Embed Size (px)
Citation preview

V
V
TRIGEMINAL NEURALGIA MAY HERALD NEUROMYELITIS OPTICA SPECTRUM DISORDERS
Gisele O. Lima, Natália C. Talim, Lívia E. C. Talim, Juliana M. S. S. Amaral, Rodrigo Kleinpaul, Márcia Prates, Carolina R. Araujo, Cristiane F. Rocha, Marco A. Lana-Peixoto.
CIEM MS Research Center, Federal University of Minas Gerais Medical School, Belo Horizonte, Brazil.
Background
Although brainstem symptoms (BSS) have been increasingly recognized as a frequent component within the neuromyelitis spectrum disorders (NMOSD), their exact frequency and time of onset are not known. The most frequent brainstem symptoms in NMOSD are incoercible nausea, vomiting and hiccups, representing involvement of the area postrema, located in the posterior aspect of the medulla oblongata. A number of other BSS have been reported, but those related to trigeminal nucleus/nerve dysfunction are rare.Herein we report a patient who presented trigeminal neuralgia 19 months prior to simultaneously developing bilateral optic neuritis and longitudinally extensive transverse myelitis. Brain MRI showed lesions which have been described as suggestive of NMOSD. To the best of our knowledge trigeminal neuralgia had not been described heralding NMOSD.
Case report
A 20-YO mulatto-female started having jolts of severe, paroxysmal and lancinating pain in her right face, most frequently located inside her right ear, or shooting from the angle of the mandible, and triggered by moving the jaw. The pain usually faded in a few seconds but the patient remained with a burned sensation in the affected area for some minutes. She had a variable number of attacks, from 2/wk to over than 10/day. She had a presumptive diagnosis of trigeminal neuralgia and was put on gabapentin with relief of the pain after three months. The family history was significant as her mother had rheumatoid arthrirtis.
Two years following the onset of the facial pain the patient simultaneously developed bilateral loss of sight, weakness and sensation disturbance in the left lower limb. The patient was treated with IV methylprednisolone for 3 days, then IV cyclophosphamide for five days followed by plasma exchange. The had a partial recovery and was then referred to our MS Center. Examination three months after the attack revealed visual acuity 20/400 OD and 20/50 OS. There was no motor deficit but touch and vibration sense were decreased in the left limbs. Brain MRI showed periependimal T2-hyperintensive lesions surrounding the third ventricles and cerebral aqueduct and edematous gadolinium-enhancing lesions in the parieto-occipital lobes. Spinal cord MRI showed a gadolinium-enhanced lesion extending from C4 to T2. CSF analysis was unrevealing. Work-up for infectious diseases, sarcoidosis and autoimmune diseases including serum indirect immunofluorescence assay for AQP4-IgG was negative. She had the diagnosis of NMO and was put on oral prednisone and azathioprine.
Conclusion
This patient meets Wingerchuk’s 2006 revised diagnostic criteria for NMO as she presented bilateral optic neuritis and longitudinally extensive transverse myelitis in addition to brain MRI which was atypical for MS. The index events of the disease, optic neuritis and transverse myelitis, however, were heralded two years previously by trigeminal neuralgia. Trigeminal neuralgia has been reported in 3% of patients with NMOSD (Kremer et al., 2013) but not preceding optic neuritis and transverse myelitis. The present report shows that NMOSD has to be included as a cause of trigeminal neuralgia occurring mainly in young individuals.
References
Wingerchuk DM, Lennon VA, Pittock SJ, Lucchinetti CF and Weinshenker BG. Revised diagnostic criteria for neuromyelitis optica. Neurology 2006; 66: 1485–1489.
Kremer L, Mealy M, Jacob A, et al. Brainstem manifestations in neuromyelitis optica: a multicenter study of 258 patients. Mult Scler, 2013.
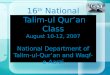
Figure 1. Brain MRI.FLAIR sequence. Periependymal hyperintense lesions in the lateral and fourth ventricles. Areas of hypointensities in the pons and medulla oblonga.
Figure 2. Spinal cord MRI showed a gadolinium-enhanced lesion extending from C4 to T2 level.