Embed Size (px)
Citation preview
A S H I S H K A K A R P T , D P T , O C S , C M T P TB O A R D C E R T I F I E D C L I N I C A L S P E C I A L I S T I N O R T H O P A E D I C
P H Y S I C A L T H E R A P Y
Utilizing Telehealth To PerformAn Evaluation
INTRODUCTION
Dr. Kakar is a Board Certified Clinical Specialist in Orthopaedic
Physical Therapy. He has an interest in treating sports injuries and
neck/low back pain with a focus on patient education and injury
prevention. In his current role he is practicing as a Physical Therapist at
Walter Reed National Military Medical Center and is the subject
matter expert for telehealth.
No relevant disclosuresDisclaimer: The views expressed in this presentation are those of the author(s) and do not necessarily reflect the official policy of the Department of Defense or the U.S. Government.
LEARNING OBJECTIVES
Identify the appropriate patient for telehealth visits.
Explain the key strategies on how to perform a telehealth evaluation
Observe a mock telehealth evaluation
TELEHEALTH TERMS
TELEMEDECINE: defined by the Federation of State Medical Boards as “the practice of medicine using electronic communication, information technology, or other means between a physician in one location, and a patient in another location, with or without an intervening health care provider”.
TELEHEALTH: “the use of electronic information and telecommunication technologies to support and promote long-distance clinical health care, patient and professional health-related education, public health and health administration”.
ASYNCHRONOUS: communication between providers, patients, and caregivers stored for future reference or response.
SYNCHRONOUS: a ‘real-time’ interaction for patient health communication. Patients can have caregivers or in-home nursing present to assist the remote physician.
BENEFITS OF TELEHEALTH
Improve access to care
Reduce travel time
Cost Savings
Reduce waiting times
Convenience
TELEHEALTH REGULATIONS
Provider must abide by state laws in which they are practicing
Informed consent must be obtained
Confirm malpractice insurance cover telehealth
Initiate dedicated training for providers
Set up office space for telehealth encounters
Develop a telehealth standards of practice (SOP)
Obtain HIPPA compliant platform
IDENTIFYING THE RIGHT PATIENT
Tech Savvy
Access to high speed internet and quiet open space
Best for patients that do not require hands on care
Non traumatic injuries
CHALLENGES
It requires High speed internet capabilities
Difficult to assess range of motion testing
Unable to perform manual muscle testing
Unable to perform passive accessory motion testing.
Difficulty with performing special tests
RANGE OF MOTION
Functional
Dysfunctional
Functional but painful
Dysfunctional and painful
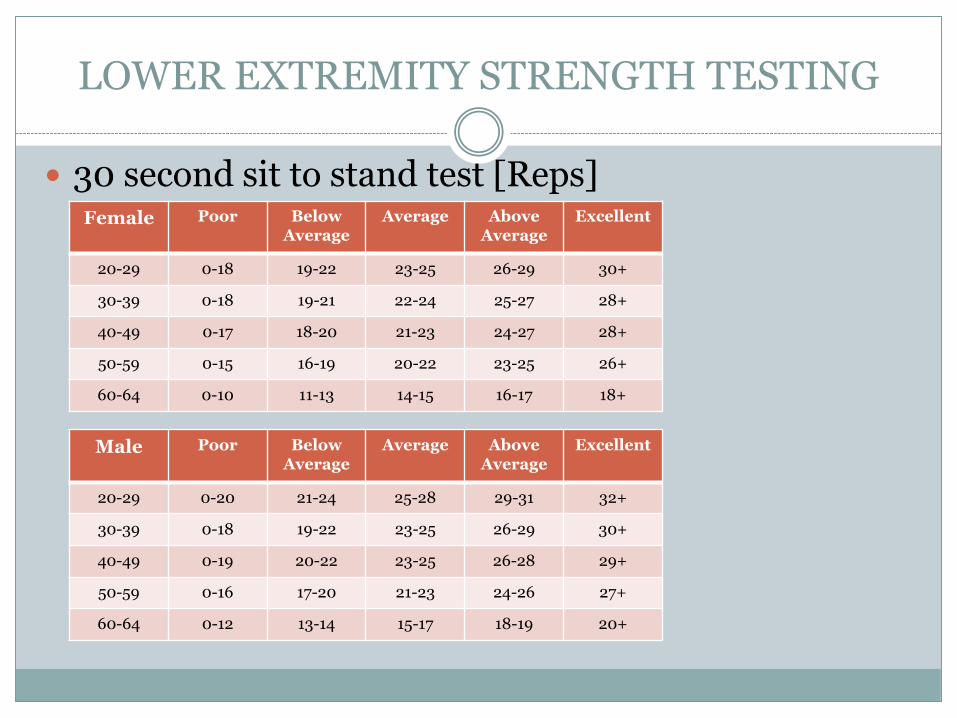
LOWER EXTREMITY STRENGTH TESTING
30 second sit to stand test [Reps]Female Poor Below
AverageAverage Above
AverageExcellent
20-29 0-18 19-22 23-25 26-29 30+
30-39 0-18 19-21 22-24 25-27 28+
40-49 0-17 18-20 21-23 24-27 28+
50-59 0-15 16-19 20-22 23-25 26+
60-64 0-10 11-13 14-15 16-17 18+
Male Poor Below Average
Average Above Average
Excellent
20-29 0-20 21-24 25-28 29-31 32+
30-39 0-18 19-22 23-25 26-29 30+
40-49 0-19 20-22 23-25 26-28 29+
50-59 0-16 17-20 21-23 24-26 27+
60-64 0-12 13-14 15-17 18-19 20+
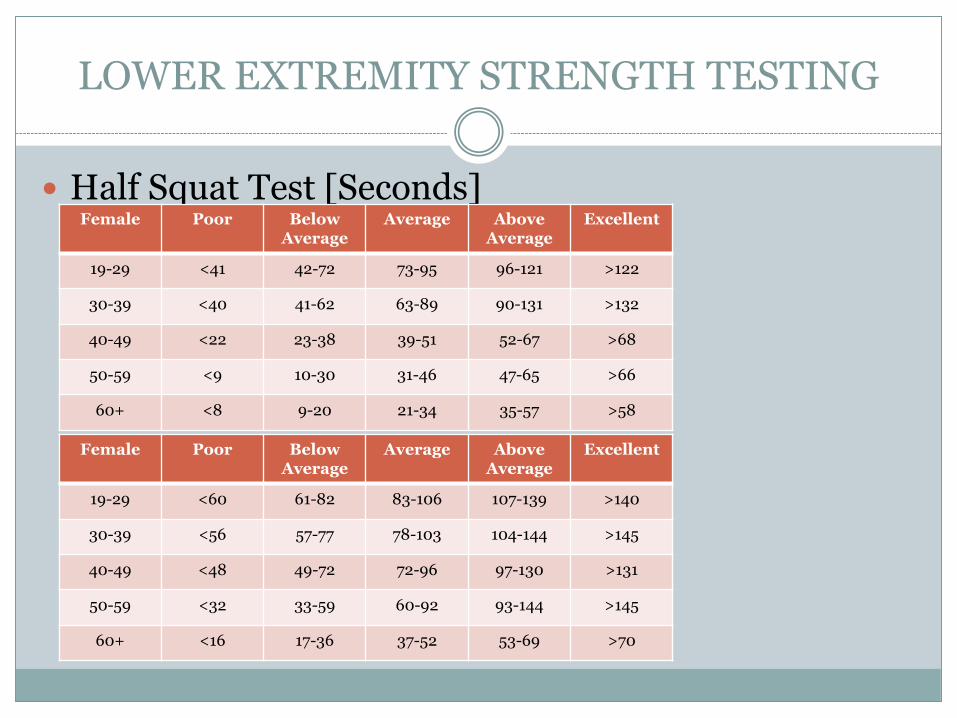
LOWER EXTREMITY STRENGTH TESTING
Half Squat Test [Seconds]Female Poor Below
AverageAverage Above
AverageExcellent
19-29 <41 42-72 73-95 96-121 >122
30-39 <40 41-62 63-89 90-131 >132
40-49 <22 23-38 39-51 52-67 >68
50-59 <9 10-30 31-46 47-65 >66
60+ <8 9-20 21-34 35-57 >58
Female Poor BelowAverage
Average Above Average
Excellent
19-29 <60 61-82 83-106 107-139 >140
30-39 <56 57-77 78-103 104-144 >145
40-49 <48 49-72 72-96 97-130 >131
50-59 <32 33-59 60-92 93-144 >145
60+ <16 17-36 37-52 53-69 >70
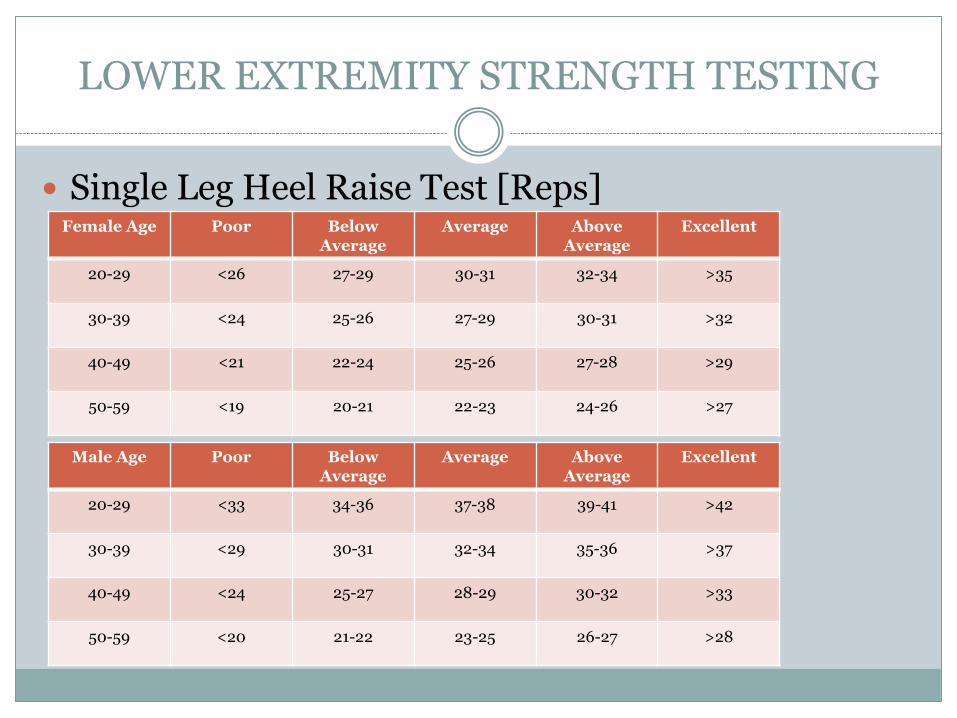
LOWER EXTREMITY STRENGTH TESTING
Single Leg Heel Raise Test [Reps] Female Age Poor Below
AverageAverage Above
AverageExcellent
20-29 <26 27-29 30-31 32-34 >35
30-39 <24 25-26 27-29 30-31 >32
40-49 <21 22-24 25-26 27-28 >29
50-59 <19 20-21 22-23 24-26 >27
Male Age Poor BelowAverage
Average Above Average
Excellent
20-29 <33 34-36 37-38 39-41 >42
30-39 <29 30-31 32-34 35-36 >37
40-49 <24 25-27 28-29 30-32 >33
50-59 <20 21-22 23-25 26-27 >28
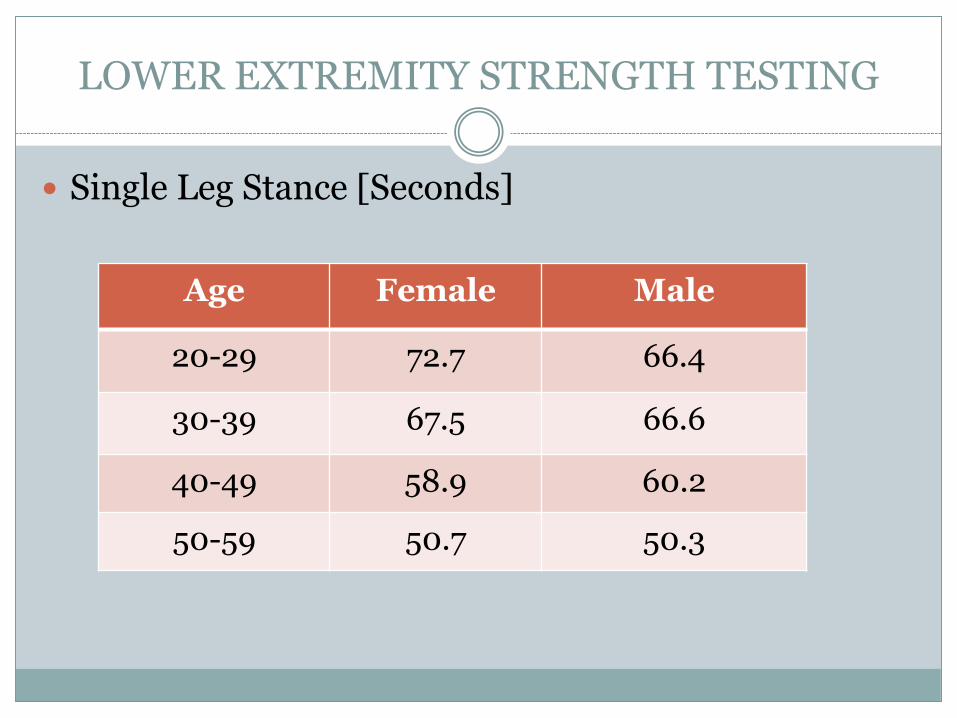
LOWER EXTREMITY STRENGTH TESTING
Single Leg Stance [Seconds]
Age Female Male
20-29 72.7 66.4
30-39 67.5 66.6
40-49 58.9 60.2
50-59 50.7 50.3
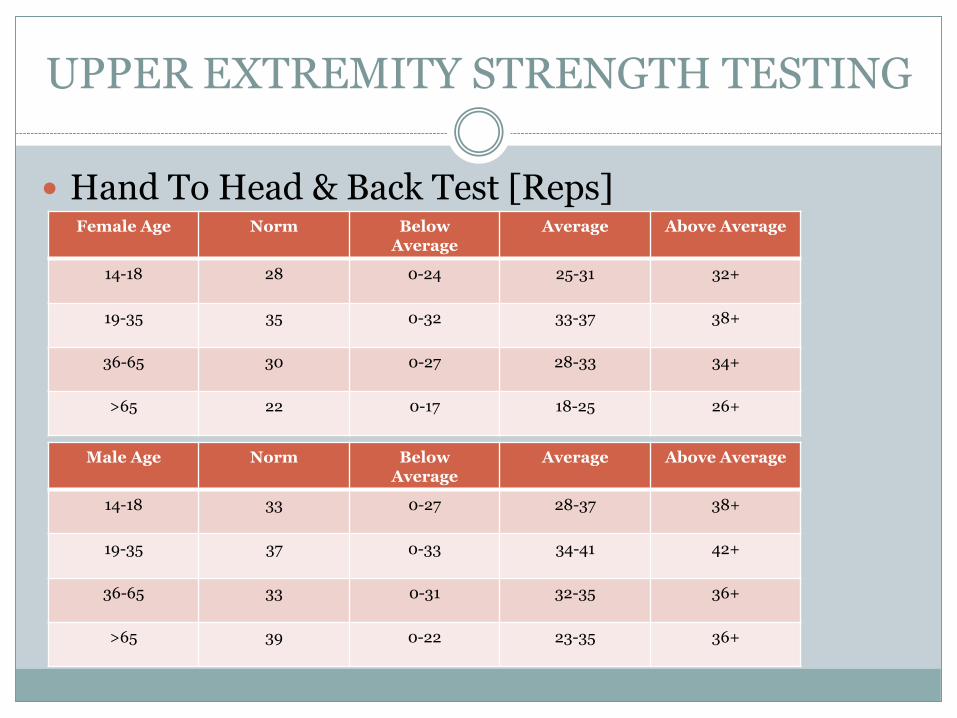
UPPER EXTREMITY STRENGTH TESTING
Hand To Head & Back Test [Reps]Female Age Norm Below
AverageAverage Above Average
14-18 28 0-24 25-31 32+
19-35 35 0-32 33-37 38+
36-65 30 0-27 28-33 34+
>65 22 0-17 18-25 26+
Male Age Norm BelowAverage
Average Above Average
14-18 33 0-27 28-37 38+
19-35 37 0-33 34-41 42+
36-65 33 0-31 32-35 36+
>65 39 0-22 23-35 36+
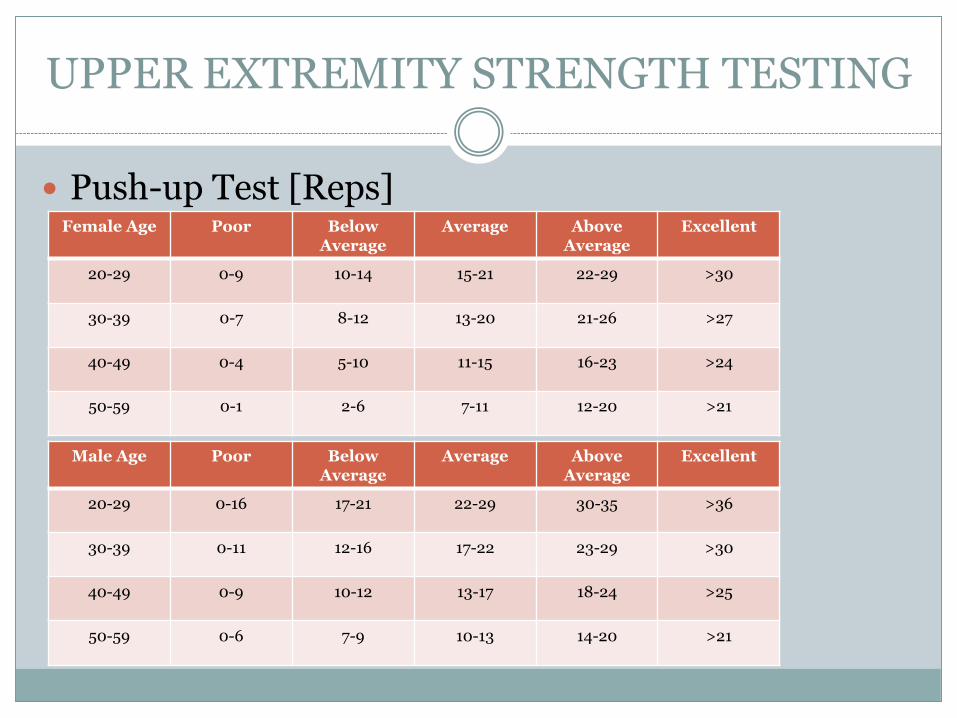
UPPER EXTREMITY STRENGTH TESTING
Push-up Test [Reps] Female Age Poor Below
AverageAverage Above
AverageExcellent
20-29 0-9 10-14 15-21 22-29 >30
30-39 0-7 8-12 13-20 21-26 >27
40-49 0-4 5-10 11-15 16-23 >24
50-59 0-1 2-6 7-11 12-20 >21
Male Age Poor BelowAverage
Average Above Average
Excellent
20-29 0-16 17-21 22-29 30-35 >36
30-39 0-11 12-16 17-22 23-29 >30
40-49 0-9 10-12 13-17 18-24 >25
50-59 0-6 7-9 10-13 14-20 >21
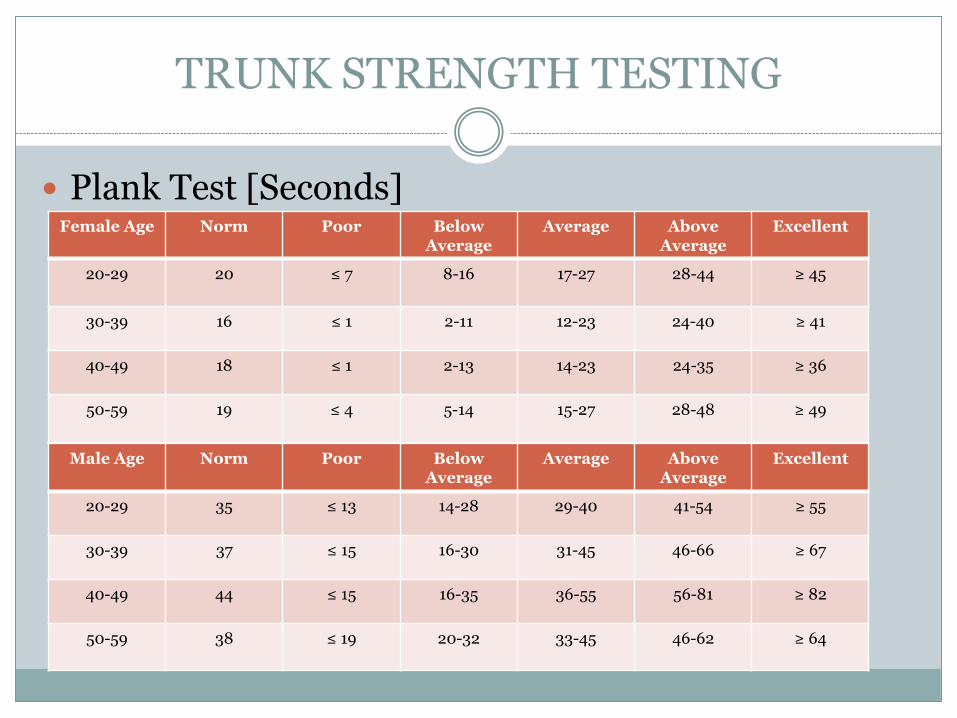
TRUNK STRENGTH TESTING
Plank Test [Seconds]Female Age Norm Poor Below
AverageAverage Above
AverageExcellent
20-29 20 ≤ 7 8-16 17-27 28-44 ≥ 45
30-39 16 ≤ 1 2-11 12-23 24-40 ≥ 41
40-49 18 ≤ 1 2-13 14-23 24-35 ≥ 36
50-59 19 ≤ 4 5-14 15-27 28-48 ≥ 49
Male Age Norm Poor BelowAverage
Average Above Average
Excellent
20-29 35 ≤ 13 14-28 29-40 41-54 ≥ 55
30-39 37 ≤ 15 16-30 31-45 46-66 ≥ 67
40-49 44 ≤ 15 16-35 36-55 56-81 ≥ 82
50-59 38 ≤ 19 20-32 33-45 46-62 ≥ 64
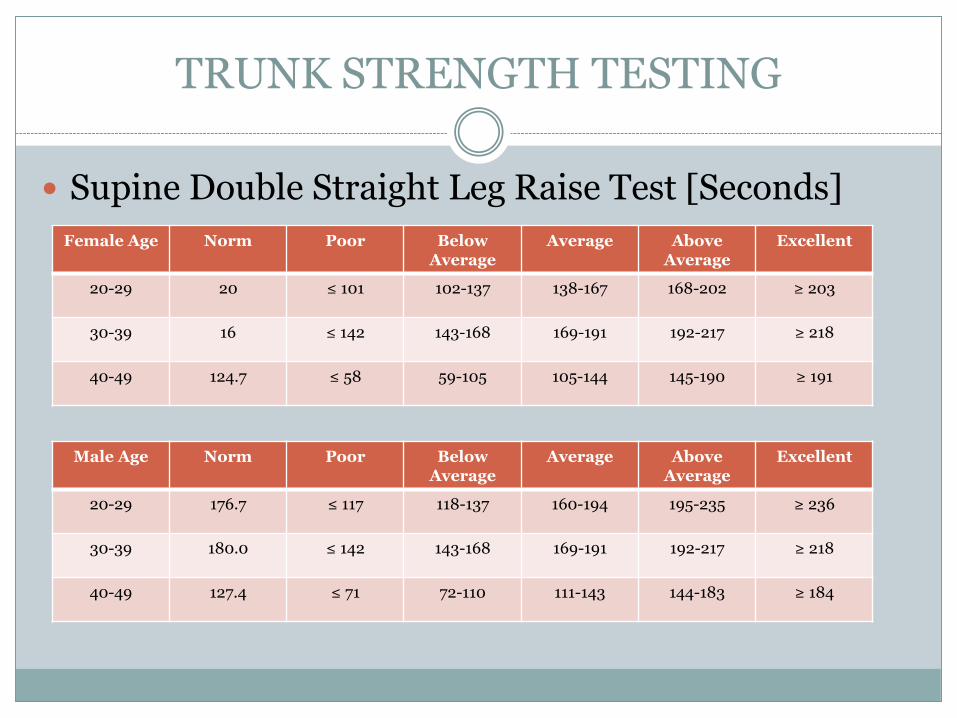
TRUNK STRENGTH TESTING
Supine Double Straight Leg Raise Test [Seconds]
Female Age Norm Poor BelowAverage
Average Above Average
Excellent
20-29 20 ≤ 101 102-137 138-167 168-202 ≥ 203
30-39 16 ≤ 142 143-168 169-191 192-217 ≥ 218
40-49 124.7 ≤ 58 59-105 105-144 145-190 ≥ 191
Male Age Norm Poor BelowAverage
Average Above Average
Excellent
20-29 176.7 ≤ 117 118-137 160-194 195-235 ≥ 236
30-39 180.0 ≤ 142 143-168 169-191 192-217 ≥ 218
40-49 127.4 ≤ 71 72-110 111-143 144-183 ≥ 184
TELEHEALTH KNEE DEMO
- Obtain patient consent, phone number and address in case of emergency
- Subjective History
- Objective Tests
- Assessment
- Plan / Home exercise program
QUESTIONS?
REFERENCES
1. Centers for Medicare and Medicaid Services (CMS). Conditions of Participation (CMS-3819-F) 2018. www.cms.gov
2. Centers for Medicare and Medicaid Services (CMS). Medicare Benefit Policy Manual – Chapter 7: Home Health Services. www.cms.gov
3. American Physical Therapy Association (APTA). Telehealth Resource page,www.apta.org 2020.
4. Health Resources & Services Administration, Telehealth Programsexternal icon.
5. Federation of State Medical Boards,Guidelines for the Structure and Function of a State Medical and Osteopathic Boardpdf icon[PDF – 6/55MB]external icon.
6. Telehealth in Rural Communities. Centers for Disease Control and Prevention. https://www.cdc.gov/chronicdisease/resources/publications/factsheets/telehealth-in-rural-communities.htm. Published August 18, 2020. Accessed October 05, 2021.
7. Getting started with telehealth. Telehealth.HHS.gov. (n.d.). Retrieved October 5, 2021, from https://telehealth.hhs.gov/providers/getting-started/.
8. Norms Ages 3 to 59: McKay MJ, et al. Reference values for developing responsive functional outcome measures across the lifespan. Neurology® 2017;88:1–8
9. Norms Ages 60 to 94. Rikli RE, Jones CJ. Functional fitness normative scores for community residing older adults, ages 60–94. J Aging Phys Act. 1999;7:162–81
10. McIntosh, Greg & L, Wilson & M, Affleck & H, Hall. Trunk and lower extremity muscle endurance: Normative data. Journal of Rehabilitation Outcomes Measurement. 1998;2(4):20-39.
11. K. Hébert-Losier et al. Updated reliability and normative values for the standing heel-rise test in healthy adults. Physiotherapy. 2017 Dec;103(4):446-452. http://dx.doi.org/10.1016/j.physio.2017.03.002
12. K. Hébert-Losier et al. Updated reliability and normative values for the standing heel-rise test in healthy adults. Physiotherapy. 2017 Dec;103(4):446-452. http://dx.doi.org/10.1016/j.physio.2017.03.002
13. Study used 120 Second Cut-Off Times. Kjær et al. Normative values for musculoskeletal and neuromotor fitness in apparently healthy Norwegian adults and the association with obesity: a cross-sectional study. BMC Sports Science, Medicine and Rehabilitation. 2016;8:37.
14. Shah KM, et al. Early Development and Reliability of the Timed Functional Arm and Shoulder Test. J Orthop Sports Phys Ther 2017;47(6):420-431. Epub 3 Mar 2017. doi:10.2519/jospt.2017.7136
15. Canadian Society for Exercise Physiology. The Canadian Physical Activity, Fitness & Lifestyle Approach (CPAFLA): CSEP-Health & Fitness Program’s Health Related Appraisal and Counseling Strategy. 3rd edition. Ottawa (Ontario): Canadian Society for Exercise Physiology; 2003
16. American College of Sports Medicine. ACSM’s Health-Related Physical Assessment Manual, 4th edition. Wolters Kluwer/Lippincott Williams & Wilkins, Baltimore 2014.
17. R.W. Bohannon et al. The prone bridge test: Performance, validity, and reliability among older and younger adults. Journal of Bodywork & Movement Therapies. 2018;(22):385-389.
18. Peterson DD. Proposed Performance Standards for the Plank for Inclusion Consideration Into the Navy's Physical Readiness Test. Strength and Conditioning Journal. 2013;13(5):22-26.
19. McIntosh, Greg & L, Wilson & M, Affleck & H, Hall. Trunk and lower extremity muscle endurance: Normative data. Journal of Rehabilitation Outcomes Measurement. 1998;2(4):20-39.