Embed Size (px)
Citation preview

Using Civil Rights Tools to Address Health Disparities
Michael Rodriguez, MD, MPH; Marc Brenman; Marianne Engelman Lado, JD; and Robert García, JD
Policy Report The City Project
2014

2
ABOUT THE CITY PROJECT
The City Project believes that all people should have access to healthy, livable communities. Our multicultural, Latino-led team works with diverse allies to ensure equal access to (1) healthy green land use through planning by and for the community; (2) physical education and schools of hope as centers of their communities; (3) health equity and wellness; and (4) economic vitality for all, including jobs and avoiding displacement as communities become greener and more desirable. The mission of The City Project is to achieve equal justice, democracy, and livability for all.
“Of all the forms of inequality, injustice in health care is the most shocking and inhuman.” - Dr. Martin Luther King, Jr.
On the cover: Los Angeles State Historic Park and the greening of the L.A. River (Artist’s rendering copyright City of L.A.)
The City Project Equal Justice, Democracy, and Livability for All
Visit our website and blog at www.cityprojectca.org 1055 Wilshire Blvd., Suite 1660, Los Angeles, CA 90017 • 213-977-1035 • [email protected]
Donations are tax deductible

3
Using Civil Rights Tools to Address Health Disparities
Michael Rodriguez, MD, MPH; Marc Brenman; Marianne Engelman Lado, JD; and Robert García, JD*
Policy Report
The City Project
2014
Table of Contents 1. Introduction 4
2. Examples of Federally Funded Programs and Activities
Food Stamps 5 Physical Education in Public Schools 6 Parks and Healthy Green Land Use 7 Limited English Proficient (LEP) Programs 11
3. What Are the Civil Rights Authorities? 12 4. What Is the Civil Rights Analysis? 13
Compliance Analysis 14 Unjustified Discriminatory Impacts 14 Intentional Discrimination 17
5. How Can Civil Rights Compliance and Enforcement Address Health Inequities? 18 6. What’s Next? 20
*Michael Rodriguez, MD, MPH, is Professor of Family Medicine at the University of California, Los Angeles and Founding Director of the UCLA Blum Center on Poverty and Health in Latin America. Marc Brenman is principal of Social Justice Consultancy and a faculty member at The Evergreen State College. Marianne Engelman Lado, JD, is Managing Attorney, Northeast Office, Earthjustice. Robert García, JD, is Founding Director and Counsel, The City Project, and Assistant Professor, Charles Drew University of Medicine and Science. Please address correspondence to the authors c/o Robert García at [email protected].

4
ABSTRACT Ethnic and racial health and health care disparities are persistent and pervasive. Despite a wide range of approaches to address these disparities, they remain largely intact. The Affordable Care Act of 2010 (ACA) is expected to reduce disparities in access to health care and addresses health discrimination. In addition, the Civil Rights Act of 1964, the cornerstone legislation that prohibits discrimination based on race, color, and national origin by recipients of federal funding, and Executive Order 12898 on environmental justice and health can be used to address health disparities. If utilized consistently and applied with renewed efforts, civil rights laws can continue to address health care issues and reduce health disparities. These legal tools cut across diverse federally funded programs and activities. This article examines four health-related areas with disparities based on race, color, or national origin: (1) food stamp programs; (2) physical education in public schools; (3) parks and healthy green land use; and (4) access to health care services for limited English proficiency (LEP) populations. Civil rights laws including Title VI offer tools that attorneys and other stakeholders working with public health professionals, community groups, government agencies, and recipients of federal funds can use to alleviate health disparities. These legal tools are not limited to a litigation strategy. Voluntary compliance with civil rights laws is the preferred means to achieve equal justice goals. Civil rights attorneys continue the struggle to uphold and strengthen these laws.1
1. INTRODUCTION Extensive literature documents widespread ethnic and racial health disparities in the United States today.2 These disparities are persistent and pervasive, prompting a need for multifaceted approaches to reduce and eliminate them. Federal dollars support programs that promote the health and welfare of US residents. Some of these programs or activities include food stamp programs (FSP), physical education classes in public schools, parks and healthy green land use, and translator and interpreter services for limited English proficient (LEP) populations in the health care setting. These programs and activities have the potential to benefit the lives of millions of people in ways that promote health and reduce health disparities. However, racial and ethnic disparities exist in access to these programs or activities.
Civil rights tools are available to address health disparities. The tools analyzed here include: Title VI of the Civil Rights Act of 1964 and its regulations, which prohibit discrimination based on race, color, or national origin in programs or activities of recipients of federal funding; Executive Order 12898 addressing environmental justice and health; and the antidiscrimination provisions of the Affordable Care Act. These authorities are analyzed in more detail below.
While public health officials working with civil rights attorneys and federal officials in and out of court have historically addressed many health discrimination issues, more remains to be done. For example, the federal Hill-Burton Act enacted in 1944 provided more than $100 million per year in direct aid to states for health and hospitals. The act explicitly provided for "separate but equal" health services and facilities.3 Ten years later, the U.S. Supreme Court in Brown v. Board of Education in 1954 held that segregated public schools are inherently unequal and violate the Equal Protection Clause of the 14th Amendment.4 The National Medical Association and NAACP Legal Defense Fund lawyers worked together, with support from U.S. Justice Department, to challenge the “separate but equal” provision. In 1963, a federal court of appeals struck down the "separate but equal" provision of the Hill-Burton Act in Simkins v. Moses H. Cone Memorial Hospital. The court ruled in favor of a class that included Black physicians, dentists and patients who were excluded from private White hospitals that received federal funding.5 Soon after, Congress passed Title VI of the Civil Rights Act of 1964, and federal agencies enacted regulations under Title VI. Congress then passed the Medicare Act in 1965. Medicare funding, coupled with the Title VI prohibition against discrimination by recipients of federal funding, has helped end discrimination in health services and facilities. In the 50 years since its passage, Title VI has been used to challenge hospital closures and relocations and other discriminatory health care practices.6 Title VI has been used to address discriminatory programs and activities in other areas that affect health, including education, park access, and transportation.7 The ACA reflects a renewed commitment by Congress and the President to eliminate health discrimination.
Lessons from the Civil Rights Movement are especially appropriate in light of the 20th anniversary of the Executive Order 12898 on environmental justice and health, the 50th anniversary of the Civil Rights Act of 1964, and the 60th anniversary of Brown v Board of Education in 2014. In addition, Civil Rights advocates are fighting to uphold the disparate impact standard of discrimination under the Fair Housing Act in the US Supreme Court in 2015. In the Inclusive Communities Project case, opponents are challenging the right to fight unfair and unjustified discriminatory impacts, even where there are less discriminatory alternatives, absent proof of intentional discrimination. This reflects a general attack on civil rights tools to combat discrimination.

5
The NAACP Legal Defense & Education Fund team in Brown v Board.
Racial and ethnic discrimination in health care persists. In 2003, the Institute of Medicine published a landmark study of health care disparities. The book includes a chapter on the civil rights dimension of racial and ethnic health disparities by Tom Perez, who later served as Assistant Attorney General for Civil Rights in the U.S. Department of Justice and Secretary of Labor. In this chapter, Perez notes that “discrimination is a root cause of health disparities, and a comprehensive strategy to eliminate disparities must incorporate a strong civil rights component.”8 The chapter further outlined a host of civil rights interventions to address these widespread and persistent disparities.
Why are civil rights protections necessary to protect health and life itself? The documented costs of health inequalities are great. Between 2003 and 2006, for example:
• The combined costs of health inequalities and premature death in the U.S. were $1.24 trillion. • Eliminating health disparities for people of color would have reduced direct medical care expenditures by $229.4
billion. • 30.6% of direct medical care expenditures for African Americans, Asians, and Hispanics were excess costs due to
health inequalities. • Eliminating health inequalities for people of color would have reduced indirect costs associated with illness and
premature death by more than one trillion dollars.9
The World Health Organization defines health as “a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity.”10 WHO recognizes that the social determinants of health – the conditions in which people live, learn, play, pray, work, and age – are significant factors in health equity and disparities, and calls for health in all policies.11 The WHO definition of health is consistent with the broad view of health under the Affordable Care Act.12
This report examines how civil rights tools, including Title VI and Executive Order 12898, can be used to promote health equity through programs or activities by recipients of federal funding. We explore health equity and disparities in four programs or activities: (1) food stamp programs; (2) physical education classes in public schools; (3) parks and healthy green land use; and (4) translator and interpreter services for limited English proficient populations in the health care setting. Finally, we discuss civil rights laws and tools that attorneys and other stakeholders can use to alleviate health disparities beyond litigation. 2. EXAMPLES OF FEDERALLY FUNDED PROGRAMS AND ACTIVITIES Food stamps
The federal food stamp program, now known as the Supplemental Nutrition Assistance Program (SNAP), provides federal financial assistance to increase the food purchasing power and nutrition of low-income households.13 Food stamps are considered by the US government to be a “first line of defense against hunger” and a central component of US policy to alleviate hunger and poverty.14 Food stamps are a valuable tool in reducing household food insecurity and improving nutrition in the US. Household food insecurity is defined as “when the availability of or ability to acquire safe and adequate food is limited or uncertain.”15 Reducing food insecurity contributes to increased academic achievement in children, lowers body mass index (BMI) and reduces the severity of metabolic syndrome conditions.16

6
Food stamp eligibility is based on two main requirements: household income lower than 135% of the federal poverty line (FPL) and at least five years as a legal resident of the United States.17 Currently, 15% of the US population receives food stamp benefits averaging $134/person per month.18 During fiscal year 2012, the program served more than 46 million people in an average month at a total annual cost of over $74 billion in benefits.19
Despite the proven success of this program with seemingly neutral eligibility criterion, only 57% of eligible households that experience food insecurity received some form of federal food or nutritional assistance in 2011.20 In 2010 in California, only 55% of the people eligible (5,840,000) participated in the food stamp program, whereas the United States had a 75% average participation rate for those eligible.21
Nationally, limited availability and access to food is 2.5 times as prevalent among Latinos and non-Latino Blacks compared with their White counterparts.22 Twice as many households headed by Latinos or Blacks are food insecure compared with households headed by Whites.23 In California, Latinos suffer the worst levels of food insecurity: 44% of low income (at or below 185% of the FPL) Latinos are considered food insecure, the highest level of any race or ethnicity in the state.24
Despite suffering high food insecurity, eligible Latinos have lower participation rates in using food stamps than the national average.25 For Latinos, limitations to food stamp access have been attributed to transportation costs, the process required to complete forms and determine eligibility, and language barriers.26 Anecdotal information indicates that many eligible Latinos are discouraged from applying for food stamps due to unequally applied practices by agencies that provide food stamps. Children of immigrants (93% of whom are US citizens) are less than half as likely as children of US-born parents to receive food stamp benefits, despite the higher poverty rates that children of immigrants have.27 Two of the major predictors of a family not participating in food stamps are working more than 40 hours per week and immigration status.28 Children of immigrant families were more likely to live in families with difficulties affording food and without food stamp benefits (20% of immigrant families vs. 40% of US-born families utilizing federal food stamps benefits).29 Physical education programs in public schools Physical education in K-12 has great potential to promote the health of students attending schools in the US.30 School environments are an efficient and effective way to best promote healthy lifestyles through physical education. No other institution has as much contact with or influence on youth during the first two decades of their lives in terms of continuity and intensity.31 In fact, federal guidelines recommend that elementary school students receive 150 minutes of school physical education per week and that middle and high school students receive 225 minutes of school physical education per week.32 Of the 50 states, 41 have instituted physical education mandates for the elementary school level, but only six states meet the 150 minute per week recommended guidelines. In addition, 37 states have mandated middle school physical education with only two adhering to the 225 minute per week guideline. Forty-one states mandated high school physical education, but no state meets the 225 minute per week guidelines for physical education.33
Physical education and regular opportunities for physical activity are important components in the fight against obesity and other related chronic conditions.34 Obesity and related conditions disproportionately affect communities of color. In 2005 in California, Samoan children had the largest percentage (54%) of all children in the state whose BMI was not within the California public school Healthy Fitness Zone standard.35 Latino children (38.9%), Native American children (36.1%), and Black children (32.4%) also had significant percentages outside of the Healthy Fitness Zone in comparison to 23.1% of non-Hispanic white children.36 This trend is seen in adults as well, where 32% of Black, 28% of Latino, and 32% of Native Hawaiian Pacific Islander adults were obese, in comparison to 19% of non-Hispanic white adults.37

7
Norwood Elementary School Physical Education Class.
Photo by Tim Wagner for Partnership for the Public’s Health. Access to physical education is a right under California law. The California Court of Appeal has held that the State Education Code requires an average of 20 minutes of physical education per day in elementary schools, and that parents and students have the right to sue a school district for failure to comply with that law. Yet, half the public school districts audited in California from 2005 to 2009 did not comply with the physical education minutes requirements.38 A 2013 study of San Francisco public schools revealed a substantial gap between reported compliance and actual compliance with state law. Eighty-three percent of elementary schools reported they met the minutes requirements for physical education, but when the schools were monitored, only 5% met the requirements.39 Unfortunately, this is a nationwide trend. A 2013 study found that states with school physical education policies which required a certain number of minutes or percentage of time engaged in physical activity were monitored only through schools self-reporting progress to the state, resulting in biased reports and insufficient opportunities for physical activity.40 A separate study showed that noncompliant districts had a higher percentage of Black and Latino students than districts that were compliant.41 The Los Angeles Unified School District, the second largest in the nation, has adopted a plan to comply voluntarily with state physical education and federal and state civil rights requirements, in response to an organizing campaign and administrative complaints.42 The Institute of Medicine recommends monitoring compliance in providing physical education minutes, addressing disparities, improving teacher education, making physical education a core subject, and addressing physical activity in the whole school environment.43 Failure to provide physical education in school may adversely impact health outcomes, as well as academic achievement. Studies have shown that: (1) physical education has either a neutral or positive effect on testing;44 (2) cognitive function may be linked positively with physical activity in elementary and middle school students;45 (3) physical education may be associated with reduced overweight or obesity, lower blood pressure and improved bone health;46 and (4) physical education is an important component in the fight against obesity and other related chronic conditions.47 Parks and healthy green land use In a historic moment, President Barack Obama recognized that there are disparities in park access for people of color, that this contributes to health disparities, and that agencies need to address these social justice issues.
Too many children . . . especially children of color, don’t have access to parks where they can run free, breathe fresh air, experience nature, and learn about their environment. . . . This is an issue of social justice. Because it’s not enough to have this awesome natural wonder within your sight – you have to be able to access it.48
President Barack Obama’s words ring true in communities across the nation. He was speaking of L.A. County when he dedicated the San Gabriel Mountains National Monument in Southern California in 2014. According to the White House, improving public access and recreational opportunities will help address the region’s public health challenges. Studies have shown that increasing recreational access to public lands translates to higher levels of youth activity and lower youth obesity rates.49

8

9
The preceding map shows communities that are disproportionately park poor, income poor, and of color in California. Numerical disparities are a starting point for analyses under civil rights and environmental justice standards. GIS and demographic analyses provide important tools for this purpose.
In 2011, the National Park Service (NPS) published a Healthy Parks, Healthy People US Strategic Action Plan and Science Plan.50 NPS recognizes that people of color and low-income people face disparities in access to parks and recreation, and these disparities can impede their health. Park agencies have an obligation to alleviate these disparities. For example, 36% of Black and 35% of Latino high school students nationwide are overweight or obese, while 24% of non-Hispanic White high school students suffer from these conditions.51 Evidence-based social science research shows that parks can play an important role in alleviating socioeconomic health disparities.52 Yet, non-Hispanic Whites have disproportionately greater access to parks, with 12 to 15 times more park acreage per capita than Latinos and African-Americans in Los Angeles County.53 This reflects disparities nationwide.54 Communities with the least amount of green access tend to have higher rates of obesity and diabetes. The National Parks Service relies on the WHO definition.55
NPS recommends a new national recreation area in the San Gabriel Mountains, where the population is disproportionately Hispanic (64%) and Asian Pacific Islander (16%), citing civil rights and environmental justice protections.56 According to NPS, economically disadvantaged people in the study area lack access and the ability to enjoy existing green space due to lack of close-to-home open space, lack of effective transportation, lack of culturally advantageous facilities or opportunities, and lack of knowledge about recreation and natural resources.57 Diversifying access to and support for the San Gabriels, including recommendations to improve transit for underserved communities, will benefit the diverse local population and the greater Los Angeles region.58
President Barack Obama discusses green justice with The City Project’s Robert García
at the San Gabriel Mountains National Monument dedication.
Furthermore, access to parks and green space has a profound effect on human health and psychological wellbeing. In 2010, a National Recreation and Park Association (NRPA) report found that green environments fostered greater mental health, with lower susceptibility to stress, anxiety disorders, depression, and aggression, as well as greater resiliency and cognitive functioning.59 Urban communities of color without access to green space, however, are particularly subject to mental health disorders. A 2001 study of Chicago’s Robert Taylor Homes, one of the poorest neighborhoods in America, revealed that residents with views of only asphalt and concrete reported systematically higher levels of aggression and violence than residents living in identical buildings with views of trees and grass.60 A follow-up study in the Ida B. Wells low-rise apartment development found that buildings with high levels of vegetation had 52% fewer total crimes, 48% fewer property crimes, and 56% fewer violent crimes than buildings with low levels of vegetation.61 Ultimately, the studies found that “more green translates to less aggression, less transgression, more socializing, and more acts of caring.”62 Furthermore, studies of 7- to 11-year old children diagnosed with attention deficit/hyperactivity disorder have found that children’s concentration performance was better after 20-minute walks in an urban park than after walks of equal length in a neighborhood or downtown area.63 Thus, park poor communities of color with limited or no access to green space are unjustly subject to mental and physical health disparities that can affect length and quality of life. The following map shows ParkIndex scores for Los Angeles County. ParkIndex measures access to green space on a scale of 0 to 100, with 100 being best access. ParkIndex offers a tool for analyzing disparities in park access.64

10
Beta

11
Limited English Proficient (LEP) programs A LEP person is defined as someone who “does not speak English as their primary language and who has a limited ability to read, write, speak or understand English.”65 More than one sixth of the US population speaks a language other than English at home, and this number is increasing.66 The fastest-growing non-English speaking groups are Latinos and Asian Americans.67 In 2006 in California, 40% and 36% of the Latino and Asian American population respectively had limited English proficiency.68 Furthermore, Latinos and Asian Americans comprise 78% of the foreign-born population nationwide since 2000.69 Health-related challenges for LEP patients include: (1) conversing with their health care professional; (2) reading health-related materials; (3) taking an active role in their own health care decisions; and (4) following instructions for care in English.70
People’s March for Climate Action, New York City, 2014
Legal tools are available to address the needs of LEP patients. Discrimination on the basis of national origin includes discrimination on the basis of language. In Lau v. Nichols, the US Supreme Court held that public schools in San Francisco discriminated against non-English speaking Chinese American children and deprived them of effective educational services when they did not provide materials in the children's native language.71 In 2000, Executive Order 13166 directed federal agencies to develop guidelines for providing services and removing language barriers for persons who are LEP.72 Forty-three states have laws addressing national origin and language discrimination in health care settings.73 In addition, hospital guidelines, including the National Culturally and Linguistically Appropriate Services (CLAS), follow joint commission standards that recommend the routine use of professional interpreters.74 Despite these laws and recommendations, professional interpreters, language assistance tools and translations continue to be underutilized and provided at an insufficient rate to meet demand and need.75 LEP patients are frequently not provided the necessary resources to improve their quality of care.76 Failure to provide appropriate and effective language assistance to LEP persons compromises the quality of care that they receive.77 Yet, in a national study examining hospitals and their level of compliance with the National Culturally and Linguistically Appropriate Services (CLAS) standards, which include culturally and linguistically competent care, 19% of hospitals surveyed did not comply with any of the standards.78 LEP status contributes to ethnic and racial disparities in certain dimensions of access to care, such as preventative services and usual source of care, and contributes to higher utilization of emergency room services and delayed service related to lower health knowledge in emergency situations.79 When patients have difficulty communicating with their physicians, they are also more likely to receive inappropriate diagnoses and treatment and lower quality of care, have lower comprehension and adherence to medication regiments, lower patient satisfaction, and lower overall health outcomes.80 Limited English proficiency status can contribute to a lack of awareness of health conditions, creating a barrier to recognizing services and treatment that are necessary.81 In addition, reduced access to care has been shown for the LEP population even when adjusting for ethnicity and socioeconomic status.82 LEP patients were also less likely to receive preventative health services such as cervical and breast cancer screenings as well as cancer-preventable vaccines, compared to their English-speaking counterparts.83 In California, Asian

12
Americans are the only racial/ethnic group for whom the leading cause of death is cancer – total deaths caused by cancer is 27.7% in Asian Americans in comparison to 23.3% for non-Hispanic whites.84 Furthermore, 29% of Asian American women are noncompliant with cervical cancer screening guidelines, in comparison to 14% non-Hispanic white women. Twenty-six percent of Asian American women are noncompliant with breast cancer screening guidelines, in comparison to 21% of non-Hispanic white women. Finally, 53% of Asian Americans were noncompliant with colorectal cancer screening guidelines, in comparison to 42% of non-Hispanic whites.85 A similar finding was found among Mexican American men, who were 1.32 times, and those with LEP 1.68 times, more likely to have never had colorectal cancer screening tests despite having a higher prevalence of diagnosis in advanced stages.86 Patients with LEP who did not receive effective language assistance services were also more likely to have poor glycemic control as compared with those who received assistance in their native language.87 This was also observed with asthma when LEP patients demonstrated poor asthma control, lower access to inpatient services, and poorer overall quality of life compared with their English-proficient counterparts.88 Spanish and Cantonese speakers were the least likely to access mental health services as compared with English-speaking Latino and non-Latino White people.89 Individuals with LEP were more likely to forego necessary medical care and less likely to have a health care visit, compared with individuals who were proficient in English.90 LEP disparities also translate into lack of services that LEP patients seek for their children, with LEP patients having greater odds of not seeking necessary care for their children, resulting in fair or poor health status.91 LEP Latino patients report fewer services and less satisfaction with health provider communication than do other patients.92 In studies examining whether clinicians provided health advisement, researchers found that obese, English-proficient Latino patients were about 50% more likely to report having received advice for physical activity and/or diet compared with LEP Latino, obese patients.93 Moreover, a 2006 study of adult patients in California found that 11% of Latinos and 7% of Asian Americans—groups with large percentages of LEP populations—perceived race-based discrimination in medical care, in comparison to 3% of non-Hispanic whites.94 Patients who had both Medicare and Medicaid had better health outcomes compared to the elderly with Medicare alone.95 This may be partially due to the federal mandate that requires Medicaid to supply interpreting services to LEP patients.96 Also, when language policies were implemented, there was greater utilization of mental health services within that population.97
Despite the federal mandate to provide LEP services, these mandates are enforced weakly, if at all.98 Patients can make a complaint with the U.S. Department of Health & Human Services, Office for Civil Rights (OCR) to initiate an investigation.99 However, LEP status presents added challenges in navigating the system for filing a complaint, underscoring the importance of greater compliance, implementation and enforcement of existing laws,100 as well as how LEP services should be provided for the complaint process itself.
3. WHAT ARE THE CIVIL RIGHTS AUTHORITIES? Health disparities raise concerns about potential intentional discrimination, and unjustified and unnecessary discriminatory impacts. The discriminatory impact standard can ferret out subtle and structural practices that have demonstrably discriminatory effects. A thoughtless policy can be as unfair as, and functionally equivalent to, intentional discrimination. As a matter of common sense, discriminatory programs or activities should be avoided in favor of those that serve everyone's interests fairly, effectively, and without discrimination. This section will discuss the legal authorities to address health inequities and will present an analytic framework.
President Lyndon B. Johnson signs the Civil Rights Act on July 2, 1964, as Dr. Martin
Luther King Jr., and others look on. Photo by Cecil Stoughton of the White House Press Office.

13
Title VI of the Civil Rights Act of 1964 prohibits intentional discrimination by recipients of federal financial assistance based on race, color, or national origin, including LEP.101 Title VI regulations adopted by federal agencies prohibit unjustified and unnecessary discriminatory impacts.102 According to President John F. Kennedy in his message to Congress on Title VI, “Simple justice requires that public funds, to which all taxpayers of all races contribute, not be spent in any fashion which encourages, entrenches, subsidizes, or results in racial discrimination.”103 Recipients of federal financial assistance sign contracts to comply with Title VI as a condition of receiving federal funds.104 California and other states have similar laws prohibiting intentional and disparate impact discrimination.105
The Affordable Care Act provides important protections against health discrimination based on race, color, national origin, LEP, and other characteristics.106 Specifically, ACA section 1557 states that no individual, on the basis of race, color, national origin, or other characteristics shall “be excluded from participation in, be denied the benefits of, or be subjected to discrimination under, any health program or activity, any part of which is receiving Federal financial assistance.”107 Section 1557 also applies to any program or activity administered by a federal executive agency. Section 1557 references prior laws that protect against health discrimination, including Title VI. The ACA includes more than 60 provisions to advance health justice through a broad range of actions, sectors and actors. Thus, the ACA includes physical activity, healthy land use, and infrastructure projects as part of its mandate.108 This underscores how equal access to wellness and prevention programs is an important component of the ACA and health promotion.109
President Bill Clinton and community activists at the signing of
Executive Order 12898 on environmental justice and health in 1994. Executive Order 12898 on environmental justice and health requires each federal agency to “make achieving environmental justice part of its mission by identifying and addressing, as appropriate, disproportionately high and adverse human health or environmental effects of its programs, policies, and activities on minority populations and low-income populations.”110 The accompanying Presidential Memorandum identifies Title VI as one of several federal laws to be applied to prevent these communities from being subject to discriminatory effects.111 Environmental justice embraces the principle that all people and communities are entitled to equal protection of our environmental, health, employment, education, housing, transportation, and Civil Rights laws, according to Dr. Robert Bullard.112 These civil rights laws may facilitate the use of health impact assessments (HIAs). A compliance analysis may require an HIA, and an HIA may inform the compliance and equity review. “Recognizing and addressing the effects of a proposal on health equity (or health disparities) between various groups has been seen as a core task of HIA, although HIA practice has sometimes been criticized for a lack of attention to health equity.”113 The major steps of an HIA are consistent with, and complementary to, the legal framework described later in this article.114 4. WHAT IS THE CIVIL RIGHTS ANALYSIS? Voluntary compliance is the preferred means to achieve health equity and other civil rights goals.115 Planning, funding, and administrative processes offer opportunities for public agencies and other stakeholders to improve the health and lives of people of color and low-income people without litigation. Collecting, analyzing, and publishing data on health disparities is an important step of any comprehensive effort to eliminate health inequities. Numerical disparities are an important starting point for analyzing compliance with civil rights and environmental justice standards under both the disparate impact and intentional discrimination standards.116 GIS and demographic analyses, as illustrated in the maps in this report, provide invaluable tools to understand disparities in access to public resources. Although statistical disparities alone are seldom sufficient to prove discrimination, data collection and analysis provides necessary information and can inform strategies to eliminate health disparities. In addition, even if the factual disparities are based on race and ethnicity, race-neutral solutions can be provided. For example, parks in underserved communities improve park access for all people.

14
Compliance Analysis A compliance and equity analysis for a program or activity by a recipient of federal financial assistance includes the following steps under Title VI and its regulations, and Executive Order 12898 addressing environmental justice and health.117
1. Describe the program or activity. 2. Analyze the burdens and benefits for all people. 3. Analyze alternatives. 4. Include people of color and low-income people in the decision-making process. 5. Implement a plan to address equity concerns and avoid discrimination.
A best practice example of how funding agencies can use a compliance analysis is the development of what is now the Los Angeles State Historic Park.
This site could have been warehouses in downtown L.A. Instead, it is now a park. Andrew Cuomo, who was then-secretary of the U.S. Department of Housing and Urban Development, withheld federal subsidies for a proposed warehouse project at the site unless a full environmental study was conducted to consider the park alternative and the impact on people who were of color or low-income. As a result, the state bought the land and created the park. HUD relied on Title VI and Executive Order 12898 on environmental justice in response to an administrative complaint filed by diverse allies.118
Los Angeles State Historic Park
Unjustified Discriminatory Impacts A compliance and equity analysis helps guard against discriminatory impacts. The disparate impact framework includes an analysis that seeks answers to the following questions:119
1. Are there numerical health disparities? Disparities can be shown through statistical or social science evidence, or anecdotally. Data collection and analyses is relevant here.
2. Are the disparities justified by business necessity? Alternatively, is there a substantial legitimate justification for the disparities?
3. Even if so, are there less discriminatory alternatives to promote similar goals? The federal court of appeals decision in Larry P. v. Riles illustrates how to apply the disparate impact analysis. The court held that the use of IQ tests to place Black students in classes for the “educable mentally retarded” violated the disparate impact standard under Title VI and its regulations using the framework shown above:120
1. The tests disproportionately placed Black students in those classes. 2. The disparities were unnecessary and unjustified because the tests were not validated for the purpose used. 3. Schools have less discriminatory alternatives to evaluate students, such as considering the full background of the
child.

15
Following this framework, thumbnail disparate impact analyses of the health inequities discussed in this article are shown below. These examples are presented here only for purposes of illustration, recognizing that a complete analysis would be much more thorough and fact-based. Food stamps
1. Data show disparities in food stamp participation, especially among Latinos. Collecting and analyzing data to disaggregate participation rates by race and ethnicity at the state and county level, where food stamp programs are administered, is necessary to understand disparities.
2. Are such disparities justified by business necessity? Or is there a substantial legitimate justification for the disparities?
3. Are there less discriminatory alternatives to promote food security and health? Researchers have called for increasing awareness of food stamps, streamlining the application process, and making food stamp applications available via phone or online. Indeed, failure to provide Spanish speakers with information about food stamps in Spanish can be a form of intentional discrimination, as discussed below.
Physical education
1. Black and Latino students are disproportionately denied physical education, as discussed above. 2. The disparities are unnecessary and unjustified. School districts can eliminate the disparities by complying with
the legislative and judicial mandates to provide physical education, as many districts do. 3. There are less discriminatory alternatives, as many school districts do comply with the minutes requirement.
Parks and healthy green land use As one example, disparate impact questions for improving green access to the San Gabriel Mountains and along the Los Angeles River would be:
1. Are there numerical disparities in green access and health? Planning studies by NPS and Army Corps of Engineers document such disparities.121
2. Are these disparities justified by business necessity? Or is there a substantial legitimate justification for these disparities? Disparities in green access in Los Angeles are not the result of unplanned growth or an efficient market. Disparities are the result of a history of discriminatory land use, mortgage and housing policies, and segregated parks.122
3. Even if so, are there less discriminatory alternatives to promote healthy green access? Proper planning, including compliance with civil rights laws, can provide equitable, sustainable alternatives that promote green access for all.
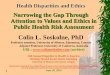
The following map shows that people of color disproportionately live in areas that are the most burdened for pollution and toxics, are the most vulnerable to health risks, and live in the most park poor communities. Thus:
1. In the areas with the 10% highest CalEnviroScreen (CES) score (most burdened) for pollution burden and vulnerability, fully 89% of the people are of color; only 11% are non-Hispanic white people. Statewide, the population average is 58% people of color.
2. In the areas with the 10% lowest CES score (least burdened) for pollution burden and vulnerability, only 31% of the people are of color; fully 69% are non-Hispanic white people.
3. 64% of people of color in the state live in areas with the 50% highest CES scores (most burdened) for pollution burden and vulnerability; only 31% of non-Hispanic white people live in those areas.
4. Only 36% of people of color in the state live in areas with the 50% lowest CES scores for pollution burden and vulnerability; fully 69% of non-Hispanic white people live in those areas.123

16
O R EGO N
NEVADA
M E X I C O
ARI Z
ONA
Pac i f i
cOcean
Fresno
Anaheim
Fremont
Oakland
San Diego
Riverside
Long Beach
Sacramento
LosAngeles
Bakersfield
San Jose
Stockton
Santa Ana
San Francisco
Ukiah
Yreka
Eureka
Salinas
El Centro
Bridgeport
Susanville
Markleeville
Independence
Crescent City
Santa Barbara
San LuisObispo
0 5025Miles
Demographics - Census 2010, US Census Bureau,provided by the CalEnviroScreen at http://oehha.ca.gov/ej/ces2.htmlCalEnivroScreen 2.0 - The CES 2.0 Score identifies communities in Californiamost burdened by pollution from multiple sources and most vulnerable to its effects, taking into account theirsocioeconomic characteristics and underlying health status. http://www.oehha.ca.gov/ej/ces2.htmlMap and analyses by The City Project and GreenInfo Network, August 2014, cityprojectca.org and greeninfo.org CC BY NC SA
No Score available for Tract
People of Color Non Hispanic White
Over State Average for People of ColorState Average = 58.4%
1
2
3
4
5
6
7
8
9
10
69%
62%
56%
52%
46%
38%
30%
24%
17%
11%
31%
38%
44%
48%
54%
62%
70%
76%
83%
89%Highest PollutionBurden &
Vulnerability
Lowest PollutionBurden &
Vulnerability
Pollution Burden, Vulnerability, and People of ColorCA - CES2.0

17
Intentional Discrimination A compliance and equity analysis also guards against intentional discrimination.124 The U.S. Supreme Court has described the kinds of evidence that are relevant to assess claims of intentional discrimination, including the following:
1. An important starting point for assessing intent is the impact of the action, and whether it bears more heavily on one racial or ethnic group than another. This is similar to the numerical inquiry under the disparate impact standard.
2. Whether there is a history of discrimination. 3. Compliance with, or departures from, substantive norms in reaching the decision. 4. Compliance with, or departures from, normal procedures. 5. Whether decision makers know of the impact of their actions. 6. Whether there is a pattern of discrimination.
The intentional discrimination standard remains an important tool in the 21st Century. Research supports evidence of numerical health disparities, as discussed above. The scientific literature demonstrates the history and legacy of discrimination that has existed in the US health care system since its inception, most frequently studied among African Americans.125 The federal Hill-Burton Act discussed above funded "separate but equal" health services and facilities until 1963, for example. In Tuskegee, public health officials diagnosed Black men with syphilis and left them uninformed and untreated for decades. In Guatemala, US public health officials intentionally infected Guatemalan victims beginning in the 1940s and left them untreated and uncompensated to the present day.126 False and discriminatory diagnoses persist. For example, Susan Matsuko Shinagawa in 1991 was told by her doctor after a sonogram revealing a solid mass in her breasts that she was “too young to have cancer, [had] no family history of cancer, and besides, Asian women don’t get breast cancer.”127 Fortunately, Shinagawa obtained a second opinion, which determined that the lump was indeed breast cancer. Substantive norms generally support equal access to publicly funded resources, including health care and wellness programs. Departures from substantive norms and normal procedures may be evidence of intent.128 Failure to collect, analyze, and publish data necessary to understand the impact of a program or activity, where there is evidence of disparities, may be evidence of intent.129 Examples of intentional discrimination and evidence demonstrating it appear below. Food stamps and LEP The district court in Almendares v. Palmer held that failure to provide bilingual information to Spanish- speaking Latino food stamp recipients can constitute intentional discrimination based on national origin, in violation of Title VI.130 Plaintiff Spanish-speaking recipients of food stamps alleged that defendant food stamp agencies purposefully discriminated against them when defendants chose to continue a policy of failing to provide bilingual services, knowing that Spanish-speaking applicants and recipients of food stamps were being harmed as the consequence.131 The court held that if this were proven at trial, this evidence would support a finding that the policy constituted intentional discrimination because of the numeric impact on LEP Spanish speakers.132 The subsequent settlement agreement included a provision requiring the state and county to conduct a demographic analysis of food stamp recipients and engage in other outreach efforts.133 Physical education For physical education concerns, the following is evidence of intentional discrimination.
1. Evidence shows that failure to provide physical education disproportionately impacts Latino and Black students, as discussed above.
2. There is a history of discrimination in public education in California. Additional research could be necessary at the individual school district level.
3. There are substantive irregularities in failing to provide physical education. Substantive quality education and health standards require physical education.
4. There are procedural irregularities in failing to provide physical education. Procedurally, districts do not seek exemptions; they simply do not provide physical education.
5. Decision makers know the impact that the failure to provide physical education has on students. Social science and advocacy can be used to establish this knowledge.
6. There is a pattern of discrimination in education in California, including the factors above.134

18
Park access Evidence of intentional discrimination for park access would include the following:
1. People of color face disparities in access to parks, as demonstrated by the studies by NPS and Army Corps of Engineers, among others.
2. Disparities in green access in Los Angeles are not the result of unplanned growth or an efficient market. Disparities are the result of a history of discriminatory land use, mortgage and housing policies, and segregated parks.135
3. Departures from substantive norms and (4) departures from normal procedures. Substantive norms support equal access to parks and public resources. Advocates argued that the city’s failure to conduct an environmental review that considered the park alternative and the impact on people who were of color and low income was a substantive and procedural irregularity in the HUD matter discussed above.
5. Proper planning includes data collection and analysis to inform decision makers and stakeholders of the impact of public actions. Disparities in health and green access are well-documented.
6. There is a pattern of discrimination in the distribution of environmental benefits and burdens, as evidenced by the CalEnviroScreen map and analyses above.
HOW CAN CIVIL RIGHTS COMPLIANCE AND ENFORCEMENT ADDRESS HEALTH INEQUITIES? Many avenues are available to alleviate health inequities through civil rights laws and international principles. For example, the US Department of Health and Human Services (US DHHS), which is primarily responsible for implementing the ACA, and other federal agencies can guard against health discrimination through planning, regulations, data collection and analyses, review of federal funding applications, contractual assurances of compliance by recipients of federal financial assistance, compulsory self-evaluations by recipients, compliance reviews after funding, investigation of administrative complaints, full and fair public participation in the compliance and enforcement process, and termination and deferral of funding. The Department of Justice has civil rights coordinating responsibility with federal agencies and can enforce civil rights laws in court. The US DHHS issued a request for information in the process of drafting regulations to implement the antidiscrimination provisions of the Affordable Care Act. This is a best practice example of using the planning and regulatory process.136 The NPS and Army Corps studies for park access in the San Gabriels and along the Los Angeles River discussed above are best practice examples of using the planning process to include civil rights compliance. Private individuals and groups can file administrative complaints with funding agencies. They should have a fair say in the investigation and resolution of those complaints. The administrative complaint process and funding decision in the HUD matter above resulting in the creation of LA State Historic Park are best practice examples. The administrative complaint and voluntary compliance with physical education and civil rights laws in the Los Angeles Unified School District cited above is a best practice example. Private individuals and groups can seek access to justice through the courts, including individual, class, and third party complaints for injunctive and declaratory relief and money damages.137 Examples of successful Title VI cases include Larry P. on IQ tests, Lau on bilingual education, and Almendares on food stamps and LEP. In addition, successful cases filed in court are often settled through mediation and before trial without resulting in a published opinion.138
There are many avenues to achieve compliance with civil rights laws. The courtroom is only one of many venues where justice can be won. Voluntary compliance should be the preferred means to achieve civil rights goals including health equity. Voluntary compliance can eliminate costly, time consuming, and risky litigation, for example, and can bring people together to support common values through democratic governance. Often, one’s perceptions of the law, lawyers, and health may be limited to litigation to resolve poor surgical or other dissatisfactory health outcomes. Yet, creative civil rights lawyers can help create broader constituencies for equitable policies in health care, wellness and prevention, community planning and revitalization, data collection and analysis, and democratic participation. The planning, funding, and administrative processes offer opportunities to advance the cause of justice and improve the health and lives of people of color and low-income people, in addition to access to justice through the courts. Today’s civil rights and racial justice lawyers are problem solvers who use many of the same strategies that corporate or transactional lawyers use on behalf of their clients: planning, data collection and analysis, media, negotiation, policy advocacy, and coalition building are all part of a comprehensive problem solving strategy. Civil rights lawyers work with

19
clients, experts, and broader coalitions to seek racial equity and overcome discrimination and structural barriers to a more equitable society. This view of civil rights and racial justice seeks to change structures and practices that perpetuate racial and ethnic disparities.
A few important lessons can guide the change needed to improve health equity. The history of health discrimination assists in understanding continued health inequities. Civil rights attorneys, public health experts, agencies, recipients of federal funding, foundations, and other stakeholders need to work together to address health inequities.
The Civil Rights Revolution has used multiple strategies to address health discrimination. The Movement includes attorneys taking cases to court, ground breaking judicial decisions, grass roots organizing in the streets, legislation by Congress, action by the President, implementation by administrative agencies, and people providing a mandate to support civil rights through the right to vote.
While Brown v Board of Education in 1954 is often seen as the starting point of the modern Civil Rights Revolution, in fact civil rights attorneys and community organizers began the struggle for equal justice culminating in Brown and its progeny decades earlier. In the first half of the twentieth century, beginning in the 1920s, African American and Mexican American parents and civil rights attorneys challenged racial segregation in schools across the United States, often working with civil rights organizations, including the NAACP, the American Civil Liberties Union (ACLU), and League of United Latin American Citizens (LULAC). Plaintiffs’ lawyers used social science research to contest segregation, a strategy pioneered in Mendez v. Westminster School District of Orange County (1946), which successfully challenged the segregation of Mexican American students in Southern California. Thurgood Marshall and the NAACP Legal Defense Fund, Inc. (LDF) adopted and developed this approach in their school segregation cases, including Brown v Board of Education.139 In Brown in 1954, the US Supreme Court struck down “separate but equal” schools. Also in 1954, the US Supreme Court held that the Equal Protection Clause protects against discrimination based on race, color, national origin, ancestry, or descent in Hernandez v Texas.140 Martin Luther King, the Student Nonviolent Coordinating Committee, the March on Washington, and other organizing efforts of the Movement in the streets led to the passage of the Civil Rights Act of 1964. President Lyndon Johnson led Congress in passing that Act and Medicare in 1965.141 Civil rights attorneys and government agencies have used Title VI and Medicare funding to help dismantle discrimination in health care administratively, as well as through litigation, as discussed above.
Today, these lessons should guide a health justice movement to seek racial and ethnic equity and overcome discrimination and structural barriers to a more equitable society. Research studies and policy prescriptions are important, but they are not enough without the force of law. The ACA creates enforceable rights; an Affordable Care "policy" would not. Finally, access to justice through the courts, as well as research, legislation, planning and funding decisions, and administrative procedures are necessary to alleviate health inequities.
Foundations have a significant role to play in supporting civil rights advocacy to address health disparities. There are structural obstacles to fund health justice through foundations and government. Foundations should fund legal advocacy and access to justice through the courts, which is a First Amendment right, but many will not fund advocacy or litigation. The more committed to the environment, the less likely a foundation will fund social justice. While environmental funders spent $10 billion between 2000 and 2009, just 15% of those dollars benefited marginalized communities, and only 11% went to advancing social justice. Foundations should invest at least 20% to benefit marginalized communities, and 25% to

20
advance social justice - policy advocacy and community organizing that works toward structural change on behalf of those who are the least well off politically, economically and socially.142 Foundations and government funding exacerbate rather than alleviate inequities in health and green access in Southern California, according to two recent peer reviewed studies. Public and nonprofit expenditures are most strongly associated with race and ethnicity. Black and Latino communities suffer from lower expenditure levels for parks and recreation by both the public and nonprofit sector.143 Some mainstream environmental organizations are now trying to increase the diversity of their staffs and boards. That is good, but it is not enough. Nonprofits that receive federal funding should comply with civil rights requirements as discussed above.
The Selma to Montgomery March, Photo Tile in The Civil Rights Park, Los Angeles, CA144
The disparate impact standard of discrimination is a lynchpin for addressing health and environmental justice. Civil rights attorneys continue the struggle to uphold and strengthen these laws. The disparate impact standard is being challenged in the US Supreme Court in 2015. Opponents are challenging the right to fight unfair and unjustified discriminatory impacts, even where there are less discriminatory alternatives, absent proof of intentional discrimination. While that case involves the Fair Housing Act, the disparate impact standard applies in other contexts including, for example, health disparities and employment discrimination. The challenge to the disparate impact standard reflects a general attack on civil rights tools to combat discrimination. Disparate impact is a long standing safeguard for civil rights. Disparate impact is a legacy of the Civil Right Movement. Freedom from discrimination benefits everyone.145 6. WHAT’S NEXT? The following recommendations can help civil rights attorneys, public health professionals, community groups, public agencies, recipients of public funding, foundations and other stakeholders alleviate health inequities through compliance with civil rights laws. Framing the issues can vary depending on the context (e.g., wellness and prevention, social determinants of health, environmental and health justice and civil rights compliance, sustainable development, equitable ecosystem services,146 smart growth) but the principles and goals are similar.

21
1. Of the many avenues to achieve compliance with civil rights laws, voluntary compliance is the preferred means to
achieve civil rights goals including health equity. 2. Discrimination is a root cause of health disparities, and a comprehensive strategy to eliminate disparities must
incorporate a strong civil rights component. 3. Stakeholders should work together on a compliance and equity plan for each program or activity by recipients of
federal funding that describes what is to be done, analyzes the impact on all communities, analyzes alternatives, includes full and fair participation by diverse communities, and alleviates health inequities.
4. Compliance and equity plans should guard against unjustified and unnecessary discriminatory impacts, as well as intentional discrimination, in health programs and activities.
5. Federal agencies should ensure compliance with civil rights laws through the many avenues they have available. This includes data collection, analyses, and publication, planning, regulations and guidance documents, review of federal funding applications, contractual assurances of compliance by recipients, compulsory self-evaluations by recipients, compliance reviews after funding, investigation of administrative complaints, full and fair public participation in the compliance and enforcement process, and denial or termination of funding. State and local agencies have similar tools to ensure compliance with federal and parallel state laws.
6. Civil rights lawyers should use comprehensive problem-solving strategies: coalition building, planning, data collection and analysis, media, negotiation, policy and legal advocacy out of court, and access to justice through the courts.
7. Foundations should support compliance with civil rights laws to ensure health equity, and support organizations for whom racial and ethnic justice is a core value. This can strengthen philanthropic efforts across a range of programs. Funding for organizational capacity is needed. Strategic funding of national, regional or local civil rights and environmental justice groups can have a significant impact.
8. Attorneys and public health experts should work together to promote better understanding of the civil rights dimension of the challenge of health disparities, and to show how to address these civil rights concerns.
9. Civil rights laws against discrimination in health and other publicly funded programs and activities should be strengthened and not rolled back. This includes the prohibition against unjustified and unnecessary discriminatory impacts, and intentional discrimination.
10. It takes a movement. The myriad of strategies of the Civil Rights Movement started the process of dismantling the most egregious forms of Jim Crow health discrimination. A continued health justice movement, drawing on the lessons of history, is needed to seek racial equity and overcome discrimination and structural barriers to a more equitable society.

22
ACKNOWLEDGEMENTS This work is made possible in part through the financial support of The California Endowment. Dr. Michael Rodriguez is also supported by UCLA/ DREW Project EXPORT, NIMHD, 2P20MD000182. The City Project also received the support of the Kresge Foundation and the Rosalinde and Arthur Gilbert Foundation. Robert García is also supported by NIH-NIMHD grant U54MD007598 (formerly U54RR026138), CDU-AXIS, Grant# U54MD007598 from NIMHD. The authors are grateful to City Project staff attorney Daphne Hsu and Anne M. Dubois for insightful comments and edits on earlier drafts; to City Project Policy Analyst Ariel Collins for research, editing, and layout; and to City Project Intern Michelle Kao and Kevin O’Fee for research and editing assistance. We thank the following colleagues for their comments:
Professor Jason Bocarro, Ph.D., Dept. of Parks, Recreation & Tourism Management, College of Natural Resources, North Carolina State University
Brian Cole, UCLA Adjunct Assistant Professor, Department of Environmental Health Sciences, UCLA Fielding School of Public Health
Leslie Fields, Director, Environmental Justice and Community Outreach Programs, Sierra Club Professor Lisa Ikemoto, UC Davis, Martin Luther King, Jr., School of Law Kay Jowers Senior Policy Associate, State Policy Program, Nicholas Institute for Environmental Policy Solutions Duke
University Amy Pickle, Director, State Policy Program, Nicholas Institute for Environmental Policy Solutions, Duke University Dr. David Martins, MD, Assistant Dean, Clinical and Community Affairs, Charles Drew University Daniel A. Mazmanian, Professor of Public Policy, USC Sol Price School of Public Policy Professor Miguel Mendez, Stanford Law School and UC Davis, Martin Luther King, Jr., School of Law Professor Gerald Torres, Cornell University Law School, and primary author of Executive Order 12898 on
environmental justice and health Omega Wilson, West End Revitalization Association (Mebane, NC)
REFERENCES 1 See generally R. García and A. Collins, Celebrate The Civil Rights Revolution: The Struggle Continues (The City Project Policy Report 2014), available at www.cityprojectca.org/blog/archives/34950; R. García, “Public Health is a Social Justice Imperative,” Mastering Public Health: Essential Skills for Effective Practice, B. S. Levy and J. R. Gaufin (eds.), Oxford Press (2011). 2 See, for example, B. D. Smedley, A. Y. Stith & A. Nelson (eds.), Unequal treatment: Confronting racial and ethnic disparities in healthcare (Washington DC: The National Academies Press, 2003); L.M. Rossen and K.C. Schoendorf, Measuring health disparities: trends in racial−ethnic and socioeconomic disparities in obesity among 2- to 18-year old youth in the United States, 2001–2010. Annals of Epidemiology. 10// 2012;22(10):698-704. 3 Hospital Survey and Construction Act, Public Law 42-725, US Statutes at Large 60 (1946), p. 999. Available at www.constitution.org/uslaw/sal/060_statutes_at_large.pdf. 4 Brown v. Board of Education (1954), 347 U.S. 483. 5 Simkins v. Moses H. Cone Memorial Hospital (1963), 323 F.2d 959. 6 J. Dittmer, The good doctors: the medical committee for human rights and the struggle for social justice in health care (New York: Bloomsbury Press, 2009); D. B. Smith, Health care divided: Race and healing a nation (Ann Arbor, MI: University of Michigan Press, 1999). 7 M. Shin, “Redressing wounds: Finding a legal framework to remedy racial disparities in medical care,” California Law Review 90/6 (2002), pp. 2049-2071. 8 T. Perez, “The civil rights dimension of racial and ethnic disparities in health status,” in B. D. Smedley, A. Y. Stith & A. Nelson (eds.), Unequal treatment: Confronting racial and ethnic disparities in healthcare (Washington DC: The National Academies Press, 2003), pp. 626-663. 9 T. A. LaVeist et al., The economic burden of health inequalities in the United States, Joint Center for Political and Economic Studies, Washington D.C., (2009). 10 Preamble to the Constitution of the World Health Organization as adopted by the International Health Conference, New York, 19 June - 22 July 1946; signed on 22 July 1946 by the representatives of 61 States (Official Records of the World Health Organization, no. 2, p. 100) and entered into force on 7 April 1948. Available at www.who.int/about/definition/en/print.html. 11 World Health Organization, Social Determinants of Health, available at www.who.int/social_determinants/sdh_definition/en/index.html. Accord, Rio Political Declaration on Social Determinants of Health (Oct. 21, 2011) (World Health Organization); World Health Organization, Meeting Report: World Conference on Social Determinants of Health, Rio de Janeiro, Brazil, 19-20 October 2011 (2012); World Health Organization, Consultation Draft on Health in All Policies, available at www.paho.org/equity/index.php?option=com_content&view=article&id=145&Itemid=1926. 12 See, for example, Patient Protection and Affordable Care Act, sections 4001, 4201, 4306, and 399w; Texas Health Institute, The Affordable Care Act & racial and ethnic health equity series: Report No. 4 public health and prevention programs for advancing health equity (Austin, TX: Texas Health Institute Press, Nov. 2013); American Public Health Association, Issue brief: Prevention provisions in the Affordable Care Act (Washington, DC: The National Academies Press, Oct. 2010). 13 The Food, Conservation and Energy Act of 2008, Public Law 110-246, US Statutes at Large 122 (2008) p. 1651. Available at www.constitution.org/uslaw/sal/122_statutes_at_large.pdf. 14 K. S. Martin et al., “Public versus private food assistance: barriers to participation differ by age and ethnicity,” Journal of Nutrition Education and Behavior 35/5 (2003), pp. 249-254. 15 Panel to Review US Department of Agriculture’s Measurement of Food Insecurity and Hunger NRC, Food insecurity and hunger in the United States: An assessment of the measure (Washington, DC: The National Academies Press, 2006). 16 H. W. Hoynes et al., Long run impacts of childhood access to the safety nets (Washington, DC: National Bureau of Economic Research, 2012); D. Jyoti et al., “Food security affects school children’s academic performance, weight gain, and social skills,” Journal of Nutrition 135/12 (2005), pp. 2831–

23
2839; A. L. Webb et al., “Food Stamp Program participation but not food insecurity is associated with higher adult BMI in Massachusetts residents living in low-income neighbourhoods,” Public Health Nutrition 11/12 (2008), pp. 1248-1255. 17 H. W. Hoynes, et al., Long run impacts of childhood access to the safety nets (Washington, DC: National Bureau of Economic Research, 2012). 18 U.S. Department of Agriculture, Supplemental Nutrition Program: Average monthly benefit per person (Washington, DC: Department of Agriculture, 2014). Available at www.fns.usda.gov/pd/18SNAPavg$PP.htm. 19 K. E. Cunnyham, State supplemental nutritional assistance program participation rates in 2010 (Washington, DC: United States Department of Agriculture, 2012). 20 A. Coleman-Jensen et al., Household food security in the United States in 2011 (Washington, DC: U.S. Department of Agriculture, 2012). 21 Ibid. 22 A. Coleman-Jensen et al., Food insecurity in households with children (Washington, DC: U.S. Department of Agriculture, 2013). 23 M. Nord, Food insecurity in households with children: Prevalence, severity and household characteristics (Washington, DC: U.S. Department of Agriculture, 2009). 24 M. P. Chaparro et al., “Nearly four million Californians are food insecure,” UCLA Center for Health Policy Research (June 2012), available at healthpolicy.ucla.edu/publications/Documents/PDF/FoodPBrevised7-11-12.pdf. 25 S. Zedlewski and K. Rader, “Recent trends in food stamp participation among poor families with children,” The Urban Institute 4/3 (June 2004). 26 S. J. Algert, et al., “Barriers to participation in the food stamp program among food pantry clients in Los Angeles,” American Journal of Public Health 96/5 (2006). 27 R. Capps et al., The health and well-being of young children of immigrants (Washington, DC: The Urban Institute, 2004). 28 L. Kaiser, “Why do low-income women not use food stamps? Findings from the California Women’s Health Survey,” Public Health Nutrition 11/12 (2008). 29 See, for example, R. Capps et al., The health and well-being of young children of immigrants (Washington, DC: The Urban Institute, 2004). 30 M. Story, et al., “Schools and obesity prevention: Creating school environments and policies to promote healthy eating and physical activity,” Milbank Quarterly 87/71 (2009), pp. 71–100. 31 Ibid. 32 L. K. Khan et al., “Recommended community strategies to prevent obesity in the United States,” Morbidity and mortality weekly report 58/7 (2009), pp. 1-26. Available at www.cdc.gov/mmwr/preview/mmwrhtml/rr5807a1.htm. 33 B. A. McCullick et al., “An analysis of state physical education policies,” Journal of Teaching in Physical Education 31/2 (2012). 34 A. L. Diamant et al., “Adolescent physical education and physical activity in California,” UCLA Center for Health Policy Research (2011). A. E. Springer et al., “Prevalence of physical activity and sedentary behaviors by metropolitan status in 4th-, 8th-, and 11th-grade students in Texas, 2004-2005,” Preventing Chronic Disease 6/1 (2009). 35 N. Ponce et al., The State of Asian American, Native Hawaiian and Pacific Islander Health in California Report (April 2009), p. 33. 36 Ibid. 37 Ibid, p. 32. 38 M. Lafleur et al., “Physical education and student activity: Evaluating implementation of a new policy in Los Angeles public schools,” Annals of Behavioral Medicine 45/1 (2013), pp. 122-130. 39 H. R. Thompson et al., “Are physical education policies working? A snapshot from San Francisco,” Preventing Chronic Disease (2013). Available at www.cdc.gov/pcd/issues/2013/pdf/13_0108.pdf. 40 J. A. Carlson et al., “State Policies About Physical Activity Minutes in Physical Education or During School.” J. Sch. Health. 2013; 83(3):150-156. 41 E. V. Sanchez-Vaznaugh et al., “Physical education compliance and children’s physical fitness,” American Journal of Preventative Medicine 42/5 (2012). 42 R. García and C. Fenwick, “Social Science, Equal Justice, and Public Health Policy: Lessons from Los Angeles,” Journal of Public Health Policy 30/S26 (2009) (physical education compliance in public schools under education and civil rights laws). 43 Institute of Medicine, Educating the student body: Taking physical activity and physical education to school (Washington, DC: The National Academies Press, 2013). 44 C. E. Basch, “Healthier students are better learners: a missing link in school reforms to close the achievement gap," Journal of School Health 81/10 (2011), pp. 593-598; A. L. Diamant et al., “Adolescent physical education and physical activity in California,” UCLA Center for Health Policy Research (2011). Available at healthpolicy.ucla.edu/publications/Documents/PDF/Adolescent%20Physical%20Education%20and%20Physical%20Activity%20in%20California.pdf; Department of Health and Human Services (DHHS), Physical activity fundamental to preventing disease home (Washington, DC: DHHS, 2002). 45 M. Efrat, “The relationship between low-income and minority children’s physical activity and academic-related outcomes a review of the literature,” Health Education and Behavior 38/5 (2011), pp. 441-451. 46 C. E. Basch, “Physical activity and the achievement gap among urban minority youth,” Journal of School Health 81/10 (2011), pp. 626-634. 47 A. L. Diamant, S. H. Babey, and J. Wolstein, “Adolescent physical education and physical activity in California,” UCLA Center for Health Policy Research (2011). A. E. Springer et al., “Prevalence of physical activity and sedentary behaviors by metropolitan status in 4th-, 8th-, and 11th-grade students in Texas, 2004-2005,” Preventing Chronic Disease 6/1 (2009). 48 Remarks by President Barack Obama at the Designation of the San Gabriel Mountains as a National Monument, Frank G. Bonelli Regional Park, San Dimas. 10 Oct. 2014. Available at www.whitehouse.gov/the-press-office/2014/10/10/remarks-president-designation-san-gabriel-mountains-national-monument. 49 R. García and M. Kao, The San Gabriel Mountains: A National Monument for All, NRPA Parks & Recreation Magazine 32 (Dec. 2014). 50 National Park Service (NPS), Healthy Parks, Healthy People US Strategic Action Plan (Washington, DC: Department of the Interior, Sept. 2011); NPS, Healthy Parks, Healthy People Science Plan 38 (Washington, DC: Department of the Interior, 2013); NPS, Healthy Parks, Healthy People Community Engagement eGuide (2014), available at www.nps.gov/public_health/hp/hphp/press/HealthyParksHealthyPeople_eGuide.pdf. 51 NPS Strategic Action Plan, supra, p. 4. 52 NPS Science Plan, supra, p. 38; R. García and S. Strongin, Healthy Parks, Schools and Communities: Mapping Green Access and Equity for Southern California (Los Angeles, CA: The City Project, 2011). Available at goo.gl/pAi7v; Craig Anthony (Tony) Arnold, Fair And Healthy Land Use: Environmental Justice and Planning (2007). 53 NPS, San Gabriel watershed and mountains special resource study and environment assessment (Washington, DC: US Department of the Interior, 2011). 54 See, e.g., P. Gordon-Larsen et al., “Inequality in the Built Environment Underlies Key Health Disparities in Physical Activity and Obesity,” 117 Pediatrics 417 (2006); M. Wen et al., “Spatial Disparities in the Distribution of Parks and Green Spaces in the USA,” 45 Annals Behav. Med. 18 (2013); D. Duncan et al., “The Geography of Recreational Open Space: Influence of Neighborhood Racial Composition and Neighborhood Poverty,” 90 J. Urb. Health 618 (2012). L. Powell et al., “Availability of Physical Activity-Related Facilities and Neighborhood Demographic and Socioeconomic Characteristics: A National Study,” 96 Am. J. Pub. Health 1676 (2006); L. Powell et al., “The Relationship between Community Physical Activity Settings and Race, Ethnicity, and Socioeconomic Status,” 1 Evidence-Based Preventive Medicine 135 (2004); R. García, “The George Butler Lecture: Social Justice and Leisure,” 45 J. Leisure Research 7 (2013); C. Sister et al., “Got Green? Addressing Environmental Justice in Park Provision,” 75 GeoJournal

24
229 (2010); J. Wolch et al., “Parks and Park Funding in Los Angeles: An Equity-based Analysis,” 26 Urban Geography 4 (2005); A. Loukaitou-Sideris & Orit Stieglitz, “Children in Los Angeles Parks: A Study of Equity, Quality and Children’s Satisfaction with Neighbourhood Parks,” 73 Town Plan. Rev. 467 (2002). 55 NPS, Healthy Parks, Healthy People US Strategic Action Plan at p. 8 (Washington, DC: Department of the Interior, Sept. 2011). 56 NPS, San Gabriel watershed and mountains special resource study: Summary and final recommendations (Washington, DC: US Department of the Interior, April 2013). 57 NPS, San Gabriel watershed and mountains special resource study and environment assessment (Washington, DC: US Department of the Interior, 2011). 58 NPS, San Gabriel watershed and mountains special resource study: Summary and final recommendations (Washington, DC: US Department of the Interior, April 2013). 59 F. E. Kuo, “Parks and Other Green Environments: Essential Components of a Healthy Human Habitat,” National Recreation and Parks Association Research Studies (2010), pp. 24. 60 Ibid, p. 11-12. 61 Ibid, p. 13. 62 Ibid, p. 14. 63 Ibid, p. 23. 64 See R. García and A. Collins, ParkIndex for Los Angeles County, The City Project Policy Report (forthcoming 2015). 65 S. Rosenbaum, “Reducing discrimination affecting persons with limited English proficiency: Federal civil rights guidelines under Title VI of the 1964 Civil Rights Act,” Public Health Reports 119/1 (2004), pp. 93-96. 66 D. Bustillos, “Limited English proficiency and disparities in clinical research,” Journal of Law, Medicine & Ethics 37/1 (2009), pp. 28-37. 67 T. Sentell and K. L. Braun, “Low health literacy, limited English proficiency, and health status in Asians, Latinos, and other racial/ethnic groups in California,” Journal of Health Communication 17/3 (2012), pp. 82-99; L. R. Snowden et al., “Federal civil rights policy and mental health treatment access for persons with limited English proficiency,” American Psychologist 62/2 (2007). 68 N. Ponce et al., The State of Asian American, Native Hawaiian and Pacific Islander Health in California Report (April 2009), p.16. 69 W. Zhang et al., “Limited English proficiency and psychological distress among Latinos and Asian Americans,” Social Science & Medicine 75/6 (2012), pp. 1006-14. 70 B. A. Tschurtz et al., “Language services in hospitals: Discordance in availability and staff use,” Journal of Healthcare Management/American College of Healthcare Executives 56/6 (2011). 71 Lau v. Nichols (1974), 414 US 563. 72 Improving Access to Services for Persons with Limited English Proficiency, Executive Order 13166, Federal Registrar 65/159 (2000), p. 50121. Available at www.justice.gov/crt/about/cor/Pubs/eolep.pdf. 73 A.H. Chen et al., “The legal framework for language access in healthcare setting: Title VI and beyond,” Journal of General Internal Medicine 22/2 (2007), pp. 362-367. 74 Y. Schenker et al., “Patterns of interpreter use for hospitalized patients with limited English proficiency,” Journal of General Internal Medicine 26/7 (2011), pp. 712-717. 75 D. Bustillos, “Limited English proficiency and disparities in clinical research,” Journal of Law, Medicine & Ethics 37/1 (2009), pp. 28-37; L. R. Snowden et al., “Federal civil rights policy and mental health treatment access for persons with limited English proficiency,” American Psychologist 62/2 (2007). 76 The Joint Commission, “What did the doctor say?”: Improving health literacy to protect patient safety (Oakbrook Terrace, Illinois: The Joint Commission, 2007). 77 L. R. Snowden et al., “Federal civil rights policy and mental health treatment access for persons with limited English proficiency,” American Psychologist 62/2 (2007). 78 L. C. Diamond et al., “Do hospitals measure up to the national culturally and linguistically appropriate services standards?” Medical Care 48/12 (2010), pp. 1080-1087. 79 C. A. DuBard et al., “Effect of language on heart attack and stroke awareness among US Hispanics,” American Journal of Preventive Medicine 30/3 (2006), p. 189; C. Fryer et al., “The effect of limited English proficiency on falls risk and falls prevention after stroke,” Age and Ageing 41/1 (2012), pp. 104-107; L. Shi et al., “The influence of English proficiency on access to care,” Ethnicity & Health 14/6 (2009), pp. 625-642; M. K. Youdelman, “The medical tongue: U.S. laws and policies on language access,” Health Affairs 27/2 (2008), pp. 424-433. 80 J. R. Pippins et al., “Association between language proficiency and the quality of primary care among a national sample of insured Latinos,” Medical Care 45/11 (2007), p. 1020; L. Shi et al., “The influence of English proficiency on access to care,” Ethnicity & Health 14/6 (2009), pp. 625-642. 81 D. Morhardt et al., “Seeking a diagnosis for memory problems: The experiences of caregivers and families in five limited English proficiency communities,” Alzheimer Disease and Associated Disorders 24/Suppl (2010). 82 L. Shi et al., “The influence of English proficiency on access to care,” Ethnicity & Health 14/6 (2009), pp. 625-642. 83 E. A. Jacobs et al., “Limited English proficiency and breast and cervical cancer screening in a multiethnic population,” Journal Information 95/8 (2005); G. T. Nguyen et al., “Awareness of anticancer vaccines among Asian American women with limited English proficiency: An opportunity for improved public health communication,” Journal of Cancer Education 24/4 (2009), pp. 280-283. 84 N. Ponce et al., The State of Asian American, Native Hawaiian and Pacific Islander Health in California Report (April 2009), p. 36. 85 Ibid, p. 25-26. 86 M. Johnson-Kozlow et al., “Colorectal cancer test use among Californians of Mexican origin: Influence of language barriers,” Ethnicity & Disease 19/3 (2009), p. 315. 87 A. Fernandez et al., “Language barriers, physician-patient language concordance, and glycemic control among insured Latinos with diabetes: the Diabetes Study of Northern California (DISTANCE),” Journal of General Internal Medicine 26/2 (2011), pp. 170-176. 88 J. P. Wisnivesky et al., “The association between language proficiency and outcomes of elderly patients with asthma,” Annals of Allergy, Asthma & Immunology 109/3 (2012). 89 See, for example, L. R. Snowden et al., “Federal civil rights policy and mental health treatment access for persons with limited English proficiency,” American Psychologist 62/2 (2007). 90 Ibid. 91 G. Flores et al., “Limited English proficiency, primary language at home, and disparities in children's health care: How language barriers are measured matters,” Public Health Reports 120/4 (2005), p. 418. 92 C. Pope, “Addressing limited English proficiency and disparities for Hispanic postpartum women,” Journal of Obstetric, Gynecologic, & Neonatal Nursing 34/4 (2005), pp. 512-520. 93 C. Lopez-Quintero et al., “Limited English proficiency is a barrier to receipt of advice about physical activity and diet among Hispanics with chronic diseases in the United States,” Journal of the American Dietetic Association 109/10 (2009), pp. 1769-1774. 94 N. Ponce et al., The State of Asian American, Native Hawaiian and Pacific Islander Health in California Report (April 2009), p. 27. 95 N. A. Ponce et al., “Language barriers to health care access among Medicare beneficiaries,” Journal Information 43/1 (2006). 96 Ibid.

25
97 L. R. Snowden et al., “Limited English proficient Asian Americans: Threshold language policy and access to mental health treatment,” Social Science & Medicine 72/2 (2011), pp. 230-237. 98 E. A. Jacobs et al., “Shared networks of interpreter services, at relatively low cost, can help providers serve patients with limited English skills,” Health Affairs 30/10 (2011), pp. 1930-1938. 99 M. K. Youdelman, “The medical tongue: U.S. laws and policies on language access,” Health Affairs 27/2 (2008), pp. 424-433. 100 Ibid. 101Title VI of the Civil Rights Act of 1964, Public Law 88-352, U.S. Statutes at Large 78 (1964), p. 252. According to the Supreme Court, the Title VI statute prohibits only intentional discrimination, not unjustified discriminatory impacts. Private individuals and organizations can enforce the statute in court. Congress did not intend to create a private cause of action to enforce the current regulations, according to the Court in Alexander v. Sandoval (2001), 532 U.S. 275. 102 See, for example, 43 C.F.R. § 17.1 (U.S. Department of Interior Title VI regulations). 103 President Kennedy’s message to Congress, June 19, 1963, quoted by Senator Hubert H. Humphrey, 110 Cong. Rec. 6543, quoted with approval in Lau v. Nichols (1974), 414 U.S. 563, 569. 104 Guardians Ass’n v. Civil Serv. Comm’n (1983), 463 U.S. 582, 629-30 (Marshall, J., dissenting on other grounds). 105 See, for example, Cal. Gov. Code § 11135; 22 CCR § 98101(i) (regulations). 106 See R. García and D. P. Hsu, “The Affordable Care Act and health justice in all policies,” KCET Green Justice column (Oct. 4, 2013), available at www.kcet.org/socal/departures/columns/green-justice/the-affordable-care-act-and-health-justice-in-all-policies.html; The Patient Protection and Affordable Care Act, Public Law 111-148, U.S. Statutes at Large 124 (2010), p. 119. Available at www.constitution.org/uslaw/sal/124_statutes_at_large.pdf. 107 Ibid. 108 See, for example, Patient Protection and Affordable Care Act, supra, sections 4001, 4201, 4306; D.P. Andrulis et al.,The Affordable Care Act & racial and ethnic health equity series: Report No. 4 public health and prevention programs for advancing health equity (Austin, TX: Texas Health Institute Press, Nov. 2013); American Public Health Association, Issue brief: Prevention provisions in the Affordable Care Act (Washington, DC: The National Academies Press, Oct. 2010). 109 Ibid. 110Federal Actions To Address Environmental Justice in Minority Populations and Low-Income Populations, Executive Order 12898, Federal Registrar 59/32 (1994). Available at www.archives.gov/federal-register/executive-orders/pdf/12898.pdf. 111 Presidential Memorandum accompanying Executive Order 12898 (1994). Available at www.epa.gov/swerffrr/documents/executive_order_12898.htm. 112 See R. Bullard et al., Environmental Justice: Milestones and Accomplishments 1964-2014, available at www.tsu.edu/academics/colleges__schools/publicaffairs/files/pdf/EJMILESTONES2014.pdf; R. García and A. White, Warren County’s Legacy for Healthy Parks, Schools, and Communities: From the Cornfield to el Congreso and Beyond, 1 Golden Gate University Environmental Law Journal 127 (2007). 113 National Research Council, Improving health in the United States: The role of health impact assessment (Washington, DC: The National Academies Press 2011). 114 Ibid. 115 See, for example, Ricci v. DeStefano, 557 U.S. 557, 581 (2009). 116 Village of Arlington Heights v. Metropolitan Housing Dev. Corp. (1977), 429 U.S. 266. 117 Federal Transit Administration, Environmental justice policy guidance for Federal Transit Administration recipients, Circular (FTA C 4703.1) (Washington, DC: Department of Transportation, Aug. 15, 2012); FTA, Title VI Requirements and Guidelines for Federal Transit Administration Recipients, Circular (FTA C 4702.1B) (Washington, DC: Oct. 1, 2012); Letters from FTA to Metropolitan Transportation Commission and San Francisco Bay Area Rapid Transit District (Jan. 15, 2010 and Feb. 12, 2010), available at www.cityprojectca.org/blog/archives/32984. 118 R. García, “The George Butler Lecture – Social Justice and Leisure,” Journal of Leisure Research 46/1 (2013), pp. 7-22; “Best Practice HUD Los Angeles State Historic Park Healthy Green Land Use for All,” The City Project Blog (Sept. 9, 2014), available at www.cityprojectca.org/blog/archives/32984. 119 Larry P. v. Riles (1984), 793 F.2d 969; U.S Department of Justice, Title VI Legal Manual at p. 51, goo.gl/k9ZQ7a. 120 Ibid; S. Carle, A New Look at the History of Title VII Disparate Impact Doctrine, 63 Fla. L. Rev. 251 (2011). 121 See “San Gabriel Mountains Best Practice Environmental Justice Framework for Parks, Health, and Conservation Values,” The City Project Blog (Sept. 5, 2014), available at http://www.cityprojectca.org/blog/archives/32899; “US Army Corps of Engineers LA River Study Best Practice Framework for Revitalization of the Los Angeles River,” The City Project Blog (Sept. 19, 2014), available at http://www.cityprojectca.org/blog/archives/33093. 122 See R. García, “The George Butler Lecture – Social Justice and Leisure,” Journal of Leisure Research 46/1 (2013), pp. 7-22; R. García and R. Sivasubramanian, “Environmental Justice for All: Struggle in Baldwin Hills and South Central Los Angeles,” Clearinghouse Review: Journal of Poverty Law and Policy (Nov/Dec 2012), available at www.cityprojectca.org/blog/archives/17836. 123 Cal EPA uses CalEnviroScreen (CES) as the tool to identify underserved communities for the distribution of cap and trade greenhouse gas reduction funds. See “Invest Cap and Trade Funds to Benefit Underserved Communities and Communities of Color,” The City Project Blog (Oct. 6, 2014), available at http://www.cityprojectca.org/blog/archives/33001. 124 Village of Arlington Heights v. Metropolitan Housing Dev. Corp. (1977), 429 U.S. 252, 265; Title VI Legal Manual, supra, at p. 51. 125 W. M. Byrd and L. A. Clayton, An American health dilemma: A medical history of African Americans and the problem of race: Beginnings to 1900 (London, UK: Routledge, 2000); W. M. Byrd and L. A. Clayton, “Racial and ethnic disparities in healthcare: a background and history,” in B. D. Smedley, A. Y. Stith & A. R. Nelson (eds.), Unequal treatment: Confronting racial and ethnic disparities in health care (Washington, DC: The National Academies Press, 2003), pp. 455-527; W. M. Byrd and L. A. Clayton, “Race, medicine, and health care in the United States: a historical survey,” J Nat’l Med Assoc 93/3 (2001). 126 M. Rodriguez and R. García, “First, Do no harm: The U.S. sexually transmitted disease experiments in Guatemala,” Am. J. of Public Health 103/12 (2013), pp. 2122-26. F. D. Gray, The Tuskegee syphilis study: the real story and beyond (Montgomery, AL: New South Books 1998). 127 Asian & Pacific Islander American Health Forum, “Susan Matsuko Shinagawa: Japanese American Breast Cancer Survivor,” A Book of Hope: Stories of Healing to Honor Asian American & Pacific Islander Cancer Survivors, (November 2007) pp. 7-11. 128 R. García and C. Fenwick, “Social Science, Equal Justice, and Public Health Policy: Lessons from Los Angeles,” Journal of Public Health Policy 30/ S26 (2009) (compliance with physical education requirements under education and civil rights laws). 129 See, for example, 28 C.F.R. § 42.406 (US Department of Justice regulations on racial and ethnic data collection); FTA, Title VI Requirements and Guidelines for Federal Transit Administration Recipients, Circular FTA C 4702.1A, chapter V (1) and V(1)(a)(2) at page V-1 (Oct. 1, 2012) (data collection including GIS and demographic analyses); FTA, Title VI Requirements and Guidelines for Federal Transit Administration Recipients, Circular FTA C 4702.1B, page IV -7 (Oct. 1, 2012); FTA, Environmental Justice Policy Guidance for Federal Transit Administration Recipients, Circular (FTA C 4703.1), pages 6, 8, 11 (Aug. 15, 2012); Executive Order 12898 Sec. 3-3 (research, data collection, and analysis). 130 Almendares v. Palmer (2002), 284 F. Supp. 2d 799, 808. 131 Ibid. 132 Ibid.

26
133 Rodriguez v. Lucas County Dep't of Job and Family Svcs, (2004) 3:00-cv-07524. 134 R. García and C. Fenwick, “Social science, equal justice, and public health policy: Lessons from Los Angeles,” Journal of Public Health 30/ S26 (2009) (compliance with physical education requirements under education and civil rights laws). 135 R. García, “The George Butler Lecture – Social Justice and Leisure,” Journal of Leisure Research 46/1 (2013), pp. 7-22. 136 U.S. Department of Health and Human Services, Request for information: Nondiscrimination in certain health programs or activities (August 2013). Available at www.regulations.gov/#!documentDetail;D=HHS-OCR-2013-0007-0001. 137 Almendares v. Palmer (2002), 284 F. Supp. 2d 799, 808; Larry P. v. Riles (1984), 793 F.2d 969; Lau v. Nichols (1974), 414 US 563. 138 See, for example, R. García and T. A. Rubin, “Cross Road Blues: Transportation Justice and the MTA Consent Decree,” in K. Lucas (ed), Running on empty (University of Bristol, UK: Policy Press, 2004); E. W. Soja, Seeking Spatial Justice (Minneapolis, MN: University of MN Press, 2010); Kevin Starr, Coast of Dreams: California on the Edge, 1990-2003, at pp. 553-554, 710-711 (N.Y., N.Y.: Alfred A Knopf, 2004). 139 See J. M. Powers, “On Separate Paths: The Mexican American and African American Legal Campaigns against School Segregation,” 121 American Journal of Education 29 (2014). 140 Hernandez v. Texas (1954), 347 U.S. 475. 141 A new wave of research on the Civil Rights Movement, Brown, and Title VI is emerging. See, for example, Gavin Wright, Sharing the Prize: The Economics of the Civil Rights Revolution in the American South (2013); Bruce Ackerman, The Civil Rights Revolution (2014); Robert Caro, The Years of Lyndon Johnson: The Passage of Power (2012); Clay Risen, The Bill of the Century: The Epic Battle for the Civil Rights Act (2014); Todd S. Purdum, An Idea Whose Time Has Come: Two Presidents, Two Parties, and the Battle for the Civil Rights Act of 1964 (2014). Earlier works include, for example, Jack Greenberg, Crusaders in the Courts: How a Dedicated Band of Lawyers Fought for the Civil Rights Revolution (1994); Richard Kluger, Simple Justice: The History of Brown v. Board of Education and Black America's Struggle for Equality (1975 and 2004); Taylor Branch, The King Years: Historic Moments in the Civil Rights Movement (2013). See generally R. García et al., Poverty & Race, “New Frontiers for Title VI,” Poverty & Race Research Action Council (July/Aug 2014), available at www.cityprojectca.org/blog/archives/34599; Centers for Disease Control and Prevention, Interview on Health and Civil Rights with Robert García, “Public Health Law News” (June 2014), available at www.cityprojectca.org/blog/archives/32237. 142 See S. Hansen, Cultivating the Grassroots: A Winning Approach for Environment and Climate Funders (Feb. 2012, National Committee for Responsive Philanthropy), available at www.ncrp.org/files/publications/Cultivating_the_grassroots_final_lowres.pdf. 143 P. Joassart-Marcelli et al., “Building the Healthy City: The Role of Non-profits in Creating Active Urban Parks,” 32 Urban Geography 682 (2011); P. Joassart-Marcelli, “Leveling the Playing Field? Urban disparities in funding for local parks and recreation in the Los Angeles region” 42(5) 1174 Environment and Planning (2010). 144 R. García, “Civil Rights Park 50th Anniversary Civil Rights Act of 1964,” KCET Green Justice column (July 2, 2014), available at www.cityprojectca.org/blog/archives/32290. 145 See, for example, Bill Lann Lee et al., Brief of Amici Curiae The Lawyers’ Committee for Civil Rights Under Law, et al., Texas Dep’t of Housing and Community Affairs et al., v. Inclusive Communities Project, Inc., No. 13-1371, U.S. Supreme Court (filed Dec. 23, 2014) (addressing disparate impact standard and residential segregation, education, economic mobility, health, environmental effects, and green access); Sherrilyn Ifill et al., Brief of Amicus Curiae NAACP Legal Defense & Educational Fund, Inc., Texas Dep’t of Housing and Community Affairs et al., v. Inclusive Communities Project, Inc., No. 13-1371, U.S. Supreme Court (filed Dec. 24, 2014) (analyzing disparate impact standard and constitutional strict scrutiny standard). The Fair Housing Act is Pub. L. No. 90-284, Title VIII of the Civil Rights Act of 1968, 82 Stat. 81 (1968). 146 J. Salzman et al., “The Most Important Current Research Questions in Urban Ecosystem Services, 25 Duke Env’l L. Policy Forum – (forthcoming 2014).