Embed Size (px)
Citation preview

UvA-DARE is a service provided by the library of the University of Amsterdam (https://dare.uva.nl)
UvA-DARE (Digital Academic Repository)
Functional MRI of the small bowelFundamentals of MRI motility measurementsde Jonge, C.S.
Publication date2019Document VersionOther versionLicenseOther
Link to publication
Citation for published version (APA):de Jonge, C. S. (2019). Functional MRI of the small bowel: Fundamentals of MRI motilitymeasurements.
General rightsIt is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s)and/or copyright holder(s), other than for strictly personal, individual use, unless the work is under an opencontent license (like Creative Commons).
Disclaimer/Complaints regulationsIf you believe that digital publication of certain material infringes any of your rights or (privacy) interests, pleaselet the Library know, stating your reasons. In case of a legitimate complaint, the Library will make the materialinaccessible and/or remove it from the website. Please Ask the Library: https://uba.uva.nl/en/contact, or a letterto: Library of the University of Amsterdam, Secretariat, Singel 425, 1012 WP Amsterdam, The Netherlands. Youwill be contacted as soon as possible.
Download date:29 May 2021

Chapter 2
Evaluation of gastrointestinal motility with MRI:
advances challenges and opportunities
C.S. de Jonge, MScA.J.P.M. Smout, MD, PhD
A.J. Nederveen, PhDJ. Stoker, MD, PhD
Neurogastroenterol Motil. 2018; 30:e13257doi: 10.1111/nmo.13257

22
ABSTRACTDynamic magnetic resonance imaging (MRI) of gastrointestinal motility has developed rapidly over the past few years. The non-invasive and non-ionizing character of MRI is an important advantage together with the fact that it is fast and can visualize the entire gastrointestinal tract. Advances in imaging and quantification techniques have facilitated assessment of gastric, small intestinal and colonic motility in a clinical setting. Automated quantitative motility assessment using dynamic MRI meets the need for non-invasive techniques. Recently, studies have begun to examine this technique in patients, including those with IBD, pseudo-obstruction and functional bowel disorders. Remaining challenges for clinical implementation are processing the large amount of data, standardization and validation of the numerous MRI metrics and subsequently assessment of the potential role of dynamic MRI. This review examines the methods, advances and remaining challenges of evaluation of gastrointestinal motility with MRI. It accompanies an article by Khalaf et al. in this journal that describes a new protocol for assessment of pan-intestinal motility in fasted and fed state in a single MRI session.

23
Chapter 2
INTRODUCTIONAbdominal magnetic resonance imaging (MRI) is very well suited to image fluids and gastrointestinal volumes in the gastrointestinal tract. Newly developed MRI parameters, previously described in this journal1, provide functional information like volumes, transit time and small bowel water content measurements, but this review focusses on the imaging of gastrointestinal motility. Dynamic MRI, also referred to as cine MRI, is a MRI technique in which sequences of images are acquired in order to obtain movies. By using post-processing techniques local or global movements in the gastrointestinal tract can be quantified. Approximately 30 years ago dynamic MRI was introduced2 as a method for the assessment of gastrointestinal motility. Only recently quantification techniques for motility assessment have matured to a level that allows for clinical evaluation. Dynamic MRI is used in the stomach to measure frequency and amplitude of antral contractions3–5. It is used for the small bowel to look at segmental and global motility using frequency measures and surrogate measures 6–12. In the colon it has been applied to assess motion and velocity of contents, wall motion and to study motility using surrogate measures13–17. So far there has been a paucity of validation studies. To our knowledge there is only one study in which dynamic MRI findings were compared to manometry, demonstrating 100% correlation between visualized colonic movements and intraluminal pressure changes.17 The clinical value of dynamic MRI is under evaluation for pathologies like inflammatory bowel disease (IBD), chronic intestinal pseudo-obstruction (CIPO) and constipation. In this issue of Neurogastroenterology and Motility, Khalaf et al. introduce a protocol for assessment of pan-intestinal motility in fasted and fed state in a single session of MRI. As part of their novel approach they quantified small bowel motility using dynamic MRI.18 In this review we discuss the challenges and opportunities in evaluating gastrointestinal motility with dynamic MRI. The first part of this review summarizes the technical aspects of the dynamic MRI technique, the second part discusses the observations made by applying the described techniques to gastrointestinal physiology, diseases and disorders.
ACQUISITION AND POST-PROCESSING METHODSImage acquisitionThere is no standard imaging protocol available yet for dynamic GI motility imaging. Most studies use two-dimensional (2D) scans (i.e. one single slice) acquired in prone or supine position. Securing good temporal and spatial resolution of the images, MRI scanners with field strengths of 1.5T and 3T from several vendors can be used. The preferred MRI sequence depends on the quantitative imaging analysis used, but

24
is one that displays the bowel wall clearly, with the ability of fast acquisition in order to acquire at a high frame rate, like the commonly used bFFE sequence (balanced steady-state free procession gradient echo sequence) (see figure 1 and movie19). Until now limited data exists to optimize imaging protocols with respect to quantitative imaging analysis. Spatial resolution requirements are based on the lower limit of bowel wall thickness, 1-3 mm in healthy subjects. Manometric, electromyographic and radiographic studies have shown that the fastest contractions occur in the small bowel, between 9 and 12 contractions per minute20, indicating that at least a temporal resolution of 1 frame every 2.5 seconds is required to capture motility. Both breath-hold and free-breathing protocols are being explored. The short observation periods associated with breath-hold protocols may seem inadequate to measure GI motility, but have shown good initial results4,10,16,21–27 and are very practical for clinical use. Recent work showed that in breath-hold scanning, using a displacement mapping quantification technique (described below), a temporal resolution of at least 1 image per second and a duration of 15 seconds is required for robust assessment of motility.28 Free-breathing scans provide more information due to longer scanning times, but the breathing artifacts in the scans and the amount of data for processing still pose a burden to handle. Three-dimensional (3D) motility imaging gains interest since it provides more coverage to assess movement in all directions, excluding ‘out of plane’ movement, but challenges lie on both the acquisition and the post-processing side. Development of a MRI sequence that meets the temporal and spatial resolution requirements is ongoing; processing the large amount of data acquired and developing automatic 3D data analysis software is a step that has not been taken yet. Until this moment, in most MRI motility studies the subjects were given bowel preparation with an oral solution, to create good contrast and distention in the GI tract for optimal visualization.29 Lately interest has emerged in assessing the bowel in an unprepared state because this allows evaluation of fasted (interdigestive) motility and the response to food.18
Although acquisition techniques require further refinement, it is safe to say that at this moment in time, we are able to visualize motility with dynamic MRI with good resolution. The main hurdle evaluating its clinical value has been the absence of a robust automatic quantification method. Therefore several post-processing/quantification techniques are in development to provide standardization and to overcome the obstacle of manual data processing.

25
Chapter 2
Quantification methodsAll methods described below can be used for gastric, small intestinal and colonic measurements. Their advantages and disadvantages are summarized in table 1.
Table 1. Advantages and disadvantages of quantification techniques
Technique Advantages Disadvantages
Visual assessment
• Straight-forward• Local and global assessment• Easy to use in clinic (no additional means necessary)
• Labor-intensive scoring• Training required• Does not provide actual quantification of motility• Through-plane movement can cause false-positive contractility*• Prone to interpersonal and intrapersonal variations• Requires bowel preparation• Limited validation studies available
Diameter measurements
• Provides quantification of peristaltic contractions• Can be implemented in semi-automatic software for fast and standardized measurements• Easy to use in clinic (manual measurements)
• Manual measurements are labor-intensive• Semi-automated software not widely available yet• Provides only local assessment• Through-plane movement can cause false-positive contractility* • Requires bowel preparation• Semi-automated analysis
Displacement mapping
• Provides local and global motility measures.• Results presented in easily readable color maps• No bowel preparation required • Software commercially available
• Metric is a surrogate outcome measure, it does not separately quantify individual measures of contractile activity (e.g. contraction frequency and amplitude)• Semi-automated analysis
GI Tagging • Fully automated analysis• No bowel preparation required• Works with breath-hold and free-breathing data • Enables assessment of motion over prolonged periods
• Long scan durations (minutes) needed for frequency measurement• Software not available
* Through-plane movement is a limitation of all 2D techniques, but is a less prominent issue in displacement mapping and GI tagging techniques.

26
Visual assessment The simplest method to interpret dynamic MR images is evaluation by visual assessment of propagation direction and incidence of phasic contractions at specified sites in the GI tract (Fig. 1A-B).30 This can be performed by a radiologist who observes all consecutive images of a bowel segment and grades the contractile activity on a 5-point scale31,32 or by using a classification system33,34.Visual assessment is a relatively simple technique that can easily be used in daily clinical practice by trained radiologists when validated. However it is relatively labor-intensive and prone to inter- and intra-observer variations.31
Diameter measurementsAnother easily understandable method is the measurement of changes in the luminal diameter over time. This method requires satisfactory distension of the lumen and good visualization of the luminal boundaries. In selected bowel segments, a line is drawn perpendicular to the wall of the segment and copied to all sequential images of the dynamic 2D MRI. The length of this line is followed over time, representing the contractility of this specific bowel segment (Fig. 1C-D). The drawing and copying of the diameter line to all sequential images can be performed manually6, or semi-automatically with software like ‘Motasso’11,12. This software-assisted method has been shown to be faster and have a higher measurement precision compared to the manual method.11 Adjustment of the software has made it possible to work with free-breathing data.35 An important limitation of the diameter measurement method is the through-plane movement of the segments that are measured. The software cannot distinguish this movement from a real contraction, leading to over-interpretation of contractility. The diameter method is a relative simple technique, especially the manual method can be used clinically, but is a relatively time-consuming task. Unfortunately, to our knowledge, the semi-automatic ‘Motasso’ software is not available to other researchers and clinicians.
Displacement mappingThe displacement mapping method, also known as motility mapping, is based on the idea that contrast in the dynamic MR images changes over time due to motility and movement of luminal content. The motion of abdominal organs between two consecutive images in time can be estimated by an automated optical-flow based algorithm, providing displacement fields (Fig. 1E). Several surrogate measures for motility are then determined using these displacement fields. This method was optimized by two independent research groups10,36.

27
Chapter 2
Motility mapping provides the reader with a color-coded map (Fig. 1F) for a global assessment of motility in all segments of the MR image. Furthermore, a region of interest (ROI) can be delineated to obtain a single, numerical motility score for that area on the scan. It should be noted however that different groups have used different calculation techniques and that interpretation of the resulting color plots requires understanding of the technique.10,18,36 It is yet to be determined what metric will be clinically most valuable, this might even be disease-specific. Displacement maps are preferably calculated from a 20-second breath-hold movie to avoid breathing artifacts and to limit data processing times, but a breath-hold protocol is not necessarily required for this technique37–39. The displacement mapping technique is more complex and less easy to understand than the previous two methods but it allows quantitative analysis of global and local GI motility. It has been automated for more repeatable and standardized results and it produces very easily readable color maps. The software has been used and validated in several studies4,7,9,10,13,18,21,23,24,26–28,40–43 and one software version is commercially available44.
GI TaggingWhereas the previous three techniques dealt with post-processing of conventionally acquired dynamic MRI data, the tagged MRI technique involves a dedicated type of MR acquisition. During image acquisition, taglines are applied to the tissue. These taglines are read-out with a delay and during this delay movement of the tagged tissue leads to deformation of the taglines. This deformation of the tag lines is thus related to motility. With a quantification technique developed by Sprengers et al. the deformation of the taglines can be tracked in free-breathing scans to measure motility in multiple frequency bands in regions of interest (Fig. 1G).8,45,46 Assessment during free-breathing allows for longer monitoring i.e. minutes vs. seconds and assessing motility at frequencies as low as 2 contractions per minute.46 With the quantification technique developed by Pritchard et al. laminar flow velocity and direction can be measured.16(Fig. 1H) GI tagging for GI applications is a new technique and the method and its clinical value are currently being explored. Therefore there is no software yet that is open to other researchers.

28
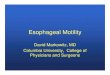
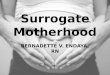
Figure 1. This figure visualizes the described quantification techniques. Coronal images A and B visualize the gastrointestinal tract at two moments in time (1 and 13 seconds) of a dynamic MRI movie used for visual assessment. A and B show contractility of the stomach (red arrows), several loops of the small bowel (green and blue arrows) and colon (yellow and orange arrows). Software-assisted (C) and manual (D) measurement of small bowel diameter are shown under the diameter measurement technique. The white circle marks the bowel segment used for analysis, below a plot of the calculated diameters representing motility.11 In E the deformation field of a coronal scan is visualized as a deformation grid used in the displacement mapping technique. Greater movement of underlying small bowel (delineated with green ROIs) occurs as greater distortion in the grid. F represents the analysis of a per-pixel deformation grid as a color-coded map.7 In G a coronal GI tagged image is visualized showing deformed taglines in the small bowel in green.46 In H a sagittal image shows movement within the colonic chime. The arrows highlight tag distortion (white arrow) and smearing and reduction of tag intensity (red arrow) due to movement.16 (Copyright granted)

29
Chapter 2
STUDY PROTOCOLSAssessment of GI motility with dynamic MRI can be carried out in various settings and protocols depending on the clinical question of interest. It is important to note that there are fundamental differences between the motility patterns in the GI tract during fasting (interdigestive state) and after ingestion of a meal (postprandial state). In the interdigestive state, the motility pattern is characterized by an alternation of periods with intense contractile activity and periods with motor quiescence.20 This cyclic pattern starts in the stomach and propagates slowly to the terminal ileum, hence the name migrating motor complex (MMC).47 Immediately after a meal, the MMC is interrupted at all levels, to be replaced by the postprandial motor pattern. In most dynamic MRI studies published so far, bowel preparation with a substantial volume of fluid, most often a mannitol solution, was given. It is likely that such preparation leads to induction of the postprandial motor pattern.40 Thus, the published results of MRI studies carried out until today pertain to a postprandial state induced by a non-physiological “meal”. This type of motility scan can be added to the standard abdomen MRI protocol and the motility can be quantified with one of the techniques described above. It has not yet been shown that the MMC can be detected with dynamic MRI, but it is likely that this is the case. Displacement mapping and MR tagging are techniques that can deal with the challenge of non-distended, “empty” bowel loops. MRI motility imaging can also be used to evaluate the response to food or a pharmacological agent. This requires a MRI protocol designed specifically for this type of response testing. These protocols can be used as a complementary test for diagnosis, but also for pathophysiological studies and drug development48. In this edition Khalaf et al. introduce a protocol with which the pan-intestinal motor response to a physiological test meal can be measured in a single MRI session.18 In their study, in a healthy volunteer cohort, the authors not only explored pan-intestinal motility and transit, but also compared the imaging parameters to GI peptide responses and to symptoms. With this novel approach, several measures of interest for the assessment of gastrointestinal motility can be obtained in one measurement session. In their paper Khalaf and co-workers set normal limits for gallbladder and gastric volumes, small bowel motility and water content, whole gut transit, GI peptides and symptom data when using this test meal. Others have described an under 60 minutes MRI protocol to examine gastric motility, accommodation and emptying together with the duodenal response following a simple water stimulus.4 We have used a practical 30-minutes stimulation test for small bowel motility assessment, demonstrating a significant response to a caloric challenge in fasted healthy subjects within a time frame of less than 10 minutes.40

30
CLINICAL IMPLEMENTATIONThe conventional techniques for evaluation of motility and transit in the human GI tract are well established, but are often invasive, ionizing, lengthy and cannot measure in the less accessible regions of the small bowel and colon. Therefore MRI is an exciting novel technique that creates new opportunities for research, clinical diagnosis, treatment follow-up and drug development. The following are examples of clinical applications of this imaging technique.
Crohn’s diseaseSeveral studies show that small bowel motility quantified with dynamic MRI can be used as a biomarker of inflammatory activity in Crohn’s disease and to differentiate healthy from diseased bowel.21,27,32,43,49 The motility in the terminal ileum was lower in Crohn’s patients in comparison to healthy subjects.43 It has been shown that the lesion detection rate is increased when static and dynamic MRI are combined.26,50 The motility patterns in Crohn’s disease revealed reduced contraction-wave frequencies, amplitudes, and decreased luminal occlusion rates.21,25
Bowel motility was inversely correlated with bowel diameter proximal to the stenosed segment.23 Motility changes of the terminal ileum showed correlation with histopathological findings both in active (P=0.006) and chronic Crohn’s disease (p=0.01).49 It was also shown that aberrant motility in Crohn’s disease is linked to inflammatory burden and patient symptoms.42 The first follow-up study in patients with Crohn’s disease receiving anti-TNFα treatment showed that MRI of small bowel motility accurately detects response to anti-TNFα therapy as early as 12 weeks. This suggests that the method allows for personalized medicine since it permits relatively early identification of nonresponse to anti-TNFα agents.41
These observations indicate that including the evaluation of small bowel motility in standard MRI of patients with Crohn’s disease may improve management.
GI motility disorders and functional bowel disordersA retrospective dynamic MRI study compared small bowel motility of patients with chronic intestinal pseudo-obstruction (CIPO) and patients with irritable bowel syndrome (IBS) to healthy subjects. The small bowel contractions in CIPO patients were found to be significantly weakened compared to IBS patients and healthy subjects.51 The results of a subsequent study in CIPO patients suggest that dynamic MRI is useful for the evaluation of the severity of CIPO by the prediction of severe clinical features.52 These findings were confirmed by a study in which the reader was blind to any clinical information, demonstrating a significantly decreased small bowel motility in CIPO patients compared to controls.24 Additionally, it was found that the response to a prokinetic drug may differ according to disease phenotype.

31
Chapter 2
A study in Ehlers-Danlos syndrome-Hypermobility type patients and controls showed that the increase in gastric motility following a water challenge was significantly lower in Ehlers-Danlos syndrome-Hypermobility type patients with functional dyspepsia compared to controls.4 In constipated patients a response assessment with an oral preparation stimulus revealed a significant difference in colonic motility between patients and healthy controls 60 minutes after ingestion.16
FUTURE PERSPECTIVESIn 1994 it was stated that MRI of the real-time motion of the gastrointestinal tract was in the embryonic state.53 Currently we can say that adolescence has been reached when it comes to the acquisition of the scans. However, the clinical field is in need of standardization and validation of the outcome metrics and subsequently assessment of the potential role of dynamic MRI. Up until this moment, motility MRI is rarely used in clinical routine but the body of (positive) evidence is growing and is opening doors to allow a widespread translational application. Future research should be aimed at improving our understanding of the pathophysiological postprandial GI response and validating the numerous MRI metrics in a range of disorders for diagnostic potential, treatment follow-up and drug development. On a technical note, more research into 3D acquisition and improved post-processing analysis techniques is eagerly awaited. Meanwhile, software must be further refined to stimulate translation into clinical routine. Ideally, the software will be fully automated, able to work with vast quantities of data, widely available and is designed with an intuitive user interface. Additionally, the software should offer the user a motility metric toolbox for local and global measurements.
CONCLUSIONSThere is a clinical need for a non-invasive technique that can assess motility and transit in the entire GI tract. Automated quantitative bowel motility assessment using dynamic MRI is likely to meet some of the hitherto unmet needs. Incorporated in clinical MRI protocols, or in the form of specifically designed motility-provoking protocols, dynamic MRI has potential as a future tool to investigate gastrointestinal motility disorders.

32
REFERENCES
1. Alyami J, Spiller RC, Marciani L. Magnetic resonance imaging to evaluate gastrointestinal function. Neurogastroenterol Motil. 2015;27(12):1687-1692.
2. Stehling MK, Evans DF, Lamont G, et al. Gastrointestinal Tract : Dynamic MR Studies with Echo-Planar Imaging. Radiology. 1989;171(1):41-46.
3. Wright J, Evans D, Gowland P, Mansfield P. Validation of antroduodenal motility measurements made by echo-planar magnetic resonance imaging. Neurogastroenterol Motil. 1999;11(1):19-25.
4. Menys A, Keszthelyi D, Fitzke H, et al. A magnetic resonance imaging study of gastric motor function in patients with dyspepsia associated with Ehlers - Danlos Hypermobility Type : A feasibility study. Neurogastroenterol Motil. 2017;(March):1-9.
5. Bickelhaupt S, Froehlich JM, Cattin R, et al. Software-supported evaluation of gastric motility in MRI: a feasibility study. J Med Imaging Radiat Oncol. 2014;58(1):11-17.
6. Wakamiya M, Furukawa A, Kanasaki S, Murata K. Assessment of small bowel motility function with cine-MRI using balanced steady-state free precession sequence. J Magn Reson Imaging. 2011;33(5):1235-1240.
7. Menys A, Taylor SA, Emmanuel A, et al. Global small bowel motility: Assessment with dynamic MR imaging. Radiology. 2013;269(2):443-450.
8. van der Paardt MP, Sprengers AMJ, Zijta FM, Lamerichs R, Nederveen AJ, Stoker J. Noninvasive automated motion assessment of intestinal motility by continuously tagged MR imaging. J Magn Reson Imaging. 2014;39(1):9-16.
9. Menys A, Plumb A, Atkinson D, Taylor SA. The challenge of segmental small bowel motility quantitation using MR enterography. Br J Radiol. 2014;87(1040).
10. Hahnemann ML, Nensa F, Kinner S, Gerken G, Lauenstein TC. Motility mapping as evaluation tool for bowel motility: Initial results on the development of an automated color-coding algorithm in cine MRI. J Magn Reson Imaging. 2014;41(2):354-360.
11. Bickelhaupt S, Froehlich JM, Cattin R, et al. Software-assisted quantitative analysis of small bowel motility compared to manual measurements. Clin Radiol. 2014;69(4):363-371.
12. Bickelhaupt S, Cattin R, Froehlich JM, et al. Automatic detection of small bowel contraction frequencies in motility plots using lomb-scargle periodogram and sinus-fitting method - Initial experience. Magn Reson Med. 2014;71(2):628-634.
13. Hoad CL, Menys A, Garsed K, et al. Colon wall motility: Comparison of novel quantitative semi-automatic measurements using cine MRI. Neurogastroenterol Motil. 2016;28(3):327-335.
14. Marciani L, Garsed KC, Hoad CL, et al. Stimulation of colonic motility by oral PEG electrolyte bowel preparation assessed by MRI: Comparison of split vs single dose. Neurogastroenterol Motil. 2014;26(10):1426-1436.
15. Lam C, Chaddock G, Marciani L, et al. Colonic response to laxative ingestion as assessed by MRI differs in constipated irritable bowel syndrome compared to functional constipation. Neurogastroenterol Motil. 2016;28(6):861-870.
16. Pritchard SE, Paul J, Major G, et al. Assessment of motion of colonic contents in the human colon using MRI tagging. Neurogastroenterol Motil. 2017;29(9):1-8.
17. Kirchhoff S, Nicolaus M, Schirra J, Reiser MF, Göke B, Lienemann A. Assessment of colon motility using simultaneous manometric and functional cine-MRI analysis: Preliminary results. Abdom Imaging. 2011;36(1):24-30.
18. Khalaf A, Hoad CL, Menys A, et al. MRI assessment of the postprandial gastrointestinal motility and peptide response in healthy humans. Neurogastroenterol Motil. 2017;(March):e13182.
19. De Jonge CS, Smout AJPM, Nederveen AJ, Stoker J. Supporting movie: 20s BH 2D bFFE sequence with a temporal resolution of 10 fps. https://onlinelibrary.wiley.com/doi/abs/10.1111/nmo.13257. Published 2018. Accessed April 14, 2019.
20. Quigley EMM. Gastric and small intestinal motility in health and disease. Gastroenterol Clin North Am. 1996:25(1):113-145.
21. Menys A, Atkinson D, Odille F, et al. Quantified terminal ileal motility during MR enterography as a potential biomarker of Crohn’s disease activity: A preliminary study. Eur Radiol. 2012;22(11):2494-2501.
22. Butt S, Menys A, Atkinson D, et al. PWE-181 Quantitative Assessment Of Global Small Bowel Motility In Chronic Intestinal Pseudo-obstruction And Controls: A Preliminary Study. Gut. 2014;25(Suppl 1):2014-2016.
23. Menys A, Helbren E, Makanyanga J, et al. Small bowel strictures in Crohn’s disease: A quantitative investigation of intestinal motility using MR enterography. Neurogastroenterol Motil. 2013;25(12):967-e775.

33
Chapter 2
24. Menys A, Butt S, Emmanuel A, et al. Comparative quantitative assessment of global small bowel motility using magnetic resonance imaging in chronic intestinal pseudo-obstruction and healthy controls. Neurogastroenterol Motil. 2016;28:376-383.
25. Bickelhaupt S, Froehlich JM, Cattin R, et al. Differentiation between active and chronic Crohn’s disease using MRI small-bowel motility examinations - Initial experience. Clin Radiol. 2013;68(12):1247-1253.
26. Hahnemann ML, Nensa F, Kinner S, et al. Improved detection of inflammatory bowel disease by additional automated motility analysis in magnetic resonance imaging. Invest Radiol. 2015;50(2):67-72.
27. Hahnemann ML, Nensa F, Kinner S, et al. Quantitative assessment of small bowel motility in patients with Crohn’s disease using dynamic MRI. Neurogastroenterol Motil. 2015;27(6):841-848.
28. de Jonge CS, Gollifer RM, Nederveen AJ, et al. Abstract 73 | Dynamic MRI for bowel motility imaging: How fast and how long? (Abstract). Neurogastroenterol Motil. 2017;29:37-38.
29. Taylor SA, Avni F, Cronin CG, et al. The first joint ESGAR/ ESPR consensus statement on the technical performance of cross-sectional small bowel and colonic imaging. Eur Radiol. 2016;27(6):1-13.
30. Nishino M, Iwata S, Hayakawa K, et al. Functional evaluation of the postoperative gastrointestinal tract using kinematic MR imaging: Quantitative assessment of peristaltic activity. Eur J Radiol. 2005;53(2):263-267.
31. Ghobrial PM, Neuberger I, Guglielmo FF, et al. Cine MR Enterography Grading of Small Bowel Peristalsis. Evaluation of the Antiperistaltic Effectiveness of Sublingual Hyoscyamine Sulfate. Acad Radiol. 2014;21(1):86-91.
32. Guglielmo FF, Mitchell DG, O’Kane PL, et al. Erratum to: Identifying decreased peristalsis of abnormal small bowel segments in Crohn’s disease using cine MR enterography: the frozen bowel sign. Abdom Imaging. 2015;40(5):1138-1149.
33. Kitazume Y, Satoh S, Hosoi H, Noguchi O, Shibuya H. Cine magnetic resonance imaging evaluation of peristalsis of small bowel with longitudinal ulcer in Crohn disease: preliminary results. J Comput Assist Tomogr. 2007;31(6):876-883.
34. Heye T, Stein D, Antolovic D, Dueck M, Kauczor H-U, Hosch W. Evaluation of bowel peristalsis by dynamic cine MRI: detection of relevant functional disturbances--initial experience. J Magn Reson Imaging. 2012;35(4):859-867.
35. Bickelhaupt S, Froehlich JM, Cattin R, et al. Software-assisted small bowel motility analysis using free-breathing MRI: Feasibility study. J Magn Reson Imaging. 2014;39(1):17-23.
36. Odille F, Menys A, Ahmed A, Punwani S, Taylor SA, Atkinson D. Quantitative assessment of small bowel motility by nonrigid registration of dynamic MR images. Magn Reson Med. 2012;68(3):783-793.
37. Hamy V, Menys A, Helbren E, et al. Respiratory motion correction in dynamic-MRI: Application to small bowel motility quantification during free breathing. Lect Notes Comput Sci (including Subser Lect Notes Artif Intell Lect Notes Bioinformatics). 2013;8150 LNCS(PART 2):132-140.
38. Hamy V, Dikaios N, Punwani S, et al. Respiratory motion correction in dynamic MRI using robust data decomposition registration - application to DCE-MRI. Med Image Anal. 2014;18(2):301-313.
39. Menys A, Hamy V, Makanyanga J, et al. Dual registration of abdominal motion for motility assessment in free-breathing data sets acquired using dynamic MRI. Phys Med Biol. 2014;59(16):4603-4619.
40. de Jonge CS, Menys A, van Rijn KL, Nederveen AJ, Stoker J. Abstract 78 | Volume vs caloric stimulation of small bowel motility in healthy controls (Abstract). Neurogastroenterol Motil. 2017;29:78.
41. Plumb AA, Menys A, Russo E, et al. Magnetic resonance imaging-quantified small bowel motility is a sensitive marker of response to medical therapy in Crohn’s disease. Aliment Pharmacol Ther. 2015;42(3):343-355.
42. Menys A, Makanyanga J, Plumb A, et al. Aberrant Motility in Unaffected Small Bowel is Linked to Inflammatory Burden and Patient Symptoms in Crohn’s Disease. Inflamm Bowel Dis. 2016;22(2):424-432.
43. Akerman A, Mansson S, Fork FT, et al. Computational postprocessing quantification of small bowel motility using magnetic resonance images in clinical practice: an initial experience. J Magn Reson Imaging. 2016;44(2):277-287.
44. Motilent, Ford, UK. http://www.motilent.co.uk/. Accessed October 4, 2017.45. Sprengers AMJ, van der Paardt MP, Zijta FM, et al. Use of continuously MR tagged imaging for
automated motion assessment in the abdomen: a feasibility study. J Magn Reson Imaging. 2012;36(2):492-497.

34
46. de Jonge CS, Sprengers AM, Nederveen AJ, Stoker J. Abstract 82 | Spectral bowel motility assessment using dynamic tagged MRI (Abstract). Neurogastroenterol Motil. 2017;29:43-44.
47. Deloose E, Janssen P, Depoortere I, Tack J. The migrating motor complex: control mechanisms and its role in health and disease. Nat Rev Gastroenterol Hepatol. 2012;9(5):271-285.
48. Hens B, Corsetti M, Spiller R, et al. Exploring gastrointestinal variables affecting drug and formulation behavior: Methodologies, challenges and opportunities. Int J Pharm. 2017;519(1-2):79-97.
49. Cullmann JL, Bickelhaupt S, Froehlich JM, et al. MR imaging in Crohn’s disease: correlation of MR motility measurement with histopathology in the terminal ileum. Neurogastroenterol Motil. 2013;25(9):749-e577.
50. Froehlich JM, Waldherr C, Stoupis C, Erturk SM, Patak MA. MR motility imaging in Crohn’s disease improves lesion detection compared with standard MR imaging. Eur Radiol. 2010;20(8):1945-1951.
51. Ohkubo H, Kessoku T, Fuyuki A, et al. Assessment of small bowel motility in patients with chronic intestinal pseudo-obstruction using cine-MRI. Am J Gastroenterol. 2013;108(7):1130-1139.
52. Fuyuki A, Ohkubo H, Higurashi T, et al. Clinical importance of cine-MRI assessment of small bowel motility in patients with chronic intestinal pseudo-obstruction: a retrospective study of 33 patients. J Gastroenterol. 2016:1-8.
53. Brown BP, Schulze-Delrieu K. Beginning the journey towards physiological imaging of gut motility. Gastroenterology. 1994;107(1):309-311.