Embed Size (px)
Citation preview
Using Neutrality To Increase Shoulder Strength SUSAN M. T. McKAY, OTR/L [email protected]
GOAL
Look at shoulder rehab in a different
way. Strength can come from
increasing flexibility and placing a joint
in proper alignment. Conversely,
strengthening a shoulder in improper
alignment can cause injury.
WHY PICK ON THE
SHOULDER?
Impairs function/limits ADL’s
Pain in shoulder
Compensatory patterns can lead to back pain
Elderly rely on upper body to move/ambulate
The sooner issues are treated, the less physiological damage there is
SHOULDER ANATOMY
Muscles and how they move
A basic review and more
Important to know…
SHOULDER ANATOMY
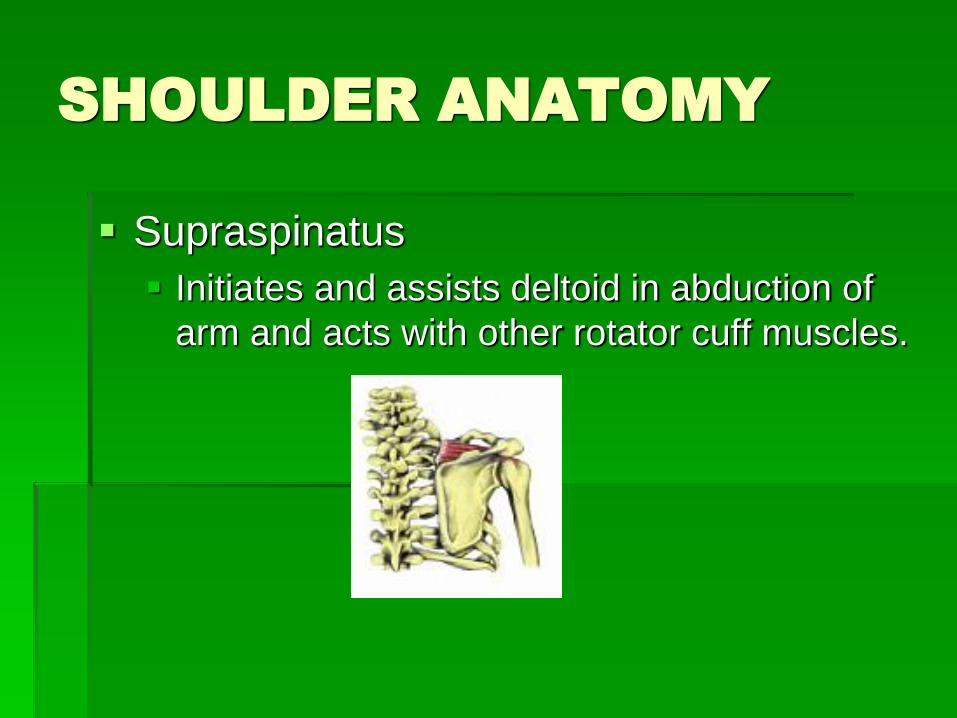
Supraspinatus
Initiates and assists deltoid in abduction of
arm and acts with other rotator cuff muscles.
SHOULDER ANATOMY
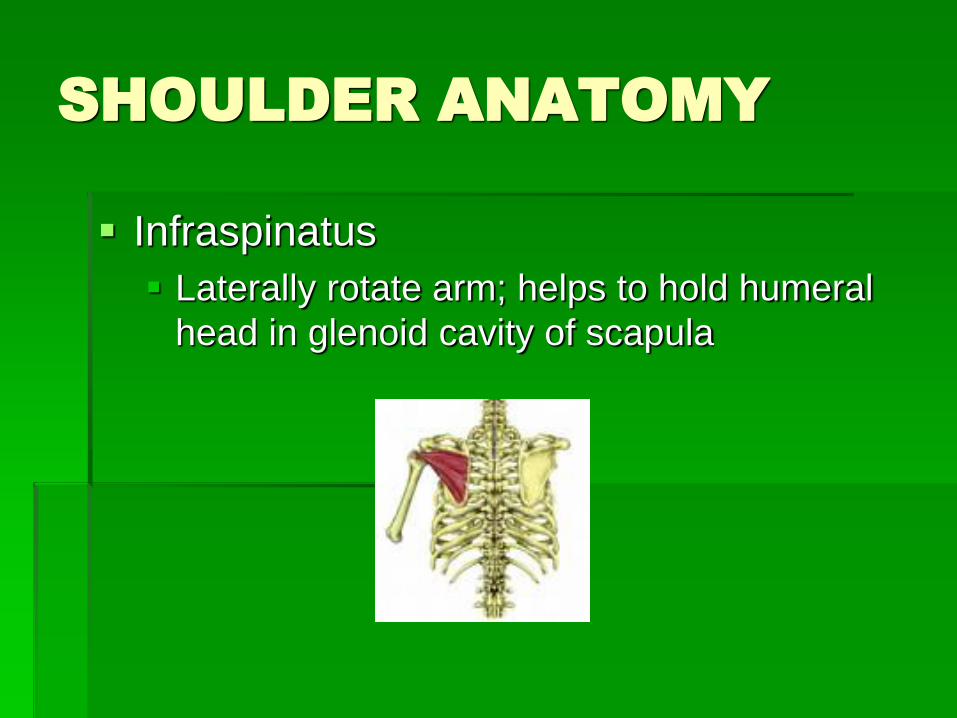
Infraspinatus
Laterally rotate arm; helps to hold humeral
head in glenoid cavity of scapula
SHOULDER ANATOMY
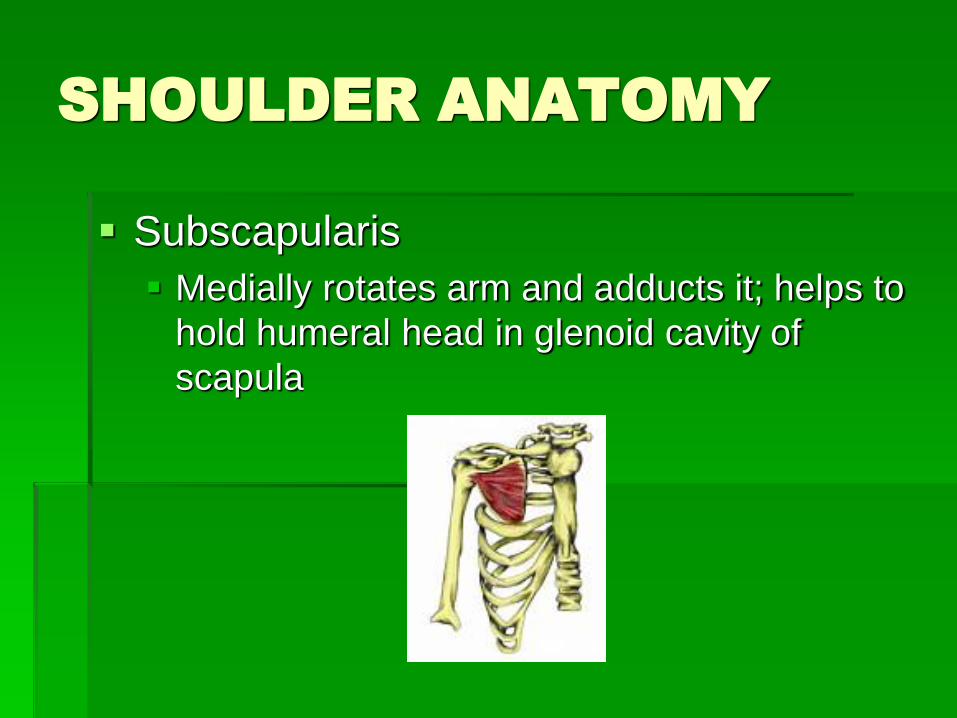
Subscapularis
Medially rotates arm and adducts it; helps to
hold humeral head in glenoid cavity of
scapula
SHOULDER ANATOMY
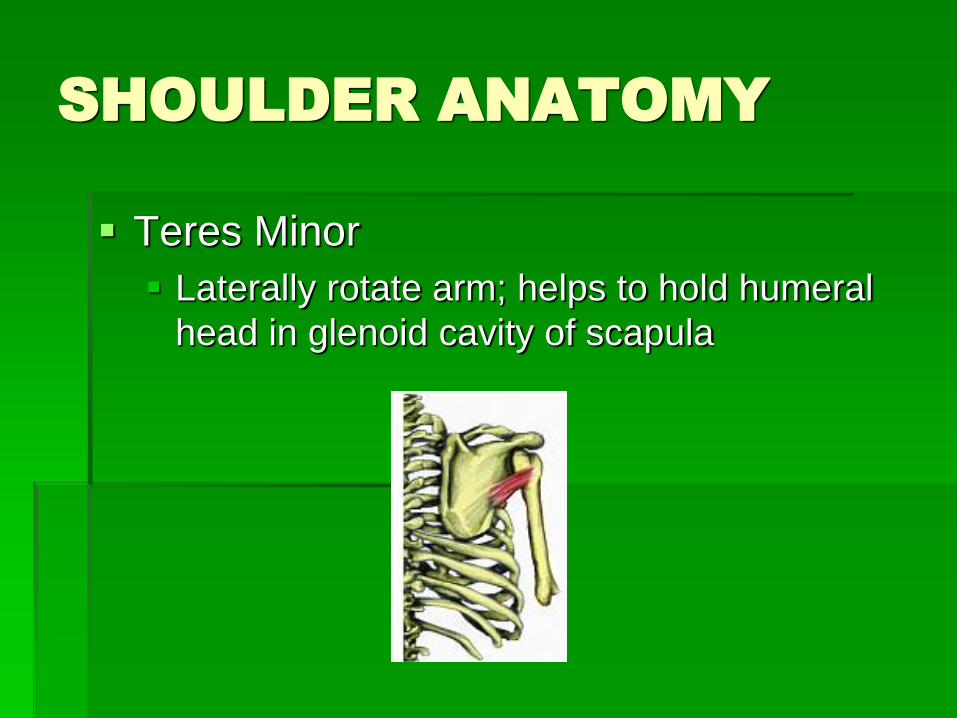
Teres Minor
Laterally rotate arm; helps to hold humeral
head in glenoid cavity of scapula
SHOULDER ANATOMY
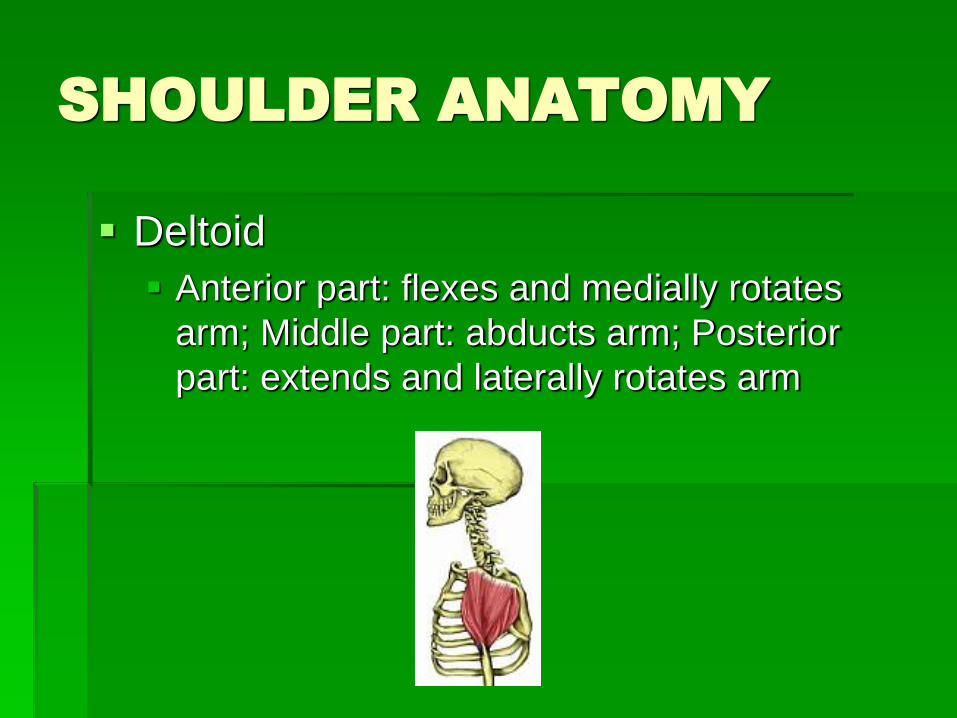
Deltoid
Anterior part: flexes and medially rotates
arm; Middle part: abducts arm; Posterior
part: extends and laterally rotates arm
SHOULDER ANATOMY
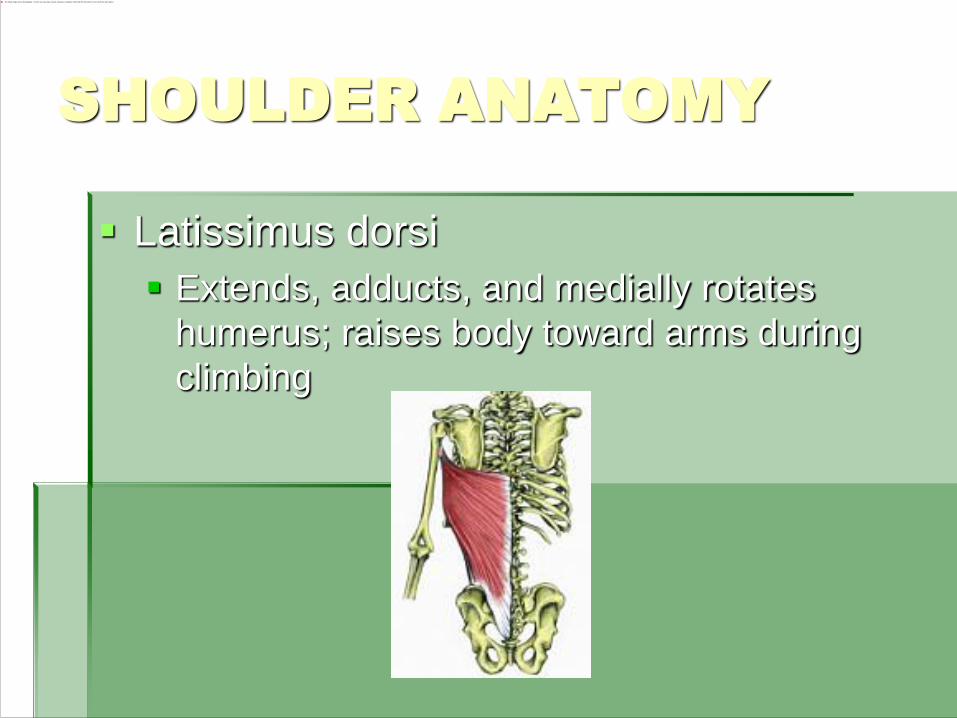
Latissimus dorsi
Extends, adducts, and medially rotates
humerus; raises body toward arms during
climbing
SHOULDER ANATOMY
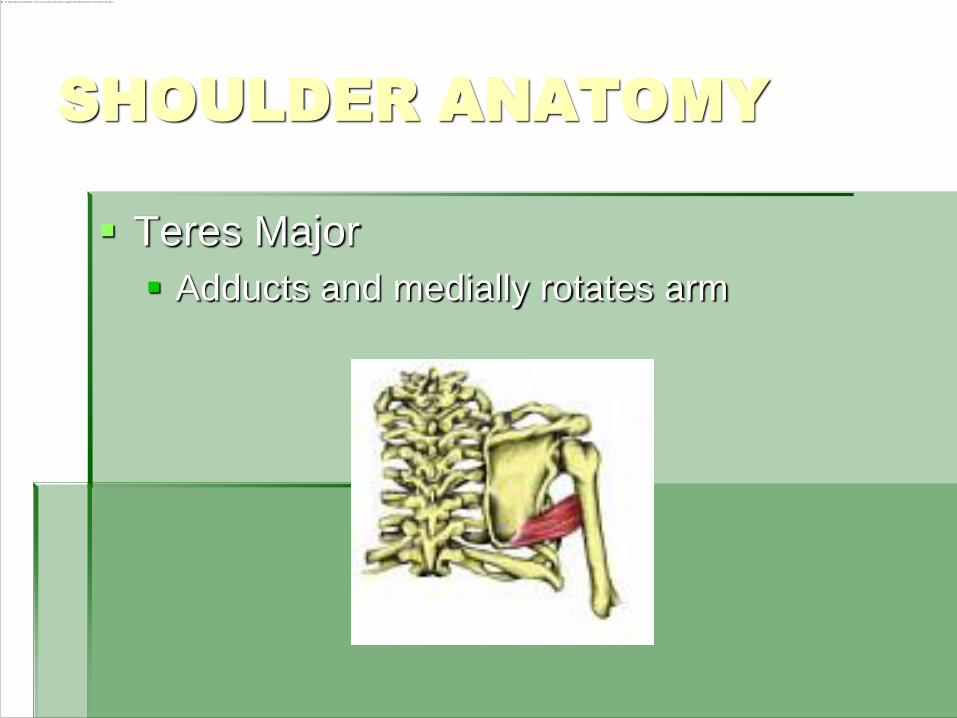
Teres Major
Adducts and medially rotates arm
SHOULDER ANATOMY
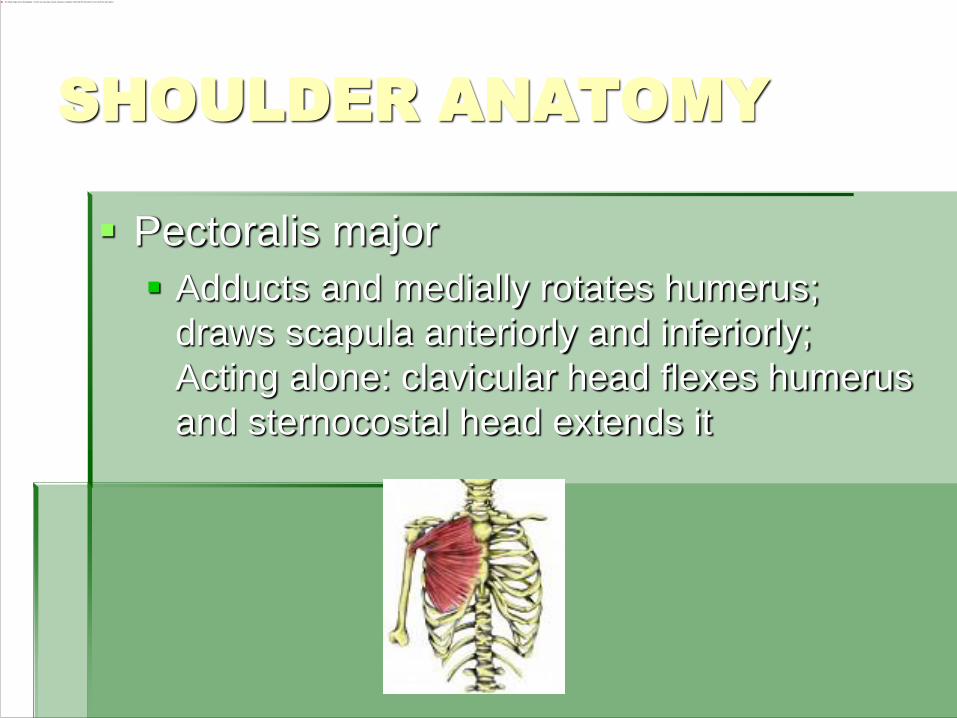
Pectoralis major
Adducts and medially rotates humerus;
draws scapula anteriorly and inferiorly;
Acting alone: clavicular head flexes humerus
and sternocostal head extends it
SHOULDER ANATOMY
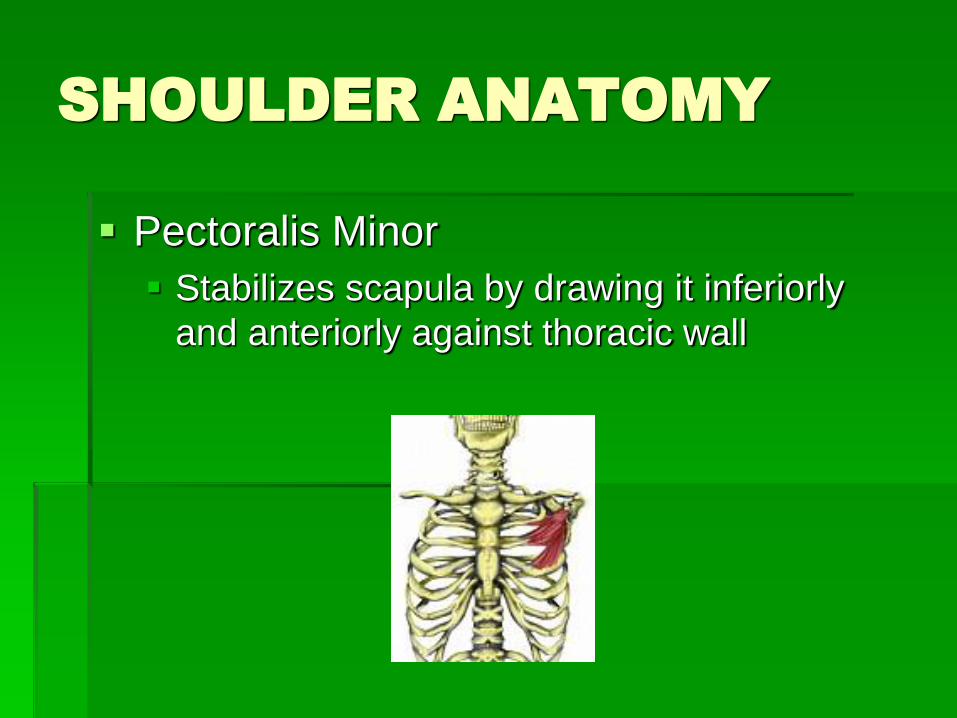
Pectoralis Minor
Stabilizes scapula by drawing it inferiorly
and anteriorly against thoracic wall
SHOULDER ANATOMY
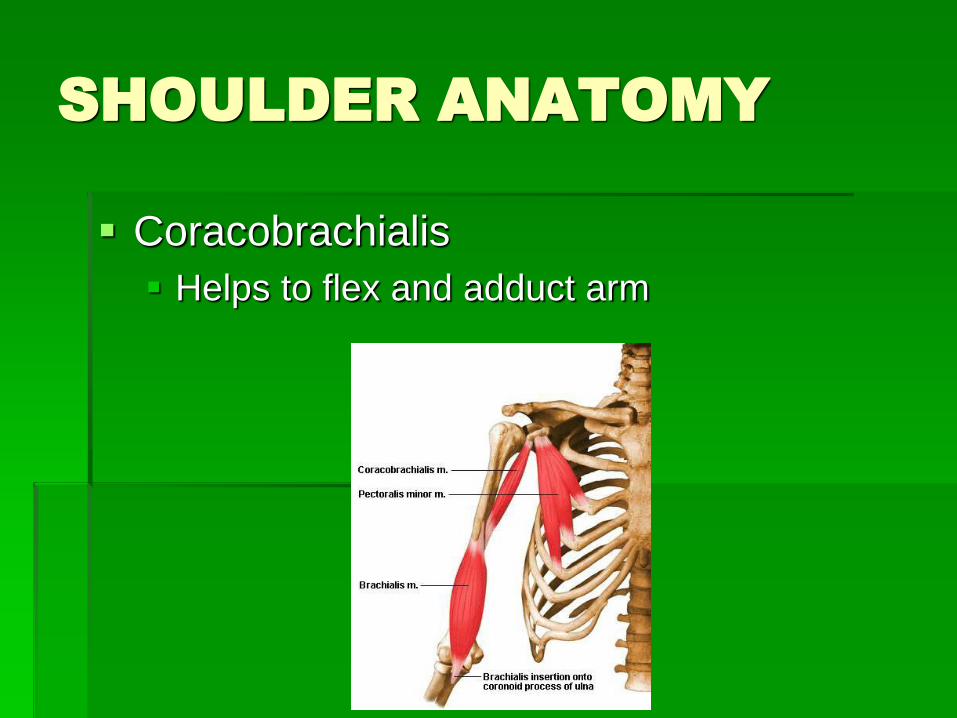
Coracobrachialis
Helps to flex and adduct arm
SHOULDER ANATOMY
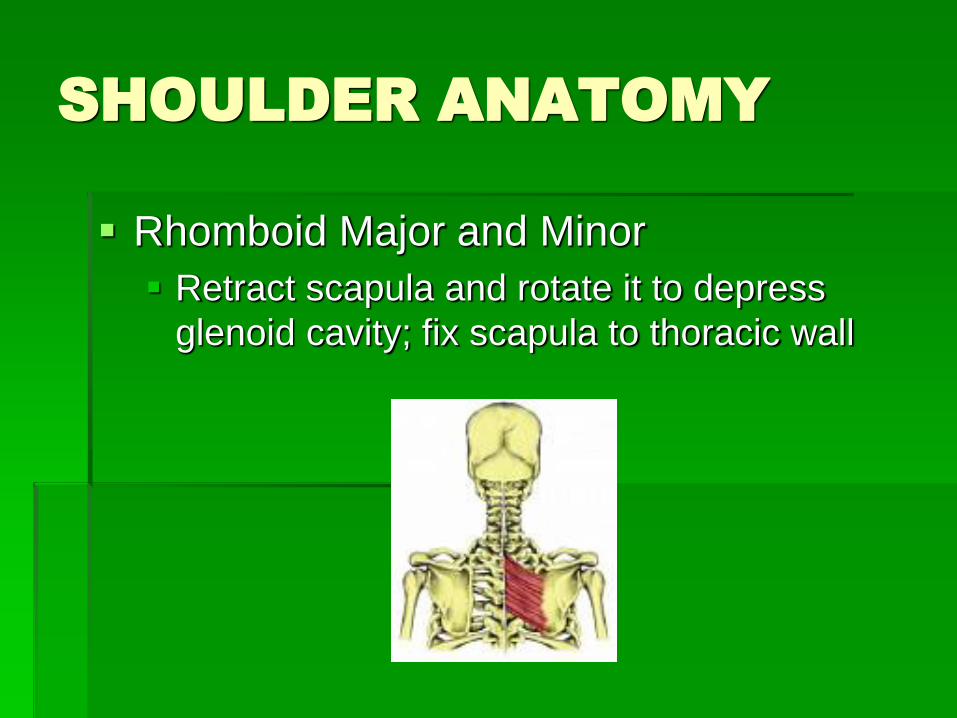
Rhomboid Major and Minor
Retract scapula and rotate it to depress
glenoid cavity; fix scapula to thoracic wall
SHOULDER ANATOMY
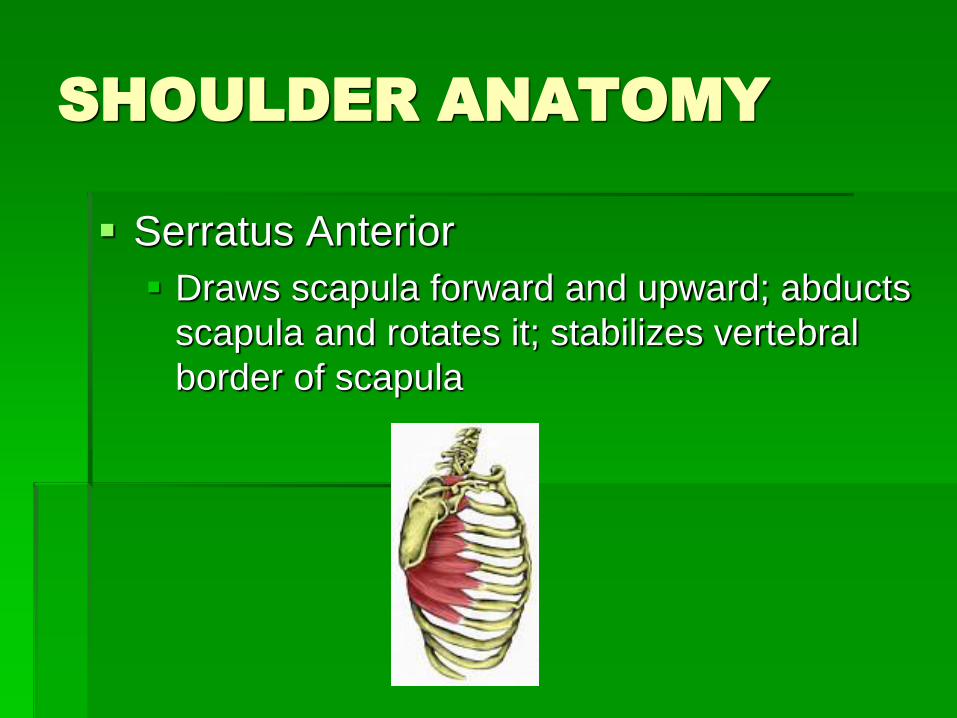
Serratus Anterior
Draws scapula forward and upward; abducts
scapula and rotates it; stabilizes vertebral
border of scapula
SHOULDER ANATOMY
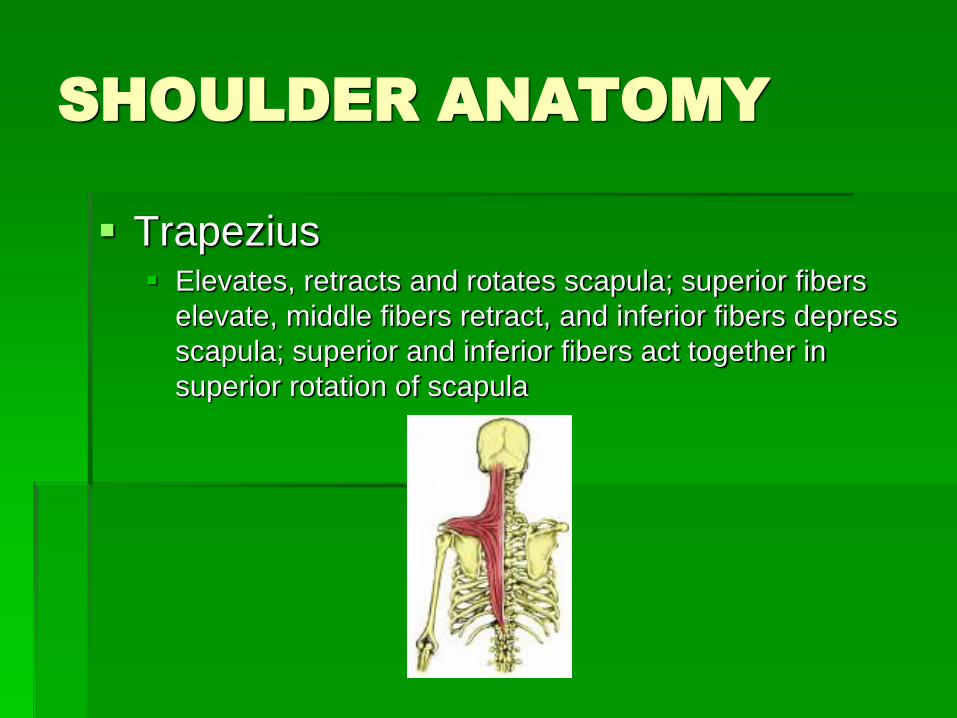
Trapezius Elevates, retracts and rotates scapula; superior fibers
elevate, middle fibers retract, and inferior fibers depress
scapula; superior and inferior fibers act together in
superior rotation of scapula
SHOULDER ANATOMY
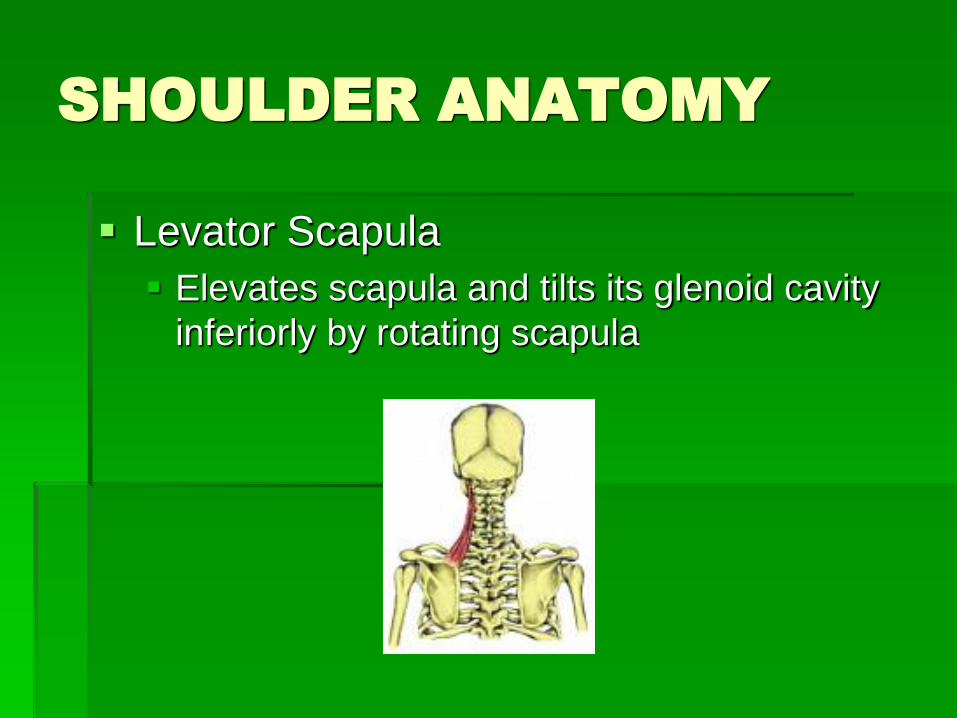
Levator Scapula
Elevates scapula and tilts its glenoid cavity
inferiorly by rotating scapula
CLAVICLE AND SCAPULA
Things you may or may not know
Very important to address when
addressing the shoulder
May be the primary reason limiting the
shoulder
CLAVICLE
Looking from the front, the medial 2/3 is convex and lateral 1/3 is concave- only long bone that is horizontal in the body
Acts as a “strut” to hold the arm away from the body and allows space for veins and nerves
Muscles/Ligament attached: Trapezius muscle
Deltoid Muscle
Coracoclavicular ligament
Sternocleidomastoid muscle
Pectoralis major muscle
Subclavius muscle
CLAVICLE
Sternoclavicular (SC) Joint Structure
Articulation of clavicle with the sternum
Only direct attachment of the upper extremity to the skeleton
Clavicle moves in 3 planes (3 degrees of freedom) Elevation and Depression of SC
Protraction and retraction of SC
Axial Rotation of clavicle
All shoulder girdle movements start at the SC joint, if it is fused not only the clavicle and scapula would be limited but the entire shoulder!
CLAVICLE
The Acromioclavicular Joint (AC) allows motion in all 3 planes, allowing the scapula to maintain contact with the posterior thorax:
Upward rotation and downward rotation
Rotation in the horizontal plane
Rotation in the sagittal plane
Acromioclavicular Ligament
Joins clavicle to acromion, prevents dislocations of the scapula
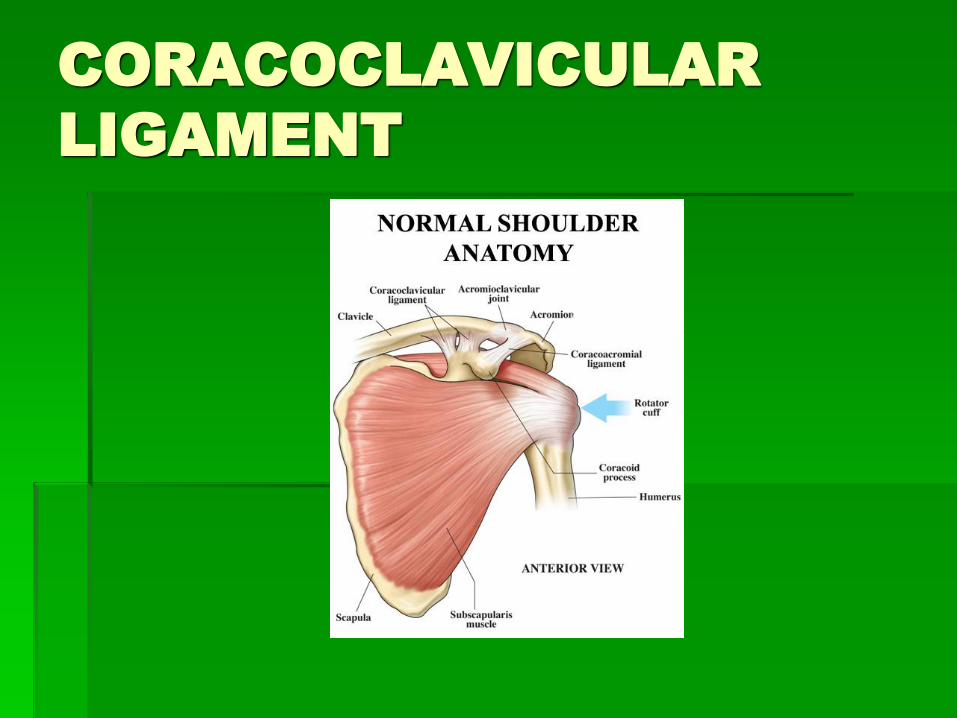
CORACOLCLAVICULAR
LIGAMENT
Attaches twice on clavicle and the
coracoids process of scapula
It is responsible for bearing most of the
weight of the hanging arm. Without this
ligament, the arm is unable to hang from
the body
CORACOCLAVICULAR
LIGAMENT
SCAPULA
The scapula is only attached to the thorax by ligaments at the AC joint
suction mechanism provided by serratus anterior
subscapualaris
Main stabilizers of the scapula: Serratus anterior
Rhomboid major and minor
Levator scapulae
Trapezius
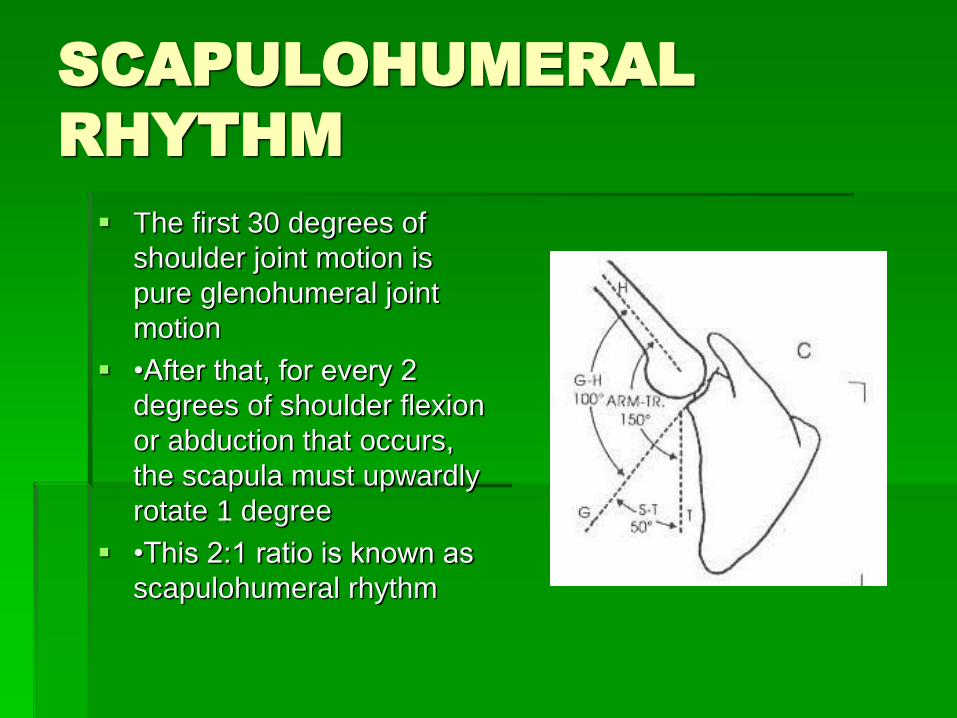
SCAPULOHUMERAL
RHYTHM
The first 30 degrees of
shoulder joint motion is
pure glenohumeral joint
motion
•After that, for every 2
degrees of shoulder flexion
or abduction that occurs,
the scapula must upwardly
rotate 1 degree
•This 2:1 ratio is known as
scapulohumeral rhythm
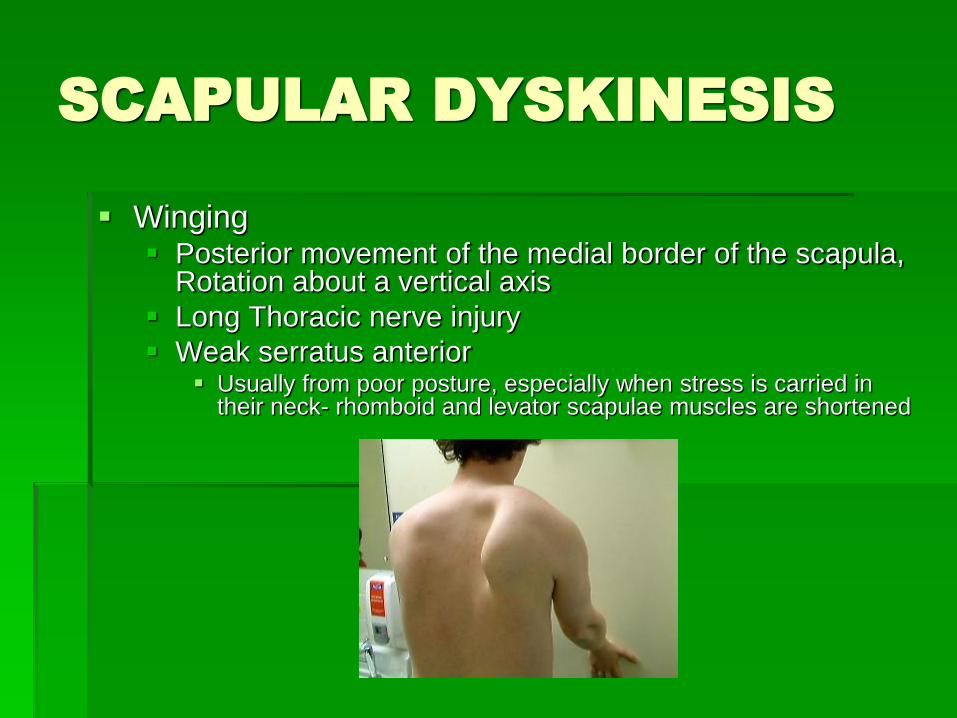
SCAPULAR DYSKINESIS
Winging Posterior movement of the medial border of the scapula,
Rotation about a vertical axis
Long Thoracic nerve injury
Weak serratus anterior Usually from poor posture, especially when stress is carried in
their neck- rhomboid and levator scapulae muscles are shortened
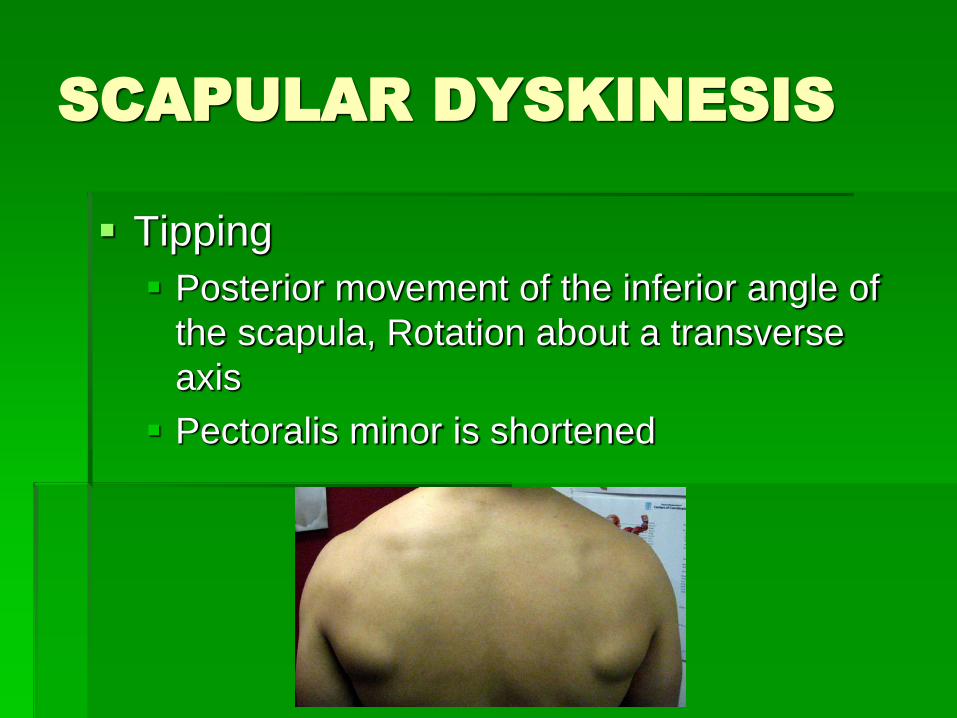
SCAPULAR DYSKINESIS
Tipping
Posterior movement of the inferior angle of
the scapula, Rotation about a transverse
axis
Pectoralis minor is shortened
RELAX
You made
It though
The hard
Part
SHOULDER POSITION
Different for everyone
Side view, ears should be in alignment
with shoulders
Shoulders should be in alignment with
hips
May not be able to achieve due to
bony/soft tissue changes and congenital
deformities
SHOULDER
POSITION/PHYSICS
Levers
The humerus is a complicated class 3 lever when
the elbow is straight. (Reminder on a class 3 lever:
Effort is in the middle (muscle): the resistance is on
one side of the effort (whatever a person is lifting)
and the fulcrum is located on the other side
(shoulder girdle))
Fulcrum is set best when the shoulder girdle is at
neutral. When shoulder girdle is no longer at
neutral, the “lever” loses effectiveness
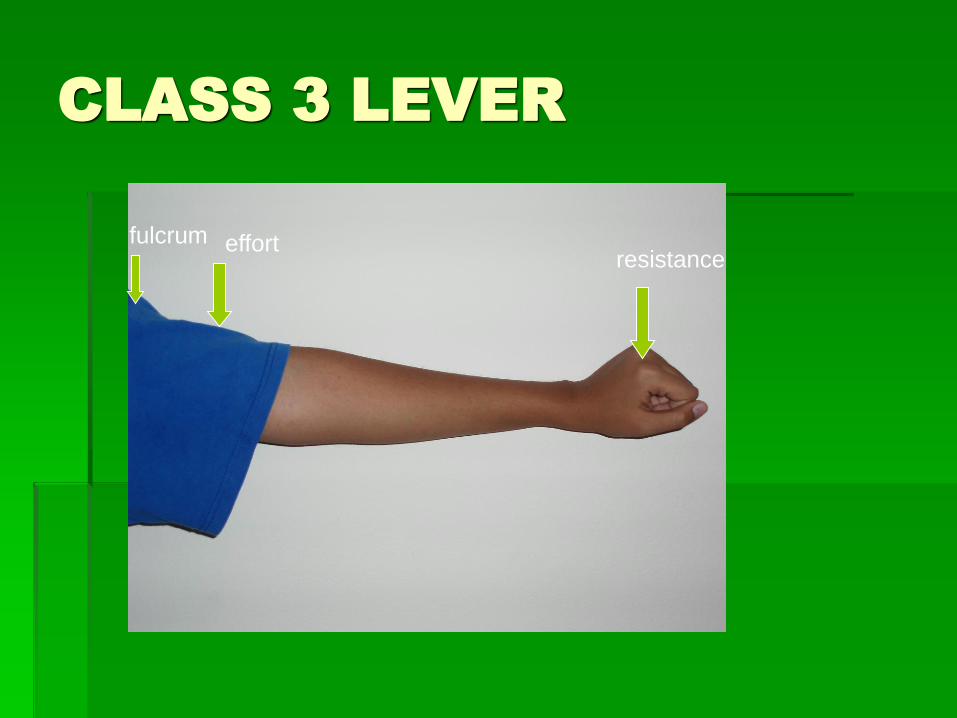
CLASS 3 LEVER
fulcrum effort resistance
EVALUATION IS
IMPORTANT
This will mostly design how the person is treated
In my experience, most people do not have
optimal strength unless they have over 150
degrees of shoulder flexion without
compensation
Most people are upwardly rotated and abducted
Pain-where is it specifically?
Additional extension, limited internal and/or external
rotation
COMPENSATION
When a person has lost range of motion,
they learn to compensate
The job must be done!!!!
Compensatory patterns will give you
clues as to areas that need to be
addressed
TYPICAL COMPENSATION
PATTERNS
Shoulder flexion- abduction of the
shoulder, lordosis of cervical/thoracic
spine
Shoulder abduction- lateral flexion of
torso/spine, shoulder flexion, protraction
of scapula
TYPICAL COMPENSATION
PATTERNS
Shoulder internal rotation- protraction of
scapula, rotation of trunk, kyphosis of
thoracic/cervical area
Shoulder external rotation- retraction of
scapula, rotation of trunk, lordosis of
thoracic/cervical area
ASSESSING RANGE OF
MOTION
How is reduced shoulder ROM limiting
ADL’s
Limited shoulder flexion: brushing/washing
hair, donning/doffing shirt/jacket, reaching
into cabinet
Limited horizontal adduction:
Donning/doffing clothing, hair care, kitchen
tasks, peri care
ASSESSING RANGE OF
MOTION
Limited internal rotation: washing back,
hooking bra, pulling up pants, peri
care, cooking, mowing the
lawn/starting mower
Limited external rotation: brushing
teeth, brushing/washing hair, using a
walker, cooking
ASSESSING RANGE OF
MOTION
Is functional ROM causing deformity?
Does that person really have functional
movement?
Need to look at the entire body
Watch for compensatory movement
Look for pain cues (wincing, grunting, etc.)
ASSESSING RANGE OF
MOTION
Where is the block? Eg. Shoulder flexion
Look at straight flexion without allowing any other movement, you will feel a slight “stop” in the movement if there is a restriction
Where is the compensatory movement?
Limited shoulder flexion can cause compensation Cervical, thoracic, lumbar vertebrae
Spillover into abduction and external rotation
ASSESSING RANGE OF
MOTION
Long term effects Pain
Arthritis
Impingement
Decreased strength
Destruction of structures of the shoulder
Biceps
Coracobrachialis
Ultimately loss of function

TREATMENT FOR
SCAPULAE
Mostly upwardly rotated and abducted
Mobilizations and soft tissue release
We must… and scapular squeeze
Tell person to try to touch shoulder
blades together and towards bottom

AIR SPLINT
AIR SPLINT
CONTRAINDICATIONS
ANY ROM RESTRICTIONS
BACK/SHOULDER/CLAVICLE/ARM FRACTURES
DIALYSIS PORTS
PICC LINES
POOR ARTERIAL/VENOUS FLOW TO ARM/DVT
AIR SPLINT CONCERNS/
CONSIDERATIONS
Recent fractures
Cardiac history
Osteoporosis
Muscle tears
Pain tolerance
Recent back
surgeries
Vascular issues
Skin integrity
IV’s
Contractures
Mastectomy/
Lumpectomy
Severe arthritis
AIR SPLINT EXERCISES
Please see additional handout
Works better initially in supine, gravity pulls shoulder into a more neutral position breaking habitual pattern of kyphosis and other compensatory patterns
Can use towel for better positioning or to grade activity
Move into sitting once patient’s shoulder girdle becomes more stable
MOBILIZATIONS
PRECAUTIONS AND
CONTRAINDICATIONS
Any condition that has not been fully evaluated
Joint ankylosis
Joint hypermobility, if techniques that take the joint through its end range are being considered, unless a positional fault is being treated
Joints that are infected
Malignancy in area treated
Fractures
Inflammatory arthritis, especially if it is exacerbated
Metabolic bone diseases (Paget’s, TB, etc)
Debilitating diseases that compromise periarticular tissue (advanced DM)
Long term use of corticosteroids
Swelling- it takes up some of the slack in the capsule making it difficult to evaluate the joint mobility correctly
Excessive joint irritability or pain
Coagulation impairments
Skin rashes or open/healing skin lesions
Protective muscle spasms to the point mobility in the area treated is unable to be evaluated
MOBILIZATIONS
Joint mobilizations are used when
ligament or capsule resistance is
encountered
Many different ones to use
See sheet for helpful ones
Thank you!!!!!
Many thanks to those who helped me:
Heather Barnes, OTR/L
Terry Giese, OTR/L
Nancy Joneth, OTR/L
Howard Whitfield, OTR/L
Scott McKay, PAC
Chad Randolph, PT
Tim Kisner, PT
My model: Beth Kohler-Rausch, OTR/L
My Photographers: Diwi Ymson, PT and Tanvi Desai, OTR/L





![In shoulder adhesive capsulitis, ultrasound-guided anterior ......articular pressure and increase the shoulder volume capacity [10]. That is why the capsular distension was used for](https://img.pdfslide.us/doc/110x75/5f788a6aa1cd42247e3c5e91/in-shoulder-adhesive-capsulitis-ultrasound-guided-anterior-articular-pressure.jpg)