Embed Size (px)
Citation preview

Using Using EMRsEMRs to Improve to Improve Patient CarePatient Care
Lee Ferguson, MDLee Ferguson, MDActing Associate Chief of Staff for Ambulatory CareActing Associate Chief of Staff for Ambulatory Care
Department of Veterans Affairs Department of Veterans Affairs Medical CenterMedical Center
Washington, DCWashington, DC

2005: Who is 2005: Who is ““VAVA””??Veterans Health AdministrationVeterans Health AdministrationVHA is an Agency of the Department of Veterans AffairsVHA is an Agency of the Department of Veterans Affairs
LocationsLocations~ 1,300 Sites ~ 1,300 Sites –– of of –– Care Care Including 157 medical centers, ~ 850 clinics, Including 157 medical centers, ~ 850 clinics, longlong--term care, term care, domiciliariesdomiciliaries, home, home--care programscare programs
AffiliationsAffiliationsAffiliations with 107 Academic Health SystemsAffiliations with 107 Academic Health SystemsAdditional 25,000 affiliated MDAdditional 25,000 affiliated MD’’ssAlmost 80,000 trainees each yearAlmost 80,000 trainees each year60% (70% MDs) US health professionals have 60% (70% MDs) US health professionals have some training in the VAsome training in the VA
Washington, DC VAMCWashington, DC VAMC

Electronic record:Electronic record:Available at >1900 sites in hospitalAvailable at >1900 sites in hospital
Easy to shareEasy to shareCannot be misplacedCannot be misplaced
Available at 4 surrounding Available at 4 surrounding Community Based Outpatient Community Based Outpatient ClinicsClinicsDedicated on site IRM staff for 24/7 Dedicated on site IRM staff for 24/7 service of the EMR, training, and service of the EMR, training, and generation of data reportsgeneration of data reports
Washington DC VAMCWashington DC VAMC
Washington, DC VAMCWashington, DC VAMC
Praise for VistAPraise for VistA……
““VHAVHA’’s integrated health information system, s integrated health information system, including its framework for using performance including its framework for using performance measures to improve quality, is considered one of measures to improve quality, is considered one of the best in the nation.the best in the nation.””
Institute of Medicine (IOM) Report, Institute of Medicine (IOM) Report, ““Leadership by Example: Leadership by Example: Coordinating Government Roles in Improving Health Care Quality Coordinating Government Roles in Improving Health Care Quality
(2002)(2002)””

““The Electronic Health Record in the Department The Electronic Health Record in the Department of Veterans Affairs is the best in the United States, of Veterans Affairs is the best in the United States, absolutely the best at large scale, and probably the absolutely the best at large scale, and probably the best in the world.best in the world.””
John Glaser, Ph.D., October 2003John Glaser, Ph.D., October 2003Vice President & CIOVice President & CIO
Partners (Harvard) HealthCare SystemPartners (Harvard) HealthCare System
(Still More) Praise . . .(Still More) Praise . . .

Highest Quality of Care For Highest Quality of Care For Patients in VA Measured Patients in VA Measured
BroadlyBroadly““Patients from the VHA received higherPatients from the VHA received higher--quality quality care according to a broad measure. Differences care according to a broad measure. Differences were greatest in areas where the VHA has were greatest in areas where the VHA has established performance measures and actively established performance measures and actively monitors performance.monitors performance.””
Annals of Internal Medicine, December 21, 2004Annals of Internal Medicine, December 21, 2004

Clinical IndicatorClinical Indicator VA 2003VA 2003 Medicare 03Medicare 03 Best Not VA or MedicareBest Not VA or MedicareAdvised Tobacco Cessation (VA x3, others x1)Advised Tobacco Cessation (VA x3, others x1) 7575 6262 68 (NCQA 2002)68 (NCQA 2002)
Beta Blocker after MIBeta Blocker after MI 9898 9393 94 (NCQA 2002)94 (NCQA 2002)
Breast Cancer ScreeningBreast Cancer Screening 8484 7575 75 (NCQA 2002)75 (NCQA 2002)
Cervical Cancer ScreeningCervical Cancer Screening 9090 6262 81 (NCQA 2002)81 (NCQA 2002)
Cholesterol Screening (all pts)Cholesterol Screening (all pts) 9191 NANA 73 (BRFSS 2001)73 (BRFSS 2001)
Cholesterol Screening (post MI)Cholesterol Screening (post MI) 9494 7878 79 (NCQA 2002)79 (NCQA 2002)
LDL Cholesterol <130 post MILDL Cholesterol <130 post MI 7878 6262 61 (NCQA 2002)61 (NCQA 2002)
Colorectal Cancer ScreeningColorectal Cancer Screening 6767 NANA 49 (BRFSS 2002)49 (BRFSS 2002)
Diabetes Hgb A1c checked past yearDiabetes Hgb A1c checked past year 9494 8585 83 (NCQA 2002)83 (NCQA 2002)
Diabetes Hgb A1c > 9.5 (lower is better)Diabetes Hgb A1c > 9.5 (lower is better) 1515 NANA 34 (NCQA 2002)34 (NCQA 2002)
Diabetes LDL MeasuredDiabetes LDL Measured 9595 8888 85 (NCQA 2002)85 (NCQA 2002)
Diabetes LDL < 130Diabetes LDL < 130 7777 6363 55 (NCQA 2002)55 (NCQA 2002)
Diabetes Eye ExamDiabetes Eye Exam 7575 6868 52 (NCQA 2002)52 (NCQA 2002)
Diabetes Kidney FunctionDiabetes Kidney Function 7070 5757 52 (NCQA 2002)52 (NCQA 2002)
Hypertension: BP Hypertension: BP << 140/90140/90 6868 5757 58 (NCQA 2002)58 (NCQA 2002)
Influenza ImmunizationInfluenza Immunization 7676 PP 68 (BRFSS 2002)68 (BRFSS 2002)
PneumocooccalPneumocooccal ImmunizationImmunization 9090 PP 63 (BRFSS 2002)63 (BRFSS 2002)
Mental Health F/U 30 D post D/CMental Health F/U 30 D post D/C 7777 6161 74 (NCQA 2002)74 (NCQA 2002)
VA Sets the U.S. Benchmark18 Comparable Indicators
Washington, DC VACOWashington, DC VACO

VHAVHA’’ss electronic record electronic record includes:includes:
• Computerized Patient Record System (CPRS)-basic EMR framework
• VistA Imaging-static and real time imaging/document scanning functionality
• My HealtheVet-veteran’s personal health record accessible from home
• Remote Data/VistA Web-access data from outside individual medical center
• Bar Code Medication Administration (BCMA)-inpatient medication administration software

Computerized Patient Record Computerized Patient Record System (CPRS)System (CPRS)
• Windows based GUI software that overlies VistAdatabase
• Clinical enduser is able to: – Review and enter progress notes– Review and enter procedure notes/operative
notes/discharge summaries– Review, order, adjust medications– Review and order labwork/imaging studies– Order consultations with specialists– Access remote views/VISTA web

The The ““gapgap”” between best between best practices and actual practicespractices and actual practices
• It is widely known and accepted that certain interventions after a myocardial infarction (“heart attack”) reduce complications and prolong life.
• Actual implementation of these “standard” therapies fall far below expected levels of use
• For example, aggressive monitoring of cholesterol after a myocardial infarction is a “no brainer”, with accepted target goals for lowering levels of LDL “bad” cholesterol
• Best practice outside VHA as recently as 2003 reveal only 79% had cholesterol levels checked (VHA was 94%)!

Why does this happen?Why does this happen?
• The reality of modern medical practice is that an older, more complicated patient population is living during a time of an ever increasing number of beneficial therapies, which is superimposed on a reimbursement system which puts pressure to minimize the time allotted between patient and care provider.
• The bottom line: leaving it to even the best trained, well intentioned physicians to remember and review everything is a losing position.

EMRsEMRs help close the help close the ““gapgap””between best practices and between best practices and
actual practicesactual practices
EMR: Improving Patient CareEMR: Improving Patient Care
• Two perspectives– Individual patient interactions-how can an EMR
improve the care of a patient sitting right in front of me?
– Aggregate care of a community-how can an EMR improve the care of a large population of patients?
“Micro and macro” views are mutually reinforcing

EMR role in improving EMR role in improving individual patient careindividual patient care
• Formatted note templates that display patient specific problem lists, allergies, and recent lab data
• Time savings/elimination of redundant care through – order entry of labs/images/medications– review of past appointments/consultants reports– test results/imaging availability
• MyHealtheVet• Vista Web remote access data retrieval• Clinical reminders

Order XOrder X--rayray
Washington, DC VAMCWashington, DC VAMC

Images Images –– Chest XChest X--rayray
Washington, DC VAMCWashington, DC VAMC

GREEN, DEAN (100-10-1000)
Remote View – VistA Web

GREEN, DEAN (100-10-1000)
Remote View Remote View –– VistA WebVistA Web

GREEN, DEAN (100-10-1000)
Remote View – VistA Web

My HealtheVetMy HealtheVet
Vista extracts sent toMy HealtheVet account• Demographics,
admissions, and appointments
• Vitals and allergies• Prescriptions• Progress notes• Discharge summaries• Problem list • Lab reports: chemistry,
microbiology, microscopy, cytology and pathology
• ECG and radiology reports
Washington, DC VAMCWashington, DC VAMC

5 self-entered metrics (e-logs)
• Blood pressure • Blood sugar• Cholesterol• Weight• Heart rate
Ability to create self -defined e-logs
My HealtheVet: Home MetricsMy HealtheVet: Home Metrics
Washington, DC VAMCWashington, DC VAMC

My Blood Pressure Log My Blood Pressure Log (Self(Self--entered)entered)

My HealthMy HealtheeVetVet

Clinical RemindersClinical Reminders
Contemporary Contemporary Expression of Expression of Practice GuidelinesPractice Guidelines
•• Time & Time & Context Context Sensitive Sensitive
•• Reduce Reduce Negative Negative VariationVariation
•• Create Create Standard DataStandard Data
•• Acquire health Acquire health data beyond data beyond care delivered care delivered in VAin VA

Clinical remindersClinical reminders

Clinical remindersClinical reminders

Power of clinical remindersPower of clinical reminders• Do the right thing in the right patient at the right time
– Avoid missed treatment– Avoid wasted time confirming issues that are
already dealt with• Gain clinician confidence that the reminders will let
them know when something is due• Produce “reminder reports” for feedback to
individuals, groups, institutions

EMR role in improving the care EMR role in improving the care of a populationof a population
• Different tools are available to identify problem areas, monitor progress over time, and compare to performance between individuals/groups– VistA data extracts– Clinical reminder reports

00
2020
4040
6060
8080
100100
Perc
ent P
atie
nts
Perc
ent P
atie
nts
00
2020
4040
6060
8080
100100
Blood PressureBlood PressureBalt
imore
Baltim
oreBalt
imore
Baltim
ore
Martinsb
urg
Martinsb
urg
Martinsb
urg
Martinsb
urg
Washin
gton
Washin
gtonWas
hington
Washin
gton
VISN 5
VISN 5
VISN 5
VISN 5
LowLow MediumMedium HighHigh
12,38312,383 14,71014,710 8,9708,970 9,9389,938 9,9589,958 10,79810,798 31,31131,311 35,44635,446
Pts. with 3+ prior elevated BPs
Washington, DC VAMCWashington, DC VAMC

Analysis at 4 month IntervalAnalysis at 4 month IntervalBalt
imore
Baltim
oreMart
insburg
Martinsb
urgWas
hington
Washington
Baltim
ore
Baltim
oreMart
insburg
Martinsb
urgWas
hington
Washington
00
2020
4040
6060
8080
100100
Perc
ent o
f Pat
ient
sPe
rcen
t of P
atie
nts
September 20, 2001September 20, 2001 January 3, 2002January 3, 2002
00
2020
4040
6060
8080
100100
High(> 160 / 100 )
Moderate(140 - 159 / 90 - 99 )
Normal(< 140 / 90 )
Washington, DC VAMCWashington, DC VAMC
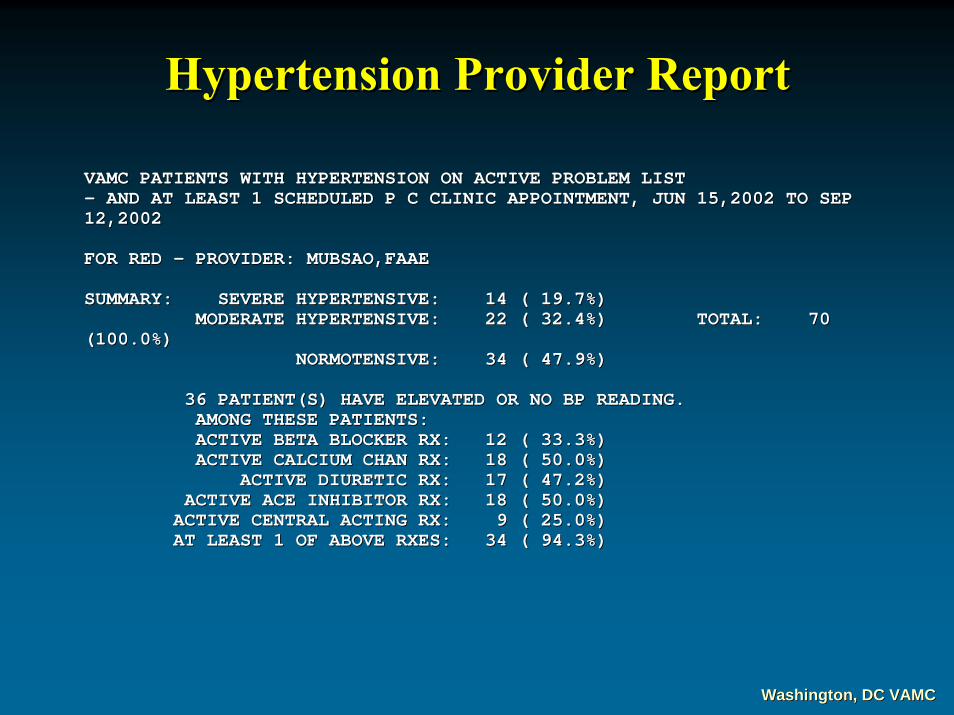
VAMC PATIENTS WITH HYPERTENSION ON ACTIVE PROBLEM LIST VAMC PATIENTS WITH HYPERTENSION ON ACTIVE PROBLEM LIST -- AND AT LEAST 1 SCHEDULED P C CLINIC APPOINTMENT, JUN 15,2002 TOAND AT LEAST 1 SCHEDULED P C CLINIC APPOINTMENT, JUN 15,2002 TO SEP SEP 12,2002 12,2002
FOR RED FOR RED -- PROVIDER: MUBSAO,FAAE PROVIDER: MUBSAO,FAAE
SUMMARY: SEVERE HYPERTENSIVE: 14 ( 19.7%) SUMMARY: SEVERE HYPERTENSIVE: 14 ( 19.7%) MODERATE HYPERTENSIVE: 22 ( 32.4%) TOTAL: MODERATE HYPERTENSIVE: 22 ( 32.4%) TOTAL: 70 70
(100.0%) (100.0%) NORMOTENSIVE: 34 ( 47.9%) NORMOTENSIVE: 34 ( 47.9%)
36 PATIENT(S) HAVE ELEVATED OR NO BP READING. 36 PATIENT(S) HAVE ELEVATED OR NO BP READING. AMONG THESE PATIENTS: AMONG THESE PATIENTS: ACTIVE BETA BLOCKER RX: 12 ( 33.3%) ACTIVE BETA BLOCKER RX: 12 ( 33.3%) ACTIVE CALCIUM CHAN RX: 18 ( 50.0%) ACTIVE CALCIUM CHAN RX: 18 ( 50.0%)
ACTIVE DIURETIC RX: 17 ( 47.2%) ACTIVE DIURETIC RX: 17 ( 47.2%) ACTIVE ACE INHIBITOR RX: 18 ( 50.0%) ACTIVE ACE INHIBITOR RX: 18 ( 50.0%)
ACTIVE CENTRAL ACTING RX: 9 ( 25.0%) ACTIVE CENTRAL ACTING RX: 9 ( 25.0%) AT LEAST 1 OF ABOVE RXES: 34 ( 94.3%) AT LEAST 1 OF ABOVE RXES: 34 ( 94.3%)
Hypertension Provider ReportHypertension Provider Report
Washington, DC VAMCWashington, DC VAMC

A. SEVERE HYPERTENSIVE: LAST BLOOD PRESSURE 160+ SBP AND/OR 100+A. SEVERE HYPERTENSIVE: LAST BLOOD PRESSURE 160+ SBP AND/OR 100+ DBP DBP
BETABETA-- CALCIUM DIURCALCIUM DIUR-- ACE CENTRAL ACE CENTRAL 44--DIG NAME || LAST BP DATE || BLOCK| CHANNEL| ETICS|INHDIG NAME || LAST BP DATE || BLOCK| CHANNEL| ETICS|INHIB| ACTING || HOMEIB| ACTING || HOME--PHONE P C APPTMENTS TO SEP 12: PHONE P C APPTMENTS TO SEP 12: ---------- ----------------------|| || --------------------------------|| || ----------| | -------------- | | ----------| | --------| | --------------|| || ------------------------ --------------------------------------------C0657 CEFHAK,PAAAF 169/80 ! 02/01/02 YES C0657 CEFHAK,PAAAF 169/80 ! 02/01/02 YES YES 589YES 589--744744--8276 JUN 25 RED SXGLWE 8276 JUN 25 RED SXGLWE P9461 PKYHMTA,OJEI 169/95!* 05/17/02 YES P9461 PKYHMTA,OJEI 169/95!* 05/17/02 YES YES 589YES 589--192192--0802 JUN 26 RED/RN WUKJWEAI 0802 JUN 26 RED/RN WUKJWEAI C2553 CEHUWOFP,TES 182/73 ! 06/12/02 YES YES C2553 CEHUWOFP,TES 182/73 ! 06/12/02 YES YES YES 589YES 589--378378--5339 AUG 26 RED ECLBA 5339 AUG 26 RED ECLBA H1312 HYFPIKBYS,CI 161/94!* 04/10/02 YES H1312 HYFPIKBYS,CI 161/94!* 04/10/02 YES 787787--506506--3987 JUN 24 RED ECLBA 3987 JUN 24 RED ECLBA L4563 LUFPIK,RIEMR 179/103!! 04/22/02 YES YES L4563 LUFPIK,RIEMR 179/103!! 04/22/02 YES YES YES NEED PHONE # JUL 1 RED ECLBA YES NEED PHONE # JUL 1 RED ECLBA G0172 GKAUS,SCURJ 168/108! 06/09/02 YES YES YES G0172 GKAUS,SCURJ 168/108! 06/09/02 YES YES YES YES 787YES 787--709709--7055 JUL 15 RED ANUFLVKW7055 JUL 15 RED ANUFLVKWG7306 GKYRNHO,SEMC 173/92!* 05/02/02 YES G7306 GKYRNHO,SEMC 173/92!* 05/02/02 YES YES YES 589YES YES 589--300300--5926 JUL 25 RED NYLEN 5926 JUL 25 RED NYLEN
B. MILD HYPERTENSIVE: LAST BLOOD PRESSURE 140B. MILD HYPERTENSIVE: LAST BLOOD PRESSURE 140--159 SBP AND/OR 90159 SBP AND/OR 90--99 DBP 99 DBP
BETABETA-- CALCIUM DIURCALCIUM DIUR-- ACE CENTRAL ACE CENTRAL 44--DIG NAME || LAST BP DATE || BLOCK| CHANNEL| ETICS|INHDIG NAME || LAST BP DATE || BLOCK| CHANNEL| ETICS|INHIB| ACTING || HOMEIB| ACTING || HOME--PHONE P C APPTMENTS TO SEP 12: PHONE P C APPTMENTS TO SEP 12: ---------- ----------------------|| || --------------------------------|| || ----------| | -------------- | | ----------| | --------| | --------------|| || ------------------------ --------------------------------------------G2650 GTAHS,AUAKAU 158/86 * 05/28/02 YES YES G2650 GTAHS,AUAKAU 158/86 * 05/28/02 YES YES YES 787YES 787--709709--9228 JUN 28 RED CREWOPTER 9228 JUN 28 RED CREWOPTER G3262 GKUZIJ,TUSAL 158/70 * 02/26/02 G3262 GKUZIJ,TUSAL 158/70 * 02/26/02 787787--166166--0314 JUL 22 RED CREWOPTER 0314 JUL 22 RED CREWOPTER S7865 SDASUKR,ADYL 142/70 * 04/08/02 YES S7865 SDASUKR,ADYL 142/70 * 04/08/02 YES YES 787YES 787--246246--8370 JUL 8 RED ECLBA 8370 JUL 8 RED ECLBA C8274 CEZMN,GUI 153/88 * 07/05/01 C8274 CEZMN,GUI 153/88 * 07/05/01 NEED PHONE # JUL 16 RED SXGLWE NEED PHONE # JUL 16 RED SXGLWE E4057 ECEHN,AOMYFU 149/84 * 06/13/02 YES E4057 ECEHN,AOMYFU 149/84 * 06/13/02 YES 787 224787 224--0778 JUN 18 RED0778 JUN 18 RED--HOLLAND HOLLAND J4264 JENHNEF,FMAL 140/64 * 06/03/02 YES YES J4264 JENHNEF,FMAL 140/64 * 06/03/02 YES YES YES 787YES 787--363363--9064 JUL 29 RED SXGLWE 9064 JUL 29 RED SXGLWE J7961 JENHNEF,NEGY 149/72 * 01/28/02 YES YES J7961 JENHNEF,NEGY 149/72 * 01/28/02 YES YES 589589--605605--7604 JUN 17 RED ANUFLVKW 7604 JUN 17 RED ANUFLVKW P6558 POOHI,LIZYB 159/81 * 06/12/02 YES YES YES P6558 POOHI,LIZYB 159/81 * 06/12/02 YES YES YES YES 787YES 787--504504--7366 AUG 1 RED7366 AUG 1 RED--HOLLAND HOLLAND
Hypertension Provider ReportHypertension Provider Report
Washington, DC VAMCWashington, DC VAMC

Improving Hypertensives Improving Hypertensives Washington, DC VAMC
0
10
20
30
40
50
60
70
1998 1999 2000 2001 2002 2003 2004
< 140, < 90 < 160, < 120 > 160, > 120
Perc
ent P
atie
nts
Perc
ent P
atie
nts
3,1333,133 6,5076,507 8,3578,357 9,4189,418 10,74510,745 12,60612,606 13,19813,198
Washington, DC VAMCWashington, DC VAMC

Hypertensive Patients Returning to < 140 / < 90Hypertensive Patients Returning to < 140 / < 90
Months
30
35
40
45
50
55
60
Perc
ent P
atie
nts
Perc
ent P
atie
nts
Jan 99 Jul 99 Jan 00 Jul 00 Jan 01 Jul 02 Jan 03 Jul 03 Jan 04Jul 01 Jan 02
Washington, DC VAMCWashington, DC VAMC

LDL Values for Patients with Previous MILDL Values for Patients with Previous MI
Low LDL < 120Low LDL < 120Highest LDL >120Highest LDL >120Missing LDLMissing LDL
Patients seen in the past 2 years Patients seen in the past 2 years ----WashingtonWashington
68.7 %68.7 %
17.2 %17.2 %
14.2 %14.2 %
Fully Satisfactory Performance Measure = 70 % Fully Satisfactory Performance Measure = 70 %
83.8 %83.8 %
14.8 %14.8 %
1.3 %1.3 %
Jul 03Jul 03 Feb 04Feb 0422 % improvement22 % improvement
Washington, DC VAMCWashington, DC VAMC

LDL MI ReportLDL MI ReportGREEN GREEN -- PROVIDER: FERON,LEEPROVIDER: FERON,LEE
SUMMARY: NO CURRENT LDL S: 2 ( 9.5%)SUMMARY: NO CURRENT LDL S: 2 ( 9.5%)HIGHEST LDL (>119): 6 ( 28.6%)HIGHEST LDL (>119): 6 ( 28.6%)
ACCEPTABLE LDL (>100): 4 ( 19.01%)ACCEPTABLE LDL (>100): 4 ( 19.01%)
LOWEST LDL (<100): 9 ( 42.9%)LOWEST LDL (<100): 9 ( 42.9%)TOTAL: 21 (100.0%)TOTAL: 21 (100.0%)
A. (*No Recent Test*:) OLD MI(S) WITH NO LDL TEST SINCE JUL 8A. (*No Recent Test*:) OLD MI(S) WITH NO LDL TEST SINCE JUL 8,2001: (6),2001: (6)
44--DIG NAME DIG NAME PHONE #PHONE #---------- -------------------------------------- ------------------------P3332 FAT,ALBERT OTTOP3332 FAT,ALBERT OTTO 555555--555555--55555555R5554 ROSE,SAMR5554 ROSE,SAM 555555--555555--55555555
B. (*Highest*:) OLD MI(S) WITH AT LEAST 1 LDL TEST SINCE JUL B. (*Highest*:) OLD MI(S) WITH AT LEAST 1 LDL TEST SINCE JUL 8,2001,8,2001,LATEST VALUE 119+: (3)LATEST VALUE 119+: (3)
# LDL LATEST# LDL LATEST--RESULT LOWESTRESULT LOWEST--RESULT HIGHESTRESULT HIGHEST--RESULT PHONE #RESULT PHONE #44--DIG NAME TESTS DIG NAME TESTS -------------------------------- ---------------------------- ---------------------------- ------------------------F0350 FLTSTNE,FRED 6 JUL 01,03 178.0 NOV 14,02 124.0 F0350 FLTSTNE,FRED 6 JUL 01,03 178.0 NOV 14,02 124.0 JUL 01,03 178.0 555JUL 01,03 178.0 555--555555--55555555R7777 WARD,RUSSR7777 WARD,RUSS 1 JUL 08,02 165.0 551 JUL 08,02 165.0 5555--555555--55555555J2222 JEFFREY,GEORGE 4 JUN 11,02 140.0 JUN 11,02 114.0 J2222 JEFFREY,GEORGE 4 JUN 11,02 140.0 JUN 11,02 114.0 JUN 04,03 140.0 555JUN 04,03 140.0 555--555555--55555555N3258 NORMAL,ABBEY 1 JUN 26,02 163.0 N3258 NORMAL,ABBEY 1 JUN 26,02 163.0 555555--555555--55555555S1451 SMITH, S1451 SMITH, ANONYMOUSANONYMOUS 2 AUG 30,02 187.0 FEB 08,02 90.0 AUG 30,02 187.0 5552 AUG 30,02 187.0 FEB 08,02 90.0 AUG 30,02 187.0 555--555555--55555555W1234 WELCH,JOHN 2 MAR 25,03 156.0 MAR 11,02 95.0 W1234 WELCH,JOHN 2 MAR 25,03 156.0 MAR 11,02 95.0 MAR 25,03 156.0 555MAR 25,03 156.0 555--555555--55555555
Washington, DC VAMCWashington, DC VAMC

Diabetes Foot Exam, Red Team Diabetes Foot Exam, Red Team Exceptional Exceptional ≥≥ 87%, FS 82 87%, FS 82 -- 86%86%
0%
20%
40%
60%
80%
100%
Mar-02 Apr-02 May-02 Jun-02 Jul-02 Aug-02 Sep-02
MarMar--0202 83%83% 73%73% 54%54% 43%43% 81%81% 81%81% 76%76%AprApr--0202 86%86% 73%73% 89%89% 39%39% 83%83% 71%71% 69%69%MayMay--0202 83%83% 88%88% 86%86% 34%34% 80%80% 88%88% 82%82%JunJun--0202 88%88% 86%86% 79%79% 54%54% 100%100% 73%73% 70%70%JulJul--0202 86%86% 96%96% 88%88% 49%49% 91%91% 78%78% 60%60%AugAug--0202 92%92% 100%100% 42%42% 63%63% 45%45%SepSep--0202 100%100% 92%92% 40%40% 100%100% 100%100% 73%73%
AA BB CC DD EE FF GG
FS 82%
EX 87%
Washington, DC VAMCWashington, DC VAMC

File Room after EMRFile Room after EMR


Electronic Health Records are Fully Electronic Health Records are Fully Deployed Throughout VA Deployed Throughout VA
Washington, DC VAMCWashington, DC VAMC

EHR (VistA) Strategies EHR (VistA) Strategies ––Summary Summary •• Use expert and nonUse expert and non--expert advisors.expert advisors.•• Local ownership Local ownership ---- Customize templates, Customize templates,
reminders and overall organization.reminders and overall organization.•• Package popular(discharge summaries,Package popular(discharge summaries,
labs, images) with unpopular (order labs, images) with unpopular (order entry, notes) componentsentry, notes) components
•• Maintain hybrid status until 60Maintain hybrid status until 60-- 70%70%use is achieved. ( use is achieved. ( ““Tipping pointTipping point””) )
•• Keep software intuitive and user friendlyKeep software intuitive and user friendlyfor rapid adoption by new providersfor rapid adoption by new providers
•• Provide real improvement in patient care.Provide real improvement in patient care.

ECG Showing Ventricular TachycardiaECG Showing Ventricular Tachycardia
Washington, DC VAMCWashington, DC VAMC

Images Images –– CineangiogramCineangiogram
Washington, DC VAMCWashington, DC VAMC

Lab .. Worksheet Graph of HgbLab .. Worksheet Graph of Hgb
Washington, DC VAMCWashington, DC VAMCAbrupt fall in Hgb with acute bleedingAbrupt fall in Hgb with acute bleeding

Images Images –– Colonoscopy Colonoscopy –– DiverticuliDiverticuli
Washington, DC VAMCWashington, DC VAMC

File Room after EHRFile Room after EHR


Lab .. Worksheet Graph of HgbLab .. Worksheet Graph of Hgb
Washington, DC VAMCWashington, DC VAMCAbrupt fall in Hgb with acute bleedingAbrupt fall in Hgb with acute bleeding

VISN 5 Performance Measures
Target patients not in complianceTarget patients not in compliance..
Create a master list from reminder reports orCreate a master list from reminder reports orhospital databasehospital database
assign to a coordinator assign to a coordinator report to providerreport to provider
Create a central clinic to correct deficiencies Create a central clinic to correct deficiencies e.g.e.g.
LDL >100 or not doneLDL >100 or not doneHbA1c >9 or not doneHbA1c >9 or not doneBP >140/90 BP >140/90 Mammography overdueMammography overdue
Washington, DC VAMCWashington, DC VAMC
Strategies

VistA outside VA VistA outside VA –– Hurricane KatrinaHurricane Katrina560 patients from Gulfport AFRH560 patients from Gulfport AFRH
evacuated to Washington DC AFRHevacuated to Washington DC AFRH16 laptop works16 laptop workstationstations in three in three buildings buildings –– internet with VPN access.internet with VPN access.Patients immediately registeredPatients immediately registeredRemote views available Remote views available –– Katrina webKatrina webMedications ordered and delivered Medications ordered and delivered thru our pharmacy thru our pharmacy -- 1000 Rx in 3 days1000 Rx in 3 daysNotes added with AFRH template Notes added with AFRH template listing meds for AFRH Walk In Cliniclisting meds for AFRH Walk In ClinicConsults, appointments requested.Consults, appointments requested.
Washington, DC VAMCWashington, DC VAMC

Images Images –– Colonoscopy Colonoscopy –– Acute bleedingAcute bleeding
Washington, DC VAMCWashington, DC VAMC

Labs Labs …… WBC Using WorksheetWBC Using Worksheet
Washington, DC VAMCWashington, DC VAMCWBC fell with antibiotic treatment of Lyme diseaseWBC fell with antibiotic treatment of Lyme disease

Discharge SummaryDischarge Summary
Washington, DC VAMCWashington, DC VAMCContent entered using templates and typing by providerContent entered using templates and typing by provider

Vital Signs Vital Signs –– Weights .. Home, Clinic, HospitalWeights .. Home, Clinic, Hospital
Washington, DC VAMCWashington, DC VAMCWeight gain over timeWeight gain over time

Vital Signs Vital Signs –– Weights .. Home, Clinic, HospitalWeights .. Home, Clinic, Hospital
Washington, DC VAMCWashington, DC VAMCWeight controlled with thorocentisis x2 and FurosemideWeight controlled with thorocentisis x2 and Furosemide

Images Images –– Chest XChest X--rays rays –– Right and Left Pleural EffusionsRight and Left Pleural Effusions
Washington, DC VAMCWashington, DC VAMCPleural effusions resolved with thorocentisis and diureticsPleural effusions resolved with thorocentisis and diuretics

Images Images ––Widening LBBB on sequential ECGsWidening LBBB on sequential ECGs
Washington, DC VAMCWashington, DC VAMCQRS increased from 0.154 TO 0.178QRS increased from 0.154 TO 0.178

Images Images –– MRI Video loop with LBBB on ECGMRI Video loop with LBBB on ECG
Washington, DC VAMCWashington, DC VAMCSeptum moves paradoxically away from left ventricleSeptum moves paradoxically away from left ventricle

EHR (VistAEHR (VistA))
Remote Views• Remote data button and remote
health summaries.• VistaWeb – patient specific data• Remote ECG view – map MUSE• Remote image view
X-ray, scanned images, and PDF files.
• Direct sign on to remote site withseparate access and verify code

Pacemaker/Device Data to EHR (VistAPacemaker/Device Data to EHR (VistA))
Future remote views• Health Data Repositry –
Data and notes from all VA visitsare integrated chronologically.
Fall 2005
• Current functionality will be preserved on Java platform

Reminders MHVReminders MHV

Reminders MHV Reminders MHV ---- WeightWeight

Self Entered InformationSelf Entered Information

My Health My Health eeLog Log (Self(Self--enteredentered ))

Weight Log Weight Log (Self(Self--enteredentered ))
Clinic Clinic Entry Entry ►►
HomeHomeEntriesEntries

OverviewWireless PDA software includes:Wireless PDA software includes:
ClinicianClinician’’s View s View –– CPRS Cover SheetCPRS Cover Sheet
Handheld Bar Code Medication Administration Handheld Bar Code Medication Administration (BCMA)(BCMA)
Vitals, I&OsVitals, I&Os
Care Collect Care Collect –– Lab and Specimen CollectionLab and Specimen Collection
Blood Transfusion Blood Transfusion –– AdministrationAdministration
ECG ECG Washington, DC VAMCWashington, DC VAMC

Medication Administration: UDMedication Administration: UD
Washington, DC VAMCWashington, DC VAMC

IRM Steering CommitteeIRM Steering CommitteeDirector and StaffDirector and Staff
IRM chiefIRM chief
Clinicians with computer expertiseClinicians with computer expertiseNational CommitteesNational CommitteesLocal applicationsLocal applications
Clinicians with high use but little computer Clinicians with high use but little computer expertiseexpertise
OrganizationOrganization
Washington, DC VAMCWashington, DC VAMC

When to declare victory?When to declare victory?
Question Question –– ““When can we set a date to stop When can we set a date to stop pulling paper records for Clinics?pulling paper records for Clinics?””
Response Response –– ““Stop now Stop now –– the paper record is no the paper record is no longer used.longer used.””
Begin to dismantle medical record and xBegin to dismantle medical record and x--ray file ray file rooms.rooms.
Road to the Paperless HospitalRoad to the Paperless Hospital
Washington, DC VAMCWashington, DC VAMC

SolutionsSolutionsData RetrievalData Retrieval
Know database structure for logical retrieval.Know database structure for logical retrieval.
Create automatic reportsCreate automatic reports
Use reports to improve computer entry.Use reports to improve computer entry.
Use reports to improve patient careUse reports to improve patient care..Assess compliance with current guidelines.Assess compliance with current guidelines.Determine outcome to define efficacious treatmentDetermine outcome to define efficacious treatment
Washington, DC VAMCWashington, DC VAMC

Low LDL <100 Higher LDL 100-119Highest LDL >120 Missing LDL
60.1%60.1%N=508N=508
15.4%15.4%N=127N=127
20.6%20.6%N=174N=174
3.2%3.2%N=30N=30
LDL Values for Patients with Previous MILDL Values for Patients with Previous MINovNov--04 04
Washington, DC VAMCWashington, DC VAMC
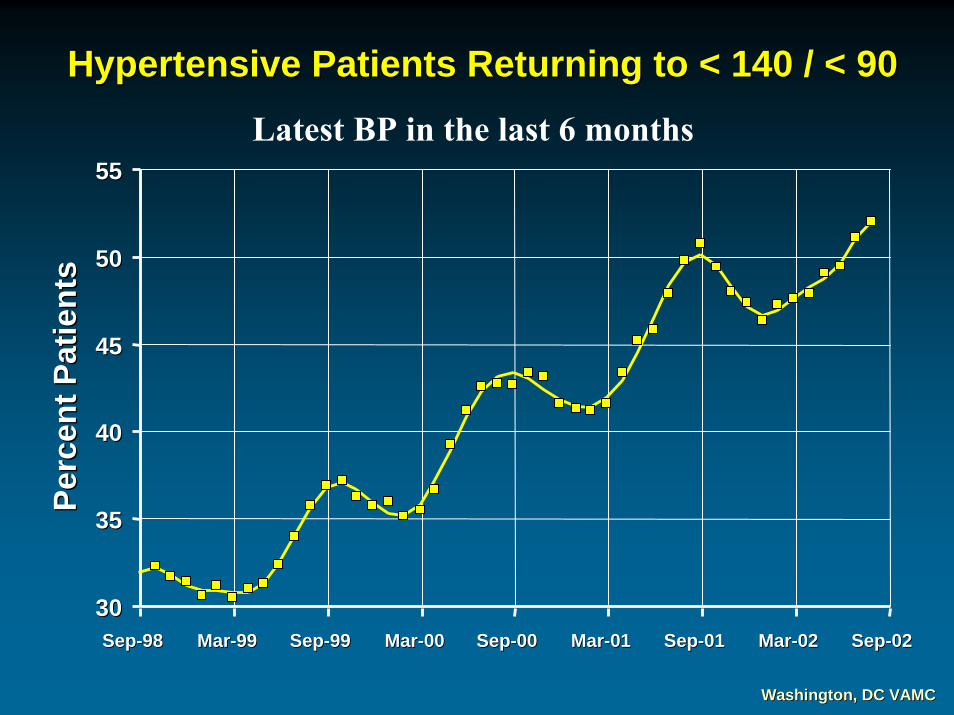
Hypertensive Patients Returning to < 140 / < 90Hypertensive Patients Returning to < 140 / < 90
3030
3535
4040
4545
5050
5555
SepSep--9898 MarMar--9999 SepSep--9999 MarMar--0000 SepSep--0000 MarMar--0101 SepSep--0101 MarMar--0202 SepSep--0202
Perc
ent P
atie
nts
Perc
ent P
atie
nts
Latest BP in the last 6 months
Washington, DC VAMCWashington, DC VAMC

Hypertensive Patients with BP > 160 >100Hypertensive Patients with BP > 160 >100
MonthsJan 99 Jul 99 Jan 00 Jul 00 Jan 01 Jul 02 Jan 03 Jul 03 Jan 04Jul 01 Jan 02
0
15
20
25
30
Perc
ent P
atie
nts
Perc
ent P
atie
nts
Washington, DC VAMCWashington, DC VAMC





























