Embed Size (px)
DESCRIPTION
Using Health Services. Perceiving and Interpreting Symptoms. Our perceptions are not very accurate There are individual differences: Some people have more symptoms There are differences in what people can tolerate Differ in how much attention is paid to internal states - PowerPoint PPT Presentation
Citation preview

Using Health Services

Perceiving and Interpreting Symptoms
Our perceptions are not very accurate There are individual differences:
Some people have more symptoms There are differences in what people can
tolerate Differ in how much attention is paid to
internal states Internally focused people overestimate
bodily changes and experience slower recovery

Personality and Hypertension:Effect of Hypertension Awareness
0123456789
1011121314
Neuroticism
Aware HyperNormotUnaware HyperNormot
Aware hypertensive > normotensive & unaware hypertensive,P < 0.001

Personality and Hypertension:
Conclusion
Awareness of hypertension status confounds assessment of the association between personality characteristics and hypertension.
Due to hypertension labeling effect; or
Due to self-selection bias

Perceiving and Interpreting Symptoms
Our perceptions are not very accurate There are individual differences:
Some people have more symptoms There are differences in what people can
tolerate Differ in how much attention is paid to
internal states Internally focused people overestimate
bodily changes and experience slower recovery
Symptoms Awareness Background stress is associated with
greater reports of symptoms Mood - positive mood associated
with fewer symptom reports than negative mood.

Expectations Prior experience, beliefs, and
knowledge influence expectations about symptoms. Ignore unexpected symptoms and
amplify expected symptoms Beliefs about the disease label, causes,
time course, and consequences influence symptom awareness and experience.
Placebos Inert substance or treatments
People can experience real symptom relief.
Furthermore taking placebos faithfully is associated with a lower likelihood of death.

Adherence with Medication
Adherent > = 66% of pills takenPoorly adherent 66% of pills takenRR = 2.11, 95% CI, 1.03-4.56, p < .05
Adherent >= 66% of pills takenPoorly adherent < 66% of pills takenRR=3.15, 95% CI, 1.34-7.44, p < .01
Placebo Group Amiodarone Group
Risk of Sudden Cardiac Death
Survival Time in Days
8006004002000
Cum
ulat
ive
Sur
viva
l
1.00
.98
.96
.94
.92
.90
Adherent
Poorly Adherent
Risk of Sudden Cardiac Death
Survival Time in Days
8006004002000
Cum
ulat
ive
Sur
viva
l
1.0
.9
.8
.7
Adherent
Poorly Adherent

Medical student’s disease - Studying symptoms leads to
greater focus on one’s own symptoms (e.g., of fatigue) that then get interpreted as indicative if disease.
Mass Psychogenic Illness Widespread symptom perception
among a large group of individuals, without any evidence for physical or environmental cause.
Factors contributing to this effect are: Cognitive exaggeration of common
symptoms Modeling Emotional distress (e.g., anxiety)
Cultural Factors
Social-cultural influences shape how one appraises and responds to physical symptoms.
Help-Seeking – Lay Referral Network Help interpret a symptom Give advice about seeking medical
attention Recommend a remedy Recommend consulting another
kay referral person
Who Uses Health Services? Age: young children and elderly
use more Gender: women use more Sociocultural: use increases with
income

Why People Don’t Use Health Services Iatrogenic conditions: medical
problems resulting from a practitioner’s error or as a normal side effect of treatment.
Not trusting practitioners Worry about confidentiality Worry about discriminatory practices

Why People Don’t Use Health Services Emotional factors:
fear of serious disease embarrassment
Social factors Not wanting to appear weak More likely to use health care system
if lay referral system encourages it

Factors influencing how people cope with health anxiety
68
70
72
74
76
78
80
82
84
Pre-info Post-info Post-exam
Blunters, high info
Blunters, low info
Monitors, highinfoMonitors, low info

Mulitvariate Predictors of Non - Adherence to Ovarian Cancer Screening
Immediate PostClinic RiskPerception
OddsRatio
95% CI P value
High vs. low 0.23 0.06 – 0.81 .03
High vs. medium 0.23 0.07 – 0.73 .01
Medium vs. low 0.99 0.32 – 3.03 .99
High RP group is 4.3 times less likely to adhere than low RP.High RP group is also 4.3 times less likely to adhere than medium.There was also a trend for high worry (p = .057) and low adaptive coping (p = .059) to be predictive of non-adherence.
Misusing Health Care Services Hypochondriacs: people who tend
to interpret real but benign bodily sensations as symptoms of illness Associated with neuroticism Does not increase with age
The Patient/Practitioner Relationship People differ in the role they want
to play in their treatment Patients who take an active role
recover better and faster Practitioners differ in the level of
participation they are willing to give

What Happens When There is a Mismatch?
Although physicians and patients agree that patients should play a role, neither tends to act this way.
If the patient wants to participate and the practitioner doesn’t want them to, conflict will result.
If the practitioner wants the patient involvement but the patient doesn’t want to participate both are uncomfortable.
The Practitioner’s Behaviour
Physicians tend to use a consistent style. Two styles: Doctor-centered
Asks close-ended questions and focuses on first problem mentioned.
Ignores attempts to discuss other problems Patient-centered
Asks open-ended questions and allows discussion Avoids jargon and encourages participation in
decisions

Medical Terms Meaning – Match terms to meanings
Antibiotics Breech Enamel Glucose Mucus Suture Protein Umbilicus
1. A hard glossy coating2. The rump or back part3. Agent to treat bacteria4. Secretion of body tissues5. Sugar produced by the body 6. The navel7. A device to join separated
tissue or bone8. Substance that makes up
plant or animal tissue

Why Physicians Use Jargon Habit Patient doesn’t need to know Patient better off not knowing Keep interactions short Reduce emotional reactions Reduce recognition of errors Elevate practitioner’s status Not aware of jargon

What to we want in a doctor?
Competency Expertise Concern, warm, sensitivity How do “good” doctors benefit?
Patient is more adherent to treatment Obtain more extensive diagnostic
information

The Patient’s Behaviour that Upsets the Doctor
Expressing anger or criticism Ignoring or not listening Insisting on procedures the physician
thinks is not necessary Requesting the doctor certify
something he/she does not think is true (e.g., disability)
Sexually suggestive remarks

How do patients impair communications?
Not indicating distress
Poor communication of symptoms
Why do people describe their symptoms differently?
Symptom perception and interpretation
Differing common sense models of illness
Emphasizing or down-playing symptoms
Difficulties in communicating (e.g., language)

Compliance Adherence Concordance
Degree to which the patient carries out the behaviours the physician recommends (e.g., taking medication).

Extent of non-adherence problem
Difficulties with assessing it: Many different kinds of medical advice
to which one could adhere Can violate advice in many different
ways Difficult to know if patient complied
(50/50 chance that the physician’s judgment of the patient’s adherence is accurate).

Adherence
60% of patients may not be adhering to long-term treatment regimen 1-2 years later
even in cardiac patients medication adherence over time is poor (i.e., 40% nonadherent 3 years later)
Good predictor of long-term adherence is adherence at entry
Distribution of adherence is tri-modal
Distribution of AdherenceAdherent Partial Adherent Non-adherent
1/3
1/31/3
Measuring Adherence in Clinical Practice
Physician impression overestimates patient-adherence by about 50% (Caron, 1985).
Electronic monitors of pills taken are impractical in routine clinical practice.
Bio-chemical measures also have limitations Self-report methods are good at detecting
those who admit to adherence difficulties but will miss-classify about 50% patients who deny problems or who are unaware of a problem.

Forms of Non-Adherence Forgetting a dose Deliberately skipped doses Occasional day or even week off
therapy Stopped therapy

Patients’ Reasons for Not Adhering
Forgetfulness (e.g., restaurant, trip) Financial (wait until pay day, take 1/2
dose to delay renewing prescription) Feeling sick Feel well (rare reason) Lazy about going to the drug store Too busy - forget Life events, stress (e.g., death in family) Don’t believe in the treatment Confused about dosage

Rational Reasons for Non-adherence
Have reason to believe the treatment isn’t working
Feel that side-effects are not worth the benefits of treatment
Don’t have enough money to pay for treatment
Want to see if the illness is still there when they stop the treatment
Non-adherence: Characteristics of the regimen Complex regimens have low
adherence Adherence decreases with duration
of the regimen Expense decreases adherence

Non-adherence: Cognitive-Emotional Factors
Patients forget much of what the doctor tells them
Instruction and advice are forgotten more readily than other kinds of information
The more patient is told, the higher the likelihood of forgetting more.
Patients remember what they are told first and what they think is most important.

Non-adherence: Cognitive-Emotional Factors
More intelligent patients do not remember more than less intelligent patients
Older patients remember as much as younger patients
Moderately anxious recall more than low or high anxious patients
The more medical knowledge the patient has, the more he/she will remember.

Non-Adherence: Psychosocial Factors
Social support Personality - Dispositional
Attitudes Affective State Knowledge and attitudes

Non-Adherence: Knowledge/Beliefs
Lack of knowledge Denial or trivialization Perceived invulnerability
Necessary but not sufficient

Non- Adherence - Behaviour
Early adherence, e.g., within first month of initiating therapy is an excellent predictor of later adherence, even 7 years later (Dunbar & Knoke, 1986)
The more similar the predictor behaviour to the predicted behaviour, the higher the correlation.
Generally, little evidence for a health-oriented behaviour pattern.

Donald E. Morisky’s Questions
1. Do you ever forget to take your medicine?2. Are you careless at time about taking your
medicine?3. When you feel better do you sometimes
stop taking your medicine?4. Sometimes if you feel worse when you take
the medicine, do you stop taking it? High adherence = all ‘no’ responses Medium adherence = 1 or 2 ‘yes’ responses Low adherence = 3 or 4 ‘yes’ responses

Brian Haynes’ Question People often have difficulty taking their
pills for one reason or another and we are interested in finding out any problems that occur so that we can understand them better.
Do you ever miss your pills? If yes What is the average number of tablets
missed per day, week, and month? Adherence defined as taking >= 90% of
pills prescribed.
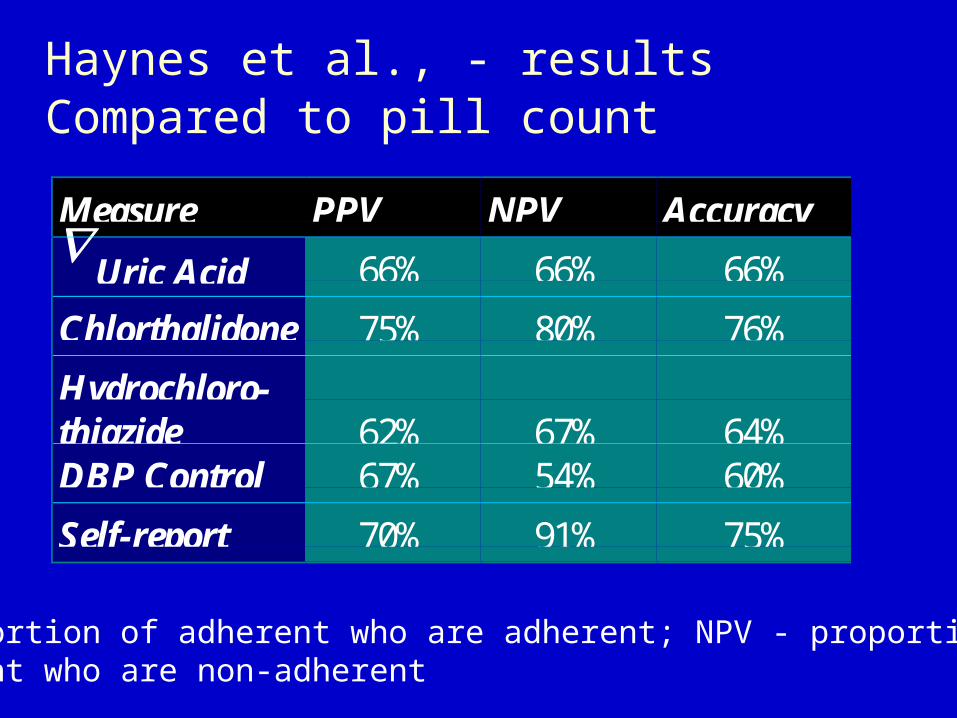
Haynes et al., - results Compared to pill count
Measure PPV NPV Accuracy Uric Acid 66% 66% 66%
Chlorthalidone 75% 80% 76%
Hydrochloro-thiazide 62% 67% 64%DBP Control 67% 54% 60%
Self-report 70% 91% 75%
PPV - proportion of adherent who are adherent; NPV - proportion ofnon-adherent who are non-adherent
Increasing Patient Adherence Use clear (jargon free) sentences Repeat key information Recruit sources of support Tailoring the regimen Providing prompts and reminders Self-monitoring Behavioural contracting