
and 16 in
the placebo group. The corresponding vaccine ecacywas 938% (95%
CI 598999%).
Figure 3 shows the cumulative incidence o hepatitis Ein
participants who were ollowed up or 19 months romthe beginning o
the study. The dierence betweenthe vaccine group and the placebo
group wassignicant (p
-
8/9/2019 Vacuna VHE 3ra fase
7/10
Articles
www.thelancet.com Published online August 23, 2010
DOI:10.1016/S0140-6736(10)61030-6 7
ticipants in the placebo group showed an antibodyresponse and
all the episodes were subclinical inection.
DiscussionIn our trial, ecacy o recombinant hepatitis E
vaccineduring the 12 months rom the 31st day ater the receipto the
third dose was 1000% (95% CI 7211000), andprotection was noted
across all age and sex subgroups.Vaccination was also benecial
under less than perectcircumstancesie, when participants did not
receive allthree doses. Vaccine ecacy ater two doses was 1000%
(95% CI 911000). Thereore, during a hepatitis Eoutbreak, or or
travellers to an endemic area, protectioncan be quickly obtained by
two vaccine doses givenwithin 1 month.
Side-eects were ew and mild and no serious adverseevents related
to vaccination. HEV 239 is unlikely toinduce rare vaccine-related
serious adverse events,because the large number o participants in
the studyaords a power o 85% to detect rare serious adverseevents i
the rate in the vaccine group is 003% and therate ratio is 50
(webappendix p 29).
The study site is endemic or inection with hepatitis Evirus,
with nearly hal the participants tested on day 0being seropositive.
The inection rate in the placebogroup was 21% during the period rom
0 months to
7 months. However, most o the inections seemed to besubclinical
and incidence o hepatitis E was estimated tobe about our per 10 000
person-years (webappendix p 1).The reason or the low attack rate is
unknown. Indeveloped countries where the zoonotic hepatitis
Egenotype 3 predominates, emerging data showed amoderate hepatitis
E virus seroprevalence but rareautochthonous cases o hepatitis E.3
These ndingssuggest that the low attack rate might be a
commoneature o both zoonotic genotypes, relating to a low-level,but
nevertheless widespread, exposure in areas where
these viruses are prevalent.Animal studies showed that HEV 239,
which is
produced with a genotype 1 isolate, coners protectionagainst
both genotypes 1 and 4.19 12 o 13 patients withhepatitis E who were
typed by sequencing, had genotype 4,all in the placebo group.
Thereore, our study substantiatesthat the vaccine cross protects
against genotype 4 inhuman beings, and the cross protection
probably extendsto other genotypes as well, given that they belong
to thesame serotype as the vaccine strain.
Data suggest that individuals with chronic liver diseaseshould
be prioritised or hepatitis E vaccination to preventserious damage
rom inection.8,9 However, because weexcluded this group, additional
study is needed to assessthe benets o HEV 239. Another limitation
was the lack
Number o adverse events (rate, 95% CI) p value*
Vaccine group Placebo group
(Continued rom previous page)
Total vaccinated cohort
Number o participants who received more than one dose 56 302 56
302
Unsolicited events within 30 days ater each dose
All 6771 (120%, 1176123) 6724 (119%, 11681221) 0666
Grade 3 839 (15%, 139159) 792 (14%, 131151) 0241
Serious adverse events within 30 days ater each dose
All 248 (04%, 039050) 245 (04%, 038049) 0892
Admission to hospital 238 (04%, 037048) 233 (04%, 036047)
0817
Disability 0 (00%, 000001) 0 (00%, 000001)
Death 10 (00%, 001003) 12 (00%, 001004) 0670
Serious adverse events during period rom month 2 to month 6
and
rom month 7 to month 19
All 1423 (25%, 240266) 1430 (25%, 241267) 0894
Admission to hospital 1328 (24%, 223249) 1336 (24%, 225250)
0875
Disability 0 (00%, 000001) 0 (00%, 000001)
Death 95 (02%, 014021) 94 (02%, 013020) 0942
Grade 3 pain, headache, and atigue were dened as prevention o
normal activities; grade 3 swelling was dened as a diameter o more
than 30 mm; grade 3 itch was
dened as body itch; and grade 3 ever was dened as temperature
greater than 390C. Symptoms with requency more than 1% in any group
are listed. The webappendix
details all serious adverse events ( pp 2528). *p values are
two-sided and were calculated by Fishers exact test. Unsolicited
adverse events included any adverse events that
happened rom day 4 to day 30 ater each dose and any adverse
events within 3 days ater each dose but had not been listed in the
diary card or registering solicited adverse
events. Most oten unsolicited adverse events in the study
included upper respiratory tract inection, headache, ever, and
gastritis. The data and saety monitoring board
did not deem any o the serious adverse events to be related to
vaccination. 22 participants died within 30 days ater each
vaccination. O the ten participants in the vaccine
group that died, eight died as the result o an accident, one
died o a cerebral haemorrhage, and one died o liver cancer ater 10
years with chronic hepatitis B.
O 12 participants in the placebo group that died, six died as
the result o an accident, three died o myocardial inarction, two
died o cerebral haemorrhage, and one died o
stomach cancer.
Table 3: Saety outcomes
-
8/9/2019 Vacuna VHE 3ra fase
8/10
Articles
8 www.thelancet.com Published online August 23, 2010
DOI:10.1016/S0140-6736(10)61030-6
o a hepatitis E case in the vaccine group, meaning that
the protective antibody concentration could not beassessed.
Further analysis o our serology data mightprovide important
inormation on the vaccines ecacyagainst subclinical inection. Both
our study and theprevious phase 2 study o the vaccine produced in
insectcells showed substantial short-term protection; however,the
duration o this protection needs urther assessment.
In our trial, we ound the vaccine well tolerated andecacious or
a general adult population. Further studiesare needed to assess the
saety and to support the benetso the vaccine or pregnant women and
or peopleyounger than 15 years or older than 65 years.
Contributors
All authors contributed towards acquisition o data or
statistical analyses,
or interpretation o data, writing and revising the report, and
nalapproval. F-CZ and JZ contributed equally to this work.
Hecolin study group
Field management and data collection F-C Zhu, X-F Zhang, Z-Z
Wang,H Wang, C-L Yang, H-M Jiang, J-P Cai, Y-J Wang, X Ai, Y-M Hu,
Q Tang,L Li, H-X Pan, W-Z Zhou, F-Y Meng, W-M Dai, Y Wu, Y-J Zhang,
X Huo,J-L Hu, Q Liang, S-X Xiu, J Xu, R-J Jiang, Y-Z Chen, H-Q
Zhang,H-M Gao, Y-S Chen, Y-P Yuan, L Chen, Y-G Zhou, Y Jing
(JiangsuProvincial Centre or Disease Control and Prevention,
Nanjing, China).Laboratory contribution C Zhou, X Yao (National
Institute or the Controlo Pharmaceuticals and Biological Products,
Beijing, China). Statisticalanalysis Y-H Wang, X-Y Kong, P-C Hu,
Y-J Yu (PPD-Excel, Beijing,China); P Liu, J-X Li (Southeast
University, Nanjing, China). Medicalwriting (protocol and article)
J Zhang, S-J Huang, M-H Ng, JW-K Shih,Y-M Li, Y Xiang, Q Yan, T Wu,
J-J Di, J Miao, N-S Xia (Xiamen University,Xiamen, China); F-C Zhu,
X-F Zhang (Jiangsu Provincial Centre orDisease Control and
Prevention, Nanjing, China). Data and safetymonitoring committee F
Chen (Nanjing Medical University, Nanjing,China), F-B Tao (Anhui
Medical University, Heei, China), L-D Diao(Consultant board o
vaccination or Ministry o Health, China), D-Y Tian(Tongji Hospital,
Huazhong University o Science and Technology,Wuhan, China), J-J
Jiang (The First Aliated Hospital o Fujian MedicalUniversity,
Fujian, China).
Conficts o interest
Y-LX and Y-ML are employees o the Xiamen Innovax. The other
authorsdeclare that they have no conficts o interest.
Acknowledgments
We thank the volunteers or their participation in this clinical
study andRobert H Purcell o the National Institute o Allergy and
InectiousDiseases, National Institutes o Health (Bethesda, MD, USA)
or hisvaluable suggestions and input. This trial was unded by
multiplegrants rom the Chinese Government: Chinese National
High-techR&D Programme (863 programme; 2006AA02A209 and
2005DFA30820); Chinese National Key Technologies R&D
Programme(2009ZX10004-704); Chinese National Science Fund or
DistinguishedYoung Scholars (30925030); Fujian Provincial
Department o Sciencesand Technology (2004YZ01); Xiamen Science and
Technology Bureau(3502Z20041008); and Fujian Provincial Science
Fund orDistinguished Young Scholars (2009J06020).
Reerences1 Labrique AB, Thomas DL, Stoszek SK, Nelson KE.
Hepatitis E:
an emerging inectious disease. Epidemiol Rev1999; 21: 16279.
2 Purcell RH, Emerson SU. Prevention. In: Thomas HC, Lemon
S,Zuckerman AJ, eds. Viral hepatitis, 3rd edn. Malden, MA:Blackwell
Publishing, 2005: 63545.
3 Dalton HR, Bendall R, Ijaz S, Banks M. Hepatitis E: an
emerginginection in developed countries. Lancet Infect Dis 2008; 8:
698709.
4 Krawczynski K, Aggarwal R, Kamili S. Epidemiology, clinical
andpathologic eatures, diagnosis, and experimental models.
In:Thomas HC, Lemon S, Zuckerman AJ, eds. Viral hepatitis, 3rd
edn.Malden, MA: Blackwell Publishing, 2005: 62434.
5 Emerson SU, Purcell RH. Hepatitis E virus. Rev Med
Virol2003;13: 14554.
6 Khuroo MS, Teli MR, Skidmore S, So MA, Khuroo MI. Incidenceand
severity o viral hepatitis in pregnancy. Am J Med1981;70:
25255.
7 Khuroo MS, Kamili S. Aetiology, clinical course and outcome
osporadic acute viral hepatitis in pregnancy.J Viral Hepat2003;10:
6169.
8 Kumar Acharya S, Kumar Sharma P, Singh R, et al. Hepatitis
Evirus (HEV) inection in patients with cirrhosis is associated
withrapid decompensation and death.J Hepatol2007; 46: 38794.
9 Hamid SS, Atiq M, Shehzad F, et al. Hepatitis E
virussuperinection in patients with chronic liver disease.
Hepatology2002; 36: 47478.
10 FitzSimons D, Hendrickx G, Vorsters A, Van Damme P. Hepatitis
Aand E: update on prevention and epidemiology. Vaccine 2010;28:
58388.
11 Teshale EH, Howard CM, Grytdal SP, et al. Hepatitis E
epidemic,Uganda. Emerg Infect Dis 2010; 16: 12629.
12 Emerson S, Anderson D, Arankalle A, et al. Hepevirus.
In:Fauquet CM, Mayo MA, Manilo J, Desselberger U, Ball LA,
eds.Virus taxonomy: eighth report o the international committee
ontaxonomy o viruses. London: Elsevier Academic Press;2004:
85357.
13 Purcell RH, Emerson SU. Hepatitis E: an emerging awarenesso
an old disease.J Hepatol2008; 48: 494503.
14 Lu L, Li C, Hagedorn CH. Phylogenetic analysis o
globalhepatitis E virus sequences: genetic diversity, subtypes
andzoonosis. Rev Med Virol2006; 16: 536.
15 Pavio N, Renou C, Di Liberto G, Boutrouille A, Eloit M.
Hepatitis E:a curious zoonosis. Front Biosci 2008; 13: 717283.
16 Worm HC, Wirnsberger G. Hepatitis E vaccines: progressand
prospects. Drugs 2004; 64: 151731.
17 Shrestha MP, Scott RM, Joshi DM, et al. Saety and ecacy o
arecombinant hepatitis E vaccine. N Engl J Med2007; 356:
895903.
18 Zhang J, Liu CB, Li RC, et al. Randomized-controlled phase
IIclinical trial o a bacterially expressed recombinant hepatitis
E
vaccine. Vaccine 2009; 27: 186974.19 Li SW, Zhang J, Li YM, et
al. A bacterially expressed particulate
hepatitis E vaccine: antigenicity, immunogenicity and
protectivityon primates. Vaccine 2005; 23: 2893901.
20 Zhang J, Ge SX, Huang GY, et al. Evaluation o antibody-based
andnucleic acid-based assays or diagnosis o hepatitis E virus
inectionin a rhesus monkey model.J Med Virol2003; 71: 51826.
21 Bendall R, Ellis V, Ijaz S, Thurairajah P, Dalton HR.
Serologicalresponse to hepatitis E virus genotype 3 inection: IgG
quantitation,avidity, and IgM response.J Med Virol2008; 80:
95101.
22 Dalton HR, Hazeldine S, Banks M, et al. Locally
acquiredhepatitis E in chronic liver disease. Lancet2007; 369:
1260.
23 Dalton HR, Bendall RP, Keane FE, et al. Persistent carriage
ohepatitis E virus in patients with HIV inection. N Engl J
Med2009;361: 102527.
24 Said B, Ijaz S, Kaatos G, et al. Hepatitis E outbreak on
cruise ship.Emerg Infect Dis 2009; 15: 173844.
25 Chen HY, Lu Y, Howard T, et al. Comparison o a
newimmunochromatographic test to enzyme-linked immunosorbentassay
or rapid detection o immunoglobulin M antibodies tohepatitis E
virus in human sera. Clin Diagn Lab Immunol2005;12: 59398.
26 Zhou C, Huang WJ, Yao X, et al. Evaluation o the diagnostic
kitsor hepatitis E and establishment o a quantication method
ordetecting anti-HEV IgG. Chin J Microbiol Immunol2009; 29:
85457.
27 Li RC, Ge SX, Li YP, et al. Seroprevalence o hepatitis E
virusinection, rural southern Peoples Republic o China.Emerg Infect
Dis 2006; 12: 168288.
28 Chan I, Bohidar N. Exact power and sample size or vaccine
ecacystudies. Commun Stat Theory Methods 1998; 27: 130522.
-
8/9/2019 Vacuna VHE 3ra fase
9/10
Comment
www.thelancet.com Published online August 23, 2010
DOI:10.1016/S0140-6736(10)61260-3 1
Hepatitis E vaccine: not a moment too soon
Hepatitis E virus (HEV) remains one o the least
understood and perplexing viruses pathogenic to
human beings. From 5% to 20% o people in developed
countries show a steady increase in the titre o anti-HEV
IgG with increasing age,1 but inection with the prevalent
genotype in Europe and the USA, genotype 3, rarely
results in symptoms. Although this genotype has been
recovered rom eral and domestic pigsand sometimes
rom people who have eaten raw pork or oal
convincing epidemiological evidence that this zoonotic
reservoir is the source o most human exposures orinections
remains elusive.2
Unlike the situation in developed countries, HEV
inection with genotypes 1, 2, and 4, which predominate
in developing countries, is not merely an academic
quandary but a major cause o disease and death. Some
areas o east and south Asia are highly endemic or the
virus. Large outbreaks (tens o thousands o cases) have
occurred in India3,4 and China5,6 since 1955; these were
deemed to have been waterborne. More recently there
have been very large outbreaks in southern Sudan7 and
nearby northern Uganda,8
in what seem to be susceptibleArican populations in which HEV
outbreaks had not
previously been recorded. In these outbreaks, the testing
o drinking water rom wells did not reveal the virus or
coliorms, and continued provision o clean water did
not prevent additional inections. Several other lines
o evidence suggest that some o these outbreaks are
attributable to person-to-person transmission.9
Whatever the source, these outbreaks have typically
extended over many months with especially high
mortality in pregnant women and inants younger than
2 years, oten with case-atality rates o 1025%. In
view o the protracted nature o the epidemics and the
associated substantial morbidity and mortality, the need
or public health interventions to interrupt transmission
has been urgent. Unortunately, interventions ocused
on basic sanitationeg, latrine-digging, education on
hand-washing and provision o soap, and guarding
unprotected surace water rom usehave not
noticeably reduced these outbreaks. Thus it is natural to
wonder whether vaccination would be eective in these
epidemic or highly endemic situations.
The approach to vaccine-antigen production has been
to ocus on the ORF 2 capsid protein-producing section
o the HEV genome, the same capsid antigen as used
or enzyme immunoassays or detection o the virus.
A recombinant vaccine produced in insect cells by the
US Army with GlaxoSmithKline Biologicals (Rixensart,
Belgium) was sae and eective when given to almost
900 young Nepalese Army recruits,10 but there are neither
plans or urther studies nor, apparently, or eventual
commercial production o this vaccine. An earlier phase 2
trial11 o the bacterial recombinant vaccine described by
Zhu and colleagues12 in the The Lancet today was used in
457 healthy Chinese adults and 155 high-school studentsand
seemed to coner protection, although inection was
deduced rom asymptomatic seroconversion or rise in
antibody titres and not by virological testing.
Thus the report by Zhu and colleagues12 o a successul
phase 3 study o this vaccine is an important event in the
prevention and control o hepatitis E. The numbers o
recipients o the vaccine (48 693) and placebo (hepatitis B
vaccine, 48 663) in the primary analysis o this study were
suciently large, and the number o people (15) inected
with HEV in the placebo group, conrmed by testing
or HEV-RNA, is convincing and credible about thevaccines ecacy
(100%, 95% CI 7211000) and saety.
To assess vaccine saety and ecacy in populations most
at risk o serious HEV-associated disease and death,
uture researchers will need to include pregnant women
and young inants. Also, the duration o protection
aorded by this vaccine remains unknown. Still, the
Published Online
August 23, 2010
DOI:10.1016/S0140-
6736(10)61260-3
See Online/Articles
DOI:10.1016/S0140-
6736(10)61030-6
Coloured transmission electron micrograph of hepatitis E virus
particles (purple)
Science
PhotoL
ibrary
-
8/9/2019 Vacuna VHE 3ra fase
10/10
Comment
2 www thelancet com Published online August 23 2010 DOI:10
1016/S0140-6736(10)61260-3
recorded 100% vaccine ecacy in recipients o two
vaccinations a month apart suggests that HEV vaccinecan be an
important component in outbreak control.
In highly endemic regions, a sae and eective vaccine
(i aordable) raises the prospect o routine HEV
vaccination to reduce both sporadic and epidemic HEV.
Because these considerations are crucial to decisions
on vaccine production, nancing, and immunisation
policies, public health and industry leaders should
immediately begin work to dene the public health roles
or an HEV vaccine.
Vaccines should never be a substitute or, or reason
to delay, basic improvements in overall sanitation.However, in
view o the slow rate o improvement o
sanitary conditions in many areas o Asia and Arica, this
vaccine might be our best new stopgap in the eort to
control the scourge o HEV in many parts o the world.
Scott D HolmbergDivision o Viral Hepatitis, National Center or
HIV, Hepatitis,
TB and STD Prevention, Centers or Disease Control and
Prevention, Atlanta, GA 30333, USA
[email protected]
I declare that I have no conficts o interest.
1 Kuniholm MH, Purcell RH, McQuillan GM, Engle RE, Wasley A,
Nelson KE.Epidemiology o hepatitis E in the United States: results
rom the ThirdNational Health and Nutrition Examination Survey,
19881994.J Infect Dis2009; 200: 4856.
2 Teshale EH, Hu DJ, Holmberg SD. The two aces o hepatitis E
virus.Clin Infect Dis 2010; 51: 32834.
3 Viswanathan R. Inectious hepatitis in Delhi (195556): a
critical study;epidemiology. Indian J Med Res 1957; 45: 4958.
4 Naik SR, Aggarwal R, Salunke PN, Mehrotra NN. A large
waterborne viralhepatitis E epidemic in Kanpur, India. Bull World
Health Organ 1992;70: 597604.
5 Zhang H, Cao XY, Liu CB, et al. Epidemiology o hepatitis E in
China.Gastroenterol Jpn 1991; 26: 13538.
6 Bi SL, Purdy MA, McCaustland KA, Margolis HS, Bradley DW. The
sequenceo hepatitis E virus isolated directly rom a single source
during an outbreakin China. Virus Res 1993; 28: 23347.
7 Guthmann JP, Klovstad H, Boccia D, et al. A large outbreak o
hepatitis E
among a displaced population in Darur, Sudan, 2004: the role o
watertreatment methods. Clin Infect Dis 2006; 42: 168591.
8 Teshale EH, Howard CM, Grytdal S, et al. Hepatitis E,
Uganda.Emerg Infect Dis 2010; 16: 12629.
9 Teshale EH, Grytdal SP, Howard C, et al. Evidence o
person-to-persontransmission o hepatitis E virus (HEV) during a
large outbreak in northernUganda. Clin Infect Dis 2010; 50:
100610.
10 Shresta MP, Scott RM, Joshi DM, et al. Saety and ecacy o a
recombinanthepatitis E vaccine. N Engl J Med 2007; 356: 895903.
11 Zhang J, Liu CB, Li RC, et al. Randomized-controlled phase II
clinical trial o abacterially expressed recombinant hepatitis E
vaccine. Vaccine 2009;27: 186974.
12 Zhu F-C, Zhang J, Zhang X-F, et al. Ecacy and saety o a
recombinanthepatitis E vaccine in healthy adults: a large-scale,
randomised, double-blind placebo-controlled, phase 3 trial. Lancet
2010; published onlineAug 23.
DOI:10.1016/S0140-6736(10)61030-6.























![manual_defensa_ls[3ra ed].pdf](https://img.pdfslide.us/doc/110x75/577c813c1a28abe054ac08d5/manualdefensals3ra-edpdf.jpg)



