Embed Size (px)
Citation preview

Utilization Of Lipid-lowering Utilization Of Lipid-lowering Therapy In Hypertensive Therapy In Hypertensive
Patients In The United States Patients In The United States
Simon S.K. Tang, MPH*Sean Candrilli, MS**Lizheng Shi, PhD*
*Department of Health Systems ManagementTulane University School of Public Health & Tropical Medicine;
**RTI Health Solutions
Oral Presentation at 2008 AcademyHealth Annual Research Meeting

BackgroundBackground
Hypertension is the leading risk factor for Cardiovascular Disease (CVD)1
Majority of patients with hypertension have multiple additional CV factors including dyslipidemia2 and are not optimally managed to goals3
Lipid-lowering therapy is effective in reducing CV risk in patients with hypertension:– ASCOT-LLA demonstrated that multiple-risk-factor hypertensive
patients without CAD who received atorvastatin 10mg led to 36% reduction of major CV events vs. placebo4
– CARDS demonstrated that patients with diabetes (with high proportion of hypertension – 84%) who received atorvastatin mg led to
37% reduction of major CV events5 1American Heart Association. Heart disease and stroke statistics – 2006 update. Circulation 2006 113:e85–e151 (available at: http://circ.ahajournals.org)
2Kannel WB. J Hum Hypertens 2000;14:83-90.
3Wong ND, Lopez V, Tang S, et al. Am J Cardiol 2006;98:204-8.
4Sever PS, Dahlöf B, Poulter NR et al. Lancet 2003;361:1149-58.
5Colhoun HM, et al. Lancet 2004;364685-96

ObjectivesObjectives
To understand factors associated with use of lipid-lowering therapy within various hypertenisve populations:– Overall HTN– HTN with Dyslipidemia (DYS)– Treated HTN without CAD (ASCOT-LLA)– HTN with Diabetes– HTN with CHD
To evaluate the extent of lipid-lowering therapy use in various hypertensive populations in the United States

MethodsMethods Design & Population:
– Cross-sectional Survey Analysis– Adult sample aged 20 years from the National Health
and Nutrition Examination Survey (NHANES) 1999-2004 with data on blood pressure and lipids (Overall n=5,403; 52% female) (HTN n=1,928; 52% female)
– HTN defined as:• BP >140/90 mm Hg (or >130/80 mm Hg if DM) • Or on antihypertensive medication
Analysis:– SPSS 15.0 software used for descriptive & SUDAAN for
multivariate analyses– Chi-square statistics used to compare between groups– Multivariate Logistic Regression Analysis was conducted
to assess odds of taking lipid-lowering therapy adjusting for covariates such as: age, gender, ethnicity, CV risk factors & comorbidities, insurance, education

Baseline CharactertisticsBaseline Charactertistics
Demographic, Disease & Demographic, Disease & Socioeconomic groupsSocioeconomic groups
Mean (SD)* or Proportion of subgroup Mean (SD)* or Proportion of subgroup (%)(%)
Hypertension 1928 (100%)
Mean Age* 62.7 years (14.91)*
Male 48%
Non-white minorities 46%
Dyslipidemia 66%
CHD 13%
Diabetes 12%
Smoker/ Obese 15%/ 40%
No health insurance 11%
Less than high school education 13%

0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
40.0%
45.0%
50.0%
Overall HTN HTN-DYS HTN-ASCOT HTN-DM HTN-CHD
Overall
Male
Female
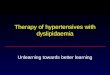
Results - GenderResults - Gender
Proportion (%) of Patients with Hypertension reported taking lipid-lowering therapy
N = 1928 1279 939 224 259

0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
Overall HTN HTN-DYS HTN-ASCOT HTN-DM HTN-CHD
Stroke
Smoker
Obese (BMI>=30)
Results – Stroke & Life-style CV risk Results – Stroke & Life-style CV risk factorsfactors
Proportion (%) of Patients with Hypertension reported taking lipid-lowering therapy
N = 1928 1279 939 224 259

0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
40.0%
45.0%
50.0%
Overall HTN HTN-DYS HTN-ASCOT
HTN-DM HTN-CHD
White
Non-White Minorities
With Insurance
No Insurance
High School or Above
Less than High SchoolEducation
Results – Socio-Cultural FactorsResults – Socio-Cultural Factors
Proportion (%) of Patients with Hypertension reported taking lipid-lowering therapy
N = 1928 1279 939 224 259*Chi-square statistics – all within-group comparisons different at p<0.0001

Summary of Descriptive ResultsSummary of Descriptive Results
Only 23% of Overall HTN patients received LLT
– Primary Prevention: 27% (HTN-ASCOT)– Mixed: 34% (HTN-DYS)– High-Risk/ Secondary Prevention: 38% (HTN-DM), 45%
(HTN-CHD) No major disparities seen between Male & Female LLT treatment is suboptimal in HTN patients with Stroke or other
life-style-related CHD risk factors Significant disparities seen among:
– Ethnic groups:• Greater of proportion of Non-hispanic whites received LLT than
other non-white minorities
– Insured vs. uninsured– High School or Above education vs. below
Disparities gap widen as CV risk increased

Adjusted Odds Ratios of Taking LLT: Adjusted Odds Ratios of Taking LLT: HTN OverallHTN Overall
IndependentVariables and Lower 95% Upper 95%Effects Odds Ratio Limit OR Limit OR-------------------------------------------------------------------------------------Intercept 0.10 0.05 0.18RIDAGEYR 1.02 1.01 1.02MALE 1.09 0.82 1.46DXDIABETES 2.43 1.50 3.94CHF 0.76 0.43 1.34CHD 3.26 2.32 4.58STROKE 1.66 0.89 3.08OBESE 1.03 0.78 1.36CURRENTSMOKER 0.90 0.51 1.59LT_HS 0.51 0.25 1.03NO_INSURANCE 0.62 0.33 1.14NON_WHITE 0.77 0.58 1.02-------------------------------------------------------------------------------------

Adjusted Odds Ratios of Taking LLT: Adjusted Odds Ratios of Taking LLT: HTN-ASCOTHTN-ASCOT
IndependentVariables and Lower 95% Upper 95%Effects Odds Ratio Limit OR Limit OR---------------------------------------------------------------------------------Intercept 0.16 0.07 0.38RIDAGEYR 1.01 1.00 1.03MALE 1.27 0.84 1.92DXDIABETES 1.73 0.95 3.15CHF 0.70 0.18 2.71STROKE 1.61 0.65 3.97OBESE 0.86 0.61 1.22CURRENTSMOKER 0.83 0.39 1.78LT_HS 0.51 0.22 1.19NO_INSURANCE 0.85 0.42 1.71NON_WHITE 0.96 0.65 1.42--------------------------------------------------------------------------------

Adjusted Odds Ratios of Taking LLT: Adjusted Odds Ratios of Taking LLT: HTN with DiabetesHTN with Diabetes
IndependentVariables and Lower 95% Upper 95%Effects Odds Ratio Limit OR Limit OR------------------------------------------------------------------------------Intercept 0.63 0.04 9.14RIDAGEYR 1.01 0.97 1.04MALE 0.70 0.30 1.60CHF 3.71 0.78 17.70CHD 1.78 0.63 5.02STROKE 1.09 0.38 3.13OBESE 0.54 0.24 1.19CURRENTSMOKER 0.73 0.27 1.94LT_HS 0.12 0.03 0.44NO_INSURANCE 0.94 0.19 4.58NON_WHITE 1.64 0.70 3.84------------------------------------------------------------------------------

Adjusted Odds Ratios of Taking LLT: Adjusted Odds Ratios of Taking LLT: HTN with CHDHTN with CHD
IndependentVariables and Lower 95% Upper 95%Effects Odds Ratio Limit OR Limit OR-------------------------------------------------------------------------------------Intercept 16.34 0.97 276.36RIDAGEYR 0.96 0.93 1.00MALE 0.91 0.50 1.69DXDIABETES 2.35 0.88 6.27CHF 0.84 0.45 1.56STROKE 1.32 0.52 3.34OBESE 0.66 0.31 1.41CURRENTSMOKER 1.04 0.48 2.25LT_HS 0.30 0.06 1.53NO_INSURANCE 0.14 0.02 0.84NON_WHITE 0.47 0.18 1.18-------------------------------------------------------------------------------------

Summary – Multivariate ResultsSummary – Multivariate Results
Overall HTN:– Age and CHD/DM comorbidities are significant factors
associated with likelihood of receiving LLT HTN ASCOT:
– Significant factors include Age HTN with Diabetes
– Significant factors include LTHS HTN with CHD
– Significant factors include No insurance

LimitationsLimitations
Associations can not imply specific causal/directional effects due to cross-sectional design
Self-reported nature of data– Disease conditions and medication use
Medication dose and treatment patterns are unknown
Adherence to medications is unknown Not all factors are accounted for in this
analysis

ConclusionsConclusions
Lipid-Lowering Therapy are not optimally used in overall & high-risk HTN populations in the US
Age, Diabetes and CHD are associated with higher LLT use in overall HTN
Less than high school education is associated with underutilization of LLT among HTN patients with Diabetes
Lack of insurance is associated with underutilization of LLT among HTN patients with CHD
Many variables become non-significant in multivariate analyses
Future analyses should leverage longitudinal databases

Significance & Policy ImplicationsSignificance & Policy Implications
Improve understanding of opportunities in aggressive LLT management of cardiovascular risk
Contribute to development of quality indicators for specific high-risk or vulnerable populations