Embed Size (px)
Citation preview
Using theBody SystemsModel
9
Refer to Chapter 2 “Assessment,” p. 62: Care Plans Developed after Using theBody Systems Assessment Model
Client’s name: Mrs. Mary JonesAge: 70 yearsDocument Includes: Scenario, activities 1–7, pathoflow sheet, assessment
(The Body Systems Model) and three care plans.
Scenario
This client was brought to the emergency room. She complained of pain in herleft thigh. She stated she tripped over a telephone cord in her kitchen and fell.An X-ray of her leg revealed a fracture of the left femur (medical diagnosis).
Activity 1Use this initial information from the client’s record to assure you are caring forthe right client chosen or assigned by your instructor.
Activity 2Examine the pathoflow sheet to determine the sequencing of events that proba-bly led to Mrs. Jones’ fall, the fracture of her femur, and the likely complications
B1
Appendix
that could follow due to immobility and the nursing diagnoses that relate toeach body system (see example provided). This process will help you providecomprehensive nursing care to your clients.
Activity 3Review the Body Systems Assessment provided (for Mrs. Jones) and becomefamiliar with this approach. Be aware that any model chosen should providethe information you need to develop comprehensive individualized care plansfor your client.
What seemed to be the most pressing need of Mrs. Jones at this time?
Activity 4Examine the first care plan and note that the client is crying and preoccupiedwith her husband’s death (see ordered and selected data). Now review theNANDA diagnoses list and note that these behaviors are categorized asGrieving, Dysfunctional.
Activity 5Examine care plan 2, to determine that the problem of altered self concept islikely less pressing than that of grieving.
Why was knowledge deficit about cast care assigned third priority?
Activity 6Examine care plan 3 and conclude that the client did not have the cast applieduntil after the first two problems were identified. Remember to use criti-cal thinking, problem solving, and decision making to meet client’s needs (prioritize).
Is each care plan individualized?
Activity 7Use the guidelines specified in Appendix A for Chapter One (IndividualizedCare Plans) to draw conclusions about Mrs. Jones’s care plans.
Note: Remember that a scenario, a pathoflow sheet, and a comprehensiveassessment help you provide comprehensive individualized client care.
10 Appendix B1
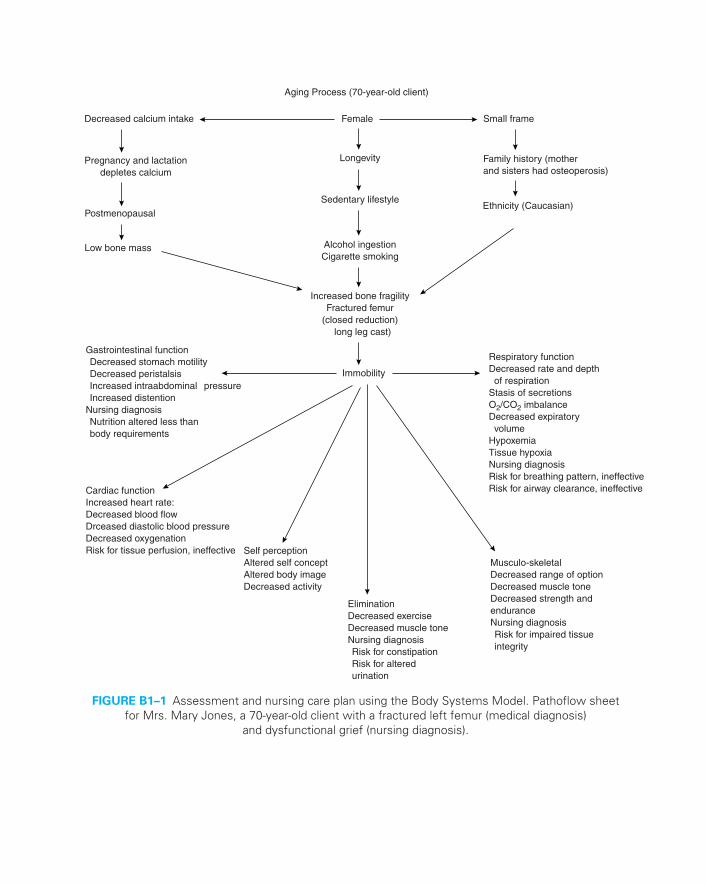
Decreased calcium intake Female Small frame
Pregnancy and lactationdepletes calcium
Postmenopausal
Low bone mass
Sedentary lifestyle
Alcohol ingestionCigarette smoking
Increased bone fragilityFractured femur
(closed reduction) long leg cast)
Immobility
Ethnicity (Caucasian)
Longevity Family history (motherand sisters had osteoperosis)
Gastrointestinal function Decreased stomach motility Decreased peristalsis Increased intraabdominal pressure Increased distentionNursing diagnosis Nutrition altered less than body requirements
Cardiac functionIncreased heart rate:Decreased blood flowDrceased diastolic blood pressureDecreased oxygenationRisk for tissue perfusion, ineffective
Respiratory functionDecreased rate and depth of respirationStasis of secretionsO2/CO2 imbalanceDecreased expiratory volumeHypoxemiaTissue hypoxiaNursing diagnosisRisk for breathing pattern, ineffectiveRisk for airway clearance, ineffective
Self perceptionAltered self conceptAltered body imageDecreased activity
EliminationDecreased exerciseDecreased muscle toneNursing diagnosis Risk for constipation Risk for altered urination
Musculo-skeletalDecreased range of optionDecreased muscle toneDecreased strength andenduranceNursing diagnosis Risk for impaired tissue integrity
Aging Process (70-year-old client)
FIGURE B1–1 Assessment and nursing care plan using the Body Systems Model. Pathoflow sheet for Mrs. Mary Jones, a 70-year-old client with a fractured left femur (medical diagnosis)
and dysfunctional grief (nursing diagnosis).
12 Appendix B1
ASSESSMENT AND NURSING CARE PLANUSING THE BODY SYSTEMS MODEL FORMRS. MARY JONES (MEDICAL MODEL)
Client Assessment Body Systems Model:
Sensory Perceptual: Mental Status and Neurological Exam
1. Mental status, physical appearance, and behaviora. Posture and movement, lying supine in bed, shoulders symmetricalb. Dress somewhat inappropriate (larger than size—loose fitting)c. Grooming and hygiene: hair hanging over face, oily skin, clean, nails
very short, evidence of frequent bitingd. Face: symmetrical, facial expressions: anxiouse. Affect: flat, somewhat withdrawn, tears in eyes
2. Speech: low volume (crying), intact comprehension of spoken words,nods “yes” and “no”
3. Level of consciousness: oriented to time, place, and person4. Cognitive abilities/mentation
a. Attention: within normal limits—not easily destructiveb. Long-term and short-term memory intactc. Judgment: abnormal preoccupation with husband’s deathd. Insight: abnormal preoccupation with husband’s death—states,
“I cannot do anything for myself.”e. Spatial perception: intact to familiar sounds, unable to draw due to
distraction with fear of surgery and husband’s deathf. Calculation: unable/reluctant to perform serial 7’s (crying spell)g. Abstract reasoning, unable, unwilling to performh. Thought process and content: consistent and coherent
5. Sensorya. Exteroceptive sensation
1. Light touch: intact on both upper and lower extremities2. Superficial pain: intact (more sensitive on left lower extremity—
broken femur)3. Temperature: normal findings (warm to touch)
b. Proprioceptive sensation1. Motion and position: normal findings (identifies changes of posi-
tion of body part)2. Vibration sense: normal findings (perceives vibration over all
bony prominences)
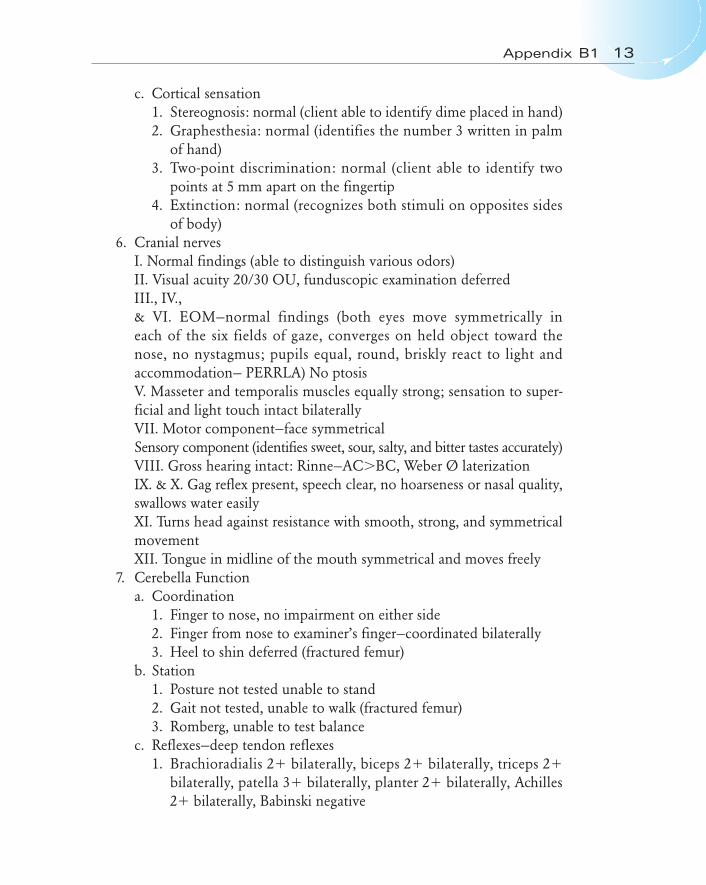
c. Cortical sensation1. Stereognosis: normal (client able to identify dime placed in hand)2. Graphesthesia: normal (identifies the number 3 written in palm
of hand)3. Two-point discrimination: normal (client able to identify two
points at 5 mm apart on the fingertip4. Extinction: normal (recognizes both stimuli on opposites sides
of body)6. Cranial nerves
I. Normal findings (able to distinguish various odors)II. Visual acuity 20/30 OU, funduscopic examination deferredIII., IV.,& VI. EOM—normal findings (both eyes move symmetrically in each of the six fields of gaze, converges on held object toward the nose, no nystagmus; pupils equal, round, briskly react to light and accommodation— PERRLA) No ptosisV. Masseter and temporalis muscles equally strong; sensation to super-ficial and light touch intact bilaterallyVII. Motor component—face symmetricalSensory component (identifies sweet, sour, salty, and bitter tastes accurately)VIII. Gross hearing intact: Rinne—AC�BC, Weber Ø laterizationIX. & X. Gag reflex present, speech clear, no hoarseness or nasal quality,swallows water easilyXI. Turns head against resistance with smooth, strong, and symmetricalmovementXII. Tongue in midline of the mouth symmetrical and moves freely
7. Cerebella Functiona. Coordination
1. Finger to nose, no impairment on either side2. Finger from nose to examiner’s finger—coordinated bilaterally3. Heel to shin deferred (fractured femur)
b. Station1. Posture not tested unable to stand2. Gait not tested, unable to walk (fractured femur)3. Romberg, unable to test balance
c. Reflexes—deep tendon reflexes1. Brachioradialis 2� bilaterally, biceps 2� bilaterally, triceps 2�
bilaterally, patella 3� bilaterally, planter 2� bilaterally, Achilles2� bilaterally, Babinski negative
Appendix B1 13
14 Appendix B1
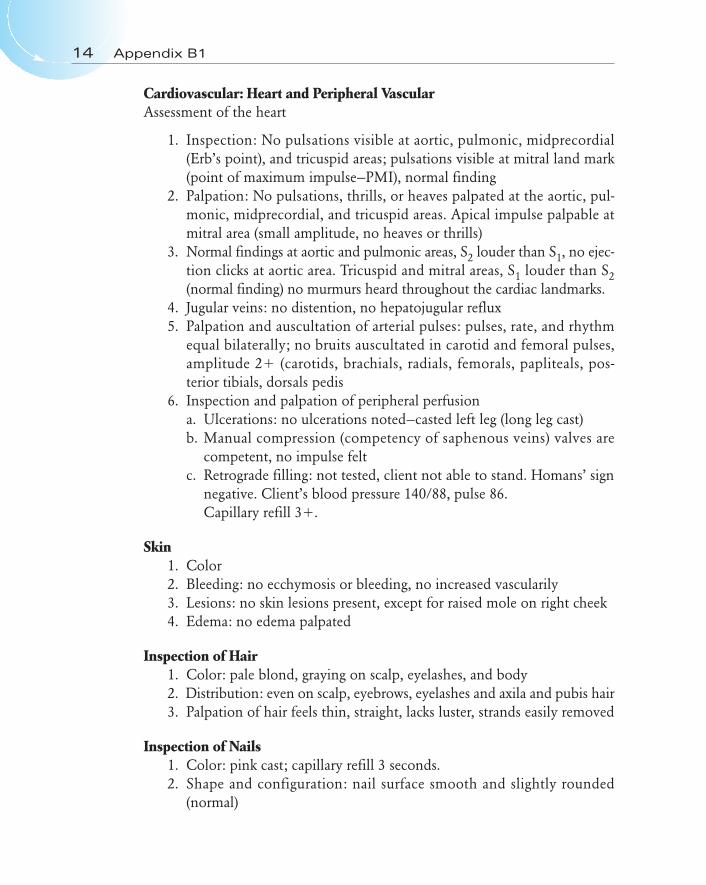
Cardiovascular: Heart and Peripheral VascularAssessment of the heart
1. Inspection: No pulsations visible at aortic, pulmonic, midprecordial(Erb’s point), and tricuspid areas; pulsations visible at mitral land mark(point of maximum impulse—PMI), normal finding
2. Palpation: No pulsations, thrills, or heaves palpated at the aortic, pul-monic, midprecordial, and tricuspid areas. Apical impulse palpable atmitral area (small amplitude, no heaves or thrills)
3. Normal findings at aortic and pulmonic areas, S2 louder than S1, no ejec-tion clicks at aortic area. Tricuspid and mitral areas, S1 louder than S2(normal finding) no murmurs heard throughout the cardiac landmarks.
4. Jugular veins: no distention, no hepatojugular reflux5. Palpation and auscultation of arterial pulses: pulses, rate, and rhythm
equal bilaterally; no bruits auscultated in carotid and femoral pulses,amplitude 2� (carotids, brachials, radials, femorals, papliteals, pos-terior tibials, dorsals pedis
6. Inspection and palpation of peripheral perfusiona. Ulcerations: no ulcerations noted—casted left leg (long leg cast)b. Manual compression (competency of saphenous veins) valves are
competent, no impulse feltc. Retrograde filling: not tested, client not able to stand. Homans’ sign
negative. Client’s blood pressure 140/88, pulse 86.Capillary refill 3�.
Skin1. Color2. Bleeding: no ecchymosis or bleeding, no increased vascularily3. Lesions: no skin lesions present, except for raised mole on right cheek4. Edema: no edema palpated
Inspection of Hair1. Color: pale blond, graying on scalp, eyelashes, and body2. Distribution: even on scalp, eyebrows, eyelashes and axila and pubis hair3. Palpation of hair feels thin, straight, lacks luster, strands easily removed
Inspection of Nails1. Color: pink cast; capillary refill 3 seconds.2. Shape and configuration: nail surface smooth and slightly rounded
(normal)
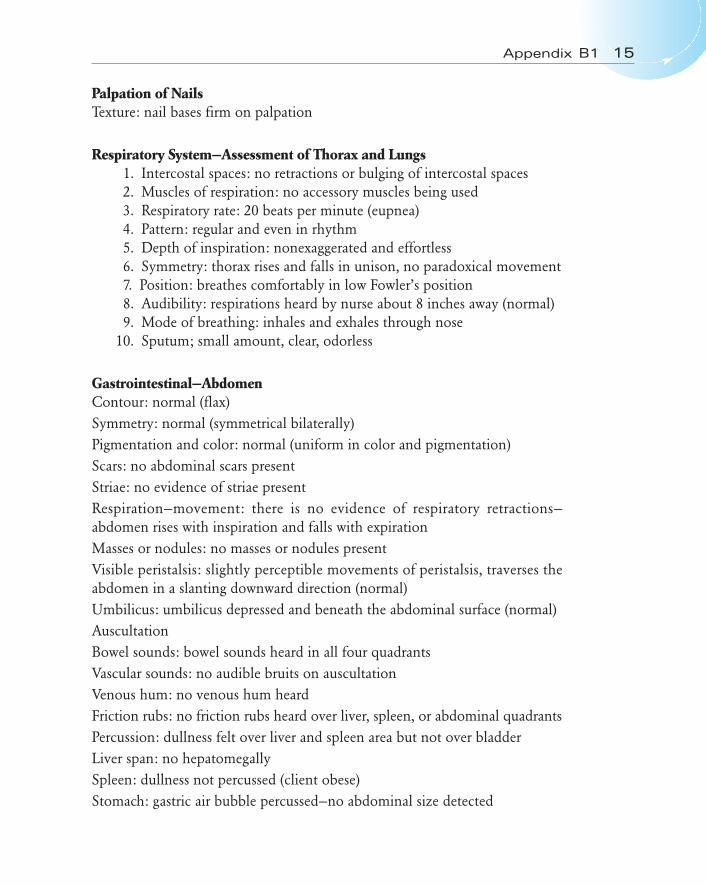
Palpation of NailsTexture: nail bases firm on palpation
Respiratory System—Assessment of Thorax and Lungs1. Intercostal spaces: no retractions or bulging of intercostal spaces2. Muscles of respiration: no accessory muscles being used3. Respiratory rate: 20 beats per minute (eupnea)4. Pattern: regular and even in rhythm5. Depth of inspiration: nonexaggerated and effortless6. Symmetry: thorax rises and falls in unison, no paradoxical movement7. Position: breathes comfortably in low Fowler’s position8. Audibility: respirations heard by nurse about 8 inches away (normal)9. Mode of breathing: inhales and exhales through nose
10. Sputum; small amount, clear, odorless
Gastrointestinal—AbdomenContour: normal (flax)Symmetry: normal (symmetrical bilaterally)Pigmentation and color: normal (uniform in color and pigmentation)Scars: no abdominal scars presentStriae: no evidence of striae presentRespiration—movement: there is no evidence of respiratory retractions—abdomen rises with inspiration and falls with expirationMasses or nodules: no masses or nodules presentVisible peristalsis: slightly perceptible movements of peristalsis, traverses theabdomen in a slanting downward direction (normal)Umbilicus: umbilicus depressed and beneath the abdominal surface (normal)AuscultationBowel sounds: bowel sounds heard in all four quadrantsVascular sounds: no audible bruits on auscultationVenous hum: no venous hum heardFriction rubs: no friction rubs heard over liver, spleen, or abdominal quadrantsPercussion: dullness felt over liver and spleen area but not over bladderLiver span: no hepatomegallySpleen: dullness not percussed (client obese)Stomach: gastric air bubble percussed—no abdominal size detected
Appendix B1 15

PalpationLight palpation: abdomen smooth with consistent softnessDeep palpation: no organ enlargement, abnormal masses, bulges, or swellingpalpated
GenitalHair distribution: pubic hair distribution, normal; shaped like an inverse tri-angle, graying, (shows some sparse areas)Presence of parasites: no parasites presentSkin color and condition: the skin color over the mons pubis hair is clear; thelabia majora and minora are wrinkled but unbroken; there are no lesions,ecchymosis, excorations, nodules, swelling, or rash.Clitoris: without lesionsMusculoskeletal: overall appearance—client 5�3� tall, body weight 165 lbs,medium body frame; approximately 37 pounds over-weight, demonstratingpain behavior (at times clinches left hip area, states, “that hurts”), unable toaccess unit area by walking.Posture: unable to assess, cannot standGait and mobility: unable to access, broken femurInspection: muscle size and shape—no accentuation notedNo evidence of hypertrophy or atrophy, strong muscle strength in upperextremity and right lower leg
16 Appendix B1
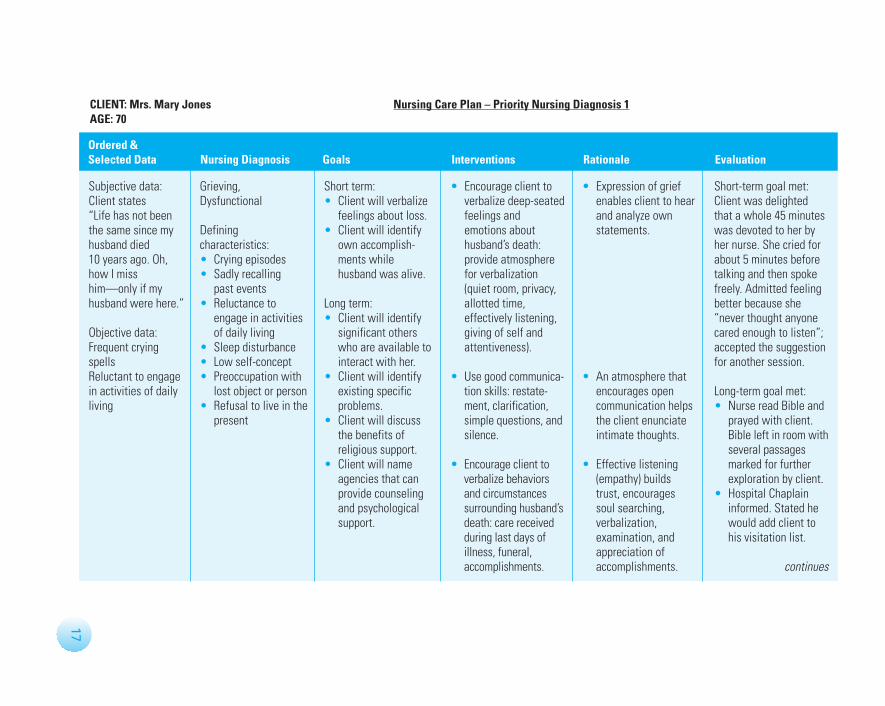
Subjective data:Client states“Life has not beenthe same since myhusband died10 years ago. Oh,how I misshim—only if myhusband were here.”
Objective data:Frequent cryingspellsReluctant to engagein activities of dailyliving
Grieving, Dysfunctional
Definingcharacteristics:• Crying episodes• Sadly recalling
past events• Reluctance to
engage in activitiesof daily living
• Sleep disturbance• Low self-concept• Preoccupation with
lost object or person• Refusal to live in the
present
Short term:• Client will verbalize
feelings about loss.• Client will identify
own accomplish-ments whilehusband was alive.
Long term:• Client will identify
significant otherswho are available tointeract with her.
• Client will identifyexisting specificproblems.
• Client will discussthe benefits ofreligious support.
• Client will nameagencies that canprovide counselingand psychologicalsupport.
• Encourage client toverbalize deep-seatedfeelings andemotions abouthusband’s death:provide atmospherefor verbalization(quiet room, privacy,allotted time,effectively listening,giving of self and attentiveness).
• Use good communica-tion skills: restate-ment, clarification,simple questions, andsilence.
• Encourage client toverbalize behaviorsand circumstancessurrounding husband’sdeath: care receivedduring last days ofillness, funeral,accomplishments.
• Expression of griefenables client to hearand analyze ownstatements.
• An atmosphere thatencourages opencommunication helpsthe client enunciateintimate thoughts.
• Effective listening(empathy) buildstrust, encouragessoul searching,verbalization,examination, andappreciation ofaccomplishments.
Short-term goal met:Client was delightedthat a whole 45 minuteswas devoted to her byher nurse. She cried forabout 5 minutes beforetalking and then spokefreely. Admitted feelingbetter because she“never thought anyonecared enough to listen”;accepted the suggestionfor another session.
Long-term goal met:• Nurse read Bible and
prayed with client.Bible left in room withseveral passagesmarked for furtherexploration by client.
• Hospital Chaplaininformed. Stated hewould add client tohis visitation list.
continues
CLIENT: Mrs. Mary Jones Nursing Care Plan – Priority Nursing Diagnosis 1AGE: 70
Ordered &Selected Data Nursing Diagnosis Goals Interventions Rationale Evaluation
17
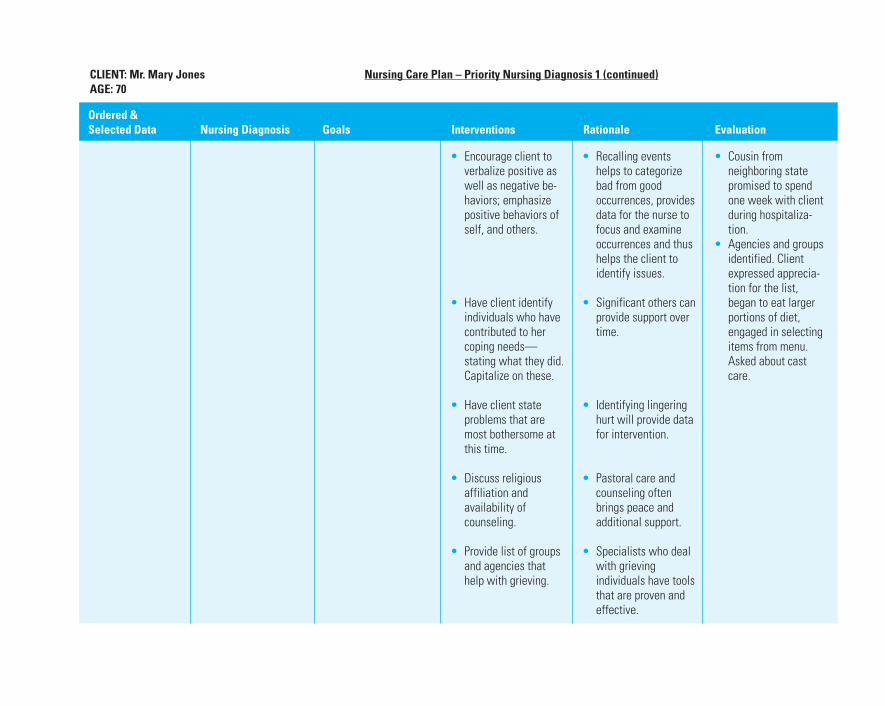
• Encourage client toverbalize positive aswell as negative be-haviors; emphasizepositive behaviors ofself, and others.
• Have client identifyindividuals who havecontributed to hercoping needs—stating what they did.Capitalize on these.
• Have client stateproblems that aremost bothersome atthis time.
• Discuss religiousaffiliation andavailability ofcounseling.
• Provide list of groupsand agencies thathelp with grieving.
• Recalling eventshelps to categorizebad from goodoccurrences, providesdata for the nurse tofocus and examineoccurrences and thushelps the client toidentify issues.
• Significant others canprovide support overtime.
• Identifying lingeringhurt will provide datafor intervention.
• Pastoral care andcounseling oftenbrings peace andadditional support.
• Specialists who dealwith grievingindividuals have toolsthat are proven andeffective.
• Cousin fromneighboring statepromised to spendone week with clientduring hospitaliza-tion.
• Agencies and groupsidentified. Clientexpressed apprecia-tion for the list,began to eat largerportions of diet,engaged in selectingitems from menu.Asked about castcare.
CLIENT: Mr. Mary Jones Nursing Care Plan – Priority Nursing Diagnosis 1 (continued)AGE: 70
Ordered &Selected Data Nursing Diagnosis Goals Interventions Rationale Evaluation
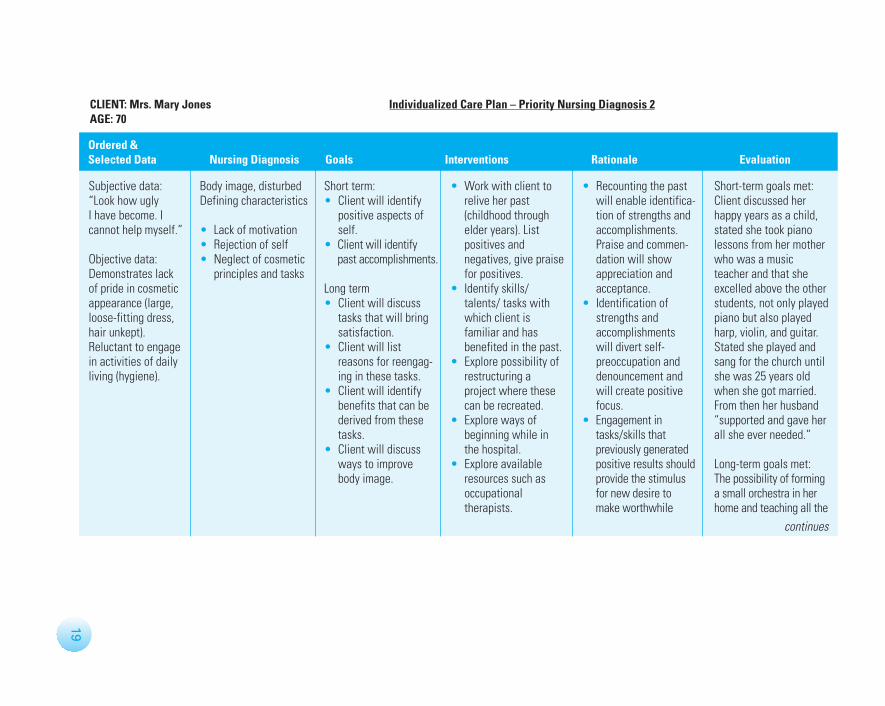
Subjective data:“Look how ugly I have become. Icannot help myself.”
Objective data:Demonstrates lackof pride in cosmeticappearance (large,loose-fitting dress,hair unkept).Reluctant to engagein activities of dailyliving (hygiene).
Body image, disturbedDefining characteristics
• Lack of motivation • Rejection of self• Neglect of cosmetic
principles and tasks
Short term:• Client will identify
positive aspects ofself.
• Client will identifypast accomplishments.
Long term• Client will discuss
tasks that will bringsatisfaction.
• Client will listreasons for reengag-ing in these tasks.
• Client will identifybenefits that can bederived from thesetasks.
• Client will discussways to improvebody image.
• Work with client to relive her past(childhood throughelder years). Listpositives andnegatives, give praisefor positives.
• Identify skills/talents/ tasks withwhich client isfamiliar and hasbenefited in the past.
• Explore possibility ofrestructuring aproject where thesecan be recreated.
• Explore ways ofbeginning while inthe hospital.
• Explore availableresources such asoccupationaltherapists.
• Recounting the pastwill enable identifica-tion of strengths andaccomplishments.Praise and commen-dation will showappreciation andacceptance.
• Identification ofstrengths andaccomplishments will divert self-preoccupation anddenouncement andwill create positivefocus.
• Engagement intasks/skills thatpreviously generatedpositive results shouldprovide the stimulusfor new desire tomake worthwhile
Short-term goals met:Client discussed herhappy years as a child,stated she took pianolessons from her motherwho was a musicteacher and that sheexcelled above the otherstudents, not only playedpiano but also playedharp, violin, and guitar.Stated she played andsang for the church untilshe was 25 years oldwhen she got married.From then her husband“supported and gave herall she ever needed.”
Long-term goals met:The possibility of forminga small orchestra in herhome and teaching all the
continues
CLIENT: Mrs. Mary Jones Individualized Care Plan – Priority Nursing Diagnosis 2AGE: 70
Ordered &Selected Data Nursing Diagnosis Goals Interventions Rationale Evaluation
19
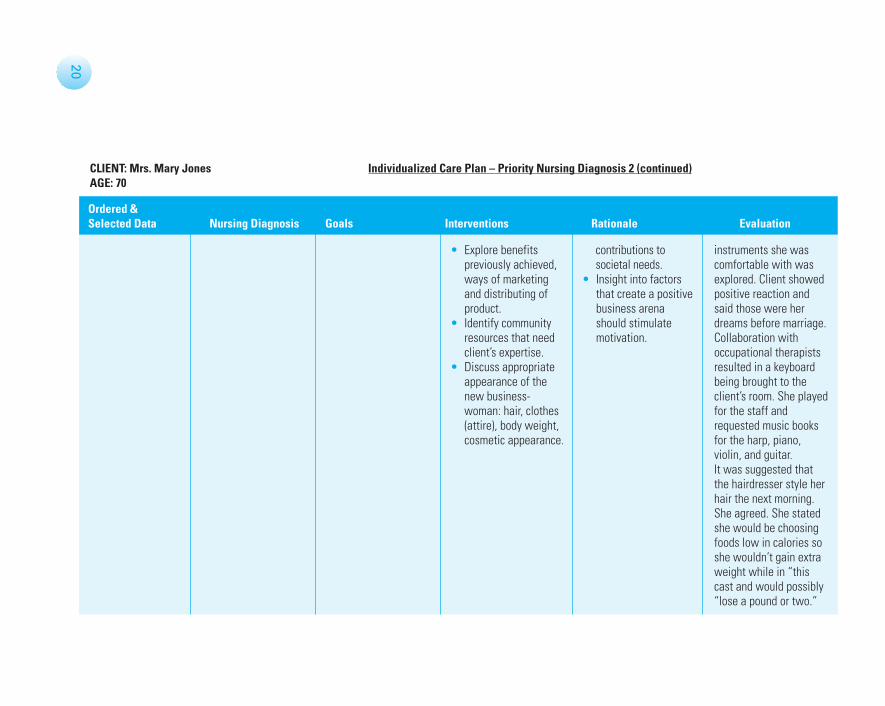
• Explore benefitspreviously achieved,ways of marketingand distributing ofproduct.
• Identify communityresources that needclient’s expertise.
• Discuss appropriateappearance of thenew business-woman: hair, clothes(attire), body weight,cosmetic appearance.
contributions tosocietal needs.
• Insight into factorsthat create a positivebusiness arenashould stimulatemotivation.
instruments she wascomfortable with wasexplored. Client showedpositive reaction andsaid those were herdreams before marriage.Collaboration withoccupational therapistsresulted in a keyboardbeing brought to theclient’s room. She playedfor the staff andrequested music booksfor the harp, piano,violin, and guitar.It was suggested thatthe hairdresser style herhair the next morning.She agreed. She statedshe would be choosingfoods low in calories soshe wouldn’t gain extraweight while in “thiscast and would possibly“lose a pound or two.”
CLIENT: Mrs. Mary Jones Individualized Care Plan – Priority Nursing Diagnosis 2 (continued)AGE: 70
Ordered &Selected Data Nursing Diagnosis Goals Interventions Rationale Evaluation
20
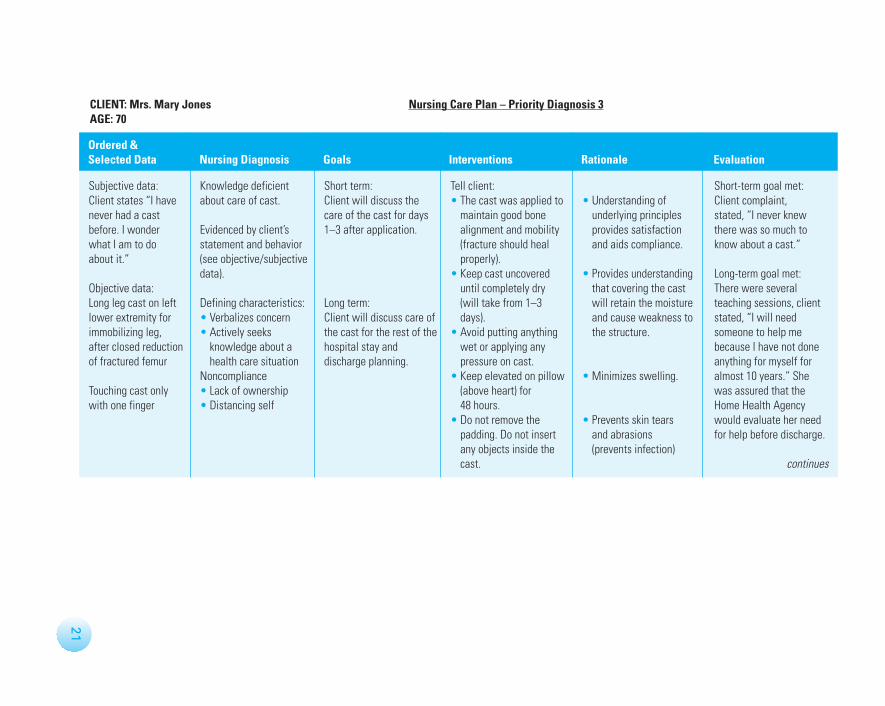
Subjective data:Client states “I havenever had a castbefore. I wonderwhat I am to do about it.”
Objective data:Long leg cast on leftlower extremity forimmobilizing leg,after closed reductionof fractured femur
Touching cast onlywith one finger
Knowledge deficientabout care of cast.
Evidenced by client’sstatement and behavior(see objective/subjectivedata).
Defining characteristics:• Verbalizes concern• Actively seeks
knowledge about ahealth care situation
Noncompliance• Lack of ownership• Distancing self
Short term:Client will discuss thecare of the cast for days1–3 after application.
Long term:Client will discuss care ofthe cast for the rest of thehospital stay anddischarge planning.
Tell client:• The cast was applied to
maintain good bonealignment and mobility(fracture should healproperly).
• Keep cast uncovereduntil completely dry(will take from 1–3days).
• Avoid putting anythingwet or applying anypressure on cast.
• Keep elevated on pillow(above heart) for 48 hours.
• Do not remove thepadding. Do not insertany objects inside thecast.
• Understanding ofunderlying principlesprovides satisfactionand aids compliance.
• Provides understandingthat covering the castwill retain the moistureand cause weakness tothe structure.
• Minimizes swelling.
• Prevents skin tearsand abrasions(prevents infection)
Short-term goal met:Client complaint,stated, “I never knewthere was so much toknow about a cast.”
Long-term goal met:There were severalteaching sessions, clientstated, “I will needsomeone to help mebecause I have not doneanything for myself foralmost 10 years.” Shewas assured that theHome Health Agencywould evaluate her needfor help before discharge.
continues
CLIENT: Mrs. Mary Jones Nursing Care Plan – Priority Diagnosis 3AGE: 70
Ordered &Selected Data Nursing Diagnosis Goals Interventions Rationale Evaluation
21
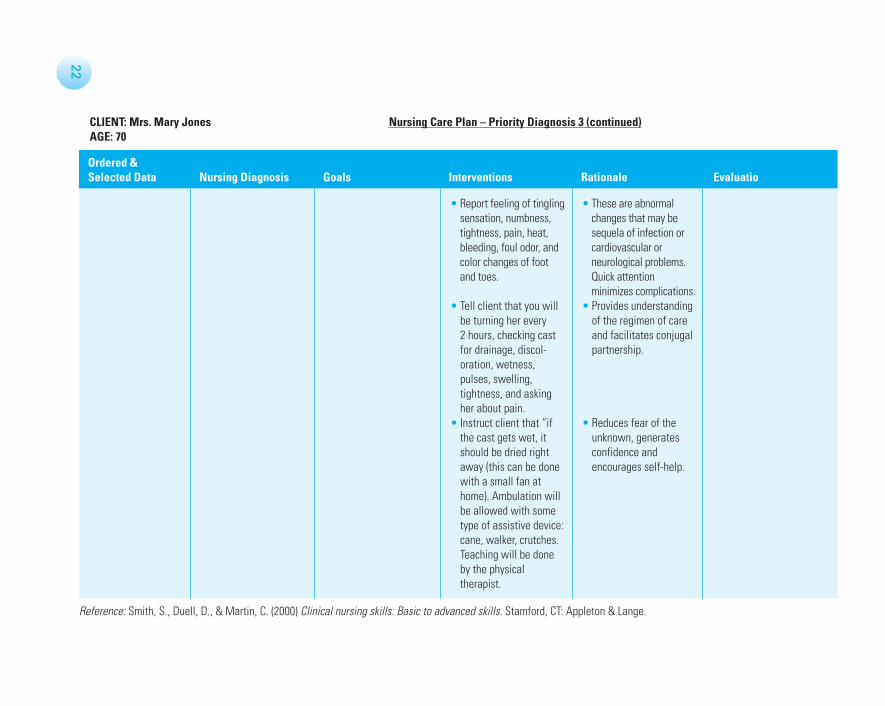
• Report feeling of tinglingsensation, numbness,tightness, pain, heat,bleeding, foul odor, andcolor changes of footand toes.
• Tell client that you willbe turning her every 2 hours, checking castfor drainage, discol-oration, wetness,pulses, swelling,tightness, and askingher about pain.
• Instruct client that “ifthe cast gets wet, itshould be dried rightaway (this can be donewith a small fan athome). Ambulation willbe allowed with sometype of assistive device:cane, walker, crutches.Teaching will be doneby the physicaltherapist.
• These are abnormalchanges that may besequela of infection orcardiovascular orneurological problems.Quick attentionminimizes complications.
• Provides understandingof the regimen of careand facilitates conjugalpartnership.
• Reduces fear of theunknown, generatesconfidence andencourages self-help.
Reference: Smith, S., Duell, D., & Martin, C. (2000) Clinical nursing skills: Basic to advanced skills. Stamford, CT: Appleton & Lange.
22
CLIENT: Mrs. Mary Jones Nursing Care Plan – Priority Diagnosis 3 (continued)AGE: 70
Ordered &Selected Data Nursing Diagnosis Goals Interventions Rationale Evaluatio

![Human Body Exergy Balance: Numerical Analysis of an Indoor ... · Human body system [1]. A human body energy balance model, or twonode model, - was used for the human body system“](https://img.pdfslide.us/doc/110x75/6000b436c5a9c34ccd5461ab/human-body-exergy-balance-numerical-analysis-of-an-indoor-human-body-system.jpg)



























