Embed Size (px)
Citation preview

ORIGINAL ARTICLE
USE OF SINGLE MRI AND 18F-FDG PET-CT SCANS IN BOTHDIAGNOSIS AND RADIOTHERAPY TREATMENT PLANNING INPATIENTS WITH HEAD AND NECK CANCER: ADVANTAGE ONTARGET VOLUME AND CRITICAL ORGAN DELINEATION
Miriam Gardner, MD, PhD,1 Philippe Halimi, MD,2 Danielle Valinta, PhD,1
Marie-Madeleine Plantet, MD,3† Jean-Louis Alberini, MD,4 Myriam Wartski, MD,4 Alain Banal, MD,5
Stephane Hans, MD,6 Jean-Louis Floiras, MD,1 Martin Housset, MD,7 Alain Labib, MD1
1 Service de Radiotherapie, Centre Rene Huguenin, Saint-Cloud, France. E-mail: [email protected] Service de Radiologie, Hopital Europeen Georges Pompidou, Paris, France3Radiologie, Centre Rene Huguenin, Saint-Cloud, France4 Service de Medecine Nucleaire, Centre Rene Huguenin, Saint-Cloud, France5ORL, Centre Rene Huguenin, Saint-Cloud, France6ORL, Hopital Europeen Georges Pompidou, Paris, France7Radiotherapie, Hopital Europeen Georges Pompidou, Paris, France
Accepted 1 August 2008Published online 15 December 2008 in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/hed.21005
Abstract: Background. The use of a single MRI and 18F-
fluoro deoxyglucose positron emission tomography-CT (18F-
FDG PET-CT) was evaluated, both in diagnostic procedure
and radiotherapy planning, in patients with head and neck
cancer.
Methods. Thirty-five patients with nasopharyngeal and oro-
pharyngeal tumors were studied. The MRI and 18F-FDG PET-
CT were used for both diagnostic work-up and gross tumor
volume and critical structure delineation. The interobserver var-
iation (IOV) of volumes determined on MRI and CT by a radio-
therapist and by a radiologist were compared as well as their
impact on dose distribution.
Results. The CT-MRI decreased the IOV of parotid glands
in 12 of 35 and target volume in 15 of 35 patients. The use of
18F-FDG PET-CT changed the treatment design in 6 of 21
patients.
Conclusions. Diagnostic imaging performed in the treat-
ment position can improve the accuracy of radiotherapy plan-
ning in case of intracranial tumor extension, heavy dental work,
or contraindication for contrast-enhanced CT, but not in the ab-
sence of these conditions. VVC 2008 Wiley Periodicals, Inc.
Head Neck 31: 461–467, 2009
Keywords: head and neck cancer; 18F-FDG PET-CT; MRI;
radiotherapy treatment planning; interobserver variability
The head and neck contain several criticalstructures close to tumor targets. The use ofconformal radiotherapy (RT) with volume tar-geting of high precision, and even more thetightly conformal doses produced by intensity-modulated radiation therapy (IMRT), makes theaccurate determination of target volume andcritical organs essential.1,2 Furthermore, it was
Correspondence to: M. Gardner
†Deceased.
VVC 2008 Wiley Periodicals, Inc.
Diagnosis and Radiotherapy Treatment Planning HEAD & NECK—DOI 10.1002/hed April 2009 461

established that sparing of the parotids can pre-vent the definite postradiotherapy xerostomia.This makes adequate delineation of the parotidsimportant. CT is commonly used in 3-dimensionalRT planning to outline the gross tumor volume(GTV) and critical organs. It provides superiorspatial accuracy and electron density informationnecessary for dose calculation algorithms. Fur-thermore, it allows more accurate visualization ofbone tumor invasion. However, poor soft-tissuecontrast with this method may make the delinea-tion difficult. The advantage of MRI is superiorsoft-tissue contrast that is necessary for moreprecise delineation of tumor invasion of surround-ing soft tissues, critical structures, and salivaryglands. A disadvantage of MRI lies in its inferiorspatial accuracy. The fusion of CT and MRI scansmay be useful in treatment planning, as the com-plementary information contained in the 2 modal-ities can provide more accurate definition of bothtumor and normal tissues.3–5
However, in some cases, neither CT nor MRIallow the detection of the pathological characterof lymph nodes having some but not all charac-teristics of tumor involvement. In the past 2 deca-des, radiation oncologists have increasingly beenincorporating functional imaging combined withstructural imaging—18F-fluoro deoxyglucose posi-tron emission tomography-CT (18F-FDG PET-CT)into their treatment planning. The advantage ofusing 18F-FDG PET-CT for RT planning waswell established, particularly in lung cancer,6,7
and there is increasing evidence for the use of18F-FDG PET-CT in management of patientswith head and neck cancer.8–10
CT, MRI, and 18F-FDG PET are widely used inthe diagnostic work-up of patients with head andneck cancer. They are part of routine staging proce-dure in our institution. In order to achieve the mostappropriate RT treatment planning for patients nottreated surgically, withoutmultiplying the examina-tions, we decided to perform all 3 examinations insuch a way that they can be used for both the diag-nostic procedure and treatment planning.
To establish the usefulness of this approach, wecompared parotid glands, chiasma, and GTV asdetermined on CTandMRI by 2 different operators,and evaluated whether the use of 18F-FDG PET-CThas changed the treatment planning volumes.
PATIENTS AND METHODS
The indication for definitive RT, with or withoutconcurrent chemotherapy, was agreed with head
and neck specialists. Patients refusing the sug-gested surgery but accepting the RT treatmentwere also included.
Patients selected by head and neck specialistsafter clinical examination, and for which thediagnostic imagery (particularly MRI and 18F-FDG PET-CT) had not been performed, weresent to the Radiotherapy Department for fabrica-tion of the custom-designed thermoplastic mask.
In the period from 2003 to 2007, we usedMRI-CT scan-fused images, both in diagnosisand treatment planning of 35 patients withhead and neck cancer (27 men and 8 women).Stages II–IV of nasopharyngeal and oropharyn-geal carcinomas were included. The median agewas 59 years (range, 39–68). There were 7 caseswith undifferentiated nasopharyngeal carcinomaand 28 with squamous cell oropharyngeal carci-nomas. All nonmetastatic patients received con-current chemoradiotherapy. IMRT was used in15 patients, and conformal RT in 20 patients.
The MRI, CT, and 18F-FDG PET-CT wereperformed in the treatment position. The treat-ment planning CT scans (Siemens SomatomEmotion, Forsheim, Germany) in serial 3-mmslices were taken from vertex to 3 cm below theclavicle.
In the first 14 patients, MRI (GE SignaExcite 1.5 Tesla) was performed in the treat-ment position without the thermoplastic mask.The treatment head position was achieved byusing laser devices, external marking performedduring the confectioning of thermoplastic mask,and temporary head-fixing devices. In 21 more-recently treated patients, the MRI acquisitionwas performed with the thermoplastic mask inplace. MRI included precontrast axial T1- andT2-weighted scans followed by T1-, T2-weightedgadolinium-enhanced images and T2 fat satvolumetric sequence. For the MRI-CT fusion,the most appropriate sequence was chosen bythe radiologist. The images were transferred tothe Radiotherapy Department for furtherutilization.
Image fusion of MRI and CT images was per-formed using the GR Advantage program ver-sion 4.0 or CORVUS version 5.0. The fusionprecision was verified both internally by thefusion program and visually by delineation ofanatomical structures easily identified both onthe CT and MRI. The fusion was accepted if theerror was less than 2 mm in all directions.
18F-FDG PET-scanning was performed in21 more-recently treated patients using 2
462 Diagnosis and Radiotherapy Treatment Planning HEAD & NECK—DOI 10.1002/hed April 2009

acquisitions: the whole body 18F-FDG PET-CTexcluding the lower extremities, to search fordistant metastases or a second tumor, anddetailed acquisition in serial 3-mm slices tar-geting the head and neck, performed in thetreatment position with the mask. Both acquis-itions were performed within the same session.
A combined 18F-FDG PET-CT system wasused (Discovery LS, GEMS, Waukesha, WI).Patients were asked to fast for at least 6 hoursbefore imaging. 18F-FDG PET was performed60 to 90 minutes after IV injection of 220-MBqof 18F-FDG. Data were analyzed by visualinterpretation of coronal, sagittal, and trans-verse slices on a workstation with viewing-dedi-cated software (eNTEGRA; ELGEMS, Haifa,Israel).
The comparison of GTV, chiasma, and sali-vary glands was performed for the purpose ofthe study. They were delineated on transversesections of CT and then at least 3 days later onMRI separately by a head and neck–specializedradiotherapist and by a radiologist. The differ-ence of each volume determined by a radiothera-pist and radiologist on CT and MRI wascalculated for every patient. Student paired ttest was used to compare the differences foreach imaging modality.
For treatment planning purposes, volumeswere delineated by a head and neck–specializedradiotherapist and reviewed by a head andneck–specialized radiologist on fused CT-MRIimages,11 taking into account 18F-FDG PET-CTimages.
RESULTS
Parotid Glands. The interobserver variation(IOV) of volumes of parotid glands and targetvolume determined by a radiotherapist andradiologist was significantly smaller if the delin-eation was done on MRI rather than CT slices.
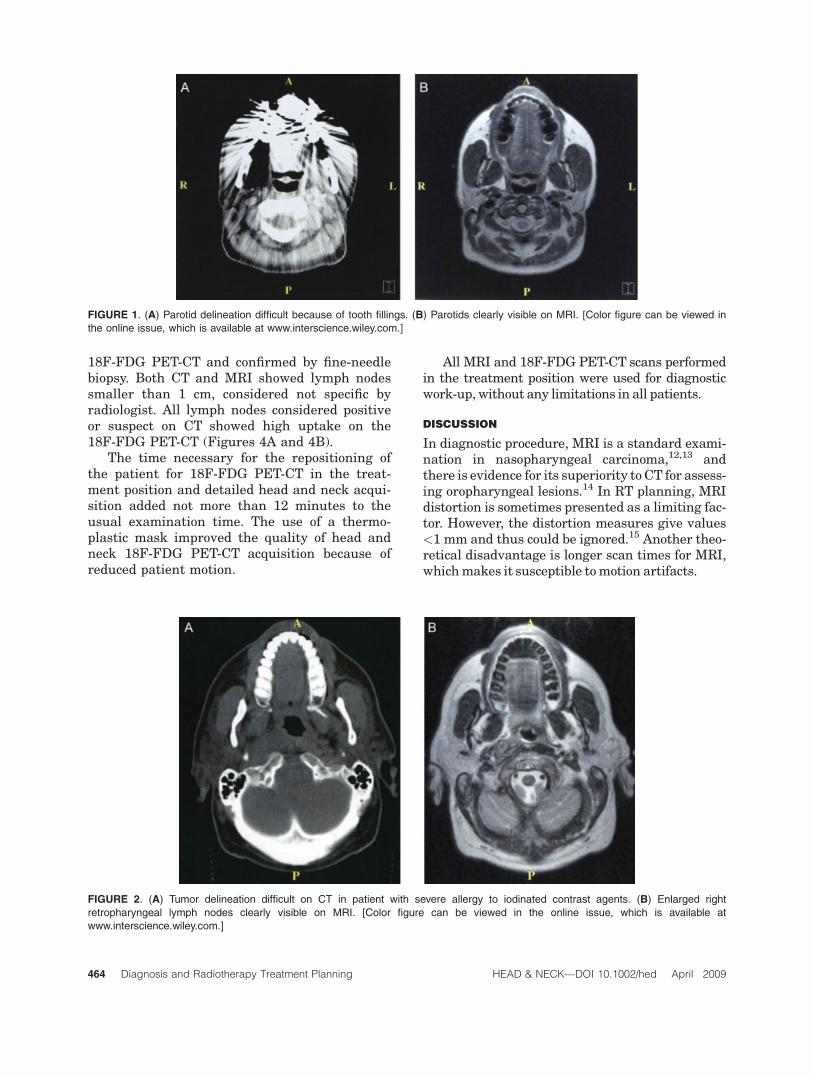
For parotid glands, the mean CT volume was18.2 mL, and the mean CT IOV (CT IOV) repre-sented 23.1% of the mean parotid volume. Themean IRM volume was 24.5 mL, and the meanMRI IOV (MRI IOV) represented 13.4% of themean parotid volume. Therefore, the CT IOVwas significantly higher than MRI IOV (p <.0001). The CT IOV was high in 10 patients,with heavy dental work making delineation onCT scan arbitrary (Figures 1A and 1B); mean
CT IOV, 39.1% of the mean parotid volume;mean MRI IOV, 15.3% of the mean parotid vol-ume (p < .000001). There was no significantIOV for patients without interference on CT—mean CT IOV 17.7%, comparing to the meanMRI IOV of 13.4% (p ¼ .76).
The differences in delineation influenced themean parotid dose—24.1 Gy for CT parotid vol-ume and 29.4 Gy to MRI volume.
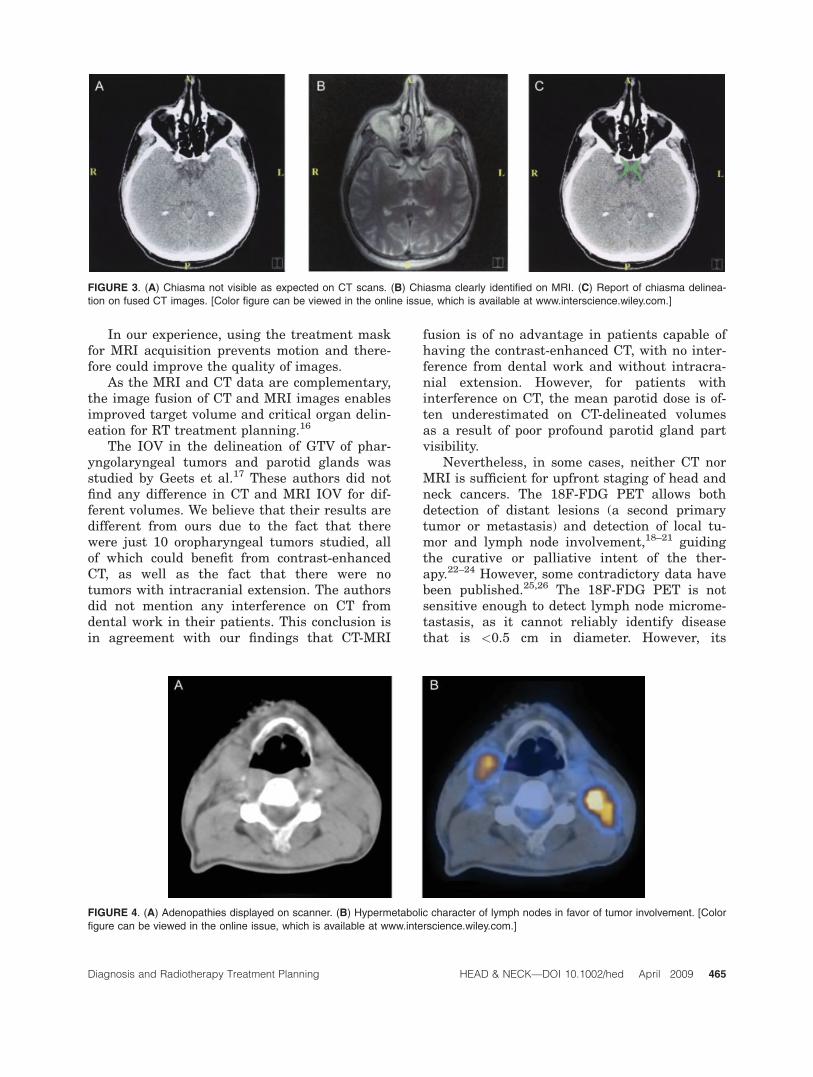
Gross Tumor Volume. For GTV, the CT IOV wasagain higher (mean, 4.22 mL) than the MRIIOV (mean, 3.28 mL; p < .0007). The CT IOVwas clearly higher in 15 patients (12 with CTdifficult to interpret—10 patients with heavydental work and 2 patients with contraindica-tion for contrast enhanced CT [Figures 2A and2B]—and 3 patients with intracranial extension;mean CT IOV, 8.38 mL, mean MRI IOV, 2.59mL; p < .000001). Out of 15 patients with highCT IOV, in 10 patients, 7.3% to 10.1% of PTV asdetermined on MRI would not be covered by the95% isodose line if the planning had been basedon CT PTV (median, 8.9%).
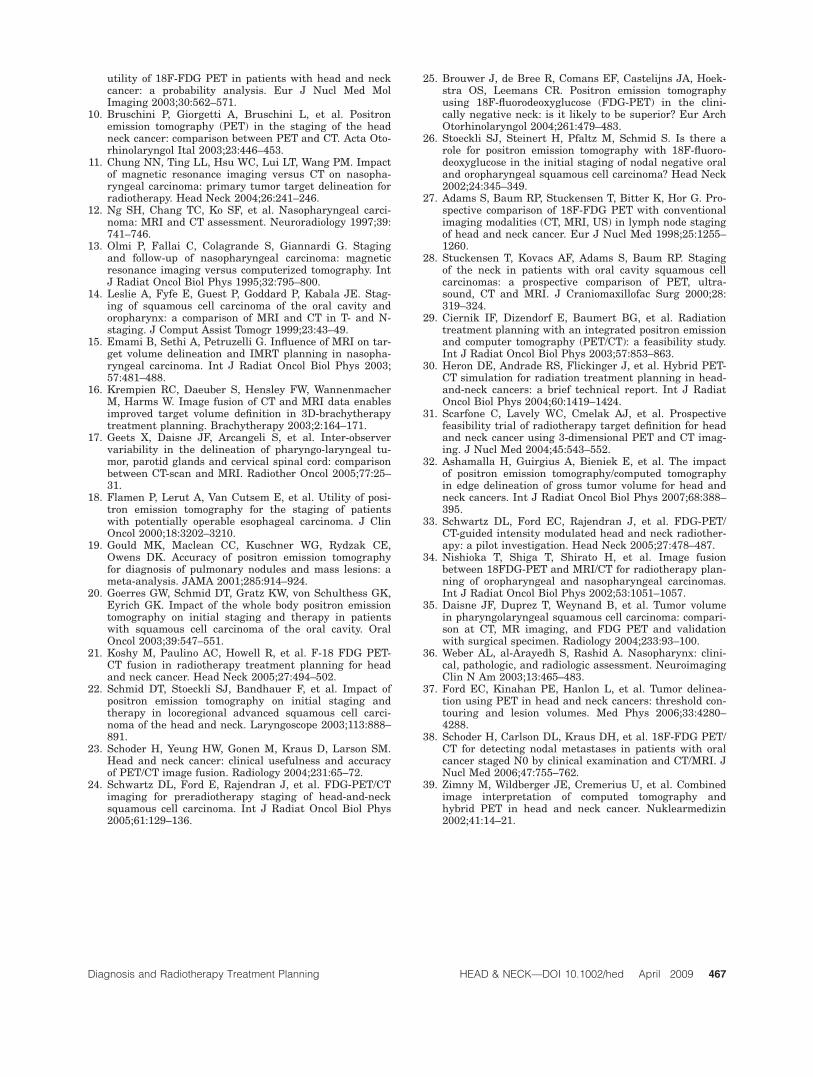
Chiasma. The chiasma, as expected, was notvisible on CT scans of any patient, makingdelineation on CT scan arbitrary, but it wasclearly identifiable on MRI. The precise delinea-tion of the chiasma was particularly importantin 7 patients treated for nasopharyngeal carci-noma (Figures 3A–3C).
CT-MRI Fusion. The MRI performed in thetreatment position was of sufficiently highquality to permit its use in both diagnosticwork-up and treatment planning in all 35patients. In all cases, a good quality CT-MRIimage fusion was achieved. The repositioningof the patient to perform the MRI in the treat-ment position did not add more than 5 minutesin any case.
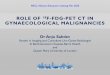
18F-FDG PET-CT. The use of 18F-FDG PET-CTchanged the treatment design in 6 of 21patients. In 2 patients, 18F-FDG PET-CT indi-cated intrathoracic metastasis, subsequentlyproved histologically, and they were switched topalliative treatment. In another patient, 18F-FDG PET-CT showed extension to the skull basewhich was not initially detected by other imagemodalities but was confirmed by bone CT. Infurther 3 patients, bilateral rather than unilat-eral lymph node extension was detected by
Diagnosis and Radiotherapy Treatment Planning HEAD & NECK—DOI 10.1002/hed April 2009 463
18F-FDG PET-CT and confirmed by fine-needlebiopsy. Both CT and MRI showed lymph nodessmaller than 1 cm, considered not specific byradiologist. All lymph nodes considered positiveor suspect on CT showed high uptake on the18F-FDG PET-CT (Figures 4A and 4B).
The time necessary for the repositioning ofthe patient for 18F-FDG PET-CT in the treat-ment position and detailed head and neck acqui-sition added not more than 12 minutes to theusual examination time. The use of a thermo-plastic mask improved the quality of head andneck 18F-FDG PET-CT acquisition because ofreduced patient motion.
All MRI and 18F-FDG PET-CT scans performedin the treatment position were used for diagnosticwork-up,without any limitations in all patients.
DISCUSSION
In diagnostic procedure, MRI is a standard exami-nation in nasopharyngeal carcinoma,12,13 andthere is evidence for its superiority toCT for assess-ing oropharyngeal lesions.14 In RT planning, MRIdistortion is sometimes presented as a limiting fac-tor. However, the distortion measures give values<1 mm and thus could be ignored.15 Another theo-retical disadvantage is longer scan times for MRI,whichmakes it susceptible tomotion artifacts.
FIGURE 1. (A) Parotid delineation difficult because of tooth fillings. (B) Parotids clearly visible on MRI. [Color figure can be viewed in
the online issue, which is available at www.interscience.wiley.com.]
FIGURE 2. (A) Tumor delineation difficult on CT in patient with severe allergy to iodinated contrast agents. (B) Enlarged right
retropharyngeal lymph nodes clearly visible on MRI. [Color figure can be viewed in the online issue, which is available at
www.interscience.wiley.com.]
464 Diagnosis and Radiotherapy Treatment Planning HEAD & NECK—DOI 10.1002/hed April 2009
In our experience, using the treatment maskfor MRI acquisition prevents motion and there-fore could improve the quality of images.
As the MRI and CT data are complementary,the image fusion of CT and MRI images enablesimproved target volume and critical organ delin-eation for RT treatment planning.16
The IOV in the delineation of GTV of phar-yngolaryngeal tumors and parotid glands wasstudied by Geets et al.17 These authors did notfind any difference in CT and MRI IOV for dif-ferent volumes. We believe that their results aredifferent from ours due to the fact that therewere just 10 oropharyngeal tumors studied, allof which could benefit from contrast-enhancedCT, as well as the fact that there were notumors with intracranial extension. The authorsdid not mention any interference on CT fromdental work in their patients. This conclusion isin agreement with our findings that CT-MRI
fusion is of no advantage in patients capable ofhaving the contrast-enhanced CT, with no inter-ference from dental work and without intracra-nial extension. However, for patients withinterference on CT, the mean parotid dose is of-ten underestimated on CT-delineated volumesas a result of poor profound parotid gland partvisibility.
Nevertheless, in some cases, neither CT norMRI is sufficient for upfront staging of head andneck cancers. The 18F-FDG PET allows bothdetection of distant lesions (a second primarytumor or metastasis) and detection of local tu-mor and lymph node involvement,18–21 guidingthe curative or palliative intent of the ther-apy.22–24 However, some contradictory data havebeen published.25,26 The 18F-FDG PET is notsensitive enough to detect lymph node microme-tastasis, as it cannot reliably identify diseasethat is <0.5 cm in diameter. However, its
FIGURE 4. (A) Adenopathies displayed on scanner. (B) Hypermetabolic character of lymph nodes in favor of tumor involvement. [Color
figure can be viewed in the online issue, which is available at www.interscience.wiley.com.]
FIGURE 3. (A) Chiasma not visible as expected on CT scans. (B) Chiasma clearly identified on MRI. (C) Report of chiasma delinea-
tion on fused CT images. [Color figure can be viewed in the online issue, which is available at www.interscience.wiley.com.]
Diagnosis and Radiotherapy Treatment Planning HEAD & NECK—DOI 10.1002/hed April 2009 465

sensitivity and specificity in detecting lymphnode involvement is still superior to other im-agery modalities.27,28
Hybrid 18F-FDG PET-CT radiation simula-tion in head and neck cancer was shown to resultin more effective target determination.29–31
Furthermore, the use of 18F-FDG PET-CT hasthe potential of reducing the equivocal targetdesign variability between different cliniciansand also has the potential of improving nodalstaging for imagery experts and nonexpertsalike.32 The 18F-FDG PET appears to detectmore accurately tumor bearing tissue comparedwith CT24 and therefore seems be useful in deter-mining volumes for IMRT.33
Each modality (CT, MRI, and 18F-FDG PET)adds complementary information, and theircombined use gives the most complete informa-tion regarding tumor extension presentlyachievable without a surgical procedure.
To our knowledge, there is just 1 study pub-lished using MRI, 18F-FDG PET-CT, and CT incombination in head and neck RT planning.34
However, the imaging procedures were per-formed specifically for the planning.
Another study comparing tumor volumes asdetermined by CT, MRI, and 18F-FDG PETwith the surgical specimen found the 18F-FDGPET to be the most accurate modality.35
Performing the same examinations sepa-rately for diagnostic and then for RT treatmentplanning requires repeated examinations, andso we investigated the possibility of using thesame examinations for both purposes.
In our experience, neither the use of a ther-moplastic mask nor performing MRI or 18F-FDG PET-CT in the treatment position can leadto any deterioration in the quality of imageryand allowed their use for diagnostic purposesand staging without any constraints.
In our experience, the use of CT-MRI fusedimages in treatment planning proved to be use-ful for diminishing the IOV in delineation ofGTV in patients with intracranial tumor exten-sion, in patients with contraindication for con-trast-enhanced CT, and in patients with heavydental work interfering with delineation of tar-get volumes and parotid glands on CT. Further-more, it allows more precise delineation of thechiasma in patients treated for nasopharyngealcarcinoma, as the chiasma is difficult to be seenon CT even if thin slice thickness is used.
In our limited number of patients, the 18F-FDG PET-CT proved to be helpful for metastasis
detection and detection of lymph node extension,and is therefore useful for more accurate treat-ment design.
The aim of the study was not to determinethe place of MRI or 18F-FDG PET or both inupfront staging of head and neck cancers. Sev-eral studies have discussed the matter.36–39
Most of them were in favor of the use of thesemodalities in pretreatment work-up, althoughsome of them failed to prove an advantage. Nostudy was published showing a negative impactof the use of these imaging modalities on patientmanagement.
Our experience shows that diagnostic imag-ing, if performed in treatment position, can beused to improve the accuracy of RT planningand should be considered in patients with intra-cranial tumor extension, heavy dental work, orcontraindication for contrast-enhanced CT. Nobenefit was found if none of these aforemen-tioned conditions was present.
REFERENCES
1. Lee N, Xia P, Fischbein NJ, Akazawa P, Akazawa C,Quivey JM. Intensity-modulated radiation therapy forhead-and-neck cancer: the UCSF experience focusing ontarget volume delineation. Int J Radiat Oncol Biol Phys2003;57:49–60.
2. Eisbruch A, Foote RL, O’Sullivan B, Beitler JJ, VikramB. Intensity-modulated radiation therapy for head andneck cancer: emphasis on the selection and delineationof the targets. Semin Radiat Oncol 2002;12:238–249.
3. Khoo VS, Dearnaley DP, Finnigan DJ, Padhani A, Tan-ner SF, Leach MO. Magnetic resonance imaging (MRI):considerations and applications in radiotherapy treat-ment planning. Radiother Oncol 1997;42:1–15.
4. Yanke BR, Ten Haken RK, Aisen A, Fraass BA, Thorn-ton AF Jr. Design of MRI scan protocols for use in 3-D,CT based treatment planning. Med Dosim 1991;16:205–211.
5. Ten Haken RK, Thornton AF, Sandler HM, et al. Aquantitative assessment of the addition of MRI to CTbased 3-D treatment planning of brain tumors. Radio-ther Oncol 1992;25:121–133.
6. Vanuytsel LJ, Vansteenkiste JF, Stroobants SG, et al.The impact of (18)F-fluoro-2-deoxy-D-glucose positronemission tomography (FDG-PET) lymph node staging onthe radiation treatment volumes in patients with non-small cell lung cancer. Int J Radiat Oncol Biol Phys2000;55:317–324.
7. Nestle U, Walter K, Schmidt S, et al. 18F-Deoxyglucosepositron emission tomography (FDG-PET) for the plan-ning of radiotherapy in lung cancer: high impact inpatients with atelectasis. Int J Radiat Oncol Biol Phys1999;44:593–597.
8. Hannah A, Scott AM, Tochon-Danguy H, et al. Evalua-tion of 18F-fluorodeoxyglucose positron emission tomog-raphy and computed tomography with histolopathologiccorrelation in the initial staging of head and neck cancer.Ann Surg 2002;236:208–217.
9. Goerres GW, Mosna-Firlejczyk K, Steurer J, vonSchulthess GK, Bachmann LM. Assessment of clinical
466 Diagnosis and Radiotherapy Treatment Planning HEAD & NECK—DOI 10.1002/hed April 2009
utility of 18F-FDG PET in patients with head and neckcancer: a probability analysis. Eur J Nucl Med MolImaging 2003;30:562–571.
10. Bruschini P, Giorgetti A, Bruschini L, et al. Positronemission tomography (PET) in the staging of the headneck cancer: comparison between PET and CT. Acta Oto-rhinolaryngol Ital 2003;23:446–453.
11. Chung NN, Ting LL, Hsu WC, Lui LT, Wang PM. Impactof magnetic resonance imaging versus CT on nasopha-ryngeal carcinoma: primary tumor target delineation forradiotherapy. Head Neck 2004;26:241–246.
12. Ng SH, Chang TC, Ko SF, et al. Nasopharyngeal carci-noma: MRI and CT assessment. Neuroradiology 1997;39:741–746.
13. Olmi P, Fallai C, Colagrande S, Giannardi G. Stagingand follow-up of nasopharyngeal carcinoma: magneticresonance imaging versus computerized tomography. IntJ Radiat Oncol Biol Phys 1995;32:795–800.
14. Leslie A, Fyfe E, Guest P, Goddard P, Kabala JE. Stag-ing of squamous cell carcinoma of the oral cavity andoropharynx: a comparison of MRI and CT in T- and N-staging. J Comput Assist Tomogr 1999;23:43–49.
15. Emami B, Sethi A, Petruzelli G. Influence of MRI on tar-get volume delineation and IMRT planning in nasopha-ryngeal carcinoma. Int J Radiat Oncol Biol Phys 2003;57:481–488.
16. Krempien RC, Daeuber S, Hensley FW, WannenmacherM, Harms W. Image fusion of CT and MRI data enablesimproved target volume definition in 3D-brachytherapytreatment planning. Brachytherapy 2003;2:164–171.
17. Geets X, Daisne JF, Arcangeli S, et al. Inter-observervariability in the delineation of pharyngo-laryngeal tu-mor, parotid glands and cervical spinal cord: comparisonbetween CT-scan and MRI. Radiother Oncol 2005;77:25–31.
18. Flamen P, Lerut A, Van Cutsem E, et al. Utility of posi-tron emission tomography for the staging of patientswith potentially operable esophageal carcinoma. J ClinOncol 2000;18:3202–3210.
19. Gould MK, Maclean CC, Kuschner WG, Rydzak CE,Owens DK. Accuracy of positron emission tomographyfor diagnosis of pulmonary nodules and mass lesions: ameta-analysis. JAMA 2001;285:914–924.
20. Goerres GW, Schmid DT, Gratz KW, von Schulthess GK,Eyrich GK. Impact of the whole body positron emissiontomography on initial staging and therapy in patientswith squamous cell carcinoma of the oral cavity. OralOncol 2003;39:547–551.
21. Koshy M, Paulino AC, Howell R, et al. F-18 FDG PET-CT fusion in radiotherapy treatment planning for headand neck cancer. Head Neck 2005;27:494–502.
22. Schmid DT, Stoeckli SJ, Bandhauer F, et al. Impact ofpositron emission tomography on initial staging andtherapy in locoregional advanced squamous cell carci-noma of the head and neck. Laryngoscope 2003;113:888–891.
23. Schoder H, Yeung HW, Gonen M, Kraus D, Larson SM.Head and neck cancer: clinical usefulness and accuracyof PET/CT image fusion. Radiology 2004;231:65–72.
24. Schwartz DL, Ford E, Rajendran J, et al. FDG-PET/CTimaging for preradiotherapy staging of head-and-necksquamous cell carcinoma. Int J Radiat Oncol Biol Phys2005;61:129–136.
25. Brouwer J, de Bree R, Comans EF, Castelijns JA, Hoek-stra OS, Leemans CR. Positron emission tomographyusing 18F-fluorodeoxyglucose (FDG-PET) in the clini-cally negative neck: is it likely to be superior? Eur ArchOtorhinolaryngol 2004;261:479–483.
26. Stoeckli SJ, Steinert H, Pfaltz M, Schmid S. Is there arole for positron emission tomography with 18F-fluoro-deoxyglucose in the initial staging of nodal negative oraland oropharyngeal squamous cell carcinoma? Head Neck2002;24:345–349.
27. Adams S, Baum RP, Stuckensen T, Bitter K, Hor G. Pro-spective comparison of 18F-FDG PET with conventionalimaging modalities (CT, MRI, US) in lymph node stagingof head and neck cancer. Eur J Nucl Med 1998;25:1255–1260.
28. Stuckensen T, Kovacs AF, Adams S, Baum RP. Stagingof the neck in patients with oral cavity squamous cellcarcinomas: a prospective comparison of PET, ultra-sound, CT and MRI. J Craniomaxillofac Surg 2000;28:319–324.
29. Ciernik IF, Dizendorf E, Baumert BG, et al. Radiationtreatment planning with an integrated positron emissionand computer tomography (PET/CT): a feasibility study.Int J Radiat Oncol Biol Phys 2003;57:853–863.
30. Heron DE, Andrade RS, Flickinger J, et al. Hybrid PET-CT simulation for radiation treatment planning in head-and-neck cancers: a brief technical report. Int J RadiatOncol Biol Phys 2004;60:1419–1424.
31. Scarfone C, Lavely WC, Cmelak AJ, et al. Prospectivefeasibility trial of radiotherapy target definition for headand neck cancer using 3-dimensional PET and CT imag-ing. J Nucl Med 2004;45:543–552.
32. Ashamalla H, Guirgius A, Bieniek E, et al. The impactof positron emission tomography/computed tomographyin edge delineation of gross tumor volume for head andneck cancers. Int J Radiat Oncol Biol Phys 2007;68:388–395.
33. Schwartz DL, Ford EC, Rajendran J, et al. FDG-PET/CT-guided intensity modulated head and neck radiother-apy: a pilot investigation. Head Neck 2005;27:478–487.
34. Nishioka T, Shiga T, Shirato H, et al. Image fusionbetween 18FDG-PET and MRI/CT for radiotherapy plan-ning of oropharyngeal and nasopharyngeal carcinomas.Int J Radiat Oncol Biol Phys 2002;53:1051–1057.
35. Daisne JF, Duprez T, Weynand B, et al. Tumor volumein pharyngolaryngeal squamous cell carcinoma: compari-son at CT, MR imaging, and FDG PET and validationwith surgical specimen. Radiology 2004;233:93–100.
36. Weber AL, al-Arayedh S, Rashid A. Nasopharynx: clini-cal, pathologic, and radiologic assessment. NeuroimagingClin N Am 2003;13:465–483.
37. Ford EC, Kinahan PE, Hanlon L, et al. Tumor delinea-tion using PET in head and neck cancers: threshold con-touring and lesion volumes. Med Phys 2006;33:4280–4288.
38. Schoder H, Carlson DL, Kraus DH, et al. 18F-FDG PET/CT for detecting nodal metastases in patients with oralcancer staged N0 by clinical examination and CT/MRI. JNucl Med 2006;47:755–762.
39. Zimny M, Wildberger JE, Cremerius U, et al. Combinedimage interpretation of computed tomography andhybrid PET in head and neck cancer. Nuklearmedizin2002;41:14–21.
Diagnosis and Radiotherapy Treatment Planning HEAD & NECK—DOI 10.1002/hed April 2009 467
![Radiomics analysis of pre-treatment [18F]FDG PET/CT for patients … · 2018. 10. 26. · ORIGINAL ARTICLE Radiomics analysis of pre-treatment [18F]FDG PET/CT for patientswith metastatic](https://img.pdfslide.us/doc/110x75/5fcdb0e68fed49190433314d/radiomics-analysis-of-pre-treatment-18ffdg-petct-for-patients-2018-10-26.jpg)
![QUANTIFICATION OF DYNAMIC [18F]FDG PET …10.1007/s11307...QUANTIFICATION OF DYNAMIC [18F]FDG PET STUDIES IN ACUTE LUNG INJURY Journal: Molecular Imaging and Biology Elisabetta Grecchi1,6,](https://img.pdfslide.us/doc/110x75/5aa9f1017f8b9a6c188d9646/quantification-of-dynamic-18ffdg-pet-101007s11307quantification-of-dynamic.jpg)
![Dynamische, kontrastverstärkte Computertomographie und ... · radioaktiv markierten 18F-Fluordesoxy-Glukose (18F-FDG), den Tumormetabolismus darstellen kann [18]. Es konnte in Studien](https://img.pdfslide.us/doc/110x75/5eab9568f429722d7b6b2910/dynamische-kontrastverstrkte-computertomographie-und-radioaktiv-markierten.jpg)

![Pulmonary 18F-FDG uptake helps refine current risk ... · self-propagating scar formation and end-stage fibrosis [10]. 18F-FDG uptake by tissues is a marker of glucose utilization,](https://img.pdfslide.us/doc/110x75/6035c829b976e577c9150e6c/pulmonary-18f-fdg-uptake-helps-refine-current-risk-self-propagating-scar-formation.jpg)















![Pharmacokinetic modeling of [18F]fluorodeoxyglucose (FDG](https://img.pdfslide.us/doc/110x75/61886b54df681277ae16a602/pharmacokinetic-modeling-of-18ffluorodeoxyglucose-fdg-.jpg)
![Regional, kinetic [18F]FDG PET imaging of a unilateral Parkinsonian animal model](https://img.pdfslide.us/doc/110x75/56d6c0051a28ab3016989e06/regional-kinetic-18ffdg-pet-imaging-of-a-unilateral-parkinsonian-animal.jpg)






