-
1
The USI Pakistan Program- A Success Story
Iodine deficiency is the worlds single greatest cause of
preventable mental retardation. Iodine
is part and requirement of a hormone, thyroxin,
which is responsible for optimal mental and
physical development, physical growth and
reproduction, maintenance of a person's
metabolic rate and helps the white cells to
inactivate bacteria. Goiter-the enlargement of
the thyroid gland (located at the base of the
neck) is also caused by a lack of iodine in a
person's diet. The most severe impacts of iodine
deficiency occur during fetal development and
in the first few years of life.
The global strategy of choice for preventing
iodine deficiency disorders (IDD) is universal salt
iodization (USI). Because salt is commonly
consumed, even in impoverished areas, it is an
ideal vehicle to carry iodine. Adding iodine to
salt provides protection from brain damage due
to iodine deficiency for whole populations,
helping people and countries reach their full
potential. While complete iodization of a
nations salt supply may not always be possible,
generally USI is considered successful if greater
than 90% of households are using iodized salt.i
Its been more than half a century when Iodine
Deficiency Disorder (IDD) was recognized as a
public health problem in Pakistan, a country
with more than half of the population
estimated to be at risk for Iodine Deficiency
Disorders as reflected in various surveys.
In 1989 the Government of Pakistan initiated a
National Iodine Deficiency Disorders (IDD)
Control Program to address the problem of IDD,
however, its impact remained limited due to the
limited knowledge & capacity of the salt
processors required for iodization, irregular and
centralized supply of Potassium Iodate (KIO3),
absence of a monitoring and supervisory
mechanism, lack of a quality control system,
weak regulatory framework along with various
rumours from consumer side and even after
many years of running of program the
utilization of iodized salt at the household level
could only reach 17 percent by the end of 2001
(UNICEF 2001-02).
In 2005 Micronutrient Initiative (MI), a leading
Canadian Non Governmental Organization
working exclusively to eliminate vitamin and
mineral deficiencies in the worlds most
vulnerable populations came forward and
carried out the first ever Pakistan Salt Sector
Survey to document the weakness and bottle
necks of the salt industry of Pakistan.
According to the survey out of the total of 0.935
million tons of edible salt processed by 1172
salt units in Pakistan at that time, only 14% was
iodized (MI-2005). Among these salt units 68
percent were small scale and more than 80
percent of them had no formal training on salt
iodization. In addition to this most of them
didnt even have the necessary equipment for
salt iodization.
In the light of the findings of this survey and
lessons learnt from the previous National IDD
Control Program, Nutrition Wing of Ministry of
Health revitalized the USI program in Pakistan
with the technical and financial assistance of MI
(getting its funding from Canadian International
Development Agency (CIDA) in 2006.
Initially the Universal Salt Iodization (USI)
program was piloted in 20 districts selected
from all over Pakistan with the salt processors
provided with iodization equipment along with
training on iodization technique and internal
quality control. Government Health officials
-
2
were also provided trainings on supervision,
monitoring of USI Program, external quality
control and in compilation and analysis of
iodization data. As the strategies adopted in the
pilot districts brought about a positive change in
salt iodization, therefore WFP joined hands in
the efforts towards control of IDD and the
Program was scaled up by including 29 high risk
northern districts of Khyber Pakhtoonkhwa (KP),
Azad Jammu & Kashmir (AJ&K), Gilgit Baltistan
(GB) and Federally Administered tribal Areas
(FATA). Community awareness and capacity
building of public health care providers, school
teachers and NGOs were also important
components of the program. During 2007,
program was further expanded to 16 large salt
producing districts of Punjab, contributing
about one third of the total edible salt
production in the country. By 2008, the salt
iodization at the production level increased
remarkably from less than 14% to 65% in these
districts as reported by the monitoring system
of Department of Health. Strong coordination
among partners, capacity building of the
government and salt industry, and provision of
KIO3, drip feeders, and other equipment
needed for salt iodization to the salt sector and
most importantly, a phased wise expansion of
the program contributed to the success of the
USI in Pakistan . The encouraging USI results
and requests from Department of Health on the
other hand led the total number of districts
being covered by the Program to reach 102 by
2010.
By this time the program had achieved 99
percent of salt iodization in the country as per
findings of the assessment of salt iodization at
production and focus was towards
improvement in the level of adequate iodization
of salt. For this purpose Quality Control
Laboratories (QCLs) have been established in
the salt producing districts. District focal
persons and MI field officers collect salt samples
from the salt processors and take it to QCLs
where they are analyzed quantitatively for their
iodine content. If the iodine content is found to
be below 30 ppm, the salt processor is notified
about it for taking corrective measures. At the
same time through provision of technical
support the Program has built the capacity of
the government health managers in external
monitoring and quality control, streamlining the
regulatory and enforcement mechanism and
internal quality control to ensure adequate
production of iodized salt. With the coordinated
efforts of MI, WFP and the Departments of
Health, district level legislation and notifications
on compulsory USI and pure food rules
amendments were enacted in 56 districts of
Pakistan during 2009-11. In the absence of
national or provincial legislation these were
used for enforcement of salt iodization at the
district level which yielded positive results.
-
3
Furthermore, throughout these years emphasis
has been placed on involving the salt producers
as equally important partners in the USI
Program. They have been supported to form
associations at the Provincial & District level
that have facilitated USI activities and
coordination amongst Program partners. The
USI Program is spread out in all provinces,
Punjab, Sindh, Balochistan, KP, AJ&K; GB &
FATA with the objective to improve the
availability and accessibility of adequately
iodized salt to the vulnerable sections of the
population.
According to the National Nutrition Survey
2011, around three-fourths (69 percent) of the
households in Pakistan now consume iodized
salt compared to 17 percent in 2001, which is
very encouraging for the USI Program. The
increased consumption of iodized salt has led to
a decrease in the percentage of children 6-12
years of age with iodine deficiency by 28
percent (i.e. NNS 2011-36 percent: NNS 2001-
64 percent). Prevalence of goiter amongst
women of childbearing age has also decreased
to one third as per NNS of 2011 and now stands
at only 3 percent.
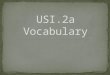
Comparison of urinary iodine excretion in mothers and school
aged children between NNS 2001 & 2011
Till 2008 Potassium iodate (KIO3) premix with
refined salt (NaCl) was being given in small
packing of 500 grams to minimise misuse and to
ensure its availability at district level for small
scale salt processors. However, since 2009, KIO3
was provided in pure form on subsidized rates
by the government with support of MI and
WFP. Keeping in view the long term
sustainability of the program, MoH after
consultation with USI partners, withdrew
subsidy on KIO3 with effect from July 2012 in a
phased manner leading to a complete
withdrawal in March 2013. A revolving fund was
established for procurement and supplies of
KIO3 to salt processors on no profit no loss
basis. The first procurement with the revolving
fund has been carried out and from April 2013,
KIO3 is being given to the salt processors on the
actual cost. Legislation on compulsory salt
iodization is already in place in Gilgit Baltistan
and most recently in Sindh. It is now important
to ensure that the legislations are enforced in
remaining provinces/regions thus ensuring that
the salt processors produce, promote and sell
only adequately iodized salt.
USI Programs phased expansion over the years,
a strong commitment and ownership by the
government, an excellent coordination and
partnership amongst USI partners and a
stringent monitoring in the field have all
positively contributed to the success of the this
program.
The challenge, however, does not end here. To
further build and sustain this achievement there
is need for a strong political commitment and
salt industry motivation. During the coming
years, the USI Program focus will be to provide
technical and operational support to salt
processor units for adequate iodization of salt
to the government in monitoring and quality
-
4
control. The USI program will be expanded to 8
additional (remaining) salt producing districts of
Sindh that are not covered by the Program so
far, thus bringing the total number of USI
districts to 110. Efforts would be made towards
the development of an open market system of
procurement and availability of the KIO3.
Advocacy will be carried out with the salt
processor associations to motivate them to
arrange for the replacement of equipment
themselves on self help basis. Priority will be
given to the component of quality control in
program implementation to ensure adequacy of
edible salt iodized and necessary steps taken in
this respect. In those provinces that do not
have compulsory salt iodization legislation,
advocacy will continue with government
departments and stake holders for
promulgation of provincial legislation on
mandatory salt iodization.
i (Assessment of Iodine deficiency disorders and monitoring
their elimination. 2007, WHO.)