Embed Size (px)
Citation preview

Use of transmission electron microscopy for studying airway remodeling
in a chronic ovalbumin mice model of allergic asthma
G. D. Leishangthem1, U. Mabalirajan
2, T. Ahmad
2, B. Ghosh
2, A. Agrawal
2, T. C. Nag
3 and A. K.
Dinda1
1Renal Pathology Laboratory, Department of Pathology, All India Institute of Medical Sciences, New Delhi, India. 2Molecular Immunogenetics Laboratory and Center for Translational Research in Asthma & Lung Disease, Institute of
Genomics & Integrative Biology, Delhi, India.
3Department of Anatomy, All India Institute of Medical Sciences, New Delhi, India.
Asthma represents chronic inflammatory process of the airways followed by healing that may result in an altered structure
referred to as airway remodeling. The mechanisms underlying airway remodeling remain unknown and so we need to
know the minute structural details of the asthmatic airway before mining mechanisms. Histopathological and transmission
electron microscopic studies were perfromed in chronic asthmatic murine lungs and they revealed the damage to bronchial
epithelial cells, goblet cell metaplasia with mucus hypersecretion and cellular infiltration in perivascular and
peribronchiolar areas. The infiltrated cells were composed mainly of eosinophils, lymphocytes and macrophages. There
was a widening of intercellular spaces between bronchial epithelia especially at abluminal regions. Basement membranes
were thickened and composed mainly of collagen. There were increased population of smooth muscle and fibroblast and in
addition there were more numbers of mitohcondria in smooth muscle. This would help us to understand the human asthma
in much better way.
Key Words asthma; in situ perfusion fixation; transmission electron microscopy
1. Introduction
Asthma is defined as a chronic airway disease characterized by reversible airflow obstruction, airway
hyperresponsiveness, airway inflammation, and structural changes of airway which otherwise called airway remodeling
[1]. To demonstrate most of these fundamental features of asthma, one obviously needs various disciplines such as
physiology, immunology and pathology. Amongst these pathology has an important role due to its illustrative nature.
Indeed the demonstration of pathological features led to novel and exciting hypotheses to understand asthma in different
dimensions. For example, pathological observations of mucus plugs and neutrophils in major bronchi in autopsied
asthmatic lungs raised a concern in viewing fatal asthma as a different subtype, acute severe asthma, and urged to
explore pathogenesis, molecular pathways and therapeutics [2, 3]. The current description of asthma cannot be complete
without mentioning the structural changes of airway as contrast to earlier description which merely emphasize the
importance of inflammation. Shortly, understanding the structural and minute features of lung may allow us to describe
asthma in a holistic view rather than different parts of it. Light microscopy (LM) can reveal most of the gross
pathological features of asthma. However, it can’t reveal the minute details of cellular and tissue structures of lung.
Electron microscopy (EM) has a lot of potential to identify and characterize these minute features at sub-cellular level.
Though EM requires high start-up and maintenance cost, the findings derived from it has extended the knowledge in
different dimensions which are crucial in developing better therapeutics. However, due to the availability of EM in
central facilities in most of the institutes, it seems that the use of EM by researchers may not be the major concern. To
illustrate the minute details of lung, we have used chronic mouse model of asthma and performed EM with lungs. In
addition, we used LM to support and add further details on the ultrastructural features.
Before dealing with microscopic features, it is important to describe the mice model of asthma briefly. First of all, it
is well accepted fact that experimental animal models are essential and sometimes inevitable tools for clear
understanding of the pathophysiology of various complex diseases such as asthma [4]. Though even a single animal
model cannot suitably reproduce human asthma completely, mouse models of asthma have been shown to be useful
tools to understand the various features of human asthma [5]. The commonly used mouse model of asthma is based on
ovalbumin (OVA) sensitization and challenge. OVA, a chicken egg protein, can elicit allergic sensitization if given
systemically along with suitable adjuvants such as aluminum hydroxide (ALUM). A series of intraperitoneal injections
of OVA+ALUM must be given to attain successful sensitization. To elicit asthmatic features, OVA should be then
administered as an inhaled aerosol or intra nasal drops referred to as challenge. It is necessary to perform physiological
lung function measurements to make sure that these mice developed asthma features. The term ‘asthma’ in mice is only
meaningful with demonstration of airway obstruction using various sophisticated instruments. We use three methods:
single, double chamber plethysmography and flexiVent which determine enhanced pause, specific airway conductance
and airway resistance respectively. Since the scope this review is restricted to microscopy, we couldn’t describe these
physiological methods in detail. However, readers may refer physiological reviews for details [6, 7]. Generally OVA-
sensitization and -challenge leads to pathological features of asthma such as infiltration of various inflammatory cells
Microscopy: Science, Technology, Applications and Education A. Méndez-Vilas and J. Díaz (Eds.)
©FORMATEX 2010 347
______________________________________________

such as lymphocytes, eosinophils, macrophages into the airway, mucus hypersecretion and goblet cell metaplasia.
However, chronic allergen exposures lead to cause both inflammatory and structural changes of airway such as
hypertrophy and hyperplasia of bronchial epithelia, goblet cell metaplasia, basement membrane thickening, sub-
epithelial fibrosis, and hypertrophy & hyperplasia of airway smooth muscle. Since there are various pathological
features, there is no single technique to demonstrate all. These techniques have been mentioned below.
2. Materials and Methods
2.1 Animals
Male BALB/c mice (8-10 weeks old at starting) were randomly divided into two groups: Sham and OVA (n=6 each).
Mice were sensitized by three intraperitoneal injections (i.p. inj.) of 50 µg OVA in 4 mg ALUM (OVA group) or 4 mg
ALUM alone (Sham group) on days 0, 7, and 14. Mice were challenged from Day 21 to Day 43 (30 minutes per day,
alternative days) with 3% OVA in PBS (OVA group) or PBS (Sham group) using a nebulizer with a flow rate of 9
L/min. After determining airway hyperresponsiveness (AHR) to methacholine on Day 44, mice were sacrificed and
lungs were taken for both LM and EM studies.
2.2 Histopathology
Lungs were fixed in 10% neutral buffered formalin, dehydrated and embedded in paraffin. For histological
examination, embedded lungs were sectioned on glass slides, deparaffinized, and stained with Hematoxylin and Eosin
(H & E), Alcian Blue-Periodic acid Schiff and Masson Trichrome stainings to assess the airway inflammation, goblet
cell metaplasia and sub-epithelial fibrosis respectively.
2.3 Transmission Electron Microscopy
Combined in situ perfusion and immersion fixation
NSS2.5%
Glutaraldehyde
1m
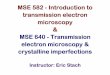
Fig. 1 Schematic diagram of in-situ perfusion fixation technique.
Each mouse was anaesthetized by i.p. inj. of sodium pentobarbitone (1-2 mg per mouse), deep anesthesia was
confirmed by absence of reflex on tweaking the foot. Thoracic cavity was opened by midsternal splitting incision to
expose the heart and posterior vena cava (PVC), 18 gauze cannula was inserted into the apex of the heart to access the
left ventricle, cannula was connected to bottle, located 1 meter above the body of the mouse, containing cacodylate
buffer via tubing and flow controlling valve (Fig. 1). Initial flush out was performed for 3-5 minutes with PBS after
cutting the PVC till achieving complete exsanguination. Then the perfusion was switched over to the cacodylate buffer
Microscopy: Science, Technology, Applications and Education A. Méndez-Vilas and J. Díaz (Eds.)
348 ©FORMATEX 2010
______________________________________________

containing glutaraldehyde fixative for 25-30 minutes with a flow rate of approx. 3ml/min. Fixation was done at room
temperature. Hardening of all the exposed organs was felt at the end of fixation. Lungs (hard and fragile) were removed
and immersed into the fixative (2.5% glutaraldehyde) and kept at 40C for overnight. Fixed lungs were dissected under
Dissection microscope (SZX-12, Olympus) and those were cut into many slices of same thickness. Each slice was made
into three blocks and they were post fixed in 1% osmium tetraoxide and then processed and embedded in epoxy resin.
Ultrathin sections of about 70-80 nm were cut and stained using uranyl acetate and lead citrate. The stained sections
were viewed under electron microscope (Morgagni 268D, Fei Electron Optics).
3. Results
3.1 Airway inflammation
D
H
p
p
p
p
E
C
E F G
M
M
p
rer
rer
n
m
n
m
n
ps
*
Br
Br
vv
BA D
Fig. 2 LM and TEM of airway inflammation in chronic model of asthma. H & E staining of lungs of Sham control mice (A, 10X)
showed no sign of inflammation whereas OVA mice showed marked infiltration of inflammatory cells at bronchovascular regions (B,
10X, Br: bronchiole, v: blood vessels). TEM of various inflammatory cells such as of plasma cells (P), eosinophils (E) and
macrophages (M) (C & D, 880X) in OVA mice. Higher magnifications showed eosinophil with secondary granules (arrow) (E,
3200X), plasma cells with characteristic rough endoplasmic reticulum (rer) occupying whole cytoplasm with eccentric nucleus (n) (F,
3200X) and alveolar macrophages with lysosome vacuole (arrow) in the cytoplasm and pseudopods (ps) (G, 3200X). Remnants of
apoptotic cell nucleus (*) were observed in the cytoplasm of Macrophage (H, 1100X).
Airway inflammation is the main feature in asthma. Airway of Sham mice showed the normal architecture without
any sign of inflammation (Fig. 2A), in contrast OVA mice showed the infiltration of various inflammatory cells around
the vessels and bronchi (Fig. 2B). There were more of perivascular cell infiltrations than peribronchial infiltration in
OVA mice. EM revealed that these cells were predominantly eosinophils, lymphocytes and macrophages (Fig. 2C &
D). The presence of eosinophilic granules, peculiar longitudinal grain shaped, indicates these cells are eosinophils (Fig.
2E). These granules have inner electron dense core which is surrounded by electron lucent matrix. In this study, we
could find inactive granules since there are intact granules without any loss of core and matrix. In addition, plasmacytes,
which are responsible for IgE production, are easily recognized by their characteristic appearance with rough
endoplasmic reticulum (Fig. 2F). Macrophages were identified by their pseudopodia (Fig. 2G). Interestingly, nuclear
elements were found in the cytoplasm of macrophages (Fig. 2H), indicate the possible phagocytosis of other
inflammatory cells such as neutrophils and also this indicate that these macrophages may be healing type which eat
most of the post inflammatory nasty substances such as necrotic and/or apoptotic remnants and also initiate the fibrotic
process.
3.2 Goblet cell metaplasia
Sham mice showed almost no or occasional PAS positive cells in the airway (Fig. 3A). On the other hand, OVA mice
showed more PAS positive cells (Fig. 3B) indicate the goblet cell metaplasia. Airway of mice is populated mainly with
ciliated cells and Clara cells and less mucous cells. EM revealed that OVA mice showed more goblet cells with lot of
mucous granules (Fig 3C & D). Ciliated cells were recognized by its columnar shape, large basal nucleus, electron
lucent cytoplasm and obviously the presence of cilia, Clara cells were by its apical projection towards its lumen and
Microscopy: Science, Technology, Applications and Education A. Méndez-Vilas and J. Díaz (Eds.)
©FORMATEX 2010 349
______________________________________________

presence of electron dense serous granules and mucous cells were by the presence of mucus which can be recognized by
membrane bound vacuoles containing electron lucent substance. Similar to other studies [8, 9] we also found the
mucous granules in Clara cell indicate the conversion of Clara cell to mucous cell.
cec
sg
sg
sgC
cec
cc
bc
B
DC
Br
vBr
A
3.3 Widening of intercellular spaces between bronchial epithelia
Fig. 4 TEM of intercellular space widening. Sham control mice (A, 880X) showed thin and regular intercellular space compared to
OVA mice which showed marked widening of intercellular space between adjacent bronchial epithelial cells (B, 880X). Arrows
indicate the junction. High power magnification showed the cytoplasmatic elongations of adjacent bronchial epithelia in OVA mice
(C, 10500X).
The adjacent bronchial epithelia are interconnected by tight junctions and these junctions control the paracellular
permeability and maintain the epithelial barrier function. In Sham mice, these intercellular spaces were thin and regular
(Fig. 4A). However, in OVA mice these spaces were widened especially at abluminal regions compared to apical
regions (Fig. 4B). Higher magnification revealed the cytoplasmatic prolongations of the adjacent epithelial cells (Fig.
4C).
3.4 Basement membrane thickening
Basement membrane is the connective tissue structure which supports the airway epithelial layer. LM cannot visualize
this structure easily unless otherwise there is a thickening. MT staining showed that Sham mice had less collagen
compared to thickened collagen layer in OVA mice (Fig. 5A & B). Sham mice showed thin basement membrane
underneath the basal cell (Fig 5C). OVA mice showed thickening of the basement membrane (Fig. 5D, 4634.4 ± 359.7
vs. 881.4 ± 142.6; OVA vs. Sham, mean ± sd). This thickened basement membrane predominantly composed of
collagen (Fig 5E).
C
Intercellular space
A B
Fig. 3 LM and TEM of mucous cell
metaplasia. AB-PAS staining of lungs of
Sham control mice (A, 10X) showed no
Goblet cell metaplasia whereas OVA
mice (B, 20X) show marked Goblet cell
metaplasia (Br: bronchiole, v: blood
vessels). Inset showed the magnified
mucous cell (60X). TEM of bronchi
showed mucous cells characterized by
the presence of electron lucent mucus
containing secretory granules (sg) and
ciliated epithelial cells (cec) were
compressed towards the side (C, 880X,
c, cilia). Clara cells (cc) were also seen
with mucus electron dense as well as
electron lucent secretory granules at the
apical projection (D, 880X).
Microscopy: Science, Technology, Applications and Education A. Méndez-Vilas and J. Díaz (Eds.)
350 ©FORMATEX 2010
______________________________________________

3.5 Smooth muscle alteration
Fig. 6 TEM of airway smooth muscle. Airway smooth muscles (asm) in Sham control mice (A, 880X) were thin whereas OVA mice
(B, 880X) showed the increased in the size. These smooth muscles from OVA mice also showed the presence of more number of
mitochondria (m) (C, 1950X).
Normally airway smooth muscle present mostly in proximal bronchi and this is responsible for most of the
bronchoconstriction. The presence of smooth muscle can be recognized by LM but detailed sub-cellular structures can
be readily recognizable with EM. While normal mice showed a single layer of smooth muscle (Fig. 6A), OVA mice
showed hyperplasia and hypertrophy of smooth muscle (Fig. 6B). Interestingly, there were more numbers of
mitochondria in these cells (Fig. 6C).
4. Discussion
Various studies have described the histopathologic features of asthma by LM. However, there are few reports to
describe the ultrastructural features by EM. This could be because of the requirement of sophisticated instrument,
trained hands, laborious work and interpreting capacity. In this study, we have described the minute details of lung
which occurs in chronic model of asthma. Airway inflammation in asthma is the infiltration of various kinds of
inflammatory cells around the airway rather than in the parenchyma. Generally this inflammation is described as
perivascular and peribronchial inflammation. This is the contrast feature compared to chronic obstructive pulmonary
Br
B A
C D
ep
BM B
M
bc
col
E
Fig. 5 TEM of Basement membrane
thickening. Masson Trichrome
staining of lungs of Sham control
mice (A, 10X) showed no fibrosis
whereas OVA mice (B, 10X) showed
marked fibrosis around the bronchi.
TEM showed the normal basement
membrane in Sham mice (C, 880X)
and thickened in OVA mice (D,
880X) and high magnification showed
the presence of collagen bundles (E,
1950X) in the basement membrane.
B C
m
m
asm
asm
A
Microscopy: Science, Technology, Applications and Education A. Méndez-Vilas and J. Díaz (Eds.)
©FORMATEX 2010 351
______________________________________________

disease in which parenchymal inflammation occurs along with small airway inflammation [10]. Since this study
describes the inflammation in a qualitative aspect due to all or none feature between OVA and Sham mice, the
quantitation to get inflammation scores hasn’t been performed. However, this scoring is inevitable if there is a need to
compare different OVA groups (e.g. in case of investigating drug effect) due to inhomogeneous distribution of
inflammation. The scoring should be in a blind manner and grades of 0 to 4 [no inflammatory cell to a thick layer (more
than 5 cells deep) of inflammatory cells around the bronchi and vessel] may be assigned [11]. The description of
inflammation may not require EM, however very often there is confusion in differentiating eosinophils from neutrophils
since book descriptions may not be found frequently. Immunohistochemistry also can differentiate eosinophil from
neutrophil but it can’t reveal the activeness of eosinophils. However, EM not only can recognize eosinophils due to the
peculiar feature of eosinophilic granules but also reveal the activeness of the granules. As shown in Fig. 2E, these
granules have two major parts: core and matrix. Intact granules indicate inactive state and granules with loss of core
and/or matrix indicate the active state. Generally it has been believed that eosinophil degranulation is absent in mice
[12]. However, it has been demonstrated that the activation is more in airway lumen of asthmatic mice [13] and
similarly we had found partial active granules in our sub-acute model of asthma (our unpublished observations).
However, we could find the intact or inactive granules in chronic model of asthma (Fig. 2E). But these mice also
showed higher IL-5 levels. This indicate that IL-5, eosinophil survival factor, may be responsible for the persistence of
these inactive eosinophils in chronic model. EM can easily recognize the plasma cells by its peculiar feature of RER
arrangement surrounding the nucleus. These plasma cells synthesize more IgE which leads to cause mast cell
degranulation and airway obstruction [14].
Airway inflammation is mostly commonly accompanied by goblet cell metaplasia. This can be recognized by PAS
staining in which goblet cell shows the presence of magenta colored mucin containing granules. On the other hand, EM
can describe minute details related to this feature such as cilia, microvilli, electron dense secretary and electron lucent
secretary granules. These minute structures can differentiate the type of epithelial cells and often the functional status of
the cells. In mice, it has been shown that Clara cells are being converted to mucus hypersecreting cell type [8, 9].
Infiltrated inflammatory cells injure the structural cells such as airway epithelia. This injury is predominantly
mediated by the toxic proteins secreted by these inflammatory cells. For example, eosinophil secretes eosinophil
peroxidase, major basic protein, eosinophil cationic protein and eosinophil-derived neurotoxin [15]. Chronic allergen
exposures lead to reduce defensive mechanisms of airway epithelia and cause the damage to those cells [16]. Also we
found earlier that bronchial epithelia of asthmatic mice have shown mitochondrial swelling and loss of cristae [11]. It
has been observed that increased numbers of mitochondria and altered mitochondria in bronchial epithelium in murine
model of asthma and asthmatic children [17-18]. This might lead to cause apoptosis at earlier stages; this is evident by
reduction in cytochrome c oxidase in bronchial epithelia, increased cytosolic cytochrome c in lung cytosols and also
there is an involvement of death receptor pathway to induce apoptosis in asthmatic bronchial epithelia [11, 19]. These
indicate the possibility of involvement of both intrinsic and extrinsic pathways of apoptosis in asthmatic bronchial
epithelia. This might be lead to shrinkage of these epithelia. This could support our observation of widening of the
intercellular space between subsequent bronchial epithelial cells. Interestingly, the widening was prominent in the
abluminal regions rather than the apical regions. However, denudation was not a frequent finding in this chronic model
of asthma; indicate that this would have occurred at earlier stage of the disease. In evident to this we have found ciliated
epithelia in BAL slides of asthmatic mice compared to normal mice (our unpublished observations). Also it has been
reported that epithelial clumps have been found in sputum and BAL fluid of human asthmatics [20].
It is known that epithelial injury is known to activate the epithelial mesenchymal trophic unit (EMTU) in the airway
[21]. In this process growth factors are getting released by both bronchial epithelia and fibroblast. Due to this activation
the attenuated fibroblast layer which is located beneath the basement membrane is transformed into myofibroblast and
start secreting both actin and collagen [21]. This leads to more accumulation of collagen beneath the epithelia, called
sub-epithelial fibrosis. Though it is called sub-epithelial fibrosis the collagen bundles were observed even between and
underneath the smooth muscle. There is hypertrophy and hyperplasia of smooth muscle which is located underneath the
fibroblast. In addition, there is increased numbers of mitochondria indicate the possibility mitochondrial biogenesis
[22]. However, the functional status of these mitochondria is not clear.
Acknowledgements GDL was supported by Indian Council of Medical Research, New Delhi, India. Authors acknowledge
Sophisticated Analytical Instrumental Facility, All India Institute of Medical sciences, New Delhi, India. We thank Sandeep Kumar
Srivastava for his help.
References
[1] Wardlaw AJ, Brightling CE, Green R, Woltmann G, Bradding P, Pavord ID. New insights into the relationship between airway
inflammation and asthma. Clin. Sci. (Lond). 2002;103:201-211.
[2] Hays SR, Fahy JV. The role of mucus in fatal asthma. Am. J. Med. 2003;115:68-69.
[3] Fahy JV. Eosinophilic and neutrophilic inflammation in asthma: insights from clinical studies. Proc. Am. Thorac. Soc.
2009;6:256-259.
Microscopy: Science, Technology, Applications and Education A. Méndez-Vilas and J. Díaz (Eds.)
352 ©FORMATEX 2010
______________________________________________

[4] Schork NJ, Nath SP, Lindpaintner K, Jacob HJ. Extensions to quantitative trait locus mapping in experimental organisms.
Hypertension 1996;28:1104–1111.
[5] Richards IM. Mouse models of allergic disease; how do they relate to asthma in man? Clin. Exp. Allergy 1996;26:618–620.
[6] Glaab T, Taube C, Braun A and Mitzner W. Invasive and noninvasive methods for studying pulmonary function in mice. Respir.
Res. 2007;8:63.
[7] Drazen JM, Finn PW, De Sanctis GT. Mouse models of airway responsiveness: Physiological Basis of Observed Outcomes and
Analysis of Selected Examples Using These Outcome Indicators. Annu. Rev. Physiol. 1999;61: 593–625.
[8] Reader JR, Tepper JS, Schelegle ES, Aldrich MC, Putney LF, Pfeiffer JW, Hyde DM. Pathogenesis of mucous cell metaplasia in
a murine asthma model Am. J. Path. 2003;162;2069-2078.
[9] Evans CM, Williams OW, Tuvim MJ, Nigam R, Mixides GP, Blackburn MR. Mucin is produced by Clara cells in the proximal
airways of antigen-challenged mice. Am. J. Respir. Cell. Mol. Biol. 2004;31:382-394.
[10] Barnes PJ, Shapiro SD, Pauwels RA. Chronic obstructive pulmonary disease: molecular and cellular mechanisms. Eur. Respir. J.
2003;22:672-688.
[11] Mabalirajan U, Dinda AK, Kumar S, Roshan R, Gupta P, Sharma SK, Ghosh B. Mitochondrial structural changes and
dysfunction are associated with experimental allergic asthma. J. Immunol. 2008;181:3540-3548.
[12] Malm-Erjefält M, Persson CG, Erjefält JS. Degranulation status of airway tissue eosinophils in mouse models of allergic airway
inflammation. Am. J. Respir. Cell. Mol. Biol. 2001;24:352-359.
[13] Clark K, Simson L, Newcombe N, Koskinen AML, Mattes J, Lee NA, Lee JJ, Dent LA, Matthaei KI, Foster PS Eosinophil
degranulation in the allergic lung of mice primarily occurs in the airway lumen J. Leukoc. Biol. 2004;75:1001–1009.
[14] Gould HJ, Sutton BJ. IgE in allergy and asthma today. Nat. Rev. Immunol. 2008;8:205-217.
[15] Weller PF, Ackerman SJ, Smith JA. Eosinophil granule cationic proteins: major basic protein is distinct from the smaller subunit
of eosinophil peroxidase Leukoc. Biol. 1988;43:1-4.
[16] Wright DT, Cohn LA, Li H, Fischer B, Li CM, Adler KB. Interactions of oxygen radicals with airway epithelium. Environ.
Health. Perspect. 1994;102 Suppl 10:85-90.
[17] Hayashi T, Ishii A, Nakai S, Hasegawa K. Ultrastructure of goblet-cell metaplasia from Clara cell in the allergic asthmatic
airway inflammation in a mouse model of asthma in vivo. Virchows. Arch. 2004;444:66-73.
[18] Konradova V, Copova C, Sukova B, Houstek J. Ultrastructure of the bronchial epithelium in three children with asthma.
Pediatr. Pulmonol. 1985;1:182-187.
[19] Druilhe A, Wallaert B, Tsicopoulos A, Lapa e Silva JR, Tillie-Leblond I, Tonnel AB, Pretolani M. Apoptosis, proliferation, and
expression of Bcl-2, Fas, and Fas ligand in bronchial biopsies from asthmatics. Am. J. Respir. Cell. Mol. Biol. 1998;19:747-757.
[20] Barnes PJ. Pathophysiology of asthma. Br. J. Clin. Pharmacol. 1996;42:3-10.
[21] Holgate ST, Davies DE, Puddicombe S, Richter A, Lackie P, Lordan J, Howarth P. Mechanisms of airway epithelial damage:
epithelial-mesenchymal interactions in the pathogenesis of asthma. Eur. Respir. J. 2003;44:24s-29s.
[22] Trian T, Benard G, Begueret H, Rossignol R, Girodet PO, Ghosh D, Ousova O, Vernejoux JM, Marthan R, Tunon-de-Lara JM,
Berger P. Bronchial smooth muscle remodeling involves calcium-dependent enhanced mitochondrial biogenesis in asthma. J.
Exp. Med. 2007;204:3173-3181.
Microscopy: Science, Technology, Applications and Education A. Méndez-Vilas and J. Díaz (Eds.)
©FORMATEX 2010 353
______________________________________________