Embed Size (px)
Citation preview
UvA-DARE is a service provided by the library of the University of Amsterdam (http://dare.uva.nl)
UvA-DARE (Digital Academic Repository)
Falling: should one blame the heart?
Jansen, Sofie
Link to publication
Citation for published version (APA):Jansen, S. (2015). Falling: should one blame the heart?
General rightsIt is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s),other than for strictly personal, individual use, unless the work is under an open content license (like Creative Commons).
Disclaimer/Complaints regulationsIf you believe that digital publication of certain material infringes any of your rights or (privacy) interests, please let the Library know, statingyour reasons. In case of a legitimate complaint, the Library will make the material inaccessible and/or remove it from the website. Please Askthe Library: http://uba.uva.nl/en/contact, or a letter to: Library of the University of Amsterdam, Secretariat, Singel 425, 1012 WP Amsterdam,The Netherlands. You will be contacted as soon as possible.
Download date: 27 Sep 2018

CHAPTER
ONE
INTRODUCTION
THE ASSOCIATION OF CARDIOVASCULAR DISORDERS AND FALLS:
A SYSTEMATIC REVIEW

1110 CHAPTER 1falling: should one blame the heart?
INTRODUCTION
Falls in older people form an increasing health care burden. Approxima-tely one in three people over the age of 65 will suffer a fall each year; one in five of these falls will lead to significant injury. As the world’s ageing population increases, healthcare costs associated with falls are set to rise over the next 30 years. It is estimated that over a third of falls may be preventable and evidence for causative, treatable factors is therefore essential. Cardiovascular disorders are among the several risk factors which have been identified to cause falls; in particular unexplained falls (defined as those for which no obvious attributable cause such as a trip or slip can be found) and recurrent falls. In part, this is due to the overlap between falls and syncope (a transient loss of consciousness due to de-creased blood supply to the brain) secondary to underlying cardiovascu-lar disease. Approximately one in three older people with syncope have amnesia for loss of consciousness and therefore present with a fall, rather than a faint or blackout.
Despite the overlap between falls and syncope in older adults, few well-designed studies have studied cardiovascular risk factors and their ma-nagement in falls prevention. Although causal associations between car-diac abnormalities, such as arrhythmias and structural cardiac abnormali-ties, and syncope have been well established, only few studies have as-sessed the association between these abnormalities and falls. Furthermo-re, very little evidence regarding the effectiveness of treatment of these conditions in reducing fall incidents exists. If we could establish the ex-tent of the associations between cardiac abnormalities and falls, this would aid into further determining which cardiovascular abnormalities deserve increased awareness in the assessment of older fallers, potential-ly leading to optimization of the care of older fallers.
Aim and outline of this thesisThe main aim of this thesis is to study the association between cardiovas-cular conditions and falls, in particular cardiac arrhythmia, conduction abnormalities and structural abnormalities. Because these conditions could lead to falls via several pathways, another aim was to study poten-tial mechanisms responsible for these associations.
In CHAPTER ONE we therefore examine which cardiovascular conditions have already been associated with falls through a systematic review of the literature. In CHAPTER TWO we report on the association between se-veral self-reported cardiovascular conditions and falls in community dwelling older adults. CHAPTER THREE AND FOUR describe the findings of a hospital study, in which clinically relevant ECG abnormalities and echo-cardiographic abnormalities were studied in hip-fracture patients compa-red with healthy controls. CHAPTER FIVE describes the findings of a general population study, in which the association between atrial fibrillation (AF), the most common cardiac arrhythmia in older adults, and falls and syn-cope was studied. The findings of chapter five led to the design of the studies described in CHAPTER SIX AND SEVEN, in which the association between AF and two important fall-related outcomes is studied. Firstly, the link between AF and mobility impairments is described. Secondly, it is shown that AF is associated with postural blood pressure changes. The second aim of this thesis is to explore the optimization of prevention of falls in older adults. Firstly, in CHAPTER EIGHT, the efficacy of extending the routine falls assessment with a comprehensive cardiovascular evalua-tion and treatment is studied. Secondly, in CHAPTER NINE it is studied which older people are aware of their increased fall risk, and wish to un-dergo a GP-based preventive treatment for falls. CHAPTER TEN provides a summary of the main findings of this thesis, and a discussion of the po-tential consequences of these findings for clinical practice and future re-search.
1312 CHAPTER 1falling: should one blame the heart?
ABSTRACT
BACKGROUND AND OBJECTIVE Cardiovascular disorders are recognized as risk factors for falls in older adults. The aim of this systematic review is to identify cardiovascular disor-ders that are associated with falls, thus providing several angles for opti-mization of fall-preventive care.
DESIGN Systematic review. A search was performed in Medline and Embase and included studies addressing persons aged 50 years and older that descri-bed cardiovascular risk factors for falls. Key search terms for cardiovascu-lar abnormalities included all synonyms for the following groups: structu-ral cardiac abnormalities, cardiac arrhythmia, blood pressure abnormali-ties, carotid sinus hypersensitivity (CSH), orthostatic hypotension (OH), vasovagal syncope (VVS), postprandial hypotension (PPH), arterial stiff-ness, heart failure and cardiovascular disease. Quality of studies was as-sed using the Newcastle-Ottawa-Scale.
RESULTS Eighty-six studies were included. Of studies that used a control group, most consistent associations with falls were observed for low blood pres-sure (4/5 studies showing a positive association), heart failure (4/5) and cardiac arrhythmia (4/6). Higher prevalences of CSH (4/6), VVS (2/2) and PPH (3/4) were reported in fallers compared to controls in the majority of studies, but most of these studies failed to show clear association measu-res. Coronary artery disease (6/10), orthostatic hypotension (9/25), gene-ral cardiovascular disease (4/9) and hypertension (7/25) all showed in-consistent associations with falls. Arterial stiffness was identified as an independent predictor for falls in one study, as were several echocardio-graphic abnormalities.
CONCLUSION Several cardiovascular associations with falls were identified, including low BP, heart failure and arrhythmia. These results provide several angles for optimizing fall-preventive care, but further work on standard definiti-ons, as well as the exact contribution of individual risk factors on fall inci-dence is now important to find potential areas for preventive interventi-ons.
THE ASSOCIATION OF CARDIOVASCULAR DISORDERS AND FALLS:
A SYSTEMATIC REVIEW
Sofie Jansen*Jaspreet Banghu*
Sophia E.J.A. de RooijJoost G. Daams
Rose Anne KennyNathalie van der Velde
*Joint first authors
Accepted for publication, J Am Med Dir Assoc

1514 CHAPTER 1falling: should one blame the heart?
METHODS
A systematic search was conducted to include all articles that addressed the question of possible cardiovascular contributions to falls in adults over the age of 50 years. Our review methodology and reporting follo-wed standard guidance 12.
Search strategyIn collaboration with a clinical librarian (JD), a systematic search was conducted in PubMed and Embase for articles published until the date of the search (March 30, 2015). A customized search strategy was conduc-ted for each database. A manual search of references in the selected arti-cles was also conducted to identify additional studies. Key search terms were ‘falls’, ‘aged’ and ‘cardiovascular’. Full details of the search strategy are available as Supplementary data, Appendix S1 as well as the actual search strategy used; Supplementary data, Appendix S2. Two reviewers (SJ and JB) first independently screened titles and abstracts for inclusion and then read the full text of the eligible articles found during this first selection. In case of differences between the two reviewers, a third inde-pendent reviewer was consulted (NV).
Inclusion/exclusion criteriaStudies were included if they were published as a primary research paper in a peer reviewed journal, included persons aged 50 years or older, de-fined falls as an outcome measure and included diagnosis or assessment of cardiovascular abnormalities. Search terms for cardiovascular abnormalities included all synonyms and differentiations for: structural cardiac abnormalities (impaired ventricular function, heart valve abnormalities), cardiac arrhythmia (CA), blood pres-sure abnormalities (SBP and DBP), carotid sinus hypersensitivity (CSH), orthostatic hypotension (OH), postprandial hypotension (PPH), arterial stiffness (AS), heart failure (HF), angina, myocardial infarction (MI) and general cardiovascular or circulatory disease (CVD). Cardiovascular as-sessments included: Electrocardiogram (ECG), holter monitoring (HM), prospective external event recorders, external loop recorders (ELR), im-plantable loop recorders (ILR), remote telemetry, echocardiogram, caro-tid sinus massage (CSM), assessment of orthostatic hypotension or im-paired BP recovery upon active stand, tilt table testing (HUT), electrop-hysiological studies, exercise stress testing and/or cardiac catheterization. Articles using self-report of doctor-diagnosed cardiovascular abnormali-ties or disease were included also, but only for the following conditions:
INTRODUCTION
Falls are the leading cause of injury in older people 1, 2. Approximately one in three people over the age of 65 will suffer a fall each year, with injuries occurring in at least one in five of these 3. As the world’s ageing population increases, healthcare costs associated with falls are set to rise over the next 30 years 4. As it is estimated that up to 40% of falls may be preventable, evidence for causative, treatable factors is essential 5.
Cardiovascular disorders are among the several risk factors which have been identified to cause falls; in particular unexplained falls (defined as those for which no attributable mechanical cause such as a trip or slip can be found) and recurrent falls 6. Syncope secondary to underlying car-diovascular disease is more common in older adults and may lead to in-jurious falls 7.
As there is considerable overlap between the symptoms of falls and syn-cope in older adults, there is likely an underestimation for the role of cardiovascular abnormalities in fall risk 8. Orthostatic hypotension, caro-tid sinus hypersensitivity, vasovagal syncope and cardiac arrhythmias are the main cardiovascular disorders that can cause syncope in older adults, but evidence linking these abnormalities to falls included in current falls guidelines is scarce.
Up to now, one systematic review has been published that addressed car-diovascular causes of falls 9. However, no quality assessment of included articles was performed in this review, and a first selection of articles was based on titles alone, potentially causing certain articles to have been overlooked. Two recent reviews have studied the association between or-thostatic hypotension and falls, but these studies did not assess other po-tential cardiovascular causes of falls 10, 11. Furthermore, as the subject has gained attention in the last five years, there is a need to update earlier reports. The aim of this review was to identify cardiovascular risk factors for falls systematically and to thereby provide a broad overview of the available literature.
1716 CHAPTER 1falling: should one blame the heart?
Data Synthesis and AnalysisAs included studies were heterogeneous in design and assessment me-thods, a descriptive approach was used to summarize study characteris-tics and outcomes. Studies that were included were categorized per ex-posure. No statistical pooling was conducted.
RESULTS
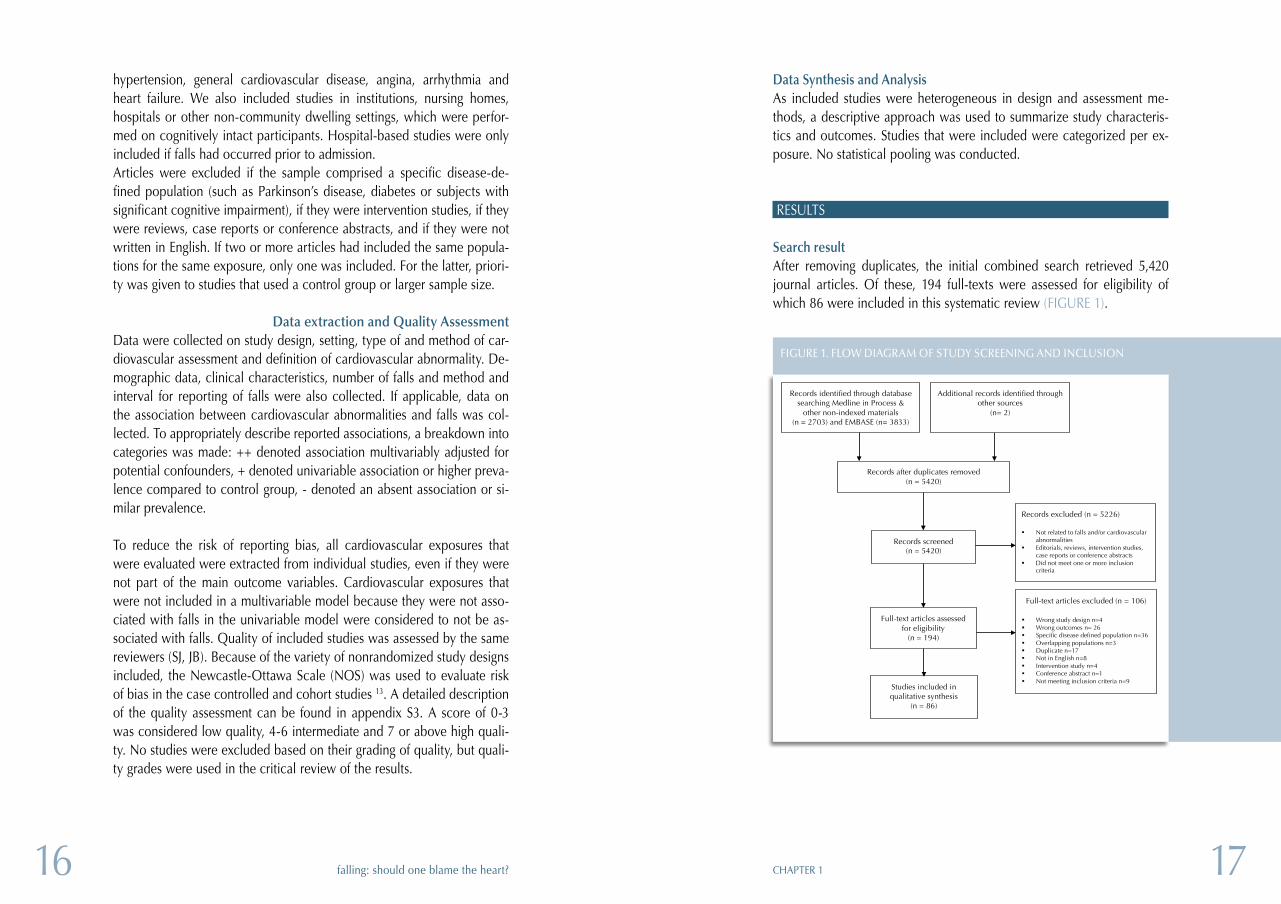
Search resultAfter removing duplicates, the initial combined search retrieved 5,420 journal articles. Of these, 194 full-texts were assessed for eligibility of which 86 were included in this systematic review (FIGURE 1).
hypertension, general cardiovascular disease, angina, arrhythmia and heart failure. We also included studies in institutions, nursing homes, hospitals or other non-community dwelling settings, which were perfor-med on cognitively intact participants. Hospital-based studies were only included if falls had occurred prior to admission. Articles were excluded if the sample comprised a specific disease-de-fined population (such as Parkinson’s disease, diabetes or subjects with significant cognitive impairment), if they were intervention studies, if they were reviews, case reports or conference abstracts, and if they were not written in English. If two or more articles had included the same popula-tions for the same exposure, only one was included. For the latter, priori-ty was given to studies that used a control group or larger sample size.
Data extraction and Quality AssessmentData were collected on study design, setting, type of and method of car-diovascular assessment and definition of cardiovascular abnormality. De-mographic data, clinical characteristics, number of falls and method and interval for reporting of falls were also collected. If applicable, data on the association between cardiovascular abnormalities and falls was col-lected. To appropriately describe reported associations, a breakdown into categories was made: ++ denoted association multivariably adjusted for potential confounders, + denoted univariable association or higher preva-lence compared to control group, - denoted an absent association or si-milar prevalence.
To reduce the risk of reporting bias, all cardiovascular exposures that were evaluated were extracted from individual studies, even if they were not part of the main outcome variables. Cardiovascular exposures that were not included in a multivariable model because they were not asso-ciated with falls in the univariable model were considered to not be as-sociated with falls. Quality of included studies was assessed by the same reviewers (SJ, JB). Because of the variety of nonrandomized study designs included, the Newcastle-Ottawa Scale (NOS) was used to evaluate risk of bias in the case controlled and cohort studies 13. A detailed description of the quality assessment can be found in appendix S3. A score of 0-3 was considered low quality, 4-6 intermediate and 7 or above high quali-ty. No studies were excluded based on their grading of quality, but quali-ty grades were used in the critical review of the results.
Records identified through database searching Medline in Process &
other non-indexed materials (n = 2703) and EMBASE (n= 3833)
(total 6536)
Additional records identified through other sources
(n= 2)
Records after duplicates removed (n = 5420)
Records screened (n = 5420)
Records excluded (n = 5226)
§ Not related to falls and/or cardiovascular abnormalities
§ Editorials, reviews, intervention studies, case reports or conference abstracts
§ Did not meet one or more inclusion criteria
Full-text articles assessed for eligibility
(n = 194)
Full-text articles excluded (n = 106)
§ Wrong study design n=4 § Wrong outcomes n= 26 § Specific disease defined population n=36 § Overlapping populations n=3 § Duplicate n=17 § Not in English n=8 § Intervention study n=4 § Conference abstract n=1 § Not meeting inclusion criteria n=9
Studies included in qualitative synthesis
(n = 86)
FIGURE 1. FLOW DIAGRAM OF STUDY SCREENING AND INCLUSION
1918 CHAPTER 1falling: should one blame the heart?
Carotid sinus hypersensitivity (CSH)Twenty-one studies had investigated CSH as an exposure (TABLE 3). Five were designed as case-control studies; one reported a positive associati-on between neurally mediated syncope and unexplained falls compared to accidental falls; three reported a higher prevalence of CSH in fallers compared to controls. Fifteen observational series were performed which reported a prevalence of between 8-73%. Eighteen studies performed both supine and upright (70⁰) carotid sinus massage; two were supine only. All studies defined CSH as asystole greater than 3 seconds on ECG or a vasodepressor drop of 50mmHg in systolic blood pressure. Five stu-dies used symptom reproduction during carotid sinus massage to diffe-rentiate carotid sinus syndrome from carotid sinus hypersensitivity. All studies had a low to intermediate NOS quality level.
Vasovagal syncope (VVS)Ten studies had investigated vasovagal syncope as an exposure for falls (TABLE 4); two used a case control design, both of which reported that VVS was more common in fallers. Eight observational series reported a prevalence of VVS between 3-46%. All studies had used a head up tilt table test as the measurement method. All were graded as low to inter-mediate on the NOS quality score.
Hypertension (HTN)Twenty-seven studies assessed hypertension as an exposure for falls; 22 were designed as cohort studies, three as case controls (TABLE 5). Of the 25 studies with a control group, five reported a positive multivariably ad-justed association between HTN and falls and two reported a higher pre-valence of HTN among fallers compared to controls. Two studies repor-ted a negative association between HTN and falls.
The two observational series reported a prevalence of HTN among fallers between 34-73%. Nine studies only used self-report of HTN; five used medical charts only, six studies used an objective measurement of BP and/or use of anti-hypertensive to diagnose HTN, five used a combinati-on of self-report and medical charts, one used both objective and self-reporting methods and one study did not report the measurement me-thod. Of studies that used an objective measurement, different cut-offs for HTN were used, ranging from >130/80 mmHg to >160/95 mmHg. Only two studies were considered high quality on the NOS scale, neither of which showed a positive association between HTN and falls.
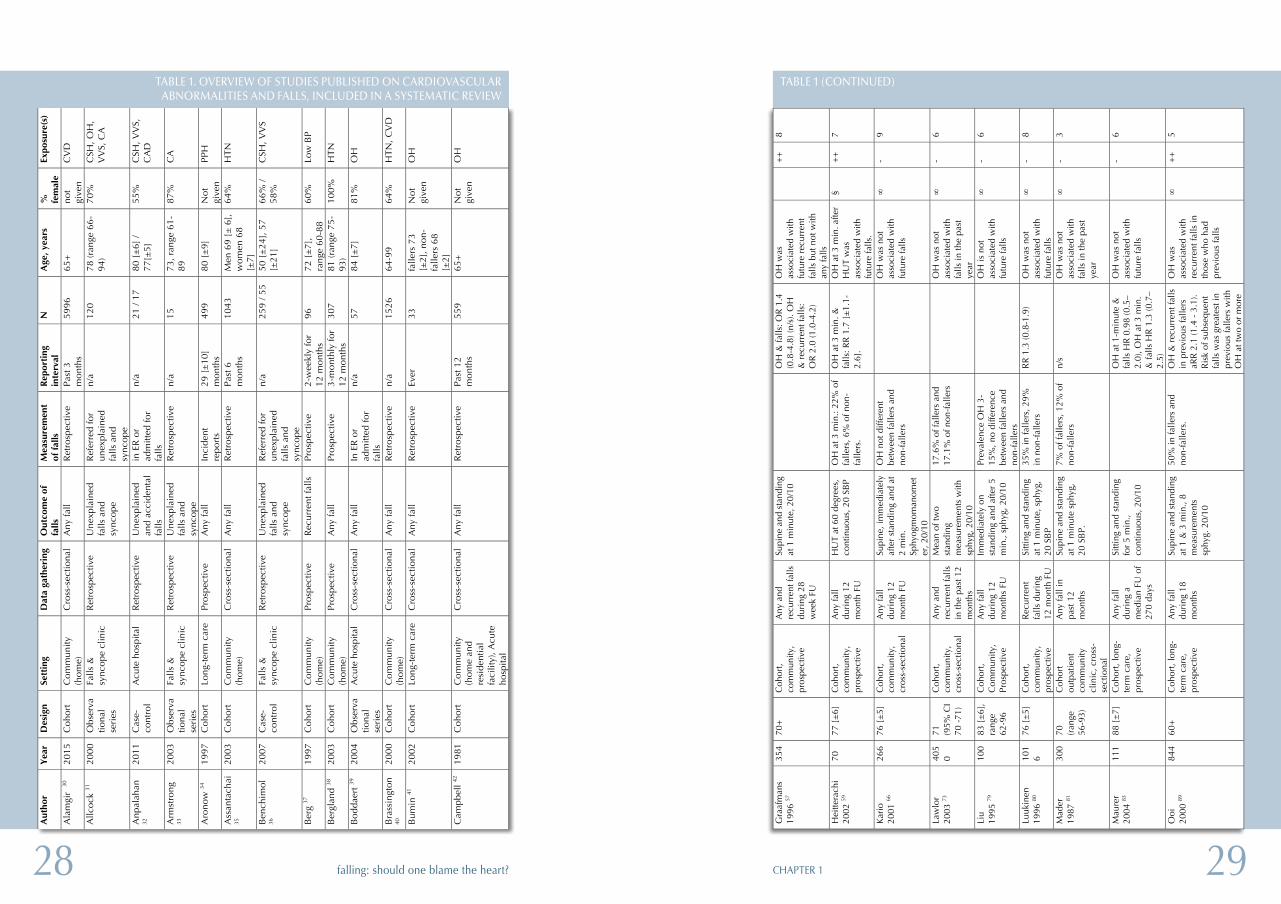
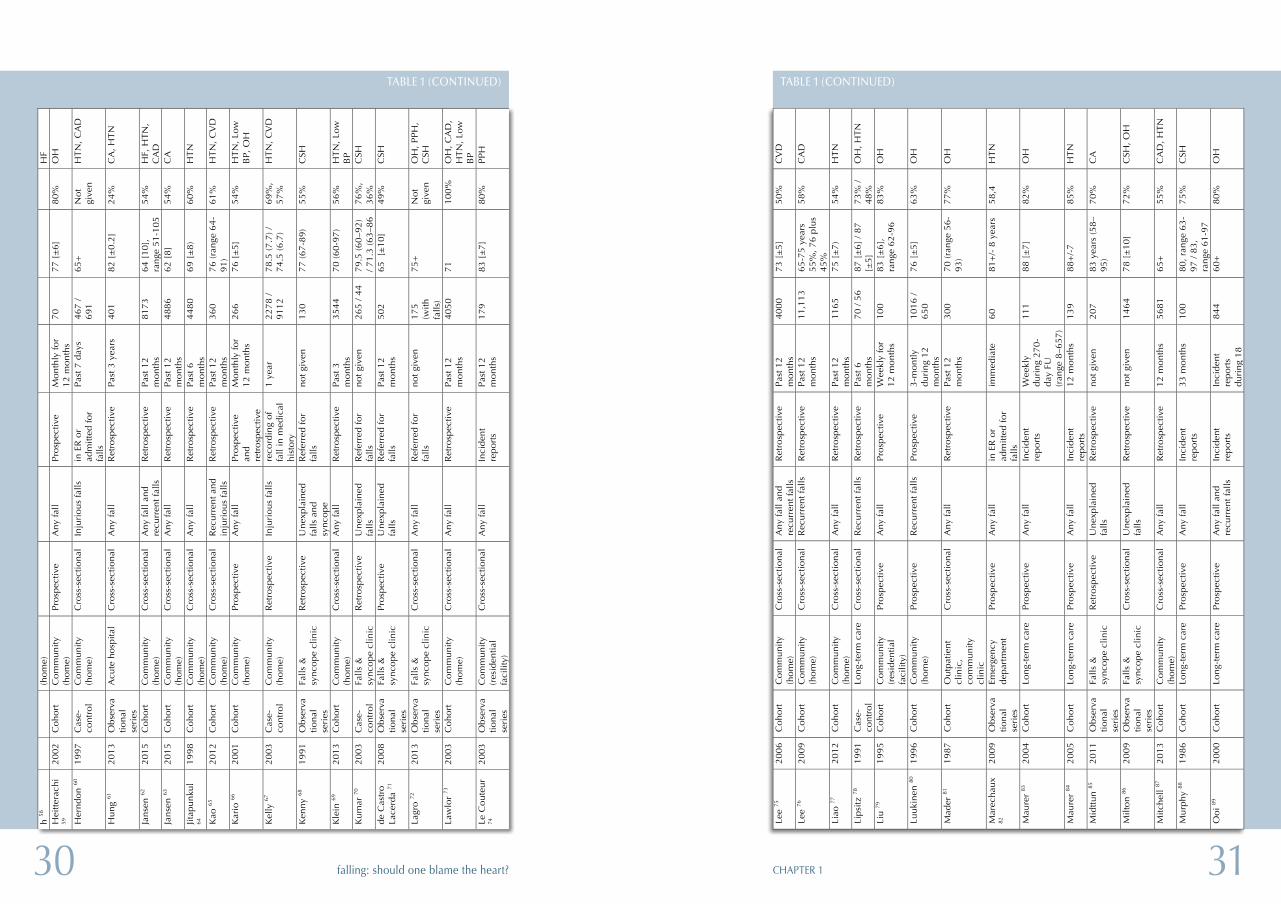
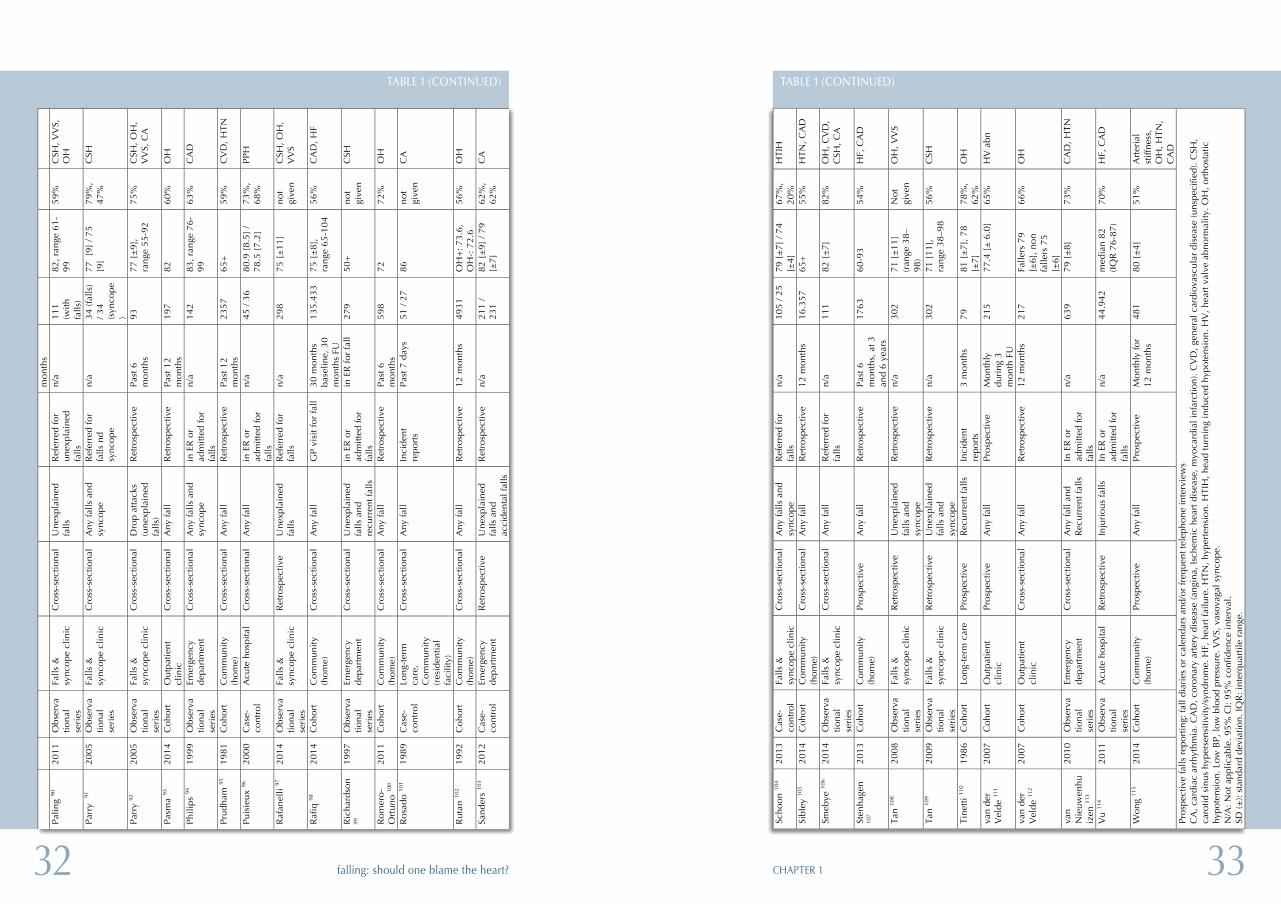
Characteristics of the Studies TABLE 1 shows the characteristics of included studies. Forty-eight stu-dies were cohort studies, thirteen were case–control studies and 25 were observational series. Numbers of study participants in each study varied from 13 to 135,433. Mean age varied from 50 to 88 years.
Of included studies, 39 were conducted in the community, nine in long-term care facilities, one in both community and long term care, 24 in outpatient clinics (20 in specialized falls- and syncope clinics), eight in emergency departments and five in acute hospital settings. Fifty-one studies used any falls as an outcome measure, eight used recur-rent falls, eight used unexplained falls, twelve studies used falls and/or syncope as an outcome, and two studies used unexplained falls descri-bed as ‘drop attacks’.Eleven types of cardiovascular abnormalities (exposures) were identified with 39 studies assessing more than one risk factor. OH as a risk factor for falls was examined in (36), followed by hypertension (27), CSH (21), general cardiovascular disease (9), Angina and MI (grouped as coronary artery disease) (14), arrhythmia (12), vasovagal syncope (10), heart failure (6), low BP (5), post prandial hypotension (4), and structural cardiac ab-normalities (3).
TABLES 2-11 show results of includes studies, categorized per cardiovas-cular risk factor and type of study
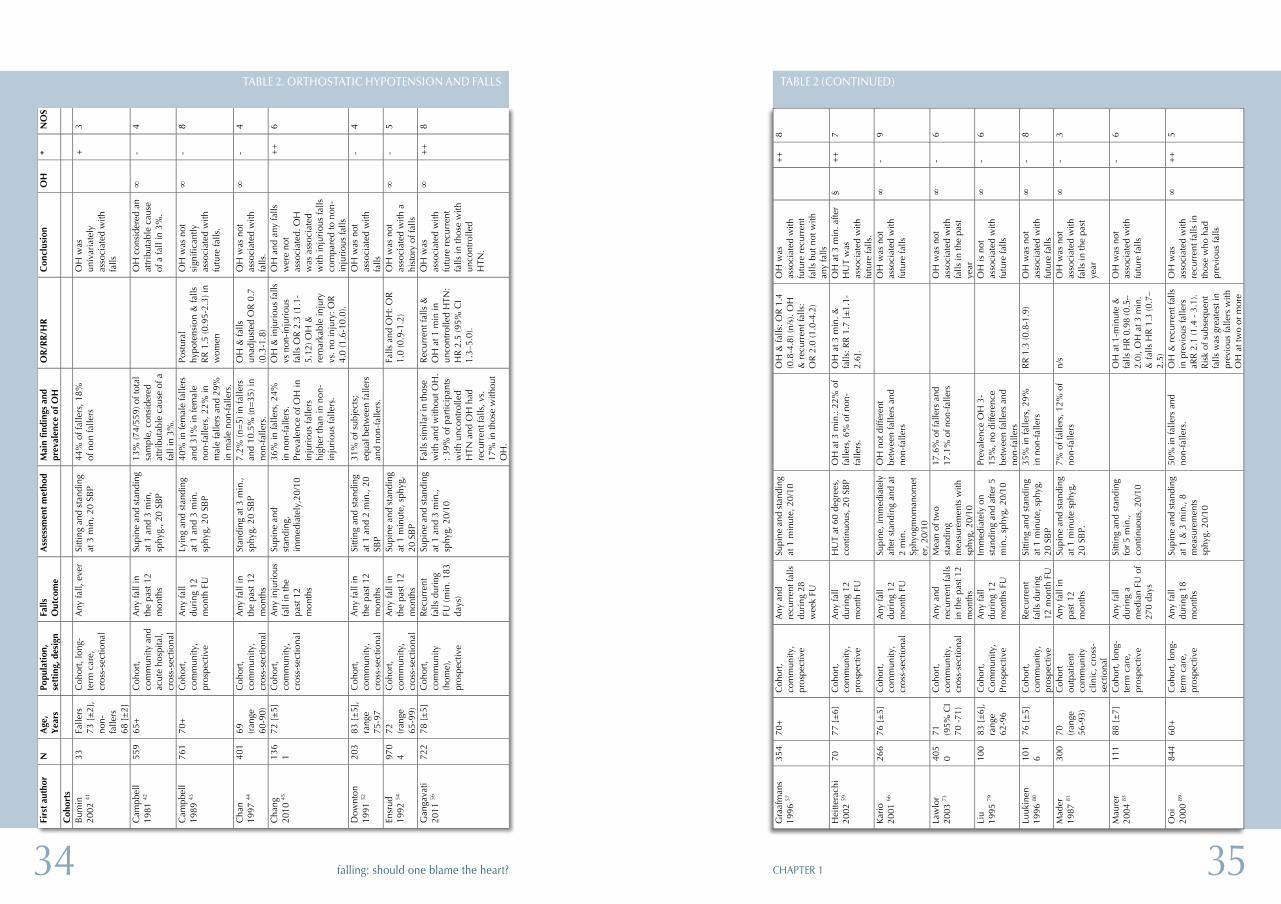
Orthostatic hypotension (OH)OH was studied as an exposure in 36 studies; 23 of which were designed as cohort studies and two as case-control studies (TABLE 2). Six studies reported a positive multivariably adjusted association with falls; three stu-dies reported a higher prevalence of OH in fallers. Eleven observational design studies reported a prevalence of between 5-56% of fallers.
OH was defined as a drop of greater than 20 mmHg SBP and/or greater than or equal to 10 mmHg DBP drop in twenty studies, greater than 20mmHg SBP drop in twelve studies while the four studies did not report a value. Fifteen studies used intermittent BP measurements, twelve stu-dies used continuous measurement with photopletysmography, two stu-dies used both methods, and seven studies did not specify their study in-strument. Seven studies were scored as high quality with the remainder (how many) scoring low and intermediate on the NOS scale
2120 CHAPTER 1falling: should one blame the heart?
one reported no association. The case control studies both reported a higher prevalence of PPH in fallers compared to controls. PPH was de-fined and measured in different ways in all studies. All studies were rated as low to moderate on the quality rating scale.
Arrhythmia Twelve studies studied cardiac arrhythmia as an exposure; three were de-signed as cohort studies, three were case-control studies (TABLE 10). Of these six studies, four reported a positive, multivariably adjusted associa-tion between arrhythmia and falls, of which three were studies on AF.
Six observational design studies reported a prevalence of between less than 1% and 27%. There was a variety of measurements performed; Im-plantable loop recorder (ILR)(for extended arrhythmia monitoring beyond 30 days) in one study, external loop recorder (ELR) (for arrhythmia moni-toring up to 30 days) in one study, holter monitoring (for arrhythmia mo-nitoring up to 24 hours), 12-lead ECG, cardiac telemetry (in-patient arr-hythmia monitoring) and medical chart review. This resulted in a variety of definitions used for cardiac arrhythmia. Two studies were graded as high quality on the NOS scale whilst the remainder were of low or inter-mediate quality.
Heart failureSix studies looked at heart failure as an exposure; five cohort studies, with four reporting a positive, multivariably adjusted association between CHF and falls (TABLE 11). One study used the New York Heart Associati-on Classification for heart failure and one study used the NHS–Read co-ding for classification. All studies that reported an association measure were of intermediate or high quality.
Structural abnormalitiesThree studies looked at exposures that could not be categorized under other exposures (TABLE 12). Wong et al. studied arterial stiffness in a prospective cohort, and found that the top quintile of pulse wave velocity (indicating arterial stiffness) was an independent predictor of future falls.
Schoon et al. studied head-turning induced hypotension in a case control study in a falls and syncope clinic. Prevalence of a drop in SBP following these movements was high, but not different between cases and controls.
Low blood pressure (LBP)Five studies looked at low blood pressure as an exposure in cohort stu-dies (TABLE 6). Four showed a positive, multivariably adjusted associati-on between low BP and falls; one did not. Prevalence of hypotension among fallers varied, from 7% to 74%. All studies used an objective mea-surement of blood pressure, but various thresholds for diagnosing hypo-tension were used, ranging from 100 mmHg to 142 mmHg for systolic blood pressure (SBP), and from 60 mmHg to 80mmHg for diastolic blood pressure (DBP). The one study that did not show an association also used the lowest BP cut-off (SBP/DBP ≤100/60). Four out of five studies were rated high quality on the NOS scale.
Coronary artery disease (CAD)Fourteen studies assessed the association between MI or angina (grouped as coronary artery disease) and falls (TABLE 7). Ten studies used a control group, of which five reported a positive multivariably adjusted associati-on between CAD and falls and four reported no association. The four observational series reported a prevalence of 0.9% for acute MI, to 76% for IHD. Six studies used self-reported history of MI or angina; four used medical chart history of MI or angina, three used a combination of medical re-cords and self-report and one used a clinical definition to define MI (myocardial infarct evidenced by chest pain and/or serial ECG’s). All co-hort studies scored intermediate or high on the NOS scale whilst the ob-servational series scored low to intermediate on the NOS scale.
General Cardiovascular Disease (CVD)Nine studies looked at general CVD without breakdown into specific car-diovascular diseases (TABLE 8). Seven used a cohort design; one was a case control study. Two out of these nine studies showed a multivariably adjusted association between cardiovascular disease and falls, two stu-dies showed a higher prevalence of cardiovacular disease among fallers and four studies did not show an association. The one observational stu-dy reported a prevalence of cardiovascular disease of 52%. Four used self-report of CVD, three used medical records while two used both me-thods. All studies were graded as low to intermediate on the NOS scale.
Postprandial hypotensionFour papers studied post-prandial hypotension (PPH) as an exposure for falls; two cohort and two case control studies (TABLE 9). One reported a positive, multivariably associated association between PPH and falls and

2322 CHAPTER 1falling: should one blame the heart?
nic damage to the areas of the brain which govern balance and gait 14 through neurodegeneration. In addition to an association with falls, LBP has been associated with stroke and cognitive impairment 15-17. Conver-sely, hypertension was associated with falls after adjustment for confoun-ders in only a small number of studies reviewed, and hypertension even showed a protective effect on fall incidence in two studies. It has been reported previously that blood pressure behaviour is not uniform throug-hout all age groups and may demonstrate a U shaped curve, especially with regard to its effect on the incidence of stroke and mortality 18, 19. Adults in the oldest age categories have not been shown to benefit from aggressive lowering of their blood pressure and in fact may be harmed by low blood pressure 19. However, whether LBP, or conditions causing LBP can been seen as causative or contributory factors to falls remains unclear. A consistent association with falls was also seen for heart failure (4/5). HF can lead to a reduction in cardiac output in demanding situati-ons such as exertion and postural changes, which may explain this fin-ding, and strengthens the finding of the association between LBP and falls. Further work on the effects of transient changes in blood pressure is needed to delineate thresholds by which older adults are more prone to falling and elucidate treatment strategies for this.
The majority of studies on arrhythmia and falls showed a positive associ-ation. Both length of monitoring time and the definition used for CA had a large influence on the reported associations. Those studies that em-ployed a monitoring time longer than 24 hours showed a positive correla-tion with CA and falls. Studies that focused on finding a causative arr-hythmia detected a prevalence of between 15-46%. However these were in predominantly observational series, limiting the applicability of this finding. Interestingly, the three studies which exclusively defined atrial fi-brillation as an arrhythmia reported a positive association with falls. As these were done in cross-sectional studies, causation could not be ascri-bed. Cardiac arrhythmias are a potentially treatable cause of falls and this review highlights the inconsistencies with which they are reported on, li-miting the ability to make a definitive statement of the contribution of CA to falls risk.
Although OH is a commonly accepted cardiovascular cause of falls in older persons, only a minority of studies reported a positive association with falls. However, quality of included studies varied and several assess-ment methods to detect OH were used. We included studies that used intermittent methods of BP detection as well as continuous methods, nei-
Van der Velde et al. assessed the association between echocardiographic abnormalities and future falls. Several heart valve abnormalities were in-dependent predictors of future falls: mitral-, tricuspid and pulmonary val-ve regurgitation and pulmonary hypertension.
DISCUSSION
Main resultsA systematic review of the literature shows strong associations between cardiovascular disorders and falls. Of studies that used a control group, the most consistent associations with falls were observed for low blood pressure (4/5), heart failure (4/5) and cardiac arrhythmia (4/6), as the ma-jority of these studies showed a positive association with falls after per-forming multivariable adjustment for potential confounders. For carotid sinus hypersensitivity (4/6), vasovagal syncope (2/2) and post-prandial hypotension (3/4), the majority of studies reported a higher prevalence of the exposure in fallers compared to controls, but only few multivariable adjusted associations were reported. Coronary artery disease (6/10), or-thostatic hypotension (9/25), general cardiovascular disease (4/9) and hy-pertension (7/25) all showed inconsistent associations with falls, with a similar or smaller amount of studies reporting positive associations as stu-dies reporting no associations with falls. Hypertension even showed a protective effect on falls in two out of 25 studies. Finally, arterial stiffness was identified as an independent predictor for falls in one study, as were several echocardiographic abnormalities.Although orthostatic hypotension, carotid sinus syndrome and vasovagal syncope are most frequently cited as important cardiovascular causes of falls, the evidence on the association between these blood pressure syn-dromes and falls was inconsistent, mainly due to a lack in adequate con-trol groups and reporting of association measures that were adjusted for potential confounders. Surprisingly, more consistent positive associations were found for LBP, heart failure and cardiac arrhythmia. A range of stu-dies examining the association of blood pressure and falls was evaluated. Although these studies differed significantly in their methods, certain trends were apparent.
Low blood pressure showed a consistent association with falls. It has been hypothesized that transient reduction in cerebral perfusion pressure may not only lead to immediate effects of cerebral hypoperfusion (e.g. synco-pe or falls during exertion or postural changes) but may also lead to chro-

2524 CHAPTER 1falling: should one blame the heart?
There is a lack of evidence regarding interventions to reduce falls risk by treating cardiovascular disorders alone. Up to now, only OH and CSH (which are commonly classified as syncope syndromes 25) have been in-cluded in intervention trials, which have shown benefit in preventing re-current syncope and falls. Multifactorial interventions that include recog-nition and treatment of OH have been shown to be effective in reducing falls 6. Furthermore, a recent Cochrane review on interventions aimed at reduction of falls rates has identified only dual chamber pacemaker inser-tion as having a proven benefit for reduction of falls in those patients with CSS 26. This review demonstrates a strong overlap between CV conditions that commonly lead to syncope and those that lead to falls. It thus enhan-ces previous guideline conclusions that have aimed to incorporate the potential impact that cardiovascular abnormalities were thought to have on falls 6.
The European Society of Cardiology (ESC) has stated the need to consider syncope as the cause of a fall in those with unexplained falls 25. Syncope mistaken for falls presents a difficult clinical challenge as up to 50% of ol-der persons suffer from retrograde amnesia after vasovagal syncope, and eye-witnesses are often absent 27. This may in part have accounted for the large variation in prevalence rates of VVS reported. Carotid sinus hyper-sensitivity is a condition that is also considered a form of reflex syncope 25. Prevalence rates of between 10-40% were consistently reported in fal-lers with two notable outliers. In addition, studies conducted in patients with unexplained and recurrent falls were able to attribute CSH as the cause of these falls. As dual chamber pacemaker insertion has been found to be beneficial for treating cardio inhibitory CSS, this has important impli-cations for clinical practice 28. Controversy exists over terminology and definitions, as some authors define carotid sinus syndrome (CSS) as an ab-normal response to carotid sinus massage (CSM) only when accompanied by symptom reproduction of syncope 29. This is distinct from carotid sinus hypersensitivity (CSH), which would produce an abnormal response to CSM without definite symptom reproduction. In this review only five studies had included the presence of symptoms in their definition of CSS but thirteen studies reported on CSS as being present. Despite difficulties in ter-minology this review does reveal a higher incidence of CSH in fallers. Ho-wever, the prevalence rates reported may be skewed by definitions used.
ther of which showed a consistent association with falls. Finucane et al. have recently reported new normative data for definitions of OH, using non-invasive, beat-to-beat BP measurements 20. Whilst they reported that initial OH (within 15 seconds) occurred in up to a third of the population, impaired blood pressure stabilization at 40 seconds was present in 16% of subjects and ‘classical’ OH at or after one minute of standing was pre-sent in a much smaller number of subjects (7%). Most studies included in this review assessed OH at one minute of standing or beyond, potentially explaining why only a minority of studies found a positive association between OH and falls. In addition, only a small amount of studies inclu-ded symptom correlation for diagnosing OH or did not specifically report these results, leaving a gap regarding the value of symptom correlation in diagnosing OH. It does appear that OH does not follow a uniform distri-bution in the population, and intermittent measurements (such as those with a standard sphygmomanometer) may underestimate the true preva-lence of OH and its clinical importance. With the rise of the use of conti-nuous measurement of OH, more complete research can be performed to determine the full association between OH and falls.Cardiovascular disease, which comprised angina, ischemic heart disease and arterial disease, showed a positive association with falls in a few stu-dies, as did arterial stiffness. However, cardiovascular disease represents a diverse group of disorders, rendering it difficult to establish individual mechanisms that may contribute to falls risk. Potential interacting mecha-nisms include direct damage to affected end organs, such as the heart or brain or downstream impacts on physiological homoeostasis.
Macro- or microvascular arterial disease may impair muscle capacity and motor- and sensory nervous function with deleterious effects on gait. Frailty syndromes have also been shown to have a higher prevalence in cardiovascular diseases contributing to increased falls risk 21. Lastly, treat-ments used for cardiovascular disorders have been linked to increases in falls both through direct effects of drugs on the cardiovascular system as well as polypharmacy 22. There is evidence that drug withdrawal of CV drugs may reduce falls rates in practice 23, potentially through an impro-vement in postural blood pressure changes 24. Although the exact mecha-nisms remain difficult to elucidate, this review has shown that clinicians should regard those patients with a diagnosis of cardiovascular disease at a higher risk of falls.

2726 CHAPTER 1falling: should one blame the heart?
CONCLUSION
Cardiovascular disease has a high prevalence in older adults with falls. There is a clear association between hypotension and falls, whilst conver-sely those patients with hypertension demonstrate a lower prevalence of falls in some studies. Furthermore, both heart failure and arrhythmia (in particular AF) are consistently associated with falls. There is also a posi-tive association demonstrated between syndromes that cause syncope such as CSH, VVS and OH, and falls, although the evidence regarding the association between OH and falls remains inconsistent. Efforts at un-locking the exact contribution of each variable to falls risk are hampered by a lack of standard definitions, methods of assessment and the low quality of available studies. Further work on standard definitions as well as the exact contribution of individual risk factors is of major importance to find potential areas for intervention.
Clinical implications and Future perspectivesThis systematic review has highlighted a number of studies, which have shown easily measurable cardiovascular parameters that may contribute to falls risk in older patients. The clinical implications of these associati-ons are important in evaluation of falls risk reduction. Consensus is nee-ded to adopt standard definitions of cardiovascular risk factors, as well as the resources and settings needed to systematically evaluate older adults at risk of falls, for the presence of cardiovascular disease. As up to 40% of falls may be preventable, a standardised assessment of cardiovascular risk factors is essential for falls prevention 5. There is a need for treatment tri-als to be designed and carried out in order to gauge the treatment bene-fits, which may accrue by systematic review and treatment of underlying CV abnormalities in older patients.
LimitationsDifferences in disease definition and the disparities between the quality of included studies make it impossible to perform a proper meta-analy-ses. This in turn limits our ability to describe the strength of associations between cardiovascular disorders and falls. Therefore, as mentioned abo-ve, it is of major importance to reach consensus for standard definitions. As we have pointed out, falls can be very difficult to distinguish as a dis-tinct clinical entity and overlap syndromes such as syncope have been reported. Therefore, caution is warranted when interpreting the data. A large majority of the studies only used self- reported falls that had occur-red in the past, and only a small minority studied falls in a prospective manner. As such, it is difficult to attribute causation to any one risk factor in isolation. Further prospective studies are therefore needed. The exact effect of cardiovascular drugs on falls risk remains a confounder in most studies. As this review specifically excluded articles where there were therapeutic interventions made, the contribution of individual medicati-ons to falls risk is beyond the scope of this article.
2928 CHAPTER 1falling: should one blame the heart?
Gra
afm
ans
1996
57
354
70+
C
ohor
t, co
mm
unity
, pr
ospe
ctiv
e
Any
and
re
curr
ent f
alls
du
ring
28
wee
k FU
Supi
ne a
nd s
tand
ing
at 1
min
ute,
20/
10
O
H &
falls
: OR
1.4
(0
.8-4
.8) (
n/s)
. OH
&
rec
urre
nt fa
lls:
OR
2.0
(1.0
-4.2
)
OH
was
as
soci
ated
with
fu
ture
rec
urre
nt
falls
but
not
with
an
y fa
lls
+
+
8
Hei
ttera
chi
2002
59
70
77 [
±6]
C
ohor
t, co
mm
unity
, pr
ospe
ctiv
e
Any
fall
duri
ng 1
2 m
onth
FU
HU
T at
60
degr
ees,
co
ntin
uous
, 20
SBP
OH
at 3
min
.: 22
% o
f fa
llers
, 6%
of n
on-
falle
rs.
OH
at 3
min
. &
falls
: RR
1.7
[±
1.1-
2.6]
.
OH
at 3
min
. afte
r H
UT
was
as
soci
ated
with
fu
ture
falls
.
§ +
+
7
Kar
io
2001
66
266
76 [
±5]
C
ohor
t, co
mm
unity
, cr
oss-
sect
iona
l
Any
fall
duri
ng 1
2 m
onth
FU
Supi
ne, i
mm
edia
tely
af
ter
stan
ding
and
at
2 m
in.
Sphy
ogm
oman
omet
er, 2
0/10
OH
not
diff
eren
t be
twee
n fa
llers
and
no
n-fa
llers
O
H w
as n
ot
asso
ciat
ed w
ith
futu
re fa
lls
∞
- 9
Law
lor
2003
73
405
0 71
(9
5% C
I 70
-71
)
Coh
ort,
com
mun
ity,
cros
s-se
ctio
nal
Any
and
re
curr
ent f
alls
in
the
past
12
mon
ths
Mea
n of
two
stan
ding
m
easu
rem
ents
with
sp
hyg,
20/
10
17.6
% o
f fal
lers
and
17
.1%
of n
on-f
alle
rs
O
H w
as n
ot
asso
ciat
ed w
ith
falls
in th
e pa
st
year
∞
- 6
Liu
1995
79
100
83 [
±6]
, ra
nge
62-9
6
Coh
ort,
Com
mun
ity,
Pros
pect
ive
Any
fall
duri
ng 1
2 m
onth
s FU
Imm
edia
tely
on
stan
ding
and
afte
r 5
min
., sp
hyg,
20/
10
Prev
alen
ce O
H 3
-15
%, n
o di
ffere
nce
betw
een
falle
rs a
nd
non-
falle
rs
O
H is
not
as
soci
ated
with
fu
ture
falls
∞
- 6
Luuk
inen
19
96 80
10
16
76 [
±5]
C
ohor
t, co
mm
unity
, pr
ospe
ctiv
e
Rec
urre
nt
falls
dur
ing
12 m
onth
FU
Sitti
ng a
nd s
tand
ing
at 1
min
ute,
sph
yg,
20 S
BP
35%
in fa
llers
, 29%
in
non
-fal
lers
R
R 1
.3 (0
.8-1
.9)
OH
was
not
as
soci
ated
with
fu
ture
falls
∞
- 8
Mad
er
1987
81
300
70
(ran
ge
56-9
3)
Coh
ort
outp
atie
nt
com
mun
ity
clin
ic, c
ross
-se
ctio
nal
Any
fall
in
past
12
mon
ths
Supi
ne a
nd s
tand
ing
at 1
min
ute
sphy
g,
20 S
BP.
7% o
f fal
lers
, 12%
of
non-
falle
rs
n/s
OH
was
not
as
soci
ated
with
fa
lls in
the
past
ye
ar
∞
- 3
Mau
rer
2004
83
111
88 [
±7]
C
ohor
t, lo
ng-
term
car
e,
pros
pect
ive
Any
fall
duri
ng a
m
edia
n FU
of
270
days
Sitti
ng a
nd s
tand
ing
for
5 m
in.,
cont
inuo
us, 2
0/10
O
H a
t 1-m
inut
e &
fa
lls H
R 0
.98
(0.5
–2.
0), O
H a
t 3 m
in.
& fa
lls H
R 1
.3 (0
.7–
2.5)
OH
was
not
as
soci
ated
with
fu
ture
falls
-
6
Ooi
20
00 89
84
4 60
+
Coh
ort,
long
-te
rm c
are,
pr
ospe
ctiv
e
Any
fall
duri
ng 1
8 m
onth
s
Supi
ne a
nd s
tand
ing
at 1
& 3
min
., 8
mea
sure
men
ts
sphy
g. 2
0/10
50%
in fa
llers
and
no
n-fa
llers
. O
H &
rec
urre
nt fa
lls
in p
revi
ous
falle
rs
aRR
2.1
(1.4
- 3
.1).
Ris
k of
sub
sequ
ent
falls
was
gre
ates
t in
prev
ious
falle
rs w
ith
OH
at t
wo
or m
ore
OH
was
as
soci
ated
with
re
curr
ent f
alls
in
thos
e w
ho h
ad
prev
ious
falls
∞
++
5
TABLE 1 (CONTINUED)
Tabl
e 1.
Ove
rvie
w o
f st
udie
s pu
blis
hed
on c
ardi
ovas
cula
r ab
norm
alit
ies
and
falls
, inc
lude
d in
sys
tem
atic
rev
iew
A
utho
r Y
ear
Des
ign
Sett
ing
Dat
a ga
ther
ing
Out
com
e of
fa
lls
Mea
sure
men
t of
fal
ls
Rep
orti
ng
inte
rval
N
A
ge, y
ears
%
fe
mal
e Ex
posu
re(s
)
Ala
mgi
r 30
20
15
Coh
ort
Com
mun
ity
(hom
e)
Cro
ss-s
ectio
nal
Any
fall
Ret
rosp
ectiv
e Pa
st 3
m
onth
s 59
96
65+
no
t gi
ven
CV
D
Allc
ock
31
2000
O
bser
vatio
nal
seri
es
Falls
&
sync
ope
clin
ic
Ret
rosp
ectiv
e U
nexp
lain
ed
falls
and
sy
ncop
e
Ref
erre
d fo
r un
expl
aine
d fa
lls a
nd
sync
ope
n/a
120
78 (r
ange
66-
94)
70%
C
SH, O
H,
VV
S, C
A
Anp
alah
an
32
2011
C
ase-
cont
rol
Acu
te h
ospi
tal
Ret
rosp
ectiv
e U
nexp
lain
ed
and
acci
dent
al
falls
in E
R o
r ad
mitt
ed fo
r fa
lls
n/a
21 /
17
80 [
±6]
/ 77
[±5]
55
%
CSH
, VV
S,
CA
D
Arm
stro
ng
33
2003
O
bser
vatio
nal
seri
es
Falls
&
sync
ope
clin
ic
Ret
rosp
ectiv
e U
nexp
lain
ed
falls
and
sy
ncop
e
Ret
rosp
ectiv
e n/
a 15
73
, ran
ge 6
1-89
87
%
CA
Aro
now
34
1997
C
ohor
t Lo
ng-t
erm
car
e Pr
ospe
ctiv
e A
ny fa
ll In
cide
nt
repo
rts
29 [
±10
] m
onth
s 49
9 80
[±
9]
Not
gi
ven
PPH
Ass
anta
chai
35
20
03
Coh
ort
Com
mun
ity
(hom
e)
Cro
ss-s
ectio
nal
Any
fall
Ret
rosp
ectiv
e Pa
st 6
m
onth
s 10
43
Men
69
[± 6
],
wom
en 6
8 [±
7]
64%
H
TN
Ben
chim
ol
36
2007
C
ase-
cont
rol
Falls
&
sync
ope
clin
ic
Ret
rosp
ectiv
e U
nexp
lain
ed
falls
and
sy
ncop
e
Ref
erre
d fo
r un
expl
aine
d fa
lls a
nd
sync
ope
n/a
259
/ 55
50 [
±24
], 5
7 [±
21]
66%
/ 58
%
CSH
, VV
S
Ber
g 37
19
97
Coh
ort
Com
mun
ity
(hom
e)
Pros
pect
ive
Rec
urre
nt fa
lls
Pros
pect
ive
2-w
eekl
y fo
r 12
mon
ths
96
72 [
±7]
, ra
nge
60-8
8 60
%
Low
BP
Ber
glan
d 38
20
03
Coh
ort
Com
mun
ity
(hom
e)
Pros
pect
ive
Any
fall
Pros
pect
ive
3-m
onth
ly fo
r 12
mon
ths
307
81 (r
ange
75-
93)
100%
H
TN
Bod
daer
t 39
2004
O
bser
vatio
nal
seri
es
Acu
te h
ospi
tal
Cro
ss-s
ectio
nal
Any
fall
In E
R o
r ad
mitt
ed fo
r fa
lls
n/a
57
84 [
±7]
81
%
OH
Bra
ssin
gton
40
20
00
Coh
ort
Com
mun
ity
(hom
e)
Cro
ss-s
ectio
nal
Any
fall
Ret
rosp
ectiv
e n/
a 15
26
64-9
9 64
%
HTN
, CV
D
Bum
in 41
20
02
Coh
ort
Long
-ter
m c
are
Cro
ss-s
ectio
nal
Any
fall
Ret
rosp
ectiv
e Ev
er
33
falle
rs 7
3 [±
2], n
on-
falle
rs 6
8 [±
2]
Not
gi
ven
OH
Cam
pbel
l 42
1981
C
ohor
t C
omm
unity
(h
ome
and
resi
dent
ial
faci
lity)
, Acu
te
hosp
ital
Cro
ss-s
ectio
nal
Any
fall
R
etro
spec
tive
Past
12
mon
ths
559
65+
N
ot
give
n O
H
TABLE 1. OVERVIEW OF STUDIES PUBLISHED ON CARDIOVASCULAR ABNORMALITIES AND FALLS, INCLUDED IN A SYSTEMATIC REVIEW
3130 CHAPTER 1falling: should one blame the heart?
Lee
75
2006
C
ohor
t C
omm
unity
(h
ome)
C
ross
-sec
tiona
l A
ny fa
ll an
d re
curr
ent f
alls
R
etro
spec
tive
Past
12
mon
ths
4000
73
[±
5]
50%
C
VD
Lee
76
2009
C
ohor
t C
omm
unity
(h
ome)
C
ross
-sec
tiona
l R
ecur
rent
falls
R
etro
spec
tive
Past
12
mon
ths
11,1
13
65-7
5 ye
ars
55%
, 76
plus
45
%
58%
C
AD
Liao
77
2012
C
ohor
t C
omm
unity
(h
ome)
C
ross
-sec
tiona
l A
ny fa
ll R
etro
spec
tive
Past
12
mon
ths
1165
75
[±
7)
54%
H
TN
Lips
itz 78
19
91
Cas
e-co
ntro
l Lo
ng-t
erm
car
e C
ross
-sec
tiona
l R
ecur
rent
falls
R
etro
spec
tive
Past
6
mon
ths
70 /
56
87 [
±6]
/ 87
[±
5]
73%
/ 48
%
OH
, HTN
Liu
79
1995
C
ohor
t C
omm
unity
(r
esid
entia
l fa
cilit
y)
Pros
pect
ive
Any
fall
Pros
pect
ive
Wee
kly
for
12 m
onth
s 10
0 83
[±
6],
rang
e 62
-96
83%
O
H
Luuk
inen
80
1996
C
ohor
t C
omm
unity
(h
ome)
Pr
ospe
ctiv
e R
ecur
rent
falls
Pr
ospe
ctiv
e 3-
mon
tly
duri
ng 1
2 m
onth
s
1016
/ 65
0 76
[±
5]
63%
O
H
Mad
er 81
19
87
Coh
ort
Out
patie
nt
clin
ic,
com
mun
ity
clin
ic
Cro
ss-s
ectio
nal
Any
fall
Ret
rosp
ectiv
e Pa
st 1
2 m
onth
s 30
0 70
(ran
ge 5
6-
93)
77%
O
H
Mar
echa
ux
82
2009
O
bser
vatio
nal
seri
es
Emer
genc
y de
part
men
t Pr
ospe
ctiv
e A
ny fa
ll in
ER
or
adm
itted
for
falls
imm
edia
te
60
81+
/- 8
yea
rs
58,4
H
TN
Mau
rer
83
2004
C
ohor
t Lo
ng-t
erm
car
e Pr
ospe
ctiv
e A
ny fa
ll In
cide
nt
repo
rts
Wee
kly
duri
ng 2
70-
day
FU
(ran
ge 8
–657
)
111
88 [
±7]
82
%
OH
Mau
rer
84
2005
C
ohor
t Lo
ng-t
erm
car
e Pr
ospe
ctiv
e A
ny fa
ll In
cide
nt
repo
rts
12 m
onth
s 13
9 88
+/-
7 85
%
HTN
Mid
ttun
85
2011
O
bser
vatio
nal
seri
es
Falls
&
sync
ope
clin
ic
Ret
rosp
ectiv
e U
nexp
lain
ed
falls
R
etro
spec
tive
not g
iven
20
7 83
yea
rs (5
8–
95)
70%
C
A
Milt
on 86
20
09
Obs
erva
tiona
l se
ries
Falls
&
sync
ope
clin
ic
Cro
ss-s
ectio
nal
Une
xpla
ined
fa
lls
Ret
rosp
ectiv
e no
t giv
en
1464
78
[±
10]
72%
C
SH, O
H
Mitc
hell
87
2013
C
ohor
t C
omm
unity
(h
ome)
C
ross
-sec
tiona
l A
ny fa
ll R
etro
spec
tive
12 m
onth
s 56
81
65+
55
%
CA
D, H
TN
Mur
phy
88
1986
C
ohor
t Lo
ng-t
erm
car
e Pr
ospe
ctiv
e A
ny fa
ll In
cide
nt
repo
rts
33 m
onth
s 10
0 80
, ran
ge 6
3-
97 /
83,
rang
e 61
-97
75%
C
SH
Ooi
89
2000
C
ohor
t Lo
ng-t
erm
car
e Pr
ospe
ctiv
e A
ny fa
ll an
d re
curr
ent f
alls
In
cide
nt
repo
rts
Inci
dent
re
port
s du
ring
18
844
60+
80
%
OH
TABLE 1 (CONTINUED)
h 58
(h
ome)
H
F H
eitte
rach
i 59
20
02
Coh
ort
Com
mun
ity
(hom
e)
Pros
pect
ive
Any
fall
Pros
pect
ive
Mon
thly
for
12 m
onth
s 70
77
[±
6]
80%
O
H
Her
ndon
60
1997
C
ase-
cont
rol
Com
mun
ity
(hom
e)
Cro
ss-s
ectio
nal
Inju
riou
s fa
lls
in E
R o
r ad
mitt
ed fo
r fa
lls
Past
7 d
ays
467
/ 69
1 65
+
Not
gi
ven
H
TN, C
AD
Hun
g 61
20
13
Obs
erva
tiona
l se
ries
Acu
te h
ospi
tal
Cro
ss-s
ectio
nal
Any
fall
Ret
rosp
ectiv
e Pa
st 3
yea
rs
401
82 [
±0.
2]
24%
C
A, H
TN
Jans
en 62
20
15
Coh
ort
Com
mun
ity
(hom
e)
Cro
ss-s
ectio
nal
Any
fall
and
recu
rren
t fal
ls
Ret
rosp
ectiv
e Pa
st 1
2 m
onth
s 81
73
64 [
10],
ra
nge
51-1
05
54%
H
F, H
TN,
CA
D
Jans
en 63
20
15
Coh
ort
Com
mun
ity
(hom
e)
Cro
ss-s
ectio
nal
Any
fall
Ret
rosp
ectiv
e Pa
st 1
2 m
onth
s 48
86
62 [
8]
54%
C
A
Jitap
unku
l 64
19
98
Coh
ort
Com
mun
ity
(hom
e)
Cro
ss-s
ectio
nal
Any
fall
Ret
rosp
ectiv
e Pa
st 6
m
onth
s 44
80
69 [
±8)
60
%
HTN
Kao
65
2012
C
ohor
t C
omm
unity
(h
ome)
C
ross
-sec
tiona
l R
ecur
rent
and
in
juri
ous
falls
R
etro
spec
tive
Past
12
mon
ths
360
76 (r
ange
64
-91
) 61
%
HTN
, CV
D
Kar
io 66
20
01
Coh
ort
Com
mun
ity
(hom
e)
Pros
pect
ive
Any
fall
Pros
pect
ive
and
retr
ospe
ctiv
e
Mon
thly
for
12 m
onth
s 26
6 76
[±
5]
54%
H
TN, L
ow
BP,
OH
Kel
ly 67
20
03
Cas
e-co
ntro
l C
omm
unity
(h
ome)
R
etro
spec
tive
Inju
riou
s fa
lls
reco
rdin
g of
fa
ll in
med
ical
hi
stor
y
1 ye
ar
2278
/ 91
12
78.5
(7.7
) /
74.5
(6.7
) 69
%,
57%
H
TN, C
VD
Ken
ny 68
19
91
Obs
erva
tiona
l se
ries
Falls
&
sync
ope
clin
ic
Ret
rosp
ectiv
e U
nexp
lain
ed
falls
and
sy
ncop
e
Ref
erre
d fo
r fa
lls
not g
iven
13
0 77
(67-
89)
55%
C
SH
Kle
in 69
20
13
Coh
ort
Com
mun
ity
(hom
e)
Cro
ss-s
ectio
nal
Any
fall
Ret
rosp
ectiv
e Pa
st 3
m
onth
s 35
44
70 (6
0-97
) 56
%
HTN
, Low
B
P K
umar
70
2003
C
ase-
cont
rol
Falls
&
sync
ope
clin
ic
Ret
rosp
ectiv
e U
nexp
lain
ed
falls
R
efer
red
for
falls
no
t giv
en
265
/ 44
79
.5 (6
0–9
2)
/ 71.
3 (6
3–8
6 76
%,
36%
C
SH
de C
astr
o La
cerd
a 71
20
08
Obs
erva
tiona
l se
ries
Falls
&
sync
ope
clin
ic
Pros
pect
ive
Une
xpla
ined
fa
lls
Ref
erre
d fo
r fa
lls
Past
12
mon
ths
502
65 [
±10
] 49
%
CSH
Lagr
o 72
20
13
Obs
erva
tiona
l se
ries
Falls
&
sync
ope
clin
ic
Cro
ss-s
ectio
nal
Any
fall
Ref
erre
d fo
r fa
lls
not g
iven
17
5 (w
ith
falls
)
75+
N
ot
give
n
OH
, PPH
, C
SH
Law
lor
73
2003
C
ohor
t C
omm
unity
(h
ome)
C
ross
-sec
tiona
l A
ny fa
ll R
etro
spec
tive
Past
12
mon
ths
4050
71
10
0%
OH
, CA
D,
HTN
, Low
B
P Le
Cou
teur
74
20
03
Obs
erva
tiona
l se
ries
Com
mun
ity
(res
iden
tial
faci
lity)
Cro
ss-s
ectio
nal
Any
fall
Inci
dent
re
port
s Pa
st 1
2 m
onth
s 17
9 83
[±
7]
80%
PP
H
TABLE 1 (CONTINUED)
3332 CHAPTER 1falling: should one blame the heart?
Scho
on 10
4 20
13
Cas
e-co
ntro
l Fa
lls &
sy
ncop
e cl
inic
C
ross
-sec
tiona
l A
ny fa
lls a
nd
sync
ope
Ref
erre
d fo
r fa
lls
n/a
105
/ 25
79 [
±7]
/ 74
[±
4]
67%
, 20
%
HTI
H
Sibl
ey 10
5 20
14
Coh
ort
Com
mun
ity
(hom
e)
Cro
ss-s
ectio
nal
Any
fall
Ret
rosp
ectiv
e 12
mon
ths
16.3
57
65+
55
%
HTN
, CA
D
Smeb
ye 10
6 20
14
Obs
erva
tiona
l se
ries
Falls
&
sync
ope
clin
ic
Cro
ss-s
ectio
nal
Any
fall
Ref
erre
d fo
r fa
lls
n/a
111
82 [
±7]
82
%
OH
, CV
D,
CSH
, CA
Sten
hage
n 10
7 20
13
Coh
ort
Com
mun
ity
(hom
e)
Pros
pect
ive
Any
fall
Ret
rosp
ectiv
e Pa
st 6
m
onth
s, a
t 3
and
6 ye
ars
1763
60
-93
54%
H
F, C
AD
Tan
108
2008
O
bser
vatio
nal
seri
es
Falls
&
sync
ope
clin
ic
Ret
rosp
ectiv
e U
nexp
lain
ed
falls
and
sy
ncop
e
Ret
rosp
ectiv
e n/
a 30
2 71
[±
11]
(ran
ge 3
8–
98)
Not
gi
ven
OH
, VV
S
Tan
109
2009
O
bser
vatio
nal
seri
es
Falls
&
sync
ope
clin
ic
Ret
rosp
ectiv
e U
nexp
lain
ed
falls
and
sy
ncop
e
Ret
rosp
ectiv
e n/
a 30
2 71
[11
],
rang
e 38
–98
56%
C
SH
Tine
tti 11
0 19
86
Coh
ort
Long
-ter
m c
are
Pros
pect
ive
Rec
urre
nt fa
lls
Inci
dent
re
port
s 3
mon
ths
79
81 [
±7]
, 78
[±7]
78
%,
62%
O
H
van
der
Vel
de 11
1 20
07
Coh
ort
Out
patie
nt
clin
ic
Pros
pect
ive
Any
fall
Pros
pect
ive
Mon
thly
du
ring
3
mon
th F
U
215
77.4
[±
6.0
] 65
%
HV
abn
van
der
Vel
de 11
2 20
07
Coh
ort
Out
patie
nt
clin
ic
Cro
ss-s
ectio
nal
Any
fall
Ret
rosp
ectiv
e 12
mon
ths
217
Falle
rs 7
9 [±
6], n
on
falle
rs 7
5 [±
6]
66%
O
H
van
Nie
uwen
huiz
en 11
3
2010
O
bser
vatio
nal
seri
es
Emer
genc
y de
part
men
t C
ross
-sec
tiona
l A
ny fa
ll an
d R
ecur
rent
falls
In
ER
or
adm
itted
for
falls
n/a
639
79 [
±8]
73
%
CA
D, H
TN
Vu
114
2011
O
bser
vatio
nal
seri
es
Acu
te h
ospi
tal
Ret
rosp
ectiv
e In
juri
ous
falls
In
ER
or
adm
itted
for
falls
n/a
44.9
42
med
ian
82
(IQR
76-
87)
70%
H
F, C
AD
Won
g 11
5 20
14
Coh
ort
Com
mun
ity
(hom
e)
Pros
pect
ive
Any
fall
Pros
pect
ive
Mon
thly
for
12 m
onth
s 48
1 80
[±
4]
51%
A
rter
ial
stiff
ness
, O
H, H
TN,
CA
D
Pros
pect
ive
falls
rep
ortin
g: fa
ll di
arie
s or
cal
enda
rs a
nd/o
r fr
eque
nt te
leph
one
inte
rvie
ws
CA
, car
diac
arr
hyth
mia
. CA
D, c
oron
ary
arte
ry d
isea
se (a
ngin
a, Is
chem
ic h
eart
dis
ease
, myo
card
ial i
nfar
ctio
n). C
VD
, gen
eral
car
diov
ascu
lar
dise
ase
(uns
peci
fied)
. CSH
, ca
rotid
sin
us h
yper
sens
itivi
ty/s
yndr
ome.
HF,
hea
rt fa
ilure
. HTN
, hyp
erte
nsio
n. H
TIH
, hea
d tu
rnin
g in
duce
d hy
pote
nsio
n. H
V, h
eart
val
ve a
bnor
mal
ity. O
H, o
rtho
stat
ic
hypo
tens
ion.
Low
BP,
low
blo
od p
ress
ure.
VV
S, v
asov
agal
syn
cope
. N
/A: N
ot a
pplic
able
. 95%
CI:
95%
con
fiden
ce in
terv
al.
SD (±
): st
anda
rd d
evia
tion.
IQR
: int
erqu
artil
e ra
nge.
TABLE 1 (CONTINUED)
mon
ths
Palin
g 90
20
11
Obs
erva
tiona
l se
ries
Falls
&
sync
ope
clin
ic
Cro
ss-s
ectio
nal
Une
xpla
ined
fa
lls
Ref
erre
d fo
r un
expl
aine
d fa
lls
n/a
111
(with
fa
lls)
82, r
ange
61-
99
59%
C
SH, V
VS,
O
H
Parr
y 91
20
05
Obs
erva
tiona
l se
ries
Falls
&
sync
ope
clin
ic
Cro
ss-s
ectio
nal
Any
falls
and
sy
ncop
e R
efer
red
for
falls
nd
sync
ope
n/a
34 (f
alls
) / 3
4 (s
ynco
pe)
77 [
9] /
75
[9]
79%
, 47
%
CSH
Parr
y 92
20
05
Obs
erva
tiona
l se
ries
Falls
&
sync
ope
clin
ic
Cro
ss-s
ectio
nal
Dro
p at
tack
s (u
nexp
lain
ed
falls
)
Ret
rosp
ectiv
e Pa
st 6
m
onth
s 93
77
[±
9],
rang
e 55
-92
75%
C
SH, O
H,
VV
S, C
A
Pasm
a 93
20
14
Coh
ort
Out
patie
nt
clin
ic
Cro
ss-s
ectio
nal
Any
fall
Ret
rosp
ectiv
e Pa
st 1
2 m
onth
s 19
7 82
60
%
OH
Phili
ps 94
19
99
Obs
erva
tiona
l se
ries
Emer
genc
y de
part
men
t C
ross
-sec
tiona
l A
ny fa
lls a
nd
sync
ope
in E
R o
r ad
mitt
ed fo
r fa
lls
n/a
142
83, r
ange
76-
99
63%
C
AD
Prud
ham
95
1981
C
ohor
t C
omm
unity
(h
ome)
C
ross
-sec
tiona
l A
ny fa
ll R
etro
spec
tive
Past
12
mon
ths
2357
65
+
59%
C
VD
, HTN
Puis
ieux
96
2000
C
ase-
cont
rol
Acu
te h
ospi
tal
Cro
ss-s
ectio
nal
Any
fall
in E
R o
r ad
mitt
ed fo
r fa
lls
n/a
45 /
36
80.9
[8.
5] /
78.5
[7.
2]
73%
, 68
%
PPH
Raf
anel
li 97
20
14
Obs
erva
tiona
l se
ries
Falls
&
sync
ope
clin
ic
Ret
rosp
ectiv
e U
nexp
lain
ed
falls
R
efer
red
for
falls
n/
a 29
8 75
[±
11]
not
give
n C
SH, O
H,
VV
S
Raf
iq 98
20
14
Coh
ort
Com
mun
ity
(hom
e)
Cro
ss-s
ectio
nal
Any
fall
GP
visi
t for
fall
30 m
onth
s ba
selin
e, 3
0 m
onth
s FU
135.
433
75 [
±8]
, ra
nge
65-1
04
56%
C
AD
, HF
Ric
hard
son
99
1997
O
bser
vatio
nal
seri
es
Emer
genc
y de
part
men
t C
ross
-sec
tiona
l U
nexp
lain
ed
falls
and
re
curr
ent f
alls
in E
R o
r ad
mitt
ed fo
r fa
lls
in E
R fo
r fa
ll
279
50+
no
t gi
ven
CSH
Rom
ero-
Ort
uno
100
2011
C
ohor
t C
omm
unity
(h
ome)
C
ross
-sec
tiona
l A
ny fa
ll R
etro
spec
tive
Past
6
mon
ths
598
72
72%
O
H
Ros
ado
101
1989
C
ase-
cont
rol
Long
-ter
m
care
, C
omm
unity
(r
esid
entia
l fa
cilit
y)
Cro
ss-s
ectio
nal
Any
fall
Inci
dent
re
port
s Pa
st 7
day
s 51
/ 27
86
no
t gi
ven
CA
Rut
an 10
2 19
92
Coh
ort
Com
mun
ity
(hom
e)
Cro
ss-s
ectio
nal
Any
fall
Ret
rosp
ectiv
e 12
mon
ths
4931
O
H+
: 73.
6,
OH
-: 7
2.6
56%
O
H
Sand
ers
103
2012
C
ase-
cont
rol
Emer
genc
y de
part
men
t R
etro
spec
tive
Une
xpla
ined
fa
lls a
nd
acci
dent
al fa
lls
Ret
rosp
ectiv
e n/
a 21
1 /
231
82 [
±9]
/ 79
[±
7]
62%
, 62
%
CA
TABLE 1 (CONTINUED)
3534 CHAPTER 1falling: should one blame the heart?
Gra
afm
ans
1996
57
354
70+
C
ohor
t, co
mm
unity
, pr
ospe
ctiv
e
Any
and
re
curr
ent f
alls
du
ring
28
wee
k FU
Supi
ne a
nd s
tand
ing
at 1
min
ute,
20/
10
O
H &
falls
: OR
1.4
(0
.8-4
.8) (
n/s)
. OH
&
rec
urre
nt fa
lls:
OR
2.0
(1.0
-4.2
)
OH
was
as
soci
ated
with
fu
ture
rec
urre
nt
falls
but
not
with
an
y fa
lls
+
+
8
Hei
ttera
chi
2002
59
70
77 [
±6]
C
ohor
t, co
mm
unity
, pr
ospe
ctiv
e
Any
fall
duri
ng 1
2 m
onth
FU
HU
T at
60
degr
ees,
co
ntin
uous
, 20
SBP
OH
at 3
min
.: 22
% o
f fa
llers
, 6%
of n
on-
falle
rs.
OH
at 3
min
. &
falls
: RR
1.7
[±
1.1-
2.6]
.
OH
at 3
min
. afte
r H
UT
was
as
soci
ated
with
fu
ture
falls
.
§ +
+
7
Kar
io
2001
66
266
76 [
±5]
C
ohor
t, co
mm
unity
, cr
oss-
sect
iona
l
Any
fall
duri
ng 1
2 m
onth
FU
Supi
ne, i
mm
edia
tely
af
ter
stan
ding
and
at
2 m
in.
Sphy
ogm
oman
omet
er, 2
0/10
OH
not
diff
eren
t be
twee
n fa
llers
and
no
n-fa
llers
O
H w
as n
ot
asso
ciat
ed w
ith
futu
re fa
lls
∞
- 9
Law
lor
2003
73
405
0 71
(9
5% C
I 70
-71
)
Coh
ort,
com
mun
ity,
cros
s-se
ctio
nal
Any
and
re
curr
ent f
alls
in
the
past
12
mon
ths
Mea
n of
two
stan
ding
m
easu
rem
ents
with
sp
hyg,
20/
10
17.6
% o
f fal
lers
and
17
.1%
of n
on-f
alle
rs
O
H w
as n
ot
asso
ciat
ed w
ith
falls
in th
e pa
st
year
∞
- 6
Liu
1995
79
100
83 [
±6]
, ra
nge
62-9
6
Coh
ort,
Com
mun
ity,
Pros
pect
ive
Any
fall
duri
ng 1
2 m
onth
s FU
Imm
edia
tely
on
stan
ding
and
afte
r 5
min
., sp
hyg,
20/
10
Prev
alen
ce O
H 3
-15
%, n
o di
ffere
nce
betw
een
falle
rs a
nd
non-
falle
rs
O
H is
not
as
soci
ated
with
fu
ture
falls
∞
- 6
Luuk
inen
19
96 80
10
16
76 [
±5]
C
ohor
t, co
mm
unity
, pr
ospe
ctiv
e
Rec
urre
nt
falls
dur
ing
12 m
onth
FU
Sitti
ng a
nd s
tand
ing
at 1
min
ute,
sph
yg,
20 S
BP
35%
in fa
llers
, 29%
in
non
-fal
lers
R
R 1
.3 (0
.8-1
.9)
OH
was
not
as
soci
ated
with
fu
ture
falls
∞
- 8
Mad
er
1987
81
300
70
(ran
ge
56-9
3)
Coh
ort
outp
atie
nt
com
mun
ity
clin
ic, c
ross
-se
ctio
nal
Any
fall
in
past
12
mon
ths
Supi
ne a
nd s
tand
ing
at 1
min
ute
sphy
g,
20 S
BP.
7% o
f fal
lers
, 12%
of
non-
falle
rs
n/s
OH
was
not
as
soci
ated
with
fa
lls in
the
past
ye
ar
∞
- 3
Mau
rer
2004
83
111
88 [
±7]
C
ohor
t, lo
ng-
term
car
e,
pros
pect
ive
Any
fall
duri
ng a
m
edia
n FU
of
270
days
Sitti
ng a
nd s
tand
ing
for
5 m
in.,
cont
inuo
us, 2
0/10
O
H a
t 1-m
inut
e &
fa
lls H
R 0
.98
(0.5
–2.
0), O
H a
t 3 m
in.
& fa
lls H
R 1
.3 (0
.7–
2.5)
OH
was
not
as
soci
ated
with
fu
ture
falls
-
6
Ooi
20
00 89
84
4 60
+
Coh
ort,
long
-te
rm c
are,
pr
ospe
ctiv
e
Any
fall
duri
ng 1
8 m
onth
s
Supi
ne a
nd s
tand
ing
at 1
& 3
min
., 8
mea
sure
men
ts
sphy
g. 2
0/10
50%
in fa
llers
and
no
n-fa
llers
. O
H &
rec
urre
nt fa
lls
in p
revi
ous
falle
rs
aRR
2.1
(1.4
- 3
.1).
Ris
k of
sub
sequ
ent
falls
was
gre
ates
t in
prev
ious
falle
rs w
ith
OH
at t
wo
or m
ore
OH
was
as
soci
ated
with
re
curr
ent f
alls
in
thos
e w
ho h
ad
prev
ious
falls
∞
++
5
TABLE 2 (CONTINUED)
Tabl
e 2.
Ort
host
atic
hyp
oten
sion
and
falls
Fi
rst
auth
or
N
Age
, Y
ears
Po
pula
tion
, se
ttin
g, d
esig
n Fa
lls
Out
com
e A
sses
smen
t m
etho
d
Mai
n fin
ding
s an
d pr
eval
ence
of O
H
OR
/RR
/HR
C
oncl
usio
n O
H
* N
OS
Coh
orts
Bum
in
2002
41
33
Falle
rs
73 [
±2]
, no
n-fa
llers
68
[±
2]
Coh
ort,
long
-te
rm c
are,
cr
oss-
sect
iona
l
Any
fall,
eve
r Si
tting
and
sta
ndin
g at
3 m
in, 2
0 SB
P 44
% o
f fal
lers
, 18%
of
non
falle
rs
O
H w
as
univ
aria
tely
as
soci
ated
with
fa
lls
+
3
Cam
pbel
l 19
81 42
55
9 65
+
Coh
ort,
com
mun
ity a
nd
acut
e ho
spita
l, cr
oss-
sect
iona
l
Any
fall
in
the
past
12
mon
ths
Supi
ne a
nd s
tand
ing
at 1
and
3 m
in,
sphy
g., 2
0 SB
P
13%
(74/
559)
of t
otal
sa
mpl
e, c
onsi
dere
d at
trib
utab
le c
ause
of a
fa
ll in
3%
.
O
H c
onsi
dere
d an
at
trib
utab
le c
ause
of
a fa
ll in
3%
.
∞
- 4
Cam
pbel
l 19
89 43
76
1 70
+
Coh
ort,
com
mun
ity,
pros
pect
ive
Any
fall
duri
ng 1
2 m
onth
FU
Lyin
g an
d st
andi
ng
at 1
and
3 m
in.
sphy
g, 2
0 SB
P
40%
in fe
mal
e fa
llers
an
d 31
% in
fem
ale
non-
falle
rs, 2
2% in
m
ale
falle
rs a
nd 2
9%
in m
ale
non-
falle
rs.
Post
ural
hy
pote
nsio
n &
falls
R
R 1
.5 (0
.95-
2.3)
in
wom
en
OH
was
not
si
gnifi
cant
ly
asso
ciat
ed w
ith
futu
re fa
lls.
∞
- 8
Cha
n 19
97 44
40
1 69
(r
ange
60
-90)
Coh
ort,
com
mun
ity,
cros
s-se
ctio
nal
Any
fall
in
the
past
12
mon
ths
Stan
ding
at 3
min
., sp
hyg,
20
SBP
7.2%
(n=
5) in
falle
rs
and
10.5
% (n
=35
) in
non-
falle
rs.
OH
& fa
lls
unad
just
ed O
R 0
.7
(0.3
-1.8
)
OH
was
not
as
soci
ated
with
fa
lls.
∞
- 4
Cha
ng
2010
45
136
1 72
[±
5]
Coh
ort,
com
mun
ity,
cros
s-se
ctio
nal
Any
inju
riou
s fa
ll in
the
past
12
mon
ths
Supi
ne a
nd
stan
ding
, im
med
iate
ly,2
0/10
36%
in fa
llers
, 24%
in
non
-fal
lers
. Pr
eval
ence
of O
H in
in
juri
ous
falle
rs
high
er th
an in
non
-in
juri
ous
falle
rs.
OH
& in
juri
ous
falls
vs
non
-inj
urio
us
falls
OR
2.3
(1.1
-5.
12) O
H &
re
mar
kabl
e in
jury
vs
. no
inju
ry: O
R
4.0
(1.6
-10.
0).
OH
and
any
falls
w
ere
not
asso
ciat
ed. O
H
was
ass
ocia
ted
with
inju
riou
s fa
lls
com
pare
d to
non
-in
juri
ous
falls
+
+
6
Dow
nton
19
91 52
203
83 [
±5]
, ra
nge
75-9
7
Coh
ort,
com
mun
ity,
cros
s-se
ctio
nal
Any
fall
in
the
past
12
mon
ths
Sitti
ng a
nd s
tand
ing
at 1
and
2 m
in.,
20
SBP
31%
of s
ubje
cts;
eq
ual b
etw
een
falle
rs
and
non-
falle
rs.
O
H w
as n
ot
asso
ciat
ed w
ith
falls
-
4
Ensr
ud
1992
54
970
4 72
(r
ange
65
-99)
Coh
ort,
com
mun
ity,
cros
s-se
ctio
nal
Any
fall
in
the
past
12
mon
ths
Supi
ne a
nd s
tand
ing
at 1
min
ute,
sph
yg,
20 S
BP
Fa
lls a
nd O
H: O
R
1.0
(0.9
-1.2
) O
H w
as n
ot
asso
ciat
ed w
ith a
hi
stor
y of
falls
∞
- 5
Gan
gava
ti 20
11 56
72
2 78
[±
5]
Coh
ort,
com
mun
ity
(hom
e),
pros
pect
ive
Rec
urre
nt
falls
dur
ing
FU (m
in. 1
83
days
)
Supi
ne a
nd s
tand
ing
at 1
and
3 m
in.,
sphy
g, 2
0/10
Falls
sim
ilar
in th
ose
with
and
with
out O
H.
: 39%
of p
artic
ipan
ts
with
unc
ontr
olle
d H
TN a
nd O
H h
ad
recu
rren
t fal
ls, v
s.
17%
in th
ose
with
out
OH
.
Rec
urre
nt fa
lls &
O
H a
t 1 m
in in
un
cont
rolle
d H
TN:
HR
2.5
(95%
CI
1.3–
5.0)
.
OH
was
as
soci
ated
with
fu
ture
rec
urre
nt
falls
in th
ose
with
un
cont
rolle
d H
TN.
∞
++
8
TABLE 2. ORTHOSTATIC HYPOTENSION AND FALLS
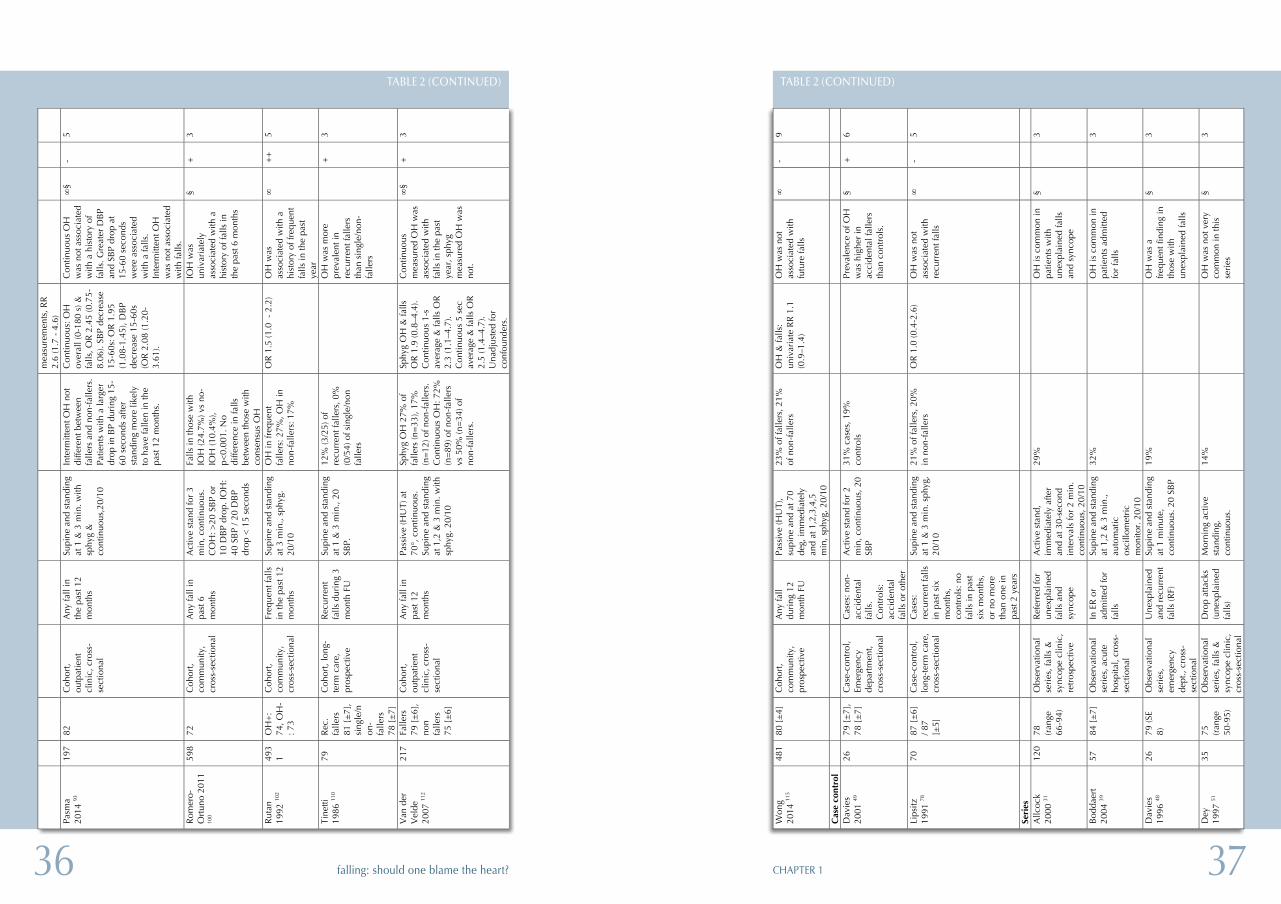
3736 CHAPTER 1falling: should one blame the heart?
Won
g 20
14 11
5 48
1 80
[±
4]
Coh
ort,
com
mun
ity,
pros
pect
ive
Any
fall
duri
ng 1
2 m
onth
FU
Pass
ive
(HU
T),
supi
ne a
nd a
t 70
deg,
imm
edia
tely
an
d at
1,2
,3,4
,5
min
, sph
yg, 2
0/10
23%
of f
alle
rs, 2
1%
of n
on-f
alle
rs
OH
& fa
lls:
univ
aria
te R
R 1
.1
(0.9
–1.4
)
OH
was
not
as
soci
ated
with
fu
ture
falls
∞
- 9
Cas
e co
ntro
l
Dav
ies
2001
49
26
79 [
±7]
, 78
[±
7]
Cas
e-co
ntro
l, Em
erge
ncy
depa
rtm
ent,
cros
s-se
ctio
nal
Cas
es: n
on-
acci
dent
al
falls
. C
ontr
ols:
ac
cide
ntal
fa
lls o
r ot
her
Act
ive
stan
d fo
r 2
min
, con
tinuo
us, 2
0 SB
P
31%
cas
es, 1
9%
cont
rols
Prev
alen
ce o
f OH
w
as h
ighe
r in
ac
cide
ntal
falle
rs
than
con
trol
s.
§ +
6
Lips
itz
1991
78
70
87 [
±6]
/ 8
7 [±
5]
Cas
e-co
ntro
l, lo
ng-t
erm
car
e,
cros
s-se
ctio
nal
Cas
es:
recu
rren
t fal
ls
in p
ast s
ix
mon
ths,
co
ntro
ls: n
o fa
lls in
pas
t si
x m
onth
s,
or n
o m
ore
than
one
in
past
2 y
ears
Supi
ne a
nd s
tand
ing
at 1
& 3
min
. sph
yg,
20/1
0
21%
of f
alle
rs, 2
0%
in n
on-f
alle
rs
OR
1.0
(0.4
-2.6
) O
H w
as n
ot
asso
ciat
ed w
ith
recu
rren
t fal
ls
∞
- 5
Seri
es
A
llcoc
k 20
00 31
12
0 78
(r
ange
66
-94)
Obs
erva
tiona
l se
ries
, fal
ls &
sy
ncop
e cl
inic
, re
tros
pect
ive
Ref
erre
d fo
r un
expl
aine
d fa
lls a
nd
sync
ope
Act
ive
stan
d,
imm
edia
tely
afte
r an
d at
30-
seco
nd
inte
rval
s fo
r 2
min
. co
ntin
uous
, 20/
10
29%
OH
is c
omm
on in
pa
tient
s w
ith
unex
plai
ned
falls
an
d sy
ncop
e
§
3
Bod
daer
t 20
04 39
57
84
[±
7]
Obs
erva
tiona
l se
ries
, acu
te
hosp
ital,
cros
s-se
ctio
nal
In E
R o
r ad
mitt
ed fo
r fa
lls
Supi
ne a
nd s
tand
ing
at 1
,2 &
3 m
in.,
auto
mat
ic
osci
llom
etri
c m
onito
r. 2
0/10
32%
OH
is c
omm
on in
pa
tient
s ad
mitt
ed
for
falls
3
Dav
ies
1996
48
26
79 (S
E 8)
O
bser
vatio
nal
seri
es,
emer
genc
y de
pt.,
cros
s-se
ctio
nal
Une
xpla
ined
an
d re
curr
ent
falls
(RF)
Supi
ne a
nd s
tand
ing
at 1
min
ute,
co
ntin
uous
. 20
SBP
19%
OH
was
a
freq
uent
find
ing
in
thos
e w
ith
unex
plai
ned
falls
§
3
Dey
19
97 51
35
75
(r
ange
50
-95)
Obs
erva
tiona
l se
ries
, fal
ls &
sy
ncop
e cl
inic
, cr
oss-
sect
iona
l
Dro
p at
tack
s (u
nexp
lain
ed
falls
)
Mor
ning
act
ive
stan
ding
, co
ntin
uous
.
14%
OH
was
not
ver
y co
mm
on in
this
se
ries
§
3
TABLE 2 (CONTINUED)
mea
sure
men
ts, R
R
2.6
(1.7
- 4
.6)
Pasm
a 20
14 93
19
7 82
C
ohor
t, ou
tpat
ient
cl
inic
, cro
ss-
sect
iona
l
Any
fall
in
the
past
12
mon
ths
Supi
ne a
nd s
tand
ing
at 1
& 3
min
. with
sp
hyg
&
cont
inuo
us,2
0/10
Inte
rmitt
ent O
H n
ot
diffe
rent
bet
wee
n fa
llers
and
non
-fal
lers
. Pa
tient
s w
ith a
larg
er
drop
in B
P du
ring
15-
60 s
econ
ds a
fter
stan
ding
mor
e lik
ely
to h
ave
falle
n in
the
past
12
mon
ths.
Con
tinuo
us: O
H
over
all (
0-18
0 s)
&
falls
, OR
2.4
5 (0
.75-
8.06
). SB
P de
crea
se
15-6
0s: O
R 1
.95
(1.0
8-1.
45),
DB
P de
crea
se 1
5-60
s (O
R 2
.08
(1.2
0-3.
61).
Con
tinuo
us O
H
was
not
ass
ocia
ted
with
a h
isto
ry o
f fa
lls. G
reat
er D
BP
and
SBP
drop
at
15-6
0 se
cond
s w
ere
asso
ciat
ed
with
a fa
lls.
Inte
rmitt
ent O
H
was
not
ass
ocia
ted
with
falls
.
∞§
- 5
Rom
ero-
Ort
uno
2011
10
0
598
72
Coh
ort,
com
mun
ity,
cros
s-se
ctio
nal
Any
fall
in
past
6
mon
ths
Act
ive
stan
d fo
r 3
min
, con
tinuo
us.
CO
H: >
20 S
BP
or
10 D
BP
drop
. IO
H:
40 S
BP
/ 20
DB
P dr
op <
15
seco
nds
Falls
in th
ose
with
IO
H (2
4.7%
) vs
no-
IOH
(10.
4%),
p<0.
001.
No
diffe
renc
e in
falls
be
twee
n th
ose
with
co
nsen
sus
OH
IO
H w
as
univ
aria
tely
as
soci
ated
with
a
hist
ory
of fa
lls in
th
e pa
st 6
mon
ths
§ +
3
Rut
an
1992
102
493
1 O
H+
: 74
, OH
-: 7
3
Coh
ort,
com
mun
ity,
cros
s-se
ctio
nal
Freq
uent
falls
in
the
past
12
mon
ths
Supi
ne a
nd s
tand
ing
at 3
min
., sp
hyg.
20
/10
OH
in fr
eque
nt
falle
rs: 2
7%, O
H in
no
n-fa
llers
: 17%
OR
1.5
(1.0
- 2
.2)
OH
was
as
soci
ated
with
a
hist
ory
of fr
eque
nt
falls
in th
e pa
st
year
∞
++
5
Tine
tti
1986
110
79
Rec
. fa
llers
81
[±
7],
sing
le/n
on-
falle
rs
78 [
±7]
Coh
ort,
long
-te
rm c
are,
pr
ospe
ctiv
e
Rec
urre
nt
falls
dur
ing
3 m
onth
FU
Supi
ne a
nd s
tand
ing
at 1
& 3
min
., 20
SB
P.
12%
(3/2
5) o
f re
curr
ent f
alle
rs, 0
%
(0/5
4) o
f sin
gle/
non
falle
rs
O
H w
as m
ore
prev
alen
t in
recu
rren
t fal
lers
th
an s
ingl
e/no
n-fa
llers
+
3
Van
der
V
elde
20
07 11
2
217
Falle
rs
79 [
±6]
, no
n fa
llers
75
[±
6]
Coh
ort,
outp
atie
nt
clin
ic, c
ross
-se
ctio
nal
Any
fall
in
past
12
mon
ths
Pass
ive
(HU
T) a
t 70
°, c
ontin
uous
. Su
pine
and
sta
ndin
g at
1,2
& 3
min
. with
sp
hyg.
20/
10
Sphy
g O
H 2
7% o
f fa
llers
(n=
33),
17%
(n
=12
) of n
on-f
alle
rs.
Con
tinuo
us O
H: 7
2%
(n=
89) o
f non
-fal
lers
vs
50%
(n=
34) o
f no
n-fa
llers
.
Sphy
g O
H &
falls
O
R 1
.9 (0
.8–4
.4).
Con
tinuo
us 1
-s
aver
age
& fa
lls O
R
2.3
(1.1
–4.7
). C
ontin
uous
5 s
ec
aver
age
& fa
lls O
R
2.5
(1.4
–4.7
). U
nadj
uste
d fo
r co
nfou
nder
s.
Con
tinuo
us
mea
sure
d O
H w
as
asso
ciat
ed w
ith
falls
in th
e pa
st
year
, sph
yg
mea
sure
d O
H w
as
not.
∞§
+
3
TABLE 2 (CONTINUED)
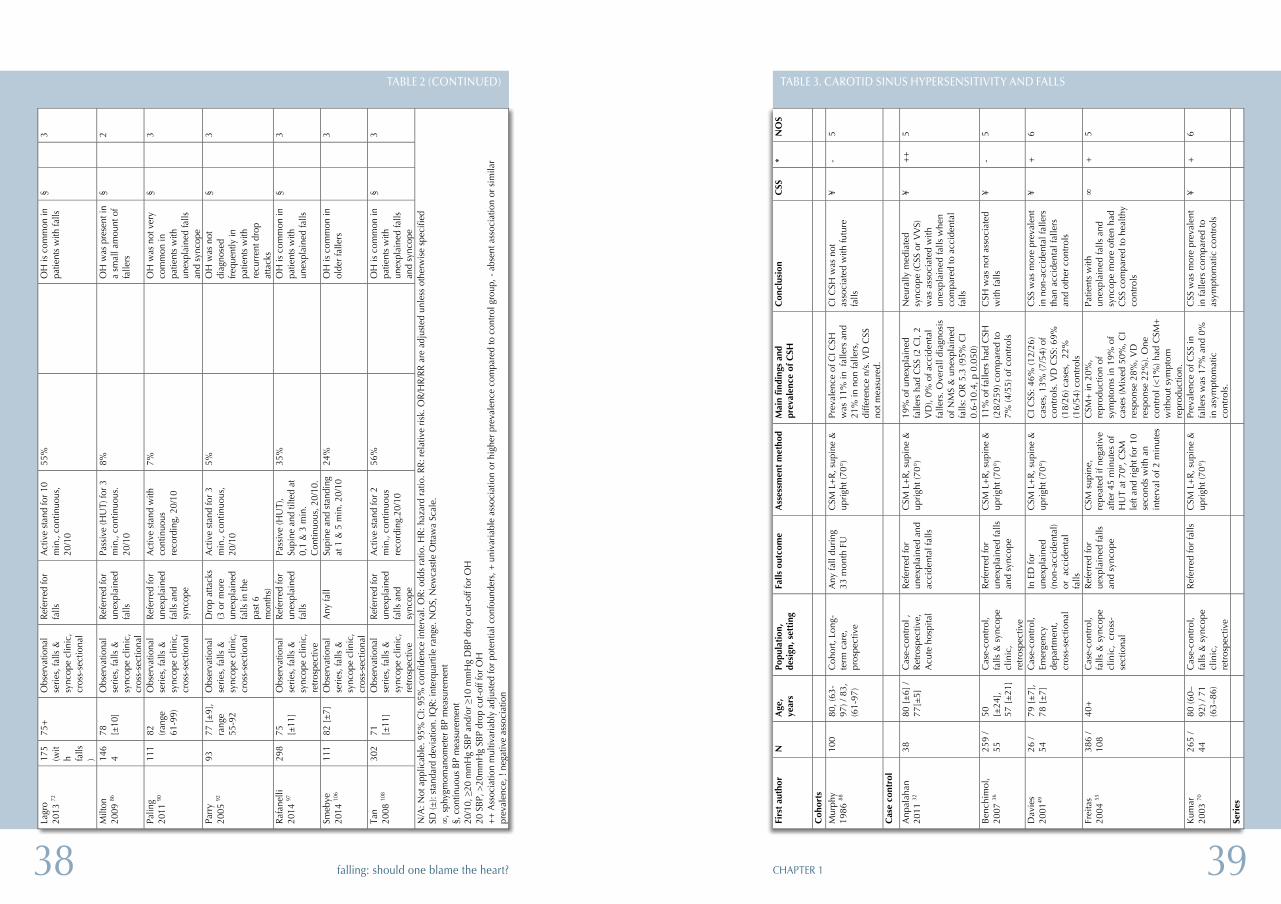
3938 CHAPTER 1falling: should one blame the heart?
Tabl
e 3.
Car
otid
sin
us h
yper
sens
itiv
ity
and
falls
Fi
rst
auth
or
N
Age
, ye
ars
Popu
lati
on,
desi
gn, s
etti
ng
Falls
out
com
e A
sses
smen
t m
etho
d M
ain
find
ings
and
pr
eval
ence
of
CSH
C
oncl
usio
n C
SS
* N
OS
Coh
orts
Mur
phy
1986
88
100
80, (
63-
97) /
83,
(6
1-97
)
Coh
ort,
Long
- te
rm c
are,
pr
ospe
ctiv
e
Any
fall
duri
ng
33 m
onth
FU
C
SM L
+R
, sup
ine
&
upri
ght (
70°)
Pr
eval
ence
of C
I CSH
w
as 1
1% in
fal
lers
and
21
% in
non
falle
rs,
diffe
renc
e n/
s. V
D C
SS
not m
easu
red.
CI C
SH w
as n
ot
asso
ciat
ed w
ith fu
ture
fa
lls
¥ -
5
Cas
e co
ntro
l
Anp
alah
an
2011
32
38
80 [
±6]
/ 77
[±5]
C
ase-
cont
rol ,
R
etro
spec
tive,
A
cute
hos
pita
l
Ref
erre
d fo
r un
expl
aine
d an
d ac
cide
ntal
falls
CSM
L+
R, s
upin
e &
up
righ
t (70
°)
19%
of u
nexp
lain
ed
falle
rs h
ad C
SS (2
CI,
2 V
D),
0% o
f acc
iden
tal
falle
rs. O
vera
ll di
agno
sis
of N
MS
& u
nexp
lain
ed
falls
: OR
5.3
(95%
CI
0.6-
10.4
, p 0
.050
)
Neu
rally
med
iate
d sy
ncop
e (C
SS o
r V
VS)
w
as a
ssoc
iate
d w
ith
unex
plai
ned
falls
whe
n co
mpa
red
to a
ccid
enta
l fa
lls
¥ +
+
5
Ben
chim
ol,
2007
36
259
/ 55
50
[±
24],
57
[±
21]
Cas
e-co
ntro
l, fa
lls &
syn
cope
cl
inic
, re
tros
pect
ive
Ref
erre
d fo
r un
expl
aine
d fa
lls
and
sync
ope
CSM
L+
R, s
upin
e &
up
righ
t (70
°)
11%
of f
alle
rs h
ad C
SH
(28/
259)
com
pare
d to
7%
(4/5
5) o
f con
trol
s
CSH
was
not
ass
ocia
ted
with
falls
¥
- 5
Dav
ies
2001
49
26 /
54
79 [
±7]
, 78
[±
7]
Cas
e-co
ntro
l, Em
erge
ncy
depa
rtm
ent,
cr
oss-
sect
iona
l
In E
D fo
r un
expl
aine
d (n
on-a
ccid
enta
l) or
acc
iden
tal
falls
CSM
L+
R, s
upin
e &
up
righ
t (70
°)
CI C
SS: 4
6% (1
2/26
) ca
ses,
13%
(7/5
4) o
f co
ntro
ls. V
D C
SS: 6
9%
(18/
26) c
ases
, 22
%
(16/
54) c
ontr
ols
CSS
was
mor
e pr
eval
ent
in n
on-a
ccid
enta
l fal
lers
th
an a
ccid
enta
l fal
lers
an
d ot
her
cont
rols
¥ +
6
Frei
tas
2004
55
386
/ 10
8 40
+
Cas
e-co
ntro
l, fa
lls &
syn
cope
cl
inic
, cr
oss-
sect
iona
l
Ref
erre
d fo
r ue
xpla
ined
falls
an
d sy
ncop
e
CSM
sup
ine,
re
peat
ed if
neg
ativ
e af
ter
45 m
inut
es o
f H
UT
at 7
0º, C
SM
left
and
righ
t for
10
seco
nds
with
an
inte
rval
of 2
min
utes
CSM
+ in
20%
, re
prod
uctio
n of
sy
mpt
oms
in 1
9% o
f ca
ses
(Mix
ed 5
0%, C
I re
spon
se 2
8%, V
D
resp
onse
22%
). O
ne
cont
rol (
<1%
) had
CSM
+
with
out s
ympt
om
repr
oduc
tion.
Patie
nts
with
un
expl
aine
d fa
lls a
nd
sync
ope
mor
e of
ten
had
CSS
com
pare
d to
hea
lthy
cont
rols
∞
+
5
Kum
ar
2003
70
265
/ 44
80
(60–
92) /
71
(63–
86)
Cas
e-co
ntro
l, fa
lls &
syn
cope
cl
inic
, re
tros
pect
ive
Ref
erre
d fo
r fa
lls
CSM
L+
R, s
upin
e &
up
righ
t (70
°)
Prev
alen
ce o
f CSS
in
falle
rs w
as 1
7% a
nd 0
%
in a
sym
ptom
atic
co
ntro
ls.
CSS
was
mor
e pr
eval
ent
in fa
llers
com
pare
d to
as
ympt
omat
ic c
ontr
ols
¥ +
6
Seri
es
TABLE 3. CAROTID SINUS HYPERSENSITIVITY AND FALLS
Lagr
o 20
13 72
17
5 (w
ith fa
lls)
75+
Obs
erva
tiona
l se
ries,
falls
&
sync
ope
clin
ic,
cros
s-se
ctio
nal
Refe
rred
for
falls
A
ctiv
e st
and
for 1
0 m
in.,
cont
inuo
us,
20/1
0
55%
OH
is c
omm
on in
pa
tient
s w
ith fa
lls
§
3
Milt
on
2009
86
146
4 78
[±
10]
Obs
erva
tiona
l se
ries,
falls
&
sync
ope
clin
ic,
cros
s-se
ctio
nal
Refe
rred
for
unex
plai
ned
falls
Pass
ive
(HU
T) fo
r 3
min
., co
ntin
uous
. 20
/10
8%
O
H w
as p
rese
nt in
a
smal
l am
ount
of
falle
rs
§
2
Palin
g 20
11 90
11
1 82
(ra
nge
61-9
9)
Obs
erva
tiona
l se
ries,
falls
&
sync
ope
clin
ic,
cros
s-se
ctio
nal
Refe
rred
for
unex
plai
ned
falls
and
sy
ncop
e
Act
ive
stan
d w
ith
cont
inuo
us
reco
rdin
g, 2
0/10
7%
O
H w
as n
ot v
ery
com
mon
in
patie
nts
with
un
expl
aine
d fa
lls
and
sync
ope
§
3
Parr
y 20
05 92
93
77
[±9]
, ra
nge
55-9
2
Obs
erva
tiona
l se
ries,
falls
&
sync
ope
clin
ic,
cros
s-se
ctio
nal
Dro
p at
tack
s (3
or m
ore
unex
plai
ned
falls
in th
e pa
st 6
m
onth
s)
Act
ive
stan
d fo
r 3
min
., co
ntin
uous
, 20
/10
5%
O
H w
as n
ot
diag
nose
d fre
quen
tly in
pa
tient
s w
ith
recu
rren
t dro
p at
tack
s
§
3
Rafa
nelli
20
14 97
29
8 75
[±
11]
Obs
erva
tiona
l se
ries,
falls
&
sync
ope
clin
ic,
retro
spec
tive
Refe
rred
for
unex
plai
ned
falls
Pass
ive
(HU
T),
Supi
ne a
nd ti
lted
at
0,1
& 3
min
. C
ontin
uous
, 20/
10.
35%
OH
is c
omm
on in
pa
tient
s w
ith
unex
plai
ned
falls
§
3
Smeb
ye
2014
106
111
82 [±
7]
Obs
erva
tiona
l se
ries,
falls
&
sync
ope
clin
ic,
cros
s-se
ctio
nal
Any
fall
Supi
ne a
nd s
tand
ing
at 1
& 5
min
. 20/
10
24%
OH
is c
omm
on in
ol
der f
alle
rs
3
Tan
2008
108
302
71
[±11
] O
bser
vatio
nal
serie
s, fa
lls &
sy
ncop
e cl
inic
, re
trosp
ectiv
e
Refe
rred
for
unex
plai
ned
falls
and
sy
ncop
e
Act
ive
stan
d fo
r 2
min
., co
ntin
uous
re
cord
ing.
20/1
0
56%
OH
is c
omm
on in
pa
tient
s w
ith
unex
plai
ned
falls
an
d sy
ncop
e
§
3
N/A
: Not
app
licab
le. 9
5% C
I: 95
% c
onfid
ence
inte
rval
. OR:
odd
s ra
tio. H
R: h
azar
d ra
tio. R
R: re
lativ
e ris
k. O
R/H
R/RR
are
adj
uste
d un
less
oth
erw
ise
spec
ified
SD
(±):
stan
dard
dev
iatio
n. IQ
R: in
terq
uarti
le r
ange
. NO
S, N
ewca
stle
Otta
wa
Scal
e.
∞, s
phyg
mom
anom
eter
BP
mea
sure
men
t §,
con
tinuo
us B
P m
easu
rem
ent
20/1
0, ≥
20 m
mH
g SB
P an
d/or
≥10
mm
Hg
DBP
dro
p cu
t-off
for O
H
20 S
BP, >
20m
mH
g SB
P dr
op c
ut-o
ff fo
r OH
++
Ass
ocia
tion
mul
tivar
iabl
y ad
just
ed fo
r pot
entia
l con
foun
ders
, + u
niva
riabl
e as
soci
atio
n or
hig
her p
reva
lenc
e co
mpa
red
to c
ontro
l gro
up, -
abs
ent a
ssoc
iatio
n or
sim
ilar
prev
alen
ce, !
neg
ativ
e as
soci
atio
n
TABLE 2 (CONTINUED)
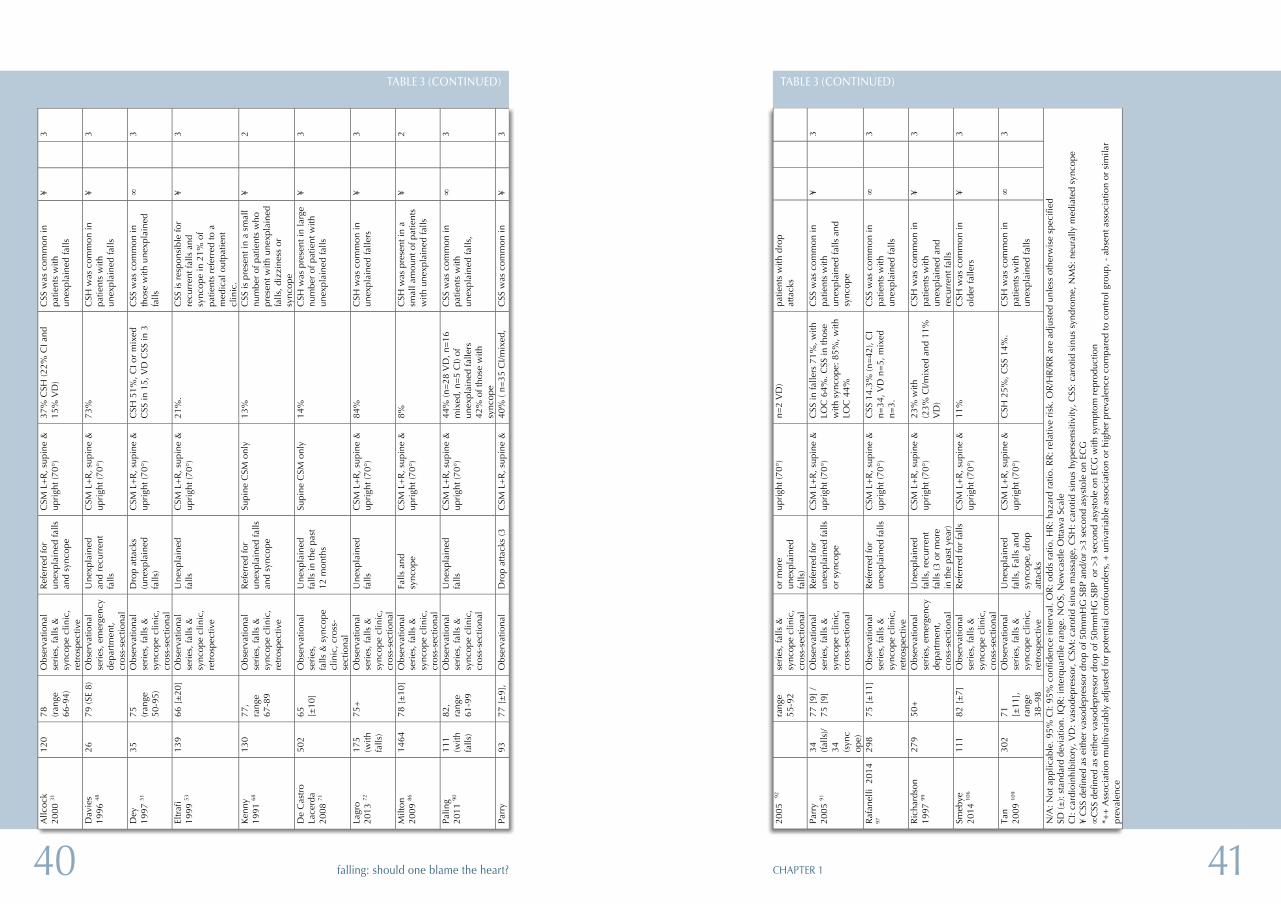
4140 CHAPTER 1falling: should one blame the heart?
2005
92
rang
e 55
-92
seri
es, f
alls
&
sync
ope
clin
ic,
cros
s-se
ctio
nal
or m
ore
unex
plai
ned
falls
)
upri
ght (
70°)
n=
2 V
D)
patie
nts
with
dro
p at
tack
s
Parr
y 20
05 91
34
(fa
lls)/
34
(syn
cop
e)
77 [
9] /
75 [
9]
Obs
erva
tiona
l se
ries
, fal
ls &
sy
ncop
e cl
inic
, cr
oss-
sect
iona
l
Ref
erre
d fo
r un
expl
aine
d fa
lls
or s
ynco
pe
CSM
L+
R, s
upin
e &
up
righ
t (70
°)
CSS
in fa
llers
71%
, with
LO
C 6
4%. C
SS in
thos
e w
ith s
ynco
pe: 8
5%, w
ith
LOC
44%
CSS
was
com
mon
in
patie
nts
with
un
expl
aine
d fa
lls a
nd
sync
ope
¥
3
Raf
anel
li 2
014
97
298
75 [
±11
] O
bser
vatio
nal
seri
es, f
alls
&
sync
ope
clin
ic,
retr
ospe
ctiv
e
Ref
erre
d fo
r un
expl
aine
d fa
lls
CSM
L+
R, s
upin
e &
up
righ
t (70
°)
CSS
14.
3% (n
=42
), C
I n=
34, V
D n
=5,
mix
ed
n=3.
CSS
was
com
mon
in
patie
nts
with
un
expl
aine
d fa
lls
∞
3
Ric
hard
son
1997
99
279
50+
O
bser
vatio
nal
seri
es, e
mer
genc
y de
part
men
t,
cros
s-se
ctio
nal
Une
xpla
ined
fa
lls, r
ecur
rent
fa
lls (3
or
mor
e in
the
past
yea
r)
CSM
L+
R, s
upin
e &
up
righ
t (70
°)
23%
with
(2
3% C
I/mix
ed a
nd 1
1%
VD
)
CSH
was
com
mon
in
patie
nts
with
un
expl
aine
d an
d re
curr
ent f
alls
¥
3
Smeb
ye
2014
106
111
82 [
±7]
O
bser
vatio
nal
seri
es, f
alls
&
sync
ope
clin
ic,
cros
s-se
ctio
nal
Ref
erre
d fo
r fa
lls
CSM
L+
R, s
upin
e &
up
righ
t (70
°)
11%
C
SH w
as c
omm
on in
ol
der
falle
rs
¥
3
Tan
2009
109
302
71
[±11
],
rang
e 38
–98
Obs
erva
tiona
l se
ries
, fal
ls &
sy
ncop
e cl
inic
, re
tros
pect
ive
Une
xpla
ined
fa
lls, F
alls
and
sy
ncop
e, d
rop
atta
cks
CSM
L+
R, s
upin
e &
up
righ
t (70
°)
CSH
25%
, CSS
14%
. C
SH w
as c
omm
on in
pa
tient
s w
ith
unex
plai
ned
falls
∞
3
N/A
: Not
app
licab
le. 9
5% C
I: 95
% c
onfid
ence
inte
rval
. OR
: odd
s ra
tio. H
R: h
azar
d ra
tio. R
R: r
elat
ive
risk
. OR
/HR
/RR
are
adj
uste
d un
less
oth
erw
ise
spec
ified
SD
(±):
stan
dard
dev
iatio
n. IQ
R: i
nter
quar
tile
rang
e. N
OS,
New
cast
le O
ttaw
a Sc
ale
C
I: ca
rdio
inhi
bito
ry, V
D: v
asod
epre
ssor
, CSM
: car
otid
sin
us m
assa
ge, C
SH: c
arot
id s
inus
hyp
erse
nsiti
vity
, CSS
: car
otid
sin
us s
yndr
ome,
NM
S: n
eura
lly m
edia
ted
sync
ope
¥ C
SS d
efin
ed a
s ei
ther
vas
odep
ress
or d
rop
of 5
0mm
HG
SB
P an
d/or
>3
seco
nd a
syst
ole
on E
CG
∞
CSS
def
ined
as
eith
er v
asod
epre
ssor
dro
p of
50m
mH
G S
BP
or
>3
seco
nd a
syst
ole
on E
CG
with
sym
ptom
rep
rodu
ctio
n *+
+ A
ssoc
iatio
n m
ultiv
aria
bly
adju
sted
for
pote
ntia
l con
foun
ders
, + u
niva
riab
le a
ssoc
iatio
n or
hig
her
prev
alen
ce c
ompa
red
to c
ontr
ol g
roup
, - a
bsen
t ass
ocia
tion
or s
imila
r pr
eval
ence
TABLE 3 (CONTINUED)
Allc
ock
2000
31
120
78
(ran
ge
66-9
4)
Obs
erva
tiona
l se
ries
, fal
ls &
sy
ncop
e cl
inic
, re
tros
pect
ive
Ref
erre
d fo
r un
expl
aine
d fa
lls
and
sync
ope
CSM
L+
R, s
upin
e &
up
righ
t (70
°)
37%
CSH
(22%
CI a
nd
15%
VD
) C
SS w
as c
omm
on in
pa
tient
s w
ith
unex
plai
ned
falls
¥
3
Dav
ies
1996
48
26
79 (S
E 8)
O
bser
vatio
nal
seri
es, e
mer
genc
y de
part
men
t,
cros
s-se
ctio
nal
Une
xpla
ined
an
d re
curr
ent
falls
CSM
L+
R, s
upin
e &
up
righ
t (70
°)
73%
C
SH w
as c
omm
on in
pa
tient
s w
ith
unex
plai
ned
falls
¥
3
Dey
19
97 51
35
75
(r
ange
50
-95)
Obs
erva
tiona
l se
ries
, fal
ls &
sy
ncop
e cl
inic
, cr
oss-
sect
iona
l
Dro
p at
tack
s (u
nexp
lain
ed
falls
)
CSM
L+
R, s
upin
e &
up
righ
t (70
°)
CSH
51%
, CI o
r m
ixed
C
SS in
15,
VD
CSS
in 3
C
SS w
as c
omm
on in
th
ose
with
une
xpla
ined
fa
lls
∞
3
Eltr
afi
1999
53
139
66 [
±20
] O
bser
vatio
nal
seri
es, f
alls
&
sync
ope
clin
ic,
retr
ospe
ctiv
e
Une
xpla
ined
fa
lls
CSM
L+
R, s
upin
e &
up
righ
t (70
°)
21%
. C
SS is
res
pons
ible
for
recu
rren
t fal
ls a
nd
sync
ope
in 2
1% o
f pa
tient
s re
ferr
ed to
a
med
ical
out
patie
nt
clin
ic.
¥
3
Ken
ny
1991
68
130
77,
rang
e 67
-89
Obs
erva
tiona
l se
ries
, fal
ls &
sy
ncop
e cl
inic
, re
tros
pect
ive
Ref
erre
d fo
r un
expl
aine
d fa
lls
and
sync
ope
Supi
ne C
SM o
nly
13%
C
SS is
pre
sent
in a
sm
all
num
ber
of p
atie
nts
who
pr
esen
t with
une
xpla
ined
fa
lls, d
izzi
ness
or
sync
ope
¥
2
De
Cas
tro
Lace
rda
2008
71
502
65
[±10
] O
bser
vatio
nal
seri
es,
falls
& s
ynco
pe
clin
ic, c
ross
-se
ctio
nal
Une
xpla
ined
fa
lls in
the
past
12
mon
ths
Supi
ne C
SM o
nly
14%
C
SH w
as p
rese
nt in
larg
e nu
mbe
r of
pat
ient
with
un
expl
aine
d fa
lls
¥
3
Lagr
o 20
13 72
17
5 (w
ith
falls
)
75+
O
bser
vatio
nal
seri
es, f
alls
&
sync
ope
clin
ic,
cros
s-se
ctio
nal
Une
xpla
ined
fa
lls
CSM
L+
R, s
upin
e &
up
righ
t (70
°)
84%
C
SH w
as c
omm
on in
un
expl
aine
d fa
llers
¥
3
Milt
on
2009
86
1464
78
[±
10]
Obs
erva
tiona
l se
ries
, fal
ls &
sy
ncop
e cl
inic
, cr
oss-
sect
iona
l
Falls
and
sy
ncop
e C
SM L
+R
, sup
ine
&
upri
ght (
70°)
8%
C
SH w
as p
rese
nt in
a
smal
l am
ount
of p
atie
nts
with
une
xpla
ined
falls
¥
2
Palin
g 20
11 90
11
1 (w
ith
falls
)
82,
rang
e 61
-99
Obs
erva
tiona
l se
ries
, fal
ls &
sy
ncop
e cl
inic
, cr
oss-
sect
iona
l
Une
xpla
ined
fa
lls
CSM
L+
R, s
upin
e &
up
righ
t (70
°)
44%
(n=
28 V
D, n
=16
m
ixed
, n=
5 C
I) of
un
expl
aine
d fa
llers
42
% o
f tho
se w
ith
sync
ope
CSS
was
com
mon
in
patie
nts
with
un
expl
aine
d fa
lls,
∞
3
Parr
y 93
77
[±
9],
Obs
erva
tiona
l D
rop
atta
cks
(3
CSM
L+
R, s
upin
e &
40
% (
n=35
CI/m
ixed
, C
SS w
as c
omm
on in
¥
3
TABLE 3 (CONTINUED)
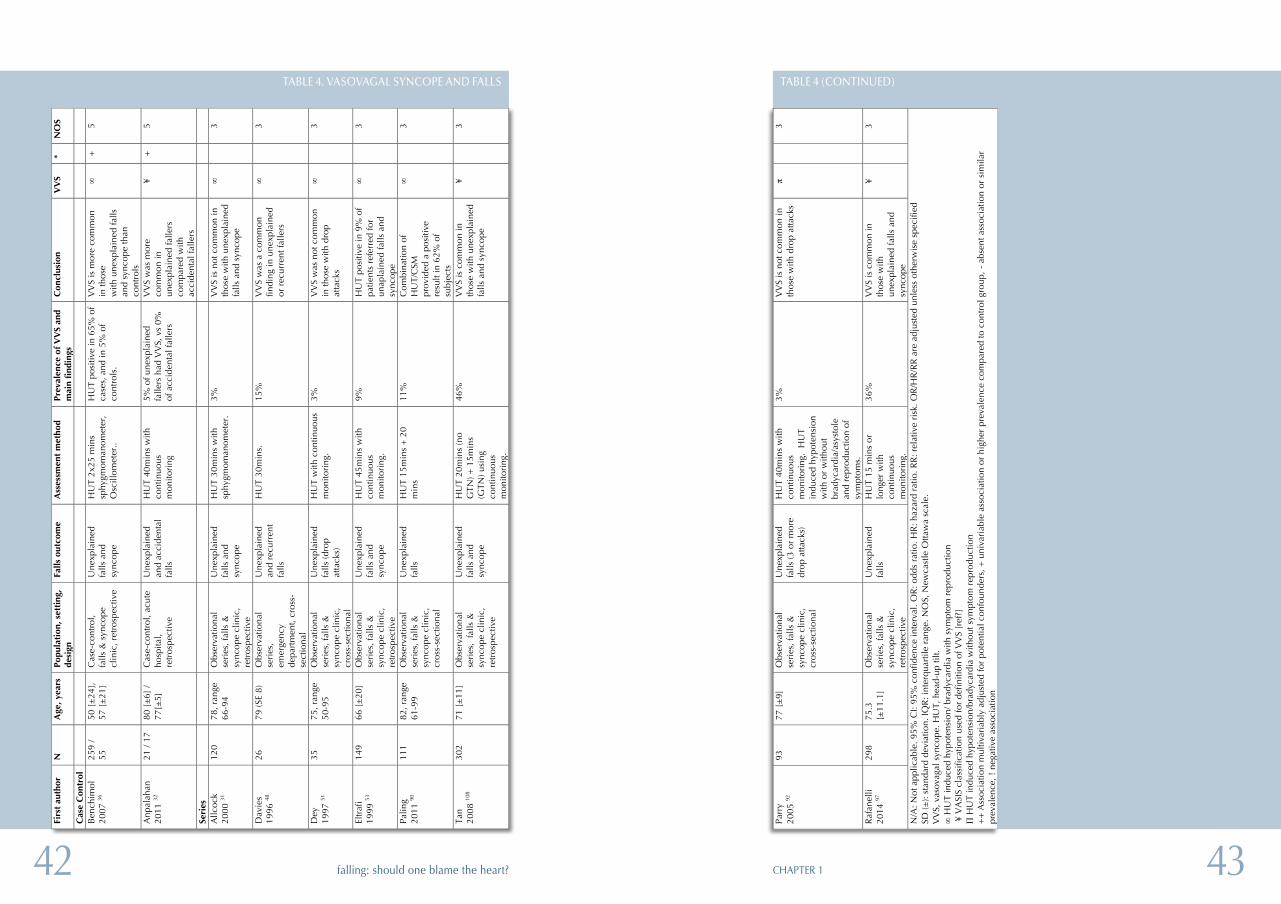
4342 CHAPTER 1falling: should one blame the heart?
Parr
y 20
05 92
93
77
[±
9]
Obs
erva
tiona
l se
ries
, fal
ls &
sy
ncop
e cl
inic
, cr
oss-
sect
iona
l
Une
xpla
ined
fa
lls (3
or
mor
e dr
op a
ttack
s)
HU
T 40
min
s w
ith
cont
inuo
us
mon
itori
ng.
HU
T in
duce
d hy
pote
nsio
n w
ith o
r w
ithou
t br
adyc
ardi
a/as
ysto
le
and
repr
oduc
tion
of
sym
ptom
s.
3%
VV
S is
not
com
mon
in
thos
e w
ith d
rop
atta
cks
π
3
Raf
anel
li 20
14 97
29
8 75
.3
[±11
.1]
Obs
erva
tiona
l se
ries
, fal
ls &
sy
ncop
e cl
inic
, re
tros
pect
ive
Une
xpla
ined
fa
lls
HU
T 15
min
s or
lo
nger
with
co
ntin
uous
m
onito
ring
.
36%
V
VS
is c
omm
on in
th
ose
with
un
expl
aine
d fa
lls a
nd
sync
ope
¥
3
N/A
: Not
app
licab
le. 9
5% C
I: 95
% c
onfid
ence
inte
rval
. OR
: odd
s ra
tio. H
R: h
azar
d ra
tio. R
R: r
elat
ive
risk
. OR
/HR
/RR
are
adj
uste
d un
less
oth
erw
ise
spec
ified
SD
(±):
stan
dard
dev
iatio
n. IQ
R: i
nter
quar
tile
rang
e. N
OS,
New
cast
le O
ttaw
a sc
ale.
V
VS,
vas
ovag
al s
ynco
pe. H
UT,
hea
d-up
tilt.
∞
HU
T in
duce
d hy
pote
nsio
n/ b
rady
card
ia w
ith s
ympt
om r
epro
duct
ion
¥ V
ASI
S cl
assi
ficat
ion
used
for
defin
ition
of V
VS
[ref
?]
Π H
UT
indu
ced
hypo
tens
ion/
brad
ycar
dia
with
out s
ympt
om r
epro
duct
ion
++
Ass
ocia
tion
mul
tivar
iabl
y ad
just
ed fo
r po
tent
ial c
onfo
unde
rs, +
uni
vari
able
ass
ocia
tion
or h
ighe
r pr
eval
ence
com
pare
d to
con
trol
gro
up, -
abs
ent a
ssoc
iatio
n or
sim
ilar
prev
alen
ce, !
neg
ativ
e as
soci
atio
n
TABLE 4 (CONTINUED)
Tabl
e 4.
Vas
ovag
al s
ynco
pe a
nd f
alls
Firs
t au
thor
N
Age
, yea
rs
Popu
lati
on, s
etti
ng,
desi
gn
Falls
out
com
e A
sses
smen
t m
etho
d Pr
eval
ence
of
VV
S an
d m
ain
find
ings
C
oncl
usio
n V
VS
* N
OS
Cas
e C
ontr
ol
Ben
chim
ol
2007
36
259
/ 55
50
[±
24],
57
[±
21]
Cas
e-co
ntro
l, fa
lls &
syn
cope
cl
inic
, ret
rosp
ectiv
e
Une
xpla
ined
fa
lls a
nd
sync
ope
HU
T 2x
25 m
ins
sphy
gmom
anom
eter
, O
scill
omet
er..
HU
T po
sitiv
e in
65%
of
case
s, a
nd in
5%
of
cont
rols
.
VV
S is
mor
e co
mm
on
in th
ose
with
une
xpla
ined
falls
an
d sy
ncop
e th
an
cont
rols
∞
+
5
Anp
alah
an
2011
32
21 /
17
80 [
±6]
/ 77
[±5]
C
ase-
cont
rol,
acut
e ho
spita
l, re
tros
pect
ive
Une
xpla
ined
an
d ac
cide
ntal
fa
lls
HU
T 40
min
s w
ith
cont
inuo
us
mon
itori
ng
5% o
f une
xpla
ined
fa
llers
had
VV
S, v
s 0%
of
acc
iden
tal f
alle
rs
VV
S w
as m
ore
com
mon
in
unex
plai
ned
falle
rs
com
pare
d w
ith
acci
dent
al fa
llers
¥ +
5
Seri
es
Allc
ock
20
00 31
12
0 78
, ran
ge
66-9
4 O
bser
vatio
nal
seri
es, f
alls
&
sync
ope
clin
ic,
retr
ospe
ctiv
e
Une
xpla
ined
fa
lls a
nd
sync
ope
HU
T 30
min
s w
ith
sphy
gmom
anom
eter
. 3%
V
VS
is n
ot c
omm
on in
th
ose
with
une
xpla
ined
fa
lls a
nd s
ynco
pe
∞
3
Dav
ies
19
96 48
26
79
(SE
8)
Obs
erva
tiona
l se
ries
, em
erge
ncy
depa
rtm
ent,
cros
s-se
ctio
nal
Une
xpla
ined
an
d re
curr
ent
falls
HU
T 30
min
s.
15%
V
VS
was
a c
omm
on
findi
ng in
une
xpla
ined
or
rec
urre
nt fa
llers
∞
3
Dey
19
97 51
35
75
, ran
ge
50-9
5 O
bser
vatio
nal
seri
es, f
alls
&
sync
ope
clin
ic,
cros
s-se
ctio
nal
Une
xpla
ined
fa
lls (d
rop
atta
cks)
HU
T w
ith c
ontin
uous
m
onito
ring
. 3%
V
VS
was
not
com
mon
in
thos
e w
ith d
rop
atta
cks
∞
3
Eltr
afi
1999
53
149
66 [
±20
] O
bser
vatio
nal
seri
es, f
alls
&
sync
ope
clin
ic,
retr
ospe
ctiv
e
Une
xpla
ined
fa
lls a
nd
sync
ope
HU
T 45
min
s w
ith
cont
inuo
us
mon
itori
ng.
9%
HU
T po
sitiv
e in
9%
of
patie
nts
refe
rred
for
unap
lain
ed fa
lls a
nd
sync
ope
∞
3
Palin
g 20
11 90
11
1 82
, ran
ge
61-9
9 O
bser
vatio
nal
seri
es, f
alls
&
sync
ope
clin
ic,
cros
s-se
ctio
nal
Une
xpla
ined
fa
lls
HU
T 15
min
s +
20
min
s 11
%
C
ombi
natio
n of
H
UT/
CSM
pr
ovid
ed a
pos
itive
re
sult
in 6
2% o
f su
bjec
ts
∞
3
Tan
2008
108
302
71 [
±11
] O
bser
vatio
nal
seri
es,
falls
&
sync
ope
clin
ic,
retr
ospe
ctiv
e
Une
xpla
ined
fa
lls a
nd
sync
ope
HU
T 20
min
s (n
o G
TN) +
15m
ins
(GTN
) usi
ng
cont
inuo
us
mon
itori
ng.
46%
VV
S is
com
mon
in
thos
e w
ith u
nexp
lain
ed
falls
and
syn
cope
¥
3
TABLE 4. VASOVAGAL SYNCOPE AND FALLS
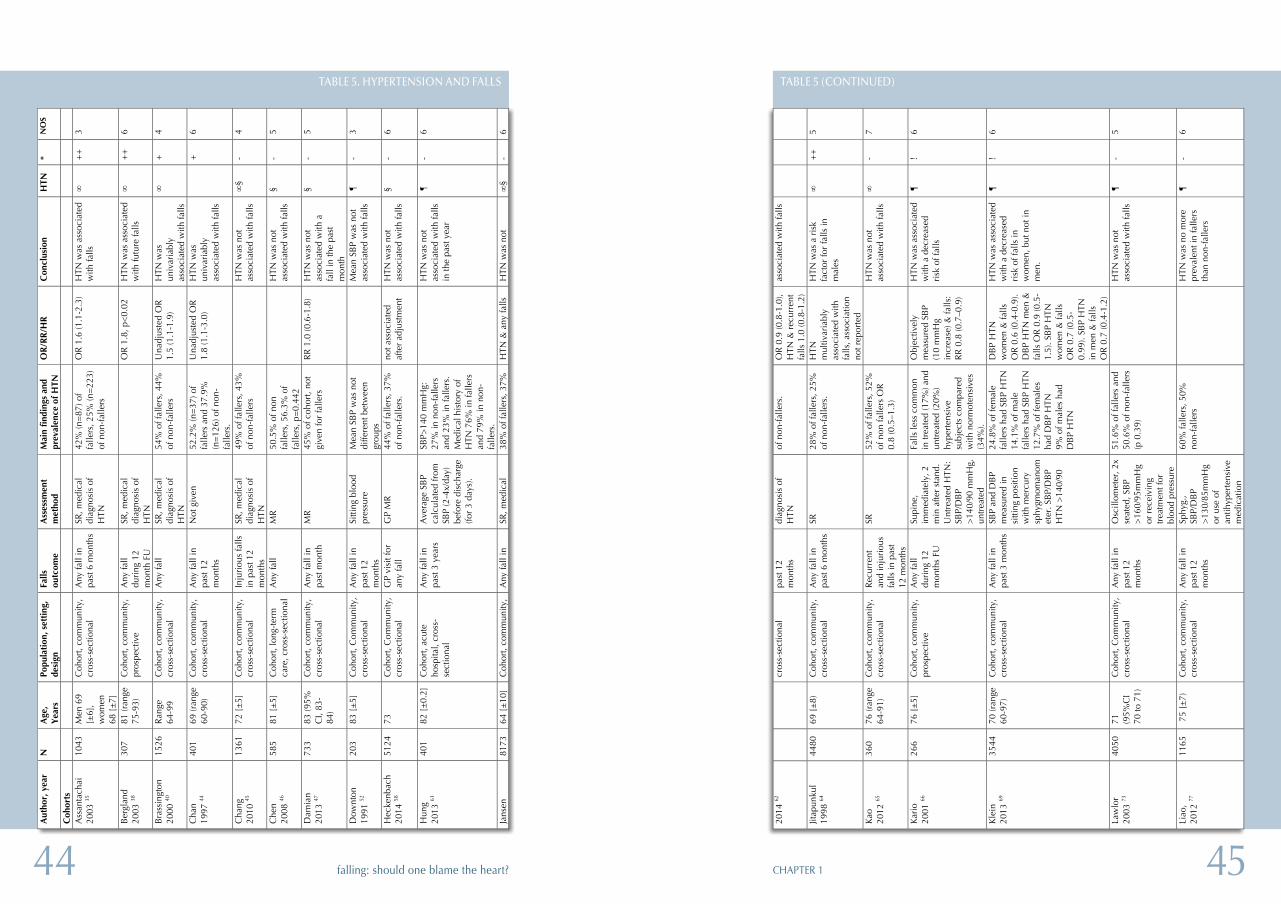
4544 CHAPTER 1falling: should one blame the heart?
2014
62
cros
s-se
ctio
nal
past
12
mon
ths
diag
nosi
s of
H
TN
of n
on-f
alle
rs.
OR
0.9
(0.8
-1.0
), H
TN &
rec
urre
nt
falls
1.0
(0.8
-1.2
)
asso
ciat
ed w
ith fa
lls
Jitap
unku
l 19
98 64
44
80
69 [
±8)
C
ohor
t, co
mm
unity
, cr
oss-
sect
iona
l A
ny fa
ll in
pa
st 6
mon
ths
SR
28%
of f
alle
rs, 2
5%
of n
on-f
alle
rs.
HTN
m
ultiv
aria
bly
asso
ciat
ed w
ith
falls
, ass
ocia
tion
not r
epor
ted
HTN
was
a r
isk
fact
or fo
r fa
lls in
m
ales
∞
++
5
Kao
20
12 65
36
0 76
(ran
ge
64-9
1)
Coh
ort,
com
mun
ity,
cros
s-se
ctio
nal
Rec
urre
nt
and
inju
riou
s fa
lls in
pas
t 12
mon
ths
SR
52%
of f
alle
rs, 5
2%
of n
on fa
llers
OR
0.
8 (0
.5–1
.3)
H
TN w
as n
ot
asso
ciat
ed w
ith fa
lls
∞
- 7
Kar
io
2001
66
266
76 [
±5]
C
ohor
t, co
mm
unity
, pr
ospe
ctiv
e
Any
fall
duri
ng 1
2 m
onth
s FU
Supi
ne,
imm
edia
tely
, 2
min
afte
r st
and.
U
ntre
ated
HTN
: SB
P/D
BP
>14
0/90
mm
Hg,
un
trea
ted
Falls
less
com
mon
in
trea
ted
(17%
) and
un
trea
ted
(20%
) hy
pert
ensi
ve
subj
ects
com
pare
d w
ith n
orm
oten
sive
s (3
4%).
Obj
ectiv
ely
mea
sure
d SB
P (1
0 m
mH
g in
crea
se) &
falls
: R
R 0
.8 (0
.7–0
.9)
HTN
was
ass
ocia
ted
with
a d
ecre
ased
ri
sk o
f fal
ls
¶
! 6
Kle
in
2013
69
3544
70
(ran
ge
60-9
7)
Coh
ort,
com
mun
ity,
cros
s-se
ctio
nal
Any
fall
in
past
3 m
onth
s SB
P an
d D
BP
mea
sure
d in
si
tting
pos
ition
w
ith m
ercu
ry
sphy
gmom
anom
eter
. SB
P/D
BP
HTN
>14
0/90
24.8
% o
f fem
ale
falle
rs h
ad S
BP
HTN
14
.1%
of m
ale
falle
rs h
ad S
BP
HTN
12
.7%
of f
emal
es
had
DB
P H
TN
9% o
f mal
es h
ad
DB
P H
TN
DB
P H
TN
wom
en &
falls
O
R 0
.6 (0
.4-0
.9).
DB
P H
TN m
en &
fa
lls O
R 0
.9 (0
.5-
1.5)
. SB
P H
TN
wom
en &
falls
O
R 0
.7 (0
.5-
0.99
). SB
P H
TN
in m
en &
falls
O
R 0
.7 (0
.4-1
.2)
HTN
was
ass
ocia
ted
with
a d
ecre
ased
ri
sk o
f fal
ls in
w
omen
, but
not
in
men
.
¶
! 6
Law
lor
2003
73
4050
71
(9
5%C
I 70
to 7
1)
Coh
ort,
Com
mun
ity,
cros
s-se
ctio
nal
Any
fall
in
past
12
mon
ths
Osc
illom
eter
, 2x
seat
ed, S
BP
>16
0/95
mm
Hg
or r
ecei
ving
tr
eatm
ent f
or
bloo
d pr
essu
re
51.6
% o
f fal
lers
and
50
.6%
of n
on-f
alle
rs
(p 0
.39)
H
TN w
as n
ot
asso
ciat
ed w
ith fa
lls
¶
- 5
Liao
, 20
12 77
11
65
75
[±7)
C
ohor
t, co
mm
unity
, cr
oss-
sect
iona
l A
ny fa
ll in
pa
st 1
2 m
onth
s
Sphy
g.,
SBP/
DB
P >
130/
85m
mH
g or
use
of
antih
yper
tens
ive
med
icat
ion
60%
falle
rs, 5
0%
non-
falle
rs
H
TN w
as n
o m
ore
prev
alen
t in
falle
rs
than
non
-fal
lers
¶
- 6
TABLE 5 (CONTINUED)
Tabl
e 5.
Hyp
erte
nsio
n an
d fa
lls
Aut
hor,
yea
r N
A
ge,
Yea
rs
Popu
lati
on, s
etti
ng,
desi
gn
Falls
ou
tcom
e A
sses
smen
t m
etho
d M
ain
findi
ngs
and
prev
alen
ce o
f HTN
O
R/R
R/H
R
Con
clus
ion
HTN
*
NO
S
Coh
orts
Ass
anta
chai
20
03 35
10
43
Men
69
[±6]
, w
omen
68
[±
7]
Coh
ort,
com
mun
ity,
cros
s-se
ctio
nal
Any
fall
in
past
6 m
onth
s SR
, med
ical
di
agno
sis
of
HTN
42%
(n=
87) o
f fa
llers
, 25%
(n=
223)
of
non
-fal
lers
OR
1.6
(1.1
-2.3
) H
TN w
as a
ssoc
iate
d w
ith fa
lls
∞
++
3
Ber
glan
d
2003
38
307
81 (r
ange
75
-93)
C
ohor
t, co
mm
unity
, pr
ospe
ctiv
e A
ny fa
ll du
ring
12
mon
th F
U
SR, m
edic
al
diag
nosi
s of
H
TN
O
R 1
.8, p
<0.
02
HTN
was
ass
ocia
ted
with
futu
re fa
lls
∞
++
6
Bra
ssin
gton
20
00 40
15
26
Ran
ge
64-9
9 C
ohor
t, co
mm
unity
, cr
oss-
sect
iona
l A
ny fa
ll SR
, med
ical
di
agno
sis
of
HTN
54%
of f
alle
rs, 4
4%
of n
on-f
alle
rs
Una
djus
ted
OR
1.
5 (1
.1-1
.9)
HTN
was
un
ivar
iabl
y as
soci
ated
with
falls
∞
+
4
Cha
n 19
97 44
40
1 69
(ran
ge
60-9
0)
Coh
ort,
com
mun
ity,
cros
s-se
ctio
nal
Any
fall
in
past
12
mon
ths
Not
giv
en
52.2
% (n
=37
) of
falle
rs a
nd 3
7.9%
(n
=12
6) o
f non
-fa
llers
.
Una
djus
ted
OR
1.
8 (1
.1-3
.0)
HTN
was
un
ivar
iabl
y as
soci
ated
with
falls
+
6
Cha
ng
2010
45
1361
72
[±
5]
Coh
ort,
com
mun
ity,
cros
s-se
ctio
nal
Inju
riou
s fa
lls
in p
ast 1
2 m
onth
s
SR, m
edic
al
diag
nosi
s of
H
TN
49%
of f
alle
rs, 4
3%
of n
on-f
alle
rs
H
TN w
as n
ot
asso
ciat
ed w
ith fa
lls
∞§
- 4
Che
n 20
08 46
58
5 81
[±
5]
Coh
ort,
long
-ter
m
care
, cro
ss-s
ectio
nal
Any
fall
MR
50
.5%
of n
on
falle
rs, 5
6.3%
of
falle
rs, p
=0.
442
H
TN w
as n
ot
asso
ciat
ed w
ith fa
lls
§ -
5
Dam
ian
2013
47
733
83 (9
5%
CI,
83-
84)
Coh
ort,
com
mun
ity,
cros
s-se
ctio
nal
Any
fall
in
past
mon
th
MR
45
% o
f coh
ort,
not
give
n fo
r fa
llers
R
R 1
.0 (0
.6-1
.8)
HTN
was
not
as
soci
ated
with
a
fall
in th
e pa
st
mon
th
§ -
5
Dow
nton
19
91 52
20
3 83
[±
5]
Coh
ort,
Com
mun
ity,
cros
s-se
ctio
nal
Any
fall
in
past
12
mon
ths
Sitti
ng b
lood
pr
essu
re
Mea
n SB
P w
as n
ot
diffe
rent
bet
wee
n gr
oups
M
ean
SBP
was
not
as
soci
ated
with
falls
¶
-
3
Hec
kenb
ach
2014
58
5124
73
C
ohor
t, C
omm
unity
, cr
oss-
sect
iona
l G
P vi
sit f
or
any
fall
GP
MR
44
% o
f fal
lers
, 37%
of
non
-fal
lers
. no
t ass
ocia
ted
afte
r ad
just
men
t H
TN w
as n
ot
asso
ciat
ed w
ith fa
lls
§ -
6
Hun
g 20
13 61
40
1 82
[±
0.2]
C
ohor
t, ac
ute
hosp
ital,
cros
s-se
ctio
nal
Any
fall
in
past
3 y
ears
A
vera
ge S
BP
calc
ulat
ed fr
om
SBP
(2-4
x/da
y)
befo
re d
isch
arge
(fo
r 3
days
).
SBP>
140
mm
Hg:
27
% in
non
-fal
lers
an
d 23
% in
falle
rs.
Med
ical
his
tory
of
HTN
76%
in fa
llers
an
d 79
% in
non
-fa
llers
.
H
TN w
as n
ot
asso
ciat
ed w
ith fa
lls
in th
e pa
st y
ear
¶
- 6
Jans
en
8173
64
[±
10]
Coh
ort,
com
mun
ity,
Any
fall
in
SR, m
edic
al
38%
of f
alle
rs, 3
7%
HTN
& a
ny fa
lls
HTN
was
not
∞
§ -
6
TABLE 5. HYPERTENSION AND FALLS
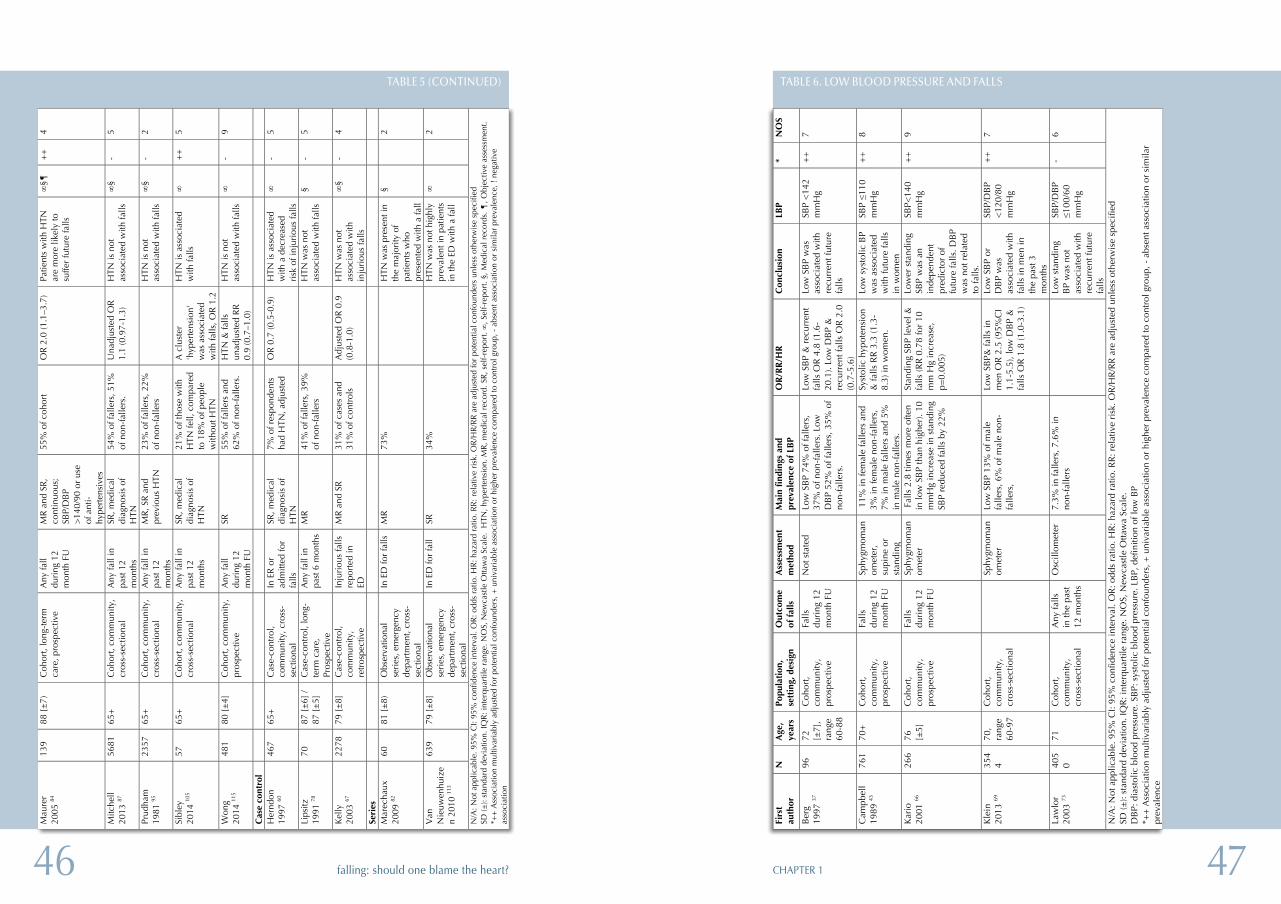
4746 CHAPTER 1falling: should one blame the heart?
Tabl
e 6.
Low
blo
od p
ress
ure
and
falls
Fi
rst
auth
or
N
Age
, ye
ars
Popu
lati
on,
sett
ing,
des
ign
Out
com
e of
fal
ls
Ass
essm
ent
met
hod
Mai
n fi
ndin
gs a
nd
prev
alen
ce o
f LB
P O
R/R
R/H
R
Con
clus
ion
LBP
* N
OS
Ber
g 19
97 37
96
72
[±
7],
rang
e 60
-88
Coh
ort,
com
mun
ity,
pros
pect
ive
Falls
du
ring
12
mon
th F
U
Not
sta
ted
Low
SB
P 74
% o
f fal
lers
, 37
% o
f non
-fal
lers
. Low
D
BP
52%
of f
alle
rs, 3
5% o
f no
n-fa
llers
.
Low
SB
P &
rec
urre
nt
falls
OR
4.8
(1.6
-20
.1).
Low
DB
P &
re
curr
ent f
alls
OR
2.0
(0
.7-5
.6)
Low
SB
P w
as
asso
ciat
ed w
ith
recu
rren
t fut
ure
falls
SBP
<14
2 m
mH
g +
+
7
Cam
pbel
l 19
89 43
76
1 70
+
Coh
ort,
com
mun
ity,
pros
pect
ive
Falls
du
ring
12
mon
th F
U
Sphy
gmom
anom
eter
, su
pine
or
stan
ding
11%
in fe
mal
e fa
llers
and
3%
in fe
mal
e no
n-fa
llers
, 7%
in m
ale
falle
rs a
nd 5
%
in m
ale
non-
falle
rs.
Syst
olic
hyp
oten
sion
&
falls
RR
3.3
(1.3
-8.
3) in
wom
en.
Low
sys
tolic
BP
was
ass
ocia
ted
with
futu
re fa
lls
in w
omen
SBP ≤1
10
mm
Hg
++
8
Kar
io
2001
66
266
76
[±5]
C
ohor
t, co
mm
unity
, pr
ospe
ctiv
e
Falls
du
ring
12
mon
th F
U
Sphy
gmom
anom
eter
F
alls
2.8
tim
es m
ore
ofte
n in
low
SB
P th
an h
ighe
r). 1
0 m
mH
g in
crea
se in
sta
ndin
g SB
P re
duce
d fa
lls b
y 22
%
Stan
ding
SB
P le
vel &
fa
lls (R
R 0
.78
for
10
mm
Hg
incr
ease
, p=
0.00
5)
Low
er s
tand
ing
SBP
was
an
inde
pend
ent
pred
icto
r of
fu
ture
falls
. DB
P w
as n
ot r
elat
ed
to fa
lls.
SBP<
140
mm
Hg
++
9
Kle
in
2013
69
354
4 70
, ra
nge
60-9
7
Coh
ort,
com
mun
ity,
cros
s-se
ctio
nal
Sp
hygm
oman
omet
er
Low
SB
P 13
% o
f mal
e fa
llers
, 6%
of m
ale
non-
falle
rs,
Low
SB
P& fa
lls in
m
en O
R 2
.5 (9
5%C
I 1.
1-5.
5), l
ow D
BP
&
falls
OR
1.8
(1.0
-3.1
)
Low
SB
P or
D
BP
was
as
soci
ated
with
fa
lls in
men
in
the
past
3
mon
ths
SBP/
DB
P <
120/
80
mm
Hg
++
7
Law
lor
2003
73
405
0 71
C
ohor
t, co
mm
unity
, cr
oss-
sect
iona
l
Any
falls
in
the
past
12
mon
ths
Osc
illom
eter
7.
3% in
falle
rs, 7
.6%
in
non-
falle
rs
Lo
w s
tand
ing
BP
was
not
as
soci
ated
with
re
curr
ent f
utur
e fa
lls
SBP/
DB
P ≤1
00/6
0 m
mH
g
- 6
N/A
: Not
app
licab
le. 9
5% C
I: 95
% c
onfid
ence
inte
rval
. OR
: odd
s ra
tio. H
R: h
azar
d ra
tio. R
R: r
elat
ive
risk
. OR
/HR
/RR
are
adj
uste
d un
less
oth
erw
ise
spec
ified
SD
(±):
stan
dard
dev
iatio
n. IQ
R: i
nter
quar
tile
rang
e. N
OS,
New
cast
le O
ttaw
a Sc
ale.
D
BP:
dia
stol
ic b
lood
pre
ssur
e. S
BP:
sys
tolic
blo
od p
ress
ure.
LB
P, d
efin
ition
of l
ow B
P *+
+ A
ssoc
iatio
n m
ultiv
aria
bly
adju
sted
for
pote
ntia
l con
foun
ders
, + u
niva
riab
le a
ssoc
iatio
n or
hig
her
prev
alen
ce c
ompa
red
to c
ontr
ol g
roup
, - a
bsen
t ass
ocia
tion
or s
imila
r pr
eval
ence
TABLE 6. LOW BLOOD PRESSURE AND FALLS
Mau
rer
2005
84
139
88 [
±7)
C
ohor
t, lo
ng-t
erm
ca
re, p
rosp
ectiv
e A
ny fa
ll du
ring
12
mon
th F
U
MR
and
SR
, co
ntin
uous
; SB
P/D
BP
>14
0/90
or
use
of a
nti-
hype
rten
sive
s
55%
of c
ohor
t
OR
2.0
(1.1
–3.7
) Pa
tient
s w
ith H
TN
are
mor
e lik
ely
to
suffe
r fu
ture
falls
∞§¶
+
+
4
Mitc
hell
2013
87
5681
65
+
Coh
ort,
com
mun
ity,
cros
s-se
ctio
nal
Any
fall
in
past
12
mon
ths
SR, m
edic
al
diag
nosi
s of
H
TN
54%
of f
alle
rs, 5
1%
of n
on-f
alle
rs.
Una
djus
ted
OR
1.
1 (0
.97-
1.3)
H
TN is
not
as
soci
ated
with
falls
∞
§ -
5
Prud
ham
19
81 95
23
57
65+
C
ohor
t, co
mm
unity
, cr
oss-
sect
iona
l A
ny fa
ll in
pa
st 1
2 m
onth
s
MR
, SR
and
pr
evio
us H
TN
23%
of f
alle
rs, 2
2%
of n
on-f
alle
rs
H
TN is
not
as
soci
ated
with
falls
∞
§ -
2
Sibl
ey
2014
105
57
65+
C
ohor
t, co
mm
unity
, cr
oss-
sect
iona
l A
ny fa
ll in
pa
st 1
2 m
onth
s
SR, m
edic
al
diag
nosi
s of
H
TN
21%
of t
hose
with
H
TN fe
ll, c
ompa
red
to 1
8% o
f peo
ple
with
out H
TN
A c
lust
er
'hyp
erte
nsio
n'
was
ass
ocia
ted
with
falls
, OR
1.2
HTN
is a
ssoc
iate
d w
ith fa
lls
∞
++
5
Won
g 20
14 11
5 48
1 80
[±
4]
Coh
ort,
com
mun
ity,
pros
pect
ive
Any
fall
duri
ng 1
2 m
onth
FU
SR
55%
of f
alle
rs a
nd
62%
of n
on-f
alle
rs.
HTN
& fa
lls
unad
just
ed R
R
0.9
(0.7
–1.0
)
HTN
is n
ot
asso
ciat
ed w
ith fa
lls
∞
- 9
Cas
e co
ntro
l
Her
ndon
19
97 60
46
7 65
+
Cas
e-co
ntro
l, co
mm
unity
, cro
ss-
sect
iona
l
In E
R o
r ad
mitt
ed fo
r fa
lls
SR, m
edic
al
diag
nosi
s of
H
TN
7% o
f res
pond
ents
ha
d H
TN, a
djus
ted
O
R 0
.7 (0
.5-0
.9)
HTN
is a
ssoc
iate
d w
ith a
dec
reas
ed
risk
of i
njur
ious
falls
∞
- 5
Lips
itz
1991
78
70
87 [
±6]
/ 87
[±
5]
Cas
e-co
ntro
l, lo
ng-
term
car
e,
Pros
pect
ive
Any
fall
in
past
6 m
onth
s M
R
41%
of f
alle
rs, 3
9%
of n
on-f
alle
rs
H
TN w
as n
ot
asso
ciat
ed w
ith fa
lls
§ -
5
Kel
ly
2003
67
2278
79
[±
8]
Cas
e-co
ntro
l, co
mm
unity
, re
tros
pect
ive
Inju
riou
s fa
lls
repo
rted
in
ED
MR
and
SR
31
% o
f cas
es a
nd
31%
of c
ontr
ols
Adj
uste
d O
R 0
.9
(0.8
-1.0
) H
TN w
as n
ot
asso
ciat
ed w
ith
inju
riou
s fa
lls
∞§
- 4
Seri
es
M
arec
haux
20
09 82
60
81
[±
8)
Obs
erva
tiona
l se
ries
, em
erge
ncy
depa
rtm
ent,
cros
s-se
ctio
nal
In E
D fo
r fa
lls
MR
73
%
H
TN w
as p
rese
nt in
th
e m
ajor
ity o
f pa
tient
s w
ho
pres
ente
d w
ith a
fall
§
2
Van
N
ieuw
enhu
ize
n 20
10 11
3
639
79 [
±8]
O
bser
vatio
nal
seri
es, e
mer
genc
y de
part
men
t, cr
oss-
sect
iona
l
In E
D fo
r fa
ll SR
34
%
H
TN w
as n
ot h
ighl
y pr
eval
ent i
n pa
tient
s in
the
ED w
ith a
fall
∞
2
N/A
: Not
app
licab
le. 9
5% C
I: 95
% c
onfid
ence
inte
rval
. OR
: odd
s ra
tio. H
R: h
azar
d ra
tio. R
R:
rela
tive
risk
. OR
/HR
/RR
are
adj
uste
d fo
r po
tent
ial c
onfo
unde
rs u
nles
s ot
herw
ise
spec
ified
SD
(±):
stan
dard
dev
iatio
n. IQ
R: i
nter
quar
tile
rang
e. N
OS,
New
cast
le O
ttaw
a Sc
ale.
HTN
, hyp
erte
nsio
n. M
R, m
edic
al r
ecor
d. S
R, s
elf-
repo
rt. ∞
, Sel
f-re
port
. §, M
edic
al r
ecor
ds. ¶
, Obj
ectiv
e as
sess
men
t. *+
+ A
ssoc
iatio
n m
ultiv
aria
bly
adju
sted
for
pote
ntia
l con
foun
ders
, + u
niva
riab
le a
ssoc
iatio
n or
hig
her
prev
alen
ce c
ompa
red
to c
ontr
ol g
roup
, - a
bsen
t ass
ocia
tion
or s
imila
r pr
eval
ence
, ! n
egat
ive
asso
ciat
ion
TABLE 5 (CONTINUED)
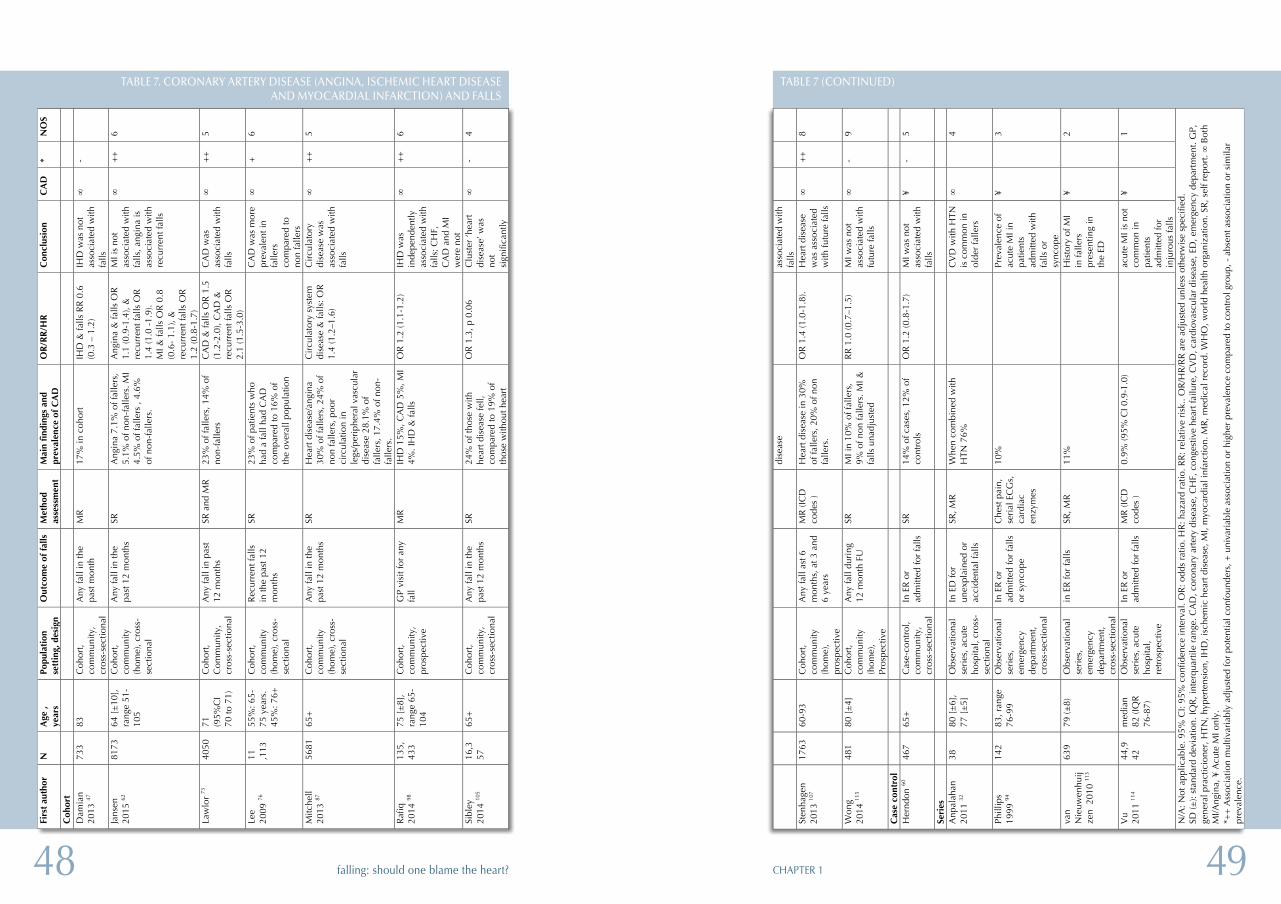
4948 CHAPTER 1falling: should one blame the heart?
dise
ase
asso
ciat
ed w
ith
falls
St
enha
gen
2013
107
1763
60
-93
Coh
ort,
com
mun
ity
(hom
e),
pros
pect
ive
Any
fall
ast 6
m
onth
s, a
t 3 a
nd
6 ye
ars
MR
(IC
D
code
s )
Hea
rt d
isea
se in
30%
of
falle
rs, 2
0% o
f non
fa
llers
.
OR
1.4
(1.0
-1.8
). H
eart
dis
ease
w
as a
ssoc
iate
d w
ith fu
ture
falls
∞
++
8
Won
g 20
14 11
5 48
1 80
[±
4]
Coh
ort,
com
mun
ity
(hom
e),
Pros
pect
ive
Any
fall
duri
ng
12 m
onth
FU
SR
M
I in
10%
of f
alle
rs,
9% o
f non
falle
rs. M
I &
falls
una
djus
ted
RR
1.0
(0.7
–1.5
) M
I was
not
as
soci
ated
with
fu
ture
falls
∞
- 9
Cas
e co
ntro
l
Her
ndon
60
467
65+
C
ase-
cont
rol,
com
mun
ity,
cros
s-se
ctio
nal
In E
R o
r ad
mitt
ed fo
r fa
lls
SR
14%
of c
ases
, 12%
of
cont
rols
O
R 1
.2 (0
.8-1
.7)
MI w
as n
ot
asso
ciat
ed w
ith
falls
¥ -
5
Seri
es
A
npal
ahan
20
11 32
38
80
[±
6],
77 [
±5]
O
bser
vatio
nal
seri
es, a
cute
ho
spita
l, cr
oss-
sect
iona
l
In E
D fo
r un
expl
aine
d or
ac
cide
ntal
falls
SR, M
R
Whe
n co
mbi
ned
with
H
TN 7
6%
C
VD
with
HTN
is
com
mon
in
olde
r fa
llers
∞
4
Phill
ips
1999
94
142
83, r
ange
76
-99
Obs
erva
tiona
l se
ries
, em
erge
ncy
depa
rtm
ent,
cros
s-se
ctio
nal
In E
R o
r ad
mitt
ed fo
r fa
lls
or s
ynco
pe
Che
st p
ain,
se
rial
EC
Gs,
ca
rdia
c en
zym
es
10%
Prev
alen
ce o
f ac
ute
MI i
n pa
tient
s ad
mitt
ed w
ith
falls
or
sync
ope
¥
3
van
Nie
uwen
huij
zen
201
0 11
3
639
79 (±
8)
Obs
erva
tiona
l se
ries
, em
erge
ncy
depa
rtm
ent,
cros
s-se
ctio
nal
in E
R fo
r fa
lls
SR, M
R
11%
His
tory
of M
I in
falle
rs
pres
entin
g in
th
e ED
¥
2
Vu
2011
114
44,9
42
med
ian
82 (I
QR
76
-87)
Obs
erva
tiona
l se
ries
, acu
te
hosp
ital,
retr
ospe
ctiv
e
In E
R o
r ad
mitt
ed fo
r fa
lls
MR
(IC
D
code
s )
0.9%
(95%
CI 0
.9-1
.0)
ac
ute
MI i
s no
t co
mm
on in
pa
tient
s ad
mitt
ed fo
r in
juro
us fa
lls
¥
1
N/A
: Not
app
licab
le. 9
5% C
I: 95
% c
onfid
ence
inte
rval
. OR
: odd
s ra
tio. H
R: h
azar
d ra
tio. R
R: r
elat
ive
risk
.. O
R/H
R/R
R a
re a
djus
ted
unle
ss o
ther
wis
e sp
ecifi
ed.
SD (±
): st
anda
rd d
evia
tion.
IQR
, int
erqu
artil
e ra
nge.
CA
D, c
oron
ary
arte
ry d
isea
se, C
HF,
con
gest
ive
hear
t fai
lure
, CV
D, c
ardi
ovas
cula
r di
seas
e, E
D, e
mer
genc
y de
part
men
t. G
P,
gene
ral p
ract
icio
ner,
HTN
, hyp
erte
nsio
n, IH
D, i
sche
mic
hea
rt d
isea
se, M
I, m
yoca
rdia
l inf
arct
ion.
MR
, med
ical
rec
ord.
WH
O, w
orld
hea
lth o
rgan
izat
ion.
SR
, sel
f rep
ort. ∞
Bot
h M
I/Ang
ina,
¥ A
cute
MI o
nly.
*+
+ A
ssoc
iatio
n m
ultiv
aria
bly
adju
sted
for
pote
ntia
l con
foun
ders
, + u
niva
riab
le a
ssoc
iatio
n or
hig
her
prev
alen
ce c
ompa
red
to c
ontr
ol g
roup
, - a
bsen
t ass
ocia
tion
or s
imila
r pr
eval
ence
.
TABLE 7 (CONTINUED)
Tabl
e 7.
Cor
onar
y ar
tery
dis
ease
(A
ngin
a, is
chem
ic h
eart
dis
ease
and
myo
card
ial i
nfar
ctio
n) a
nd f
alls
Firs
t au
thor
N
A
ge ,
year
s Po
pula
tion
se
ttin
g, d
esig
n O
utco
me
of f
alls
M
etho
d as
sess
men
t M
ain
find
ings
and
pr
eval
ence
of
CA
D
OR
/RR
/HR
C
oncl
usio
n C
AD
*
NO
S
Coh
ort
D
amia
n 20
13 47
73
3 83
C
ohor
t, co
mm
unity
, cr
oss-
sect
iona
l
Any
fall
in th
e pa
st m
onth
M
R
17%
in c
ohor
t IH
D &
falls
RR
0.6
(0
.3 –
1.2
) IH
D w
as n
ot
asso
ciat
ed w
ith
falls
∞
-
Jans
en
2015
62
8173
64
[±
10],
ra
nge
51-
105
Coh
ort,
com
mun
ity
(hom
e), c
ross
-se
ctio
nal
Any
fall
in th
e pa
st 1
2 m
onth
s SR
A
ngin
a 7.
1% o
f fal
lers
, 5.
1% o
f non
-fal
lers
. MI
4.5%
of f
alle
rs ,
4.6%
of
non
-fal
lers
.
Ang
ina
& fa
lls O
R
1.1
(0.9
-1.4
), &
re
curr
ent f
alls
OR
1.
4 (1
.0 -
1.9)
. M
I & fa
lls O
R 0
.8
(0.6
- 1.
1), &
re
curr
ent f
alls
OR
1.
2 (0
.8-1
.7)
MI i
s no
t as
soci
ated
with
fa
lls, a
ngin
a is
as
soci
ated
with
re
curr
ent f
alls
∞
++
6
Law
lor
73
4050
71
(9
5%C
I 70
to 7
1)
Coh
ort,
Com
mun
ity,
cros
s-se
ctio
nal
Any
fall
in p
ast
12 m
onth
s SR
and
MR
23
% o
f fal
lers
, 14%
of
non-
falle
rs
CA
D &
falls
OR
1.5
(1
.2-2
.0),
CA
D &
re
curr
ent f
alls
OR
2.
1 (1
.5-3
.0)
CA
D w
as
asso
ciat
ed w
ith
falls
∞
++
5
Lee
2009
76
11
,113
55
%: 6
5-75
yea
rs.
45%
: 76+
Coh
ort,
com
mun
ity
(hom
e), c
ross
-se
ctio
nal
Rec
urre
nt fa
lls
in th
e pa
st 1
2 m
onth
s
SR
23%
of p
atie
nts
who
ha
d a
fall
had
CA
D
com
pare
d to
16%
of
the
over
all p
opul
atio
n
C
AD
was
mor
e pr
eval
ent i
n fa
llers
co
mpa
red
to
non
falle
rs
∞
+
6
Mitc
hell
2013
87
5681
65
+
Coh
ort,
com
mun
ity
(hom
e), c
ross
-se
ctio
nal
Any
fall
in th
e pa
st 1
2 m
onth
s SR
H
eart
dis
ease
/ang
ina
30%
of f
alle
rs, 2
4% o
f no
n fa
llers
, poo
r ci
rcul
atio
n in
le
gs/p
erip
hera
l vas
cula
r di
seas
e 28
.1%
of
falle
rs, 1
7.4%
of n
on-
falle
rs.
Cir
cula
tory
sys
tem
di
seas
e &
falls
: OR
1.
4 (1
.2–1
.6)
Cir
cula
tory
di
seas
e w
as
asso
ciat
ed w
ith
falls
∞
++
5
Raf
iq
2014
98
135,
433
75 [
±8]
, ra
nge
65-
104
Coh
ort,
com
mun
ity,
pros
pect
ive
GP
visi
t for
any
fa
ll M
R
IHD
15%
, CA
D 5
%, M
I 4%
. IH
D &
falls
O
R 1
.2 (1
.1-1
.2)
IHD
was
in
depe
nden
tly
asso
ciat
ed w
ith
falls
; CH
F,
CA
D a
nd M
I w
ere
not
∞
++
6
Sibl
ey
2014
105
16,3
57
65+
C
ohor
t, co
mm
unity
, cr
oss-
sect
iona
l
Any
fall
in th
e pa
st 1
2 m
onth
s SR
24
% o
f tho
se w
ith
hear
t dis
ease
fell,
co
mpa
red
to 1
9% o
f th
ose
with
out h
eart
OR
1.3
, p 0
.06
Clu
ster
‘hea
rt
dise
ase’
was
no
t si
gnifi
cant
ly
∞
- 4
TABLE 7. CORONARY ARTERY DISEASE (ANGINA, ISCHEMIC HEART DISEASE AND MYOCARDIAL INFARCTION) AND FALLS
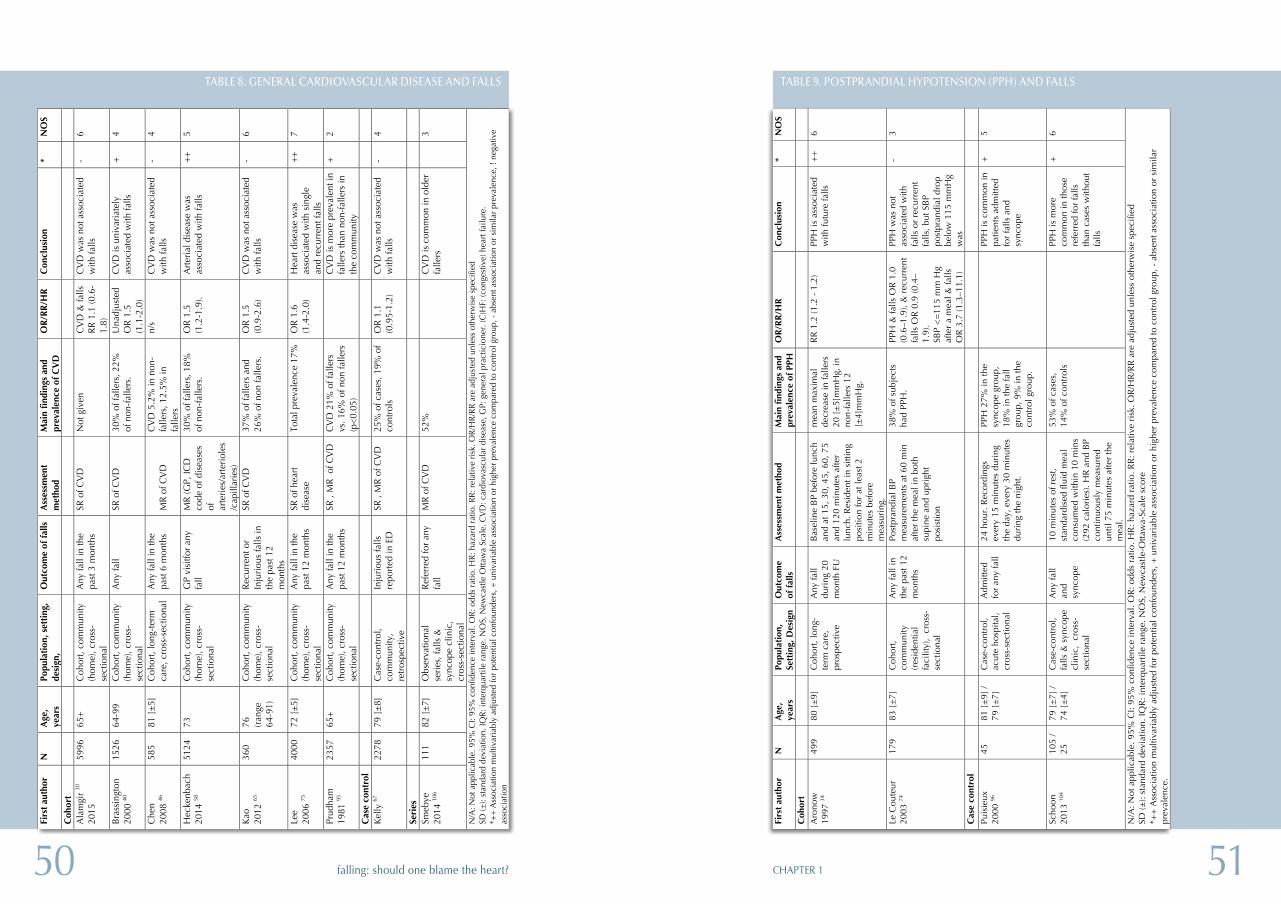
5150 CHAPTER 1falling: should one blame the heart?
Tabl
e 9.
Pos
tpra
ndia
l hyp
oten
sion
(PP
H)
and
falls
Fi
rst
auth
or
N
Age
, ye
ars
Popu
lati
on,
Sett
ing,
Des
ign
Out
com
e of
fal
ls
Ass
essm
ent
met
hod
Mai
n fi
ndin
gs a
nd
prev
alen
ce o
f PP
H
OR
/RR
/HR
C
oncl
usio
n *
NO
S
Coh
ort
A
rono
w
1997
34
499
80 [
±9]
C
ohor
t, lo
ng-
term
car
e,
pros
pect
ive
Any
fall
duri
ng 2
0 m
onth
FU
Bas
elin
e B
P be
fore
lunc
h an
d at
15,
30,
45,
60,
75
and
120
min
utes
afte
r lu
nch.
Res
iden
t in
sitti
ng
posi
tion
for
at le
ast 2
m
inut
es b
efor
e m
easu
ring
.
mea
n m
axim
al
decr
ease
in fa
llers
20
[±
5]m
mH
g, in
no
n-fa
llers
12
[±4]
mm
Hg.
RR
1.2
(1.2
- 1
.2)
PPH
is a
ssoc
iate
d w
ith fu
ture
falls
+
+
6
Le C
oute
ur
2003
74
179
83 [
±7]
C
ohor
t, co
mm
unity
(r
esid
entia
l fa
cilit
y),
cros
s-se
ctio
nal
Any
fall
in
the
past
12
mon
ths
Post
pran
dial
BP
mea
sure
men
ts a
t 60
min
af
ter
the
mea
l in
both
su
pine
and
upr
ight
po
sist
ion
38%
of s
ubje
cts
had
PPH
. PP
H &
falls
OR
1.0
(0
.6–1
.9),
& r
ecur
rent
fa
lls O
R 0
.9 (0
.4–
1.9)
. SB
P <
=11
5 m
m H
g af
ter
a m
eal &
falls
O
R 3
.7 (1
.3–1
1.1)
PPH
was
not
as
soci
ated
with
fa
lls o
r re
curr
ent
falls
, but
SB
P po
stpr
andi
al d
rop
belo
w 1
15 m
mH
g w
as
- 3
Cas
e co
ntro
l
Puis
ieux
20
00 96
45
81
[±
9] /
79 [
±7]
C
ase-
cont
rol,
acut
e ho
spita
l, cr
oss-
sect
iona
l
Adm
itted
fo
r an
y fa
ll 24
hou
r. R
ecor
ding
s ev
ery
15 m
inut
es d
urin
g th
e da
y, e
very
30
min
utes
du
ring
the
nigh
t.
PPH
27%
in th
e sy
ncop
e gr
oup,
18
% in
the
fall
grou
p, 9
% in
the
cont
rol g
roup
.
PP
H is
com
mon
in
patie
nts
adm
itted
fo
r fa
lls a
nd
sync
ope
+
5
Scho
on
2013
104
105
/ 25
79
[±
7] /
74 [
±4]
C
ase-
cont
rol,
falls
& s
ynco
pe
clin
ic,
cros
s-se
ctio
nal
Any
fall
and
sync
ope
10 m
inut
es o
f res
t, st
anda
rdis
ed fl
uid
mea
l co
nsum
ed w
ithin
10
min
s (2
92 c
alor
ies)
. HR
and
BP
cont
inuo
usly
mea
sure
d un
til 7
5 m
inut
es a
fter
the
mea
l.
53%
of c
ases
, 14
% o
f con
trol
s
PPH
is m
ore
com
mon
in th
ose
refe
rred
for
falls
th
an c
ases
with
out
falls
+
6
N/A
: Not
app
licab
le. 9
5% C
I: 95
% c
onfid
ence
inte
rval
. OR
: odd
s ra
tio. H
R: h
azar
d ra
tio. R
R: r
elat
ive
risk
. OR
/HR
/RR
are
adj
uste
d un
less
oth
erw
ise
spec
ified
SD
(±):
stan
dard
dev
iatio
n. IQ
R: i
nter
quar
tile
rang
e. N
OS,
New
cast
le-O
ttaw
a-Sc
ale
scor
e *+
+ A
ssoc
iatio
n m
ultiv
aria
bly
adju
sted
for
pote
ntia
l con
foun
ders
, + u
niva
riab
le a
ssoc
iatio
n or
hig
her
prev
alen
ce c
ompa
red
to c
ontr
ol g
roup
, - a
bsen
t ass
ocia
tion
or s
imila
r pr
eval
ence
.
TABLE 9. POSTPRANDIAL HYPOTENSION (PPH) AND FALLS
Tabl
e 8.
Gen
eral
car
diov
ascu
lar
dise
ase
and
falls
Firs
t aut
hor
N
A
ge,
year
s Po
pula
tion,
set
ting,
de
sign
, O
utco
me
of fa
lls
Ass
essm
ent
met
hod
Mai
n fin
ding
s an
d pr
eval
ence
of C
VD
O
R/RR
/HR
C
oncl
usio
n *
NO
S
Coh
ort
Ala
mgi
r 30
20
15
5996
65
+ C
ohor
t, co
mm
unity
(h
ome)
, cro
ss-
sect
iona
l
Any
fall
in th
e pa
st 3
mon
ths
SR o
f CV
D
Not
giv
en
CV
D &
falls
R
R 1
.1 (0
.6-
1.8)
CV
D w
as n
ot a
ssoc
iate
d w
ith fa
lls
-
6
Bra
ssin
gton
20
00 40
15
26
64-9
9 C
ohor
t, co
mm
unity
(h
ome)
, cro
ss-
sect
iona
l
Any
fall
SR o
f CV
D
30%
of f
alle
rs, 2
2%
of n
on-f
alle
rs.
Una
djus
ted
OR
1.5
(1
.1-2
.0)
CV
D is
uni
vari
atel
y as
soci
ated
with
falls
+
4
Che
n 20
08 46
58
5 81
[±5
] C
ohor
t, lo
ng-t
erm
ca
re, c
ross
-sec
tiona
l A
ny fa
ll in
the
past
6 m
onth
s M
R o
f CV
D
CV
D 5
.2%
in n
on-
falle
rs, 1
2.5%
in
falle
rs
n/s
CV
D w
as n
ot a
ssoc
iate
d w
ith fa
lls
- 4
Hec
kenb
ach
2014
58
5124
73
C
ohor
t, co
mm
unity
(h
ome)
, cro
ss-
sect
iona
l
GP
visi
tfor
any
fall
MR
(GP,
ICD
co
de o
f dis
ease
s of
ar
teri
es/a
rter
iole
s/c
apill
arie
s)
30%
of f
alle
rs, 1
8%
of n
on-f
alle
rs.
OR
1.5
(1
.2-1
.9).
Art
eria
l dis
ease
was
as
soci
ated
with
falls
++
5
Kao
20
12 65
36
0 76
(r
ange
64
-91)
Coh
ort,
com
mun
ity
(hom
e), c
ross
-se
ctio
nal
Rec
urre
nt o
r In
juri
ous
falls
in
the
past
12
mon
ths
SR o
f CV
D
37%
of f
alle
rs a
nd
26%
of n
on fa
llers
. O
R 1
.5
(0.9
-2.6
) C
VD
was
not
ass
ocia
ted
with
falls
-
6
Lee
2006
75
4000
72
[±5
] C
ohor
t, co
mm
unity
(h
ome)
, cro
ss-
sect
iona
l
Any
fall
in th
e pa
st 1
2 m
onth
s SR
of h
eart
di
seas
e To
tal p
reva
lenc
e 17
%
OR
1.6
(1
.4-2
.0)
Hea
rt d
isea
se w
as
asso
ciat
ed w
ith s
ingl
e an
d re
curr
ent f
alls
++
7
Prud
ham
19
81 95
23
57
65+
Coh
ort,
com
mun
ity
(hom
e), c
ross
-se
ctio
nal
Any
fall
in th
e pa
st 1
2 m
onth
s SR
, M
R o
f CV
D
CV
D 2
1% o
f fal
lers
vs
. 16%
of n
on fa
llers
(p
<0.0
5)
C
VD
is m
ore
prev
alen
t in
falle
rs th
an n
on-f
alle
rs in
th
e co
mm
unity
+ 2
Cas
e co
ntro
l
K
elly
67
2278
79
[±8
] C
ase-
cont
rol,
com
mun
ity,
retr
ospe
ctiv
e
Inju
riou
s fa
lls
repo
rted
in E
D
SR ,
MR
of C
VD
25
% o
f cas
es, 1
9% o
f co
ntro
ls
OR
1.1
(0
.95-
1.2)
C
VD
was
not
ass
ocia
ted
with
falls
-
4
Seri
es
Smeb
ye
2014
106
111
82 [
±7]
Obs
erva
tiona
l se
ries
, fal
ls &
sy
ncop
e cl
inic
, cr
oss-
sect
iona
l
Ref
erre
d fo
r an
y fa
ll M
R o
f CV
D
52%
CV
D is
com
mon
in o
lder
fa
llers
3
N/A
: Not
app
licab
le. 9
5% C
I: 95
% c
onfid
ence
inte
rval
. OR
: odd
s ra
tio. H
R: h
azar
d ra
tio. R
R: r
elat
ive
risk.
OR
/HR
/RR
are
adj
uste
d un
less
oth
erw
ise
spec
ified
SD
(±):
stan
dard
dev
iatio
n. IQ
R: i
nter
quar
tile
rang
e. N
OS,
New
cast
le O
ttaw
a Sc
ale.
CV
D: c
ardi
ovas
cula
r di
seas
e, G
P: g
ener
al p
ract
icio
ner.
(C)H
F: (c
onge
stiv
e) h
eart
failu
re.
*++
Ass
ocia
tion
mul
tivar
iabl
y ad
just
ed fo
r po
tent
ial c
onfo
unde
rs, +
uni
vari
able
ass
ocia
tion
or h
ighe
r pr
eval
ence
com
pare
d to
con
trol
gro
up, -
abs
ent a
ssoc
iatio
n or
sim
ilar
prev
alen
ce, !
neg
ativ
e as
soci
atio
n
TABLE 8. GENERAL CARDIOVASCULAR DISEASE AND FALLS
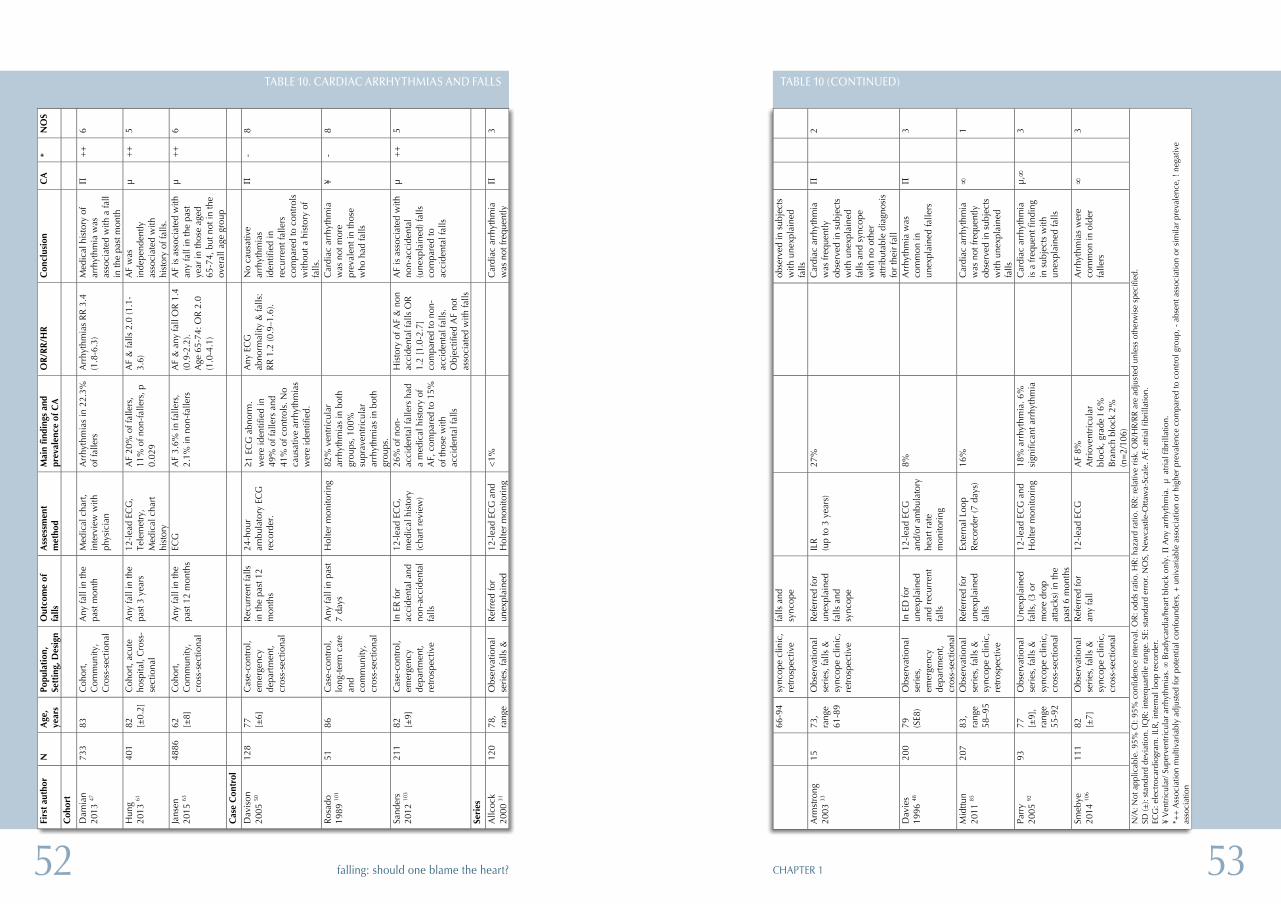
5352 CHAPTER 1falling: should one blame the heart?
66-9
4 sy
ncop
e cl
inic
, re
tros
pect
ive
fa
lls a
nd
sync
ope
obse
rved
in s
ubje
cts
with
une
xpla
ined
fa
lls
Arm
stro
ng
2003
33
15
73,
rang
e 61
-89
Obs
erva
tiona
l se
ries
, fal
ls &
sy
ncop
e cl
inic
, re
tros
pect
ive
Ref
erre
d fo
r un
expl
aine
d fa
lls a
nd
sync
ope
ILR
(u
p to
3 y
ears
) 27
%
C
ardi
ac a
rrhy
thm
ia
was
freq
uent
ly
obse
rved
in s
ubje
cts
with
une
xpla
ined
fa
lls a
nd s
ynco
pe
with
no
othe
r at
trib
utab
le d
iagn
osis
fo
r th
eir
fall
Π
2
Dav
ies
1996
48
200
79
(SE8
) O
bser
vatio
nal
seri
es,
emer
genc
y de
part
men
t, cr
oss-
sect
iona
l
In E
D fo
r un
expl
aine
d an
d re
curr
ent
falls
12-l
ead
ECG
an
d/or
am
bula
tory
he
art r
ate
mon
itori
ng
8%
A
rrhy
thm
ia w
as
com
mon
in
unex
plai
ned
falle
rs
Π
3
Mid
ttun
20
11 85
20
7 83
, ra
nge
58–9
5
Obs
erva
tiona
l se
ries
, fal
ls &
sy
ncop
e cl
inic
, re
tros
pect
ive
Ref
erre
d fo
r un
expl
aine
d fa
lls
Exte
rnal
Loo
p R
ecor
der
(7 d
ays)
16
%
C
ardi
ac a
rrhy
thm
ia
was
not
freq
uent
ly
obse
rved
in s
ubje
cts
with
une
xpla
ined
fa
lls
∞
1
Parr
y 20
05 92
93
77
[±
9],
rang
e 55
-92
Obs
erva
tiona
l se
ries
, fal
ls &
sy
ncop
e cl
inic
, cr
oss-
sect
iona
l
Une
xpla
ined
fa
lls, (
3 or
m
ore
drop
at
tack
s) in
the
past
6 m
onth
s
12-l
ead
ECG
and
H
olte
r m
onito
ring
18
% a
rrhy
thm
ia. 6
%
sign
ifica
nt a
rrhy
thm
ia
C
ardi
ac a
rrhy
thm
ia
is a
freq
uent
find
ing
in s
ubje
cts
with
un
expl
aine
d fa
lls
µ,∞
3
Smeb
ye
2014
106
111
82
[±7]
O
bser
vatio
nal
seri
es, f
alls
&
sync
ope
clin
ic,
cros
s-se
ctio
nal
Ref
erre
d fo
r an
y fa
ll 12
-lea
d EC
G
AF
8%
Atr
iove
ntri
cula
r bl
ock,
gra
de I
6%
Bra
nch
bloc
k 2%
(n
=2/
106)
A
rrhy
thm
ias
wer
e co
mm
on in
old
er
falle
rs
∞
3
N/A
: Not
app
licab
le. 9
5% C
I: 95
% c
onfid
ence
inte
rval
. OR
: odd
s ra
tio. H
R: h
azar
d ra
tio. R
R: r
elat
ive
risk
. OR
/HR
/RR
are
adj
uste
d un
less
oth
erw
ise
spec
ified
. SD
(±):
stan
dard
dev
iatio
n. IQ
R: i
nter
quar
tile
rang
e. S
E: s
tand
ard
erro
r. N
OS,
New
cast
le-O
ttaw
a-Sc
ale.
AF:
atr
ial f
ibri
llatio
n.
ECG
: ele
ctro
card
iogr
am. I
LR, i
nter
nal l
oop
reco
rder
. ¥
Ven
tric
ular
/ Sup
erve
ntri
cula
r ar
rhyt
hmia
s. ∞
Bra
dyca
rdia
/hea
rt b
lock
onl
y. Π
Any
arr
hyth
mia
. µ
atr
ial f
ibri
llatio
n.
*++
Ass
ocia
tion
mul
tivar
iabl
y ad
just
ed fo
r po
tent
ial c
onfo
unde
rs, +
uni
vari
able
ass
ocia
tion
or h
ighe
r pr
eval
ence
com
pare
d to
con
trol
gro
up, -
abs
ent a
ssoc
iatio
n or
sim
ilar
prev
alen
ce, !
neg
ativ
e as
soci
atio
n
TABLE 10 (CONTINUED)
Tabl
e 10
. Car
diac
arr
hyth
mia
s an
d fa
lls
Firs
t au
thor
N
A
ge,
year
s Po
pula
tion
, Se
ttin
g, D
esig
n O
utco
me
of
falls
A
sses
smen
t m
etho
d M
ain
findi
ngs
and
prev
alen
ce o
f CA
O
R/R
R/H
R
Con
clus
ion
CA
*
NO
S
Coh
ort
Dam
ian
2013
47
733
83
Coh
ort,
Com
mun
ity,
Cro
ss-s
ectio
nal
Any
fall
in th
e pa
st m
onth
M
edic
al c
hart
, in
terv
iew
with
ph
ysic
ian
Arr
hyth
mia
s in
22.
3%
of fa
llers
A
rrhy
thm
ias
RR
3.4
(1
.8-6
.3)
Med
ical
his
tory
of
arrh
ythm
ia w
as
asso
ciat
ed w
ith a
fall
in th
e pa
st m
onth
Π
++
6
Hun
g 20
13 61
40
1 82
[±
0.2]
C
ohor
t, ac
ute
hosp
ital,
Cro
ss-
sect
iona
l
Any
fall
in th
e pa
st 3
yea
rs
12-l
ead
ECG
, Te
lem
etry
, M
edic
al c
hart
hi
stor
y
AF
20%
of f
alle
rs,
11%
of n
on-f
alle
rs, p
0.
029
AF
& fa
lls 2
.0 (1
.1-
3.6)
A
F w
as
inde
pend
ently
as
soci
ated
with
hi
stor
y of
falls
.
µ +
+
5
Jans
en
2015
63
4886
62
[±
8]
Coh
ort,
Com
mun
ity,
cros
s-se
ctio
nal
Any
fall
in th
e pa
st 1
2 m
onth
s EC
G
AF
3.6%
in fa
llers
, 2.
1% in
non
-fal
lers
A
F &
any
fall
OR
1.4
(0
.9-2
.2).
A
ge 6
5-74
: OR
2.0
(1
.0-4
.1)
AF
is a
ssoc
iate
d w
ith
any
fall
in th
e pa
st
year
in th
ose
aged
65
-74,
but
not
in th
e ov
eral
l age
gro
up
µ +
+
6
Cas
e C
ontr
ol
Dav
ison
20
05 50
12
8 77
[±
6]
Cas
e-co
ntro
l, em
erge
ncy
depa
rtm
ent,
cros
s-se
ctio
nal
Rec
urre
nt fa
lls
in th
e pa
st 1
2 m
onth
s
24-h
our
ambu
lato
ry E
CG
re
cord
er.
≥1 E
CG
abn
orm
. w
ere
iden
tifie
d in
49
% o
f fal
lers
and
41
% o
f con
trol
s. N
o ca
usat
ive
arrh
ythm
ias
wer
e id
entif
ied.
Any
EC
G
abno
rmal
ity &
falls
: R
R 1
.2 (0
.9–1
.6).
No
caus
ativ
e ar
rhyt
hmia
s id
entif
ied
in
recu
rren
t fal
lers
co
mpa
red
to c
ontr
ols
with
out a
his
tory
of
falls
.
Π
- 8
Ros
ado
1989
101
51
86
Cas
e-co
ntro
l, lo
ng-t
erm
car
e an
d co
mm
unity
, cr
oss-
sect
iona
l
Any
fall
in p
ast
7 da
ys
Hol
ter
mon
itori
ng
82%
ven
tric
ular
ar
rhyt
hmia
s in
bot
h gr
oups
, 100
%
supr
aven
tric
ular
ar
rhyt
hmia
s in
bot
h gr
oups
.
C
ardi
ac a
rrhy
thm
ia
was
not
mor
e pr
eval
ent i
n th
ose
who
had
falls
¥ -
8
Sand
ers
20
12 10
3 21
1 82
[±
9]
Cas
e-co
ntro
l, em
erge
ncy
de
part
men
t, re
tros
pect
ive
In E
R fo
r ac
cide
ntal
and
no
n-ac
cide
ntal
fa
lls
12-l
ead
ECG
, m
edic
al h
isto
ry
(cha
rt r
evie
w)
26%
of n
on-
acci
dent
al fa
llers
had
a
med
ical
his
tory
of
AF,
com
pare
d to
15%
of
thos
e w
ith
acci
dent
al fa
lls
His
tory
of A
F &
non
ac
cide
ntal
falls
OR
1.
2 [1
.0-2
.7]
com
pare
d to
non
-ac
cide
ntal
falls
. O
bjec
tifie
d A
F no
t as
soci
ated
with
falls
AF
is a
ssoc
iate
d w
ith
non-
acci
dent
al
(une
xpla
ined
) fal
ls
com
pare
d to
ac
cide
ntal
falls
µ +
+
5
Seri
es
Allc
ock
2000
31
120
78,
rang
e O
bser
vatio
nal
seri
es, f
alls
&
Ref
rred
for
unex
plai
ned
12-l
ead
ECG
and
H
olte
r m
onito
ring
<
1%
C
ardi
ac a
rrhy
thm
ia
was
not
freq
uent
ly
Π
3
TABLE 10. CARDIAC ARRHYTHMIAS AND FALLS
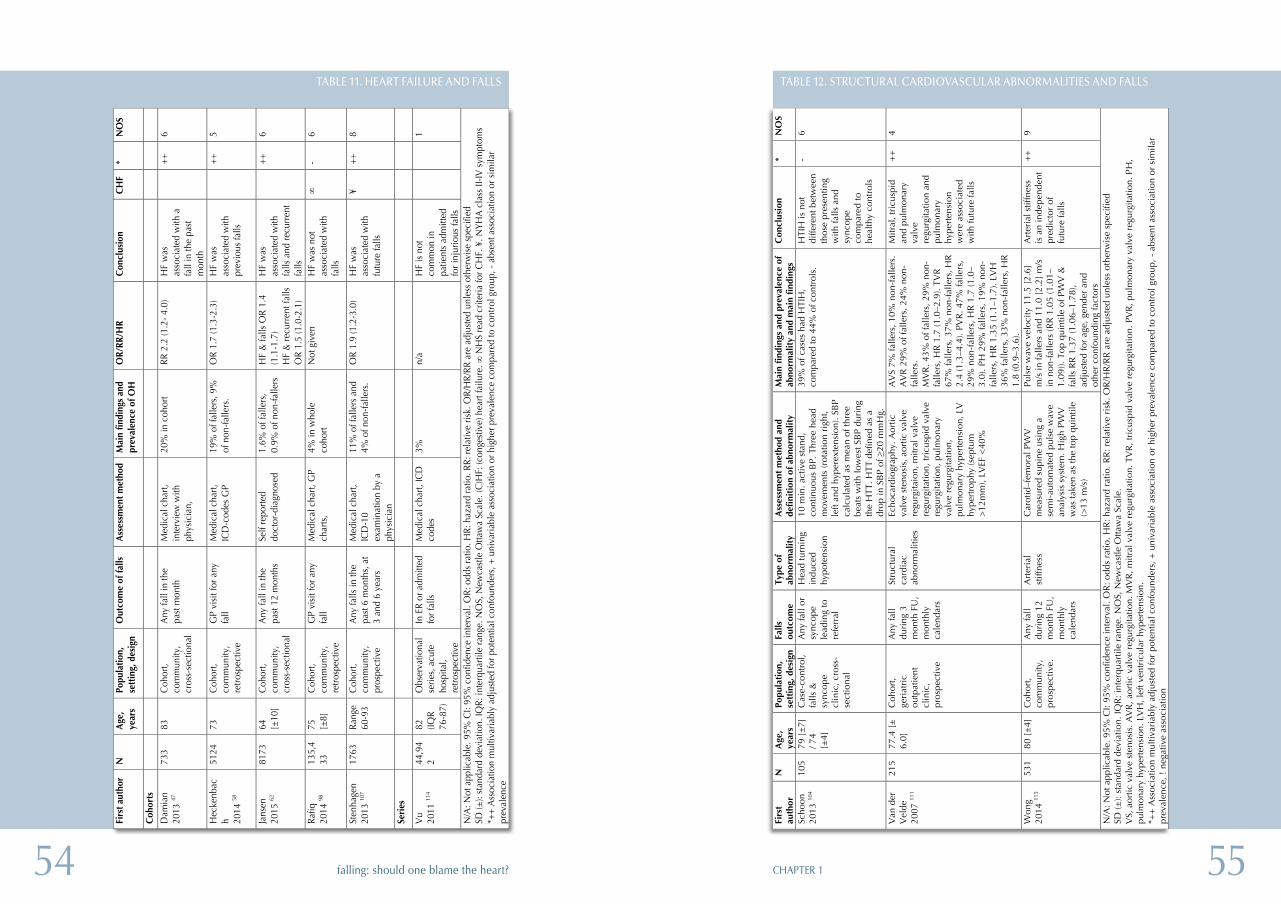
5554 CHAPTER 1falling: should one blame the heart?
Tabl
e 12
. Str
uctu
ral c
ardi
ovas
cula
r ab
norm
alit
ies
and
falls
Fi
rst
auth
or
N
Age
, ye
ars
Popu
lati
on,
sett
ing,
des
ign
Falls
ou
tcom
e Ty
pe o
f ab
norm
alit
y A
sses
smen
t m
etho
d an
d de
fini
tion
of
abno
rmal
ity
Mai
n fi
ndin
gs a
nd p
reva
lenc
e of
ab
norm
alit
y an
d m
ain
find
ings
C
oncl
usio
n *
NO
S
Scho
on
2013
104
105
79 [
±7]
/ 7
4 [±
4]
Cas
e-co
ntro
l, fa
lls &
sy
ncop
e cl
inic
, cro
ss-
sect
iona
l
Any
fall
or
sync
ope
lead
ing
to
refe
rral
Hea
d tu
rnin
g in
duce
d hy
pote
nsio
n
10 m
in. a
ctiv
e st
and,
co
ntin
uous
BP.
Thr
ee h
ead
mov
emen
ts (r
otat
ion
righ
t, le
ft an
d hy
pere
xten
sion
). SB
P ca
lcul
ated
as
mea
n of
thre
e be
ats
with
low
est S
BP
duri
ng
the
HTT
. HTT
def
ined
as
a dr
op in
SB
P of
≥20
mm
Hg.
39%
of c
ases
had
HTI
H,
com
pare
d to
44%
of c
ontr
ols.
H
TIH
is n
ot
diffe
rent
bet
wee
n th
ose
pres
entin
g w
ith fa
lls a
nd
sync
ope
com
pare
d to
he
alth
y co
ntro
ls
- 6
Van
der
V
elde
20
07 11
1
215
77.4
[±
6.
0]
Coh
ort,
geri
atri
c ou
tpat
ient
cl
inic
, pr
ospe
ctiv
e
Any
fall
duri
ng 3
m
onth
FU
, m
onth
ly
cale
ndar
s
Stru
ctur
al
card
iac
abno
rmal
ities
Echo
card
iogr
aphy
. Aor
tic
valv
e st
enos
is, a
ortic
val
ve
regu
rgita
ion,
mitr
al v
alve
re
gurg
itatio
n, tr
icus
pid
valv
e re
gurg
itatio
n, p
ulm
onar
y va
lve
regu
rgita
tion,
pu
lmon
ary
hype
rten
sion
, LV
hy
pert
roph
y (s
eptu
m
>12
mm
), LV
EF <
40%
AV
S 7%
falle
rs, 1
0% n
on-f
alle
rs.
AV
R 2
9% o
f fal
lers
, 24%
non
-fa
llers
. M
VR
. 43%
of f
alle
rs, 2
9% n
on-
falle
rs, H
R 1
.7 (1
.0–2
.9).
TVR
67
% fa
llers
, 37%
non
-fal
lers
, HR
2.
4 (1
.3–4
.4).
PVR
. 47%
falle
rs,
29%
non
-fal
lers
, HR
1.7
(1.0
–3.
0). P
H 2
9% fa
llers
, 19%
non
-fa
llers
, HR
1.3
5 (1
.1–1
.7).
LVH
36
% fa
llers
, 33%
non
-fal
lers
, HR
1.
8 (0
.9–3
.6).
Mitr
al, t
ricu
spid
an
d pu
lmon
ary
valv
e re
gurg
itatio
n an
d pu
lmon
ary
hype
rten
sion
w
ere
asso
ciat
ed
with
futu
re fa
lls
++
4
Won
g 20
14 11
5 53
1 80
[±
4]
Coh
ort,
com
mun
ity,
pros
pect
ive.
Any
fall
duri
ng 1
2 m
onth
FU
, m
onth
ly
cale
ndar
s
Art
eria
l st
iffne
ss
Car
otid
–fem
oral
PW
V
mea
sure
d su
pine
usi
ng a
se
mi-
auto
mat
ed p
ulse
wav
e an
alys
is s
yste
m. H
igh
PWV
w
as ta
ken
as th
e to
p qu
intil
e (>
13 m
/s)
Puls
e w
ave
velo
city
11.
5 [2
.6]
m/s
in fa
llers
and
11.
0 [2
.2]
m/s
in
non
-fal
lers
(RR
1.0
5 (1
.01–
1.09
)). T
op q
uint
ile o
f PW
V &
fa
lls R
R 1
.37
(1.0
6–1.
78),
adju
sted
for
age,
gen
der
and
othe
r co
nfou
ndin
g fa
ctor
s
Art
eria
l stif
fnes
s is
an
inde
pend
ent
pred
icto
r of
fu
ture
falls
++
9
N/A
: Not
app
licab
le. 9
5% C
I: 95
% c
onfid
ence
inte
rval
. OR
: odd
s ra
tio. H
R: h
azar
d ra
tio. R
R: r
elat
ive
risk
. OR
/HR
/RR
are
adj
uste
d un
less
oth
erw
ise
spec
ified
SD
(±):
stan
dard
dev
iatio
n. IQ
R: i
nter
quar
tile
rang
e. N
OS,
New
cast
le O
ttaw
a Sc
ale.
V
S, a
ortic
val
ve s
teno
sis.
AV
R, a
ortic
val
ve r
egur
gita
tion.
MV
R, m
itral
val
ve r
egur
gita
tion.
TV
R, t
ricu
spid
val
ve r
egur
gita
tion.
PV
R, p
ulm
onar
y va
lve
regu
rgita
tion.
PH
, pu
lmon
ary
hype
rten
sion
. LV
H, l
eft v
entr
icul
ar h
yper
tens
ion.
*+
+ A
ssoc
iatio
n m
ultiv
aria
bly
adju
sted
for
pote
ntia
l con
foun
ders
, + u
niva
riab
le a
ssoc
iatio
n or
hig
her
prev
alen
ce c
ompa
red
to c
ontr
ol g
roup
, - a
bsen
t ass
ocia
tion
or s
imila
r pr
eval
ence
, ! n
egat
ive
asso
ciat
ion
TABLE 12. STRUCTURAL CARDIOVASCULAR ABNORMALITIES AND FALLSTa
ble
11. H
eart
failu
re a
nd fa
lls
Firs
t aut
hor
N
Age
, ye
ars
Popu
latio
n,
sett
ing,
des
ign
Out
com
e of
falls
A
sses
smen
t met
hod
Mai
n fin
ding
s an
d pr
eval
ence
of O
H
OR/
RR/H
R C
oncl
usio
n C
HF
* N
OS
Coh
orts
Dam
ian
2013
47
733
83
Coh
ort,
com
mun
ity,
cros
s-se
ctio
nal
Any
fall
in th
e pa
st m
onth
M
edic
al c
hart,
in
terv
iew
with
ph
ysic
ian,
20%
in c
ohor
t RR
2.2
(1.2
- 4.0
) H
F w
as
asso
ciat
ed w
ith a
fa
ll in
the
past
m
onth
++
6
Hec
kenb
ach 20
14 58
5124
73
C
ohor
t, co
mm
unity
, re
trosp
ectiv
e
GP
visi
t for
any
fa
ll M
edic
al c
hart,
IC
D-c
odes
GP
19%
of f
alle
rs, 9
%
of n
on-fa
llers
. O
R 1.
7 (1
.3-2
.3)
HF
was
as
soci
ated
with
pr
evio
us fa
lls
++
5
Jans
en
2015
62
8173
64
[±
10]
Coh
ort,
com
mun
ity,
cros
s-se
ctio
nal
Any
fall
in th
e pa
st 1
2 m
onth
s Se
lf re
porte
d do
ctor
-dia
gnos
ed
1.6%
of f
alle
rs,
0.9%
of n
on-fa
llers
H
F &
falls
OR
1.4
(1.1
-1.7
) H
F &
recu
rren
t fal
ls
OR
1.5
(1.0
-2.1
)
HF
was
as
soci
ated
with
fa
lls a
nd re
curr
ent
falls
++
6
Rafiq
20
14 98
13
5,4
33
75
[±8]
C
ohor
t, co
mm
unity
, re
trosp
ectiv
e
GP
visi
t for
any
fa
ll M
edic
al c
hart,
GP
char
ts,
4% in
who
le
coho
rt N
ot g
iven
H
F w
as n
ot
asso
ciat
ed w
ith
falls
∞
- 6
Sten
hage
n 20
13 10
7 17
63
Rang
e 60
-93
Coh
ort,
com
mun
ity,
pros
pect
ive
Any
falls
in th
e pa
st 6
mon
ths,
at
3 an
d 6
year
s
Med
ical
cha
rt,
ICD
-10
ex
amin
atio
n by
a
phys
icia
n
11%
of f
alle
rs a
nd
4% o
f non
-falle
rs.
OR
1.9
(1.2
-3.0
) H
F w
as
asso
ciat
ed w
ith
futu
re fa
lls
¥ ++
8
Seri
es
Vu
2011
114
44,9
42
82
(IQR
76-8
7)
Obs
erva
tiona
l se
ries,
acu
te
hosp
ital,
retro
spec
tive
In E
R or
adm
itted
fo
r fal
ls
Med
ical
cha
rt, IC
D
code
s 3%
n/
a H
F is
not
co
mm
on in
pa
tient
s ad
mitt
ed
for i
njur
ious
falls
1
N/A
: Not
app
licab
le. 9
5% C
I: 95
% c
onfid
ence
inte
rval
. OR:
odd
s ra
tio. H
R: h
azar
d ra
tio. R
R: re
lativ
e ris
k. O
R/H
R/RR
are
adj
uste
d un
less
oth
erw
ise
spec
ified
SD
(±):
stan
dard
dev
iatio
n. IQ
R: in
terq
uarti
le ra
nge.
NO
S, N
ewca
stle
Otta
wa
Scal
e. (C
)HF:
(con
gest
ive)
hea
rt fa
ilure
. ∞ N
HS
read
crit
eria
for C
HF.
¥. N
YHA
cla
ss II
-IV s
ympt
oms
*++
Ass
ocia
tion
mul
tivar
iabl
y ad
just
ed fo
r pot
entia
l con
foun
ders
, + u
niva
riabl
e as
soci
atio
n or
hig
her p
reva
lenc
e co
mpa
red
to c
ontr
ol g
roup
, - a
bsen
t ass
ocia
tion
or s
imila
r pr
eval
ence
TABLE 11. HEART FAILURE AND FALLS
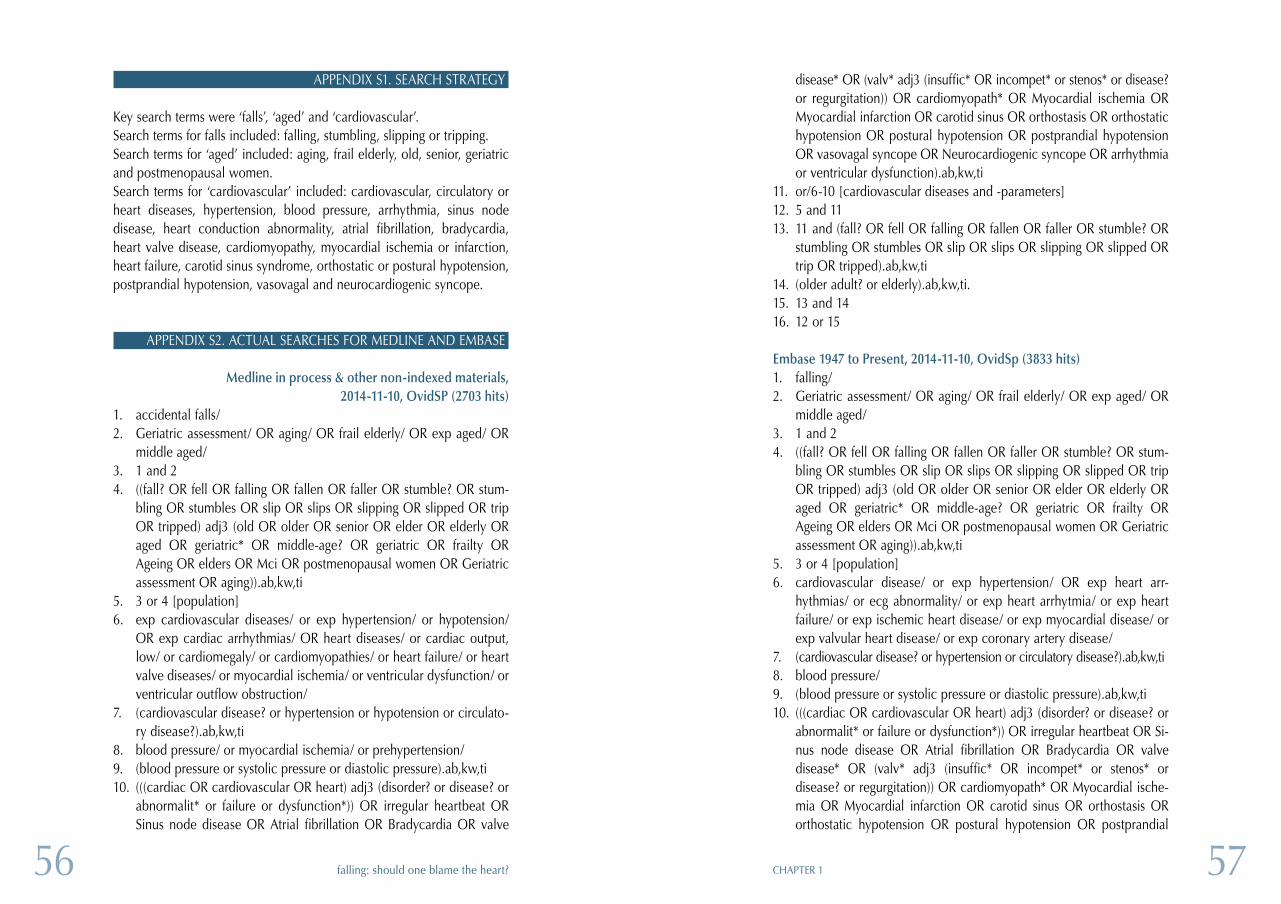
5756 CHAPTER 1falling: should one blame the heart?
APPENDIX S1. SEARCH STRATEGY
Key search terms were ‘falls’, ‘aged’ and ‘cardiovascular’. Search terms for falls included: falling, stumbling, slipping or tripping. Search terms for ‘aged’ included: aging, frail elderly, old, senior, geriatric and postmenopausal women. Search terms for ‘cardiovascular’ included: cardiovascular, circulatory or heart diseases, hypertension, blood pressure, arrhythmia, sinus node disease, heart conduction abnormality, atrial fibrillation, bradycardia, heart valve disease, cardiomyopathy, myocardial ischemia or infarction, heart failure, carotid sinus syndrome, orthostatic or postural hypotension, postprandial hypotension, vasovagal and neurocardiogenic syncope.
APPENDIX S2. ACTUAL SEARCHES FOR MEDLINE AND EMBASE
Medline in process & other non-indexed materials, 2014-11-10, OvidSP (2703 hits)
1. accidental falls/2. Geriatric assessment/ OR aging/ OR frail elderly/ OR exp aged/ OR
middle aged/3. 1 and 24. ((fall? OR fell OR falling OR fallen OR faller OR stumble? OR stum-
bling OR stumbles OR slip OR slips OR slipping OR slipped OR trip OR tripped) adj3 (old OR older OR senior OR elder OR elderly OR aged OR geriatric* OR middle-age? OR geriatric OR frailty OR Ageing OR elders OR Mci OR postmenopausal women OR Geriatric assessment OR aging)).ab,kw,ti
5. 3 or 4 [population]6. exp cardiovascular diseases/ or exp hypertension/ or hypotension/
OR exp cardiac arrhythmias/ OR heart diseases/ or cardiac output, low/ or cardiomegaly/ or cardiomyopathies/ or heart failure/ or heart valve diseases/ or myocardial ischemia/ or ventricular dysfunction/ or ventricular outflow obstruction/
7. (cardiovascular disease? or hypertension or hypotension or circulato-ry disease?).ab,kw,ti
8. blood pressure/ or myocardial ischemia/ or prehypertension/9. (blood pressure or systolic pressure or diastolic pressure).ab,kw,ti10. (((cardiac OR cardiovascular OR heart) adj3 (disorder? or disease? or
abnormalit* or failure or dysfunction*)) OR irregular heartbeat OR Sinus node disease OR Atrial fibrillation OR Bradycardia OR valve
disease* OR (valv* adj3 (insuffic* OR incompet* or stenos* or disease? or regurgitation)) OR cardiomyopath* OR Myocardial ischemia OR Myocardial infarction OR carotid sinus OR orthostasis OR orthostatic hypotension OR postural hypotension OR postprandial hypotension OR vasovagal syncope OR Neurocardiogenic syncope OR arrhythmia or ventricular dysfunction).ab,kw,ti
11. or/6-10 [cardiovascular diseases and -parameters]12. 5 and 1113. 11 and (fall? OR fell OR falling OR fallen OR faller OR stumble? OR
stumbling OR stumbles OR slip OR slips OR slipping OR slipped OR trip OR tripped).ab,kw,ti
14. (older adult? or elderly).ab,kw,ti.15. 13 and 1416. 12 or 15
Embase 1947 to Present, 2014-11-10, OvidSp (3833 hits)1. falling/2. Geriatric assessment/ OR aging/ OR frail elderly/ OR exp aged/ OR
middle aged/3. 1 and 24. ((fall? OR fell OR falling OR fallen OR faller OR stumble? OR stum-
bling OR stumbles OR slip OR slips OR slipping OR slipped OR trip OR tripped) adj3 (old OR older OR senior OR elder OR elderly OR aged OR geriatric* OR middle-age? OR geriatric OR frailty OR Ageing OR elders OR Mci OR postmenopausal women OR Geriatric assessment OR aging)).ab,kw,ti
5. 3 or 4 [population]6. cardiovascular disease/ or exp hypertension/ OR exp heart arr-
hythmias/ or ecg abnormality/ or exp heart arrhytmia/ or exp heart failure/ or exp ischemic heart disease/ or exp myocardial disease/ or exp valvular heart disease/ or exp coronary artery disease/
7. (cardiovascular disease? or hypertension or circulatory disease?).ab,kw,ti8. blood pressure/9. (blood pressure or systolic pressure or diastolic pressure).ab,kw,ti10. (((cardiac OR cardiovascular OR heart) adj3 (disorder? or disease? or
abnormalit* or failure or dysfunction*)) OR irregular heartbeat OR Si-nus node disease OR Atrial fibrillation OR Bradycardia OR valve disease* OR (valv* adj3 (insuffic* OR incompet* or stenos* or disease? or regurgitation)) OR cardiomyopath* OR Myocardial ische-mia OR Myocardial infarction OR carotid sinus OR orthostasis OR orthostatic hypotension OR postural hypotension OR postprandial
5958 CHAPTER 1falling: should one blame the heart?
hypotension OR vasovagal syncope OR Neurocardiogenic syncope OR arrhythmia or ventricular dysfunction).ab,kw,ti
11. or/6-10 [cardiovascular diseases and -parameters]12. 5 and 1113. 11 and (fall? OR fell OR falling OR fallen OR faller OR stumble? OR
stumbling OR stumbles OR slip OR slips OR slipping OR slipped OR trip OR tripped).ab,kw,ti
14. (older adult? or elderly).ab,kw,ti.15. 13 and 1416. 12 or 15
APPENDIX S3. QUALITY ASSESSMENT
Quality of included studies was assessed by the same reviewers. Because of the variety of nonrandomized study designs included, the Newcastle-Ottawa Scale (NOS) was used to evaluate risk of bias in the case control-led and cohort studies [1]. The scale was adjusted to allow for appropri-ate quality assessment of falls. As prospective reporting of falls through calendars or diaries is considered the gold standard for falls reporting, studies using this method were allotted two stars. All other types of falls reporting were allotted one star. A score of 0-3 was considered low qua-lity, 4-6 intermediate and 7 or above high qualityCohort studies could be allotted a maximum of eleven stars and case con-trol studies could be allotted a maximum of nine stars. As observational series were also included in our review, the NOS for case-control studies was used, omitting the items on comparability and selection and ascer-tainment of controls, allowing a maximum of three stars for these studies.
QUALITY REVIEW FOR- CASE-CONTROL STUDIES OR OBSERVATIONAL SERIES
SelectionIs the case definition adequate?
Requires some independent validation (e.g. >1 person/record/time/pro-cess to extract information, or reference to primary record source such as medical/hospital records).• Yes, with independent validation *• Yes, with record linkage (e.g. ICD codes in database) or self-report• No description
Representativeness of the casesAll eligible cases with outcome of interest over a defined period of time, all cases in a defined catchment area, all cases in a defined hospital or clinic, group of hospitals, health maintenance organisation, or an appro-priate sample of those cases (e.g. random sample)• Consecutive or obviously representative series of cases *• Not satisfying requirements or not stated.
Selection of Controls (n/a for obs series)This item assesses whether the control series used in the study is derived from the same population as the cases and essentially would have been cases had the outcome been present.• community controls * (i.e. same community as cases and would be
cases if had outcome)• Hospital controls, within same community as cases (i.e. not another
city) but from a hospitalised population• No description
Definition of controls (n/a for obs series)If cases are first occurrence of outcome, then it must explicitly state that controls have no history of this outcome. If cases have new (not necessa-rily first) occurrence of outcome, then controls with previous occurrences of outcome of interest should not be excluded.• no history of disease (endpoint) *• no mention of history of outcome• N/A
ComparabilityComparability of cases and controls on the basis of the design or analysis (n/a for obs series)Either cases and controls must be matched in the design and/or confoun-ders must be adjusted for in the analysis. Statements of no differences between groups or that differences were not statistically significant are not sufficient for establishing comparability. Note: If the odds ratio for the expo- sure of interest is adjusted for the confounders listed, then the groups will be considered to be comparable on each variable used in the adjustment.• Controlled for age and/or gender *• Controlled for other factors *• no desciption
6160 CHAPTER 1falling: should one blame the heart?
Exposure Ascertainment of exposure (risk factor)
• secure record (cardiovascular assessment) *• structured interview where blind to case/control status *• interview not blinded to case/control status• written self report or medical record only• no description
Same method of ascertainment for cases and controls (n/a for obs series)• yes *• no
Non-response rate (n/a for obs series)• same rate for both groups *• non respondents described• rate different and no designation• no description
QUALITY REVIEW FOR COHORT STUDIES
SelectionRepresentativeness of the exposed cohort
• truly representative of the average older persons in the community *• somewhat representative of the average older persons in the
community *• selected group of users eg volunteers• no description of the derivation of the cohort
Selection of the non exposed cohort• drawn from the same community as the exposed cohort *• drawn from a different source• no description of the derivation of the non exposed cohort
Ascertainment of exposure (cohort)• Some form of independent validation (e.g. cardiovascular assessment) *• structured interview *• written self report or medical record only• no description
Demonstration that outcome of interest was not present at start of studyyes *no
ComparabilityComparability of cohorts on the basis of the design or analysisEither exposed and non-exposed individuals must be matched in the de-sign and/or confounders must be adjusted for in the analysis. Statements of no differences between groups or that differences were not statistically significant are not sufficient for establishing comparability. Note: If the relative risk for the exposure of interest is adjusted for the confounders listed, then the groups will be considered to be comparable on each vari-able used in the adjustment.• Controlled for age and/or gender *• Controlled for other factors *• No description
OutcomeAssessment of outcome• Prospective self-report through fall calenders **• Incident report (e.g. in nursing homes) *• Medical record (e.g. patient with fall-related injury in ED) *• Retrospective self report• No description
Was follow-up long enough for outcomes to occur (N/A for cross-sectional studies)?• yes (six months or more) *• no
Adequacy of follow up of cohorts (N/A for cross-sectional studies)• complete follow up - all subjects accounted for *• subjects lost to follow up unlikely to introduce bias - small number lost *• subjects lost to follow up likely to introduce bias• No description
Reference1. Wells G, Shea B, O’connell D, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analy-ses, 2000.
6362 CHAPTER 1falling: should one blame the heart?
22. Fried TR, O’Leary J, Towle V, Goldstein MK, Tren-talange M, Martin DK. Health outcomes associated with polypharmacy in community-dwelling older adults: a syste-matic review. J Am Geriatr Soc. 2014;62(12):2261-72.
23. van der Velde N, Stricker BHC, Pols HAP, van der Cam-men TJM. Risk of falls after wit-hdrawal of fall-risk-increasing drugs: a prospective cohort study. Br J Clin Pharmacol. 2007;63(2):232-7.
24. van der Velde N, van den Meiracker AH, Pols HA, Stricker BH, van der Cammen TJ. Wit-hdrawal of fall-risk-increasing drugs in older persons: effect on tilt-table test outcomes. J Am Geriatr Soc. 55. United States2007. p. 734-9.
25. Moya A, Sutton R, Am-mirati F, Blanc JJ, Brignole M, Dahm JB, et al. Guidelines for the diagnosis and management of syncope (version 2009). Eur Heart J. 2009;30(21):2631-71.
26. Gillespie LD, Robertson MC, Gillespie WJ, Sherrington C, Gates S, Clemson LM, et al. Interventions for preventing falls in older people living in the community. Cochrane Database Syst Rev. 2012;9:Cd007146.
27. Parry SW, Steen IN, Baptist M, Kenny RA. Amnesia for loss of consciousness in carotid sinus syndrome: implications for presentation with falls. J Am Coll Cardiol. 2005;45(11):1840-3.
28. Kenny RA, Richardson DA, Steen N, Bexton RS, Shaw FE, Bond J. Carotid sinus syndrome: a modifiable risk factor for no-naccidental falls in older adults (SAFE PACE). J Am Coll Cardiol. 2001;38(5):1491-6.
29. Solari D, Maggi R, Oddone D, Solano A, Croci F, Donateo P, et al. Clinical context and outcome of carotid sinus syn-drome diagnosed by means of the ‘method of symptoms’. Eu-ropace. 2014;16(6):928-34.
30. Alamgir H, Wong NJ, Hu Y, Yu M, Marshall A, Yu S. Epidemiology of falls in older adults in Texas. South Med J. 2015;108(2):119-24.
31. Allcock LM, O’Shea D. Di-agnostic yield and development of a neurocardiovascular inves-tigation unit for older adults in a district hospital. Journals of Gerontology Series A-Biological Sciences & Medical Sciences. 2000;55(8):M458-62.
32. Anpalahan M, Gibson S. The prevalence of Neurally Me-diated Syncope in older patients presenting with unexplained falls. European Journal of Inter-nal Medicine. 2012;23(2):e48-52.
33. Armstrong VL, Lawson J, Kamper AM, Newton J, Kenny RA. The use of an implantable loop recorder in the investiga-tion of unexplained syncope in older people. Age & Ageing. 2003;32(2):185-8.
34. Aronow WS, Ahn C. Association of postprandial hypotension with incidence of falls, syncope, coronary events, stroke, and total mortality at 29-month follow-up in 499 older nursing home residents. Journal of the American Geriatrics Soci-ety. 1997;45(9):1051-3.
35. Assantachai P, Chat-thanawaree W, Thamlikitkul V, Praditsuwan R, Pisalsarakij D. Risk factors for falls in the Thai elderly in an urban com-munity. Journal of the Medical Association of Thailand. 2003;86(2):124-30.
36. Benchimol M, Oliveira-Souza R. Diagnostic relevance of the carotid sinus massage during a head up tilt table test (HUTT). Arquivos Brasileiros de Cardiologia. 2008;90(4):264-7.
37. Berg WP, Alessio HM, Mills EM, Tong C. Correlates of recurrent falling in independent community-dwelling older adults. Journal of Motor Behavior. 1997;29(1):5-16.
38. Bergland A, Jarnlo GB, Laake K. Predictors of falls in the elderly by location. Aging-Cli-nical & Experimental Research. 2003;15(1):43-50.
39. Boddaert J, Tamim H, Ver-ny M, Belmin J. Arterial stiffness is associated with orthostatic hypotension in elderly subjects with history of falls. Journal of the American Geriatrics Society. 2004;52(4):568-72.
40. Brassington GS, King AC, Bliwise DL. Sleep problems as a risk factor for falls in a sample of community-dwelling adults aged 64-99 years. Journal of the American Geriatrics Society. 2000;48(10):1234-40.
41. Bumin G, Uyanik M, Aki E, Kayihan H. An investigation of risk factors for falls in elderly people in a Turkish rest home: A pilot study. Aging - Clinical and Experimental Research. 2002;14(3):192-6.
1. Centers for Disease Control and Prevention NCfIPaC. Web–based Injury Statistics Query and Reporting System (WIS-QARS) 2013 [May 8, 2015]. Available from: http://www.cdc.gov/injury/wisqars/.
2. Tinetti ME, Williams CS. Falls, injuries due to falls, and the risk of admission to a nursing home. N Engl J Med. 1997;337(18):1279-84.
3. CDC - Falls Among Older Adults: An Overview - Home and Recreational Safety - Injury Center 2014. Available from: http://www.cdc.gov/home-andrecreationalsafety/falls/adultfalls.html.
4. Hartholt KA, Polinder S, Van der Cammen TJM, Panneman MJM, Van der Velde N, Van Lieshout EMM, et al. Costs of falls in an ageing population: A nationwide study from the Ne-therlands (2007–200 9). Injury. 2012;43(7):1199-203.
5. Tinetti ME, Speechley M. Prevention of falls among the elderly. N Engl J Med. 1989;320(16):1055-9. 6. Summary of the Updated American Geriatrics Society/British Geriatrics Society cli-nical practice guideline for prevention of falls in older persons. J Am Geriatr Soc. 2011;59(1):148-57.
7. Soteriades ES, Evans JC, Larson MG, Chen MH, Chen L, Benjamin EJ, et al. Incidence and prognosis of syncope. N Engl J Med. 2002;347(12):878-85.
8. Kenny RA, Bhangu J, King-Kallimanis BL. Epidemiology of syncope/collapse in younger and older Western patient po-
pulations. Prog Cardiovasc Dis. 2013;55(4):357-63.
9. McCarthy F, Fan CW, Kearney PM, Walsh C, Kenny RA. What is the evidence for cardiovascular disorders as a risk factor for non-syncopal falls? Scope for future research. European Geriatric Medi-cine.1(4):244-51.
10. Shaw BH, Claydon VE. The relationship between orthosta-tic hypotension and falling in older adults. Clin Auton Res. 2014;24(1):3-13.
11. Angelousi A, Girerd N, Benetos A, Frimat L, Gautier S, Weryha G, et al. Association between orthostatic hypoten-sion and cardiovascular risk, cerebrovascular risk, cognitive decline and falls as well as overall mortality: a systematic review and meta-analysis. J Hypertens. 014;32(8):1562-71; discussion 71.
12. Liberati A, Altman DG, Tet-zlaff J, Mulrow C, Gotzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of stu-dies that evaluate healthcare in-terventions: explanation and ela-boration. BMJ. 2009;339:b2700.
13. Wells G, Shea B, O’connell D, Peterson J, Welch V, Losos M, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised stu-dies in meta-analyses. 2000.
14. Kennelly S, Collins O. Wal-king the cognitive ”minefield” between high and low blood pressure. J Alzheimers Dis. 012;32(3):609-21.
15. Ryan DJ, Kenny RA, Chris-tensen S, Meaney JF, Fagan AJ, Harbison J. Ischaemic stroke or TIA in older subjects associated with impaired dynamic blood pressure control in the absence of severe large artery stenosis. Age Ageing. 2015.
16. Ryan DJ, Harbison JA, Meaney JF, Rice CP, King-Kal-limanis B, Kenny RA. Syncope causes transient focal neurologi-cal symptoms. QJM. 2015.
17. Mossello E, Pieraccioli M, Nesti N, Bulgaresi M, Lorenzi C, Caleri V, et al. Effects of Low Blood Pressure in Cognitively Impaired Elderly Patients Tre-ated With Antihypertensive Drugs. JAMA Intern Med. 2015.
18. Muller M, Sigurdsson S, Kjartansson O, Aspelund T, Lopez OL, Jonnson PV, et al. Joint effect of mid- and late-life blood pressure on the brain: the AGES-Reykjavik study. Neuro-logy. 2014;82(24):2187-95.
19. Muller M, Smulders YM, de Leeuw PW, Stehouwer CD. Treatment of hypertension in the oldest old: a critical role for frailty? Hypertension. 2014;63(3):433-41.
20. Finucane C, O’Connell MD, Fan CW, Savva GM, Sorag-han CJ, Nolan H, et al. Age-rela-ted normative changes in phasic orthostatic blood pressure in a large population study: findings from The Irish Longitudinal Study on Ageing (TILDA). Circu-lation. 2014;130(20):1780-9.
21. Singh M, Stewart R, White H. Importance of frailty in patients with cardiovas-cular disease. Eur Heart J. 2014;35(26):1726-31.
REFERENCES
6564 CHAPTER 1falling: should one blame the heart?
63. Jansen S, Frewen J, Finuca-ne C, de Rooij SE, van der Velde N, Kenny RA. AF is associated with self-reported syncope and falls in a general population cohort. Age Ageing. 2015.
64. Jitapunkul S, Songkhla MN, Chayovan N, Chirawatkul A, Choprapawon C, Kachond-ham Y, et al. Falls and their as-sociated factors: a national sur-vey of the Thai elderly. Journal of the Medical Association of Thailand. 1998;81(4):233-42.
65. Kao S, Wang YC, Tzeng YM, Liang CK, Lin FG. In-teractive effect between depression and chronic me-dical conditions on fall risk in community-dwelling elders. International Psychogeriatrics. 2012;24(9):1409-18.
66. Kario K, Tobin JN, Wolfson LI, Whipple R, Derby CA, Singh D, et al. Lower standing systolic blood pressure as a predictor of falls in the elderly: a community-based prospective study. Journal of the American College of Car-diology. 2001;38(1):246-52.
67. Kelly KD, Pickett W, Yiannakoulas N, Rowe BH, Schopflocher DP, Svenson L, et al. Medication use and falls in community-dwelling older persons. Age and Ageing. 2003;32(5):503-9.
68. Kenny RA, Traynor G. Carotid sinus syndrome--clinical characteristics in elderly patients. Age & Ageing. 1991;20(6):449-54.
69. Klein D, Nagel G, Kleiner A, Ulmer H, Rehberger B, Concin H, et al. Blood pressure and falls in community-dwelling people aged 60 years and older in the VHM&PP cohort. BMC Geriatrics. 2013;13:50.
70. Kumar NP, Thomas A, Mudd P, Morris RO, Masud T. The usefulness of carotid sinus massage in different patient groups. Age & Ageing. 2003;32(6):666-9.
71. Lacerda Gde C, Pedrosa RC, Lacerda RC, Santos MC, Perez Mde A, Teixeira AB, et al. Cardioinhibitory carotid sinus hypersensitivity: prevalence and predictors in 502 outpatients. Arquivos Brasileiros de Cardio-logia. 2008;90(3):148-55.
72. Lagro J, Meel-van den Abeelen A, de Jong DL, Schalk BW, Olde Rikkert MG, Claas-sen JA. Geriatric hypotensive syndromes are not explained by cardiovascular autonomic dysfunction alone. Journals of Gerontology Series A-Biological Sciences & Medical Sciences. 2013;68(5):581-9.
73. Lawlor DA, Patel R, Ebra-him S. Association between falls in elderly women and chronic diseases and drug use: cross sectional study. BMJ. 2003;327(7417):712-7.
74. Le Couteur DG, Fisher AA, Davis MW, McLean AJ. Post-prandial systolic blood pressure responses of older people in residential care: association with risk of falling. Gerontology. 2003;49(4):260-4.
75. Lee JSW, Kwok T, Leung PC, Woo J. Medical illnesses are more important than medi-cations as risk factors of falls in older community dwellers? A cross-sectional study. Age and Ageing. 2006;35(3):246-51.
76. Lee PG, Cigolle C, Blaum C. The co-occurrence of chronic diseases and geriatric syndromes: the health and retirement study. Journal of the American Geriatrics Society. 2009;57(3):511-6.
77. Liao KC, Pu SJ, Lin CH, Chang HJ, Chen YJ, Liu MS. Association between the meta-bolic syndrome and its compo-nents with falls in community-dwelling older adults. Metabolic Syndrome & Related Disorders. 2012;10(6):447-51.
78. Lipsitz LA, Jonsson PV, Kelley MM, Koestner JS. Causes and correlates of recurrent falls in ambulatory frail el-derly. Journal of Gerontology. 1991;46(4):M114-22.
79. Liu BA, Topper AK, Reeves RA, Gryfe C, Maki BE. Falls among older people: relation-ship to medication use and or-thostatic hypotension. Journal of the American Geriatrics Society. 1995;43(10):1141-5.
80. Luukinen H, Koski K, Kivela SL, Laippala P. Social sta-
tus, life changes, housing condi-tions, health, functional abilities and life-style as risk factors for recurrent falls among the home-dwelling elderly. Public Health. 1996;110(2):115-8.
81. Mader SL, Josephson KR, Rubenstein LZ. Low prevalence of postural hypotension among community-dwelling elderly. JAMA. 1987;258(11):1511-4.
82. Marechaux S, Lubret R, Delsart P, Hattabi M, Six-Car-pentier MM, Carpentier E, et al. Clinical significance of unsus-pected rise in cardiac troponin in the setting of falls in older people. Emergency Medicine Journal. 2010;27(6):446-50.
83. Maurer MS, Cohen S, Cheng H. The degree and timing of orthostatic blood pressure changes in relation to falls in nursing home resi-dents. Journal of the American Medical Directors Association. 2004;5(4):233-8.
42. Campbell AJ, Reinken J, Allan BC, Martinez GS. Falls in old age: a study of frequency and related clinical factors. Age & Ageing. 1981;10(4):264-70.
43. Campbell AJ, Borrie MJ, Spears GF. Risk factors for falls in a community-based prospec-tive study of people 70 years and older. Journal of Geronto-logy. 1989;44(4):M112-7.
44. Chan KM, Pang WS, Ee CH, Ding YY, Choo P. Epide-miology of falls among the elderly community dwellers in Singapore. Singapore Medical Journal. 1997;38(10):427-31.
45. Chang NT, Yang NP, Chou P. Incidence, risk factors and consequences of falling injuries among the community-dwelling elderly in Shihpai, Taiwan. Aging-Clinical & Experimental Research. 2010;22(1):70-7.
46. Chen YM, Hwang SJ, Chen LK, Chen DY, Lan CF. Risk fac-tors for falls among elderly men in a veterans home. Journal of the Chinese Medical Associa-tion: JCMA. 2008;71(4):180-5.
47. Damian J, Pastor-Barriuso R, Valderrama-Gama E, de Pe-dro-Cuesta J. Factors associated with falls among older adults living in institutions. BMC Geri-atrics. 2013;13:6.
48. Davies AJ, Kenny RA. Falls presenting to the accident and emergency department: types of presentation and risk factor profile. Age & Ageing. 1996;25(5):362-6.
49. Davies AJ, Steen N, Kenny RA. Carotid sinus hypersensiti-vity is common in older patients presenting to an accident and emergency department with un-explained falls. Age & Ageing. 2001;30(4):289-93.
50. Davison J, Brady S, Kenny RA. 24-hour ambulatory elec-trocardiographic monitoring is unhelpful in the investigation of older persons with recurrent falls. Age & Ageing. 2005;34(4):382-6.
51. Dey AB, Stout NR, Kenny RA. Cardiovascular syncope is the most common cause of drop attacks in the elderly. Pacing & Clinical Electrophysiology. 1997;20(3 Pt 2):818-9.
52. Downton JH, Andrews K. Prevalence, characteris-tics and factors associated with falls among the elderly living at home. Aging-Clinical & Experimental Research. 1991;3(3):219-28.
53. Eltrafi A, King D, Silas JH, Currie P, Lye M. Role of carotid sinus syndrome and neurocar-diogenic syncope in recurrent syncope and falls in patients referred to an outpatient clinic in a district general hospital. Postgraduate Medical Journal. 2000;76(897):405-8.
54. Ensrud KE, Nevitt MC, Yunis C, Hulley SB, Grimm RH, Cummings SR. Postural hypotension and postural diz-ziness in elderly women. The study of osteoporotic fractures. The Study of Osteoporotic Fractures Research Group. Archives of Internal Medicine. 1992;152(5):1058-64.
55. Freitas J, Santos R, Azeve-do E, Carvalho M. Carotid sinus syndrome in an unselected po-pulation of eight hundred con-secutive patients with syncope. Prevalence and clinical profile. Revista Portuguesa de Cardiolo-gia. 2004;23(6):835-40.
56. Gangavati A, Hajjar I, Quach L, Jones RN, Kiely DK, Gagnon P, et al. Hypertension, orthostatic hypotension, and the risk of falls in a community-dwelling elderly population: the maintenance of balance, independent living, intellect, and zest in the elderly of Boston stu-dy. Journal of the American Ge-riatrics Society. 011;59(3):383-9.
57. Graafmans WC, Ooms ME, Hofstee HMA, Bezemer PD, Bouter LM, Lips P. Falls in the elderly: A prospective study of risk factors and risk profiles. American Journal of Epidemio-logy. 1996;143(11):1129-36.
58. Heckenbach K, Ostermann T, Schad F, Kroz M, Matthes H. Medication and falls in elderly outpatients: an epidemiological study from a German Pharma-covigilance Network. Springer-plus. 2014;3:483.
59. Heitterachi E, Lord SR, Meyerkort P, McCloskey I, Fitzpatrick R. Blood pressure changes on upright tilting pre-dict falls in older people. Age & Ageing. 2002;31(3):181-6.
60. Herndon JG, Helmick CG, Sattin RW, Stevens JA, De Vito C, Wingo PA. Chronic medical conditions and risk of fall injury events at home in older adults. Journal of the American Geria-trics Society. 1997;45(6):739-43.
61. Hung CY, Wu TJ, Wang KY, Huang JL, Loh EW, Chen YM, et al. Falls and atrial fibrillation in elderly patients. Acta Cardiolo-gica Sinica. 2013;29(5):436-43.
62. Jansen S, Kenny RA, de Rooij SE, van der Velde N. Self-reported cardiovascular conditions are as-sociated with falls and syncope in community-dwelling older adults. Age Ageing. 2015;44(3):525-9.
6766 CHAPTER 1falling: should one blame the heart?
104. Schoon Y, Olde Rik-kert MGM, Rongen S, Lagro J, Schalk B, Claassen JAHR. Head Turning-Induced Hypotension in Elderly People. PLoS ONE. 2013;8(8).
105. Sibley KM, Voth J, Munce SE, Straus SE, Jaglal SB. Chronic disease and falls in community-dwelling Canadians over 65 years old: a population-based study exploring associations with number and pattern of chronic conditions. BMC Geria-trics. 2014;14:22.
106. Smebye KL, Granum S, Wyller TB, Mellingsaeter M. Medical findings in an interdis-ciplinary geriatric outpatient clinic specialising in falls. Tidsskrift for Den Norske Laege-forening. 2014;134(7):705-9.
107. Stenhagen M, Ekstrom H, Nordell E, Elmstahl S. Falls in the general elderly population: a 3- and 6- year prospective study of risk factors using data from the longitudinal population study ‘Good ageing in Skane’. BMC Geriatrics. 2013;13:81.
108. Tan MP, Newton JL, Chadwick TJ, Parry SW. The relationship between carotid sinus hypersensitivity, orthosta-tic hypotension, and vasovagal syncope: A case-control study. Europace. 2008;10(12):1400-5.
109. Tan MP, Newton JL, Reeve P, Murray A, Chadwick TJ, Parry SW. Results of carotid sinus massage in a tertiary referral unit - Is carotid sinus syndrome still relevant? Age and Ageing. 2009;38(6):680-6.
110. Tinetti ME, Williams TF, Mayewski R. Fall risk index for elderly patients based on number of chronic disabilities. American Journal of Medicine. 1986;80(3):429-34.
111. van der Velde N, Stricker BH, Roelandt JR, Ten Cate FJ, van der Cammen TJ. Can echo-cardiographic findings predict falls in older persons? PLoS ONE [Electronic Resource]. 2007;2(7):e654.
112. van der Velde N, van den Meiracker AH, Stricker BH, van der Cammen TJ. Measuring orthostatic hypotension with the Finometer device: is a blood pressure drop of one heartbeat clinically relevant? Blood Pressu-re Monitoring. 2007;12(3):167-71.
113. van Nieuwenhuizen RC, van Dijk N, van Breda FG, Scheffer AC, Korevaar JC, van der Cammen TJ, et al. Assessing the prevalence of modifiable risk factors in older patients visiting an ED due to a fall using the CAREFALL Triage Instrument. American Journal of Emergency Medicine. 2010;28(9):994-1001.
114. Vu T, Finch CF, Day L. Patterns of comorbidity in community-dwelling older peo-ple hospitalised for fall-related injury: a cluster analysis. BMC Geriatrics. 2011;11:45.
115. Wong AKW, Lord SR, Trollor JN, Sturnieks DL, Del-baere K, Menant J, et al. High arterial pulse wave velocity is a risk factor for falls in communi-ty-dwelling older people. Jour-nal of the American Geriatrics Society. 2014;62(8):1534-9.
84. Maurer MS, Burcham J, Cheng H. Diabetes mellitus is associated with an increased risk of falls in elderly residents of a long-term care facility. Journals of Gerontology Series A-Biological Sciences & Medical Sciences. 2005;60(9):1157-62.
85. Midttun M. Diagnosis ef-fectiveness of arrhythmia with R-test electrocardiogram in old fallers. European Geriatric Me-dicine. 2011;2(5):270-2.
86. Milton JC, Lee TC, Jackson SHD. Determinants of a positive response to carotid sinus mas-sage and head-up tilt testing. European Journal of Internal Medicine. 2009;20(7):709-11.
87. Mitchell RJ, Watson WL, Milat A, Chung AZ, Lord S. Health and lifestyle risk factors for falls in a large population-based sample of older people in Australia. Journal of Safety Research. 2013;45:7-13.
88. Murphy AL, Rowbotham BJ, Boyle RS, Thew CM, Far-doulys JA, Wilson K. Carotid sinus hypersensitivity in elderly nursing home patients. Austra-lian & New Zealand Journal of Medicine. 1986;16(1):24-7.
89. Ooi WL, Hossain M, Lipsitz LA. The association between orthostatic hypo-tension and recurrent falls in nursing home residents. Ame-rican Journal of Medicine. 2000;108(2):106-11.
90. Paling D, Vilches-Moraga A, Akram Q, Atkinson O, Staniland J, Paredes-Galan E. Carotid sinus syndrome is com-mon in very elderly patients undergoing tilt table testing and carotid sinus massage because of syncope or unexplained falls. Aging-Clinical & Experimental Research. 2011;23(4):304-8.
91. Parry SW, Steen IN, Baptist M, Kenny RA. Amnesia for loss of consciousness in carotid sinus syndrome: Implications for presentation with falls. Journal of the American College of Cardio-logy. 2005;45(11):1840-3.
92. Parry SW, Kenny RA. Drop attacks in older adults: Syste-matic assessment has a high diagnostic yield. Journal of the American Geriatrics Society. 2005;53(1):74-8.
93. Pasma JH, Bijlsma AY, Klip JM, Stijntjes M, Blauw GJ, Mul-ler M, et al. Blood pressure as-sociates with standing balance in elderly outpatients. PLoS ONE. 2014;9(9).
94. Phillips JR, Carroll J, Ehsanullah M. Screening for acute myocardial infarction in elderly patients with collapse, confusion and falls. Internatio-nal Journal of Clinical Practice. 1999;53(2):93-5.
95. Prudham D, Evans JG. Fac-tors associated with falls in the elderly: a community study. Age & Ageing. 1981;10(3):141-6.
96. Puisieux F, Bulckaen H, Fauchais AL, Drumez S, Salomez-Granier F, Dewailly P. Ambulatory blood pressure mo-nitoring and postprandial hypo-tension in elderly persons with falls or syncopes. Journals of Gerontology Series A-Biological Sciences & Medical Sciences. 2000;55(9):M535-40.
97. Rafanelli M, Ruffolo E, Chisciotti VM, Brunetti MA, Ceccofiglio A, Tesi F, et al. Clinical aspects and diagnostic relevance of neuroautonomic evaluation in patients with un-explained falls. Aging-Clinical & Experimental Research. 2014;26(1):33-7.
98. Rafiq M, McGovern A, Jones S, Harris K, Tomson C, Gallagher H, et al. Falls in the elderly were predicted op-portunistically using a decision tree and systematically using a database-driven screening tool. Journal of Clinical Epidemio-logy. 2014;67(8):877-86.
99. Richardson DA, Bexton RS, Shaw FE, Kenny RA. Prevalence of cardioinhibitory carotid sinus hypersensitivity in patients 50 years or over presenting to the accident and emergency department with ”unexplained” or ”recurrent” falls. Pacing & Clinical Electrophysiology. 1997;20(3 Pt 2):820-3.
100. Romero-Ortuno R, Cogan L, Foran T, Kenny RA, Fan CW. Continuous nonin-vasive orthostatic blood pres-sure measurements and their relationship with orthostatic intolerance, falls, and frailty in older people. Journal of the American Geriatrics Society. 2011;59(4):655-65.
101. Rosado JA, Rubenstein LZ, Robbins AS, Heng MK, Schulman BL, Josephson KR. The value of Holter monitoring in evaluating the elderly pa-tient who falls. Journal of the American Geriatrics Society. 1989;37(5):430-4.
102. Rutan GH, Hermanson B, Bild DE, Kittner SJ, LaBaw F, Tell GS. Orthostatic hypotension in older adults. The Cardiovascular Health Study. CHS Collabora-tive Research Group. Hyperten-sion. 1992;19(6 Pt 1):508-19.
103. Sanders NA, Ganguly JA, Jetter TL, Daccarett M, Was-mund SL, Brignole M, et al. Atrial fibrillation: an indepen-dent risk factor for nonacciden-tal falls in older patients. Pacing & Clinical Electrophysiology. 2012;35(8):973-9.





























