Embed Size (px)
Citation preview

UvA-DARE is a service provided by the library of the University of Amsterdam (http://dare.uva.nl)
UvA-DARE (Digital Academic Repository)
Bonded orthodontic retainersClinical survival, adhesion and material aspectsLie-Sam-Foek, D.J.
Link to publication
Creative Commons License (see https://creativecommons.org/use-remix/cc-licenses):Other
Citation for published version (APA):Lie-Sam-Foek, D. J. (2018). Bonded orthodontic retainers: Clinical survival, adhesion and material aspects.
General rightsIt is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s),other than for strictly personal, individual use, unless the work is under an open content license (like Creative Commons).
Disclaimer/Complaints regulationsIf you believe that digital publication of certain material infringes any of your rights or (privacy) interests, please let the Library know, statingyour reasons. In case of a legitimate complaint, the Library will make the material inaccessible and/or remove it from the website. Please Askthe Library: https://uba.uva.nl/en/contact, or a letter to: Library of the University of Amsterdam, Secretariat, Singel 425, 1012 WP Amsterdam,The Netherlands. You will be contacted as soon as possible.
Download date: 12 Sep 2020

Dave Lie Sam Foek
BONDED ORTHODONTIC RETAINERS:CLINICAL SURVIVAL, ADHESION
AND MATERIAL ASPECTS

Bonded orthodontic retainers:
Clinical survival, adhesion and material aspects
Dave Lie Sam Foek

ISBN: 978-90-9030900-2 Bookdesign: Sgaar Groningen, Saar de VriesCover: Dave Lie Sam FoekPrinted by: Drukkerij van der Eems Heerenveen © D.J. Lie Sam Foek, 2018
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form or by any means, mechanically, by photocopy, by recording or otherwise, without permission of the author.
Bonded orthodontic retainers:
Clinical survival, adhesion and material aspects
ACADEMISCH PROEFSCHRIFT
ter verkrijging van de graad van doctoraan de Universiteit van Amsterdamop gezag van de Rector Magnificus
prof. dr. ir. K.I.J. Maexten overstaan van een door het College voor Promoties ingestelde commissie,
in het openbaar te verdedigen in de Agnietenkapelop vrijdag 8 juni 2018, te 10:00 uur
doorDave Johan Lie-Sam-Foek
geboren te Paramaribo, Suriname

Paranimfen:
Drs. M.P.E. Tacken
Drs. C.G. Sabajo
Promotiecommissie:
Promotoren: Prof. dr. M. Özcan Rijksuniversiteit Groningen Prof. dr. A.J. Feilzer Universiteit van Amsterdam
Overige leden: Prof. dr. M.S. Cune Rijksuniversiteit Groningen Prof. dr. F.J.M. Roeters Universiteit van AmsterdamProf. dr. C.J. Kleverlaan Universiteit van Amsterdam Dr. I. Nedeljkovic Universiteit van AmsterdamDr. T.J. Algera Universiteit van Amsterdam
Faculteit der Tandheelkunde

CONTENTS
Chapter 1 Introduction 9
Chapter 2 Survival of flexible, braided, bonded stainless steel lingual retainers: A historic cohort study
19
Chapter 3 Adhesive properties of bonded orthodontic retainers to enamel: Stainless steel wire versus fiber-reinforced composites
33
Chapter 4 Fatigue resistance, debonding force, and failure type of fiber-reinforced composite, polyethylene ribbon-reinforced, and braided stainless steel wire lingual retainers in vitro
55
Chapter 5 Clinical survival of multi-stranded stainless steel bonded lingual retainers as a function of composite type: Up to 3.5 years follow-up
69
Chapter 6 Displacement of teeth without and with bonded fixed orthodontic retainers: 3D analysis using triangular target frames and optoelectronic motion tracking device
85
Chapter 7 General discussion and clinical implications 103
Chapter 8 Summary 111
Chapter 9 Samenvatting 117
Acknowledgement 125
Curriculum Vitae 133
The studies of this thesis were conducted at:- The Kolff / BMSA institute (Institute for Biomedical engineering, Material Sciences
and Application, University Medical Center Groningen, University of Groningen,
The Netherlands.
- The Department of Prosthodontics and Dental Materials, University of Bologna,
Italy.
- The Division of Dental Materials, University of Zurich, Switzerland.
- Academic Center for Dentistry Amsterdam (ACTA), Department of Dental Material
Science, Amsterdam, The Netherlands.
This thesis was supported by ACTA Research Institute of the Academic Center
for Dentistry Amsterdam (ACTA), University of Amsterdam and VU University, the
Netherlands.

Chapter 1
Introduction

10 11
along the fiber orientation.24-27 Commonly used FRC materials are carbon, kevlar,
polyethylene and glass fibers with unidirectional or woven fiber orientations.28
Some of such fibers are readily silanized and pre-impregnated with resin matrix,
whereas others need to be silanized and impregnated by the operator.29 Today,
FRCs are widely used in the fabrication of crowns, fixed dental prosthesis (FDP)
made directly at chairside or indirectly in a dental laboratory,24 root-canal posts,25
periodontal splints26 and orthodontic splints.27 In prosthodontic applications, the
two most important mechanical properties of FRCs are strength and stiffness.30,31
Stiffness or rigidity of the material is referred to as the modulus of elasticity. A
high modulus is necessary for FRC FDP, as it is expected to support the more
brittle overlying restorative resin composite. Typical preimpregnated unidirectional
dental FRCs incorporate approximately 45% glass fibers, having flexure modulus
in the range of 28 to 34 GPa and flexure strengths of about 600 to 1000 MPa.29
These values are almost 10 times higher than those for dental resins alone.33
From the available biocompatible fibers, glass fibers have drawn the most
attention due to their aesthetic qualities and easy manipulation in orthodontics
(Fig. 1b).32 Important factors influencing the mechanical properties of FRCs
include inherent material properties of fibers and polymer matrices, fiber surface
treatment (sizing) and impregnation of fibers with resin adhesion of fibers to the
polymer matrix, quantity of fibers, direction, position, orientation of fibers and
water sorption of the FRC matrix.3
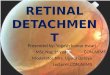
A B
Figures. 1a-b: Lingual orthodontic retainer made of a) multi-stranded stainless steel wire and b) fiber reinforced composite bonded using resin composite.
Clinical challenges associated with the adhesion of orthodontic retainersOrthodontic retainers made of either stainless steel or FRCs in general
require conditioning of the enamel on the lingual or palatal tooth surfaces with
phosphoric acid (35-37%) which yields to dissolution of hydroxyapatite through
which micromechanical retention of the resin material is achieved for bonding
Bonded orthodontic retainersOrthodontic retainers are used at the end of an orthodontic treatment to retain the
achieved tooth position. Without a phase of retention, there is a tendency for the
teeth to relapse towards their initial position after completion of the treatment.1-3
The aetiology of relapse is not fully understood but relates to a number of factors
that involves periodontal and occlusal aspects.4-6 Soft tissue pressures through lip
and tongue or physiological growth have also been reported as factors that affect
the tooth position and the incidence of relapse.7-9
Retention, which refers to the fixation of the achieved orthodontic result, can
be accomplished using removable or fixed retainers.3,10 Due to the advances
in adhesive technologies, the use of fixed retainers bonded to lingual or palatal
surfaces of incisor teeth has been widely used for more than three decades and
replaced removable retainers to a great extent.11,12
Materials used for orthodontic retainersStainless steel wiresThe most frequently used bonded orthodontic retainer material is stainless steel
wire, with varying stiffness and configuration (Fig. 1a).1,2,13 Lingual retainers are
either fabricated from relatively thick flat or round wires (0.030 - 0.032 inch) or from
thinner multistranded wires (0.0195 - 0.0215 inch).1,2,14 Typically, such wires are
bonded to each six anterior teeth in the maxilla and/or mandible. In some cases,
these wires are solely bonded to mandibular canines without bonding the retainer
onto the incisors.15,16 Clinical reports to date are more in favour of multistranded
(5-stranded 0.0215-inch wire) wires compared to single or multistranded wires
containing 3 or less strands that should be bonded to all anterior teeth in a
segment.1,2 Moreover, the use of multistranded wires decreases wire breakage
due to fatigue as a consequence of increased wire flexibility.2 Additionally, the
use of multistranded wires, reduces the individual mobility of the bonded teeth
while maintaining physiologic mobility.2,17 Yet, based on the previous clinical
reports, several shortcomings of the use of stainless steel wires remains to be
debonding, wire breakage, torque differences in the bonded teeth yielding to
positional changes of the teeth, metal allergy and aesthetic concerns.18-23 Due to
such limitations of these stainless steel wires, almost two decades ago, resin-
based bonded retainers were introduced.
Fiber Reinforced Composites Fiber reinforced composites (FRCs) are typically composed of fibers and a resin
matrix. In FRC structures, fibers are the main reinforcement elements while the
matrix bonds the fibers together in a given shape and transfers stresses between
the reinforcing fibers. The primary function of the fibers is to carry the loads

12 13
forces may be considered as factors for failures, which did not receive much
attention in the orthodontic literature.
Objectives of this thesisThe following research questions were addressed in this thesis:
1 What is the survival of flexible, braided, bonded stainless steel lingual retain-
ers as a function of gender, age, location and operator experience?
2 Do the fiber-reinforced composite retainers adhere better than stainless
steel retainers on enamel?
3- Are fiber-reinforced composite retainers more fatigue resistant compared to
braided stainless steel wires?
4 Is the survival of flexible, braided, stainless steel lingual retainers affected by
the type of resin composite used for their adhesion to tooth surfaces?
5 Does incremental loading increase the level of tooth displacement and what
are the margins of displacement in non-bonded and bonded conditions?
the retainers.1,34 Durable adhesion between the retainer and the tooth surface is
crucial in order to maintain the achieved orthodontic result.30 Debonding of the
retainer yield to unwanted tooth movement towards the original tooth position
prior to the orthodontic treatment.35 This could be referred as dental relapse often
requiring re-treatment which is both costly and time consuming for the patient,
orthodontist and the health care systems.31
Previous studies showed that the use of multi-stranded stainless steel wires may
show a higher success rate due to the reduced stress on the wire compared to
single-strand stainless steel wires.2,35,36-39 Detachment from the tooth surface and
breakage of such conventional retainers however do occur in clinical practice.22,35
In fact, failure rates varying from 5.9 to 53% have been reported over an average
period of 3 years.1,19,21,23,35,40-43 The failures reported were frequently associated
with loss of adhesion and/or micro-cracks at or around the composite-stainless
steel wire interface that resulted in detachment of the wires from the composite
mass.2 Due to the fact that multi-stranded wires present retentive morphologies,
the adhesion of the resin composite to the wire is mainly mechanical and not
chemical. The failures related to metal wires could be also multifactorial where,
location, operator experience and age is of significance.2,3,10,19,21 Therefore, the
chemical adhesion of FRC retainers to both the resin composite and the teeth
was anticipated to solve the adhesion problem experienced with stainless steel
wire retainers. Since a fiber bundle has a larger surface area and could be bonded
to each tooth due to its resinous matrix, more adhesion could be expected from
an FRC retainer after photo-polymerization. Certainly, the tooth-coloured FRC
presents more aesthetic outcome as opposed to metal ones, which could also be
considered as a solution to metal allergy experienced with metal retainers that is
reported to be 17% in female population.44
To date, there are no clear guidelines for the application mode of the polyethylene
or glass FRC retainers in orthodontics. While some manufacturers recommend
direct application of the FRC bundle on the tooth surface that is then covered
by the low-viscosity resin composite, others advice embedding the FRC bundle
in the bed of the low-viscosity resin, followed by coverage of the bundle again
with low-viscosity resin. Not only the application mode and adhesion forces
but also the fatigue conditions and the physico-chemical properties of the resin
composite could have direct impact on the durability of adhesion and thereby
clinical longevity of the retainers. An FRC retainer is flexible at the initial stage
before photo-polymerization that needs to be contoured to the tooth surface.
Direct application and pliability of FRC retainers allows for single appointment
application and eliminates laboratory procedures that can be the case with metal
retainers. Moreover, in contrast to the stainless steel wire retainers, in case of
chipping or fracture, FRC materials could be repaired easier.45 Furthermore, the
physiologic adaptation to the new position of the teeth resisting the adhesive

14 15
18. Will LA. Stability and Retention. Front Oral Biol 2016;18:56-63.
19. Segner D, Heinrici B. Bonded retainers-clinical reliability. J Orofac Orthop 2000;61:352-358.
20. Menezes LM, Campos LC, Quinta CC. Bolognese AM. Hypersensitivity to metals in orthodontics Am J Orthod Dentofacial Orthop 2004;126:58-64.
21. Lie Sam Foek DJ, Özcan M, Verkerke GJ, Sandham A, Dijkstra PU. Survival of flexible, braided, bonded stainless steel lingual retainers: a historic cohort study. Eur J Orthod 2008:30:199-204.
22. Renkema AM, Renkema A, Bronkhorst E, Katsaros C. Long-term effectiveness of canine-to-canine bonded flexible spiral wire lingual retainers. Am J Orthod Dentofac Orthop 2011;139:614-612.
23. Pandis N, Fleming PS, Kloukos D, Polychronopoulou A, Katsaros C, Eliades T. Survival of bonded lingual retainers with chemical or photo polymerization over a 2-year period: a single-center, randomized controlled clinical trial. Am J Orthod Dentofacial Orthop 2013;144:169-175.
24. De Boer J, Vermilyea SG, Brady RE. The effect of carbon fiber orientation on the fatigue resistance and bending properties of two denture resins. J Prosthet Dent 1984;51:119-121.
25. Karna JC. A fiber composite laminate endodontic post and core. Am J Dent 1996;9:230-232.
26. Strassler HE. Tooth stabilization improves periodontal prognosis: a case report. Dent Today 2009;28:88-92.
27. Rose E, Frucht S, Jonas IE. Clinical comparison of a multistranded wire and a direct-bonded polyethylene ribbon reinforced resin composite used for lingual retention. Quintessence Int 2002;33:579-83.
28. Freilich MA, Karmaker AC, Burstone CJ, Goldberg AJ. Development and clinical appli-cations of a light-polymerized fiber-reinforced composite. J Prosthet Dent 1998;80:311-318.
29. Freilich MA, Meiers JC, Duncan JP, Goldberg AJ. Clinical evaluation of fiber-reinforced fixed bridges. J Am Dent Assoc 2002;133:1524-1534
30. Freudenthaler JW, Tischler GK, Burstone CJ. Bond strength of fiber-reinforced composite bars for orthodontic attachment. Am J Orthod Dentofacial Orthop 2001;120:648-653.
31. Lie Sam Foek DJ, Özcan M, Krebs E, Sandham E. Adhesive properties of bonded orthodontic retainers to enamel: stainless steel wire versus fiber-reinforced-composites. J Adhes Dent 2009;11:381-390.
32. Karacaer O, Dogan A, Dogan OM, Usanmaz A. Dynamic mechanical properties of dental base material reinforced with glass fiber. J Appl Polym Sci 2002;85:1683-1697.
REFERENCES
1. Zachrisson BU, Büyükyilmaz T. Bonded retainers. In: Graber LW, Vanarsdall RL, Vig KW, editors. Orthodontics: Current principles and techniques. 5th ed. Philadelphia: Elsevier Mosby; 2012. p. 756-784.
2. Zachrisson BU. Multistranded wire bonded retainers: From start to success. Am J Orthod Dentofacial Orthop 2015;148:724-727.
3. Littlewood SJ, Millet DT, Doubleday B, Bearn DR, Worhington HV.Retention procedures for stabilising tooth position after treatment with orthodontic braces. Cochrane Database of Systematic Reviews. 2016;29: CD002283.
4. Southard T, Southard K, Tolley E. Periodontal force: a potential cause of relapse. Am J Orthod Dentofacial Orthop 1992;101:221-227.
5. Thilander B. Orthodontic relapse versus natural development. Am J Orthod Dentofacial Orthop 2000;117:562-563.
6. Thilander B. Biological basis for Orthodontic relapse. Semin Orthod 6 Part 3 2000:190-205.
7. Boese LR. Fiberotomy and reproximation without lower retention 9 years in retrospect: part II. Angle Orthod 1980;50:169-178.
8. Proffit WR, McGlone RE, Barrett MJ. Lip and tongue pressures related to dental arch and oral cavity size in Australian Aborigines. J Dent Res 1975;54:1161–1172
9. Gkantidis N, Christou P, Topouz N. The orthodontic-periodontic interrelationship in inte-grated treatment challenges: a systematic review. J Oral Rehabil 2010;37:377-390.
10. Zachrisson BU. Differential retention with bonded retainers. World J Orthod 2007;8:190-196.
11. Zachrisson BU. The bonded lingual retainer and multiple spacing of anterior teeth. Swed Dent J 1982;15:247-255.
12. Zachrisson BU. Third-generation mandibular bonded lingual 3-3 retainer. J Clin Orthod 1995;29:39-48.
13. Renkema AM, Sips E, Bronkhorst E, Kuijpers-Jagtman AM. A survey on orthodontic retention procedures in the Netherlands. Eur J Orthod 2009;31:432-437.
14. Årtun J, Zachrisson BU. Improving the handling properties of a composite resin for direct bonding. Am J Orthod Dentofacial Orthop 1982;81:269-276.
15. Knierim R. Invisible lower cuspid-to- cuspid retainer. Angle Orthod 1973:43:218-220.
16. Wolfsen J, Servoss JM. Bandless but fixed retention. Am J Orthod Dentofacial Orthop 1974; 66:431-434.
17. Watted N, Wieder M, Teuscher T, Schmitz N. Comparison of incisor mobility after insertion of canine-to-canine lingual retainers bonded to two or to six teeth. A clinical study. J Orofac Orthop 2000;62:387-396.

16 17
33. Lassila LVJ, Nohrstrom T, Vallittu PK. The influence of short-term water storage on the flexural properties of unidirectional glass fiber-reinforced composites. Biomaterials 2002;23:2221-2229.
34. Burstone CJ, Kuhlberg AJ. Fiber-reinforced composites in orthodontics. J Clin rthodont 2000;34:271-279.
35. Dahl E H, Zachrisson BU. Long term experience with direct bonded lingual retainers. J Clin Orthodont 1991;25:619-630.
36. Zachrisson BU. Clinical experience with direct-bonded orthodontic retainers Am J Orthod 1977;71:440-448.
37. Zachrisson BU. Improving orthodontic results in cases with maxillary incisors missing Am J Orthod 1978;73:274-289.
38. Zachrisson BU. The bonded lingual retainer and multiple spacing of anterior teeth. Swed Dent J 1982;15:247-255.
39. Radlanski RJ, Zain ND. Stability of the bonded lingual wire retainer-a study of the initial bond strength. J Orofac Orthop 2004;65:321-335.
40. Andrén A, Asplund J, Azarmidohkt E, Svensson R, Varde P, Mohlin B. A clinical evaluation of long term retention with bonded retainers made from multi-strand wires. Swed Dent J 1998;22:123-131.
41. Årtun J, Spadafora A T, Shapiro PA. A 3-year follow-up study of various types of orthodontic canine-to-canine retainers. Eur J Orthodont 1997;19:501-509.
42. Lumsden K W, Saidler G, McColl JH. Breakage incidence with direct bonded lingual retainers. Br J Orthod 1999;26:191-194.
43. Störmann I, Ehmer UA. Prospective randomized study of different retainer types. J Orofac Orthoped 2002;63:42-50.
44. Milheiro A, Kleverlaan C, Muris J, Feilzer AJ, Pallav P. Nickel release from orthodontic retention wires-the action of mechanical loading and pH. Dent Mater 2012;28:548-553.

Chapter 2
Survival of flexible, braided, bonded stainless steel lingual retainers: A historic cohort study
Lie Sam Foek D.J.
Özcan M
Verkerke G.J.
Sandham A
Dijkstra P.U.
Eur J Orthod. 2008 Apr;30(2):199-204.

20 21
INTRODuCTION
Bonded retainers are extensively used after orthodontic treatment with fixed
appliances in order to maintain the achieved result by preventing secondary
crowding of incisors after tooth alignment (Keim et al., 2002; Zachrisson and
Büyükyilmaz, 2005). Despite the various forms of retainers, the most commonly
used are the thick mandibular canine-to-canine (3-3) bonded retainer bar (0.030
or 0.032 inch) and the thin 0.0215 inch, flexible, spiral wire retainers (Littlewood
et al., 2004, 2006; Zachrisson and Büyükyilmaz, 2005). These types of bonded
retainers have been reported to have fairly high long-term (up to 15 years)
success rates (Zachrisson, 1978, 1982, 1986, 1995, 1996; Dahl and Zachrisson,
1991; Bearn, 1995; Årtun et al., 1997). Failure types reported in these studies
were loosening (debonding) and wire breakage. For a thin flexible spiral wire
in the mandible, failure rates of less than 10% have been reported, particularly
with the five-stranded Penta-One wire up to 2 - 3 years (Årtun and Urbye, 1988;
Dahl and Zachrisson, 1991; Bearn, 1995; Årtun et al., 1997). However, given the
importance of this phenomenon, relatively limited clinical research has been
performed, with reported mandibular failure rates ranging from 5.9% to 53%
(Dahl and Zachrisson, 1991; Årtun et al., 1997; Andrén et al., 1998; Lumsden et
al., 1999; Störmann and Ehmer, 2002). Although this wire type is the one most
often recommended, the range of failures shows high variation, indicating that
successful treatment maintenance with such wires cannot be achieved in the
long-term.
When these flexible spiral wire retainers are placed meticulously, they have the
advantage of allowing for safe retention of the treatment results. On the other
hand, when correct retention is difficult or impossible to achieve with traditional
removable appliances, flexible spiral wire retainers are considered appropriate,
and they are independent of patient cooperation. They also allow slight movement
of all bonded teeth and segments of teeth; they are highly efficient and, almost,
invisible (Segner and Heinrici, 2000; Zachrisson and Büyükyilmaz, 2005). The
disadvantages of flexible spiral wire retainers are that they may be subject
to mechanical stress and, if too thin, or not placed passively onto the enamel
surface, they may result in undesirable tooth movement (Årtun and Thylstrup,
1986; Dahl and Zachrisson, 1991; Årtun et al., 1997).
Due to the limited number of clinical studies that have been conducted to date
(Årtun et al., 1997; Lumsden et al., 1999; Zachrisson and Büyükyilmaz, 2005) and
the large range in failure rates with twisted wires, an alternative flexible, braided
wire retainer (Quad Cat stainless steel, twisted wire, 0.022 × 0.016 inch, GAC
International, Bohemia, New York, USA) is available for orthodontic treatment
purposes. Unfortunately, limited clinical information is available concerning such
braided wires (Southard and Southard, 1990; Zachrisson and Büyükyilmaz, 2005).
SuMMARy
The objectives of this study were to retrospectively evaluate the clinical survival
rate of flexible, braided, rectangular bonded stainless steel lingual retainers, and
to investigate the influence of gender, age of the patient, and operator experience
on survival after orthodontic treatment at the Department of Orthodontics,
University of Groningen, between the years 2002 and 2006.
The study group comprised of 277 patients [162 females: median age 14.8 years,
interquartile range (IQR) 13.6 - 16.5 years and 115 males: median age 15.3 years,
IQR 14.2 - 16.7 years]. After acid etching the lingual surfaces of each tooth, an
adhesive resin was applied and retainers were bonded using a flowable resin
composite. Data concerning, failures, gender, age of the patient, and operator
experience were retrieved from the patient files that were updated by chart
entries every 6 months or when failure was reported by the patient. The maximum
follow-up period was 41.7 months. All 277 patients received flexible, braided,
bonded mandibular canine-to-canine retainers. Eighteen failures were observed
in the maxilla. A failure was recorded when there was debonding, fracture, or
both, occurring in one arch. Only first failures were used for statistical analysis.
When failures occurred in both jaws, these were considered as two separate
incidences.
Ninety-nine debonding (35.7%), two fractures (0.7%), and four debonding and
fracture (1.4%) events were observed. No significant effect (P > 0.05) of gender
(females: 41%, males: 32%) or patient age (<16 years: 37%, ≥ 16 years 38.7%)
was observed. The failure rate did not differ due to operator experience (n = 15;
less experienced: 38.0%; moderately experienced: 28.9%, professional: 46.7%;
P > 0.05; chi-square test). Kaplan- Meier survival curves showed a 63% success
rate for the bonded lingual retainers over a 41.7 month period.

22 23
assumption was made that there must have been a bonded retainer in the maxilla
as well as in the mandible.
Follow-upThe patient data included the information derived from chart entries of clinical
examinations carried out every 6 months, or when the patient reported a failure.
The inclusion period for this retrospective cohort study was from December 2002
to May 2006, therefore the maximum follow-up period possible was 42 months.
Failure of a retainer occurs as a result of debonding, fracture, debonding and
fracture, or retainer loss. Information was unavailable on the site of failure e.g.
single tooth bond failure, enamel/adhesive failure, or adhesive wire failure. In
all cases where debonding was recorded, rebonding was undertaken. When
fracture and/or retainer loss occurred, a new retainer was made (Bond-A-Braid,
dead soft wire, Hilgers, Reliance Orthodontic Products Inc., Itasca, Illinois, USA)
at the chairside and bonded to the enamel surfaces after cleaning the enamel of
remnants of the adhesive and/or resin (Birnie, 2007).
In total, 87 failures occurred in the mandible (1 fracture, 82 debonding, and 4
debonding plus fractures). In the maxilla, 18 failures were observed (1 fracture
and 17 debonding). Due to the delegation strategy at the department (system
of work), different operators working under the supervision of one experienced
orthodontist were allowed to place the retainers. The experience of the operators
placing the retainers was categorized as 0 - 5 years (least experienced), 6 - 10
years (moderately experienced), 11 - 15 years (experienced), 16 - 20 years (most
experienced), and 21 years or more (very experienced).
Statistical analysisStatistical analysis was performed using the Statistical Package for Social
Sciences (version 12.0, SPSS Inc., Chicago, Illinois, USA). Descriptive statistics
and Kaplan-Meier curves were calculated. In the Kaplan-Meier curves, the cu-
mu lative survival rate of the retainers was compared against the time interval
between placement of the retainers and occurrence of the first failure. Only first
failures were counted and no distinctions were made in failure location in case of
debonding. A reported failure in the maxilla or in the mandible was counted as a
separate incidence. In addition, multiple failure sites in one retainer were counted
as one failure. Furthermore, failure was considered when there was debonding,
fracture, debonding and fracture, or retainer loss. A chi-square test was used in
order to analyse the influence of gender, age of the groups, and experience of
the operators on the survival rate. P values less than 0.05 were considered to be
statistically significant.
Therefore, the aims of this study were to analyse the survival rate of flexible,
braided, rectangular, bonded, lingual stainless steel wire retainers by means of a
historic cohort study, and to investigate the influence of gender, patient age, and
operator experience on survival.
SuBJECTS AND METHODS
Sample Initially, patient files, without pre-selection were retrieved from the Department
of Orthodontics, Groningen, The Netherlands by undertaking a search of the
computer program (OrtWin 2.0, Netpoint, Kaatsheuvel, The Netherlands). All
selected patients (n = 277) satisfied the inclusion criteria of having finished
their orthodontic treatment with fixed appliances and having received a bonded
retainer between December 2002 and May 2006.
One hundred and sixteen patients were treated with removable functional and
fixed appliances (combined treatment) and 161 only with fixed appliances. All 277
patients [162 females: median age 14.8 years, interquartile range (IQR) 13.6 - 16.5
years and 115 males: median age 15.3 years, IQR 14.2 - 16.7 years] received a
mandibular flexible bonded retainer from canine to canine (3-3). It is not known
which proportion of the total sample also received a bonded retainer in the maxilla
at baseline. A modified maxillary removable Hawley retainer was usually worn for
a period of 1 year by some patients after completion of orthodontic treatment.
Application of retainers The flexible, braided, rectangular, stainless steel wire retainers (Quad Cat, 0.022 ×
0.016 inch, GAC International) were initially prepared for the maxilla and mandible
on plaster cast models by dental technicians (Ortholab Dental Technicians, Doorn,
The Netherlands). Since such flexible retainers need to be bonded to each tooth
(Zachrisson and Büyükyilmaz, 2005), the enamel was acid etched for 10 seconds
per tooth with 38% H3PO4 and rinsed thoroughly, before the bonding adhesive
(Heliobond, Ivoclar Vivadent, Schaan, Liechtenstein) was applied and air thinned.
All retainers were bonded using a flowable resin composite (Tetric Flow, Cavifill
210 A3, Ivoclar Vivadent) and light polymerized for 20 seconds per tooth using
a light-emitting diode polymerization device (Ortholux™, 3M Unitek, St Paul,
Minnesota, USA) and placed by orthodontists (n = 1), postgraduate students
(n = 4), dental hygienists (n = 8), or dental assistants (n = 2). Moisture control for
the retainers was accomplished using cotton rolls and saliva ejectors. All subjects
(n = 277) received a mandibular bonded retainer. Due to the retrospective
nature of this study, the exact number of bonded retainers placed in the maxilla
was unknown. If failure of a bonded retainer in the maxilla was reported, the

24 25
RESuLTS
The maximum follow-up period was 41.7 months (median 19.9 months, IQR 15.2
- 23.7, mean 19.1 months, SD 7.2). Table 1 shows a summary of the demographic
characteristics of the patient population and the effect of confounding factors on
the survival rate.
Of the total number of treated patients, 66.1% were younger than 16 years and
33.9% were older than 16 years; 58.5% were female and 41.5% were male.
In total, 99 debonding (35.7%), two fracture (0.7%), and four debonding plus
fracture (1.4%) failures were observed. No significant effect of gender [females:
41% (confidence interval, CI: 16.3 - 83.9), males: 32% (CI: 24.8 - 41.8)], patient
age [<16 years: 37% (CI: 30.3 - 44.0), ≥16 years: 38.7% (CI: 29.4 - 48.9)], and
operator experience (least experienced: 38.5%, moderately experienced: 28.9%,
very experienced: 46.7%) on failure rate was found (chi-square test; P > 0.05;
Figure 1).
Kaplan-Meier survival curves showed a gradual decrease in failure rate, being
highest at 6 months at 78%. According to the plot, if the retainers survived the
first 2 years, they usually continued to function well. Figure 2 shows that the
cumulative survival rate for the bonded lingual retainers was 63%. Exact data for
the mandibular definition indicated a survival rate of 68.4%.
Table 1: Summary of the demographic characteristics of the patient population and the effect of confounding factors on the failure rate of lingual bonded retainers.
Number of retainers placed
Failure (%) 95% Confidence Interval
Gender
Females 162 41.4 34.1, 49.1
Males 115 33.3 25.3, 42.4
Age*
<16 years 181 37.0 30.3, 44.3
≥16 years 93 38.7 29.4, 48.9
Operator experience**
0-5 years 200 38.5 32.0, 45.4
6-10 years - - -
11-15 years - - -
16-20 years 45 28.9 17.7, 43.4
≥21 years 30 46.7 30.3, 63.9 *Data of three patients missing. †Number of patients treated by operators (n = 15). Note that data of two patients were missing.
Cu
mu
lati
ve S
urv
ival
Time (months)
Female
Male
0,00 10,00 20,00 30,00 40,00 50,00
0,0
0,2
0,4
0,6
0,8
1,0
Figure 2: Kaplan-Meier survival curve showing a 63% success rate for the bonded lingual retainers over a 41.7 month period.
Cu
mu
lati
ve S
urv
ival
Time (months)
0
0,0
0,2
0,4
0,6
0,8
1,0
6 12 18 24 30 36 42
Figure 1: Cumulative survival rates of bonded lingual retainers for females (n = 162) and males (n = 115).

26 27
ments of the retainer wire during the setting process of the adhesive could impair
ideal adhesion. In vitro and in vivo studies (Ibe and Segner, 1995; Hajrassie and
Khier, 2007) have also concluded that a certain percentage of bonding sites may
be unsatisfactory, although the mean bond strength may be initially sufficient.
The in vitro findings could be expected to apply even more strongly for in vivo
placements due to a less favourable working environment. Such sites with
insufficient bond strength will manifest themselves in the first week or months
after bonding.
Other explanations for the early failures could be based on biological reasons.
Tuverson (1980) suggested that rotational relapse may be due to small contact
points at the axial part of the bonded teeth which seem to be unstable. Surbeck
et al. (1998) commented that the presence of more crowded and irregular
dentitions prior to treatment may not necessarily be a sole indicator of greater risk
for relapse after treatment. In addition, factors such as orthodontic expansion,
incomplete tooth alignment, and interdental spacing might be responsible for
post-treatment relapse leading to failure of bonded retainers. Unfortunately, in
retrospective studies, such aspects cannot always be identified.
Huang and Årtun (2001) found an association between a narrow intercanine width
and relapse of the maxillary and mandibular incisors. Fudalej and Årtun (2007)
concluded that neither forward nor backward rotational growth patterns, at the
time of appliance removal, are associated with increased risk of post-retention
relapse. Particularly, in adolescent orthodontic patients, the type of post-
treatment growth is difficult to predict. The sample in the present study consisted
mostly of adolescent patients which could perhaps explain the high rate of failure.
On the other hand, Yoshida et al. (1999) suggested that rapid remodelling of the
periodontal ligament and the surrounding alveolar bones could be the main cause
of tooth relapse. While different factors play a role in post-treatment relapse, it is
most likely that the forces exceed the adhesive strength of the bonded retainers
causing them to fail.
Successful clinical outcomes are often reported by experienced orthodontists
(Dahl and Zachrisson, 1991; Årtun et al., 1997) especially in private practice
settings. The experience of the operator is expected to be the most likely key
factor influencing the failure rates. Higher failure rates could be expected when
less experienced operators are involved. Interestingly, however, in the present
study, neither different operators nor experience played a significant role in
failure rate. Due to the considerable design differences of the retainers placed
by different operators, a high failure rate ranging from 28.9% to 46.7% between
practitioners was observed. However, in clinical trials, particularly in dentistry,
experience may not be always quantified in years of practice. Also in this study,
the number of retainers bonded by the experienced operators decreased with
the increase in delegation. It is also difficult to distinguish the transition between
DISCuSSION
Total survival rate for the flexible, lingual, braided bonded retainers was 63%
over an observation period of 41.7 months. The survival rate decreased during
this time, with the highest number of failures being observed within the first 6
months after placement. This finding is in accordance with the results of Årtun
et al. (1997) and Segner and Heinrici (2000). Although the retrospective design
of the study contributed to the lack of data for the precise number of retainers
placed in the maxilla, exact data concerning the failure rate for the mandible was
found to be 31.6%. These results are slightly lower than the findings of Andrén et
al. (1998) who reported a failure rate of 35% for the mandible. On the other hand,
they were higher than the 18%failure rate for the 0.0195 inch and lower than the
53% failure rate for the 0.0215 inch retainer reported by Störmann and Ehmer
(2002). However, the failure rate found in this study was higher than the 27.2 per
cent for the thin, flexible spiral wires reported by Årtun et al. (1997). Similarly,
Dahl and Zachrisson (1991) reported a failure rate of 10.3% with the use of three-
stranded spiral wire (Triflex or Wildcat) and 5.9% with the five-stranded spiral
wire (Penta-One). In their investigation, as in most previous studies (Zachrisson,
1982; Dahl and Zachrisson, 1991; Årtun et al., 1997), the retainer wires were
bonded with a chemically polymerized resin composite (Concise).
The failure rates recorded in the present investigation are less favourable than
those published previously by Dahl and Zachrisson (1991) and Årtun et al. (1997).
In both of those studies, all the retainers were bonded in private practice by one
or two experienced operators, while in the present study the retainers were
bonded by 15 different operators, with a great difference in experience. Similar
to the study of Segner and Heinrici (2000) where the retainers were bonded by
28 different operators, in the present study bonding was undertaken by multiple
operators. This may account for the difference in failure rates.
The position in the present study of the wire on the lingual surfaces of the teeth,
being either more cervical or more incisal, is unknown. According to Andrén et al.
(2001), a more incisal positioning of the retainer results in less flexibility.
Some studies (Dahl and Zachrisson, 1991; Bearn, 1995; Andrén et al., 1998;
Segner and Heinrici, 2000) reported higher failure rates for the maxilla compared
with the mandible but this could not be verified in this investigation due to missing
data for the maxilla. The fracture rate in the present study was found to be 0.2%,
but the true fracture rate might be slightly higher than the figures calculated due
to the incomplete data.
A noticeable finding of the present investigation was that the failures occurred
mostly in the first 6 months after the retainers were bonded. One explanation
for this could be insufficient composite bond strength to enamel that is often
technique sensitive. Factors such as a lack of moisture control or minute move-

28 29
REFERENCES
1. Andrén A, Asplund J, Azarmidohkt E, Svensson R, Varde P, Mohlin B 1998 A clinical evaluation of long term retention with bonded retainers made from multi-strand wires. Swedish Dental Journal 22 : 123-131
2. Årtun J, Thylstrup A 1986 Clinical and scanning electron microscopic study of surface changes of incipient caries lesions after debonding. Scandinavian Journal of Dental Research 94 : 193-201
3. Årtun J, Urbye K S 1988 The effect of orthodontic treatment on periodontal bone support in patients with advanced loss of marginal periodontium. American Journal of Orthodontics and Dentofacial Orthopedics 93 : 143-148
4. Årtun J, Spadafora A T, Shapiro P A 1997 A 3-year follow-up study of various types of orthodontic canine-to-canine retainers. European Journal of Orthodontics 19 : 501-509
5. Audenino G, Giannella G, Morello G M, Ceccarelli M, Carossa S, Bassi F 2006 Resin-bonded fixed partial dentures: ten-year follow-up. International Journal of Prosthodontics 19 : 22-23
6. Bearn D R 1995 Bonded orthodontic retainers: a review. American Journal of Ortho-dontics and Dentofacial Orthopedics 108 : 207-213
7. Birnie D 2007 Stability and retention. Excellence in Orthodontics, London, pp. 411-432.
8. Dahl E H, Zachrisson B U 1991 Long term experience with direct bonded lingual re-tainers. Journal of Clinical Orthodontics 25 : 619-630
9. Davidson C L, de Gee A J 2000 Light-curing units, polymerization, and clinical implica-tions. Journal of Adhesive Dentistry 2 : 167-173
10. Fudalej P, Årtun J 2007 Mandibular growth rotation effects on postretention stability of mandibular incisor alignment. Angle Orthodontist 77 : 199-205
11. Hajrassie M, Khier S 2007 In-vivo and in-vitro comparison of bond strengths of orthodontic brackets bonded to enamel and debonded at various times. American Journal of Orthodontics and Dentofacial Orthopedics 131 : 384-390
12. Huang L, Årtun J 2001 Is the postretention relapse of maxillary and mandibular incisor alignment related? American Journal of Orthodontics and Dentofacial Orthopedics 120 : 9-19
13. Ibe D, Segner D 1995 Improvement in the adhesive strength of orthodontic brackets on unit-cast and Fired dental alloys by microsandblasting. Journal of Orofacial Orthopedics 56 : 110-117
14. Keim R G, Gottlieb E I, Nelson A H, Vogels 3rd D S 2002 JCO study of orthodontic diagnosis and treatment procedures. 1. Results and trends. Journal of Clinical Orthodontics 36 : 553-568
15. Littlewood S J, Millett D T, Doubleday B, Bearn D R, Worthington H V 2004 Retention procedures for stabilising tooth position after treatment with orthodontic braces. Cochrane Database of Systematic Reviews 1: CD002283
the least experienced and the experienced. Nevertheless, the findings of this
research represent a more real-life clinical situation.
The results did not show significant differences in failure rates between genders
and age, in agreement with the findings of Lumsden et al. (1999) where the mean
age of the subjects was 15.5 years. The results related to age were, however,
lower than those reported by Dahl and Zachrisson (1991) where the mean age
of the patient population was 31.2 years. It should, however, be noted that their
sample size was only 17 for the mandible, whereas for the present study the total
sample was 277. A direct comparison is therefore not possible since the reason
for failures could be related to the relapse response in the adults or simply to the
low power of the study.
Although previous investigations (Dahl and Zachrisson, 1991; Årtun et al., 1997;
Störmann and Ehmer, 2002) have shown a difference in failure rate when different
types of retainers are used, no randomized controlled clinical trials have been
performed to date. Future investigations should concentrate on this aspect. In the
current study, moisture control was achieved using only saliva ejectors and cotton
rolls. However, the survival rate of resin-bonded restorations has been reported
to be higher when bonding procedures are performed under rubber dam isolation
(Audenino et al., 2006). Prospective studies should also perhaps concentrate on
other confounding factors such as effective moisture control, light intensity of
the polymerization device (Davidson and de Gee, 2000), and the composite and
adhesive resin used.
Conclusions
The following conclusions can be drawn from this study:
1. The success rate of the flexible, braided, bonded lingual retainers was 63%
over 41.7 months.
2. The survival rate for the mandible was 68.4%.
3. Most failures occurred during the first 6 months.
4. Gender and age of the patient and operator experience did not affect the
failure rate.
AcknowledgementThe authors would like to extend their gratitude to Dr. M.W.J. Bierman for helpful
discussions.

3130
16. Littlewood S J, Millett D T, Doubleday B, Bearn D R, Worthington H V 2006 Retention procedures for stabilising tooth position after treatment with orthodontic braces. Cochrane Database of Systematic Reviews 1: CD002283
17. Lumsden K W, Saidler G, McColl J H 1999 Breakage incidence with direct bonded lingual retainers. British Journal of Orthodontics 26: 191-194
18. Segner D, Heinrici B 2000 Bonded retainers-clinical reliability. Journal of Orofacial Orthopedics 61 : 352-358
19. Southard K A, Southard T E 1990 Conservative management of anterior spacing and deep bite: a case report. Quintessence International 21: 801-811
20. Störmann I, Ehmer U 2002 A prospective randomized study of different retainer types. Journal of Orofacial Orthopedics 63: 42-50
21. Surbeck B T, Årtun J, Hawkins N R, Leroux B 1998 Associations between initial, posttreatment, and postretention alignment of maxillary anterior teeth. American Journal of Orthodontics and Dentofacial Orthopedics 113: 186-195
22. Tuverson D L 1980 Anterior interocclusal relations. Part II. American Journal of Orthodontics 78: 361-393
23. Yoshida Y, Sasaki T, Yokova K, Hiraide T, Shibasaki Y 1999 Cellular roles in relapse processes of experimentally - moved rat molars. Journal of Electron Microscopy 48: 147-157
24. Zachrisson B U 1978 Improving orthodontic results in cases with maxillary incisors missing. American Journal of Orthodontics 73: 274-289
25. Zachrisson B U 1982 The bonded lingual retainer and multiple spacing of anterior teeth. Swedish Dental Journal 15: 247-255
26. Zachrisson B U 1986 Bonding in orthodontics. In: Graber L W (ed). Orthodontics: current principles and techniques. Mosby, St Louis, pp. 526-561
27. Zachrisson B U 1995 Third-generation mandibular bonded lingual 3-3 retainer. Journal of Clinical Orthodontics 29: 39-48
28. Zachrisson B U 1996 Clinical implications of recent orthodonticperiodontic research findings. Seminars in Orthodontics 2: 4-12
29. Zachrisson B U, Büyükyilmaz T 2005 Bonding in orthodontics. In: Graber L W (ed). Orthodontics: current principles and techniques, 4th edn. Mosby, St Louis, pp. 621- 659.

Chapter 3
Adhesive properties of bonded orthodontic retainers to enamel: stainless steel wire versus fiber-reinforced composites
Lie Sam Foek D.J.
Özcan M
Krebs E
Sandham A
J Adhes Dent. 2009 Oct;11(5):381-90.

34 35
INTRODuCTION
During orthodontic treatment, the position of teeth is adjusted in order to correct
malocclusion. There is an inherent tendency for teeth to relapse to their original,
pretreatment position after the removal of orthodontic appliances.1,11 With the
possibility of acid etching and bonding, it has become common practice to
apply bonded fixed retainers for long-term retention of the achieved orthodontic
results.2,7 Currently, such retainers are often made of either stainless steel wires
or fiber-reinforced composites (FRC) of diverse types. Limited clinical studies
have shown that there is a relatively high failure rate ranging between 2.9% to
47% in a comparatively short follow-up period.1-3,7,15 The failure type is usually
either detachment of the wire retainer from the tooth surface or at the wire and/
or resin composite interface. Although the reasons for these failures have not
been extensively studied, several factors are described in the dental literature,
such as insufficient composite material and/or abrasion of the composite,3,4 less
abrasion resistance and wear as a consequence of chewing or tooth brushing,3,4
thickness of the wire,15 and intermittent forces of mastication.3,4 Another reason
for debonding rates was attributed to the forces resulting from tension in the
wire or between the wire and the teeth when the wire has not been adapted
properly to the surface of the teeth.3 Nevertheless, detachment of the bonded
retainers has negative consequences for the treatment result, since the teeth
may change position or relapse to their original position after the completion of
the orthodontic treatment. This is costly for both the medical system and the
patient, as it renders the lengthy and costly previous treatment ineffective, possi-
bly making retreatment necessary.
Recently, FRC materials have been introduced for the fabrication of fixed dental
prostheses (FDP), root posts, periodontal splints, and also as possible alternatives
to stainless steel wire retainers for both active and passive applications in
orthodontics. Resin pre-impregnated FRCs have a suitable flexural modulus
and flexural strength for functioning successfully in the mouth as restorative
materials.16,31 It is thought that elimination of the metal wire in the retainer by
using FRC systems may lead to more stable bonding, since adhesion of such
retainers would solely rely on adhesion of the flowable composite or the resin
matrix of the FRC to the etched and bonded enamel. Theoretically, FRC materials
are attractive because of their elastic modulus, esthetics, pliability, and the
possibility of chemical adhesion both to the composite materials and the tooth,
as opposed to the metal wires. Considering the clinical failures with stainless
steel retainers related to debonding, especially the adhesion aspect warrants the
comparison of FRC materials to their metallic counterparts.
FRC materials are available in different forms and volumes, either preimpregnated
with different resin monomer matrices or requiring impregnation prior to application
ABSTRACT
Purpose: The objectives of this study were to compare the bond strength of a
stainless steel orthodontic wire versus various fibre-reinforced-composites (FRC)
used as orthodontic retainers on enamel, analyze the failure types after debonding
and to investigate the influence of different application procedures of stainless
steel wires on bond strength.
Materials and Methods: Caries-free, intact human mandibular incisors (N=80, n=10
per group) were selected and randomly distributed into 8 groups. After etching with
37% H3PO4 for 30 seconds, rinsing and drying, bonding agent (Stick Resin) was
applied, light polymerized and one of the following FRC materials were applied on
the flowable composite (Stick Flow) using standard molds: Group 1: Angelus Fibrex
Ribbon; Group 2: DentaPreg Splint; Group 3: everStick Ortho and Group 4: Ribbond.
In Group 5, Quad Cat Wire was applied in the same manner as in FRC groups.
In Group 6, after bonding agent (Stick Resin), Quad Cat Wire was placed directly
on the tooth surface and covered with Stick Flow composite. In Group 7, after
bonding agent (Heliobond) was applied, Quad Cat Wire was placed directly on the
tooth surface and covered with Tetric Flow composite. In Group 8, after applying
bonding agent (Heliobond), Tetric Flow composite was applied, not polymerized
and Quad Cat Wire was placed and covered with Tetric Flow again. Specimens
were thermocycled for 6000 cycles between 5-55°C and loaded in a universal
testing machine under shear stress (crosshead speed: 1 mm/min) until debonding
occurred. The failure sites were examined under an optical light microscope. Data
were analyzed using 1-way ANOVA and Tukey-Kramer adjustment test (α = 0.05).
Results: Significant differences were found between the groups (p = 0.0011)
(ANOVA). Bond strength results did not significantly differ neither between the
FRC groups (Groups 1-4) (6.1±2.5 to 8.4±3.7 MPa) (p > 0.05) or the wire groups
(Groups 5-8) (10.6±3.8 to 14±6.7 MPa) (p > 0.05). Failure types varied within the
FRC groups, but mainly composite was found left adhered on the enamel surface at
varying degrees. In the stainless steel wire groups, when the retainer was applied
onto the bonding agent and then covered with flowable resin, partially attached
composite on the enamel was often found after debonding. When the wires were
embedded in the flowable composite, the Heliobond group (Group 8) showed more
adhesive failures between the enamel and the composite compared to Group 5,
where bonding agent was Stick Resin.
Conclusion: Regardless of their application mode, stainless steel orthodontic
bonded retainers delivered higher bond strengths than those of fiber retainers.
The differences were statistically significant compared to those of Angelus Fibrex
Ribbon and DentaPreg Splint.
Keywords: bond strength, fiber-reinforced composite, lingual retainer, orthodontics,
relapse, stainless steel wire.

36 37
MATERIALS AND METHODS
Specimen PreparationEighty caries-free human mandibular central incisors of similar size, stored in
distilled water with 0.1% (wt/vol) thymol at room temperature, were selected
from a pool of recently extracted teeth. To determine that the enamel was free
of crack lines, all teeth were evaluated under blue light transillumination. The
roots were then sectioned with a diamond bur under water cooling. The crowns
were mounted in polyethylene rings (diameter: 15 mm, thickness: 10 mm), with
the buccal surface exposed, using autopolymerized polymethyl methacrylate
(Candulor; Wangen,Switzerland) (Fig 1). Before embedding, the teeth were
cleaned of any remaining soft tissue and calculus and stored in distilled water with
0.1% (wt/vol) thymol up to 2 months until the experiments. The enamel surfaces
were cleaned and polished using water and fluoride-free pumice (Zircate Prophy
Paste, Dentsply Caulk; Milford, DE, USA, batch #077809) with a prophylaxis
brush (Hawe Prophy- Cup Latch-Type, KerrHawe; Bioggio, Switzerland, batch
#960/30), rinsed with water, and dried using an air syringe.
Bonding ProceduresIn all groups, labial enamel surfaces were etched with a 37% orthophosphoric
acid (TopDent, DAB Dental; Upplands Väsby, Sweden) for 30 s and then rinsed
thoroughly using an oil-free air-water spray for 20 s. The enamel surfaces
were air dried until they appeared frosty. Description of brands, compositions,
manufacturers, and batch numbers of FRC and wire retainers are listed in Table 1.
Representative SEM (JSM-5500, JEOL Instruments; Tokyo, Japan) micrographs
of the FRC materials and stainless steel wire are presented in Figure 2.
by the clinician. The adhesive performance of the FRCs may vary depending on
the variations in their inherent properties and impregnation. Although individual
studies exist on adhesion of resin based materials to enamel, to the authors’
knowledge, no research has been conducted to date comparing the adhesive
properties of FRC splint materials with conventionally bonded stainless steel
wires in the same study design. Both FRC and stainless steel wires are bonded
to enamel in orthodontic wire applications using resin based materials, but their
flexural behavior may vary due to the variations in the adhesion of resin materials
to resins and metals. Furthermore, different application modes of stainless
steel wires have been noted in the orthodontic literature, i.e., placing the wire
directly on the etched and bonded enamel 3,4 or embedding the wire in flowable
resin composite or bonding agents with various properties/compositions3,4,35
that may affect the bond strength and the failure types. Because resin-based
materials adhere better to enamel than do metals,21 it was hypothesized that FRC
materials would demonstrate higher bond strength than the metal ones, and that
the bond strength of the stainless steel wires would increase when the wires
were embedded in flowable composite, instead of being applied directly onto the
bonding agent on the enamel.
Preimpregnated systems usually involve monomers like urethane dimethacrylate
(UDMA), urethane tetramethacrylate (UTMA), bisphenol glycidylmethacrylate
(bis-GMA), or polymethyl methacrylate (PMMA).9,19 Evidence is still lacking on
whether ultrahigh molecular weight polyethylene (UHMWPE) fibers can be used
to fabricate durable FRC restorations.10,27,31 Criticism has been focused on the
inadequate interfacial adhesion between polyethylene fibers and dental polymers30
compared to glass and silica fibers, which can be silanized.13,30 Therefore, it was
also hypothesized that silanized and pre-impregnated glass-fiber FRCs would
possess better adhesive properties than plasma-coated, custom impregnated
polyethylene FRC materials.
Therefore, the objectives of this study were twofold: 1. to compare the bond
strength and failure types of a commonly used stainless steel orthodontic wire
with differently impregnated FRC materials with various textures, and 2. to
investigate the influence of different application procedures of stainless steel
wires.
Figure 1: Mandibular incisor embedded in auto-polymerized polymethylmethacrylate with the labial surface exposed for bonding purposes.

38 39
Table 1: The brand names, group numbers, compositions, manufacturers and batch numbers of the materials used in this study.
Brand name Groups Composition Manufacturer Batch number
Angelus Interlig 1 E-glass/Bis-GMA Angelus, Londrina, Brazil
2199
DentaPreg Splint 2 S2-glass, mixture of dimethacrylates, initiators and stabilizers
ADM a.s., Brno, Czech Republic
4742
everStick Ortho 3 E-glass/PMMA/Bis-GMA StickTech Ltd, Turku, Finland
88
Ribbond 4 Ultra High Molecular Weight Polyethylene
Ribbond Inc., Seattle, USA
9543
Quad Cat Wire 5-8 Stainless steel, three-strand twisted wire 0.022” x 0.016”
Quad Cat, GAC International, New York, USA
197
Stick Resin Silanated silica 30% - 70% 2,2- bis[4-(2-hydroxy-3-methacryloxyropoxyl)]-phenonylpropane 30% - 70% Triethyleneglycol dimethacrylate
StickTech Ltd, Turku, Finland
5504765
Heliobond Monomer matrix: dimethacrylate < 60% Bis-GMA < 40% Triethyleneglycol
Ivoclar Vivadent, Schaan, Lichtenstein
H29583 154518
Stick Flow Mixture of resin based on Bis-GMA, Methacrylates, catalysts, stabilizers, pigments
StickTech Ltd, Turku, Finland
D3-DA3-3
Tetric Flow < 14% Bis-GMA < 8% Triethylene glycoldimethacrylate < 15% Urethanedimethacrylate
Ivoclar Vivadent, Schaan, Lichtenstein
J01476 154518
FRC Retainers (Groups 1 to 5) All FRC retainers were bonded following the same procedures with the same
adhesive resin and the flowable resin material. The FRCs were cut by means of
a pair of special scissors (Ribbond fiber cutter, Ribbond; Seattle, WA, USA) to
the same length (3 mm). A filler- and solvent-free lightcuring bonding agent (Stick
Resin, StickTech; Turku, Finland) was applied with a microbrush on the acid-
etched enamel surface and blown into a thin layer. It was then light polymerized
for 40 s with a conventional halogen light curing unit (Demetron LC, SDS Kerr;
Danbury, CT, USA) (light output: 400 mW/cm2). The irradiation distance between
the exit window and the resin surface was maintained at 2 mm to obtain adequate
Figures 2a-e: Representative SEM pictures ofa) Angelus Fibrex Ribbon (original magnification x80),b) DentaPreg Splint (original magnification x80),c) everStick Ortho (original magnification x 80). Note the resin impregnation of the fibers on as-received samples,d) Ribbond (original magnification x40), ande) Quad Cat stainless steel-wire (original magnification x40).
A
C
E
B
D

40 41
flowable composite was applied and the wire was placed in the bed of this
flowable resin. The wire was then covered again with flowable composite, and
light polymerization was performed. The specimens were stored in distilled water
with 0.1% (wt/vol) thymol solution at 37°C for one week and thermocycled 6000
times between 5ºC and 55°C (dwell time: 30 s, transfer time from one bath to the
other: 2 s) (Willytec; Gräfelfing, Germany).
Shear Bond TestingThe specimens were mounted in the jig of the universal testing machine (Zwick
ROELL Z2.5 MA 18-1-3/7; Ulm, Germany) where the force was applied at the
composite/ retainer-enamel interface from the occluso-cervical direction.
The shearing blade had a taper of 45 degrees at the tip. The specimens were
loaded at a crosshead speed of 1.0 mm/min until failure occurred, and the
stress-strain curve was analyzed with the proprietary software program
(Zwick ROELL). The force required to shear-peel the retainer was recorded
and converted into MPa using the known surface area of the mold (7.04 mm2)
representing the bonded area. Schematic drawings of the FRC and wires in
relation to their application modes and the shear blade are depicted in Fig 4.
Subsequently, digital photographs (Nikon D1, Micro Nikon 60 lens; Tokyo,
Japan) were taken of the substrate surfaces and the debonded retainers.
polymerization. Flowable resin composite (Stick Flow, StickTech) was applied to
the enamel surface and the respective FRC material was placed on the bed of
the flowable composite, arranged horizontally on the largest area of the incisor in
a rectangular polyethylene mold (3.2 x 2.2 x 1.5 mm) (Fig 3). The FRC materials
were rewetted with the bonding agent (Stick Resin) and then covered with the
flowable resin (StickFlow, StickTech). This was also light polymerized for 40 s
from a distance of 2 mm.
Stainless Steel Wires (Groups 5 to 8)The orthodontic retainer wire used in this study was a flexible, braided, rectangular,
stainless-steel wire (Quad Cat,0.022 in x 0.016 in, GAC International; Bohemia,
NY, USA).
Specimens in group 5 were prepared in the same manner with the procedure
used for the FRC materials. In groups 6 to 8, the attempt was made to simulate
different aspects of commonly used clinical methods. In groups 7 and 8, a
different bonding agent and a flowable composite was used.
Group 6: A filler and solvent-free light-curing bonding agent (Stick Resin, StickTech)
was applied with a microbrush on the acid-etched enamel surface and blown into
a thin layer. It was then light polymerized for 40 s with a conventional halogen
light curing unit (Demetron LC, SDS
Kerr) (light output: 400 mw/cm2). The irradiation distance between the exit
window and the resin surface was maintained at 2 mm to obtain adequate
polymerization. A piece of wire (3 mm) which was previously bent to adapt to
the individual surface of each specimen, was placed on the tooth surface, and
flowable composite (Stick Flow) was applied on top of the wire. This was then
light polymerized for 40 s.
Group 7: The same protocol was followed as described for group 6 but a different
bonding agent (Heliobond, Ivoclar Vivadent; Schaan, Liechtenstein) and flowable
resin (Tetric Flow, Cavifill 210 A3, Ivoclar Vivadent) were used. Group 8: The same
materials were used as in group 7, but this time after bonding agent application,
Figure 4a: Schematic drawings of the cross-section of a specimen showing FRC or wire in relation to their application modes and the position of the shearing blade of the universal testing machine.
Figure 4b: Schematic drawings of the cross-section of a specimen in Group 6 showing wire in relation to their application modes and the position of the shearing blade of the universal testing machine.
Ena
mel
Fiber or Wire
Flowable composite
Shearing blade
Figure 3: Rectangular polyethylene mold (3.2x2.2x1.5 mm) used for positioning the retainer and the flowable resin in a controlled manner.
Ena
mel
Fiber or Wire
Flowable composite
Shearing blade
A B

42 43
Table 2: The mean (±standard deviations-SD) shear bond strength (MPa) values for the experimental groups. *The same letters indicate no significant differences (Tukey’s test, α=0.05).
Groups Mean (+SD) Homogeneous groups
1 6.9±2.2 B C
2 6.1±2.5 C
3 7.6±2.6 A B C
4 8.4±3.7 A B C
5 11.7±2.5 A B C
6 10.6±3.8 A B C
7 13±6.6 A B
8 14±6.7 A
Figure 5: Mean shear bond strength results per experimental group.
Failure TypesTable 3 presents the modes of failures for the FRC and stainless steel retainers
after debonding. Enamel fractures were slightly more frequent (5 out of 40) in
the FRC retainer groups than in the wire groups (2 out of 40). In none of the FRC
retainer groups were adhesive failures between the enamel and the composite
observed. Failure types varied within the FRC retainer groups. The most frequently
observed failure types were 1a (5/40) and 1b (17/40), where flowable composite
remained adhered to the enamel surface at varying degrees after debonding. This
failure type was followed by the cohesive failures within the FRCs, regardless
of their preimpregnation and texture (16/40). In the stainless steel wire groups,
when the retainer was applied on the bonding agent and then covered by
flowable resin (groups 6 and 7), partially attached composite was often found on
Failure AnalysisAfter debonding, the failure sites were examined by two calibrated operators (E.K.,
M.Ö.) both visually and using an optical microscope at different magnifications
(up to 40X). A scoring system was created for failure type evaluation considering
adhesive or cohesive failures at two interfaces, namely, enamel base/flowable
resin, base or covering flowable resin/FRC/wire retainer, as well as cohesive
failures within FRC or wire retainer.
Statistical AnalysisStatistical analysis was performed using Statistix 8.0 for Windows (Analytical
Software, Version 8.0, 2003; Tallahase,FL, USA). The means of each group were
analyzed with one-way ANOVA. Because of the significant group factor (p =
0.0011), multiple comparisons were made with the Tukey-Kramer adjustment test
to determine the significant differences between groups, where the dependant
variable was shear bond strength and the independent variable was various
combinations of application procedures and materials. P values less than 0.05
were considered to be statistically significant in all tests.
RESuLTS
Shear Bond StrengthThe results of the shear bond strength test for the FRC and stainless steel wire are
presented in Table 2 and Fig 5. One-way ANOVA showed a significant difference
between the groups (p = 0.0011).
Bond strength results did not significantly differ either between the FRC groups
(groups 1 to 4) (6.1 ± 2.5 to 8.4 ± 3.7 MPa) (p > 0.05) or the stainless steel wire
groups (groups 5 to 8) (10.6 ± 3.8 to 14 ± 6.7 MPa) (p > 0.05) (Tukey’s test).
Of the stainless steel wire groups, group 8 (14 ± 6.7 MPa) showed significantly
higher results than those of two FRC materials, namely group 1 (Angelus Fibrex
Ribbon) (6.9 ± 2.2 MPa) and group 2 (DentaPreg Splint) (6.1 ± 2.5 MPa) (p < 0.05).
Both E-glass or S2-glass FRC retainers (groups 1 to 3) did not show significant
differences compared to UHMWP FRC (group 4) (p > 0.05).
0
5
10
15
20
25
1 2 3 4 5 6 7 8
Shear Bond Strength (MPa)

44 45
compared to that of a commonly used stainless steel orthodontic wire.
Mean bond strength results did not significantly differ between the FRC groups,
although their compositions and textures were different. Except Ribbond,
the other FRC materials used were silanized, pre-impregnated glass FRCs.
Interestingly, between pre-impregnated glass FRCs and Ribbond, there were
no significant differences. In fact, preimpregnation of fibers not only improves
handling characteristics and enables a higher fiber volume, but also results in
improved adhesion because of the semi-IPN (interpenetrating polymer network)
structure of the polymer matrix.13 Based on this information, one could expect
more adhesive failures between the FRC and the flowable composite (failure
types 3 or 5, see Table 2); however these failure types were not observed with
the Ribbond fiber. The manufacturer of Ribbond suggests the use of any adhesive
monomer for its pre-impregnation. In this study, Stick Resin was used for pre-
impregnation. Apparently, this resin with a mixture of mono- and di-functional
methacrylates was sufficient to achieve good adhesion of the flowable resin to
the fibers.
The incidence of attached flowable composite on the enamel (failure types 1a
and 1b) after debonding was more frequent in group 3 (everStick Ortho) than
those of other groups, which indicates good adhesion compared to failure type
0. Although there were differences in terms of failure types, considering that
the mean bond strength values between the FRC retainer groups did not differ
significantly, the hypotheses could be partially rejected. The failure behavior of
FRC materials is very complex because of their anisotropic character.11,27,28,31
Laminated composites are known to have a relatively poor ability to absorb energy
due to local impact damage.33 For this reason, application of more fibers in a given
composite volume may change the load bearing capacity of the whole structure.
Clinically, however, this approach is not desirable and almost impossible; the
splint should be kept at minimum thickness in order to avoid bulky constructions
that may cause plaque accumulation and sometimes irritations for the tongue.
Static compression tests demonstrated that with the increasing fiber content, the
flexural strength increases linearly. 5,18 This information is often derived from bar-
shaped specimens prepared according to the ISO norms, where usually 2 mm of
veneering composite was placed on the FRC material. Considering the geometry
of the specimens prepared in this study, made to represent the clinical situation
as closely as possible, and the insignificant differences between the four FRC
materials, it can be stated that the adhesion of the flowable base composite is
also one of the predominant factors that play a role in the bond strength results.
On the other hand, considering the higher bond strength results obtained from
the stainless steel wire groups vs those of some FRCs tested, it appears that
the FRC actually weakens instead of strengthens the fiber/ composite complex.
It was expected that the FRC materials would show higher bond strengths
the enamel after debonding. When the retainers were embedded in the flowable
composite, the Heliobond + Tetric Flow group (group 8) showed more adhesive
failures between the enamel and the composite compared to group 5, where the
bonding agent was Stick Resin and the flowable composite was Stick Flow.
Table 3: Failure types and their distribution per experimental group for FRC or stainless steel wire retainers.
Groups Dislodged* Score of type of failures Cohesive enamel fracture
0 1a 1b 2 3 4 5
1 0 0 1 3 0 0 6 0 0
2 0 0 1 2 0 0 5 2 2
3 0 0 2 7 0 0 1 0 1
4 0 0 1 6 0 0 4 0 2
5 0 1 1 6 0 0 0 2 1
6 0 0 9 0 0 0 1 0 0
7 0 2 8 0 0 0 0 0 0
8 0 6 4 0 0 0 0 0 1
Score 0= no composite left on the enamel surfaceScore 1a= less than half of the composite left;Score 1b= more than half of the composite left;Score 2= cohesive failure within the base flowable resin; Score 3= all composite left on the enamel surface, with a distinct impression of theFRC/wire; Score 4= cohesive failure within the FRC separation/fracture of the wire; Score 5= adhesive failure between the FRC/wire and the covering flowable resin.*During thermocycling or testing.
DISCuSSION
Although much research is currently being conducted in diverse fields of FRC
applications in dentistry, very few studies have focused on the use of FRCs as
orthodontic retainers.6,11,25 High failure rates of bonded orthodontic post-treatment
stabilization splints have been reported,1-4 and therefore FRCs were considered
as possible alternative materials for such applications. Since debonding remains a
clinical problem, one aspect needing research was FRC bond strength to enamel
compared to conventional retainer material, which is generally stainless steel.
Therefore, in this study, adhesive aspects of several FRC retainer materials were

46 47
In the shear-peel tests, the cutting blade was placed between the tooth surface
and the flowable composite in such a manner that the cutting edge was as
close to the enamel surface as possible. One could assume that what is being
inadvertently measured is the adhesion of the composite rather than the effect
of the wire or fiber. In this study, however, there were no significant differences
between wire groups either when they were applied in the bed of flowable
composite (groups 5 and 8) or directly on the bonding agent (groups 6 and 7).
Furthermore, there were significant differences between some FRC groups
(groups 1 and 2) and all the wire groups (groups 5 to 8). This clearly indicates that
the debonding forces are diverted differently, regardless of whether there was
flowable composite on the bonded surface or not. The height of the specimens
was kept at 1.5 mm in order to achieve grasp of the blade in the universal testing
machine. This was determined during the preliminary experiments. In clinical
practice, this thickness may still be considered high. The dilemma remains of how
to control the thickness of the flowable composite in bonded retainers clinically.
It should also be emphasized that in shear bond strength tests, the adherend is
bonded to enamel surfaces that are not completely flat. Although an attempt
was made to control this by using lower central incisors which have relatively
more flat surfaces, the true shear stresses cannot be measured. Similarly lingual
retainers are placed on the lingual sufaces of the anterior teeth that present even
promounced concavity.
The mean bond strength values of the FRC retainers in this study (6.1 to 8.4
MPa) were lower than those reported in other studies (14 to 23 MPa).16,28,29
Several factors might have contributed to this result, such as application methods
and materials,26,29 the direction of the load on the fiber,12,13,29 and storage
conditions.16,28,29 Reynolds and von Fraunhofer24 reported that a minimum bond
strength of 6 to 8 MPa could give a satisfying clinical performance and successful
clinical bonding of brackets in orthodontics. The results obtained from the wire
retainers (10 to 14 MPa) exceed these recommended values. However, in this
study, specimens were thermocycled for 6000 cycles. It can be anticipated that
the temperature elevations and water uptake of the adhesive resin might result
in lower bond strength. Although the results obtained in all groups were within or
exceeded this range, the recommended bond strength values should be evaluated
with caution, because thermal or other types of aging procedures were not taken
into consideration.20-22,24 It should also be noted that the retainers are expected
to remain intact as long as possible after orthodontic treatment, whereas a
semi-permanent kind of adhesion is expected from the brackets. In this context,
perhaps recommended adhesion values to etched enamel should serve as the
golden standard, which is known to be on the order of 15 to 30 MPa.14,33 In that
respect, the bond strengths obtained in this study are not sufficient to function
as well as restorative composites. The occurrence of enamel fractures indicates,
than the wire, because the adhesive properties between the fiber and the
composite are chemical, contrary to those of the wire, which rely on mechanical
retention. Reports on the causes of failure of bonded orthodontic wire retainers
often indicate that the composite covering the wire is insufficient, resulting in
detachment of the wire.4 It was advised that by increasing the surface area
(diameter) of the wire3 or using less abrasive composite materials, debondings
could be avoided.4 However, Bearn et al4 found no significant difference in the
retention of differently shaped 3- and 6-stranded wires in a composite material.
In another study, insufficient composite thickness was reported to play a major
role in clinical failures.10 Due to this contradiction, in this study, the retainers were
completely covered with the flowable resin.
Comparative studies regarding the shear strength of FRCs incorporated into
particulate resin composites on enamel generally showed no difference when
compared to the control groups where no FRC was used.16,17 A significant increase
in shear strength was reported for some fibers,16 but other studies showed no
significant increase in shear bond strength.16,28,29 Meiers et al17 reported that
a nonimpregnated fiber, Connect (Kerr, Orange, CA, USA), showed higher
shear bond strengths than Ribbond (Seattle, WA, USA) and preimpregnated
unidirectional woven Splint-it (Jeneric/Pentron; Wallingford, CT, USA). In that
study, the specimens were thermocycled 1000 times. In an other study, Meiers
et al16 compared the same fiber materials and also found a significant increase
in the shear bond strengths to enamel with the use of Connect, while the other
fibers showed no significant difference compared to each other and the control
flowable composite (Tetric Flow) without a fiber. In contrast, another study28
found no significant differences between any groups when bond strengths of
EverStick and StickTech’s preimpregnated FRCs that were applied either directly
on a bed of flowable composite (Tetric Flow) or in combination with particulate
filler composite (Filtek Z250) on human enamel were compared. The addition of
flowable composite did not improve bond strength values. It was also found that
the addition of bidirectional or random continuous fibers (StickNet, everStickNet,
and an experimental random FRC) did not yield any significant improvement
in bond strength to enamel and dentin compared to the control of particulate
filler composite (Filtek Z250).29 In these studies, composites covering the fibers
were 4 to 5 mm thick. Therefore, a different effect of reinforcement and crack
propagation could be expected than in this study.
It should also be emphasized that in shear bond strength tests, the adherend is
bonded to enamel surfaces that are not completely flat. Although an attempt was
made to control this by using mandibular central incisors which have relatively
more flat surfaces, the true shear stresses cannot be measured. Similarly, lingual
retainers are placed on the lingual surfaces on the anterior teeth that present even
more pronounced concavity.

48 49
Conclusions
1. Bond strength results did not significantly differ either between the FRC
groups or the stainless steel wire groups. Only group 8, in which Heliobond
and Tetric Flow were used and the wire was placed in the bed of the flowable
resin, showed significantly higher mean bond strengths than those of
DentaPreg Splint and Angelus Fibrex Ribbon.
2. Preimpregnated and custom impregnated FRC materials performed the
same in terms of bond strength.
3. Changing the application mode of wire retainers did not result in significant
changes in bond strength, but the failure modes showed variations between
the experimental groups.
Clinical relevanceRegardless of their application mode, stainless steel orthodontic bonded retainers
delivered higher bond strengths than those of fiber retainers but the failure types
varied between the tested materials.
Acknowledgements We express our appreciation to the ADM a.s., Brno, Czech Republic, Ribbond
Inc., Seattle, USA, and Angelus® Dental Solutions, Brazil for donation of some of
the fiber materials used in this study.
however, that the adhesion exceeded the cohesive strength of the enamel itself
in some cases in the FRC groups (5 enamel fractures out of 40 specimens).
Enamel fractures may present a clinical problem during bracket debonding. Yet
for lingual retainers, from which retention is desired to maintain the achieved
orthodontic result for a long time, this aspect would not be considered a problem.
Nonetheless, one could speculate that the failure is not only a result of adhesion
or bond strength. After orthodontic treatment, when the teeth tend to revert to
their original position, the interfacial forces might exceed the adhesive strength
of the flowable composite to the tooth surface. In this case, variations between
the flowable composites may affect the results. However, in this study, wire
retainers bonded with either StickFlow or Tetric Flow composites presented no
significant differences (groups 5 to 8). Although the results were higher (but not
significantly), the group in which Heliobond was used as a bonding agent showed
more adhesive failures (failure type 0) when compared to StickResin. This may
be due to 2,2-bis[4-(2- hydroxy-3-methacryloxyropoxyl)]-phenonylpropane in the
composition of the latter that might have better surface wettability properties.
In one clinical study by Rose et al,25,20 patients were randomly assigned to receive
Ribbond fiber or multistranded wire retainers from canine to canine following
the completion of orthodontic treatment. The retainers remained in place for
an average of 11.5 and 23.6 months, respectively, with a statistically significant
difference. This limited clinical evidence indicates that the multistranded
wire is superior to the plasma-treated woven polyethylene ribbon, which is a
nonpreimpregnated fiber. Nevertheless, both retainers presented unacceptable
survival rates. Therefore, it can be concluded that orthodontists are still confronted
with debonding of bonded retainers.
Fixed lingual retainers connect at least two teeth and are therefore certainly longer
than 3 mm. One limitation of this study could be short length of the retainer
compared to the clinical situation. Adhesion tests require some standardization
before complex situations can be tested. Hence, this study solely dealt with the
adhesive properties of various fibers placed at different locations and in different
manners. Other factors, such as length and curvature of the teeth, had to be
excluded in order to isolate the effect of the retainer type and location on the
bond results. Because no significant difference has been found between bonding
results to buccal and lingual surfaces,8,35 the attempt was made to eliminate
the convexity factor by using only the labial surfaces of the teeth for adhesion
purposes.
Under the influence of compressive cyclic stresses, the damage associated with
delamination may reduce the overall stiffness as well as the residual strength,
leading to structural failure. The behavior of FRC and metal wires under fatigue
conditions is being investigated in our laboratories.

5150
17. Meiers JM, Kazemi RB, Freilich MA. Direct intra-oral applications of fiber-reinforced composites. The influence of FRC on particulate resin composite to enamel shear bond strengths. In: Vallitu PK, editor. The Second International Symposium on Fiber-Reinforced Plastics in Dentistry, 10-13 October, Nijmegen, The Netherlands. University of Turku Publishing Office, 2001.
18. Narva KK, Lassila LV, Vallittu PK. The static strength and modulus of fiber reinforced denture base polymer. Dent Mater 2005;21:421-428.
19. Nohrström TJ, Vallittu PK, Yli-Urpo A. The effect of placement and quantity of glass fibers on the fracture resistance of interim fixed partial dentures. Int J Prosthodont 2000;13:72-78.
20. Øilo G. Bond strength testing, what does it mean? Int Dent J 1993;43:492-498.
21. Özcan M, Pfeiffer P, Nergiz. A brief history and current status of metal/ceramic surface conditioning concepts for resin bonding in dentistry. Quintessence Int 1998;29:713-724.
22. Pickett KL. In vivo orthodontic bond strength: comparison with in vitro results. Angle Orthodont 2001;71:141-148.
23. Reynolds IR. A review of direct orthodontic bonding. Br J Orthod 1975;2:171-178.
24. Reynolds IR, Von Fraunhofer JA. Direct bonding in orthodontic attachments to teeth: the relation of adhesive bond strength to gauze mesh size. Brit J Orthodont 1975;3:91-95.
25. Rose E, Frucht S, Jonas IE. Clinical comparison of a multistranded wire and a direct-bonded polyethylene ribbon reinforced resin composite used for lingual retention. Quintessence Int 2002;33:579-583.
26. Scribante A, Cacciafesta V, Sfondrini MF. Effect of various adhesive systems on the shear ond strength of fiber-reinforced composite. Am J Orthod Dentofacial Orthop 2006;130:224-227.
27. Takagi K, Fujimatsu H, Usami H, Ogasawara S. Adhesion between high strength and high modulus polyethylene fibers by use of polyethylene gel as an adhesive. J Adhesion Sci Technol 1996;9:869-882.
28. Tezvergil A, Lassila LVJ, Vallitu PK. Strength of adhesive-bonded fiber-reinforced composites to enamel and dentin substrates. J Adhesive Dent 2003;5:301-311.
29. Tezvergil A, Lassila LVJ, Vallitu PK. The shear bond strength of bidirectional and random-oriented fiber-reinforced composite to tooth structure. J Dent 2005;33:509-516.
30. Vallittu PK. Glass fiber reinforcement in repaired acrylic resin removable dentures: preliminary results of a clinical study. Quintessence Int 1997;28:39-44.
31. Vallitu PK. The effect of glass fiber reinforcement on the fracture resistance of a pro-visional fixed partial denture. J Prosthet Dent 1998;79:125-130.
32. Vallitu PK. Strength and interfacial adhesion of FRC-tooth system. In: Vallitu PK, editor. The Second International Symposium on Fiber-Reinforced Plastics in Dentistry, 10-13 October, Nijmegen, The Netherlands. University of Turku Publishing Office, 2001. p.2-28.
REFERENCES
1. Andrén A, Asplund J, Azarmidohkt E, Svensson R, Varde P, Mohlin B. A clinical evaluation of long term retention with bonded retainers made from multi-strand wires. Swed Dent J 1998;22:123-131.
2. Årtun J, Spadafora A, Shapiro P. A 3-year follow-up study of various types of orthodontic canine-to-canine retainers. Eur J Orthod 1997;19:501-509.
3. Bearn DR. Bonded orthodontic retainers: a review. Am J Orthod Dentofacial Orthop 1995;108:207-213.
4. Bearn DR, McCabe JF, Gordon PH, Aird JC. Bonded orthodontic retainers: The wire-composite interface. Am J Orthod Dentofacial Orthop 1997;111:67-77.
5. Behr M, Rosentritt M, Lang R, Handel G. Flexural properties of fiber reinforced composite using a vacuum/pressure or a manual adaptation manufacturing process. J Dent 2000; 28: 509-514.
6. Cacciafesta V, Sfondrini MF, Lena A, Scribante A, Vallittu PK, Lassila LV. Flexural strengths of fiber-reinforced composites polymerized with conventional light-curing and additional postcuring. Am J Orthod Dentofacial Orthop 2007;132:524-527.
7. Dahl E, Zachrisson BU. Long term experience with direct bonded lingual retainers. J Clin Orthod 1991;25:619-630.
8. Tüfekçi E, Almy DM, Carter JM, Moon PC, Lindauer SJ. Bonding properties of newly erupted and mature premolars. Am J Orthod Dentofacial Orthop 2007;131:753-758.
9. Freilich MA, Meiers JC, Duncan JP, Goldberg AJ. Fiber-reinforced composites in clinical dentistry. Chicago: Quintessence Pub; 1999. p.9-21.
10. Gutteridge DL. Reinforcement of poly(methyl methacrylate) with ultrahigh-modulus polyethylene fiber. J Dent 1992;20:50-54.
11. Karaman A., Kir N, Belli S. Four applications of reinforced polyethylene fiber material in orthodontic practice. Am J Orthod Dentofacial Orthop 2002;121:650-654.
12. Lassila LV, Tezvergil A, Dyer SR, Vallitu PK. The bond strength of particulate filler composite to differently oriented fiber-reinforced composite substrate. J Prosthodont 2007;16:10-17.
13. Lastumaki TM, Kallio TT, Vallitu PK. The bond strength of light-curing composite resin to finally polymerized and aged glass fiber-reinforced composite substrate. Biomat 2002;23:4533-4639.
14. Latta MA, Barkmeier WW. Dental adhesives in contemporary restorative dentistry. Dent Clin North Am 1998;42:567-577.
15. Lie Sam Foek DJ, Özcan M, Verkerke GJ, Sandham A, Dijkstra PU. Survival of bonded stainless steel lingual retainers: A historic cohort study. Eur J Orthod 2008;30:199-204.
16. Meiers JC, Kazemi RB, Donadio M. The influence of fiber reinforcement of composites on shear bond strengths to enamel. J Prosthet Dent 2003;89:388-393.

52 53
33. Van Meerbeek B, Perdigao J, Lambrechts P, Vanherle G. The clinical performance of adhesives. J Dent 1998;26:1-20.
34. Wang J, Crouch SL, Mogilevskaya SG. Numerical modelling of the elastic behaviour of fiber-reinforced composites with inhomogeneous interphases. Compos Sci Technol 2006;66:1-18.
35. Wang WN, Tarng TH, Chen YY. Comparison of bond strength between lingual and buccal surfaces on young premolars. Am J Orthod Dentofacial Orthop 1993;104:251-253.
36. Zachrisson BU, Büyükyilmaz T 2005 Bonding in Orthodontics. In Graber L W (ed): Orthodontics: Current principles and techniques. Mosby, St. Louis, 4th p. 621-659.

Chapter 4
Fatigue resistance, debonding force, and failure type of fiber-reinforced composite, polyethylene ribbon-reinforced, and braided stainless steel wire lingual retainers in vitro
Lie Sam Foek D.J.
Yetkiner E
Özcan M
Korean J Orthod. 2013 Aug;43(4):186-92.

56 57
INTRODuCTION
Lingual retainers are generally used for long-term retention.1 They are preferred
particularly when the post treatment intercanine width should be maintained and
periodontal tissue support is lacking.1,2 However, breakage of the retainer material
and debonding of the resin pad that attaches the retainer onto the tooth surface
are commonly experienced in clinical practice.2-5 The main factors determining
the longevity and success of lingual retainers are the type of retainer material,
type of composite resin used for bonding, number of units included for bonding,
and location of the retainer (i.e., maxillary or mandibular arch).2-5
The most frequently used retainer material is stainless steel wire, with varying
stiffness and integral properties.2,5 Initially, lingual retainers were fabricated from
relatively thick round wires (0.030 - 0.032 inch) bonded only to the ends of the
retention area.3,4 With this type of retainer, the intercanine width could be well
preserved and the retention area was easily accessible to oral hygiene instruments,
but rotation of the interlying teeth was evident because they were not bonded
to the retainer. Thinner multistranded wire (0.0195 - 0.0215 inch) bonded to each
interlying tooth was introduced to overcome this problem.3,4 However, this retainer
type increased the susceptibility to plaque accumulation and presented higher
failure rates due to wire breakage and resin pad detachment.2,5 Subsequently,
fiber-reinforced composite (FRC) was introduced to replace stainless steel wire,
thus allowing chemical adhesion of the retainer to the bonding agent.6 FRC
was expected to reinforce the resistance of the bonding agent by transferring
the loads acting on the retainer complex to the glass fibers. Furthermore, the
bonding interface of two materials with different physical properties (i.e., wire
and composite resin) would be eliminated.6,7 Nevertheless, retainer failures still
occurred and clinical survival studies did not reveal significant results. Therefore,
multistranded stainless steel wire is still the most frequently used material for
lingual retainers.1,2,5
The causes of lingual retainer failures are still not clear. The most frequent problems
of metal retainers are failure of the wire-composite interface, breakage of the
wire, and detachment of the resin pads at the composite-enamel interface.1-4,7
Wire-composite interface failure is attributable to two main factors. First, the
composite covering the retainer, usually a small resin pad, becomes thinner and
weaker because of abrasion caused by brushing and food consumption. This, in
turn, results in detachment of the retainer from the resin pad, which stays stable
on the tooth surface.1-4,7 Second, propagation of internal cracks due to constant
movement of the retainer between the overlying and the underlying resin pads
during physiological tooth movement is linked to wire-composite interface
failure.1,2,7 This is also a possible reason for breakage of the retainer due to the
stress accumulation at bending points.3,4 On the other hand, composite-enamel
ABSTRACT
Objective: To analyze the fatigue resistance, debonding force, and failure type of
fiber-reinforced composite, polyethylene ribbon-reinforced, and braided stainless
steel wire lingual retainers in vitro.
Methods: Roots of human mandibular central incisors were covered with silicone,
mimicking the periodontal ligament, and embedded in polymethylmethacrylate.
The specimens (N = 50), with two teeth each, were randomly divided into five
groups (n = 10/ group) according to the retainer materials: (1) Interlig (E-glass),
(2) everStick Ortho (E-glass), (3) DentaPreg Splint (S2-glass), (4) Ribbond
(polyethylene), and (5) Quad Cat wire (stainless steel). After the recommended
adhesive procedures, the retainers were bonded to the teeth by using flowable
composite resin (Tetric Flow). The teeth were subjected to 10,00,000 cyclic loads
(8 Hz, 3 - 100 N, 45o angle, under 37 ± 3°C water) at their incisoproximal contact,
and debonding forces were measured with a universal testing machine (1 mm/
min crosshead speed). Failure sites were examined under a stereomicroscope
(×40 magnification). Data were analyzed by one-way analysis of variance.
Results: All the specimens survived the cyclic loading. Their mean debonding
forces were not significantly different (p > 0.05). The DentaPreg Splint group (80%)
showed the highest incidence of complete adhesive debonding, followed by the
Interlig group (60%). The everStick Ortho group (80%) presented predominantly
partial adhesive debonding. The Quad Cat wire group (50%) presented overlying
composite detachment.
Conclusions: Cyclic loading did not cause debonding. The retainers presented
similar debonding forces but different failure types. Braided stainless steel wire
retainers presented the most repairable failure type.
Key words: Lingual, Bonding, Relapse, Retention

58 59
MATERIALS AND METHODS
Specimen preparation One hundred caries-free human mandibular central incisors stored in 0.1% thymol
solution at 40C up to 6 months were selected under blue-light transillumination to
ensure that the enamel was free of cracks. The roots of pairs (i.e., right and left)
of the selected teeth were dipped in hot liquid wax (Modern Materials utility wax;
Heraeus Kulzer GmbH, Hanau, Germany) and embedded in silicone impression
material (Adisil® blau 9:1; Böhme & Schöps GmbH, Goslar, Germany) in a plastic
mold with axial contact. After the impression material had set, the same process
was repeated with polymethylmethacrylate (Vertex 2 SMS, 24 × 24 × 33 mm;
Vertex-Dental B.V., Zeist, The Netherlands). The wax layer was removed with hot
water (100oC) and the created space was filled with light-body silicone (Pro Fill;
Heraeus Kulzer GmbH) to mimic the periodontal ligament, supposedly allowing
some physiological movement during cyclic loading.19,20 The roots of the teeth
were then inserted into the silicone (Figure 1). Fifty specimens, each containing a
pair of incisors, were used for the experiments.
Figure 1: Representative photographs of human mandibular central incisor pairs embedded in polymethylmethacrylate up to the cementoenamel junction to receive bonded lingual retainers: a, lingual and b, proximal views.
Before the bonding procedures, the lingual surfaces of the embedded teeth were
polished with fluoridefree pumice (Zircate Prophy Paste; Dentsply Caulk, Milford,
DE, USA) by using a prophylaxis brush (Hawe Prophy Cup and Brush, latch-type;
Kerrhawe Sa, Bioggio Svizzera, Switzerland) for 20 seconds, rinsed with water,
and air-dried. The mesiodistal dimensions of the two teeth in each specimen
were measured and the midpoint 3 mm below the incisal edges was marked as
the area for bonding by using a permanent marker.
interface failure is attributable to adhesion failure of the resin pad. Debonding of
the resin pad from the tooth surface is mostly associated with deficient bonding
procedures, such as inadequate moisture control or mishandling of the resin
material.1,3,7 Furthermore, increased tooth mobility due to a widened periodontal
ligament space or lack of bone support could cause deterioration of the adhesion
at the composite-enamel interface.1
The in vivo failure and survival rates of lingual retainers, in vitro testing of different
retainer material complexes, and interpretation of the results are highly con
troversial.5,8,16 In a recent clinical report of metal and FRC retainers, the conventional
multistranded wire retainers were suggested to remain the gold standard for
orthodontic retention and the use of FRC retainers was discouraged because
of their high failure rate (12% vs 51%, respectively).14 Similarly, multistranded
wire retainers were reported to be significantly superior to polyethylene ribbon-
reinforced retainers.13 On the other hand, a recent 6-year clinical follow-up
study showed no significant differences between FRC and multi stranded wire
retainers; the results indicated that FRC retainers could be a viable alternative to
multistranded wire retainers.15 Two recent clinical studies showed a 37.9% failure
rate in a 6-month period with multi stranded wire retainers11 and a 94.8% survival
rate in a 4.5-year period with FRC retainers.16 From the adhesion perspective, the
debonding force of FRC retainers was not found to be dependent on the type of
bonding agent used.17 Contrarily, superior adhesion has been reported with the
use of a specific lingual retainer adhesive instead of a flowable composite resin.18
The disagreement among such studies is highlighted in a review by Littlewood et
al.,5 implying that further research for retainer comparisons is necessary.17
The objective of this in vitro study was to analyze the fatigue resistance,
debonding force, and failure type of FRC, polyethylene ribbon-reinforced, and
braided stainless steel wire lingual retainers. The null hypotheses were that the
fatigue resistance of the FRC and polyethylene ribbon-reinforced retainers would
not be greater and their debonding forces would not be higher than those of the
braided stainless steel wire retainer.
A B

60 61
debonding occurred. Only the maximum force causing debonding of the retainers
was recorded.
Table 1: Details of the retainer materials tested in this study (GMA, Glycidyl methacrylate; PMMA, polymethyl methacrylate).
Codes Composition Manufacturer Batch No.
Interlig ANG E-glass, bis-GMA Angelus, Londrina, Brazil 2199
everStickOrtho
EST E-glass, PMMA, bis-GMA
StickTech Ltd, Turku, Finland
000088
DentaPregSplint
DTP S2-glass, mixture of dimethacrylate initiators and stabilizers
ADM a.s., Brno, Czech Republic
4742
Ribbond RIB Ultra High Molecular Weight Polyethylene
Ribbond Inc., Seattle, USA
9543
Quad Cat Wire
QC Stainless steel, three-strand twisted wire 0.022” x 0.016
Quad Cat, GAC International, New York, USA
0197
Failure analysisFailure sites were examined under a stereomicroscope at varying magnifications
(up to ×40). After the initial evaluation of the specimens, four types of failure were
categorized, as follows: type 1, complete adhesive debonding of the retainer from
the tooth surface; type 2, partial adhesive detachment of the retainer from one
of the teeth; type 3, retainer did not debond from the tooth surface but fractured;
and type 4, retainer did not debond from the tooth surface but the overlying
composite detached.
Retainer materialsThe specimens were randomly divided into five groups (n = 10 per group)
according to the main retainer materials: (1) E-glass (Interlig; Angelus Ltd.,
Londrina, Brazil), (2) E-glass (everStick Ortho; Stick Tech Ltd., Turku, Finland), (3)
S2-glass (DentaPreg Splint; ADM a.s., Brno, Czech Republic), (4) polyethylene
(Ribbond; Ribbond Inc., Seattle, WA, USA), and (5) stainless steel (Quad Cat wire;
GAC International Inc., Islandia, NY, USA).
Retainer placementBraided stainless steel wires (0.022 × 0.016 inch) were adapted to the lingual
surfaces of the teeth in each specimen and ultrasonically cleaned in ethyl alcohol
(Vitasonic; Vita Zanhfabrik H. Rauter GmbH & Co. KG, Bad Säckingen, Germany)
for 20 seconds. The marked bonding area was then etched with 38% H3PO4
(Top Dent; DAB Dental, Tillverkare, Sweden) for 20 seconds, rinsed with water
for 20 seconds, and air-dried. An adhesive resin (Heliobond; Ivoclar Vivadent,
Schaan, Liechtenstein) was applied by using a microbrush (ApplyTip; Hager &
Werken, Oisterwijk, The Netherlands), gently air-blown, and photo-polymerized
for 20 seconds on each tooth surface with an LED polymerization lamp (Ortholux
LED curing light, light output = 400 mW/ cm2; 3M Unitek, Landsberg am Lech,
Germany). A thin layer of flowable composite resin (Tetric Flow, Cavifill 210, shade
A3; Ivoclar Vivadent) was applied and the retainer was placed in the composite
resin. After initial polymerization, the composite resin was applied to cover the
retainer surface and photo-polymerized for 40 seconds on each tooth surface.
The irradiation distance between the light-source tip and the resin surface was
maintained at 2 mm.
Retainers fabricated from standard lengths of the FRCs and polyethylene ribbon
were bonded in exactly the same manner as described for the stainless steel wire
retainers.
The brand names, abbreviations, compositions, manufacturer details, and batch
numbers of the tested materials are listed in Table 1.
Cyclic loading and debonding force testing The specimens were subjected to 10,00,000 cyclic loading. The load was applied
at the incisoproximal contact of the tooth pair from the lingual side to the labial side
by using a jig (Figure 2). The force vector formed an approximately 450 angle with
the long axis of the tooth pair. The load frequency was 8 Hz and alternated from 3
N to 100 N. The specimens were kept in 37 ± 30C water during the procedure.21
Following fatigue formation, the specimens were tested for the debonding force
by using a universal testing machine (Z2.5MA, 18-1-3/7; Zwick GmbH & Co. KG,
Ulm, Germany) at a crosshead speed of 1 mm/min. The debonding force was
applied with the same settings and jig as in the cyclic loading experiment until
Figure 2: The loading jig used for measuring the debonding force of the bonded lingual retainers.

62 63
Table 2: Frequencies (%) of failure of the bonded lingual retainers subjected to cyclic loading.
Retainer Type 1 Type 2 Type 3 Type 4 Dislodged*
ANG 60 - 30 0 10
EST 20 80 0 0 -
DTP 80 20 0 0 -
RIB 50 - 40 0 10
QC 20 10 0 50 20
Type 1: complete adhesive debonding of the retainer from the tooth surface; Type 2: partial adhesive detachment of the retainer from one of the teeth; Type 3: retainer did not debond from the tooth surface but fractured; Type 4: retainer did not debond from the tooth surface but the overlying composite detached.
See Table 1 for detailed description of the groups. *Each specimen consisted of a pair of teeth
DISCuSSION
In this study, none of the retainers failed during cyclic loading and all the tested
materials showed similar debonding forces. However, their failure types varied.
The null hypotheses that the fatigue resistance of the FRC and polyethylene
ribbon-reinforced retainers would not be superior to that of the stainless steel
wire retainer and they would not have higher debonding forces were accepted.
Under clinical conditions, lingual retainers are subjected to cyclic stresses
because of mastication, occlusion, and intraoral habits.22-24 This repeated sub-
critical loading induces fatigue and may cause partial or total failure of one or
more components of the retainer complex. These forces are usually below the
maximum debonding forces in in vitro studies, but they may have the destructive
effect of high-magnitude sudden impacts that seldom occur in real life.22-24
Therefore, fatigue tests are expected to clarify the clinical durability better than
static tests.22-24 However, the degree of fatigue necessary to induce failure in
initially intact specimens cannot be easily predicted.
The two main factors determining the effect of fatigue on composite materials
are (1) the factors associated with the cyclic load (i.e., quantity, magnitude, and
direction of load application) and (2) the factors associated with the test material
(e.g., type of rein forcement, filler-matrix ratio, and interfacial strength). The
cyclic load quantity in previous fatigue studies ranged from 20,000 to 2,000,000,
showing great variation.7,24 Supposedly, 2,000,000 cycles correspond to approxi-
mately 4 years of normal occlusal and masticatory activities.24 Although merely
an estimation, 1,000,000 cycles, as applied in this study, would correspond to
approximately 2 years of clinical service. This quantity was used on the basis of
Statistical analysis Statistical analysis was performed by using Statistix 8.0 for Windows (Analytical
Software Inc., Tallahassee, FL, USA). Means were analyzed by one-way analysis
of variance (ANOVA). p -values less than 0.05 were considered significant.
RESuLTS
All the specimens survived the cyclic loading. The mean debonding forces were
706 ± 312 N, 772 ± 348 N, 830 ± 258 N, 731 ± 329 N, and 670 ± 323 N in the
Interlig, everStick Ortho, DentaPreg Splint, Ribbond, and Quad Cat wire groups,
respectively, without significant differences ( p > 0.05) (Figure 3).
According to the failure analysis, the highest incidence of type 1 failure occurred
in the DentaPreg Splint group (eight specimens) followed by the Interlig group (six
specimens). The everStick Ortho group presented predominantly type 2 failure
(eight specimens) and the Quad Cat wire group showed type 4 failure in five
specimens (Table 2)
.
Figure 3: Mean and standard deviation of the debonding force of the bonded lingual retainers. See Table 1 for a detailed description of the groups.

64 65
that the same bonding agent was used in all the groups, this failure type indicates
that the interfacial strength between the tested material and the bonding resin
exceeded the adhesion between the bonding resin and enamel. In contrast,
the everStick Ortho retainers (80%) presented partial adhesive debonding
from one of the teeth. The Ribbond retainers presented adhesive failure and
material breakage in 50% and 40% of the specimens, respectively. Resin
adhesion to polyethylene FRCs was less favorable in previous in vitro studies
mainly because of the difficulty in plasma coating, silanization, and impregnation
of the polyethylene fibers.7 Such combinations of failure types may not cause
direct enamel damage but will necessitate removal of the attached retainers by
using rotary instruments and renewal of the bonding procedure. The potential
detrimental effects of debonding a retainer from enamel during either bracket
debonding or retainer removal present an iatrogenic problem. Therefore, all these
material options cannot be considered durable and favorable.
The Quad Cat wire group presented type 4 failure in 50% of the specimens.
This result implies that either the adhesion at the composite-enamel interface
was superior to the adhesion at the composite-wire interface or the cyclic
load weakened the latter. This type of failure could surely allow repair of the
detached composite part without removal of the remnants. Therefore, it could
be considered a reversible situation and perhaps more favorable than the other
failure types. Reinforcement of the composite in the other materials might have
been accomplished, but the lack of flexibility eventually led to different failure
types in the Quad Cat wire group.
Conclusions
1. Fatigue created by cycling loading did not cause failure of the lingual retainer
materials tested.
2. All the tested materials performed similarly in terms of the debonding force
following fatigue formation.
3. The failure types varied among the materials. The braided stainless steel wire
retainer presented the most repairable failure type.
AcknowledgementWe would like to acknowledge mr. Anne Wietsma for preparing the specimen
molds, Mrs. Graciela Galhano for her assistance with the cyclic loading
experiments and K.G. Bijlstra Stichting for their financial support to purchase the
materials used in the study.
the outcomes of clinical studies in which retainer failures due to debonding were
reported within this period.2-4,9 Another factor affecting fatigue formation is the
magnitude of the load acting on the test material. In previous studies, constant
or varying forces between 40 and 600 N were applied.21-25 In the present study, a
load ranging from 3 N to 100 N was applied at a frequency of 8 Hz. In reality, the
applied force is considered zero in the absence of occlusal contact or function;
however, to maintain the contact of the load cell on the specimen, 3 N was
applied as the minimum load. Nevertheless, a standard method for fatigue tests
has not been established, because chewing cycles vary in every individual as well
as experimental settings. Therefore, these tests still present limitations and their
outcomes should be interpreted with caution.
The adverse effect of fatigue on materials with similar physical properties is more
predictable, because cyclic loading will have an equal impact on them.21-25 Therefore,
elimination of wires in the retainer complex by using FRC might improve stability
and reduce fatigue formation, because adhesion would rely only on bonding of
the flowable composite resin or resin matrix of the FRC to the etched enamel.
However, in the present study, none of the retainers failed during fatigue formation
and no significant differences were observed in terms of the debonding force.
These results are attributable to the specimen properties, where only two units
were included, forming a very short retainer complex compared with that used
clinically. However, the cyclic load could not be applied on 4- or 6-unit retainer
specimens because of the experimental settings and design.
From the chemical perspective, hydrolysis, which can break the covalent bonds
in the resin,25 and plasticization, which can diminish the mechanical resistance
of the polymer,26 were possibly not effective enough to cause failure during
fatigue formation. This lack of an effect might be attributable to the relatively
stable water temperature (37 ± 30C) in which the specimens were kept during
fatigue formation; clinically, higher temperatures are encountered. Future studies
should incorporate temperature alterations in the fatigue formation procedures
for testing lingual retainers.
The lack of debonding during cyclic loading and the insignificant difference in
the debonding forces of the retainers may initially suggest that all the tested
materials behaved similarly. Interestingly, even the stainless steel wire retainer,
with its smaller bonding area than that of the FRC retainers, demonstrated a
similar debonding force. The extent of fatigue created in this design cannot be
determined, and the failure types deserve more attention than the performance
of the tested materials. The failure types should be evaluated with regard to not
only the adhesion quality but also the clinical reversibility, with the least damage
to enamel during removal or repair of the failed retainer. The FRC retainers
themselves showed various failure types. Those composed of Interlig (60%) and
DentaPreg Splint (80%) mainly presented complete adhesive debonding. Given

66 67
16. Kumbuloglu O, Saracoglu A, Özcan M. Pilot study of unidirectional E-glass fibre-reinforced composite resin splints: up to 4.5-year clinical follow-up. J Dent 2011;39:871-7.
17. Meiers JC, Kazemi RB, Donadio M. The influence of fiber reinforcement of composites on shear bond strengths to enamel. J Prosthet Dent 2003;89:388- 93.
18. Scribante A, Cacciafesta V, Sfondrini MF. Effect of various adhesive systems on the shear bond strength of fiber-reinforced composite. Am J Orthod Dentofacial Orthop 2006;130:224-7.
19. Fokkinga WA, Le Bell AM, Kreulen CM, Lassila LV, Vallittu PK, Creugers NH. Ex vivo fracture resistance of direct resin composite complete crowns with and without posts on maxillary premolars. Int Endod J 2005;38:230-7.
20. Özcan M, Valandro LF. Fracture strength of endodontically- treated teeth restored with post and cores and composite cores only. Oper Dent 2009;34:429- 36.
21. Baldissara P, Özcan M, Melilli D, Valandro LF. Effect of cyclic loading on fracture strength and microleakage of a quartz fiber dowel with different adhesive, cement and resin core material combinations. Minerva Stomatol 2010;59:407-14.
22. McCabe JF, Carrick TE, Chadwick RG, Walls AW. Alternative approaches to evaluating the fatigue characteristics of materials. Dent Mater 1990;6:24- 8.
23. Ruse ND, Shew R, Feduik D. In vitro fatigue testing of a dental bonding system on enamel. J Biomed Mater Res 1995;29:411-5.
24. Grandini S, Chieffi N, Cagidiaco MC, Goracci C, Ferrari M. Fatigue resistance and structural integrity of different types of fiber posts. Dent Mater J 2008; 27:687-94.
25. Sahafi A, Peutzfeldt A, Ravnholt G, Asmussen E, Gotfredsen K. Resistance to cyclic loading of teeth restored with posts. Clin Oral Investig 2005;9:84-90.
26. De Munck J, Van Landuyt K, Peumans M, Poitevin A, Lambrechts P, Braem M, et al. A critical review of the durability of adhesion to tooth tissue: methods and results. J Dent Res 2005;84:118-32.
REFERENCES
1. Renkema AM, Renkema A, Bronkhorst E, Katsaros C. Long-term effectiveness of canine-to-canine bonded flexible spiral wire lingual retainers. Am J Orthod Dentofacial Orthop 2011;139:614-21.
2. Bearn DR. Bonded orthodontic retainers: a review. Am J Orthod Dentofacial Orthop 1995;108:207-13.
3. Dahl EH, Zachrisson BU. Long-term experience with direct-bonded lingual retainers. J Clin Orthod 1991; 25:619-30.
4. Artun J, Spadafora AT, Shapiro PA. A 3-year followup study of various types of orthodontic canine-tocanine retainers. Eur J Orthod 1997;19:501-9.
5. Littlewood SJ, Millett DT, Doubleday B, Bearn DR, Worthington HV. Orthodontic retention: a systematic review. J Orthod 2006;33:205-12.
6. Burstone CJ, Kuhlberg AJ. Fiber-reinforced composites in orthodontics. J Clin Orthod 2000;34:271-9.
7. Foek DL, Özcan M, Krebs E, Sandham A. Adhesive properties of bonded orthodontic retainers to enamel: stainless steel wire vs fiber-reinforced composites. J Adhes Dent 2009;11:381-90.
8. Lumsden KW, Saidler G, McColl JH. Breakage incidence with direct-bonded lingual retainers. Br J Orthod 1999;26:191-4.
9. Lie Sam Foek DJ, Özcan M, Verkerke GJ, Sandham A, Dijkstra PU. Survival of flexible, braided, bonded stainless steel lingual retainers: a historic cohort study. Eur J Orthod 2008;30:199-204.
10. Lee KD, Mills CM. Bond failure rates for V-loop vs straight wire lingual retainers. Am J Orthod Dentofacial Orthop 2009;135:502-6.
11. Taner T, Aksu M. A prospective clinical evaluation of mandibular lingual retainer survival. Eur J Orthod 2012;34:470-4.
12. Cooke ME, Sherriff M. Debonding force and deformation of two multi-stranded lingual retainer wires bonded to incisor enamel: an in vitro study. Eur J Orthod 2010;32:741-6.
13. Rose E, Frucht S, Jonas IE. Clinical comparison of a multistranded wire and a direct-bonded polyethylene ribbon-reinforced resin composite used for lingual retention. Quintessence Int 2002;33:579-83.
14. Tacken MP, Cosyn J, De Wilde P, Aerts J, Govaerts E, Vannet BV. Glass fibre reinforced versus multistranded bonded orthodontic retainers: a 2 year prospective multi-centre study. Eur J Orthod 2010; 32:117-23.
15. Bolla E, Cozzani M, Doldo T, Fontana M. Failure evaluation after a 6-year retention period: a comparison between glass fiber-reinforced (GFR) and multistranded bonded retainers. Int Orthod 2012; 10:16-28.

Chapter 5
Clinical survival of multi-stranded stainless steel bonded lingual retainers as a functionof resin composite type: Up to 3.5 years follow-up
Lie Sam Foek D.J.
Feilzer A.J.
Özcan M
Submitted to: American Journal of Orthodontics and Dentofacial Orthopedics, 2017.

70 71
INTRODuCTION
After an orthodontic treatment, it is essential to maintain and stabilize the
achieved result as long as possible.1,2 In the absence of retention, after 10 to 20
years 40 to 90% relapse could be expected.1,3,4 Since the cause for the relapse is
multifactorial,3-11 the orthodontist is obliged to choose the best way of retention
that require long-term stability.
Orthodontic retainers could be either categorized as removable or bonded
retainers.12 Due to the fact that removable retainers require patient’s cooperation
by large13 and bonded lingual retainers are considered more patient friendly, the
latter is classified as golden standard in orthodontics.14 Bonded retainers made of
wires present various configurations where the most commonly used ones are
individually adjusted multi-stranded stainless steel wires.15 Failure of such bonded
retainers is however a frequently observed clinical problem, which inevitably
results in full or partial loss of the retainer in function and when unobserved, may
lead to relapse.16
From the configuration type of view, Zachrisson et al. has reported that the
optimal wire retainer, when bonded to all the lingual or palatal surfaces of the
teeth in a segment, would be a 5-stranded 0.0215-in wire.17 Based on clinical
reports, among all wire types, multi-stranded wires consisting of five or even more
number of wires are preferred over single or 3-stranded wires.15,18-20 Moreover,
multi-stranded wires with 3 or less strands show considerably more wire-fatigue
fractures, debonding of the wire at the enamel-composite interface.15,18,19 Arnold
et al. showed that rectangular braided wires had better resistance to torsional
forces in comparison to round braided ones.21 In terms of bond strength, round
and rectangular braided wires revealed higher bond strength in comparison to
plain rectangular smooth wires.22 Yet, one of the most frequent failure type of
orthodontic retainers remains to be debonding ranging from 23 to 58% in the
maxilla and 5 to 37% in the mandible up to 10 years, regardless of the retainer
type used.23,24 In addition to possible relapse which is a clinical problem, revisits
to the orthodontist for rebonding are both timely and costly procedures both
for the patient and the clinician. The recent Cochrane review listed a number
of possible factors for the cause of relapse such as the recoil of fibers that hold
the teeth in the jaw bone, pressures form the lip, cheeks and tongue and further
growth which consequently could also yield to failure of the retainer.23 However,
material aspects received no attention in the reviewed material that could also
have potential effect on debonding of the retainers.
It has to be noted that the clinical adhesion of bonded retainers start with etching
the enamel, application of resin adhesive, placement of the wire and then coverage
of the wire with resin-based composite either using flowable or highly filled resin
composite materials. Since highly filled resin composites typically present higher
ABSTRACT
Objectives: This prospective clinical trial evaluated the survival of multi-stranded
stainless steel lingual retainers (SSR) bonded using different resin composite
types.
Methods: Between April 2011 and March 2013, a total of 75 patients (40 women,
35 men; mean age: 16.3 years old) received full arch orthodontic treatment after
which SSRs (Multi-strand 1 x 3 high performance wire, 0.022” x 0.016”, PG
Supply Inc.) (N=150) were bonded in the maxilla and/or mandible on all 6 anterior
teeth. After etching enamel surfaces with 35% H3PO4, adhesive resin was
applied (Clearfil SE Bond) and photo-polymerized for 20 s. SSRs were bonded
using one of the following resin composites: a) Hybrid (Clearfil AP-X, Kuraray
Noritake) (H1), b) Hybrid (Light Cure Retainer, Reliance Orthodontic Products Inc.)
(H2), c) Flowable (Clearfil Majesty Flow, Kuraray) (FL). At baseline and thereafter
at 1, 2, 3, 6, 12 and 24 months, SSRs were checked upon macroscopically for
partial or complete debonding or fracture. SSRs were scored as failed if any
operative intervention was indicated for repair, partial or total replacement. Data
were analyzed using Kaplan-Meier and Log Rank (Mantel-Cox) (α=0.05).
Results: SSRs were observed for a minimum of 6, and maximum 43 months
(mean: 19.5 months). At the final control (24 months), 10 patients could not be
followed up (H1: 12, H2: 4, FL: 4) due to drop out. In total, in 150 SSRs, 28
failures were observed (n=19 in the maxilla, n=9 in the mandible). The majority
of the failures were observed with FL (n=12), followed by H1 (n=8) and H2 (n=8)
being not statistically significant (maxilla: p=0.133; mandible: p=0.551). Overall,
3 fractures of the SSR were observed all of which were in the maxilla. Overall,
cumulative survival rate was 81.3% up to 43 months (Kaplan-Meier). Location of
the SSRs did not show significant difference (maxilla: 74.7%, CI: 29.4-37.7 and
mandible: 88% (CI: 35.7-41.7) (p>0.05). No significant difference was observed
between gender type (female: 78.8%; male: 81.3%) (p=0.059).
Conclusion: Although microhybrid flowable resulted in slightly more frequent
incidence of failures, the type of composite, the location and the gender did not
significantly affect the clinical survival of multi-stranded stainless steel bonded
lingual retainers in the studied sample.
Keywords: Adhesion; Adhesive dentistry, Clinical study, Orthodontic retainers,
Resin composite

72 73
suction and cotton rolls. Lingual enamel surfaces of all frontal teeth were etched
with 35% H3PO4 (Temrex Gel Etch, Temrex Corporation 112 Albany Avenue,
Freeport, NY, USA) for 20 seconds, rinsed with copious water and air-sprayed
and dried for about 5 seconds until the frosted enamel was visible. When this
was not the case, the particular tooth was etched again in the same manner.
Table 1: The brand, type, manufacturer, and chemical composition of the main materials used in this study.
Brand Type Manufacturer Chemical composition
1 x 3 high performance wire
Multi-stranded wire, 0.022” x 0.016”
PG Supply Inc., Avon, CT, USA
Stainless steel
ClearfilAP-X
Resincomposite
KurarayNoritake, Okayama, Japan
Bis-phenol A diglycidylmethacrylate <12 w%triethylene glycol dimethacrylate <5 w%Silanated barium glass filler Silanated silica fillerSilanated colloidal silica (80 w%, 70 v%)dl-Camphorquinone catalysts Accelerators, pigments
Light Cure Retainer
Resincomposite
Reliance Orthodontic Products Inc., Itasca, IL, USA
Glass filler 75 v%bis-phenol A diglycidylmethacrylate 10-30 w%Triethylene glycol 5 w% Dimethacrylate 5-10w%Amorphous silica 1-5 w%
Clearfill MajestyFlow
Resincomposite
KurarayNoritake
Triethylene glycol dimethacrylate <7 w%Hydrophobic aromatic dimethacrylate Silanated barium glass filler Silanated colloidal silica (80 w%, 62 v%)dl-CamphorquinoneAccelerators, pigments
TemrexEtch
Etchingagent
Temrex Corporation, NY, USA
35% H3PO4
ClearfilSE Bond
Adhesiveresin
KurarayNoritake
Bis-phenol A diglycidylmethacrylate 25-45%2-hydroxyethyl methacrylate 20-40%10-Methacryloyloxydecyl dihydrogen phosphateHydrophobic aliphatic methacrylate Colloidal silicadl-Camphorquinone initiators Accelerators
tensile strength and elasticity modulus,24 it could be anticipated that the use of
hybrid resin material could increase the survival rate of bonded retainers.
The objective of this study therefore was to evaluate the survival of multi-stranded
stainless steel lingual retainers (SSR) bonded using different resin composite
types. The hypothesis tested was that hybrid resin composite used for bonding
SSRs would result in higher rate of clinical survival compared to low viscosity
composite.
MATERIALS AND METHODS
Study designThe brands, types, chemical compositions and manufacturers of the materials
used in this study are listed in Table 1.
Inclusion and exclusion criteriaBetween April 2011 and March 2013, a total of 75 patients (40 women, 35 men;
mean age: 16.3 years old) received full arch orthodontic treatment after which
SSRs (Multi-strand 1 x 3 high performance wire, 0.022” x 0.016”, PG Supply Inc.,
Avon, CT, USA) (N=150) were bonded in the maxilla and mandible on all 6 anterior
teeth in private practice settings where specialized orthodontists deliver dental
services solely in orthodontics. As the bonded retainers in this study were made
as a part of standard dental care employed after orthodontic treatment, no ethical
committee approval was requested.
Information was given to each patient regarding the function of the retainers, and
informed consent was signed. The inclusion criteria were as follows: having no
active periodontal or pulpal diseases, having no primary caries, not allergic to resin-
based materials, not pregnant or nursing, having antagonist teeth opposing the
SSR, willing to return for follow-up examinations as outlined by the investigators.
Clinical proceduresAll bonded retainers were placed 1 month prior to the debonding of the
orthodontic appliances and thus with the fixed appliances in situ. At least one
week prior to retainer placement, the lingual and interproximal tooth surfaces
were cleaned from calculus and stain with a scaler or cavitron (H6-H7 Hu-Friedy
Mfg. Co., Chicago, IL USA and/or W&H Dentalwerk Bürmoos GmbH, Bürmoos,
Austria) On the appointment of retainer placement, all surfaces were cleaned
with non-fluoride containing pumice (Polo Dent Polish, American Dental Trading.
BV, Oisterwijk, The Netherlands) using silicone rubbers and cups (Hawe Kerr,
Kerr Corp. CA, USA). A cheek retractor (Reliance Orthodontic Products., IL, USA)
was used for better visibility of the working area. Dry field was created only with

74 75
RESuLTS
Distribution of SSRs in the maxilla and mandible is presented in Table 2. SSRs
were observed for a minimum of 6, and maximum 43 months (mean: 19.5
months). At the final control (24 months), 10 patients could not be followed up
(H1: 12, H2: 4, FL: 4) due to drop out. In total, in 150 SSRs, 28 failures were
observed (n=19 in the maxilla, n=9 in the mandible) (Table 3).
Table 2: Distribution of stainless steel bonded lingual retainers in the maxilla and mandible using two hybrid (H1 and H2) and one flowable (FL) resin composite material (H1: Clearfil AP-X; H2: Light Cure Retainer; FL: Clearfil Majesty Flow).
Maxilla Mandible Total (N)
H1 H2 FL H1 H2 FL
Females 13 12 15 13 12 15 75
Males 12 13 10 12 13 10 75
25 25 25 25 25 25
Total (N) 75 75 150
Table 3: Distribution of failure types of stainless steel bonded lingual retainers in the maxilla and mandible using two hybrid (H1 and H2) and one flowable (FL) resin composite material. See Table 2 for group abbreviations.
Maxilla Mandible Total (N)
H1 H2 FL H1 H2 FL
Partial debonding 4 3 8 3 2 4 24
Complete debonding 1 0 0 0 0 0 1
Wire fracture 3 3
Total (N)5 6 8 3 2 4
19 9 28
The majority of the failures were observed with FL (n=12), followed by H1 (n=8)
and H2 (n=8) being not statistically significant (maxilla: p=0.133; mandible:
p=0.551). Overall, 3 fractures of the SSR were observed all of which were in the
maxilla in H2 group. Regardless of the composite type, six partial debondings in
25 SSRs involved the canines. Except for 4 failures that occurred at 12 months
follow up, all other were observed within the first 6 months.
Overall, cumulative survival rate was 81.3% up to 43 months (Kaplan-Meier) (Fig.
1). Location of the SSRs did not show significant difference (maxilla: 74.7%, CI:
After etching enamel surfaces, adhesive resin was applied (Clearfil SE Bond,
Kuraray Noritake, Okayama, Japan) a thin coat using microbrush, air-thinned and
photo-polymerized for 20 s using an LED device (3M ESPE Elipar S10, St. Paul,
Minn, USA) with an output of ~ 1000 mW/cm2. SSRs were bonded using one of
the following resin composites: a) Hybrid (Clearfil APX, Kuraray) (H1), b) Hybrid
(Light Cure Retainer, Reliance, Itasca, IL, USA) (H2), c) Flowable microhybrid
(Clearfil Majesty Flow, Kuraray) (FL). Two operators who had experience in
orthodontics (>1-3 years since specialization) and 6 orthodontic assistants under
their supervision (>1-5 years) have bonded the SSRs with one of the resin
materials depending on their preference of materials.
Dental floss was placed between the central incisors and distal parts of the lateral
incisors in order to hold the SSRs in place that was individually bent in place. Each
layer of resin composite, covering the SSR in small buds (2 to 4 mm) was photo-
polymerized using an LED polymerization device (ESPE Elipar) for 20 s on each
tooth. The output of the polymerization device was controlled every 4 weeks.
After occlusion control using occlusion papers (Dr. Jean Bausch GmbH & Co. KG,
Köln, Germany), premature contact points were removed with carborundum burs
(Hager & Meisinger GmbH, Neuss, Germany) at 30.000 rpm under water. Excess
adhesive resin remnants were removed with a scaler (H6-H7 Hu-Friedy Mfg. Co.,
Chicago, IL USA). Resin composite surfaces were finished with carborundum
burs (Hager & Meisinger GmbH, Neuss, Germany) and polished with rubbers.
Patients received individual instructions to maintain their plaque control.
EvaluationAt baseline and thereafter at 1, 2, 3, 6, 12 and 24 months, SSRs were checked
upon macroscopically for partial or complete debonding or fracture. SSRs were
scored as failed if any operative intervention was indicated for repair, due to partial
or complete rebonding or total replacement due to fracture. Patients were asked
to contact the practice if they would perceive any problem or change in the SSRs.
Only the first experienced failures were considered as absolute failures over the
observation time.
Statistical analysisSurvival analyses were performed with statistical software program (SPSS 14.0;
SPSS Inc, Chicago, IL, USA) using Kaplan-Meier and Log Rank (Mantel-Cox)
tests to obtain the cumulative survival rates in relation to observation time. P
values less than 0.05 were considered to be statistically significant in all tests.

76 77
DISCuSSION
This study was undertaken in an attempt to evaluate the survival of SSRs bonded
using different resin composite types at private practice settings. Based on
the results, the incidence of failures were more frequent with FL which was a
microhybrid low viscosity resin composite compared to other hybrid composites,
but the survival statistics did not show significant difference between the resin
composites used for bonding the SSRs. Thus, the tested hypothesis was rejected.
Various types of resin composite have been described for the bonding of SSRs
in the literature25 but to our knowledge no study has looked at the differences
between resin composite type having different thixotropies. The amount of filler
content in resin composites is associated with higher mechanical properties.26
Hybrid composites, usually used for Class II, III and IV restorations are typically
highly filled, show higher elasticity moduli, fracture resistance, wear resistance
and therefore are less pliable in comparison to flowable composites.26 This is
one reason why the latter is often preferred in bonding SSRs in orthodontics.27
The insignificant difference between the FL and other hybrid composites could
be attributed to the filler content of 62 v% which could still be considered a high
amount for a low viscosity composite. Yet, the hybrid composites tested presented
70 v% for H1 and 75 v% for LCR being higher than that of FL. The failures related
to low viscosity resin materials may also be ascribed as a consequence of water
sorption over time. Hybrid composites used in this study, were meant to be less
prone to water sorption and showed higher depth of polymerization in comparison
to a similar composites used for the bonding of SSRs.28 However, the incidences
of the majority of the SSR failures in this study were experienced within the first
6 months. Therefore, the possible water sorption effect on the failures of resin
composites could not be disclosed in this study.
The majority of the failures were partial adhesive debonding of the SSRs from the
tooth surface. One reason for this type of failure could be lack of ideal conditioning
of the enamel surface which typically starts with etching with 35-37% H3PO4.
Adhesive types of failures are an indication of less adhesive forces between
the adhesive resin and the enamel surface. In this study, enamel surfaces
were etched only and no attempt was made to remove the most upper layer
of the enamel by roughening which is not a common practice in orthodontics
considering the age of the patient. Although enamel tissue removal is usually
not needed in orthodontics, due to the prerequisite of temporary adhesion,
SSRs serve a different purpose and lifespan and therefore require a different
application procedure. A commonly used application in reconstructive dentistry
is the removal of the possible aprismatic enamel at different levels using either
burs, disks or air-borne particle abrasion. The aim of these methods is to increase
the surface area and therefore enhance adhesion of the resin based material onto
29.4-37.7 and mandible: 88% (CI: 35.7-41.7) (p>0.05) (Figs. 2a-b). Annual failure
rate was 6.4%. No significant difference was observed between gender type
(female: 78.8%; male: 81.3%) (p=0.059).
The debonded SSRs were rebonded using the same resin composite and the
corresponding protocol.
Figures 2a-b: Event-free survival rates of stainless steel bonded lingual retainers ina) maxilla (n=75; 19 failures), b) mandible (n=75; 9 failures)(1: Clearfil AP-X; 2: Light Cure Retainer; 3: Clearfil Majesty Flow)
Cu
mu
lati
ve S
urv
ival
(%
)
Months
Survival Functions Maxilla
ResinComposite
Type
0
0,0
0,2
0,4
0,6
1,0
1231-censored2-censored3-censored
10 20 30 40 50
0,8
A
Cu
mu
lati
ve S
urv
ival
(%
)
Months
ResinComposite
Type
0
0,0
0,2
0,4
0,6
1,0
10 20 30 40 50
0,8
1231-censored2-censored3-censored
Survival Functions Mandible
B

78 79
adhesive dentistry, the high of failures indicates that other factors may play a
more dominant role in the debonding of SSRs. A number of factors have been
assigned for the failures of SSRs in orthodontics. Since the location, gender,
composite type, humidity control, operator factor could not be disclosed in this
study the cause of failures needs further investigations focusing on the effect
of orthodontic forces that disturb the microenvironment of the periodontal
ligament that in turn cause relapse and thereby increase forces between the SSR
and the tooth surface.41-43
One limitation of this study was that out of 150 SSRs, 20 of them could not be
followed up at 24 months follow up (H1: 12, H2: 4, FL: 4). Bearing in mind that the
oral environment is complex and that resin composites are susceptible to aging,
the survival of SSRs may decrease over time which needs long-term evaluations.
Conclusions
1. Resin composite type and the location did not significantly affect the clinical
survival of multi-stranded stainless steel lingual retainers.
2. Failures were in general due to partial or complete adhesive debonding of the
retainer from the tooth surface.
AcknowledgementsThe authors would like to extend their gratitude to Dr. M.P.E. Tacken for the helpful
discussions and cooperation during treatment of the patients and the whole
team of orthodontic assistants for their support and labour at the Apeldoorn
Orthodontie Welgelegen practice.
Conflict of interestThe authors did not have any commercial interest in any of the materials used in
this study.
enamel by means of micromechanical retention. Enamel, is the hardest structure
in the human body and is made of arranged hydroxyapatite prisms, consisting of
96 wt% inorganic matter.29,30 Hydroxyapatite crystals of enamel show a unique
structure with small rods. Each rod is usually built out of about 100 crystals. 29,30
Dental restorations and orthodontic appliances, largely depend on the surface
preparation of the enamel for their adhesion.31 Moreover, untreated enamel usually
smooth and non-retentive, impairs adhesion due to the existence of a pellicle
layer and the possible presence of the top aprismatic enamel layer that is usually
between 20 and 80 mm thick.29,31 Enhancement of adhesion, may be achieved by
enamel preparation by means of rotating instruments, which in turn leave a smear
layer behind which also compromises adhesion. Therefore, subsequent enamel
conditioning either chemically or mechanically is needed to expose fresh enamel
surface and increase the surface area for micromechanical retention.
Micro retention is achieved after acid etching with H3PO4 that can easily be
wetted by hydrophobic resin-based adhesives. Penetration of the applied
adhesive resin on the etched enamel surface through capillary action and
subsequent photo polymerization of the applied resin facilitates micromechanical
adhesion. Although the most commercially available enamel-etching agents have
a concentration ranging between 30-40%, a concentration of 37% has been
shown to be superior. Lower concentrations may lead to dicalcium phosphate
dihydrate precipitation in the micro retention cracks of the enamel surface which
are very difficult to remove by rinsing.32-34 In this study, in case of no frosted
appearance after etching, a second attempt was made to etch the enamel.
Adhesive procedures should be at best performed in dry environment. In this
study, this was achieved by not using rubberdam but cotton rolls and suction.
Saliva control could be anticipated to be less compared to maxilla leading to
higher survival in the maxilla. Yet, in this study, the failures were more common
in the maxilla than that of mandible, again disclosing the possible humidity control
effect in the mandible. In other words, since the location did not affect the results
significantly, it could be stated that cotton rolls and suction could be sufficient
when used ideally. The high incidence of failures in the maxilla however is in line
with previous studies where different materials were used that could be also due
to the continuous contact with anterior incisors as a result of bite depth during
mastication.35-37 Similarly, the lack of gender effect on the survival of SSRs is n
agreement with previous studies.38-40
The incidence of wire breakage was observed only in 3 SSRs. Likewise, previous
studies reported less incidence of failures in terms of wire fracture as opposed to
debonding.18-20 Although the exact reason is unknown, heat treatment seems to
decrease wire stiffness unpredictably yielding to early wire breakage which was
also practiced in this study.21
Nevertheless, even though adhesion to enamel is known to be the best in

80 81
18. Zachrisson BU. Clinical experience with direct-bonded orthodontic retainers. American Journal of Orthodontics and Dentofacial Orthophedics 1977;71:440-448.
19. Zachrisson BU. Improving orthodontic results in cases with maxillary incisors missing. Amer-ican Journal of Orthodontics and Dentofacial Orthophedics 1978;73:274-289.
20. Zachrisson, B.U. The bonded lingual retainer and multiple spacing of anterior teeth. Journal of Clinical Orthodontics 1983;17:838-844.
21. Arnold DT, Dalstra M, Verna C. Torque resistance of different stainless steel wires commonly used for fixed retainers in orthodontics. Journal of Orthodontics 2016;43:121-129.
22. Paolone MG, Kaitsas R, Obach P, Kaitsas V, Benedicenti S, Sorrenti E, Barberi F. Tensile test and interface retention forces between wires and composites in lingual fixed retainers. International Orthodontics 2015;13:210-220.
23. Artun J, Spadafora AT, Shapiro PA. A 3-year follow-up study of various types of orthodontic canine-to-canine retainers. Eur J Orthod. 1997;19:501-509.
24. Milheiro A, de Jager N, Feilzer A J, Kleverlaan CJ. In vitro debonding of orthodontic retain-ers analyzed with finite element analysis. European Journal of Orthodontics 2015;37:491-496.
25. Littlewood SJ, Millett DT, Doubleday B, Bearn DR, Worthington HV. Retention procedures for stabilising tooth position after treatment with orthodontic braces. Cochrane Database of Systematic Reviews 2016;29:CD002283.
26. Lohbauer U, Frankenberger R, Krämer N, Petschelt A. Strength and fatigue performance versus filler fraction of different types of direct dental restoratives. Journal of Biomedical Materials Research B Applied Biomaterials 2006;76:114-120.
27. Talic NF. Failure rates of orthodontic fixed lingual retainers bonded with two flowable light-cured adhesives: a comparative prospective clinical trial. Journal of Contemporary Dental Practice 2016;17:630-644.
28. Catalbas B, Uysal T, Nur M, Demir A, Gunduz B. Effects of thermocycling on the degree of cure of two lingual retainer composites Dental Materials Journal 2010;29:41-46.
29. Özcan M, Sadiku M. Analysis of structural, morfological alterations, wettability characteristics and adhesion to enamel after various surface conditioning methods. Journal of Adhesion Science and Technology 2016;22:2453-2465
30. Hellwig E, Klimek J, Attin T. Einführung in die Zahnerhaltung: Prüfungswissen Kariologie, Endodontologie und Parodontologie; mit 60 Tabellen, ed. 6. Köln: Dt. Ärzte-Verl.; 2013.
31. Shahabi M, Ahrari F, Mohamadipour H, Moosavi H. Microleakage and shear bond strength of orthodontic brackets bonded to hypomineralized enamel following different surface preparations. Journal of Clinical Experimental Dentistry 2014;6:e110-e115.
32. Lasers in Restorative Dentistry: A Practical Guide. Rome: Springer; 2015. p.3-6.
REFERENCES
1. Little RM, Riedel RA, Artun J. An evaluation of changes in mandibular anterior alignment from 10 to 20 years postretention. American Journal of Orthodontics and Dentofacial Orthophedics 1988;93:423-428.
2. Shah AA. Postretention changes in mandibular crowding: a review of the literature. Ameri-can Journal of Orthodontics and Dentofacial Orthophedics 2003;124:298-308.
3. Riedel RA. A review of the retention problem. Angle Orthodontics 1960;30:179-199.
4. Boese LR. Fiberotomy and reproximation without lower retention 9 years in retrospect: part II. Angle Orthodontist 1980;50:169–178.
5. Southard T, Southard K, Tolley E. Periodontal force: a potential cause of relapse. American Journal of Orthodontics and Dentofacial Orthophedics 1992;101:221-227.
6. Al Yami EA, Kuijpers-Jagtman AM, van ‘t Hof MA. Stability of orthodontic treatment outcome: follow-up until 10 years postretention. American Journal of Orthodontics and Dentofacial Orthophedics 1999;115:300-304.
7. Kim TW, Little RM. Postretention assessment of deep overbite correction in Class II Division 2 malocclusion. Angle Orthodontist 1999;69:175-186.
8. Thilander B. Biological basis for Orthodontic relapse. Seminars in Orthodontics 2000;6:195-205.
9. Thilander B. Orthodontic relapse versus natural development. American Journal of Ortho-dontics and Dentofacial Orthophedics 2000;117:563-565.
10. Proffit WR, Fields HM, Sarver DM. Contemporary orthodontics. 4th edn. St. Louis: CV Mos-by, 2007.
11. Gkantidis N, Christou P, Topouz N. The orthodontic–periodontic interrelationship in integrat-ed treatment challenges: a systematic review. Journal of Oral Rehabilation 2010;37:377-390.
12. Daskalogiannakis J. Glossary of Orthodontic terms. 1st edition Berlin: Quintessence Publishing Co. 2000;230.
13. Ackerman MB, Thornton B. Posttreatment compliance with removable retention in a teenage population: a short-term randomized clinical trial. Orthodontics (Chic.) 2011; 12:22.
14. Bearn DR. Bonded orthodontic retainers: a review. American Journal of Orthodontics and Dentofacial Orthophedics 1995;108: 207-213.
15. Zachrisson BU. Multistranded wire bonded retainers: from start to success. American Jour-nal of Orthodontics and Dentofacial Orthophedics 2015;148:724-727.
16. Radlanski RJ., Zain ND. Stability of the bonded lingual wire retainer – a study of the initial bond strength. Journal of Orofacial Orthophedics 2004;65:321-335.
17. Dahl EH, Zachrisson BU. Long-term experience with direct-bonded lingual retainers. Journal of Clinical Orthodontics 1991;25:619-630.

82 83
33. Schwartz RS. Fundamentals of operative dentistry: A contemporary approach. Quintessence books. Chicago: Quintessence Publ; 1996. p. 209.
34. Kugel G, Ferrari M. The science of bonding: from first to sixth generation. Journal of American Dental Association 2000;131 Suppl:20S-25S.
35. Schneider E, Ruf S. Upper bonded retainers. Angle Orthodontist 2011;81:1050-1056.
36. Renkema AM, Sips ET, Bronkhorst E, Kuijpers-Jagtman AM. A survey on orthodontic retention procedures in The Netherlands. European Journal of Orthodontics 2009;31:432-437.
37. Lie Sam Foek DJ, Özcan M, Verkerke GJ, Sandham A, Dijkstra PU. Survival of flexible, braided, bonded stainless steel lingual retainers: a historic cohort study. European Journal of Orthodontics 2008;30:199-204.
38. Lumsden KW, Saidler G, McColl JH Breakage incidence with direct bonded lingual retainers British Journal of Orthodontics 1999;26:191-194.
39. Yoshida Y, Sasaki T, Yokoya K, Hiraide T, Shibasaki Y. Cellular roles in relapse processes of experimentally-moved rat molars. Journal of Electron Microscopy (Tokyo). 1999;48:147-57.
40. Jónsdóttir SH1, Giesen EB, Maltha JC. The biomechanical behaviour of the hyalinized periodontal ligament in dogs during experimental orthodontic tooth movement. European Journal of Orthodontics. 2012;34:542-546.
41. Feng L, Yang R, Liu D, Wang X, Song Y, Cao H, He D, Gan Y, Kou X, Zhou Y. PDL progenitor-mediated PDL recovery contributes to orthodontic relapse. Journal of Dental Research 2016;95:1049-1056.

Chapter 6
Displacement of teeth without and with bonded fixed orthodontic retainers:3D analysis using triangular target frames and optoelectronic motion tracking device
Chakroun F
Colombo V
Lie Sam Foek D.J.
Gallo L
Feilzer A.J.
Özcan M
Submitted to: Journal of the Mechanical Behavior of Biomedical Materials, 2017.

86 87
Keywords: Adhesion; bonded retainers; dynamic stereometry; periodontal
ligament; three- dimensional; tooth movement
INTRODuCTION
After an orthodontic treatment, the aligned teeth in their achieved positions need
to be stabilized using bonded retainers (Little et al., 1998; Shah, 2003). In the
absence of retention, 40 to 90% of relapse has been reported up to 10 to 20 years
(Little et al., 1998; Al Yami et al., 1999; Kim et al. 1999). Failure of such bonded
retainers is however a frequently observed clinical problem after the active
treatment and when unnoticed they may lead to unwanted tooth movement
(Radlanski et al., 2004). This is due to the fact that teeth have a tendency to
return to their former position which is typically described as orthodontic relapse
(Joondeph, 2011). Possible causes for such unwanted post-treatment tooth
movements are multifactorial and have been attributed to the reorganization
of the supporting tissues surrounding the teeth, neuromuscular imbalances,
continued facial growth, aging and continuous unwanted oral habits (Reitan et
al., 1960, 1967; Vaden et al., 1997; Blake et al., 1998; Rossouw, 1999; Joondeph,
2011; Heyman et al., 2012). Prevention of these unwanted tooth movements is a
necessity in order to maintain the achieved orthodontic result (Dahl et al., 1991)
Bonded retainers usually made of single or multi-stranded stainless steel wires are
considered as golden standard in orthodontics with the advantage of allowance
for physiologic tooth movement compared to more stiff materials such as fiber
reinforced composites (Bearn, 1995; Zachrison, 2015) Yet, a high incidence
of failures, varying from 5.9 to 53% has been reported in previous studies,
regardless of the variations in material types, configurations and application
modes of bonded retainers (Segner and Heinici, 2000; Lie Sam Foek et al., 2008;
Pandis et al., 2013) Nevertheless, former studies have shown that failure rates
were often independent of gender, age and operator experience which leads to
the assumption that the biological and physiological factors are more responsible
causes for unwanted tooth movement and thereby debonding of the retainers (Lie
Sam Foek et al., 2008; Maltha et al., 2017) In this context, periodontal ligaments
(PDL) and gingival fibers composing the periodontium are stretched during tooth
movement of any kind, which may cause strain between the bonded retainer and
the tooth surface (Gerami et al., 2012; Franzen et al., 2013; Maltha et al., 2017).
The role of PDL on relapse has been studied in animal experiments mainly on
two teeth without considering the arch formation (Maltha et al., 2017). In fact, the
force distribution could be anticipated to decraese when they are disseminated
on multiple teeth in an arch where the retainers are bonded. To the best of our
knowledge, no study has looked at the tooth displacement in a configuration
ABSTRACT
Purpose: The objective of this study was to evaluate the anterior tooth movement
without and with bonded fixed orthodontic retainers under incremental loading
conditions.
Materials and Methods: Six extracted mandibular anterior human teeth were
embedded in acrylic resin in True Form I Arch type and 3D reconstruction of Digital
Volume Tomography (DVT) images (0.4 mm3 voxels) were obtained. The anatomy
of each tooth was segmented and digitally reconstructed using 3D visualization
software for medical images (AMIRA, FEI SVG). The digital models of the teeth
were repositioned to form an arch with constant curvature using a CAD software
(Rhinoceros) and a base holder was designed fitting the shape of the roots. The
clearance between the roots and their slot in the holder was kept constant at
0.3 mm to replicate the periodontal ligament thickness. The holder and the teeth
were then manufactured by 3D printing (Objet Eden 260VS, Stratasys) using a
resin material for dental applications (E=2-3 GPa). The 3D printed teeth models
were then positioned in the holder and the root compartments were filled with
silicone. The procedure was repeated to obtain three identical arch models. Each
model was tested for tooth mobility by applying force increasing from 5 to 30
N with 5 N increments applied perpendicular on the lingual tooth surface on
the incisal one third (crosshead speed: 0.1 mm/s). The teeth on each model
were first tested without retainer (control) and subsequently with the bonded
retainers (braided bonded retainer wire; Multi-strand 1x3 high performance wire,
0.022” x 0.016”). Tooth displacement was measured in terms of complicance
(F/Δ movement) (N/mm) using custombuilt optoelectronic motion tracking
device (OPTIS) (accuracy: 5 mm; sampling rate: 200 Hz). The position of the
object was detected through three LEDs positioned in a fixed triangular shape on
a metal support (Triangular Target Frame). The measurements were repeated for
three times for each tooth. Data were analysed using mixed model with nesting
(alpha=0.05).
Results: The use of retainer showed a significant effect on tooth mobility
(0.008±0.004) compared to non-bonded teeth (control) (0.014±0.009)
(p<0.0001). The amount of displacement on the tooth basis was also significantly
different (p=0.0381) being the most for tooth no. 42 (without: 0.024±0.01; with:
0.012±0.002) (p=0.0018). No significant difference was observed between
repeated measurements (p=0.097) and the incremental magnitude of loading
(5-30 N: 0.07±0.01- 0.09±0.02) (p>0.05).
Conclusion: Mandibular anterior teeth showed less tooth mobility when bonded
with stainless steel wire as opposed to non-bonded teeth but the tooth mobility
varied depending on the tooth type. Intermittent increase in loading from 5 to 30
N did not increase tooth displacement.

88 89
Experimental proceduresTooth mobility was tested by applying force increasing from 5 to 30 N with 5
N increments applied perpendicular on the lingual tooth surface on the incisal
one-third at a crosshead speed of 0.1 mm/s. Each model was mounted on a
custom-made loading device (RPETS, University of Zurich) allowing precise and
repeatable positioning of the arch. The device was composed of two main parts:
a metal support where the arch could be aligned with the teeth to be tested and
motor controlled loading mechanism, pressing a conic shaped tip (single point
force application) on the selected tooth with a prescribed force, measured by
means of a force sensor (ME Messsysteme GmbH, Henningsdorf, Germany).
The teeth on each model were first tested without retainer that acted as the control
group and subsequently with the bonded retainers (braided bonded retainer wire;
Multi-strand 1x3 high performance wire, 0.022” x 0.016”, PG Supply Inc., Avon,
Connecticut, USA). On the lingual surfaces of each tooth an adhesive resin was
applied (Heliobond, Ivoclar Vivadent, Ivoclar Vivadent, Schaan, Lichtenstein) and
photo-polymerized for 20 s (Bluephase, Ivoclar Vivadent). The lingual retainer was
individually bent on all teeth and made sure to have a passive fit. The retainers
were bonded on all teeth using resin composite (Tetric Evo Ceram, Ivoclar
Vivadent) and photo polymerized for 20 s on each tooth (Figs. 1a-d).
Figs. 1a-d Workflow of the model preparation. a) The anatomy of six anterior teeth (canine to canine) was acquired with DVT and digitally reconstructed; b) digital models of the teeth were repositioned to form a standard arch form, c) base holder was designed fitting the shape of the roots; d) holder and the teeth were manufactured using 3D printing and positioned in the holder where the root compartments were filled with silicone.
of the frontal mandibular arch. Yet, it is an easy task to study the amount of
tooth displacement in a complete arch segment under administered magnitudes
of forces. Establishment of a model for measurement of tooth mobility under
different bonded materials would also allow making measurements for different
adhesives and retainer materials.
The objectives of this study therefore were to investigate the anterior tooth
movement without and with bonded fixed orthodontic retainers under incremental
loading conditions. The hypotheses tested were that:
a) the use of bonded retainer would show less tooth mobility as opposed to
non-bonded ones,
b) the tooth mobility would increase with the increased magnitude of force,
c) displacement amount would be similar regardless of the tooth type.
MATERIAL AND METHODS
Model preparationSix extracted mandibular anterior human teeth were embedded in acrylic resin
(Technovit, Kulzer GmbH, Wehrheim, Germany), in True Form I Arch type (G&H
Wires, Franklin, Indiana, USA) and 3D reconstruction of Digital Volume Tomography
(DVT) images (Kavo 3D Exam1, Kavo GmbH, Leutkirsch, Germany) (0.4 mm3
voxels) were obtained. All teeth used in the present study were extracted for
reasons unrelated to this project. Written informed consent for research purpose
of the extracted teeth was obtained by the donor prior to extraction according
to the directives set by the National Federal Council. Ethical guidelines were
strictly followed and irreversible anonymization was performed in accordance
with State and Federal Law (World Medical Association, Declaration of Helsinki,
2013; Human Research Act, 2015). The anatomy of each tooth was segmented
and digitally reconstructed using 3D visualization software for medical images
(AMIRA, FEI SVG, Thermo Fisher Scientific, Hillsboro, Oregon, USA). The digital
models of the teeth were repositioned to form an arch with constant curvature
using CAD software (Rhinoceros, Mc Neel Euope, Barcelona, Spain) and a base
holder was designed fitting the shape of the roots. The clearance between the
roots and their slot in the holder was kept constant at 0.3 mm to replicate the
periodontal ligament thickness (Provatidis, 2000). The holder and the teeth were
then manufactured by 3D printing (Obect Eden 260VS, Stratasys, Commerce
Way Eden Prairie, Minesota, USA) using a resin material for dental applications
(Clear Biocompatible, MED 610, Stratasys, Commerce Way Eden Prairie) (E=
2-3 GPa). The 3Dprinted teeth models were then positioned in the holder and
the root compartments were filled with silicone (President, Coltene, Altstätten,
Switzerland). The procedure was repeated to obtain three identical arch models.
A
C
B
D
89
Experimental proceduresTooth mobility was tested by applying force increasing from 5 to 30 N with 5
N increments applied perpendicular on the lingual tooth surface on the incisal
one-third at a crosshead speed of 0.1 mm/s. Each model was mounted on a
custom-made loading device (RPETS, University of Zurich) allowing precise and
repeatable positioning of the arch. The device was composed of two main parts:
a metal support where the arch could be aligned with the teeth to be tested and
motor controlled loading mechanism, pressing a conic shaped tip (single point
force application) on the selected tooth with a prescribed force, measured by
means of a force sensor (ME Messsysteme GmbH, Henningsdorf, Germany).
The teeth on each model were fi rst tested without retainer that acted as the control
group and subsequently with the bonded retainers (braided bonded retainer wire;
Multi-strand 1x3 high performance wire, 0.022” x 0.016”, PG Supply Inc., Avon,
Connecticut, USA). On the lingual surfaces of each tooth an adhesive resin was
applied (Heliobond, Ivoclar Vivadent, Ivoclar Vivadent, Schaan, Lichtenstein) and
photo-polymerized for 20 s (Bluephase, Ivoclar Vivadent). The lingual retainer was
individually bent on all teeth and made sure to have a passive fi t. The retainers
were bonded on all teeth using resin composite (Tetric Evo Ceram, Ivoclar
Vivadent) and photo polymerized for 20 s on each tooth (Figs. 1a-d).
Figs. 1a-d Workfl ow of the model preparation. a) The anatomy of six anterior teeth (canine to canine) was acquired with DVT and digitally reconstructed; b) digital models of the teeth were repositioned to form a standard arch form, c) base holder was designed fi tting the shape of the roots; d) holder and the teeth were manufactured using 3D printing and positioned in the holder where the root compartments were fi lled with silicone.

90 91
parameter “compliance” was observed as a measure of the response of the arch
to the pressure in terms of elasticity, being the inverse of the elastic modulus (K)
according to the following formulas:
K= F/ΔM (1)
where K was the elasticity modulus (GPa), F, the applied force (N), ΔM, change
in movement (mm)
C=1/K (2)
where C was the Compliance and K the elasticity modulus.
The measurements were repeated for three times for each tooth on each model
yielding to 54 measurements.
Statistical analysisData were analyzed using a statistical software package (IBM SPSS Software V.23,
Chicago, IL, USA). Kolmogorov-Smirnov and Shapiro-Wilk tests were used to test
normal distribution of the data. Values of mean, standard deviation, maximum and
minimum were calculated for all teeth in an arch in the two observed conditions
(without and with the retainer) and for each tooth. In order to determine the
dependency of tooth mobility as a function of 1) the use of a retainer, 2) the tooth
position and 3) the repetition, a mixed effects statistical model with nesting was
employed. “Arch” and “individual tooth” were considered as random factors and
“individual tooth” was nested in “arch”. In contrast, “retainer”, “tooth position”
and “repetition” were reflected as fixed factors. Furthermore, the logarithm of
the slopes was taken in the mixed effects model in order not to violate modelling
assumptions. P values less than 0.01 were considered to be statistically significant
in all tests.
RESuLTS
Descriptive statistics results of the compliance derived from the control condition
and with the retainer are presented in Table 1. Overall, the mean value of the
compliance was smaller with the retainer than in the control condition.
The use of retainer showed a significant effect on tooth displacement
(0.008±0.004) compared to non-bonded teeth (control) (0.014±0.009)(p<0.0001).
Tooth displacement was measured using custombuilt optoelectronic motion
tracking device (OPTIS, University of Zurich, Switzerland) based on 3 non-collinear
Charge-coupled device (CCD) cameras (Spectral Instruments, Tuscan, AZ, USA)
recording the movements of Light Emitting Diodes (LEDs) with an accuracy of 5
mm and a sampling rate of 200 Hz. In order to define the position of the object
to be detected, three LEDs are positioned in a fixed triangular shape on a metal
support called Triangular Target Frame (TTF). One TTF was glued to each tooth
and the other to the arch holder through which the relative movement of the
tested tooth was determined. Digital models of the teeth were animated with
the tracked movements by means of a custom-made software application (Figs.
2a-c).
Figs. 2a-c. a) Custom-made device for force application on the lingual surfaces of the teeth on the mandibular arch composed of a metal support in which the arch is aligned with the tooth to be tested and electronically controlled loading mechanism, b) the arch model in its base holding the Triangular Target Frame (TTF) with light emitting diode (LED)s used during the kinematic recording and the conic shaped tip applying force on the selected tooth with the administered force, c) 3 non-collinear charge-coupled device (CCD) cameras used recording the movements of LEDs with an accuracy of 5 μm and a sampling rate of 200 Hz.
The mid-incisal point (IP) of each tooth was marked and its trajectory was
determined. The vector between two subsequent recorded positions of IP was
computed. The relationship between the force and displacement for each tooth
was determined by calculating the linear regression line between the values of
the displacement vector obtained for each tooth at each adminstered force. The
A
C
B

92 93
Table 1: Descriptive statistics of the compliance results regardless of the tooth type and force in all tested mandibular arch models.
Without Bonded Retainer (Control)
With Bonded Retainer
Mean 0.014 0.008
Median 0.013 0.008
Std. Deviation 0.009 0.004
Minimum -0.001 -0.015
Maximum 0.038 0.016
CI Lower Bound 0.011 0.007
CI upper Bound 0.016 0.009
Std. Error 0.001 0.001
Tab
le 2
: De
scri
ptiv
e st
atis
tics
of
the
com
plia
nce
re
sult
s d
ep
en
din
g o
n to
oth
po
siti
on
for
cont
rol a
nd
bo
nd
ed
reta
ine
r m
od
els
.
R2 = 0,9513
05 10 15 20 25 30
0
0,1
0,2
0,3
0,4
0,5
0,6
0 5 10 15 20 25 30
Dis
plac
emen
t (m
m)
Force [N]
Tooth - based
)$
)%
)&
)'
)(
)#
32
31
41
42
43
33
Arch - based
Dis
plac
emen
t (m
m)
0,1
0,2
0,3
0,4
0,5
0,6
A
R2 = 0,9513
05 10 15 20 25 30
0
0,1
0,2
0,3
0,4
0,5
0,6
0 5 10 15 20 25 30
Dis
plac
emen
t (m
m)
Force [N]
Tooth - based
)$
)%
)&
)'
)(
)#
32
31
41
42
43
33
Arch - based
Dis
plac
emen
t (m
m)
0,1
0,2
0,3
0,4
0,5
0,6
B
Figures. 3a-b. Displacement (mm) of teeth a) regardless of the tooth type in all mandibular arches tested, b) on the basis of tooth type as a function of incremental force application from 5 to 30 N.
Wit
ho
ut
Bo
nd
ed R
etai
ner
(C
on
tro
l)W
ith
Bo
nd
ed R
etai
ner
t3
3t3
2t3
1t4
1t4
2t4
3t3
3t3
2t3
1t4
1t4
2t4
3
Mea
n0.
015
0.01
20.
010
0.01
30.
024
0.0
08
0.0
09
0.0
08
0.0
070.
00
90.
012
0.0
02
Med
ian
0.01
40.
014
0.01
00.
014
0.0
270.
00
60.
00
90.
00
80.
00
60.
00
90.
011
0.0
05
Std
. Dev
iati
on
0.01
00.
00
40.
00
30.
00
40.
010
0.0
08
0.0
03
0.0
010.
00
20.
00
20.
00
20.
007
Min
imu
m0.
00
40.
007
0.0
06
0.0
070.
012
-0.0
010.
00
50.
00
60.
00
30.
00
60.
00
9-0
.015
Max
imu
m0.
02
90.
016
0.01
60.
018
0.0
38
0.01
90.
015
0.01
00.
00
90.
011
0.01
60.
00
8
CI L
ow
er B
ou
nd
0.0
070.
00
90.
00
80.
010
0.01
70.
001
0.0
070.
007
0.0
05
0.0
070.
010
0.01
0
CI u
pp
er B
ou
nd
0.0
23
0.01
50.
012
0.01
60.
03
20.
014
0.01
20.
00
90.
00
80.
010
0.01
30.
013
Std
. Err
or
0.0
03
0.0
010.
001
0.0
010.
00
30.
00
30.
001
0.0
00
0.0
010.
001
0.0
010.
001

94 95
30 N is considerably less compared to normal masticatory forces. However, the
linear increase exceeding 30 N was not significant in this study and therefore
the threshold value of 30 N was considered as the highest magnitude of force.
Nevertheless, in this study in none of the cases, debonding or other types of
retainer failures were experienced. In both model scenarios without and with
bonded retainers, the maximum complianc did not exceed 0.038 witout and 0.016
with retainer ndicating that this amount of mobility does not yield to debonding,
providing that some degree of tooth movement could also be dictated by the
flexibility of the wire tested.
Typically, teeth are surrounded by the PDL which is a thin membrane consisting
of collagen fibers. This ligament provides the attachment of the tooth to the
surrounding alveolar bone, and under normal circumstances there is no direct
contact between the root and the bone. Forces applied to the crown of the tooth
are transmitted to the alveolar bone through this layer, stretching, and compressing
the ligament (Van Schepdael et al., 2012). Different cell types, like fibroblasts,
osteocytes and osteoblasts, respond to the changes in mechanical environment.
This biological environment has been tried to be simulated using different
materials in the dental literature. Some authors preferred to simulate the PDL with
polyether (Behr et al., 1999; Rosentritt et al., 2006; Xie et al., 2007; Kolbeck et al.,
2008; Minami et al., 2009), others gum resin (Kern et al., 1994; Chitmongkolsuk
et al., 2002; Attia et al., 2006; Att et al., 2007), latex (Kohorst et al., 2007), wax
(Pfeiffer and Grube, 2003), polysulfide (Grajower et al., 1981) or silicone (Wolfart
et al., 2007). Provatidis (2000) followed the work of Haack and Haft (1972) in
representing the root of a maxillary central incisor as a paraboloid, surrounded by
the ligament. In the analyzed in vitro studies, dipping the roots in these materials
simulated the presence of PDL. This simplistic approach considered neither the
elastic modulus nor the thickness of the used PDL materials. Furthermore, since
lateral displacement forces are dominated with the thickness of the PDL material,
it can be expected that the forces would be unfavourable when PDL is thicker.
In this study, although the tooth morphology varied in the studied sample, in an
attempt to standardize the PDL thickness the clearance between the root surfaces
and the model was maintained at 0.25 mm. A thickness of 0.229 mm was found
to be common on maxillary incisors (Provatidis, 2000). Also, the measurements
were made consecutively in order to avoid the stiffness of the silicone material
over time. Yet, due to the lack of neuromuscular forces silicone PDL could still be
considered as a simplistic approach and therefore can only provide prediction of
tooth displacement in relation to the used retainer or adhesive materials and the
administered force applied.
Although initially no significant difference was expected on the tooth type basis,
interestingly, tooth number 42 showed the highest mean values for compliance.
One possible explanation could be the root morphology of this very tooth
The amount of displacement on the tooth basis was also significantly different
(p=0.0381) being the most for tooth no. 42 (without: 0.024±0.01; with:
0.012±0.002) (p=0.0018) (Table 2)
No significant difference was observed between repeated measurements
(p=0.097) and the inceremental magnitude of loading (5-30 N: 0.07±0.01- 0.09
±0.02) (p>0.05) (Figs. 3a-b).
DISCuSSION
This study was undertaken in order to investigate the anterior tooth movement
without and with bonded fixed stainless steel orthodontic retainers under loading
conditions. Based on the results of this study, since the presence of retainer
significantly decreased the tooth mobility, the first hypothesis could be accepted.
However, the increased magnitude of force did not significantly effect the tooth
displacement. Thus, the second hypothesis could be rejected. Displacement
amount was similar in all teeth except for one, namely tooth number 42) and
therefore, the third hypothesis could only be partially accepted.
A number of factors alone or simultaneously cause the failures of bonded
retainers in orthodontics. Since the location, gender, composite type, humidity
control, operator factor could not be disclosed in previously studies (Lie Sam
Foek et al., 2008; Segner and Heinrici, 2000), tooth mobility was of focus in this
study. In an attempt to make a close approximation to the clinical situation, an
ideal mandibular arch model was chosen and the extracted human teeth from
the same patient were positioned accordingly. The association between the
debonding of retainers and tooth mobility was assessed previously on simplified
models where the retainers were adhered to only two teeth set up (Lie Sam Foek
et al., 2009; Paolone et al., 2015). However, the contradictory clinical findings
and the ones obtained from such simplified models, encouraged us to use of a
full segment when studying tooth displacement under loading and stability of
bonded retainers. Furthermore, in an arch model, ‘free wire’ which should be
ideally 2.5 mm in between the buds of resin composite adhered on the tooth
surface allows for more flexibility of the wire compared to simplified models
(Milheiro et al., 2015).
The methodology used in this study proved to be reproducible. Since the models
with the teeth were replicas of the extracted human anterior teeth, the employed
method could be used to study tooth displacement using other bonded retainer
types. In this study, tooth displacement was measured under compression
where the forces were increased by 5 N up to 30 N. Three dimensional tooth
displacement was linearly correlated with the applied force. One can argue that

96 97
AcknowledgementsThe authors acknowledge Mr. A. Trottmann, University of Zurich, Center for
Dental and Oral Medicine, Zürich, Switzerland, for his assistance with the speci-
men preparation, Mr. C. Lüscher for his support with the development of the
custom made device, Mr. S. Erni from the Clinic of Masticatory Disorders, for
his assistance with the analysis, Dr. E. Yetkiner for his assistance during model
preparations, and Dr. D. Widemeier, University of Zurich, Switzerland for his
support with the statistical analysis.
Conflict of interestThe authors did not have any commercial interest in any of the materials used in
this study.
which possibly differed from those of others. Since the clearance values was
standard, the lack of significant difference in terms of compliance could be not be
considered surprising. However, the significantly higher variation of compliance
observed with tooth number 42 raises the question whether root morphology
plays a role in the torsional component of the applied compressive load.
Measurement of tooth movement is a complex procedure and includes translational
and rotational components of motion. In this study, only translations were
quantified and they were linearly related to the force applied with compression
steps of 5 N. It could be estimated that not only the compression but also torsional
forces could be responsible for debonding of retainers. Furthermore, force in this
study was applied at a constant speed and in clinical situations variable speeds
of force may occur during function which may cause debonding of the retainers.
Nevertheless, the analysis of tooth displacement could be instrumental for finite
elements analysis of the stresses at the roots of the teeth with different types of
lingual retainers or adhesives used. The tooth mobility obtained using stainless
steel wires should be compared with those of fiber reinforced retainers where
contradictory clinical results are presented some of which attributes the failures
to the lack of mobility due to the stiffness of the material. The utilized method with
its favourable reproducibility in this study could be instrumental for measurement
of tooth displacement with fiber reinforced composite retainer types.
Conclusions
From this study, the following could be concluded:
1. Mandibular anterior teeth showed less tooth displacement when bonded
with stainless steel wire compared to the non-bonded control group.
2. Tooth displacement varied on the mandibular arch depending on the tooth
type being the highest for tooth number 42 in both bonded and non-bonded
models.
3. Increase in the magnitude of force on the inciso-lingual direction on the teeth,
intermittent from 5 to 30 N did not result in increased tooth displacement and
the simulated model showed reliable reproducibility.
Clinical RelevanceBonded stainless steel lingual retainers in the studied arch model resulted in less
tooth movement compared to non-bonded ones not exceeding the mean value of
0.008. Intermitttent increase of loading from 5 to 30 N did not cause debonding
of the retainer with the tested materials.

98 99
17. Kim TW, Little RM. Postretention assessment of deep overbite correction in Class II Division 2 malocclusion. Angle Orthod 1999;69:175-186.
18. Kohorst P, Herzog T, Borchers L, Stiesch-Scholz M. Load-bearing capacity of all-ceramic posterior four-unit fixed partial dentures with different zirconia frameworks. Eur J Oral Sci 2007;115:161-166.
19. Kolbeck C, Behr M, Rosentritt M, Handel G. Fracture force of tooth-tooth- and implant-tooth-supported all-ceramic fixed partial dentures using titanium vs. customised zirconia implant abutments. Clin Oral Implants Res 2008;19:1049-1053.
20. Lie Sam Foek DJ, Özcan M, Verkerke GJ, Sandham A, Dijkstra PU. Survival of flexible, braided, bonded stainless steel lingual retainers: a historic cohort study. Eur J Orthod 2008;30:199-204.
21. Lie Sam Foek DJ, Özcan M, Krebs E, Sandham A. Adhesive properties of bonded orthodontic retainers to enamel: stainless steel wire vs fiber-reinforced composites. J Adhes Dent 2009;11:381-390.
22. Little RM, Riedel RA, Artun J. An evaluation of changes in mandibular anterior alignment from 10 to 20 years postretention. Am J Orthod Dentofacial Orthop 1988;93:423-428.
23. Maltha JC, Kuijpers-Jagtman AM, Von den Hoff JW, Ongkosuwito EM. Relapse revisited-Animal studies and its translational application to the orthodontic office. Semin Orthod 2017 (EPub).
24. Milheiro A, de Jager N, Feilzer AJ, Kleverlaan CJ. In vitro debonding of orthodontic retainers analyzed with finite element analysis. Eur J Orthod 2015;37:491-496.
25. Pandis N, Fleming PS, Kloukos D, Polychronopoulou A, Katsaros C, Eliades T. Survival of bonded lingual retainers with chemical or photo polymerization over a 2-year period: a single-center, randomized controlled clinical trial. Am J Orthod Dentofacial Orthop 2013;144:169-175.
26. Pfeiffer P, Grube L. In vitro resistance of reinforced interim fixed partial dentures. J Prosthet Dent 2003;89: 170-174.
27. Paolone MG, Kaitsas R, Obach P, Kaitsas V, Benedicenti S, Sorrenti E, Barberi F. Tensile test and interface retention forces between wires and composites in lingual fixed retainers. Int Orthod 2015;13:210-220.
28. Provatidis CG. A comparative FEM-study of tooth mobility using isotropic and anisotropic models of the periodontal ligament. Finite element method. Med Eng Phys 2000;22:359-370.
29. Radlanski RJ., Zain ND. Stability of the bonded lingual wire retainer - A study of the initial bond strength. J Orofac Orthop 2004;65:321-335.
30. Rosentritt M, Behr M, Gebhard R, Handel G. Influence of stress simulation parameters on the fracture strength of all-ceramic fixed-partial dentures. Dent Mater 2006;22:176-182.
REFERENCES
1. Al Yami EA, Kuijpers-Jagtman AM, van ‘t Hof MA. Stability of orthodontic treatment outcome: follow-up until 10 years postretention. Am J Orthod Dentofacial Orthop 1999;115:300-304.
2. Attia A. Influence of surface treatment and cyclic loading on the durability of repaired all-ceramic crowns. J. Appl Oral Sci 2010;18:194-200.
3. Attia A, Abdelaziz K, Freitag S, Kern M. Fracture load of composite resin and feldspathic all-ceramic CAD/CAM crowns. J Prosthet Dent 2006;95:117-123.
4. Bearn DR. Bonded orthodontic retainers: a review. Am J Orthod Dentofacial Or-thop 1995;108:207-213.
5. Behr M, Rosentritt, M, Leibrock A, Schneider-Feyrer S, Handel G. In-vitro study of fracture strength and marginal adaptation of fibre-reinforced adhesive fixed partial inlay dentures. J Dent 1999;27:163-168.
6. Blake M, Bibby K. Retention and stability: a review of the literature. Am J Orthod Dentofacial Orthop 1998;114:299-306.
7. Chitmongkolsuk S, Heydecke G, Stappert C, Strub J. Fracture strength of all-ceramic lithium disilicate and porcelain-fused-to-metal bridges for molar replacement after dynamic loading. Eur J Prosthodont Restor Dent 2002;10:15-22.
8. Dahl EH, Zachrisson BU. Long-term experience with direct-bonded lingual retainers. J Clin Orthod 1991;25:619-630.
9. Franzen TJ, Brudvik P, Vandevska-Radunovic V. Periodontal tissue reaction during orthodontic relapse in rat molars. Eur J Orthod. 2013;35:152-159.
10. Geramy A, Retrouvey JM, Sobuti F, Salehi H. anterior teeth splinting after orthodontic treatment: 3D analysis using finite element method. J Dent (Tehran). 2012;9:90-98.
11. Grajower R, Stern N, Zamir S, Kohavi D. Temporary space maintainers retained with composite resin. Part II: Fracture load in vitro. J Prosthet Dent 1981;45:49-51.
12. Haack DC, Haft EE. Ananalysis of stresses in a model of the periodontal ligament. Int J Eng Sci 1972;10: 1093-1106.
13. Heymann GC, Grauer D, Swift EJ Jr. Contemporary approaches to orthodontic retention. J Esthet Restor Dent 2012;24:83-87.
14. Human Research Act (810.30), Art. 2 and 32, Human Research Ordinance (810.301), Art. 30. 2015.
15. Joondeph DR. Retention and relapse. In Graber TM, Vanarsdall R, Vig KWI., eds. Orthodontics, current principles and techniques. 5th ed. Philadelphia: Elsevier Mosby; 2011:991-1019.
16. Kern M, Fechtig T, Strub J. Influence of water storage and thermal cycling on the fracture strength of all-porcelain, resin-bonded fixed partial dentures. J Prosthet Dent 1994;71:251-256.

31. Rossouw PE. Terminology: semantics of postorthodontic treatment changes in the dentition. Semin Orthod 1999;5:138-141.
32. Segner D, Heinrici B. Bonded retainers-clinical reliability. J Orofac Orthop 2000;61:352-358.
33. Shah AA. Postretention changes in mandibular crowding: a review of the literature. Am J Orthod Dentofacial Orthop 2003;124:298-308.
34. Vaden JL, Harris EF, Gardner RL. Relapse revisited. Am J Orthod Dentofacial Orthop 1997;111:543-553.
35. Van Schepdael A, Geris L, Van der Sloten J. Analytical determination of stress patterns in the periodontal ligament during orthodontic tooth movement. Med Eng Phys 2013;35:403-410.
36. World Medical Association (WMA): Declaration of Helsinki – Ethical Principles for Medical Research Involving Human Subjects. 64th WMA General Assembly, Fortaleza, Brazil, October 2013.
37. Xie Q, Lassila L, Vallittu P. Comparison of load-bearing capacity of direct resin-bonded fiber-reinforced composite FPDs with four framework designs. J Dent 2007;35:578-582.
38. Zachrisson BU. Multistranded wire bonded retainers: from start to success. Am J Orthod Dentofacial Orthop 2015;148:724-727.
101 100

Chapter 7
General discussion and clinical implications

104 105
the literature.6 However, before undertaking any clinical trials, more information
was targetted to be collected for adhesion and fatigue properties of such retainer
materials and compare their performance with the golden standard, stainless steel
wires.7 Interestingly however, adhesion results did not differ significantly between
any of the FRCs tested and the stainless steel wire when the wire was applied in
the bed of flowable resin and covered with flowable resin again.8 This indicated
that the amount of resin composite on the stainless steel wire was sufficient to
provide adequate adhesion. Nevertheless, failure types showed different trends
among the tested retainer materials, namely the stainless steel resulted in partial
debondings with less than half of the composite left on the enamel surface. On
the other hand, FRCs showed failures where more composite was left adhered
or more cohesive failures within the retainer material. This indicated in part the
limited flexibility of the FRC compared to the metal wires.
Such results highlighted the importance of interpretation of failure types rather
than evaluating the bond strength only. It was however still not clear whether
hydrothermal aging would be sufficient to simulate aging between wire-resin-
tooth interfaces. Therefore, the adhesion behaviour of the tested retainers
was further investigated under fatigue conditions where they were exposed to
100.000 cycles of fatigue at 37 °C in water.9 Fatigue cycling however, did not
show debonding of retainers. Hence, they were subsequently loaded until failure.
The results showed no significant difference in debonding force regardless of the
retainer type. Though, again failure types varied in that the stainless steel wire
showed higher incidence of cohesive failures in the overlying resin composite
followed by complete adhesive failure. On the contrary, E-glass (Angelus) and
S2 glass (Dentapreg) resulted in mainly complete adhesive detachment meaning
that adhesion was not favourable with these fibers. Polyethylene FRC on the
other hand, showed rather adhesive failures or FRC fractures both of which could
be considered unfavourable in clinical situations. In addition, PMMA impregnated
E-glass (Everstick) presented also complete adhesive or partial detachment of
resin composite, which was a low viscous one (Tetric Flow). Basically, none of
the retainer materials showed complete durability and most likely the flexibility
of the wire resulted in less complete debondings. However, the model employed
in this study consisted of only two teeth and in fact, in an arch segment different
force distribution could be expected. Since only flowable composite was used
in this study, it was also thought that the resin composite type could affect the
debonding rate of stainless steel retainers.
In order to answer this question, 150 retainers bonded using 2 hybrid and one
flowable resin composite were observed in a private practice setting.10 Similar to
the above-mentioned study at the university setting, also in this study multiple
operators were involved and no significant difference between the factors of age,
gender, location, and operators were noted. Although the use of flowable resin
GENERAL DISCuSSION AND FuTuRE PERSPECTIVES
This thesis evaluated several aspects of the clinical problem related to debonding
of bonded retainers used in orthodontics with a particular emphasis on retainer
material properties, adhesive resins and application modes of retainers.
Clinical problem – Retainer DebondingWithout a phase of retention, the teeth tend to relapse towards their initial
position after completion of the orthodontic treatment.1,2 Thus, durable retention
of the retainers are crucial in maintaining the achieved results. The objectives
of this thesis was initiated as a consequence of recognition of high incidence
of retainer debondings both based on the reports in the literature and our own
observations at the University of Groningen, Department of Orthodontics. Since
the stainless steel retainers were bonded with multiple operators and dental
hygienists at the university settings, it was anticipated that the operator factor
could be one factor affecting the incidence of such failures. Using the historic
cohort available, 277 patient recordings were retrospectively investigated with
the outcome measure of retainer debonding in an attempt to gain an overview
on possible factors affecting retainer debondings under the conditions when the
same retainer material (multi-stranded stainless steel wire) and adhesives were
used.3 Similar to previous findings, our results also indicated that most failures
occurred within the first 6 months and the gender and age did not affect the
failure incidence. Opposite to the expectations, operator factor was also disclosed
in failure incidence. However, 37% of failures already in a mean observation time
of 41 months were discouraging and created the need for the analysis of other
possible factors in these types of failures.
Adhesion and material perspectivesThe clinical problem of retainer debonding with stainless steel wires was expected
to be solved after the introduction of fiber reinforced composites (FRC) as retainer
materials in orthodontics.4 FRCs allow for larger bonding surface and that there
is more chemical adhesion of the resin composite to the FRC as opposed to the
stainless steel wires where mainly mechanical retention is present. At the early
phase of this thesis and soon after the introduction of FRC retainers in our clinic,
some cases were treated using FRC retainers of various kinds. It was however,
soon recognized that the application modes differed significantly between the
FRC products and that there were no guidelines available for practitioners.
Furthermore, while some FRC materials were readily preimpregnated with a
monomer resin, others had to be silanized and impregnated by the operator at
chairside which could affect their mechanical properties.5 Mechanical properties
due to fiber orientation and volume were mentioned in favour of glass FRCs in

106 107
stranded stainless steel wires should still be preferred over the use of FRC ones.
Starting with humidity control, slight enamel preparation in order to remove
the aprismatic enamel, calibration of the operators for adhesion protocols to be
employed, weekly controls of the output of the photo-polymerization devices, the
use of highly filled hybrid resin composites would most likely maximize the survival
of bonded orthodontic retainers. Since of the retainer debondings mostly occur
within the first 6 months after completion of the orthodontic treatment, strict
follow up of the patients is essential and therefore patients should be reimbursed
by the health care systems. Furthermore, clinical follow up studies should report
on more detailed information on failure location and types on the tooth and arch-
basis. Likewise, accurate methods should be developed for the measurement of
tooth displacement and possible associated simultaneous forces in vivo.
composite showed slightly higher incidence of retainer debondings, no significant
difference was found between resin composite materials during the follow up
period. The flowable resin used in this study was highly filled (62 v%) which
might have affected the results being more in favour of the one (Tetric Flow) used
in university settings presented in this thesis.10
Nevertheless, in a mean observation time of 43 months, 19.7% failures with
the vast majority occurring within the first 6 months indicated that retainer
debonding problem is not a consequence of material choice and perhaps more
related to post-treatment tooth displacement resulting in more tension between
the retainer-resin-tooth complex.
Tooth displacement- a reason for debonding?The use of multistranded wires was postulated to reduce the individual mobility
of the bonded teeth while maintaining physiologic mobility.11 On the contrary, with
the FRC materials, less mobility of teeth and thereby less incidence of retainer
debondings were expected. In the meantime, clinical studies reporting on the
survival of FRC retainers demonstrated survival of 49% in 2 years4, 79% in 1
year12,13 and 79.6% in 6 years.14 These figures clearly show that the debonding
problem is not completely resolved even with the use of FRC materials. Thus,
the most likely governing factor for retainer debonding was estimated to be the
tooth displacement after immediate orthodontic treatment. The amount of tooth
displacement was measured using 3D analysis where triangular target frames
and optoelectronic motion tracking device was employed. Based on the results,
mandibular anterior teeth showed less tooth mobility when bonded with stainless
steel wire compared to the non-bonded control group. The experimental model
showed very good reproducibility which could be used15 for further investigations
on tooth displacement in conjunction with FRC materials.
Concluding remarks and clinical implicationsThe results of a series of investigations and the clinical studies presented in this
thesis, clearly indicates that the retainer debonding in orthodontics is an unsolved
problem which occurs in a considerably short follow up time. Early observations
of debondings could not be related to fatigue related phenomena. In spite of
the fact that multiple factors have been attributed to the cause of this clinical
problem, in this thesis, at least several aspects such as age, gender, operator,
resin composite type could be disclosed.
Biological simulation of tooth displacement is a difficult task in laboratory
settings but future studies would focus on the parameter of tooth displacement
accompanied with rotational and torsional forces also involving differences in root
morphologies.
Based on the results obtained in this thesis and the available literature, multi-

108 109
REFERENCES
1. Al Yami EA, Kuijpers-Jagtman AM, van ‘t Hof MA. Stability of orthodontic treatment outcome: follow-up until 10 years postretention. Am J Orthod Dentofacial Orthop 1999;115:300-304.
2. Joondeph DR. Retention and relapse. In Graber TM, Vanarsdall R, Vig KWI., eds. Orthodontics, current principles and techniques. 5th ed. Philadelphia: Elsevier Mosby; 2011:991-1019.
3. Lie Sam Foek DJ, Özcan M, Verkerke GJ, Sandham A, Dijkstra PU. Survival of flexible, braided, bonded stainless steel lingual retainers: a historic cohort study. Eur J Orthod 2008:30:199-204.
4. Rose E, Frucht S, Jonas IE. Clinical comparison of a multistranded wire and a direct-bonded polyethylene ribbon reinforced resin composite used for lingual retention. Quintessence Int 2002;33:579-83.
5. Freilich MA, Karmaker AC, Burstone CJ, Goldberg AJ. Development and clinical applications of a light-polymerized fiber-reinforced composite. J Prosthet Dent 1998;80:311-318.
6. De Boer J, Vermilyea SG, Brady RE. The effect of carbon fiber orientation on the fatigue resistance and bending properties of two denture resins. J Prosthet Dent 1984;51:119-121.
7. Bearn DR. Bonded orthodontic retainers: a review. Am J Orthod Dentofacial Or-thop 1995;108:207-213.
8. Lie Sam Foek DJ, Özcan M, Krebs E, Sandham A. Adhesive properties of bonded orthodon-tic retainers to enamel: stainless steel wire vs fiber-reinforced composites. J Adhes Dent 2009;11:381-390.
9. Lie Sam Foek DJ, Yetkiner E, Özcan M. Fatigue resistance, debonding force, and failure type of fiber-reinforced composite, polyethylene ribbon-reinforced, and braided stainless steel wire lingual retainers in vitro. Korean J Orthod. 2013;43:186-192.
10. Lie Sam Foek DJ, Feilzer AJ, Özcan M. Clinical survival of multi-stranded stainless steel bonded lingual retainers as a function of resin composite type: Up to 3.5 years follow-up. (Unpublished data)
11. Zachrisson BU. Multistranded wire bonded retainers: From start to success. Am J Orthod Dentofacial Orthop 2015;148:724-727.
12. Sobouti F, Rakhshan V, Saravi MG, Zamanian A, Shariati M. Two-year survival analysis of twisted wire fixed retainer versus spiral wire and fiber-reinforced composite retainers: a preliminary explorative single-blind randomized clinical trial. Korean J Orthod 2016;46:104-110.
13. Scribante A, Sfondrini MF, Broggini S, D’Allocco M, Gandini P. Efficacy of esthetic retainers: clinical comparison between multistranded wires and direct-bond glass fiber-reinforced composite splints. Int J Dent 2011;548356.
14. Bolla E, Cozzani M, Doldo T, Fontana M. Failure evaluation after a 6-year retention period: a comparison between glass fiber-reinforced (GFR) and multistranded bonded retainers. Int Orthod 2012;10:16-28.
15. Chakroun F, Colombo V, Lie Sam Foek DJ, Gallo L, Feilzer AJ, Özcan M. Displacement of teeth without and with bonded fixed orthodontic retainers: 3D analysis using triangular tar-get frames and optoelectronic motion tracking device. (Unpublished data).

Chapter 8
Summary

112 113
Specimens were thermocycled for 6000 cycles between 5-55°C and loaded in
a universal testing machine under shear stress (crosshead speed: 1 mm/min)
until debonding occurred. The failure sites were examined under an optical light
microscope. Significant differences were found between the groups (p = 0.0011).
Bond strength results did not significantly differ neither between the FRC groups
(Groups 1-4) (6.1±2.5 to 8.4±3.7 MPa) (p > 0.05) or the wire groups (Groups
5-8) (10.6±3.8 to 14±6.7 MPa) (p > 0.05). Failure types varied within the FRC
groups, but mainly composite was found left adhered on the enamel surface
at varying degrees. In the stainless steel wire groups, when the retainer was
applied onto the bonding agent and then covered with flowable resin, partially
attached composite on the enamel was often found after debonding. When the
wires were embedded in the flowable composite, the Heliobond group (Group
8) showed more adhesive failures between the enamel and the composite
compared to Group 5, where bonding agent was Stick Resin. Regardless of their
application mode, stainless steel orthodontic bonded retainers delivered higher
bond strengths than those of fiber retainers. The differences were statistically
significant compared to those of Angelus Fibrex Ribbon and DentaPreg Splint.
The aim of Chapter 4 was to analyze the fatigue resistance, debonding force, and
failure type of fiber-reinforced composite, polyethylene ribbon-reinforced, and
braided stainless steel wire lingual retainers in vitro. Roots of human mandibular
central incisors were covered with silicone, mimicking the periodontal ligament,
and embedded in polymethylmethacrylate. The specimens (N = 50), with two
teeth each, were randomly divided into five groups (n = 10/ group) according
to the retainer materials: (1) Interlig (E-glass), (2) everStick Ortho (E-glass), (3)
DentaPreg Splint (S2-glass), (4) Ribbond (polyethylene), and (5) Quad Cat wire
(stainless steel). After the recommended adhesive procedures, the retainers
were bonded to the teeth by using flowable composite resin (Tetric Flow). The
teeth were subjected to 10,00,000 cyclic loads (8 Hz, 3 - 100 N, 45o angle,
under 37 ± 3°C water) at their incisoproximal contact, and debonding forces
were measured with a universal testing machine (1 mm/min crosshead speed).
Failure sites were examined under a stereomicroscope (×40 magnification). All
the specimens survived the cyclic loading. Their mean debonding forces were
not significantly different (p > 0.05). The DentaPreg Splint group (80%) showed
the highest incidence of complete adhesive debonding, followed by the Interlig
group (60%). The everStick Ortho group (80%) presented predominantly partial
adhesive debonding. The Quad Cat wire group (50%) presented partial overlying
composite detachment. Cyclic loading did not cause debonding. The retainers
presented similar debonding forces but different failure types. Braided stainless
steel wire retainers presented the most repairable failure type.
In Chapter 5, in a prospective clinical trial the survival of multi-stranded stainless
steel lingual retainers (SSR) bonded using different resin composite types was
The debonding of bonded orthodontic retainers is one of the most frequently
reported failure type in orthodontics as a consequence of multiple reasons. This
thesis was conducted in an attempt to identify some of the possible factors
causing the failure of bonded orthodontic retainers.
The objectives of the retrospective clinical study in Chapter 2 were to evaluate the
clinical survival rate of flexible, braided, rectangular bonded stainless steel lingual
retainers, and to investigate the influence of gender, age of the patient, and
operator experience on survival after orthodontic treatment at the Department
of Orthodontics, University of Groningen, between the years 2002 and 2006.
The study group comprised of 277 patients (162 females: median age 14.8 years
and 115 males: median age 15.3 years). Data concerning, failures, gender, age
of the patient, and operator experience were retrieved from the patient files that
were updated by chart entries every 6 months or when failure was reported by
the patient. The maximum follow-up period was 41.7 months. All 277 patients
received flexible, braided, bonded mandibular canine-to-canine retainers. A failure
was recorded when there was debonding, fracture, or both, occurring in one arch.
Eighteen failures were observed in the maxilla. Only first failures were used for
statistical analysis. Ninety-nine debonding (35.7%), two fractures (0.7%), and four
debonding and fracture (1.4%) events were observed. No significant effect (P
> 0.05) of gender (females: 41%, males: 32%) or patient age (<16 years: 37%,
≥ 16 years 38.7%) was observed. The failure rate did not differ due to operator
experience (n = 15; less experienced: 38.0%; moderately experienced: 28.9%,
professional: 46.7%; P > 0.05). Kaplan- Meier survival curves showed a 63%
success rate for the bonded lingual retainers over a 41.7 month period.
In Chapter 3 the bond strength of a stainless steel orthodontic wire was
compared versus various fibre-reinforced-composites (FRC) used as orthodontic
retainers on enamel, analyze the failure types after debonding and to investigate
the influence of different application procedures of stainless steel wires on
bond strength. Caries-free, intact human mandibular incisors (N=80, n=10 per
group) were selected and randomly distributed into 8 groups. After etching with
37% H3PO4 for 30 seconds, rinsing and drying, bonding agent (Stick Resin) was
applied, light polymerized and one of the following FRC materials were applied
on the flowable composite (Stick Flow) using standard molds: Group 1: Angelus
Fibrex Ribbon; Group 2: DentaPreg Splint; Group 3: everStick Ortho and Group
4: Ribbond. In Group 5, Quad Cat Wire was applied in the same manner as in
FRC groups. In Group 6, after bonding agent (Stick Resin), Quad Cat Wire was
placed directly on the tooth surface and covered with Stick Flow composite. In
Group 7, after bonding agent (Heliobond) was applied, Quad Cat Wire was placed
directly on the tooth surface and covered with Tetric Flow composite. In Group 8,
after applying bonding agent (Heliobond), Tetric Flow composite was applied, not
polymerized and Quad Cat Wire was placed and covered with Tetric Flow again.

114 115
was tested for tooth mobility by applying force increasing from 5 to 30 N with 5 N
increments applied perpendicular on the lingual tooth surface on the incisal one
third (crosshead speed: 0.1 mm/s). The teeth on each model were first tested
without retainer (control) and subsequently with the bonded retainers (braided
bonded retainer wire; Multi-strand 1x3 high performance wire, 0.022” x 0.016”).
Tooth displacement was measured in terms of complicance (F/Δ movement) (N/
mm) using custombuilt optoelectronic motion tracking device (OPTIS) (accuracy:
5 mm; sampling rate: 200 Hz). The position of the object was detected through
three LEDs positioned in a fixed triangular shape on a metal support (Triangular
Target Frame). The measurements were repeated for three times for each tooth.
The use of retainer showed a significant effect on tooth mobility compared to
non-bonded teeth (control) (p<0.0001). The amount of displacement on the tooth
basis was also significantly different (p=0.0381) being the most for tooth no. 42
(without: 0.024±0.01; with: 0.012±0.002) (p=0.0018).
evaluated. Between April 2011 and March 2013, a total of 75 patients (40 women,
35 men; mean age: 16.3 years old) received full arch orthodontic treatment after
which SSRs (Multi-strand 1 x 3 high performance wire, 0.022” x 0.016”, PG
Supply Inc.) (N=150) were bonded in the maxilla and/or mandible on all 6 anterior
teeth. After etching enamel surfaces with 35% H3PO4, adhesive resin was
applied (Clearfil SE Bond) and photo-polymerized for 20 s. SSRs were bonded
using one of the following resin composites: a) Hybrid (Clearfil AP-X, Kuraray
Noritake) (H1), b) Hybrid (Light Cure Retainer, Reliance Orthodontic Products Inc.)
(H2), c) Flowable (Clearfil Majesty Flow, Kuraray) (FL). At baseline and thereafter
at 1, 2, 3, 6, 12 and 24 months, SSRs were checked upon macroscopically for
partial or complete debonding or fracture. SSRs were scored as failed if any
operative intervention was indicated for repair, partial or total replacement.
SSRs were observed for a minimum of 6, and maximum 43 months (mean: 19.5
months). At the final control (24 months), 10 patients could not be followed up
(H1: 12, H2: 4, FL: 4) due to drop out. In total, in 150 SSRs, 28 failures were
observed (n=19 in the maxilla, n=9 in the mandible). The majority of the failures
were observed with FL (n=12), followed by H1 (n=8) and H2 (n=8) being not
statistically significant (maxilla: p=0.133; mandible: p=0.551). Overall, 3 fractures
of the SSR were observed all of which were in the maxilla. In total, cumulative
survival rate was 81.3% up to 43 months (Kaplan-Meier). Location of the SSRs
did not show significant difference (maxilla: 74.7%, and mandible: 88%) (p>0.05).
No significant difference was observed between gender type (female: 78.8%;
male: 81.3%) (p=0.059). Although microhybrid flowable resulted in slightly more
frequent incidence of failures, the type of composite, the location and the gender
did not significantly affect the clinical survival of multi-stranded stainless steel
bonded lingual retainers in the studied sample.
In Chapter 6 the objective was to evaluate the anterior tooth movement without
and with bonded fixed orthodontic retainers under incremental loading conditions.
Six extracted mandibular anterior human teeth were embedded in acrylic resin
in True Form I Arch type and 3D reconstruction of Digital Volume Tomography
(DVT) images (0.4 mm3 voxels) were obtained. The anatomy of each tooth was
segmented and digitally reconstructed using 3D visualization software for medical
images (AMIRA, FEI SVG). The digital models of the teeth were repositioned
to form an arch with constant curvature using a CAD software (Rhinoceros)
and a base holder was designed fitting the shape of the roots. The clearance
between the roots and their slot in the holder was kept constant at 0.3 mm
to replicate the periodontal ligament thickness. The holder and the teeth were
then manufactured by 3D printing (Objet Eden 260VS, Stratasys) using a resin
material for dental applications (E=2-3 GPa). The 3Dprinted teeth models were
then positioned in the holder and the root compartments were filled with silicone.
The procedure was repeated to obtain three identical arch models. Each model

Chapter 9
Samenvatting

118 119
Flow) waarbij gebruik gemaakt werd van gestandaardiseerde mallen: Groep 1:
Angelus Fibrex Ribbon; Groep 2: DentaPreg Splint; Groep 3: everStick Ortho and
Groep 4: Ribbond. In Groep 5, werd Quad Cat draad op dezelfde manier als in de
FRC-groepen vastgeplakt. In Groep 6 werd, na het appliceren van een bonding
agent (Stick Resin), Quad Cat draad direct op het tandoppervlak geplaats, waarna
deze werd bedekt en vastgezet met Stick Flow composiet. In Groep 7 werd, na
het appliceren van een bonding agent (Heliobond), Quad Cat draad direct op het
tandoppervlak geplaatst, waarna deze werd bedekt en vastgezet met Tetric Flow
composiet. In Groep 8 werd, na het appliceren van een bonding agent (Heliobond),
het tandoppervlak eerst bedekt met een laag van Tetric Flow composiet doch nog
niet uitgehard. Vervolgens werd het Quad Cat draad geplaats, waarna er opnieuw
een laag Tetric Flow overheen werd geplaatst en uitgehard. De proefmonsters
ondergingen vervolgens een thermische veroudering van 6000 cycli tussen
5-55°C, waarna zij werden belast door een universal testing machine onder schuif
krachten (1 mm/min) tot dat debonderig optrad. Alle mislukkingen werden onder
een optische licht microscoop bekeken en geanalyseerd. Significante verschillen
werden gevonden tussen de verschillende groepen (p = 0.0011). Resultaten
met betrekking tot de hechtsterkte verschilden niet significant tussen de FRC-
groepen (Groepen 1-4) (6.1±2.5 to 8.4±3.7 MPa) (p > 0.05) en de draad groepen
(Groepen 5-8) (10.6±3.8 to 14±6.7 MPa) (p > 0.05). De mislukkingen varieerden
in de FRC-groepen, waar voornamelijk alleen composiet in verschillende mate
gefixeerd aan het glazuur gevonden is. In de roestvrijstalen draad groepen,
waarbij de draad spalk direct op de bonding agent geplaatst werd en waarna
deze afgeplakt werd met een flowable composiet werd veelal gedeeltelijke
composiet breuk waargenomen. Wanneer de draad spalken na het appliceren
van een bonding agent in een bedje van flowable composiet werden geplaatst
en vervolgens weer afgedicht werden met dezelfde composiet, de Heliobond
groep (Group 8) werden meer adhesieve mislukkingen tussen het glazuur en de
composiet waargenomen dan in vergelijking met Groep 5, waar de bonding agent
Stick Resin was. Ongeacht de applicatie methode vertoonden de roestvrijstalen
draad spalken de grootste hechtsterkte waarden in vergelijking met de FRC’s.
De verschillen bleken statistisch significant in vergelijking met de groepen van
Angelus Fibrex Ribbon and DentaPreg Splint.
In Hoofdstuk 4 werd de verouderingsresistentie, debondeer kracht en type
mislukkingen van glasvezel versterkte composieten en gevlochten roestvrijstalen
retentie spalken in vitro onderzocht. De radices van humane, mandibulaire
centrale incisieven werden bedekt met een flinterdun siliconen laag, teneinde
het parodontaal ligament na te bootsen en waarna deze ingebed werden in
polymethylmethacrylate. De test monsters (N = 50), elk met 2 incisieven,
werden gerandomiseerd verdeeld in vijf groepen (n = 10/ groep) aan de hand
van het retainer materiaal: (1) Interlig (E-glass), (2) everStick Ortho (E-glass), (3)
Het debonderen van orthodontische retentie spalken is een veel voorkomend
en ruim beschreven probleem, waarbij gedacht wordt dat de mogelijke oorzaak
multifactorieel van aard is. Het doel van het onderzoek dat onderwerp is van
dit proefschrift, is om mogelijke factoren met name vanuit materiaalkundig
perspectief, die voor het debonderen van deze retentie spalken zorgen te
identificeren.
In Hoofdstuk 2 wordt retrospectief gekeken naar het klinische succespercentage
van flexibele, gevlochten, rechthoekige, roestvrijstalen retentie spalken en
de invloed van geslacht, leeftijd van de patiënt en ervaring van de operateur
in relatie tot het succespercentage aan Afdeling Orthodontie, Universiteit van
Groningen, van patiënten behandeld tussen 2002 en 2006. De onderzoeksgroep
bestond uit 277 patiënten (162 meisjes: met een gemiddelde leeftijd van 14.8
jaar en 115 jongens: met een gemiddelde leeftijd van 15.3 jaar). Alle benodigde
gegevens inzake het debonderen, geslacht, leeftijd van de patiënt en ervaring
van de operateur is verkregen uit de patiëntenkaarten welke om de zes maanden
bijgewerkt werden of wanneer er een debond plaatsvond. De maximale follow-
up periode bedroeg 41.7 maanden. Alle 277 patiënten kregen een retentie spalk
in de onderkaak, welke van de hoektand tot de hoektand liep en welke op alle
elementen van het onderfront bevestigd was. Een faalmoment of mislukking
werd gescoord wanneer er een debonding, draadbreuk of een combinatie
van één van deze optrad. Achttien faalmomenten werden geobserveerd in de
maxilla. Alleen het eerste moment van mislukking werd gescoord en gebruikt
voor de statistische analyse. Negenennegentig debonderingen (35.7%), twee
draadbreuken (0.7%), en vier mislukkingen met een combinatie van beide (1.4%)
werden geobserveerd. Geen significant effect (P > 0.05) voor leeftijd (meisjes:
41%, jongens: 32%), patiënten leeftijd (<16 jaar: 37%, ≥ 16 jaar 38.7%) werd
geobserveerd. Het percentage voor falen van een retentie spalk bleek ook voor de
ervaring van de operateur niet significant te zijn (n = 15; weinig ervaring: 38.0%;
gemiddelde ervaring: 28.9%, professional: 46.7%; P > 0.05). Kaplan- Meier
overleving curves weergaven een succespercentage van 63% voor gefixeerde
linguale retentie spalken weer over een periode van 41.7 maanden.
In Hoofdstuk 3 is de hechtsterkte van roestvrijstalen retentie spalken vergeleken
met verschillende glasvezel versterkte composieten (FRC), welke als retentie
spalk op glazuur zijn geplakt en vervolgens geanalyseerd op het faal type.
Tevens is er ook gekeken naar de invloed van verschillende applicatie methoden
van roestvrijstalen retentie spalken en hun hechtsterkte. Intacte, cariës-vrije,
humane mandibulaire incisieven (N=80, n=10 per groep) werden geselecteerd
en gerandomiseerd verdeeld in acht groepen. Na etsen met 37% H3PO4 voor
30 seconden, spoelen en drogen, werd er een bonding agent (Stick Resin)
geappliceerd, met behulp van licht uitgehard en vervolgens werd één van de
volgende FRC materialen geplakt op een bedje van flowable composiet (Stick

120 121
DentaPreg Splint (S2-glass), (4) Ribbond (polyethylene), en (5) Quad Cat wire
(roestvrij staal). Na de geadviseerde adhesieve procedure, werden de retainers
geplakt op de tanden met een flowable composiet (Tetric Flow). De monsters
ondergingen vervolgens cyclische belasting van 10,00,000 (8 Hz, 3 - 100 N, 45o
hoek, onder 37 ± 3°C water). Aan hun incisoproximale contactpunt, werden de
debonding krachten gemeten met een universal testing machine (1 mm/min
crosshead speed). De exacte locaties en type mislukkingen werden beoordeeld
met behulp van een stereomicroscoop (×40 vergroting). Alle monsters
overleefden de cyclische belasting. De gemiddelde debondeer krachten bleken
niet significant te verschillen (p > 0.05). De DentaPreg Splint groep (80%)
vertoonde het meeste aantal complete adhesieve debonderingen, gevolgd door
de Interlig groep (60%). De everStick Ortho groep (80%) vertoonde voornamelijk
partiële adhesieve debonderingen. De Quad Cat draad groep (50%) vertoonde
voornamelijk het gedeeltelijk losraken van het overliggende composiet. Cyclische
belasting resulteerde niet in debonderingen. De retainers presenteerden allemaal
vergelijkbare debondeer krachten, maar verschillende typen mislukkingen. De
roestvrijstalen retentie spalken vertoonden de meest eenvoudig te repareren
mislukkingen.
In Hoofdstuk 5, is prospectief de levensduur van de roestvrijstalen, gevlochten,
draad retentie spalken (SSR) klinisch onderzocht aan de hand van verschillende
typen composiet. Van april 2011 tot en met maart 2013 kregen in totaal 75
patiënten, (40 meisjes, 35 jongens; gemiddelde leeftijd: 16.3 jaar oud) na
behandeld te zijn met volledige, vaste orthodontische apparatuur, een linguale
retentie spalk in zowel de boven- als de onderkaak. Zowel in de bovenkaak als de
onderkaak werd de retentie spalk SSRs (Multi-strand 1 x 3 high performance wire,
0.022” x 0.016”, PG Supply Inc.) (N=150) op alle 6 anterieure tanden geplakt. Na
het etsen van de glazuur oppervlakken met 35% H3PO4, werd bonding geplaatst
(Clearfil SE Bond) en met behulp van licht uitgehard voor 20 s. Alle SSRs werden
hierna vastgeplakt met één van de volgende composieten: a) Hybrid (Clearfil AP-
X, Kuraray Noritake) (H1), b) Hybrid (Light Cure Retainer, Reliance Orthodontic
Products Inc.) (H2), c) Flowable (Clearfil Majesty Flow, Kuraray) (FL). Vanaf T=0 en
hierna, 1, 2, 3, 6, 12 en 24 maanden, werden de SSRs klinisch beoordeeld op partiële
of complete debonderingen of op draadfractuur. Een SSRs werd als mislukking
gescoord wanneer er (reparatieve) interventie nodig was, bij het zij partiële of
totale vervanging en reparatie. Alleen eerste mislukkingen werden gescoord. Alle
SSRs werden ten minste zes maanden en maximaal 43 maanden na plaatsing
gevolgd en beoordeeld (gemiddelde observatie tijd: 19.5 maanden). Bij de finale
controlegroep (24 maanden), konden 10 patiënten niet vervolgd worden (drop-
outs) (H1: 12, H2: 4, FL: 4). In totaal, werden bij de 150 SSRs, 28 mislukkingen
waargenomen (n=19 in de bovenkaak, n=9 in de onderkaak), waarbij de meeste
mislukkingen geobserveerd werden in de FL groep (n=12), gevolgd door de H1
groep (n=8) en tot slot de H2 groep (n=8). Al deze mislukkingen bleken statistisch
niet significant (bovenkaak: p=0.133; onderkaak: p=0.551). Over het geheel
werden drie draadbreuken van de SSR’s waargenomen, welke allemaal in de
bovenkaak voorkwamen. Het totale, cumulatieve overlevingspercentage bedroeg
81.3% voor een totale periode van 43 maanden (Kaplan-Meier). De locatie van de
SSRs bleek niet significant te verschillen (bovenkaak: 74.7%, en onderkaak: 88%)
(p>0.05). Zo werd ook geen statistische significantie waargenomen voor het
geslachtstype en leeftijd (meisjes: 78.8%; jongens: 81.3%) (p=0.059). Hoewel
de microhybride flowable composiet net iets meer mislukkingen vertoonde,
bleek ook het verschil in gebruikte composiet types de klinische levensduur van
gevlochten roestvrijstalen retentie spalken niet significant te beïnvloeden.
Het doel van Hoofdstuk 6 was om de mate van anterieure tand verplaatsing
in of zonder de aanwezigheid van een retentie spalk onder dezelfde condities
te onderzoeken. Zes geëxtraheerde, humane mandibulaire snijtanden en
hoektanden werden in een acrylhars ingebed. Vervolgens werden deze modellen
3D gereconstrueerd met behulp van Digital Volume Tomography (DVT), waarna
hier foto’s (0.4 mm3 voxels) van zijn vervaardigd. De anatomie van elk element
werd gesegmenteerd en digitaal gereconstrueerd middels 3D visualisatie
software voor medische foto’s (AMIRA, FEI SVG). De hieruit verkregen digitale
informatie van deze zes elementen werd volgens een in de orthodontie veel
voorkomende boogvorm, de True Form I Arch type, gepositioneerd en met
behulp van CAD software (Rhinoceros) werd er een zogenaamde basishouder
vervaardigd. De exacte en hierbij horende inclinatie en angulatie van de radices
werd hierin geprogrammeerd. Er werd een vaste vrije ruimte rondom elke radix
en de basishouder (0.3 mm) gecreëerd. Zowel de houder als de elementen
werden vervaardigd met behulp van 3D printing (Object Eden 260VS, Stratasys),
waarbij gebruik gemaakt is van materiaal voor tandheelkundige doeleinden.
(Clear Biocompatible, MED 610, Stratasys, Commerce Way Eden Prairie) (E=2-
3 GPa). Vervolgens werden de 3D geprinte elementen geplaatst in de houder
en werd de vrije ruimte tussen de houder en de elementen met siliconen
opgevuld met als doel het parodontaal ligament na te bootsen. De procedure
werd in totaal drie keer herhaald onder exact dezelfde condities. Elk model
werd getest op tandverplaatsing waarbij elke tand onderworpen werd aan
krachten variërend tussen de 5 tot 30 N en waarbij er elke keer stappen van
5 N werden aangebracht perpendiculair aan de linguale tandoppervlakken van
het incisaal 1/3 deel van de tand (crosshead speed: 0.1 mm/s). De elementen in
het model werden eerst getest zonder de aanwezigheid van een retentie spalk
(controlegroep) en vervolgens met een retentie spalk (braided bonded retainer
wire; Multi-strand 1x3 high performance wire, 0.022” x 0.016”, PG Supply Inc. Avon, Connecticut, U.S.A). Tandverplaatsing werd gemeten met behulp van een
specifiek hiervoor vervaardigde optoelectronische, bewegingvolgend apparaat

122 123
(OPTIS) (nauwkeurigheidsgraad: 5 mm; sampling rate: 200 Hz). Hierbij werd de
positie van het element met behulp van drie LEDs, welke triangulair gefixeerd
waren aan een metalen standaard, gemeten. Alle metingen werden voor elk
model en voor elk element in drievoud herhaald. Het gebruik van een retentie
spalk vertoonde een significant effect op tandverplaatsing (0.008±0.004),
in vergelijking met de modellen zonder een retentie spalk (controlegroep)
(0.014±0.009) (p<0.0001). Het verschil in tandverplaatsing bij de basis van de
elementen bleek ook statistisch significant te zijn (p=0.0381), waarbij dit het meest
gold voor tand nummer 42 (zonder retentie spalk: 0.024±0.01; met retentie spalk:
0.012±0.002) (p=0.0018). Er werd statistisch geen verschil gevonden tussen
de herhaalde metingen(p=0.097) en het stapsgewijs verhogen van de kracht
(5-30 N: 0.07±0.01- 0.09±0.02) (p>0.05). Het mandibulair onderfront segment,
bestaande uit snijtanden en hoektanden vertoonde een verminderde mate van
tandverplaatsing wanneer er een retentie spalk van roestvrijstaal werd gebruikt
in vergelijking met de elementen waarbij er geen retentie spalk werd gebruikt.
Echter varieerde de mate van tandverplaatsing per element type en bleek een
verhoging van de kracht tussen de 5 en 30 N de mate van tandverplaatsing niet
te vergroten.

Acknowledgement

126 127
tandheelkunde heb ik de verschillende practica Materiaalkunde, onder jouw lei-
ding mogen volgen. Zelf had ik nooit gedacht dat wij elkaar, nu onder deze om-
standigheden, weer zouden tegenkomen. Dank voor jouw bereidwilligheid om te
opponeren.
Dr. I. Nedeljkovic, member of the reading committee, Dear Ivana thank you for
your willingness to participate as a member of the reading committee. Thank you
for getting in touch via Linkedin.
Dr. T. J. Algera, lid van de leescommissie, Beste Tjalling, hartelijk dank voor jouw
enthousiaste reactie tijdens het BSSO-congres in Haarlem en jouw bereidwillig-
heid om te opponeren en derhalve zitting te nemen in de leescommissie.
Prof. dr. A. Sandham, Dear Andrew, I started the post graduate specialty training
under your supervision which I really enjoyed. Although the time we have worked
together was limited due to your departure to Australia, I admired your way of
finding solutions for problems, within and through your internationally orientated
circle of colleagues. I hope all is well and wish you all the best. Thank you for all
your help.
Prof. dr. y. Ren, beste Yijin, de opleiding tot orthodontist heb ik na prof. dr. A.
Sandham onder uw leiding mogen afronden. Wetenschappelijk gezien was dit
voor mij een roerige periode daar ook prof. dr. M. Özcan naar Zürich vertrok. Hier-
door hebben wij ondanks ieders beste intenties nooit de lopende projecten zoda-
nig samen kunnen integreren dat deze vruchtbaar waren. Dit vind ik oprecht heel
spijtig, daar ik Groningen en de faculteit nog altijd een zeer warm hart toe draag.
Desalniettemin, wil ik u oprecht dankzeggen voor alle hulp en inspanningen.
Drs. M. Bierman, beste Michiel, ik heb mijn klinische opleiding onder jouw su-
pervisie genoten. Een goed, waar ik jou elke dag zeer dankbaar voor ben. Het is
niet altijd even gemakkelijk geweest, maar nu ik zelf full-time in de praktijk werk,
begrijp ik jou eindelijk een heel stuk beter. Ik ben jouw opmerking tijdens de Oud
Assistentendag in ‘t Feithhuis, onder het genot van een goed glas wijn; je moet
het afmaken!, nooit vergeten. Ik wil jou oprecht bedanken dat jij, ondanks enige
moeite in het begin, mij toch hebt gesteund dit onderzoek te continueren en af te
maken. Alle goeds wens ik jou en jouw familie toe.
Dhr. A. Wietsma, Beste Anne, ik wil jou bedanken voor jouw praktische hulp,
jouw bescheidenheid, doch zeer rijke klinische ervaring en jouw hulp met het
ontwikkelen van alle siliconen mallen en samen proefondervindelijk een opstelling
bedenken welke uiteindelijk geresulteerd heeft in een gepubliceerd artikel. Nu de
3D technologie verder ontwikkeld is, hebben wij onze ideeën van toen uitgebreid
en kunnen optimaliseren waardoor wij hopelijk weer een stapje dichterbij zijn bij het
antwoord op de vraag ‘wat gebeurt er nou eigenlijk’. Dank voor alle hulp.
DANKWOORD (ACKNOWLEDGEMENTS)
Naar alle waarschijnlijk is dit het meest toegankelijke deel van het proefschrift dat
bovendien door veel mensen vaak als eerste wordt gelezen. Wat mij betreft is
dat volkomen terecht, want vanzelfsprekend is mijn proefschrift geen ‘one man
show’. Het is tot stand gekomen dankzij de hulp van velen. Mijn dank gaat dan
ook uit naar alle personen die mij gesteund hebben bij het verwezenlijken hiervan.
Graag wil ik bij deze gelegenheid stil staan en een aantal mensen persoonlijk
bedanken.
Prof. dr. M. Özcan, hooggeleerde eerste promotor, Dear Mutlu, this journey
started a long time ago in the basement of the faculty of Dentistry in Gronin-
gen. Young and not knowing at all where this journey would end, we joined
forces. Although it took some time to get this Phd done, we finally finished it.
I would sincerely like to thank you for all your effortless help, drive, dedication,
love of honest and sound dentistry which always gets me enthusiastic, your hon-
est and upfront feedback, but most of all I would like to thank you for becoming
and being a dear friend. Without you, I would not be standing here today. It has
really been a privilege being able to work with you. Not knowing what the future
holds for us, I wish you well and thank you for everything!
Prof. dr. A.J. Feilzer, hooggeleerde tweede promotor, beste Albert. De cirkel is
rond. Ik heb mijn studie Tandheelkunde in Amsterdam genoten en nu sta ik hier
weer, dit keer echter ter verdediging van mijn proefschrift. In de korte tijd dat ik
jou als promotor heb mogen leren kennen, heb ik jouw manier van wetenschap-
pelijk denken in relatie tot de klinische toepasbaarheid leren waarderen. Dit is een
manier van werken en denken die mij heel erg aanspreekt. Dank voor jouw snelle
en kritische, doch praktische kijk op zaken. Dank voor alle hulp.
Prof. dr. M.S. Cune, lid van de leescommissie, beste Marco, erg fijn dat jij in
de beoordelingscommissie van mijn promotie wilt participeren. Bedankt hiervoor.
Hoewel ik jou nog niet in ‘real life’ de hand heb mogen schudden, werken wij al
geruime tijd samen in de praktijk. Ik waardeer de prettige en hoogwaardige sa-
menwerking tussen ons bij al die ingewikkelde, multidisciplinaire casussen, wel-
ke wij samen mogen behandelen. Ik zou het oprecht fijn vinden (ondanks onze erg
drukke agenda’s) een keer rustig samen te kunnen zitten, teneinde van gedachten
te wisselen hoe wij deze moeilijke behandelingen kunnen verbeteren. Dank voor
de zeer fijne samenwerking.
Prof. dr. F.J. M. Roeters, lid van de leescommissie, beste Joost, hartelijk dank dat
u tijdens mijn promotie wil opponeren.
Prof. Dr. C.J. Kleverlaan, lid van de leescommissie, Beste Cees, als student

128 129
Sandra Tolhuizen, lieve Sandra, ik wil jou ook hartelijk bedanken voor je lange en
rijke ervaring in dit vak, jouw bereidwilligheid om samen de protocollen te bedenken
en de daar uit voortvloeiende klinische handelingen te plannen, welke de basis zijn
geweest voor dit onderzoek. Je bent altijd positief en flexibel. Dank voor al jouw hulp
bij het samen plaatsen van alle (glasvezel) spalken, het leerrijk weekend in het mega
koude Turku, Finland, na een gecancelde vlucht en een busrit waarbij je het gevoel
kreeg alsof wij op weg waren naar de Noordpool. Maar vooral dank voor de leuke tijd
samen tijdens de opleiding. Alle goeds voor jou en de boys.
Dr. T.J.M. Van Steenbergen, beste Martijn dank dat jij mij tijdens deze ‘high
stress period’ op een zeer plezierige en goede manier hebt weten te leiden en dat
jij mij hebt bijgestaan. Excuses voor al mijn foutjes, maar fijn dat wij naderhand
hierom konden lachen.
Dr. N. Al-Haj Husain, dear Nadin, it is finally finished. I would sincerely like to thank
you for always being there to help us. All the long weekends at the University, late
on saturday night or very early on the sunday mornings. Thank you for helping me
with all the figures and always making sure, we never had an empty stomach. Thank
you for everyting! I wish you all the best in Bern.
Dr. B. van Eggermont – Oosterkamp, beste Barbara, dank voor jouw hulp en advies
op cruciale momenten tijdens deze reis. Zonder jouw advies, was ik Mutlu wellicht
nooit tegengekomen en al helemaal niet op het juiste moment. Zo ook op het mo-
ment toen ik het even niet meer zag zitten om dit traject überhaupt af te ronden.
Dank voor jouw positieve en praktische kijk op zaken. Ik wens jou, Bas en de kids
alle goeds toe en bovenal goede gezondheid.
Jaargenoten: Dima, Heleen, Manon en Huib, bedankt voor de leuke tijd samen
tijdens de opleiding! De tosti’s kan ik inmiddels weer ‘verdragen’, maar wat een
tijd was dat vergeleken met nu. We zien elkaar helaas niet zo vaak meer, daar een-
ieder druk aan het werk is in de praktijk. Toch denk ik nog altijd met veel plezier en
waardering voor jullie allemaal terug aan de tijd die wij samen hebben doorgebracht.
Oprecht wens ik jullie allen zowel in het vak, maar zeer zeker ook privé alle goeds
toe. Speciaal voor jullie een dikke kus van Baba Ganoush en ik hoop jullie eens een
keer weer te zien aan de Pfeillgasse (mit Auspuff!) Dank voor alles.
Drs. Mr. A.M. Essed, beste oom Thoon, dank voor uw positieve, doch kriti-
sche noot(en)! Ik waardeer u en tante Thecla zeer en zal de herhaaldelijke vraag
‘WANNEER is het proefschrift nu eindelijk af’ ECHT nooit meer vergeten. Zonder
uw aanmoediging, oprechte gesprekken en hulp, vanaf het begin (1997-1998)
stond ik hier vandaag niet. Tot de dag van vandaag, waardeer ik het ritje naar het
Alto Visto kapel te Aruba! Many thanks voor alles en nu samen een goed glas
wijn heffen!
Dr. F.L. Gulje, Beste Felix, zonder jouw hulp hadden Michel en ik ons nooit kun-
nen vestigen in Apeldoorn. Hier ben ik jou zeer erkentelijk voor. De bereidheid
om jouw vakkundigheid en berg aan klinische ervaring te delen, waardeer ik zeer.
Maar het is vooral de laagdrempeligheid en gelijkwaardigheid waarin wij elkaar
kunnen aanspreken over moeilijke multidisciplinaire behandelingen wat ik erg
prettig vind. Ik hoop dat wij nog lang samen mogen werken. Dank voor alles.
Team Mondhoek, Beste Jessica, Azzie en dames. Dank dat jullie ons destijds
onderdak hebben geboden en oprecht dank voor de zeer prettige samenwerking.
Alle collegae (verwijzers) Apeldoorn en omstreken, Geachte collegae, zonder
jullie kunnen wij er niet zijn. Ik zou graag van de gelegenheid gebruik willen ma-
ken en jullie oprecht dankzeggen voor het in mij (ons) gestelde vertrouwen. Als
broekies een praktijk opzetten lijkt eenvoudig, maar is het helemaal niet. Dit is ons
dan ook niet geleerd tijdens de opleiding. Vallen en weer opstaan in de breedste
zin van het woord, heeft ervoor gezorgd dat wij nu zijn waar wij nu zijn. Elke dag
is weer een nieuwe dag en elke dag leren wij weer van elkaar, met elkaar en van
onze patiënten. Ik hoop nog lang samen met u allen op dezelfde plezierige manier
te mogen samenwerken.
Kaakchirurgie Gelre Ziekenhuizen, Apeldoorn, Beste Peter en Steven, Rob en
Bert- Jan, ook jullie wil ik bedanken voor de plezierige en hoogwaardige samen-
werking. We begonnen met niets en mede door jullie enthousiasme en wil om
te verbeteren zijn de OSU spreekuren nu wat ze zijn. Door alle technologische
veranderingen binnen de 3D planning kunnen wij nu de gezamenlijke patiënten
beter van dienst zijn hetgeen tot een kwaliteitsverbetering leidt. Het is erg prettig
om op deze manier van elkaar en met elkaar te leren. Thanks heren!
Kaakchirurgie St. Antonius, Nieuwegein, Beste Joost, Kelly en Leander, ook
jullie waardeer ik zeer. Jullie kennis, kunde en de bereidwilligheid deze met ons,
mij te delen zijn allemaal aspecten die ervoor zorgen dat wij samen een zeer fijne
en hoogwaardige samenwerking hebben. Dank hiervoor.
Alle collegae (verwijzers) Nieuwegein en omstreken, Geachte collegae, dank
voor het vertrouwen en de aangename samenwerking. Werken in de randstad,
vraagt toch een andere manier van werken dan werken in Gelderland. In het begin
ging dit niet vanzelf, maar mede dankzij jullie support en vertrouwen hebben wij
ons dit een beetje eigen gemaakt.
Patiënten van de verschillende klinische onderzoeken, bedankt voor het vertrou-
wen en jullie participatie in de verschillende klinische onderzoeken.
Medewerkers van Ortholab, Beste Emanuel, Carlos, Yoni, Berisha en Stefan,
dank voor jullie hulp met alle (verschillende) retentie draden en advies over de

130 131
pad gekozen, soms naar een ver land en soms iets dichterbij. Hoewel wij elkaar
vanwege de afstand en het tijdsverschil niet zo vaak zien of spreken, wil ik dat
jullie weten dat ik jullie liefheb. Jullie zijn mijn matties en I aint got nothing but
love for you guys!
Alle familieleden en vrienden, In het bijzonder tante Joan en oom George, dank
dat jullie mij destijds hebben opgevangen. Zo ook dank aan u, oom Robby en tante
Alice, na de grote orkaan Luis in 1995. Jane, Jim en tante Mem, dank voor jullie
hulp en dank aan eenieder die belangstelling en steun heeft getoond tijdens deze
reis.
Lieve Monique, Rob, Jamie en Darren, vanwege het feit dat ik zo vroeg het ou-
derlijk huis uit ben gegaan hebben jullie niet altijd alles meegekregen van wat mij
bezighield en waar ik mee bezig was. Andersom is dit natuurlijk ook zo geweest.
Dit was dan ook niet altijd even goed bij te houden na minimaal 25 keer te zijn
verhuisd naar en binnen 5 verschillende (ei)landen. Heel veel hebben wij destijds
via de telefoon en met brieven moeten delen, maar ondanks dat er toen nog geen
skype, whatsapp of andere social media bestond, is de band tussen ons altijd heel
hecht gebleven. Dank dat jullie er altijd voor mij, ons zijn! Ik wil jullie bedanken
voor jullie steun en liefde en wil dat jullie weten dat jullie te allen tijde op mij kun-
nen rekenen. Ik denk aan jullie en mis jullie elke dag! Love Always.
Lieve pa en ma, zonder jullie aanmoediging, onvoorwaardelijke steun en liefde
stond ik vandaag hier niet. Het is me dan ook een eer jullie dit proefschrift te mo-
gen overhandigen. Jullie hebben mij nooit iets in de weg gelegd om mij verder
te kunnen ontwikkelen. Jullie hebben mij altijd gestimuleerd om verder te kijken
en open te staan voor (andere) mogelijkheden of uitdagingen. Op kruispunten in
mijn leven kon ik altijd op jullie onvoorwaardelijke steun, liefde en advies rekenen.
Jullie hebben mij geleerd altijd nederig en bescheiden te blijven en dankbaar te
zijn. Maar ook het fundament te leggen in het besef dat wat de wetenschap ook
aan kennis moge brengen, de werkelijke wijsheid in het kennen van de Here ligt.
Woorden schieten te kort om jullie te bedanken voor alles wat jullie voor mij heb-
ben gedaan en hebben geleerd!
Pa en ma, jullie beiden zijn altijd mijn rolmodellen geweest, dank voor alles! Ik
draag dit proefschrift dan ook op aan jullie beiden en vind het erg fijn de vreugde
van dit moment met jullie te mogen delen.
Mijn laatste dank gaat uit naar mijn lieve vrouw, Kim. Jij bent de grote motor thuis
en jij bent mijn steun en toeverlaat. Jij brengt de rust en zorgt voor het evenwicht.
Jij bent de onvoorwaardelijke supporter achter dit proefschrift. Ik realiseer mij dan
ook heel goed dat ik (te) vaak tekort geschoten ben door veel te laat thuis zijn of
het ‘even’ doch ‘alweer’ naar Zürich vliegen teneinde dit onderzoek af te maken
spalken. Het ziet er allemaal zo eenvoudig uit, tot je het zelf moet doen! Dank
voor jullie geduld. Sorry, dat ik altijd weer aan de telefoon hang, foto’s stuur over
wat wij anders kunnen doen teneinde te verbeteren of te bespreken wat fout
ging. Ik waardeer jullie oprecht en waardeer ook de prettige samenwerking.
Medewerkers van Apeldoorn Orthodontie Welgelegen en Orthodontieprak-tijk Nieuwegein, Lieve dames, zonder jullie kunnen wij niet werken en kunnen
wij niet bestaan. Ik realiseer mij dan ook dat ik mijn waardering wellicht te wei-
nig laat blijken, hiervoor mijn oprechte excuses. Ik waardeer jullie ZEER. Jullie
zijn allemaal toppers en zeer belangrijk. Eenieder van jullie vormt elk een unieke
schakel in de ketting die het wiel uiteindelijk moet draaien en draaiende moeten
houden. Dank voor al jullie hulp en inzet.Saskia, hoewel jij een ander avontuur
bent aangegaan, wil ik jou in het bijzonder bedanken voor al jouw inspanningen
om al die patiënten te traceren en herhaaldelijk op te bellen zodat wij aan alle data
konden komen.
Mw. S. de Vries, lieve Saar sorry dat ik zo slecht bereikbaar ben en op de meest
onchristelijke tijden app of mail. Dit komt echt door de dagelijkse drukte en andere
verplichtingen, maar zoals je inmiddels weet, reageer ik altijd. Hartelijk dank voor
jouw hulp. Mede door jouw inzet ziet dit proefschrift er nu zo mooi uit.
Drs. L.B.H.G. Tacken, Beste vader Tacken dank voor al uw kritische adviezen op
de juiste momenten. Ik waardeer dit oprecht.
Drs. M.P.E Tacken, Bro wat kan het leven raar lopen. Wie had ooit kunnen beden-
ken dat wij elkaar, zonder van elkaar af te weten, elkaar tijdens het najaarscongres
2005 van de Nederlandse Vereniging van Orthodontisten, de hand zouden schud-
den naar aanleiding van mail contact over soortgelijk onderzoek om vervolgens in
2009 samen een praktijk op te zetten. Ik wil jou dankzeggen voor de fijne samen-
werking en waardeer je oprecht. Dank dat jij mijn paranimf wil zijn. God Bless!
Drs. C.G. Sabajo, Lieve Claire, zoveel jaren kennen wij elkaar al. Alles begon in
het inmiddels gesloopte Wentgebouw toen wij samen Farmacie studeerden. Wij
hebben door de jaren heen heel veel mooie momenten, maar ook minder plezie-
rige momenten gekend en gedeeld. Dit heeft ons heel close gemaakt en zijn wij,
ondanks dat wij elkaar niet elke dag zien of spreken, haast broer en zus gewor-
den. Ik wil je dankzeggen voor jouw vertrouwen, liefde en begrip, maar bovenal
dat wij altijd onszelf kunnen zijn in bijzijn van elkaar. Sinds kort heb je een man
in je leven, iemand die ik zeer waardeer en respecteer. Ik wil jullie dan ook alle
goeds toewensen en vanzelfsprekend kom ik jullie ook helpen verhuizen naar jul-
lie nieuw stekkie. Dank voor de vriendschap en dank dat je mijn paranimf wil zijn.
Martin, Maurice en Jimmy, waar gaat de tijd. Rimini, Bangkok, New King, Rio
de Janeiro, wat een tijd. Eenieder van ons is ouder geworden en heeft zijn eigen

132 133
en altijd maar weer achter die computer te zitten. Ik wil jou oprecht bedanken
voor alle begrip, onvermoeibare en oprechte steun maar bovenal voor jouw on-
voorwaardelijke liefde. Ik ben blij dat ik altijd bij jou terecht kan en hoop dat ik dit
ook voor jou mag doen, op weg naar de afronding van jouw eigen proefschrift. Wij
hebben het afgelopen jaar samen een heel moeilijk jaar doorstaan, maar saam-
pjes staan we sterk en gaan we door. Stap voor stap. Dank dat je de beste moe-
der bent voor onze lieve, zoon Luca. Hij is werkelijk een geschenk van God en
altijd het zonnetje in huis. Vervult met blijdschap kijk ik uit naar eind juli, en kan me
alleen maar voorstellen hoe fijn het straks zal zijn met ons vieren. Ik hou van jullie!
Curriculum Vitae
Dave Lie Sam Foek was born on July 6th, 1977 in Paramaribo, Suriname (South
America). He received his primary and part of secondary education at the
Bernadetteschool and Christus Koningschool both in Paramaribo, Suriname. After
having finished secondary school in 1997 at Milton Peters College (HAVO) on Sint
Maarten (Dutch West Indies), he continued to finish his pre-university education in
1998 at the Collegio Arubanu (VWO) on Aruba (Dutch Antilles). In 1998 he started
a study on Pharmacy at the University of Utrecht, Netherlands and in 1999 he
was accepted at the University of Amsterdam to study dentistry. During his study
the author was active in several (student) committees and worked in a private
practice as a dental assistant. During the last year of his dentistry education, he
joined an international collaboration with the University of São Jóse dos Campos,
Brazil, on which he wrote his master thesis. He graduated in 2004 and took on
a partial position as a staff member on the pre-clinic (Department of Cariology
and Endodontics) as well as working in several private practices as a dentist.
In 2005 he started his speciality training at the Department of Orthodontics,
University Medical Center, University of Groningen, Groningen, The Netherlands.
He currently works in two private practices restricted to orthodontics.
Dr. Dave J. Lie Sam Foek, DDS Apeldoorn Orthodontie Welgelegen
Burgemeester Jonkheer Quarles van Uffordlaan 103
7321 ZN Apeldoorn
The Netherlands
T +31(0) 555766480
M +31(0) 642129950