Embed Size (px)
Citation preview
rslgA
Hm
u
0d
Usefulness of Platelet Response to Clopidogrel by Point-of-CareTesting to Predict Bleeding Outcomes in Patients Undergoing
Percutaneous Coronary Intervention (from the AntiplateletTherapy for Reduction of Myocardial Damage During Angioplasty-
Bleeding Study)
Giuseppe Patti, MDa, Vincenzo Pasceri, MDb, Vincenzo Vizzi, MDa, Elisabetta Ricottini, MDa, andGermano Di Sciascio, MDa,*
Platelet reactivity predicts ischemic outcomes in patients who undergo percutaneouscoronary intervention (PCI), but the correlation of heightened platelet response withbleeding has not been characterized. The aim of this study was to evaluate whether lowplatelet reactivity by point-of-care measurement after clopidogrel administration correlateswith bleeding complications of PCI. A total of 310 patients receiving clopidogrel before PCIwere prospectively enrolled. Platelet reactivity was measured with the VerifyNow P2Y12assay. The primary end point was the 30-day incidence of major bleeding or entry-sitecomplications according to quartile distribution of P2Y12 reaction units (PRU). Theprimary end point occurred more frequently in patients with preprocedural PRU levels inthe lowest quartile compared to those in the highest quartile (10.1% vs 1.3%, p � 0.043),due mainly to entry-site hemorrhages. Absolute PRU levels were lower in patients withmajor bleeding (171 � 49 vs 227 � 68 in patients without, p � 0.002). On multivariateanalysis, pre-PCI PRU levels in the first quartile were associated with a 4.5-fold increasedrisk for major bleeding (odds ratio 4.5, 95% confidence interval 1.9 to 25.9, p � 0.01). Byreceiver-operating characteristic curve analysis, the optimal cutoff for the primary endpoint was a pre-PCI PRU value <189 (area under the curve 0.76, 95% confidence interval0.66 to 0.87, p � 0.001). In conclusion, this study suggests that an enhanced response toclopidogrel may be associated with higher risk for early major bleeding or entry-sitecomplications in patients who undergo PCI. Point-of-care monitoring of platelet reactivityafter clopidogrel administration may help identify patients in whom individualized strat-egies are indicated to limit bleeding complications after coronary intervention. © 2011
Elsevier Inc. All rights reserved. (Am J Cardiol 2011;107:995–1000)sot
M
sCDpdiamc
Significant interindividual variability in clopidogrel re-sponse has been demonstrated,1,2 and various investigationscorrelated low clopidogrel responsiveness with enhancedrisk for early and late adverse cardiac events in the settingof percutaneous coronary intervention (PCI).3–5 Conversely,there is a gap of knowledge on the possible relation betweenhigher clopidogrel responsiveness and increased bleeding risk.Because periprocedural bleeding complications strongly im-pair prognosis after PCI,6 assays measuring residual plateleteactivity after clopidogrel administration might help rapidlytratify patients according to their bleeding risk. The Antiplate-et Therapy for Reduction of Myocardial Damage During An-ioplasty (ARMYDA) study group3,7–11 has designed theRMYDA–Bleeding Study (ARMYDA-BLEEDS) to pro-
aDepartment of Cardiovascular Sciences, Campus Bio-Medico Univer-sity of Rome; and bInterventional Cardiology Unit, San Filippo Neri
ospital, Rome, Italy. Manuscript received September 19, 2010; revisedanuscript received and accepted November 16, 2010.
*Corresponding author: Tel: 39-06-225411612; fax: 39-06-225411638.E-mail address: [email protected] (G. Di Sciascio); g.patti@
nicampus.it (G. Patti).
002-9149/11/$ – see front matter © 2011 Elsevier Inc. All rights reserved.oi:10.1016/j.amjcard.2010.11.025
pectively evaluate levels of platelet reactivity by a point-f-care assay that may correlate with bleeding complica-ions in patients who undergo coronary stent implantation.
ethods
ARMYDA-BLEEDS is a prospective study of 310 con-ecutive clopidogrel-treated patients who underwent PCI atampus Bio-Medico University of Rome from April 1 toecember 31, 2009. This population represents 69% ofatients (310 of 449) who underwent PCI at our institutionuring the enrollment period. Inclusion criteria were (1)ndication for percutaneous coronary revascularization forngina with inducible myocardial ischemia or non–ST-seg-ent elevation acute coronary syndromes (ACS) and (2)
lopidogrel therapy initiated before PCI, as a 600-mg load7
given �6 hours before intervention (n � 104) or long-termclopidogrel therapy 75 mg/day for �5 days (n � 206).Exclusion criteria were indication for long-term therapywith vitamin K antagonists, intervention for ST-segmentelevation acute myocardial infarction �24 hours (represent-ing most patients excluded from the study from the whole
cohort of PCI patients during the enrollment period), plate-www.ajconline.org
pbpjwfrftaiTTtbwalcmdwg
lacbct
996 The American Journal of Cardiology (www.ajconline.org)
let count �70 � 109/L, coronary bypass surgery in therevious 3 months, and severe chronic renal failure withaseline serum creatinine �2 mg/dl. All interventions wereerformed using the femoral approach, with weight-ad-usted intravenous unfractionated heparin (70 IU/kg bodyeight). During PCI, bivalirudin was used instead of un-
ractionated heparin in patients considered at high bleedingisk (age �75 years, history of previous bleeding, renalailure, low body weight); periprocedural use of glycopro-ein IIb/IIIa inhibitors was left to the operator’s discretionccording to the presence of thrombus at the site of thendex stenosis, occurrence of no-reflow, or vessel closure.he sheath size was 6Fr (7Fr in case of bifurcating lesions).he arterial sheath was removed when the activated clotting
ime was �180 seconds. The femoral arteries were closedy manual compression in all cases; manual compressionas performed until the achievement of full hemostasis plus
n additional 5 minutes. By protocol, patients receivingong-term clopidogrel therapy were not reloaded in theatheterization laboratory. Clopidogrel was continued (75g/day) for 1 month after PCI, except in patients receiving
rug-eluting stents or treated for ACS, in whom the drugas discontinued 1 year after intervention. Aspirin was
Table 1Main clinical and procedural features
Characteristic Firs(n
Age (years) 6Women 16Diabetes mellitus 30Hypercholesterolemia (�200 mg/dl) 55Body mass index (kg/m2) 2Previous myocardial infarction 20Previous transient ischemic attack/stroke 2Previous PCI 34Previous major bleeding 2Clinical presentationUnstable angina/non–ST-segment elevation myocardial infarction 19Stable angina 58Left ventricular ejection fraction (%) 5Serum creatinine (mg/dl) 1.1Hemoglobin (g/L) 13.Vessel treated
Left anterior descending coronary artery 41Left circumflex coronary artery 18Right coronary artery 28Left main coronary artery 1
Lesion type B2/C 48Multivessel intervention 14Use of drug-eluting stents 19Statin therapy 64Sheath size
6Fr 727Fr 5
Antithrombotic therapyUnfractionated heparin 64Bivalirudin 13Glycoprotein IIb/IIIa inhibitors 9
Data are expressed as mean � SD or as number (percentage).
iven to all patients and continued indefinitely.
Platelet reactivity was evaluated in the catheterizationaboratory immediately before PCI and at 8 and 24 hoursfter intervention using the VerifyNow P2Y12 assay (Ac-umetrics, Inc., San Diego, California), a rapid cartridge-ased assay specifically measuring the direct effects oflopidogrel on the platelet P2Y12 receptor. Technical de-ails have been described elsewhere.12 Results are expressed
as P2Y12 reaction units (PRU), which inversely correlatewith the degree of P2Y12 receptor inhibition by clopi-dogrel. Twenty-five randomly selected patients were ana-lyzed to assess intra-assay variability, which was 2.0 �1.1% (coefficient of variation 6%). Blood samples were alsodrawn before and at 8 and 24 hours in all patients tomeasure hemoglobin levels; further hemoglobin determina-tions were performed if clinically indicated. Patients wereclinically evaluated after PCI for the detection of bleedingevents and entry-site complications (hematoma, pseudoan-eurysm, or arteriovenous fistula). One-month clinical fol-low-up was then obtained by office visit in all patients. Eachpatient gave informed consent to the study.
The primary end point of ARMYDA-BLEEDS was the30-day incidence of major bleeding or significant entry-sitecomplications in relation to periprocedural quartile distri-
le Second Quartile Third Quartile Fourth Quartile p Value(n � 77) (n � 77) (n � 79)
65 � 10 68 � 11 68 � 9 0.0712 (16%) 19 (25%) 20 (25%) 0.5926 (34%) 25 (32%) 34 (43%) 0.6851 (66%) 52 (68%) 62 (79%) 0.4428 � 6 27 � 5 28 � 4 0.4926 (34%) 24 (31%) 21 (27%) 0.92
2 (3%) 4 (5%) 2 (3%) 133 (43%) 25 (32%) 31 (39%) 0.611 (1%) — 2 (3%) 0.73
26 (34%) 29 (38%) 26 (33%) 0.5051 (66%) 48 (62%) 53 (67%) 0.5055 � 7 54 � 11 57 � 8 0.12
3 1.10 � 0.21 1.12 � 0.25 1.08 � 0.3 0.778 13.5 � 1.73 13.0 � 1.72 13.1 � 1.33 0.27
47 (51%) 44 (50%) 45 (45%) 125 (27%) 21 (24%) 25 (25%) 120 (22%) 23 (26%) 29 (29%) 0.64
— — 1 (1%) 0.8056 (73%) 50 (65%) 55 (70%) 0.7015 (19%) 14 (18%) 15 (19%) 123 (30%) 29 (38%) 24 (30%) 0.5172 (94%) 70 (91%) 74 (94%) 0.12
72 (94) 71 (92) 73 (92) 15 (6) 6 (8) 6 (8) 1
68 (88%) 66 (86%) 74 (94%) 0.299 (12%) 11 (14%) 5 (6%) 0.298 (10%) 11 (14%) 6 (8%) 0.83
t Quarti� 77)
5 � 9(21%)(39%)(71%)
8 � 4(26%)(3%)(44%)(3%)
(25%)(75%)
4 � 101 � 0.22 � 1.7
(47%)(20%)(32%)(1%)(62%)(18%)(25%)(83%)
(94)(6)
(83%)(17%)(12%)
bution of platelet reactivity measured by PRU assay. Major
tvt2t22
lmdyimti
997Coronary Artery Disease/High Clopidogrel Response Predicts PCI Bleeding
bleeding was defined according to the Thrombolysis InMyocardial Infarction criteria.13 Significant entry-site com-plications were defined as hematoma �10 cm in diameter,pseudoaneurysm, or arteriovenous fistula. Secondary endpoints were (1) evaluation of absolute PRU values in pa-tients with or without major bleeding and (2) correlation ofPRU values with minor bleeding13 or post-PCI hematoma�10 cm in diameter.
Continuous variables were compared using Student’s ttests for normally distributed values; otherwise, Mann-Whitney U tests were used. Proportions were comparedusing Fisher’s exact test when the expected frequency was�5; otherwise, chi-square tests were applied. Odds ratiosand 95% confidence intervals investigating the independentpredictive role of PRU quartiles on the occurrence of theprimary end point were assessed by logistic regression. Thefollowing parameters were first evaluated in a univariatemodel: PRU quartile, age, gender, body mass index, diabe-tes mellitus, clinical presentation (stable angina vs ACS),chronic renal failure, hemoglobin levels, previous transientischemic attack or stroke, previous major bleeding, use ofbivalirudin versus unfractionated heparin, and use of glyco-protein IIb/IIIa inhibitors. Variables with p values �0.15were then entered into the final model of multivariate lo-gistic regression analysis. The ability of the assay to dis-criminate between patients with and without major bleedingat 30 days was evaluated using receiver-operating charac-teristic curve analysis. The optimal cut-off value was cal-culated by determining the PRU value providing the great-est sum of sensitivity and specificity. Results are expressedas mean � SD. Two-tailed p values �0.05 were consideredsignificant. Analysis was performed using SPSS version12.0 (SPSS, Inc., Chicago, Illinois).
Results
Clinical and procedural characteristics according to pre-
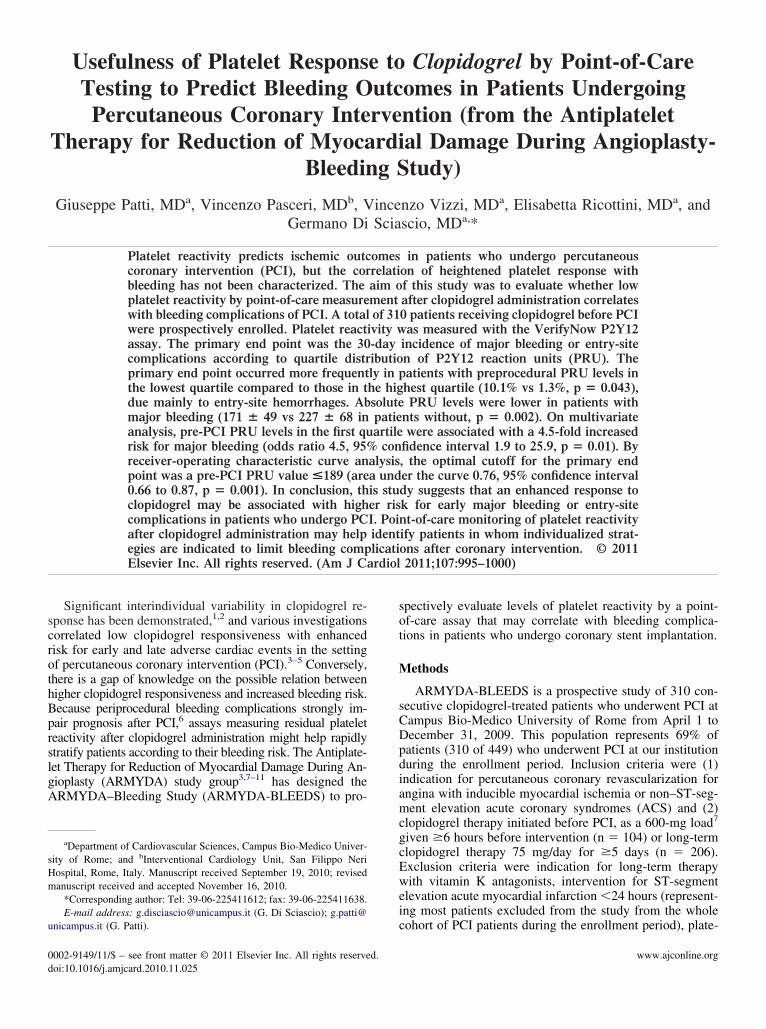
Figure 1. Incidence of the primary end point (major bleeding or entry-sitecomplications at 30 days) according to quartile distribution of preinterventionPRU values.
intervention PRU quartiles are listed in Table 1. Procedural
success was achieved in 98% of patients, without need forrepeat PCI or coronary artery bypass grafting at 30 days.
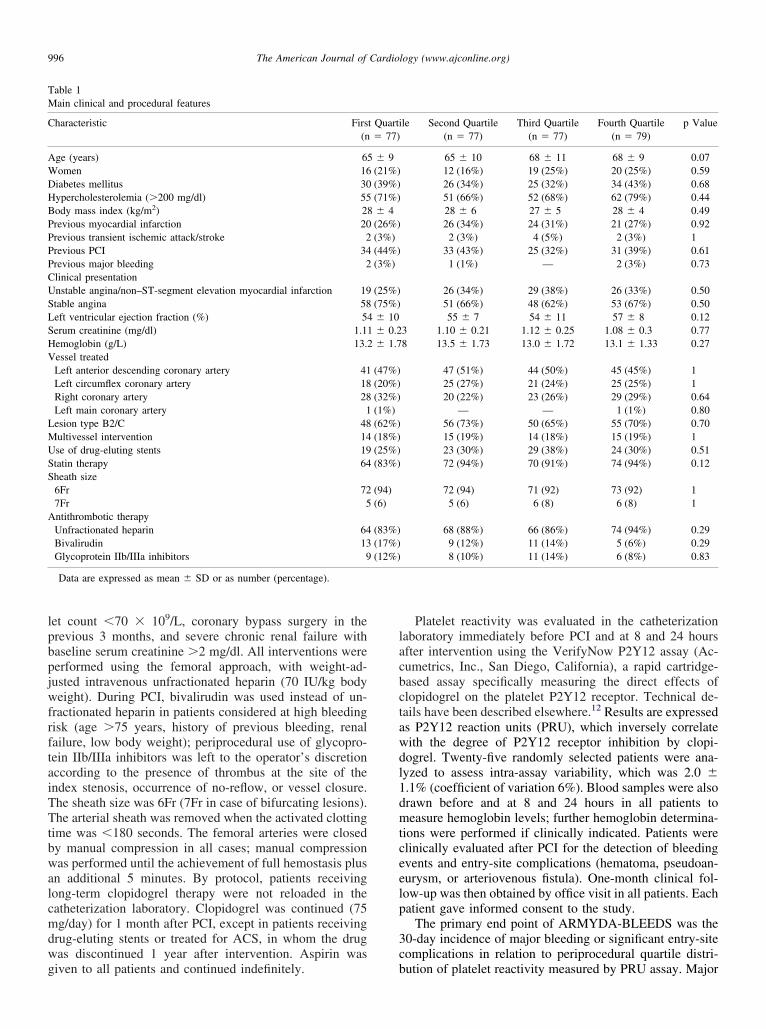
The overall incidence of major bleeding or entry-sitecomplications was 4.8% (15 of 310 patients): 3 patients hadgastrointestinal bleeding, 2 had bladder or urethral bleeding,and the remaining had entry-site hematomas �10 cm. Pa-tients in the lowest PRU quartile before PCI had a higherincidence of major bleeding at 1 month (10.1%) comparedto those in the highest quartile (1.3%, p � 0.043) and thehird quartile (1.4%, p � 0.05) (Figure 1). Absolute PRUalues before PCI were lower in patients with compared tohose without major bleeding at 30 days (171 � 49 vs27 � 68, p � 0.002). Periprocedural PRU values in pa-ients with or without major bleeding are reported in Figure; PRU increased at 8 hours after PCI and decreased over4 hours.
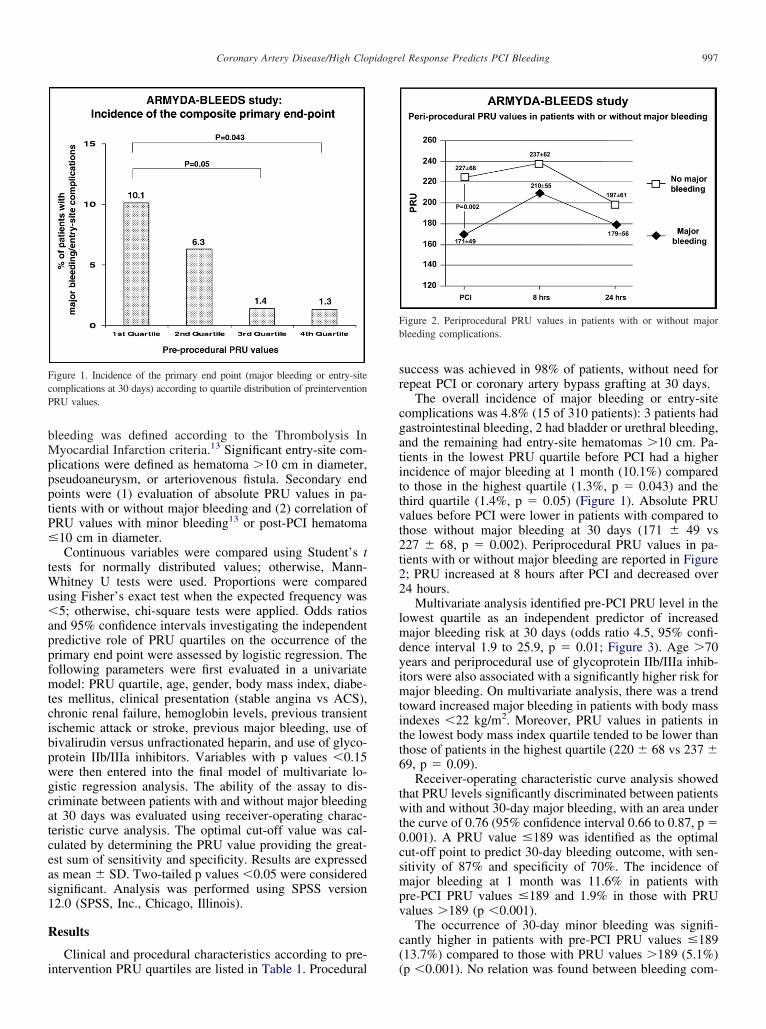
Multivariate analysis identified pre-PCI PRU level in theowest quartile as an independent predictor of increasedajor bleeding risk at 30 days (odds ratio 4.5, 95% confi-
ence interval 1.9 to 25.9, p � 0.01; Figure 3). Age �70ears and periprocedural use of glycoprotein IIb/IIIa inhib-tors were also associated with a significantly higher risk forajor bleeding. On multivariate analysis, there was a trend
oward increased major bleeding in patients with body massndexes �22 kg/m2. Moreover, PRU values in patients in
the lowest body mass index quartile tended to be lower thanthose of patients in the highest quartile (220 � 68 vs 237 �69, p � 0.09).
Receiver-operating characteristic curve analysis showedthat PRU levels significantly discriminated between patientswith and without 30-day major bleeding, with an area underthe curve of 0.76 (95% confidence interval 0.66 to 0.87, p �0.001). A PRU value �189 was identified as the optimalcut-off point to predict 30-day bleeding outcome, with sen-sitivity of 87% and specificity of 70%. The incidence ofmajor bleeding at 1 month was 11.6% in patients withpre-PCI PRU values �189 and 1.9% in those with PRUvalues �189 (p �0.001).
The occurrence of 30-day minor bleeding was signifi-cantly higher in patients with pre-PCI PRU values �189(13.7%) compared to those with PRU values �189 (5.1%)
Figure 2. Periprocedural PRU values in patients with or without majorbleeding complications.
(p �0.001). No relation was found between bleeding com-

gupbpt
a
ptnPldletattwa
e interv
998 The American Journal of Cardiology (www.ajconline.org)
plications and PRU levels measured at 8 and 24 hours afterintervention (p �0.39), probably because entry-site bleed-ing complications occurred earlier, while in the hours afterPCI, there was an increase of platelet reactivity due to theprocedure in the groups of patients with and without majorbleeding.
Discussion
This prospective study indicates that low residual plateletreactivity after clopidogrel, as measured by a point-of-careassay at the time of intervention, is associated with a sig-nificantly higher incidence of 30-day major bleeding orentry-site complications after PCI.
Residual platelet reactivity after clopidogrel administra-tion in an index population follows a Gaussian distribu-tion,14 reflecting the interindividual variability of drug re-sponse15,16; of note, CYP2C19*17 carrier status17 and somedrugs18 may promote the cytochrome activity and acceleratethe rate of clopidogrel activation in the liver, thus causing anenhanced degree of platelet inhibition in response to thedrug and a possible increase in bleeding risk. Various stud-ies have focused on PCI patients with low response toclopidogrel, demonstrating a significantly higher incidenceof periprocedural myocardial infarction3 and adverse car-diac events during follow-up.19,20 Accordingly, more ag-ressive antiplatelet strategies in patients with ACS, partic-larly those who undergo PCI, increase the degree oflatelet inhibition and significantly reduce ischemic events,ut at the price of higher bleeding complications (aspirinlus clopidogrel vs aspirin alone, prasugrel vs clopidogrel,icagrelor vs clopidogrel).21–23
The prognostic role of bleeding is now largely recog-nized in interventional cardiology; in particular, a fourfoldincrease in the risk for death at 30 days was observed inpatients with ACS with major bleeding24,25 and threefoldhigher mortality at 1 year in patients with early bleedingcomplications after PCI.6 Although ARMYDA–Platelet Re-ctivity Predicts Outcome (ARMYDA-PRO)3 and other
Figure 3. Results of multivariate analysis showing that patients with preintermajor bleeding or entry-site complications (odds ratio 4.5, 95% confidenc
studies19,20,26 have established an efficacy threshold of c
latelet inhibition (i.e., 240 PRU by the VerifyNow assay),he optimal safety threshold for bleeding complications hasot been identified. In our study, the relation between lowRU values and bleeding complications in the multiple
ogistic regression model was independent of various pre-ictors of bleeding (i.e., older age, presentation with ACS,ow body mass index, renal failure, previous bleedingvents, and concomitant antithrombotic therapies). In par-icular, a pre-PCI PRU value in the lowest quartile wasssociated with a 4.5-fold increased risk for postinterven-ion major bleeding or entry-site complications compared tohe highest quartile. More pronounced platelet inhibitionas also associated with higher incidence of minor bleeding
t 30 days. In a prospective study,27 the in-hospital inci-dence of major bleeding was 3.5-fold higher in PCI patientswith enhanced clopidogrel responsiveness (defined as �188aggregation units) measured before the procedure by themultiple electrode aggregometry. In contrast, in a recentinvestigation on patients who underwent elective PCI,28
several platelet function tests failed to predict postdischargebleeding events up to 1 year.
Receiver-operating characteristic analysis in our studyindicated that the VerifyNow assay can predict periproce-dural bleeding outcomes, with an optimal cut-off point todiscriminate patients at higher risk for 30-day major bleed-ing of �189 PRU and sensitivity of 87%. Thus, ARMYDA-BLEEDS confirms the usefulness of a rapid point-of-careassay for monitoring residual platelet reactivity after clopi-dogrel administration, to identify a clinically driven thresh-old of platelet reactivity defining patients at increased riskfor bleeding complications, in whom individualized thera-peutic strategies (i.e., limited use of glycoprotein IIb/IIIainhibitors, more extensive utilization of bivalirudin, re-stricted use of drug-eluting stents, and more liberal use ofgastroprotective agents) may be indicated. In our study,most bleeding events were large entry-site hematomas; thus,a radial approach, which has been associated with a lowerincidence of vascular complications,29 might be also indi-
PRU levels in the lowest quartile had a significantly higher risk for 30-dayal 1.9 to 25.9, p � 0.01). BMI � body mass index.
vention
ated in patients with higher degrees of platelet inhibition in
999Coronary Artery Disease/High Clopidogrel Response Predicts PCI Bleeding
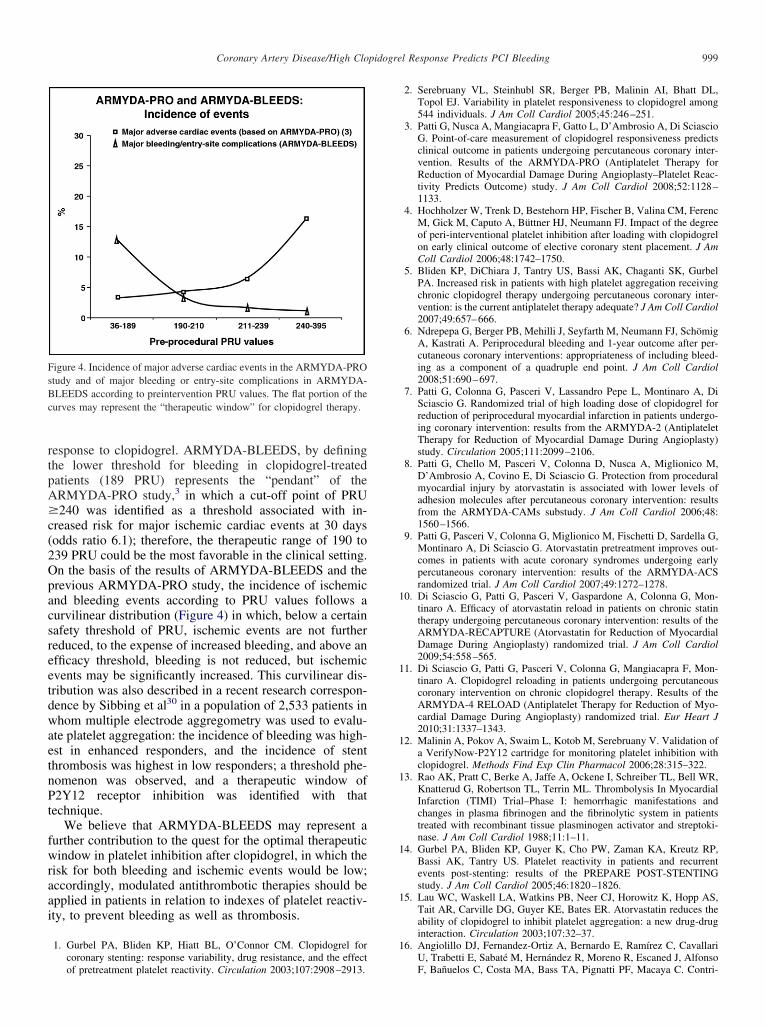
response to clopidogrel. ARMYDA-BLEEDS, by definingthe lower threshold for bleeding in clopidogrel-treatedpatients (189 PRU) represents the “pendant” of theARMYDA-PRO study,3 in which a cut-off point of PRU�240 was identified as a threshold associated with in-creased risk for major ischemic cardiac events at 30 days(odds ratio 6.1); therefore, the therapeutic range of 190 to239 PRU could be the most favorable in the clinical setting.On the basis of the results of ARMYDA-BLEEDS and theprevious ARMYDA-PRO study, the incidence of ischemicand bleeding events according to PRU values follows acurvilinear distribution (Figure 4) in which, below a certainsafety threshold of PRU, ischemic events are not furtherreduced, to the expense of increased bleeding, and above anefficacy threshold, bleeding is not reduced, but ischemicevents may be significantly increased. This curvilinear dis-tribution was also described in a recent research correspon-dence by Sibbing et al30 in a population of 2,533 patients inwhom multiple electrode aggregometry was used to evalu-ate platelet aggregation: the incidence of bleeding was high-est in enhanced responders, and the incidence of stentthrombosis was highest in low responders; a threshold phe-nomenon was observed, and a therapeutic window ofP2Y12 receptor inhibition was identified with thattechnique.
We believe that ARMYDA-BLEEDS may represent afurther contribution to the quest for the optimal therapeuticwindow in platelet inhibition after clopidogrel, in which therisk for both bleeding and ischemic events would be low;accordingly, modulated antithrombotic therapies should beapplied in patients in relation to indexes of platelet reactiv-ity, to prevent bleeding as well as thrombosis.
1. Gurbel PA, Bliden KP, Hiatt BL, O’Connor CM. Clopidogrel forcoronary stenting: response variability, drug resistance, and the effect
Figure 4. Incidence of major adverse cardiac events in the ARMYDA-PROstudy and of major bleeding or entry-site complications in ARMYDA-BLEEDS according to preintervention PRU values. The flat portion of thecurves may represent the “therapeutic window” for clopidogrel therapy.
of pretreatment platelet reactivity. Circulation 2003;107:2908–2913.
2. Serebruany VL, Steinhubl SR, Berger PB, Malinin AI, Bhatt DL,Topol EJ. Variability in platelet responsiveness to clopidogrel among544 individuals. J Am Coll Cardiol 2005;45:246–251.
3. Patti G, Nusca A, Mangiacapra F, Gatto L, D’Ambrosio A, Di SciascioG. Point-of-care measurement of clopidogrel responsiveness predictsclinical outcome in patients undergoing percutaneous coronary inter-vention. Results of the ARMYDA-PRO (Antiplatelet Therapy forReduction of Myocardial Damage During Angioplasty–Platelet Reac-tivity Predicts Outcome) study. J Am Coll Cardiol 2008;52:1128–1133.
4. Hochholzer W, Trenk D, Bestehorn HP, Fischer B, Valina CM, FerencM, Gick M, Caputo A, Büttner HJ, Neumann FJ. Impact of the degreeof peri-interventional platelet inhibition after loading with clopidogrelon early clinical outcome of elective coronary stent placement. J AmColl Cardiol 2006;48:1742–1750.
5. Bliden KP, DiChiara J, Tantry US, Bassi AK, Chaganti SK, GurbelPA. Increased risk in patients with high platelet aggregation receivingchronic clopidogrel therapy undergoing percutaneous coronary inter-vention: is the current antiplatelet therapy adequate? J Am Coll Cardiol2007;49:657–666.
6. Ndrepepa G, Berger PB, Mehilli J, Seyfarth M, Neumann FJ, SchömigA, Kastrati A. Periprocedural bleeding and 1-year outcome after per-cutaneous coronary interventions: appropriateness of including bleed-ing as a component of a quadruple end point. J Am Coll Cardiol2008;51:690–697.
7. Patti G, Colonna G, Pasceri V, Lassandro Pepe L, Montinaro A, DiSciascio G. Randomized trial of high loading dose of clopidogrel forreduction of periprocedural myocardial infarction in patients undergo-ing coronary intervention: results from the ARMYDA-2 (AntiplateletTherapy for Reduction of Myocardial Damage During Angioplasty)study. Circulation 2005;111:2099–2106.
8. Patti G, Chello M, Pasceri V, Colonna D, Nusca A, Miglionico M,D’Ambrosio A, Covino E, Di Sciascio G. Protection from proceduralmyocardial injury by atorvastatin is associated with lower levels ofadhesion molecules after percutaneous coronary intervention: resultsfrom the ARMYDA-CAMs substudy. J Am Coll Cardiol 2006;48:1560–1566.
9. Patti G, Pasceri V, Colonna G, Miglionico M, Fischetti D, Sardella G,Montinaro A, Di Sciascio G. Atorvastatin pretreatment improves out-comes in patients with acute coronary syndromes undergoing earlypercutaneous coronary intervention: results of the ARMYDA-ACSrandomized trial. J Am Coll Cardiol 2007;49:1272–1278.
10. Di Sciascio G, Patti G, Pasceri V, Gaspardone A, Colonna G, Mon-tinaro A. Efficacy of atorvastatin reload in patients on chronic statintherapy undergoing percutaneous coronary intervention: results of theARMYDA-RECAPTURE (Atorvastatin for Reduction of MyocardialDamage During Angioplasty) randomized trial. J Am Coll Cardiol2009;54:558–565.
11. Di Sciascio G, Patti G, Pasceri V, Colonna G, Mangiacapra F, Mon-tinaro A. Clopidogrel reloading in patients undergoing percutaneouscoronary intervention on chronic clopidogrel therapy. Results of theARMYDA-4 RELOAD (Antiplatelet Therapy for Reduction of Myo-cardial Damage During Angioplasty) randomized trial. Eur Heart J2010;31:1337–1343.
12. Malinin A, Pokov A, Swaim L, Kotob M, Serebruany V. Validation ofa VerifyNow-P2Y12 cartridge for monitoring platelet inhibition withclopidogrel. Methods Find Exp Clin Pharmacol 2006;28:315–322.
13. Rao AK, Pratt C, Berke A, Jaffe A, Ockene I, Schreiber TL, Bell WR,Knatterud G, Robertson TL, Terrin ML. Thrombolysis In MyocardialInfarction (TIMI) Trial–Phase I: hemorrhagic manifestations andchanges in plasma fibrinogen and the fibrinolytic system in patientstreated with recombinant tissue plasminogen activator and streptoki-nase. J Am Coll Cardiol 1988;11:1–11.
14. Gurbel PA, Bliden KP, Guyer K, Cho PW, Zaman KA, Kreutz RP,Bassi AK, Tantry US. Platelet reactivity in patients and recurrentevents post-stenting: results of the PREPARE POST-STENTINGstudy. J Am Coll Cardiol 2005;46:1820–1826.
15. Lau WC, Waskell LA, Watkins PB, Neer CJ, Horowitz K, Hopp AS,Tait AR, Carville DG, Guyer KE, Bates ER. Atorvastatin reduces theability of clopidogrel to inhibit platelet aggregation: a new drug-druginteraction. Circulation 2003;107:32–37.
16. Angiolillo DJ, Fernandez-Ortiz A, Bernardo E, Ramírez C, CavallariU, Trabetti E, Sabaté M, Hernández R, Moreno R, Escaned J, Alfonso
F, Bañuelos C, Costa MA, Bass TA, Pignatti PF, Macaya C. Contri-
1000 The American Journal of Cardiology (www.ajconline.org)
bution of gene sequence variations of the hepatic cytochrome P4503A4 enzyme to variability in individual responsiveness to clopidogrel.Arterioscler Thromb Vasc Biol 2006;26:1895–1900.
17. Sibbing D, Koch W, Gebhard D, Schuster T, Braun S, Stegherr J,Morath T, Schömig A, von Beckerath N, Kastrati A. Cytochrome2C19*17 allelic variant, platelet aggregation, bleeding events, andstent thrombosis in clopidogrel-treated patients with coronary stentplacement. Circulation 2010;121:512–518.
18. Lau WC, Gurbel PA, Watkins PB, Neer CJ, Hopp AS, Carville DG,Guyer KE, Tait AR, Bates ER. Contribution of hepatic cytochromeP450 3A4 metabolic activity to the phenomenon of clopidogrel resis-tance. Circulation 2004;109:166–171.
19. Price MJ, Endemann S, Gollapudi RR, Valencia R, Stinis CT, LevisayJP, Ernst A, Sawhney NS, Schatz RA, Teirstein PS. Prognostic sig-nificance of post-clopidogrel platelet reactivity assessed by a point-of-care assay on thrombotic events after drug-eluting stent implantation.Eur Heart J 2008;29:992–1000.
20. Marcucci R, Gori AM, Paniccia R, Giusti B, Valente S, Giglioli C,Buonamici P, Antoniucci D, Abbate R, Gensini GF. Cardiovasculardeath and nonfatal myocardial infarction in acute coronary syndromepatients receiving coronary stenting are predicted by residual plateletreactivity to ADP detected by a point-of-care assay: a 12-monthfollow-up. Circulation 2009;119:237–242.
21. Yusuf S, Zhao F, Mehta SR, Chrolavicius S, Tognoni G, Fox KK;Clopidogrel in Unstable Angina to Prevent Recurrent Events TrialInvestigators. Effects of clopidogrel in addition to aspirin in patientswith acute coronary syndromes without ST-segment elevation. N EnglJ Med 2001;345:494–502.
22. Wiviott SD, Braunwald E, McCabe CH, Montalescot G, Ruzyllo W,Gottlieb S, Neumann FJ, Ardissino D, De Servi S, Murphy SA,Riesmeyer J, Weerakkody G, Gibson CM, Antman EM; TRITON-TIMI 38 Investigators. Prasugrel versus clopidogrel in patients withacute coronary syndromes. N Engl J Med 2007;357:2001–2015.
23. Wallentin L, Becker RC, Budaj A, Cannon CP, Emanuelsson H,Held C, Horrow J, Husted S, James S, Katus H, Mahaffey KW,
Scirica BM, Skene A, Steg PG, Storey RF, Harrington RA; PLATOInvestigators, Freij A, Thorsén M. Ticagrelor versus clopidogrel inpatients with acute coronary syndromes. N Engl J Med 2009;361:1045–1057.
24. Rao SV, Eikelboom JA, Granger CB, Harrington RA, Califf RM,Bassand JP. Bleeding and blood transfusion issues in patients withnon-ST-segment elevation acute coronary syndromes. Eur Heart J2007;28:1193–1204.
25. Eikelboom JW, Mehta SR, Anand SS, Xie C, Fox KA, Yusuf S.Adverse impact of bleeding on prognosis in patients with acute coro-nary syndromes. Circulation 2006;114:774–782.
26. Mangiacapra F, Barbato E, Patti G, Gatto L, Vizzi V, Ricottini E,D’Ambrosio A, Wijns W, Di Sciascio G. Point-of-care assessment ofplatelet reactivity after clopidogrel to predict myonecrosis in patientsundergoing percutaneous coronary intervention. JACC Cardiovasc In-terv 2010;3:318–323.
27. Sibbing D, Schulz S, Braun S, Morath T, Stegherr J, Mehilli J,Schömig A, von Beckerath N, Kastrati A. Antiplatelet effects ofclopidogrel and bleeding in patients undergoing coronary stent place-ment. J Thromb Haemost 2010;8:250–256.
28. Breet NJ, van Werkum JW, Bouman HJ, Kelder JC, Ruven HJ, BalET, Deneer VH, Harmsze AM, van der Heyden JA, Rensing BJ,Suttorp MJ, Hackeng CM, ten Berg JM. Comparison of platelet func-tion tests in predicting clinical outcome in patients undergoing coro-nary stent implantation. JAMA 2010;303:754–762.
29. Agostoni P, Biondi-Zoccai GG, de Benedictis ML, Rigattieri S, TurriM, Anselmi M, Vassanelli C, Zardini P, Louvard Y, Hamon M. Radialversus femoral approach for percutaneous coronary diagnostic andinterventional procedures; Systematic overview and meta-analysis ofrandomized trials. J Am Coll Cardiol 2004;44:349–356.
30. Sibbing D, Steinhubl SR, Schulz S, Schomig A, Kastrati A. Plateletaggregation and its association with stent thrombosis and bleeding in
clopidogrel-treated patients: initial evidence of a therapeutic window.J Am Coll Cardiol 2010;56:317–318.




























