Embed Size (px)
Citation preview


Dissertation for the Degree of Doctor of Philosophy (Faculty of Pharmacy) inPharmacokinetics and Drug Therapy presented at Uppsala University in 2002
ABSTRACT
Wählby, U. 2002. Methodological Studies on Covariate Model Building in PopulationPharmacokinetic-Pharmacodynamic Analysis. Acta Univ. Ups. Comprehensive Summaries ofUppsala Dissertations from the Faculty of Pharmacy 280. 60 pp. Uppsala. ISBN 91-554-5469-0
Population pharmacokinetic (PK) – pharmacodynamic (PD) modelling, using nonlinear mixedeffects models, is increasingly being applied to obtain PK-PD information in drugdevelopment. Covariate modelling, the establishment of relationships between modelparameters and patient characteristics, is undertaken to explain PK-PD variability andfacilitate dose adjustment decisions, and is consequently an important objective of populationPK-PD.
The aims of this thesis were to increase the efficiency, predictability and robustness ofcovariate model building by examining in detail a number of aspects related to covariatemodelling. The thesis demonstrates that the likelihood ratio (LR) test can be applied withconfidence, in the assessment of statistical significance of parameter-covariate relationships(in NONMEM analyses), only if an estimation method appropriate for the data- and error-structure is utilised. Conversely, caution is needed in the interpretation of the LR test whenvariance or covariance parameters are modelled, since the type I error rate may be severelyupward biased if the assumptions of normally distributed residuals and/or enough informationin the data are violated. The two stepwise covariate model building procedures, usinggeneralised additive models and NONMEM, were found to perform similarly in the examplesexamined. However, differences in performance may prevail in other situations, e.g. whensparse sampling precludes reliable individual parameter estimates. Stepwise selection wasshown to result in over-estimated covariate effects (selection bias), but the imprecision in theestimates exceeded this bias. Important information about the PK-PD characteristics of a drugis obtainable on the application of covariate models for time-varying covariates that accountfor differences in variability between and within individuals, or estimate interindividualvariability in the covariate effect. The knowledge gained in this thesis will contribute to thedevelopment of more predictable and robust covariate models, important both inindividualisation of dosage and the development of new drugs.
Ulrika Wählby, Department of Pharmaceutical Biosciences, Division of Pharmacokineticsand Drug Therapy, Biomedical Centre, Box 591, SE-751 24 Uppsala, Sweden
© Ulrika Wählby 2002
ISSN 0282-7484ISBN 91-554-5469-0
Printed in Sweden by Uppsala University, Tryck & Medier, Uppsala 2002


PAPERS DISCUSSED
This thesis is based on the following papers, which will be referred to by their Romannumerals in the text.
I. Wählby U., Jonsson E. N. and Karlsson M. O., Assessment of ActualSignificance Levels for Covariate Effects in NONMEM, J PharmacokinPharmacodyn 28(3): 231-252, 2001
II. Wählby U., Bouw M. R., Jonsson E. N. and Karlsson M. O., Assessment ofType I Error Rates for the Statistical Sub-model in NONMEM, JPharmacokin Pharmacodyn 29(3): 251-269, 2002
III. Wählby U., Matolcsi K., Karlsson M. O. and Jonsson E. N., Evaluation ofType I Error Rates when Modeling Ordered Categorical Data in NONMEM,in manuscript
IV. Wählby U., Jonsson E. N. and Karlsson M. O., Comparison of StepwiseCovariate Model Building Strategies in Population Pharmacokinetic-Pharmacodynamic Analysis, AAPS PharmSci 2002; 4 (4) article 27(http://www.aapspharmsci.org)
V. Wählby U., Thomson A. H., Milligan P. A. and Karlsson M. O., TwoModels Specific to Time-varying Covariates; Application in PopulationPharmacokinetic-Pharmacodynamic Model Building, in manuscript
VI. Kerbusch T., Wählby U., Milligan P. A. and Karlsson M. O., PopulationPharmacokinetic Modeling of Saturable First Pass Metabolism, CYP2D6-Genotype and Formulation-dependent Bioavailability of Darifenacin and itsMetabolite Across 18 Phase 1 and 2 Studies, submitted
Reprints were made with permission from the publishers.

CONTENTS
Abbreviations & Nomenclature 7
1 Introduction 91.1 Overview 9
1.2 The mixed effects model 101.2.1 Model definition 101.2.2 Model estimation 12
1.3 Covariate modelling 131.3.1 Covariate data – graphical presentation 141.3.2 Identification of candidate covariates 141.3.3 Formulating the covariate model 171.3.4 Model selection 201.3.5 Assessing the performance 21
1.4 Simulations – methodological studies 23
2 Aims of the thesis 24
3 Methods 253.1 Simulation and analysis of data – software 25
3.2 Data & models 253.2.1 Simulations to assess the Type I error rate 253.2.2 Real data to assess the Type I error rate 263.2.3 Simulated data to compare stepwise covariate modelling 273.2.4 Real data to compare stepwise covariate modelling 273.2.5 Simulated data to assess selection bias 273.2.6 Data sets & models – time-varying covariates 283.2.7 Darifenacin data & model 30

3.3 Analysis procedures & methodology 303.3.1 Covariate model 303.3.2 Estimation of Type I error rates of the LR test 303.3.3 Covariate randomisation – Type I error rates for real data 323.3.4 Comparison of stepwise covariate model building procedures 323.3.5 Assessment of selection bias 333.3.6 Application of two models for time-varying covariates 333.3.7 Darifenacin covariate analysis 34
3.4 Model comparison 353.4.1 Comparison of covariate models 353.4.2 Assessment of predictive performance 35
4 Results 364.1 Type I error rates of the LR test 36
4.1.1 Inclusion of a false covariate effect 364.1.2 Inclusion of a false variance of covariance term 38
4.2 Comparison of stepwise covariate model building procedures 40
4.3 Selection bias in stepwise covariate modelling 42
4.4 Two models for time-varying covariates 43
4.5 Darifenacin covariate analysis 45
5 Discussion 46
6 Summary & Conclusions 50
7 Acknowledgments 52
8 References 54

7
ABBREVIATIONS & NOMENCLATURE
AIC Akaike information criteriaALB albuminALKP alkaline phosphataseALT alanine aminotransferaseAST aspartate aminotransferaseAV artificial ventilationBCOV baseline covariate valueBIL bilirubinBSA body surface areaCirc0 baseline neutrophil cell countCobs,ij observed concentration for individual i at time-point jCpred,ij predicted concentration for individual i at time-point jCAT concomitant treatment with catecholamineCEN centreCI confidence intervalCL clearanceCL/F clearance scaled by bioavailabilityCLCR creatinine clearanceCON concomitant medicationCOV covariateCYP cytochrome P450DCOV difference in covariate from baseline covariate valueEM extensive metaboliser (CYP2D6/2C19)df degrees of freedomfn() a functionF bioavailabilityFDA (US) Food and Drug AdministrationFO the first-order estimation method in NONMEMFOCE the first-order conditional estimation method in NONMEMFOCE INTER FOCE with interaction between interindividual and residual errorGAM generalised additive modelsGAM-NM stepwise covariate model building procedure using GAM and NONMEMGLAS Glasgow scoreGLS generalised least squaresh hoursHCTZ concomitant treatment with hydrochlorothiazidehet-EM heterozygous extensive metaboliserheteroscedastic error varying in magnitude (unequal variance)hom-EM homozygous extensive metaboliserhomoscedastic constant error (equal variance)HR heart rateHT heightIIV interindividual variabilityIOV interoccasion variability; within-individual between-occasion variability

8
IU international unitsiv intravenousKa first order absorption rate constantkg kilogramL litreLR likelihood ratioM mole per litremg milligramMLR multiple linear regressionMPE mean prediction error; measure of biasMTT mean transit timen number (general)NM-NM stepwise covariate model building procedure within NONMEMOFV minimum objective function value∆OFV difference in OFV; likelihood ratioP typical (mean) value of the parameter P in the populationPi individual estimate of the parameter PPD pharmacodynamicPE prediction errorposthoc individual empirical Bayes’ estimate; estimated a posterioriPK pharmacokineticPM poor metaboliser (CYP2D6/2C19)PROP concomitant treatment with propranololPT prothrombin levelQ intercompartment clearanceRMSE root mean square error; measure of precisionSAPS simplified acute physiology scoreSBP systolic blood pressureSE standard errorSECR serum creatinineSlope coefficient in the linear drug effectSMOK smokingType I error rate the probability of a false positive resultV volume of distribution (V1 – central volume of distribution)V/F volume of distribution scaled by bioavailabilityWT body weightXi individual covariate
α the intercept in GAM or MLRβ linear regression coefficient in MLRγ feedback parameter (in neutrophil count model)ε the difference between observed and individual predicted concentration, residual errorη the difference between population and individual parameter estimateθ fixed effects parameter, the typical value of a parameterκ the difference in the individual parameter between occasionsπ2 variance of the κsσ2 variance of the εsω2 variance of the ηsΩ variance-covariance matrix of the ηs

9
INTRODUCTION
1.1 Overview
Population pharmacokinetic (PK) – pharmacodynamic (PD) modelling involves theapplication of nonlinear mixed effects models to repeated measurements data from agroup of people, in order to estimate mean PK-PD and variability parameters and todescribe variability in terms of patient characteristics. Modelling provides a tool forlearning/understanding the relationship between the drug dose and its concentration(PK) and between the drug concentration and its effects/toxicity in the body (PD) (1).PK-PD modelling can be utilised to support decisions in drug therapy, and to makepredictions and dosage recommendations (2), and thereby contributes to the efficiencyof the drug development process.
The population approach to analysis was originally proposed for application toroutinely collected clinical data (3, 4), i.e. sparse and unbalanced observations from alarge group of heterogeneous individuals. However, it is now applied more frequentlyin clinical studies for assessing PK and PD characteristics (5, 6), and may entailfrequent or infrequent measurements in small and/or large populations through allphases of drug development (7-11). The US Food and Drug Administration (FDA)also encourage the use of the population approach for the evaluation of PK (9).
Traditional PK studies usually involve frequent sampling in a small, and oftenhomogeneous, group of individuals (12). Data are analysed using the so-called two-stage method, where individual pharmacokinetic parameters are first calculated, andmeans and variability are determined in a second stage. In population PK-PD analysis(hereafter referred to as population PK), data from all individuals are analysedsimultaneously, although the model is able to differentiate between interindividual andintraindividual data (5), and mean and variability parameters are estimated at the sametime. This is a more efficient way of utilising the data, as information can be sharedamong individuals. It enables parameter estimates to be obtained even for thoseindividuals with too few observations to allow estimation using alternative methods.The nonlinear mixed effects approach has advantages over traditional PK methods(13), in that it provides a more accurate estimate of the variability in the population.Further, since this method does not necessitate frequent sampling, samples can bedrawn at regular visits to the clinic. The PK and PD of a drug can therefore more easilybe characterised in the patient group for which the drug is intended. Sparse samplingalso allows the study of populations which are difficult to study from an ethical

10
perspective, such as neonates, the elderly, or the severely ill.
One of the main aims of population PK is covariate model building, i.e. theestablishment of relationships between model parameters and covariates. Covariatesare individual-specific variables that describe patient demographics (e.g. age, weight),disease (e.g. organ function indices) or environmental factors (e.g. concomitantmedication, alcohol consumption). The parameter-covariate relationships can (partly)explain why drug PK or PD varies among individuals. More importantly, sub-groupsin the patient population that are at risk of receiving toxic/ineffective concentrationscan be identified, and the need for and benefits of dose adjustment can be assessed. Inaddition, covariate models can be used to help decide how dose adjustment optimallyshould be achieved (e.g. (14-16)).
1.2 The mixed effects model
1.2.1 Model definition
Population PK utilises nonlinear mixed effects models, where the term ‘mixed’denotes the combination of fixed and random effects. The population PK model can beviewed as comprising three sub-models: structural, statistical and covariate. Thestructural (PK-PD) sub-model describes the overall trend in the data (e.g. one-compartment model, or Emax-model), using fixed effects parameters (e.g. clearance(CL), or Emax). The statistical sub-model accounts for variability by using two levelsof random effects, interindividual variability (IIV) and residual variability. Thecovariate sub-model expresses relationships between covariates and model parameters,using fixed effects parameters.
The individual parameter (e.g. CLi) can be described by:
CLi = θCL + ηi (1.1)
The subscript i denotes individual, the fixed effects parameter θCL represents the mean(typical) value of CL in the population, and ηi is a random effect accounting for theindividual difference from the typical value (IIV). The ηi values are assumed to benormally distributed in the population, with a mean of zero, and an estimated varianceof ω2. The variance-covariance matrix of the ηs (Ω) is estimated. If CL is dependent onrenal function, CLi can be described as a function of a covariate reflecting renalfunction, e.g. creatinine clearance (CLCR):
CLi = θCL + θCLCR × CLCR + ηi (1.2)
θCLCR is a fixed effects parameter describing the linear dependence of CL on the fixedeffect CLCR.

11
Even if the mean parameters for an individual were known, and these were used topredict the drug concentration in that individual at a certain point in time, j, themeasured (or observed) concentration (Cobs,ij) would differ from the predicted (Cpred,ij).This discrepancy, εij, is referred to as residual error; it may be the result of assay error,errors in dose or sampling time, and model misspecification.
Cobs,ij = Cpred,ij + εij (1.3)
The εij values are assumed to be normally distributed with a mean of zero, and anestimated variance of σ2.
In equations 1.1 and 1.3, the models for the residual error and the IIV are additive, i.e.a constant (homoscedastic) error is assumed, although different models may be used.The error may be proportional to the predicted concentration (or the parameter), Cobs,ij
= Cpred,ij(1+εij), and the distribution may be assumed to be lognormal (rather thannormal), e.g. CLi=θCL×expηi. In these cases, the error increases proportionally withincreases in the concentration/parameter (with a constant coefficient of variation), andthus is heteroscedastic. The additive and proportional residual error models can also becombined, and in some situations more elaborate models are required, e.g. using log-transformation, including auto-correlation (17) or varying residual error magnitudebetween subjects (18).
If parameters show random variation within individuals between study occasions,known as inter-occasion variability (IOV), this variability can also be quantified in thepopulation PK model (19). Equation 1.4 shows the model for IOV, where the CL ofdrug in individual i at occasion k (CLik) differs from the mean CLi by an additional(zero mean, variance π2) random effect, κik, which accounts for the intraindividual,between-occasion variability.
CLik = θCL + ηi + κik (1.4)
The three sub-models are interrelated, and the choice of structural (and statistical)model may affect the choice of covariate model and vice versa (20). The process offinding a model that adequately describes the data is thus an elaborate task, wheremodel refinement/checking must be performed in several steps. In a general approachto building the population PK model, after identifying an acceptable structural model,including adequate random effects, the influences of covariates are explored, andfinally the model components are re-tested for relevance.

12
1.2.2 Model estimation
There are a number of software packages for estimating population PK (21, 22), all ofwhich are based on hierarchical nonlinear mixed effects modelling (23). The methodscan be categorised into three groups: parametric, (semi-)nonparametric and Bayesian.The parametric methods (e.g. NONMEM (24), NLME in S-PLUS (25), NLINMIX inSAS (26), WinNonMix (27)) differ from the nonparametric methods (e.g. NPML (28),NPEM (29), (semi-nonparametric) NLMIX (30)) by the assumption of a specificdistribution of the random effects. In the Bayesian (e.g. POPKAN (31), BUGS (32))software, prior information on the parameters is utilised in the estimation. Limitedcomparisons of the software have been made, and these showed no major differencesin the resulting models (33, 34). However, the covariates are handled in different waysin these software groups. The general issues on covariate modelling discussed in thisthesis apply to all parametric methods, although the focus will be on NONMEM (24)as this software was used in the analyses.
1.2.2.1 Estimation in NONMEM
In NONMEM, parameters are estimated via a maximum likelihood approach, wherebya joint function (the objective function) of all model parameters and the data (theobservations) is evaluated. This function expresses the likelihood that the observationsarise from the model parameters (the probability of the data, given the modelparameters); the greater the likelihood, the better the fit of the model to the data. Themaximum likelihood parameter estimates are the parameter estimates yielding thegreatest probability that the given data occur.
NONMEM estimates parameters by minimising the extended least squares objectivefunction, which is approximately proportional to minus two times the logarithm of thelikelihood (-2log likelihood) of the data (24). Under the assumption of normality,maximum likelihood estimates are obtained at the minimum objective function value(OFV) (35). Standard errors for the parameter estimates can also be obtained viamaximum likelihood estimation.
The explicit likelihood function is difficult to specify (and evaluate) because therandom effects enter the model nonlinearly. In NONMEM, this is handled by usingapproximations to the nonlinear model, involving linearization in the random effects.The first and (to date) most frequently used method is the so-called first-order (FO)method. In this method, a first-order linearization (Taylor series expansion) around theexpected values of the random effects, i.e. η and ε equal to zero, is employed. Themethod only provides estimates of the population parameters, although individualparameter estimates can be obtained a posteriori, based on the population mean

13
parameters, as empirical Bayes (posthoc) estimates (36). These are also referred to asconditional estimates.
The first-order conditional estimation (FOCE) method (36) is more elaborate. It differsfrom the FO method in that the linearization is performed around the individualconditional estimates of the η values. This method is more time-consuming, sinceindividual estimates need to be obtained during each iteration. The FOCE method ismore useful when the number of observations per individual increases, and the modelbecomes more nonlinear (36).
There is a more sophisticated version of the FOCE method, which incorporates theinteraction between interindividual and intraindividual (residual) random effects (36)(FOCE INTER). This method differs from the FOCE method in the way that theresidual error is handled. With the interaction option, the dependence of the model forintraindividual error on the η values is preserved during computation of the OFV. Thismeans that the residual error is evaluated at the predictions based on the conditionalparameter estimates, rather than at the typical predictions (which is the case if theinteraction option is not used). This method appeared to be valuable in the analysis ofrich data containing interactions between η and ε (37). It is noteworthy that it isreasonable to assume such interactions in most PK-PD data sets.
The Laplacian estimation method is similar to the FOCE method; however, instead offirst-order derivatives, second-order derivatives with respect to the η values are used.This method is especially useful when there is a high degree of nonlinearity in themodel (36, 38).
The likelihood option is required for estimating discrete data, using logistic (mixedeffects) models. The individual predictions are then set to the value of the conditionallikelihood of η for the observations (rather than to a prediction of the observation). TheOFV is then equal to -2log likelihood of the data.
1.3 Covariate modelling
Building the covariate model can be a time-consuming and often difficult task –especially if there are a large number of covariates to consider. Apart from findingimportant (predictive) covariates, the functional form of the relationship also has to bespecified. Suggestions on how to aid covariate model building have been made (e.g.(39-42)), and several approaches to covariate model building are employed, althoughto date there is no consensus regarding how to best build these models.

14
1.3.1 Covariate data – graphical presentation
An exploratory analysis, using graphical techniques (43), is recommended to makeeffective use of the data (2). Histograms of covariates can be useful for assessingcovariate distributions and identifying outliers, missing values, and sub-groups inwhich there are few individuals. The combination of groups with few subjects,exclusion of outliers from the analysis, or transformation of covariate data can then beconsidered before modelling. Scatter plots of one covariate versus another (pairs plots)are valuable for assessing the correlations between covariates, and these can becombined with the calculation of correlation coefficients (43). It may be necessary tochoose between two highly correlated covariates, as the correlation may affect theparameter estimates and their precision (44), and also the power of detecting covariaterelationships (45).
1.3.2 Identification of candidate covariates
Covariate modelling is an iterative procedure, and the identification of potentialcovariates often starts from a defined model without parameter-covariate relationships(basic model). The covariates may be screened within the mixed effects model or, asthis may be very time-consuming, methods of reducing the number of covariates to tryin the model may be applied. These methods usually make use of the empirical Bayes(posthoc) estimates of the parameters in graphical analysis (39), stepwise generalisedadditive models (GAM) (40), stepwise multiple linear regression, or tree-basedmodelling (46). The covariates identified as important are usually either included inthe model using stepwise forward inclusion, or combined in a model including allfound variables (full model) from which covariates are tested using stepwise backwarddeletion. An automated procedure where the covariate model is built withinNONMEM in a stepwise fashion has also been presented (41). Although theseprocedures are frequently used, no previous comparison of their performance has beenmade.
Stepwise testing of covariates is frequently employed. In 1999 to 2002, 94 of 98 papersconcerning covariate model building in NONMEM included stepwise methods. Thereare, however, general problems associated with stepwise regression, one being that themultiple testing performed may lead to a high risk of false variables included in themodel (47). Another issue is that stepwise procedures tend to select effects withrelatively larger coefficients and to overestimate these (i.e. selection bias) (48-50).Until now, no investigation has been made regarding the magnitude (and implications)of selection bias in the area of nonlinear mixed effects modelling.

15
There are alternatives to stepwise methods. One is to specify a ‘best-guess’ modelbased on the known characteristics of the drug (49, 51). This may not always bestraightforward and, if the purpose of the covariate modelling is to screen for newcovariates, it is of little use. Kowalski and Hutmacher (42) have presented analgorithm for screening covariates, employing a full model (including all potentialparameter-covariate relationships) approach. All possible sub-models are evaluatedfrom the parameter estimates and the covariance matrix of the estimates from the fullmodel fit, and ranks of the most probable covariate models are derived.
1.3.2.1 Graphics
To identify potential influential covariates, plots of weighted residuals versus thecovariates were originally recommended. However, these plots did not indicate whichmodel parameter the covariate was likely to affect. Parameter-covariate correlationsmay be revealed from plots of posthoc estimates of the parameters versus thecovariates (exemplified in Fig.1.1), as proposed by Maitre et al. (39). The shape of therelationship may also be discernable in the plots, and may be enhanced by the use ofnonparametric smooth curves. These plots are commonly used (52-57). However, thereare drawbacks associated with graphical exploration, as pointed out by Wakefield andBennett (58), as decisions based on graphics tend to be somewhat subjective. Inaddition, the quality of the posthoc parameter estimates may influence the usefulnessof these graphs. In cases where there is little information about individual parametersbecause of sparse sampling, the estimates tend to be biased towards the populationmean.
0
2
4
6
8
10
0 50 100 150
CLCR (mL/min)
CL
(L
/h)
Figure 1.1 Individual empiricalBayes (posthoc) estimates of CL,from a basic model, versus CLCR.The solid line is a nonparametricsmooth of the data.

16
1.3.2.2 Stepwise generalised additive modelling
The procedure, proposed by Mandema et al., for identifying possibly importantcovariates utilises stepwise built GAM (40). In this procedure, the individual posthocparameter estimates (Pi), obtained from a model without covariates, are (separately)regressed on the individual covariates (Xi) according to the general equation:
Pi = α + f1(X1i) + f2(X2i) + … + fn(Xni) (1.5)
The α is an intercept, and the function fn() represents any function, e.g. linear or splinefunctions. For each covariate, a range of optional models is first defined. For example,in the program Xpose (59), the model scope is: not included, included in a linearrelationship, included in a nonlinear (spline) relationship. The model for the parameteris built using stepwise addition/deletion, where the covariates are allowed in the modelin any of the pre-defined relationships. In each step, the single added (or deleted) termthat decreases the Akaike information criteria (AIC, proportional to the residual sum ofsquares from the GAM fit, plus a penalty for the number of parameters) to the greatestextent is retained in the model. The search stops when no further decrease in AIC isachievable.
The GAM procedure has been used in a number of applications, e.g. (60-74). It canalso be used for assessing the stability of covariate selection in a method called thebootstrap of the GAM (59, 75). In this method, bootstrap data sets are created byrandom sampling (with replacement) of the posthoc parameters and the associatedcovariates. The GAM procedure is applied to each of the bootstrap data sets, and thefrequency with which a covariate/covariate model appears in the model is assessed.Apart from relying on the quality of the posthoc estimates, there are two otherimportant drawbacks with the GAM: it does not account for time-varying parametersand/or covariates, or for parameter-covariate correlations.
1.3.2.3 Stepwise multiple linear regression
Stepwise multiple linear regression (MLR) can also be used to identify potentialcovariates. The major difference from the GAM procedure is that the models for thecovariates are restricted to being linear.
Pi = α + β1×X1i + β2×X2i + … + βn×Xni (1.6)
The α is the intercept, and the βs are the linear regression coefficients. The model canbe built in a similar stepwise addition/deletion fashion to that used with the GAMprocedure. MLR has been employed in a number of analyses, e.g. (43, 76-88). Themethod suffers from the same drawbacks as the GAM procedure, but as the linearassumption does not always hold, the GAM procedure may be more effective.

17
1.3.2.4 Stepwise automated covariate model building within NONMEM
In the stepwise procedure suggested by Jonsson and Karlsson (41) the covariate modelis built in an automated fashion within the mixed effects model in NONMEM. Startingfrom a basic model, the covariate model is first built up using forward inclusion. Ineach step, all possible parameter-covariate relationships are tested individually. Theterm that most reduces the OFV, provided that the reduction is greater than a specifiedvalue (e.g. 3.84, p<0.05, see section 1.3.4.2), is retained in the model. Continuouscovariates are first tried in linear functions and, once included in the model, in the nextstep in a nonlinear function (two linear splines joined at the median covariate value).When no more covariates can be included (according to the specified criterion) a fullmodel is defined. From this full model, all parameter-covariate relationships are re-tested by stepwise backward deletion applying a stricter criterion (e.g. p<0.01). A‘final’ model is obtained when all covariates are ‘significant’ according to thiscriterion.
This procedure handles most of the drawbacks seen with the GAM and MLRprocedures, although it can be very computer-intensive (time-consuming).
1.3.3 Formulating the covariate model
Covariates are usually included in the mixed effects model to influence structuralparameters, although covariate effects can also be considered in the statistical sub-model. For example, the magnitude of IIV may differ between sub-types of apolymorphic enzyme, or the residual error magnitude may vary at different study sites.
1.3.3.1 Categorical covariates
Categorical covariates are qualitative variables. These can be binary (e.g. concomitantmedication: yes/no, sex: male/female), or have multiple categories and be ordered (e.g.smoking: no, <20 cigarettes/day, >20 cigarettes/day) or non-ordered (e.g. race). Abinary covariate can be handled in the model by use of an indicator variable, coded aszero or one; e.g. patients can be treated with a concomitant drug (DRUG=1) or not(DRUG=0).
P = θ1 + θ2 × DRUG (1.7)
θ1 is the typical value of the parameter (P) in a patient not treated with the drug, and θ2
will represent the increase/decrease in P caused by the treatment with the concomitantdrug. The model can be re-parameterised (Eq.1.8) so that θ2 represents the fractionalchange in P:
P = θ1 × [1+ θ2 × DRUG] (1.8)

18
If the covariate has multiple categories, each category is assigned an indicator variable(COV=1, 2, 3 etc.). The model can be formulated as in Eq.1.9, where each categoryhas its own parameter estimate. Eq.1.10 may be preferred if the covariate is ordered, asthis ensures an ordered effect (if parameter estimates are constrained to beingpositive).
θ1 if COV = 1 θ1 if COV = 1P = θ2 if COV = 2 (1.9) P = θ1+ θ2 if COV = 2 (1.10)
θ3 if COV = 3 θ1+ θ2+ θ3 if COV = 3
1.3.3.2 Continuous covariates
Continuous covariates have a defined scale, and can be quantified (e.g. body weight(WT), age, CLCR). The simplest model (apart from treating the covariate ascategorical) is one in which the parameter is a linear function of the continuouscovariate, here exemplified by WT:
P = θ1 + θ2 × WT (1.11)
θ1 is the typical value at WT=0 and θ2 represents the change in P with each unitchange in the covariate. To give θ1 a more meaningful value, Eq.1.11 can be re-parameterised so that the relationship is centred on a value in the covariate distribution,e.g. the (baseline or overall) median covariate value:
P = θ1 × [1 + θ2 × (WT – median WT)] (1.12)
In this case, θ1 represents the estimate of P in an individual with median WT (ratherthan the estimate in an individual weighing 0 kg), and θ2 the fractional change in Pwith each kg change in WT from median WT. This parameterisation prevents P frombecoming negative, by setting constraints on the value of θ2.
In many cases, and especially if the covariate covers a large range of values, the datamay not be satisfactorily described by linear models. The simplest nonlinear modelcombines linear splines as in Eq.1.13.
θ1 × [1 + θ2 × (WT – median WT)] if WT ≤ median WTP = (1.13)
θ1 × [1 + θ3 × (WT – median WT)] if WT > median WT

19
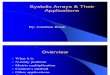
Other nonlinear relationships are obtained using a power model (Eq.1.14), a (sigmoid)Emax-model (Eq.1.15), or an exponential model (Eq.1.16), see Fig.1.2.
P = θ1× [WT / median WT]θ2 (1.14)
P = θ1 × WTθ3 / (θ2θ3 + WTθ3) (1.15)
P = θ1 × exp[θ2 × (WT – median WT)] (1.16)
The covariate could also be transformed, e.g. by log-transformation, before it is used inthe model, resulting in a log-linear relationship (Eq.1.17, Fig.1.2).
P = θ1 × [1 + θ2 × log(WT / median WT)] (1.17)
In these models, time-varying covariates are treated in the same way as time-constantcovariates. However, it may be of value to consider models that allow time-varyingcovariates to be treated differently, as additional information may be linked to themagnitude or frequency of change of the covariate (89).
0
2
4
6
8
10linear model
0 50 100 150
two-spline model log-linear model
0 50 100 150
power model emax model
0 50 100 150
0
2
4
6
8
10exponential model
weight (kg)
Typ
ica
l valu
e o
f P
Figure 1.2 Schematic pictures of the models (in Eq.1.11-1.17) for continuous covariates,the typical value of the parameter versus weight.

20
1.3.4 Model selection
The decision to include a covariate in a final model should preferably be based on acombination of statistical significance, mechanistic plausibility and the clinicalrelevance of the relationship. Statistical significance can be judged using the so-calledlikelihood ratio (LR) test (see section 1.3.4.2). The mechanistic plausibility varies fromdrug to drug, and has to be decided based on subject-matter information (1). Clinicalrelevance (impact on labelling) also differs between situations, and is thereforedifficult to include in the model building process (although it has been done usingBayesian modelling (58)). The clinical significance can be evaluated from thereduction in IIV (and residual error) associated with the covariate, or can be appraisedfrom the effect of the covariate in individuals with extreme covariate values, althoughthis is approximate since the value of the covariate coefficient will depend on whichother covariates are in the model (58). In addition, covariate relationships supported byonly a few individuals are normally not included in the model (90).
1.3.4.1 Graphical analysis
Graphical analysis can be used to check modelling assumptions in all stages of modeldevelopment (18), and it is also an important tool for judging goodness-of-fit.Goodness-of-fit plots include observed (measured) versus predicted response,observed response versus individual predictions, and residual diagnostics. In addition,graphs of posthoc η values versus covariates can be used to check a final model, as notrends should be visible if no further covariates influence the parameters.
1.3.4.2 Statistical comparison
The OFV output by NONMEM is approximately proportional to -2log likelihood ofthe data, under the assumption that the model is the true model (23, 91) and that theerrors are normally distributed (35). The difference in OFV (∆OFV, likelihood ratio)between two nested models (i.e. the larger model can be reduced to the smaller) isapproximately χ2-distributed, with degrees of freedom (df) equal to the number ofdiffering parameters. Based on this, the improvement in model fit from the inclusion(or deletion) of a model parameter can be assigned a significance level. ∆OFVs of 3.84and 6.63 correspond to nominal p values of <0.05 and 0.01 (df=1), respectively. TheLR test is frequently used for assessing the statistical significance of includedparameters (covariates) in a model. There are indications, from studies of confidenceintervals based on standard errors (SE) (92, 93) or from using the LR test (94), that thetype I error rate (the risk of a false positive result) could larger than expected. Thismay (in part) be due to the asymptotic properties of the test, and the approximations

21
made to the model during estimation. Despite these indications, no systematicexploration of the performance of the LR test has been reported in the literature.
Although no significance levels can be assigned to differences in OFV between non-nested models, comparison can be made using the AIC. This is computed in the sameway as the ∆OFV, but differing numbers of parameters (nP) in the models are adjustedfor: AIC=OFV1-OFV2 + 2 × (nP1-nP2). Confidence intervals for parameter estimatescan be calculated from the estimated SEs, although the CI derived in this way isgenerally too narrow (92, 93), and is assumed to be symmetrical (which is notnecessarily true). Non-symmetrical CI can be derived from likelihood profiling (95),where the parameter value associated with a fixed ∆OFV is determined (by repeatedlyfixing the parameter to increasing/decreasing values), or by bootstrapping (96). A largenumber of bootstrap data sets are then created (by random re-sampling of individuals,with replacement), the model is fitted to each of these and the CI can be computedfrom the resulting distribution of parameter estimates.
1.3.5 Assessing the performance
Depending on the objective of the analysis, the need for model validation may vary. Ifthe model is going to be used for predictions, clinical trial simulation (97, 98), orincorporated in the drug label (9) validation is essential. There is no consensus on howvalidation should be performed (9, 99), and “innovative approaches” are encouragedby the FDA (9). However, the focus is mainly on predictive performance, which is animportant aspect if the model is intended for predictive purposes.
Predictive performance is generally assessed by fixing the final model parameters andusing them to predict another data set. This data set should optimally be a separate(external) data set, and although this has been achieved in some analyses (e.g. (100-103)), it is generally not feasible. Data splitting or re-sampling (bootstrap) techniquesare therefore frequently applied; these provide nearly unbiased estimates ofperformance. Data splitting involves randomly splitting the data set into an ‘index’part, used for model development, and a ‘test’ part, on which the final modelparameters are applied. It has been utilised in population PK studies, e.g. (85, 86, 104,105), although the sample size often precludes the use of data splitting. Cross-validation is a repeated data splitting method (described in (96)), in which the full dataset is used to develop the model. The data are then randomly split into a number (n) ofparts of approximately equal size. The final model parameters are estimated on n-1parts, and these are used to predict the excluded part of the data. This procedure is thenrepeated n times, so that predictions are obtained for all parts. Cross-validation can beapplied with various numbers of splits (e.g. (106-109)), from two to maximally the

22
number of individuals in the data set (i.e. leaving one individual out at a time).Bootstrapping (110) can also be used for internal validation of population models (e.g.(74, 75, 111-113)). The full data set is used for model development, and the modelperformance can be assessed on the bootstrap data sets.
1.3.5.1 Metrics for assessing performance
The prediction errors (PE), calculated on concentrations, are frequently used forevaluating predictive performance. This is defined as the difference between observedand (population) predicted concentrations.
PE = Cobs – Cpred (1.18)
The mean prediction error (MPE) is a measure of bias (114), and for an unbiasedprediction the CI of the MPE should include zero. The root mean square error (RMSE)is a measure of precision (114); the smaller the RMSE the more precise the prediction.
To account for heteroscedasticity in the data, the PE can be weighted by the standarddeviation (SD) of the prediction, yielding a standardised PE (115) (used by e.g. (76,100, 103, 116)). The SD of the prediction can be derived from the model inNONMEM. Another way to handle heteroscedasticity is to log-transformconcentrations before calculating the PE (e.g. (41)). If there is more than oneconcentration per individual, this presents a further problem, as concentrations withinan individual are not independent. One way of solving this is to choose a specific time-point of interest.
A model could also be validated using model parameters (104). The final model is thenapplied to predict individual parameters, and bias and precision in comparison to thepopulation prediction can be determined. The improvement in bias/precision can becompared to that of the basic model.

23
1.4 Simulations – methodological studies
Methodological PK studies often utilise (Monte Carlo) simulations (117). Simulateddata have certain advantages compared to real data, the most important being that thetruth (i.e. the true underlying model) is known. This makes it possible to addresscertain questions when all other conditions are known (and fixed). In addition, itenables making replicates so as to make inferences. However, simulated data oftenlack the complexity of data collected in real trials. Covariate data are especiallydifficult to mimic in simulations, because of the difficulty of defining the distributions,including the correlations between covariates and the potential time-variation. As acompromise, the covariate structure can be adopted from a real data set while the PK(PD) data are simulated. The studies comprising this thesis combine simulations withanalysis of real data.

24
AIMS OF THE THESIS
The aims of this thesis were to enhance knowledge and understanding of methods usedin nonlinear mixed effects covariate model building by exploiting new models andmethods, to improve decision-making in model building, and to make covariatemodelling more efficient, predictable and robust. In particular, the aims were:
To investigate the properties, performance and limitations of the LR test whenjudging statistical significance in NONMEM analyses, with particular emphasison improving understanding of the conditions under which this test may or maynot be reliable.
To compare frequently used stepwise covariate model building methods withrespect to performance, to guide data analysts in the choice of method.
To assess the magnitude and implications of selection bias in the estimates ofstepwise selected covariate effects.
To investigate whether extended covariate models, applicable to time-varyingcovariates, can enhance knowledge of the PK-PD characteristics of a drug andimprove therapeutic decision-making.
To illustrate the use of covariate model building strategies, and apply thefindings in this thesis, using real data.

25
METHODS
3.1 Simulation and analysis of data - software
All simulations and model fitting were carried out using NONMEM (24) version V orVI (beta). When the properties of the LR test were explored, different estimationmethods were applied: the FO method, the FOCE method, the FOCE INTER method,the Laplacian method, and a generalised least squares (GLS) method, which usedpredictions from a first fit in the residual error of a second fit. The Laplacian methodwith the likelihood option was used for the categorical data. The FOCE INTERmethod was used in all other studies; however, for the darifenacin analysis, becausethe FOCE INTER method was not successful, a GLS related approach was applied.
S-PLUS for Windows (v. 2000, Insightful Corporation, Seattle, WA), and Xpose (v.3.0) (59) were used for graphics. The GAM routine, as implemented in Xpose, wasused for covariate identification. Perl (v. 5.6) was used for scripts for data-extractionand simulation routines.
3.2 Data & models
Linear PK was assumed in all studies, thus the term ‘nonlinear model’ refers to acurve-linear model and not saturable PK.
3.2.1 Simulations to assess the Type I error rate (Papers I-III)
Data were simulated to assess the frequency of type I errors (the risk of a false positiveresult), when the LR test is applied to test the inclusion of an additional (false)parameter in a model. Alterations were made to the simulation model and to the dataset, to explore the properties of the LR test.
3.2.1.1 One-compartment pharmacokinetic model (Papers I-II)
PK data were simulated from a one-compartment intravenous (iv) bolus model. Thedefault data set contained 50 individuals, with 2 samples per individual drawn at 1.75and 7 hrs after drug administration. The typical values of CL and V were set to 10 L/hrand 100 L, respectively. IIV (ω) for both parameters was set to 0.3 (diagonal variance-covariance structure), and lognormally distributed. The residual error was simulated tobe proportional to the individual concentrations (i.e. heteroscedastic), lognormallydistributed, and with σ=0.1. A dose of 1 unit was assumed.

26
The number of subjects in the data set and the number of samples per subject, thesampling times, and the magnitudes of the interindividual and residual errors werevaried. Modifications were also made to the model. For example, the heteroscedasticresidual error was varied so as to be normally distributed or heavy-tailed(symmetrically) distributed, and an additive (homoscedastic) residual error model wasinvestigated. Data were also simulated without the η-ε interaction, i.e. where theresidual error magnitude was proportional to the population predicted concentrations.A linear model with homoscedastic error, corresponding to a log-transform of thedefault model, was also used.
3.2.1.2 Logistic model for ordered categorical data (Paper III)
Categorical data with 4 ordered levels (e.g. corresponding to an effect judged as none,mild, moderate, or severe) were simulated from a logistic model for 200 individuals. 8observations per subject were made. The (population) average baseline probability ofbeing in each category was 25%, and IIV (ω=1) was included. No drug effect wasassumed in the model.
The number of subjects in the data set, the number of samples per subject, and themagnitude and distribution of IIV were varied.
3.2.2 Real data to assess the Type I error rate (Paper I)
This data set originated from a study of the anti-hypertensive agent prazosin, in which64 individuals were treated with repeated oral doses of the drug. Data from the firstvisit, with 9-10 samples per individual, were used.
A one-compartment model with first order absorption (CL/F, V/F and Ka) was appliedto the data. IIV in all PK parameters, and the population covariance between CL/F andV/F, were estimated. A proportional residual error was used. The data set containedten covariates, six categorical and four continuous: sex (SEX; male 42, female 22);race (RACE; Caucasian 44, Black 20); smoking (SMOK; yes 16, no 48); concomitantmedication with hydrochlorothiazide (HCTZ; yes 35, no 29); concomitant medicationwith propranolol (PROP; yes 10, no 54); other concomitant medication (CON; yes 51,no 13); age (AGE; 24-69 years); height (HT; 140-188 cm); weight (WT; 51-137 kg);serum creatinine (SECR; 0.7-1.8mg/dl). A dichotomous dummy covariate (0, n=32; 1,n=32) was randomly assigned to each individual.

27
3.2.3 Simulated data to compare stepwise covariate modelling (Paper IV)
Ten simulated data sets (previously used (41)) were generated from a one-compartment model with first-order absorption, under steady-state conditions. Thedata sets included approximately 3 observations from each of 64 individuals (230observations in total). Samples were drawn either at 0.5, 2, 4, and 6, or at 0.5, 2, 8, and12 hours post-dose. The IIV was lognormally distributed (ωCL/F=ωV/F=0.25, ωKa=0.20),and a proportional residual error (σ=0.15) was applied in the simulations. CL/F wasrelated to sex (males had a 19.5% higher typical CL/F than women) and nonlinearly toage (constant below median age, and linearly decreasing by 3.85% for each unitincrease in age from median). V/F increased linearly with bodyweight (0.6%higher/lower V/F with each unit increase/decrease in WT from median WT) and wasrelated to concomitant medication with hydrochlorothiazide (56% lower V/F inpatients receiving HCTZ). The absorption rate constant was not influenced by anycovariate. The covariate data, adopted from a clinical trial of the antihypertensive drugprazosin, are summarised in 3.2.2.
3.2.4 Real data to compare stepwise covariate modelling (Paper IV)
The data originated from a study of multiple iv infusions of the antibiotic agentpefloxacin to 74 critically ill patients. Approximately 3 samples were drawn perindividual at each of 1 to 3 occasions (337 plasma concentration measurements intotal). A basic one-compartment model was used to describe the data. IOV wasmodelled in CL and V, and IIV in CL, assuming lognormal distributions, and aproportional residual error model was used.
The covariate data included 4 categorical and 12 continuous covariates: SEX (male 57,female 17); centre (CEN; 1 [30], 2 [44]); concomitant medication with catecholamine(CAT; yes 22, no 91); artificial ventilation (AV; yes 71, no 42); WT (43-125 kg); AGE(18-84 years); CLCR (0.4-312 mL/min); Glasgow score (GLAS; 3-15); simplifiedacute physiology score (SAPS, 1-26); albumin (ALB; 17-40 g/L); bilirubin (BIL; 4-150 mmol/L); alanine aminotransferase (ALT; 3-200 IU/L); alkaline phosphatase(ALKP; 32-615 IU/L); prothrombin level (PT; 36-100 %normal); systolic bloodpressure (SBP; 60-175 mm Hg); heart rate (HR; 60-170 beats/minute).
3.2.5 Simulated data to assess selection bias (Paper IV)
100 data sets were simulated from a model for the pefloxacin data (described in 3.2.4).The model included 9 parameter-covariate relationships: CL was related to SEX, CENand linearly to BIL, CLCR, and AGE; V was related (linearly) to WT, CLCR, BIL andALKP.

28
3.2.6 Data sets & models – time-varying covariates (Paper V)
3.2.6.1 Gentamicin
The PK data set came from a study of 210 cancer patients treated with iv doses ofgentamicin. Patients were followed for one to five courses (median one), over amaximum of 25 months, and 1-9 samples per patient and occasion were drawn,resulting in 574 samples in total. The model, adopted from Rosario et al. (105), was atwo-compartment model which estimated IIV in CL and intercompartment clearance(Q), and also encompassed a combined additive and proportional residual error model.CL was related to CLCR, and V1 was related to body-surface area (BSA) and ALB.
CL (L/h) = θCL × [1 + θCLCR × (CLCR - 81)] (3.1)
V1 (L) = θV × BSA × [1 - θlog(ALB) × (log (ALB) - log(34))] (3.2)
The covariates all varied with time, and the baseline values (BCOV) and individualchanges from baseline (DCOV), based on observed values in each individual, were(median, range): BCLCR (71.7, 14.8-180 mL/min), DCLCR (1.4, -65.8 – +79.4mL/min), BALB (35, 14-47 g/L), DALB (-2, -16 – +13 g/L), BBSA (1.7, 1.3-2.3 m2),DBSA (0, -0.2 – +0.1 m2).
3.2.6.2 Pefloxacin
The data set, pefloxacin PK, is described in detail in 3.2.4. The model for the data(adopted from Karlsson et al. (19)) was a one-compartment model which estimatedonly IOV (i.e. not IIV) in CL and V, and included a proportional residual error. Onlythe covariate model for CL was considered, this included CLCR, BIL, AGE, CEN,SBP and WT (up to median WT; above median WT θWT=0) according to the followingmodel:
CL (L/h) = θCL× exp [θCLCR× (CLCR-100) - θBIL× (BIL-25) - θAGE× (AGE-45)
+ θCEN× CEN - θSBP× (SBP-115) + θWT× (WT-65)] (3.3)
CLCR, BIL and WT varied over time, and BCOV and DCOV were (median, range):BCLCR (105, 0.4-312 mL/min), DCLCR (13, -128 - +203 mL/min), BBIL (21, 6-150µmol/L), DBIL (-1.5, -69 – +40 µmol/L), BWT (67, 43-125 kg), DWT (-3, -16 – +8kg).

29
3.2.6.3 Voriconazole
The data set originated from two paediatric studies where children, aged 2-11 years,were treated with iv infusions of the antifungal agent voriconazole on one to fiveoccasions. In total, 355 plasma voriconazole concentrations were measured (onaverage 10 per individual) over 0.2-7.6 days. The PK model (118) included 2compartments, and IIV was modelled for CL (only). The analysis was performed usinglog-transformed data with an additive residual error, which varied in magnitude amongindividuals (18). The disposition parameters were normalised to bodyweight and theinfluence of CYP2C19 genotype (poor metaboliser [PM]=1, else 0) on CL wasincluded. The model also included relationships between CL and the two time-varyingcovariates ALT and ALKP.
CL (L/h) = θCL× WT× [1-θlog(ALT)× (log(ALT)-log(25))]
× [1-θlog(ALKP)× (log(ALKP)-log(136))] × [PM× (1-θPM)] (3.4)
The BCOV and DCOV were (median, range): BALT (25, 7-159 IU/L), DALT (2.5, -136 – +437 IU/L), BALKP (136, 47-309 IU/L), DALKP (-13, -101 – +453 IU/L).
3.2.6.4 Paclitaxel myelosuppression
The data comprised neutrophil counts monitored in 45 cancer patients receiving ivinfusions of paclitaxel. In total, 530 observations were collected over 196 courses (1-18 courses per patient, median 3). Unbound plasma concentrations of paclitaxel weremeasured in two of the courses (3.5 samples per patient on average). The neutrophil-time data were described using a semi-physiological model (119), in which the time-course of the neutrophil counts was related to the concentration-time profile ofunbound paclitaxel. Parameters estimated included the baseline cell count (Circ0), themean transit time (MTT) of the cells through the transit compartments, a feedbackparameter (γ) affecting cell proliferation, and the linear drug effect (Slope). IIV wasestimated in Circ0, MTT and Slope, and a proportional residual error model was used.
The time-varying covariate BIL affected Slope and MTT.
Slope (µM-1) = θSlope× [1-θBIL× (BIL-6)] (3.5)
MTT (h) = θMTT× [1-θBIL× (BIL-6)] (3.6)
The BCOV and DCOV were (median, range): BBIL (6, 4-37 µmol/L), DBIL (-1, -24 –+36 µmol/L).

30
3.2.7 Darifenacin data & model (Paper VI)
Plasma concentration data from 337 individuals were pooled from 17 Phase I studies(292 subjects, median 28 darifenacin observations per subject) and 1 Phase II study (45subjects, median 7 darifenacin observations per subject). The covariate informationincluded dose (1-45 mg), formulation (1 iv and 5 oral), single/multiple dose,concomitant administration with ketoconazole/erythromycin, CYP2D6 genotype(homozygous-extensive metaboliser [hom-EM] 177, heterozygous-extensivemetaboliser [het-EM] 70, PM 28); phenotype (EM 152, PM 21); RACE (Caucasian281, Black 9, Japanese 42, other 5); AGE (18-85 years); WT (50-115 kg); HT (1.49-1.95 m); SECR (0.418-1.42 mg/dL); ALB (2.4-7.5 g/dL); BIL (0.193-5.85 mg/dL);aspartate aminotransferase (AST; 4-68 IU/L); ALT (7-63 IU/L); ALKP (3-289 IU/L));SEX (male 293; female 44); alcohol use (0 units/week 70, 1-15 units/week 203, 16-30units/week 21, >30 units/week 1); SMOK (yes 192, no 95); food (fasted 256, high-fatfed 65, low-fat fed 16); observation time (8am-24pm 8272 observations, 24pm-8am1032 observations).
The established basic model for darifenacin was a two-compartment model with firstorder absorption. IIV was modelled in CL, V, Ka and the bioavailability (F), and IOVwas modelled in F, assuming lognormal distributions. A combined additive plusproportional residual error model was used, and the residual errors of the ivformulation were estimated separately from those of the oral formulations.
3.3 Analysis procedures & methodology
3.3.1 Covariate model
Covariates were modelled, in the mixed effects model, as being proportional to thetypical parameter, as shown for a categorical (dichotomous 0/1) covariate in Eq.3.7.Continuous covariates were centred on the median value (Eq.3.8).
P = θP × [1 + θCOV × COV] (3.7)
P = θP × [1 + θCOV × (COV – median COV)] (3.8)
3.3.2 Estimation of Type I error rates of the LR test (Papers I, II & III)
Two nested models (reduced and full) were fitted to the simulated data set. Thereduced model was the same model as that used for simulation (apart from theapproximations inferred by the estimation method), and the full model differed fromthe reduced one by the addition of one parameter. The ∆OFV between model fits wascalculated. One thousand replications were generated, yielding an empirical

31
distribution of ∆OFVs under the null hypothesis. The 1000 ∆OFVs were ranked andthe fraction of values larger than 3.84 was determined. This fraction represent anestimate of the type I error rate when the LR test is applied at p<0.05.
The added parameter in the full model was either a covariate influencing a structural(fixed effects) parameter (Papers I & III), a covariate influencing a variance parameter(Paper II), or a parameter describing variance or covariance (Papers II & III).
Apart from the variations in the simulation model and data set (described in 3.2.1),different estimation methods were also investigated (see section 3.1).
3.3.2.1 Inclusion of a false covariate effect
A dichotomous (0/1) covariate was added to the data set; each individual wasrandomly assigned either 0 or 1, with a probability of 0.5 of being assigned 1. Thedichotomous covariate was included in the full model as influencing CL or V (PaperI), the IIV in CL or V (Paper II), or the residual error variability (Paper II). In the firstcase, a sub-group effect in CL (or V) was estimated, and in the two latter cases,variability was partitioned into two groups.
In the logistic model (Paper III), a false drug effect was estimated in the full model.Each individual was then assigned a dummy dose of 1 unit, so that 4 observations weremade at baseline and 4 after dosing. The false drug effect was modelled as a stepfunction, and influenced the probabilities of experiencing the different effect scores.
3.3.2.2 Inclusion of false covariance
The data were always simulated using a diagonal variance-covariance structure (i.e. nocovariance between parameters). The additional parameter in the full model was onedescribing population covariance between CL and V (Paper II), implemented by usingthe BLOCK(2) option in NONMEM.
3.3.2.3 Inclusion of false variance
In these situations, the data were simulated without IIV (i.e. ω was set to zero) in V(Paper II) or in the baseline probability (Paper III). The additional parameter in the fullmodel was a parameter estimating IIV, i.e. ωV (Paper II) or ωBaseline probability (Paper III).

32
3.3.3 Covariate randomisation - Type I error rates for real data (Paper I)
A randomisation test (120) was used to estimate the type I error rates for a real dataset, and also to determine the critical value (∆OFV) corresponding to a desiredsignificance level for a specific data set and model parameter. Individual covariatevectors were first randomly permuted between individuals, thus breaking any existingcovariate-parameter relationships while maintaining the relevant structure of the PKand covariate data, generating a ‘pseudo-new’ data set. Second, a model including aparameter-covariate relationship (full model) was fitted to the ‘pseudo-new’ data set,and the ∆OFV from the reduced model was determined. The permutation/full modelfitting was repeated 1000 times. Estimates of the type I error rate were obtained asdescribed in 3.3.2. The value corresponding to the 5th percentile was noted, this is anestimate of the ∆OFV that should be used for p<0.05.
The procedure was repeated for CL/F and V/F, using each of the 10 covariates in thedata set and the dummy covariate.
3.3.4 Comparison of stepwise covariate model building procedures (Paper IV)
Covariate models were built for 10 simulated and 1 real data sets, applying twostepwise procedures in which the model was either built using NONMEM in bothforward inclusion and backward deletion steps (NM-NM), or using GAM in theforward inclusion part followed by backward deletion in NONMEM (GAM-NM).Different variants of the procedures (e.g. to evaluate time-saving options or account fortime-varying covariates) were investigated. Covariate models were evaluated andcompared with respect to included covariates, and predictive performance (describedin 3.4.2).
3.3.4.1 NM-NM
The covariate model was built using the automated stepwise procedure withinNONMEM (41). Forward inclusion, starting from the basic model, was carried out,applying p<0.05. Backward deletion, to re-test the found parameter-covariaterelationships, was performed from the full model applying p<0.01.
The variants of the NM-NM procedure comprised fixing part of the parameters duringestimation and, for the real data set, treating all observations as originating from thesame individual (naïve pooling).

33
3.3.4.2 GAM-NM
Empirical Bayes (posthoc) parameter estimates were obtained from a fit of the basicmodel. The GAM procedure (40) was used, regressing each parameter on thecovariates and trying linear and nonlinear relationships. All parameter-covariaterelationships detected in the GAM procedure were combined in the nonlinear mixedeffects model in a full model. Backward deletion was carried out from the full model,in the same manner as described in 3.3.4.1.
The most important variants of the GAM procedure were: utilising the posthocparameters or the η values, only considering linear models (similar to MLR), andtreating separate occasions as different individuals (for the real data set).
3.3.5 Assessment of selection bias (Paper IV)
The model used for simulation was fitted to each simulated data set. The stepwise NM-NM routine (described in 3.3.4.1) was also applied to each of the data sets, startingfrom the basic model. Two sets of estimates (simulation model and stepwise) of thecovariate coefficients resulted.
The biases in the stepwise coefficients were calculated as the MPE between the truecoefficients and the stepwise estimates. The true coefficients were the estimatesobtained from applying each of the stepwise selected covariate models to a separatelarge data set. The biases were compared to the precision of the simulation modelestimates; i.e. the RMSE between simulation coefficients and simulation modelestimates.
3.3.6 Application of two models for time-varying covariates (Paper V)
Two extended models applicable to time-varying covariates were applied to 4 dataexamples. In the first model, it was acknowledged that the covariate effect may differbetween individuals and within an individual. The standard covariate model was splitinto a BCOV effect, describing variation between individuals, and a DCOV effect, thatdescribed variation within individuals:
P = θP × [1 + θBCOV × (BCOV – median BCOV) + θDCOV × DCOV] (3.9)
In this model, θBCOV is the effect of interindividual variation, and corresponds to thefractional change in P with each unit difference in BCOV from median BCOV. θDCOV
describes the effect of intraindividual covariate variation, and is the fractional changein P with each unit change in DCOV. If the values of θBCOV and θDCOV are similar,there is no indication of different inter- and intraindividual models, and the original

34
model can be used. If they are different, both may prove to be important for predictingthe parameter, or the model may be reduced by the term not proving valuable.
The second model, which can be used independently of or in combination with thefirst, estimates IIV in the covariate effect:
Pi = θP × [1 + θCOV × expηcov, Pi× (COV – median COV)] expηPi (3.10)
ηcov, Pi is a random variable (zero mean, variance ω2) which allows the covariate effectto vary in magnitude between individuals. A change of one unit in the covariate maythus cause Pi to alter substantially in one individual, while in another individual theeffect may be moderate. In Eq.3.10, DCOV (but not BCOV) can be used instead ofCOV. In all situations where DCOV was found to be important, IIV in DCOV wasalso tested.
3.3.7 Darifenacin covariate analysis (Paper VI)
Covariate modelling was carried out starting from the defined basic two-compartmentmodel for darifenacin. In the analysis, the choice of model building methods was madeconsidering both ‘best-practices’ approaches and practical aspects. Special emphasiswas put on the choice of estimation method, covariate model building method,handling of time-varying covariates, and the criteria used in model building.
Covariate distributions were examined and data transformation was considered beforethe analysis. Covariate relationships, expected from prior findings to be important,were included in the model before screening for other influential covariates. Plots ofposthoc ηi values for the darifenacin PK parameters (from the model including the pre-defined covariates) versus the covariates were constructed to demonstrate potentialrelationships. The computer run times governed the choice of model buildingprocedure, therefore slightly different approaches than those described previously wereused. The GAM procedure was applied to identify possibly influential covariates, inpart treating data from different occasions within one individual as data from separateindividuals to account for time-varying covariates. The covariates identified asimportant were included in the nonlinear mixed effects model using a stepwiseprocedure. The covariates were first included univariately in the model and rankedaccording to the associated ∆OFV. Variables were then tested stepwise in the model,in descending order. Only covariates producing a ∆OFV>3.84 were included in themodel. When no more variables could be incorporated into the model according to thiscriterion, backward deletion was performed. Stricter criteria were then applied; onlycovariates that were deemed as physiologically plausible and associated with anincrease in ∆OFV>10.83 were retained in the model.

35
3.4 Model comparison
3.4.1 Comparison of covariate models (Papers IV, V & VI)
Covariate model comparison was based on differences in OFV, using the LR test.Visual assessment of goodness-of-fit graphs and evaluation of parameter estimates andthe standard errors (SE) of the estimates were also used to guide the choice of finalmodel.
In paper IV, the covariate models selected stepwise were compared with respect toincluded parameter-covariate relationships.
3.4.2 Assessment of predictive performance (Paper IV)
3.4.2.1 External data
The abilities of the final covariate models (for the simulated prazosin and pefloxacindata sets) to predict a large (simulated) test data set were assessed. Parameters of eachfinal model were fixed and used to predict the observations in the test data set. TheRMSE and the MPE were calculated using log-transformed observed and predictedconcentrations.
3.4.2.2 Cross-validation
Cross-validation was applied to assess predictive ability in the real pefloxacin dataexample. The data set was split into 10 approximately equal parts (random allocationof individuals). The final model was estimated on 9/10 of the data, and the parameterestimates were fixed and used to predict the remaining 1/10. This was repeated so thatpredictions for all parts of the data set were obtained. The abilities to predict CL and Vwere assessed separately. One observation (concentration) per individual was used tocalculate predictive performance. These observations were chosen to be parameter-information-rich based on the partial derivatives with respect to the parameter, e.g. foreach individual the observation with the largest partial derivative with respect to CL(ηCL) was chosen to predict CL. The RMSE and MPE, standardised to the SD of thepredicted concentration, were calculated.

36
RESULTS
4.1 Type I error rates of the LR test (Papers I, II & III)
4.1.1 Inclusion of a false covariate effect
When the FO method was used, the estimated type I error rates for including a falsecovariate relationship affecting a structural parameter exceeded the expected type Ierror rate. The number of individuals in the data set had no major influence, althoughthe type I error rate increased considerably with more frequent sampling (Fig.4.1). Forexample, a type I error rate of 0.45 was seen, versus the expected 0.05, when 19observations per individual were used. Also an increased residual error magnitude(σ=0.4) affected the type I error rate (Fig.4.2).
The FOCE method performed consistently better than the FO method (Fig.4.1),although the type I error rate still deviated substantially from the expected whenfrequent sampling was applied. No further improvement was seen when the Laplacianmethod was used. When FOCE INTER was applied, however, a considerableimprovement was evident. When the level of residual error was low (σ=0.1), theestimated type I error rates were in close agreement with the expected, regardless ofsampling strategy (Fig.4.1). This was also true with a higher level of residual error(σ=0.4), except when the number of samples per individual was low or when therewere very few individuals in the data set (Fig.4.2).
For the FO method, different structural and residual error models were compared. Itwas evident that the type I error rate was affected by the residual error magnitudewhen the residual error model was heteroscedastic, but not when the residual error washomoscedastic (Fig.4.3). The sampling frequency influenced the type I error rate to alarge extent when the structural model was nonlinear, but not when it was linear(Fig.4.3). If FOCE was used for the nonlinear model with homoscedastic error, andFOCE INTER for the models with heteroscedastic error, the type I error rates werereduced to close to the expected. The performance of the LR test was also improvedwhen the FO method was used in a GLS type procedure, or to analyse data lacking η-εinteraction, i.e. data where the residual error was simulated to be proportional to thepopulation prediction. When a false covariate (drug effect) was included in the logisticmodels, the estimated type I error rates were similar to the expected in all situations.

37
Figure 4.1 σ=0.1. Estimatedtype I error rate for falsecovariate inclusion for anexpected type I error rate of 5%versus the number ofindividuals in the data set. Eachpanel represents one samplingstrategy with 2, 4 and 19samples per individual,respectively. Results fromanalysing each data set usingthe FO method (closedtriangles), FOCE (opendiamonds) and FOCE INTER(open squares) are shown.
50 250 1000 50 250 1000 50 250 1000
Number of individuals
0.05
0.15
0.25
0.35
0.45
Est
imate
d ty
pe
I err
or r
ate
2 observations 4 observations 19 observations
FOCE INTER
FO
FOCE
Figure 4.2 σ=0.4. Estimatedtype I error rate for falsecovariate inclusion for anexpected type I error rate of 5%versus the number ofindividuals in the data set. Eachpanel represents one samplingstrategy with 2, 4 and 19samples per individual,respectively. Results fromanalysing each data set usingthe FO method (closedtriangles), and FOCE INTER(open squares) are shown.
50 250 1000 50 250 1000 50 250 1000
Number of individuals
0.05
0.15
0.25
0.35
0.45
Est
ima
ted
type
I err
or
rate
2 observations 4 observations 19 observations
FO
FOCE INTER
0.05
0.15
0.25
0.35
0.45
Est
imate
d ty
pe I
err
or
rate
Residual error variability Number of samples per individual Number of individuals
L-homo
1000
a b
NL-homo
NL-hetero
L-hetero
logistic
5020420.50.40.30.1 0.2 250
c
Figure 4.3 Estimated type I error rate for false covariate inclusion for an expected type I error rate of5%, using the FO method and a nonlinear model with heteroscedastic (exponential) error (closedsquares) or homoscedastic error (open squares), a linear model with heteroscedastic (normal) error(closed circles) or homoscedastic error (open circles). A logistic model for dichotomous data (opentriangles) was also used. The result from changes in the residual error magnitude, the number ofsamples per individual, and the number of individuals in the data set are shown in panels a, b and c,respectively.

38
The estimated type I error rates of the FO method were also found to be parameter-(and sample spacing-) dependent. The former was confirmed with real data; the type Ierrors estimated by using covariate randomisation were on average 0.34 and 0.25 (forthe expected 0.05) for CL/F and V/F, respectively. (The corresponding values withFOCE INTER were 0.06 and 0.05.) The appropriate ∆OFVs, to use for a type I errorrate of 0.05 with the FO method, were estimated to be 15 for CL/F and 10 for V/F.
For the FOCE INTER method, the type I error rates for covariates affecting the IIV orthe residual error magnitude were also in agreement with the expected. This was notthe case for the FO method.
4.1.2 Inclusion of a false variance or covariance term
When the additional parameter in the model was a false variance term affecting V, andthe FOCE INTER method was used, the type I error rate was affected by the residualerror distribution. With a proportional residual error with normal distribution, the typeI error rates were slightly below the expected. On the other hand, when an exponentialmodel was applied (lognormal distribution of the errors), the type I error rates wereinflated both when the residual error magnitude was increasing (Fig.4.4), and whenthere were increasing numbers of subjects in the data set (data not shown). Similartrends were seen when the residual error distribution was heavy-tailed (symmetrical).
Inclusion of a false variance parameter in the logistic model resulted in type I errorrates well below the expected in all situations, e.g. the estimated type I error rate was0.014 versus the expected 0.05 with the default data set. No major influences wereseen from any of the variations tried.
When the FOCE INTER method was used and the additional parameter included in themodel was a covariance term, the residual error distribution also influenced the type Ierror rate. With an increasing residual error magnitude, increased type I error rateswere evident if the residual error distribution was lognormal (exponential model),while if the error distribution was normal, the type I error rates were unaffected byresidual error magnitude if there was enough information in the data (4 observationsper individual; Fig.4.5). However, even with a normally distributed error, largedeviations from the expected type I error rate were evident when the informationcontent in the data was low (few samples per individual, sampling at un-informativetime-points, large residual variability; Fig.4.5). In the situation when the information-content per individual was especially low (2 samples per individual, σ=0.3) the type Ierror rate increased considerably with increasing numbers of individuals in the dataset, while this was not the case when the sampling frequency was increased to 4samples per individual (data not shown).

39
Figure 4.4 Estimated type I error rate, for an expected type I error of 5% for inclusion ofa false variance term, versus the residual error magnitude. The FOCE INTER methodwas used with residual error distributions that were lognormal (exponential model;filled symbols) or normal (proportional model; open symbols). Two (circles), 4(triangles), or 19 (squares) observations per individual were used. A heavy-tailed(symmetric) residual error was also applied, with 2 observations per individual (semi-filled circle).
0.1 0.2 0.3 0.4
Residual error variability (SD of ε)
0.05
0.25
0.45
0.65
0.85E
stim
ated
typ
e I e
rror
rat
e
2 obs
heavy-tailed prop. error
2 obs
Exponential residual errorProportional residual error
4 obs
19 obs
Figure 4.5 Estimated type I error rate, for an expected type I error of 5% for inclusion ofa false covariance term, versus the residual error magnitude. The FOCE INTER methodwas used with residual error distributions that were lognormal (exponential model;filled symbols) or normal (proportional model; open symbols). Four observations perindividual (squares) and 3 observations per individual when the last sample was drawnat 18 hr (circles) or at 12 hr (diamonds) were used.
0.1 0.2 0.3 0.4 0.5
Residual error variability (SD of ε)
0.05
0.25
0.45
0.65
0.85
Est
imat
ed typ
e I
err
or r
ate 4 obs
3 obs -12h
3 obs -18h
Exponential residual errorProportional residual error
3 obs -18h
-12h
4 obs

40
4.2 Comparison of stepwise covariate model building procedures (Paper IV)
The two stepwise procedures performed similarly in the data sets explored – thevariability between procedures was of the same magnitude as the variability withinprocedures (between data sets). For the simulated data sets, the final models of theNONMEM procedure and the GAM procedure using posthoc η values were the same(Table 4.1). These procedures also identified the majority of the covariate relationshipssupported by the data (determined by backward elimination from the true covariatemodel), and the predictive performances of the models were not very different fromthat of the supported model (Fig.4.6). When some parameters were fixed duringestimation in the NONMEM procedure, or only linear relationships were explored inthe GAM procedure, a diminished ability to find true covariates was evident and theprecision in the prediction of the separate data set was reduced (Fig.4.6). There wasalso a tendency for the linear GAM procedure to find more false covariaterelationships, although most of these were eliminated in the backward step.
For the real data set, the full NM-NM model had a lower OFV than the full GAM-model where each occasion was treated as a separate individual. However, the finalmodels of these two procedures were exactly the same. The NM-NM procedure usedwith the (naïve) pooled data approach resulted in the largest number of parameter-covariate relationships. Apart from this, only small differences in the final covariatemodels found by the variants of the procedures were seen. The predictiveperformances (based on cross-validation) of the final models overlapped, both withrespect to standardised MPE and RMSE (data not shown). A small negative bias in thepoints influencing CL was seen, while a small positive bias and a tendency to betterprecision in the prediction of the points influencing V were found.

41
Table 4.1 The total number of true and false covariates in the final models found, for CL andV, by the different stepwise procedures, in the 10 simulated prazosin data sets.
CL V AGEa SEX False HCTZ WT falseGAM(eta)-NM 9 (7) 5 2 10 3 2GAM(parameter)-NM 8 (6) 4 2 10 2 2Linear GAM(parameter)-NM 7 (0) 3 1 10 2 2
NM-NM 9 (7) 5 2 10 3 2NM-NM fixed thetas 8 (2) 3 2 10 3 2NM-NM fixed parameters 6 (0) 2 2 10 1 -
Supportedb 9 (7) 6 10 4 aNumber of times identified in the right functional form (i.e. nonlinear) in parenthesesbModel resulting after backward elimination in NONMEM, starting from the true model
Figure 4.6 Box-and-whiskers plot ofthe RMSE between the log of theobserved and predicted concentrationsobtained with the basic, NM-NM withfixed parameters, NM-NM with fixedthetas, GAM(parameter), GAM(eta)-NM, linear GAM(parameter)-NM,NM-NM, supported, simulation(estimated) models and the simulationcoefficients for the 10 simulatedprazosin data sets. The filled dotrepresents the median, the box rangeis the interquartile range, and thewhiskers extend to values lessthan/greater than/equal to 1.5 timesthe interquartile range. Values beyondthese limits are shown as empty dots.Simulation coefficients
Simulation model
Supported model
NM-NM
GAM(eta)-NM
GAM(parameter)-NM
NM-NM fix theta
Linear GAM(parameter)-NM
NM-NM fixed
Basic model
0.45 0.50 0.55
RMSE

42
4.3 Selection bias in stepwise covariate modelling (Paper IV)
Of the 100 simulated data sets, the stepwise NM-NM procedure selected therelationships CL-BIL and V-WT in 99, CL-CLCR in 96, V-CLCR in 80, CL-CEN in75, CL-SEX and CL-AGE in 66, V-AP in 63, and V-BIL in 60. For the covariateeffects that were selected in the majority of the data sets (e.g. CL-BIL and V-WT; datanot shown), there were only minor differences between the simulation model andstepwise estimates (Fig.4.7). However, when the effects were found less frequently,upward biases in the stepwise estimates were evident. Nonetheless, the RMSE of thesimulation model estimates always exceeded the MPE of the stepwise estimates,indicating that the bias is less important (Table 4.2). The predictions of the stepwisemodel estimates were only slightly less precise than those of the simulation modelestimates, and the biases were of similar magnitude (data not shown).
Table 4.2 Bias of stepwise model estimates in the subset of data sets where the covariateeffect was identified, and precision of simulation model estimates from all (100) data sets, forcovariate effects on CL in the simulated pefloxacin data.
Covariate
Bias stepwiseestimates, subset
%MPEa
Precision simulationmodel estimates, 100
%RMSEbRatio
Bias/precisionAGE -12 35 -0.34BIL 2 11 0.19CEN -14 39 -0.35
CRCL 8 22 0.38SEX -8 27 -0.30
aExpressed as the percentage of the true coefficientbExpressed as the percentage of the simulation coefficient
Figure 4.7 Box-and-whiskers plot ofestimated covariate coefficients forCL in the simulated pefloxacin datasets. All values are normalised bydivision with the respective valuesused for simulation. For eachcovariate, from top to bottom, thestepwise NM-NM model estimates,the simulation model estimates fromthe subset of data sets where thecovariate effects were found(indicated by the number), and thesimulation model estimates from all100 data sets, are shown. The filleddot represents the median, the boxrange is the interquartile range, andthe whiskers extend to values lessthan/greater than/equal to 1.5 timesthe interquartile range. Values beyondthese limits are shown as empty dots.
AGE simulation model 100
AGE simulation model 66
AGE NM-NM model 66
SEX simulation model 100
SEX simulation model 66
SEX NM-NM model 66
CEN simulation model 100
CEN simulation model 75
CEN NM-NM model 75
CLCR simulation model 100
CLCR simulation model 96
CLCR NM-NM model 96
BIL simulation model 100
BIL simulation model 99
BIL NM-NM model 99
-0.5 0.0 0.5 1.0 1.5 2.0 2.5
estimated value / simulated value

43
4.4 Two models for time-varying covariates (Paper V)
The time-variation in the covariates can be demonstrated in a plot of the covariateversus time, as is shown in Fig.4.8 for gentamicin CLCR. The overlaid non-parametricsmoother can help identify trends in the data. In addition, to illustrate how the timechanges affect PK (or PD) observations, the time-points at which the observationswere made can be added to the graph, as shown in Fig.4.9 for voriconazole ALKP.
The two extended models for time-varying covariates provided significantly (p<0.01)better descriptions, than the original models, of all four data sets. In all, the modelswere applied to 10 parameter-covariate relationships, and in only 2 of these did thefinal models not differ from the original starting models (Table 4.3). The model wheredifferent inter- and intraindividual covariate effects were estimated was found to besignificantly better in 3 of the parameter-covariate relationships, although in 2 of theseonly one parameter (θBCOV or θDCOV) was supported (Table 4.3). In 3 of the caseswhere this extended model did not provide a significant improvement in fit, it wasfound that only DCOV (1 case) or only BCOV (2 cases) was supported.
The second model, in which the covariate effect was allowed to differ betweenindividuals, was found to provide significant improvement to the model in 4 cases;pefloxacin CL-CLCR, voriconazole CL-log(ALT), CL-log(DALKP), and paclitaxelPD Slope-DBIL (Table 4.3).
Table 4.3 Application of the two extended models for time-varying covariates
Data set - model θBCOV (%RSE) θDCOV (%RSE) Improvement† Final modelGentamicin
CL-CLCR 0.0098 (5.4) 0.0069 (22) S BCOV, DCOVV-log(ALB) -0.36 (30) -0.60 (30) NS originalV-BSA 8.63 (2.5) 3.89 (110)‡ NS BCOV
PefloxacinCL-CLCR 0.0035 (18) 0.0024 (40) NS* IIV*
CL-BIL -0.0064 (12) -0.0016 (130)‡ S BCOVCL-WT 0.036 (22) -0.012 (180)‡ NS BCOV
VoriconazoleCL-log(ALT) 0.35 (3) 0.32 (21) NS* IIV*
CL-log(ALKP) -0.16 (192)‡ 0.56 (26) NS* DCOV+IIV*
Paclitaxel PDMTT-BIL -0.012 (95) -0.020 (81) NS original
Slope-BIL -0.0047 (250)‡ -0.040 (22) S DCOV+IIV*
†S=significant based on LR test (p<0.01), NS=non-significant (p>0.01)‡Not supported in model*Significant improvement when IIV in the covariate effect was included

44
Figure 4.9 Log(ALKP) versus time, voriconazoledata set. Data from the same individual areconnected, the broken line is a smooth of the data,and the time-points where the PK observationswere made are indicated by vertical tick marks.
4.0
4.5
5.0
5.5
6.0
6.5
0 2 4 6
time (days)
log
(AL
KP
) (I
U/L
)
Figure 4.8 CLCR versus time, gentamicin data set.Data from the same individual are connected, andthe broken line is a smooth of the data.
50
100
150
0 50 100 150 200 250 300
time (days)
CL
CR
(m
L/m
in)

45
4.5 Darifenacin covariate analysis (Paper VI)
Several covariates that were expected from prior findings to be important wereincluded in the model, before screening for other parameter-covariate relationships. CLdiffered between CYP2D6 genotypes (EM/PM) and was affected by concomitantadministration of ketoconazole. The F was dose- and formulation-dependent, and wasinfluenced by genotype (EM/PM) and co-administration of ketoconazole anderythromycin. The Ka differed between formulations.
Since there were insufficient numbers of individuals in all the race groups, the race-covariate was dichotomised: Japanese were treated as one group and all other raceswere combined in another. In the 18% of subjects missing genotype information,phenotype information was substituted when possible.
The preferred estimation method was FOCE INTER, since the data were characterisedby frequent sampling and heteroscedastic error. However, because of numericalproblems, this method could not be used and a GLS-related approach with FOCE waschosen. Further, the computer run times limited the choice of model buildingapproaches, and necessitated slightly different strategies from those describedpreviously.
The GAM procedure was chosen in order to limit the number of potential covariates toevaluate. This was combined with a stepwise inclusion and backward deletionapproach in NONMEM. To be included in the final model, covariates were to bestatistically significant and mechanistically plausible. When applying these criteria, thecovariates remaining in the final model were a race effect on F, and a gender andnight-time effect on CL. Japanese subjects demonstrated a 55.5% lower F thanCaucasians. Females had a 31.1% lower CL than males. Night-time observations werecharacterised by a 9.9% lower CL. The genotype effect on F was split into threecategories (hom-EM, het-EM and PM) to accommodate differing metabolisingcapacities between hom-EM and het-EM subjects. This improved the fit slightly, butthe effect of het-EM was not supported on CL. The covariate model for the othercovariates was not changed compared to the two-category model.

46
DISCUSSION
When studying the literature on population PK-PD covariate model building, it isevident that statistical significance based on the LR test is extensively used as a modelbuilding criterion, singly or in combination with other criteria. It is also clear thatseveral different approaches are used to build the covariate model, although the vastmajority of these include stepwise methods.
For the FO method, the application of the LR test often resulted in large differencesbetween the estimated and expected type I error rates. The differences were especiallypronounced in cases when frequent sampling was applied and/or there was large(heteroscedastic) residual variability in the data. This deviation seems to be caused bythe approximations made to the model during estimation: (i) the approximation of theinfluence of the random effects of nonlinear models, and (ii) ignoring any interactionbetween η-ε present in the data. Nonlinearity in the random effects is handled better bythe FOCE method. Thus, the type I error rate is always lower with this method thanwith the FO method. When there is no residual error (and therefore no interaction)such as in the logistic model, the result of the LR test is the expected. Also, when theheteroscedastic residual error is properly accounted for by the use of the η-ε interactionoption (FOCE INTER) the estimated type I error rates are in agreement with theexpected. Data collected in PK-PD trials are expected to contain both nonlinearity andsome degree of heteroscedasticity (i.e. interaction), and accordingly FOCE INTERwould be the method of choice if statistical significance is to be used as a modelbuilding criterion. However, due to the asymptotic properties of the test, even withFOCE INTER, deviations from the expected type I error rate are likely when theinformation in the data is sparse (few individuals, few observations per individualand/or large residual variability). In situations when the FOCE INTER method is notpracticable, type I error rates closer to the expected can be obtained by using othermethods to account for the heteroscedasticity, such as a GLS-type procedure, or bylog-transforming the data (which may reduce both nonlinearity and heteroscedasticity).However, for a better control of the significance level, the critical value (∆OFV) to usefor a desired type I error rate with a certain method/data set/parameter can bedetermined by randomisation testing with a covariate.
The implications of the inflated type I error rates of the LR test (when the FO methodis applied) may differ depending on the purpose of the statistical test. If the test is used

47
to screen for covariate relationships, there is a high risk of false variables beingincluded. Thus, many of the models found in the covariate literature are likely tocontain too many covariates. The false covariates may lead to less precise modelpredictions, or collection of unnecessary information in future studies. The applicationof a stricter criterion, e.g. corresponding p<0.001, during model building is sometimesseen. Although this is likely to reduce the number of false covariates, it cannot fullyprotect from false variables, and it could also result in the discarding of importantrelationships by applying a criterion that is too stringent. It can be argued thatstatistical significance is not the only, and in some situations not the most important,criterion in covariate modelling. The risk of inclusion of false covariates may bereduced if the LR test is combined with other methods/criteria (graphics, mechanisticplausibility, clinical importance). The most important consequence may therefore bewhen a pre-specified covariate effect is to be tested for significance, such as a drugeffect in dose-effect studies or an interaction in a drug-drug interaction study.
The results of the LR test for assessing statistical significance for the inclusion ofcovariates when the FO method is applied also illustrate what the effects of modelapproximations can be. This may be valuable in the development of new methods. Ithas already had an impact on the development of NONMEM, in that new methods willbe available in future versions of NONMEM (Stuart Beal, personal communication),e.g. the interaction option will be possible with methods other than FOCE.
The LR test is also often employed to assess statistical significance when modellingthe variance part of the model. The present results show that the LR test cannot beused with confidence when including variance or covariance parameters in the model,since the type I error rate is sensitive both to deviations from the assumptions ofnormality of the residuals and to insufficient information per individual in the data.The use of other methods, such as graphical diagnostics, therefore gains extraimportance when modelling the statistical part of the model. This sensitivity todeviations from normality has previously been seen with linear mixed effects models(121), and thus appears to be a general problem related to the LR test.
The two stepwise covariate model building procedures, utilising GAM andNONMEM, performed similarly in the examples investigated. Thus the choice ofprocedure could be based on other more practical aspects, e.g. analyst- or computer-time efficiency. However, there are other situations when larger differences betweenprocedures could be expected – such as when the sampling design (too fewobservations per individual) precludes estimation of individual parameters with decentquality, or when time-variations in covariates and/or parameters are not easilyaccounted for. In these cases, the NONMEM procedure would be preferred. Both

48
stepwise methods will be affected by selection bias, although this was only exploredusing the NONMEM procedure. Upward biases in the stepwise estimated covariatecoefficients were evident, but the selection bias seemed to be of minor importance incomparison to the imprecision in the estimates in this example.
If the model is intended for individual dose predictions, simplicity as well as goodpredictive ability are required. Consequently, covariates that do not improve thepredictive performance should not be included. The stepwise procedures are onlybased on statistical criteria, although it would be sensible to include predictive abilityas a model building criterion. A concern with the stepwise procedures is that the over-estimated coefficients may result in poor predictive performance for the model. Whilethe difference in predictive performance between the stepwise selected and true(simulation) models was relatively small in our example, it may be an issue in othercases. Other strategies for building covariate models may therefore be considered. Oneway to obtain unbiased estimates of the covariate effects is to specify the covariatemodel based on prior knowledge and expectations about the drug in a best-guessmodel (49, 51), and estimate these effects. This is a sensible strategy, but it is notalways straightforward since covariate relationships known to be of importance maynot be supported by the data due to design issues, for example no age effect will befound if the age range in the study is too narrow. Model parameters may therefore stillneed to be tested, e.g. by backward deletion. Furthermore, the knowledge about a newdrug may be limited, in which case an exploratory search is still necessary. A rationalapproach to exploratory analysis is to limit the covariate scope to only plausiblecovariates, since this saves run time and reduces the risk of selecting false variables asa result of multiple testing. Then again, implausible covariates are sometimes testedpurposely to verify a lack of effect. The covariate scope can also be reduced bychoosing one of two highly correlated covariates, this avoids the problems withaccuracy and precision that can occur if two co-linear variables enter the modelsimultaneously (44).
Normally, time-varying covariates are not handled differently in the model from time-constant covariates. It is thus implied that the parameter associated with a covariatewill change with every change in the covariate, and that this relationship is the samefor all individuals. This may not always be the case, as was evident when the extendedmodels for time-varying covariates were applied. There may be extra knowledgelinked to the covariate change, and this can be gained by the implementation of thesemodels. This knowledge is potentially valuable for decisions regarding drug therapy.The time variation in the covariate may not be related to changes in the parameter, inwhich case only the baseline covariate is important. In such a situation there would be

49
no additional gain in measuring the covariate more than at baseline. Largeinterindividual variability in a covariate relationship may indicate that individual doseadjustment based on the covariate is less useful, as the effect of the covariate changewill differ between individuals. More frequent monitoring of the patients maytherefore be needed.
This thesis calls attention to a number of issues to consider when building the covariatemodel. These are summarised and illustrated with the darifenacin covariate analysis:
1. The choice of estimation method.
The darifenacin data set included frequent sampling in the majority of individuals, andthe residual error was heteroscedastic. Thus, the preferable method would be FOCEINTER, although this method was in fact unusable because of numerical problems.Since covariate randomisation was not practicable because of long run times(regardless of method) the choice of method was FOCE, with a GLS-related approachto account for the η-ε interaction.
2. The choice of covariate model building approach.
Covariates indicated to be important in previous findings were first specified in themodel. However, the aim of the modelling was to search for new potential covariateinfluences. Thus, an exploratory search was also carried out. The long run timedominated in the decisions on modelling approach, and precluded the use of thestepwise NONMEM method. The GAM procedure was therefore used to limit thenumber of covariates to test, and a modified stepwise approach was applied toincorporate covariates in the mixed effects model.
3. The handling of time-varying covariates in the model.
To account for time variation, data originating from different study occasions weretreated as separate individuals in the GAM. None of the covariates in the final modelvaried with time.
4. Criteria to include a covariate in the final model.
Apart from being statistically significant, the mechanistic plausibility of the covariatesin the final model was also considered: (i) the race effect in F may have been due toextrinsic factors (such as diet), (ii) the gender effect in CL may be explainable bylower CYP2D6 activity in females (122), and (iii) the night-time effect in CL indicatesa circadian rhythm.

50
SUMMARY & CONCLUSIONS
The aims of this thesis were to increase the efficiency, predictability and robustness ofcovariate model building. To meet these goals, the following were carried out: (i) thefirst systematic investigation of the performance of the LR test when modelling withNONMEM, (ii) the first comparison of covariate model building strategies, (iii) thefirst assessment of the magnitude of selection bias in PK-PD nonlinear mixed effectsmodelling, and (iv) the first systematic study where models for time-varying covariateswere applied. The conclusions from these studies are:
The frequency of type I errors, when the LR test is applied for testing covariateeffects in a model, is severely upward biased when an inappropriate estimationmethod is used. If a method suitable for the data and error structure is utilised,e.g. FOCE INTER for a nonlinear model with heteroscedastic error, the type Ierror rates are in agreement with the expected, and the LR test can be used withconfidence for assessing statistical significance.
Covariate randomisation provides a means of obtaining agreement betweenestimated and expected type I error rates in situations where an otherwiseappropriate estimation method is not practicable.
The LR test is only applicable for testing inclusion of variance/covarianceparameters in the model if an appropriate estimation method is used and if theunderlying assumptions of normality of the residuals and enough information inthe data hold true.
The stepwise covariate model building methods performed similarly in theexamples investigated, allowing the choice of procedure to be based on morepractical aspects. There may however be other situations where differences inperformance may prevail, such as when sampling is too sparse to give reliableindividual parameter estimates or it is not possible to account for time variationin the GAM procedure.
Selection bias was evident in the stepwise selected covariate coefficients,although this bias was minor in comparison to the imprecision. If the model isintended for prognostic purposes it may still have to be considered, and otherways of building the model may be required.

51
By applying covariate models that estimate interindividual variability in thecovariate effect, or account for differences in variability between and withinindividuals in a time-varying covariate, important knowledge can be gainedabout the PK-PD characteristics of a drug. This knowledge is of value fordecisions on drug therapy and in drug development.
Regardless of what may be perceived as “best-practice” with respect tocovariate model building, modelling practicalities, such as run times, governwhich methods are possible to use. Knowledge of properties and limitations ofother methods allows the modeller to make an informed choice betweenalternative modelling approaches.

52
ACKNOWLEDGMENTS
The work behind this thesis was carried out at the Department of PharmaceuticalBiosciences, Division of Pharmacokinetics and Drug Therapy, Faculty of Pharmacy,Uppsala University, Sweden.
First of all, I would like to sincerely thank my supervisor, Professor Mats Karlsson. Ithas been a privilege to work with you and learn pharmacometrics from you, I haveenjoyed it a lot. Your enthusiasm, knowledge and grand ideas have been invaluable!
A huge thank you to Dr Niclas Jonsson – my second supervisor, and “big brother” inthe covariate world – for your thoughtfulness, and for all good advice and assistance. Ithas been fun working with you! Thanks also for reconsidering the extensive (220+)search…
Many thanks to Professor Margareta Hammarlund-Udenaes, head of the division, forproviding excellent working facilities, and for your interest in my work.
I would also like to thank Professor Emeritus Lennart Paalzow for your contributionsto the field of pharmacokinetics and pharmacodynamics – for founding the division,and for providing nice working facilities.
Dr René Bouw, Katalin Matolcsi, Dr Alison Thomson, Dr Peter Milligan, and DrThomas Kerbusch, my co-authors – thank you for contributions to my thesis! A specialthanks to Thomas – for many laughs and for being a good mentor and friend!!
I would like to express my gratitude to Astrazeneca R&D Mölndal, the SwedishAcademy of Pharmaceutical Sciences, and the Faculty of Pharmacy for financialsupport.
Lena & Dr Ulrika – my room-mates and friends, thank you for both work relateddiscussions and gossiping… for the fun travels we have made together and manylaughs - I’m sure there’ll be more!!
Siv – du är en pärla! Thank you for letting me ‘älta’ things when I have needed to, andfor all fun during our travelling together. I also appreciate your help with the thesis.
Dr Marie, thank you for looking out for me, and for all your pep talks!

53
Thanks to all past and present fellow PhD-students and colleagues – for making thedivision the best place to work! Anja, Karin, Emma B, Anubha, Lasse, MaMa, Jakob,Jacob, Anders, Jörgen, Johan, Emma H, Ann-Marie, Ulrika E, Mia, Kristin, Rikard,Fredrik, Leslie, Marianne, Karin S, Anna-Sofia, Jessica, Agneta, Kjell, Britt, Annica –I am going to miss all of you! Thanks also to the Astrazeneca boys – PH and Marcus –for lots of fun during travels! Special thanks to Leslie, for helping me with reading mythesis, and to Lasse, for nursing the computers!
Thanks are also due to sid, enos, effie, doris, joe, jack, avarell, william, gandalf,gollum & Co without whom there would not have been a thesis...
Tack också till alla mina vänner, och då särskilt:
Dr Sanna, för ditt stöd, och många roliga stunder!
Jenny S, för din generositet och din omtanke – och allt roligt (och mindre roligt) somvi delat!
Jenny F, för din ovärderliga vänskap, för att du alltid ställer upp och för alla dina klokatankar! Jag kommer att sakna att ha dig i närheten. Domo arigato gozaimashita!
Lillebror Anders, Lina & Jonis – tack för er omtanke och gästfrihet, ni är guld värda!Ante – tack också för hjälp med bilder!
Storebror Urban, Eva, Ingrid & Luvan – mille grazie för ’goda råd från Rolf’, ochmånga mysiga stunder. Jag saknar er!
Mor Lena & Pappa Lennart, tack för att ni alltid finns där, med kärlek, trygghet ochstöd i alla lägen.
Min älskade Bengt. Du är bäst ♥Tack för din omtanke och generositet,ditt stöd och stora tålamod.Nu är det vår tur.
Ulrika

54
REFERENCES
1. Sheiner, L. and Wakefield, J. Population modelling in drug development. Stat Methods MedRes 8:183-193 (1999).
2. Ette, E. I., Williams, P., Fadiran, E., Ajayi, F. O., and Onyiah, L. C. The process of knowledgediscovery from large pharmacokinetic data sets. J Clin Pharmacol 41:25-34 (2001).
3. Sheiner, L. B., Rosenberg, B., and Melmon, K. L. Modelling of individual pharmacokineticsfor computer-aided drug dosage. Comput Biomed Res 5:441-459 (1972).
4. Sheiner, L. B., Rosenberg, B., and Marathe, V. V. Estimation of population characteristics ofpharmacokinetic parameters from routine clinical data. J Pharmacokin Biopharm 5:445-479(1977).
5. Sheiner, L. B. and Ludden, T. M. Population pharmacokinetics/dynamics. Annu RevPharmacol Toxicol 32:185-209 (1992).
6. Sheiner, L. B. and Steimer, J. L. Pharmacokinetic/pharmacodynamic modeling in drugdevelopment. Annu Rev Pharmacol Toxicol 40:67-95 (2000).
7. Aarons, L. Sparse data analysis. Eur J Drug Metab Pharmacokinet 18:97-100 (1993).8. Vozeh, S., Steimer, J. L., Rowland, M., Morselli, P., Mentre, F., Balant, L. P., and Aarons, L.
The use of population pharmacokinetics in drug development. Clin Pharmacokinet 30:81-93(1996).
9. FDA. Guidance for Industry Population pharmacokinetics. U.S. Food and DrugAdministration, Department of Health and Human Services, Rockville MD,(http://www.fda.gov/cder/guidance/index.htm), 1999.
10. Balant, L. P. and Gex-Fabry, M. Modelling during drug development. Eur J Pharm Biopharm50:13-26 (2000).
11. Aarons, L., Karlsson, M. O., Mentre, F., Rombout, F., Steimer, J. L., and van Peer, A. Role ofmodelling and simulation in Phase I drug development. Eur J Pharm Sci 13:115-122 (2001).
12. Aarons, L. Population pharmacokinetics. Int J Clin Pharmacol Ther Toxicol 30:520-522(1992).
13. Sheiner, B. L. and Beal, S. L. Evaluation of methods for estimating populationpharmacokinetic parameters. II. Biexponential model and experimental pharmacokinetic data.J Pharmacokin Biopharm 9:635-651 (1981).
14. Minto, C. and Schnider, T. Expanding clinical applications of population pharmacodynamicmodelling. Br J Clin Pharmacol 46:321-333 (1998).
15. Jönsson, S. and Karlsson, M. O. A Rational Approach for Selection of Optimal Covariate-Based Dosing Strategies. Clin Pharmacol Ther, accepted for publication.
16. Sandstrom, M., Karlsson, M. O., Ljungman, P., Hassan, Z., Jonsson, E. N., Nilsson, C.,Ringden, O., Oberg, G., Bekassy, A., and Hassan, M. Population pharmacokinetic analysisresulting in a tool for dose individualization of busulphan in bone marrow transplantationrecipients. Bone Marrow Transplant 28:657-664 (2001).
17. Karlsson, M. O., Beal, S. L., and Sheiner, L. B. Three new residual error models forpopulation PK/PD analyses. J Pharmacokin Biopharm 23:651-672 (1995).
18. Karlsson, M. O., Jonsson, E. N., Wiltse, C. G., and Wade, J. R. Assumption testing inpopulation pharmacokinetic models: illustrated with an analysis of moxonidine data fromcongestive heart failure patients. J Pharmacokin Biopharm 26:207-246 (1998).

55
19. Karlsson, M. O. and Sheiner, L. B. The importance of modeling interoccasion variability inpopulation pharmacokinetic analyses. J Pharmacokin Biopharm 21:735-750 (1993).
20. Wade, J. R., Beal, S. L., and Sambol, N. C. Interaction between structural, statistical, andcovariate models in population pharmacokinetic analysis. J Pharmacokin Biopharm 22:165-177 (1994).
21. Aarons, L. Software for population pharmacokinetics and pharmacodynamics. ClinPharmacokinet 36:255-264 (1999).
22. Barrett, J. S., Population Pharmacokinetics, in Pharmacokinetics in Drug Discovery andDevelopment, Schoenwald, R.D., Editor. 2002, CRC Press: Boca Raton, Florida.
23. Davidian, M. and Giltinan, D. M. Nonlinear Models for Repeated Measurement Data. In Cox,D.R., et al. (eds.), Monographs on Statistics and Applied Probability 62, Chapman & Hall,London, 1995.
24. Beal, S. L. and Sheiner, L. B. NONMEM Users Guides. In (eds.), University of California,San Francisco, CA, 1992.
25. Lindstrom, M. L. and Bates, D. M. Nonlinear mixed effects models for repeated measuresdata. Biometrics 46:673-687 (1990).
26. Wolfinger, R. D. Laplace's approximation for nonlinear mixed models. Biometrika 80:791-795(1993).
27. WinNonMix Users Guide, v. 2.0. Pharsight Corporation, Mountain View, CA, 2000.28. Mallet, A. A maximum likelihood estimation method for random coefficient regression
models. Biometrika 73:645-656 (1986).29. Schumitzky, A. Nonparametric EM algorithms for estimating prior distributions. Applied
Mathematics and Computation 45:143-157 (1991).30. Davidian, M. and Gallant, A. R. The nonlinear mixed effects model with a smooth random
effects density. Biometrika 80:475-488 (1993).31. Wakefield, J. C., Smith, A. F. M., Racine-Poon, A., and Gelfand, A. E. Bayesian Analysis of
Linear and Nonlinear Population Models using the Gibbs Sampler. Appl Statist 41:201-221(1994).
32. Spiegelhalter, D. J., Thomas, A., Best, N. G., and Gilks, W. R. BUGS: Bayesian inferenceUsing Gibbs Sampling, version 0.5, (version ii). MRC Biostatistics Unit, Cambridge, UK,1996.
33. Bennett, J. E. and Wakefield, J. C. A comparison of a Bayesian population method with twomethods as implemented in commercially available software. J Pharmacokin Biopharm24:403-432 (1996).
34. Roe, D. J. Comparison of population pharmacokinetic modeling methods using simulateddata: results from the Population Modeling Workgroup. Stat Med 16:1241-1257; discussion1257-1262 (1997).
35. Beal, S. L. Population pharmacokinetic data and parameter estimation based on their first twostatistical moments. Drug Metabolism Reviews 15:173-193 (1984).
36. Beal, S. L. and Sheiner, L. B. NONMEM Users Guide, Part VII. In (eds.), University ofCalifornia, San Francisco, CA, 1992.
37. Wallenstein, G. C., Stangier, J., and Ludden, T. M. Analyzing rich data using differentmethods provided by NONMEM: pharmacokinetics of telmisartan following intravenousinfusion to healthy volunteers. Pharm Res 16:772-776 (1999).
38. Wakefield, J. and Walker, S. A population approach to initial dose selection. Stat Med16:1135-1149 (1997).
39. Maitre, P. O., Buhrer, M., Thomson, D., and Stanski, D. R. A three-step approach combiningBayesian regression and NONMEM population analysis: application to midazolam. JPharmacokin Biopharm 19:377-384 (1991).

56
40. Mandema, J. W., Verotta, D., and Sheiner, L. B. Building population pharmacokinetic-pharmacodynamic models. I. Models for covariate effects. J Pharmacokin Biopharm 20:511-528 (1992).
41. Jonsson, E. N. and Karlsson, M. O. Automated covariate model building within NONMEM.Pharm Res 15:1463-1468 (1998).
42. Kowalski, K. G. and Hutmacher, M. M. Efficient screening of covariates in population modelsusing Wald's approximation to the likelihood ratio test. J Pharmacokin Pharmacodyn 28:253-275 (2001).
43. Ette, E. I. and Ludden, T. M. Population pharmacokinetic modeling: the importance ofinformative graphics. Pharm Res 12:1845-1855 (1995).
44. Bonate, P. L. The effect of collinearity on parameter estimates in nonlinear mixed effectmodels. Pharm Res 16:709-717 (1999).
45. Ribbing, J. and Jonsson, E. N. The effect of collinearity on the selection of covariates inpopulation pharmacokinetic anaysis. Poster, Eleventh PAGE meeting, Paris (2002).
46. Verotta, D., Building population pharmacokinetic-pharmacodynamic models using trees, inThe population approach: measuring and managing variability in response, concentrationand dose, Aarons, L., et al., Editors. 1997, European Commission: Brussels.
47. Harrell, F. E. Regression Modeling Strategies. Springer Series in Statistics, Springer, NewYork, 2001.
48. Miller, A. J. Subset Selection in Regression. Monographs on Statistics and AppliedProbability, Chapman & Hall, London, 1990.
49. Steyerberg, E. W., Eijkemans, M. J., Harrell, F. E., Jr., and Habbema, J. D. Prognosticmodelling with logistic regression analysis: a comparison of selection and estimation methodsin small data sets. Stat Med 19:1059-1079 (2000).
50. Vach, K., Sauerbrei, W., and Schumacher, M. Variable selection and shrinkage: comparison ofsome approaches. Stat Neerl 55:53-75 (2001).
51. Harrell, F. E., Jr., Lee, K. L., and Mark, D. B. Multivariable prognostic models: issues indeveloping models, evaluating assumptions and adequacy, and measuring and reducing errors.Stat Med 15:361-387 (1996).
52. Hossain, M., Wright, E., Baweja, R., Ludden, T., and Miller, R. Nonlinear mixed effectsmodeling of single dose and multiple dose data for an immediate release (IR) and a controlledrelease (CR) dosage form of alprazolam. Pharm Res 14:309-315 (1997).
53. Laporte, S., Mismetti, P., Piquet, P., Doubine, S., Touchot, A., and Decousus, H. Populationpharmacokinetic of nadroparin calcium (Fraxiparine) in children hospitalised for open heartsurgery. Eur J Pharm Sci 8:119-125 (1999).
54. Schuttler, J. and Ihmsen, H. Population pharmacokinetics of propofol: a multicenter study.Anesthesiol 92:727-738 (2000).
55. Garcia Sanchez, M. J., Manzanares, C., Santos-Buelga, D., Blazquez, A., Manzanares, J.,Urruzuno, P., and Medina, E. Covariate effects on the apparent clearance of tacrolimus inpaediatric liver transplant patients undergoing conversion therapy. Clin Pharmacokinet 40:63-71 (2001).
56. Mirochnick, M., Cooper, E., Capparelli, E., McIntosh, K., Lindsey, J., Xu, J., Jacobus, D.,Mofenson, L., Bonagura, V. R., Nachman, S., Yogev, R., Sullivan, J. L., and Spector, S. A.Population pharmacokinetics of dapsone in children with human immunodeficiency virusinfection. Clin Pharmacol Ther 70:24-32 (2001).
57. Williams, P. J., Lane, J. R., Turkel, C. C., Capparelli, E. V., Dziewanowska, Z., and Fox, A.W. Dichloroacetate: population pharmacokinetics with a pharmacodynamic sequential linkmodel. J Clin Pharmacol 41:259-267 (2001).

57
58. Wakefield, J. and Bennett, J. The Bayesian Modeling of Covariates for PopulationPharmacokinetic Models. J Am Statist Assoc 91:917-927 (1996).
59. Jonsson, E. N. and Karlsson, M. O. Xpose--an S-PLUS based populationpharmacokinetic/pharmacodynamic model building aid for NONMEM. Comput MethodsPrograms Biomed 58:51-64 (1999).
60. McFadyen, M. L., Miller, R., and Ludden, T. M. Ketotifen pharmacokinetics in children withatopic perennial asthma. Eur J Clin Pharmacol 52:383-386 (1997).
61. du Preez, M. J., Botha, J. H., McFadyen, M. L., and Holford, N. H. The pharmacokinetics oftheophylline in premature neonates during the first few days after birth. Ther Drug Monit21:598-603 (1999).
62. Zhou, X. J., Sheiner, L. B., D'Aquila, R. T., Hughes, M. D., Hirsch, M. S., Fischl, M. A.,Johnson, V. A., Myers, M., and Sommadossi, J. P. Population pharmacokinetics of nevirapine,zidovudine, and didanosine in human immunodeficiency virus-infected patients. AntimicrobAgents Chemother 43:121-128. (1999).
63. Gallo, J. M., Laub, P. B., Rowinsky, E. K., Grochow, L. B., and Baker, S. D. Populationpharmacokinetic model for topotecan derived from phase I clinical trials. J Clin Oncol18:2459-2467 (2000).
64. Gwilt, P., Tempero, M., Kremer, A., Connolly, M., and Ding, C. Pharmacokinetics oflevamisole in cancer patients treated with 5- fluorouracil. Cancer Chemother Pharmacol45:247-251 (2000).
65. Freyer, G., Tranchand, B., Ligneau, B., Ardiet, C., Souquet, P. J., Court-Fortune, I., Riou, R.,Rebattu, P., Boissel, J. P., Trillet-Lenoir, V., and Girard, P. Population pharmacokinetics ofdoxorubicin, etoposide and ifosfamide in small cell lung cancer patients: results of amulticentre study. Br J Clin Pharmacol 50:315-324 (2000).
66. Ouellet, D., Periclou, A. P., Johnson, R. D., Woodworth, J. R., and Lalonde, R. L. Populationpharmacokinetics of pemetrexed disodium (ALIMTA) in patients with cancer. CancerChemother Pharmacol 46:227-234 (2000).
67. Troconiz, I. F., Armenteros, S., Planelles, M. V., Benitez, J., Calvo, R., and Dominguez, R.Pharmacokinetic-Pharmacodynamic Modelling of the antipyretic effect of two oralformulations of ibuprofen. Clin Pharmacokinet 38:505-518 (2000).
68. Zhou, H., Chen, T. L., Marino, M., Lau, H., Miller, T., Kalafsky, G., and McLeod, J. F.Population PK and PK/PD modelling of microencapsulated octreotide acetate in healthysubjects. Br J Clin Pharmacol 50:543-552 (2000).
69. Barrett, J. S., Gibiansky, E., Hull, R. D., Planes, A., Pentikis, H., Hainer, J. W., Hua, T. A.,and Gastonguay, M. Population pharmacodynamics in patients receiving tinzaparin for theprevention and treatment of deep vein thrombosis. Int J Clin Pharmacol Ther 39:431-446(2001).
70. Cullberg, M., Eriksson, U. G., Larsson, M., and Karlsson, M. O. Population modelling of theeffect of inogatran, at thrombin inhibitor, on ex vivo coagulation time (APTT) in healthysubjects and patients with coronary artery disease. Br J Clin Pharmacol 51:71-79 (2001).
71. Kerbusch, T., Mathjt, R. A., Keizer, H. J., Ouwerkerk, J., Rodenhuis, S., Schellens, J. H., andBeijnen, J. H. Population pharmacokinetics and exploratory pharmacodynamics of ifosfamideand metabolites after a 72-h continuous infusion in patients with soft tissue sarcoma. Eur JClin Pharmacol 57:467-477 (2001).
72. Takama, H., Tanaka, H., Sudo, T., Tamura, T., and Tanigawara, Y. Populationpharmacokinetic modeling and model validation of a spicamycin derivative, KRN5500, inphase 1 study. Cancer Chemother Pharmacol 47:404-410 (2001).
73. Milligan, P. A., Marshall, S. F., and Karlsson, M. O. A population pharmacokinetic analysis ofsildenafil citrate in patients with erectile dysfunction. Br J Clin Pharmacol 53 Suppl 1:45S-52S (2002).

58
74. Shen, M., Schilder, R. J., Obasaju, C., and Gallo, J. M. Population pharmacokinetic andlimited sampling models for carboplatin administered in high-dose combination regimens withperipheral blood stem cell support. Cancer Chemother Pharmacol 50:243-250 (2002).
75. Ette, E. I. Stability and performance of a population pharmacokinetic model. J Clin Pharmacol37:486-495 (1997).
76. de Alwis, D. P., Aarons, L., and Palmer, J. L. Population pharmacokinetics of ondansetron: acovariate analysis. Br J Clin Pharmacol 46:117-125 (1998).
77. Bressolle, F., Joulia, J. M., Pinguet, F., Ychou, M., Astre, C., Duffour, J., and Gomeni, R.Circadian rhythm of 5-fluorouracil population pharmacokinetics in patients with metastaticcolorectal cancer. Cancer Chemother Pharmacol 44:295-302 (1999).
78. Campbell, D., Thomson, A. H., and Stack, B. Population pharmacokinetics of aminoglycosideantibiotics in patients with cystic fibrosis. Ther Drug Monit 21:281-288 (1999).
79. Moore, K. H., Yuen, G. J., Hussey, E. K., Pakes, G. E., Eron, J. J., Jr., and Bartlett, J. A.Population pharmacokinetics of lamivudine in adult human immunodeficiency virus-infectedpatients enrolled in two phase III clinical trials. Antimicrob Agents Chemother 43:3025-3029(1999).
80. Ingwersen, S. H., Pedersen, P. C., Groes, L., Nielsen, K. K., and Aarons, L. Populationpharmacokinetics of tiagabine in epileptic patients on monotherapy. Eur J Pharm Sci 11:247-254 (2000).
81. Jorga, K., Banken, L., Fotteler, B., Snell, P., and Steimer, J. L. Population pharmacokinetics oflevodopa in patients with Parkinson's disease treated with tolcapone. Clin Pharmacol Ther67:610-620 (2000).
82. Jorga, K., Fotteler, B., Banken, L., Snell, P., and Steimer, J. L. Population pharmacokinetics oftolcapone in parkinsonian patients in dose finding studies. Br J Clin Pharmacol 49:39-48(2000).
83. Peng, A. W., Hussey, E. K., and Moore, K. H. A population pharmacokinetic analysis ofzanamivir in subjects with experimental and naturally occurring influenza: effects offormulation and route of administration. J Clin Pharmacol 40:242-249. (2000).
84. Xuan, D., Lu, J. F., Nicolau, D. P., and Nightingale, C. H. Population pharmacokinetics oftobramycin in hospitalized patients receiving once-daily dosing regimen. Int J AntimicrobAgents 15:185-191. (2000).
85. Chan, E., Lee, H. S., and Hue, S. S. Population pharmacokinetics of carbamazepine inSingapore epileptic patients. Br J Clin Pharmacol 51:567-576 (2001).
86. Phillips, L., Grasela, T. H., Agnew, J. R., Ludwig, E. A., and Thompson, G. A. A populationpharmacokinetic-pharmacodynamic analysis and model validation of azimilide. ClinPharmacol Ther 70:370-383 (2001).
87. Kuipers, J. A., Boer, F., de Roode, A., Olofsen, E., Bovill, J. G., and Burm, A. G. Modelingpopulation pharmacokinetics of lidocaine: should cardiac output be included as a patientfactor? Anesthesiol 94:566-573 (2001).
88. Nguyen, L., Tranchand, B., Puozzo, C., and Variol, P. Population pharmacokinetics model andlimited sampling strategy for intravenous vinorelbine derived from phase I clinical trials. Br JClin Pharmacol 53:459-468 (2002).
89. Taright, N., Mentré, F., and Mallet, A. Non-Stationarity of Kinetic Parameters in Multi-Occasion Designs. Oral presentation, Sixth PAGE meeting, Glasgow (1997).
90. Aarons, L., Balant, L. P., Mentre, F., Morselli, P. L., Rowland, M., Steimer, J. L., and Vozeh,S. Practical experience and issues in designing and performing populationpharmacokinetic/pharmacodynamic studies. Eur J Clin Pharmacol 49:251-254 (1996).
91. Beal, S. L. and Sheiner, L. B. Estimating population kinetics. Crit Rev Biomed Eng 8:195-222(1982).

59
92. Sheiner, L. B. and Beal, S. L. A note on confidence intervals with extended least squaresparameter estimates. J Pharmacokin Biopharm 15:93-98 (1987).
93. White, D. B., Walawander, C. A., Tung, Y., and Grasela, T. H. An evaluation of point andinterval estimates in population pharmacokinetics using NONMEM analysis. J PharmacokinBiopharm 19:87-112 (1991).
94. White, D. B., Walawander, C. A., Liu, D. Y., and Grasela, T. H. Evaluation of hypothesistesting for comparing two populations using NONMEM analysis. J Pharmacokin Biopharm20:295-313 (1992).
95. Sheiner, L. B. Analysis of pharmacokinetic data using parametric models. III. Hypothesis testsand confidence intervals. J Pharmacokin Biopharm 14:539-555 (1986).
96. Efron, B. and Tibshirani, R. J. An Introduction to the Bootstrap. In Cox, D.R., et al. (eds.),Monographs on Statistics and Applied Probability 57, Chapman & Hall, New York, 1993.
97. CDDS, Simulation in Drug Development: Good Practices. In Holford, N.G.H., et al. (eds.),CDDS: Georgetown University (http://cdds.georgetown.edu/research/sddgp723.html),Washington, DC, 1999.
98. Holford, N. H., Kimko, H. C., Monteleone, J. P., and Peck, C. C. Simulation of clinical trials.Annu Rev Pharmacol Toxicol 40:209-234 (2000).
99. Mentre, F. and Ebelin, M.-E., Validation of population pharmacokinetic/pharmacodynamicanalyses: review of proposed approaches, in The population approach: measuring andmanaging variability in response, concentration and dose, Aarons, L., et al., Editors. 1997,European Commission: Brussels.
100. Blanco Serrano, B., Garcia Sanchez, M. J., Otero, M. J., Buelga, D. S., Serrano, J., andDominguez-Gil, A. Valproate population pharmacokinetics in children. J Clin Pharm Ther24:73-80 (1999).
101. Blanco-Serrano, B., Otero, M. J., Santos-Buelga, D., Garcia-Sanchez, M. J., Serrano, J., andDominguez-Gil, A. Population estimation of valproic acid clearance in adult patients usingroutine clinical pharmacokinetic data. Biopharm Drug Dispos 20:233-240 (1999).
102. Capparelli, E. V., Lane, J. R., Romanowski, G. L., McFeely, E. J., Murray, W., Sousa, P.,Kildoo, C., and Connor, J. D. The influences of renal function and maturation on vancomycinelimination in newborns and infants. J Clin Pharmacol 41:927-934 (2001).
103. Falcao, A. C., Buelga, D. S., Mendez, M. E., Garcia, M. J., and Pardo, M. Population kineticsof tobramycin in neonates. Ther Drug Monit 23:202-208 (2001).
104. Bruno, R., Vivler, N., Vergniol, J. C., De Phillips, S. L., Montay, G., and Sheiner, L. B. Apopulation pharmacokinetic model for docetaxel (Taxotere): model building and validation. JPharmacokin Biopharm 24:153-172 (1996).
105. Rosario, M. C., Thomson, A. H., Jodrell, D. I., Sharp, C. A., and Elliott, H. L. Populationpharmacokinetics of gentamicin in patients with cancer. Br J Clin Pharmacol 46:229-236(1998).
106. Valodia, P. N., Seymour, M. A., McFadyen, M. L., Miller, R., and Folb, P. I. Validation ofpopulation pharmacokinetic parameters of phenytoin using the parallel Michaelis-Menten andfirst-order elimination model. Ther Drug Monit 22:313-319 (2000).
107. Zomorodi, K., Donner, A., Somma, J., Barr, J., Sladen, R., Ramsay, J., Geller, E., and Shafer,S. L. Population pharmacokinetics of midazolam administered by target controlled infusion forsedation following coronary artery bypass grafting. Anesthesiol 89:1418-1429 (1998).
108. Schnider, T. W., Gaeta, R., Brose, W., Minto, C. F., Gregg, K. M., and Shafer, S. L.Derivation and Cross-validation of Pharmacokinetic Parameters for Computer-controlledInfusion of Lidocaine in Pain Therapy. Anesthesiol 84:1043-1050 (1996).
109. Frame, B. C., Facca, B. F., Nicolau, D. P., and Triesenberg, S. N. Population pharmacokineticsof continuous infusion ceftazidime. Clin Pharmacokinet 37:343-350 (1999).

60
110. Efron, B. Bootstrap Methods: Another Look at the Jackknife. Annals of Statistics 7:1-26(1979).
111. Parke, J. and Charles, B. G. Factors affecting oral cyclosporin disposition after hearttransplantation: bootstrap validation of a population pharmacokinetic model. Eur J ClinPharmacol 56:481-487 (2000).
112. Reith, D. M., Hooper, W. D., Parke, J., and Charles, B. Population pharmacokinetic modelingof steady state carbamazepine clearance in children, adolescents, and adults. J PharmacokinPharmacodyn 28:79-92 (2001).
113. Crul, M., Mathot, R. A., Giaccone, G., Punt, C. A., Rosing, H., Hillebrand, M. X., Ando, Y.,Nishi, N., Tanaka, H., Schellens, J. M., and Beijnen, J. H. Population pharmacokinetics of thenovel anticancer agent KRN7000. Cancer Chemother Pharmacol 49:287-293 (2002).
114. Sheiner, L. B. and Beal, S. L. Some suggestions for measuring predictive performance. JPharmacokin Biopharm 9:503-512 (1981).
115. Vozeh, S., Maitre, P. O., and Stanski, D. R. Evaluation of population (NONMEM)pharmacokinetic parameter estimates. J Pharmacokin Biopharm 18:161-173 (1990).
116. Krishna, S., Nagaraja, N. V., Planche, T., Agbenyega, T., Bedo-Addo, G., Ansong, D.,Owusu-Ofori, A., Shroads, A. L., Henderson, G., Hutson, A., Derendorf, H., and Stacpoole, P.W. Population pharmacokinetics of intramuscular quinine in children with severe malaria.Antimicrob Agents Chemother 45:1803-1809 (2001).
117. Bonate, P. L. A brief introduction to Monte Carlo simulation. Clin Pharmacokinet 40:15-22.(2001).
118. Walsh, T. J., Wood, N., Milligan, P. A., Karlsson, M. O., Lutsar, I., Arguedas, A., Driscoll, T.,and Adamson, P. Pharmacokinetics of intravenous voriconazole in children after single andmultiple dose administration. Abstracts of the 41st Interscience Conference on AntimicrobialAgents and Chemotherapy, Chicago, IL, Abstract A17 (2001).
119. Friberg, L. E., Henningsson, A., Maas, H., Nguyen, L., and Karlsson, M. O. Model ofChemotherapy-Induced Myelosuppression with Parameter Consistency Across Drugs. J ClinOncol, accepted for publication.
120. Manly, B. F. J. Randomization, Bootstrap and Monte Carlo Methods in Biology. In Chatfield,C. and Zidek, J.V. (eds.), Texts in Statistical Science, Chapman & Hall, London, 1997.
121. Vonesh, E. F., Chinchilli, V. M., and Pu, K. Goodness-of-fit in generalized nonlinear mixed-effects models. Biometrics 52:572-587 (1996).
122. Tanaka, E. Gender-related differences in pharmacokinetics and their clinical significance. JClin Pharm Ther 24:339-346 (1999).