Embed Size (px)
Citation preview

Utility of transesophageal echocardiography in the examination of adult patients with patent ductus arteriosus
Alejandra Andrade, MD, Jesus Vargas-Barron, MD, Mar ia Rij laarsdam, MD,
Angel Romero-Cardenas , MD, Candace Keirns, MD, and Nilda Espinola, MD Mexico City, Mexico
Thirteen patients with clinical suspicion of patent ductus ar- teriosus were evaluated by transthoracic and transesoph- ageal echocardiographic studies. Findings were corrobo- rated during corrective surgery in 8 patients and by cardiac catheterization in 5. Transthoracic echocardiography con- firmed the diagnosis in 7 patients; in 2 of the patients endar- teritis of the pulmonary artery was demonstrated, and in one infective vegetations in aortic and mitral valves. With trans- esophageal echocardiography, patent ductus arteriosus was established in all 8 patients and endarteritis of the pul- monary artery was shown in 3, including I not discovered by transthoracic technique. In 1 of these patients, vegetations were also found on the pulmonic valve. Both techniques demonstrated significant pulmonary hypertension in 5 cases; contrast studies showed the venoarterial shunt between the pulmonary artery and the aorta with particular clarity in transesophageal images. On the basis of these findings it may be concluded that transesophageal echo- cardiography complements the information provided by transthoracic recordings in adult patients with patent ductus arteriosus, especially when it is associated with pulmonary hypertension or pulmonary endarteritis. (AM HEART J 1995;130:543-6.)
In newborns and infants , direct visual izat ion of a pa t en t ductus ar ter iosus (PDA) is usual ly successful wi th conventional t rans thorac ic echocardiography (TTE) and color coded Doppler. However , in adul ts TTE can fail to obtain diagnostic informat ion be- cause the ductus m a y be located far f rom a t rans- ducer on the chest wall. Transesophagea l echocardi- ography (TEE), par t icu lar ly wi th biplane or multi- p lane t ransducers , has increased the informat ion available in the examina t ion o f in t racard iac diseases
From the Department of Echocardiography, Instituto Nacional de Cardio- logia ]gnacio Chavez.
Received for publication Dec. 19, 1994; accepted March 1, 1995.
Reprint requests: Jesus Vargas-Barron, MD, Department of Echocardiog- raphy, Instituto Nacional de Cardiologia Ignacio Chavez, Juan Badiano No. 1, 14080 Mexico , D.F., Mexico.
CoPyrigl~t © 1995 by Mosby-Year Book, Inc. 0002-~703/95/$3.00 + 0 4/1/65038
and those of the grea t ar ter ies . The purpose of this s tudy was to compare the diagnostic ut i l i ty of TTE and b ip lanar T E E in adolescent and adul t pa t ien ts wi th PDA.
METHODS
Thirteen patients with a clinical diagnosis of PDA were examined. The 11 women and 2 men ranged in age from 16 to 55 years (average 29 years). In five cases the diagnosis was corroborated by cardiac catheterization performed to evaluate pulmonary resistance when pulmonary hyper- tension was present. In the remaining patients diagnosis was confirmed during the surgical closure of the ductus arteriosus.
Conventional TTE was practiced on all patients. TEE was performed to identify associated defects and/or the cause of pulmonary hypertension or because the informa- tion obtained from the conventional transthoracic study was incomplete. The transesophageal exploration was performed with local oropharyngeal anesthesia with 2% xylocaine: A 5 MHz biplane transducer was used. Trans- gastric and transesophageal transverse and longitudinal plane images were obtained. Blood flow in the four cardiac chambers, great arteries, and systemic and pulmonary venous return were analyzed with Doppler. PDA was es- tablished by using images in a longitudinal plane with the aortic recording at a level distal to the ductus. After this recording the transducer was slowly withdrawn and slightly rotated to the right to obtain images of progres- sively higher sections. The shunt between aorta and pul- monary artery was corroborated with color-coded Doppler. Spectral analysis of the pulmonary flow showed increased velocity both in systole and diastole.
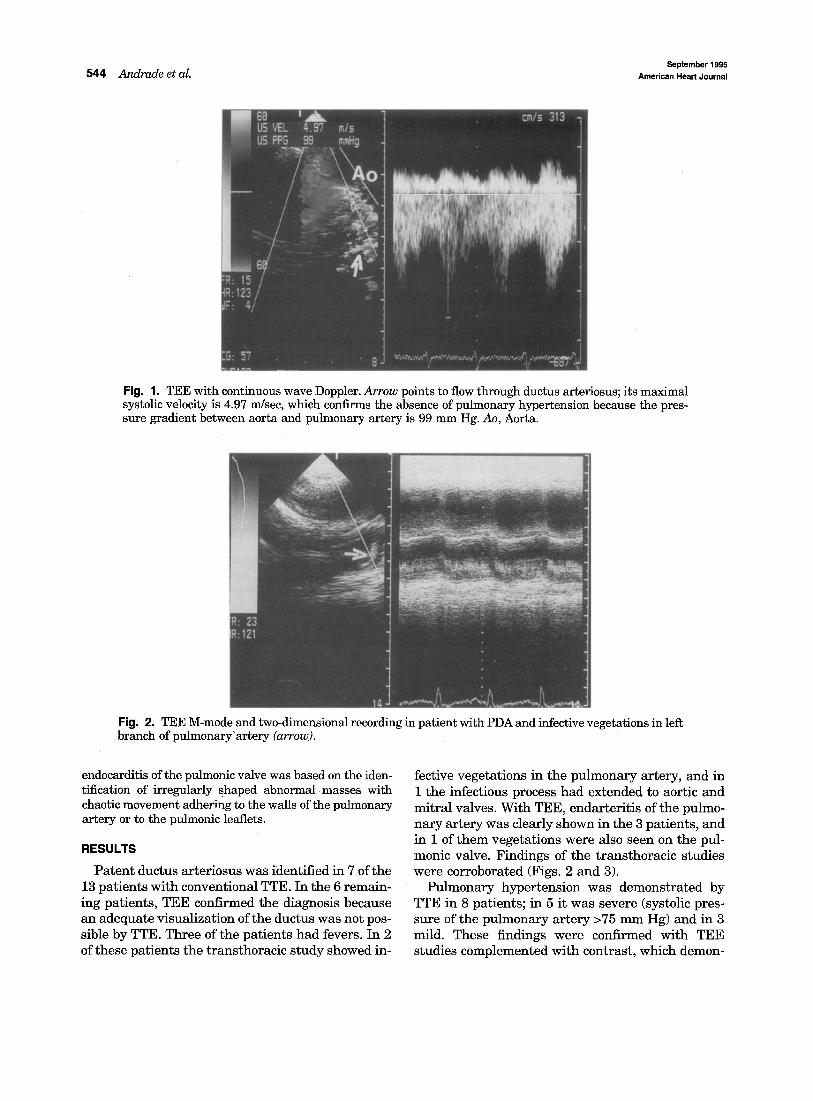
The calculation of systolic pressure in the pulmonary artery was performed with TTE on the basis of the deter- mination of the maximal velocity of tricuspid regurgitant flow. Quantification of pulmonary arterial systolic pres- sure was also obtained from TEE studies by aligning the ultrasound beam in the direction of the ductus itself; the difference between aortic systolic pressure and the gradi- ent across the ductus corresponded to the systolic pressure in the pulmonary artery (Fig. 1).
Diagnosis of endarteritis of the pulmonary artery and
543
September 1995 544 Andrade et al. American Heart Journal
Fig. 1. TEE with continuous wave Doppler. Arrow points to flow through ductus arteriosus; its maximal systolic velocity is 4.97 m/sec, which confirms the absence of pulmonary hypertension because the pres- sure gradient between aorta and pulmonary artery is 99 mm Hg. Ao, Aorta.
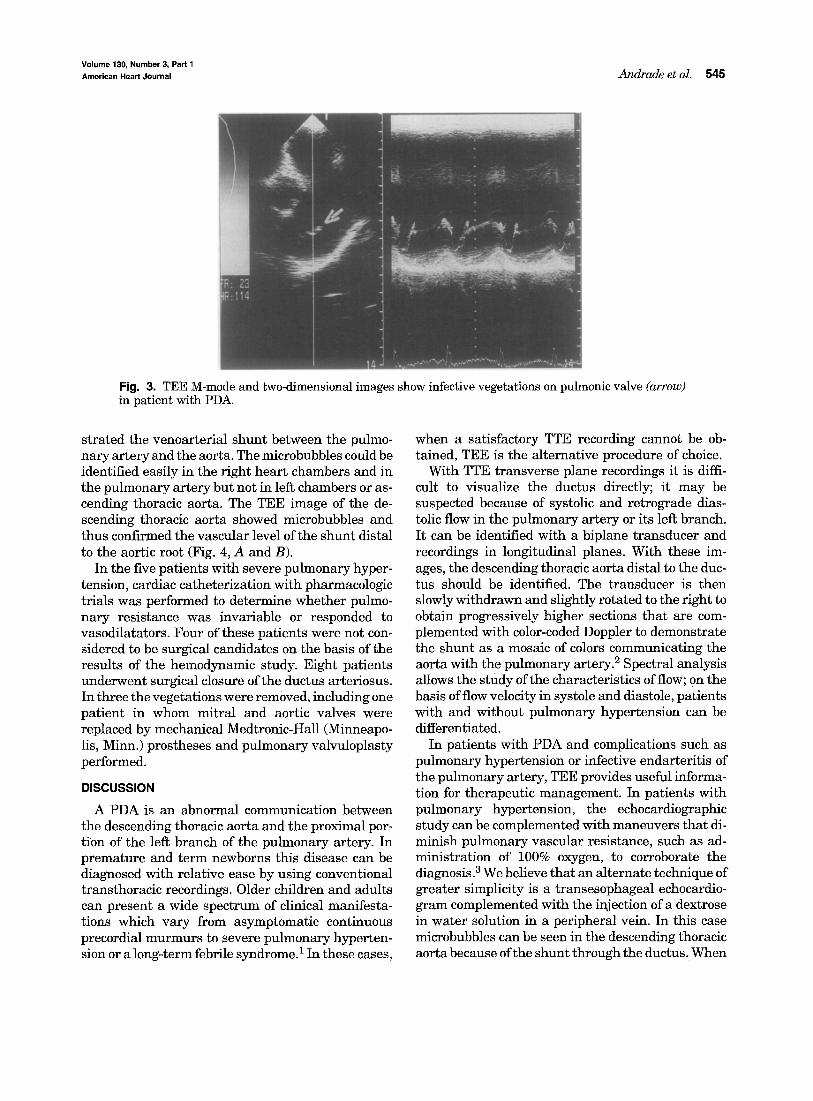
Fig. 2. TEE M-mode and two-dimensional recording in patient with PDA and infective vegetations in left branch of pulmonary'artery (arrow).
endocarditis of the pulmonic valve was based on the iden- tification of irregularly shaped abnormal masses with chaotic movement adhering to the walls of the pulmonary artery or to the pulmonic leaflets.
R E S U L T S
Patent ductus arteriosus was identified in 7 of the 13 patients with conventional TTE. In the 6 remain- ing patients, TEE confirmed the diagnosis because an adequate visualization of the ductus was not pos- sible by TTE. Three of the patients had fevers. In 2 of these patients the transthoracic study showed in-
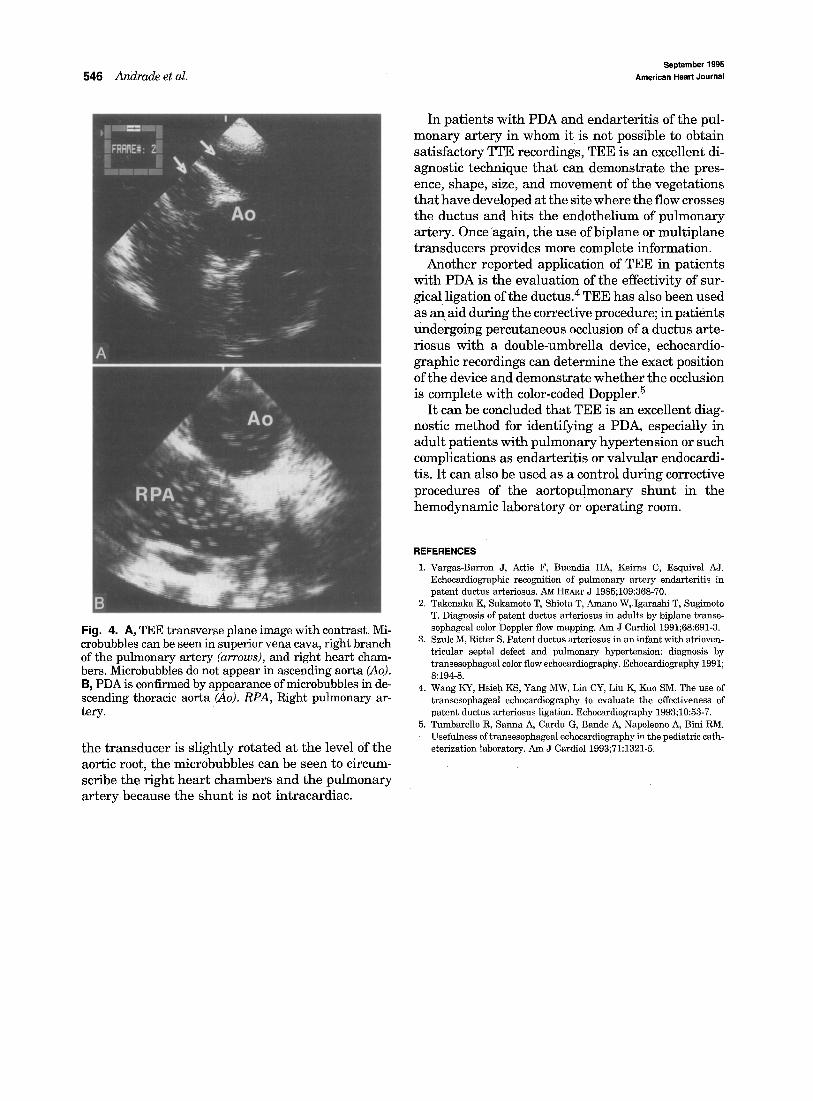
fective vegetations in the pulmonary artery, and in 1 the infectious process had extended to aortic and mitral valves. With TEE, endarteritis of the pulmo- nary artery was Clearly shown in the 3 patients, and in 1 of them vegetations were also seen on the pul- monic valve. Findings of the transthoracic studies were corroborated (Figs. 2 and 3).
Pulmonary hypertension was demonstrated by TTE in 8 patients; in 5 it was severe (systolic pres- sure of the pulmonary artery >75 mm Hg) and in 3 mild. These findings were confirmed with TEE studies complemented with contrast, which demon-
Volume 130, Number 3, Part 1
American Heart Journal Andrade et al. 545
Fig. 3. TEE M-mode and two-dimensional images show infective vegetations on pulmonic valve (arrow) in patient with PDA.
strated the venoarterial shunt between the pulmo- nary artery and the aorta. The microbubbles could be identified easily in the right heart chambers and in the pulmonary artery but not in left chambers or as- cending thoracic aorta. The TEE image of the de- scending thoracic aorta showed microbubbles and thus confirmed the vascular level of the shunt distal to the aortic root (Fig. 4, A and B).
In the five patients with severe pulmonary hyper- tension, cardiac catheterization with pharmacologic trials was performed to determine whether pulmo- nary resistance was invariable or responded to vasodilatators. Four of these patients were not con- sidered to be surgical candidates on the basis of the results of the hemodynamic study. Eight patients underwent surgical closure of the ductus arteriosus. In three the vegetations were removed, including one patient in whom mitral and aortic valves were replaced by mechanical Medtronic-Hall (Minneapo- lis, Minn.) prostheses and pulmonary valvuloplasty performed.
DISCUSSION
A PDA is an abnormal communication between the descending thoracic aorta and the proximal por- tion of the left branch of the pulmonary artery. In premature and term newborns this disease can be diagnosed with relative ease by using conventional transthoracic recordings. Older children and adults can present a wide spectrum of clinical manifesta- tions which vary from asymptomatic continuous precordial murmurs to severe pulmonary hyperten- sion or a long-term febrile syndrome.1 In these cases,
when a satisfactory TTE recording cannot be ob- tained, TEE is the alternative procedure of choice.
With TTE transverse plane recordings it is diffi- cult to visualize the ductus directly; it may be suspected because of systolic and retrograde dias- tolic flow in the pulmonary artery or its left branch. It can be identified with a biplane transducer and recordings in longitudinal planes. With these im- ages, the descending thoracic aorta distal to the duc- tus should be identified. The transducer is then slowly withdrawn and slightly rotated to the right to obtain progressively higher sections that are com- plemented with color-coded Doppler to demonstrate the shunt as a mosaic of colors communicating the aorta with the pulmonary artery. 2 Spectral analysis allows the study of the characteristics of flow; on the basis of flow velocity in systole and diastole, patients with and without pulmonary hypertension can be differentiated.
In patients with PDA and complications such as pulmonary hypertension or infective endarteritis of the pulmonary artery, TEE provides useful informa- tion for therapeutic management. In patients with pulmonary hypertension, the echocardiographic study can be complemented with maneuvers that di- minish pulmonary vascular resistance, such as ad- ministration of 100% oxygen, to corroborate the diagnosis. 3 We believe that an alternate technique of greater simplicity is a transesophageal echocardio- gram complemented with the injection of a dextrose in water solution in a peripheral vein. In this case microbubbles can be seen in the descending thoracic aorta because of the shunt through the ductus. When
September 1995 546 Andrade et al. American Heart Journal
In patients with PDA and endarteritis of the pul- monary artery in whom it is not possible to obtain satisfactory TTE recordings, TEE is an excellent di- agnostic technique that can demonstrate the pres- ence, shape, size, and movement of the vegetations that have developed at the site where the flow crosses the ductus and hits the endothelium of pulmonary artery. Once again, the use of biplane or multiplane transducers provides more complete information.
Another reported application of TEE in patients with PDA is the evaluation of the effectivity of sur- gical ligation of the ductus~ 4 TEE has also been used as an aid during the corrective procedure; in patients undergoing percutaneous occlusion of a ductus arte- riosus with a double-umbrella device, echocardio- graphic recordings can determine the exact position of the device and demonstrate whether the occlusion is complete with color-coded Doppler. 5
It can be concluded that TEE is an excellent diag- nostic method for identifying a PDA, especially in adult patients with pulmonary hypertension or such complications as endarteritis or valvular endocardi- tis. It can also be used as a control during corrective procedures of the aortopulmonary shunt in the hemodynamic laboratory or operating room.
Fig. 4. A, TEE transverse plane image with contrast. Mi- crobubbles can be seen in superior vena cava, right branch of the pulmonary artery (arrows), and right heart cham- bers. Microbubbles do not appear in ascending aorta (Ao). B, PDA is confirmed by appearance of microbubbles in de- scending thoracic aorta (Ao). RPA, Right pulmonary ar- tery.
the transducer is slightly rotated at the level Of the aortic root, the microbubbles can be seen to circum- scribe the right heart chambers and the pulmonary artery because the shunt is not intracardiac.
REFERENCES
1. Vargas-Barron J, Attie F, Buendia HA, Keirns C, Esquivel AJ. Echocardiographic recognition of pulmonary artery endarteritis in patent ductus arteriosus. AM HEART J 1985;109:368-70.
2. Takenaka K, Sakamoto T, Shiota T, Amano W, Igarashi T, Sugimoto T. Diagnosis of patent ductus arteriosus in adults by biplane transe- sophageal color Doppler flow mapping. Am J Cardiol 1991;68:691-3.
3. Szulc M, Ritter S. Patent ductus arteriosus in an infant with atrioven- tricular septal defect and pulmonary hypertension: diagnosis by transesophageal color flow echocardiography. Echocardiography 1991; 8:194-8.
4. Wang KY, Hsieh KS, Yang MW, Lin CY, Liu K, Kuo SM. The use of transesophageal echocardiography to evaluate the effectiveness of patent ductus arteriosus ligation. Echocardiography 1993;10:53-7.
5. Tumbarello R, Sanna A, Cardu G, Bande A, Napoleone A, Bini RM. Usefulness of transesophageal echocardiography in the pediatric cath- eterization laboratory. Am J Cardiol 1993;71:1321-5.