Embed Size (px)
Citation preview

This study did n
*Reprint req
Hadassah Hebre
Israel.
E-mail add
(Y.A. Weil).
J Shoulder Elbow Surg (2014) -, 1-6
1058-2746/$ - s
http://dx.doi.org
www.elsevier.com/locate/ymse
Use of three-dimensional fluoroscopy to determineintra-articular screw penetration in proximal humeralfracture model
Yoram A. Weil, MD*, Shaul Beyth, MD, PhD, Asala Abu-Ahmad, MD,Amal Khoury, MD, Meir Liebergall, MD, Ori Safran, MD
Department of Orthopaedics, Hadassah Hebrew University Medical Center, Jerusalem, Israel
Background: Proximal humeral locking plates have significantly improved the treatment of proximal hu-meral fractures in recent years; however, they are not devoid of complications. Inadvertent screw penetra-tion into the joint is a well-documented complication. Intraoperative 3-dimensional (3D) imaging mayassist in detecting intra-articular implant penetration. This study compared the performance of a standardC-arm fluoroscope with a novel 3D imaging fluoroscope in detecting penetrating implants in a proximalhumeral fracture model.Methods: Zinc-sprayed proximal humerus sawbones were affixed with a proximal humeral locking plate.Six different constructs were assembled. In each specimen, 1 screw, 2 screws, or no screws were inserted 2-mm proud of the articular surface. Each specimen was imaged with a conventional fluoroscope and a 3Dimaging fluoroscope. Overall, 36 image sets were prepared for each modality. These were evaluated by 2fellowship-trained surgeons for intraobserver and interobserver reliability as well for the accuracy ofdetecting prominent implants in the 2 imaging methods.Results: Overall accuracy for observer A was 89.9% compared with 100% for C-arm fluoroscopy and 3Dimaging fluoroscopy (P < .01) and for observer B was 91.1% and 100% (P ¼ .01), respectively. The kvalues were 0.74 with C-arm fluoroscopy and 1.0 for the 3D imaging fluoroscopy for observer A, and0.93 and 1.0, respectively, for observer B.Conclusions: In a proximal humeral fracture model, C-arm fluoroscopy is a highly accurate imaging mo-dality that can minimize the incidence of penetrating screws into the joint. Further clinical studies arerequired to establish this modality.Level of evidence: Basic Science Study, Imaging, Surgical Technique.� 2014 Journal of Shoulder and Elbow Surgery Board of Trustees.
Keywords: Proximal humeral fracture; intra-articular implants; three-dimensional fluoroscopy
ot require Investigational Review Board approval.
uests: Yoram A. Weil, MD, Orthopaedic Trauma Service,
w University Hospital, PO Box 12000, Jerusalem 91120,
resses: [email protected]; [email protected]
ee front matter � 2014 Journal of Shoulder and Elbow Surgery
/10.1016/j.jse.2013.12.007
The incidence of proximal humeral fractures hadincreased in recent years.1,6 Although nonoperative treat-ment can be offered to most patients,18 many fracturesrequire surgical management. Because fixation techniqueshave evolved recently, especially with regards to fixed-angle devices such as locked plates, the option of open
Board of Trustees.

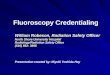
Figure 1 A zinc sprayed sawbone with 6 screws fixed to thebone. The screws were designated A-I. Overall, 6 such constructswere assembled.
2 Y.A. Weil et al.
reduction and internal fixation (ORIF) of proximal humeralfractures has gained popularity.1,6,13
ORIF has achieved excellent results in many patients;however, many recent reports describe a considerably highcomplication rate, especially in treating 3-part and 4 part-fractures with ORIF.2,7,8,19,23 These complications includeloss of reduction, varus collapse, avascular necrosis, andscrew cutout of the humeral head.7,8,15 The latter compli-cation can occur as a primary complication or secondary tofracture settling due to medial instability.9 The screws insome patients, however, are originally placed penetratinginto the glenohumeral joint, with a reported incidence of upto 10% to 15%.7,15 Because most of these procedures relyon conventional C-arm fluoroscopy as the single means ofintraoperative imaging, missing intra-articular screw pene-tration is not avoidable.
In recent years, more sophisticated intraoperative im-aging devices emerged that have enabled 3-dimensional(3D) imaging using specialized fluoroscopes. These weremost useful in delineating the complex anatomy of intra-articular fracture reduction10,16,22 but also assisted indetecting inadvertent violation of joint spaces by screws.3
However, despite the potential advantages, clinicians didnot commonly use these systems, probably due to their highcost, inferior image quality, and the at time, considerableradiation dose delivered to the patient and staff during eachscan.21
Recently, a prototype software module, C-InSight (MazorSurgical Technologies, Caesarea, Israel), has emerged thatallows the use of a conventional 2-dimensional C-arm fluo-roscope, coupled with a target array, to capture and produce3D fluoroscopic images similar to the ones produced bycurrently available 3D devices such as the Siremobil ISO-C3D (Siemens, Erlangen, Germany). Thus, intra-operative3D imaging can now be performed with conventional fluo-roscopes with the potential advantages of decreased cost andreduced radiation time. The goal of this study was to assessthe accuracy and feasibility of the use of intraoperative 3Dfluoroscopy compared with conventional 2D fluoroscopy indetecting intra-articular screw penetration in a proximalhumeral fracture model.
Materials and methods
Zinc sprayed humeral sawbones (Sawbones, Vashon, WA, USA)were used. A PHILOS proximal humeral locking plate (Synthes,Oberdorf, Switzerland) was fixed to the bone using 6 lockingscrews inserted through its proximal part through holes designatedA-I (Fig. 1).
Overall, 6 different constructs were created. Four constructswere made with a single, predefined screw (A, B, E, or I) inserted2-mm proud of the articular surface, as measured using a caliper.The fifth construct had 2 predefined screws (F and H) inserted 2-mm proud of the articular surface, and the sixth construct had nopenetrating screws.
Each construct underwent C-arm fluoroscopy with a 12-inchOEC 9800 fluoroscope (GE, St. Giles, UK) using an ante-roposterior, lateral, and 2 oblique views of 45� (Fig. 2).
3D fluoroscopic process
The C-InSight system consists of a computer station that feedsdirectly from the video output to a conventional C-arm unit, animage adaptor that mounts onto the C-arm image intensifier, and amultiuse plastic target, draped in a disposable sterile sheath, whichis placed over the anatomic region of interest (Fig. 3). This plastictarget is identical to the one placed during spine robotic surgery4
and was successfully tried clinically in our center in otheranatomic regions such as the pelvis and wrist.
A continuous 20-second fluoroscopic scan is performed as theC-arm is moved through its entire arc of rotation (120�), whiletranslating the C-arm forwards or backwards to keep the target atthe image’s center. The software then calculates the position of thescanned anatomic object relative to the plastic target array. Duringthe C-InSight scan, the system captures a real-time video streamof X-ray scans, and the frames are processed sequentially todetermine the target array location because the region of interestmay shift due to C-arm rotation. Once all frames are processed,the system can colocate them in space relative to the target array.Then, the image reconstruction process iteratively builds slabssimilar to computed tomography (CT). Volume reconstruction andreformatting produces axial, sagittal, and coronal images as well

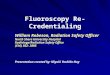
Figure 2 No apparent screw penetration can be seen in 4 fluoroscopic views (anteroposterior, lateral, and 2 obliques) of a specimen usingconventional fluoroscopy.
Figure 3 The C-InSight 3-dimensional (3D) imaging system (Mazor Surgical Technologies, Caesarea, Israel): (A) A conventional C-armis mounted with a calibration frame connected to the computer station. (B) A specialized plastic target array is used to detect the location ofthe anatomic structures to be studied. (C) The array can be wrapped in a sterile bag and placed over the area of interest during surgery.
3D fluoroscopy for proximal humeral fractures 3
as a 3D model in the Digital Imaging and Communications inMedicine format (Fig. 4).
Each construct was scanned 6 times using both imaging mo-dalities. The specimens were repositioned after each scan tosimulate a more realistic scenario in the operating room. Alto-gether, 36 sets of scans were produced for each modality and werearchived on the C-InSight station.
Evaluation of scans
Of the 36 conventional fluoroscopic image sets, 6 PowerPoint(Microsoft Corp, Redmond, WA, USA) presentations were con-structed, each containing 9 scans (4 images each) placed in arandom order. Three of these image sets were duplicates selectedin a random order by using the randomize option in Excel soft-ware (Microsoft Corp).
The C-InSight scans were stored in the computer comprisingthe station and sorted in a random order while the 18 duplicateswere placed in between the scans.
Two shoulder and elbow fellowship-trained surgeons evaluatedthe conventional C-arm image sets and were asked to designate
which screw(s), if at all, were penetrating the humeral head intothe joint. Their decisions were marked on a special form. Inaddition, each evaluator, after a short introductory training, wasinstructed to evaluate the different 3D construct scans (includingduplicates), and designate, in a similar manner, which screw(s), ifat all, were penetrating into the joint.
Statistical analysis
The data were analyzed for interobserver reliability, intraobserverreliability, and accuracy. The power was 98%. Significance wasset at a level of 0.05.
Accuracy was defined as the amount of detection of pene-trating screws. For calculation purposes, the term ‘‘agreement withtruth’’ was defined as complete (2 screws in cases of 2 screws oraccurate screw detection), partial (1 of 2 screws), or null (nocorrelation with truth). The McNemar test was used for statisticalanalysis and interclass coefficient (k value) was calculated.SPSS 18 software (SPSS/IBM Corp, Chicago, IL, USA) was usedfor the analysis. All statistical analyses were performed by abiostatistician.

Figure 4 Two coronal reformats obtained with the C-InSightsystem (Mazor Surgical Technologies, Caesarea, Israel). Apparentscrew perforation is seen in both images.
Table I Accuracy of both observers in detecting penetratingscrews using conventional fluoroscopy
Outcome Observer A) Observer B)
Frequency Percent Frequency Percent
No agreement 4 11.1 1 2.8Partial agreement 7 19.5 2 5.6Absolute agreement 25 69.4 33 91.7Total 36 100.0 36 100.0
) P < .01.
Table II Accuracy of both observers in detecting pene-trating screws using the C-InSight system)
Outcome Observer Ay Observer By
Frequency Percent Frequency Percent
No agreement 0 0 0 0Partial agreement 1 2.8 0 0Absolute agreement 35 97.2 36 100Total 36 100.0 36 100.0
) Mazor Surgical Technologies, Caesarea, Israel.y P < .01.
4 Y.A. Weil et al.
Results
The overall accuracy of both observers in detecting thecorrect protruding screw(s) using the conventional fluoro-scopic images is summarized in Table I. Observer A had anoverall agreement with truth, including complete and par-tial, of 88.9%, whereas observer B achieved 91.7% ofoverall agreement with truth.
When tested for accuracy using the C-InSight system,both observers achieved100%agreementwith truth, whereasobserver A had 1 case of partial agreement and observer Bachieved 100%complete agreement in all 36 scans (Table II).
The interobserver reliability was 72.2% using conven-tional fluoroscopy and 97.2% for the C-InSight system.These differences were statistically significant (P < .01).
Intraobserver reliability (k values) were 0.74 with fluo-roscopy and 1.0 for the C-InSight system for observer Aand 0.93 and 1.0, respectively, for observer B (P < .01).
Discussion
Our study demonstrated a significantly better interpretationof screw penetration when using 3D fluoroscopy than aconventional 2D fluoroscopy in a proximal humeral fracturemodel. Despite conventional fluoroscopy being the goldstandard imaging device in fracture surgery, it has an inherentlimitation in detecting penetrating implants in 3D sphericalstructures. The fact that using this 3D novel system reducedthe error of detection of penetrating implants from9% to 10%to almost 0% confirms our initial hypothesis. The mis-detection of 9% to 10% in the conventional 2D fluoroscopy is
similar to the clinically described incidence of misplacedimplants in the proximal humerus.15,17 Although it may beargued that many of the protruding screws are a result ofsecondary collapse and cutout,8,20 we and others argue that acertain proportion of cases result from initial screw malpo-sitioning during surgery.5,7,14
The phenomenon of misdetection of penetrating im-plants into joints is well described in experimental andclinical examples in the acetabulum, distal radius, andankle.8,11,12 Although authors generally agree that fluoros-copy is limited in this respect, possible suggested solutionsin case of suspected intra-articular implants are reposi-tioning it intraoperatively11 or performing a postoperativeCT scan.24 The authors of a study of the proximal humerussuggest using a blunt-tipped wire to assess the tactileimpact of the bone to avoid penetration.5 The use of post-operative imaging can result in unnecessary secondaryanesthesia and surgery that could have been prevented withappropriate intraoperative imaging.
The use of 3D fluoroscopy has been described as changingintraoperative decisionmaking, not only for articular fracturereduction16 but also for repositioning of the implant.3 Despitethe potential advantages of this modality, it has not gainedvast popularity for several reasons. First, most systemsrequire an isocentric movement (ie, rotation of the robotic C-arm around a fixed center of rotation). Thismay be performedrather easily in the foot and ankle on a radiolucent table butwould be hard to achieve in shoulder surgery in a beach chairposition. Possible collision with the patient’s head and torsowould make this mode of imaging almost impossible.However, the C-InSight system used in this study does notdepend on an isocentric axis but calculates it using the plastic

3D fluoroscopy for proximal humeral fractures 5
target array. Therefore, changes of axis during fluoroscopyare possible, avoiding collisions and making 3D fluoroscopytechnically feasible in the clinical scenario.
Another potential advantage of the new system is thelower radiation dose delivered to the patient (approximately20 seconds of standard fluoroscopic time) compared with adose equivalent to 50% of limb CT delivered in othercorresponding systems.21
Although intra-operative 3D fluoroscopes are oftencriticized for their poor image quality, we found it sufficientfor 2 surgeons to detect intra-articular screw prominence. Aprevious study using the same system25 found it was infe-rior to other 3D imaging modalities, such as CT, but suf-ficient for detection of a clinically relevant articularmalreduction in a cadaveric model.
A limitation of the study is the use of a high-contrastgood-quality sawbones as a model that might positivelybias the results compared with an osteoporotic bone with athick soft-tissue envelope that may obscure the bone bor-ders as seen on the image. Improving image quality withnewer image-processing algorithms and better hardwaremay be required to solve this issue. Also, cadaveric studieswith osteoporotic specimens, followed by clinical studies,are needed to validate our preliminary results. However, westress that even with the high-quality bone image, the newerimaging modality improved detection of implant penetra-tion missed by the 2D fluoroscopy.
Also, a limitation of the system is that the operationrequires knowledge of the plastic target position and scan.Future improvement should make it more user-friendly andoperable by common C-arm technicians rather than byspecial operators. In addition, the conventional fluoroscopywas done using 4 static images rather than a ‘‘continuous’’fluoroscopy mode. Thus, theoretically, fewer missed screwswould have been detected. However, even if the lattertechnique is being used in common practice, the rate ofpenetrating implants is still high. Also, for the ease ofimage analysis, the 2D fluoroscopic method had to besimplified for the purpose of image analysis.
Conclusions
Intraoperative 3D fluoroscopic imaging has a promisingpotential for significantly reducing the incidence ofmisplaced implant penetrating into the glenohumeraljoint in ORIF of proximal humeral fractures. Futureclinical studies and improvements in the systems arerequired to support this.
Disclaimer
The authors, their immediate families, and any researchfoundations with which they are affiliated have not
received any financial payments or other benefits fromany commercial entity related to the subject of thisarticle.
References
1. Aaron D, Shatsky J, Paredes JC, Jiang C, Parsons BO, Flatow EL.
Proximal humeral fractures: internal fixation. Instr Course Lect 2013;
62:143-54.
2. Aksu N, Gogus A, Kara AN, Isiklar ZU. Complications encountered in
proximal humerus fractures treated with locking plate fixation. Acta
Orthop Traumatol Turc 2010;44:89-96. http://dx.doi.org/10.3944/
AOTT.2010.2313
3. Atesok K, Finkelstein J, Khoury A, Peyser A, Weil Y, Liebergall M,
Mosheiff R. The use of intraoperative three-dimensional imaging
(ISO-C-3D) in fixation of intraarticular fractures. Injury 2007;38:
1163-9. http://dx.doi.org/10.1016/j.injury.2007.06.014
4. Barzilay Y, Liebergall M, Fridlander A, Knoller N. Miniature robotic
guidance for spine surgery–introduction of a novel system and analysis
of challenges encountered during the clinical development phase at
two spine centres. Int J Med Robot 2006;2:146-53. http://dx.doi.org/
10.1002/rcs.90
5. Bengard MJ, Gardner MJ. Screw depth sounding in proximal humerus
fractures to avoid iatrogenic intra-articular penetration. JOrthopTrauma
2011;25:630-3. http://dx.doi.org/10.1097/BOT.0b013e318206eb65
6. Berkes MB, Little MT, Lorich DG. Open reduction internal fixation of
proximal humerus fractures. Curr Rev Musculoskelet Med 2013;6:47-
56. http://dx.doi.org/10.1007/s12178-012-9150-y
7. Brorson S, Rasmussen JV, Frich LH, Olsen BS, Hrobjartsson A.
Benefits and harms of locking plate osteosynthesis in intraarticular
(OTAType C) fractures of the proximal humerus: a systematic review.
Injury 2012;43:999-1005. http://dx.doi.org/10.1016/j.injury.2011.08.
025
8. Egol KA, Ong CC, Walsh M, Jazrawi LM, Tejwani NC,
Zuckerman JD. Early complications in proximal humerus fractures
(OTATypes 11) treated with locked plates. J Orthop Trauma 2008;22:
159-64. http://dx.doi.org/10.1097/BOT.0b013e318169ef2a
9. Gardner MJ, Weil Y, Barker JU, Kelly BT, Helfet DL, Lorich DG. The
importance of medial support in locked plating of proximal humerus
fractures. J Orthop Trauma 2007;21:185-91. http://dx.doi.org/10.1097/
BOT.0b013e3180333094
10. Geerling J, Kendoff D, Citak M, Zech S, Gardner MJ, Hufner T,
Krettek C, Richter M. Intraoperative 3D imaging in calcaneal fracture
care-clinical implications and decision making. J Trauma 2009;66:
768-73. http://dx.doi.org/10.1097/TA.0b013e31816275c7
11. Giordano V, Gomes AF, Amaral NP, Albuquerque RP, Pires RE.
Preventing surgical complications: A survey on surgeons’ perception
of intra-articular malleolar screw misplacement in a cadaveric study.
Patient Saf Surg 2011;5:24. http://dx.doi.org/10.1186/1754-9493-5-24
12. Gras F, Marintschev I, Klos K, Muckley T, Hofmann GO, Kahler DM.
Screw placement for acetabular fractures: which navigation modality
(2-dimensional vs. 3-dimensional) should be used? An experimental
study. J Orthop Trauma 2012;26:466-73. http://dx.doi.org/10.1097/
BOT.0b013e318234d443
13. Gregory TM, Vandenbussche E, Augereau B. Surgical treatment of
three and four-part proximal humeral fractures. Orthop Traumatol
Surg Res 2013;(1 Suppl):S197-207. http://dx.doi.org/10.1016/j.otsr.
2012.12.006
14. Hernigou P, Germany W. Unrecognized shoulder joint penetration
during fixation of proximal fractures of the humerus. Acta Orthop Scand
2002;73:140-3. http://dx.doi.org/10.1080/000164702753671704

6 Y.A. Weil et al.
15. Jost B, Spross C, Grehn H, Gerber C. Locking plate fixation of frac-
tures of the proximal humerus: analysis of complications, revision
strategies and outcome. J Shoulder Elbow Surg 2013;22:542-9. http://
dx.doi.org/10.1016/j.jse.2012.06.008
16. Kendoff D, Citak M, Gardner MJ, Stubig T, Krettek C, Hufner T. Intra-
operative 3D imaging: value and consequences in 248 cases. J Trauma
2009;66:232-8. http://dx.doi.org/10.1097/TA.0b013e31815ede5d
17. Kettler M, Biberthaler P, Braunstein V, Zeiler C, Kroetz M,
Mutschler W. [Treatment of proximal humeral fractures with the
PHILOS angular stable plate. Presentation of 225 cases of dislocated
fractures]. Unfallchirurg 2006;109:1032-40. http://dx.doi.org/10.1007/
s00113-006-1165-7
18. Lefevre-Colau MM, Babinet A, Fayad F, Fermanian J, Anract P,
Roren A, et al. Immediate mobilization compared with conventional
immobilization for the impacted nonoperatively treated proximal hu-
meral fracture. A randomized controlled trial. J Bone Joint Surg Am
2007;89:2582-90. http://dx.doi.org/10.2106/JBJS.F.01419
19. Lu Y, Wang MY, Zhu YM, Jiang CY. Complications of the locking
plate for displaced proximal humeral fractures. Chin Med J (Engl)
2010;123:2671-5.
20. Owsley KC, Gorczyca JT. Fracture displacement and screw cutout
after open reduction and locked plate fixation of proximal humeral
fractures [corrected]. J Bone Joint Surg Am 2008;90:233-40. http://dx.
doi.org/10.2106/JBJS.F.01351
21. Rock C, Kotsianos D, Linsenmaier U, Fischer T, Brandl R, Vill F,
et al. [Studies on image quality, high contrast resolution and dose
for the axial skeleton and limbs with a new, dedicated CT system
(ISO-C-3 D)]. Rofo 2002;174:170-6. http://dx.doi.org/10.1055/
s-2002-20107
22. Rubberdt A, Feil R, Stengel D, Spranger N, Mutze S, Wich M, et al.
[The clinical use of the ISO-C(3D) imaging system in calcaneus
fracture surgery]. Unfallchirurg 2006;109:112-8. http://dx.doi.org/10.
1007/s00113-005-1015-z
23. Sproul RC, Iyengar JJ, Devcic Z, Feeley BT. A systematic review of
locking plate fixation of proximal humerus fractures. Injury 2011;42:
408-13. http://dx.doi.org/10.1016/j.injury.2010.11.058
24. Takemoto RC, Gage M, Rybak L, Zimmerman I, Egol KA. Accuracy
of detecting screw penetration of the radiocarpal joint following volar
plating using plain radiographs versus computed tomography. Am J
Orthop (Belle Mead NJ) 2012;41:358-61.
25. Weil YA, Liebergall M, Mosheiff R, Singer SB, Joskowicz L,
Khoury A. Assessment of two 3-D fluoroscopic systems for articular
fracture reduction: a cadaver study. Int J Comput Assist Radiol Surg
2011;6:685-92. http://dx.doi.org/10.1007/s11548-011-0548-6