Embed Size (px)
Citation preview

Use of new FDA-approved Assay for improved detection of Bordetella pertussis and Bordetella parapertussis leading to improved turn around time in diagnosis.
BACKGROUND• Pertussis is a contagious, prolonged respiratory illness caused by the Gram-negative bacterium Bordetella
pertussis.• Despite high childhood vaccination rates1,2, pertussis is one of the most poorly controlled bacterial
vaccine-preventable diseases in the United States. 3• While culture is considered the “gold standard” diagnostic test, it may take up to 2 weeks to return, has
very low sensitivity, with estimates ranging from 12%-60%.4,5
• Real-time PCR (RT-PCR) allows for rapid diagnosis.• For the past decade Montefiore Medical Center which includes Children’s Hospital at Montefiore
(CHAM) has used a high complexity in-house laboratory developed PCR test to detect Pertussis PCR which takes 1-5 days to report results due to:
• Internal control failure contributing to indeterminate results, with subsequent need for repeat testing on samples
• Testing only on weekdays due to high complexity assay requiring specially trained staff
AIMS• To validate and implement a new FDA-approved pertussis PCR for the detection of B. pertussis and B.
parapertussis.• To reduce the reporting time in the detection of B. pertussis or B. parapertussis to 1 day in the Microbiology
lab between Jan 1 2019 to April 30 2019.
• We evaluated the performance of the Diasorin Simplexa Bordetella Direct™, a CLIA moderate complexity PCR assay in comparison to our high complexity, in-house laboratory developed test (LDT) with Cepheid reagents.
• One hundred and five nasopharyngeal swab clinical specimens from 2007-2018 were tested. This included 74 previous positives and 31 previous negatives.
• Limit of detection was determined by preparing a 0.5 McFarland solutions of combined Bpp and Bpisolates in either saline or VTM followed by 1:10 dilutions. The specimens were then serially diluted 6 times to test for limit of detection. Additionally, reproducibility was measured over 3 days.
DISCUSSION• Improved internal controls, leading to 0 indeterminate test results• No need to repeat PCR assay contributing to delayed reporting to
clinicians• No longer a need for multiple rooms used for reagent preparation• Nearly 100% of samples took less than a day to report after
implementation of the FDA-approved assay.
METHODS
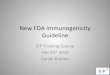
RESULTS/TABLES/FIGURESTable 1: Validation of Viral Transport Media (VTM) Figure 1: Diasorin Simplexa Bordatella Direct™ PCR Assay Results
REFERENCES1. Seither R, Masalovich S, Knighton CL, Mellerson J, Singleton JA, Greby SM. Vaccination coverage among children in kindergarten—United
States, 2013–2014 school year. MMWR. 2014;63(41):913–20. 2. Elam-Evans LD, Yankey D, Singleton JA, Kolasa M. National, state, and selected local area vaccination coverage among children aged 19–35
months—United States, 2013. MMWR. 2014;63(34):741–8. 3. CDC. Preventing tetanus, diptheria, and pertussis among adolescents: Use of tetanus toxoid, reduced diptheria toxoid, and acellular pertussis
vaccines: Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR. 2006;55(No. RR-3):1–46.4. CDC. Summary of notifiable diseases—United States, 2012. MMWR. 2014;61(53):1–124. 5. Lee AD, Cassiday PK, Pawloski LC, et al. Clinical evaluation and validation of laboratory methods for the diagnosis of Bordetella pertussis
infection: Culture, polymerase chain reaction (PCR) and anti-pertussis toxin IgG serology (IgG-PT). PLoS One. 2018;13(4):e0195979.
CONCLUSIONS
ABSTRACTPrompt and accurate diagnosis of pertussis is essential to curtail the spread of disease. We evaluated the the performance of the Diasorin Simplexa Bordatella Direct™, a CLIA moderate complexity PCR assay in comparison to our high complexity, in-house laboratory developed test (LDT) with Cepheid reagents. The Simplexa assay uses the LIAISON® MDX instrument for the qualitative detection and differentiation of Bordatella pertussis (Bp) and Bordatella parapertussis (Bpp) nucleic acids (IS 481 and IS 1001 respectively).
One hundred and five nasopharyngeal swab clinical specimens stored at (-20° C) in normal saline from 2007-2018 were tested. This included 74 previous positives and 31 previous negatives. 72/74 previously tested Bppositive samples were positive with the Diasorin assay (2 false negatives (FN)) and 29/31 previously tested negative Bp samples were negative (2 false positives (FP)). Diasorin FN specimens were retested with the Cepheid assay and were negative on retest. Additionally the original positives were relatively weak (Cts 32 and 34, positive < 35) and were from 2012 and 2013. The Diasorin FP specimens were from 11 week old and 14 month infants, both having clinical findings of pertussis. No further testing was done on the FP samples. Control samples (7 Bp and Bpp positive, 1 Bp positive, and 3 Bpp positive) were all positive with the Diasorinassay. The Diasorin assay limit of detection in viral transport medium for Bp and Bpp was approximately 10 cfu/mL. The assay was reproducible over 3 days at 3 dilutions.
The positive percent agreement for the Diasorin assay for qualitative detection of Bp in patient samples was (97%) and the negative percent agreement was (93%) indicating excellent agreement with our LDT (Kappa coeeficient 0.908 (95% CI; 0.82-0.99). Due to small number of specimens for Bpp the percent agreement was not determined, although all known specimens were detected.
This new FDA-approved assay is reproducible, exhibits a low limit of detection, is simple to run, and provides an easier format compared to the in-house LDT. Additional large scale, prospective study is indicated to confirm our results.
Jyotsna Bhattacharya, MD1, David Goldman, MD1, Stacia Semple, MD2, Shaomin Hu, MD-PhD2, Wendy A. Szymczak, PhD2, Michael H. Levi, ScD2
1. Pediatric Infectious Disease, Montefiore/Albert Einstein College of Medicine, New York, NY, United States.
2. Department of Pathology, Montefiore/Albert Einstein College of Medicine, Bronx, NY, United States.
Concentration(CFU/ml)
IS481 IS1001 Internal Control Interpretation
106 Detected Detected Valid Bp and Bpp detected105 Detected Detected Valid Bp and Bpp detected104 Detected Detected Valid Bp and Bpp detected103 Detected Detected Valid Bp and Bpp detected102 Detected Detected Valid Bp and Bpp detected101 Detected Detected Valid Bp and Bpp detected0 Not Detected Not Detected Valid Negative
BLANK Not Detected Not Detected Valid Negative
Concentration(CFU/ml) IS481 IS1001 Internal Control INTERPRETATION
RUN 1103 Detected Detected Valid Bp and Bpp detected
102 Detected Detected Valid Bp and Bpp detected
101 Detected Detected Valid Bp and Bpp detected
IS481 IS1001 Internal Control INTERPRETATION
RUN 2103 Detected Detected Valid Bp and Bpp detected
102 Detected Detected Valid Bp and Bpp detected
101 Detected Detected Valid Bp and Bpp detected
IS481 IS1001 Internal Control INTERPRETATION
RUN 3
103 Detected Detected Valid Bp and Bpp detected
102 Detected Detected Valid Bp and Bpp detected101 Detected Detected Valid Bp and Bpp detected
The 2 Diasorin false negative specimens were retested with the Cepheid assay and were negative on retest. Furthermore, the original positives were relatively weak (Cts32 and 34, positive < 35) and were from 2012 and 2013. The 2 Diasorin false positive specimens were from 11 week old and 14 month infants, both having clinical findings of pertussis. No further testing was performed on these samples.
72
29
2
2
Positives (n=74) Negatives (n=31)
False Negatives
False Positives
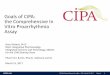
Figure 2: % Patients with >1 day of reporting turnaround time
(n=38)
n=30
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
Jan 1-Apr 30 2018 Jan 1-Apr 30 2019
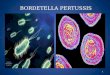
Performed on a Weekend7/15(47%)
Internal Control lssue
8/15(53%)
Figure 3: Factors contributing to patients with >1 day of reporting turnaround time in 2018
Table 2: Accuracy Validation performed in VTM
Bp and Bpp were detected in every dilution of VTM (up to 10 organisms can be detected with this method).Note: Limit of detection for Bp and Bpp in saline were 10^2 CFU/ml.
Using Simplexa PCR method, reproducibility was done over 3 days showing repeat and consistent results at 10 CFU/ml
• This new FDA-approved assay is accurate, reproducible and exhibits a low limit of detection, is simple to run 7 days a week, and provides an easier format compared to the in-house LDT.
• Additional large scale prospective study is indicated to confirm our results.