Embed Size (px)
Citation preview

Social Science & Medicine 53 (2001) 1575–1585
Using an interactive framework of society and lifecourse toexplain self-rated health in early adulthood
Clyde Hertzmana,*, Chris Powerb, Sharon Matthewsb, Orly Manorc
aDepartment of Health Care and Epidemiology, University of British Columbia, 5804 Fairview Avenue, Vancouver BC, Canada V6T 1Z3bDepartment of Epidemiology and Public Health, Institute of Child Health, University of London, UK
cSchool of Public Health and Community Medicine, Hebrew University, Jerusalem, Israel
Abstract
This paper presents an integrated model of the determinants of adult health combining lifecourse factors andcontemporary circumstances. Using the 1958 British Birth Cohort, it operationalises lifecourse influences in terms of
factors from birth to age 33, which might act through latent, pathway, or cumulative effects. Contemporarycircumstances are represented by variables at different levels of social aggregation: macro (socio-economiccircumstances); meso (involvement in civil society functions); micro (personal social support); and intersecting (job
insecurity and life control). Multiple regression models were fitted, using self-rated health at age 33 as the healthoutcome. To allow for temporal ordering of events, early life factors were entered first in the final model, followed bylater childhood factors and, finally current factors. Self-rated health was predicted by variables representing both early
and later stage of the lifecourse and also contemporary societal-level factors. The effects of childhood factors were notremoved by including contemporary factors, and conversely, contemporary factors contributed to the prediction of self-rated health over and above lifecourse factors. The factors were not collinear; supporting the notion that eachdimension was distinct from the others. Although the model accounted for only 9% of the variance in self-rated health,
the general conclusion is that both lifecourse and contemporary circumstances should be considered together inexplaining adult health. # 2001 Elsevier Science Ltd. All rights reserved.
Keywords: Longitudinal; Self-rated health; Socioeconomic status; Child development; Latent effects; Pathway effects; Cumulative
effects
Introduction
The study of the social determinants of healthinvolves two broad perspectives: one based upon thelifecourse and the other emphasising contemporary life
circumstances. Within these broad perspectives, alter-native models have been proposed connecting specificfactors with adult health. What is needed is a unified
framework that consolidates these models and integratesthe two perspectives.With regard to the lifecourse perspective, investigators
have postulated three processes whereby early life
environments may affect adult health: first, latent effectsby which early life environment affects adult health
independent of intervening experience; second, pathwayeffects, through which early life environment setsindividuals onto life trajectories that in turn affect
health status over time; and, third, cumulative effectswhereby the intensity and duration of exposure ofunfavourable environments adversely affects health
status, according to a dose–response relationship (Kuh& Ben-Shlomo, 1997; Marmot & Wadsworth, 1997;Power & Hertzman, 1997; Davey-Smith, Hart, Blane,
Gillis, & Hawthorne, 1997; Lynch, Kaplan, & Shema,1997). The essence of the latency model is that specificbiological (e.g. low birthweight) or developmental (e.g.visual acuity) factors at sensitive periods in (early) life
have a lifelong impact on health and well-being,
*Corresponding author. Tel.: +1-604-822-3002; fax: +1-
604-822-4994.
E-mail address: [email protected] (C. Hertzman).
0277-9536/01/$ - see front matter # 2001 Elsevier Science Ltd. All rights reserved.
PII: S 0 2 7 7 - 9 5 3 6 ( 0 0 ) 0 0 4 3 7 - 8

regardless of subsequent living conditions. It has beenargued that the link between low birthweight and
cardiovascular disease in adulthood is evidence of alatency effect (Barker, 1992). Similarly, the results fromearly childhood stimulation programs for disadvantaged
children are consistent with a latency effect, given theireffectiveness in improving adult outcomes even withoutany attempt to provide them with special help in theintervening years (Palmer, 1979; Schweinhart, Barnes, &
Weikart, 1993).In practice, latency effects can be difficult to disen-
tangle from pathway effects. This is because the path-
ways model acknowledges that differences in early lifeenvironment may direct children onto different lifecourses. To illustrate, stimulation, stability and security
in early childhood affect the child’s readiness forschooling (Case & Griffin, 1991). In turn, lack of schoolreadiness leads to an increased risk of behavioural
problems and, also, to school failure (Pulkkinen &Tremblay, 1992). Behavioural problems and failure inschool lead to low levels of mental well-being in earlyadulthood (Power, Manor, & Fox, 1991). Meanwhile,
the status of one’s parents helps to determine thecommunity where one grows up, which, by the earlyschool years, starts to influence the child’s life chances
through the social networks, community values, andopportunities which present themselves (Haan, Kaplan,& Camacho, 1987).
The third process linking early life environment andadult health recognizes the importance of cumulativeeffects, wherein the focus is on the accumulation ofadvantage or disadvantage over time, based upon the
duration and intensity of exposure to the factor(s) ofinterest. For instance, a cumulative effect of income issuggested by the stronger association with mortality
found for earnings over several years than for single-year earnings (McDonough, Duncan, Williams, &House, 1997). With respect to socio-economic circum-
stances, it was shown that mortality risk in a prospectivestudy of Scottish men was graded by cumulative socialclass, comprising class of origin, at labour market entry,
and in later adulthood (Davey-Smith et al., 1997).Cumulative and pathway effects have also been estab-lished in the 1958 cohort (Power, Manor, & Mathews,1999): socio-economic conditions from birth to age 33
had a cumulative effect on self-rated health in additionto that of level of education achieved (a pathway effect).Simultaneous examination of education and cumulative
soico-economic conditions showed independent associa-tions, though with slightly diminished effects afteradjusting for the other factor.
As explained above, there is in addition to thelifecourse perspective, a major focus on contemporarycircumstances as determinants of adult health. These can
be organized according to three levels of social aggrega-tion. At the most ‘‘macro’’ or broadest level there is the
national socioeconomic environment. The principaldeterminants of health at this level are income per
capita and how equitably it is distributed (Wilkinson,1997; Kaplan, Pamuk, Lynch, Cohen, & Balfour,1996). Among countries with per capita income below
$10–15,000 US, increasing national income stronglycorrelates with increasing health status (World Bank,1993); above this level, equity of income distributionmatters more than variations in national income
per se.At the ‘‘meso’’ or civil society level, there are a
series of factors that include voluntarism; social
affiliation, trust, and cohesion; and the capacity ofimportant social institutions to respond to currentand changing human needs. Variables as diverse as
psychosocial work characteristics and the level ofmembership in service organizations can be regardedas aspects of civil society. This construct has been
studied by different investigators (Putnam, 1993; Rose,1995; Kaplan et al., 1996; Kawachi, Kennedy, Lochner,& Prothrow-Stith, 1997), often under the label ‘‘socialcapital’’. We avoid this term because it is not clear
whether the characteristics of ‘‘capital’’, as understoodby economists, applies here. Finally, at the most‘‘micro’’ level, there are the determinants of health
associated with private life (Berkman, 1995): the qualityof intimate relationships, access to social support, andthe availability of informal help to solve the problems of
daily life.To date, it has not been resolved as to how the
lifecourse perspective fits with models of the determi-nants of health that focus exclusively on contemporary
adult circumstances. Our purpose here is to propose anintegrated model of the determinants of adult healththat combines lifecourse and contemporary circum-
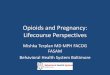
stances. Fig. 1 presents our conceptual framework. Itrepresents contemporary circumstances at three levels ofsocial aggregation (macro, meso and micro) in the form
of a bullseye, while representing the individual lifecourseas an arrow passing through the bullseye at an arbitrarylifestage. The arrow runs left to right, from gestation to
old age, subsuming latent, pathway and cumulativeeffects. Latent factors are, by definition, found towardsthe beginning of the arrow, whilst pathway andcumulative factors unfold along it. The underlying
assumption of this framework is that adult health isdetermined by both lifecourse and contemporary factors,and not exclusively one or the other.
We propose to test the validity of this frameworkusing data from the 1958 British birth cohort; whichis one of the few studies with sufficient data to model
both lifecourse and contemporary circumstances, usingself-rated health at age 33 as the outcome. To ourknowledge, this is the first time that such an exercise has
been attempted with detailed longitudinal data frombirth.
C. Hertzman et al. / Social Science & Medicine 53 (2001) 1575–15851576

Methods
Study sample and overview of determinants of health
The 1958 birth cohort includes all children born in
England, Wales and Scotland during the 3–9 March1958. The study originated in the Perinatal MortalityStudy, which gathered information on 16,964 live births(97% of all births, after excluding deaths and refusals).
Information was obtained from parents, teachers,medical officers and individuals themselves at subse-quent follow-up at ages 7, 11, and 16, and from a
personal interview with study subjects at ages 23 and 33.Despite sample attrition, those remaining in the study(11,405 subjects at age 33) were found to be generally
representative of the original sample (Ferri, 1993).We have operationalised the socio-economic environ-
ment with individual cohort member’s reports of their
circumstances; the civil society with their organizationalparticipation, social trust, and job control; their socialsupport with marital status and perceived emotionalsupport; and intersecting factors with job insecurity and
life control.Lifecourse influences which have been identified as
predictors of adult health, and are available in the 1958
cohort, include birth weight and rate of physicaldevelopment, early cognitive and behavioural develop-ment, socio-economic circumstances of the family,
quality of the home environment from the standpointof stimulation and support; academic success and soico-emotional adjustment during adolescence. In terms ofsocietal level influences, socio-economic status, social
trust and participation, marital status, and availabilityof social support are all recorded for analysis. Further-more, the 1958 cohort includes additional factors, such
as job insecurity and life control, which representinteractions between lifecourse and societal level factors.
Health measure
At age 33 cohort members gave a general assessment
of their health, rates as (1) excellent, (2) good, (3) fair or(4) poor.
Lifecourse factors
Early life (age 0–7)Birthweight was recorded in pounds/ounces and
converted into grams. Height at age 7 was measured bythe medical staff, to the nearest inch and converted intometres, and used as a continuous measure in meters and
as a percentage of adult height at age 33. Social andemotional status at age 7 was assessed by teachers usingthe Bristol Social Adjustment Scale (Stott, 1969). The
scale consists of 146 ‘items of behaviour’ representing thefollowing syndromes: unforthcomingness, withdrawal,
depression, anxiety for acceptance, disregarding adults,restlessness, inconsequential behaviour and other symp-
toms. The total score of these items was transformed(square root transformation) to improve the normality ofthe distribution. High scores are indicative of poor
emotional adjustment. Parental interest in the child’seducation at age 7, (both parents, unless single parenthousehold) assessed by the teacher, was categorised assome interest versus little interest. Frequency of parents’
reading to the child at age 7, was based on reportedweekly reading habits. Oral, reading and creative abilityat age 7, was assessed by the teacher and categorised as
in Table 2. Walking unaided by 1.5 years and talking byage 2 was reported by mothers in 1964. Enuresis: daytime(wet by day after age 3) and night-time (wet by night
after age 5) was reported by mother in 1964.
Cumulative (age 7–33)
Here and in the tables we use ‘cumulative’ as a term ofconvenience to refer to all the lifecourse variablesbeyond early childhood.Childhood socio-economic circumstances is indicated by
social class, based on father’s occupation at the time ofthe respondent’s birth, and when the respondent wasaged 7, 11, and 16. To minimise sample attrition, where
social class data was not available, social class from theprevious sweep was used. A score was calculated fromthe number of ages in which subjects lived in social
classes: I & II (professional and managerial), III non-manual (unskilled), III manual (skilled), and IV & V(unskilled manual). The score ranged from 4 for the most
favourable to16 for the least favourable childhood socio-economic circumstances. Adolescent social and emotionalstatus is indicated by the Rutter behaviour scale at ages11 and 16. The scale (teacher’s assessment) comprises 26
items of behaviour and emotional status, such asrestlessness, and truancy. Total scores were transformed(square root transformation) (Rutter, 1967; Ghodsian,
Fogelman, Lambert, & Tibbenham, 1980; Elander &Rutter, 1995) and summed across the two ages to form asummary measure. End of school qualifications was
grouped as: more than 2 ‘A’ levels, more that 4 ‘O’levels but less than 2 ‘A’ levels; up to 4 ‘O’ levels, and lessthan ‘O’ level. Educational qualifications obtained by age33 was classified as: above ‘A’ level, ‘A’ level or
equivalent, ‘O’ level or equivalent, less than ‘O’ level,and no qualifications. (This ordinal scale roughlytranslates into the North American ordinal: completed
college or university, some college or university, highschool completion, some high school, no high school.)
Societal-level factors
Macro level
Prevailing national socio-economic conditions wererepresented by: socio-economic circumstances, as
C. Hertzman et al. / Social Science & Medicine 53 (2001) 1575–1585 1577

indicated by social class from the cohort member’s ownoccupation at age 33 (categorised as professional and
managerial (I & II), unskilled non-manual (IIInm), skilledmanual (IIIm), or unskilled manual (IV & V)). Men andwomen were classified on the basis of their own current or
most recent occupation. Current material circumstanceswere indicated by a composite variable derived from threedichotomous items: (1) no savings at age 33, (2) rentedhousing at age 33, and (3) receipt of social security
benefits (income support, supplementary or unemploy-ment benefit) by subject or partner at age 33).
Meso levelFour variables were used to represent civil society:
Social trust, as indicated by respondent’s choice between
two statements: ‘‘I find that most people can be trusted’’or ‘‘I find that I cannot be too careful in dealing withother people.’’ Availability of financial support, as
indicated by respondent’s assessments of whether or notthey could borrow a large sum of money, either frompersonal sources (e.g. spouse/partner, other relatives orfriends), or organisational sources (e.g. charity, social
services or financial institutions). Psychosocial job strainat age 33, based on lack of learning opportunities,monotony, inability to vary work pace, and inflexible
break times, experienced in the main work place(including home and family care). Negative character-istics were summed to indicate high psychosocial strain
(Matthews, Hertzman, Ostry, & Power, 1998). Organisa-tional participation, was based on respondent’s reports atage 33 of all organisations they had ‘ever’ belonged to,
including: political parties, charities, women’s groups,parent school organisations, and residents associations.
Micro level
Social support at age 33 was represented by: Currentmarital status: categorised as married or cohabitingversus single, separated or divorced. Emotional support
was reported for advice seeking, confiding, and problemsharing and individuals with few sources of support wereidentified (Matthews, Stansfeld, & Power, 1999).
Intersecting factors
Current factors at age 33 representing: Job insecurity,was based on respondent’s assessments of the futureusefulness of their work skills. Life control, respondentsidentified statements that were mostly true from (1) ‘I
never really seem to get what I want out of life’ or ‘Iusually get what I want out of life’. (2) ‘I usually have afree choice and control over my life’ or ‘Whatever I do
has no real effect on what happens to me’. (3) ‘usually Ican run my life more or less as I want to’ or ‘I usuallyfind life’s problems just too much for me’. These three
items were summed to indicate degree of perceived lifecontrol.
Data analysis
A series of multiple linear regression models werefitted, using self-rated health (scored 1,2,3 and 4) at age33 as the dependent health outcome. We selected
multiple linear regression because it provides a simplemethod with which to identify the strongest correlates ofhealth within each factor, and by adding factors inblocks, it afforded a simple way to impose the frame-
work on the data. Although linear regression is moreappropriate for a continuous outcome variable, it isrecognised as a robust method in other circumstances,
especially when the sample size is large (Miller, 1986).The analysis was performed in three stages. First, the
effects of groups of factors on self-rated health were
assessed in 6 analyses, that is for the 2 groupsrepresenting lifecourse factors (early life and cumulativefactors), and for the four groups representing societal
level factors (socio-economic, civil society, social sup-port and intersecting factors). Second, those variablesfrom across the six groups which were most significantly(p50:05) associated with self-rated health were selected
and incorporated into a further model, with theadditional inclusion of gender. Variables that weresignificant (p50:05) or of borderline significance were
then selected for a final model. To allow for thetemporal ordering of events, early life factors wereentered first in the final model, followed by cumulative
factors and, finally, current factors. We examine maineffects and not interactions between the factors. Initially,all analyses were conducted before and after adjustingfor gender. These analyses showed similar results and
hence gender is omitted from the analyses reported here.A potential problems in some of the regression models iscollinearity arising from the correlation between the
independent variables. Using the variance inflatingfactors method (Kleinbaum, Kupper, & Muller, 1988),we assessed the size of this problem and its impact on the
estimated parameters and found that the results werenot affected by collinearity.Individuals numering 6464 were included in the final
model. We therefore examined whether this sample wasrepresentative of those included in the original birthsurvey. Table 1 shows that the sample used for the finalmodel had a similar social class distribution to the
original birth sample. We also compared the samplesused in preliminary stages of analysis and found noserious biases with respect to social class at birth. Table
2 gives details (range and categories) of the measuresused in the analyses.
Results
Table 3 presents the regression coefficients and theassociated level of significance for the two groups of
C. Hertzman et al. / Social Science & Medicine 53 (2001) 1575–15851578

lifecourse factors. Several early life factors were sig-nificantly associated with self-rated health at age 33. Thegreatest effects were seen for reading ability at age 7 andthe percentage of adult height attained by age 7.
Intermediate effects were found for parental frequencyof reading to their child, height, socio-emotional statusand parental interest in education all at age 7. Smaller
significant effects emerged for oral ability at age 7 andwalking unaided by 1.5 years. Consequently, self-ratedhealth declined with decreasing reading and oral ability,
poorer emotional adjustment, parental reading fre-quency and interest in education, and with decreasingstature. In contrast, the positive coefficient for percen-tage of adult height attained by age 7 suggested that
health deteriorated with increasing percentage of heightattained during childhood. Further analyses revealedthat health was poorer for those with delayed and with
accelerated growth in childhood. These birth to age 7factors accounted for 3% of the variance in self-ratedhealth at age 33, whereas cumulative factors accounted
for 5% of the variance. All four cumulative factors weresignificantly associated with adult self-rated health, withthe strongest effect emerging for educational qualifica-
tions achieved by age 33 (standardised b ¼ 0:114),followed by adolescent socio-emotional status (standar-dised b ¼ 0:078). Thus, self-rated health deterioratedwith increasing socio-economic, emotional and educa-
tional disadvantage.Associations between societal level factors and self-
rated health are presented in Table 4. The variance
explained by the different societal level factors rangedfrom 6 (intersecting factors) to 0.5% (micro level). Ateach societal level, all except availability of financial
support and organisational participation (meso level)were significantly associated with self-rated health.Within each societal level, the strongest effects werefound for current material circumstances as age 33
(Standardised b ¼ 0:154) at the macro level; psychoso-
cial job strain at age 33 (standardised b ¼ 0:108) at themeso level; current marital status (standardised
b ¼ 0:065) at the micro level; and finally, life control(standardised b ¼ 0:207) as an intersecting factor.Health deteriorated with poorer material circumstances,
greater job strain, single marital status and lack ofperceived life control.All variables in Tables 3 and 4 that were significantly
associated with self-rated health were included in a
further multiple regression model. Twenty variableswere analysed simultaneously (results not shown).Height at age 7, parental interest in education, oral
ability, reading ability, walking alone by age 1.5 years,educational qualifications and social class at age 33,marital status, and emotional support were no longer
significant (p > 0:05) in this multivariate analysis andwere therefore excluded from the final model. Table 5presents the final model for self-rated health at age 33 as
predicted by 11 variables, representing each of the twogroups of lifecourse factors and three of the four groupsof societal-level factors. The strongest effects wereobserved for life control and job insecurity (intersecting
factor), current material circumstances (macro levelfactor), and also for end of school qualifications andsocio-economic circumstances from birth to age 16 years
(cumulative factors). Overall, the model accounted for9% of the variance in self-rated health.
Discussion
The framework presented here, performed well inidentifying distinct groups of lifecourse and contempor-ary factors that influence self-rated health by age 33. Inso doing, the notion that lifecourse and contemporary
factors ought to be considered together has beenvalidated. However, the proportion of variance ex-plained by this specific model, using the variables
available to us, was not very high. Thus, we mustregard this analysis as a starting point and furtherrefinements of the framework and analytic methods are
a priority.Our outcome measure, self-rated health, could be
criticised for its subjectivity. Subjectivity could be
especially problematic when investigating ‘sense ofcontrol of life’ as a determinant of health, since a lackof good health may well be experienced by the individualas loss of control. Although this is a legitimate concern,
self-rated health also has notable strengths as anoutcome measure. It is recognized as a valid surrogateindicator for fitness (Allied Dunbar National Fitness
Survey, 1992) and for morbidity (Power et al., 1991). Aswell, it has been consistently shown to predict mortality(Kaplan & Camacho, 1983; Wannanethee & Shaper,
1991; Idler & Angel, 1990; Cox, Huppert, & Whichelow,1993); such that mortality rates increase monotonically
Table 1
Social class distribution of the analysis samplea compared with
the original birth sample
Social class
at birth
Original birth
sample
Analysis samplea
% (n) % (n)
I & II 17.0 (2879) 18.1 (1170)
IIInm 9.4 (1593) 10.6 (686)
IIIm 49.3 (8371) 50.4 (3255)
IV & V 21.3 (3611) 18.9 (1219)
No male head
of household
3.0 (510) 2.1 (134)
Total 16964 6464
aAnalysis sample=6464 individuals with complete data
included in the best-fit model.
C. Hertzman et al. / Social Science & Medicine 53 (2001) 1575–1585 1579

Table 2
Details of measures (range) and categorisation
Self-rated health Range Categories
1–4 Excellent! good! fair! poor
Lifecourse factors
Birthweight – per 100 ga 5.943–59.996 Low weight to high weight
Height at age 7ma 0.91–1.55 Short to tall
Social and emotional status 0.61–7.96 Well adjusted to poorly adjusted
Parental interest in child’s education, age 7 0, 1 Some interest or little interest
Reading to child age 7–reading score 0–4 Reads every week to hardly ever
Oral ability at age 7 1–5 Expresses well, good vocabulary, average, below
average, very poor ability
Reading ability at age 7 1–5 Avid reader, above average, average reader, poor
average, non reader
Creative ability at age 7 1–5 Marked creativity, good, some, little, no creativity
Walking unaided by 1.5 years 0–1 Yes/don’t know or no
Talking by age 2 0–1 Yes/don’t know or no
Daytime enuresis after age 3 0–1 No/don’t know or yes
Night-time enuresis after age 5 0–1 No/don’t know or yes
% of adult height by age 7a 56.1–99.6 Low to high
Cumulative factors
Socio-economic circumstances, at birth,
7, 11, 16 years
4–16 Social class I & II at all 4 ages to social class IV & V
at all 4 ages (Cronbach’s alpha=0.90)
Socio-emotional status, ages 11 and 16 0–13.6 Well adjusted to poorly adjusted
End of school qualifications 1–4 More than 2 A levels, more than 4 O levels but less
than 2 A levels, up to 4 O levels, less than O level
Educational qualifications by age 33 1–5 Above A level, A level or equivalent, O level or
equivalent, less than O level, no qualifications
Societal level factors
Macro level
Current material circumstances, age 33 0–3 Sum of rented housing, social security benefits
recipient, no savings
Socio-economic circumstances, age 33 1–4 Social class I & II, IIInm, IIIm, IV & V
Meso level
Social trust 0–1 ‘I find most people can be trusted’ or ‘can not be too
careful’
Availability of financial support 0–1 Support or low support
Psychosocial job strain 0–4 No negative work characteristics to all 4 negative
work characteristics (Cronbach’s alpha=0.32)
Organisational participationa 0–7 Number of organisations: low to high participation
Micro level
Marital status 0–1 Married or cohabiting versus single/divorced–sepa-
rated/widowed
Emotional support 1–4 Supported to lacking support
Intersecting factors
Job insecurity – present skills will be useful in
5 years time
1–5 Very true, somewhat true, neither true/untrue,
somewhat untrue, not at all true
Life control score 0–3 No control on 0, 1, 2 or 3 dimensions (Cronbach’s
alpha=0.63)
a Indicates variables where the higher scores are the ‘‘better’’ state. In all other cases, higher sources are ‘‘worse’’.
C. Hertzman et al. / Social Science & Medicine 53 (2001) 1575–15851580

with successively poorer self-rating of health (Idler &Benyamini, 1997). Self-rated health is treated in ourstudy as a proxy measure for incidence, rather than a
prevalence measure because approximately 70% of
those reporting fair and poor self-rated health at age33 had not done so at age 23. Thus, most of those withfair or poor health fit the definition of incident cases.
This is important, because an incident measure can be
Table 3
Regression coefficients for lifecourse factors and adult self-rated health (age 33)a
Lifecourse factors Std b b (SE)
(a) Early life (age 0–7) (n ¼ 7941)
Birthweight 0.0008 0.0001 (0.002)***
Height at age 7 �0.054 �0.650 (0.152)***
Socio-emotional status, at age 7 0.048 0.025 (0.007)***
Parental interest in education, at age 7 0.049 0.103 (0.025)***
Parents read to child at age 7 �0.054 0.029 (0.006)*
Oral ability at age 7 0.037 0.028 (0.011)***
Reading ability at age 7 0.069 0.054 (0.012)
Creativity ability at age 7 0.018 0.015 (0.013)*
Walking unaided by age 1.5 0.027 0.099 (0.041)
Talking by age 2 �0.0002 �0.0007 (0.034)
Daytime enuresis after age 3 0.007 0.024 (0.043)
Night-time enuresis after age 5 �0.007 �0.017 (0.027)
% of adult height by age 7 0.065 0.012 (0.002)***
(b) Cumulative factors (n ¼ 8530)
Socio-economic circumstances, at birth, 7, 11, 16 y 0.067 0.013 (0.002)***
Socio-emotional status, at ages 11 and 16 0.078 0.025 (0.004)***
End of school qualifications 0.042 0.028 (0.009)**
Educational qualifications by age 33 0.114 0.062 (0.008)***
a r (r2 adjusted)=0.19 (0.03) for lifecourse factors and 0.22 (0.05) for cumulative factors.
*p50.05; **p50.01; ***p50.001.
Table 4
Regression coefficients for societal level factors and adult self-rated health (age 33)a
Societal-level factors Std b b (SE)
(c) Macro level (n ¼ 11026)
Socio-economic:
current material circumstances at age 33 0.154 0.139 (0.009)***
socio-economic circumstances at age 33 0.113 0.069 (0.006)***
(d) Meso level (n ¼ 9885)
Civil society:
social trust 0.099 0.146 (0.015)***
availability of financial support �0.016 �0.022 (0.014)***
psychosocial job strain, at age 33 0.108 0.077 (0.007)***
organisational participation, by age 33 �0.015 �0.014 (0.009)
(e) Micro level (n ¼ 10341)
Social support:
current marital status at age 33 0.065 0.099 (0.015)***
emotional support at age 33 0.025 0.017 (0.007)**
(f) Intersecting factors (n ¼ 10132)
job insecurity at age 33 0.093 0.055 (0.006)***
level of control in life 0.207 0.187 (0.009)***
a r (r2 adjusted)=0.22 (0.05) for macro level, 0.22 (0.05); 0.15 (0.02) for meso level, 0.07 (0.005) for micro level, and 0.24 (0.06) for
intersecting factors.
*p50.05; **p50.01; ***p50.001.
C. Hertzman et al. / Social Science & Medicine 53 (2001) 1575–1585 1581

the outcome of the time-dependent factors in the model,
whereas a prevalent measure may not be.Another potential refinement concerns our use of self-
reports of social participation and trust, rather thandirect measures of the civic qualities of the communities
where the cohort members lived and worked. None-theless, these variables proved to be stronger predictorsof self-rated health than the ‘‘micro’’ level factors
examined. The latter should be more fully exploredbefore their potential influence can be dismissed. Inparticular, it would be useful to have more details about
how well an individual’s personal support buffers thestresses of daily living. Inclusion of such variables waslikely to improve the explanatory power of the model
which, using our existing variables, explained only 9%of the variance. Finally, alternative statistical techni-ques, such as hierarchical modeling, may improve theapproach to the temporal relationships between different
lifecourse influences and, also, to factors operating atdifferent levels of social aggregation. Yet, futureattempts at more complex modeling will only be useful
if they maintain the clarity of the approach taken here,and produce results that are easily understood in termsof the framework in Fig. 1.
The analysis reveals general insights into the frame-work and, also, specific insights into the predominantinfluences on self-rated health in early adulthood. Threegeneral points are worthy of note. First, adult health was
predicted by variables representing the lifecourse, both
early life and cumulative/pathway factors, and alsocontemporary circumstances, as identified in Fig. 1.Most importantly, the effects of childhood factors were
not removed by including contemporary factors, andconversely, contemporary factors contributed to theexplanation of adult health over and above lifecourse
factors. Second, five of the six groups of factors, that is,all except micro level (social support) made a contribu-tion. Third, the finding that the factors were statistically
independent from one another supports the validity ofthe integrative framework in Fig. 1.In creating a unified framework, we have gone beyond
the hitherto disparate approaches of previous studies
that tend to focus exclusively on life course explanations
Table 5
Final model for explaining self-rated health at age 33 (n ¼ 6:464)a
Item Std b b Se
Early life (ages 0–7)
Socio-emotional status, at age 7 0.031 0.016 (0.007)*
Parents read to child at age 7 0.043 0.022 (0.006)***
% of adult height at age 7 0.031 0.006 (0.002)*
Cumulative
Socio-economic circumstances at birth, 7, 11, 16 years 0.057 0.011 (0.003)***
Socio-emotional status, at ages 11 and 16 end of school qualifications 0.041 0.013 (0.004)**
End of school qualifications 0.065 0.042 (0.009)***
Macro: socioeconomic
Current material circumstances at age 33 0.070 0.065 (0.012)***
Meso: civil society
Social trust 0.036 0.054 (0.018)**
Psychosocial job strain 0.035 0.026 (0.009)**
Intersection factors
Job insecurity at age 33 0.056 0.034 (0.008)***
Life control 0.139 0.127 (0.012)***
a r (r2 adjusted)=0.30 (0.09).
*p50:05; **0.01; ***p50:001.
Fig. 1. Framework for human development and the determi-
nants of health.
C. Hertzman et al. / Social Science & Medicine 53 (2001) 1575–15851582

for adult health outcomes (Wannamethee, Whincup,Shaper, & Walker, 1996; Gliksman et al., 1995; Vagero
& Leon, 1994; Mare, 1990) or alternatively on con-temporary circumstances (Drever & Whitehead, 1997;Kaplan et al., 1996; Kawachi et al., 1997). Our research
has shown that this fragmentation in approach is notjustified and that future work should attempt to betterunderstand how lifecourse and contemporary circum-stances act together to support or undermine health.
We carried out additional analyses to establish thevalidity of the results obtained from multiple linearregression. We examined residual plots and found no
evidence of a major violation of the model’s assump-tions. We also extended previous work in which therelationship between lifetime social class and self-rated
health was examined with alternative statistical meth-ods, including logistic regression and several regressionmodels for ordered categorical variables (Manor,
Mathews, & Power, 2000). We found that results fromlinear regression were broadly similar to those obtainedusing the alternative statistical methods. Finally, wecompared results from the final multiple linear regres-
sion model with a parallel logistic regression analysis inwhich self-rated health was dichotomised (excellent andgood health versus fair or poor) and found similar
results.As regards the specific findings on the influences on
self-rated health, several observations are noteworthy.
The strongest factors in the final model } notablycurrent level of control in life and material circum-stances, qualifications achieved by the end of school,cumulative socio-economic circumstances, and job
insecurity } emphasize current and cumulative circum-stances, as might emerge from a cross-sectional analysisof this health indicator. However, the persisting though
weakened effect of early life factors, most notably‘parents read to child at age 7’, suggests the enduringimportance of a stimulating early environment. Given
that the effect of this factor is weakened in the finalmodel suggests that it is on a pathway leading to latereducational achievement and adult circumstances, and
thence, to poor self-rated health in adulthood. Stimula-tion in the early home environment, as indexed byfrequency of parental reading with their child, is alsolikely to affect the child’s social and emotional develop-
ment. The latter is known to link subsequently with arange of adult characteristics that affect health eitherdirectly (such as in terms of psychological status), or
indirectly, possibly through health-related behaviours.Thus, the child’s socio-emotional development providesan additional pathway through to adult health. We
cannot discount the possibility, however, that these earlylife factors operate not just through pathways but thatthey also have a latent effect. Nor can we determine,
from the approach use here, whether the association forslow growth in childhood (indexed by ‘percent of adult
height achieved by age 7’) is reflecting a latent orpathway effect. Arguments could be made for either of
these lifecourse models. Irrespective of how the parti-cular early life factors identified here relate to adult self-rated health, the findings are consistent with other
observations, such as the finding that both rate ofgrowth and socio-emotional functioning are influencedby early life stimulation (Grantham-McGregor, Powell,Walker, & Himes, 1991).
We have shown elsewhere that cumulative socio-economic circumstances influence the risk of poor healthrating in early adulthood (Power et al., 1999). From the
evidence presented here, it appears as though the effectof duration of exposure to disadvantage is distinct fromother influences, in that it is not merely representing a
range of home and individual factors, such as parentalreading and the child’s growth, that predict poor-ratedhealth in early adulthood. In terms of contemporary
circumstances, social trust and psychosocial job strainare shown to predict self-rated health even aftereducation and current material circumstances areconsidered. Although these have been developed as
distinct theoretical constructs, this is the first empiricaldemonstration that their effects on health status mayalso be distinct. Similarly, we found that job insecurity
predicted self-rated health after allowing for the effectsof educational level. This was surprising because it wasexpected that our measure of job insecurity may also be
a proxy for educational and skill level.Notwithstanding the fact that most of the factors had
an independent effect on self-rated health, the micro-level factors were the most weakly predictive on their
own, and did not contribute at all to the final model.These results may be seen as surprising, since socialsupport, one of the micro-level variables, is widely
acknowledged as a predictor of mortality in later life.However, to our knowledge, micro-level variables suchas social support have rarely been analysed in a younger
adult cohort, and never with so many other lifecourseand contemporary factors being considered simulta-neously. In the context of the 1958 birth cohort, it will be
important to assess the influence of micro-level variablesas the cohort ages.The results of this research have relevance to policy
discussions, especially with respect to policies on child
development. The finding that factors in childhoodindependently contribute to adult health supplies arationale for policies that improve the circumstances in
which children grow up, live, and learn. Moreover,attention to childhood factors should be seen as part ofa strategy for addressing inequalities in health. In
Canada, these perceptions have already motivated theannouncement, in the l999 Speech from the Throne, ofan inter-sectoral National Children’s Agenda, wherein
improving the socio-economic and psychosocial circum-stances of children is proposed as a way to improve
C. Hertzman et al. / Social Science & Medicine 53 (2001) 1575–1585 1583

developmental trajectories and, therefore, health statusin adult life. In Britain, the recent Acheson Report
(1998) makes recommendations that are consistent withthe perspective that policies to reduce health inequalitiesthrough intervening in contemporary circumstances
need to be supplemented with policies to improvecircumstances in early childhood. Our research suggeststhat these recommendations should be given closeconsideration.
Acknowledgements
The research was supported by the Canadian Institutefor Advanced Research (who support C. Hertzman and
C. Power) and the UK Economic and Social ResearchCouncil under the Health Variations Programme(L128251021).
Data acknowledgementCentre for Longitudinal Studies, Institute of Educa-
tion, National Child Development Study CompositeFile including selected Perinatal Data and sweeps one to
five [computer file]. National Birthday Trust Fund,National Children’s Bureau, City University SocialStatistics Research Unit [original data producers].
Colchester Essex: The Data Archive [distributor], 21June 1994. SN: 3148.
References
Acheson, D. (1998). Independent inquiry into inequalities in
health. London: The Stationary Office.
Allied Dunbar National Fitness Survey. (1992). London: Sports
Council and Health Education Authority.
Barker, D. J. P. (1992). Fetal and infant origins of adult disease.
London: British Medical Journal.
Berkman, L. F. (1995). The role of social relations in health
promotion. Psychosomatic Medicine, 57, 245–254.
Case, R., & Griffin, S. (1991). Rightstart: An early intervention
program for insuring that children’s first formal learning of
arithmetic is grounded in their intuitive knowledge of numbers.
Report to the James S. McDonnell Foundation.
Cox, B. D., Huppert, F. A., & Whichelow, M. J. (1993). The
health and lifestyle survey: Seven years on. Aldershot:
Darmouth Publishing.
Davey Smith, G., Hart, C., Blane, D., Gillis, C., & Hawthorne,
V. (1997). Lifetime socioeconomic position and mortality:
Prospective observational study. British Medical Journal,
314, 547–552.
Drever, F., & Whitehead, M. (1997). Health inequalities. Office
for National Statistics Decennial (Suppl. 15, pp. 2–6).
London: The Stationary Office.
Elander, J., & Rutter, M. (1995). Use and development of the
Rutter parents’ and teachers scales. International Journal of
Methods in Psychiatric Research, 5(151), 1–16.
Ferri, E. (ed.), (1993). Life at 33: The fifth follow-up of the
national child development study. London: National Chil-
dren’s Bureau.
Ghodsian, M., Fogelman, K., Lambert, L., & Tibbenham, A.
(1980). Changes in behaviour ratings of a national sample of
children. British Journal of Social and Clinical Psychology,
19, 247–256.
Gliksman, M. D., Kawachi, I., Hunter, D., Colditz, G. A.,
Manson, J. E., Stampfer, M. J., Speizer, F. E., Willett, W.
C., & Hennekens, C. H. (1995). Childhood socioeconomic
status and risk of cardiovascular disease in middle aged US
women: a prospective study. Journal of Epidemiology and
Community Health, 49, 10–15.
Grantham-McGregor, S. M., Powell, C. A., Walker, S. P., &
Himes, J. H. (1991). Nutritional supplementation, psycho-
social stimulation, and mental development of stunted
children: the Jamaica Study. Lancet, 338, 1–5.
Haan, M., Kaplan, G. A., & Camacho, T. (1987). Poverty
and health: prospective evidence from the Alameda
Country study. American Journal of Epidemiology, 125,
989–997.
Idler, E. L., & Angel, R. L. (1990). Self rated health and
mortality in the NHANES-1 epidemiologic follow up study.
American Journal of Public Health, 80(4), 446–452.
Idler, E. L., & Benyamini, Y. (1997). Self-rated health and
mortality: A review of twenty-seven community studies.
Journal of health and Social Behaviour, 23, 21–37.
Kaplan, G. A., & Camacho, T. (1983). Perceived health and
mortality: A nine-year follow-up of the human population
laboratory cohort. American Journal of Epidemiology, 117,
292–304.
Kaplan, G. A., Pamuk, E. R., Lynch, J. W., Cohen, R. D., &
Balfour, J. L. (1996). Inequality in income and mortality in
the United States: analysis of mortality and potential
pathways. British Medical Journal, 312, 999–1003.
Kawachi, I., Kennedy, B. P., Lochner, K., & Prothrow-Stith,
D. (1997). Social capital, income inequality, and mortality.
American Journal of Public Health, 87, 1491–1498.
Kleinbaum, D. G., Kupper, L. K., & Muller, K. E. (1988).
Applied regression analysis and other multivariable methods.
California: Duxbury Press.
Kuh, D. L., & Ben-Shlomo, Y. (1997). A life course approach to
chronic disease epidemiology: Tracing the origins of ill health
from early to adult life. Oxford: Oxford University Press.
Lynch, J. W., Kaplan, G. A., & Shema, S. J. (1997). Cumulative
impact of sustained economic hardship on physical,
cognitive, psychological, and social functioning. New
England Journal of Medicine, 337(26), 1889–1895.
McDonough, P., Duncan, G. J., Williams, D., & House, J.
(1997). Income dynamics and adult mortality in the United
States, 1972–1989. American Journal of Public Health, 87,
1476–1483.
Manor, O., Matthews, S., & Power, C. (2000). Dichotomous or
categorical response? Analysing self-rate health and lifetime
social class. International Journal of Epidemiology, 29, 149–
157.
Mare, R. D. (1990). Socio-economic careers and differential
mortality among older men in the United States. In J.
Vallin, S. de Souza, & A. Polloni (Eds.), Measurement and
mortality: New approaches (pp. 362–387). New York:
Oxford University Press.
C. Hertzman et al. / Social Science & Medicine 53 (2001) 1575–15851584

Marmot, M., & Wadsworth, M. (Eds). (1997). Fetal and early
childhood environment: Long term health implications.
British Medical Bulletin, 53, 1.
Matthews, S., Hertzman, C., Ostry, A., & Power, C. (1998).
Gender, work roles and psychosocial work characteristics as
determinants of health. Social Science and Medicine, 46(11),
1417–1424.
Matthews, S., Stansfeld, S., & Power, C. (1999). Social
support at age 33: the influence of gender, employment
status and social class. Social Science and Medicine, 49,
133–142.
Miller, R. G. (1986). Beyond ANOVA, Basics of applied
statistics. New York: Wiley.
Palmer, F. H. (1979). Long-term gains from early intervention:
findings from longitudinal studies. In: E. Zigler & J.
Valentine (Eds.), Project Head Start: A Legacy of the war
on poverty. New York: The Free Press.
Power, C., & Hertzman, C. (1997). Social and biological
pathways linking early life and adult disease. British Medical
Bulletin, 53(1), 210–221.
Power, C., Manor, O., & Fox, J. (1991). Health and class: The
early years. London: Chapman & Hall.
Power, C., Manor, O., & Matthews, S. (1999). Duration and
timing of exposure: Effects of socio-economic environment
on adult health. American Journal of Public Health, 89,
1059–1065.
Pulkkinen, L., & Tremblay, R. E. (1992). Patterns of boys’
social adjustment in two cultures and at different ages: a
longitudinal perspective. International Journal of Behaviour-
al Development, 15, 527–553.
Putnam, R. D. (1993).Making democracy work: Civic traditions
in modern Italy. Princeton: Princeton University Press.
Rose, R. (1995). Russia as an hour-glass society: A constitution
without citizens. East European Constitutional Review, 4,
34–42.
Rutter, M. (1967). A children’s behaviour questionnaire for
completion by teachers. Journal of Child Psychology and
Psychiatry, 8, 1–11.
Schweinhart, L. J., Barnes, H. V., & Weikart, D. P. (1993).
Significant benefits: The high/scope Perry preschool study
through age 27. Monographs of the High/Scope Educational
Research Foundation, 10, XV–XX.
Stott, D. H. (1969). The social adjustment of children. London:
University of London.
Vagero, D., & Leon, D. (1994). Effect of social class in
childhood and adulthood on adult mortality. Lancet, 343,
1224–1225.
Wannamethee, G., & Shaper, A. G. (1991). Self-assessed health
status and mortality in middle-aged British men. Interna-
tional Journal of Epidemiology, 20, 239–245.
Wannamethee, G., Whincup, P., Shaper, G., & Walker, M.
(1996). Influence of father’s social class on cardiovascular
disease in middle-aged men. Lancet, 348, 1259–1263.
Wilkinson, R. G. (1997). Health inequalities: Relative or
absolute material standards? British Medical Journal, 314,
591–595.
World Bank. (1993). World Development Report. Investing in
health. World development indicators. New York: Oxford
University Press.
C. Hertzman et al. / Social Science & Medicine 53 (2001) 1575–1585 1585


![Lifecourse Health Development: Past, Present and Future · Lifecourse Health Development: Past, Present and Future ... ness, injury, and infectious diseases [1–3]. As evidence subsequently](https://img.pdfslide.us/doc/110x75/5f0c6b3e7e708231d4354e4a/lifecourse-health-development-past-present-and-lifecourse-health-development.jpg)