Embed Size (px)
Citation preview

USING A MULTIFAMILY THERAPY GROUP TO ENGAGE PATIENTS, FAMILIES, AND
PROVIDERS IN THE TREATMENT OF EATING DISORDERS
Syracuse UniversityDepartment of Marriage and Family Therapy
Syracuse, NYOctober 5, 2007
Mary Tantillo PhD RN CS FAEDDirector, Western NY Comprehensive Care for Eating Disorders
Unity Health System, Rochester, NYClinical Associate Professor, University of Rochester

In Loving Memory ofJean Baker Miller, MD
1927-2006
“I think that the source of hope lies in believing that one has or can move toward a sense of connection.”
Jean Baker Miller Training Institute - jbmti.org

Why is the Concept of Disconnections so Important in regards to Eating Disorders
and Recovery?

Disconnections
Disconnection: A disturbance in the flow of relationship thatprevents or interrupts the experience of perceived mutuality andis characterized by: • Low self-worth• Disempowerment• Low energy, tension, feeling locked up or out• Feeling confused re: the self, other, and the relationship; intolerance of difference• Wanting less connection; isolation

Relational/Cultural Theory• A woman’s disturbances in her relationship with
food and in her relationships with others occur due to the absence of mutually empathic and empowering relationships that are required for women’s psychological growth, commitment to change, and recovery.
(Surrey, 1984; Tantillo, Nappa Bitter & Adams, 2001)

Perceived Mutuality, Disconnections, Eating Disorders, and Mental Health
Relationships characterized by a decreased sense of Perceived Mutuality and increased disconncction may create risk fordevelopment and maintenance of mental health problems such as ED’s (Genero et al., 1992; Jack & Dill, 1992; Miller & Stiver, 1997; Powell, Denton, & Mattson, 1995; Steiner-Adair, 1990, 1991; Sperberg & Stabb, 1998; Surrey, 1984; Tantillo, 2000, 2004, 2006; Walker & Rosen, 2004).
Low PM with mothers & fathers correlates with eating disordersymptoms and general psychological variables characteristic of thosewith ED’s (Sanftner & Tantillo, 2001; Sanftner, Tantillo & Seidlitz, 2004; Tantillo & Sanftner, 2003; Tantillo & Sanftner, 2006).
For mothers and fathers, PM predicts several EDI-2 scales above andbeyond the variance accounted for by FEICS perceived criticism and emotional involvement. (Sanftner, Cameron, Sippel et al., 2003).

EATING DISORDERS ARE DISEASES OF DISCONNECTION
- Disconnect patient from herself and others
- Disconnect family from other families
- Disconnect family from staff
- Disconnect treatment team from one another

Disconnection and Carer Relationships with the Patient
“I do not trust her anymore, especially with regards to what she told us she was eating…There is a lot of tension and conflict…She can bevery distant. She is afraid that I meddle with her affairs. Our relationship lacks openness. I am afraid to say anything wrong.”
“We just avoided the issues that became too awkward…because wecould already see the sickness and the pain that she was in, and wedidn’t want to cause any more.”
(Highet, Thompson, & King - focus groups with carers, 2005; Honey
& Halse – in-depth interviews with parents of adolescents, 2005)

Disconnection and Partner Relationships
“When I think of my family, if I had a picture, it would be myself and my daughter standing out the front, and the others perhaps in the background…I isolate my partner and other daughter.”
“During her sickest times, she doesn’t want to be touched…hugged. She feels so uncomfortable about herself…you start to doubt your relationship…our sex life has completely stopped…That really did affect the relationship because maybe it’s me, maybe she is falling out of love with me…why can’t I do more to make it better?”
(Highet, Thompson, & King - focus groups with carers, 2005)

Disconnection and Sibling Relationships
“With the boys, the type of thing they say, little things thatmightn’t worry us, but you’re watching everything yousay…and now the boys don’t say anything at all.”
“They have lost their friendship; they lost it last year because her sister was no fun anymore…It was like having a total stranger in the house…There is sometimes a real sadness that she hasn’t got a real sister; she’s onlygot a sometimes sister.”
(Highet, Thompson, & King - focus groups with carers, 2005)

Disconnection and Social Relationships
“Because so much of adult interactioninvolves food…I’ve said on a number of occasions to our friends that don’t know about the eating disorder, if it involves food, we can’t do it. Or I go to things by myself sometimes as well.”
(Highet, Thompson, & King - focus groups with carers, 2005)

Disconnection with Professional Team Members
“…we’d sort of put ourselves in the hands of thedoctors, then. Obviously we hadn’t been able tofix the problem, so we had to hand her over. Andso part of that was putting up with whatever treatment we got. We had to. We had to rely on them totally.”
(Honey & Halse – in-depth interviews with parents of adolescents, 2005)

Disconnection with Professional Team Members
“…we’d been [her] mum and dad for 16 years andwe were used to working problems through withher, and then suddenly, these barriers came down and wefelt that things were happening to her and beingdiscussed with her and that we were being blocked out ofit; yet we were the ones she had to come back to whenthey had had their little go with her.”
(Tierney – qualitative interviews with parents of adolescents, 2005)

It’s All About Relationships
• Parallels between relationships patient has with herself, others, and food and relationships among staff

Mutual RelationshipsMutual relationships are characterized by
“The Five Good Things:”• Self-worth• Sense of energy/zest• Increased clarity re: oneself, the other, and the
relationship• Increased sense of empowerment• Increased desire for more connection

Perceived Mutuality
• Bidirectional flow of thoughts, feelings, activity
• Sensing one influences others and allowing oneself to be influenced by others
• Involves emotional vulnerability, attunement, responsiveness to subjective experience of the other
• Takes in the wholeness of the other (similarities and differences)

Mutual relationships occur only when difference and similarity are honored in relationship, when there is space for each person in the relationship and attention to the integrity of the connection.

I YOUWE
Mutual relationships honor the integrity of the connectionbetween people and space for each person in the connection.Mutual relationships allow for difference in connection.

Disconnections
Disconnection: A disturbance in the flow of relationship thatprevents or interrupts the experience of perceived mutuality andis characterized by: • Low self-worth• Disempowerment• Low energy, tension, feeling locked up or out• Feeling confused re: the self, other, and the relationship; intolerance of difference• Wanting less connection; isolation

Serious and Repeated Disconnections
The most damaging disconnections arethose that occur without relationalrepair. They prevent family membersfrom embracing difference (e.g., different thoughts, feelings, needs) anderode mutual empathy andempowerment required for healing, growth, and recovery.

Family stress and illness can lead to an
experience of decreased perceived mutuality and put family members at risk for increased disconnection, e.g., experience of low self-worth, shame, disempowerment, inability to tolerate difference, tension, feeling “locked up or locked out” in relationship, self-doubt, confusion re: oneself, others and the relationship, and increased isolation.

Relational Reframing of Etiology of Eating Disorders
• Eating Disorders are Diseases of
Disconnection:
- Biology: Serotonergic Disturbance; Starvation; B/P
- Psychology: Disconnections; Relational mismatches
- Socio-Cultural: Toxic Societal Values that objectify
women’s (and men’s) bodies and teach us to value
ourselves from the outside in
- Spirituality: Hopelessness; Meaninglessness; Isolation

Genes and Environment
Family aggregation, twin, and linkage andassociation studies all suggest a role for genetic risk & environment:
- Heritability estimates: AN – 48%-76%; BN – 54%-85% - Family morbidity and comorbidity- What is inheritable may be eating regulatory mechanisms,
temperament and character styles, and biologic predispositions such as ovarian hormone activity
- chromosome 1 (AN-R) and 10 (BN)- polymorphisms on various candidate genes regulating body
weight, appetite, eating behavior, and serotonin- disconnection in how brain integrates information


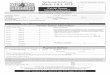
Figure 2.6 Structures of the social brain. The structures represented here are hidden beneath the surface of the brain (Cozolino, 2006 in Siegel, 2007, p. 39).

Disconnections Within the Brain 1. Consistent findings:
a) unilateral hypometabolism, predominantly in the temporal region (66-75%)
b) severe deficits in executive functioning (e.g., cognitive rigidity (poor set shifting) and in visuo-spatial memory (66%)
2. The hypometabolism & cognitive deficits persist at follow up, independent of weight/BMI, mood, EDE
3. There is a significant correlation between the hypoperfusion and the cognitive deficits
(Lask, 2006)

Key Dysfunctions in AN and Their Primary Structures
i) Distorted body image Somato-sensory cortex
ii) Increased anxiety Amygdala
iii) OCD and excessive drive Basal ganglia
iv) Enhanced sense of reward Nucleus accumbens
v) Visuo-spatial deficits Parietal cortex
vi) Executive impairments Frontal cortex
How might these be connected? (Lask, 2006)

Frontal
(executive deficits)
Amygdala
(extreme anxiety)
Parietal Lobe
(visuospatial deficits)
Somato-sensory Cortex
(DBI)
Basal Ganglia
(obsessional drive)
Insula
Nucleus Accumbens(reward)
Hippocampus
(contextual memory)

The Integrative and Regulatory Roles of the Insula
i) ANS regulationii) Appetite and eating regulation – modulates the reward value of foodiii) Self-recognitioniv) Monitors body state and body imagev) Monitors the gut (hippocampus of the gut)vi) Reception, perception & integration of tastevii) Perception and integration of disgustviii) Perception of pain ix) Integrates thoughts and feelings
(Lask, 2006)

The Insular Hypothesis
The insula fails in its role as a connection and regulator between those cortical and sub-cortical structures most relevant in AN
(Lask, 2006)

Starvation and Disconnection

Keys, et al
The Biology of Human Starvation
U Minnesota Press
1950

SYMPTOMS OF LOW ENERGY INTAKE (STARVATION)
• Hair
• Skin
• Headache
• Fainting, dizziness
• Chest pain
• Constipation
• Loss of menses
• Fatigue, weakness
• Cold intolerance
• Irritability
• Depression
• Obsessive-Compulsive traits
• Social withdrawal
• Conflict
• Food related habits
• Body image distortion
• Loss of appetite
Kreipe, 2005

SIGNS AND SYMPTOMS OF VOMITING OR LAXATIVE ABUSE
• Weight loss• Electrolyte disturbance
K CO2
• Dental enamel erosion• Low blood volume• Knuckle calluses
• Guilt• Depression• Anxiety• Confusion
Kreipe, 2005
Physical health Mental health

Disconnections – The Neurobiology of Shame
• Sudden decrease in pleasure (stress produces corticosteroids that decrease endorphins)
• Rapid inhibition of excitement (less activity in excitatory ventral tegmental limbic forebrain-midbrain circuit and more activity in inhibitory noradrenergic lateral tegmental limbic forebrain-midbrain circuit – Robins and Everett, 1982)
• Cardiac deceleration by vagal stimulation• Parasympathetic conservation-withdrawal in helpless, hopeless situations• Individuals become inhibited and avoid attention – promotes
inauthenticity• Individuals “want to be unseen” (Schore)
(Banks, 2003)

The Neurobiology of Disconnections
Trauma and early unresponsive relationships characterized bychronic and serious disconnections can lead to:
• Increased corticosteroids and neuronal cell death in affective centers of the limbic system (Kathol, Jaeckle, Lopez & Mella, 1989; Perry, 1997)
• Developmental overpruning (d/t toxic effect of overwhelming stress). Overpruning of the corticolimbic system that contains genetically encoded underproduction of synapses can lead to high risk conditions (Schore, 1997).
• Permanent alterations in opiate, dopamine, norepinephrine, and serotonin receptors (Lewis et. al. 1990; Martin et. al. 1991; Rosenblum et al. 1994; Van der Kolk, 1983).
• Physiological reexperiencing of disconnections.

Neurobiology, the Mind, and Relationships
“Human connections shape the neural connections from which the mind emerges.” (Siegel, 1999, pg. 2)
“…An individual’s abilities to organize emotions – a product, in part, of earlier attachment relationships – directly shapes the ability of the mind to integrate experience and adapt to future stressors.” (Siegel, 1999, pg. 4)
“Either form of disconnection [excessive integration or excessive differentiation] can result in the movement of the individual away from complexity, stressing the system, entering reactive states of rigidity or chaos, and moving away from the balanced capacity for self-organization (Siegel and Hartzell, 2003, pg. 218)

EATING DISORDERS: DISEASES OF DISCONNECTION
…the most terrifying and destructive feeling that a person can experience is psychological isolation…It is a feeling that one is locked out of the possibility of human connection and of being powerless to change the situation...People will do almost anything to escape this combination of condemned isolation and powerlessness.
(Miller and Stiver, 1997)

In the face of significant and especially repeated
experiences of disconnection, we believe that we yearn even more for connection to others. However, we also become so afraid of engaging with others about our experiences that we keep important parts of ourselves out of connection; that is we develop strategies for disconnection.
(Miller, J. B., & Stiver, I.P. (1994). Movement in therapy: Honoring the strategies of disconnection. Work in Progress, No. 65, Wellesley, MA: The Stone Center.)

Disconnecting from Oneself to Maintain Connections
“In situations with family, it’s so inappropriate to have different opinions,…the smallest trace of being different makes it easier to not be liked…I was so cautious of the way I sat and the words I used when I was over there tonight. I didn’t want to make a wrong move, make the wrong comment, or even sit, walk wrong. I have to close off every part of myself when I’m with them. I have to lock it away.”
(Betty, 10/21/03)

Lessons Learned through Serious and Chronic Disconnections
Difficult/different feelings/thoughts:
1. Cannot exist between us.
2. Are all mine.
3. Mean something is wrong with me.
4. My feelings/thoughts are wrong/bad.
5. So, I am wrong/bad. I am the problem.
6. My feelings/thoughts/actions lead to isolation. I am unable to change things.

Power and Disconnection:In any relationship in which a person has more power over the other, the danger of harm increases. That person can exert a greater influence on what happens in the interaction and will be less likely to seek mutual engagement. It is more difficult for the less powerful person to alter the course of an interaction. (Miller & Stiver, 1997, p. 66).

Relational Images and Meanings that Lead to Strategies for Disconnection
Relational Image: When I try to convey my
experience, no one is listening to me.
Relational Meaning: This is because I am
unlovable, unworthy, defective, to blame.
Strategies for Disconnection: (To avoid the
pain r/t the above image and meanings and to
maintain available connections) – e.g., eating
disorder behaviors/thoughts & denial of illness.

My mother called to say she had left my daughter’s
birthday cake out on the counter. She said she forgot to put it away. She knew this could be a trigger for me. I said, “That’s OK, mom. It’s too late anyway.” I had already binged on the cake…I didn’t want her to make that cake anyway. My daughter had planned for me to get her a special princess cake, but my mother said she needed to bake her one. She didn’t listen to me. She never listens to me…I guess my binging took care of all that.
(Holly, 1/05)

Toxic Sociocultural Values
• Thinness, ultra-independence, control, appearance, performance, consumerism, individualism bordering on narcissism, etc.
• Linking control and success with thinness and appearance• Objectifying women’s bodies• Socializing women and men to value themselves from the
outside in• Multiple, ambiguous, and contradictory role expectations for
women • Doing vs. Being (together) e.g., decreased family meals• Emphasis on the “I” and the “me,” not the “we”

Spirituality and Disconnection
• Meaninglessness
• Isolation – Condemned isolation
• Aloneness

EATING DISORDERS: DISEASES OF DISCONNECTION
Eating disorders are “diseases of disconnection” in which a biogenetically vulnerable individual has difficulty staying connected to and developing an authentic sense of self within relationships with others. This struggle is intensified with the effects of starvation, binging or purging and a culture that emphasizes thinness, appearance, and performance.

Genetic Neurobiological Vulnerability to Disconnections and Mutual Connections
Genotype can create neurobiologicalvulnerability to disconnections and can moderate the impact of environmental pathogens (e.g., disconnections) on a person. However, another variable, e.g., perceived mutuality or social support, can moderate that gene by environment interaction (Caspi, 2006).

Multifamily Therapy Group: Review of the Literature
Schizophrenia:
• Lacquer, LaBurt, & Morong (1964)
• Detre, Sayer, & Norton (1961)
• McFarlane (2002), Dyck et al. (2000) – manualized PMFTG treatment and conducted empirical research

Multifamily Therapy Group: Review of the Literature
Schizophrenia:• McFarlane (2002), Dyck et al. (2000) – Research
findings:
-vastly more effective than individual
treatment or meds alone
-more effective in decreasing morbidity and
relapse rates and improving vocational outcomes
in comparison to Psychoed Single Family Tx

Multifamily Therapy Group: Review of the Literature
Schizophrenia: McFarlane (2002); Dyck et al. (2000) PMFTG Research findings:
-benefits that increase with time up to 4 or more yrs
-specifically more effective than single family
approaches for 1st episode and high risk patients,
poor responders to meds, and patients in families
with high expressed emotion – emotional
overinvolvement, hostility, criticism (Vaughn, 1989;
van Furth et al, 1996).

Multifamily Therapy Group: Review of the Literature
Chronic Medical Illness:
(Gonzales and Steinglass, 2002)
Chemical Dependency:
(Kaufman and Kaufman, 1979)
Child Abuse:
(Asen, George, Piper, & Stevens, 1980)

Multifamily Therapy Group: Review of the Literature
Eating Disorders:• Asen, Stein, Stevens, McHugh, Greenwood, & Cooklin, 1981 • Cooklin, Miller, & McHugh, 1983 • Dare & Eisler, 2000 • Scholz & Asen, 2001 • Shekter-Wolfson & Woodside, 1991• Slagerman & Yager, 1989• Wooley & Lewis, 1987

Multifamily Therapy Group: Review of the Literature
Eating Disorders: PMFTG Research Findings –• Lack randomized controlled trials• Decrease in family distress and high expressed emotion
in families of ED pts (esp. emotional overinvolvement) (Uehara et al, 2001)
• Symptomatic Improvement (wt gain, decreased B/P episodes, stabilized eating, return of menses) (Dare & Eisler, 2000; Scholz & Asen, 2001)

Multifamily Therapy Group: Review of the Literature
Eating Disorders: PMFTG Research Findings –• Improved family’s perception of patient
symptoms (Uehara et al, 2001)• Reduced inpt LOS; Reduced number relapses;
Quicker recovery after relapse (Sholz & Asen, 2001)
• High patient/family satisfaction (Dare & Eisler, 2000; Scholz & Asen, 2001).

Unity Multifamily Therapy Group (U-MFTG): Integrated Model
Psychoeducational/CBT: (Garner, 1997; Fairburn, Marcus, & Wilson, 1993); Siegel, Brisman, & Weinshel, 1997; Wilson, Fairburn, & Agras, 1997)
Motivational/Stages of Change Theory: (Garner, Vitousek, & Pike, 1997; Miller & Rollnick, 2002; Prochaska, Norcross, and DiClemente, 1994)
Family Systems PMFTG: (Dare & Eisler, 1997; Lock, LeGrange, Agras, & Dare, 2001; McFarlane, 2002)

Unity Multifamily Therapy Group (U-MFTG): Integrated Model
- U-MFTG - Combined focus on psychoeducation, strategies to manage the eating disorder, improve communication, and cope but also moves beyond emphasis on scientific problem-solving to importance of promoting perceived mutuality in relationships.
Relational-Cultural Theory: (Gilligan, 1982; Miller and Stiver, 1997; Tantillo, 2000, 2004; Tantillo & Sanftner, 2003; Walker & Rosen, 2004)

U-MFTG Family Systems Assumptions
• Ed’s have a multi-factorial Biopsychosocial etiology (involving levels of disconnection)
• Main initial emphasis is on refeeding as starvation and B/P episodes can create disconnection from oneself and others and obstruct optimal use of therapy
• Disconnections and negative relational patterns can exist in the family before or after onset of ED.

U-MFTG Family Systems Assumptions
• The family did not create the ED.• The ED is presented as something outside the family,
creating disconnection, burden, and obstructing normal development for patient and family.
• Patient not in control of the ED and strategies for disconnection (ED symptoms, social isolation) are unconsciously driven, driven by starvation, etc.)

U-MFTG Family Systems Assumptions
• ED can operate in the family to promote a certain mode of organization and interaction
• The therapist must be active in helping family members identify points of tension or disconnection and address these to release the patient from the grasp of the ED.
• Emphasis on seriousness of ED and the need to work together• Most families can help and have some skills and/or are
receptive to learning new skills• Emphasis on mutual empowerment among family and staff• Role of therapist and process of therapy demystified

U-MFTG Family Systems Assumptions
• Experience in relationships is co-constructed• Emphasis on validation• Importance of meaning, adaptive nature of
symptoms/strategies for disconnection, and relational patterns• Critiques toxic societal values/norms that oppress and
objectify women and men• Transferential or symbolic aspects of therapy always kept in
mind while authenticity and real relationships emphasized with family members.

Healing within a Relational Therapy Approach to Multifamily Group
• Understanding the impact of the eating disorder and recovery on relationships and vice versa
• Experiencing mutual empathy and empowerment within the group’s diverse therapeutic social network (difference within connection).
• Perceived mutuality = recognizing we impact others and allowing ourselves to be open to the influence of others
• Understanding the connections between the patient’s relationships with food/illness, self, and others

Healing within a Relational Therapy Approach to Multifamily Group
• Honoring difference within a strong connection with one another
• Practice identifying various disconnections that keep the eating disorder in place
• Transform strategies for disconnection into strategies for connection that don’t focus mainly on food/illness
• Patients, families, and therapist grow through interaction

Healing within a Relational Therapy Approach to Multifamily Group
RT promotes development of mutual
empathy and empowerment through:
• Focus on patient & therapist authenticity
• Use of real relationship
• Attention to transferential relationship
• Use of judicious self-disclosure

Relational/Cultural Theory emphasizes that mutuality involves not only the therapist’s ability to appreciate her/his impact on the patient and family, but also an openness to being moved by what the patient and family say and do, and a willingness to convey to them that s/he has been moved.
(Miller & Stiver, 1997; Tantillo, Nappa Bitter Adams, 2001).

Therapist Self-Disclosure within a Relational Therapy Approach
Therapist self-disclosure promotes a sense of perceived mutuality because it helps the patient and family recognize that the therapist has been moved in response to their experiences or behaviors. This process leads to increased self-empathy for each family member and mutual empathy among family members. The patient and family realize their experiences do matter and can be part of relationship (Miller, 1999; Tantillo, 2004).

Purposes of Therapist Self-Disclosure within a Relational Therapy Approach
• Promote perceived mutuality (mutual empathy and mutual empowerment)
• Demystify the therapist’s role• Create shared value and expertise• Promote egalitarianism• Demystify process of therapy• Normalize and validate symptoms/struggles • Promote universality

Purposes of Therapist Self-Disclosure within a Relational Therapy Approach
• Identify relational dilemmas • Identify negative relational images, meanings, and
patterns• Identify strategies for disconnection• Move relationship from disconnection to new/better
connection• Identify relational paradox

Purposes of Therapist Self-Disclosure within a Relational Therapy Approach
• Convey flexibility and openness to difference• Apologize/Admit errors• Convey therapist limitations• Create connection by allowing patients and
families in your head (how you think/feel)

The therapist’s ability to remain aware of her/his own strategies for disconnection is important for movement with the patients and families along the entire spiral of change, but is especially critical in helping them jointly contemplate and eventually commit to change.

Each dynamic in group is viewed as a means of
maintaining connection or as a strategy for disconnection (e.g., food restriction, binging, purging, denial of illness, minimization, avoidance, social isolation). These strategies of disconnection are responses to a central relational paradox , i.e., an intense longing for mutual relationships and a fear of allowing oneself to participate in these relationships because of severe anxiety, past hurts, and violations.
(Fedele, 1994; Tantillo, Nappa Bitter Adams, 2001).

Aims of U-MFTG
1. Improve quality of family life through decreasing stigma, stress, disconnection, and the burden incurred by the ED.
2. Improve ED symptoms and a sense of perceived mutuality.
3. Promote relapse prevention.

U-MFTG GOALS
1. Build mutually empathic and empowering relationships among patients and families.
2. Increase understanding re: impact of disconnections on the ED and recovery.
3. Increase understanding re: how the ED promotes disconnection in relationships and obstructs recovery.
4. Increase understanding re: ED and stages and processes of change, to help families interact with patients in ways that promote motivation for treatment and recovery.

U-MFTG GOALS
5. Identify and challenge dysfunctional thoughts (e.g., all/nothing thoughts) that obstruct recovery.
6. Develop and practice new coping strategies and relational skills that promote recovery.
7. Promote a sense of hopefulness and positive, healing energy that enables patients and families to remain connected and engaged in their work.
8. Decrease isolation and expand families’ and patients’ social networks.

U-MFTG Format • Outpt.: Closed-ended 8 week group cycle with up to 5 families• PHP: Open-ended 7/8 week group cycle
with up to 9-12 families• 1 ½ hours long• Program director is group leader along
with trainee • Patient plus significant others• Ages 12 and up• Adults and adolescents are seen in
individual treatment when attending outpt U-MFTG

U-MFTG Schedule: Moving from Disconnection to New and Better
Connection
1. Introduction: The recovery process and the spiral of change
2. Biopsychosocial risk factors for ED’s
3. Strategies to promote mutual connection
4. The Family Context: Rules and Relationships

U-MFTG Schedule: Moving from Disconnection to New and Better
Connection
5. Identifying points of tension and disconnection related to the ED and recovery
6. Nourishing and empowering the “We”
7. Waging good conflict in connection
8. Wrap-up, good-byes and next steps

Multifamily Therapy Group Sessions Session 1:
• Group introductions and orientation• Promote universality and mutual exchange • Spiral, stages, and processes of change• Strategies that support patients to stay engaged in treatment • Distinguish illness from patient• Validate burden of illness for patient and family• Emphasize how neither patient nor family caused
or can alone cure and control the ED. • Introduce idea that ED thrives on disconnection
and isolation and importance of tolerance of difference.

Multifamily Therapy Group Sessions Session 2:
• Biopsychosocial risk factors r/t ED’s • Introduce relational risk factors• Perceived mutuality and negative impact of serious/persistent disconnections• Negative relational images, meanings & patterns• Disconnections can be “handed down”• Importance of relational repair• Judicious therapist self-disclosure re:
disconnections• Validate and normalize family/patient dilemmas• Foster increased authenticity and mutual
connection

Multifamily Therapy Group Sessions Session 3:
• Develop strategies for connection that don’t involve food and the ED• Discuss self, other, and relationship as all needing attention in mutual connections• Relationships greater than the sum of its
parts – can provide healing energy for recovery
• Strategies for connection foster ability to see and experience the wholeness of others beyond the ED

Multifamily Therapy Group Sessions Session 4:
• Identify implicit and explicit rules r/t the ED and relationships
• Discuss how rules develop, e.g., previous generations, personalities, and culture.
• Discuss how rules need to change over time to promote growth of individuals and relationships
• Discuss challenges that occur when rules and the nature of connections don’t change
• Practice being open to different perceptions of the rules
• Rate rules according to criteria such as ability to embrace/avoid difference; focus on appearance or performance

UNITY MULTIFAMILY THERAPY GROUPSESSION IV
CRITERIA TO RATE FAMILY RULES
• Is the rule consistently or inconsistently applied? • Is the rule predictable or unpredictable?• Is the rule rigid or flexible?• Does it apply to some members and not others?• Does the rule promote or inhibit conflict negotiation?• Does the rule help people embrace or avoid difference?• Does the rule focus mainly on physical appearance or
performance?

Multifamily Therapy Group Sessions Session 5:
• Identify points of tension and disconnection r/t ED and recovery/relationships and problem solve• ED’s are diseases of disconnection – can evolve from them and perpetuate them to obstruct
recovery• Impact of serious/persistent disconnections on recovery – note all/nothing thinking• Strategies for working through disconnection• Put connection at the heart of the relationship• Stay connected to ourselves (genuine thoughts, feelings, needs) and in relationships with others,
higher power, nature, etc.

Multifamily Therapy Group Sessions
Session 6-8: • Strategies for moving out of disconnection
to new/better connection• Empowering the “we” to move out of
disconnection• Identify points of tension/disconnection and problem solve • Termination, evaluations, accomplishments,
next steps, follow-up

It’s All About Relationships – Team Building Considerations
• Learn the language and values of the patient and family
• Build a new culture of shared meanings and common language with the patient, family, and staff

Demographics of U-MFTG families seen 2001-2004 in Eating Disorders
Partial Hospitalization (PHP) and Outpatient (Outpt) Programs
Program n #Grp #Family Diagnosis Age Ethnicity Gender Cycles Members________________________________________________________________________ PHP 141 16 mothers (54) AN (48) <18 (36) W (134 ) F (139)
fathers (43) BN (61) 18> (105) AA (1) M (2) siblings (30) EDNOS (32) H (4)
grndpts (5) ASA (1) partners (20) friends (30)
________________________________________________________________________Outpt 9 3 mothers (5) AN (3) <18 (1) W (9) F (9) fathers (4) BN (2) 18> (8) AA (0) M (0)
siblings (8) EDNOS (4) H (0) partners (5) ASA (0)
grndpts (1) friends (1)________________________________________________________________________
Note: grp = group; grndprts = grandparents; AN = anorexia nervosa; BN = bulimia nervosa;EDNOS = eating disorder not otherwise specified; W = white; AA = African American; H = Hispanic; ASA = Asian American; F = female; M = male

Implications for Research and Practice
Need more randomized controlled trials of
PMFTG to identify:• Most effective group format/frequency• Clarify impact of PMFTG on family
functioning, pt symptom improvement, family perception of pt symptoms, duration and frequency of relapse, and tx drop out rates.
• Compare to single family and other approaches esp. for 1st episode, high risk patients, poor responders to meds, and patients in families with high expressed emotion

Implications for Research and Practice
PMFTG approaches should:• target predisposing, precipitating, and
perpetuating risk factors for ED’s (e.g.,
negative self-evaluation, high parental
achievement expectations, low parental
contact, and low paternal care)
*These are potential sources of disconnection

Implications for Research and Practice
PMFTG approaches should:• Promote favorable prognostic factors, e.g.,
friendships, increased self-esteem, more moderate level of expressed emotion in families, esp. parental criticism.
• Promote family/patient strengths and resilience
*These involve a family’s ability to embrace and
work through difference.