Embed Size (px)
Citation preview

UvA-DARE is a service provided by the library of the University of Amsterdam (http://dare.uva.nl)
UvA-DARE (Digital Academic Repository)
Determinants of malaria control in a rural community in Eastern Rwanda
Kateera, F.K.
Link to publication
Citation for published version (APA):Kateera, F. K. (2016). Determinants of malaria control in a rural community in Eastern Rwanda.
General rightsIt is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s),other than for strictly personal, individual use, unless the work is under an open content license (like Creative Commons).
Disclaimer/Complaints regulationsIf you believe that digital publication of certain material infringes any of your rights or (privacy) interests, please let the Library know, statingyour reasons. In case of a legitimate complaint, the Library will make the material inaccessible and/or remove it from the website. Please Askthe Library: https://uba.uva.nl/en/contact, or a letter to: Library of the University of Amsterdam, Secretariat, Singel 425, 1012 WP Amsterdam,The Netherlands. You will be contacted as soon as possible.
Download date: 26 Jul 2020


DETERMINANTS OF MALARIA CONTROLIN A RURAL COMMUNITY IN EASTERN RWANDA
Fredrick Karambizi Kateera


DETERMINANTS OF MALARIA CONTROL IN A RURAL COMMUNITY IN EASTERN RWANDA
ACADEMISCH PROEFSCHRIFT
ter verkrijging van de graad van doctor
aan de Universiteit van Amsterdam
op gezag van de Rector Magnificus
prof. dr. ir. K.I.J. Maex
ten overstaan van een door het College voor Promoties ingestelde commissie,
in het openbaar te verdedigen in de Agnietenkapel
op donderdag 22 september 2016, te 14:00 uur
door Fredrick Karambizi Kateera
geboren te Mbale, Uganda


PROMOTIECOMMISSIE
Promotor: Prof. dr. M.P. Grobusch Universiteit van AmsterdamCopromotores: Dr. P.F. Mens Koninklijk Instituut voor de Tropen
Dr. M. van Vugt Universiteit van Amsterdam
Overige leden: Prof. dr. M. Boele van Hensbroek Universiteit van AmsterdamDr. J.T. Bousema Radboud Universitair Medisch centrum Prof. dr. F.G.J. Cobelens Universiteit van AmsterdamDr. T. van Gool Universiteit van AmsterdamProf. dr. T.F. Rinke de Wit Universiteit van AmsterdamDr. H.D.F.H. Schallig Koninklijk Instituut voor de Tropen Prof. dr. M. Yazdanbakhsh Universiteit Leiden
Faculteit der Geneeskunde

These studies were conducted as part of a project, contributing to the elimination of malaria in Rwanda through involving the community in the Rwandan health system (MEPR-project). The overall objective of the project is ‘To assist the Rwandan ambition to move towards malaria elimination by connecting community mobilisation to the national and district malaria control program and (inter)national expert knowledge bases.’ The MEPR-project isone of the eight programmes funded by WOTRO, belonging to the Dutch Global HealthPolicy and Health Systems (GHPHS) research programme, The Hague, The Netherlands.
Fredrick Kateera was supported by this programme.
© Copyright 2016, Fredrick Karambizi Kateera
Cover illustration photograph: used with permission
Cover design: Fredrick Kateera, Rwanda
Printing:

This thesis is dedicated to the memory of my late Mother – Asinati Mukandoli –
The essence of fortitude, industry and resilience and my number one fun
It is most unfortunate that you short lived the harvest of your labours. Words can never
express not just how much you gave yourself away for your children and who you were to us
and me in particular – beauty far beyond the radiance of 1000 suns. Thank you.

4
TABLE OF CONTENTS
Chapter 1 General introduction 6
Part 1 The Parasite Chapter 2 Clinical profiles and genetic diversity of Plasmodium falciparum parasite at
two sites with different malaria transmission intensities in RwandaChapter 3 Molecular surveillance of Pfcrt, Pfmdr1, Pfdhps and Pfdhfr SNPs reveals
partial recovery of Chloroquine Susceptibility but sustained intense levels of Sulfadoxine - Pyrimethamine resistance-conferring mutations at two sites of different malaria transmission intensities in Rwanda
25
50
Part 2 Malaria: burden, distribution, association with other diseases and active surveillance
Chapter 4 Malaria parasite carriage and risk determinants in a rural population: a malariometric survey in Rwanda
Chapter 5 Malaria, anaemia and under-nutrition: three frequently co-existing conditions among pre school-children in rural Rwanda
78
103
Part 3 Malaria Control Themes and associated challengesChapter 6 Long-lasting insecticidal net source, ownership and use in the context of
universal coverage: a household survey in eastern Rwanda.Chapter 7 Using reactive case finding surveillance to measure - malaria Prevalence,
Spatial Clustering and Risk Factors in a Low Endemic Area of Eastern Rwanda: A Cross Sectional Study
130
154
Part 4 Community oriented approachesChapter 8 Stakeholder analysis paper 179Chapter 9 General Discussion 198
Addendum
Portfolio 208Summary 210Authors and affiliations 220Acknowledgement 223Biography & List of Publications 224

A r
ice
field
in R
uhuh
a Se
ctor
, Bug
eser
a D
istr
ict,
Eas
tern
Rw
anda

6
CHAPTER 1
General Introduction

7
Global Malaria Burden
Malaria still accounts for huge medical, social, and economic burdens worldwide with the
United Nation’s calling for a reversal in the progression of this scourge by 2015 [1].
However, significant progress following scale up and use of malaria control interventions
including long lasting insecticide treated nets (LLINs), indoor residual spraying (IRS)
and use of artemisinin combinational therapies (ACTs) in treatment of uncomplicated
malaria have lead to substantial reductions in malaria burden [2]. Globally, the World
Health Organization (WHO) reported declines in in cases from 227 million in 2000 to
~198 million cases in 2014 and malaria mortality rates also declined by 47% globally and
by 54% in the WHO African Region [3].
Malaria Parasite diversity
Plasmodium falciparum parasite is the most prevalent and cause of malaria morbidity and
mortality in Rwanda. P. falciparum virulence is mediated, in part, by its population-level
genetic diversity which has been reported to influence malaria disease pathology [4],
acquisition of immunity [5], drug resistance profiles and infection transmission intensity
[6-7]. High malaria endemic area are generally characterised by extensive malaria
parasite genetic diversity with infected humans often found with multiple genotypes and,
conversely, P. falciparum population in a low transmission area tends to have limited
genetic diversity with a higher proportion of infections being monoclonal [8-9].
Therefore, higher malaria diversity may be strong predictor of higher malaria intensity.
Because no study to-date, in Rwanda, has characterised the local p. falciparum parasite
population genetic diversity, we compared among malaria confirmed patient identified at
two sites of presumed low (Mubuga sector, western Rwanda) and high (Ruhuha sector,
eastern Rwanda) different malaria transmission intensities, clinical profiles, parasitaemia
densities and parasite diversity.
Malaria parasite resistance to Chloroquine and Sulphadoxine - Pyrimethamine
Antimalarial drugs have long been used to prevent illness, reduce transmission and
treating illnesses. Two important drugs that were used in the past for preventing illness
but were withdrawn due to high-level resistance and the associated high mortality and

8
morbidity were chloroquine and Sulfadoxine–Pyrimethamine (SP). Chloroquine (CQ)
was used for malaria chemoprophylaxis among pregnant women and for treating
uncomplicated malaria but was stopped after developing high level resistance that lead to
lose of effect and severe increases in disease morbidity and mortality [10-11]. SP use in
Intermitted presumptive therapy in pregnancy (IPTp) and Intermitted presumptive
therapy among infants (IPTi) is now threated by the noted substantial increases in
resistance in many malaria endemic countries [12-14]. In Rwanda, intense CQ resistance
lead to its replacement with SP in 2006, and subsequently, SP was replaced with an ACT
(Artemether – Lumefantrine (AL)) in 2006, as treatments for non-complicated clinical
malaria. However, SP use continued for 2 more years and, in 2008, was withdrawn from
use for Intermitted presumptive therapy among pregnant women.]. Concerns about a
similar trend in resistance to the current efficacious ACTs for which resistance to P.
falciparum is accumulating in mainland Southeast Asia at a time when optional effective
antimalarial drugs are limited [15]. Currently in Rwanda, no malaria chemoprevention is
available for any population group. With regard to chloroquine however, re-emergence of
parasite sensitive strains after periods of complete CQ withdrawal policy has been
reported in multiple settings [16-17]. In contrast, although a few studies have reported
declines in prevalence of SP-associated resistance molecular markers [18-20], an
overwhelming majority of studies have reported sustained or even increasing prevalences
of SP- resistance associated molecular markers [13,14, 21-23]. A return to CQ and/or SP
sensitivity may open a door for their use, plausible as combinational therapies, in malaria
chemoprevention (either as chemoprophylaxis or intermittent preventive therapy) towards
preventing malaria illnesses and/or reduction of malaria transmission. Chapter 4 in this
thesis describes a surveillance update on CQ and SP resistance mediating polymorphisms
at two sites of presumed low and high malaria transmission intensities. This data may
guide rational drug policy implementation and effective malaria management.
Malaria parasite carriage rates and risk determinants of infection
There is paucity of systematic data on asymptomatic malaria burden and associated risk
determinants in general populations (reservoir): - This sources of sustained malaria
transmission. Control programmes need these data to plan interventions targeted at

9
optimal reduction of overall and area-specific malaria transmission as well as to mitigate
the effect of local malaria transmission, foci-associated risk factors. Currently, the
principal source of data on population level asymptomatic malaria parasitaemia is the
nationally representative demographic and health surveys (DHSs) conducted every five
years. DHSs are conducted primarily to provide data for a wide range of monitoring and
impact evaluation indicators in population, health, and nutrition issues [24]. However,
because of their large coverage, DHSs are not powered for an accurate assessment of
malaria reservoirs (asymptomatic-carrying, parasitaemic persons in a population in a
given area) or to identify risk determinants of community-based, residual, malaria
parasitaemia. The WHO recommends field surveys that characterize baseline malaria
transmission epidemiology with the aim of identifying Plasmodium spp. carriers and at-
risk populations to inform targeted control for optimal impact [25]. Measurement of
malaria parasitaemia rates among asymptomatic community based individuals and
characterization of risk determinants for these malaria infections was done in Ruhuha
sector, eastern Rwanda. These findings provide a strong baseline quantification of the
reservoir pool size and also delineate barriers to continued malaria infection reduction
that can then be targeted for optimal impact.
Malaria, anaemia and malnutrition
Malaria is a major cause of anaemia, a major global public health concerns impacting the
social and economic development of particularly women and children in Southern and
Central Asia and regions of Africa. Malaria may be associated with up to half of all
severe anaemia cases in areas of high Malaria endemicity [26]. Anaemia is an important
indicator of the effectiveness of malaria control program [27-28]. We study anaemia
epidemiology in the community. Malaria impacts growth and development in children.
This study will monitor growth parameters over time and across different malaria
endemicity levels
Insecticide treated bed nets
Along side scale-up of IRS and ACTs in treating malaria illnesses, LLINs are the core
tools for current malaria control campaigns [29]. Because of LLIN cost effectiveness in

10
malaria prevention, the WHO has, since 2007, recommended universal coverage (defined
as one LLIN per two persons) [30-32]. However, community and individual level
effectiveness of LLINs hinges on access, ownership and use. Previously, studies have
highlighted disparities between bed net ownership and use [33-35]. Hitherto, studies on
bed net use have predominantly focused on at risk populations of children <5 years and
pregnant women with limited studies on ITN use in the context of universal long-lasting
insecticidal net coverage (ULC) where all age and gender groups are included. Bed net
ownership, access and use at household-level in Ruhuha sector were evaluated. These
data can highlight implementational gaps that can be targeted to optimize bed net impact.
Active surveillance to identify malaria hotspots
Rwanda is broadly divided into four malaria ecologic zones based on altitude, climate,
level of transmission, and disease vector prevalence [36]. Similar heterogeneities in
spatial malaria have been reported in different malaria endemic settings attributed to
many risk factors including altitude, climate, occupation and socio-economic status [37-
38]. However, at all malaria endemicity levels, and particularly in low incidence areas,
malaria tends to cluster in ‘hotspots’ – defined as geographical part of a focus of malaria
transmission where transmission intensity exceeds the average level’ and ‘hot’
populations that become sources of continued infection [39]. Active and timely
identification of these hotspots and associated risk factors is essential for targeting
interventions to optimize malaria control [40]. Unfortunately, in targeting malaria
transmission reductions and achieving malaria pre-elimination levels, passively collected
monthly routine data alone are sub-optimal accurately characterising community level hot
spots. We employed active surveillance techniques (reactive case finding) and used HC
attendees with presumed malaria (positive or negative) as entry points for identification
of malaria infections at the HH level using a two-phase health facility and HH cross-
sectional survey. We measured malaria burden and evaluate for associated malaria risk
factors for both symptomatic and asymptomatic residents of the same household and
study area (Ruhuha sector). We also investigated for spatial malaria clustering using
geographical information system (GIS) and spatial statistical techniques. These data help
to highlight malaria infection “hot spot” areas and risk factors for both symptomatic and

11
asymptomatic malaria infected cases. By tailoring control strategies to identified hotspots
and risk determinants of continued malaria infection, cost effective and area relevant use
of interventions can be achieved even as local malaria transmission is arrested.
Stakeholder engagement in community-based malaria studies
A variety of stakeholders play multiple roles in various aspects of malaria control
strategies and practices as a community level. These stakeholders range from the locally
based community members to the nationally situated national malaria control programs
with various group-implementing partners that differ between places and in their roles.
To optimize impact of malaria control efforts and promote sustainability of used
interventions, active engagement and collaboration with all stakeholders. To this end, a
stakeholder analysis - a program-planning tool focused on identifying and analysing
stakeholders’ motivations for promoting or threatening malaria-associated interventions
is recommended [41-42]. Stakeholder analysis was aims to understand stakeholder
behaviour, intentions, interests and interrelations and to assess stakeholder influences and
resources that they may bring to decision making or implementation and analysis
processes [41, 43-44]. This stakeholder analysis was conducted to identify key
stakeholders and seek in future how to best establish an appropriate framework for
participation in project selection, design, implementation, monitoring, and evaluation and
in planning for efficient collaboration with other institutions.
Research Setting
Rwanda is a small, land-locked country located in central Africa. It lies within the east
African great Lakes region and is surrounded by countries of Uganda, Burundi, the
democratic Republic of the Congo, and Tanzania. Its projected population size is 12.4
million (projections based on the 2012 census results). Geopolitically, Rwanda is divided
into 5 provinces, 30 districts that are further divided into, sectors, cells, and villages
(about 15,000 villages of 50-100 households each) locally called “umudugudus”.
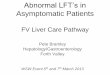
The primary studies reported in this thesis were conducted in Ruhuha sector, Bugesera
District, in the eastern province of Rwanda (Figure 1). Ruhuha sector – made up of 35

12
villages that are grouped into five cells, is located 42 kilometers from Kigali City, covers
54 km2, with a reported population was 21,606 individuals living in 5,100 households.
Ruhuha is a predominantly rural setting the lies with in a high malaria endemic zone.
Ruhuha sector, surrounded by lowland marshes and water-streams draining into the
Akagera River System, is separated from Burundi by Lake Cyohoha in the south. The
area experiences two high malaria transmission peaks associated with rainy seasons
observed generally from October to November and March to May. The choice for this
study area was made on the basis of our existing contacts with the staff of the health
centre and representatives of the community of Ruhuha and our prior collaborations on
previous research conducted at the Ruhuha health centre.

Figu
re 1
. Map
of
Rw
anda
sho
win
g th
e al
l-30
dist
ricts
with
the
dis
trict
(K
alon
gi a
nd B
uges
era)
whe
re t
he s
tudy
site
s ar
e lo
cate
d
high
light
in o
rang
e.

14
Situational analysis of Malaria in Rwanda
Rwanda is broadly divided into four malaria ecologic zones based on altitude, climate,
level of transmission, and disease vector prevalence [36]. Topographically, malaria
transmission is considered meso-endemic in the plain regions of eastern and southern
provinces while being epidemic prone in the high plateau and hill settings of northern and
western provinces, respectively [36]. Rwanda achieved the 2005 global community
commitment of reducing the malaria burden by at least 50% by 2010 [45]. With respect
to LLINs distribution between the 2005-2010 period, household ownership of at least one
LLIN increased from 15% to 82%, use in children under 5 years increased from 13% to
70% while use in pregnant women also increased from 17% to 72% [46]. ACTs are now
sufficiently accessible in many facilities (government, private and faith-based) as well as
at the community level where they can be accessed through community health workers
(CHWs) and private pharmacies [47]. In five of the high-risk districts, coverage with IRS
had reached 97.7% of households by end of 2007 [47]. A combination of mass
distribution of LLIN targeting children < 5 years and pregnant women and scaling up
ACTs in the public sector country wide showed reductions of 55% and 67% in In-patient
malaria cases and deaths respectively in periods 2001–2005/6 prior and 2007 after
intervention introduction [48]. However, malaria reduction gains are very fragile where
the potential for transmission remains. In 2009, malaria resurgences reported in Rwanda,
(Sao Tome and Principe, and Zambia) was partially attributed to delays in purchase and
distribution of LLINs [49-50]. According to the National Malaria Control Program
(NMCP), Rwanda has now embraced a new 2013–2017 Malaria Strategic Plan (MSP)
who principal target is achieving malaria pre-elimination status country-wide by 2017 by
lowering malaria morbidity to pre-elimination levels of < 5% test positivity rate among
presumed malaria patients and reducing mortality by 50% from the 2011 baseline level
[36]. These targets, it is hoped, will be achieved by sustain scale up of malaria control
including ULC with LLINs, IRS with insecticide and use of ACTs.
We hypothesis that characterising asymptomatic parasite community based reservoirs and
the determinants of continued transmission at community level can 1) be cost-effective
by matching resources to local burden and risk factors; 2) optimize impact of available

15
resources and interventions; 3) allows for a more active surveillance based approach that
identifies and effectively clears residual infections in malaria hotspots, 4) characterise
and proactively responds to determinants of limited impact of used interventions like
LLINs, IRS, 5) allow for engagement with and leveraging of stakeholder resources to
promote local ownership, sustainability and involvement. This thesis was based on
biomedical aspects of this community based approach that characterizes malaria
associated burden, risk factors of infection, gaps in knowledge and challenges in malaria
control interventions used. By pin pointing these, evidence based setting specific
approach can then be used to plausibly lead to further reductions in malaria transmission.

16
References
1. United Nations: The Millennium Development Goals Report 2010 United Nations
Department of Economic and Social Affairs (DESA); 2010. Available at:
http://www.un.org/en/development/desa/news/statistics/mdg-2010.shtml. Accessed April
10th 2012.
2. WHO/GMP: The Global malaria action Plan: For a malaria free world. Available at:
http://www.rbm.who.int/gmap/gmap.pdf. Accessed may 11th 2012.
3. WHO: World Malaria Report 2014. Available at:
http://www.who.int/malaria/publications/world_malaria_report_2014/wmr-2014-no-
profiles.pdf. Accessed 3rd June 2012.
4. Ofosu-Okyere A, Mackinnon MJ, Sowa MP, Koram KA, Nkrumah F, Osei YD, et al.
Novel Plasmodium falciparum clones and rising clone multiplicities are associated with
the increase in malaria morbidity in Ghanaian children during the transition into the high
transmission season. Parasitology 2001; 123: 113–123.
5. Onway DJ, Cavanagh DR, Tanabe K, Roper C, Mikes ZS, Sakihama N, et al. A principal
target of human immunity to malaria identified by molecular population genetic and
immunological analyses. Nat Med 2000; 6:689–692.
6. Mobegi VA, Loua KM, Ahouidi AD, Satoguina J, Nwakanma DC, Amambua-Ngwa A,
Conway DJ. Population genetic structure of Plasmodium falciparum across a region of
diverse endemicity in West Africa. Malar J 2012; 11:230.
7. Babiker HA, Charlwood JD, Smith T, Walliker D. Gene flow and cross-mating in
Plasmodium falciparum in households in a Tanzanian village. Parasitology 1995;
111:433-442
8. Haddad D, Snounou G, Mattei D, Enamorado IG, Figueroa J, Stahl S, Berzins K. Limited
genetic diversity of Plasmodium falciparum in field isolates from Honduras. Am J Trop
Med Hyg 1999; 60:30-34.
9. Babiker HA, Lines J, Hill WG, Walliker D. Population structure of Plasmodium
falciparum in villages with different malaria endemicity in east Africa. Am J Trop Med
Hyg 1997; 56:141-147
10. Brabin BJGM, Alpers M, Brabin L, Eggelte T, Van der Kaay HJ. Failure of chloroquine
prophylaxis for falciparum malaria in pregnant women in Madang, Papua New Guinea.

17
Ann Trop Med Parasitol 1990; 84:1–9.
11. Trape JF, Pison G, Preziosi MP, Enel C, Desgrées du Loû A, Delaunay V, et al. Impact of
chloroquine resistance on malaria mortality. C R Acad Sci Paris Serie III. 1998; 321:689–
697.
12. Geiger C1, Compaore G, Coulibaly B, Sie A, Dittmer M, Sanchez C, Lanzer M, Jänisch
T. Substantial increase in mutations in the genes pfdhfr and pfdhps puts sulphadoxine-
pyrimethamine-based intermittent preventive treatment for malaria at risk in Burkina
Faso. Trop Med Int Health. 2014; 19(6): 690-697.
13. Lobo E, de Sousa B, Rosa S, Figueiredo P, Lobo L, Pateira S, et al. Prevalence of pfmdr1
alleles associated with artemether-lumefantrine tolerance/resistance in Maputo before and
after the implementation of artemisinin-based combination therapy. Malar J 2014;
13:300.
14. Shah M, Omosun Y, Lal A, Lal A, Odero C, Gatei W, et al. Assessment of molecular
markers for anti-malarial drug resistance after the introduction and scale-up of malaria
control interventions in western Kenya. Malar J. 2015; 14: 75.
15. Dondorp AM, Nosten F, Yi P, Das D, Phyo AP, Tarning J, et al. Artemisinin resistance in
Plasmodium falciparum malaria. N. Engl. J. Med. 2009; 361: 455-467.
16. Ndiaye M, Faye B, Tine R, Ndiaye JL, Lo A, Abiola A, et al. Assessment of the
Molecular Marker of Plasmodium falciparum Chloroquine Resistance (Pfcrt) in Senegal
after Several Years of Chloroquine Withdrawal. Am J Trop Med Hyg 2012; 87(4): 640–
645.
17. Mwai L, Ochong E, Abdirahman A, Kiara SM, Ward S, Kokwaro G, et al. Chloroquine
resistance before and after its withdrawal in Kenya. Malar Journal 2009; 8:106.
18. Tessema SK, Kassa M, Kebede A, Mohammed H, Leta GT, Woyessa A, et al. Declining
trend of Plasmodium falciparum dihydrofolate reductase (dhfr) and dihydropteroate
synthase (dhps) mutant alleles after the withdrawal of Sulfadoxine-Pyrimethamine in
North Western Ethiopia. PLoS ONE 2015; 10(10), e0126943.
19. Pearce RJ, Ord R, Kaur H, Lupala C, Schellenberg J, Shirima K, et al. A community-
randomized evaluation of the effect of intermittent preventive treatment in infants on
antimalarial drug resistance in southern Tanzania. J Infect Dis 2013; 207: 848–859.
20. Raman J, Sharp B, Kleinschmidt I, Roper C, Streat E, Kelly V et al. Differential effect of

18
regional drug pressure on dihydrofolate reductase and dihydropteroate synthetase
mutations in southern Mozambique. Am J Trop Me. Hyg 2008; 78: 256–261.
21. Iriemenam NC, Shah M, Gatei W, van Eijk AM, Ayisi J, Kariuki S, et al. Temporal
trends of sulphadoxine-pyrimethamine (SP) drug-resistance molecular markers in
Plasmodium falciparum parasites from pregnant women in western Kenya. Malar J 2012;
11:134.
22. Mbogo GW, Nankoberanyi S, Tukwasibwe S, Baliraine FN, Nsobya SL, et al. Temporal
Changes in Prevalence of Molecular Markers Mediating Antimalarial Drug Resistance in
a High Malaria Transmission Setting in Uganda. Am J Trop Med Hyg 2014; 91 (1): 54-
61.
23. Matondo SI, Temba GS, Kavishe AA, Kauki JS, Kalinga A, van Zwetselaar M, et al.
High levels of sulphadoxine-pyrimethamine resistance Pfdhfr-Pfdhps quintuple
mutations: a cross sectional survey of six regions in Tanzania. Malar J 2014; 13:152
24. USAID. Demographic Health Survey Overview. Available at:
http://www.dhsprogram.com/What-We-Do/Survey-Types/DHS.cfm. Accessed 12th May
2014.
25. GMP/WHO. From malaria control to malaria elimination: a manual for elimination
scenario planning. Available at:
http://apps.who.int/iris/bitstream/10665/112485/1/9789241507028_eng.pdf. Accessed
March 13th 2014.
26. Newton CR, Warn PA, Winstanley PA, Peshu N, Snow RW, Pasvol G, et al. Severe
anaemia in children living in a malaria endemic area of Kenya. Trop Med Int Health
1997; 2:165–178
27. Menendez C, Kahigwa E, Hirt R, Vounatsou P, Aponte JJ, Font F, et al. Randomised
placebo-controlled trial of iron supplementation and malaria chemoprophylaxis for
prevention of severe anaemia and malaria in Tanzanian infants. Lancet 1997; 350:844–
850.
28. Shiff C, Checkley W, Winch P, Premji Z, Minjas J, Lubega P. Changes in weight gain
and anaemia attributable to malaria in Tanzanian children living under holoendemic
conditions. Trans R Soc Trop Med Hyg 1996; 90(3):262-265.
29. WHO: World Malaria Report 2013. Geneva: World Health Organization; 2014. Available

19
at: www.who.int/iris/bitstream/.../9789241564694_eng.pdf. Accessed 2nd July 2012.
30. Guillet P, Alnwick D, Cham MK, Neira M, Zaim M, Heyman D, Mukelabai K. Long-
lasting treated mosquito nets: breakthrough in malaria prevention. Bull World Health
Organ 2001; 79:998.
31. Kilian A, Boulay M, Koenker H, Lynch M. How many mosquito nets are needed to
achieve universal coverage? Recommendations for the quantification and allocation of
long-lasting insecticidal nets for mass campaigns. Malar J 2010; 9:330.
32. WHO: Insecticide treated mosquito nets: a position statement Global Malaria
Programme. Geneva: World Health Organization; 2007. Available at:
http://www.who.int/mediacentre/news/releases/2007/pr43/en/. Accessed 22nd April 2012.
33. Binka FN, Adongo P. Acceptability and use of insecticide impregnated bed nets in
northern Ghana. Trop Med Int Health 1997; 2:499-507.
34. Korenromp EL, Miller J, Cibulskis RE, Kabir Cham M, Alnwick D, Dye C. Monitoring
mosquito net coverage for malaria control in Africa: possession vs. use by children under
5 years. Trop Med Int Health 2003; 8:693-703.
35. Alaii JA, Hawley WA, Kolczak MS, ter Kuile FO, Gimnig JE, Vulule JM et al. Factors
affecting use of permethrin-treated bed nets during a randomized controlled trial in
western Kenya. Am J Trop Med Hyg 2003; 68:137-141.
36. PMI/MOH-Rwanda. President’s malaria initiative Rwanda malaria operational plan FY.
2015. http://www.pmi.gov/docs/default-source/defaultdocument-library/malaria-
operational-plans/fy-15/fy-2015-rwandamalaria- operational-plan.pdf?sfvrsn=3.
Accessed 22nd Sep 2015.
37. Bousema T, Drakeley C, Gesase S, Hashim R, Magesa S, et al. Identification of hot spots
of malaria transmission for targeted malaria control. J Infect Dis 2010; 201: 1764–1774.
38. Clark TD, Greenhouse B, Njama-Meya D, Nzarubara B, Maiteki-Sebuguzi C, et al.
Factors Determining the Heterogeneity of Malaria Incidence in Children in Kampala,
Uganda. J Infect Dis 2008; 198: 393–400
39. Bousema T, Griffin JT, Sauerwein RW, Smith DL, Churcher TS, et al. Hitting Hotspots:
Spatial Targeting of Malaria for Control and Elimination. PLoS Med 2012; 9(1):
e1001165.
40. WHO: Malaria elimination: a field manual for low and moderate endemic countries.

20
WHO: 2007; Geneva: World Health Organization. Available at:
http://apps.who.int/iris/bitstream/10665/43796/1/9789241596084_eng.pdf. Accessed
March 14th 2014.
41. Brugha R, Varvasovszky Z. Stakeholder analysis: a review. Health Policy and Planning,
2000; 15(3), 239-246.
42. Reed MS, Graves A, Dandy N, Posthumus H, Hubacek K, Morris J, et al. Who's in and
why? A typology of stakeholder analysis methods for natural resource management. J
Environ Manage 2009; 90(5): 1933-1949.
43. Ancker S, Rechel B. HIV/AIDS policy-making in Kyrgyzstan: a stakeholder analysis.
Health Policy Plan 2015; 30(1): 8-18.
44. Freeman RE, John AM. A Stakeholder Approach to Strategic Management. 2001.
45. WHO/RBM: Global Strategic Plan, 2005–2015. Available at:
www.rollbackmalaria.org/forumV/docs/gsp_en.pdf. Accessed 5th April 2012
46. Ministry of Health Rwanda. Interim Demographic and Health Survey 2007-08 Kigali,
Rwanda, 2009; DHS 2010 (Preliminary Report).
47. President’s Malaria Initiative (PMI). Malaria Operational Plan: Rwanda FY 2011.
Washington, DC: PMI, 2010. Available at: http://www.pmi.gov/docs/default-
source/default-document-library/malaria-operational-plans/fy11/rwanda_mop-
fy11.pdf?sfvrsn=6. Accessed August 13th 2014.
48. Otten M, Aregawi M, Were W, Karema C, Medin A, Bekele W, et al. Initial evidence of
reduction of malaria cases and deaths in Rwanda and Ethiopia due to rapid scale-up of
malaria prevention and treatment. Malar J 2009; 14; 8:14.
49. WHO: World malaria report 2010. Available at:
http://www.who.int/malaria/world_malaria_report_2010/worldmalariareport2010.pdf.
Accessed 13 May 2012.
50. Office of the Inspector General. Audit Report on the Global Fund Grants to Rwanda.
2011.

21
Aims of the thesis
Based on health facility slide positivity rates, Rwanda recorded significant declines in
malaria burden (cases and death) that were attributed to scale up on WHO recommended
interventions on ITNs, IRS and use of ACTs. This prompted a laudable call to achieve
malaria pre-elimination levels by end of 2018. However, what the reported numbers do
not tell is the level of malaria infection reservoir in the general population: A key
determinant for continued malaria transmission. Studies described in thesis aimed at
characterising key of malaria control in a community by focusing on five major themes of
the malaria parasite (diversity and clinical profiles), the malaria disease (burden and
distribution), malaria infection and its associations with two key diseases among the
malaria high risk under-5 year old populations, malaria control tools (Insecticidal treated
bed nets) and challenges (anti-malarial drug resistance) and the key players in malaria
control in a community. Findings from these studies will provide much needed and
currently lacking evidence on malaria control determinants that can guide policy decision
and strategic planning towards a more targeted use of available results for optimal impact
and further malaria transmission towards achieving malaria pre-elimination levels.
Study context
Studies reported in this thesis were performed in the context of an integrated PhD training
Program titled “Malaria elimination Programme - Rwanda” (MEPR). MEPR was set up,
in part, to provide capacity building for 4 doctoral students enrolling in different
Universities in the Netherlands but engaged in a 4-themed series of integrated studies
around the theme of community empowerment towards malaria elimination. The four
streams include:
1. Biomedical sciences
2. Behavioural sciences
3. Entomological sciences
4. Finance and health economics
Elimination of malaria has been back on the agenda since 2007 [1, 2, 3]. However, It is
generally acknowledged that although this is an achievable target, it requires new and
integrated approaches with no clear single effective intervention [4, 5, 6]. The transition

22
from predominantly vertically driven malaria control strategies by the national malaria
control programs to community identified and targeted efforts that target achievement of
pre-elimination status requires new ways of organizing health care delivery, targeting
deployment of control intervention based on local evidence, engaging with and
harnessing human potential and involvement through community mobilization and
empowerment and empowering communities to ensure ownership and sustainability. We
hypothesis that these targeted community-tailored approaches when introduced to
complement current malaria control efforts are what will effect further malaria
transmission reductions and achieve malaria pre-elimination in the most cost-effective
manner. MEPR’s idea was to engage communities to actively participate in malaria
elimination processes by identifying challenges to malaria control, investing in health
interventions while participating in a comprehensive multi-disciplinary research effort.
The thesis “Determinants of malaria transmission dynamics in a rural community in
Eastern Rwanda” is about Project 1 work. Project 2, 3 and 4 are subjects of three other
theses by my colleagues with in this integrated PhD programme.

23
Thesis outline
Chapter 1 introduction
In part 1, we described the p. falciparum parasite diversity and the clinical and
parasitological profiles of cases seen at two sites of different malaria endemicities
(Chapter 2). In chapter 3, we described current prevalences and distributions of molecular
marker correlates of resistance for two prior used anti-malarial (Chloroquine and
Sulphodoxine – Pyrimethamine) at two study sites of variable transmission intensities.
In part 2, we measured the baseline asymptomatic malaria parasite carriage rates for all
age groups and gender (Chapter 4) and in chapter 5, we characterised malaria infections
and its association with under-nutrition and anaemia – two frequently co-existing disease
among > 5 year old children.
In part 3, we studied determinants of bed net source, ownership and use households 8
months after a universal LLIN net distribution campaign (Chapter 6). In chapter 7, using
reactive case finding surveillance, in health facility presumed malaria cases and their
asymptomatic household members; we measured malaria parasite carriage rates and
characterized malaria infection spatial clustering and risk factors in the Ruhuha site.
Part 4 concerns one community-level reviews. In chapter 8 a review of malaria control
stakeholders operating in the study area (Ruhuha sector) in done.

24
References
1. Greenwood B. Can malaria be eliminated? Trans R Soc Trop Med Hyg 2009;103:S2-S5.
2. Hommel M. Towards a research agenda for global malaria elimination. Malar Journal
2008; 7(Suppl 1):S1
3. Aguas R, White LJ, Snow RW, Gomes MG. Prospects for malaria eradication in sub-
Saharan Africa. PLoS ONE 2008;3:e1767.
4. Van Nam N, de Vries PJ, Van Toi L, Nagelkerke N. Malaria control in Vietnam: the Binh
Thuan experience. Trop Med Int Health 2005;10(4):357-65.
5. Hung lQ, de Vries PJ, Giao PT, Nam NV, Binh TQ, Chong MT, et al. Control of malaria:
a successful experience from Viet Nam. Bull World Health Organ 2002;80(8):660-666.
6. McKenzie FE, Baird JK, Beier JC, Lal AA, Bossert WH. A biologic basis for integrated
malaria control. Am J Trop Med Hyg 2002;67:517.
7. Otten M, Aregawi M, Were W, Karema C, Medin A, Bekele W, et al. Initial evidence of
reduction of malaria cases and deaths in Rwanda and Ethiopia due to rapid scale-up of
malaria prevention and treatment. Malar J 2009;8:14.

25
CHAPTER 2
Malaria case clinical profiles and Plasmodium falciparum parasite
genetic diversity: a cross sectional survey at two sites of different
malaria transmission intensities in Rwanda
Fredrick Kateera1, 2, *, Sam L. Nsobya3, 4, Stephen Tukwasibwe3, Petra F.
Mens2, 5, Emmanuel Hakizimana1, Martin P. Grobusch2, Leon Mutesa6,
Nirbhay Kumar7, Michele van Vugt2
1Medical Research Centre Division, Rwanda Biomedical Centre, PO Box 7162 Kigali,
Rwanda, Tel: +250 78 4684871 2Centre of Tropical Medicine and Travel Medicine, Department of Infectious Diseases,
Division of Internal Medicine, Meibergdreef 9, 1100 DD Amsterdam, The Netherlands 3Molecular Research Laboratory, Infectious Disease Research Collaboration, New
Mulago Hospital Complex, PO Box 7051, Kampala, Uganda 4Department of Pathology, School Biomedical Science, College of Health Science,
Makerere University PO Box 7072 Kampala Uganda 4Royal Tropical Institute/Koninklijk Instituutvoor de Tropen, KIT Biomedical Research,
Meibergdreef 39, 1105 AZ Amsterdam, Netherlands 5School of Medicine - College of Medicine and Health Sciences, University of Rwanda,
PO Box 3286 Kigali, Rwanda 6Department of Tropical Medicine, School of Public Health and Tropical Medicine,
Vector-Borne Infectious Disease Research Centre, Tulane University, 333 S Liberty
Street, Mail code 8317, New Orleans, LA 70112, USA
Published in: Malaria Journal 2016; 15:237

26
Abstract
Background
Malaria remains a public health challenge in sub-Saharan Africa with Plasmodium
falciparum being the principal cause of malaria disease morbidity and mortality. P.
falciparum virulence is attributed, in part, to its population-level genetic diversity, a
characteristic that has yet to be studied in Rwanda. Characterizing P. falciparum
molecular epidemiology in an area is needed to understand malaria transmission and thus
inform choice of malaria control strategies.
Methods
In this health-facility based survey, malaria case clinical profiles and parasite densities
and genetic diversity were compared among P. falciparum-infected patients identified at
two sites of different malaria transmission intensities in Rwanda. Data on demographics
and clinical features and finger-prick blood samples for microscopy and parasite
genotyping were collected. Nested PCR was used to genotype msp-2 alleles of FC27 and
3D7.
Results
Patients’ variables of age group, sex, fever (both by report and measured), parasite
density, and bed net use were found differentially distributed between the higher endemic
(Ruhuha) and lower endemic (Mubuga) sites. Overall multiplicity of P. falciparum
infection (MOI) was 1.73. However, mean MOI varied significantly, being 2.13 at
Ruhuha and 1.29 at Mubuga (p <0.0001). At Ruhuha, expected heterozygosity (EH) for
FC27 and 3D7 alleles were 0.62 and 0.49, respectively, whilst at Mubuga, EH for FC27
and 3D7 were 0.26 and 0.28, respectively.
Conclusions
In his study, a higher geometrical mean parasite counts; more polyclonal infections,
higher MOI and higher allelic frequency were noted at higher malaria-endemic Ruhuha
compared to the lower malaria-endemic Mubuga area. These differences in malaria risk

27
and MOI should be considered when, choosing setting-specific malaria control strategies;
assessing parameters such as drug resistance, immunity and impact of used interventions,
and in proper interpretation of malaria vaccine studies.
Keywords – Malaria - Plasmodium falciparum - Parasite density - Multiplicity of
infection - Rwanda

28
Background
In spite of the significant decline in malaria cases and deaths being reported globally,
malaria still accounted for about 200 million cases and over 500,000 deaths in 2014 [1].
The malaria burden decline, particularly in sub-Saharan Africa, has been associated with
the rapid scaling-up of interventions, including long-lasting insecticide-treated nets
(LLINs), indoor residual spraying (IRS) with insecticides, and use of artemisinin-based
combinational therapy (ACT) for managing uncomplicated malaria cases [2]. Scaling-up
of LLINs, IRS and ACT implementation in Rwanda was associated with a more than
50% decline in malaria morbidity and mortality among children under five years old
between 2005 and 2010 [3]. In spite of the decline however, malaria remains a public
health challenge with the entire Rwandese population considered as being at risk.
Human malaria infections exhibit a broad clinical spectrum ranging from asymptomatic
infection to severe life-threatening disease. Disease severity is influenced by interactions
between parasite, human host and environmental factors, including, but not limited to,
anti-malaria therapies used, levels of immunity, age, sex, and pregnancy status [4]. In
Rwanda, following emerging resistance in P. falciparum, Chloroquine was replaced with
amodiaquine + suplhodoxine – Pyrimethamine in 2001 and the later, subsequently,
replaced with artemether–lumefantrine (AL) in 2006, as first line antimalarial therapies
for uncomplicated malaria. Malaria transmission levels and the associated risk of
morbidity and mortality show a spatial heterogeneity even within small countries such as
Rwanda [5,6]. Current Rwandan malaria heterogeneity is partly influenced by the
variations in type and intensity of malaria control interventions deployed across different
settings as well as the baseline residual transmission potentials at the four different
malaria transmission zones [5]. Understanding malaria disease severity, including clinical
features and parasitaemia levels associated with malaria disease, in populations from
areas of differing malaria transmission intensities is needed for decision making on which
control tools may have optimal impact.
Plasmodium falciparum is the most prevalent cause of malaria morbidity and mortality in
Rwanda [5]. Plasmodium falciparum virulence is mediated, in part, by its population-

29
level genetic diversity which has been reported to influence malaria disease pathology [7-
9], acquisition of immunity [10-11], infection transmission intensity [12-14], and vaccine
development [15-16]. High malaria-endemic areas tend to have extensive malaria parasite
genetic diversity with infected humans often found with multiple genotypes. Conversely,
low transmission areas tend to yield limited P. falciparum parasite genetic diversity with
a higher proportion of infections being monoclonal [17-20].
Studying plasmodial molecular epidemiology is essential to understanding malaria
transmission. Currently, malaria disease severity among health facility-identified cases as
well as population-level parasite diversity remains unknown in Rwanda. This study
compared clinical profiles of malaria-confirmed cases, parasite densities and P.
falciparum genetic diversity [21-22] based on the msp-2 gene – a valid, reliable and
highly discriminatory and polymorphic marker used for genetic finger printing, at two
sites of differing malaria transmission intensities in Rwanda.
Methods
Study design and sites
Rwanda is divided into four malaria ecologic zones based on altitude, climate, level of
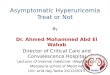
transmission, and disease vector prevalence [5]. Malaria cases for this cross-sectional
survey were recruited from rural Ruhuha sector (Bugesera District, Eastern Province) and
Mubuga sector (Karongi District, Western Province) (Figure 1) located within the highest
and lowest malaria transmission zones, respectively [5], in the months of January and
February 2015.

30
Fig. 1. Location map showing study sites of Ruhuha and Mubuga sectors in Rwanda. # Ruhuha sector is located in Bugesera District, Eastern Rwanda whilst Mubuga sectors is located in Karongi District, Western Rwanda
Baseline demographics, clinical features and blood sample collection: All health
facility-visiting cases aged ≥six months with microscopically confirmed P. falciparum
infection by the health facility laboratory technicians were eligible for enrolment. Upon
provision of written informed consent, a brief structured questionnaire was administered
and data on demographics (sex, age, area of residence), fever history, and bed net use on
the night before the survey were collected. In addition, body temperature was measured
using an electronic tympanic thermometer and finger-prick blood samples were taken to
prepare thick and thin smears – analysed by our study laboratory technicians - and for
blotting on to filter papers (Whatman 3MM) for use in performing molecular studies.

31
Preparation of blood films, microscopic examination and quality assurance
Thick blood smears were stained with 3% Giemsa for 60 min and slides read by two
blinded study microscopists. In case of three discordant results, a third reader was used to
resolve the discrepancy. Using the thick blood smear, parasite densities were enumerated
as the number of counts of asexual parasites per 200 leukocytes, assuming a median
leukocyte count of 8,000/μL. Thin smears were used to differentiate Plasmodium species.
External quality control was done on a 10% sample of randomly selected thick and thin
smears by microscopists at the National Reference Laboratory, Kigali, Rwanda whose
results were in agreement with those reported by the study technicians
Plasmodium falciparum DNA extraction and msp-2 allelic typing
DNA was extracted with Chelex 100 Resin (Bio-Rad Laboratories, Hercules, CA, USA)
as previously described [23]. The surface antigen loci msp-2 was amplified using
previously described primers [24]. Briefly, 2 μL of template DNA was amplified using
nested polymerase chain reaction (nPCR), with second-round primers specific to msp-2
allelic families. PCR products were then separated on a 2.5% agarose gel (UltraPure
Agarose; Invitrogen, Carlsbad, CA, USA) and stained with ethidium
bromide. GelCompar II software (Applied Maths, Sint-Martens-Latem, Belgium) was
used to select alleles and estimate PCR product size as described elsewhere [21].
Statistical analysis
Demographics, clinical features and bed net use data were collected using hard copy
study case record forms while laboratory results were transcribed into study laboratory
registers. Both datasets were double entered into EPI Info™ 7 (Centres for Disease
Control and Prevention, GA, USA) database and later transferred into STATA (version
13.1, College Station, TX, USA) for analysis. Parasitaemia - the number of parasites/μL
was graded as low (<1,000), moderate (1,000-9,999) and high (>10,000) as per WHO
parasitaemia cut-off for severe malaria in low transmission settings [25]. MOI was
defined as the proportion of people who carry more than one allele (genotype) for any of
the examined genes. Mean multiplicity of infection (MOI) was estimated by dividing the
total number of distinct msp2 genotypes detected by the number of positive samples.

32
Descriptive statistics of proportions and means were used to summarize distributions of
allelic families, baseline demographics, MOI, and other covariate data. Chi-square tests
were used to compare mean MOI and allelic variant distributions between study sites.
Independent t-test was used to compare mean MOI outcome by independent factors of
age group, study site, history of fever, and presence of measured fever (≥37.50C), sex and
bed net use. Expected heterozygosity index (HE), which measures locus diversity, was
calculated using the formulae HE = [n/(n-1)] [(1-!Pi2)], where n = sample size, Pi =
allelic frequency. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated
to evaluate the strengths of associations. Statistical significance was defined as P value
≤0.05 [22].
Ethical clearance
All adults and carers of children <18 years old were informed of the purpose and
procedures of the study, and recruited only after obtaining informed written consent. The
study was approved by the National Health Research Committee (NHRC) and the
Rwanda National Ethics Committee (No. 20/RNEC/2015), Kigali, Rwanda.
Results
Baseline study participant demographics
A total of 407 patients who were microscopically confirmed with malaria by health
facility laboratory technicians were enrolled and of these, 402 (98.8%) was
microscopically reconfirmed by study-trained technicians to be malaria positive. Of the
402, final data analysis was performed on 388 (96.5%) who were successfully genotyped
for the msp-2 alleles. Stratifying them by site, 195 (50.3%) of the participants were
enrolled at Ruhuha and 193 (49.7%) patients were enrolled at Mubuga. Details of study
participants’ demographics are reported in Table 1. A higher proportion (55.4%) of study
participants were females. The overall group mean age was 15.5 (SD±13.6 years).
Overall geometric mean parasite density was 1,119.3 parasites/μL.

Tab
le 1
Dem
ogra
phic
s, m
alar
ia p
reve
ntio
n, c
linic
al p
rofil
es a
nd g
eom
etri
c m
ean
para
site
den
sitie
s/*μ
L f
or m
alar
ia
case
s ide
ntifi
ed in
Ruh
uha
and
Mub
uga
site
s in
Rw
anda
χ² =
Chi
squa
re te
st
Var
iabl
es
Ruh
uha
site
n =
195
Mub
uga
site
n =
193
Pear
son'
s
χ²te
st
Dem
ogra
phic
sV
aria
ble
sub-
grou
psn
(%)
n (%
)
Age
gro
ups
6 m
onth
s to
5 ye
ars
52 (2
6.7)
22 (1
1.4)
-
6-1
5 ye
ars
95 (4
8.7)
93 (4
8.2)
-
16-7
3 ye
ars
48 (2
4.6)
78 (4
0.4)
<0.0
001
Sex
Mal
es77
(39.
5)
96 (4
9.7)
-
Fem
ales
118
(60.
5)97
(50.
3)0.
042
Mal
aria
pre
vent
ion
used
No.
repo
rting
bed
net
use
nig
ht p
rior t
o su
rvey
129
(66.
2)15
0 (7
7.7)
0.01
1
Feve
r hi
stor
y an
d
expe
rienc
e
No.
with
his
tory
of f
ever
in p
revi
ous 2
4 ho
urs
192
(98.
5)16
2 (8
3.9)
<0.0
001
No.
with
tym
pani
c te
mpe
ratu
re o
f ≥37
.5°C
78
(41.
5)11
0 (5
8.5)
0.00
1
Para
sito
logy
Para
site
cou
nt ra
nges
/per
μL
Lo
w (<
1,00
0)63
(32.
3)11
3 (5
8.6)
Mod
erat
e (1
,000
-9,9
99)
58 (2
9.7)
74 (3
8.3)
Seve
re (≥
10,0
00)
74 (3
8.0)
6 (3
.1)
<0.0
001
Geo
met
ric m
ean
para
sita
emia
(par
asite
s/μL
)
2,34
7.3
(95%
CI:
1,77
2.1-
3,10
9.2)
529.
7
(95%
CI:
402.
3-69
7.4)
<0.0
001

34
Demographics, clinical features, parasitological and malaria control characteristic
distributions among participants from the two study sites
The results of group comparisons of demographic, bed net use, fever experiences, and parasite
density among patients from the two study sites are shown in Table 1. Significant differences in
proportions of participant characteristics of sex (p=0.04) and age group (p=<0.0001) between
patients from Ruhuha and Mubuga sites were noted. At Ruhuha, a higher proportion (60.5%) of
patients were females compared to Mubuga (50.3%). Among children aged <five years, a higher
proportion was seen at Ruhuha (26.7%) compared to Mubuga (11.4%) while among those aged
>15 years, a higher proportion was enrolled at Mubuga (40.4%) compared to Ruhuha (24.6%).
With regard to history of reported fever, a significantly (p=0.001) higher proportion (99%) was
noted at Ruhuha compared to that reported at Mubuga (84%). In contrast, a significantly higher
proportion of patients (p=0.001) with a measured temperature of ≥37.5oC was seen at Mubuga
(58.5%) compared to that reported from Ruhuha (41.5%). A significantly higher proportion
(38.0%) of patients at Ruhuha had high parasite count (>10,000 parasites/μL) than those seen at
Mubuga (3.1%; p <0.0001). Similarly, geometric mean parasitaemia counts were higher at
Ruhuha (95% CI: 5,686.5-7,394.8) than at Mubuga (95% CI: 1,383.3-2,251.7). Bed net use was
significantly higher at Mubuga (77.7%) than at Ruhuha (66.2%) (p=0.001).
Infection clones and allelic diversity
Overall, a range of one to six infection clones per sample was seen. At both sites, about 55.4% of
the infections were monoclonal, with isolates from the Mubuga site carrying a significantly
higher proportion of monoclonal infections (73%) compared to those from Ruhuha (38%) (p
<0.0001). The numbers of strains per isolate are presented in Table 2. Overall, a total of 80
(27.8%) samples were co-infected by both FC27 and 3D7 types but with the number of strains
per isolate noted to be higher at Ruhuha (p <0.0001) compared to Mubuga (Table 2). In total,
more 3D7 allelic variants were detected (298) compared to FC27 variant (184) alleles.

35
Table 2 Plasmodium falciparum msp-2 PCR product numbers, size by base pair range and
HE for isolates with ≥one allele identified
Variable characteristic Variable sub-groupRuhuhan (%)
Mubugan (%)
Number of clones per sample 1 74 (38.0) 141 (73.0)2 60 (30.8) 48 (24.9)3 35 (17.9) 3 (1.6)4 18 (9.2) 1 (0.5)5 3 (1.5) 0 (0.0)6 5 (2.6) 0
msp-2 strain distribution 3D7 strain# 0 33 (16.9) 65 (33.7)
1 93 (47.7) 122 (63.2)2 53 (27.2) 5 (2.6)3 15 (7.7) 1 (0.3)4 1 (0.5) 0 (0.0)
FC27 strain$ 0 78 (40.0) 86 (44.6)1 86 (44.1) 99 (51.3)2 15 (7.7) 8 (4.2)3 11 (5.6) 0 (0.0)4 5 (2.6) 0 (0.0)
PCR products per base pair rangeFC27 300-330 95 (51.9) 114 (85.1)
350- 380 58 (31.4) 17 (12.7)400-430 15 (8.1) 2 (1.5)450-600 16 (8.6) 1 (0.7)Total FC27 PCR products 184 134HE (Average HE (0.44) 0.62 0.26
3D7 200-300 166 (55.7) 120 (83.3)320-400 132 (44.3) 22 (16.7)Total 3D7 PCR products 298 144HE (Average HE (0.39) 0.49 0.28
#3D7 strain difference in distribution = χ² <0.0001$FC27 strain difference in distribution = χ²=0.001

36
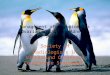
Allelic frequency and heterozygosity
For both FC27 and 3D7 alleles, 760 distinct P. falciparum clones were detected (Table 2).
Parasite allelic frequency varied among isolates from the two study sites (Figures 2 and 3).
Overall, the majority (68%) of isolates carried the FC27 300–330-bp size fragment (Figure 3)
while 70% carried the 3D7 200-300-bp size fragment (Figure 2). At Ruhuha, HE for 3D7 and
FC27 were 0.49 and 0.62 while at Mubuga, HE for 3D7 and FC27 was 0.28 and 0.26,
respectively (Table 2). At each of the 3D7 (Figure 2) and FC27 (Figure 3) alleles, higher levels
of polymorphisms were seen among isolates from Ruhuha than isolates from Mubuga.
Fig. 2. Distribution of msp-2 3D7 alleles across Ruhuha and Mubuga study sites in Rwanda

37
Fig. 3. Distribution of msp-2 FC27 alleles between Ruhuha and Mubuga study sites, Rwanda
Multiplicity of infection
Results for determinants of MOI are shown in Table 3. Overall, MOI for all infections at both
sites was ~1.7. However, MOI varied significantly (p value = <0.0001) between Mubuga (1.3)
and Ruhuha (2.1). In this study, MOI was seen to increase proportional to age group being from
1.7 among those under five years old to 1.9 among those aged six to 15 years and 1.5 among
those >15 years. Isolates from Ruhuha also had higher MOI compared to those from Mubuga.

Tab
le 3
Biv
aria
te a
naly
sis f
or c
ovar
iate
det
erm
inan
ts o
f mul
tiplic
ity o
f inf
ectio
n (M
OI)
Var
iabl
e V
aria
ble
sub-
grou
pn
(%)
$ MO
1 R
uhuh
a,
n=19
5$ M
OI M
ubug
a,
n=19
3O
vera
ll $ M
OI,
(± S
D)
Pva
lue
Stud
y si
teA
ll38
8(1
00%
)2.
131.
291.
72 (±
1.0
2)<0
.000
1
Stud
y pa
rtici
pant
s age
gro
up
≤5 y
ears
74
(19.
1)1.
921.
321.
74 (±
1.0
5)
6-15
yea
rs18
8 (4
8.4)
2.
341.
371.
86 (±
1.0
7)
≥16
year
s 12
6 (3
2.5)
1.
961.
211.
49 (±
0.8
9)0.
008
Sex
Mal
e17
3 (4
4.6)
2.
141.
271.
66 (±
0.9
7)
Fem
ale
215
(55.
4)
2.13
1.32
1.76
(±
1.06
)0.
321
Mea
sure
d fe
ver ≥
37.5
°C
Yes
188
(48.
4)2.
121.
291.
79 (±
1.1
0)
No
200
(51.
6)2.
151.
301.
63 (±
0.9
2)0.
119
Rep
orte
d fe
ver
Yes
354
(91.
2)2.
141.
291.
75 (±
1.0
5)
No
34 (8
.8)
2.00
1.32
1.38
(±
0.65
)0.
046
Para
site
den
sity
(par
asite
s/μL
)
<1,0
0017
6 (4
5.4)
1.91
1.28
1.51
(± 0
.82)
1,00
0-9,
999
132
(34.
0)2.
391.
311.
79 (±
1.1
0)
≥10,
000
80 (2
0.6)
2.12
1.33
2.06
(± 1
.18)
0.00
02
Num
ber o
f Pla
smod
ium
spec
ies
P.fa
lcip
arum
only
215
(55.
4)2.
331.
111.
73 (±
1.0
3)
P.fa
lcip
arum
and
P.ov
ale)
173
(44.
6)
2.13
1.30
1.42
(± 0
.67)
0.30
3
Pres
ence
of g
amet
ocyt
e
Yes
10 (2
.8)
1.50
1.38
1.30
(± 0
.56)
No
378
(97.
2)2.
141.
291.
72 (±
1.0
3)0.
322
His
tory
of s
leep
ing
unde
r a b
ed n
et
the
nigh
t bef
ore
surv
ey
Yes
279
(71.
9)2.
211.
281.
71 (±
1.0
9)
No
109
(28.
1)1.
991.
351.
73 (±
0.8
4)0.
834
$ MO
I = M
ultip
licity
of i
nfec
tion;
χ² =
Chi
squa
re te
st; S
D =
Sta
ndar
d de
viat
ion

39
Discussion
This study reports, for the first time in Rwanda, a differential spatial distribution of patient
demographics of age and sex, fever, parasite density and P. falciparum genetic diversity across
the two study sites. A higher geometrical mean parasite counts (2,347 vs 530 parasites), more
polyclonal infections, higher MOI and higher allelic frequency were observed at higher malaria-
endemic Ruhuha compared to the lower malaria-endemic Mubuga area.
A higher proportion of children aged <five years was enrolled at Ruhuha compared to Mubuga
while, in contrast, a higher proportion of patients aged >15 years was recruited at Mubuga
compared to Ruhuha. Higher malaria burden in younger age groups in settings of high malaria
transmission intensity have been reported previously [26-28]. The age-related association of
disease severity across different malaria transmission zones is currently poorly elucidated
particularly in the era of scaled-up interventions, such as LLINs and IRS and their impact on
reducing malaria transmission and influencing age-related malaria risk. As reported elsewhere,
scale-up of LLINs has been done[29-32], this study provides further evidence of a shift towards
higher malaria risk in older age groups. Results from this study may be confounded by the age-
distribution differences between the two sites, with the higher malaria-endemic Ruhuha sector
having a higher proportion of sick children aged <five years. A higher risk of P. falciparum
infection among younger age groups has been reported from elsewhere, particularly for severe
malaria [33]. The apparent higher risk of malaria among younger age groups at the higher
endemic Ruhuha site was probably due to a lower clinical protective immunity among the
younger age group (<five years) relative to older age groups (six to 15 years and >15 years) who
may have a higher degree of partially protective immunity already in high transmission settings.
In contrast, where malaria control activities, particularly LLIN usage, were scaled up, malaria
risk has been observed to shift to older age groups for reasons including delays in acquiring
immunity and less bed net use among the older age groups of six to 15 years, compared to
children <five years. A spatial and temporal analysis of changing transmission intensities may
provide clarity on allelic frequency epidemiology as determinants of setting-specific malaria risk.
Among patients enrolled at Ruhuha, a significantly higher proportion were females in contrast to

40
those recruited at Mubuga where both sexes were proportionally represented. The association
between malaria risk and sex remains equivocal. In contrast to this study’s findings, at the
Ruhuha site, a number of previous studies, including two conducted at the Ruhuha site, reported
a bias towards higher malaria risk among males [31,32,34-35]. The observed higher proportion
of females at Ruhuha in this study may be a chance occurrence due to the non-randomized study
design used. In addition, females, as seen in Rwanda, tend to have better health-seeking
behaviour, including more frequent visits to health facilities and are more likely to be recruited in
health system-based studies than their male counterparts. This is the most probable reason for
findings reported here, particularly given that it has been previously established that males had a
higher malaria risk in Ruhuha compared to females [31,34].
In this study, the proportion of patients with a reported fever experiences and by a fever >
≥37.5oC differed across the two sites. Whilst a higher proportion of Ruhuha-recruited patients
self-reported a history of fever in the 24 hours compared to those from Mubuga, in contrast, a
lower proportion of the same patients from Ruhuha were confirmed with a measured fever
(tympanic temperature ≥37.5oC) compared to Mubuga patients. Fever is a common malaria-
associated symptom and a major determinant of seeking care for suspected malaria in endemic
settings. At the higher malaria-endemic Ruhuha site, it is plausible that residents are more likely
to associate fever with malaria and hence the higher proportion of reported fevers. On the other
hand, at the lower malaria-endemic Mubuga site, with, presumably, a lower proportion of
individuals with at least partially protective levels of immunity, patients are more likely to have
symptomatic malaria infections presenting with fever than those at Ruhuha. However, the higher
proportion of children <five years old in Ruhuha may have confounded the observed higher
proportion of reported fevers in Ruhuha compared to Mubuga with malaria being associated with
fever or recent history of fever in infants. In contrast, the higher malaria endemicity in Ruhuha
may plausibly be associated with higher levels of protective immunity leading to a lower
proportion of malaria compared to persons from the lower-endemic Mubuga site, as previously
reported from the Ruhuha site [31,34]. Characterizing the association between fever experiences
and malaria risk is complicated by other determinants of measured fevers, including population
access to and use of antipyretic medications prior to visiting a health facility.

41
In this study, mean MOI was significantly higher at the higher malaria-endemic Ruhuha site
compared to the lower malaria-endemic Mubuga site. While many studies have reported
comparable findings of higher MOI in higher endemic settings and correspondingly lower MOI
in low endemic settings [17,20,36-37], a study in Ghana did not find any association between
MOI and transmission intensity [38]. A plausible reason for higher MOI in higher endemic
settings may be the greater diversity and the more frequent meiotic recombination in higher
malaria transmission settings. In this study, MOI was noted to significantly decrease with
increasing age. Previous studies on associations between MOI and age groups have shown mixed
findings, with some reporting no association [36,39-40], while others have reported comparable
findings of lower MOI with increasing age have been demonstrated in Nigeria, Ghana and
Senegal as seen in this study [11,38,41]. In a Tanzanian study conducted among children, MOI
was noted to peak among those aged three to seven years suggesting that younger age groups
(<ten years) may be contributing significantly to driving parasite diversity [42]. A possible
reason for the conflicting findings to those in this study may include differences in study age
groups and study site malaria intensities. It is plausible that multiple strains are needed to
develop immunity in younger children and hence the higher diversity in younger children.
Contrastingly, pre-existing immunity in older age groups may be selectively clearing out some
strain types and hence the noted inverse association between MOI and age.
In this study, MOI was positively correlated with parasite density. This finding accords with
previous studies where higher MOI among individuals with higher parasite densities has been
demonstrated [11,43]. In contrast, no association between MOI and level of parasitaemia was
reported elsewhere [36]. Because parasite densities are influenced by multiple determinants
including age, levels of exposure to malaria infections and area-specific transmission levels,
these latter factors may partially - either individually or collectively - account for the lack of
MOI and parasitaemia level associations observed elsewhere.
About 55% of the P. falciparum msp-2 confirmed isolates carried monoclonal (single allele)
infection. By study site, a higher proportion of monoclonal infections were seen at Mubuga
(73.1%) compared to Ruhuha (38.0%). These data are similar to other studies where higher
proportions of >50% and up to 100% polyclonal infections have been seen in meso-endemic and

42
holo-endemic settings [35,44-45]. Similarly, based on msp-1 genetic diversity marker, higher
proportions of polyclonal infection have been seen in high endemicity settings, suggesting that
malaria parasite polyclonality may be a useful proxy measure of level of endemicity [46].
Overall, genetic diversity was higher at the more malaria-endemic Ruhuha site than at Mubuga
whilst 3D7 allelic families were more frequent than the FC27 families. At Ruhuha, 3D7 PCR
products were 1.6-fold more than FC27 PCR products. Based on msp-1, similar observations of
higher diversity at a holo-endemic site in Tanzania compared to hypo-endemic south-western
Brazilian Amazon and meso-endemic southern Vietnam has been reported, with 3D7 reported as
the most frequently circulating allele in this study [47].
The majority of msp-2 FC27 alleles belonged to the 300-330-bp allele family while the most
prevalent msp-2 3D7 allele belonged to the 200-300-bp allele family. Between the two sites,
while the 300-330-bp allele was more frequent at Mubuga, the larger size (350-380, 400-450,
480-600) allelic families were more common at Ruhuha. In contrast to the FC27 gene, the 200-
330-bp allele was the most frequent circulating allele at both Ruhuha and Mubuga. Of interest,
findings from Mubuga of lower allelic diversity and lower frequency of circulating alleles point
to a high likelihood of re-infection with the same allele. Differentiating between recrudescence
and re-infection using msp-2 in a low-endemic setting such as Mubuga may be limited by the
msp-2 low discriminatory power.
A number of factors, including an adequate sample size, use of validated genetic marker for
diversity and allelic frequency, use of an automated gel reader to determine allelic family base
pair sizes, and a comparative analysis for the two study groups drawn from settings of different
malaria transmission intensities, are major strengths of this study. However, there were some
limitations. Firstly, there was a lack of earlier data on transmission intensity at either study sites
to delineate local malaria endemicities. Secondly, being a cross-sectional survey design, study
findings can only provide a baseline comparator for current diversity and disease clinical profiles
but is unable to determine the value of diversity on other disease outcomes other than parasite
density as well as time and impact of used intervention related effects. Thirdly, the study was
done at two sites whilst in Rwanda, malaria risk is categorized into four malaria ecologic zones.
Therefore, study findings may have limited generalizability, restricted to settings of comparable

43
transmission and malaria control tool implementation levels. Fourthly, due to cost restrictions,
we used a valid but lower discriminatory power assay (agarose gel electrophoresis) compared to
other assays (e.g. capillary electrophoresis) and thus findings may be of a lower accuracy. Lastly,
although msp-2 is a validated molecular marker of diversity, use of one marker may miss
variations at other polymorphic loci and underestimate the real magnitude of diversity.
Conclusion
This study demonstrated a differential distribution in demographics, measured temperature,
malaria parasite density as well as P. falciparum genetic diversity and allelic distribution
between individuals from two sites of variable malaria transmission intensities. HE and mean
MOI were higher among isolates collected from the higher malaria Ruhuha site. Locally,
characterising malaria disease severity, based on clinical features and parasitaemia levels, across
populations from settings of differing malaria transmission intensities is important in profiling
malaria risk maps and in decision making on which control tools may have optimal impact.
The difference in diversity may have differential effects on multiple parameters including drug-
resistant profiles, immunological responses to anti-malarial drug and effectiveness of vaccines
tested in Rwanda in the future.

44
Competing interests
The authors have declared that they have no competing interests.
Authors’ contributions
FK conceived the idea, designed the study, participated in performance of the experiments,
analysed the data and drafted the manuscript. SLN participated in performing the experiments
and revised the manuscript substantially. ST performed the experiments and provided in put in
writing the manuscript. EH, PFM and MPG provided substantial contribution to the manuscript
writing. KN supported study protocol development and provided substantial input in the writing
of the manuscript. MvV was involved in the conception of the study, supported field
implementation work and participated in the writing of manuscript. All authors read and
approved the final version of the manuscript.
Acknowledgments
We thank study participants, their parents and/or guardians as well as health facility leadership
and personnel for participating and supporting conduct of the study. This study was financially
supported by the NIH Fogarty International Centre through Grant #5R25TW009340 to FK as
part of his Fogarty Global Health Fellowship. Supplementary financial support for sample
analysis was received from the Netherlands Organization for Tropical Scientific Research
(NWO-WOTRO through Grant # SA358001 to the Academic Medical Centre, University of
Amsterdam, The Netherlands.

45
References
1. WHO: World Malaria Report 2014. Geneva, World Health Organization, 2014. Available at:
http://www.who.int/malaria/publications/world_malaria_report_2014/wmr-2014-no-
profiles.pdf. Accessed 3rd May 2015.
2. Steketee R, Campbell C. Impact of national malaria control scale-up programmes in Africa:
magnitude and attribution of effects. Malar J 2010; 9:299.
3. Otten M, Aregawi M, Were W, Karema C, Medin A, Bekele W, et al. Initial evidence of
reduction of malaria cases and deaths in Rwanda and Ethiopia due to rapid scale-up of
malaria prevention and treatment. Malar J 2009; 8:14.
4. Maitland K, Marsh K. Pathophysiology of severe malaria in children. Acta Trop 2004;
90:131–140.
5. USAID: Presidential Malaria Initiative – Rwanda, Malaria Operational Plan FY 2015.
Available at: http://www.pmi.gov/docs/default-source/default-document-library/malaria-
operational-plans/fy-15/fy-2015-rwanda-malaria-operational-plan.pdf?sfvrsn=3. Acessed 2nd
February 2016.
6. Karema C, Aregawi MW, Rukundo A, Kabayiza A, Mulindahabi M, Fall IS, et al. Trends in
malaria cases, hospital admissions and deaths following scale-up of anti-malarial
interventions, 2000–2010 Rwanda. Malar J 2012; 11:236.
7. Healer J, Murphy V, Hodder AN, Masciantonio R, Gemmill AW, Anders RF, et al. Allelic
polymorphisms in apical membrane antigen-1 are responsible for evasion of antibody-
mediated inhibition in Plasmodium falciparum. Mol Microbiol 2004; 52:159–168.
8. Ofosu-Okyere A, Mackinnon MJ, Sowa MP, Koram KA, Nkrumah F, Osei YD, et al. Novel
Plasmodium falciparum clones and rising clone multiplicities are associated with the increase
in malaria morbidity in Ghanaian children during the transition into the high transmission
season. Parasitology 2001; 123:113–123.
9. Sakihama N, Ohmae H, Bakote’e B, Kawabata M, Hirayama K, Tanabe K. Limited allelic
diversity of Plasmodium falciparum merozoite surface protein 1 gene from populations in the
Solomon Islands. Am J Trop Med Hyg 2006; 74: 31– 40.
10. Onway DJ, Cavanagh DR, Tanabe K, Roper C, Mikes ZS, Sakihama N, et al. A principal
target of human immunity to malaria identified by molecular population genetic and
immunological analyses. Nat Med 2000; 6:689–692.

46
11. Engelbrecht F, Togel E, Beck HP, Enwezor F, Oettli A, Felger I. Analysis of Plasmodium
falciparum infections in a village community in Northern Nigeria: determination of MSP-2
genotypes and parasite-specific IgG responses. Acta Trop 2000; 74: 63–71.
12. Owusu-Agyei S, Smith T, Beck HP, Amenga-Etego L, Felger I. Molecular epidemiology of
Plasmodium falciparum infections among asymptomatic inhabitants of a holoendemic
malarious area in northern Ghana. Trop Med Int Health 2002; 7: 421–428.
13. Mobegi VA, Loua KM, Ahouidi AD, Satoguina J, Nwakanma DC, Amambua-Ngwa A, et al.
Population genetic structure of Plasmodium falciparum across a region of diverse endemicity
in West Africa. Malar J 2012; 11:230.
14. Babiker HA, Charlwood JD, Smith T, Walliker D. Gene flow and cross-mating in
Plasmodium falciparum in households in a Tanzanian village. Parasitology 1995; 111:433-
442.
15. Chaitarra V, Holm I, Bentley GA, Petres S, Longacre S. The crystal structure of C-terminal
merozoite surface protein 1 at 1.8 resolution, a high protective malaria vaccine candidate.
Mol Cell 1999; 3:457–464.
16. Ferreira MU, Hartl DL. Plasmodium falciparum: worldwide sequence diversity and evolution
of the malaria vaccine candidate merozoite surface protein-2 (MSP-2). Exp Parasitol 2007;
115:32–40.
17. Haddad D, Snounou G, Mattei D, Enamorado IG, Figueroa J, Stahl S, et al. Limited genetic
diversity of Plasmodium falciparum in field isolates from Honduras. Am J Trop Med Hyg
1999; 60:30-34.
18. Babiker HA, Lines J, Hill WG, Walliker D. Population structure of Plasmodium falciparum
in villages with different malaria endemicity in east Africa. Am J Trop Med Hyg 1997;
56:141-147.
19. Peyerl-Hoffmann G, Jelinek T, Kilian A, Kabagambe G, Metzger WG, von Sonnenburg F.
Genetic diversity of Plasmodium falciparum and its relationship to parasite density in an area
with different malaria endemicities in West Uganda. Trop Med Int Health 2001; 6:607-613.
20. Babiker H, Ranford-Cartwirht LC, Walliker D. Genetic structure and dynamics of
Plasmodium falciparum infection in the kilombero region of Tanzania. Trans R Soc Med
Hyg 1999; 93:11–14.

47
21. Cattamanchi A, Kyabayinze D, Hubbard A, Rosenthal PJ, Dorsey G. Distinguishing
recrudescence from reinfection in a longitudinal antimalarial drug efficacy study: comparison
of results based on genotyping of msp-1, msp-2, and glurp. Am J Trop Med Hyg 2003;
68:133-139.
22. Mwingira F, Nkwengulila G, Schoepflin S, Sumari D, Beck H-P, Snounou G, et al.
Plasmodium falciparum msp1, msp2 and glurp allele frequency and diversity in sub-Saharan
Africa. Malar J 2011; 10:79.
23. Plowe CV, Djimde A, Bouare M, Doumbo O, Wellems TE. Pyrimethamine and proguanil
resistance-conferring mutations in Plasmodium falciparum dihydrofolate reductase:
polymerase chain reaction methods for surveillance in Africa. Am J Trop Med Hyg 1995;
52:565–568.
24. Zwetyenga J, Rogier C, Tall A, Fontenille D, Snounou G, Trape JF, et al. No influence of age
on infection complexity and allelic distribution in Plasmodium falciparum infections in
Ndiop, a Senegalese village with seasonal, mesoendemic malaria. Am J Trop Med Hyg 1998;
59:726-735.
25. WHO: Guidelines for the treatment of malaria. 2nd ed. Geneva, World Health Organization,
2010; page 35.
26. Snow RW, Bastos de Azevedo I, Lowe BS, Kabiru EW, Nevill CG, Mwankusye S, et al.
Severe childhood malaria in two areas of markedly different falciparum transmission in east
Africa. Acta Trop 1994; 57:289–300.
27. Snow RW, Omumbo JA, Lowe B, Molyneux CS, Obiero JO, Palmer A, et al. Relation
between severe malaria morbidity in children and level of Plasmodium falciparum
transmission in Africa. Lancet 1997; 349:1650-1654.
28. Carneiro I, Roca-Feltrer A, Griffin JT, Smith L, Tanner M, Schellenberg JM, et al. Age-
patterns of malaria vary with severity, transmission intensity and seasonality in sub-Saharan
Africa: a systematic review and pooled analysis. PLoS One 2010; 5:e8988.
29. Akhwale WS, Lum JK, Kaneko A, Eto H, Obonyo C, Björkman A, et al. Anemia and malaria
at different altitudes in the western highlands of Kenya. Acta Trop 2004; 91:167–175.
30. Sintasath D, Ghebremeskel T, Lynch M, Kleinau E, Bretas G, Shililu J, et al. Malaria
prevalence and associated risk factors in Eritrea. Am J Trop Med Hyg 2005; 72:682–687.

48
31. Winskill P, Rowland M, Mtove G, Malima RC, Kirby MJ. Malaria risk factors in north-east
Tanzania. Malar J 2011; 10:98.
32. Kateera F, Mens PF, Hakizimana E, Ingabire CM, Muragijemariya L, Karinda P, et al.
Malaria parasite carriage and risk determinants in a rural population: a malariometric survey
in Rwanda. Malar J 2015; 14:16.
33. Ceesay SJ, Koivogui L, Nahum A, Taal MA, Okebe J, Affara M, et al. Malaria prevalence
among young infants in different transmission settings, Africa. Emerg Infect Dis 2015;
21:1114–1121.
34. Rulisa S, Kateera F, Bizimana JP, Agaba S, Dukuzumuremyi J, Baas L, et al. Malaria
prevalence, spatial clustering and risk factors in a low endemic area of Eastern Rwanda: a
cross sectional study. PLoS One 2013; 8:e69443.
35. Pathak S, Rege M, Gogtay NJ, Aigal U, Sharma SK, Valecha N, et al. Age-dependent sex
bias in clinical malarial disease in hypoendemic regions. PLoS One 2012; 7:e35592.
36. Atroosh WM, Al-Mekhlafi HM, Mahdy M, Saif-Ali R, Al-Mekhlafi AM, Surin J. Genetic
diversity of Plasmodium falciparum isolates from Pahang, Malaysia based on MSP-1 and
MSP-2 genes. Parasit Vectors 2011; 4:233.
37. Arnot D. Unstable malaria in Sudan: the influence of the dry season. Clone multiplicity of
Plasmodium falciparum infections in individuals exposed to variable levels of disease
transmission. Trans R Soc Trop Med Hyg 1998; 92:580–585.
38. Agyeman-Budu A, Brown C, Adjei G, Adams M, Dosoo D, Dery D, et al. Trends in
multiplicity of Plasmodium falciparum infections among asymptomatic residents in the
middle belt of Ghana. Malar J 2013; 12:22.
39. Branch OH, Takala S, Kariuki S, Nahlen BL, Kolczak M, Hawley W, et al. Plasmodium
falciparum genotypes, low complexity of infection, and resistance to subsequent malaria in
participants in the Asembo Bay Cohort Project. Infect Immun 2001; 69:7783-7792.
40. Takala SL, Coulibaly D, Thera MA, Dicko A, Smith DL, Guindo AB, et al. Dynamics of
polymorphism in a malaria vaccine antigen at a vaccine-testing site in Mali. PLoS Med 2007;
4:e93.
41. Ntoumi F, Contamin H, Rogier C, Bonnefoy S, Trope JF, Mercereau-Puijalon O. Age
dependent carriage of multiple Plasmodium falciparum merozoite surface antigen-2 alleles in
asymptomatic malaria infection. Am J Trop Med Hyg 1995; 52:81–88.

49
42. Smith T, Felger I, Kitua A, Tanner M, Beck HP. Dynamics of multiple Plasmodium
falciparum infections in infants in a highly endemic area of Tanzania. Trans R Soc Trop Med
Hyg 1999; 93:35–39.
43. Smith T, Beck HP, Kitua A, Mwankusye S, Felger I, Fraser-Hurt N, et al. Age dependence of
the multiplicity of Plasmodium falciparum infections and of other malariological indices in
an area of high endemicity. Trans R Soc Trop Med Hyg 1999; 93:15-20.
44. Mohammed H, Mindaye T, Belayneh M, Kassa M, Assefa A, Tadesse M, et al. Genetic
diversity of Plasmodium falciparum isolates based on MSP-1 and MSP-2 genes from Kolla-
Shele area, Arbaminch Zuria District, southwest Ethiopia. Malar J 2015; 14:73.
45. Legrand E, Volney B, Lavergne A, Tournegros C, Florent L, Accrombessi D, et al.
Molecular analysis of two local falciparum malaria outbreaks on the French Guiana coast
confirms the msp1 B-K1/varD genotype association with severe malaria. Malar J 2005; 4:26.
46. Babiker HA. Plasmodium falciparum population in the unstable malaria area of eastern
Sudan is stable and genetically complex. Trans R Soc Trop Med Hyg 1998; 92:585-9.
47. Ferreira MU, Kaneko O, Kimura M, Liu Q, Kawamoto F, Tanabe K. Allelic diversity at the
merozoite surface protein-1 (MSP-1) locus in natural Plasmodium falciparum populations: a
brief overview. Mem Inst Oswaldo Cruz 1998; 93:631-638.

50
CHAPTER 3
Molecular surveillance of chloroquine and sulphadoxine Pyrimethamine
resistance markers reveals partial recovery of Chloroquine Susceptibility but
sustained intense levels of Sulfadoxine - Pyrimethamine mutations at two sites
of different malaria transmission intensities in Rwanda
Fredrick Kateera1, 2, Sam L. Nsobya3, 4, Steven Tukwasibwe3, Emmanuel
Hakizimana1, 5, Leon Mutesa6, Petra F. Mens2, 7, Martin P. Grobusch2, Michèle van
Vugt2, Nirbhay Kumar8
1. Medical Research Centre Division, Rwanda Biomedical Centre, PO Box 7162 Kigali,
Rwanda.
2. Centre of Tropical Medicine and Travel Medicine, Department of Infectious Diseases,
Division of Internal Medicine, Meibergdreef 9, 1100 DD Amsterdam, The Netherlands.
3. Molecular Research Laboratory, Infectious Disease Research Collaboration (IDRC), New
Mulago Hospital Complex, PO Box 7051, Kampala, Uganda.
4. School of Biomedical Science, College of Medicine Makerere University.
5. Malaria & Other Parasitic Diseases Division, Rwanda Biomedical Centre, Kigali, Rwanda.
6. College of Medicine & Health Sciences, University of Rwanda, P.O. Box 3286, Kigali,
Rwanda.
7. Royal Tropical Institute/Koninklijk Instituutvoor de Tropen, KIT Biomedical Research,
Meibergdreef 39, 1105 AZ Amsterdam, Netherlands.
8. Department of Tropical Medicine, School of Public Health and Tropical Medicine, Vector-
Borne Infectious Disease Research Centre, Tulane University, 333 S Liberty Street, Mail
code 8317, New Orleans, LA 70112
Submitted to Acta Tropica Journal

51
Abstract
Faced with intense level of chloroquine (CQ) resistance in Plasmodium falciparum malaria,
Rwanda replaced CQ with amodiaquine (AQ) + sulfadoxine-pyrimethamine (SP) in 2001, and
subsequently with artemether–lumefantrine (AL) in 2006, as first-line treatment for
uncomplicated malaria. Following years of discontinuation of CQ use, re-emergence of CQ-
susceptible parasites has been reported in countries including Malawi, Kenya and Tanzania. In
contrast, high SP resistance levels continue to be reported even in countries of reduced SP drug
selection pressure. The prevalences and distributions of genetic polymorphisms of gene loci
linked with CQ and SP resistance at two sites of different malaria transmission intensities are
described here to better understand drug-related genomic adaptations over time and exposure to
varying drug pressures in Rwanda. Using filter paper blood isolates collected from malaria
patients, Plasmodium DNA was extracted and a nested PCR performed to identify resistance-
mediating polymorphisms in the pfcrt, pfmdr1, pfdhps and pfdhfr genes. Amplicons from a total
of 399 genotyped samples were analysed by ligase detection reaction fluorescent microsphere
assay. CQ susceptible pfcrt 76K and pfmdr1 86N wild-type parasites were found in about 50%
and 81% of isolates, respectively. Concurrently, SP susceptible pfdhps double (437G-540E),
pfdhfr triple (108N-51I-59R), the quintuple pfdhps 437G-540E / pfdhfr 51I-59R-108N and
sextuple haplotypes were found in about 84%, 85%, 74% and 18% of isolates, respectively.
High-level SP resistance associated pfdhfr 164L and pfdhps 581G mutants were noted to decline.
Mutations pfcrt 76T, pfdhfr 59R and pfdhfr 164L were found differentially distributed between
the two study sites with the pfdhfr 164L mutants found restricted in at Ruhuha site, eastern
Rwanda. Overall, sustained intense levels of SP resistant mutants and a slow recovery of CQ
susceptible parasites were found in this study after 7 years and 14 years of the drug withdrawal
from use, respectively. Most likely, the high prevalence of resistant parasites selected by the
continued use of dhfr/dhps inhibitors like trimethoprim-sulfamethoxazole (TS) for the treatment
of and prophylaxis against bacterial infections among HIV infected individuals as well as the
continued use of IPTp-SP within the East and Central African regions for malaria prevention
among pregnant women may partly account for the observed sustained SP resistant parasite
prevalent. With regard to Chloroquine, the slow recovery of CQ susceptible parasites may have
been caused partly by the continued use of CQ and/or or CQ mimicking antimalarial drugs like
AQ in spite of policies to withdraw it from Rwanda and neighbouring countries Uganda and

52
Tanzania. Continued surveillance of P. falciparum CQ and SP associated polymorphisms is
recommended for guiding future rational drug policy-making and mitigation of future risk of
anti-malaria drug resistance development.

53
Background
Globally, malaria accounts for about 214 million cases and over 438,000 deaths annually (World
Health Organization, 2015). A major hindrance to malaria control is the development of
resistance in malaria parasites to available antimalarial therapies. Currently, artemisinin-based
combination therapies (ACTs) – consisting of a combination of a fast-acting artemisinin
component (artesunate, artemether, or dihydroartemisinin) and a longer-acting partner drug
(lumefantrine, amodiaquine, piperaquine, or mefloquine), that are widely used and largely still
effective against P. falciparum, are beginning to show clinical failure. Discouragingly, evidence
for ACT resistance is now accumulating in Southeast Asia raising concerns of a possible lack of
malaria treatment in the near future at a time when anti-malarial therapy options are limited
(Dondorp et al., 2009; Ashley et al., 2015). However, this does not seem to be a problem (as yet)
in Sub-Saharan Africa. Prior to introduction of ACTs, widespread resistance to two cost-
effective and safe anti-malarial therapies of chloroquine (CQ), - a highly effective first line anti-
malarial monotherapy used for about 50 years, and anti-folate drug sulphadoxine -
pyrimethamine (SP), led to their withdrawal from primary use in many malaria-endemic settings
(Young & Moore. 1961; Harinasuta et al., 1965; Enosse et al., 2008; Hastings et al., 2002;
Kublin et al., 2002; Pearce et al., 2009, White. 1999).
Resistance to anti-folate drugs like SP has been associated with polymorphisms in the P.
falciparum dihydrofolate reductase (pfDHFR) and dihydropteroate synthase (pfDHPS) genes
while polymorphisms in the P. falciparum CQ resistance transporter (pfCRT) gene is the major
mediator of resistance to CQ and amodiaquine (AQ) (Kublin et al., 2002; Ecker et al., 2012). In
addition, the P. falciparum multidrug resistance (pfMDR1) glycoprotein gene polymorphisms are
associated with increased sensitivity to lumefantrine, mefloquine, and dihydroartemisinin, and to
decreased sensitivity to CQ and AQ (Rosenthal, 2013; Koenderink et al., 2010).
Faced with emerging resistance in P. falciparum in Rwanda, CQ was replaced with AQ + SP in
2001 and the later subsequently replaced with artemether–lumefantrine (AL) in 2006, as first line
antimalarial therapies for uncomplicated malaria (Zeile et al., 2012). For SP however, its use in
intermittent preventive treatment of malaria in pregnancy (IPTp) continued until 2008 when it
was withdrawndue to increasing anti-folate resistance (Karema et al., 2012). Elsewhere, after
periods of complete CQ withdrawal, re-emergence of CQ-sensitive parasite strains, albeit at

54
varying rates over time and across different geographic settings, has been reported (Ndiaye et al.,
2012; Mwai et al., 2009). Malawi has been emblematic to this recovery of CQ susceptibility,
suggesting that CQ-sensitive parasites may have a fitness advantage over resistant parasites in
the absence of CQ drug selection pressure (Laufer et al., 2006). This is further evidenced by the
notably lower prevalence of mutant pfcrt 76T and pfmdr1 86Y alleles in low malaria
transmission settings where drug pressure is presumably less (Ord et.al, 2009). Similar to the CQ
experience, use of SP has been associated with ever increasing levels of resistance in P.
falciparum in malaria endemic countries, including Rwanda (Matondo et al., 2014; Karema et
al., 2010). However, four years after cessation of SP use, high-level SP resistance was still
observed in Rwanda (Karema et al., 2010).
Data on anti-malarial drug resistance is needed for rational drug policy-making, effective malaria
management and for designing strategies that mitigate risk and burden of drug resistance. For
Rwanda, there is paucity of data on the current prevalence of CQ and SP resistance years after
CQ and SP withdrawal. This study measured the prevalence and distributions of P. falciparum
molecular markers of resistance to CQ and SP, 14 and 7 years after a policy change involving
withdrawal of these two drugs from use, respectively, at two sites of different transmission
intensities.
Materials and methods
Study area and design
Rwanda is broadly divided into four malaria ecologic zones based on altitude, climate, level of
transmission, and disease vector prevalence (President’s Malaria Initiative, 2015).
Topographically, malaria transmission is considered meso-endemic in the plain regions of
eastern and southern provinces while being epidemic-prone in the high plateau and hill settings
of northern and western provinces, respectively. Ruhuha sector, Bugesera district, eastern
province is located within the high malaria transmission zone whilst Mubuga sector, Kalongi
district, western province is located in the low transmission zone (President’s Malaria Initiative,
2015) (Figure 1). P. falciparum infected isolates were collected from malaria confirmed cases
seen at two rural health facilities located in the two sectors in a cross-sectional survey carried out
between January and February 2015.

55
Figure 1. Location map showing study sites of Ruhuha and Mubuga in Rwanda.
Study participant enrolment and assessments
Study inclusion was limited to health-facility area residents who were microscopically confirmed
with P. falciparum infections and who were aged ≥ 6 months. Upon provision of a written
informed consent, finger-prick blood samples were then collected and used for preparation of
thick and thin blood film for microscopy and for blotting on to filter papers.
Ligase Detection Reaction-Fluorescent Microsphere (LDR-FM) Assay
DNA was extracted from filter paper bloodspots using Chelex® (Bio-Rad, Germany) as
described elsewhere (Kain et al., 1991). Genomic DNA representing s ingle nucleotide
polymorphisms (SNPs) mediating resistances in pfcrt, pfmdr1 and pfdhfr and pfdhps genes were
then amplified by nested PCR as previously described (LeClair et al., 2013) with the ligase
detection reaction-fluorescent microsphere assay used to analyse all SNPs of interest. SNPs were
categorized as wild type (WT), mutant and mixed alleles against the comparator control
reference strain DNA.

56
Statistical analysis
All statistical analyses were done using STATA version 13.1 (STATA Corp Inc., TX, USA).
Differences in characteristics distribution of the study population for the different sites were
tested by analysis of variance (ANOVA). Prevalence of SNPs was calculated for WT or mixed
infections or pure mutants. In the final analysis, all pure mutant and mixed infections were
summed up to generate the number of mutant genotypes per codon. Genotype proportions
between the two study sites were compared using Pearson’s chi square test. A p value of < 0.05
was considered statistically significant.
Ethical clearance
All adults and caregivers of children < 18 years were informed of the study purpose and
procedures; recruitment was done only after obtaining informed written consent. The study was
reviewed and approved by the National Health Research Committee (NHRC) and the Rwanda
National Ethics Committee (No. 020/RNEC/2015), Kigali, Rwanda.
Results
Patient characteristics and variable distributions
Four hundred and two (402) patients aged 6 months to 73 years were enrolled, of these, 399
patients whose isolates provided at least one genotype result were included in the current study.
Table 1 describes study participant baseline data.

Tab
le 1
. Dem
ogra
phic
cha
ract
eris
tics a
t enr
olm
ent f
or 3
99 st
udy
part
icip
ants
from
Ruh
uha
and
Mub
uga
site
s, R
wan
da. *
*Sho
ws M
ean
+ st
anda
rd d
evia
tion
(SD
); #
show
s 95%
Con
fiden
ce In
terv
al (C
I)
Var
iabl
e
Var
iabl
e
sub -
grou
p
Mub
uga
n =2
05
Ruh
uha
n=19
4
Ove
rall
N=3
99
Age
(M
ean
± SD
)-
17.7
± 1
4.0*
13.1
± 1
2.7
15.5
± 1
3.5)
Age
Gro
up0
-5 y
ears
26 (1
2.7)
51 (2
6.3)
77 (1
9.3)
6-1
5 ye
ars
96 (4
6.8)
94 (4
8.4)
190
(47.
6)
≥ 16
Yea
rs83
(40.
5)49
(25.
3)13
2 (3
3.1)
Sex
Mal
e10
0 (4
8.8)
79 (4
0.7)
179
(44.
9)
Fem
ale
105
(51.
2)11
5 (5
9.3)
220
(55.
1)
Geo
met
ric
Mea
n
Para
site
/μl
blo
od-
599.
5
(95%
CI# : 4
57.2
-78
6.0)
2190
.7
(95%
CI# : 1
649.
1 –
2910
.2)
1125
.7
(95%
CI# : 9
16.7
-13
82.4
)

58
Genotyping efficacy at each codon
Per codon, typing was achieved in 97.2% (388) of samples for pfcrt 76 (Figure 1); 95.7% (382)
for 86, 86.7% (346) for 184, 94.7% (378) for 1034, 97.5% (389) for 1042 and 97.0% (387) for
1246 at pfmdr1 codons (Table 2); 94.2% (376) for 51, 95.5% (381) for 59, 95.0% (379) for 108
and 94.5% (377) for 164 pfdhfr codons; 91.2% (364) for 437, 91.0% (363) for 540, 91.0% (363)
for 581, and 362 (90.7) for 613 pfdhps codons (Table 3). Among the typed polymorphisms,
purely susceptible WT infections were observed for alleles pfmdr1 1042N and 1034S and pfdhps
613A, while mixed type infections were identified for pfcrt 76 (14%), Pfmdr1 86 (17%), 184
(32%) and 1246 (16%), pfdhfr 51 (1%) and 59 (17%) and for pfdhps 437 (8%), 540 (0.5%) and
581 (9%), respectively. Saturation (100%) mutant level was only identified in pfdhfr codon 108.
Table 2. A comparison of Pfmdr1 genotype proportions by study site Mubuga and. Ruhuha
Ruhuha Mubuga All sites
Pfmdr1
genotypes
Wild
Type
n (%)
Mixed*
n (%)
Mutant
n (%)
Wild type
n (%)
Mixed
n (%)
Mutant
n (%)
Total Mutants
(Mixed + pure mutants)
n (%)
N86Y 146 (78.5) 31 (16.7) 9 (4.8) 163 (83.2) 28 (14.3) 5 (2.6) 73 (19.1)
Y184F 64 (37.4) 54 (31.6) 53 (31.0) 75 (42.9) 58 (33.1) 42 (24.0) 207 (59.8)
N1042C 188 (100) 0 (0) 0 (0) 201 (100) 0 (0) 0 (0) 0 (0)
S1034C 188 (100) 0 (0) 0 (0) 190 (100) 0 (0) 0 (0) 0 (0)
D1246Y 141 (79.2) 29 (16.3) 8 (4.5) 162 (82.2) 19 (9.6) 16 (8.1) 72 (19.2)
N86Y, D1246Y 177 (91.2) 17 (8.8) 190 (92.7) 15 (7.3) 32 (8.0)
*Mixed infection denotes an isolate in which both WT and mutant genotypes were detected.

Tab
le 3
. Pre
vale
nce
of p
fdhr
fand
pfdh
psge
noty
pes b
y st
udy
site
Mub
uga
and
Ruh
uha
Ruh
uha
Mub
uga
All
site
s
pfdh
fral
lele
sW
ild T
ype
n (%
)M
ixed
*n
(%)
Mut
ant
n (%
)W
ild ty
pen
(%)
Mix
edn
(%)
Mut
ant
n (%
)
All
Mut
ants
(M
ixed
+ p
ure
mut
ants
) (%
) N
51I
0 (0
)2
(1.1
)18
8 (9
8.9)
1 (0
.5)
0 (0
)18
5 (9
9.5)
375
(99.
7)C
59R
30 (1
5.8)
33 (1
7.4)
127
(66.
8)7
(3.7
)24
(12.
6)16
0 (8
3.8)
344
(90.
3)S1
08N
0 (0
)0
(0)
190
(100
)0
(0)
0 (0
)18
9 (1
00)
379
(100
.0)
I164
L16
8 (8
9.8)
9 (4
.8)
10 (5
.3)
190
(100
)0
(0)
0 (0
)19
(5.0
)N
51I,
C59
R, S
108N
34 (1
7.5)
160
(82.
5)26
(12.
7.)
179
(87.
3)33
9 (9
0.2)
N51
I, C
59R
, S10
8N, I
164L
194
(100
)0
(0)
187
(91.
2)18
(8.8
)18
(4.5
)pf
dhps
alle
les
A43
7G15
(8.2
)15
(8.2
)15
4 (8
3.7)
11 (6
.1)
28 (1
5.6)
141
(78.
3)33
8 (9
2.9)
K54
0E10
(5.5
)1
(0.5
)17
2 (9
4.0)
10 (5
.6)
1 (0
.6)
169
(93.
9)34
3 (9
4.5)
A61
3S10
0.0
(100
)0.
0 (0
)0.
0 (0
)10
0.0
(100
)0.
0 (0
)0.
0 (0
)0
(0.0
)A
581G
134
(73.
2)16
(8.7
)33
(18.
0)14
1 (7
8.3)
14 (7
.8)
25 (1
3.9)
88 (2
4.2)
Dou
ble
pfdh
fr(A
437G
-K54
0E)
39 (1
9.0)
166
(81.
0)26
(13.
4)16
8 (8
6.6)
334
(83.
7)Tr
iple
pfd
hfr
(A43
7G-K
540E
-A58
1G)
34 (1
7.5)
160
(82.
5)29
(12.
7)17
9 (8
7.3)
339
(85.
0)Q
uint
uple
pfdh
frE5
40-G
437
/ pf
dhfr
51I-
59R
-108
N)
51 (2
6.3)
143
(73.
7)52
(25.
4)15
3 (7
4.6)
296
(74.
2)
Sext
uple
pfd
hfr
E540
-G43
7 /
pfdh
fr51
I-59
R-1
08N
+ p
fdhp
s A58
1)15
2 (7
8.4)
42 (2
1.6)
174
(84.
9)31
(15.
1)73
(18.
3)
*M
ixed
infe
ctio
n de
note
s an
isol
ate
in w
hich
bot
h W
T an
d m
utan
t gen
otyp
es w
ere
dete
cted
.

60
Age related association with in prevalence of mutations
For each of pfcrt 76, pfmdr1 86, Pfdhfr (51, 59, 108) and Pfdhps (437, 540, 581) genes, no
statistically significant difference in mean number of mutant strains between age groups 0-5
years versus 6-15 years versus >15 years and age groups 0-5 years versus > 5 years was found
(data not shown).
Pfcrt gene
Overall, for the 388 total isolates typed, 50.8% (197) carried the WT pfcrt 76K allele while
10.1% (39) were pure mutants and 39.2% (152) mixed infections. Stratified by site, WT, mixed
and mutant pfcrt 76T genotype prevalence were 45.1%, 14.1%, 40.8%, respectively at Ruhuha
and 56.3%, 6.1%, and 37.6% at Mubuga, respectively (Figure 1). Pfcrt 76T mutant (includes
both pure and mixed mutants) distribution varied significantly (p = 0.026) with higher
proportions seen at Ruhuha (55%) compared to Mubuga (44%).
Pfmdr1 gene
Pfdmr1 WT 86N alleles were found in 309 (80.9%) isolates while 59 (15.4%) and 14 (3.7%) of
isolates carried mixed and mutant type infection, respectively. WT alleles 184Y and 1246D were
found in 40% and 80% isolates, respectively (Table 2). The distribution of all mutant alleles at
typed pfdmr1 codons were comparable for isolates from the two sites (Table 4).

Tab
le 4
. Com
pari
sons
in p
ropo
rtio
nal d
istr
ibut
ions
of C
hlor
oqui
ne a
nd S
ulph
adox
ine
–Py
rim
etha
min
e po
lym
orph
ism
s by
stud
y si
tes.
C
*P
valu
e co
mpa
ring
prop
ortio
ns o
f mut
ant p
aras
ites w
ere
base
d on
a 2
-sam
ple
t-tes
t.Si
gnifi
cant
val
ues a
re in
bol
dfac
e.
Alle
lePo
lym
orph
ism
Num
ber
(%) o
f mut
ant a
llele
sPe
arso
n's
X2te
stP
valu
e*R
uhuh
a -n
(%)
Mub
uga
-n (%
)pf
crt
76T
105
(55.
0)86
(43.
7)4.
971
0.02
6pf
mdr
186
Y40
(21.
5)33
(16.
8)1.
346
0.24
618
4Y10
7 (6
2.6)
100
(57.
1)1.
0611
0.30
310
42C
00
--
1034
C0
0-
-12
46Y
37 (2
0.8)
35 (1
7.8)
0.54
970.
458
pfdh
ps61
3S0
058
1G49
(26.
8)39
(21.
7)43
7G16
9 (9
1.9)
169
(93.
9)0.
572
0.45
054
0E17
3 (9
4.5)
170
(94.
4)0.
001
0.97
0pf
dhfr
51I
190
(100
)18
5 (9
9.5)
2.98
20.
225
59R
160
(84.
2)18
4 (9
6.3)
19.5
10<
0.00
0110
8N19
0 (1
00)
189
(100
)-
-16
4L19
(10.
2)0
(0)
20.3
29<
0.00
01G
roup
edal
lele
sD
oubl
epf
dhps
(540
E-43
7G)
168
(91.
8)16
6 (9
2.2)
2.31
10.
129
Trip
lepf
dhfr
(51I
-59R
-108
N)
160
(84.
2)17
9 (9
6.2)
1.83
00.
176
Qua
drup
le(5
1I-5
9R-1
08N
-164
L)18
(8.8
)0
(0.0
)17
.839
< 0.
0001
Qui
ntup
lepf
dhfr
540E
-G43
7G /
pfdh
fr51
I-59
R-1
08N
)14
3 (7
3.7)
153
(74.
6)0.
044
0.83
3Se
xtup
le p
fdhf
rE5
40-G
437-
581G
/ p
fdhf
r51
I-59
R-1
08N
)42
(21.
7)31
(15.
1)2.
8411
0.09
2

Pfdhps gene
High-level prevalence for pfdhps mutant (includes both pure and mixed mutants) alleles
437G and 540E of 92.9% and 94.5%, respectively, was seen. At 581G and 613S codons,
mutant prevalence was 24.2% and 0%, respectively. The distributions of 437G, 540E and
581G mutant alleles were comparable across the two study sites.
Pfdhfr gene
Pfdhfr mutant (includes both pure and mixed mutants) allele prevalence at codons 51I,
59R, 108N and 164L were 99.7%, 90.3%, 100% and 5%, respectively, whilst the
prevalence of the pfdhfr triple (108N-51I-59R) haplotype was 85% (Table 3). The
distribution for each of pfdhfr 164L and 59R mutants varied significantly (p < 0.0001) by
study sites. Notably, all 19 164L mutants were seen at the Ruhuha site of higher malaria
endemicity. For the 59R mutants, a higher prevalence was observed at the lower malaria
endemic Mubuga site (96.3%) compared to the Ruhuha site (84.2%).
Combination haplotypes
Only 46 of 374 (12.2%) samples typed carried both the pfcrt 76K and pfdmr1 86N WT
alleles. Notably, the proportion of double pfcrt 76T and pfdmr1 86Y mutant alleles was
2-fold higher at Ruhuha compared to Mubuga (p = 0.018). The prevalence of the pfdhps
double (437G-540E), pfdhfr triple (108N-51I-59R), and pfdhps/pfdhfr quintuple
haplotypes were 83.7%, 85.0% and 73.7%, respectively (Table 3). The distributions of
the pfdhps double, pfdhfr triple (108N-51I-59R) and the pfdhps / pfdhfr quintuple
polymorphisms were comparable across the two study sites (Table 4). In contrast, a
borderline significant (p = 0.06) higher distribution for the triple pfdhps 437G, 540E and
581G haplotype combination was seen at Ruhuha (25.3%) compared to the Mubuga
(17.6%) site (Table 4). In total, about 18.3% (73 isolates) carried the sextuple (51I, 59R,
108N, 540E, 437G, 581G) mutant, with its occurrence being restricted to the Ruhuha site
(p = 0.005).

63
Discussion
The key findings of this study were a slow emergence of CQ susceptible WT parasites 14
years after CQ withdrawal, sustained high levels of SP resistance marker polymorphisms
7 years after complete SP withdrawal and a decline in prevalence of the high resistance -
associated pfdhps 581G and pfdhfr 164L mutants - with the later mutant found restricted
at the higher malaria transmission intensity Ruhuha site, and a differential distribution in
pfdhfr 164L, pfdhfr 59R and pfcrt 76T mutants between the two study sites.
In Rwanda, CQ was replaced with AQ+SP in 2001 and the later combination was then
used for only five years. No study or report on anti-malaria drug resistance exists neither
before CQ withdrawal (2001) nor after AQ+SP withdrawal (2006) and thus the impact of
AQ on CQ resistance was never estimated. The only reported study (conducted in 2010)
where molecular correlates of CQ are reported is here used as a baseline comparator with
a 74% Pfcrt76T given that both studies were conducted in the same high malaria
transmission zone in Rwanda. In a study conducted in 2010 among under five-year old
children in the high malaria endemic Butare setting, southern Rwanda, a 74% pfcrt 76T -
the principal CQ resistance mediating polymorphism, mutant prevalence was reported
(Zeile et al., 2012). Our study conducted 5 years later showed a 49% pfcrt 76T
prevalence equivalent. Presuming a similar pfcrt 76T resistance levels in high malaria
transmission eastern and southern Rwanda province settings, ~ 25% recovery of WT
pfcrt 76K strains was observed. Recovery of CQ-susceptibility after years of CQ
withdrawal has shown a mixed pattern, both within and between countries. While CQ
recovery rates of >85% have been shown in countries including Tanzania (Mohammed et
al., 2013; Malmberg et al., 2013) and Malawi (Kublin et al., 2003), slower recovery rates
have been reported elsewhere including Kenya (Mwai et al., 2009) and Uganda (Nsobya
et al., 2010; Kamugisha et al., 2012). In our study, the noted CQ recovery occurred in
spite of the large-scale use of AL. AL use has been shown to select for the chloroquine-
susceptible pfcrt K76 allele in two separate studies conducted in Tanzania. (Malmberg et
al., 2013; Sisowath et al., 2009). A number of reasons may contribute to the observed
slow CQ susceptibility recovery including the possible continued use of CQ in spite of
policies to withdraw CQ as has been reported in Uganda, Rwanda and Tanzania (Karema

64
et al., 2010; Frosch et al., 2011; Eriksen et al., 2005) and the continued use of CQ related
antimalarial molecules such as AQ that was report to account for the observed minimal
change from 100% to 97% prevalence of pfcrt 76T mutant over a 4 years after CQ
withdrawal from nation treatment guidelines (Frank et al., 2011; Djimde et al., 2006). AQ
has been shown to strongly select for the resistance conferring pfcrt 76T allele (Djimde et
al., 2006). Other influencers of CQ recovery rates include time since actual CQ drug
withdrawal from use, time since policy to withdrawal for CQ from use, baseline CQ
resistance levels and area malaria transmission intensities.
Polymorphisms in the P. falciparum pfmdr1 gene have been shown mixed sensitivity
responses between different anti-malarial drugs (Rosenthal, 2013). Our study showed
high prevalence of >80% for pfmdr1 WT 86N and 1246D alleles and in consequence, a
75% prevalence for the pfmdr1 86N/1246D/184Y CQ susceptible triple haplotype.
However, only 40% of isolates carried the WT 184Y alleles. Compared to a study done 5
years prior in southern Rwanda where WT allelic prevalence of 61%, 88% and 48% for
pfmdr1 86N, 1246D and 184Y, respectively, with ~ 60% prevalence for the pfmdr1
86N/184Y/1246D wild-type haplotype were reported, our study demonstrated a slow
recovery of WT 86N alleles and the triple pfmdr1 (86N/184Y/1246D) haplotype but not
the 1246Y and 184F mutants whose levels remained relatively stable (Gahutu et al.,
2011). A comparably high 66% prevalence for the pfmdr1 86Y/184F/1246Y mutant
haplotype was reported in 2013 from Kenya (Okombo et al., 2014). This mixed selective
pressure for CQ among alleles at this locus, with recovery reported for some alleles (86N
and 1246D) while for other alleles (184F), mutant levels remained high, has been
reported previously to be partly associated with scaled-up use of AL (Okombo et al.,
2014). Our results are consistent with those from Zanzibar, Burkina Faso, Tanzania
where findings of increased prevalence of pfmdr1 86Y (Sisowath et al., 2005;
Dokomajilar et al., 2006; Humphreys et al., 2007) whilst the pfmdr1 184F has been noted
to come under selection in settings of AL resistance (Vinayak et al., 2010). Analysis of
health facility PCR-confirmed P. falciparum infected samples in Mozambique showed a
mixed temporal trend in the prevalence of WT 86N, 184Y and 1246D alleles: Between
the 2003–2005 and 2010–2012 periods, pfmdr1 86N prevalence rose from 19.5% to

65
73.2%, while 184Y WT allelic prevalence remained fairly stable (from 19.6% to 22.7%).
The WT 1246D alleles marginally increased from 74.4% to 96.7%, in tandem with ACT
use in the 2010-2012 period (Dokomajilar et al., 2006; Lobo et al., 2014). Thus, recovery
to CQ susceptible pfmdr1 alleles shows a variable temporal trend, with AL being a major
influence. It is noteworthy, however, that pfmdr1 86N, 184F, and 1246D alleles have
been selected by treatment with AL raising concerns of a possible alteration to AL drug
sensitivity by these alleles (Baliraine & Rosenthal, 2011).
High levels of >92% for each of pfdhps 437G and 540E mutants and, in consequence, a
84% prevalence of the pfdhps double 437G-540E polymorphisms were observed in this
study. Within Rwanda, these figures accord with prior reported prevalence of 96%, 94%
and about 32% for 437G, 540E and pfdhps double mutants, respectively, in southern
Rwanda in 2010 (Zeile et al., 2012). Within East Africa, our findings accord with
reported pfdhps double mutant prevalences of 97% at Mbeya, Tanzania (Matondo et al.,
2014), 94% at Asembo, Kenya (Shah et al., 2015), 99% at Nyanza, Kenya (Iriemenam et
al., 2012) and a >90% in Tororo, Uganda (Mbogo et al., 2014). In contrast, declines in
pfdhfr and pfdhps resistance imparting polymorphisms after SP withdrawal have been
reported from in a few studies from Ethiopia (Hailemeskel et al, 2013; Tessema et al.,
2015), Tanzania (Gesase et al., 2009; Matondo et al., 2014) and Mozambique (Raman et
al., 2008). Where re-emergence of SP susceptible parasites has been observed, this may
be due to drug-resistant p. falciparum parasite having a competitive disadvantage where
SP drug pressure is absent or reduced. Three reasons may partly account for the observed
sustained high intensity of pfdhps-mediated SP resistance in spite of the reduced or
absent SP selection pressure. Firstly, a high malaria endemicity in the study areas;
secondly, the continued use of Pfdhfr/Pfdhps inhibitors like trimethoprim-
sulfamethoxazole (TS) for the treatment of and prophylaxis against bacterial infections
among HIV infected individuals; and thirdly, the continued use of IPTp-SP especially in
the East and Central African regions. Our findings demonstrate sustained high levels of
SP resistant in Rwanda. It is plausible that SP resistant parasites that continue to be
selected may constitute the infectious reservoir that supplies the high prevalence of
circulating drug resistant alleles.

66
Our study revealed intense levels of 85% of the pfdhfr triple mutants responsible for SP
resistance. This is higher than the 75% pfdhfr triple mutant prevalence reported in
southern Rwanda (Zeile et al., 2012). In 2007-2008, comparably high-level pfdhfr triple
mutant was reported in Rukara, eastern Rwanda (84%) but a much lower prevalence
(49%) was reported at Mashesha, western Rwanda (Karema et al., 2010). These data
show increased pfdhfr triple mutant prevalence in sites in eastern and western Rwanda,
respectively, in spite of the presumed 7 years absence of SP drug pressure. Similar to the
high levels of pfdhps seen in this study, a possible source of pfdhfr mutants may be the
use of TS. P. falciparum in vitro culture studies have demonstrated a TS cross-resistance
with SP that may lead to the development of pfdhfr and pfdhps mutants (Khalil et al.,
2003; Iyer et al., 2001). In our study, 74% of parasites carried the quintuple (pfdhfr triple
and pfdhps double) mutants. Similarly, high levels of the quintuple mutants have been
associated with reduced efficacy of SP-IPTp (Allen et al., 2009). These results compare
to those from Kenya and Uganda where the prevalence of the five pfdhfr and pfdhps
resistance polymorphisms were observed over a > 10 year period of observation in
absence of SP drug pressure conditions (Iriemenam et al., 2012; Mbogo et al., 2014).
However, the appropriateness of these comparison data is complicated by the observation
that in both Uganda and Kenya, unlike in Rwanda, IPT-Sp continues to be used and
hence may be contributing a significantly high SP-related drug pressure”. However in
this study, the low levels of pfdhps 581G (24%) accounted for a lower prevalence of
sextuple mutants (18.3%) compared to the Kenyan and Ugandan studies (Iriemenam et
al., 2012; Mbogo et al., 2014).
The two super-resistance-imparting polymorphism of pfdhfr 164L and pfdhps 581G have
been associated with increased therapeutic failure of SP in south-eastern Africa (Karema
et al., 2010; Lynch et al., 2008; Gesase et al., 2009). In our study, the pfdhps 581G
mutants were found in 24% of isolates typed. Higher prevalence of >50% have been
reported among malaria cases in Northern Tanzania and among HIV infected patients in
Uganda (Gesase et al., 2009; Gasasira et al., 2010). a >50% pfdhps 581G prevalence was
reported (Gesase et al., 2009; Spalding et al., 2010). In Kisumu, Kenya, the levels of
Pfdhps 581G were noted to emerge from 0% to 85% over a 3-5 year period (Spalding et

67
al., 2010) whilst among pregnant women at three sites in Nyanza province, western
Kenya, pfdhps 581G levels increased from 0% to 5.3% between 1996-2000 and 2008-
2009 period (Iriemenam et al., 2012). Similar high levels of >50% Pfdhps 581G
prevalence has also been reported from Eastern Kenya and Northern Tanzania (Spalding
et al., 2010; Gesase et al., 2009). A possible reason for higher 581G levels in Kenya and
Tanzania may be due to continued IPTp-SP use with 581G being associated with
reduction in the effectiveness of SP (Harrington et al. 2009). Also 581G-associated
highly SP-resistant sextuple mutated haplotype is associated with significant reduction in
birth weight of newborns of malaria-infected women presumably by reducing the
effectiveness of IPTp-SP (Minja et al., 2013). When delineated by study area, the 581G
allelic prevalence (26.8%) declined at Ruhuha, eastern Rwanda vs. 60% reported in the
2005-2006 period at Rukara, eastern Rwanda (Karema et al., 2010). In contrast, 581G
allelic prevalence remained comparable for the Mubuga (29%) and Masheshe (21.7%)
sites in western Rwanda between 2015 and 2005-2006 and 2015 periods, respectively
(Karema et al., 2010). We postulate that differences in malaria transmission intensity may
partly account for the differential 581G allelic prevalence and temporal effects in this
study. In this study, the pfdhfr 164L mutants were carried by 5% of isolates: All of which
were from Ruhuha, eastern Rwanda. Similarly, 164L mutants were found restriction to
eastern Rwanda when compared to western Rwanda had been reported from Rwanda
before (Karema et al., 2010). Elsewhere, the 164L mutants have been reported to be
preferentially concentrated in the eastern Africa region, albeit at variable prevalence. A
study in Nyanza, Kenya and another in Fort Portal, Uganda, reported 164L allelic
prevalence of < 1% and 36%, respectively (Lobo et al., 2013; Spalding et al., 2010).
Unlike at Rukara where the 164L pfdhfr mutants occurred only in association with the
pfdhps double or triple mutants; in our study, 164L alleles occurred only in association
with the pfdhps double (100%) but with ~95% (18/19) of alleles concurrently seen
alongside the triple pfdhfr mutant. The overall reduction in prevalence of the pfdhfr 164L
and pfdhfr 581G polymorphisms is probably due to the reduced drug pressure and the
lower fitness of mutant parasites in absence of drug pressure.

68
We also identified variable site-specific genotype differences in distribution for three of
the 14 genotyped alleles. The proportion of pfcrt 76T mutant infection was significantly
(p = 0.026) higher at the lower-endemic Mubuga site (56%) compared to the higher-
endemic Ruhuha site (45%). A number of factors may account for this variability
including differences, in the past and currently, of drug selection pressure on pfcrt 76T
resistant parasites and plausibly, difference in external sources of pfcrt 76T mutants
particularly in settings neighbouring other countries where population of variable
resistance profiles may be interacting extensively. With regard to the pfdhfr 164L mutant
that has been associated with intense SP resistance, all mutants were found exclusively in
the high malaria endemic Ruhuha site. Our findings are consistent with the observed
pattern among sub-Saharan countries and within Rwanda where, again, the pfdhfr 164L
mutants were only present among isolates from the high endemic Ruhuha site in eastern
Rwanda (Karema et al., 2010). Elsewhere, the pfdhfr 164L mutant prevalences have been
reported to vary between low (Braun et al., 2015; Alifrangis et al., 2009) and
concentrated local hotspots in Rwanda and southwest Uganda (Karema et al., 2010;
Lynch et al., 2008). In this study, a significantly higher prevalence of the pfdhfr 59R
mutants was observed at Mubuga, western Rwanda compared to Ruhuha, eastern
Rwanda: Similarly to previous findings of higher prevalence (~84%) of the triple (pfdhfr
108N-51I-59R) mutant haplotype at another site in Eastern Rwanda relative to the
comparator Western Rwanda site (Karema et al., 2010). A possible reason for the
contrasting finding may be differences in possible determinants of continued parasite
population resistance at the four study sites. The Mashesha site in Western Rwanda
borders the Democratic Republic of Congo and Burundi and hence may be more
influenced by drug resistance pressure from across the border due to highly dynamic
human populations, relative to the other sites.
Our study had some limitations. Samples were collected from only two sites located in
the low and high malaria intensities zones where as malaria risk in Rwanda is categorised
into four ecologic zones. Therefore, study results may not be generalizable to all
Rwandan settings. That notwithstanding, our findings provide the most recent accurate
surveillance data for key CQ and SP resistance- mediating polymorphisms at two sites of

69
variable malaria transmission intensities.
Conclusions
Overall, sustained intense levels of SP resistance and a slow recovery of CQ susceptible
parasites were found in our study conducted after 7 years and 14 years of the complete
drug withdrawal from use, respectively. Most likely, the high prevalence of resistant
parasites selected by the continued use of Pfdhfr/Pfdhps inhibitors like TS used in the
treatment of and prophylaxis against bacterial infections among HIV infected individuals
and the continued use of IPTp-SP for malaria prevention among pregnant women. The
slow recovery of CQ susceptive parasites may have been caused partly by the continued
use of CQ and CQ mimicking AQ in spite of policies to withdrawal CQ from use in
Rwanda and neighbouring countries. Interestingly, the prevalence for the two high-level
SP resistance imparting pfdhfr 164L and pfdhps 581G mutants were observed to decline
with the pfdhfr 164L mutant noted to be restricted to the Eastern Rwanda site pointing to
a reducing risk of SP therapeutic failure within Rwanda. Molecular marker distribution
between two study sites, apart from pfcrt 76T, pfdhfr 164L and pfdhfr 59R mutants, did
not vary significantly suggesting the epidemiology of the studies molecular marker may
not vary significantly between sites of different malaria transmission intensities.
Continued surveillance of P. falciparum polymorphisms and characterization of the
determinants of anti-malarial drug sensitivity epidemiology is recommended for guiding
future rational drug policy-making and mitigation of future risk of anti-malaria drug
resistance development.

70
Competing interests
The authors have declared that they have no competing interests.
Authors’ contributions: FK conceived the idea, designed the study, participated in
performance of the experiments, analysed the data and drafted the manuscript. SLN
participated in performing the experiments and revised the manuscript substantially. ST
performed the experiments and revised the manuscript. NK helped in data analysis and
writing and editing of the manuscript. EH, PFM, MPG and MvV contributed to the
writing of the manuscript. KN supported study protocol development, and provided
substantial input into the writing of the manuscript. All authors read and approved the
final version of the manuscript.
Acknowledgments. We thank study participants at both Ruhuha and Mubuga health
centres who provided samples for analysis and the health facility leadership, study
laboratory personnel for supporting study conduct.
Financial support. This work was financially supported by a Fogarty International
Center, National Institutes of Health, Training grant #TW007375. Supplementary support
was received from The Netherlands Organisation for Scientific Research (NWO-
WOTRO) under Grant# AMC A1050243 to the Academic Medical Centre – The
Netherlands.

71
References
1. Alifrangis M, Lusingu JP, Mmbando B, Dalgaard MB, Vestergaard LS, Ishengoma D, et
al. Five- year surveillance of molecular markers of Plasmodium falciparum antimalarial
drug resistance in Korogwe District, Tanzania: accumulation of the 581G mutation in the
P. falciparum dihydropteroate synthase gene. Am J Trop Med Hyg 2009; 80:523–527.
2. Allen EN, Little F, Camba, T, Cassam Y, Raman J, Boulle A, at al. Efficacy of
sulphadoxine-pyrimethamine with or without artesunate for the treatment of
uncomplicated Plasmodium falciparum malaria in southern Mozambique: a randomized
controlled trial. Malar J 2009; 8:141.
3. Ashley EA, Dhorda M, Fairhurst RM, Amaratunga C, Lim P, Suon S, et al. Spread of
artemisinin resistance in P. falciparum malaria. N Engl J Med 2015; 371:411-423.
4. Baliraine FN, Rosenthal PJ. Prolonged Selection of pfmdr1 Polymorphisms After
Treatment of Falciparum Malaria With Artemether-Lumefantrine in Uganda. J Infect Dis
2011; 204 (7): 1120-1124.
5. Braun V, Rempis E, Schnack A, Decker S, Rubaihayo J, Tumwesigye NM, et al. Lack of
effect of intermittent preventive treatment for malaria in pregnancy and intense drug
resistance in western Uganda. Malar J 2015; 14:372
6. Djimde AA, Fofana B, Sagara I, Sidibe B, Toure S, Dembele D, et al. Efficacy, safety,
and selection of molecular markers of drug resistance by two ACTs in Mali. Am J Trop
Med Hyg 2008; 78: 455-461.
7. Dokomajilar C, Nsobya SL, Greenhouse B, Rosenthal PJ, Dorsey G. Selection of
Plasmodium falciparum pfmdr1 alleles following therapy with artemether–lumefantrine
in an area of Uganda where malaria is highly endemic. Antimicrob Agents Chemother.
2006; 50:1893–1895.
8. Dondorp AM, Nosten F, Yi P, Das D, Phyo AP, Tarning J, et al. Artemisinin resistance in
Plasmodium falciparum malaria. N Engl J Med 2009; 361: 455-467.
9. Ecker A, Lehane AM, Clain J, Fidock, DA. pfcrt and its role in anti- malarial drug
resistance. Trends Parasitol 2012; 28:504–514.
10. Enosse S, Magnussen P, Abacassamo F, Gómez-Olivé X, Rønn AM, Thompson R, et al.
Rapid increase of Plasmodium falciparum dhfr/dhps resistant haplotypes, after the

72
adoption of sulphadoxine-pyrimethamine as first line treatment in 2002, in southern
Mozambique. Malar J 2008; 7:115.
11. Eriksen J, Nsimba SE, Minzi OM, Sanga AJ, Petzold M, Gustafsson LL, et al. Adoption
of the new antimalarial drug policy in Tanzania–a cross-sectional study in the
community. Trop Med Int Health 2005; 10:1038–1046.
12. Frank M, Lehners N, Mayengue PI, Gabor J, Dal-Bianco M, Kombila DU, et al. A
thirteen-year analysis of Plasmodium falciparum populations reveals high conservation of
the mutant pfcrt haplotype despite the withdrawal of chloroquine from national treatment
guidelines in Gabon. Malaria J 2011; 10: 304.
13. Frosch AE, Venkatesan M, Laufer MK. Patterns of chloroquine use and resistance in sub-
Saharan Africa: a systematic review of household survey and molecular data. Malar J
2011; 10:116.
14. Gahutu JB, Steininger C, Shyirambere C, Zeile I, Cwinya-Ay N, Danquah I, et al.
Prevalence and risk factors of malaria among children in southern highland Rwanda.
Malar J 2011; 10:134.
15. Gasasira AF, Kamya MR, Ochong EO, Vora N, Achan J, Charlebois E, et al. Effect of
trimethoprim- sulphamethoxazole on the risk of malaria in HIV-infected Ugandan
children living in an area of widespread antifolate resistance. Malar J 2010; 9:177.
16. Gesase S, Gosling RD, Hashim R, Ord R, Naidoo I, Madebe R, et al. High resistance of
Plasmodium falciparum to sulphadoxine/pyrimethamine in northern Tanzania and the
emergence of dhps resistance mutation at Codon 581. PLoS One 2009; 4(2): e4569.
17. Hailemeskel E, Kassa M, Taddesse G, Mohammed H, Woyessa A, Tasew G, et al.
Prevalence of sulfadoxine-pyrimethamine resistance-associated mutations in dhfr and
dhps genes of Plasmodium falciparum three years after SP withdrawal in Bahir Dar,
Northwest Ethiopia. Acta Trop 2013; 128:636–641.
18. Harinasuta T, Suntharasamai P, Viravan C. Chloroquine-resistant falciparum malaria in
Thailand. Lancet 1965; 2:657-660.
19. Harrington WE, Mutabingwa TK, Muehlenbachs A, Sorensen B, Bolla MC, Fried M, et
al. Competitive facilitation of drug-resistant Plasmodium falciparum malaria parasites in
pregnant women who receive preventive treatment. Proc Natl Acad Sci 2009; 106: 9027–
9032

73
20. Hastings MD, Bates SJ, Blackstone EA, Monks SM, Mutabingwa TK, Sibley CH. Highly
Pyrimethamine-resistant alleles of dihydrofolate reductase in isolates of Plasmodium
falciparum from Tanzania. Trans R Soc Trop Med Hyg 2002; 96(6): 674-676.
21. Humphreys GS, Merinopoulos I, Ahmed J, Whitty CJ, Mutabingwa TK, Sutherland CJ,
et al. Amodiaquine and artemether– lumefantrine select distinct alleles of the
Plasmodium falciparum mdr1 gene in Tanzanian children treated for uncomplicated
malaria. Antimicrob Agents Chemother 2007; 51:991–997.
22. Iriemenam NC, Shah M, Gatei W, van Eijk AM, Ayisi J, Kariuki S, et al. Temporal
trends of sulphadoxine-pyrimethamine (SP) drug-resistance molecular markers in
Plasmodium falciparum parasites from pregnant women in western Kenya. Malar J 2012;
11:134.
23. Iyer JK, Milhous WK, Cortese JF, Kublin JG, Plowe CV. Plasmodium falciparum cross-
resistance between trimethoprim and pyrimethamine. The Lancet 2001; 358:1066-1067.
24. Kain KC, Lanar DE. Determination of genetic variation within P. falciparum by using
enzymatically amplified DNA from filter paper disks impregnated with whole blood. J
Clin Microbiol 1991; 29:1171-1174.
25. Kamugisha E, Bujila I, Lahdo M, Pello-Esso S, Minde M, et al. Large differences in
prevalence of Pfcrt and Pfmdr1 mutations between Mwanza, Tanzania and Iganga,
Uganda-a reflection of differences in policies regarding withdrawal of chloroquine? Acta
Trop 2012; 121:148–151.
26. Karema C, Aregawi MW, Rukundo A, Kabayiza A, Mulindahabi M, Fall IS, et al. Trends
in malaria cases, hospital admissions and deaths following scale-up of anti-malarial
interventions, 2000-2010, Rwanda. Malar J 2012; 11:236.
27. Karema C, Imwong M, Fanello CI, Stepniewska K, Uwimana A, Nakeesathit S, et al.
Molecular Correlates of High-Level Antifolate Resistance in Rwandan Children with
Plasmodium falciparum Malaria. Antimicrob Agents Chemother. 2010; 54: 477–483.
28. Khalil I, Ronn AM, Alifrangis M, Gabar HA, Satti GM, Bygbjerg IC. Dihydrofolate
reductase and dihydropteroate synthase genotypes associated with in vitro resistance of
Plasmodium falciparum to pyrimethamine, trimethoprim, sulfadoxine, and
sulfamethoxazole. Am J Trop Med Hyg 2003; 68:586-589.

74
29. Koenderink JB, Kavishe RA, Rijpma SR, Russel FG. The ABCs of multidrug resistance
in malaria. Trends Parasitol 2010; 26:440–446.
30. Kublin JG, Cortese JF, Njunju EM, Mukadam RA, Wirima JJ, et al. Reemergence of
chloroquine- sensitive Plasmodium falciparum malaria after cessation of chloroquine use
in Malawi. J Infect Dis 2003; 187:1870–1875.
31. Kublin JG, Dzinjalamala FK, Kamwendo DD, Malkin EM, Cortese JF, Martino LM, et
al. Molecular markers for failure of sulfadoxine- pyrimethamine and chlorproguanil-
dapsone treatment of Plasmodium falciparum malaria. J Infect Dis 2002; 185(3): 380-
388.
32. Laufer MK, Thesing PC, Eddington ND, Masonga R, Dzinjalamala FK, Takala SL, et al.
Return of chloroquine antimalarial efficacy in Malawi. N Engl J Med 2006; 355:1959–
1966.
33. LeClair NP, Conrad MD, Baliraine FN, Nsanzabana C, Nsobya SL, Rosenthal PJ.
Optimization of a ligase detection reaction-fluorescent microsphere assay for
characterization of resistance-mediating polymorphisms in African samples of
plasmodium falciparum. J Clin Microbiol 2013; 51:2564–2570.
34. Lobo E, de Sousa B, Rosa S, Figueiredo P, Lobo L, Pateira S, et al. Prevalence of
pfmdr1 alleles associated with artemether-lumefantrine tolerance/resistance in Maputo
before and after the implementation of artemisinin-based combination therapy. Malar J
2014; 13: 300.
35. Lynch C, Pearce R, Pota H, Cox J, Abeku TA, Rwakimari J, et al. Emergence of a dhfr
mutation conferring high-level drug resistance in Plasmodium falciparum populations
from southwest Uganda. J Infect Dis 2008; 197:1598–1604.
36. Malmberg M, Ngasala B, Ferreira PE, Larsson E, Jovel I, Hjalmarsson A, et al. Temporal
trends of molecular markers associated with artemether-lumefantrine tolerance/ resistance
in Bagamoyo district, Tanzania. Malar J 2013; 12:103.
37. Matondo SI, Temba GS, Kavishe AA, Kauki JS, Kalinga A, van Zwetselaar M, et al.
High levels of sulphadoxine-pyrimethamine resistance Pfdhfr-Pfdhps quintuple
mutations: a cross sectional survey of six regions in Tanzania. Malar J 2014; 13: 152.

75
38. Minja D, Schmiegelow C, Mmbando B, Boström S, Oesterholt M, Magistrado P, et al.
Plasmodium falciparum Mutant Haplotype Infection during Pregnancy Associated with
Reduced Birthweight, Tanzania. Emerg Infect Dis 2013; 19(9): 1446–1454.
39. Mbogo GW, Nankoberanyi S, Tukwasibwe S, Baliraine FN, Nsobya SL, Conrad MD, et
al. Temporal Changes in Prevalence of Molecular Markers Mediating Antimalarial Drug
Resistance in a High Malaria Transmission Setting in Uganda. Am J Trop Med Hyg
2014; 91(1): 54-61.
40. Mohammed A, Ndaro A, Kalinga A, Manjurano A, Mosha JF, Mosha DF, et al. Trends in
chloroquine resistance marker, Pfcrt-K76T mutation ten years after chloroquine
withdrawal in Tanzania. Malar J 2013; 12:415.
41. Mwai L, Ochong E, Abdirahman A, Kiara SM, Ward S, Kokwaro G, et al. Chloroquine
resistance before and after its withdrawal in Kenya. Malar J 2009; 8:106.
42. Ndiaye M, Faye B, Tine R, Ndiaye JL, Lo A, Abiola A, et al. Assessment of the
Molecular Marker of Plasmodium falciparum Chloroquine Resistance (Pfcrt) in Senegal
after Several Years of Chloroquine Withdrawal. Am J Trop Med Hyg 2012; 87(4): 640–
645.
43. Nsobya SL, Kiggundu M, Nanyunja S, Joloba M, Greenhouse B, Rosenthal PJ. In vitro
sensitivities of Plasmodium falciparum to different antimalarial drugs in Uganda.
Antimicrob Agents Chemother 2010; 54:1200–1206.
44. Okombo J, Kamau AW, Marsh K, Sutherland CJ, Ochola-Oyier LI. Temporal trends in
prevalence of Plasmodium falciparum drug resistance alleles over two decades of
changing antimalarial policy in coastal Kenya. Int J Parasitol Drugs Drug Resist 2014; 4
(3): 152–163.
45. Ord R, Alexander N, Dunyo S, Hallett R, Jawara M, Targett G, et al. Seasonal carriage of
pfcrt and pfmdr1 alleles in Gambian Plasmodium falciparum imply reduced fitness of
chloroquine-resistant parasites. J Infect Dis 2007; 196:1613–1619.
46. Pearce RJ, Pota H, Evehe MS, Bâ el-H, Mombo-Ngoma G, Malisa AL, et al. Multiple
origins and regional dispersal of resistant dhps in African Plasmodium falciparum
malaria. PLoS Med 2009; 6(4):e1000055.

76
47. PMI/MOH-Rwanda. President’s Malaria Initiative Rwanda Malaria Operational Plan FY
2015. http://www.pmi.gov/docs/default-source/default-document-library/malaria-
operational-plans/fy-15/fy-2015-rwanda-malaria-operational-plan.pdf?sfvrsn=3.
48. Raman J, Sharp B, Kleinschmidt I, Roper C, Streat E, Kelly V, et al. Differential effect of
regional drug pressure on dihydrofolate reductase and dihydropteroate synthetase
mutations in southern Mozambique. Am J Trop Med Hyg 2008; 78:256–261.
49. Rosenthal PJ. The interplay between drug resistance and fitness in malaria parasites. Mol
Microbiol. 2013; 89:1025–1038.
50. Shah M, Omosun Y, Lal A, Lal A, Odero C, Gatei W, Otieno K, et al. Assessment of
molecular markers for anti-malarial drug resistance after the introduction and scale-up of
malaria control interventions in western Kenya. Malar J 2015; 14:75.
51. Sisowath C, Petersen I, Veiga MI, Mårtensson A, Premji Z, Björkman A, et al. In vivo
selection of Plasmodium falciparum parasites carrying the chloroquine-susceptible pfcrt
K76 allele after treatment with artemether-lumefantrine in Africa. J Infect Dis 2009;
199(5): 750-757.
52. Sisowath C, Stromberg J, Martensson A, Msellem M, Obondo C, Bjorkman A, et al. In
vivo selection of Plasmodium falciparum pfmdr1 86N coding alleles by artemether–
lumefantrine (Coartem). J Infect Dis 2005; 191:1014–1017.
53. Spalding MD, Eyase FL, Akala HM, Bedno SA, Prigge ST, Coldren RL, et al. Increased
prevalence of the pfdhfr/phdhps quintuple mutant and rapid emergence of pfdhps
resistance mutations at codons 581 and 613 in Kisumu, Kenya. Malar J 2010; 9:338.
54. Tessema SK, Kassa M, Kebede A, Mohammed H, Leta GT, Woyessa A et al. Declining
trend of Plasmodium falciparum dihydrofolate reductase (dhfr) and dihydropteroate
synthase (dhps) mutant alleles after the withdrawal of Sulfadoxine-Pyrimethamine in
North Western Ethiopia. PLoS ONE 2015; 10(10): e0126943.
55. Vinayak S, Alam MT, Sem R, Shah NK, Susanti AI, Lim P, et al. Multiple genetic
backgrounds of the amplified Plasmodium falciparum multidrug resistance (pfmdr1) gene
and selective sweep of 184F mutation in Cambodia. J Infect Dis 2010; 201:1551–1560.
56. White NJ. Antimalarial drug resistance and combination chemotherapy. Philos Trans R
Soc Lond B Biol Sci. 1999; 354:739–749.
57. World Health Organization, World Malaria Report 2015. Available at:

77
http://apps.who.int/iris/bitstream/10665/200018/1/9789241565158_eng.pdf. Accessed
January 13th 2016.
58. Young MD, Moore DV. Chloroquine resistance in Plasmodium falciparum. Am J Trop
Med Hyg 1961; 10:317-320.
59. Zeile I, Gahutu JB, Shyirambere C, Steininger C, Musemakweri A, Sebahungu F, et al.
Molecular markers of Plasmodium falciparum drug resistance in southern highland
Rwanda. Acta Tropica 2012; 121:50–54.

78
CHAPTER 4
Malaria parasite carriage and risk determinants in a rural population:
a malariometric survey in Rwanda
Fredrick Kateera1,2, Petra F. Mens2,3, Emmanuel Hakizimana1,4, Chantal M.
Ingabire1, Liberata Muragijemariya5, Parfait Karinda1, Martin P
Grobusch2, Leon Mutesa6, Michèle van Vugt2
1Medical Research Centre Division, Rwanda Biomedical Centre, Kigali, Rwanda, 2Division of Internal Medicine, Department of Infectious Diseases, Centre of Tropical
Medicine and Travel Medicine, Academic Medical Centre, Meibergdreef 9, Amsterdam,
1100 DE, The Netherlands, 3Royal Tropical Institute/Koninklijk Instituut voor de Tropen, KIT Biomedical Research,
Meibergdreef 39, Amsterdam, 1105 AZ, The Netherlands, 3Malaria and Other Parasitic Diseases Division, Rwanda Biomedical Centre, Kigali,
Rwanda, 4Department of Cultural Anthropology and Development Studies and Centre for
International Development Issues, Radboud University, Nijmegen, 6500 HE, The
Netherlands, 5Ruhuha Health Centre, Ruhuha Sector, Bugesera, Rwanda 6College of Medicine and Health Sciences, University of Rwanda, Kigali, Rwanda,
Published in: Malaria Journal 2015; 21:14:16.

79
Abstract
Background
Based on routine health facility case data, Rwanda has achieved a significant malaria
burden reduction in the past ten years. However, community-based malaria parasitaemia
burden and reasons for continued residual infections, despite a high coverage of control
interventions, have yet to be characterized. Measurement of malaria parasitaemia rates
and evaluation of associated risk factors among asymptomatic household members in a
rural community in Rwanda were conducted.
Methods
A malariometric household survey was conducted between June and November 2013,
involving 12,965 persons living in 3,989 households located in 35 villages in a sector in
eastern Rwanda. Screening for malaria parasite carriage and collection of demographic,
socio-economic, house structural features, and prior fever management data, were
performed. Logistic regression models with adjustment for within- and between-
households clustering were used to assess malaria parasitaemia risk determinants.
Results
Overall, malaria parasitaemia was found in 652 (5%) individuals, with 518 (13%) of
households having at least one parasitaemic member. High malaria parasite carriage risk
was associated with being male, child or adolescent (age group 4–15), reported history of
fever and living in a household with multiple occupants. A malaria parasite carriage risk-
protective effect was associated with living in households of, higher socio-economic
status, where the head of household was educated and where the house floor or walls
were made of cement/bricks rather than mud/earth/wood materials. Parasitaemia cases
were found to significantly cluster in the Gikundamvura area that neighbours marshlands.
Conclusion
Overall, Ruhuha Sector can be classified as hypo-endemic, albeit with a particular ‘cell of

80
villages’ posing a higher risk for malaria parasitaemia than others. Efforts to further
reduce transmission and eventually eliminate malaria locally should focus on investments
in programmes that improve house structure features (that limit indoor malaria
transmission), making insecticide-treated bed nets and indoor residual spraying
implementation more effective.

81
Background
Significant decline in malaria burden, attributed to scale-up of interventions including
indoor residual spraying (IRS), insecticide-treated bed nets (predominantly long-lasting
insecticide-treated net (LLIN) type) and use of artemisinin combination therapy (ACT)
after confirmed diagnosis with microscopy or rapid diagnostic tests (RDTs), have been
widely reported in multiple malaria-endemic countries, including Rwanda, during the last
decade [1,2].
Following these gains, a new ‘Rwanda malaria control strategic plan 2013-2018’, aiming
at achieving malaria pre-elimination status, with near-zero deaths from malaria and a
slide positivity rate less than 5% among fever cases by 2018, is being finalized [3]. This
change in strategy from successful individual case treatment (with a focus on reducing
health facility-identified malaria cases) to improved large-scale control, reducing
transmission (by increasingly targeting community-based, asymptomatic parasitaemic
individuals and foci of infection) will require higher coverage and optimal use of
implemented control measures and generation of area-specific, timely and accurate data
to inform targeted control decisions [4]. For Rwanda, reported data stem from health
facilities (HFs) that routinely monitor and report slide positivity rates (SPRs) that are
important for surveillance [2,5]. These data are, however, representative of symptomatic
cases captured by the health care system but not the total burden of malaria parasitaemic
individuals, a significant proportion of whom are asymptomatic individuals in
communities who are believed to be the reservoir pool for continued malaria transmission
[6,7].
The epidemiology of asymptomatic malaria in the population (reservoir) is relevant
information needed by control programmes to reduce both overall and area-specific
malaria transmission, as well as to mitigate the effect of local malaria-transmission, foci-
associated, risk factors. Currently, a major source of data on population level
asymptomatic malaria parasitaemia is the nationally representative demographic and
health surveys (DHSs) conducted every five years, which primary aim is to provide data

82
for a wide range of monitoring and impact evaluation indicators in population, health,
and nutrition issues [8]. However, because of the large coverage, DHSs are not powered
to facilitate an accurate assessment of malaria reservoirs (asymptomatic-carrying,
parasitaemic persons in a population in a given area) or to identify risk determinants of
community-based, residual, malaria parasitaemia. The World Health Organization
recommends field surveys that characterize baseline malaria transmission epidemiology
with the aim of identifying Plasmodium spp. carriers and at-risk populations to inform
targeted control for optimal impact [9]. Up to now, no study has been published on
understanding malaria reservoirs and associated risk determinants in Rwanda.
As Rwanda embraces a transition towards achieving malaria pre-elimination status, it
becomes very important to know the specific local determinants that predict parasite
carriage. This paper describes a community-based, malariometric survey to measure
baseline parasite carriage rates and to study associated risk factors of residual malaria
parasitaemia in order to optimize malaria control interventions targeted to specific local
needs.
Methods
Study site and population
Geopolitically, Rwanda is divided into provinces, districts, sectors, cells, and villages
with district being the basic political administrative unit. This study was conducted in 35
villages located in five cells that constitute Ruhuha Sector (Figure 1), a rural, agricultural,
traditionally high malaria transmission setting in eastern Rwanda. The area experiences
two high malaria transmission peaks associated with rainy seasons observed generally
from October to November and March to May. The reported total sector population was
21,606 individuals living in 5,100 households (Ananie Sibomana, pers. comm.). Study
eligibility criteria included: 1) having spent the night prior to the interview in a studied
household (HH); 2) aged ≥ six months; and, 3) provision of informed consent.

83
Figure 1: Map showing five cells that constitute Ruhuha Sector and the sector (red circle) location in Bugesera District (grey polygon) in Eastern Province, Rwanda.
Study design and selection of study participants
To provide baseline assessment of local malaria transmission and informed decision-
making on follow-up interventions, a sector-wide, HH-based, cross-sectional survey was
conducted between June and November 2013 (rainy season was late August to
November). In summary, the night prior to the survey, a designated village area
community health care worker (CHW) identified HHs to be visited from an enumeration
list and proceeded to request the head of household (HoH) (a self-reported principal
responsible adult ≥18 years) and HH members to stay at home at the appointed survey
date if possible. The survey consisted of two parts: a questionnaire administered to the
HoH and a laboratory survey in which all HH members were asked to participate. On the
survey day, the study team members, including a laboratory technician and an interviewer
(in company of the CHW) visited the prior-notified HH and proceeded to administer the
questionnaire and perform all study clinical evaluations (see Laboratory methods) after
the HoH had provided written consent. Where no member was found present in an HH, a
return visit was scheduled in the next seven days to optimize study enrolment; in case the

84
survey was not conducted on this follow-up visit, the HH was omitted from study
enrolment.
Questionnaire and interviews
An interviewer-administered questionnaire was held with the HoH. Information on
demographics (sex, age, literacy, occupation, religion, and marital status); malaria
prevention measures ((LLIN ownership, (number and use, and IRS history); HH
structural features (type of wall, floor and roof); prior fever management practices and
socio-economic status indicators (HH utilities like water source for domestic use, lighting
and cooking) was collected. The questionnaire, written in English language, was field-
tested at three sites to ensure consistency and comprehension. Field workers were trained,
across all subject areas and related questions, to administer the interviews in the local
dialect (Kinyarwanda). Questionnaire data were collected in electronic form using Open
Data Kit (ODK) Collect setup [10]. ODK is an open-source suite of tools that include
ODK Collect, an android-based mobile client that acts as the interface between the user
and the underlying form used to collect data [10]. The collected data were then
electronically loaded onto a central server.
Laboratory methods
Study participants were asked to provide a finger-prick blood sample for malaria
diagnosis. A thick blood smear was prepared, dried and stained with 2% Giemsa
immediately in the field and later. Light microscopy was performed at Ruhuha Health
Centre (RHC). Two trained technicians independently examined all blood smears and a
third reader was used in the event of any discordant readings between the two readers.
Experienced microscopists at the National Reference Laboratory in Kigali performed
quality control for all positive slides and 5% of all negative smears. Asexual stage
parasites were counted per 200 white blood cells (WBC). A blood smear was considered
positive in the presence of any asexual parasites and negative if examination of 100 high-
power fields did not reveal any asexual parasites. Field laboratory data were collected and
transcribed directly into hard-copy field laboratory registers and later entered into
Microsoft Access software.

85
Statistical analysis
Laboratory and questionnaire data were merged and entered into STATA version 12.1
(STATA Corp., College Station, TX, USA) for analysis. Data analysis was conducted in
two parts: at HH and individual level to ensure adjusting for within- and between-HH
correlations. Univariate logistic regression was used to assess the effect of predictor
variables on the primary outcome. All variables with possible malaria risk association (p
<0.15) were included in subsequent adjusted multivariate logistic regression models. At
individual level, a random effects model was used to adjust for within- and between-HH
clustering, allowing for a reduced weighting for each subsequent malaria-parasitaemic
individual recorded from a HH after the index cases. At HH level, a stepwise backwards-
elimination approach was used in the multivariate logistics regression model to exclude
any variable with no significant effect. At both levels, malaria risk statistical significance
was considered for any variable with an effect associated with a p-value >0.05. Wald
tests were used to analyse the effect of included variable in the model on the primary
outcome. The dependent variables were: 1) malaria parasitaemia per individual - the
presence of any asexual parasites in the blood smear examined by light microscopy; and,
2) malaria parasitaemia per HH, defined as the presence of asexual malaria parasites
detected on a thick peripheral blood smear for at least one HH member. Independent
study variables included individual and HH demographic data (age, sex, religion, marital
status, area of residence), socio-economic indicator variables (see section below),
reported knowledge on malaria prevention practices (including availability and use of
LLINs, HH use of IRS as well as reported prior fever management experiences), and
household structural features, including type of roof, floor and wall material.
Household socio-economic status (SES)
In total, nine SES indicator variables (Table 1) were used to generate a SES score for
each HH by principal component analysis (PCA) as described elsewhere [11]. The PCA
output was taken as a weight for each variable and the sum of the weights for each HH
taken as the dependent variable household’s SES score. The scores were then ranked in
terciles with the highest 33% of HHs considered high SES, the lowest 33% as low SES
and the rest as middle SES [12].

86
Table 1 Baseline demographic, household and malaria control characteristics Demographics n % Household economic variables indicators n %
HoH level of education Does HoH belong to an economic group?None 1,414 (35.63) No 1,807 45.53
Primary 2,056 51.80 Yes 2,162 54.47Secondary 374 9.42 Does HoH have health insurance?
Tertiary 125 3.15 No 1,337 33.69HoH religion Yes 2,632 66.31
Catholic 1,440 36.28 Has HH saved any money in last 3 months?Protestant 1,330 33.51 No 3,163 79.7Moslem 72 1.81 Yes 806 20.3SDA 806 20.32 Does HH own current house of residence?JHW 43 1.08 No 698 17.6No religion 251 6.32 Yes 3,271 82.4Others 27 0.68 Source of water for domestic use
HoH marital status Open (well, lake) 1,624 40.9Never married 444 11.89 Closed (piped water) 2,345 59.1Married 1,663 41.89 Type of material house wall is made ofLiving together 886 22.32 Mud/wood 1,171 29.5Separate/Divorced 255 6.42 Cement/bricks 2,798 70.5
Widow/widower 717 18.08 Type of material house floor is made ofHoH main occupation Earth/clay/dung 3,136 79
Farmer 3,073 77.43 Bricks/cement 833 21Public office 171 4.31 HH source of power for cookingSelf employed 326 8.21 Firewood/straw 3,787 95.4Private officer 170 4.28 Electricity/charcoal 182 4.6Student 31 0.78 HH source of power for lightingUnemployed 92 2.32 Kerosene/candles/firewood/touches 3,385 85.3Others 106 2.67 Electricity 584 14.7
HH wealth and occupancyAny birth in HH in last 5 years? Malaria control variables
No 1,792 45.15 HH bed net ownership of at least 1 netYes 2,177 54.85 No 282 7.11
Number of persons in HH Yes 3,687 92.891-3 1,493 37.62 IRS done in last 6 months?4-5 1,454 36.63 No 217 5.476-7 757 19.07 Yes 3,752 94.538+ 265 6.68
SES scoreLow 1150 33.4 Household with at least 1 case of malaria 518 13.05Medium 1147 33.3 Household without any malaria carriers 3,450 86.95High 1146 33.3

87
Study consent and ethical approval
Written informed consent was obtained from the HoH and assent from all HH members
aged ≥12 years. Study protocols received ethical and scientific approved by the National
Health Research Committee (NHRC) and the Rwanda National Ethics Committee (No
384/RNEC/2012), Kigali, Rwanda.
Results
Study population: In total, 4705 households occupied by 19,925 individuals were
surveyed. In the final analysis, only data from 12,965 (65%) eligible individuals (3,968
households), who had complete questionnaire and laboratory data on all covariates, were
included. A flow chart of the survey process and selection of participants is detailed in
Figure 2. A greater proportion of study participants were female (53.5%) and the age
distribution was 15.1, 32.58 and 52.31% for age groups six to 59 months, five to 15 years
and ≥16 years, respectively (Table 2).
Figure 2: Flow chart of study household/participant enrolment and malaria screening.

88
Table 2: Univariate and multivariate regression analysis of individual risk factors
for malaria slide positivity
Variable N = 12,965 n (%) Univariate analysis, OR(95% CI), P value
Multivariate analysisOR (95% CI), P value
Malaria infection (positive) 652 (5.03) -- --Gender
Female 7,567 (58.36) 1 1Male 5,398 (41.64) 1.409 (1.191-1.667), 1.201 (1.009-1.428), 0.039
Age group0-4 2,199 (16.96) 15-15 4,431 (34.18) 1.905 (1.514-2.397), 1.938 (1.541-2.438), <0.000116+ 6,335 (48.86) 0.359 (0.275-0.468), 0.384 (0.294-0.503), <0.0001
Fever in last 6 monthsNo 4,838 (37.32) 1 1Yes 8,127 (62.68) 1.464 (1.209-1.773), 1.306 (1.072-1.590), 0.008
HH wall typesBricks/cement 3,780 (29.16) 1 11
Wood/mud 9,185 (70.84) 0.550 (0.458-0.661), 0.001 0.543 (0.442-0.668), <0.0001HH roof type
Wooden poles 24 (0.19) 1 1Tiles/Iron sheets 12,941 (99.81) 0.558 (0.037-0.933, 0.04 0.239 (0.053-1.074), 0.062
HH floor typeClay/Earth/Dung 10,301 (79.45) 1 1Cement/bricks 2,664 (20.55) 0.384 (0.289-0.511), 0.529 (0.389-0.719), <0.0001
Wealth indexLow 3,608 (27.83) 1Medium 6,672 (51.46) 0.618 (0.509-0.751), 0.726 (0.592-0.890), 0.005High 2,685 (20.71) 0.479 (0.3760-0.610), 0.599 (0.451-0.797), 0.002
Residential cellBiharwe 2,249 (17.35) 1
Gatanga 2,822 (21.77) 0.920 (0.678-1.250), 0.595 1.016 (0.741-1.392), 0.923Gikundamvura 2,565 (19.78) 1.883 (1.418-2.504), 2.432 (1.797-3.293), <0.0001
Kindama 3,341 (25.77) 1.023 (0.977-1.304), 0.876 1.487 (1.091-2.025), 0.012Ruhuha 1,988 (15.33) 0.631 (0.440-0.905), 0.012 0.957 (0.650-1.408), 0.822Malaria control tools usedIRS done in HH
No 217 (5.47) 1Yes 3,752 (94.53) 1.150 (0.729-1.815), 0.549
Own ≥1 LLIN in HH No 282 (7.11) 1Yes 3,687 (92.89) 1.144 (0.761-1.722), 0.517

89
Malaria prevalence, control intervention coverage and fever management
Overall, individual Plasmodium parasite carriage prevalence was 5.03% (95% CI 4.65-
5.41%). At HH level, 518 HHs (prevalence of 13% (95% CI 12.01-14.10%) had at least
one member with malaria parasitaemia. HH ownership of ≥ one LLIN was 92.9% (95%
CI 92.193.7%) and the proportion of HHs where IRS had been conducted within
12 months prior to survey was 94.5% (95% CI 93.8-95.2%). In 2,254 (56.8%) HHs, at
least one member was reported to have had fever in the previous six months and in 1,277
(32.2%) of these HHs, fever was reported to have occurred in the four weeks prior to the
survey date. Of the reported fever cases, 1,654 (41.67%) were treated in the government
health care system, 449 (11.31%) purchased drugs from the pharmacy, while 151 (3.8%)
used either local medicinal herbs or home-based, malaria medications from previous
episodes.
Univariate analysis
Individual risk factor analysis
Results of the univariate analysis (with adjustment for within- and between-household
clustering) are shown in Table 2. Sex (males had 1.4-fold increase in odds), age groups
(with age-groups five to 15 years and ≥16 having 1.9 and about 0.4 times more risk than
children aged six to 59 months, respectively) and a reported history of fever during the
previous six months (1.46-fold higher odds of parasitaemia) showed a significant risk
effect. Significantly higher malaria risk was also associated with SES-related variables.
House structural features had significant effect on malaria risk. Living in houses with
cement/brick walls had a reduced risk (odds ratio: 0.55) odds of parasitaemia compared
to wood/mud-walled houses. Living in houses roofed with tiles/iron sheets versus
straw/wooden planks/tent roofs was associated with a reduced risk (odds ratio: 0.56) of
parasitaemia and living in houses with cement/bricks floors versus clay/mud/dung floors
was associated with a reduced (odds ratio: 0.38) risk of parasitaemia.

90
Household risk factor analysis
Results of the univariate analysis for HH level risk determinants are shown in Table 3. In
summary, the risk of finding parasitaemia at HH was significantly higher with increasing
number of HH occupants. However, the risks were lower in HHs where the HoH had any
level of education (OR = 0.777 (95% CI 0.634-0.952), was able to save some money in
the previous three months (OR = 0.675, 95% CI 0.524-0.869), had any form of health
insurance (OR = 0.759 (95% CI 0.628-0.919), and where the HH had parameter values
associated with a medium and high SES class.

91
Table 3: Baseline household characteristics, univariate and multivariate analysis
Univariate analysis
OR (95% CI), P value
Multivariate analysis
OR (95% CI), P value
Household demographics
HoH education level
None 1
Primary - Tertiary 0.777 (0.634-0.952), 0.015 0.810 (0.655-0.999), 0.05
Occupation
Farmer 1
Public office 0.829 (0.425-1.617), 0.582 1.287 (0.634-2.609), 0.485
Self employed 0.581 (0.381-0.888), 0.012 0.789 (0.506-1.231), 0.297
Private officer 0.467 (0.168-1.296), 0.144 0.667 (0.233-1.908), 0.45
Student 1.890 (0.754-4.737), 0.174 3.076 (1.121-8.436), 0.029
Unemployed 0.756 (0.376-1.522), 0.434 0.85 (0.411-1.756), 0.66
Others 0.713 (0.305-1.671), 0.437 0.740 (0.309-1.774), 0.5
Number of persons in HH
1-3 1 1
4-5 2.555 (1.976-3.303), <0.0001 2.504 (1.895-3.309), <0.0001
6 + 4.102 (3.167-5.314), <0.0001 4.911 (3.702-6.517), <0.0001
Household structure features
Type of house wall material
Mud/wood 1 1
Cement/bricks 0.622 (0.513-0.753), <0.0001 0.706 (0.567-0.878), 0.002
Type of house floor material
Earth/clay/dung 1 1
Bricks/cement 0.381 (0.283-0.513), <0.0001 0.640 (0.435-0.941), 0.023
HH source of power for lighting
Kerosene/firewood/touches 1 1
Electricity 0.194 (0.122-0.310), <0.0001 0.258 (0.142-0.466), <0.0001

92
Multivariate analysis
Individual level predictors
In the multivariate analysis (Table 2), significant malaria parasitaemia risk factors that
remained were sex (male associated with a OR = 1.2), age group (with five to 15 year
olds having a 1.94-fold increase while individuals of age group ≥16 year had a reduced
risk (OR = 0.38), a reported history of fever and study participant residential cell. As in
HH level predictors, parameters HH floor, roof and wall material types, values associated
with medium and high SES levels, were associated with significantly lower odds of
parasitaemia (Table 2).
Household level predictors
In the multivariate model (Table 3), significant HH level malaria risk effect was
associated with HoH reported education level, occupation, housing structural features
(walls and floors that were constructed with cement/brick had a protective effect of
OR = 0.706 (p = 0.002) and OR = 0.640 (p = 0.023), respectively), source of lighting
(electricity was associated with reduced (OR = 0.258, p <0.0001)). Malaria risk also
varied by number of people living in a HH.
Discussion
In this study, malaria parasite carriage prevalence was 5.03% among study participants,
and 13% of HHs had at least one malaria-parasitaemic member. Risk factor analysis
identified variables that, alone or in combination, significantly influenced risk of malaria
to include age group, sex, administrative cell of residence, number of HH occupants, HH
structural features, and HH SES indicators. LLIN ownership and IRS activity were not
associated with malaria risk.
Malaria parasite carriage prevalence among all age participants was 5 and 9.7% among
children two to ten years. In an earlier study in this area, asymptomatic parasitaemia rates
among HH members (of fever cases identified at the hospital) was 5.1%, suggesting that
asymptomatic carriage rates have remained stable over the last two years [7]. Parasite
carriage rates in a community are a marker of malaria endemicity since they correlate

93
with the frequency and duration of parasite exposure [13]. Based on endemicity
classifications, the area studied was at hypo-endemic transmission level (<10% parasite
rates in children two to ten years).
However, some areas within the Ruhuha sector showed significantly higher malaria
transmission. Living in Gikundamvura cell was associated with a significantly increased
malaria risk, relative to the other residential cells. A similar finding was also shown in
2011 [7]. Gikundamvura is an area surrounded in the northeast by a vast expanse of
marshland used for rice cultivation, which is a major source of food and income. It is
plausible that the marshlands support mosquito breeding and increased malaria
transmission risk for neighbouring HHs. A follow-up study on environmental,
entomological and spatial risk features to better characterize the observed high malaria
risk is planned.
The studied area showed a high IRS coverage and LLIN ownership (both over 90%).
However, neither LLINs nor IRS showed any significant effect on malaria risk in this
area. With respect to LLINs, possible reasons for no observed protective effect may
include infrequent net use and poor quality of nets being used poor quality of nets being
used as reported elsewhere [14]. In a previous study in this area, only in 18% of visited
HHs was a bed net found to be physically hung onto a bed or sleeping space suggesting
that bed net use may be sub-optimal and that ownership of a bed net does not
automatically lead to usage of the net [7]. It is also plausible that most malaria-causing
bites occur in the evening and early night hours when most individuals are still outdoors
and use no control measure. Additionally, a change in mosquito biting preferences to
biting outdoors may increase risk of Plasmodium parasite transmission despite the
population having and using recommended malaria prevention indoor control measures.
Males were associated with higher malaria risk in this study, as has been shown in
comparable settings elsewhere, suggesting that males may exhibit a behaviour pattern
subjecting them to higher risk of exposure [15]. However, other studies, including one
previous study from this area, have shown either no sex differences in malaria risk, or

94
with the risk changing across sex by seasonality [7, 16-18]. Either inherent differences or
social, occupational or cultural determinants of exposure risk behaviour across different
settings may explain these observed risk difference by sex.
Age is an established risk factor for malaria - although its effect is influenced by area-
specific endemicity levels [15,19-20]. In this region, reported routine data (slide positive
rates) suggested reduced malaria transmission after the scaling-up of LLINs and IRS
coverage in 2000–2010 [2]. This transition in malaria transmission may have influenced
age-related risk of malaria parasitaemia. Compared to children under four years, children
aged five to 15 years, had increased odds of malaria risk while individuals aged ≥16 years
had significantly lower risk of parasitaemia. Other studies in Kenya and Eritrea
demonstrated an increased higher risk in older age groups relative to < five year olds in
numeric order [15, 21-22]. Similarly, a prior study conducted in Ruhuha [7] showed a
significantly higher risk in older age groups. In particular, a shift in the age at which
malaria peak prevalence was observed towards older children has been seen where
mosquito net coverage has increased concomitantly [20], and in association with reducing
entomological inoculation rates (EIRs) [23]. A reduction in exposure to Plasmodium spp.
inoculation leading to delays (in older age groups) or failure in acquiring protective
immunity is unlikely to account for the lower risk in the older age groups as they were
carrying asymptomatic parasitaemia and hence had not lost their immunity to malaria.
Human activity and mosquito-biting habits may also play a part in differential mosquito-
human exposure patterns. Behavioural patterns, including older children working and
playing where the Anopheles vector is present, especially at dusk when Anopheles
becomes active, have been suggested elsewhere [24]. Apart from younger children being
more likely to sleep under bed nets compared to older siblings [15, 25], older children, as
observed in this area, stay out longer in the evening and are more likely to be bitten by
malaria-carrying mosquitoes outdoors before returning later to their households. In the
Nigeria Garki malaria elimination project a major reason for failure to achieve
elimination was poor control of transmission, important outdoor-feeding and resting
vector populations [26]. Age-group differences in risk of exposure to mosquito bites

95
including use of malaria preventive measures like LLINs are more plausible reasons for
the observed risk of parasitaemia patterns in this study.
In this study, an increasing malaria risk was associated with higher house occupancy. In a
recent study in southeastern Tanzania, mosquitoes were found to be more attracted to
houses with high occupancy [27]. The presence of multiple sleepers leads to production
of larger volumes of mosquito-attracting human emanations and hence the increased risk
of transmission in comparison to houses with lower occupancy [28,29].
House structural features, such as types of floor, roof and wall material, have previously
been shown to influence risk of malaria infection [16, 22,30-31]. Study findings
confirmed that HH features associated with ease of entry, hiding and resting places within
HHs, factors that favour mosquito survival, biting and transmission chances, pose a
higher risk of malaria parasitaemia. HHs with wall structures made of bricks and cement
(vs wood and mud) and whose floor was made of bricks/cement (vs earth/dung/clay) had
a protective effect. Houses made of poor quality wall and roof materials are likely to have
eaves and openings that allow mosquitoes to easily access and stay longer in HH [32]. In
this study, type of roofing was not a significant risk determinant, but this could be
because 99.3% of all houses in the area are roofed with iron sheets and not enough
statistical power could be generated to see an effect. This study highlights the potential
value of improved house design to prevent mosquito entry and to minimize risk of indoor
malaria transmission as efforts supplementary to maintaining high coverage of other
interventions, including IRS and LLIN [27].
Compared to low SES HHs, medium and high SES HHs were associated with 0.73 and
0.48-fold reduction in risk of parasitaemia. Similarly, a malaria parasitaemia protective
effect found in HHs of high SES has been previously reported [33-36]. In one study,
improving house structural features was associated with lower malaria risk, possibly due
to better restriction of mosquito entry [37]. These findings are particularly consistent with
studies based on confirmatory parasitaemia as opposed to self-reported malaria/fever
classifications [33,38,39]. Other socio-economic indicator variables associated with a

96
reduced malaria risk for family members included HHs, where HoH reported having an
education (vs no education) and where the HH main source of lighting was electricity (vs
kerosene/candles/firewood/torches). Both variables are a proxy measure of higher SES, a
feature associated with lower risk. A possible reason for this may be that high SES
individuals may have a higher purchasing capacity for, and access to malaria-protective
measures including better housing facilities. Conversely, HHs where the HoH reported to
be a student (as the principal occupation) were associated with a higher risk of having a
HH with malaria.
This study has several limitations. To ensure all HH in the study area were visited,
enumeration lists generated by CHWs were used. However, during study implementation,
a number of HHs could not be found and there was no systematic strategy to identify
these missing households. Another limitation may be the detection method of malaria.
Malaria parasitaemia was diagnosed by light microscopy, which is known to have a lower
detection limit compared to molecular methods, especially in cases with low
parasitaemia. This may have underestimated the malaria burden, especially for
asymptomatic cases that tend to have low parasite carriage rates. In addition, the survey
period covered (June to November) was longer than initially planned (June to August).
This period covered times when both primary and secondary schools were either open or
closed (during school breaks) as well as before and after rainy season periods. For
households visited during the school season, many of the schoolchildren were not present
in the HH, and laboratory data could not be captured and were hence missed in the final
analysis, which may have limited study representativeness. Because reported study
results were derived from a cross-sectional survey, associations observed may be
confounded by unmeasured factors and are not suitable for drawing causal inferences.
Areas visited during the rainy season may have had a greater risk of malaria than those
visited outside the rainy period (such as Gikundamvura). However, in a previous study
done in the same sector [7] that had no seasonality bias, Gikundamvura cell showed a
greater risk as well, indicating that the rainy season may not have significantly influenced
malaria parasitaemia risk in this area.

97
Conclusion
Study results demonstrated malaria-hypoendemic levels of transmission, with the
distribution shown to vary spatially in this area. Age, sex, house structural features, and
socio-economic status indicators were key risk determinants for malaria parasitaemia.
Study findings showed a higher prevalence of asymptomatic parasitaemia in children
aged 5–15 years as well as in individuals aged over 16 years compared to children aged
below five years. In addition, improving HH socio-economic status and having house
structural features that limit indoor malaria transmission could reduce the risk of
parasitaemia and hence transmission within the community. For this area, despite high
coverage of IRS and LLIN distribution, current determinants of continued malaria
transmission risk remain unknown, including, but not limited to, which are the foci of
transmission, whether malaria transmission occurs primarily indoors or outdoors or both,
and which factors are responsible for the higher risks in males and older age groups.
Evaluation of spatial covariates to explain possible malaria parasitaemia clustering, a
characterization of entomological risk determinants of individual and HH malaria
parasitaemia risk and identification of cost-effective measures to improve house structure
features and HH socio-economic status are needed to sustainably reduce malaria
transmission in Ruhuha sector.

98
Acknowledgements
The Netherlands Organization for Tropical Scientific Research (NWO - WOTRO (AMC
Project Number SA358001) funded the study. We thank Ruhuha community members,
Ruhuha Health Centre leadership and the sector leadership for their support and study
participation.
Competing interests
The authors have declared that they have no competing interests.
Authors’ contributions
FK, MV and MFP participated in conception and design of the study. FK, EH, CMI, LM,
and PK were involved in study implementation. FK performed statistical analysis and PM
and MV provided critical reviews of the methods and results. FK wrote all drafts and
final manuscript versions. FK, PM, EH, CMI, LM, PK, SK, MV, and MPG contributed to
data analysis and manuscript writing. All authors read and approved the final manuscript.

99
References
1. Steketee RW, Sipilanyambe N, Chimumbwa J, Banda JJ, Mohamed A, Miller J, et al.
National malaria control and scaling up for impact: the Zambia experience through 2006.
Am J Trop Med Hyg 2008; 79:45–52.
2. Karema C, Aregawi MW, Rukundo A, Kabayiza A, Mulindahabi M, Fall IS, et al.
Trends in malaria cases, hospital admissions and deaths following scale-up of anti-
malarial interventions, 2000–2010 Rwanda. Malar J 2012; 11:236.
3. President’s Malaria Initiative. Rwanda Malaria Operational Plan FY 2014. Available
at: http://www.pmi.gov/docs/default-source/default-document-library/malaria-
operational-plans/fy14/rwanda_mop_fy14.pdf?sfvrsn=8. Accessed 15th August 2014.
4. Bousema T, Griffin JT, Sauerwein RW, Smith DL, Churcher TS, Takken W, et al.
Hitting hotspots: spatial targeting of malaria for control and elimination. PLoS Med
2012; 9:e1001165.
5. WHO. World malaria report 2011. Geneva: World Health Organization; 2011.
6. Laishram DD, Sutton PL, Nanda N, Sharma VL, Sobti RC, Carlton JM, et al. The
complexities of malaria disease manifestations with a focus on asymptomatic malaria.
Malar J 2012; 11:29.
7. Rulisa S, Kateera F, Bizimana JP, Agaba S, Dukuzumuremyi J, Baas L, et al. Malaria
prevalence, spatial clustering and risk factors in a low endemic area of Eastern Rwanda: a
cross sectional study. PLoS One 2013; 8:e69443.
8. USAID. Demographic Health Survey Overview. Available at:
http://www.dhsprogram.com/What-We-Do/Survey-Types/DHS.cfm. Accessed 12th May
2014.
9. GMP/WHO. From malaria control to malaria elimination: a manual for elimination
scenario planning. Available at:
http://apps.who.int/iris/bitstream/10665/112485/1/9789241507028_eng.pdf. Accessed 13
March 2014.
10. Raja A, Tridane A, Gaffar A, Lindquist T, Pribadi K. Android and ODK based data
collection framework to aid in epidemiological analysis. Online Journal of Public Health
Informatics. 2014; 5:228.
11. Vyas S, Kumaranayake L. Constructing socio-economic status indices: how to use

100
principal components analysis. Health Policy Plan 2006; 21:459–468.
12. Filmer D, Pritchett LH. Estimating wealth effect without expenditure data or tears: an
application to educational enrollments in states of India. Demography 2001; 38:115–132.
13. WHO. Systems for the early detection of malaria epidemics in Africa: an analysis of
current practices and future priorities. Geneva: World Health Organization; 2006.
14. Githinji S, Herbst S, Kistemann T, Noor AM. Mosquito nets in a rural area of
Western Kenya: ownership, use and quality. Malar J 2010; 9:250.
15. Winskill P, Rowland M, Mtove G, Malima RC, Kirby MJ. Malaria risk factors in
north-east Tanzania. Malar J. 2011; 10:98.
16. Ghebreyesus TA, Haile M, Witten KH, Getachew A, Yohannes M, Lindsay SW, et al.
Household risk factors for malaria among children in the Ethiopian highlands. Trans R
Soc Trop Med Hyg 2000; 94:17–21.
17. Giha HA, Rosthoj S, Dodoo D, Hviid L, Satti GM, Scheike T, et al. The
epidemiology of febrile malaria episodes in an area of unstable and seasonal
transmission. Trans R Soc Trop Med Hyg 2000; 94:645–651.
18. Brooker S, Clarke S, Njagi JK, Polack S, Mugo B, Estambale B, et al. Spatial
clustering of malaria and associated risk factors during an epidemic in a highland area of
western Kenya. Trop Med Int Health 2004; 9:757–766.
19. Smith T, Beck HP, Kitua A, Mwankusye S, Felger I, Fraser-Hurt N, et al. Age
dependence of the multiplicity of Plasmodium falciparum infections and of other
malariological indices in an area of high endemicity. Trans R Soc Trop Med Hyg 1999;
93:15–20.
20. Smith T, Hii JL, Genton B, Muller I, Booth M, Gibson N, et al. Associations of peak
shifts in age-prevalence for human malarias with bednet coverage. Trans R Soc Trop
Med Hyg 2001; 95:1–6.
21. Willis S, Akhwale JKL, Kaneko A, Eto H, Obonyo C, Björkman A, et al. Anemia and
malaria at different altitudes in the western highlands of Kenya. Acta Trop. 2004;
91:167–175.
22. Sintasath D, Ghebremeskel T, Lynch M, Kleinau E, Bretas G, Shililu J, et al. Malaria
prevalence and associated risk factors in Eritrea. Am J Trop Med Hyg 2005;72:682–687.
23. Beier JC, Killeen GF, Githure JI. Entomologic inoculation rates and Plasmodium

101
falciparum malaria prevalence in Africa. Am J Trop Med Hyg 1999; 61:109–113.
24. Peterson I, Borrell LN, El-Sadr W, Teklehaimanot A. Individual and household level
factors associated with malaria incidence in a highland region of Ethiopia: a multilevel
analysis. Am J Trop Med Hyg 2009; 80:103–111.
25. Lengeler C. Insecticide-treated bed nets and curtains for preventing malaria.
Cochrane Database Syst Rev. 2004; 2
26. Molineaux L, Gramiccia G. The Garki project. Geneva: World Health Organization.
1980; p. 311.
27. Lwetoijera DW, Kiware SS, Mageni ZD, Dongus S, Harris C, Devine GJ, et al. A
need for better housing to further reduce indoor malaria transmission in areas with high
bed net coverage. Parasit Vectors 2013; 6:57.
28. Takken W, Knols B. Odor-mediated behavior of Afrotropical malaria mosquitoes.
Annu Rev Entomol 1999; 44:131–157.
29. Port GR, Boreham PFL, Bryan JH. The relationship of host size to feeding by
mosquitoes of the Anopheles gambiae Giles complex (Diptera: Culicidae) Bull Entomol
Res 1980; 70:133–144.
30. Guthmann JP, Hall AJ, Jaffar S, Palacios A, Lines J, Llanos-Cuentas A.
Environmental risk factors for clinical malaria: a case–control study in the Grau region of
Peru. Trans R Soc Trop Med Hyg 2001; 95:577–583.
31. Butraporn P, Sornmani S, Hungsapruek T. Social, behavioural, housing factors and
their interactive effects associated with malaria occurrence in east Thailand. Southeast
Asian J Trop Med Public Health 1986; 17:386–392.
32. West PA, Protopopoff N, Rowland M, Cumming E, Cumming E, Rand A, et al.
Malaria risk factors in North West Tanzania: the effect of spraying, nets and wealth.
PLoS One 2013; 8:e65787.
33. Koram KA, Bennett S, Adiamah JH, Greenwood BM. Socio-economic risk factors
for malaria in a peri-urban area of The Gambia. Trans R Soc Trop Med Hyg 1995;
89:146–150.
34. Tshikuka JG, Scott ME, Gray-Donald K, Kalumba ON. Multiple infection with
Plasmodium and helminths in commu- nities of low and relatively high socio-economic
status. Ann Trop Med Parasitol 1996; 90:277–293.

102
35. Ayele DG, Zewotir TT, Mwambi HG. Prevalence and risk factors of malaria in
Ethiopia. Malar J 2012; 11:195.
36. Messina JP, Taylor SM, Meshnick SR, Linke AM, Tshefu AK, Atua B, et al.
Population, behavioural and environmental drivers of malaria prevalence in the
Democratic Republic of Congo. Malar J 2011; 10:161.
37. Atieli H, Menya D, Githeko A, Scott T. House design modifications reduce indoor
resting malaria vector densities in rice irrigation scheme area in western Kenya. Malar J
2009; 8:108.
38. Somi M, Butler J, Vahid F, Njau J, Kachur SP, Abdulla S. Is there evidence for dual
causation between malaria and socioeconomic status? Findings from rural Tanzania. Am
J Trop Med Hyg 2007; 77:1020–1027.
39. Clarke SE, Bogh C, Brown RC, Pinder M, Walraven GE, Lindsay SW. Do untreated
bednets protect against malaria? Trans R Soc Trop Med Hyg 2001; 95:457–462.

103
CHAPTER 5
Malaria, anaemia and under-nutrition: three frequently co-existing
conditions among preschool children in rural Rwanda
Fredrick Kateera1,2*, Chantal M. Ingabire2, Emmanuel Hakizimana3, Parfait
Kalinda2, Petra F. Mens1,4, Martin P. Grobusch1, Leon Mutesa5 and Michèle
van Vugt1
Author Affiliations 1Division of Internal Medicine, Department of Infectious Diseases, Centre of Tropical
Medicine and Travel Medicine, Academic Medical Centre, Meibergdreef 9, Amsterdam,
1100 DE, The Netherlands, 2Medical Research Centre Division, Rwanda Biomedical Centre, Kigali, Rwanda, 3Malaria and Other Parasitic Diseases Division, Rwanda Biomedical Centre, Kigali,
Rwanda, 4Royal Tropical Institute, Koninklijk Instituut voor de Tropen, KIT Biomedical Research,
Meibergdreef 39, Amsterdam, 1105 AZ, The Netherlands, 5College of Medicine and Health Sciences, University of Rwanda, Kigali, Rwanda
Published in: Malaria Journal 2015; 14:440

104
Abstract
Background
Malaria, anaemia and under-nutrition are three highly prevalent and frequently co-
existing diseases that cause significant morbidity and mortality particularly among
children aged less than 5 years. Currently, there is paucity of conclusive studies on the
burden of and associations between malaria, anaemia and under-nutrition in Rwanda and
comparable sub-Saharan and thus, this study measured the prevalence of malaria
parasitaemia, anaemia and under-nutrition among preschool age children in a rural
Rwandan setting and evaluated for interactions between and risk determinants for these
three conditions.
Methods
A cross-sectional household (HH) survey involving children aged 6–59 months was
conducted. Data on malaria parasitaemia, haemoglobin densities, anthropometry,
demographics, socioeconomic status (SES) and malaria prevention knowledge and
practices were collected.
Results
The prevalences of malaria parasitaemia and anaemia were 5.9 and 7.0 %, respectively,
whilst the prevalence of stunting was 41.3 %. Malaria parasitaemia risk differed by age
groups with odds ratio (OR) = 2.53; P = 0.04 for age group 24–35 months, OR = 3.5;
P = 0.037 for age group 36–47 months, and OR = 3.03; P = 0.014 for age group 48–
60 months, whilst a reduced risk was found among children living in high SES HHs
(OR = 0.37; P = 0.029). Risk of anaemia was high among children aged ≥12 months,
those with malaria parasitaemia (OR = 3.86; P ≤ 0.0001) and children living in HHs of
lower SES. Overall, under-nutrition was not associated with malaria parasitaemia.
Underweight was higher among males (OR = 1.444; P = 0.019) and children with
anaemia (OR = 1.98; P = 0.004).

105
Conclusions
In this study group, four in 10 and one in 10 children were found stunted and
underweight, respectively, in an area of low malaria transmission. Under-nutrition was
not associated with malaria risk. While the high prevalence of stunting requires urgent
response, reductions in malaria parasitaemia and anaemia rates may require, in addition
to scaled-up use of insecticide-treated bed nets and indoor residual insecticide spraying,
improvements in HH SES and better housing to reduce risk of malaria.

106
Background
Malaria, anaemia and under-nutrition are each associated with significant morbidity and
mortality, particularly among children in sub-Saharan Africa [1–3]. Globally, malaria is
responsible for over 450,000 deaths among children under 5 years [1]; anaemia is
prevalent in 273 million (43 %) of children aged 6–59 months [2]; and severe under-
nutrition affects about 20 million preschool-aged children living mostly in African and
South-East Asia Regions [4]. In the majority of the affected children, all three conditions
frequently co-exist and have been associated with long-term complications, including
deficits in physical and cognitive development and poor school performance [5–8].
Anaemia is characterized by a reduction in haemoglobin concentration causing
impairment in meeting the oxygen demands of the body. Anaemia results broadly from
either ineffective erythropoiesis or increased loss of erythrocytes or both. The main
causes of anaemia include acute or chronic blood loss, nutritional deficiencies (including
vitamins A, B12, C and folic acid and iron) [9], infectious diseases [10–12] and genetic
disorders [13-14].
Malaria causes a substantial proportion of anaemia observed in malaria endemic settings
[15,16]. However, how much of the anaemia burden is associated with malaria, relative
to other causes, and across the different strata of malaria endemicities has not been
studied.
Studies elucidating associations between malaria and under-nutrition yield conflicting
results [8]; with some suggesting that under-nutrition is associated with higher malaria
morbidity and all-cause mortality outcomes [17–19], while others show no effect of
under-nutrition on malaria [20]. Conversely, some studies have associated malaria with
increased risk of under-nutrition [21] and Plasmodium falciparum infection has been
associated with acute weight loss [22]. Additionally, improvements in growth and other
anthropometric indexes have been described in children protected from malaria, by using
both malaria chemoprophylaxis and long-lasting insecticide-treated bed nets (LLINs) [23,
24].

107
Given the extensive temporal and spatial correlation between malaria, anaemia and
under-nutrition, any interaction (causal or increasing the likelihood of poor health
outcomes on either diseases) may lead to synergistic deleterious effects on child health
and development. Studies on interactions between malaria, anaemia and under-nutrition
particularly among community preschool-aged children are few and inconclusive [15].
Most of these children carry these disease conditions in “hidden” pre-clinical stages and
rarely present to medical personnel in the national health care system. This study
measured the prevalence, investigated co-existence and assessed for risk determinants of
malaria parasitaemia, anaemia and under-nutrition among preschool-going children in a
rural Rwandan community.
Methods
Study site
Regarding administration, Rwanda has 30 districts: Each divided into sectors, cells, and
villages locally term “umudugudus” (of about 50–100 households). This survey was
conducted in 35 villages that are aggregated into five cells that constitute Ruhuha sector,
Bugesera District in Eastern Rwanda (Fig. 1). Ruhuha sector is located 42 kms from
Kigali city, has an area of 54 square meters and is separated from Burundi in the south by
Lake Cyohoha. The sector has a population of ~23,900 individuals living in 5098
households (HHs): By sector, Gatanga has 1048 HHs, Ruhuha 696 HHs, Gikundamvura
869 HHs, Bihari 957 HHs and Kindama 1528 HHs. Ruhuha is a rural agricultural
traditionally high malaria transmission setting with prior reported health facility slide
positivity rates among sick individuals and community-based asymptomatic malaria
positivity rates of 22 % and 5 %, respectively [25-26].

Fig
1. M
ap o
f Ruh
uha
sect
or, B
uges
era
dist
rict s
how
ing
lay
out o
f the
5 c
ells
and
ass
ocia
ted
key
geog
raph
ical
feat
ures
of e
leva
tion,
wet
land
s, ro
ad n
et a
nd a
lake

109
Study design and selection of study participants
A larger descriptive cross-sectional survey involving all study area HHs was conducted to
study social, economic, entomological and biomedical determinants of residual
asymptomatic malaria burden and transmission intensity. In summary, the night prior to
the survey, a village community health care worker identified HHs to be visited from an
enumeration list and requested heads of households (HoH) and family members to stay
in-house. Upon providing consent, the study team (consisting of an interviewer and a
laboratory technician) visited the notified HH and administered an interviewer-guided
questionnaire to HoHs. In HHs where no member or no HoH or spouse was found
present, a return visit was scheduled and attempted within 7 days. All HHs where the
study team failed to conduct a survey on the return visit were excluded. Study findings
from this larger sector-wide HH survey conducted between June and November 2013
have since been published [26]. For this sub-study, final data analysis was performed for
only children aged 6–59 months who had complete laboratory and questionnaire data.
Study procedures
Head of household interviews
A structured questionnaire was administered to the child’s primary caregiver to collect
data on (1) demographics (sex, age, literacy, occupation, religion and marital status); (2)
malaria prevention bed net (LLIN ownership, number and use) and indoor residual
spraying (IRS) experience; (3) SES related variables (incomes, savings, land ownership,
animals and sources of utilities like water, lighting and cooking) and HH structural
features including type of outside wall, floor and roof materials); and (4) fever
management practices. For each HH, location data was captured using a geographic
positioning function based on the Samsung Galaxy 2 Android platforms (Samsung
Electronics Co. Ltd, South Korea). The questionnaire used was written in English and
was field-tested at three sites in order to minimize ambiguity, ensure consistency of
comprehension of questions by both interviewers and respondents. Field workers were
trained to administer the interviews in the local dialect (Kinyarwanda). Questionnaire
data was collected using an electronic format developed using the open source Open Data
Kit Collect setup on Android tablets [27].

110
Anthropometric measurements
Measures of under-nutrition indices (stunted, underweight, and wasted) were deduced
from data on (1) age-in-months as reported by parents, (2) weight measured using
UNICEF provided a digital Seca 874 weight scales (seca GmbH & Co. KG.) to the
nearest 0.1 kg, and (3) height measured using a mobile measuring Seca 210 (seca GmbH
& Co. KG.) mat for children 0 to 99 centimetres and a recumbent length board for
children of height > 99 centimetres to the nearest centimetre, respectively.
Laboratory methods
From all HH members aged ≥6 months; finger-prick blood samples for malaria smear-
based diagnosis and haemoglobin measurement were collected. Each smear was stained
with 2 % Giemsa, processed and read independently by two study-trained
microscopists at Ruhuha Health Centre laboratory. In case of a discrepancy, a tiebreaker
third microscopist determined the final result. Expert microscopists at the National
Reference Laboratory, Kigali, conducted quality control for all positive slides and a
random sample of 5 % of all negative slides. Haemoglobin densities were measured on
the spot in the field using a portable automated HemoCue ® Hb 301 haemoglobinometer
system (HemoCue AB, Angelholm, Sweden) according to the product instruction.
Outcome and predictor variables
A blood smear was considered negative when light microscopy examination of 100 high-
power fields did not reveal any asexual parasites and considered positive if any asexual
parasites were detected on thick blood microscopy. In this study, malaria diagnosis was
assessed based on presence of malaria parasites in blood by microscopy only. Data on
reported symptoms or clinical signs was not collected. Anaemia was defined as
moderate-to-severe haemoglobin levels of <90 g/L as recommended for disease
surveillance, especially in areas of high anaemia prevalence [28]. Weight-for-height
(wasting), height-for-age (stunting) and weight-for-age (underweight) z scores were
calculated on the basis of the WHO Global Database on Child Growth and Malnutrition
[29]. Z scores of <−2 SD were considered indicative of wasting, stunting, and
underweight, respectively, while corresponding Z scores of <−3 SD were considered

111
indicative of severe under-nutrition. Predictor variables included HoH demographics
(including age, sex, religion, marital status), cell of residence), malaria prevention
practices (including availability and use of LLINs, HH use of IRS, reported prior fever
management experiences, HH structure materials including type of floor (soil/clay/dung
vs. brick/cement), roof (iron sheets vs. grass/tents), and outside walls (cement/brick
versus mud/wood wall). A HH level SES/wealth index (used to categorize each HH as
low, middle and high SES category) was generated using 10 indicator variables using
principal component analysis [30].
Study consent and ethical approval
Written informed consent to participate in the study as well to allow study findings to be
published in a relevant scientific journal was obtained from the HoH on behalf of all
household members including minors. The National Health Research Committee
(NHRC) and the Rwanda National Ethics Committee, Kigali, Rwanda (No
384/RNEC/2012) granted ethical and scientific approval for the study protocol.
Statistical analysis
Data was collected using handheld android platforms on which open data kit software-
hosted electronic questionnaire was loaded. These data was then relayed onto a server.
Laboratory and anthropometric data was manually recorded in laboratory registers and
later entered into Microsoft Access software. The two datasets were then merged and
transferred into STATA 12.1 (STATA Corp., College Station, TX, USA) for analysis.
Continuous variables were compared between groups (including stratification by age and
sex) using Mann–Whitney U tests, and variable proportions were compared by Χ 2 test.
Associations between predictor variables and primary outcomes were statistically
assessed for using both bivariate and multivariate logistic regression analysis. Odds ratios
(ORs) and 95 % confidence intervals (CIs) were computed. Any covariate with a p value
<0.15 in bivariate analysis were subsequently included in the final multivariable logistic
model. Multi-collinearity tests were performed for all potentially correlated variables
included in the final multivariate model for each of the five primary outcomes. Any risk
estimate with a p-value <0.05 was considered statistically significant after adjustment for

112
HH-level clustering and influence of other variables.
Results
Study population
As reported in the earlier publication for the larger survey, a total of 4705 HHs were
surveyed and of these, data from 12,965 (all-ages) individuals from 3968 (84.3 %) HHs
that had complete laboratory and questionnaire data was aggregated in the primary
database [26]. From this primary database, data for 3182 children (aged 6–59 months)
from 2228 HHs were extracted and analysed in this study. However for the final analysis,
only 1882 (59.1 %) children with complete data on all primary outcome covariates
(malaria slide positivity, haemoglobin densities and anthropometric data on age by
months, height and weight) were considered.
Of the 1882 children, 50 % were female; the median age was 31.1 months (interquartile
range (IQR), 18.4–45.7 months); the mean height was 85.8 cm and mean weight was 12.1
kgs. The median number of HH occupants was 5 (IQR 4–6) (Table 1). The prevalence of
P. falciparum parasitaemia, moderate-to-severe anaemia and under-nutrition parameters
of stunting, wasting and underweight were 5.9 %, 16.4 %, 41.3 %, 8.8 % and 15.8 %,
respectively (Table 1).

113
Table 1: Study population baseline and demographic characteristics. 1
Variable Value (%) N = 1882Sex Male 941 (50)
Female 941 (50)Study group median age 31.1 (IQR - 18.4-45.70)Study group mean weight in Kilograms 12.10 (± 2.97)Study group mean height in meters 85.93 ± 12.35Study group mean haemoglobin density in g/dl 11.30 (± 1.53)Number of children per Cell Biharwe 296 (15.7)
Gatanga 474 (25.2)Gikundamvura 372 (19.8)
Kindama 423 (22.5)Ruhuha 317 (16.8)
Number of children with malaria parasite carriage (Yes) 110/1876 (5.9%)Number of children with moderate-severe anaemia (<90 g/l) 132 /1876 (7.0%)Number of children with under weight (Z score of < -2 SD of mean) 297 /1882 (15.8%)Number of children with stunting (Z score of < -2 SD of mean) 777/1882 (41.3%)Number of children with wasting (Z score of < -2 SD of mean) 166 /1876 (8.8%)Number of children reported ownership of ≥ 1 Bednet in HH (Yes) 1,799/1882 (95.6%)Number of HHs with reported IRS done in last 12 months (Yes) 1,805/1882 (95.9%)Number of children with reported fever in last 6 months (Yes) 1,293 /1882 (68.7%)Number of HoH per education level None 620 (33%)
Primary/Secondary/Tertiary 1259 (67%)Number of HH occupants. 1-3 298 (15.83%)
4-7 1373 (72.95%)8+ 211 (11.22%)
Number of children per age grou 6-11 225 (11.96%)12-23 435 (23.11%)24-35 434 (23.06%)36-47 372 (19.77%)48- 60 416 (22.10%)
1 Plus – Minus Values are means ± SD, HH – Households, IQR – Interquartile range,
The proportions of children with co-morbidity were: 23/1882 (1.2 %) with malaria and
anaemia; 59/1882 (3.1 %) with any under-nutrition and malaria 82/1882 (4.4 %) with any
under-nutrition and anaemia. Only five children were found to have all three conditions
concurrently (Table 2).

114
Table 2: Frequency of malaria, anaemia and under-nutrition co-morbidity1
Malaria n (%)
Anaemia - n (%) Malnutrition - n(%)
Totals (n)
Malaria 38 (34.5) 23 (20.9) 59 (53.6) 110Anaemia 23 (17.4) 27 (20.5) 82 (62.1) 132Under-nutrition 59 (6.4) 82 (8.9) 782 (84.7) 923
1 The total number of children with malaria, anaemia and under-nutrition was 5.
Factors associated with malaria
Malaria prevalence differed by sex (7.5 % in females vs. 5.5 % in males: OR = 0.718;
P = 0.034), age groups (compared to children aged <24 months, 24–35 months
OR = 2.53; P = 0.04, 36–47 months age group OR = 3.5; P = 0.037, and for 48–60 age
group, OR = 3.03; P = 0.014); and by cell of residence (10.9 % in Gikundamvura vs.
2.2 % in Ruhuha) (Table 3). By bivariate analysis, living in Gikundamvura (relative to
living in Biharwe) cell was associated with a two-fold increase in odds of
infection (P = 0.004). In the final multivariable model, malaria prevalence was
significantly higher among older children (age-groups > 24 months), but was lower
among children from high SES HHs (OR = 0.37; P = 0.029) (Table 4). A reduced malaria
prevalence (borderline significant) was found among children; whose HH had used
domestic water collected from a closed source (taps and boreholes) compared to HH
where the used domestic water collected from an open source (OR = 0.62; P = 0.059),
whose HoH had any education (OR = 0.63; P = 0.045); and whose house structure walls
were made of bricks/cement (OR = 0.62; P = 0.061) (Table 4).

Tab
le 3
. Mal
aria
par
asita
emia
and
ana
emia
dis
trib
utio
ns a
nd u
niva
riat
e an
alys
is st
ratif
ied
by se
x, r
esid
ence
and
age
gro
up
Abb
revi
atio
ns: O
R–
Odd
s rat
io, C
I –C
onfid
ence
inte
rval
P
valu
es fo
r cat
egor
ical
var
iabl
es w
ere
base
d on
the
2te
st.
Var
iabl
esM
alar
ia p
aras
itaem
iaM
oder
ate
-sev
ere
anae
mia
n (%
)O
R (9
5% C
I), P
-val
uen
(%)
OR
(95%
CI)
, P-v
alue
Sex
M
ale
49 (5
.24)
0.79
6 (0
.540
-1.1
73),
0.24
8 70
(7.4
)1.
139
(0.7
99-1
.624
), 0.
470
Fem
ale
61 (
6.49
)1
62 (6
.6)
1A
ge-G
roup
6-11
6 (2
.68)
129
(12.
9)1
12-2
319
(4.3
7)1.
659
(0.6
53-4
.216
), 0.
287
33 (7
.6)
0.55
5 (0
.327
-0.9
40),
0.02
924
-35
28 (6
.51)
2.53
1 (1
.032
-6.2
06),
0.04
230
(6.9
)0.
502
(0.2
93-0
.860
), 0.
012
36-4
725
(6.7
4)2.
625
(1.0
59-6
.502
),0.
037
21 (5
.6)
0.40
4 (0
.225
-0.7
28),
0.00
348
-59
32 (7
.69)
3.02
8 (1
.246
-7.3
56),
0.01
4 19
(4.6
)0.
323
(0.1
77-0
.591
), <
0.00
01R
esid
ence
Bih
arw
e19
(6.4
2)1
18 (6
.1)
1G
atan
ga23
(4.8
5)0.
743
(0.3
98-1
.390
), 0.
353
33 (6
.9)
1.15
6 (0
.638
-2.0
92),
0.63
3G
ikun
dam
vura
38 (1
0.30
)1.
674
(0.9
43-2
.969
), 0.
078
33 (8
.9)
1.50
3 (0
.829
-2.7
28),
0.18
0K
inda
ma
23 (5
.46)
0.84
3 (0
.450
-1.5
77),
0.59
2 26
(6.2
)1.
011
(0.5
44-1
.881
), 0.
971
Ruh
uha
7 (2
.22)
0.33
0 (0
.137
-0.7
98),
0.01
422
(6.9
)1.
152
(0.6
05-2
.193
), 0.
667

Tab
le 4
.Mul
tivar
iate
risk
fact
ors a
naly
sis f
or a
naem
ia, u
nder
-nut
ritio
n pa
ram
eter
s and
mal
aria
par
asita
emia
Var
iabl
eA
naem
iaSt
untin
gW
astin
gU
nder
wei
ght
Mal
aria
Mal
aria
par
asita
emia
(pos
itive
)3.
857
(2.2
08-6
.740
), <0
.000
1Pr
esen
ce o
f ana
emia
(Y
es)
1.85
7 (1
.093
-3.
155)
, 0.0
22
3.89
8 (2
.297
-6.6
15),
<0.0
001
Pres
ence
of s
tunt
ing
(yes
)1.
428
(0.9
60-2
.126
), 0.
079
0.04
6 (0
.024
-0.0
88),
< 0.
0001
20
.412
(12.
304-
33.8
62),
<0.0
001
Pres
ence
of w
astin
g (y
es)
0.05
5 (0
.030
-0.0
98),
<0.
0001
59.1
39 (3
2.50
6-10
7.59
4), <
0.00
01Pr
esen
ce o
f und
er w
eigh
t (ye
s)
1.97
9 (1
.240
-3.1
58),
0.00
420
.256
(12.
464-
32.9
21),
<0.0
001
60.7
1 (3
1.99
4-11
5.19
7), <
0.00
01Se
x (m
ale)
1.44
4 (1
.061
-1.9
66),
0.01
9Fe
ver (
Yes
)1.
331
(1.0
70 -
1.65
6), 0
.010
Is
HH
in a
n ec
onom
ic g
roup
0.
758
(0.6
18 -
0.93
1), 0
.008
W
as IR
S do
ne in
HH
(Yes
)0.
471(
0.22
2-0.
997)
, 0.0
490.
589
(0.3
97-0
.873
), 0.
008
Doe
s HH
ow
ns ≥
1 ne
t (Y
es)
0.55
1 (0
.338
-0.
899)
, 0.0
17
Stud
y pa
rtici
pant
age
Gro
up6-
11-
-12
-23
0.52
2 (0
.297
-0.
916)
, 0.0
231.
262
(0.6
97 -
2.28
3), 0
.443
1.
989
(0.7
66 -
5.16
9), 0
.158
24
-35
0.40
5 (0
.227
-0.7
21),
0.00
21.
849
(1.0
31 -
3.31
6), 0
.039
3.15
7 (1
.259
-7.
920)
, 0.0
14
36-4
70.
340
(0.1
81-0
.639
), 0.
001
2.12
4 (1
.159
-3.
894)
, 0.0
153.
528
(3.1
384
-8.9
92),
0.00
8
48-6
00.
257
(0.1
35-0
.490
), <0
.000
12.
123
(1.1
69 -
3.85
5), 0
.013
3.
699
(1.4
79 -
9.25
1), 0
.005
HH
SES
Lev
elLo
w Mid
dle
0.58
8 (0
.373
-0.9
28),
0.02
2 0.
793
(0.4
15 -
1.51
6), 0
.483
H
igh
0.56
8 (0
.352
-0.9
16),
0.02
0 0.
372
(0.1
52 -
0.90
6), 0
.029
Doe
s H
H h
ave
a cl
osed
wat
er
sour
ce (
Yes
)1.
465
(0.9
69-2
.214
), 0.
070
0.62
0 (0
.377
-1.
018)
, 0.0
59H
ouse
wal
l m
ater
ial
(Bric
ks
and
ston
es v
s. w
ood/
mud
/tent
) 0.
615
(0.3
70 -
1.02
4), 0
.061
Hou
se
floor
m
ater
ial
(cem
ent/c
oncr
ete
vs.
mud
/ear
th/d
ung)
0.
447
(0.2
76 -
0.72
3), 0
.001
Hig
hest
HoH
educ
atio
n le
vel
(Non
e vs
. any
) 0.
633
(0.4
04 -
0.99
0), 0
.045

117
Factors associated with anaemia
Anaemia distribution was similar across both sexes but decreased with increasing age
and, similar to malaria parasitaemia, showed a higher proportion among children in
Gikundamvura cell (10.2 %) vs. children in the other four cells with proportions ranging
from 5.4 to 6.3 % (Table 3). By bivariate analysis, living in Gikundamvura was
associated with a 1.9-fold (P = 0.008) higher odds of having anaemia compared to living
in Biharwe cell while the risk of anaemia decreased with increasing age group (Table 3).
In the final multivariate model, anaemia risk was high among children with malaria
infection (OR = 3.86) and underweight (OR = 1.98) and decreased with increasing age,
and among children living in wealthier HHs of middle and high SES (OR = 0.59;
P = 0.022 and OR = 0.57; P = 0.020, respectively) (Table 4).
Factors associated with under-nutrition
Under-nutrition parameters showed varying co-existence patterns (Table 5). In summary,
(1) underweight was associated with stunting (OR = 20.41; P ≤ 0.0001) and wasting (OR
59.14; P ≤ 0.0001); (2) stunting was associated with underweight (OR = 20.26;
P ≤ 0.0001) but not wasting (OR = 0.06; P ≤ 0.0001); and (3) wasting was associated
with underweight (OR = 60.71; P ≤ 0.0001) but not stunting (OR = 0.05; P ≤ 0.0001). In
the final multivariate model, other predictors of (1) stunting were a reported fever history
(OR = 1.33; P = 0.01); living in a house where the HoH belonged to a higher economic
group (OR = 0.79; P = 008) and living in HHs that has a reported ownership of ≥1 LLIN
(OR = 0.55; P = 0.017) (2) wasting were reported IRS applied in the HH (OR = 0.59;
P = 0.008), and domestic water source (HHs using closed source had OR = 1.47;
P = 0.07) and (3) underweight were sex (male 0R = 1.44; P = 0.019), age group, house
floor material (bricks/cement OR = 0.45; P = 0. 001). Collinearity analysis between all
variables included in each of final multivariate model for the five primary outcomes
showed mean variance inflation factor (VIF) values ranging from 2.17 to 7.23. For each
of the five-outcome models, no variable showed a VIF >10: This is the cut-off marker of
multicolinearity.

Tab
le 5
. Stu
ntin
g, u
nder
-wei
ght a
nd w
astin
gdi
stri
butio
ns a
nd u
niva
riat
e an
alys
is st
ratif
ied
by se
x, r
esid
ence
and
age
gro
up
P va
lues
for c
ateg
oric
al v
aria
bles
wer
e ba
sed
on th
e 2
test
OR
–O
dds r
atio
, CI –
Con
fiden
ce in
terv
al
Var
iabl
esSt
untin
gU
nder
wei
ght
Was
ting
n (%
)O
R (9
5% C
I), P
-val
uen
(%)
OR
(95%
CI)
, P-v
alue
n (%
)O
R (9
5% C
I), P
-val
ueSe
x
M
ale
404
(42.
93)
1.14
6 (0
.953
-1.3
77),
0.14
7 16
7 (1
7.75
)1.
346
(1.0
49-1
.727
), 0.
020
79 (8
.41)
0.89
7 (0
.652
-1.2
35),
0.50
6 Fe
mal
e 37
3 (3
9.64
)1
130
(13.
82)
187
(9.2
8)1
Age
-Gro
up6-
1184
(37.
33)
125
(11.
11)
122
(9.7
8)1
12-2
319
1 (4
3.91
)1.
314
(0.9
45-1
.827
), 0.
105
59 (1
3.56
)1.
255
(0.7
63-2
.066
), 0.
371
41 (9
.45)
0.96
3 (0
.558
-1.6
60),
0.89
124
-35
193
(44.
47)
1.34
4 (0
.967
-1.8
69),
0.07
978
(17.
97)
1.75
3 (1
.082
-2.8
40),
0.02
338
(8.8
4)0.
894
(0.5
15-1
.553
), 0.
692
36-4
714
6 (3
9.25
)1.
084
(0.7
71-1
.525
), 0.
641
65 (1
7.47
)1.
694
(1.0
33-2
.777
), 0.
037
32 (8
.63)
0.87
1 (0
.493
-1.5
40),
0.63
548
-59
163
(39.
18)
1.08
1 (0
.774
-1.5
11),
0.64
670
(16.
83)
1.61
8 (0
.993
-2.6
39),
0.05
333
(7.9
3)0.
795
(0.4
51-1
.399
), 0.
427
Res
iden
ceB
ihar
we
114
(38.
51)
152
(17.
57)
127
(9.1
2)1
Gat
anga
217
(45.
78)
1.34
8 (1
.003
-1.8
12),
0.04
883
(17.
51)
0.99
6 (0
.680
-1.4
59),
0.98
438
(8.0
30.
870
(0.5
19-1
.458
), 0.
598
Gik
unda
mvu
ra14
8 (3
9.78
)1.
055
(0.7
71-1
.442
), 0.
738
64 (1
7.20
)0.
975
(0.6
52-1
.458
), 0.
902
35 (9
.46)
1.04
1 (0
.614
-1.7
63),
0.88
1 K
inda
ma
160
(37.
83)
0.97
1 (0
.715
-1.3
18),
0.85
2 58
(13.
71)
0.74
6 (0
.496
-1.1
21),
0.15
838
(9.0
)0.
986
(0.5
88-1
.654
), 0.
957
Ruhu
ha13
8 (4
3.53
)1.
231
(0.8
91-1
.699
), 0.
207
40 (1
2.62
)0.
678
(0.4
33-1
.059
), 0.
088
28 (8
.89)
0.97
2 (0
.558
-1.6
92),
0.92
0

119
Discussion
At least 4/10 and 1/10 preschool-age children in this rural setting were found stunted and
underweight, respectively. Observed malaria parasite rates of <10 % suggest that this area
is hypo-endemic for malaria. In this study, the proportion of children aged under 5 years
with malaria (6.5 %) was almost two-fold higher than the 3.4 % reported in the same
province in 2010 [31]. These differences in proportions infected with malaria may be
partially explained by malaria-associated temporal patterns, seasonality and/or
differences in sampling technique used in the two surveys. However, the parasite rates
observed in this study are comparable to the <10 % malaria infection rates reported
among community members previously [25-26], [31] suggesting that this area is of hypo-
endemic transmission intensity [26].
In this study, risk of malaria increased with increasing age. Findings in this study are
consistent with an increasingly observed trend of higher malaria risk among older age
groups, as reported previously elsewhere and in this area, following the scale-up of
control interventions [25-26], [32-33]. A reduction in malaria transmission and hence a
lower frequency of exposure to malaria parasite inoculation and the associated infections
impedes and, plausibly, delays development of a malaria protective immunity leading to
an increased risk of malaria in older age groups. However, two reasons may account for
the higher risk in older children observed in this study: (1) younger children are more
likely to sleep under ITNs and hence be more protected, and (2) in contrast, older
children are likely to tolerate malaria parasites without developing a fever and hence have
an increased prevalence of asymptomatic malaria parasitaemia.
In this study, a protective malaria risk was associated with living in a high SES HHs.
However, studies on associations between malaria and SES have hitherto yielded
conflicting results, with some indicating no associated effect [34, 35] while others have
shown that higher SES induces a protective effect [36, 40]. It is plausible that a protective
effect may exist where improved house structural features lead to a reduction in indoor
malaria transmission by restricting mosquito entry [40]. Individuals living in houses
whose wall structure were made of wood/mud (vs cement/bricks) showed a significantly
higher risk of malaria in this study. Houses whose walls are made of mud have been

120
associated with having more eaves (that support mosquito entry), higher risk of indoor
mosquito bites and, by creating cooler and darker conditions in comparison to
brick/cement houses, creating a favourable indoor resting environment for mosquitoes
[41–43].
The proportion of children under 5 years found with anaemia in this study (6.8 %) was
three-fold higher than the 2.0 % reported for the same province in 2010 [31]. After
adjusting for all predictors, anaemia risk was associated with malaria parasitaemia, age
group, HH SES and underweight, with a borderline significant outcome noted among
children with stunting and those coming from HHs where IRS was applied. Individuals
found with moderate-to-severe anaemia had an almost four-fold increased risk of being
malaria-infected. In malaria-endemic settings, malaria is the most common cause of
anaemia [10] and among parasitaemic patients in comparable settings; a similarly
increased risk of anaemia has been previously demonstrated [35, 44-45]. In one study
among preschool-going children in Uganda, malaria was found to be the only risk
determinant for anaemia [16]. Additionally, effective malaria control programmes have
been shown to significantly reduce anaemia burden, with anaemia now considered a
surrogate indicator of impact of malaria control programmes [46-47]. Interestingly in this
study, the risk of anaemia decreased with increasing age groups in contrast to the
observed increasing risk of malaria across the same age groups in our study and some
studies other malaria-endemic settings [15, 35, 48]. However, in all the other settings, the
reported malaria parasite carriage rates were significantly higher than the 6.8 % reported
in this study. In study areas of lower parasitaemia carriage, and especially following
reduction in malaria burden, malaria may make a less significant attributable contribution
to anaemia relative to other risk factors [46].
Anaemia, but not malaria, was significantly associated with underweight in this study.
Evidence for the impact of under-nutrition on development of anaemia in young children
living in malaria-endemic areas had been reported previously [9]. Previous studies on
malaria and under-nutrition associations have shown contrasting results. In Ghana and in
The Gambia, under-nutrition was associated with increased risks of malaria-associated

121
mortality and the risk of having multiple malaria episodes, respectively [17-18]. In
contrast, in Burkina Faso and Uganda, no association between under-nutrition and
malaria morbidity was demonstrated [35, 49]. Although this study did not assess for other
causal factors associated with anaemia, it is plausible that children who are malnourished
are more likely to also have had micronutrient deficiencies that may have partly
contributed to the burden of anaemia observed.
Children from middle and high SES HHs were found to have a significantly reduced risk
of having anaemia than children from low SES HHs. Two plausible reasons for this are
the differential nutritional intakes and house structural features that determine risk of
indoor malaria transmission between the two SES levels. Presumably, children from low
SES HHs are likely to have poorer nutritional intake and also live in houses whose
structure are more conducive for indoor malaria transmission, with the increased risk of
malaria causing a concurrent deleterious effect on anaemia risk.
Among preschool-aged children in the same province in 2010, stunting, wasting and
underweight proportions in comparison to findings in this study were 43.9 %, 3.2 % and
11.5 % vs. 41.6 %, 8.8 % and 15.8 %, respectively [31]. Both surveys point to very high
prevalence of stunting in this age group in this area. In our study, male sex was associated
with a 1.44-fold increase in risk of underweight. Sex differences in risk of under-nutrition
have been shown elsewhere [50], [51], but studies elucidating the observed sex-
dependent risk of under-nutrition are lacking. As reported previously, the risk of being
underweight significantly increased with increasing age in this study [52-53]. Possible
reasons for increased risk of underweight with increasing age could include but are not
limited to (1) short birth intervals with mothers not having adequate gestational weight
gains and hence having smaller than expected babies at birth; (2) reduced breast feeding
periods; (3) poor weaning diets and; (4) reduced care given to older children following
successive births [53].
Other risk determinants for malaria, anaemia and under-nutrition metrics were also
identified. Living in houses where the HoH was not educated and in houses where

122
domestic water was sourced from an open source compared to HHs where domestic
water was drawn a closed source were associated with a high risk of malaria infection.
Lack of education may likely be associated with low SES status and limited malaria
control-associated knowledge and practice factors, which may be related to lower
availability and use of malaria control measures like LLINs. Regarding the domestic
water sources, open water sources may also serve as potential mosquito breeding sites
and hence pose an increased risk. Anaemia risk was interestingly found to be lower by
almost 50 % among individuals living in HHs where IRS was carried out. It is plausible
that the IRS effect on lower anaemia risk was mediated primariry through reducing
malaria risk. However, other unmeasured risk determinants may have contributed to the
high risk among individuals from HHs where no IRS was applied of anaemia. Other
identified risk determinants for under-nutrition included SES indicator variables (HoH
belonging to an economic group and type of material house floor is made of) and prior
fever experience and malaria control measures (LLIN availability and IRS experience).
Given that the study area is predominantly agricultural, HHs where the HoHs reported
being a member of an economic group are more likely to have better food security and
hence a lower risk of under-nutrition. Individuals who reported having had a fever during
the past 6 months are likely to have had malaria: A risk determinant of stunting [18]. The
use of malaria control measures (LLIN and IRS) could have reduced the risk of malaria
and limited long-term development of under-nutrition.
This study had several limitations. Being a cross-sectional study design, associations
observed may have been confounded by unmeasured factors. Also, causal inferences
cannot be drawn from study findings due to the study design employed. The lack of
additional haematological assessments including mean cell volume, micronutrients and
haemolysis parameters limited the characterization of anaemia types. With regard to
under-nutrition, only weight and height measurements were collected. The lack of other
under-nutrition related data including skin fold thickness, oedema and body mass index
did not allow for a more robust nutritional assessment. In this survey, statistical
adjustments for correlation with and between HH members were conducted to ensure
study finding were robust. However, given the multi-factorial causal factors associated

123
with anaemia and under-nutrition, data on important covariates including but not limited
to helminthic infection, micronutrient levels, co-infections like HIV, genetic haemoglobin
disorders and breast feeding need to be collected in future studies to be able to perform a
more robust analysis.
Conclusion
Study findings pointed to high rates of under-nutrition and anaemia but not malaria
parasitaemia in preschool-going children. A strong association between malaria and
anaemia but not between malaria and under-nutrition was observed. Although the study
design limits the interpretation of cause and effect between these three disease
determinants, control of malaria may have a substantial indirect reduction on anaemia
burden among preschool-going children in this area. Integrated rather than vertical
programmes covering nutritional rehabilitation, malaria control including the scaled up
LLIN and IRS coverage, improvements in HH SES and better housing that limits
mosquito entry are need to realize optimal child health outputs.

124
Authors’ contributions
FK conceived the study, participated in study design, coordinated study implementation,
performed statistical analysis and drafted the manuscript. CMI participated in study
design and implementation. EH participated in design of study questionnaire and study
implementation. PK was involved in study implementation and coordinated data
management. PFM reviewed statistical analysis processes and critically reviewed the
manuscript. MPG provided guidance on the data analysis process and critically reviewed
the manuscript. LM participated in study implementation. MV participated in study
conception, participated in its implementation and helped in draft and reviewing the
manuscript. All authors read and approved the final manuscript.
Acknowledgements
We thank the Ruhuha community members, Ruhuha Health Centre leadership and the
sector leadership for their support and study participation.
Financial support
The Netherlands Organization for Tropical Scientific Research (NWO–WOTRO (AMC
Project Number SA358001) funded the study.
Competing interests
The authors have declared that they have no competing interests.

125
References
1. WHO: World Malaria Report 2013. Geneva: World Health Organization. 2013. Available
at: http://www.who.int/iris/…/9789241564694_eng.pdf. Accessed 24 Sept 2014.
2. Stevens GA, Finucane MM, De-Regil LM, Paciorek CJ, Flaxman SR, Branca F, et al.
Global regional, and national trends in hemoglobin concentration and prevalence of total
and severe anemia in children and pregnant and non-pregnant women for 1995–2011: a
systematic analysis of population representative data. Lancet Global Health 2013; 1:16-
25.
3. UNICEF: United Nations Interagency Group for Child Mortality Estimation. Levels and
trends in child mortality. 2014, New York: United Nations Children’s Fund. Available at:
http://www.childmortality.org/files_v17/download/UNICEF%202014%20IGME%20chil
d%20mortality%20Report_Final.pdf. Accessed 12 Oct 2014.
4. WHO. Guideline: Updates on the management of severe acute malnutrition in infants and
children 2012, Geneva: World Health Organization. Available at:
http://apps.who.int/iris/bitstream/10665/95584/1/9789241506328_eng.pdf. Accessed 13th
March 2014.
5. Hall A, Khanh LN, Son TH, Dung NQ, Lansdown RG, Dar DT, et al. An association
between chronic undernutrition and educational test scores in Vietnamese children. Eur J
Clin Nutr 2001; 55:801-804.
6. Grantham-McGregor S, Ani C. A review of studies on the effect of iron deficiency on
cognitive development in children. J Nutr 2001; 131:649S-666S.
7. Agarwal DK, Upadhyay SK, Agarwal KN. Influence of malnutrition on cognitive
development assessed by Piagetian tasks. Acta Paediatr Scand 1989; 78:115-122.
8. Hutchinson SE, Powell CA, Chang SPW, Grantham-Mc SM, Gregor SM. Nutrition,
anaemia, geohelminth infection and school achievement in rural Jamaican primary school
children. Eur J Clin Nutr 1997; 51:729-735.
9. Müller O, Traore C, Jahn A, Becher H. Severe anaemia in west African children: malaria
or malnutrition? Lancet 2003; 361:86-87.
10. Best C, Neufingerl N, van Geel L, van den Briel T, Osendarp S. The nutritional status of
school-aged children: why should we care? Food Nutr Bull 2010; 31:400-417.
11. Menendez C, Fleming AF, Alonso PL. Malaria-related anaemia. Parasitol Today. 2000;

126
16:469-476.
12. Kabatereine NB, Brooker S, Koukounari A, Kazibwe F, Tukahebwa EM, Fleming FM, et
al. Impact of a national helminth control programme on infection and morbidity in
Ugandan schoolchildren. Bull World Health Organ 2007; 85:91-99.
13. Morris CR, Singer ST, Walters MC. Clinical hemoglobinopathies: iron, lungs and new
blood. Curr Opin Hematol 2006; 13:407-418.
14. Wambua S, Mwangi TW, Kortok M, Uyoga SM, Macharia AW, Mwacharo JK, et al. The
effect of thalassaemia on the incidence of malaria and other diseases in children living on
the coast of Kenya. PLoS Med. 2006; 3:e158.
15. Ehrhardt S, Burchard GD, Mantel C, Cramer JP, Kaiser S, Kubo M, et al. Malaria,
anemia, and malnutrition in children—defining intervention priorities. J Infect Dis 2006;
194:108-114.
16. Green H, Sousa-Figueiredo J, Basáñez M, Betson M, Kabatereine NB, Fenwick A, et al.
Anaemia in Ugandan preschool-aged children: the relative contribution of intestinal
parasites and malaria. Parasitology 2011; 138:1534-1545.
17. Mockenhaupt FP, Ehrhardt S, Burkhardt J, Bosomtwe SY, Laryea S, Anemana SD, et al.
Manifestation and outcome of severe malaria in children in northern Ghana. Am J Trop
Med Hyg 2004; 71:167-172.
18. Deen JL, Walraven GE, von Seidlein L. Increased risk for malaria in chronically
malnourished children under 5 years of age in rural Gambia. J Trop Pediatr 2002; 48:78.
19. Friedman JF, Kwena AM, Mirel LB, Kariuki SK, Terlouw DJ, Phillips-Howard PA, et al.
Malaria and nutritional status among pre-school children: results from cross-sectional
surveys in western Kenya. Am J Trop Med Hyg 2005; 73:698-704.
20. Snow RW, Byass P, Shenton FC. The relationship between anthropometric
measurements and measurements of iron status and susceptibility to malaria in Gambian
children. Trans R Soc Trop Med Hyg 1991; 85:584-589.
21. Nyakeriga AM, Troye-Blomberg M, Chemtai AK, Marsh K, Williams TN. Malaria and
nutritional status in children living on the coast of Kenya. Am J Clin Nutr 2004; 80:1604-
1610.
22. Bayley NB. Scales of Infant Development. 2nd ed. PsychCorp Harcourt Assessment, Inc.,
San Antonio; 1993.

127
23. Bradley-Moore AM, Greenwood BM, Bradley AK, Kirkwood BR, Gilles HM. Malaria
chemoprophylaxis with chloroquine in young Nigerian children. III. Its effect on nutrition.
Ann Trop Med Parasitol 1985; 79:575-584.
24. Ter Kuile FO, Terlouw DJ, Kariuki SK, Phillips-Howard PA, Mirel LB, Hawley WA, et
al. Impact of permethrin-treated bed nets on malaria, anemia, and growth in infants in an
area of intense perennial malaria transmission in western Kenya. Am J Trop Med Hyg
2003; 68:68-77.
25. Rulisa S, Kateera F, Bizimana JP, Agaba S, Dukuzumuremyi J, Baas L, et al. Malaria
prevalence, spatial clustering and risk factors in a low endemic area of eastern Rwanda: a
cross sectional study. PLoS One 2013; 8:e69443.
26. Kateera F, Mens PF, Hakizimana E, Ingabire CM, Muragijemariya L, Karinda P, et al.
Malaria parasite carriage and risk determinants in a rural population: a malariometric
survey in Rwanda. Malar J 2015; 14:16.
27. Hartung C, Anokwa Y, Brunette W, Lerel A, Tseng C, Boriello G. Open Data Kit: tools
to build information services for developing regions. Information and Communication
Technologies and Development (ICTD). 2010. London, UK. Available at:
http://opendatakit.org/wp-content/uploads/2010/10/ODK-Paper-ICTD-2010.pdf. Accessed
12 Aug 2014.
28. Stoltzfus RJ. Rethinking anaemia surveillance. Lancet 1997; 349:1764-1766.
29. WHO. Global Database on Child Growth and Malnutrition. 2006. Geneva: World Health
Organization. Available at: http://www.who.int/nutgrowthdb/en/. Accessed 13 Nov 2014.
30. Yvas S, Kumaranayake L. Constructing socio-economic status indices: how to use
principal components analysis. Health Policy Plan 2006; 21:459-468.
31. National Institute of Statistics of Rwanda: Rwanda Demographic Health Survey. 2010.
Available at: http://dhsprogram.com/pubs/pdf/FR259/FR259.pdf. Accessed 11 Nov 2014.
32. Winskill P, Rowland M, Mtove G, Malima RC, Kirby MJ. Malaria risk factors in north-
east Tanzania. Malar J 2011; 10:98.
33. Smith T, Hii JL, Genton B, Müller I, Booth M, Gibson N, et al. Associations of peak
shifts in age-prevalence for human malarias with bednet coverage. Trans R Soc Trop Med
Hyg 2001; 95:1-6.
34. Luckner D, Lell B, Greve B, Lehman LG, Schmidt-Ott RJ, Matousek P, et al. No

128
influence of socioeconomic factors on severe malarial anaemia, hyperparasitaemia or
reinfection. Trans R Soc Trop Med Hyg 1998; 92:478-481.
35. Osterbauer B, Kapisi J, Bigira V, Mwangwa F, Kinara S, Kamya MR, et al. Factors
associated with malaria parasitaemia, malnutrition, and anaemia among HIV-exposed and
unexposed Ugandan infants: a cross-sectional survey. Malar J 2012; 11:432.
36. Yé Y, Hoshen M, Louis V, Séraphin S, Traoré I, Sauerborn R. Housing conditions and
Plasmodium falciparum infection: protective effect of iron-sheet roofed houses. Malar J
2006; 5:8.
37. Koram KA, Bennett S, Adiamah JH, Greenwood BM. Socio-economic risk factors for
malaria in a peri-urban area of The Gambia. Trans R Soc Trop Med Hyg 1995; 89:146-
150.
38. Tshikuka JG, Scott ME, Gray-Donald K, Kalumba ON. Multiple infection with
Plasmodium and helminths in communities of low and relatively high socio-economic
status. Ann Trop Med Parasitol 1996; 90:277-293.
39. Messina JP, Taylor SM, Meshnick SR, Linke AM, Tshefu AK, Atua B, et al. Population,
behavioural and environmental drivers of malaria prevalence in the Democratic Republic
of Congo. Malar J 2011; 10:161.
40. Atieli H, Menya D, Githeko A, Scott T. House design modifications reduce indoor
resting malaria vector densities in rice irrigation scheme area in western Kenya. Malar J
2009; 8:108.
41. Kirby MJ, Green C, Milligan PM, Sismanidis C, Jasseh M, Conway DJ, et al. Risk
factors for house-entry by malaria vectors in a rural town and satellite villages in The
Gambia. Malar J 2008; 7:2.
42. Harbison JE, Mathenge EM, Misiani GO, Mukabana WR, Day JF. A simple method for
sampling indoor-resting malaria mosquitoes Anopheles gambiae and Anopheles funestus
(Diptera: Culicidae) in Africa. J Med Entomol 2006; 43:473-479.
43. Lwetoijera DW, Kiware SS, Mageni ZD, Dongus S, Harris C, Devine GJ et al.. A need
for better housing to further reduce indoor malaria transmission in areas with high bed net
coverage. Parasit Vectors 2013; 6:57.
44. McElroy PD, ter Kuile FO, Lal AA, Bloland PB, Hawley WA, Oloo AJ, et al. Effect of
Plasmodium falciparum parasitemia density on hemoglobin concentrations among full-

129
term, normal birth weight children in western Kenya, IV. The Asembo Bay Cohort
Project. Am J Trop Med Hyg 2000; 62:504-512.
45. Bloland PB, Boriga DA, Ruebush TK, McCormick JB, Roberts JM, Oloo AJ, et al.
Longitudinal cohort study of the epidemiology of malaria infections in an area of intense
malaria transmission II. Descriptive epidemiology of malaria infection and disease among
children. Am J Trop Med Hyg 1999; 60:641-648.
46. Korenromp EL, Armstrong-Schellenberg JR, Williams BG, Nahlen BL, Snow RW.
Impact of malaria control on childhood anaemia in Africa—a quantitative review. Trop
Med Int Health 2004; 9:1050-1065.
47. Mathanga DP, Campbell CH, Vanden J, Wolkon EA, Bronzan RN, Malenga GJ, et al.
Comparison of anaemia and parasitaemia as indicators of malaria control in household and
EPI-health facility surveys in Malawi. Malar J 2010; 9:107.
48. Knoblauch AM, Winkler MS, Archer C, Divall MJ, Owuor M, Yapo RM, et al. The
epidemiology of malaria and anaemia in the Bonikro mining area, central Côte d’Ivoire.
Malar J 2014; 13:194.
49. Müller O, Garenne M, Kouyate B, Becher H. The association between protein-energy
malnutrition, malaria morbidity and all-cause mortality in West African children. Trop
Med Int Health 2003; 8:507-511.
50. Medhin G, Hanlon C, Dewey M, Alem A, Tesfaye F, Worku B, et al. Prevalence and
predictors of undernutrition among infants aged six and twelve months in Butajira,
Ethiopia: the P-MaMiE birth cohort. BMC Public Health 2010; 10:27.
51. Wamani H, Astrom AN, Peterson S, Tumwine JK, Tylleskär T. Boys are more stunted
than girls in sub-Saharan Africa: a meta-analysis of 16 demographic and health surveys.
BMC Pediatr 2007; 7:17.
52. Deribew A, Alemseged F, Tessema F, Sena L, Birhanu Z, Zeynudin A, et al. Malaria and
under-nutrition: a community based study among under-five children at risk of malaria,
south-west Ethiopia. PLoS One 2010; 5:e10775.

130
CHAPTER 6
Long-lasting insecticidal net source, ownership and use in the context of
universal coverage: a household survey in eastern Rwanda.
Fredrick Kateera1,2*, Chantal M. Ingabire1, Emmanuel Hakizimana3, Alexis
Rulisa4, Parfait Karinda1, Martin P. Grobusch2, Leon Mutesa5, Michèle van
Vugt2, Petra F. Mens2,6
1Medical Research Centre Division, Rwanda Biomedical Centre, Kigali, Rwanda, 2Division of Internal Medicine, Department of Infectious Diseases, Centre of Tropical
Medicine and Travel Medicine, Academic Medical Centre, Meibergdreef 9, Amsterdam,
1100 DE, The Netherlands, 3Malaria and Other Parasitic Diseases Division, Rwanda Biomedical Centre, Kigali,
Rwanda, 4Department of Cultural Anthropology and Development Studies and Centre for
International Development Issues, Radboud University, Nijmegen, 6500 HE, The
Netherlands, 5College of Medicine and Health Sciences, University of Rwanda, Kigali, Rwanda, 6Royal Tropical Institute/Koninklijk Instituut voor de Tropen, KIT Biomedical Research,
Meibergdreef 39, Amsterdam, 1105 AZ, The Netherlands
Published in: Malaria Journal 2015, 5:14(1): 440.

131
Abstract
Background
Universal long-lasting insecticidal net (LLIN) coverage (ULC) has reduced malaria
morbidity and mortality across Africa. Although information is available on bed net use
in specific groups, such as pregnant women and children under 5 years, there is paucity
of data on their use among the general population. Bed net source, ownership and
determinants of use among individuals from households in an eastern Rwanda
community 8 months after a ULC were characterized.
Methods
Using household-based, interviewer-administered questionnaires and interviewer-direct
observations, data on bed net source, ownership and key determinants of net use,
including demographics, socio-economic status indicators, house structure characteristics,
as well as of bed net quantity, type and integrity, were collected from 1400 randomly
selected households. Univariate and mixed effects logistic regression modelling was done
to assess for determinants of bed net use.
Results
A total of 1410 households and 6598 individuals were included in the study. Overall, the
proportion of households with at least one net was 92 % while bed net usage was reported
among 72 % of household members. Of the households surveyed, a total ownership of
2768 nets was reported, of which about 96 % were reportedly LLINs received from the
ULC. By interviewer-physical observation, 88 % of the nets owned were of the LLIN
type with the remaining 12 % did not carry any mark to enable type recognition. The
odds of bed net use were significantly lower among males and individuals: from
households of low socio-economic status, from households with <two bed nets, from
households reporting use of ≥two sleeping spaces, and those reporting to have not slept
on a bed.

132
Conclusion
In this study, despite high a bed net coverage, over 25 % of members reported not to have
slept under a bed net the night before the survey. Males were particularly less likely to
use bed nets even where nets were available. Household socio-economic status, number
of bed nets and type and number of sleeping spaces were key determinants of bed net use.
To maximize impact of ULC, strategies that target males as well as those that ensure ITN
coverage for all, address barriers to feasible and convenient bed net use including
covering over all sleeping space types, and provide net hanging supports, are needed.

133
Background
Insecticide-treated bed nets (ITNs) are a cornerstone of malaria control in sub-Saharan
Africa [1, 2]. The World Health Organization (WHO) recommends universal access to,
and use of long-lasting insecticidal nets (LLINs) for all individuals at risk of malaria so
as to optimize ITN effectiveness [3]. ITNs act by placing a physical barrier between the
mosquito and humans and through the repellent toxic effects of the ITN-impregnated
insecticides. ITNs have been shown to reduce malaria burden at both individual and
community level leading to decreased morbidity, mortality and overall transmission
potential [1, 4, 5]. With ITNs also shown to be the most cost-effective intervention in
reducing malaria transmission [6], universal long-lasting insecticidal net coverage (ULC)
has been recommended and is now widely implemented as a key intervention in malaria
control efforts [7].
The impact of LLIN scale-up on reducing malaria burden has been observed in Rwanda
[8]. With financial support mainly from The Global Fund to Fight AIDS, Tuberculosis
and Malaria and the President’s Malaria Initiative, Rwanda achieved ULC—defined as a
reported household ownership of at least one bed net per two individuals, as early as
February 2011 [9]. However, despite the observed initial decline in health facility-
recorded malaria cases and deaths following LLIN scale-up in Rwanda, increases in
malaria burden continue to be reported [8, 10-11]. While the resurgence in 2009 was
mainly attributed to a reduced effectiveness of LLINs due to delays in provision of new
nets at a time when the effectiveness of the previously provided LLINs was waning [10],
later resurgence may have been partly associated with the reported deployment of bed
nets with sub-optimal concentrations of insecticide [11]. However, although the reasons
for the resurgence were not systematically characterized, continued scale-up and use of
LLINs is needed if gains made in malaria burden decline in the past are to be sustained
[10]. To achieve and maintain ULC, Rwanda adopted the WHO’s recommendations for
high malaria burden countries of using multiple distribution channels, including free
ULCs that are supplemented by continuous LLIN distributions through programmes such
as antenatal care (ANC) and immunization services for pregnant women and infants,
respectively [3, 9].

134
A key determinant of ITN impact is bed net use, with previous studies showing
disparities between bed net ownership and use [12–17]. One such determinant of bed net
use is seasonality. While higher net use has been reported more in the rainy season due to
the associated high mosquito density, lower net use has been associated with hot dry
months due to heat-related discomfort [12, 14]. Other previously reported determinants of
net use include number of nets owned per household, sex: with women more likely to use
nets [15], age [15], head of household (HoH) education levels, disruptive sleeping
arrangements [16], and net misuse such as bed nets being used for activities in agriculture
and fishing [17]. Hitherto, studies on bed net use have mostly focused on
children <5 years and pregnant women, two groups preferentially targeted for net
coverage in the past because of their high malaria risk. There is limited and inconclusive
data on ITN effectiveness under routine field settings after ULC targeting of all age and
gender groups. Understanding these household-level bed net use patterns is needed to
inform malaria control programmes on how to optimize bed net public health impact.
Here, a community-based evaluation of bed net source, ownership and determinants of
use was conducted 8 months after ULC.
Methods
Study area description and malaria risk
This cross-sectional survey was conducted among a representative sample of households
randomly selected from 35 villages of a rural, predominantly agricultural, Ruhuha sector
of Bugesera District in the eastern province of Rwanda from November 2014 to January
2015. Rwanda is broadly divided into four malaria ecologic zones based on altitude,
climate, level of transmission, and disease vector prevalence [18]. Topographically,
malaria transmission is considered meso-endemic in the plain regions of eastern and
southern provinces while being epidemic-prone in the high plateau and hill settings of
northern and western provinces, respectively [18]. Ruhuha sector is a rural agricultural
community that is located in the high malaria transmission zone. The main malaria
control interventions used in the study area include ULC, indoor residual spraying (IRS)
with insecticide and use of artemisinin combination therapy (ACT).

135
Study population and eligibility criteria
This study is part of a larger project that aims to use an integrated (biomedical,
anthropological, entomological, and economical), community-based approach targeting
reduction of malaria transmission at household level [19]. A sample of 1400 households
was randomly selected from a sampling frame of 4522 sector households generated
2 months prior to the survey as part of an enumeration exercise conducted while planning
for IRS exercise for the sector. To identify the randomly selected households for study
inclusion, study team members visited a particular village and identified the households
by the named HoH on the enumeration sheet. This study and the associated follow-up
procedures were then introduced to the HoH or their spouses who were then requested to
provide a written informed consent before enrolment. Data on household members
aged >6 months and who had spent the night prior to the survey at the household were
collected. A household was defined as any unit headed by a male or female with his/her
dependents and/or spouse who shared a cooking pot/common eating-place.
Study questionnaire and variables definitions
A pre-coded questionnaire, that was largely adapted from the standard malaria indicator
survey (MIS) and the demographic health survey (DHS), was administered to the HoH or
their spouse [20]. Data on demographics (age, sex, education level, occupation, and
marital status), household socio-economic status (SES) indicators (including ownership
of land and animals, main sources of household amenities (including lighting, cooking
and drinking water), ownership of items (such as telephone, television, refrigerator,
bicycle and radio), house structural features (such as type of material used to construct
house wall and floor), malaria prevention knowledge and practices, bed net
characteristics (of ownership, source and use), and IRS activity within 12 months prior to
survey, were collected. In addition, a spot check was performed to verify bed net number,
brand, shape and integrity (having holes or no holes). A bed net was classified as having
holes if it had any finger-sized hole or larger. In this study, three degrees of severity of
net deterioration including finger size, fist size and head size were assessed for.

136
Data collection
Field workers were trained for 10 days on key survey aspects of study objectives,
variable data to be collected and question intent. Additionally, classroom role-plays and
piloting of questionnaires were conducted, with daily feedback reviews conducted to
ensure consistency of translation and appropriateness of the wording in the local language
(Kinyarwanda). Although the questionnaire was developed in English and data captured
onto an English language electronic format, both the training and data collection exercise
were conducted using paper-based questionnaires that were translated into Kinyarwanda.
The electronic format questionnaire was developed using Open Data Kit (ODK) Collect
set-up [21]. ODK is an open-source suite of tools that include ODK Collect, an android-
based mobile client that acts as the interface between the user and the underlying form
used to collect data [21]. The collected data were then electronically uploaded onto a
central server and later exported into Microsoft Excel 2007 version (Microsoft Corp) for
further analysis.
Bed net distribution
Between January 2012 and December 2014, nets were distributed in the study area using
multiple channels, including a ULC targeting the general population, mass distribution of
bed nets for all children aged <5 years, and continuous distribution through ANC and
immunization services. Prior to the ULC, community health care workers (CHWs)
enumerated each household for type and number of sleeping spaces and number of bed
nets available. Among the general population, 5600 LLINs were distributed in May 2012
and an additional 4550 distributed in May 2013 to achieve complete coverage of all
sleeping spaces. However, following these two rounds of net distribution, the LLIN brand
(Netprotect®) provided was later confirmed impregnated with sub-optimal amounts of the
insecticide [11]. This led to a replacement exercise conducted in March 2014 where
10,150 LLINs were distributed to replace the sub-standard LLINs (Mukamana, pers
comm). Concurrently, three supplementary distribution campaigns were run in which
3283 LLINs were distributed to cover children aged <5 years in 2012, 540 LLINs
distributed to pregnant women through the ANC between 2012 and 2014, and 1295
LLINs distributed through the immunization service to cover infants.

137
Ethical approval
Study protocols received ethical and scientific approval from the National Health
Research Committee (NHRC) and the Rwanda National Ethics Committee (No.
20/RNEC/2015), Kigali, Rwanda.
Statistical analysis
Data analysis was performed using STATA version 13.0 (STATA Corp., College Station,
TX, USA) software. Descriptive statistics of frequencies, proportions, cross tabulations
with crude Pearson’s Chi square tests between outcome and dependent variables were
performed. The primary outcome was bed net use—defined as a reported history of
sleeping under a bed net the night before the survey. Independent covariates reported by
other studies as associated with net use, including but not limited to, age, sex, HoH
education level at individual level and number of ITNs, number of residents per
household and SES levels at household level were analysed individually for an
association with bed net use. All variables that showed evidence for a possible
association with bed net use (p value < 0.1) were then included in the final mixed effect
logistic regression model. This model was chosen to ensure adjustment for individual
intra-cluster and household inter-cluster correlation. The risk of no bed net use under
final multivariate model was considered significant for variables with an effect with a P
value ≤0.05 based on Wald tests.
Generating household-level socio-economic status (SES) scores
Measures of household wealth can be reflected by income, consumption or expenditure-
related indicator information. To generate household-level SES scores using principal
component analysis (PCA) as described elsewhere [22], [23], 17 indicators were used: (1)
any household member ownership of television (yes/no), radio (yes/no), bicycle (yes/no),
and telephone (yes/no); (2) HoH ownership of house lived in (yes, no—pay rent, no—use
without paying rent); (3) type of sources for: (a) lighting (electricity, kerosene, oil, gas or
paraffin lamps, solar, firewood, candles/battery/flash lights, others), (b) cooking
(electricity, biogas/LPG/natural gas, paraffin, charcoal, firewood/straw, others), (c)
domestic water (private connection to pipeline, public well, borehole, harvested rain

138
water, river, stream, lake, or other surface water, public tap, public tap/standpipe, bottled
water, others), and (d) toilet (flash toilet, pit latrine, ventilated improved pit (VIP) latrine,
no facility/bush/field); (4) material used to construct: (a) house walls (burnt bricks,
cement/concrete blocks, adobe/un-burnt bricks, mud/poles, others) and (b) house floors
(carpet, parquet, polished wood, mosaic or tiles, cement/concrete, bricks, clay/earth,
dung/sand); (5) HoH enrolment into any health insurance (yes/no); (6) HoH membership
into an economic group (yes/no); (7) ability of HoH to save any money in past 3 months
(yes/no); (8) ability of HoH to pay for medical services (yes/no) and ability of HoH to
pay for medications prescribed (yes/no); and, (9) highest level of HoH education (none,
primary, secondary, tertiary). Other SES indicator variables for whom data was collected
but that had a frequency of <1 % were omitted due to their low ability to differentiate
between households. The PCA derived scores were considered as weight (eigenvectors of
the correlation matrix) for each variable and the sum of the weights per household
considered as the household level SES score. The scores were then ranked in terciles with
the highest 33 % of household considered high SES, the lowest 33 % as low SES and the
rest as middle SES [23].
Results
Baseline household characteristics
Of the pre-selected 1410 households, six were unoccupied as household members were
reported to have moved out of the sector, six HoH did not provide study consent, ten did
not have an eligible person to be interviewed, and 23 households could not be identified
because the residents did not know the named HoH. For all omitted households, the
nearest household in the same village was identified as a replacement.
Data collected covered 1400 households and 6598 individuals of whom the mean (±SD)
age was 22.9 (±18.3), 3282 (53.3 %) were female, 582 (9.0 %) were children <5 years.
The mean (±SD) number of household members was 4.7 (±1.9) (Table 1).

139
Table 1. Household (N = 1410) socio-demographic and house structural features, Ruhuha
sector, Rwanda, 2015
Variable name Variable groups Frequency - n (%)Sex of head of household (HoH) Male 1,021 (72.4)
Female 389 (27.6)Age of HoH in years Mean (± SD) 44.7 (± 1 4.5)*Highest educational level attained by HoH None 415 (29.4)
Primary school 790 (56.0)Post primary/vocational 36 (2.6)Secondary or higher 169 (12.0)
Marital status of HoH Never married 46 (3.3)Married 654 (46.4)Living together 319 (22.6)Separated/Divorced 108 (7.6)Widowed 283 (20.1)
Household (HH) member size Mean (± SD) 4.69 (± 1.9)*Proportion of HoH with no formal education None 415 (29.4)HH socio-economic status (SES) score Low 470 (33.4)
Middle 470 (33.4)High 468 (33.2)
Does the HH own the house currently lived in? Yes 1,250 (88.8)No 158 (11.2)
Type of sleeping spaces used in HH Beds 1,819 (62.9)Floor 1,075 (37.1)
Average number sleeping spaces in HH visited Mean (± SD) 2.17 (± 0.9)*Number of sleeping spaces per HH 1 294 (20.9)
2 697 (49.5)3 339 (24.0)≥ 4 79 (5.6)
Average number of rooms in household visited Mean (± SD)* 2.96 (±1.2)Number of rooms in house lived in 1 141 (10.1)
2 250 (17.7)3 738 (52.4)4 175 (12.4)≥5 105 (7.4)
Number of windows in the house lived in 0-2 419 (29.7)≥3 991 (70.1)
Did the house have a ceiling? Yes 101 (7.1)
* Standard deviations

140
The majority (70.9 %) of households had permanent (bricks/cement) wall structures
whilst the others households had walls made of temporary (mud and poles) materials.
Only 7.1 % and 8.9 % of the households had permanent structured walls and ceilings,
structures beneath the roof where bed nets are usually hung, respectively (Table 1).
Two types of sleeping space were identified including a raised up platform (bed) and
floor-based spaces. The majority (although not quantified in this study) of the floor-based
spaces (although not quantified in this study) were fixed and consistently used spaces,
where a mattress or other beddings were placed on the floor. The majority (70.3 %) of the
households reported using ≥ two sleeping places while the commonest type of sleeping
space used was a bed (62.9 %) (Table 1). By households SES levels, the proportions of
bed net use among individuals of low, middle and high SES households were 56.5, 64.3
and 65.4 %, respectively.
Bed net ownership, source and integrity
A majority of 91.7 % households reported owning at least one bed net with a total
ownership of 2769 nets reported (1.96 nets/HH). Of the total nets, 86.2 % were reported
not frequently in use, with commonest reasons for not using these nets including not
needed or lack of where to hang them or not easy to use them due to shape and/or
distance between point of hanging and levels of bedding. The majority (95.6 %) of nets
were received through the ULC with the others either purchased (n = 19), or received
from family members (n = 28) or received from the ANC and immunization clinics
(n = 75). By on-spot study interviewer observations on net integrity and brand type, 344
(12.9 %) of the nets had at least one hole (of any size) while a total of 2281 (87.9 %) nets
were identified as LLINs (Tuzanet, Mamanet and PermaNet ® ) while the remaining
12.1 % were found not to carry any mark to enable brand/type recognition, respectively.
Details of net source, ownership and integrity are reported in Table 2.

141
Table 2. Bed net source, ownership and use, Ruhuha Sector, Rwanda, 2015
Variable Variable groups Frequency n (%)Bed net ownership per HH Number of HHs with at least one bed net 1,292 (91.7)
Number of HHs without any bed net 118 (8.3)Bed net source From government through mass LLIN campaigns 2,647 (95.6)
From government through ANC and EPI clinics 75 (2.7)Privately purchased 19 (0.7)Provided for by family/relatives 28 (1.0)
Number of bed nets ownership per HH 1 326 (23.3)2 595 (42.6)3 275 (11.7)≥ 4 96 (6.8)
No responses 104 (7.4)Total number of nets owned in HHs visited N 2,768Number of nets used night before the survey n (%) 2,386 (86.2)Mean number of bed nets per HH Mean (± SD) 2.1 (± 0.3)*Mean number of sleeping spaces (N = 6,603) Mean (± SD) (2.1 ± 0.9)*Ratio of bed nets per sleeping space Mean (± SD) 1.0 (± 0.4)*Number of persons who slept under net n (%) 3,525 (72.3)Number of bed net used by sex Female 1,895 (72.9)
Male 1,630 (71.6)Number of bed net used by age group <5 years 432 (74.9)
5-15 years 810 (68.9)>15 years 3,523 (73.1)
Number of bed net used by sleeping space type Slept on beds 1,387 (81.6)
Slept with no beds 576 (64.2)Bed net integrity: presence and size of holes Number of nets with no hole 2,425 (87.7)
Number of nets with at least one finger size hole 200 (7.2)Number of nets with at least one hand size hole 81 (2.9)Number of nets with at least one head size hole 62 (2.2)
*: Standard deviations

142
Individual net use
Overall, 72.3 % individuals reported use of a bed net the night before survey with
females (72.9 %) reporting a slightly higher proportion compared to males (71.6 %). By
age group, 5–15 year olds reported a lower net use (68.9 %) relative to children <5 years
(74.9 %) and persons aged ≥16 years (73.1 %), respectively (Table 2). Notably, net use
was much higher for individuals who slept on a bed (81.6 %) compared to 64.2 % those
who reported sleeping on a mattress placed on the floor (Table 2). In 53.9 % of the
household, at least one person did not sleep on a permanent bed but used a sleeping place
laid on the ground. However, because individual level data on type of sleeping space used
night before survey were not collected, it was impossible to directly assess the association
between bed net use and type of sleeping space. In total, 13.8 % of the nets were
reportedly not in frequent use although owned, with the commonest reasons as reported
by interviewees but not verified by study team, for not using a bed net being the
discomfort associated the hot season period (38.9 %), infestation with bed bugs that was
associated with use of bed nets (18.3 %), no particular reason (6.6 %), net being damaged
(2.6 %), and no need to use a bed net as after a recent IRS activity (2.4 %).
Determinants of net use
Based on univariate analysis, a strong relation was found between net use and house
structure characteristics. Persons living in houses with walls made of brick/cement blocks
had a 2.4-fold higher odds of net use relative to persons living in houses with walls were
made of mud and poles. In addition, the number of doors and windows a house had
influenced bed net use by univariate analysis. Individuals from houses with ≥two doors
and those from houses with ≥three windows had six- and fourfold more odds of bed net
use than individuals with <two and <three doors and windows, respectively. Univariate
results are shown in Table 3. However, for both number of doors and number of windows
variables, this effect did not retain significance after adjusting for all the other
determinants in the final model.

143
Table 3 Logistic regression analysis of determinants of bed net use among individuals
(n = 6,598) from households with ≥one net Ruhuha sector, Rwanda, 2015.
CI: Confidence interval Ref: Reference
VariableVariableSub-group
Univariate OR (95% CI), P value
Multivariate OR (95% CI), P value
SexFemale (ref.) - -Male 0.57 (0.44-0.74), <0.0001 0.42 (0.28-0.64), <0.0001
Age group of all HH members in years
0-5 years (ref.) - -6-15 0.38 (0.23-0.63), <0.0001 0.197 (0.01-3.01), 0.243>15 0.86 (0.54-1.36), 0.510 0.35 (0.03-4.69), 0.431
Age group of HoH in years.
18-30 (ref.) - -31-55 0.93 (0.42-2.07), 0.852 -56 + 0.36 (0.14-0.96), 0.042 -
Education level of HoH Any vs. none (ref.) 2.53 (1.29-4.96), 0.007 0.86 (0.38-1.94), 0.720
Household SES score level
Low (ref.) - -Middle 1.95 (0.92-4.12), 0.079 2.26 (1.06-4.82), <0.0001Upper 1.88 (0.89 -3.97), 0.099 2.92 (1.31– 6.46), < 0.0001
Number of members per HH
1-3 (ref.) - -4-6 0.38 (0.19-0.76), 0.006 0.73 (0.33-1.62), 0.4327+ 0.68 (0.27-1.67), 0.398 1.86 (0.59-5.89), 0.291
Slept on a bed last night? Yes vs. No (ref.) 5.24 (3.15-8.72), <0.0001 3.01 (1.79-5.08), <0.0001
Number of sleeping space used in HH
1 (reference) - -2 1.02 (0.86-1.22), 0.790 0.34 (0.12-0.99), 0.0483 1.32 (1.08-1.61), 0.007 0.11 (0.03-0.40), 0.0014+ 1.67 (1.23 -2.27), <0.0001 0.07 (0.01-0.49), 0.007
Does ITN have any holes? Yes vs. No (ref.) 0.26 (0.11-0.58), 0.001 0.53 (0.23-1.18), 0.119
Number of rooms per HH
1 (ref.) - -2 14.49 (3.30-63.64), <0.0001 2.43 (0.60-9.84), 0.2143+ 22.91 (5.96–88.01), <0.0001 2.14 (0.49-9.35), 0.313
Number of doors per HH
1 (ref.) -2 5.26 (2.28-12.11), <0.0001 2.42 (0.84-6.98), 0.1023+ 8.55 (2.15-34.02), 0.002 1.22 (0.23-6.64), 0.817
Number of windows per HH
1 (ref.) - -2 3.44 (0.70-16.83), 0.127 3.32 (0.82-13.42), 0.0923 10.74 (2.41-47.79), 0.002 1.81 (0.45-7.28), 0.4064+ 6.74 (1.24-36.72), 0.027 1.11 (0.19-6.38), 0.908
Number of bed nets used per HH
1 (ref.) - -2 7.10 (4.08-12.33), <0.0001 4.72 (2.08-10.72), <0.00013 12.18 (5.88-25.23), <0.0001 16.83 (5.42-52.24), <0.00014+ 40.32 (8.11-200.51), <0.0001 110.15 (11.99-1012.17), <0.0001

144
By univariate analysis, nets with holes were significantly less used than nets without
holes (OR = 0.26, P = 0.001). However, this significance was not sustained after
adjusting for other variables in the final multivariate model (Table 3). Variables,
including a reported history of a family member experiencing a febrile illness in the past
3 months, IRS application, bed net age, HoH education, household size, houses with
ceilings or houses having eaves, did not influence net use in this study.
In the final multivariate model, only five of the 13 explanatory variables including sex,
household level SES level, type and number of sleeping arrangements and the number of
bed nets owned showed significantly effect on bed net use (Table 3). Males showed 0.4
[95 % CI: 0.28–0.64] times lower odds of sleeping under a net compared to females.
Also, individuals living in households of middle/high SES showed twofold higher odds
of net use compared to those living in household low SES household.
Sleeping on a bed was associated with three-fold higher odds of net use (95 % CI: 1.79–
5.08) compared to not sleeping on a bed. Although a reported ownership of ≥two ITNs on
the night before the survey was associated with higher odds of net use in general, bed net
use was also influenced by the number of sleeping places in a house. Persons from
households that reported using ≥two-sleeping spaces the night before the survey were
associated with higher odds of net use compared to household that had only one sleeping
space. Multivariate results are shown in Table 3.
Discussion
This study demonstrated a 92 % household ownership with at least one net and a 72 %
bed nets use among 1400 households visited. Particularly among men, and in households
of the low SES group with ≥two sleeping places, where individuals reported not sleeping
on a bed, with a reported ownership of only one bed net, lower odds of net use were
observed. Also, higher odds of net use with increasing number of nets in household were
observed.

145
Comparable to the 92 % household bed net ownership in this study, high coverage rates
have been reported elsewhere following UCL, including Sierra Leone (87.6 %), Togo
(96.7 %) and Ethiopia (91.0 %) [24-26]. Similarly as shown in this study, bed net use in
these three settings was lower than bed net coverage, varying from 65.0 % in Ethiopia to
68.3 % in Togo and 76.5 % in Sierra Leone. This finding highlights a major need to
supplement ULC with appropriate effective strategies that promote bed net use.
As observed in this study, previous studies have shown that females were more likely to
use bed nets relative to males [27–29]. A possible reason for the sex disparity in net use
could be the traditionally high focus on promoting net use among females through health
centres and ANC-based campaigns to target reduction of malaria risk for vulnerable
pregnant women. This focus may have spilled over into higher rates of net use among
females even in settings of ULC and in spite of the observed lower likelihood of net use
amongst men. However, the specific reasons for low rates of net use among men were not
explored in this study. Characterizing these reasons is key to identifying implementation
gaps and targeting strategies towards promoting net use specifically among men.
In this study, individuals who reported not to have slept on a bed had lower odds of net
use compared to those who slept on beds. In one study in Kenya conducted before and
after a ULC, lower odds by 0.24 and 0.31-fold decrease among individuals who reported
sleeping on the floor compared to those who slept on a bed was observed [30]. In this
same study, sleeping on the floor was almost fully associated with not using a net [30].
Possible reasons for lower compliance to bed net use among those not sleeping on a bed
range from practical house structural challenges, including difficulty in spreading a net
over a sleeping material or a mattress, lack of a suitable structure for net hanging and
disruptive sleeping arrangements that complicate ease of bed net use [16], [31]. Although
not studied here, it is plausible that bed net use is particularly difficult among those who
did not sleep on a bed as the sleeping spaces are generally larger, irregular and much
further from the point of net hanging and hence less amenable to feasible bed net use. In
this study, 93 % of the houses visited had no ceiling, structures onto which nets are
usually hung. It is plausible that lack of a place to hang or a need to improvise, such as by

146
tying a long string from wall to wall onto which a net can be secured and as well as
difficulty in securing net around floor-based sleeping arrangements, are some reasons for
reduced likelihood of bed net use. Bed net hanging increases likelihood of bed net use
[32]. Further characterization of feasibility of bed net hanging and convenience of net use
among those who do not sleep on a bed is needed to promote bed net use in this group. .
Households with ≥two sleeping spaces were associated with lower odds of net use. Given
the bed net to household ratio of almost 2:1 (2769 bed nets for 1410 households) in the
study area, it is likely, although not specifically assessed in this study, that households
with more sleeping places did not have enough bed nets to cover each sleeping space. In
this study, a progressive increase in odds of net use proportional to number of used nets
the night before the survey was observed. Comparable findings to this study have been
reported elsewhere. In Ethiopia, a household level net density of >one net per two people
was associated with a fivefold (in 2006) and a twofold (in 2007) higher net use when
compared to households with net densities of <one net per two persons [32]. In Sierra
Leone, a ULC was associated with a 137 % increase in bed net use within 6 months [24].
In Uganda, following a ULC, LLIN availability was the only determinant of bed net use
[31]. This is plausible in this study area where there is a discrepancy between mean of
household members size (4.7) and mean number of available nets (2.1), which is lower
than the target of having one net per two household occupants. Therefore, since a greater
intra-household access to an ITN is a strong determinant of net use, efforts to increase
access to enough bed nets, particularly in households with many members, is required. To
further increase net use among all age and gender sub-groups, net distribution campaigns
should target coverage of at least of all sleeping spaces and ideally coverage of two nets
per three persons or even one net per person.
Medium and high SES group households were associated with higher odds of bed net use
in this study. Similar to findings in this study, higher net use amongst households with
higher SES has been reported previously in Uganda [33], and in Ethiopia [34]. A possible
reason for this observation may be that individuals from medium and high SES
households have better information on access and capacity to buy supplementary LLINs

147
and hence are more likely to use bed nets. Interestingly, associations between household
SES and net use have been reported with mixed outcomes. In a smaller, prospective,
hospital-based study in Nigeria, household SES did not influence bed net use [35]. In
contrast, Auta et al. in a study based on data extracted from a demographic and health
survey exercise in Nigeria found higher rates of net use among individuals from the
lowest wealth quintile [36]. In the latter study, higher rates of net used was associated
partly with a higher perception of malaria risk in the poorest settings that may have arisen
from more concerted public health campaigns conducted in the area [36]. On the
contrary, higher SES group households may have greater access to more nets or more
favourable factors that enhance adherence to net use.
The methodology employed and study findings had major strengths. Interviewer-spot
checks in assessing bed net ownership, integrity and brand as well as verifying house
structural feature characteristics limited potential recall and socio-desirability bias. In
addition, both the interview questions used that were adapted from the standardized MIS
and DHS tools and the quantitative analysis employed served to optimize study accuracy.
This study evaluated for a key outcome of bed net use in a setting of high net coverage
and hence provided rich data on the effectiveness of a UCL in a real community setting.
The methodology used in this study had some limitations. Firstly, the decision to replace
the 35 non-enrolled houses randomly selected households with nearest neighbour
households may have had an effect on representativeness of the study findings. This most
likely did no affect accuracy of study findings given that the proportion of replaced
households was <2.5 % of total sample size. Secondly, this being a cross-sectional
survey, study findings may be confounded by unmeasured factors, not be suitable for
drawing causal inferences, and not be appropriate for showing how net ownership and
use may vary over time. A possible social desirability bias of over-reporting may also
have influenced rates of reported net ownership and use. In addition, the study area has
had many bed net campaigns that may have positively influenced knowledge and
attitudes on malaria prevention and in particular, led to higher rates of net use. Study
findings may not be representative of low malaria endemic settings with low bed net
coverage and limited awareness of bed net use. Given that this survey covered a

148
relatively limited area, findings may not be generalizable to the entire country and more
so in settings when ULC were not conducted.
Conclusion
Bed net ownership of ≥one net among households visited and a reported individual use
among household members of 92% and 72 % was observed in the study area. This study
confirmed that males in general and individuals from households of low SES, with one or
more nets, where ≥two sleeping spaces are used, and those who slept on the floor relative
to those who used beds, were less likely to use a net. Supplementary to LLIN scale-up
campaigns, strategies to promote bed net use, particularly among males and houses with
structural features that prevent mosquito entry and those that adapt bed net feasibility
towards ease of use in groups such as those who do not sleep on a bed, are needed. Also,
further studies on feasibility and cost-effectiveness research of ULC, as well as in-depth
anthropological studies characterizing bed net use patterns, including reasons for lower
net use among males, perceptions on bed net hanging, net characteristics that may lead to
reduced bed net use, such as dirtiness, smells, shape, and colour and challenges of net use
among those do not sleep on beds, would provide rich contextual data to inform future
strategies aimed at improved net use.

149
Authors’ contributions
FK conceived the study, supervised the fieldwork, analysed the data and drafted the
manuscript. CMI was involved in study conception and study implementation. EH and
AL were both involved in developing study tools, training field interviewers and study
implementation. MPG provided guidance on the manuscript draft. LM was involved in
study implementation and critically reviewed draft manuscript. MvV was involved in
study conception and provided input on draft manuscript preparation. PFM prepared data
collection tools, provided guidance on data analysis and interpretation and substantially
revised the manuscript. All authors read and approved the final manuscript.
Acknowledgements
We thank Ruhuha sector households and their members who participated in this study,
the area CHWs and the leadership of Ruhuha Health Centre for their partnership. The
Netherlands Organization for Scientific Research (NWO-WOTRO) funded this work
(Grant: AMC A1050243). Florance Mukamana provided data on bed nets distributed.
Compliance with ethical guidelines
Competing interests The authors declare that they have no competing interests.

150
References
1. Lengeler C. Insecticide-treated bed nets and curtains for preventing malaria.
Cochrane Database Syst Rev 2004; 2:CD000363.
2. Alonso PL, Armstrong JR, Lindsay SW. Malaria, bed nets, and mortality. Lancet
1991; 338:897.
3. WHO. WHO recommendations for achieving universal coverage with long-lasting
insecticidal nets in malaria control. World Health Organization, Geneva. 2014.
Available at:
http://www.who.int/malaria/publications/atoz/who_recommendations_universal_cover
age_llins.pdf. Accessed 13 April 2015.
4. Hawley WA, Phillips-Howard PA, Kuile FO, Terlouw DJ, Vulule JM, Ombok M, et
al. Community-wide effects of permethrin-treated bed nets on child mortality and
malaria morbidity in western Kenya. Am J Trop Med Hyg 2003; 68:121-127.
5. Eisele TP, Steketee RW. African malaria control programs deliver ITNs and achieve
what the clinical trials predicted. PLoS Med 2011; 8:e1001088.
6. WHO Global Malaria Programme. A WHO Position statement on ITNs. Available at:
http://www.ivcc.com/sites/ivcc.mrmdev.co.uk/files/content/itnspospaperfinal.pdf.
Accessed 11 April 2015.
7. Teklehaimanot A, Sachs JD, Curtis C. Malaria control needs mass distribution of
insecticidal bednets. Lancet 2007; 369:2143-2146.
8. Otten M, Aregawi M, Were W, Karema C, Medin A, Bekele W, et al. Initial evidence
of reduction of malaria cases and deaths in Rwanda and Ethiopia due to rapid scale-up
of malaria prevention and treatment. Malar J 2009; 8:14.
9. President’s Malaria Initiative. Rwanda malaria operational plan FY 2014. Available
at: http://www.pmi.gov/docs/default-source/default-document-library/malaria-
operational-plans/fy14/rwanda_mop_fy14.pdf?sfvrsn=8. Accessed 23rd May 2015.
10. Karema C, Aregawi MW, Rukundo A, Kabayiza A, Mulindahabi M, Fall IS, et al.
Trends in malaria cases, hospital admissions and deaths following scale-up of anti-
malarial interventions, 2000–2010, Rwanda. Malar J 2012; 11:236.
11. Binagwaho A, Karema C. A call for international accountability—preserving hope
amid false protection. Lancet Glob Health 2015; 3:e188-e189.

151
12. Binka FN, Adongo P. Acceptability and use of insecticide impregnated bednets in
northern Ghana. Trop Med Int Health 1997; 2:499-507.
13. Thwing J, Hochberg N, Vanden Eng J, Issifi S, Eliades MJ, Minkoulou E, et al.
Insecticide-treated net ownership and usage in Niger after a nationwide integrated
campaign. Trop Med Int Health 2008; 13:827-834.
14. Korenromp EL, Miller J, Cibulskis RE, Kabir Cham M, Alnwick D, Dye C.
Monitoring mosquito net coverage for malaria control in Africa: possession vs. use by
children under 5 years. Trop Med Int Health 2003; 8:693-703.
15. Baume CA, Marin MC. Intra-household mosquito net use in Ethiopia, Ghana, Mali,
Nigeria, Senegal, and Zambia: are nets being used? Who in the household uses them?
Am J Trop Med Hyg 2007; 77:963-971.
16. Alaii JA, Hawley WA, Kolczak MS, ter Kuile FO, Gimnig JE, Vulule JM, et al.
Factors affecting use of permethrin-treated bed nets during a randomized controlled
trial in western Kenya. Am J Trop Med Hyg 2003; 68:137-141.
17. Ingabire C, Rulisa A, Van Kempen L, Muvunyi C, Koenraadt C, Van Vugt M, et al.
Factors impeding the acceptability and use of malaria preventive measures:
implications for malaria elimination in eastern Rwanda. Malar J 2015; 14:136.
18. PMI/MOH-Rwanda. President’s malaria initiative Rwanda malaria operational plan
FY. 2015. Available at: http://www.pmi.gov/docs/default-source/default-document-
library/malaria-operational-plans/fy-15/fy-2015-rwanda-malaria-operational-
plan.pdf?sfvrsn=3. Accessed 22 Sep 2015.
19. Rulisa S, Kateera F, Bizimana JP, Agaba S, Dukuzumuremyi J, Mens Petra F, et al.
Malaria prevalence, spatial clustering and risk factors in a low endemic area of eastern
Rwanda: a cross sectional study. PLoS One 2013; 8:e69443.
20. USAID. The DHS program, demographic and health surveys. Available at:
http://www.dhsprogram.com. Accessed 24 May 2015.
21. Raja A, Tridane A, Gaffar A, Lindquist T, Pribadi K. Android and ODK based data
collection framework to aid in epidemiological analysis. Online J Public Health
Inform 2014; 5:228.
22. Vyas S, Kumaranayake L. Constructing socio-economic status indices: how to use
principal components analysis. Health Policy Plan 2006; 21:459-468.

152
23. Filmer D, Pritchett LH. Estimating wealth effect without expenditure data or tears: an
application to educational enrollments in states of India. Demography 2001; 38:115-
132.
24. Bennett A, Smith SJ, Yambasu S, Jambai A, Alemu W, Kabano A, et al. Household
possession and use of insecticide-treated mosquito nets in Sierra Leone 6 months after
a national mass-distribution campaign. PLoS One 2012; 7:e37927.
25. Stevens ER, Aldridge A, Degbey Y, Pignandi A, Dorkenoo MA, Hugelen-Padin J.
Evaluation of the 2011 long-lasting, insecticide-treated net distribution for universal
coverage in Togo. Malar J 2013; 12:162.
26. Baume CA, Reithinger R, Woldehanna S. Factors associated with use and non-use of
mosquito nets owned in Oromia and Amhara regional states, Ethiopia. Malar J 2009;
8:264.
27. Wanzira H, Yeka A, Kigozi R, Rubahika D, Nasr S, Sserwanga A, et al. Long-lasting
insecticide-treated bed net ownership and use among children under 5 years of age
following a targeted distribution in central Uganda. Malar J 2014; 13:185.
28. Ter Kuile FO, Terlouw DJ, Phillips-Howard PA, Hawley WA, Friedman JF, Kolczak
WS, et al. Impact of permethrin-treated bed nets on malaria and all-cause morbidity in
young children in an area of intense perennial malaria transmission in western Kenya:
cross-sectional survey. Am J Trop Med Hyg 2003; 68:100-107.
29. Garley AE, Ivanovich E, Eckert E, Negroustoueva S, Yazoume Y. Gender differences
in the use of insecticide-treated nets after a universal free distribution campaign in
Kano State, Nigeria: post-campaign survey results. Malar J 2013; 12:119.
30. Larson PS, Minakawa N, Dida GO, Njenga SM, Ionides EL, Wilson ML. Insecticide-
treated net use before and after mass distribution in a fishing community along Lake
Victoria, Kenya: successes and unavoidable pitfalls. Malar J 2014; 13:466.
31. Iwashita H, Dida G, Futami K, Sonye G, Kaneko S, Horio M, et al. Sleeping
arrangement and house structure affect bed net use in villages along Lake Victoria.
Malar J 2010; 9:176.
32. Graves PM, Ngondi JM, Hwang J, Getachew A, Gebre T, Mosher AW, et al. Factors
associated with mosquito net use by individuals in households owning nets in
Ethiopia. Malar J 2011; 10:354.

153
33. Njau JD, Stephenson R, Menon M, Kachur SP, McFarland DA. Exploring the impact
of targeted distribution of free bed nets on households bed net ownership, socio-
economic disparities and childhood malaria infection rates: analysis of national
malaria survey data from three sub-Saharan Africa countries. Malar J 2013; 12:245.
34. Sena LD, Deressa WA, Ali AA. Predictors of long-lasting insecticide-treated bed net
ownership and utilization: evidence from community-based cross-sectional
comparative study, Southwest Ethiopia. Malar J 2013; 12:406.
35. Edelu BO, Ikefuna AN, Emodi JI, Adimora GN. Awareness and use of insecticide-
treated bed nets among children attending outpatient clinic at UNTH, Enugu—the
need for an effective mobilization process. Afr Health Sci 2010; 10:117-119.
36. Auta A. Demographic factors associated with insecticide treated net use among
Nigerian women and children. N Am J Med Sci 2012; 4:40-44.

154
CHAPTER 7
Malaria Prevalence, Spatial Clustering and Risk Factors in a Low
Endemic Area of Eastern Rwanda: A Cross Sectional Study
Stephen Rulisa1, 2,3*, Fredrick Kateera2, 4*#, Jean Pierre Bizimana5, Steven
Agaba3, Javier Dukuzumuremyi3, Lisette Baas3, Jean de Dieu
Harelimana3, Petra F. Mens2, 3, 6, Kimberly R. Boer3, 6, Peter J. de Vries2, 3,7
*These Authors equally contributed to this manuscript and share first Authorship
1 University Teaching Hospital of Kigali, National University of Rwanda, Kigali,
Rwanda, 2 Academic Medical Center, Division of Infectious Diseases, Tropical Medicine and
AIDS, Amsterdam, The Netherlands, 3 Amsterdam Institute for Global Health and Development, INTERACT Project, Kigali,
Rwanda, 4 Medical Research Centre, Rwanda Biomedical Centre, Kigali, Rwanda, 5 Geography Department, Faculty of Science, National University of Rwanda, Huye,
Rwanda, 6 Royal Tropical Institute/Koninklijk Instituutvoor de Tropen (KIT), KIT Biomedical
Research, Amsterdam, The Netherlands, 7 Department of Internal Medicine, Tergooiziekenhuizen, Hilversum, The Netherland
Published in: PLoS One. 2013; 23: 8(7): e69443.

155
Abstract
Background
Rwanda reported significant reductions in malaria burden following scale up of control
intervention from 2005 to 2010. This study sought to; measure malaria prevalence,
describe spatial malaria clustering and investigate for malaria risk factors among health-
centre-presumed malaria cases and their household members in Eastern Rwanda.
Methods
A two-stage health centre and household-based survey was conducted in Ruhuha sector,
Eastern Rwanda from April to October 2011. At the health centre, data, including malaria
diagnosis and individual level malaria risk factors, was collected. At households of these
Index cases, a follow-up survey, including malaria screening for all household members
and collecting household level malaria risk factor data, was conducted.
Results
Malaria prevalence among health centre attendees was 22.8%. At the household level, 90
households (out of 520) had at least one malaria-infected member and the overall malaria
prevalence for the 2634 household members screened was 5.1%. Among health centre
attendees, the age group 5–15 years was significantly associated with an increased
malaria risk and a reported ownership of ≥4 bednets was significantly associated with a
reduced malaria risk. At the household level, age groups 5–15 and >15 years and being
associated with a malaria positive index case were associated with an increased malaria
risk, while an observed ownership of ≥4 bednets was associated with a malaria risk-
protective effect. Significant spatial malaria clustering among household cases with
clusters located close to water- based agro-ecosystems was observed.
Conclusions
Malaria prevalence was significantly higher among health centre attendees and their
household members in an area with significant household spatial malaria clustering.
Circle surveillance involving passive case finding at health centres and proactive case

156
detection in households can be a powerful tool for identifying household level malaria
burden, risk factors and clustering.

157
Introduction
From 2005 to 2010, Rwanda achieved the 2005 global community commitment of
reducing the malaria burden by at least 50% [1]. During this period, a rapid malaria
assessment conducted at 30 out of 40 Hospitals in Rwanda showed reductions of; 74%
among confirmed outpatients cases of all ages, 26% in slide positivity rates, 65% among
inpatients of all ages, and 55% in malaria deaths [2]. These gains followed rapid scale-up
of insecticide-treated mosquito nets (ITNs), indoor residual spraying (IRS), use of
artemisinin combination therapies (ACTs) and laboratory confirmation of presumed
malaria cases with microscopy (at health facilities) and rapid diagnostic tests (RDTs) (by
community health workers) as recommended by WHO’s Roll Back Malaria program [1].
Despite these gains, malaria still causes significant morbidity; 7.8% of all febrile patients
presenting at the health centre (HC) had malaria and 12.9% of all age mortality were
malaria associated in 2010, with a malaria resurgence recorded in 2009 [2-4].
These observations highlight the fragility of gains in malaria reduction achieved,
especially in areas with a high baseline malaria transmission potential.
Current anecdotal Rwandan national routine data suggests a heterogeneous spatial
malaria distribution with the entire population remaining at risk with the exception of the
very high altitude zones [3, 5]. Malaria heterogeneity has been reported across the
different malaria endemic settings and has been attributed to risk factors including
altitude, climate, occupation and socio-economic status [6-10]. However, at all malaria
endemicity levels, and particularly in low incidence areas, malaria tends to cluster in
‘hotspots’ and ‘hot’ populations that become sources of continued infection.
We defined a ‘hotspot’ of malaria transmission as ‘a geographical part of a focus of
malaria transmission where transmission intensity exceeds the average level [11]. In a
community, asymptomatic and minimally symptomatic malaria cases, whose symptoms
may not be severe enough to seek care, can serve as significant parasite reservoirs for
maintaining transmission [7, 8, 12]. Active and timely identification of these hotspots and
associated risk factors is essential for targeting interventions to optimize malaria control
[13].

158
Risk factors associated with malaria clustering for which we also investigated include
distance of households (HHs) from potential mosquito-breeding sites, house roofing and
wall materials and bednet use [7]. In Rwanda, however, there is paucity of systematic HH
studies on malaria burden or associated risk factors with most reported data being
aggregated routine health facility data. Despite its tendency to underestimate malaria
burden, routine data can be helpful in reflecting malaria trends [14], particularly in low
malaria incidence settings where the majority of the population access health services
from the reporting health facilities. The passively identified health facility cases may
reflect area malaria transmission levels in places where malaria cases tend to cluster in
time and place. Index cases may also act as entry points to community HHs where
identification of hotspots that could be targeted for optimal malaria control. Malaria
hotspots may serve to perpetuate residual malaria transmission in low transmission
seasons and hinder efforts to eliminate malaria [15].
In this study, we used HC attendees with presumed malaria as entry points for reactive
case identification of malaria infections at the HH level. In a two-phase health facility
and HH cross-sectional survey, we employed circle surveillance technique to measure
malaria burden and evaluate for associated malaria risk factors. We also investigated for
spatial malaria clustering using geographical information system (GIS) and spatial
statistical techniques [16-18].
Materials and Methods
Ethical Statement
Ethical approval was granted by Rwanda National Ethics Committee. Prior to study
initiation, sector and community leaders were informed about the study and their support
and verbal consent requested. Written consents were obtained from adult participants and
parents/guardians of participating children and from heads of HHs or the oldest person
present for the HH surveys.

159
Study area
The complete survey was conducted in Ruhuha Sector, Bugesera district [19], Eastern
Rwanda (Figure1). The sector covers 54 km2, has a population of about 19,606 persons
living in 4279 HHs. It is predominantly rural and traditionally a high malaria endemic
area. Ruhuha sector, surrounded by lowland marshes and water-streams draining into the
Akagera River System, is separated from Burundiby Lake Cyohoha in the south.
Fig 1. Location of Ruhuha Sector (Red), Bugesera District (Grey) in
Rwanda
Source: MINITRACO/CGIS-NUR, 2001 and NISR 2006.
Study Design and Participants
A two-phase cross-sectional survey was conducted between April and October 2011.
First, a fever survey was conducted among patients presenting at Ruhuha Health Centre
(RHC) with a fever or history of fever in the last 24 hours. Patients of all ages were
recruited and after signing the informed consent form, malaria diagnosis by microscopy
and individual level risk factor data were collected. Thereafter, study participants were
invited to participate in a follow-up HH survey where HH level malaria risk factor data

160
was collected and malaria screening for all HH members performed.
Study Procedures
Health centre (HC) fever survey
At the HC, an interviewer-administered questionnaire, adapted from the Measures group
Demographic Health Surveys tools and previous studies [20, 21], was administered to
adult patients or, in the case of minors, to parents/guardians of the children. Study-trained
personnel administered the pre-tested questionnaire. Data collected included personal
demographics, fever characteristics, malaria perception, knowledge and practices
including malaria preventive measures, and house structural features (walls and roofs).
Preparation of blood films, microscopic examination and quality assurance
To identify malaria among HC attendees, Giemsa stained thick and thin blood films were
prepared and read by two independent experienced microscopists at the RHC laboratory.
A third microscopist based at National Reference Laboratory (NRL) settled discrepancies
between two readings. Parasite negative results were based on screening of 100
microscopic fields at 1000x magnification. Malaria parasites were counted against 200
white blood cells on thick blood films for enumeration of parasite density and thin smears
used for species identification. In addition, 10% of all microscopy slides were sent to the
NRL for external quality control.
Household survey
HC-recruited study participants (regardless of their malaria diagnosis status) who
consented to a home visit and provided HH locator information were visited 1 to 4
months later for a follow-up HH survey. At this visit, all HHs were enumerated and
assigned a unique identification number. An interviewer-administered questionnaire was
used to collect data on HH level malaria risk factor characteristics including, bednet
availability, type, integrity and use, HH water sources and environmental factors.
Rapid diagnostic test (RDT) screening
In addition to the questionnaire data, all HH members were screened for presence of

161
malaria parasites to measure asymptomatic or minimally symptomatic parasitaemia
prevalence using RDTs (First Response® Combo Malaria Ag (pLDH/HRP2) card test,
Premier Medical Corporation Ltd, India). If HH members were not at home at the time
of the survey, they were actively sought out and subsequently screened by the field team.
RDTs were performed according to the manufacturer’s instruction by trained field team
members. All RDTs used were from one batch that was directly obtained through the
manufacturer and stored according to the manufacturer’s recommendations. However, no
external quality control was done on these RDTs. Follow-up confirmatory microscopy
was provided at the Ruhuha HC for all RDT-positive individuals to confirm accuracy and
inform a malaria treatment decision.
Mapping households and geographical features
GIS was used to capture, manage and geographically integrate data from different
sources. Location data for each HH and key geographical feature was collected using a
handheld GPS receiver, GPSMAP 60CSx (Garmin etrex legend®, Garmin International
Inc. USA). Digitized data from pre-existing shapefiles provided base layers (topography,
land use, rivers and surface water) on which study data was overlaid into one geo-
database compatible with ArcGIS10. Boundaries shapefiles of administrative units
(“cells”), wetlands, water bodies and the elevation contour lines for Ruhuha sector were
obtained from the GIS Remote Sensing Training and Research Centre of the National
University of Rwanda.
Statistical analysis
Statistical analysis was performed using STATA software (version 12, College Station,
TX, USA). Univariate analysis to assess for malaria risk for all variables was done using
logistic regression and variables with possible malaria risk (p<0.2) were included in the
initial multivariate logistic regression model. HH data was analyzed using generalized
estimating equation (GEE) models with adjustment for HH level malaria case clustering.
The level of significance for study statistics was p>0.05 and Wald tests were used to
quantify variable effects in the model. Possible interaction effects were also assessed for.

162
Spatial clustering
The Kulldorff spatial scan statistic, using SaTScanTM version 9.1.1 software
(http://satscan.org), was used to test for spatial clustering of malaria cases and/or to
determine whether the cases were distributed randomly over space [Kulldorff &
Nagarwalla. [1995]]. HHs, used as the unit of analysis, were located using the Cartesian
coordinate system to specify coordinates with the maximum spatial cluster size set at
50% of the population at risk. As in other studies, SatScan generated circular windows of
different sizes for detecting clustering [22, 23]. The number of cases in each window was
compared to the expected number of cases based on the total number of cases and
population size. We used purely spatial analyses based on the Bernoulli probability
model that is appropriate for 0/1 event data such as cases/controls. The controls
represented the background distribution population. The P-value was obtained from a
likelihood ratio test based on Monte Carlo simulation replications of the data set. Spatial
scans were performed for both HC attendee and HH member cases. A HC case was
defined as being microscopy positive with HC controls defined if they were microscopy
negative; a HH member was defined as being a case if they were identified as RDT
positive with HH controls defined if they were RDT negative.
Results
In total, 769 HC attendees who presented with fever or with a history of fever in last 24
hours at the outpatient clinic were screened. Of the 769; 175 (22.8%) were diagnosed
with malaria, 458 (59.6%) were female, 277 (36.0%) were aged <5 years, 147 (19.1%)
aged 5–15 years and 345 (44.9) aged >15 years. A flow chart of study participant
enrolment, malaria screening and participation is shown in Figure 2. HH visits were
planned for all 769 HC attendees. However, because of the long period between HC case
enrolment and HH survey (1–4 months versus the planned 2–4 weeks) and the inaccurate
location data reported by study participants, the HH survey was not conducted in HHs of
200 index participants. Among HC attendees, malaria prevalence was comparable
between those whose HH were not visited (30.5% (CI. 23.4–38.4) and those visited.

163
Figure 2. Flow chart of study participant enrolment, malaria screening and
participation in a two-phase survey.
Of the 557 (72.4%) surveyed HHs, 520 HHs had complete data. Only data from these 520
HHs were analysed. In total, 2634 HH members were screened for malaria. Of the 2634,
599 (22.2%) were aged <6 years, 763 (28.3%) aged 6 to 15 years and 1331 (49.4%) aged
>15 years. Only 90 (17.3%) HHs had at least one member diagnosed with malaria and the
overall malaria prevalence (RDT confirmed) was 5.1% (95% CI 4.34–6.03). All visited
HHs had ≥1 bednet and in total, 873 bed nets were observed. HH bednet and indoor
residual spraying coverage by self-report were 97.1% and 98.2%, respectively. Basic

164
knowledge about malaria was high, with 696 (91%) reporting bed nets as the principle
malaria preventive measure while 748 (97.3%) reported that fever was the principal
malaria symptom. Interestingly, 447 (82.5%) of HHs visited had bednets in their
possession but these were not physically hung (Table 1).
Table 1. Reported and observed bednet characteristics.
Characteristics of bed nets as reported by HC attendees. Characteristics of bed nets observed during
house hold visits (n = 557 HHs)
Reported Malaria preventive
measures used.
Are bednets in your HH
treated? n (%)
How many holes are in
your bed nets? n (%)
Observed No (%) of
hanged bed nets
Observed No (%) of
Bednet in HH
Bed Nets
Clear bushes
No protection
Others
Missing
696 (82.6)
66 (7.8)
64(7.6)
11 (1.3)
6 (0.7)
No
yes
Don’t know
Missing
21 (2.92)
615 (85.65)
55 (7.66)
27 (3.76)
No Holes
1-10 holes
> 10 holes
Missing
649 (91.28)
31 (4.36)
4 (0.56)
27 (3.80)
None
One
> 1
447 (82.47)
93 (17.16)
2(0.37)
0
1
2
≥ 3
Missing
88 (11.4)
279 (36.3)
240 (31.2)
134 (17.4)
28 (3.7)
Univariate Analysis
Results of univariate analysis for individual and HH (after adjusting for possible house-
level clustering of cases) risk factors are displayed in Tables 2 and 3, respectively.
Malaria risk among HC attendees was associated with both age and reported bednet
ownership. Compared to children ≤5 years, malaria prevalence was three times higher in
the 6–15 year olds while a reported ownership of ≥4 bednets was associated with a
significant protective effect. HC attendees were evaluated for symptoms predictive of
having clinical malaria. Having a measured fever (≥37.5°C) at presentation was
associated with higher odds of malaria risk than no fever. Similar to HC cases, malaria
risk among their HH members was significantly associated with age and observed bednet
coverage. Additionally, HH members living in houses made of wood/mud/tent, when
compared to those HH members living in dwellings whose walls were made of stone or
bricks, and HH ownership of an in-house open water vessel were associated with higher
odds of malaria

Tab
le 2
. Hea
lth fa
cilit
y at
tend
ee c
hara
cter
istic
s and
mal
aria
ris
k fa
ctor
s.
Bas
elin
e C
hara
cter
istic
s N
(%)
HC
at
tend
ees
with
M
alar
ia (n
=175
) (%
)H
C a
tten
dees
with
No
Mal
aria
(n=5
84) (
%)
Uni
vari
ate
Ana
lysi
suO
R (9
5% C
I),
P-va
lue
Mul
tivar
iate
Ana
lysi
saO
R (9
5% C
I), P
-val
ueIn
divi
dual
var
iabl
esA
ge g
roup
<
5 ye
ars
5-1
5ye
ars
>15
year
s
277
(36.
02)
147
(19.
12)
345
(44.
86)
57(3
2.6)
57(3
2.6)
61 (3
4.8)
220
(37.
0)80
(13.
5)28
4(49
.5)
1.0
2.44
4 (1
.572
-3.8
01),
< 0.
0001
0.82
9 (0
.555
-1.2
39),
0.36
1.0
3.02
(1.8
90-4
.824
), <
0.00
01
1.02
7 (0
.663
-1.5
91),
0.90
6G
ende
rM
ale
Fem
ale
311
(40.
44)
458
(59.
56)
73(4
1.7)
102
(58.
3)23
8(40
.1)
356(
59.9
)0.
934
(0.6
63-1
.316
), 0.
696
1.0
----
----
---
Mal
aria
Exp
erie
nce
Mea
sure
d T
emp
at H
C<
37.5˚ C
≥ 37
.5˚ C
381(
49.5
)38
8 (5
0.5)
69(3
9.4)
106(
60.6
)31
2(52
.5)
282(
47.5
)1.
01.
700
(1.2
06-2
.396
), 0.
002
1.0
1.63
6 (1
.119
-2.3
92),
0.01
1W
hen
did
feve
r ep
isod
e st
art
Toda
yY
este
rday
D
ay
befo
re
yeste
rday
Lo
ng a
go
47
(6.1
1)49
4 (6
4.24
)16
2 (2
1.07
)66
(8.5
8)
10(5
.7)
109(
62.3
)46
(26.
3)10
(5.7
)
37(6
.2)
385(
64.8
)11
6(19
.5)
56(9
.5)
1.0
1.04
8 (0
.505
-2.1
74),
0.90
1 1.
467
(0.6
74-3
.193
), 0.
334
0.66
1 (0
.250
-1.7
43),
0.40
2 --
----
----
---
Mal
aria
ep
isod
es
in
past
12
m
onth
sN
one
1-3
epis
odes
>3 e
piso
des
520
(67.
62)
232
(30.
17)
17 (2
.21)
105
64 6
415
168
11
1.0
1.50
6 (1
.052
-2.1
56),
0.02
52.
156
(0.7
80-5
.964
), 0.
139
----
----
----
--1.
408
(0.9
59-2
.068
), 0.
081
2.16
3 (0
.737
-6.3
46),
0.16
0M
alar
ia p
reve
ntio
nD
oes H
H o
wn ≥
1 be
d ne
tY
esN
o74
2 (9
6.61
)26
(3.
39)
167
857
518
0.65
3 (0
.279
-1.5
30),
0.32
7 1.
0--
----
----
--R
epor
ted
No
of b
ed n
ets i
n H
HO
neTw
oTh
ree
≥ 4
88
(11.
88)
279
(37.
65)
240
(32.
39)
134
(18.
08)
24 65 59 19
64 214
181
115
1.0
0.81
0 (0
.470
-1.3
97),
0.44
9 0.
869
(0.5
00-1
.512
), 0.
620
0.44
1 (0
.224
-0.8
65),
0.01
7
1.0
0.6
54 (0
.372
-1.1
50),
0.14
10.
687
(0.3
86-1
.220
), 0.
200
0.35
2 (0
.175
-0.7
07),
0.00
3

166
Table 3. Household characteristics and malaria Risk factors
Multivariate Analysis
VariablesFrequency (%)
HH with ≥ 1 malaria case
HH with No malaria case
UnivariateOR (95% CI) - P value
MultivariateOR (95% CI) -P value
Gender of HH membersFemaleMale
1167(44.3)1467 (55.7)
6466
1,0911,408
1.247 (0.894- 1.740), 0.194 1.0
1.191 (0.852-1.667),0.3061.0
Age Group0-5 years6-15 years≥ 16 years
589 (22.40) 742(28.22) 1,298 (49.37)
267133
5636711,265
1.02.398 (1.528-3.766), <0.00010.586 (0.350-0 .982), 0.042
1.02.437 (1.543-3.847),<0.0001 0.584 (0.344-0.992), 0.047
HH member associatedwith
Negative Index casePositive Index case
2,047 (77.86) 582 (22.14)
7753
1,970529
1.02.557(1.608-4.066),< 0.0001
1.01.267 (1.068-1.503), 0.007
Bed net characteristicsObserved No of bed nets
OneTwo BednetsThree Bednets ≥ Four bednets
256 (9.77) 2,212 (84.46) 55 (2.10) 96 (3.67)
229927
2342,1135389
1.00.490 (0.204-1.179) 0.1110.526 (0.217-1.274) 0.1550.367(0.143-0.940) 0.037
1.00.456 (0.202-1.029) 0.0590.461 (0.207-1.024) 0.0570.384 (0.165-0.892) 0.026
Household structure characteristics and IRS use.House wall material
Bricks and stonesWood/mud/tent
364 (70) 156 (30)
5832
306124
1.01.324 (1.134-1.546), <0.0001
1.01.288 (1.082-1.534), 0.004
Type of HH roof material Corrugated Iron sheetsGrass thatched/tent/others
457 (87.9)63 (12.1)
7911
37852
1.00.849 (0.662-1.088), 0.196
1.00.837 (0.636-1.102), 0.204
Was IRS of HH walls done? Yes
No490 (94.4)30 (5.6)
883
40227
1.01.033 (0.742-1.435), 0.852 ------
Water source and Environmental CharacteristicsPresence of outside water source Yes
No205(36.80)352 (63.20)
4545
150280
1.00.762(0.489-1.190), 0.232 ------
Have an open water vessel in Hh Yes
No171 (32.88)349 (67.12)
3555
136294
1.00.666(0.425-1.045), 0.077
1.00.712 (0.351-1.444), 0.347
Green environment around HH? very green (grass & trees)moderate green (only grass)
no grass at all
300 (53.86)174 (31.24)83 (14.90)
47358
24412462
1.01.720 (1.076-2.750), 0.023 0.825(0.383-1.773), 0.622
1.01.412 (0 .691-2.886), 0.344 0.578 (0.218-1.528) 0.269
Economic CharacteristicsDoes your HH have Electricity Yes
No34 (6.10)523 (93.90)
486
25405
0.512(0.154-1.710), 0.2771.0
0.634 (0.248-1.617), 0.3401.0
Have Domestic Animals in HH? Yes
No376(67.50)181 (32.50)
6228
291139
0.931 (0 .564-1.537), 0.7791.0 ------

167
At the individual level, an adjusted multivariate logistic regression model showed
significantly higher odds of clinical malaria risk among children aged 5–15 years (OR =
3.02, P value <0.0001) but a protective effective was noted in those with a reported
ownership of 4 of more bed nets (OR = 0.352, P value 0.003). Having a fever (≥37.5°C)
was predictive of having clinical malaria (OR = 1.64, P value 0.011). House level malaria
risk remained significantly associated with age, type of material HH dwelling was made
of, observed bednet coverage and malaria status of index case after adjusting for malaria
case clustering in HHs (Table 3). Compared to the ≤5 year age group, malaria risk was
significantly higher among the 6–15 year age group (OR = 2.44, P-value <0.0001) but
interestingly lower, albeit with a borderline statistical significance, among the ≥16 year
age group (OR = 0.58, P-value 0.047). Living in dwellings made of wood or mud or tent
material was associated with a higher malaria risk while an observed ownership of ≥4
more bed nets was associated with a protective effect.
Malaria Clustering
Malaria positivity among HC attendees was significantly correlated with a HH having at
least one confirmed member (OR = 2.31, P = 0.001) but no spatial clustering for HC
malaria cases was observed. However, three clusters of HHs with significantly higher risk
than expected RDT tested members were identified (Table 4). These HH clusters were
located; 1. North East (radius of 2.04 Kilometers (Kms), relative risk of 3.40 and P value
0.0001), 2. South (radius of 0.51 Kms, relative risk of 5.6, (P value 0.0001), and 3. A
smaller cluster (not indicated in Figure 3) of only one HH (where 4 of its members tested
RDT positive) with a relative risks of 20.8, P value 0.002 (Figure 3). Two of these
clusters (1 and 2) were located next to water-based agro-ecosystems.

Figu
re 3
. ¥ Spa
tial m
alar
ia c
lust
ers a
nd lo
catio
n of
HH
s.
(Yel
low
dot
s - c
ontro
l HH
with
no
mal
aria
infe
cted
cas
e an
d sm
all R
ed d
ots
- cas
e H
H w
ith a
t lea
st o
ne m
alar
ia in
fect
ed c
ase)
in R
uhuh
a se
ctor
. ¥ T
he u
sed
adm
inis
trat
ive
boun
dari
es a
nd g
eogr
aphi
c fe
atur
es s
hape
file
s w
ere
obta
ined
from
the
Cen
tre
for
Rese
arch
and
Tra
inin
g in
GIS
and
Rem
ote
Sens
ing
of th
e N
atio
nal U
nive
rsity
of R
wand
a.

Tab
le 4
Spa
tial c
lust
erin
g of
the
mor
e th
an e
xpec
ted
hous
ehol
d ca
ses.
Clu
ster
Yea
rN
o of
HH
s in
clus
ter
P-v
alue
Obs
erve
d N
o of
HH
cas
esE
xpec
ted
No
of C
ases
Rel
ativ
e ri
sk
120
1160
0.00
002
3814
.064
3.41
3
220
1111
0.00
015
163.
169
5.62
2
320
111
0.00
247
40.
198
20.8
08

170
Discussion
In this study, members of HHs where the index case had clinical malaria showed 1.3
times greater odds of being malaria infected compared to members of HH where the
index patient was malaria negative. Comparable findings of a greater risk for malaria
infection among HH members of a HC identified clinical malaria case have been shown
by Stresman et al. (2010) in Zambia [24]. These findings support the value of circle
surveillance as a useful tool for studying HH level malaria burden, risk factors and
clustering. In this study, slide/RDT positivity rates of 22.8% and 5.1% among HC
malaria presumed cases and HH based asymptomatic cases respectively were found. This
demonstrates that circle surveillance can show differences in HH malaria risk and
clustering, even in areas of high malaria prevalence as in Ruhuha. A part from living in a
HH where the index case had malaria, risk factor analysis identified participant’s age and
a reported ownership of a ≥4 bednet as variables that, either alone or in unison,
significantly influenced malaria risk.
Compared to children aged <5 year, older children and adults had a higher risk of parasite
carriage, for both HC attendees and HH members groups. This is in contrast to previous
findings of a higher malaria risk in children <5 years [25]. However, a shift to higher
malaria risk among older age groups has been reported after the increased coverage with
insecticide-treated bed nets and the observed follow-up reduced malaria transmission in
some communities [26-27]. The reductions in malaria transmission may decrease the risk
of malaria inoculation and infections leading to an increase in the age at which malaria
infections are first acquired. Additionally, there is a greater likelihood of younger age
groups (<5 year olds) using malaria preventive bed nets compared to their older siblings,
although this data was not collected in this study [26].
In this study, the reported and observed ownership of bed nets was associated with
significant malaria protective effect. This protective effect of insecticide-treated mosquito
net use has also been affirmed in multiple previous studies [28]. Ruhuha sector is a
traditionally high transmission setting with high bednet coverage. This high coverage
follows the government’s massive free bednet distribution after campaigns run between
2009 to 2011 in which government aimed to achieve universal bednet coverage [5, 29-

171
30]. Study Participants reported a good level of knowledge of malaria symptoms,
transmission and preventive measures with over 82% of respondents reporting use of bed
nets the night before the survey. However, in only 18% of visited HHs was a bednet
found physically hung onto a bed or a sleep space suggesting that bednet use may be sub-
optimal. Possible reasons for sub-optimal bednet use may be associated with local house
structures and/or sleeping arrangements for the HH members. Most houses in Ruhuha
have 1–2 bedrooms with limited structures on which to hang bed nets. Additionally, most
occupants share sleeping spaces on the floor. These factors may complicate use of
available bed nets and partially explain the low bednet hanging rates observed and
limited bednet protective effects in HHs with bed nets. Studies exploring how to optimise
bednet usage and effectiveness are recommended.
In this study and others, the quality of housing, apart from being an indicator of HH
economic status has been reported, to influence the ease with which mosquitoes can enter
and hide in a home and hence contribute to malaria risk [7, 31-32]. Occupants of houses
with walls made of mud/grass/wood had 1.3 times greater odds (P value 0.016) of having
at least one malaria case more than those living in houses with walls made of brick or
stone. However, interventions to address type of housing as a malaria risk factor are
complex and difficult to achieve and are rarely components of public health programs. A
current campaign in Rwanda to phase out grass-thatched houses (locally known as
“nyakatsi”) and replace them by houses made of brick and iron sheet roofs could impact
malaria transmission.
For high transmission countries where essential clinical services are adequately available,
the transition from control to elimination is recommended at SPR of <5% [12].
Achieving pre-elimination levels in Ruhuha, given current SPR of >22%, will probably
require introduction of novel area-relevant interventions to supplement existing control
tools (mainly ITNs and IRS). As malaria transmission declines, a community-based
evaluation of transmission intensity and size of infectious reservoir will be required. In
this study, malaria prevalence among HH members by RDT was 5.1%. However, since
RDTs have a lower sensitivity, as compared for example to molecular tools, the level of
true malaria infection prevalence among the predominantly asymptomatic carrier HH

172
members, may have been underestimated [33-34]. In addition, the HH survey was
conducted 1 to 4 months, rather than the planned 2–4 weeks, after the initial HC-based
fever survey. This delay may have complicated a fair comparison of malaria risk between
HC index cases and their HH members. Ruhuha sector is served by only one HC
managed primarily by community health workers with most children ≤5 years. The area
population is therefore challenged by inadequate access to health care. Consequently,
malaria data reported from this health centre may underestimate the population malaria
burden. This further complicates a fair comparison of health centre versus HH level
malaria risk [13].
Two hundred HHs could not be identified due to; wrong directions, non-existing HHs
and, possibly, out of area study participants who gave wrong data. Given the delay in the
follow-up HH surveys and the significant loss to follow-up of index cases, a repeat robust
reactive case identification study to assess for clustering, particularly in areas of lower
malaria transmission intensity is recommended [12, 15]. In this study, HH cases were
RDT confirmed while HC cases were microscopically confirmed in keeping with national
malaria guidelines. However, no quality control for used RDTs was conducted. Also,
being a cross- sectional survey, malaria burden reported could not reflect seasonal
malaria trends and prospective malaria incidence risk.
Despite study limitations above, this study showed that having malaria among HC
attendees was significantly predictive of finding at least one malaria-infected case among
his/her HH members (OR = 2.4, P value = 0.001) suggesting that HC-based passive case
identification can be a feasible entry point for identifying community hotspots of malaria
infection. Guidelines on how to manage asymptomatic and minimally symptomatic RDT
positive cases identified through active case detection are lacking and would be required
in the event that circle surveillance is implemented in the future. The currently
recommended first line treatment for uncomplicated malaria in Rwanda is Artemether –
Lumefantrine (AL). AL has anti-gametocidal effects and an ability to reduce asexual
parasitaemia levels and infectivity among malaria-infected individuals [35-37]. It is
plausible that AL can be used among asymptomatic and minimally symptomatic cases to
clear local reservoir pools and reduce their malaria transmission potential.

173
Significant spatial clustering for HH cases (but not HC cases) with the clusters located
near water-based agro-ecosystems is an interesting finding. The bigger cluster (radius of
5 km) is neighbouring marshlands where traditional rice cultivation is done (North East),
while the smaller cluster (0.5 km radius) is located between multiple water streams and
Lake Cyohoha in the south where vegetable and other agriculture crops are grown. We
speculate that these water agro-ecosystems may provide significant reservoirs for
mosquito breeding and hence increased vector intensity for malaria transmission. This
finding suggests that future malaria control efforts should consider targeting potential
breeding sites and engaging farming communities. To this end, an entomological
evaluation of mosquito breeding capacity and endemicity may guide introduction of
integrated vector management practices while community-based environmental
management approaches for malaria control, as shown to be effective in settings
comparable to Ruhuha, may be two potential effective area relevant strategies to employ
[32]. To achieve malaria pre-elimination status in Ruhuha, the bednet and IRS strategies,
which are principally used, may need to be complimented by interventions that target
area breeding sites and malaria risk factors identified through spatial clustering technique
as was done in this study may be required [12].
Conclusion
In this study, HC malaria confirmed cases were significantly associated with finding at
least one malaria-infected case among their HH members. Reactive case finding, by
linking HC-identified passive cases to actively identified HH malaria infection, is a
potentially powerful surveillance system for identifying HHs with significant malaria risk
and detecting asymptomatic carriers. Especially in low transmission settings, identifying
and treating asymptomatic carriers is key in interrupting transmission. Therefore, circle
surveillance, when combined with knowledge on the individual, the HH and the
environmental malaria risk factors in a given community, can aid detection of hotspots
and inform use of targeted malaria control strategies.

174
Author Contributions
Conceived and designed the experiments: PFM KRB PJdV. Performed the experiments:
SR SA JD JdDH LB. Analyzed the data: FK JB PFM PJdV. Wrote the paper: FK JB
PFM KRB PJdV.
Funding
This study was funded by Netherlands-African partnership for capacity development and
clinical interventions against poverty-related diseases (NACCAP) through the Infectious
diseases Network for Treatment and Research in Africa (INTERACT) - programme
(Rwanda/Uganda) URL: http://www.nwo.nl/nwohome.nsf/pages/NWOA
_6LRD4R_Eng. The funders had no role in study design, data collection and analysis,
decision to publish, or preparation of the manuscript.
Competing interests
All authors have declared: no support from any organization for this submitted work; no
financial relationships with any organizations with possible interest in work submitted
work; no other relationships or activities that could possibly influence this submitted
work.

175
References
1. Roll Back Malaria Partnership. Global Strategic Plan, 2005–2015. Available:
http://www.rollbackmalaria.org/forumV/do cs/gsp_en.pdf. Accessed May 15th 2012.
2. WHO: World malaria report 2011. Available:
http://www.who.int/malaria/world_malaria _report_2011/9789241564403_eng.pdf.
Accessed May 13th 2012.
3. President’s Malaria Initiative (PMI). Malaria Operational Plan: Rwanda FY 2012.
Washington, DC: PMI, 2011. Available: http://www.pmi.gov/countries/mops/fy12/r
wanda_mop_fy12.pdf. Accessed May 15th 2012.
4. Ministry of Health, Health sector strategic plan, July 2009-June 2012. 2009; pp. 82,
Kigali, Rwanda.
5. Karema C, Aregawi M, Rukundo A, Kabayiza A, Mulindahabi M, et al. Trends in
malaria cases, hospital admissions and deaths following scale-up of anti-malarial
interventions, 2000–2010, Rwanda. Malaria Journal 2012; 11: 236.
6. Martens W. Climate change and malaria: exploring the risks. Med War 1995; 11:
202–213.
7. Bousema T, Drakeley C, Gesase S, Hashim R, Magesa S, et al. Identification of hot
spots of malaria transmission for targeted malaria control. J Infect Dis 2010; 201:
1764–1774.
8. Greenwood BM. The microepidemiology of malaria and its importance to malaria
control. Trans R Soc Trop Med Hyg 1989; 83: 25–29.
9. Greenwood BM, Bradley AK, Greenwood AM, Byass P, Jammeh K, et al. Mortality
and morbidity from malaria among children in a rural area of The Gambia, West
Africa. Trans R Soc Trop Med Hyg 1987; 81: 478–486.
10. Clark TD, Greenhouse B, Njama-Meya D, Nzarubara B, Maiteki-Sebuguzi C, et al.
Factors Determining the Heterogeneity of Malaria Incidence in Children in Kampala,
Uganda. J Infect Dis 2008; 198: 393–400.
11. Bousema T, Griffin JT, Sauerwein RW, Smith DL, Churcher TS, et al. Hitting
Hotspots: Spatial Targeting of Malaria for Control and Elimination. PLoS Med 2012;
9(1): e1001165.
12. Baliraine FN, Afrane YA, Amenya DA, Bonizzoni M, Menge DM, et al. High
Prevalence of Asymptomatic Plasmodium falciparum Infections in a Highland Area

176
of Western Kenya: a Cohort Study. J Infect Dis. 2009; 200(1): 66–74.
13. World Health Organizatioin. Malaria elimination: a field manual for low and
moderate endemic countries. Geneva: WHO 2007.
14. Rowe AK, Kachur SP, Yoon SS, Lynch M, Slutsker L, et al. Caution is required
when using health facility-based data to evaluate the health impact of malaria control
efforts in Africa. Malaria Journal 2009; 8: 209.
15. Moonen B, Cohen JM, Snow RW, Slutsker L, Drakeley C, et al. Operational
strategies to achieve and maintain malaria elimination. Lancet 2010; 376: 1592–1603.
16. Omumbo J, Hay S, Snow R, Tatem A, Rogers D. Modelling malaria risk in East
Africa at high-spatial resolution. Trop Med Int Health 2005; 10: 557–566.
17. Goovaerts P. Geostatistical analysis of disease data: accounting for spatial support
and population density in the isopleth mapping of cancer mortality risk using area-to-
point Poisson kriging. Int J Health Geogr 2006; 5: 52.
18. Mmbando BP, Kamugisha ML, Lusingu JP, Francis F, Ishengoma DS, et al. Spatial
variation and socioeconomic determinants of Plasmodium falciparum infection in
northeastern Tanzania. Malaria Journal 2011; 10:145.
19. Government of Rwanda (GOR) (2010) Bugeseradistrict Available:
http://www.bugesera.gov.rw/index.php?opt
ion=com_content&view=article&id=73:about -the-district&catid=34:about-the-ditrict
&Itemid=27&lang=en. Accessed 2012 May 15.
20. Tsuang A, Lines J, Hanson K. Which family members use the best nets? An analysis
of the condition of mosquito nets and their distribution within households in
Tanzania. Malaria Journal 2010; 9(1): 211.
21. Pettifor A, Taylor E, Nku D, Duvall S, Tabala M, et al. Bed net ownership, use and
perceptions among women seeking antenatal care in Kinshasa, Democratic Republic
of the Congo (DRC): Opportunities for improved maternal and child health. BMC
Public Health, 2008; 8(1): 331.
22. Haque U, Hashizume M, Sunahara T, Hossain S, Ahmed SM, et al. Progress and
challenges to control malaria in a remote area of Chittagong hill tracts, Bangladesh.
Malar J 2010 9:156.
23. Loha E, Lunde TM, Lindtjorn B. Effect of bednets and indoor residual spraying on
spatio-temporal clustering of malaria in a village in South Ethiopia: a longitudinal

177
study. PLoS One 2012; 7: e47354.
24. Stresman GH, Kamanga A, Moono P, Hamapumbu H, Mharakurwa S, et al. A
method of active case detection to target reservoirs of asymptomatic malaria and
gametocyte carriers in a rural area in Southern Province, Zambia. Malaria J 2010; 9:
265.
25. Smith T, Beck HP, Kitua A, Mwankusye S, Felger I, et al. Age dependence of the
multiplicity of Plasmodium falciparum infections and of other malariological indices
in an area of high endemicity. Trans R Soc Trop Med Hyg 1999; 93: 15–20.
26. Winskill P, Rowland M, Mtove G, Malima RC, Kirby MJ. Malaria risk factors in
north-east Tanzania.Malaria Journal 2011; 10: 98.
27. Smith T, Hii JL, Genton B, Müller I, Booth M, et al. Associations of peak shifts in
age-prevalence for human malarias with bednet coverage. Trans R Soc Trop Med
Hyg 2001; 95:1–6.
28. Lengeler C. Insecticide-treated bed nets and curtains for preventing malaria.
Cochrane Database Syst Rev 2004. CD000363.
29. Ministry of Health -Rwanda. Interim Demographic and Health Survey 2007–08
Kigali, Rwanda, 2009; DHS 2010 (Preliminary Report).
30. President’s Malaria Initiative (PMI). Malaria Operational Plan: Rwanda FY 2011.
Washington, DC: PMI, 2010. Available: http://pmi.gov/countries/mops/fy11/rwand
a_mop-fy11.pdf. Accessed 15th September 2012.
31. Coleman M, Coleman M, Mabaso ML, Mabuza AM, Kok G, et al. Household and
microeconomic factors associated with malaria in Mpumalanga, South Africa. Trans
R Soc Trop Med Hyg 2010; 104:143–147.
32. Konradsen F, Amerasinghe P, van der Hoek W, Amerasinghe F, Perera D, et al.
Strong association between house characteristics and malaria vectors in Sri Lanka.
Am J Trop Med Hyg 2003; 68: 177–181.
33. Fontecha GA, Mendoza M, Banegas E, Poorak M, De Oliveira AM, et al.
Comparison of molecular tests for the diagnosis of malaria in Honduras. Malar J
2012; 11: 119.
34. Dal-Bianco MP, Köster KB, Kombila UD, Kun JF, Grobusch MP, et al. High
prevalence of asymptomatic Plasmodium falciparum infection in Gabonese adults.
Am J Trop Med Hyg 2007; 77: 939–942.

178
35. Von Seidlein L, Bojang K, Jones P, Jaffar S, Pinder M, et al. A randomized
controlled trial of artemether/benflumetol, a new antimalarial and
pyrimethamine/sulfadoxine in the treatment of uncomplicated falciparum malaria in
African children. Am J Trop Med Hyg 1998; 58: 638–644.
36. White NJ. Antimalarial drug resistance. J Clin Invest. 2004; 113: 1084–1092.
37. Sutherland CJ, Ord R, Dunyo S, Jawara M, Drakeley CJ, et al. Reduction of malaria
transmission to Anopheles mosquitoes with a six-dose regimen of coartemether.
PLoS Med 2005; 2: e92.

179
CHAPTER 8
Stakeholder engagement in community-based malaria studies in a
defined setting in the eastern province, Rwanda
Chantal Marie Ingabire, Msc1, 2* Fredrick Kateera, MD, Msc2, 3, Emmanuel
Hakizimana, Msc4, 5, Alexis Rulisa, MPH2, 6, Bart Van Den Borne, PhD2,
Claude Muvunyi, MD, PhD7, Ingmar Nieuwold, Msc8, Constantianus JM
Koenraadt, PhD5, Leon Mutesa, MD, PhD7, Michele Van Vugt, MD, PhD3,
Jane Alaii, PhD9
1 Medical Research Center, Rwanda Biomedical Center, Kigali, Rwanda 2 Department of Health Promotion, Maastricht University, The Netherlands 3 Academic Medical Center, Amsterdam, The Netherlands 4 Malaria & Other Parasitic Diseases Division, Rwanda Biomedical Center, Kigali,
Rwanda 5 Laboratory of Entomology, Wageningen University, Wageningen, The Netherlands 6 Department of Cultural Anthropology and Development Studies, Radboud University
Nijmegen, Nijmegen, the Netherlands 7 College of Medicine and Health Sciences, University of Rwanda, Rwanda 8 Foundation The100th Village, Amsterdam, The Netherlands 9 Context Factor Solutions, Nairobi, Kenya
Published in: Mediterranean Journal of Social Sciences 2016, 7:2S1

180
Abstract
Aim
The value of engaging stakeholders for locally relevant responses and sustainable gains in
disease control programs has been increasingly acknowledged. As opposed to a
traditional top-down implementation of malaria intervention strategies, community
bottom up initiatives require that all stakeholders be identified and strategies of
engagement are designed at an early stage of program planning, implementation, and
evaluation, to promote optimal intervention impact and program ownership and
sustainability.
Methods
A stakeholder analysis was conducted as part of a formative analysis in multiple
community based studies under the malaria elimination program (MEPR) in Eastern
Province of Rwanda. Starting with an initial list of stakeholders a snowball sampling
technique was employed to identify other potential stakeholders from national and local
public/private institutions and community/faith-based organizations. Individual
interviews with nineteen stakeholders and eight focus group discussions with a total of 69
stakeholders were conducted.
Results
Stakeholders were classified into primary (lay community), secondary (local
administrative and health institutions) and key stakeholders (policy makers and funders).
Most of the stakeholders consulted were further classified depending on their type and
degree of involvement unto information, consultation/collaboration, co-decision and
empowerment categories. The MEPR team independently assigned participatory
communication techniques to stakeholders for further engagement. In addition to
awareness about MEPR activities, stakeholders’ reported willingness to contribute to the
promotion of malaria preventive measures, participation in supportive hands-on trainings
and in the MEPR planning (pre-engagement meetings and trainings), implementation
(formative research and project interventions) and knowledge translation activities, such

181
as the development of project materials as well as participation in lay and scientific
workshops where research findings dissemination and interpretation were discussed.
Conclusion
Overall, the analysis enabled the MEPR to know who to engage for a particular project
activity and the appropriate time to do so. Stakeholders appreciated the early consultation
by the MEPR and solicited continuous updates on malaria activities and key findings.
Subsequently, stakeholder identification has been updated to evolve with shifting
stakeholder interests over time.

182
Introduction
Significant progress in the fight against malaria in Rwanda has been made as a result of
the increased access to insecticide treated nets (LLINs) since 2004, indoor residual
spraying (IRS) in malaria endemic districts since 2009 and the prompt treatment using
artemisinin-based combination therapy (WHO, 2014). From 2005-2010, significant
declines in malaria incidence (70%), outpatient malaria cases (60%) and inpatient malaria
deaths (54%) among children under five years have been reported (Karema et al., 2012).
The maximization of the use of available preventive measures is important in a country
whose national malaria strategic plan targets achievement of malaria pre-elimination
levels by 2018 (Program, 2012).
Community participation at multiple levels is an important factor to achieve locally
meaningful responses towards further malaria control and sustain the achieved gains
(Atkinson, Vallely, Fitzgerald, Whittaker, & Tanner, 2011). One approach towards
sustainability of used interventions is effectively engaging with all stakeholders. To this
end, a stakeholder analysis, a program-planning tool focused on identifying and analysing
stakeholders’ motivations for promoting or threatening malaria associated interventions,
has been reported as necessary (Brugha & Varvasovszky, 2000; Reed et al., 2009).
Stakeholder analysis aims to understand stakeholder behaviour, intentions, interests and
interrelations and to assess the influence and resources stakeholders may bring to
decision making or implementation and analysis processes (Ancker & Rechel, 2015;
Freeman, 2001; Varvasovszky & Brugha, 2000). As part of a social assessment,
stakeholder analysis serves to identify key stakeholders and, based on their degree of
involvement, establish an appropriate framework for participation in project selection,
design, implementation, monitoring, and evaluation (Kansas, 2014; Luyet, Schlaepfer,
Parlange, & Buttler, 2012; Narayan, 1998; Prell, Hubacek, & Reed, 2009; Reed et al.,
2009; Reed, Stringer, Fazey, Evely, & Kruijsen, 2014). In health care, stakeholder
analysis is a tool that an organization can use to achieve specific advantages in
collaborating with other institutions (Brugha & Varvasovszky, 2000). Stakeholders with a
common vision for the desired goals are an important strength for overcoming obstacles
throughout program implementation (Njau, de Savigny, Gilson, Mwageni, & Mosha,
2009).

183
A malaria elimination program (MEPR) was initiated in a community (Ruhuha sector) in
the Eastern Province of Rwanda in 2012 (Ingabire et al., 2014) to complement the
national malaria control program used interventions by stimulating the local community’s
active participation from an early stage in the planning, implementation and evaluation of
local malaria activities. To achieve this, a stakeholder analysis was conducted to 1)
identify local institutions and processes upon which to build further malaria control
interventions, 2) be informed of stakeholders’ participatory activities, (3) identify
stakeholders’ degree of involvement, and (4) determine the participatory and
communication methods to be employed by the MEPR in engaging with stakeholders.
Methods
Study site and sampling
The MEPR activities are implemented in the moderate-low malaria transmission Ruhuha
sector, Bugesera district, eastern province of Rwanda. The sector population is estimated
to be 23893 individuals living in about 5098 households (Source: Ruhuha sector socio-
economic categorization report, 2015).
Purposive sampling within and outside the Ruhuha sector was used to target all persons
and groups with a stake in malaria control in Ruhuha sector and to ensure that a
representative cross section of all relevant stakeholders were selected including members
of district, regional and national malaria control efforts and those involved in designing
and implementing malaria control policy (Hardon, 2001). Stakeholder identification was
done using an iterative process. A preliminary list drawn from community
representatives who participated in previous open space discussions that aimed at
exploring different ways community can contribute towards malaria reduction towards
elimination (Ingabire et al., 2014), was updated by MEPR team (PhD students) in close
consultations with key informants from the National Malaria Control Program (NMCP),
district health office, the local Ruhuha health centre and Ruhuha sector administrative
office to generate a comprehensive stakeholder inventory. Based on the generated
inventory list, a maximum variation sampling approach was used to purposively select a

184
representative group of the entire cross section of stakeholders for interviews. A snowball
technique was also employed where listed stakeholders were asked to identify additional
potential stakeholders who may have considerable influence on MEPR activities
including empowering the community towards eliminating malaria. With the exception of
the community-level participants, the selection of all other respondents was conducted so
as to purposely prioritise leaders in their respective organizations. Stakeholders were
included from health, educational, religious, business and administrative sectors and also
represented community-based organizations and the lay community. To generate a
knowledge mapping, a checklist of open-ended questions (used during one-on-one
interviews and group interviews) was developed to explore awareness of the MEPR and
the stakeholder’s proposed participatory actions towards malaria elimination.
Data collection
Interview appointments were made with all selected stakeholders. Initially, one-on-one
followed by homogeneous group interviews were conducted as follows. Nineteen (19)
stakeholders were interviewed in one-on-one interviews lasting approximately 30
minutes for each representative of public and private organizations such as non-
governmental organizations (NGOs), churches, administrative and health professionals.
Eight (8) group discussions (lasting approximately one hour each) were conducted with a
total of sixty-nine (69) participants for homogeneous stakeholder groups of community
health workers (CHWs) (10), members of local agricultural cooperatives (32), local
school representatives (8), Ruhuha community members (10) and Ruhuha youth (9). All
interviews and discussions were conducted in the local language ‘Kinyarwanda” by CMI
(First author). Responses were recorded, transcribed and translated into English, coded
and categorized for further comparison and analysis.
Analysis
We analysed our data using the analysis framework described elsewhere (Kansas, 2014;
Luyet et al., 2012) in which four steps were followed. Firstly, interviewed individuals
were categorized into primary (beneficiaries), secondary (involved with/or responsible
for beneficiaries) and key (government officials, policy makers and donors) stakeholder
groups. Secondly, analysis of stakeholders’ knowledge about the MEPR programme and

185
its activities followed by analysis of stakeholders’ participatory actions related to malaria
control and/or elimination was done. Thirdly, a description of stakeholders’ degree of
involvement was analysed in support of a model elaborated by Luyet et al. (Luyet et al.,
2012), the degree of stakeholder involvement occurs on various levels and thus an
illustration of this was guided by the authors’ deliberation and judgment as previously
recommended (Bryson, Cunningham, & Lokkesmoe, 2002). The Luyet et al ’s model
(Luyet et al., 2012) describes five levels of analysis, however in our study, two levels
were combined due to minor differences observed in our data to generate a 4-step model
that includes: (1) information—explaining the project to the stakeholders; (2)
consultation/collaboration—presenting the project to stakeholders, collecting their
suggestions, and noting decision making with or without taking stakeholder input into
account, (3) co-decisions—cooperating with stakeholders to achieve an agreement for
solution and implementation, and (4) empowerment—delegating decision-making for
project development and implementation to the stakeholders. The MEPR team
established methods of communication for stakeholders and a further classification was
made accordingly in the last step of analysis.
Results
Stakeholder participation
Eighty-eight (88) individual stakeholders were included in the analysis. The largest
representation (32) was from locally based cooperatives group members. These
cooperatives included stakeholders who worked in agriculture, transport, sewing, events
decoration and security. The technical sector was made up of individuals from the
NMCP, community health workers (CHWs) and local health centre staff, participants
from community-based health insurance (CBHI) programs and representatives from the
health district level, private clinics, drugstores and NGOs provided 22 participants. The
community category included ten (10) adults and nine youth (age range of 21-35 years).
Participants also included stakeholders from eight schools (three secondary schools, four
primary schools and one vocational training school), five churches and two
administrative-level staff from Ruhuha sector. Finally, stakeholders were classified into
three categories depending on the nature of their participation (primary, secondary or key

186
stakeholder) (table 1). The lay community was considered as the primary stakeholder,
while 10 secondary stakeholders were identified, mostly from the health sector, but also
from schools, churches and NGOs. Lastly, the health district office, Caritas Kigali
(catholic organization that provides supervisory leadership to the Ruhuha health centre)
and NMCP staffs were considered as key stakeholders.
Table 1. Stakeholder Categorization Primary stakeholders Secondary stakeholders Key stakeholders
Lay community in the Ruhuha sector
Community health workers Health district office staffRuhuha health centre staff NMCP staff
Caritas KigaliCommunity-based health insurance staffAdministrative sector office staffDrugstore staffPrivate clinic staffCooperative membersSchool staffChurch leadersNGOs staff
Awareness about MEPR
Participants in both one-on-one and group sessions appeared almost universally aware of
the MEPR organization and the activities being implemented in Ruhuha. Their awareness
was mainly attributable to the prior active stakeholders’ participation in the launch and
follow-up of MEPR activities. Stakeholders including the Ruhuha health centre staff and
CHWs were also directly involved in ongoing implementation of the MEPR including
mobilizing households for project uptake and treating malaria cases identified during the
project’s conducted household baseline surveys.
Participatory actions
Based on the perceived seriousness of malaria in the area, stakeholders across all the
interviews appeared in favour of the MEPR. Most stakeholders suggested partnering with
the MEPR in community mobilization and sensitization for malaria preventive measures.
On one hand, the health sector was more willing to assist the project with training

187
community members to equip them with comprehensive malaria knowledge. On the other
hand, stakeholders in this category suggested that the MEPR generates evidence that
would be valuable to assess the impact of project interventions on the current malaria
burden. The administrative sector was more interested in a mutual partnership with the
health sector by mobilizing and sensitizing communities to increase the uptake of malaria
preventive measures at this level. The business sector, general community members and
youth preferred to focus on peer education and promoting a CBHI as important elements
for prompt health care seeking. The private sector stakeholders, including staff from
drugstores and private clinics acknowledged the need for prompt health-care seeking and
a rational use of malaria medication based on confirmed cases, which suggests the
establishment of a referral system in close collaboration with the local health centre.
Lastly, the educational sector and youth suggested establishing anti-malaria clubs as a
channel to share malaria-related information among the young generation in order to
nurture pro-active action against malaria and trickling down to family members.
Stakeholders by potential degree of involvement
Of the 88 individuals, 75 were eligible for all steps of engagement. The first two steps
(information and consultation/collaboration) were found to be more commonly reported
as important for stakeholders. However, it was apparent that not every identified
stakeholder was involved in all actions of the project as highlighted in table 2: the
religious and education sector were not directly involved in the implementation of the
MEPR, however were regularly informed, consulted and later on participated in the
MEPR knowledge translation activities.
Table 2. Degree of involvement in MEPR Stakeholders Informa Consultation
/CollaborationCo-decision Empowerment
Lay community * * * *Business sector * * * *Religious sector * *Education sector * *Health sector * * * *Administrative sector
* * * *

188
Stakeholder participatory methods for communication
Following identification, categorization of stakeholders and highlighting their degrees of
involvement and identifying their potential contributory actions towards MEPR activities,
the study team established communication methods to gather data, share information
and/or identify key research and malaria control related activities for further collaboration
(table 3). All stakeholders participated in the data collection processes, either through
open space discussions, annually conducted surveys or individual or group interviews.
Some of the stakeholders participated in the MEPR implementation and were therefore
provided with hands-on trainings to equip them with knowledge and practical skills
needed to perform their activities. Phone messaging was used as a reminder for regular
meetings and monthly progress reports. All stakeholders were invited to attend meetings
where study findings were presented and follow up discussions on presented findings
were held. In addition, study findings and key MEPR activities were printed and
distributed using brochures. Lastly, virtual stakeholders were targeted using peer-
reviewed publications, policy briefs as well as online blogs and documentaries.
Table 3. Communication/engagement methods by stakeholder
Stakeholders Community Business Religious
sector
Education
sector
Health
sector
Administrative
sectorMethod
Open space * * * * * *
Household survey * * * * * *
Focus group discussions * * * * * *
One-to-one meetings * * * * *
Peer-reviewed journals * * *
Scientific workshops * * *
Lay workshops * * * *
Hands-on trainings * * * *
Phone messages * * * *
Brochures or Pamphlets * * * * * *
Online blogs * * * * * *
Video or Documentary * * * * * *
Policy briefs * *

189
Application of stakeholder analysis: insights into MEPR
The MEPR deploys a bottom-up approach towards maximizing the use of available
preventive malaria control tools to further reduce the local malarial burden and seeks to
adapt its goals to the needs and priorities of likely users (Reed et al., 2014; Thomas &
Palfrey, 1996). Two elements of engagement as described by Pretty (1995) were
conceptually applied in this analysis. The first element was self-mobilization emerging
from community initiatives and stakeholders making key decisions in regular meetings
(Pretty, 1995). Based on this principle, some identified stakeholders were further grouped
in a platform called community malaria-action teams (CMATs) to collectively identify
local malaria-related problems and adopt solutions to remedy these problems. The
platforms also served as liaisons between the MEPR project and the community at large
and facilitated knowledge exchange among members and MEPR team through feedback
sessions that were set up to promote CMATs and MEPR project activities
implementation. Within a year of being established (2013-2014), CMATs were found to
have largely contributed to the MEPR’ s goal of further malaria control by facilitating
community preparedness for planned MEPR research activities and promoting active
community mobilization towards the use of available malaria preventive measures such
as the use of LLINs, acceptance of IRS, clearing peridomestic potential mosquito
breeding sites and supporting community member’s health care seeking behaviours. A
reported significant reduction in presumed malaria/fever cases from 68% to 21.4 % and
an increase in health insurance coverage from 66.3 % to 91% were observed among
others (Household surveys 2013 and 2014). Furthermore, on-going community
sensitization contributed to an increase in community acceptance of IRS, which led to
100% coverage in early 2015 compared to 91 % coverage reported in 2014.
The second element of engagement was interaction- the provision of greater
opportunities for stakeholders to be involved in decision making and consideration of
stakeholders as a means of achieving predetermined project objectives (Pretty, 1995).
Thus, the MEPR team further engaged identified stakeholders from rice cooperatives in a
mosquito-larval source management program in the irrigated rice fields that harbour the
malaria mosquito larvae. These stakeholders reported that being involved in the planning

190
stage contributed to an increase in their level of ownership and knowledge based on
reflective learning.
Effective knowledge exchange has been highlighted as an important aspect to enhance
the impact on policy and practice and foster positive relationships (McInnes et al., 2012;
Reed et al., 2014). In this regard, the MEPR researchers held a series of results-
dissemination and interpretation meetings as part of the stakeholder engagement strategy.
The audiences for the series included policymakers and the scientific and lay
communities to create awareness on the MEPR findings and to highlight future
provisions. Although, the initial analysis did not involve stakeholders from the media
sector, the contribution of media became apparent during the results dissemination and
thus their engagement was prioritized.
MEPR researchers also interviewed stakeholders with regard to their expertise and based
on their reported willingness to participate in funding MEPR project activities and
supporting the packaging of research findings for knowledge translation. With this, hands
–on trainings on how to engage various stakeholders in the field using online blogs,
brochures, documentaries, policy briefs and dialogues were held in collaboration with
one of the stakeholders with an extensive expertise in knowledge translation. This led to a
positive partnership between MEPR team and their network of stakeholders as well as the
stakeholders’ actions that led to increased awareness about MEPR activities and findings
(http://ktnetafrica.net/coalitions/empowering-community-towards-malaria-elimination-0,
http://ktnetafrica.net/sites/default/files/MEPR_Policy%20Brief_English.pdf), better
sensitization of Ruhuha community members about on-going malaria elimination efforts,
and promoted the sharing of best practices with all stakeholders.
Discussion
Input from a wide range of stakeholders is essential for developing a participatory,
consensus-building process that meets the needs and expectations of both the community
and program implementers. Our initial interviews provided a substantive list of
stakeholders, across various categories, and identified the support they could potentially
provide to the MEPR activities. A large number of stakeholders expressed their

191
willingness to provide technical support in relation to the project implementation as well
as active participation in malaria related educational activities. The local administrative
office expressed particular interest in providing political support to facilitated project
acceptance and engagement in MEPR related activities at the community level.
Many stakeholders actively participated in implementation of project interventions,
which fostered a sense of reflective learning and ownership in malaria elimination efforts.
With financial and technical support provided to the MEPR by one of its stakeholders for
research-related knowledge translation activities, packaging of study findings from
research conducted was noted as essential to increasing awareness and subsequent use of
research findings beyond the scope of participating stakeholders.
Our study findings suggest that all primary and secondary stakeholders appeared strongly
interested in the MEPR as a result of being directly affected by malaria. However, due to
high levels of interdependency between stakeholders, successful change requires a close
partnership with the three stakeholder categories; primary, secondary, and key
stakeholder categories to achieve a greater impact.
The innovative idea of establishing malaria clubs among school children and youth at
large aligns well with what has been previously reported in the same community and
underscores the importance of this idea for further malaria control (Ingabire et al., 2014;
Ingabire et al., 2015). The MEPR project has thus far informed and consulted the
educational sector in regards to proper implementation of activities. Future collaboration
may require the creation of such clubs and exploration of their impact in reversing
malaria burden, specifically among young generation.
The systematic identification of stakeholders in a research process has been reported as
an effective way to increase the value and likelihood of community engagement (Reed et
al., 2014), especially when tackling an issue recognized as a priority to the stakeholder
audience and hence participation requires that all interests and/or concerns of
stakeholders are addressed (Mallery C, 2012; Namazzi et al., 2013). The multi
stakeholder-based approach in the early stage of the project facilitated MEPR team’ s

192
knowledge of who, when and how to engage and thus resulted in the support and
agreement of malaria control related interventions and processes as also suggested
elsewhere (Hyder et al., 2010; Namazzi et al., 2013; Reed et al., 2009).
Previous experience has shown that communication content and processes within
research settings are influenced by the socio-cultural environment. Thus adapting
approaches based on cognizance of the context enhances wider access to relevant
information for various levels of stakeholders (Hyder et al., 2010). In our study,
identification of communication channels between MEPR and stakeholders was key
importance for planning and implementation of MEPR project activities and served as
platform to share and/or receive tailored messages for both project team and stakeholders.
Active participation of stakeholders was eminent throughout in the conducted MEPR
activities. In contrast in Uganda, where a study evaluating the role and influence of actors
in malaria treatment policy making reported the lay community as non-participatory
actors, rather considered by policy makers as beneficiaries (Nabyonga-Orem, Nanyunja,
Marchal, Criel, & Ssengooba, 2014). This Ugandan study recommended availability of
structures and systems to enable community participation in both research process and
decision-making(Nabyonga-Orem et al., 2014).
Despite the ability of stakeholder analysis to predict and generate information, the results
of this analysis are amenable change as influenced by stakeholders’ interests, position,
leadership and other attributes and thus requires continued close monitoring (Brugha &
Varvasovszky, 2000). To maintain constant engagement of stakeholders and relevance of
the analysis throughout the duration of research, it has been important for MEPR
facilitators to manage the conduct and content of stakeholder engagement by tailoring
support and maintaining contact with stakeholders through meetings or workshops as
observed elsewhere (Brugha & Varvasovszky, 2000; Concannon et al., 2014). For this
reason, the MEPR operationalized a bi-directional communication and feedback strategy.
Annually, research results dissemination and interpretation workshops with community,
scientific, funders and policy makers were organized to validate the findings, discuss
implications and propose a way forward. In addition, quarterly meetings for hands-on
trainings and discussions on action plan with primary stakeholders, mostly through

193
CMAT members were organized to implement malaria related prevention activities in
close collaboration with the community. Lastly, regular formal and informal meetings
with secondary stakeholders, mostly local administrative and health offices for proper
planning and execution of project activities were planned and implemented. Similarly to
other settings, these one-to-one meetings were reported to foster relationships and
promote understanding of research priorities and clarify specific stakeholder roles
(Christen O’Haire, 2011). As a result, Ruhuha area where MEPR activities are being
implemented, reported positive changes such as the reduction of presumed malaria cases,
increase of health insurance coverage as well as complete household coverage of IRS.
The MEPR partnership with relevant stakeholders has therefore contributed to the
capacity building of the local community in terms of knowledge and skills while
accelerating the achievement of the main project goal of malaria elimination through
community-based and context-tailored approaches.
The combination of individual and group interviews was preferred considering that
creating social conditions for heterogeneous groups is often challenging (Jinks, Ong, &
O'Neill, 2009). This resulted in gathering evidence for stakeholder identification,
categorization and engagement. The fact that some stakeholders were already linked with
the project was not necessarily regarded as a limitation to the analysis but as positively
contributory to the perceived awareness on MEPR activities and purpose among area
stakeholders.
This paper illustrates the steps taken to identify and engage relevant stakeholders in the
MEPR related activities. Further studies focusing on a detailed evaluation of the overall
stakeholder contribution to the main goal of malaria reduction moving towards
elimination, highlighting some of the pitfalls and generating recommendations towards a
sustainable stakeholder engagement are recommended. Findings from this analysis
should be interpreted in view of some limitations as some of the interviews were
conducted with individuals from institutions or organizations while individuals may not
necessarily represent the views of the institutions from which they represented.

194
Conclusion
In our study, a stakeholder-focused approach enabled identification of multiple
stakeholders from different levels of administrative units and lay community; definition
of their role as well as their degree of involvement in planning and implementation of an
effective community-based malaria elimination project in Ruhuha sector, Rwanda.
Stakeholder identification was inclusive of all relevant individuals and organizations and
the analysis was performed at an early stage and updated to evolve with shifting
stakeholder interests over time. Appropriate analysis in relation to stakeholder expertise
was considered so the MEPR could learn who to engage for a particular project activity
and the appropriate time to do so. This process highlighted the value of stakeholder
engagement in ensuring sustainability, ownership and collaboration for optimal impact of
malaria control programs in a defined community.

195
References
1. Ancker S, Rechel B. HIV/AIDS policy-making in Kyrgyzstan: a stakeholder analysis.
Health Policy Plan 2015; 30(1): 8-18.
2. Atkinson JA, Vallely A, Fitzgerald L, Whittaker M, Tanner M. The architecture and
effect of participation: a systematic review of community participation for
communicable disease control and elimination. Implications for malaria elimination.
Malar J 2011; 10(1): 225.
3. Brugha R, Varvasovszky Z. Stakeholder analysis: a review. Health Policy and
Planning, 2000; 15(3), 239-246.
4. Bryson JM, Cunningham GL, Lokkesmoe K J. What to Do When Stakeholders Matter:
The Case of Problem Formulation for the African American Men Project of Hennepin
County, Minnesota. Public Administration Review 2002; 62(5): 568-584.
5. Christen O’Haire, M. M., Erika Nakamoto, Lia LaBrant, Carole Most, Kathy Lee,
Elaine Graham, Erika Cottrell, Jeanne-Marie Guise. Methods for Engaging
Stakeholders To Identify and Prioritize Future Research Needs. 2011.
6. Concannon TW, Fuster M, Saunders T, Patel K, Wong JB, Leslie LK, Lau J. A
systematic review of stakeholder engagement in comparative effectiveness and
patient-centered outcomes research. J Gen Intern Med 2014; 29(12), 1692-1701.
7. Freeman RE, AM John. A Stakeholder Approach to Strategic Management
8. Hardon A, Boonmongkon P, Streefland P, Tan L. Applied Health Research Manual:
Anthropology of Health and Health Care: New Jersey: Transaction Publishers. Hyder
A, Syed S, Puvanachandra P, Bloom G, Sundaram S, Mahmood S. 2001.
9. Peters D. Stakeholder analysis for health research: case studies from low- and middle-
income countries. Public Health 2010; 124(3): 159-166
10. Ingabire C, Alaii J, Hakizimana E, Kateera F, Muhimuzi D, Nieuwold I, et al.
Community mobilization for malaria elimination: application of an open space
methodology in Ruhuha sector, Rwanda. Malar J 2014; 13(1): 167.
11. Ingabire C, Rulisa A, Van Kempen L, Muvunyi C, Koenraadt C, Van Vugt M, et al.
Factors impeding the acceptability and use of malaria preventive measures:
implications for malaria elimination in eastern Rwanda. Malar J 2015; 14(1): 136.

196
12. Jinks C, Ong B, O'Neill T. The Keele community knee pain forum: action research to
engage with stakeholders about the prevention of knee pain and disability. BMC
Musculoskeletal Disorders 2009; 10(1): 85.
13. Kansas U. 2014. Identifying and Analyzing Stakeholders and Their Interests
14. Karema C, Aregawi M, Rukundo A, Kabayiza A, Mulindahabi M, Fall I, et al. Trends
in malaria cases, hospital admissions and deaths following scale-up of anti-malarial
interventions, 2000-2010, Rwanda. Malar J 2012; 11(1): 236.
15. Luyet V, Schlaepfer R, Parlange MB, Buttler A. A framework to implement
Stakeholder participation in environmental projects. Journal of Environmental
Management 2012; 111(0): 213-219.
16. Mallery CG, Fernandez J, Smeeding L, Robinson S, Moon M, Lavallee D, Siegel J.
Innovative Methods in Stakeholder Engagement: An Environmental Scan. 2012.
17. McInnes E, Middleton S, Gardner G, Haines M, Haertsch M, Paul C, Castaldi P. A
qualitative study of stakeholder views of the conditions for and outcomes of successful
clinical networks. BMC Health Services Research, 2012; 12(1): 49.
18. Nabyonga-Orem J, Nanyunja M, Marchal B, Criel B, Ssengooba F. The roles and
influence of actors in the uptake of evidence: the case of malaria treatment policy
change in Uganda. Implement Sci 2014; 9: 150.
19. Namazzi G, Kiwanuka SN, Waiswa Peter, Bua J, Katharine Allen, et al. Stakeholder
analysis for a maternal and newborn health project in Eastern Uganda. BMC
Pregnancy and Childbirth, 2013; 13(1): 58.
20. Jennifer Rietbergen-McCracken, Deepa Narayan-Parker. 1998. Participation and
Social Assessment: Tools and Techniques. Library of Congress Cataloging-in-
Publication Data.
21. Njau RJ, de Savigny D, Gilson L, Mwageni E, Mosha FW. Implementation of an
insecticide-treated net subsidy scheme under a public-private partnership for malaria
control in Tanzania-challenges in implementation. Malar Journal 2009; 8:201.
22. Prell C, Hubacek K, Reed M. Stakeholder Analysis and Social Network Analysis in
Natural Resource Management. Society & Natural Resources 2009; 22(6): 501-518.
23. Pretty JN. Participatory learning for sustainable agriculture. World Development,
1995; 23(8), 1247-1263.
24. Program, RN. (2012). Rwanda Malaria Control Strategic Plan July 2013- June 2018.

197
25. Reed MS, Graves A, Dandy N, Posthumus H, Hubacek K, Morris J, Stringer LC.
Who's in and why? A typology of stakeholder analysis methods for natural resource
management. J Environ Manage 2009; 90(5): 1933-1949.
26. Reed MS, Stringer LC, Fazey I, Evely AC, Kruijsen JH. Five principles for the
practice of knowledge exchange in environmental management. Journal of
Environmental Management 2014; 146(0): 337-345.
27. Thomas P, Palfrey C. Evaluation: Stakeholder-focused Criteria. Social Policy &
Administration, 1996; 30(2): 125-142.
28. Varvasovszky Z, Brugha R. A stakeholder analysis. Health Policy and Planning, 2000;
15(3): 338-345.
29. WHO. World Malaria Report 2014. Avalilable at:
www.who.int/malaria/.../world_malaria_report_2014/en/. Accessed 13th May 2015.

198
CHAPTER 9
General Discussion of key study findings To achieve pre-elimination levels in Ruhuha, given current SPR of 22.8%, will probably
require introduction of novel area-relevant interventions to supplement existing control
tools (mainly ITNs and IRS). As malaria transmission declines, a community-based
evaluation of transmission intensity and size of infectious reservoir will be required.
Also a prospective continued engagement with all stakeholders around well defined goals
of malaria control and an explicit assignment of each party to specific roles is required to
leverage all the available resources towards between outcomes.
The studies described in this thesis are focused on the biomedical aspects, with studies
covering the three other streams each a subject of a different thesis. Given the absence of
any prior studies in this area, we conducted baseline studies to characterise key
determinants on malaria control. Because these studies we principally cross sectional
based, findings reported can not be used to infer causal inferences, detect temporal and
spatial trends not be generalised to lesser malaria endemic settings or settings of different
socio-economic status. Anyhow, we contend that comprehensive malaria reduction and
hence achievement of malaria elimination with require a community based integrated
approach that identifies and targeted area specific challenges to malaria control.
Future perspectives on how to achieve malaria pre-elimination levels
This thesis focuses on community level determinants of malaria control. Overall,
molecular aspects (genetic diversity as well as molecular marker of resistance to two
previous used anti-malarials) in chapter 2 and 3 of the malaria parasite, malaria disease
prevalence (for both health facility identified sick patients and household identified
asymptomatic individuals (chapter 4 and 7), risk factors and spatial distribution are
characterised (chapter 7). In addition, among the under 5 year old children, associations
between and risk factors for three commonly co-existing disease conditions of malaria,
anaemia and under-nutrition were analysed (chapter 5). Regarding the principal malaria

199
control intervention of bed nets (Chapter 6), we characterised net access, ownership and
use, 9 months after a universal coverage campaign. Lastly, with in the context of out
community-oriented studies, we undertook a stakeholder analysis to review the potential
roles and contributions each can make towards further control (chapter 8). However,
while most of discussed interventions have been effective in reducing malaria burden
from high to medium to low levels, these have been driven primarily vertically using a
top to bottom approach by the NMCP. In order to both sustain gains made in malaria
burden reduction and move from low to pre-elimination levels, I recommend the
following strategies.
Technical feasibility
Hitherto, malaria control in Rwanda has been primarily managed and led at the central
level by the NMCP. The transition from success control to pre-elimination target requires
a change in strategy and a more technical rigorous set up of experts including but not
limited to epidemiologist, entomologists, anthropologists, cost effectiveness skills and
experts in active surveillance and prompt response activities. An assessment of the
whether the NMCP has the technical capacity, either in house of through the various
implementing partners is recommended. Because of the heterogeneous nature of the
current malaria transmission patters in Rwanda, multiple strategies may be needed to
optimize available resources, ensure cost effectiveness and employ a more evidence
based strategic plan rather the usually one-size-fits all approach of implementing WHO
recommended interventions and only relying on generally inaccurate, poorly
representative routine collected data. For this to happen, a team of multifaceted technical
capacities is recommended to define feasible targets, design setting relevant intervention
packages and employ a flexible response approach that is in line with the transitioning
epidemiology of each area.
Continued scale up of interventions
Despite high coverage with malaria control interventions, malaria burden remains high in
the study area (chapters 4 and 7). Also in Rwanda, resurgences in malaria burden have
been reported. In consequence, resurgences have also been associated with weaknesses in
sustaining the coverage or potential use of ineffective interventions in Rwanda including

200
low levels of coverage with LLINs and supplied of LLINs that were of limited
effectiveness due to being impregnated with suboptimal insecticide concentrations. This
has been observed in annual previous malaria burden reports on Rwanda [16-18] where
increasing burden has been observed. This pointed to the fragile nature of gains in decline
in malaria burden made and need to maintain high levels of coverage of deployed
interventions to ensure sustainable impact. Understanding the current malaria
transitioning epidemiology as well as delineating the determinants and distribution of this
residual transmission is required as evidence based platforms to inform decision-making.
This ensures that deployed interventions are cost effective and area relevant and have a
greater chance of being effective. Strategies to also optimize use of these interventions
including use of bed nets, increased access to accurate malaria diagnostics and effective
anti-malarials at community level are required.
Evidence based targeting of current at risk populations and potential breeding sites
In Rwanda, key interventions of LLINs and IRS activities have been differentially
implemented being concentrated in the 6 high endemic districts. A shift in strategy to
targeting achievement of pre-elimination levels will require a strategic focus on also the
traditionally low endemic settings as well. Investments in implementation research, by
either government units line the NMCP, or tertiary institutions line the university and
individual NGOs in conducting this research, with a priority on malaria transmission
dynamics is recommended. To guide this process, identifying current setting specific
research gaps and priorities is key to guiding which research is most appropriate at which
period and malaria transmission setting. From studies conducted in this area, some but
not all, of the existing research gaps include,
1. What is the individual attributable effect of bed nets and IRS in malaria
transmission impact
2. What accounts for the increased malaria infection risk among males and children
5-15 year olds
3. What are the additional impact of larval source techniques as complements of IRS
and LLIN use in achieving optimal malaria reduction?
4. What strategies are need to increase bed net use among who do not sleep on beds
and among males

201
5. What is the indirect impact on anaemia burden by declines in malaria burden
6. What strategies can be used to improve quality of housing that limits indoor
malaria transmission
7. What are the determinants of existing malaria hotspots in the study sites and what
interventions are most appropriate to arrest transmission within these clusters
8. What is the role and impact of an active surveillance program as an intervention
on reducing community level malaria reservoir pool
9. What set of integrated interventions is most cost effective and best suited to study
site epidemiology to optimally reduce local transmission.
Improving SES and housing quality
The integration of existing interventions with environmental management and socio-
economic development through house improvement and screening offers a non-
insecticidal, complementary approach to increasing protection against mosquito bites. We
identified that low SES was associated with high malaria risk (chapter 4 and 7). In our
study (chapter 4 and 7), Individuals living in houses whose wall structure were made of
wood/mud (vs. cement/bricks) showed a significantly higher risk of malaria in this study.
The protective positive impact of window screening, covering up of all eaves as well as
other house modification adjustments including use of window screens and ceilings have
been demonstrated elsewhere [14]. These measures provide a protective effect by
obstructing mosquito entry and hence reducing in indoor malaria transmission. In
addition to ITNs and IRS, significant efforts should focus on improving house design to
prevent mosquito entry and eliminate indoor malaria transmission. However, especially
for these resources limited settings where malaria is most concentrated, strategies to
ensure low cost housing modifications that are easily scalable are accessible for
communities are needed particularly in settings targeting achievement of malaria
elimination.
Controlling drug and insecticide resistance
Anti-malarial drug resistance remains a major hindrance to malaria control efforts. In the
recent past, resistance to two first line anti-malaria drugs of Chloroquine and
sulphodoxine – Pyrimethamine (SP) was a major set back that led to significant mortality

202
and morbidity. Chloroquine resistance in P. falciparum has been shown to be multigenic
involving, initially a mutations in a gene encoding a transporter (PfCRT), and later a
mutation in the gene encoding a second transporter (PfMDR1). For SP, resistance is often
administered in synergistic combination with anti-folates following a sequential
acquisition of resistance mediating mutations in the genes dhps and dhfr - In this study,
(chapter 2) molecular surveillance for prevalence of key mutations that are resistance
mediating for chloroquine and SP were studied. In a nutshell, a sustained high intensity
resistance to SP was observed but in contrast, a moderate return of wilt type strains
susceptible to chloroquine was observed. We recommend that an evaluation of
determinants of no SP and sub-optimal CQ recovery in the presence of reduced drug
pressure be characterized. These factors may plausibly influence resistant to other anti-
malarials in future unless we can identify and modify their impact.
Novel setting and malaria transmission level specific techniques
Novel strategies to complement existing ones may be needed to achieve malaria pre-
elimination. Larval source management (LSM) - the management of aquatic habitats
where mosquitoes may be breeding in order to arrest development of immature stages of
mosquito development is one such strategy. LSM is the targeted management of
mosquito breeding sites to reduce the number of mosquito larvae and pupae. LSM is an
appropriately intervention to reduce the numbers of both indoor and out-door biting
mosquitoes. In particular, in settings targeting achievement of malaria elimination, LSM
can be a useful complementary tool to other recommend interventions in reduce the
mosquito population in remaining malaria ‘hotspots’ as seen in out study area. Although
not reported in this thesis, our group has evaluated the feasibility of use of a larvicide
(Bacillus thuringiensis subsp. israelensis (Bti) by a select group of trained community
member and assessed their impact on mosquito vector density. Because the study area has
where larval habitats that few, fixed and findable – this technique may provide a
significant complementary effect on mosquito vector density and hence risk of malaria
and needs to be systematic characterized on a wider scale and over a larger area and
period to measure its potential impact.

203
Active surveillance and prompt responses
As malaria case numbers continue to decline and become more clustered in specific
hotspots, as observed in one of our studies, an active surveillance process that combines
rapid and community feasible diagnostics and effective response will be needed. A strong
pro-active surveillance system may guide the continued reduction in current burden and
also be a useful intervention in guiding further reduction in transmission by identifying
and targeting the setting specific pool of infected individuals. Hitherto in Rwanda, mainly
routine surveillance using health facility monthly reported slide positivity rate data has
been used for monitoring functions. In our study (chapter 7) we demonstrated that an
active surveillance system can identify community based hotspots and to strengthen the
current yield and value of surveillance, a progressive shift from routine to active types of
surveillance will be needed commensurate with levels of transmission, a clear
demonstration of focus in terms of type of surveillance needed in terms of time (weekly
or monthly), area to be monitor (high risk vs. moderate vs. low endemic levels),
seasonality (wet or dry season), or populations (costs involved, personnel needed,
training, capacity for implementation -transportation, and commodities) and type of
information required including type and level of geographical information systems
needed).
Community engagements
In our study, we demonstrated the feasibility of engagement with the community and the
value this has in promoting community mobilization, sensitization and pooling of
resources– all essential attributes for a more sustainable deployment of interventions.
Implementation of any intervention, including supply of nets, conducting IRS activities,
providing diagnostic services and use of antimalarial therapies, will require the
engagement of communities, to various degrees. In a setting of limited access to
government health facilities, community health care workers are increasing access to
malaria diagnosis and treatment but are also serving as focal points in organizing and
implementing both UCL and IRS activities. However engagement of other community
stakeholders such as churches, schools and cooperative units are essential in promoting
adherence to interventions, promoting information relay, education and behavioural
change among the community and participating in implementations of these

204
interventions. Ultimately, engagement of communities requires continuous Interaction
with their members and involving them in planning and decision-making and will serve
to promote ownership, sustainability and pooling of resources for optimal impact.
Partnerships
To increase and sustain coverage with existing control tools as well as build a broader
more impactful stakeholder base, all available channels – including private and public
entities–will be needed especially in resource-limited settings. Particular if the target is
achieving malaria pre-elimination, further malaria control will needs an active
engagement of all public and private sectors. In many countries, policy makers and
managers are leveraging existing public private partnerships (PPPs) to ensure that
resources and knowledge are pooled and that different strengths, skill sets, values and
efforts of public and private organizations are combined for an optimal impact. The
NMCP will need to invest in and prioritize building these partnerships to ensure
sustainable impact.
Conclusion
This thesis has presented findings on community level malaria burden among
asymptomatic cases and analysed for risk determinants of malaria infection. Gender, age,
household SES, type of materials house is made of and geographic location of households
were key determinants of malaria risk. We also studied malaria infection and co-
morbidities of anaemia and under-nutrition among pre-school going children – a
population that is usually neglected but yet most affected by the three disease conditions.
Overall, while malaria and anaemia shared a strong temporal association, malaria and
malnutrition were generally not associated. This thesis also presents findings from a
survey to characterise access, ownership and use of bed nets in a community 9 months
after a UCL activity. Bed net coverage and use were > 90%. Bed net use significantly
differed by gender, age group, among whether individuals sleep/don’t sleep on a bed and
number of sleeping space available in household. We also discussed a an assessment of
feasibility of use of an active surveillance technique called reactive case finding to use
health facility identified symptomatic cases to identify community – based asymptomatic
cases and study malaria case spatial distributions. Finally, this thesis also evaluated major

205
stakeholders who participate in malaria control in the study area. We sought to
understand their knowledge of MEPR activities as well as their willingness to collaborate
on future malaria control activities. Recommendations of which interventions and in
which combinations can be used for a further reduction in malaria transmission for
Rwanda are proposed.

206
References
1. Haddad D, Snounou G, Mattei D, Enamorado IG, Figueroa J, Stahl S, Berzins K. Limited
genetic diversity of Plasmodium falciparum in field isolates from Honduras. Am J Trop
Med Hyg 1999; 60:30-34
2. Babiker HA, Ranford-Cartwright LC, Walliker D. Genetic structure and dynamics of
Plasmodium falciparum infections in the Kilombero region of Tanzania. Trans R Soc
Trop Med Hyg 1999; 93:11-14.
3. Hviid L, Staalsoe T: Malaria immunity in infants: a special case of a general
phenomenon? Trends Parasitol 2004; 20:66–72
4. Karema C, Imwong M, Fanello CI, Stepniewska K, Uwimana A, Nakeesathit S, et al.
Molecular Correlates of High-Level Antifolate Resistance in Rwandan Children with
Plasmodium falciparum Malaria. Antimicrob Agents Chemother 2010; 54: 477–483.
5. Frosch AE, Venkatesan M, Laufer MK. Patterns of chloroquine use and resistance in sub-
Saharan Africa: a systematic review of household survey and molecular data. Malar J
2011; 10:116.
6. Rulisa S, Kateera F, Bizimana JP, Agaba S, Dukuzumuremyi J, Baas L, et al. Malaria
prevalence, spatial clustering and risk factors in a low endemic area of Eastern Rwanda: a
cross sectional study. PLoS One 2013; 8:e69443.
7. National Institute of Statistics of Rwanda: Rwanda Demographic Health Survey. 2010.
Available at: http://dhsprogram.com/pubs/pdf/FR259/FR259.pdf. Accessed 11 Nov 2014.
8. Winskill P, Rowland M, Mtove G, Malima RC, Kirby MJ. Malaria risk factors in north-
east Tanzania. Malar J 2011; 10:98.
9. Smith T, Beck HP, Kitua A, Mwankusye S, Felger I, Fraser-Hurt N, et al. Age
dependence of the multiplicity of Plasmodium falciparum infections and of other
malariological indices in an area of high endemicity. Trans R Soc Trop Med Hyg 1999;
93:15–20.
10. Smith T, Hii JL, Genton B, Muller I, Booth M, Gibson N, et al Associations of peak
shifts in age-prevalence for human malarias with bednet coverage. Trans R Soc Trop
Med Hyg 2001; 95:1–6.
11. Tshikuka JG, Scott ME, Gray-Donald K, Kalumba ON. Multiple infection with
Plasmodium and helminths in communities of low and relatively high socio-economic
status. Ann Trop Med Parasitol 1996; 90:277–93.

207
12. Messina JP, Taylor SM, Meshnick SR, Linke AM, Tshefu AK, Atua B, et al. Population,
behavioural and environmental drivers of malaria prevalence in the Democratic Republic
of Congo. Malar J 2011; 10:161.
13. Atieli H, Menya D, Githeko A, Scott T. House design modifications reduce ndoor resting
malaria vector densities in rice irrigation scheme area in western Kenya. Malar J 2009;
8:108.
14. Lwetoijera DW, Kiware SS, Mageni ZD, Dongus S, Harris C, Devine GJ, et al. A need
for better housing to further reduce indoor malaria transmission in areas with high bed net
coverage. Parasit Vectors 2013; 6:57.
15. Atieli H, Menya D, Githeko A, Scott T. House design modifications reduce indoor
resting malaria vector densities in rice irrigation scheme area in western Kenya. Malar J
2009; 8:108.
16. Karema C, Aregawi MW, Rukundo A, Kabayiza A, Mulindahabi M, Fall IS, et al. Trends
in malaria cases, hospital admissions and deaths following scale-up of anti-malarial
interventions, 2000–2010, Rwanda. Malar J 2012; 11:236.
17. WHO. World malaria report 2011. Geneva: World Health Organization; 2013. Available
at: http://www.who.int/iris/bitstream/10665/97008/1/9789241564694_eng.pdf. Accessed
11th November 2015.
18. WHO. World malaria report 2011. Geneva: World Health Organization; 2014. Available
at: http://www.who.int/malaria/publications/world_malaria_report_2014/wmr-2014-
profiles.pdf. Accessed 11th November 2015.

208
Portfolio - Fredrick KateeraYear Hours/ECT
PhD Student: Fredrick Kateera
PhD period: 2011 - 2015
Name PhD supervisor: Michele van Vugt, Petra F. Mens, Martin P. Grobusch
1. PhD training
General courses
Qualitative Data Analysis: Procedures and Strategies, Universiteit van Wageningen. 2011 1.5
Quantitative Data Analysis: Multivariate Techniques Universiteit van Wageningen. 2011 1.5
Reference Manager 2011 1.5
Computing in R 2011 1
Data collection using mobile technology, International Centre of Insect Physiology
and Ecology, Kisumu, Kenya 2012 -
Malaria Immunology in the tropics, Makerere University/Uganda Virus Research
Institute, Entebbe –Uganda 2012 -
Microsoft Access, Universiteit van Wageningen. 2013 1.5
Introduction to R, Academic Medical Centre 2013 1.5
Using Geographical Information systems, KIT Health/ Royal Tropical Institute 2014 3
2. Parameters of esteem
Grants
Principal Investigator: P. Falciparum Chloroquine and Sulfadoxine - Pyrimethamine
Resistance Marker Prevalence and Diversity in Rwanda by Fogarty Global Health
Fellowship, USA 2015
Co-Principal Investigator: Feasibility and Acceptability of Drug shop and Pharmacy
retailer initiated malaria diagnosis in Rwanda (FAPIM Study) - Joint Afro-TDR Small
Grants Program 2014

209
Awards and Prizes
Travel Grant for the 6th MIM Pan African Malaria conference - South Africa.
Oral presentation: Malaria prevalence, spatial clustering and risk factors in a low
endemic area of Eastern Rwanda: A cross sectional study.
3. Conferences Attended
Oral presentation at the 6th MIM Pan African Malaria conference - South Africa.
Malaria prevalence, spatial clustering and risk factors in a low endemic area of
Eastern Rwanda: A cross sectional study. 2013
Oral presentation at "The Intersection of Human and Veterinary Parasitology" -
Netherlands. Topic: Malaria parasite carriage and risk determinants in a rural
population: a malariometric survey in Rwanda 2015
Poster presentation at the 64th Annual Meeting American Society of Tropical
Medicine and Hygiene - USA. Topic: Malaria parasitemia, anemia and malnutrition
prevalences and interactions among preschool aged children in rural Rwanda - a
community-based survey. 2015

Summary
Malaria disease – particularly that caused by infection with Plasmodium falciparum
parasite - remains a leading cause of severe morbidity and mortality particularly in sub-
Saharan Africa, of which Rwanda is part.
Infection of P. falciparum parasites into the body after a bite with in infected mosquito is
followed by invasion of these parasites into red blood cells where they are transported
around the body including into vital organs like the kidneys and brain where they
frequently sequestrate to cause to severe disease forms. However, despite the severity of
the disease, malaria remains largely preventable. Control measures include use of
artemisinin-based combination therapies (ACTs) for effective treatment; insecticidal
treated nets (ITNs) and indoor residual spraying (IRS) with insecticides and intermittent
preventive therapy for pregnant women (IPTp).
In this thesis, we assessed key determinants of malaria control in a defined community in
eastern Rwanda where malaria transmission, despite high levels of coverage with the
principal malaria control tools of LLINs, IRS and access to ACTs for the treatment of
malaria clinical cases, burden remains high. We explored P. falciparum parasite
characteristics, malaria clinical disease epidemiology for both clinical and asymptomatic
cases, bed net access, ownership and use following mass LLIN distribution, and a malaria
control stakeholder analysis to better characterise current malaria situation as well as
identify key gaps that, when addressed, may lead to declines in malaria transmission and
eventually achievement of malaria pre-elimination status in the study site.
In Chapter 2 of this thesis, we reported a health-facility based survey, malaria case
clinical profiles and parasite densities and genetic diversity were compared among P.
falciparum-infected patients identified at two sites of different malaria transmission
intensities in Rwanda.
This study demonstrated variability in proportional distribution of patient variables of
sex, age group, parasite density, fever experience, and use of bed nets between patients at
two study sites. P. falciparum diversity and allelic frequency were higher at the higher
endemic Ruhuha site compared to the lower endemic Mubuga site. These differences in

211
malaria risk and MOI should be considered when choosing setting-specific, targeted,
malaria control strategies and when assessing parameters such as drug resistance,
immunity and impact of used interventions. The overall results suggest that malaria
diversity can be a proxy measure for malaria transmission intensities, impact of control
interventions and malaria disease severity.
In Chapter 3, we conducted a molecular surveillance of resistance markers to the two
previously used, but later withdrawn antimalarial drugs chloroquine (CQ) and
sulphodoxine-pyrimethanmine (SP) among malaria infected patients identified at two
sites of low and high malaria transmission intensities in Rwanda.
We found a slow emergence of CQ susceptible wild-type parasites 14 years after CQ
withdrawal, and sustained high levels of SP resistance marker polymorphisms 7 years
after complete SP complete withdrawal. Most likely, the high prevalence of SP resistant
parasites and the slow recovery of CQ susceptive parasites is partially associated with the
continued use of Pfdhfr/Pfdhps inhibitors (like trimethoprim-sulfamethoxazole used in
treatment of prophylaxis against bacterial infections among HIV infected individuals) and
IPTp-SP within the East and Central African regions for malaria prevention among
pregnant women and the continued use of CQ or CQ mimicking antimalarial
amodiaquine (AQ), respectively. Continued surveillance of P. falciparum CQ and SP
associated polymorphisms including a delineation of the determinants of anti-malarial
drug sensitivity is recommended for guiding future rational drug policy-making and
mitigation of future risk of anti-malaria drug resistance development.
In Chapter 4, we conducted a cross-sectional study of all households in the sector
seeking to study asymptomatic parasite carriage rates and determinants of malaria
infections among community based predominantly asymptomatic individuals. Overall,
5.1% of all individuals of all ages and gender and 6.5% among children 2-10 years were
found infected with malaria parasites suggesting that the study area is of hypo-endemic
transmission intensity whilst in about 13% of households, at least one household member
was found to be malaria parasitaemic. High malaria parasite carriage risk was associated
with being male, child or adolescent (age group 5–15), reported history of fever and

212
living in a household with multiple occupants. In contrast, risk of malaria parasite
carriage was significantly lower among individuals living in households of, higher socio-
economic status, where the head of household was educated and where the house floor or
walls were made of cement/bricks rather than mud/earth/wood materials. This study
highlights the potential value of improved house design to prevent mosquito entry and to
minimize risk of indoor malaria transmission as efforts supplementary to maintaining
high coverage of other interventions, including IRS and LLIN.
In Chapter 5, we assessed children <5 years for the temporal associations between the
three common medical conditions of malaria, anaemia and undernutrition and explored,
for each medical condition, the associated risk factors for their occurrence. In this study
group, four in ten and one in ten children were found stunted and underweight,
respectively, in an area of low malaria transmission. These findings pointed to high rates
of under-nutrition and anaemia but not malaria parasitaemia in preschool-going children.
A strong association between malaria and anaemia but not between malaria and under-
nutrition was observed. We note that control of malaria may have a substantial indirect
effect of reduction in anaemia burden among pre-school going children in this area.
Integrated rather than vertical programmes covering nutritional rehabilitation, malaria
control including the scaled up LLIN and IRS coverage, improvements in HH SES and
better housing that limits mosquito entry are need to realize optimal child health outputs.
In Chapter 6, we explored bed net source, ownership and use in Ruhuha sector 8 months
after a universal coverage campaign with long-lasting insecticide (UCL) nets.
A 92% household ownership of at least one net and a 72% individual bed nets use was
noted. This study confirmed that males in general and individuals from households of low
socio-economic status (SES), with one or more nets, where more than two sleeping
spaces are used, and those who slept on the floor relative to those who used beds, were
less likely to use a net. To maximize impact of ULC, strategies that target males as well
as those that ensure ITN coverage for all, address barriers to feasible and convenient bed
net use including covering over all sleeping space types, and provide net hanging
supports, are needed.

213
In Chapter 7, a two-stage health facility and household-based survey was conducted
from April to October 2011 to measure malaria prevalence, describe spatial malaria
clustering and investigate for malaria risk factors among health facility presumed malaria
cases and their household members in Eastern Rwanda.
In this study, slide/RDT positivity rates of about 23% and 5% among health centre
malaria presumed cases and HH based asymptomatic cases, respectively, were found. In
addition, reactive case finding by linking health facility identified passive cases to
actively identified household malaria infection, is a potentially powerful surveillance
system for identifying malaria case clusters (hotspots) – households in which malaria risk
is higher than average for a defined area in the community. Also, residents of houses
made of local materials that are porous to vector entry and household where a health
facility malaria confirmed clinical cases was found had higher odds of an asymptomatic
community based member found to be infected with malaria parasites. Especially in low
transmission settings, identifying and treating asymptomatic carriers is key in interrupting
transmission. Therefore, circle surveillance, when combined with knowledge on the
individual, the HH and the environmental malaria risk factors in a given community, can
aid detection of hotspots and inform use of targeted malaria control strategies.
Finally in Chapter 8, an analysis of the value of different community stakeholders within
the community based malaria interventions in the Ruhuha study site was conducted. The
systematic identification of community-based stakeholders in a research process is an
effective way of harnessing resources, leveraging the contributions of various
stakeholders, optimising opportunities and effectively engaging and working with
community members especially when tackling an issue of significant public health
priority. The multiple-stakeholder-based approach in the early stage of the project
facilitated the study team’ s knowledge of whom, when and how to engage and thus
resulted in the support and agreement of malaria control related interventions and
processes as also suggested elsewhere. Due to high levels of interdependency between
stakeholders, platforms to facilitate teamwork are needed to pool together their combined
efforts. The contextual value of stakeholder involvement and strategies to guide their

214
contributions towards the one goal of reducing malaria transmission in a sustainable,
community owned manner are needed.
This thesis shows that, further declines in malaria transmission will require a concerted
community engagement, optimal use of existing interventions and improvements in
household level SES and better quality of housing. For optimal malaria control,
integrated scaled-up interventions that are accessible to all at risk populations is required.
Across the different malaria transmission settings, epidemiological studies including
coverage and impact of deployed tools, residual malaria parasite reservoir, determinants
of continued malaria infections and drug effectiveness are needed to inform area specific
control strategies.

215
Samenvatting
De ziekte malaria - met name die veroorzaakt wordt door infectie met de
Plasmodium falciparum parasiet - blijft een van de voornaamste redenen voor morbiditeit
en mortaliteit in Sub-Sahara Africa, waar Rwanda onderdeel van is.
Infectie met P. falciparum na een beet van een geïnfecteerde mug wordt gevolgd door
invasie van deze parasieten in de rode bloedcellen waarna ze getransporteerd worden
door het lichaam waaronder de vitale organen zoals nie en en hersenen waar
de parasieten sequestreren en ernstige ziekte veroorzaken. Malaria kan ondanks de ernst
van de ziekte voor een groot deel voorkomen worden. Controle mechanismen behelzen
onder andere Artemisinine combinatie therapie (ACTs) voor effectieve behandeling,
Insecticide behandelde klamboes (LLIN) en het binnenshuis sprayen van
insecticiden (IRS) en intermitterende preventieve therapie voor zwangere vrouwen.
In dit proefschrift hebben we de belangrijkste determinanten voor malaria controle
bestudeerd in een specifieke gemeenschap in Oost Rwanda waar ondanks een hoge
dekkingsgraad van malaria controle strategieën zoals LLIN, IRS en ACTs voor
behandeling van klinische malaria gevallen de malaria transmissie hoog blijft. We hebben
de P. falciparum karakteristieken, epidemiologie van zowel klinische malaria als
asymptomatische infectie, toegang tot, bezit en gebruik van klamboes na een massa
distributie campagne onderzocht en een malaria stakeholder analyse uitgevoerd om de
huidige malaria situatie te karakteriseren en de te identificeren die wanneer
aangepakt zouden kunnen leiden tot vermindering in malaria transmissie en uiteindelijk
het behalen van malaria pre-eliminatie status in het studiegebied.
In hoofdstuk 2 van dit proefschrift, rapporteren wij een gezondheidscentrum gebaseerd
onderzoek waarin het klinische profiel, parasiet dichtheden en genetische variabiliteit
wordt onderzocht in twee verschillende in Rwanda met verschillende malaria
transmissie intensiteit. Deze studie liet variabiliteit zien tussen beide studielocaties in de
proportionele distributie van de patiënten variabelen; geslacht, leeftijdsgroep,
parasietdichtheid, koortsbeleving en het gebruik van klamboes. P. falciparum diversiteit

216
en allel frequentie was hoger in het hoog endemische gebied Ruhuha in vergelijking met
he laag endemische gebied Mubuga. Deze verschillen in malaria risico en MOI moeten in
ogenschouw worden genomen wanneer gebied-specifieke malaria controle strategieën
worden gekozen en wanneer parameters zoals drug resistentie, immuniteit en impact van
interventies worden bestudeerd. In totaliteit suggereren de resultaten dat malaria
diversiteit een proxy kan zijn voor malaria transmissie intensiteit, impact van controle
interventie en malaria ziekte ernst.
In hoofdstuk 3, hebben we een moleculaire studie gedaan naar resistentie markers
van twee eerder gebruikte, maar later teruggetrokken antimalaria middelen chloroquine
(CQ) en sulphodoxine-pyrimethanmine (SP
Wij vonden een langzame terugkeer van CQ gevoelige wild-type parasieten 14 jaar na het
van de markt halen van CQ en een constant hoog niveau van SP resistente
polymorfismen 7 jaar na de volledige terugtrekking van SP. Waarschijnlijk is de hoge
prevalentie van SP resistente parasieten en de langzame terugkeer van CQ gevoelige
parasieten voor een deel te wijten aan het continue gebruik van Pfdhfr/Pfdhps inhibitoren
zoals trimethoprim-sulfamethoxazole dat gebruikt wordt ter voorkoming van bacteriële
infecties in HIV geïnfecteerde personen, IPTp-SP in Oost en Centraal Afrika ter
voorkoming van malaria in zwangere vrouwen en het continue gebruik van CQ of
middelen die at betreft werkingsmechanisme lijken op CQ zoals
amodiaquine. Continue surveillance van P. falciparum CQ en SP geassocieerde
polmorfismen inclusief het ontcijferen van de determinanten die zorgen voor
antimalaria gevoeligheid is aan te raden om toekomstig gebruik en
beleid te l den en om toekomstige antimalaria resistentie te voorkomen.
In hoofdstuk 4 hebben we een cross-sectionele studie gedaan van alle huishoudens in de
sector om de hoeveelheid asymptomatische parasite dragers te identificeren en de
determinanten van Plasmodium infecties onder de gemeenschap te identificeren.
5.1% van alle individuen van alle leeftijden en geslacht en 6.5% van de kinderen tussen

217
de 2-10 jaar had een infectie met malaria parasieten. Hieruit volgt dat het studiegebied
hypoendemisch is. In 13% van de huishoudens was op zijn minst een lid geïnfecteerd met
malaria parasieten. Hoge parasietendragerschap was geassocieerd met geslacht (mannen
hadden hoger risico), leeftijd (kinderen tussen 5-15 hadden hoger risico), geschiedenis
van koorts en wonen in een huishouden met meerdere leden. Het risico op infectie was
significant lager bij individuen die woonden in een huishouden met een hoge socio-
economische status, waar het hoofd van een huishouden opgeleid was en waar vloeren en
muren gemaakt waren van cement of stenen in plaats van modder aarde of hout.
Deze studie benadrukt de potentiele waarde van verbeteringen aan huizen om muggen
toegang te voorkomen en om het risico om malaria transmissie binnenshuis te verkleinen
als aanvulling op het behouden van hoge klamboe bezit en vector controle door middel
van insecticide spraying.
In hoofdstuk 5, hebben we kinderen jonger dan 5 bestudeerd voor associaties tussen en
risico factoren van 3 bekende medische aandoeningen; malaria anemie en ondervoeding.
In deze studiegroep was 4 op de 10 kinderen achter in groei en 1 op de 10 heeft
ondergewicht. Er waren weinig malaria positieve kinderen in deze setting. Er was een
sterke associatie tussen malaria en anemie maar niet tussen ondervoeding en malaria. We
zien dat de controle van malaria indirect ook een substantieel effect op anemie in deze
jonge kinderen kan hebben. Geïntegreerde in plaats van verticale programma’s die zowel
voedings-programma’s als malaria controle programma’s met klamboes en binnenshuis
vector controle en verbeteringen in socio-economische status behelzen kunnen een goed
begin zijn om de jeugdgezondheidsuitkomsten te verbeteren.
In hoofdstuk 6, hebben we klamboe oorsprong, bezit en gebruik in Ruhuha sector
bestudeerd, 8 maanden na een universele distributie campagne met langdurig
geïmpregneerde klamboes.
92% van de huishoudens had op zijn minst 1 klamboe en in 72% werd klamboe gebruik
gevonden. Deze studie bevestigd dat mannen en personen komende van een huishouden
van lage socio-economische status met 1 of meerdere klamboes en een huis met meerdere
slaapplaatsen op de vloer in plaats van een bed, minder vaak een klamboe gebruikten in

218
vergelijking met andere groepen. Om de impact van de klamboes te vergroten zijn
strategieën die op mannen gericht zijn en strategieën die barrières voor het gebruik
weghalen (zoals klamboesgeschikt voor alle soorten slaapplaatsen en het helpen met het
bevestigen van klamboes) nodig.
Hoofdstuk 7 beschrijft een tweedelige studie in een gezondheidscentrum en in
huishoudens. De studie werd uitgevoerd tussen van April tot Oktober 2011 om malaria
prevalentie, spatiele malaria clustering en malaria risico factoren te bestuderen bij
patiënten in het gezondheidscentrum met koorts en hun huisgenoten.
In deze studie was het microscopie en of RDT positieve gevallen onder bezoekers met
koorts van het gezondheidscentrum en zijn of haar asymptomatische huisgenoten
respectievelijk 23% en 5%. Daarbij komt dat “reactive case finding” doormiddel van het
linken van patiënten die zich presenteren bij het ziekenhuis met malaria aan hun
huisgenoten mogelijk een krachtige surveillance methode is om malaria clusters oftewel
hotspots (huishoudens met meer dan gemiddeld malaria risico in een gemeenschap) te
identificeren. Naast dat huishoudens met een in de kliniek bevestigde malaria patiënt een
hogere kans hadden om asymptomatisch parasietdragers in het huishouden te hebben
blijkt ook uit deze studie dat huizen die gemaakt zijn van lokale materialen die het
binnendringen van de vector mogelijk maken een hogere kans hebben op
asymptomatische dragers in het huishouden. Met name in gebieden waar de transmissie
laag is, is het essentieel om asymptomatisch dragers te identificeren en te behandelen.
Cirkel surveillance, gecombineerd met kennis van de index case, het huishouden en de
risico factoren uit de omgeving van een specifieke gemeenschap kan de detectie van
hotspots verbeteren en informatie verschaffen ten behoeve van gerichte malaria controle
strategieën.
In hoofdstuk 8, is een analyse van de waarde van verschillende stakeholders van de
gemeenschap binnen de gemeenschap-gebasseerde interventies onderzocht in Ruhuha,
het studiegebied waar de interventies plaatsvonden. De systematische identificatie van
stakeholders in een onderzoeksproces is een effectieve methode om de contributies van
stakeholders in kaart te brengen, processen te optimaliseren en draagvlak te creëren Dit is

219
belangrijk als er een probleem met grote gezondheid impact wordt aangepakt. D
meerdere-stakeholder gebaseerde methode die toegepast werd vanaf het begin van het
project heft eraan bijgedragen dat het studie team wist wie, wanneer, wat deed en welke
interactie nodig was. Vanwege de hoge afhankelijkheid tussen de verschillende
stakeholders is een platform om de samenwerking te coördineren nodig.
Dit proefschrift laa zien dat verdere reducties in malaria transmissie een go de
samenwerking tussen stakeholders behoeft. Gemeenschapszin, optimaal gebruik van
bestaande interventies en verbetering van de levensstandaard zijn essentieel. Voor
optimale controle van malaria is een geïntegreerde opschaling van deze interventies
nodig die toegankelijk zijn voor alle groepen die risico lopen op malaria.
Epidemiologische studies die verspreiding en impact van de gebruikte interventies,
overgebleven malaria reservoirs, en determinanten van continuerende transmissie en
effectiviteit bestude blijven nodig om beleid te kunnen informeren
over de te nemen controle strategieën .

220
AUTHORS AND AFFILIATIONS
Alexis Rulisa
Department of Cultural Anthropology and Development Studies and Centre for
International Development Issues, Radboud University, Nijmegen, The Netherlands
Bart Van Den Borne
Department of Health Promotion, Maastricht University, The Netherlands
Chantal M. Ingabire
Department of Health Promotion, Maastricht University, The Netherlands
Claude Muvunyi
School of Medicine, College of Medicine and Health Sciences, University of Rwanda,
Kigali, Rwanda
Constantianus JM Koenraadt
Laboratory of Entomology, Wageningen University, Wageningen, The Netherlands
Emmanuel Hakizimana
Malaria & Other Parasitic Diseases Division, Rwanda Biomedical Center, Kigali,
Rwanda
Ingmar Nieuwold
Foundation The100th Village, Amsterdam, The Netherlands
Jane Alaii
Context Factor Solutions, Nairobi, Kenya
Javier Dukuzumuremyi
Amsterdam Institute for Global Health and Development, INTERACT Project, Kigali,
Rwanda

221
Jean de Dieu Harelimana
Amsterdam Institute for Global Health and Development, INTERACT Project, Kigali,
Rwanda
Jean Pierre Bizimana
Geography Department, Faculty of Science, National University of Rwanda, Huye,
Rwanda,
Kimberly R. Boer
Amsterdam Institute for Global Health and Development, INTERACT Project, Kigali,
Rwanda
Leon Mutesa
School of Medicine, College of Medicine and Health Sciences, University of Rwanda,
Kigali, Rwanda
Liberata Muragijemariya
Ruhuha Health Centre, Ruhuha Sector, Bugesera, Rwanda
Lisette Baas
Amsterdam Institute for Global Health and Development, INTERACT Project, Kigali,
Rwanda
Martin P. Grobusch
Centre of Tropical Medicine and Travel Medicine, Department of Infectious Diseases,
Division of Internal Medicine, Amsterdam, The Netherlands
Michele van Vugt
Centre of Tropical Medicine and Travel Medicine, Department of Infectious Diseases,
Division of Internal Medicine, Amsterdam, The Netherlands

222
Nirbhay Kumar
Department of Tropical Medicine, School of Public Health and Tropical Medicine,
Vector-Borne Infectious Disease Research Centre, Tulane University, New Orleans, LA,
USA
Parfait Karinda
Medical Research Centre Division, Rwanda Biomedical Centre, Kigali, Rwanda
Peter J. de Vries
Department of Internal Medicine, Tergooiziekenhuizen, Hilversum, The Netherland
Petra F. Mens
Royal Tropical Institute/Koninklijk Instituutvoor de Tropen, KIT Biomedical Research,
Amsterdam, The Netherlands
Sam L. Nsobya
Department of Pathology, School Biomedical Science, College of Health Science,
Makerere University, Kampala, Uganda
Stephen Rulisa
University Teaching Hospital of Kigali, National University of Rwanda, Kigali, Rwanda,
Stephen Tukwasibwe
Molecular Research Laboratory, Infectious Disease Research Collaboration, New Mulago
Hospital Complex, Kampala, Uganda
Steven Agaba
Amsterdam Institute for Global Health and Development, INTERACT Project, Kigali,
Rwanda

223
Acknowledgements
The success of my doctoral training has largely been due to the work and support of a
number of people who have greatly impacted my career growth, academic training,
personal guidance and helped shape my thinking and this thesis.
First and foremost, I would like to mention my “first-line of defence” co-promoters, Dr
Michele van Vugt, Dr. Petra F. Mens, my Rwandan PI Dr. Leon Mutesa and my
Promoter Prof. Martin P. Grobusch. Michele – You became a “mother” and fount of
support in every way and I always knew that if I needed anything, you love and care
would provide. Petra - I am extremely grateful for your thorough and principled yet
unyielding commitment every step of the way. You reviewed every word, sentence,
paragraph and all the punctuation marks with diligence and passion to better our work.
Dr. Leon – I shall never forget how you picked up the program and team in Rwanda at
time of gloom and uncertainty. Prof Martin – I still don’t get it! – How you make time to
go through every word in every draft and provide wonderful guidance and counsel in
spite of your super-hectic schedule. To you four –I am eternally grateful for your
kindness, guidance, support and belief in me that made me feel important and valued.
This PhD training was an integrated endeavour shared with my colleagues: Chantal
Ingabire; Emmanuel Hakizimana and Alexis Rulisa. Siblings of “common suffrage”. I
also want to acknowledge Prof. Nirbhay Kumar – Tulane University and Dr. Sam Nsobya
and Stephen Tukwasibwe for their collaborations. Thank you to NWO-WOTRO program
for funding my PhD training and MEPR project for the field support.
Now, to the triple-braided cord that cannot be broken and upon which my life is
anchored: My wife Brenda for her prayers, encouragement, support and in particularly,
for managing our home and family alone every time I was away. To my greatest hope
and deepest love – My sons Ian Nshuti and Shaun Irakunda – you are everything to me.
Finally and MOST IMPORTANTLY, to my heavenly father – my God, the desire of all
Nations and hope of Ages to come: I am persuaded of your utmost love to me. You surely
perfect that which concerns me. To you my most precious DAD -a million thank.

224
Biography & List of Publications
Biography
Fredrick Kateera was born the 24th December 1975 in Mbale District, Eastern Uganda.
He undertook his primary and secondary education in Jinja District, advanced level
education in Tororo district, from which he joining Makerere University and obtained his
Bachelors of Medicine and Bachelors of Surgery M.B.Ch.B (general Medicine).
He obtained two Masters of science degrees: Msc Epidemiology from the London School
of Hygiene and Tropical Medicine and MSc Immunology & Immunogenetics from the
University of University of Manchester, Manchester, UK.
He later started his PhD at the Center of Tropical Medicine and Travel Medicine of the
Academic Medical Center of Amsterdam under the supervision of dr. Michèle van Vugt
and dr. Petra Mens with promotion over sight from Prof. Martin Grobusch. For his PhD,
he carried out studies on determinants of malaria control in a community in rural eastern
Rwanda. Results of this research are presented in this PhD thesis.
Since January 2016, Fredrick is employed by Harvard University affiliated Non-
Governmental Organization called Partners In Health Rwanda as its research Director.
With over 10 years of experience in clinical care, research implementation, and program
management, with in East Africa, he now works as a epidemiologist: to design, test and
share innovative health care delivery systems that minimize poverty related barriers to
access to medical care; to set up and monitor longitudinally disease and health metric
changes longitudinally in a defined population in Rwanda and in academia. His passion is
in leveraging health systems at community level to identify innovative prevention, early
detection and prompt management of patients for better outcomes.
Fredrick is married Brenda Asiimwe with whom they have two children: Ian and Shaun.

225
Publications
1. Gasasira AF, Kamya MR, Ochong EO, Vora N, Achan J, Charlebois E, Ruel T, Kateera
F, Meya DN, Havlir D, Rosenthal PJ, Dorsey G. Effect of trimethoprim-
sulphamethoxazole on the risk of malaria in HIV-infected Ugandan children living in an
area of widespread antifolate resistance. Malar J 2010; 23(9): 177.
2. Stephen Rulisa, Fredrick Kateera, Jean Pierre Bizimana, Steven Agaba, Javier
Dukuzumuremyi, Lisette Baas, Jean de Dieu Harelimana, Petra F Mens, Kimberly R
Boer, Peter J de Vries. Malaria prevalence, spatial clustering and risk factors in a low
endemic area of Eastern Rwanda: a cross sectional study. PLoS One 2013; 8(7): e69443.
3. Chantal Marie Ingabire, Jane Alaii, Emmanuel Hakizimana, Fredrick Kateera, Daniel
Muhimuzi, Ingmar Nieuwold, Karsten Bezooijen, Stephen Rulisa, Nadine Kaligirwa,
Claude Muvunyi, Constantianus Jm Koenraadt, Leon Mutesa, Michele Van Vugt, Bart
Van Den Borne. Community mobilization for malaria elimination: application of an open
space methodology in Ruhuha sector, Rwanda. Malaria Journal, 2014; 13:167.
4. Kateera Fredrick, Petra F Mens PF, Emmanuel Hakizimana, Chantal M Ingabire,
Liberata Muragijemariya, Parfait Karinda, Martin P Grobusch, Leon Mutesa, Michèle
van Vugt. Malaria parasite carriage and risk determinants in a rural population: a
malariometric survey in Rwanda. Malaria Journal, 2015; 14:16.
5. Kateera Fredrick, Walker TD, Mutesa L, Mutabazi V, Musabeyesu E, Mukabatsinda C,
Bihizimana P, Kyamanywa P, Karenzi B, Orikiiriza JT. Hepatitis B and C seroprevalence
among health care workers in a tertiary hospital in Rwanda. Trans R Soc Trop Med Hyg.
2015; 109(3): 203-208.
6. Kateera Fredrick, Ingabire CM, Hakizimana E, Rulisa A, Karinda P, Grobusch MP,
Mutesa L, van Vugt M, Mens PF. Long-lasting insecticidal net source, ownership and use
in the context of universal coverage: a household survey in eastern Rwanda. Malar J.
2015; 14(1): 390.
7. Kateera F, Ingabire CM, Hakizimana E, Kalinda P, Mens PF, Grobusch MP, et al.
Malaria, anaemia and under-nutrition: three frequently co-existing conditions among
preschool children in rural Rwanda. Malar J 2015; 14(1): 440.

226
8. Egziabher TG, E. Ngoga, B. Karenzi, F. Kateera. Obstetric fistula management and
predictors of successful closure among women attending a public tertiary hospital in
Rwanda: a retrospective review of records. BMC Res Notes 2015; 8:774.
9. Bitwayiki R, Orikiiriza JT, Kateera F, Bihizimana P, Karenzi B, Kyamanywa P, Walker
TD. Dyspepsia prevalence and impact on quality of life among Rwandan healthcare
workers: A cross-sectional survey. S Afr Med J. 2015; 105(12): 1064-1069.
10. Ingabire CM, Kateera F, Hakizimana E, Rulisa A, Muvunyi C, Mens P, Koenraadt CJ,
Mutesa L, Van Vugt M, Van Den Borne B, Alaii J. Determinants of prompt and adequate
care among presumed malaria cases in a community in eastern Rwanda: a cross sectional
study. Malar J. 2016; 15(1): 227.
11. Kateera F, Nsobya SL, Tukwasibwe S, Mens PF, Hakizimana E, Grobusch MP, Mutesa
L, Kumar N, van Vugt M. Malaria case clinical profiles and Plasmodium falciparum
parasite genetic diversity: a cross sectional survey at two sites of different malaria
transmission intensities in Rwanda. Malar J 2016; 15 (1): 237.