-
Vaccination in Cancer Prevention: Cervical Cancer is Largely
Preventable,
But is Increasing Globally
Douglas R. LowyDeputy Director, National Cancer Institute
National Institutes of Health
National Academy of MedicineOctober 15, 2018
The views expressed are my own and do not necessarily reflect
those of NCI/NIH
-
Disclosures• National Institutes of Health (NIH) has patents
on
papillomavirus L1 virus-like particle (VLP) vaccine technology.
I am an inventor.
• NIH has licensed L1 VLP technology to Merck and
GlaxoSmithKline, the two companies with commercial versions of the
vaccine.
• Licensees of other NIH technologies of which I am an inventor:
GlaxoSmithKline, Sanofi, Shanta Biotech, CytosBiotech, Aura
Biosciences, Etna Biotech, Acambis, PanVax
-
Figure 1
Gastroenterology 2016 151, 472-480.e1DOI:
(10.1053/j.gastro.2016.05.048)
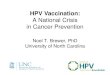
Hepatitis B Virus vaccination can reduce liver cancer risk, but
high impact takes many years
From Chang et al, Gastroenterology 2016
• Universal HPV vaccination at birth begun in Taiwan in 1986•
Very long interval between infection and development of cancer
PresenterPresentation NotesComparison of the incidence rates for
HCC and incidence rate ratios (95% CI) by age for birth cohorts
born before vs after the start of the universal HBV vaccination
program. There is a significant reduction in the incidence of HCC
in vaccinated birth cohorts in all age groups between 6 and 26
years old.
-
The paradox of cervical cancer: a largely preventable cancer
that globally is still common
• A cancer that disproportionally affects women from poor
countries & poor women
• Current high quality cervical cancer screening and HPV
vaccination need to become more cost-effective for their widespread
dissemination to less developed regions of the world
-
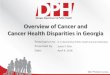
Cervical cancer mortality rates will continue to increase in
less developed regions of the world
Projections developed from Globocan 2012
CRPV
100,000
200,000
300,000
400,000
230,000
0
2015 2012
Less developedregions
251,000
363,000
More developed regions
36,000 37,000 41,000
2030 Less developed regions: Where ~90% of worldwide cervical
cancer deaths occur; where cervical cancer accounts for ~10% of
female cancer deaths; where cervical cancer represents ~90% of
HPV-associated cancer
-
Global control of cervical cancer and other HPV-associated
cancers should soon be feasible
• Research for vaccination and screening is likely to lead to
changes in standard of care with increased cost-effectiveness in
the near future
• Once that point has been reached, resources are needed to
widely implement the interventions; there may be sufficient global
commitment to marshal these resources
-
Precancer = Cervical Intraepithelial Neoplasia Grade 3Lehtinen
Lancet Oncol 2011; Munoz JNCI 2010; Huh Lancet 2017
First successful vaccines against a local sexually transmitted
infection2016: 9-valent vaccine approved for 2 doses for 9-14 year
olds
High efficacy of HPV L1 VLP vaccines against new cervical
precancer and genital warts by vaccine-targeted types in randomized
trials
End Point Sex Age Vaccine Targeted HPV Types Efficacy(95%
CI)
Precancer Female 15-26 Quadrivalent / GardasilHPV 6, 11, 16, 18
100%
(85.5-100)
GenitalWarts Female 15-26
Quadrivalent / Gardasil HPV 6, 11, 16, 18
96.4% (91.4-98.4)
Precancer Female 15-25 Bivalent / Cervarix HPV 16, 18100%
(90.5-100)
Precancer Female 16-26 Nonavalent / Gardasil-9HPV 6, 11, 16, 18,
31, 33, 45, 52, 58
97.1%(83.5-99.9)
In women with no genital HPV infection detected in at the start
of each trial
PresenterPresentation NotesThe important point here is that the
vaccines have very high efficacy if the analysis is restricted to
protection disease caused from new infection by vaccine-targeted
types. The vaccines have limited prophylactic activity against
other HPV types and don’t induce lesion regression. The mostly
likely explanation for the the somewhat lower efficacy in men is
that it is easier miss pre-existing infections of the maie
genitalia.
-
Herd Immunity: Decreased incidence of genital warts in
heterosexual Australian men following female HPV vaccine
implementation in 2007
Ali et al, BMJ 2013
>30 years21-30 years
-
Trends in U.S. Vaccination Rates: Ages 13-17 YearsMMWR Vol. 67,
#33, August 24, 2018
-
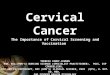
From Aimee Kreimer et al, unpublished data
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
40.0%
45.0%
3 doses 2 doses 0/6 1 dose UCG
N = 956 N = 62 N = 112 N = 1,107
HPV 16/18 HPV 31/33/45 Other HPV
The Costa Rica Vaccine Trial: Prevalent HPV infection 11 years
after bivalent HPV vaccination: One dose is not inferior to three
doses (post-hoc analysis)
0 dose
-
2 3 4 5 6 7 8 9 10 1110
100
1000
10000
HPV
16 A
ntib
ody
Geom
etric
Mea
ns (E
U/m
L)
3 doses
2 doses (0/6)
1 dose
natural Immunity
100% of HPV-vaccinated women remained HPV16 seropositive 11
years after HPV vaccination
Stable HPV seropositivity for 11 years
From Aimee Kreimer et al, unpublished data
-
Summary and Conclusions• Basic research led to identification of
HPV as the cause of
several cancers and to development of the HPV vaccines– The
vaccines can confer high protection and herd immunity
• Increased vaccine uptake in US is needed to achieve personal
protection for more individuals and greater herd immunity
• Control of cervical cancer and other HPV-associated cancers as
worldwide public health problems may soon be feasible
Slide Number 1DisclosuresSlide Number 3The paradox of cervical
cancer: a largely preventable cancer that globally is still
commonSlide Number 5Global control of cervical cancer and other
HPV-associated cancers should soon be feasible Slide Number 7Slide
Number 8Slide Number 9Slide Number 10Slide Number 11Summary and
Conclusions