Embed Size (px)
Citation preview

UvA-DARE is a service provided by the library of the University of Amsterdam (https://dare.uva.nl)
UvA-DARE (Digital Academic Repository)
Nuchal translucency beyond Down syndrome screening
Timmerman, E.
Publication date2013
Link to publication
Citation for published version (APA):Timmerman, E. (2013). Nuchal translucency beyond Down syndrome screening.
General rightsIt is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s)and/or copyright holder(s), other than for strictly personal, individual use, unless the work is under an opencontent license (like Creative Commons).
Disclaimer/Complaints regulationsIf you believe that digital publication of certain material infringes any of your rights or (privacy) interests, pleaselet the Library know, stating your reasons. In case of a legitimate complaint, the Library will make the materialinaccessible and/or remove it from the website. Please Ask the Library: https://uba.uva.nl/en/contact, or a letterto: Library of the University of Amsterdam, Secretariat, Singel 425, 1012 WP Amsterdam, The Netherlands. Youwill be contacted as soon as possible.
Download date:21 Jul 2021

Increased nuchal translucency in euploid fetuses - what should we be telling the parents
C.M. Bilardo, E. Timmerman, E. Pajkrt and M.C. van Maarle
Prenatal Diagnosis 2010; 30: 93–102.
9Chapter
chapter 9.indd 121 22-4-2013 09:01:14

Chapter 9
122
ABSTRACT
Nuchal translucency (NT) measurement between 11 and 14 weeks’ gestation is an undisputed marker for aneuploidies. When conventional karyotyping is normal, enlarged NT is a strong marker for adverse pregnancy outcome, associated with miscarriage, intrauterine death, congenital heart defects, and numerous other structural defects and genetic syndromes. The risk of adverse outcome is proportional to the degree of NT enlargement. Although the majority of structural anomalies are amenable to ultrasound detection, unspecified genetic syndromes involving developmental delay may only emerge after birth. Concern over these prenatally undetectable conditions is a heavy burden for parents. However, following detection of enlarged NT the majority of babies with normal detailed ultrasound examination and echocardiography will have an uneventful outcome with no increased risk for developmental delay when compared to the general population. Counselling should emphasize this to help parents restore hope in normal pregnancy outcome and infant development.
proefschrif Timmerman.indb 122 18-4-2013 10:30:27

Parental counselling after enlarged NT
Chapter
9
INTRODUCTION
Although NT screening was introduced over 15 years ago, there is not yet a general consensus on how to counsel parents of a euploid fetus with enlarged NT. In an editorial published in 2001 entitled ‘Nuchal translucency in the first trimester of pregnancy: ten years on and still a pain in the neck?’ Ville 1 clearly depicts how challenging it can be to give parents realistic and correct information on the subject. The visual impact on the parents of the nuchal fluid collection seen at ultrasound examination can raise anxiety about future development and postnatal outcome 2-4. Even if this accumulation usually tends to disappear after 14 weeks, the uncertainty can persist and be exacerbated by excessively cautious or defensive counselling by the medical practitioner. This is also reflected by the fact that some couples in these circumstances request pregnancy termination even in the absence of clear fetal anomalies 5-7. In this overview of the most recent literature, the current knowledge on the association between an enlarged NT in karyotypically normal fetuses and fetal outcome will be discussed and guidelines for objective parental counselling suggested.
The test: NT measurementThere is much evidence that NT measurement alone or as part of the combined test is an excellent screening test for fetal aneuploidies 8-10. The measurement should be made between 11 and 14 weeks, with best performance obtained at 11–12 weeks 10,11 when the measurement is performed by qualified ultrasonographers undergoing regular quality assessment 12,13. Of fetuses with NT above the 95th centile, about 20–30% have a chromosomal aberration 6,14. In the presence of a normal karyotype, there remains an increased risk of adverse pregnancy outcome because of spontaneous fetal loss, isolated anomalies, and genetic syndromes 5,6,15-19. The normal range of NT measurement changes with gestational age and enlarged NT is variably defined in the literature using a fixed cut off (2.5 or 3 mm, 95th or 99th percentile) or the multiple of the median (MoM) approach 20. Whether a distinction should be made between NT and cystic hygroma in the first trimester 10,21 is questionable, and of limited clinical relevance since the management is identical 22.
Pathological associations with increased NT in euploid fetuses In euploid fetuses, the prevalence of fetal death increases exponentially with increasing NT. In the combined data from three studies reporting on a total of 4991 euploid fetuses with increased NT, the prevalence of miscarriage or fetal death increased from 1.6% in those with NT between the 95th and 99th centiles to about 20% for NT of ≥6.5 mm 5,6. However, this is likely to be an underestimation of true mortality rate, as in cases of
123
chapter 9.indd 123 22-4-2013 08:47:46

Chapter 9
deteriorating fetal hydrops up to 30% of couples decide to terminate pregnancy before intra uterine fetal death occurs 6.
Fetal death A large variety of structural anomalies and developmental disorders have been described in the setting of an enlarged NT 5. Congenital heart defects (CHDs) are predominant, followed by cleft lip and palate 6, diaphragmatic hernia 23, skeletal dysplasias 24-26, and renal anomalies. The prevalence of major abnormalities in euploid fetuses increases exponentially with NT size, from 2.5% for NT between the 95th and 99th centiles, to about 45% for an NT of ≥6.5 mm 6,18,27.
Congenital heart defects The prevalence of CHD is in the order of six times higher in fetuses with a NT ≥99th percentile than in an unselected population 28-30. There does not seem to be an association between any specific CHD and enlarged NT 31. The chance of CHD increases exponentially with increasing NT from 0.6 to 5% when the NT is between 2.5 and 3.5 mm, to 64% when it is >8.5 mm 28-30, 32-39. At present, it is not possible to draw a definitive conclusion on the role of NT measurement in screening for major CHD. The first large study on the subject reported a sensitivity of 56% for critical CHD, requiring surgical treatment 32. A subsequent meta-analysis including other seven studies 40 reported a sensitivity of 30%. In a pooled analysis of data from four large centres the same author found that a NT ≥2.5 and ≥3.5 mm was found in 35.5 and 23%, respectively, of 397 euploid fetuses with major CHD 41. Low detection rates for CHD (around 15%) are reported in studies where NT is measured in unselected or low-risk populations 42,43 and when fetuses with cystic hygromas are excluded 39. However, two recent studies, a meta-analysis of four studies and a 10-year overview of the association between nuchal fluid accumulation and CHD diagnosed at referral centres, re-evaluated the role of NT measurement in screening for CHD 44,45 and showed enhanced detection and improved neonatal outcome in duct dependent CHD, such as transposition of the great arteries 44. Study of ductus venosus (DV) flow patterns in these fetuses may improve the selection of those requiring specialized echocardiography as absent or reversed flow during the a-wave is associated with a three-fold increase in the likelihood of a major CHD 46,47. Tricuspid regurgitation (TR) at 11–13 + 6 weeks’ gestation may also play a role in identifying fetuses with CHD as those with TR have an 8-fold increased risk 48.
Genetic syndromes The list of genetic syndromes presenting with an increased NT is growing constantly (Table 1). Most of these syndromes are sporadic with prevalence in the order of 1 : 10.000 or lower, making it impossible to prove a definite association between specific syndromes and
124
chapter 9.indd 124 22-4-2013 08:47:46

Parental counselling after enlarged NT
Chapter
9increased NT. For syndromes such as Noonan, Smith-Lemli-Opitz, spinal muscular atrophy and other muscle-skeletal disorders the association with increased NT is undisputed. However, an enlarged NT is a nonspecific indicator of abnormal development, common to several different pathologic pathways 15.
Table 1. Genetic syndromes and chromosomal aberrations described in fetuses with increased NT and reported after publication of Souka’s overview (2005)
Pallister Killian syndrome 96, 97, 98
Apert syndrome 99, 100
Walker-Warburg syndrome 101
Coffin-Siris syndrome 6
Fryn’s syndrome 6 Ritscher-Schinzel syndrome 102
Split-hand/foot malformation 103
Diastrophic dysplasia 6
Spondyloepiphyseal dysplasia congenita (SEDC) 25
Cerebro-fronto-facial syndrome (Dandy-Walker variant and frontofacial dysmorphisms) 104
Chondroectodermal dysplasia (Ellis-Van Creveld syndrome) 105
Thrombocytopenia-absent-radius (TAR) syndrome 106
Cardiofaciocutaneous syndrome 107
Multiple pterygium syndrome 108 Orofaciodigital syndrome Type IV (Mohr-Majewski) 109
Arthrogryposis, renal dysfunction, cholestasis (ARC) 110
Thanatophoric dysplasia 111
Type I 112
Osteochondrodysplasia with severe osteopenia, preaxial polydactyly, clefting and dysmorphic features resembling filamin-related disorders 113
Androgen insensitivity syndrome 114
Unbalanced translocations: 115
—mono 9p24.3-pter and tri17q24.3-qter 116
—46,XY,invdup(9)(p22.1p24) [arrCGH 9p22.1p24 (RP11-130C19–>RP11- 87O1)x3] 117
—Trisomy 15q due to t(X;15) (q22.3;q11.2) translocation 118
Deletions:—Chromosome 8 deletion 6
—De novo proximal interstitial 9q deletion 68
—Six-megabase deletion of chromosome 14q = 46,XX,der[14]t[13;14][q34;q32.2] 119
—13q-syndrome 120
—Partial deletion of chromosome 6p21 (46,XX,del(6)(p21)) 121
—De novo 16p13.11 microdeletion 70 —Chromosome 5q subtelomeric deletion syndrome 122
Marker chromosome (16) (p13.1–>q12.2) 123
Trisomy 1q 124
125
chapter 9.indd 125 22-4-2013 08:47:46

Chapter 9
Neurodevelopmental delay There is still limited information on the real prevalence of neurodevelopmental delay in euploid fetuses with increased NT. Studies on large series and long term follow-up with standardized clinical evaluation of the infants are necessary to provide reliable data and prevent underestimation 5,49. Nine long-term follow-up studies have thus far reported an incidence of developmental delay varying between 0 and 8.7% (Table 2) in chromosomally and anatomically normal fetuses with increased NT. The studies are heterogeneous in cohort size, cut off used for increased NT, follow-up length and methodology. Normality was reported by questionnaire completed by parents in four studies. In five studies, all infants were examined clinically, but only two used a control group. In Senat’s paper, follow-up at the age of 2 using the Ages and Stages questionnaire filled in by 162 couples, reassuring results were reported. The incidence of developmental delay in children with enlarged NT was 1.2%, which was not statistically different when compared to a control group of 370 unselected infants 50. These results are in keeping with the incidence of developmental delay in our series: 1.6% (7/425), of which only 1/3 was not associated with ultrasound features that may have triggered suspicion (0.5%) 6. In our experience, all seven cases with developmental delay occurred in fetuses with an NT >4 mm. In only three out of seven cases syndrome recognition was possible.
Table 2. Long-term follow-up of chromosomally and anatomically normal fetuses with increased NT
Reference NT cut off
Method Control group
Age (month)
Lost (%)
Developmental delay [n (%)]
Brady (1998) 125 3.5 mm Clinical examination Yes 6–42 1 1/89 (1.1)
Van Vugt (1998) 126 3.0 mm Questionnaire No 7–75 32 1/34 (2.9)
Adekunle (1999) 127 4.0 mm Questionnaire No 13–38 26 2/23 (8.7)
Maymon (2000) 128 >p95 Questionnaire/telephone No 12–36 0 0/36 (0)
Hiippala (2001) 129 3.0 mm Clinical examination No 24–84 15 1/50 (2)
Souka (2001) 18 3.5 mm NA No — 0 4/980 (0.4)
Senat (2002) 19 4.0 mm Clinical examination No 12–72 7 3/54 (5.6)
Cheng (2004) 130 3.0 mm Clinical examination No 8–30 0 1/14 (7.1)
Senat (2007) 48 >p99 Clinical examination ASQ scores Yes 0–24 0 2/162 (1.2)
Bilardo (2007) 6 >p95 Questionnaire/telephone No 6–60 3.3 7/425 (1.6)
p95 and p99: 95th and 99th percentiles; ASQ, Ages and Stages Questionnaires; —, information not provided.
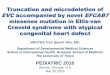
Management of euploid fetuses with increased NT A recent survey on which protocol should be used in fetuses with increased first trimester screening and normal karyotype 51 points out that increased NT should always trigger detailed assessment of fetal cardiac anatomy (Figure 1).
126
proefschrif Timmerman.indb 126 18-4-2013 10:30:27

Parental counselling after enlarged NT
Chapter
9The current consensus is that fetal echocardiography should be offered in all cases in which NT is >3.5 mm (99th percentile). The cost-effectiveness of using lower cut offs (2.5 mm, 95th centile) needs, in view of the rather low positive predictive value (PPV) (2–3%) further investigation. Our recommendation is that all cases of euploid fetuses with NT above 3.5 mm are referred to tertiary level centres for further investigations. However, if resources are available and parents are particularly anxious earlier, detailed investigations may be
Figure 1. Proposed management protocol for euploid fetuses with enlarged NT
pregnant women with NT > 3.5 mm
(99th percentile)
Normal cytogenetics
invasive diagnostics:-conventional karyotyping-storage cultured cells
13 -16 weeks of gestation:- US examination- Markers DV, TR -
18-22 weeks of gestation:- detailed US examination-fetal echocardiography
array -CGH in case of MCA and/or
MR
−examination by clinical geneticist−pathology
If indicated:examination by
clinical geneticist
PrenatalPostnatal
Birthpregnancy termination or intrauterine demise
Invasive procedures(AP, CVS)
Chromosomal aberrations
•AP: Amniocentesis•CVS: Chorionvilli sampling•MCA: multiple congenital anomalies•MR: mental retardation
Heart defect
Testing for 22q11 deletion
invasive diagnostics:-conventional karyotyping-storage cultured cells
13 -16 weeks of gestation:- US examination- Markers DV, TR - fetal echocardiography
18-22 weeks of gestation:- detailed US examination-fetal echocardiography
array -CGH in case of MCA and/or
MR
−examination by clinical geneticist
−pathology
If indicated:examination by
clinical geneticist
Birthpregnancy termination or intrauterine demise
Invasive procedures(AP, CVS)
••••
Testing for 22q11 deletion
127
proefschrif Timmerman.indb 127 18-4-2013 10:30:28

Chapter 9
offered at lesser degrees of enlargement (95th centile). Maymon et al. 20 recommend use of NT MoM of 2 or a delta NT of 1.5 as cut off for further investigations. In experienced hands and with high-resolution ultrasound equipment the majority of severe malformations, as well as major CHD, may be detected by the end of the first trimester
52-57. This enables early reassurance for most women. Where anomalies are present it allows time for additional investigations, counselling and, if appropriate, for an ‘unrushed’ decision on termination of pregnancy (TOP) at an earlier stage where emotional impact may be less 58, although this is debated 59. Some authors have proposed that, in fetuses with enlarged NT and obvious structural anomalies, TOP may be offered directly, saving the costs of karyotyping 60,61. However karyotyping is important not only to define recurrence risk, but also to help parents in the decision making process. Other first trimester screening markers can give an indication of the risk of detecting additional anomalies in euploid fetuses. For example, abnormal DV flow is associated with poor pregnancy outcome (cardiac and other anomalies, perinatal deaths) and should be regarded as an additional risk factor warranting close ultrasound surveillance 47,62,63. Infection screening should not be routinely performed 64, but it may be appropriate when NT enlargement evolves in the second trimester into an increased nuchal fold, generalized edema, or unexplained hydrops or in women with young children who have been recently ill or have been ill themselves 65,66. Additional genetic investigations in fetuses with enlarged NT and normal conventional karyotype, such as molecular testing (subtelomere MLPA and CGH microarrays) are promising techniques for identifying microscopic genomic aberrations (microdeletions, unbalanced translocations) responsible for syndromic associations including structural anomalies and mental retardation 67-70. However, as their value has not yet been investigated prospectively in large series, caution should be used in interpreting isolated findings in fetuses without structural anomalies. Screening for 22q11 deletions should only be performed in fetuses with confirmed cardiac defects 71,72. When at subsequent scans even subtle anomalies and/or dysmorphic features are found, a genetic opinion should be sought to attempt identification of a classifiable syndrome. A thorough family history, including consanguinity, should be taken to distinguish inherited syndromes (autosomal recessive or dominant) with a high recurrence risk from sporadic syndromes (featuring a de novo mutation). In our experience the latter are predominant. On occasions a careful diagnostic workup, including examination of the parents, can reveal a specific syndrome or carrier status in one of them 73. In couples known to be carriers of conditions with a high recurrence risk NT may be used as early reassurance or warning sign of likely recurrence 6,34,76,77.
128
proefschrif Timmerman.indb 128 18-4-2013 10:30:28

Parental counselling after enlarged NT
Chapter
9
How to counsel parents
Before first trimester screening Not all women undergoing first trimester screening are aware of its possibilities and limitations 76. Women should also be properly informed that first trimester screening is not only for Down syndrome, but may reveal additional risk factors for the pregnancy requiring further investigations. The amount of anxiety that this uncertainty can cause should not be underestimated 77. It is therefore mandatory that all pregnant women are properly counselled about prenatal screening 76, 78-81 and that Health systems provide guidelines to allow parents to make an informed choice regarding first trimester screening 82.
After increased NT and normal karyotype After a normal karyotype has been established the first question parents usually ask is: ‘What is now the chance of a normal pregnancy outcome?’ Based on the literature, the overall chance of adverse outcome varies substantially according to the cohort characteristics. When fetuses with increased NT are part of a cohort of unselected fetuses undergoing first trimester screening, the incidence of adverse outcome (anomalies, miscarriages, TOP and fetal and neonatal death) varies between 3% 7,27 and 6% 15. In contrast, in selected cohorts of fetuses with an enlarged NT the adverse outcome rate is about 3–6 times higher (∼20%) 5,6,83. The five largest studies published since 2000 comprise a total of 2271 fetuses and report a mean incidence of 10.6% (range 2.1–26%) for isolated structural anomalies and 4.4% (0.5–6.4%) for genetic disorders detected before birth with an additional 2.5% (2.2–6.6%) of anomalies detected after birth 6,18,19,27 (Table 3). However, these studies are difficult to compare 20 due to differences in populations, definitions of NT enlargement (3 mm, 95th centile, 99th
Table 3. Largest studies published after 2000 reporting on structural anomalies and genetic disorders detected in fetuses with enlarged nuchal translucency and percentage of anomalies only detected after birth.
Euploid fetuses (n)
NT (mm) Structural anomalies
Genetic disorders
Anomalies detected after birth
Mangione (2001) 131 202 ≥3.0 mm 23/202 (11.4%) 1/202 (0.5%) —
Souka (2001) 18 1320 ≥3.5 mm 162/1320 (12.3%) 44/1320 (3.3%) 22/980 (2.2%)
Michailidis (2001) 27 235 ≥P95 5/235 (2.1%) — —
Senat (2002) 19 89 ≥4 mm 23/89 (25.8%) 4/62 (6.4%) 4/62 (6.5%)
Bilardo (2007) 6 425 ≥P95 27/425 (6.3%) 23/425 (5.4%) 10/375 (2.7%)
Total 2271 240/2271 (10.6%)(range 2.1-25.8%)
72/1629 (4.4%)(range 0.5-6.4%)
36/1417 (2.5%)(range 2.2-6.5%)
P95, 95th centile—, not reported.Genetic disorders include neurodevelopmental delay
129
proefschrif Timmerman.indb 129 18-4-2013 10:30:29

Chapter 9
centile or 4 mm) and NT distribution 84. Table 4 gives an overview of the frequency of various outcome variables according to degree of NT thickness 6. In Figure 2, the chance of favourable outcome reported by two studies is presented per degree of NT thickness. This information may be used for parental counselling, particularly for couples who can understand the concept of risk and statistics. In case of very large NT parents should be informed that there is a high chance of spontaneous lethality and that not all anomalies, and especially cardiac, are amenable to prenatal detection 85. Recently, it has also been observed that an enlarged NT is more frequently observed in male fetuses. Boys with marginal degrees of NT enlargement (>95th–99th percentile) have a higher chance of uneventful outcome than females 86.
0
10
20
30
40
50
60
70
80
90
100
%
p95-p99 p99-4,4 4,5-5,4 5,5-6,4 > 6,5 NT
Bilardo 2007
Souka 2005
Figure 2. Chance of favorable outcome after different degrees of NT enlargement (according to Bilardo et al., 2007 and Souka et al., 2005)
Common questions from parents When faced with the question by parents: ‘What is the cause for the extra fluid in the neck?’ it is easier to find a plausible explanation when increased NT is found in the setting of a definite spectrum of malformations: cardiac, skeletal, neuromuscular, diaphragmatic hernia
5,87, than in the absence of a clear cause. We still totally ignore the origin of ‘physiological’ nuchal fluid accumulation, as seen exclusively between 11 and 14 weeks. Variable degrees of nuchal edema may be present before full establishment of lymphatic development 87,88 and prior to establishment of the intervillous circulation and renal function maturation 89,90.
130
proefschrif Timmerman.indb 130 18-4-2013 10:30:29

Parental counselling after enlarged NT
Chapter
9
This can ‘normalize’ before 14 weeks in one out of five fetuses 91. However, at present there is still insufficient data to equate a disappearing enlarged NT with true ‘normality’. In about 3% of fetuses with increased NT nuchal edema, isolated or in combination with other forms of fluid accumulation, can persist at the time of the 20 weeks scan 6. It is not clear whether this finding represents failure of resolution or if it has a different etiology 92. During embryogenesis tyrosine phosphatase (SHP2) deficiency affects neural crest cell function and triggers the events leading to the typical heart and skull anomalies seen, for instance, in Noonan syndrome (NS) fetuses 93. When nuchal edema persists parents should be counselled that there is a 10% risk of evolution to hydrops and perinatal death or a live birth with a genetic syndrome, such as Noonan syndrome 5. Follow-up scans to monitor evolution of the condition are indicated. After family history is taken a geneticist may advise on appropriateness of DNA testing for certain genetic conditions, such as spinal muscular atrophy. Noonan syndrome is one of the most frequent genetic syndromes encountered in association with nuchal fluid or cystic hygroma in pregnancy. The exact incidence of NS in these fetuses is uncertain, but it may vary between 1 and 3% 94. Genetic testing for this condition is possible, but it takes a long time and it is not always clear-cut, due to the heterogeneity of the condition. In fact, half of the NT cases do not show a PTPN11 mutation
94. Parents should also be informed that, in the absence of severe cardiac anomalies, the prognosis of the condition is generally good, with a good chance of normal intellectual development in the vast majority of cases 95.
Residual risk of adverse outcome after ‘normal’ scans After a normal mid-gestation scan the crucial question of parents is: ‘What is the residual chance that abnormal development will emerge after birth?’ Based on our series of 451 fetuses with increased NT, adverse outcome in fetuses with normal ultrasound examination occurred in 4% of cases and included an equal proportion of intrauterine deaths, undetected heart defects and genetic syndromes. In Senat’s report anomalies were detected after birth in 18/179 (11%) of fetuses with negative findings at ultrasound (US) 50. Both Souka et al. 5 and our studies 6 found that, if at the 20 weeks scan no features of abnormal development were detected, including subtle anomalies (persistence of nuchal edema, pericardial effusion etc.), the chance of uneventful outcome was similar to the general population regardless of increase in NT (Figure 3). However, this observation needs to be substantiated by larger series as the numbers surviving with very large NT’s is small 85. Longer term follow-up is also required as some conditions may only present later in childhood. Thus, one case of NS syndrome with mild pulmonary stenosis was only diagnosed at 3 years of age after publication of our series 6. Moreover, ultrasound examination is not very specific. Critical examination of our data showed that 7 (14%) of the 50 fetuses with suspicious ultrasound findings had an uneventful outcome. This
131
proefschrif Timmerman.indb 131 18-4-2013 10:30:29

Chapter 9
means that obsessive searching for subtle ultrasound features of abnormal development may also lead to anxiety and unnecessary TOP in healthy fetuses 6.
CONCLUSION
Grossly, one out of five fetuses with enlarged NT and normal karyotype has an adverse outcome. The chance of an uneventful pregnancy outcome is inversely related to the initial degree of enlargement. Cases with suspicious ultrasound findings detected at the mid-trimester detailed scan should undergo extra investigations and counselling by a geneticist. Based on current knowledge, in pregnancies where the increased NT resolves and detailed ultrasound examinations reveal no additional anomalies, parents can be confidently reassured that the residual chance of structural anomalies and abnormal neurodevelopment may not be higher than in a the general population. However, larger studies conducted with uniform protocols and with standardized long-term follow-up are necessary to definitively reinforce this conclusion.
0102030405060708090
100
%
P95-P99 P99-4,4 4,5-5,4 5,5-6,4 >6,5 NT
Figure 3. Chance of favourable outcome after normal scan in euploid fetuses with different degrees of NT enlargement (according to Bilardo et al., 2007)
132
proefschrif Timmerman.indb 132 18-4-2013 10:30:30

Parental counselling after enlarged NT
Chapter
9
REFERENCES
1. Ville Y. 2001. Nuchal translucency in the first trimester of pregnancy: ten years on and still a pain in the neck? Ultrasound Obstet.Gynecol. 18(1): 5–8.
2. Bilardo CM. 2001. Increased nuchal translucency and normal karyotype: coping with uncertainty. Ultrasound Obstet Gynecol 17(2): 99–101.
3. Bilardo CM, Müller MA, Pajkrt E. 2001. Outcome of fetuses with increased nuchal translucency. Curr Opin Obstet Gynecol 13(2): 169–174.
4. Weinans MJ, Kooij L, Müller MA, Bilardo KM, van Lith JM, Tymstra T. 2004. A comparison of the impact of screen-positive results obtained from ultrasound and biochemical screening for Down syndrome in the first trimester: a pilot study. Prenat.Diagn. 24(5): 347–351.
5. Souka AP, von Kaisenberg CS, Hyett JA, Sonek JD, Nicolaides KH. 2005. Increased nuchal translucency with normal karyotype. Am.J.Obstet.Gynecol. 192(4): 1005–1021.
6. Bilardo CM, Müller MA, Pajkrt E, Clur SA, van Zalen MM, Bijlsma EK. 2007. Increased nuchal translucency thickness and normal karyotype: time for parental reassurance. Ultrasound Obstet Gynecol 30(1): 11–18.
7. Westin M, Saltvedt S, Almstrom H, Grunewald C, Valentin L. 2007. By how much does increased nuchal translucency increase the risk of adverse pregnancy outcome in chromosomally normal fetuses? A study of 16,260 fetuses derived from an unselected pregnant population. Ultrasound Obstet.Gynecol. 29(2): 150–158.
8. Snijders RJ, Noble P, Sebire N, Souka A, Nicolaides KH. 1998. UK multicentre project on assessment of risk of trisomy 21 by maternal age and fetal nuchal-translucency thickness at 10–14 weeks of gestation. Fetal Medicine Foundation First Trimester Screening Group. Lancet 352(9125): 343–346.
9. Avgidou K, Papageorghiou A, Bindra R, Spencer K, Nicolaides KH. 2005. Prospective first-trimester screening for trisomy 21 in 30,564 pregnancies. Am J Obstet Gynecol 192(6): 1761–1767.
10. Malone FD, Canick JA, Ball RH, et al. 2005b. First-trimester or second-trimester screening, or both, for Down’s syndrome. N.Engl.J.Med. 353(19): 2001–2011.
11. Wright D, Kagan KO, Molina FS, Gazzoni A, Nicolaides KH. 2008. A mixture model of nuchal translucency thickness in screening for chromosomal defects. Ultrasound Obstet.Gynecol. 31(4): 376–383.
12. Evans MI, Van DH, Nicolaides KH. 2007. Nuchal translucency measurements for first-trimester screening: the ‘price’ of inaccuracy. Fetal Diagn.Ther. 22(6): 401–404.
13. D’Alton ME, Cleary-Goldman J, Lambert-Messerlian G, et al. 2009. Maintaining quality assurance for sonographic nuchal translucency measurement: lessons from the FASTER Trial. Ultrasound Obstet Gynecol 33(2): 142–146.
14. Kagan KO, Avgidou K, Molina FS, Gajewska K, Nicolaides KH. 2006. Relation between increased fetal nuchal translucency thickness and chromosomal defects. Obstet.Gynecol. 107(1): 6–10.
15. Bilardo CM, Pajkrt E, de Graaf I, Mol BW, Bleker OP. 1998. Outcome of fetuses with enlarged nuchal translucency and normal karyotype. Ultrasound Obstet Gynecol 11(6): 401–406.
16. Souka AP, Snijders RJ, Novakov A, Soares W, Nicolaides KH. 1998. Defects and syndromes in chromosomally normal fetuses with increased nuchal translucency thickness at 10–14 weeks of gestation. Ultrasound Obstet.Gynecol. 11(6): 391–400.
17. Pajkrt E, Mol BW, Bleker OP, Bilardo CM. 1999. Pregnancy outcome and nuchal translucency measurements in fetuses with a normal karyotype. Prenat.Diagn. 19(12): 1104–1108.
18. Souka AP, Krampl E, Bakalis S, Heath V, Nicolaides KH. 2001. Outcome of pregnancy in chromosomally normal fetuses with increased nuchal translucency in the first trimester. Ultrasound Obstet.Gynecol. 18(1): 9–17.
133
proefschrif Timmerman.indb 133 18-4-2013 10:30:30

Chapter 9
19. Senat MV, De KB, Audibert F, Montcharmont G, Frydman R, Ville Y. 2002. Pregnancy outcome in fetuses with increased nuchal translucency and normal karyotype. Prenat.Diagn. 22(5): 345–349.
20. Maymon R, Tercanli S, Dreazen E, Sartorius G, Holzgreve W, Herman A. 2004b. Comparison of pregnancy outcome of euploid fetuses with increased nuchal translucency (NT) expressed in NT MoM or delta-NT. Ultrasound Obstet.Gynecol. 23(5): 477–481.
21. Malone FD, Ball RH, Nyberg DA, et al. 2005a. First-trimester septated cystic hygroma: prevalence, natural history, and pediatric outcome. Obstet.Gynecol. 106(2): 288–294.
22. Molina FS, Avgidou K, Kagan KO, Poggi S, Nicolaides KH. 2006. Cystic hygromas, nuchal edema, and nuchal translucency at 11–14 weeks of gestation. Obstet.Gynecol. 107(3): 678–683.
23. Sepulveda W, Wong AE, Casasbuenas A, Solari A, Alcalde JL. 2008. Congenital diaphragmatic hernia in a first-trimester ultrasound aneuploidy screening program. Prenat.Diagn. 28(6): 531–534.
24. Tonni G, Ventura A, de FC. 2005. First trimester increased nuchal translucency associated with fetal achondroplasia. Am.J.Perinatol. 22(3): 145–148.
25. Chitty LS, Tan AW, Nesbit DL, Hall CM, Rodeck CH. 2006. Sonographic diagnosis of SEDC and double heterozygote of SEDC and achondroplasia–a report of six pregnancies. Prenat Diagn 26(9): 861–865.
26. Ngo C, Viot G, AubryMC, et al. 2007. First-trimester ultrasound diagnosis of skeletal dysplasia associated with increased nuchal translucency thickness. Ultrasound Obstet.Gynecol. 30(2): 221–226.
27. Michailidis GD, Economides DL. 2001. Nuchal translucency measurement and pregnancy outcome in karyotypically normal fetuses. Ultrasound Obstet.Gynecol. 17(2): 102–105.
28. Ghi T, Huggon IC, Zosmer N, Nicolaides KH. 2001. Incidence of major structural cardiac defects associated with increased nuchal translucency but normal karyotype. Ultrasound Obstet.Gynecol. 18(6): 610–614.
29. Atzei A, Gajewska K, Huggon IC, Allan L, Nicolaides KH. 2005. Relationship between nuchal translucency thickness and prevalence of major cardiac defects in fetuses with normal karyotype. Ultrasound Obstet Gynecol 26(2): 154–157.
30. Clur SA, Mathijssen IB, Pajkrt E, et al. 2008. Structural heart defects associated with an increased nuchal translucency: 9 years experience in a referral centre. Prenat Diagn 28(4): 347–354.
31. Simpson JM, Sharland GK. 2000. Nuchal translucency and congenital heart defects: heart failure or not? Ultrasound Obstet.Gynecol. 16(1): 30–36.
32. Hyett JA, Perdu M, Sharland GK, Snijders RS, Nicolaides KH. 1997b. Increased nuchal translucency at 10–14 weeks of gestation as a marker for major cardiac defects. Ultrasound Obstet.Gynecol. 10(4): 242–246.
33. Hyett J, Perdu M, Sharland G, Snijders R, Nicolaides KH. 1999. Using fetal nuchal translucency to screen for major congenital cardiac defects at 10–14 weeks of gestation: population based cohort study. BMJ 318(7176): 81–85.
34. Galindo A, Comas C, Martinez JM, et al. 2003. Cardiac defects in chromosomally normal fetuses with increased nuchal translucency at 10–14 weeks of gestation. J.Matern.Fetal Neonatal Med. 13(3): 163–170.
35. Lopes LM, Brizot ML, Lopes MA, Ayello VD, Schultz R, Zugaib M. 2003. Structural and functional cardiac abnormalities identified prior to 16 weeks’ gestation in fetuses with increased nuchal translucency. Ultrasound Obstet.Gynecol. 22(5): 470–478.
36. Hyett J. 2004. Does nuchal translucency have a role in fetal cardiac screening? Prenat.Diagn. 24(13): 1130–1135.
37. McAuliffe FM, Hornberger LK, Winsor S, Chitayat D, Chong K, Johnson JA. 2004. Fetal cardiac defects and increased nuchal translucency thickness: a prospective study. Am.J.Obstet.Gynecol. 191(4): 1486–1490.
38. Bahado-Singh RO, Wapner R, Thom E, et al. 2005. Elevated firsttrimester nuchal translucency increases the risk of congenital heart defects. Am J Obstet Gynecol 192(5): 1357–1361.
134
proefschrif Timmerman.indb 134 18-4-2013 10:30:30

Parental counselling after enlarged NT
Chapter
9
39. Simpson LL, Malone FD, Bianchi DW, et al. 2007. Nuchal translucency and the risk of congenital heart disease. Obstet.Gynecol. 109(2 Pt 1): 376–383.
40. Makrydimas G, Sotiriadis A, Ioannidis JP. 2003. Screening performance of first-trimester nuchal translucency for major cardiac defects: a meta-analysis. Am.J.Obstet.Gynecol. 189(5): 1330–1335.
41. Makrydimas G, Sotiriadis A, Huggon IC, et al. 2005. Nuchal translucency and fetal cardiac defects: a pooled analysis of major fetal echocardiography centers. Am.J.Obstet.Gynecol. 192(1): 89–95.
42. Westin M, Saltvedt S, Bergman G, Almstrom H, Grunewald C, Valentin L. 2006. Is measurement of nuchal translucency thickness a useful screening tool for heart defects? A study of 16,383 fetuses. Ultrasound Obstet.Gynecol. 27(6): 632–639.
43. Müller MA, Clur SA, Timmerman E, Bilardo CM. 2007. Nuchal translucency measurement and congenital heart defects: modest association in low-risk pregnancies. Prenat.Diagn. 27(2): 164–169.
44. Wald NJ, Morris JK, Walker K, Simpson JM. 2008. Prenatal screening for serious congenital heart defects using nuchal translucency: a meta-analysis. Prenat.Diagn. 28(12): 1094–1104.
45. Vogel M, Sharland GK, McElhinney DB, et al. 2009. Prevalence of increased nuchal translucency in fetuses with congenital cardiac disease and a normal karyotype. Cardiol Young. 19(5): 441–445.
46. Maiz N, Plasencia W, Dagklis T, Faros E, Nicolaides K. 2008. Ductus venosus Doppler in fetuses with cardiac defects and increased nuchal translucency thickness. Ultrasound Obstet.Gynecol. 31(3): 256–260.
47. Maiz N, Valencia C, Emmanuel EE, Staboulidou I, Nicolaides KH. 2008b. Screening for adverse pregnancy outcome by ductus venosus Doppler at 11–13 + 6 weeks of gestation. Obstet.Gynecol. 112(3): 598–605.
48. Faiola S, Tsoi E, Huggon IC, Allan LD, Nicolaides KH. 2005. Likelihood ratio for trisomy 21 in fetuses with tricuspid regurgitation at the 11 to 13 + 6-week scan. Ultrasound Obstet.Gynecol. 26(1): 22–27.
49. Bekker MN. 2007. A normal 20-week scan of a euploid fetus with a history of first-trimester increased nuchal translucency: caution or reassurance? Ultrasound Obstet Gynecol 30(1): 8–10.
50. Senat MV, Bussieres L, Couderc S, et al. 2007. Long-term outcome of children born after a first-trimester measurement of nuchal translucency at the 99th percentile or greater with normal karyotype: a prospective study. Am.J.Obstet.Gynecol. 196(1): 53–56.
51. Alfirevic Z. 2008. DISQ 8: Management of patients with an increased first-trimester Down syndrome screening risk and normal fetal karyotype. Ultrasound Obstet Gynecol 31(2): 232.
52. Becker R, Wegner RD. 2006. Detailed screening for fetal anomalies and cardiac defects at the 11-13-week scan. Ultrasound Obstet Gynecol 27(6): 613–618.
53. Dane B, Dane C, Sivri D, Kiray M, Cetin A, Yayla M. 2007. Ultrasound screening for fetal major abnormalities at 11–14 weeks. Acta Obstet Gynecol Scand 86(6): 666–670.
54. Lombardi CM, Bellotti M, Fesslova V, Cappellini A. 2007. Fetal echocardiography at the time of the nuchal translucency scan. Ultrasound Obstet.Gynecol. 29(3): 249–257.
55. Chen M, Lee CP, Lam YH, et al. 2008. Comparison of nuchal and detailed morphology ultrasound examinations in early pregnancy for fetal structural abnormality screening: a randomized controlled trial. Ultrasound Obstet Gynecol 31(2): 136–146.
56. Timmerman E, Pajkrt E, van Zalen-Sprock MM, Robles de Medina PG, Bilardo CM. 2008. OP09.13 The impact of additional anomalies at the 11–14 weeks scan on the prediction of fetal outcome in fetuses with enlarged nuchal translucency. 18th World Congress on Ultrasound in Obstetrics and Gynecology, Chicago Aug 2008. Abstract in Ultrasound Obstet Gynecol 32: 340.
57. Timor-Tritsch IE, Fuchs KM, Monteagudo A, D’alton ME. 2009. Performing a fetal anatomy scan at the time of first-trimester screening. Obstet Gynecol. 113(2 Pt 1): 402–407.
58. Korenromp MJ, Christiaens GC, van den BJ, et al. 2005. Longterm psychological consequences of pregnancy termination for fetal abnormality: a cross-sectional study. Prenat.Diagn. 25(3): 253–260.
59. Statham H, Solomou W, Chitty L. 2000. Prenatal diagnosis of fetal abnormality: psychological effects on women in low-risk pregnancies. Baillieres Best Pract Res Clin Obstet Gynaecol. 14(4): 731–747.
135
proefschrif Timmerman.indb 135 18-4-2013 10:30:30

Chapter 9
60. Bronshtein M, Zimmer EZ, Blazer S. 2008. The utility of detailed first trimester ultrasound examination in abnormal fetal nuchal translucency. Prenat Diagn 28(11): 1037–1041.
61. Weiner Z, Weizman B, Beloosesky R, Goldstein I, Bombard A. 2008. Fetal cardiac scanning performed immediately following an abnormal nuchal translucency examination. Prenat.Diagn 28(10): 934–938.
62. Bilardo CM, Müller MA, Zikulnig L, Schipper M, Hecher K. 2001. Ductus venosus studies in fetuses at high risk for chromosomal or heart abnormalities: relationship with nuchal translucency measurement and fetal outcome. Ultrasound Obstet Gynecol 17(4): 288–294.
63. Oh C, Harman C, Baschat AA. 2007. Abnormal first-trimester ductus venosus blood flow: a risk factor for adverse outcome in fetuses with normal nuchal translucency. Ultrasound Obstet.Gynecol. 30(2): 192–196.
64. Sebire NJ, Bianco D, Snijders RJ, Zuckerman M, Nicolaides KH. 1997. Increased fetal nuchal translucency thickness at 10–14 weeks: is screening for maternal-fetal infection necessary? Br.J.Obstet.Gynaecol. 104(2): 212–215.
65. Markenson G, Correia LA, Cohn G, Bayer L, Kanaan C. 2000. Parvoviral infection associated with increased nuchal translucency: a case report. J.Perinatol. 20(2): 129–131.
66. Kempe A, Rosing B, Berg C, et al. 2007. First-trimester treatment of fetal anemia secondary to parvovirus B19 infection. Ultrasound Obstet.Gynecol. 29(2): 226–228.
67. Lespinasse J, Testard H, Nugues F, et al. 2004. A submicroscopic unbalanced subtelomeric translocation t(2p;10q) identified by fluorescence in situ hybridization: fetus with increased nuchal translucency and normal standard karyotype with later growth and developmental delay, rhombencephalosynapsis (RES). Ann.Genet. 47(4): 405–417.
68. Chen CP, Chern SR, Chang TY, et al. 2005. Prenatal diagnosis of de novo proximal interstitial deletion of 9q and review of the literature of uncommon aneuploidies associated with increased nuchal translucency. Prenat Diagn 25(5): 383–389.
69. Farina A, Volinia S, Arcelli D, et al. 2006. Evidence of genetic underexpression in chorionic villi samples of euploid fetuses with increased nuchal translucency at 10–11 weeks’ gestation. Prenat Diagn 26(2): 128–133.
70. Law LW, Lau TK, Fung TY, Leung TY, Wang CC, Choy KW. 2008. De novo 16p13.11 microdeletion identified by high-resolution array CGH in a fetus with increased nuchal translucency. BJOG 116(2):
339–343.
71. Donnenfeld AE, Cutillo D, Horwitz J, Knops J. 2006. Prospective study of 22q11 deletion analysis in fetuses with excess nuchal translucency. Am.J.Obstet.Gynecol. 194(2): 508–511.
72. Lautrup CK, Kjaergaard S, Brondum-Nielsen K, et al. 2008. Testing for 22q11 microdeletion in 146 fetuses with nuchal translucency above the 99th percentile and a normal karyotype. Acta Obstet.Gynecol.Scand. 87(11): 1252–1255.
73. Van Huizen ME, Pighetti M, Bijlsma EK, Knegt AC, Bilardo CM. 2005. Increased nuchal translucency thickness: a marker for chromosomal and genetic disorders in both offspring and parents. Ultrasound Obstet.Gynecol. 26(7): 793–794.
74. Hyett J, Noble P, Sebire NJ, Snijders R, Nicolaides KH. 1997. Lethal congenital arthrogryposis presents with increased nuchal translucency at 10–14 weeks of gestation. Ultrasound Obstet. Gynecol. 9(5): 310–313.
75. De Vreede I, Bilardo CM, van Rijn RR, Clur SA, Heij HA. 2008. Intrapericardial extralobar pulmonary sequestration presenting as a prenatal intrathoracic mass. Pediatr.Cardiol. 29(5): 980–982.
76. Favre R, Moutel G, Duchange N, et al. 2008. What about informed consent in first-trimester ultrasound screening for Down syndrome? Fetal Diagn.Ther. 23(3): 173–184.
77. Kleinveld JH, Ten Kate LP, van den BM, van Vugt JM, Timmermans DR. 2009. Does informed decision making influence psychological outcomes after receiving a positive screening outcome? Prenat.Diagn. 29(3): 271–273.
78. Layng J. 1998. Screening for nuchal translucency. Counselling should be considered an integral part of screening programmes. BMJ 317(7160): 749.
136
proefschrif Timmerman.indb 136 18-4-2013 10:30:30

Parental counselling after enlarged NT
Chapter
9
79. Müller MA, Bleker OP, Bonsel GJ, Bilardo CM. 2006. Women’s opinions on the offer and use of nuchal translucency screening for Down syndrome. Prenat.Diagn. 26(2): 105–111.
80. Chervenak FA, McCullough LB, Sharma G, Davis J, Gross S. 2008. Enhancing patient autonomy with risk assessment and invasive diagnosis: an ethical solution to a clinical challenge. Am J Obstet Gynecol 199(1): 19–14.
81. Favre R, Guige V, Weingertner AS, et al. 2009. Is the non-respect of ethical principles by health professionals during first-trimester sonographic Down syndrome screening damaging to patient autonomy? Ultrasound Obstet Gynecol. 34(1): 25–32.
82. Seror V. 2008. Fitting observed and theoretical choices—women’s choices about prenatal diagnosis of Down syndrome. Health Econ. 17(5): 557–577.
83. Maymon R, Weinraub Z, Herman A. 2005. Pregnancy outcome of euploid fetuses with increased nuchal translucency: how bad is the news? J.Perinat.Med. 33(3): 191–198.
84. Maymon R, Herman A. 2004a. The clinical evaluation and pregnancy outcome of euploid fetuses with increased nuchal translucency. Clin.Genet. 66(5): 426–436.
85. Scott F, Evans J, McLennan A. 2009. Perinatal outcome in fetuses with extremely large nuchal translucency measurement. Aust N Z J Obstet Gynaecol. 49(3): 254–257.
86. Timmerman E, Pajkrt E, Bilardo CM. 2009. Male gender as a favorable prognostic factor in pregnancies with enlarged nuchal translucency. Ultrasound Obstet Gynecol 34(4): 373–378.
87. Haak MC, van Vugt JM. 2003. Pathophysiology of increased nuchal translucency: a review of the literature. Hum.Reprod.Update. 9(2): 175–184.
88. Bellini C, Rutigliani M, Boccardo FM, et al. 2009. Nuchal translucency and lymphatic system maldevelopment. J Perinat Med 37(6): 673–676.
89. Van Splunder P, Stijnen T, Wladimiroff JW. 1996. Fetal atrioventricular flow-velocity waveforms and their relation to arterial and venous flow-velocity waveforms at 8 to 20 weeks of gestation. Circulation 94(6): 1372–1378.
90. Allan LD. 2006. The mystery of nuchal translucency. Cardiol Young 16(1): 11–17.
91. Müller MA, Pajkrt E, Bleker OP, Bonsel GJ, Bilardo CM. 2004. Disappearance of enlarged nuchal translucency before 14 weeks’ gestation: relationship with chromosomal abnormalities and pregnancy outcome. Ultrasound Obstet.Gynecol. 24(2): 169–174.
92. Maymon R, Zimerman AL, Weinraub Z, Herman A, Cuckle H. 2008. Correlation between nuchal translucency and nuchal skinfold measurements in Down syndrome and unaffected fetuses. Ultrasound Obstet.Gynecol 32(4): 501–505.
93. Nakamura T, Gulick J, Colbert MC, Robbins J. 2009. Protein tyrosine phosphatase activity in the neural crest is essential for normal heart and skull development. Proc Natl Acad Sci USA. 106(27): 11270–11275.
94. Lee K, Williams B, Roza K, et al. 2008. PTPN11 analysis for the prenatal diagnosis of Noonan syndrome in fetuses with abnormal ultrasound findings. Clin.Genet 75(2): 190–194.
95. Van den Burgt I. 2007. Noonan syndrome. Orphanet J.Rare.Dis. 2: 4.
96. Abad DE, Gabarre JA, Izquierdo AM, Lopez-Sanchez C, Garcia-Martinez V, Izquierdo AG. 2006. Pallister-Killian syndrome presenting with a complex congenital heart defect and increased nuchal translucency. J Ultrasound Med 25(11): 1475–1480.
97. Kim MH, Park SY, Kim MY, Lee BY, Lee MH, Ryu HM. 2008. Prenatal diagnosis of Pallister-Killian syndrome in two fetuses with increased nuchal translucency. Prenat.Diagn. 28(5): 454–456.
98. Liberati M, Melchiorre K, D’Emilio I, et al. 2008. Fetal facial profile in Pallister-Killian syndrome. Fetal Diagn.Ther. 23(1): 15–17.
99. Aleem S, Howarth ES. 2005. Apert syndrome associated with increased fetal nuchal translucency. Prenat Diagn 25(11): 1066–1067.
137
proefschrif Timmerman.indb 137 18-4-2013 10:30:30

Chapter 9
100. David AL, Turnbull C, Scott R, et al. 2007. Diagnosis of Apert syndrome in the second-trimester using 2D and 3D ultrasound. Prenat.Diagn. 27(7): 629–632.
101. Blin G, Rabbe A, Ansquer Y, Meghdiche S, Floch-Tudal C, Mandelbrot L. 2005. First-trimester ultrasound diagnosis in a recurrent case of Walker-Warburg syndrome. Ultrasound Obstet Gynecol 26(3): 297–299.
102. Rusnak AJ, Hadfield MI, Chudley AE, Marles SL, Reid GJ, Chodirker BN. 2008. Increased nuchal translucency thickness: a potential indicator for Ritscher-Schinzel Syndrome. Fetal Diagn.Ther. 24(4): 395–399.
103. Bijlsma EK, Knegt AC, Bilardo CM, Goodman FR. 2005. Increased nuchal translucency and split-hand/foot malformation in a fetus with an interstitial deletion of chromosome 2q that removes the SHFM5 locus. Prenat Diagn 25(1): 39–44.
104. Tonni G, Azzoni D, Ambrosetti F, de FC, Ventura A. 2007. Cerebrofronto-facial syndrome (Dandy-Walker Variant and frontofacial dysmorphisms): report of the first case identified by increased nuchal translucency beyond 13(+6) weeks. Congenit.Anom.(Kyoto) 47(2): 68–71.
105. Venkat-Raman N, Sebire NJ, Murphy KW, Carvalho JS, Hall CM. 2005. Increased first-trimester fetal nuchal translucency thickness in association with chondroectodermal dysplasia (Ellis-Van Creveld syndrome). Ultrasound Obstet.Gynecol. 25(4): 412–414.
106. Witters I, Claerhout P, Fryns JP. 2005. Increased nuchal translucency thickness in thrombocytopenia-absent-radius syndrome. Ultrasound Obstet.Gynecol. 26(5): 581–582.
107. Witters I, Denayer E, Brems H, Fryns JP, Legius E. 2008. The cardiofaciocutaneous syndrome: prenatal findings in two patients. Prenat.Diagn. 28(1): 53–55.
108. Gundogan M, Fong K, Keating S, Pierre-Louis J, Chitayat D. 2006. First trimester ultrasound diagnosis of lethal multiple pterygium syndrome. Fetal Diagn.Ther. 21(5): 466–470.
109. Rosing B, Kempe A, Berg C, et al. 2008. Orofaciodigital syndrome Type IV (Mohr-Majewski): early prenatal diagnosis in siblings. Ultrasound Obstet.Gynecol. 31(4): 457–460.
110. Sanseverino MT, de Souza CF, Gissen P, Sordi AO, Magalhaes JA, Schuler-Faccini L. 2006. Increased nuchal translucency in arthrogryposis, renal dysfunction and cholestasis (ARC) syndrome and discovery of a Portuguese specific mutation in the VPS33B gene. Ultrasound Obstet.Gynecol. 28(2): 233–234.
111. Wong HS, Kidd A, Zuccollo J, et al. 2008. A case of thanatophoric dysplasia: The early prenatal 2d and 3d sonographic findings and molecular confirmation of diagnosis. Fetal Diagn.Ther. 24(1): 71–73.
112. De Biasio P, Ichim IB, Scarso E, Baldi M, Barban A, Venturini PL. 2005. Thanatophoric dysplasia type I presenting with increased nuchal translucency in the first trimester. Prenat.Diagn. 25(5): 426–428.
113. Colombani M, Laurent N, Le MM, et al. 2006. A new osteochondrodysplasia with severe osteopenia, preaxial polydactyly, clefting and dysmorphic features resembling filamin-related disorders. Prenat Diagn 26(12): 1151–1155.
114. Yalinkaya A, Yayla M, Erdemoglu M. 2007. Prenatal diagnosis of a fetus with androgen insensitivity syndrome (AIS). Prenat.Diagn. 27(9): 856–857.
115. Cheng PJ, Chang SD, Shaw SW, Soong YK. 2005. Nuchal translucency thickness in fetuses with chromosomal translocation at 11–12 weeks of gestation. Obstet Gynecol 105(5): 1058–1062.
116. Brisset S, Kasakyan S, L’Hermine AC, et al. 2006. De novo monosomy 9p24.3-pter and trisomy 17q24.3-qter characterised by microarray comparative genomic hybridisation in a fetus with an increased nuchal translucency. Prenat Diagn 26(3): 206–213.
117. Kasakyan S, Lohmann L, Aboura A, et al. 2008. De novo complex intra chromosomal rearrangement after ICSI: characterisation by BACs micro array -CGH. Mol.Cytogenet. 1(1): 27.
118. Stankiewicz P, Kuechler A, Eller CD, et al. 2006. Minimal phenotype in a girl with trisomy 15q due to t(X;15)(q22.3;q11.2) translocation. Am.J.Med.Genet.A 140(5): 442–452.
119. De Pater JM, Nikkels PG, Poot M, et al. 2005. Striking facial dysmorphisms and restricted thymic development in a fetus with a 6-megabase deletion of chromosome 14q. Pediatr.Dev.Pathol. 8(4): 497–503.
138
proefschrif Timmerman.indb 138 18-4-2013 10:30:30

Parental counselling after enlarged NT
Chapter
9
120. Hindryckx A, De CL, Van EH, Fryns JP, Moerman P, Devlieger R. 2008. First trimester prenatal diagnosis of 13q-syndrome presenting with increased nuchal translucency, Dandy-Walker malformation and small parietal encephalocoele. Prenat.Diagn. 28(5): 445–446.
121. Hulsbergen MH, Van Calenbergh SG, Fryns JP. 2007. Abnormal first trimester screen in partial deletion of chromosome 6p21: a casereport. Genet.Couns. 18(2): 243–245.
122. Rauch A, Dorr HG. 2007. Chromosome 5q subtelomeric deletion syndrome. Am.J.Med.Genet.C.Semin.Med.Genet. 145C(4): 372–376.
123. De Pater J, Van dS-B, Prins M, Derks J, Albrechts J, Engelen J. 2006. Prenatal identification of a marker chromosome 16 by chromosome microdissection and reverse FISH. Eur.J.Med.Genet. 49(4): 306–312.
124. Wax JR, Carpenter M, Chard R, Cartin A, Pinette MG, Blackstone J. 2008. Prenatal sonographic features of trisomy 1q. J.Clin.Ultrasound 36(4): 231–236.
125. Brady AF, Pandya PP, Yuksel B, Greenough A, Patton MA, Nicolaides KH. 1998. Outcome of chromosomally normal livebirths with increased fetal nuchal translucency at 10–14 weeks’gestation. J Med Genet 35: 222–224.
126. Van Vugt JMG, Tinnemans BW, Van Zalen-Sproch RM. 1998. Outcome and early childhood follow-up of chromosomally normal fetuses with increased nuchal translucency at 10–14 weeks’gestation. Ultrasound Obstet Gynecol 11: 407–409.
127. Adekunle O, Gopee A, el Sayed M, Thilaganathan B. 1999. Increased first trimester nuchal translucency: pregnancy and infant outcomes after routine screening for Down’s syndrome in an unselected antenatal population. Br J Radiol 72: 457–460.
128. Maymon R, Jauniaux E, Cohen O, Dreazen E, Weinraub Z, Herman A. 2000. Pregnancy outcome and infant follow-up of fetuses with abnormally increased first trimester nuchal translucency. Hum Reprod 15: 2023–2027.
129. Hippala A, Eronen M, Taipale P, Salonen R, Hiilesmaa V. 2001. Fetal nuchal translucency and normal chromosomes: a longterm follow-up study. Ultrasound Obstet Gynecol 18: 18–22.
130. Cheng CC, Bahado-Singh RO, Chen SC, Tsai MS. 2004. Pregnancy outcomes with increased nuchal translucency after routine Down syndrome screening. Int J Gynaecol Obstet 84: 5–9.
131. Mangione R, Guyon F, Taine L, Wen ZQ, Roux D, Vergnaud A, Maugey-Laulom B, Horovitz J, Saura R. 2001. Pregnancy outcome and prognosis in fetuses with increased first-trimester nuchal translucency. Fetal Diagn Ther. 16: 360–363.
139
proefschrif Timmerman.indb 139 18-4-2013 10:30:31