-
nts
Faculty of Health and Social Care, Peel House Campus, University
of Salford, Albert Street,
environment in which learning occurs. It demonstrates how a UK
pre-registrationnursing student engaged on a problem-based learning
curriculum supported by avisionary mentor was able to combine
aspects of critical thinking, problem solvingand evidence based
practice to enhance care delivery.c 2005 Elsevier Ltd. All rights
reserved.
Problem-basedlearning;Childrens
orthopaedic;Nursing;Mentorship;
Editors comment
practice setting. needs will be supported by appropriate
membersof the inter-disciplinary team.
The joint publication from the Department ofHealth and The
English National Board reinforcedthe necessity for collaborative
working partnerships
1361-3111/$ - see front matter c 2005 Elsevier Ltd. All rights
reserved.doi:10.1016/j.joon.2005.07.003
* Tel.: +44 161 295 2774; fax: +44 161 295 2963.E-mail address:
[email protected].
Journal of Orthopaedic Nursing (2005) 9, 127133
Journal ofOrthopaedic NursingBackground
Learning for pre-registration student nurses occurswithin a
complex environment, which has both aca-demic and clinical
components. The academiccomponent provides nurses with the
educationalcontent, which supports learning within the clinical
The clinical learning environment is an integralcomponent of any
nurse education and trainingcurriculum. These clinical placements
must complywith guidelines Placements in Focus (ENB/DOH2001) and
facilitate the learning needs of studentsaccessing the placement.
Pre-registration studentshave an expectation that their identified
learningPersonal and professional development is central to life
long learning for nurses and health care professionals generally.
This casestudy explores some of the issues using a pre-registration
nursing students experience in the childrens orthopaedic setting.
PDInformation technologyManchester M30 ONN, UK
Summary This paper focuses on a single case study to unravel the
complex careKEYWORDSBernadette Burns MA, BEd (Hons), RGN, RSCN,
ONC, Lecturer in Nursing *Utilising information techproblem-based
learning sresolve practice dilemmaorthopaedic settingology
andrategies toin a childrens
www.elsevierhealth.com/journals/joon
-
to be enhanced between Higher Education Institutes
Pre-registration nursing students require supportfrom clinical
mentors who have undergone formal
of key skills taught in the classroom to enhance the
of care delivery.
to the pelvic fractures (Dandy and Edwards, 1998).
128 B. Burnseducation and training for the role and
understandhow the curriculum outcomes can be achieved inthe
clinical practice setting. A variety of factorsimpact on clinical
learning experiences, these in-clude the nursementor relationship,
ease of ac-cess to educational support systems, sensitivelyplanned
duty rotas, staff student ratios, workloadbalance and many more
factors. However, fromthe students perspective access to quality
mentorsupport is fundamental to the successful achieve-ment of
practice-based outcomes (Koh, 2002; Pappet al., 2003). The
importance of this studentmen-tor relationship will be discussed
through the pre-sentation of a case study.
The student had commenced the final place-ment in the third year
of training having completeda theoretical module, which focused on
childrenwith complex care needs; it was the second weekin clinical
practice. Action plans identified theneed to manage the care of a
child with complexcare needs and be involved in clinical decision
mak-ing activities surrounding all aspects of care deliv-ery. These
action plans were closely linked to thestudents academic
assignment. Nicklin and Wilson(2000) identify that action plans
form part of a sup-portive learning relationship allowing
learningopportunities to be maximised and encouragingstudents to
take ownership of problems, whilstreceiving supportive facilitation
from their mentor.
Theory underpinning curriculumdelivery
The theoretical model underpinning the nursingcurriculum was
Benners (1984) novice to expertmodel. Students commencing
nurse-training movefrom novice in their first year, through the
ad-vanced beginner stage and in the third year movetowards
achieving competence. The philosophy ofproblem-based learning (PBL)
supported the deliv-ery of curriculum content and enabled the
transferand National Health Service Trusts (UKCC, 1996;UKCC, 1999).
These organizations were required towork harmoniously ensuring
student nurses in train-ing were fit for purpose and practice. This
was to beachieved through a variety of mechanisms
includingeffective mentor preparation, reinforcing the needfor
evidence based practice and enhancing the roleof clinical and
educational audit. These elementswere aimed at improving the
quality of studentsclinical learning and ultimately improving the
qual-ity of care delivered to the client.Personal and professional
development
The student undertook a re-assessment of the childsneeds at the
request of the mentor, which would as-sist in meeting the outcomes
identified within theaction plan. The case-notes indicated that
theorthopaedic consultant had conducted a medicalexamination and
reviewed the X-rays. The cervicalspine was intact and the cervical
collar could be re-moved. The pelvic fractures were not
infiltratingbladder structures and there was no risk of
peritoni-tis. The catheter was to be removed to minimise therisks
associated with long term catheterisation.
Whilst conducting the client re-assessment thestudent was
uncertain of the names of the bonesthat formed the pelvic girdle
and requested clarifi-cation from the clinical mentor. This proved
to bethe start of a learning journey for both student andCase
study
The care setting was a childrens orthopaedic ward.The client was
a female adolescent involved in aserious road traffic accident in
Europe and flownhome to England by air ambulance three days
follow-ing the accident. Injuries sustained included un-displaced
fracture of the left pubic ramus and ashear fracture of the left
ala bone of the pelvis. Onarrival on the ward a soft cervical
collar was evidentand a Foley catheter had been inserted as part of
theemergency care received, but also to assist in thechilds comfort
throughout the air journey. Pughsskin traction had been applied to
provide stabilitypractice learning. Glen and Wilkie (2000)
definePBL as a student centred process, which encour-ages
independent learning and allows students toidentify gaps in their
understanding of relevantclinical problems.
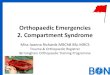
PBL was facilitated via The Onion Model (Darvilland McLoughlin,
2001) where care delivery is di-vided into four domains:
Personal and professional development; Care delivery; Care
management; Professional and ethical.
The inner circles of the model (Fig. 1) ensure theholistic needs
of the client are addressed includingpsychosocial, spiritual,
cultural and physiological.This model was used to unravel the
complexities
-
Onion model.
Utilising information technology and problem-based learning
strategies 129mentor. Ward based text-books identified the
loca-tion of the superior and inferior Pubic Rami but didnot
identify the location of the ala bone (Dandy andEdwards, 1998) and
the mentor acknowledgeduncertainty re the location of this
bone.
Nolan (1998) found that students who feel re-garded as part of
the nursing care team; give anadded bonus to the learning
environment addingto the body of professional knowledge. The
studentwas encouraged to utilise the information technol-ogy skills
developed within the university and ac-cessed the ward computer to
search forinformation surrounding the location of the ala
Figure 1(Oakey and Doyle, 2000). Furthermore, the avail-ability
of upto date resources materials and accessto the Internet are
essential tools in the mainte-nance of a quality learning
environment (QualityAssurance Agency, 2001).
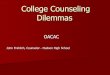
Using Ask Jeeves (www.ask.co.uk) as a quicksearch engine and
using ala bone as the keywords,information was retrieved on the
location of thebone. The ala is a small bone which provides
stabil-ity to the posterior pelvis by attachment to
spinalvertebrae. Furthermore, the ala ligament runsfrom the
posterior pelvis to the base of the skulladding further support to
the pelvis (www.photo-search.com2004). This diagram was subject
tocopyright and the student printed off a differ-ent version from
the university home
page(www.isd.salford.ac.uk/resources/eresources/int-eractivehip2004)
(Fig. 2) and added this to wardbased resource. Academics may argue
that web-sites such as Ask Jeeves do not always produce ac-cess to
quality resource materials but as an initialsearch engine it gave a
prompt answer. The seniorradiographer was contacted, and
interpreted thepelvic X-rays providing the student with a copy
ofthe X-rays to label and use as a teaching aid. Anexample of an
X-ray demonstrating fractures of LPubic Rami was downloaded from
(http://www.trauma.org/cases/classic001.html).
Armed with this new information an in-depth pa-tient
re-assessment was undertaken utilising anadaptation of the Roper
Logan and Tierney Modelof Nursing (Roper et al., 1990). The
problems wereidentified as:
Figure 2 The ala bone.
-
Inability to ambulate (mobilising) due to a frac-
bly some local damage to the pudendal nerve.Uncertain of the
location of this nerve the Internet
to be based on custom and practice rather than evi-dence.
Sackett et al. (1996) discusses the increasingemphasis placed on
evidence based healthcare andhow healthcare professionals need to
analyse theavailable evidence. The student focused on thedecision
making processes that had influenced caredelivery. An online
article by Muir (2004) enhancedknowledge in this area. Muir cites
Carroll and John-sons (1990) information processing model and
theseven stages of temporal decision-making wereused to review
clinical decision-making:
1. Recognition of the situation2. Formulation of explanation3.
Generation of other ideas4. Information gathering5. Making
judgements
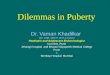
130 B. Burnsonce again proved a valuable resource for
obtainingphysiological diagrams (www.gmedmedia/web-lec01/lec24,
1999) (Fig. 3).
A neurology textbook identified that the puden-dal nerve is
occasionally damaged in pelvic frac-tures and can initiate sensory
pain in theperineum region (Gilroy, 2000). The nerve routepassed
close to the fracture sites and pressure onthe nerve was increased
during bedpan use. The in-ter-disciplinary team had been targeting
pain med-ications to relieve bone pain rather than nerve painand
the pain management plan was revised to takeaccount of the complex
nature of the pain.tured pelvis. Communicating about the management
of painassociated with the fractures and the anxietysurrounding the
accident itself.
Problems related to eliminating focused on theunwillingness to
use bedpans because of pain.
Nutrition (eating and drinking) problems focusedon ensuring
sufficient dietary intake of foodsthat would aid bone healing.
All of these problems were interdependent andPBL strategies were
used to address professionaldevelopment issues in the clinical
setting.
Care management
Issues surrounding eliminating identified severalfactors
requiring clarification. Since the removalof the Foley catheter and
removal of the skin trac-tion on day four, the childs pain had
worsened. Thiswas verified through review of the medicine
admin-istration sheet and the pain assessment chart. Painhad been
scored at a maximum four on the adaptedWong and Baker faces scale
(Day and Jonas, 1998)and dispensing of pain medication increased
follow-ing the use of bedpans. The child complained of ashooting
pain, originating in her left groin and trav-elling into her hip
each time a bedpan was used.
Several issues required addressing and the prob-lem posed by the
student to the mentor was: Is theconstant raising of the pelvis
during the insertion ofbedpan destabilising the fracture site. The
studenthypothesized that a contributing factor associatedwith the
enhanced pain experience surroundedthe removal of Pughs traction
which had providedsome limited stabilisation to the pelvis when
usingbedpans. The mentor encouraged the student toseek answers to
these questions. The consultantwas the expert and explained that
there was possi-Gabapentin was introduced, which has a
positiveeffect on neuropathic pain. The mentor had com-pleted a
paediatric pain module studying the useof Gabapentin in the
orthopaedic setting and pro-vided articles (McClain and Ennevor,
2000; Harden,1999). These authors identify that the mechanismsthat
generate neuropathic pain are varied andcomplex, but are frequently
associated with crushor compression injuries similar to those
experi-enced in road traffic accidents. Wilder et al.(1992)
acknowledges that there is often a psycho-genic component to
neuropathic pain when experi-enced by children.
The student accessed the Internet to enhanceknowledge
surrounding neuropathic pain in chil-dren. University education had
informed the stu-dents learning surrounding levels of evidence,
andthe expert opinion of the consultant, the mentorand the lead
pain nurse proved valuable resources(Tarling and Croft, 2002). The
student raised con-cerns with the mentor that care delivery
appeared
Figure 3 Proximal course of the pudendal nerve 1988.
-
6. Hypothesize: Take action the job which include ward
management, care
the understanding that holistic assessment is thecornerstone of
quality in care delivery. The mentor
Utilising information technology and problem-based learning
strategies 1317. Dissemination
The decision to remove the Foley catheter hadplayed a crucial
role in the enhanced pain experi-ence and this decision was not
taken using a riskversus benefit approach.
The risks were perceived as the development ofa urinary tract
infection as evidenced by the liter-ature surrounding long term
indwelling catheters(Simpson, 2001). This corresponds to the
recogni-tion stage of Carroll and Johnsons model. How-ever, the
benefits of retaining the catheter hadnot been explored or
discussed with the child. Withimproved knowledge of the
underpinning physiol-ogy it was argued that if the catheter had
remainedin place then the pain associated with bedpanusage could be
minimised until the fracture wassticky, around day ten. These
actions supportedby good hygiene standards could reduce the riskof
acquired urinary tract infection, formulationand generation.
Information gained from reliabledatabase sources had provided
insight into the is-sues influencing care delivery, information
gather-ing. The mentor acknowledged that the acquisitionand
utilisation of Web based literature did not formpart of her key
priorities. However, working collab-oratively with the student had
allowed the mentorto develop key skills in the area of database
search-ing. Papp et al. (2003) explored how students learnin the
clinical environment and found the moresupportive the relationship
between student andmentor the more learning is enhanced.
The student raised many valid questions whichthe mentor alone
was unable to answer. Chowand Suen (2001) evaluated student nurses
learningexperiences in the clinical environment and whendiscussing
the role of mentors as advisors andguides, students identified that
some mentors weretask orientated and had a mind-set of sticking
toward routine. The mentor acknowledged that itwas routine practice
to remove bladder catheterswhen no underlying bladder pathology was
evident;however no clinical guidelines were available tosupport
these actions, which caused the mentorto reflect on the knowledge
base from which theyoperated, making judgements. The mentor hadbeen
qualified for 7 years and successfully com-pleted a teaching and
assessing in clinical practicecourse five years previously. Indeed
the mentoridentified that the questioning of decision makingin
clinical practice did not figure as a key compo-nent of the
pre-registration curriculum at that time(Nicklin and Wilson,
2000).
The clinical mentors role is complex and has tocompete with a
variety of other responsibilities ofallowed the student to
undertake a comprehensivereview of care which resulted in improved
under-standing of the origins of the childs problems.
Thissupportive and facilitative role allowed the studentthe
opportunity to access the evidence to supporther clinical decision
making. These actions supportfindings from Spouses (1996) research
study whoafter analysing the studentmentor relationshipfound it
could be supportive of student-centredlearning and dovetails
closely with the philosophyof PBL.
The revised plan of care was discussed with thechild to
ascertain her understanding of the care shewas receiving. The
anxieties associated with theaccident were causing disturbed sleep
patternsand the student felt that the child might be expe-riencing
post traumatic stress acknowledging thatshe was afraid of falling
asleep (Rogers and Guer-nay, 2001). The flashbacks were a
psychologicalcomponent of the injury, which appeared to inten-sify
the pain experience which also supports Suresh(2000). This
information was shared with thedelivery and continuing professional
developmentand include the pressure of home and family (Phil-lips,
2000). The mentor acknowledged that contin-uing professional
development had not featuredhigh on the personal agenda but
completion ofthe pain module had re-awakened the need toquestion
practice.
The student hypothesized that the medicalmodel of care required
challenging. If nursing staffhad engaged in meaningful discussions
with the con-sultant, expressing concerns that the removal of
thecatheter may potentiate pain associated with thefractured ala
and bedpan usage, then the decisionto remove the catheter could
have been delayed.This would have allowed nursing staff to develop
agreater insight into the origins of the pain and hope-fully
improve the overall management. Carroll andJohnson (1990) suggest
that these actions demon-strate sound clinical decision making is
taking placeand consultant feedback changed the way care
wasmanaged, demonstrating improvements to clientcare through
multi-professional working.
Care delivery
The care delivery system should meet the clientgroup care needs
and provide continuity and con-sistency in all aspects of care
delivery. The studentacted as an associate nurse to the named
nurse(Department of Health, 1992) and operated from
-
clinical mentor and the house officer and with the
cussed. It was explained that by applying tractionto the lower
limbs this relieved the pressure on
and ethical aspects of care delivery which re-
tice were at the students fingertips and accessedby using key
skills of information technology and
132 B. Burnsthe fracture site (Dandy and Edwards, 1998).However,
the removal of the traction would notaffect the healing of the
fractures but was possi-bly a contributing factor to the disturbed
sleeppatterns experienced. The child acknowledgedthat she had
insufficient information when takingthe decision to have the
traction removed whichreinforced the need to gain full informed
con-sent. The ability to link these practice eventsto prior
learning facilitated increased understand-ing of the Frazer
guidelines (1996) and priorknowledge of child development
identified thata 14 year old should have sufficient
cognitiveability to understand the issues involved. The stu-dent
relied on her knowledge of child protectionEvery Child Matters
(DOH, 2001), which clearlystates that, childrens views should be
taken intoconsideration when planning interventions.
The mentor found time to listen to the stu-dents concerns and
felt that some important is-sues were being raised surrounding
professionalchilds consent she was referred to the clinical
psy-chologist (Carter, 1994). Furthermore, the pain re-lief
medication was upsetting her digestion whichmade her reluctant to
eat; it was also difficult toeat when lying flat on one pillow.
Whilst awaiting the psychology referal, theX-rays were used to
explain the nature of the inju-ries and how these contributed to
the pain experi-enced when moving onto a bedpan. The child
wasencouraged to read about her injuries and the wardschoolteachers
provided a website where she couldfind out more about her injuries.
Gradually shebegan taking limited lessons and work sent in byher
school, was used by hospital teachers (DfEE,1996). Input from the
play specialist was requestedand appropriate distraction techniques
were devel-oped to support pharmacological painmanagement.A
numerical pain rating scale was substituted for theWong and Baker
scale and the child was encouragedto score and describe her pain
and engage indecisions surrounding pain management.
Professional and ethical
It became evident that these actions wereempowering in nature,
allowing the child to be-come involved in decisions surrounding her
carerather than being a passive recipient. One aspectof care she
questioned surrounded the removal ofthe Pugh skin traction on day
five. Once againdecisions surrounding risk versus benefit were dis-
problem solving. The orthopaedic consultant held
overall responsibility for the childs care but thenamed nurse
remains professionally accountablefor the continuity of care. The
medical model pro-vided only part of the answer to the childs
prob-lems and some nurses had become taskorientated and were
unwilling to challenge prac-tice. Other nurses were practicing with
a limitedknowledge of anatomy and physiology and thishad a direct
impact on the quality of care deliv-ered. Access to clinical
experts allowed for clarifi-cation of problems and led to improved
ways ofworking. However, information gained from reli-able Internet
sources allowed the child to beviewed, holistically and the
psychosocial needsassociated with the impact of trauma were
ad-dressed. This had been a valuable learning experi-ence for both
student and mentor and thesupport gained from each other was
beneficial topatient care. The ward setting proved to be a
valu-able learning environment (DOH/ENB, 2001). Thestudent
reflected and understood why these eventshad reinforced the
selection of childrens nursing asa positive career choice. Indeed
the events hadquired further exploration. The mentor had
facil-itated new learning and supported the studentthrough some
difficult learning experiences (Nurs-ing and Midwifery Council,
2002). It was impor-tant that these experiences were disseminatedto
the wider healthcare team with the hope ofinfluencing future
practice. These actions corre-spond to the final stage of Carroll
and Johnsons(1990) model. Following discussion with the wardmanager
student and mentor presented this casestudy to a multi-professional
audience includingpre-registration student nurses, qualified
nurses,radiography staff, house officer and the ortho-paedic
consultant. Nurses tend not to get in-volved in multi-professional
case presentationsyet the benefits of inter-professional workinghad
proved beneficial to patient care. Childrensnurses must value their
nursing uniqueness andshare this with other healthcare
professionals.At the end of week one, a comprehensive
mul-ti-professional, evidence based plan of care wasdeveloped,
which had a direct impact on thequality of future care delivery and
achieved thegoals identified in the students action plan.
Conclusion
Answers to problems identified within clinical prac-
-
provided a deeper insight and understanding of
Nursing Standard 16 (19), 3842.McClain, B.C., Ennevor, S., 2000.
The use of gabapentin in
Nicklin, Wilson, 2000. In: Nicklin, Kenworthy (Eds.),
Teaching
Nursing and Midwifery Council, 2002. Code of
ProfessionalConduct. NMC, London.
www.qaa.ac.uk.Rogers, P., Guernay, K., 2001. Phobias: nature and
assessment.
Utilising information technology and problem-based learning
strategies 133pediatric patients with neuropathic pain. Seminars in
Anes-thesia, Perioperative Medicine and Pain 19 (2),
8387http://gateway.ut.ovid.com/gw1/ovidweb.cgi .
Muir, J., 2004. Clinical decision-making: theory and
practice.Available from:
http://www.nursingstandard.co.uk/archives/ns/vol18-36/.Acknowledgement
I would like to thank Dorothy Lothian (Pain Nurse)for her
expertise when discussing the use of Gaba-pentin for the management
of neuropathic pain.
References
Benner, P., 1984. From Novice to Expert: Excellence and Powerin
Clinical Nursing. Addison- Wesley, California, USA.
Carroll, J., Johnson, E., 1990. Decision Research: A Field
Guide.Sage, California.
Carter, B., 1994. Child and Infant Pain. Chapman Hall,
London.Chow, F.L.W., Suen, L.K.P., 2001. Clinical staff as mentors
in
pre-registration undergraduate nursing education:
Studentsperceptions of the mentors roles and responsibilities.
NurseEducation Today 21, 350358.
Dandy, D., Edwards, D.J., 1998. Essential Orthopaedics
andTrauma. Churchill Livingstone, London.
Darvill, A, McLoughlin, M., 2001. The Onion Model,
Pre-Registration Diploma in Nursing Curriculum,
SalfordUniversity.
Day, A., Jonas, D., 1998. Management of paediatric
pain.Community Nurse 4 (2), 46, 4850.
Department for Education & Employment 1996. The
EducationAct. HMSO, London.
Department of Health 1992. The Patients Charter.
HMSO,London.
Department of Health, 2001. Informed consent. HMSO,
London.Department of Health, 2001. Every Child Matters. HMSO,
London.English national Board/Department of Health, 2001a.
Place-
ments in Focus. English National Board, London.Frazer, 1996.
Gillick v West Norfolk and Wisbech Area Health
Authority [3 All ER 402 HL].Gilroy, J., 2000. Basic Neurology,
third ed. McGraw-Hill, Detroit,
p. 605.Glen, S., Wilkie, K., (Eds.) 2000. Problem-based learning
in
Nursing. A new model for a new context, London.Harden, R., 1999.
Gabapentin: a new tool in the treatment of
neuropathic pain. Acta Neurologia Scandinavia (Suppl.
100),4347.
Koh, L.C., 2002. Practice-based teaching and nurse
education.Available from:
http://www.nursing-standard.co.uk/archives/ns/vol15-30/7-41.
Roper, N., Logan, W., Tierney, A., 1990. The Elements ofNursing.
Churchill Livingstone, London.
Sackett, D., Rosenberg, W.M., Gray, J.A., Haynes, R.B.,
Rich-ardson, W.S., 1996. Evidence based medicine: what it is
andwhat it isnt. British Medical Journal 312 (7023), 7172.
Simpson, L., 2001. Indwelling urethral catheters. Availablefrom:
http://www.nursing-standard.co.uk/archives/ns1546/47/53.
Spouse, J., 1996. The effective mentor: A model for
student-centred learning. Nursing Times 92 (13), 3235.
Suresh, S., 2000. Chronic Pain Management in Children
andAdolescents The Childs Doctor: Journal of Childrens Memo-rial
Hospital. Available from: http:www.childdoc.org.
Stoller, D.W., Galante, J., Haddad, F., Muirhead-Allwod,
S.K.,Chipendale, A., Maheson, M.V.S., Chao, E.S., 2004.
Interac-tive Hip Primal Pictures. Available from:
www.isd.sal-ford.ac.uk/resources/eresources/interactivehip.
Tarling, M., Crofts, L. (Eds.), 2002. The Essential
ResearchersHandbook. Bailliere Tindall.
United Kingdom Central Council for Nursing, Midwifery andHealth
Visiting, 1999. Fitness for Practice: UKCC Commissionfor Nursing
and Midwifery Education. UKCC, London.
UKCC, 1996. Guidelines for Professional Practice.
UKCC,London.
Wilder, R.T., Berde, C.B., Wolohan, M., Vieryra, M.A.,
Masek,B.J., Micheli, L.J., 1992. reflex sympathetic dystrophy
inchildren. Clinical characteristics and follow-up of
seventypatients. Journal of Bone Joint Surgery 74, 910919.
Further reading
Proximal Course of the Pudendal Nerve, 1988. Available
from:http://www.gmedmedia/weblec01/lec24.
Richtmeiser, J., 1999. The basics of the pelvis and theperineum:
The proximal course of the pudendal
nerve.http://oac.med.jhmi.edu/Weblec/Weblec01/lec24.html.
Wong, D., Baker, C., 1988. Pain in children: comparison
ofassessment scales. Pediatric Nursing 14 (1), 9017.Oakey, D.,
Doyle, M., 2000. A Strategic Approach to Undergrad-uate Key Skills
Development: Salford Key Skills Project, FinalReport, University of
Salford.
Papp, I., Markkanen, M., Bonsdorff, M., 2003. Clinical
environ-ment as a learning environment: student nurses
perceptionsconcerning clinical learning experience. Nurse
EducationToday 23, 262268.
Phillips, T., 2000. Practice and Assessment in Nursing
andMidwifery: Doing it for real English National Board, London.
Quality Assurance Agency, 2001. Available from:professional role
issues and the student felt fit forpurpose and practice (UKCC,
1996).
and Assessing in Nursing Practice. Bailliere Tindall,
London(Chapter 9).
Nolan, 1998. Available from:
http://www.trauma.org/cases/classic001.html.
Utilising information technology and problem-based learning
strategies to resolve practice dilemmas in a children " s
orthopaedic settingBackgroundTheory underpinning curriculum
deliveryCase studyPersonal and professional developmentCare
managementCare deliveryProfessional and
ethicalConclusionAcknowledgementReferencesFurther reading