Embed Size (px)
Citation preview
1/14/2014
1
Use of Local Anesthesia in Hand Surgery
Andrew W. Gurman, MD
January 21, 2014
Traditionally, hand surgery has been performed under tourniquet control
Which requires anesthesia
1/14/2014
2
And that is expensive
• Pre-op consultation
• MD/DO + CRNA
• Pharmacy
• IV
• Pre-testing – EKG, CXR, Labs
• Recovery room
• Total cost = $$$$
The use of epinephrine obviates the need for a tourniquet
11th Commandment of Hand Surgery Thou shalt not use epinephrine in the hand
1/14/2014
3
Sterling Bunnell
• Father of Hand Surgery
• Injected a local anesthetic with epinephrine
• The finger died
• 60+ years of absolute obedience to #11
• Phentolamine described as antidote
• #11 is disproved
• Bunnell probably used procaine, which has a short shelf life
WALANT
• W ide
• A wake
• L ocal
• A nesthesia
• N o
• T ourniquet
Advantages of WALANT
• Cost
• Patient satisfaction > 90%
• Patient safety – no anesthesia side effects
• Patient safety – no stopping anticoagulants
• Patient safety – no stopping diet, insulin, etc.
• Quality – intra-operative assessment of tension of tendon repairs and transfers
• Quality – assessment of adequacy of release
• Increased compliance when patients watch
1/14/2014
4
Personal experience
• Started January 1, 2011
• > 1,000 cases
• Age range 12 to 100
• Excellent patient acceptance
• Some cases are just better this way
WALANT technique
WALANT technique
• Buffer the medication
• Slow injection
• Adequate time to “soak in”
• Pre-op and intra-op coaching
1/14/2014
5
Hemostasis
Sharing
No separate reimbursement when local anesthesia is administered by the surgeon
1/14/2014
6
WIN – WIN - WIN
• Physicians are rewarded for extra work and liability
• Patients receive better care
• Highmark saves money
LOSE – LOSE - LOSE
• Physicians are forced to perform cases under local if they are not comfortable
• Physicians are not trained in WALANT
• Patients get poorer care
• Costly complications
Thank you
1/14/2014
1
The Role of Wide Awake
Surgery in an Academic Hand
Surgery Practice
Peter C. Amadio, M.D. Lloyd A. and Barbara A. Amundson
Professor of Orthopedics Mayo Clinic
Disclosures
• None relevant to this talk
Academic Practice
Differences from Private Practice
• Patients may be more complex
• Patients may be more diverse
• Cultures
• Where they live
• Median distance of Mayo patient home from Rochester MN- 100 miles
• Mean distance- far greater
• High volumes/competition for resources
1/14/2014
2
Academic Practice
Favorable setup for WAS
• Reduced surgical morbidity in an environment where this is already very high due to case mix
• Reduced resource demand in an environment where this is already very high due to case mix
• Anesthesia staff
• Recovery room
• OR time
But not for everyone
• Some patients want to be asleep/unaware for personal or cultural reasons
• In some cases OR time/resource use not much different with/without tourniquet
• CTR
• Trigger, DeQuervain’s etc
Academic Practice Potential for improved quality
• Better outcomes?
• Fewer reoperations?
• Better patient satisfaction?
1/14/2014
3
Main Indications
• Cases where a tourniquet is contraindicated, and a bloodless field is helpful, such as hand surgery in patients with ipsilateral lymphedema or dialysis access, or with recent upper limb vascular surgery (for example, need for additional reconstruction in recent postop period after vascular reconstruction for trauma)
Main Indications
• Cases where hemostasis could use a boost, such as patients with recent angioplasty who must remain anticoagulated during hand surgery
• Prolonged white finger? Phentolamine rescue
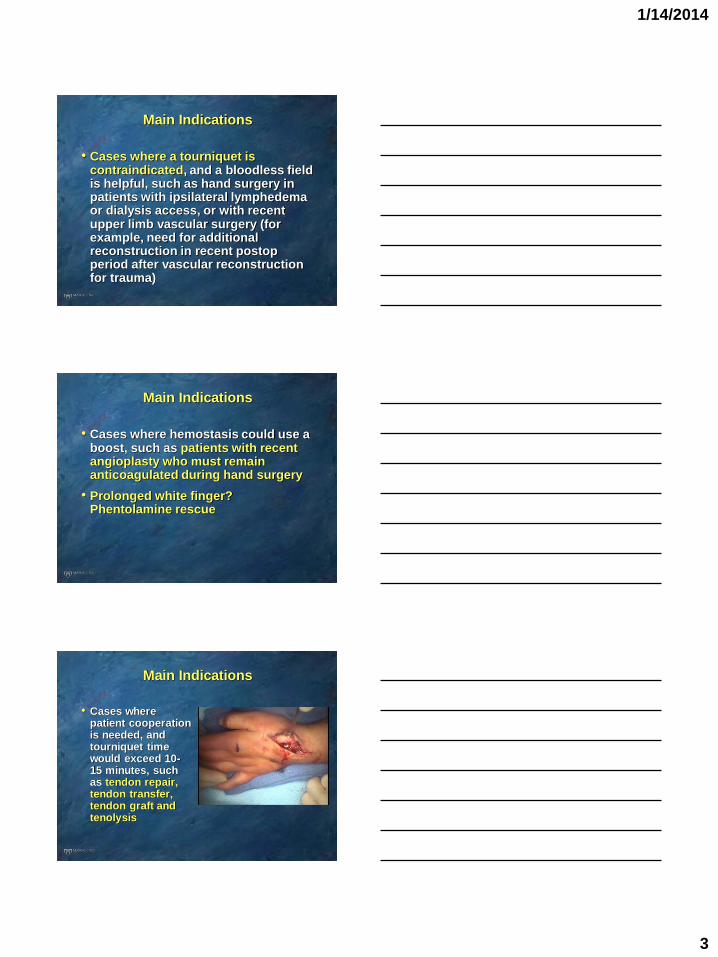
Main Indications
• Cases where patient cooperation is needed, and tourniquet time would exceed 10-15 minutes, such as tendon repair, tendon transfer, tendon graft and tenolysis
1/14/2014
4
Arthroplasty
• The patient knows everything that is going on, especially if they watch (which I always encourage). A better informed patient is a happier patient and a better partner in postop recovery
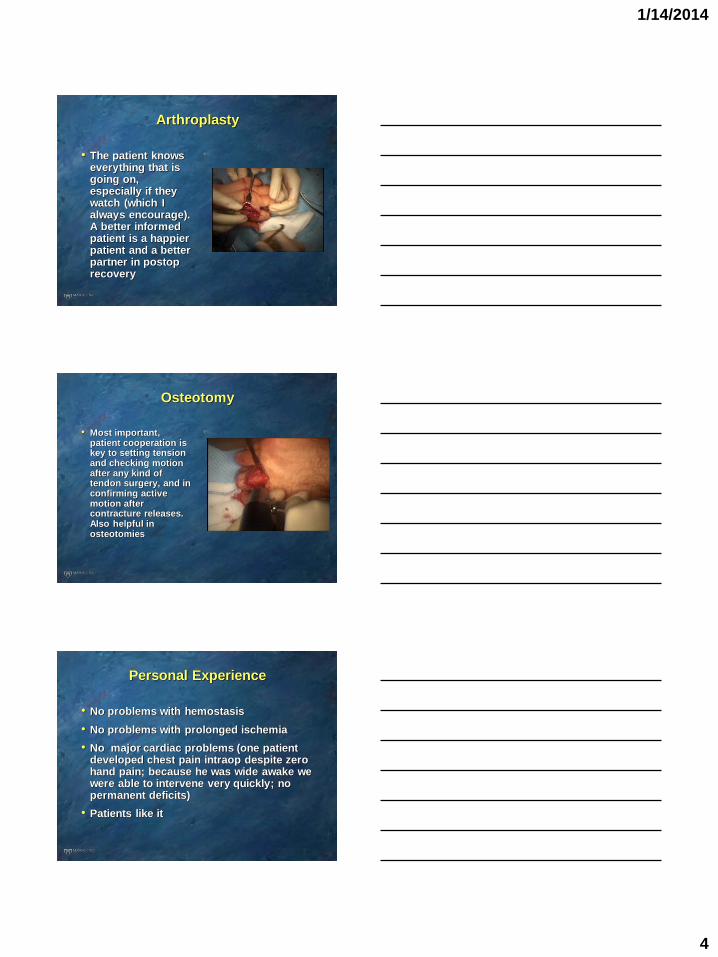
Osteotomy
• Most important, patient cooperation is key to setting tension and checking motion after any kind of tendon surgery, and in confirming active motion after contracture releases. Also helpful in osteotomies
Personal Experience
• No problems with hemostasis
• No problems with prolonged ischemia
• No major cardiac problems (one patient developed chest pain intraop despite zero hand pain; because he was wide awake we were able to intervene very quickly; no permanent deficits)
• Patients like it
1/14/2014
5
Best part
patients love it (so far ages 12-92)
• “thanks, doctor. I really enjoyed the surgery!”
• “People definitely need to put this on their ‘bucket list’. It was great!”
Summary
• Very useful
• Low morbidity
• Phentolamine readily available for rescue but likelihood of needing it is low
1/20/2014
1
Exemplary Care Cutting-edge Research World-class Education
Rafael J. Diaz-Garcia, M.D.
Hand and Upper Extremity Fellow
Alex Andoga, BS
Research Assistant
Mark E. Baratz, M.D. Clinical Professor and Vice-Chair
Department of Orthopaedics
University of Pittsburgh Medical Center
Economics of Wide-Awake Hand Surgery
Exemplary Care Cutting-edge Research World-class Education
• Healthcare expenditures in the U.S. per year
>$2.6 trillion 1000% increase since 1980
• Congress’ solution: cut Medicare
reimbursement.
• Our solution? Provide care at lower costs.
• Wide-awake hand surgery may be an easy
method to improve value in your practice.
The Problem
Exemplary Care Cutting-edge Research World-class Education
Wide-Awake Hand Surgery
Surgery under local anesthesia is a
cost-saving multiplier
1/20/2014
2
Exemplary Care Cutting-edge Research World-class Education
The Costs of the Status Quo
• Anesthesia raises the costs of care
•Direct - Medicare: $105 for 30min
Private: $275 for 30min
• Indirect - Preoperative testing, labs, medical
clearance
Medicare: ~ $120
• Costs of excess materials
•Drapes, basins, tourniquet, etc: $91.81
Potential Savings of $300-600 dollars per patient
Exemplary Care Cutting-edge Research World-class Education
Current Patient Treatment Course
Surgeon
Clinic
EMG/NC
S
PCP
Wait
List
Preop
Test/H&P
Sedation
+/- block
Surgeon
Clinic
PACU
Surgery
Exemplary Care Cutting-edge Research World-class Education
Does This Really Save Money?
• Leblanc, et al. found that use of main OR time
was 4x as expensive and less than 1/2 as
efficient as ambulatory clinic setting.1
• Chatterjee, et al. found that total cost was
double for endoscopic CTR and quadruple for
open CTR when comparing main OR to clinic.2
1 Leblanc MR, Lalonde J, Lalonde DH. A detailed cost and efficiency analysis of carpal tunnel surgery in the main operating room versus ambulatory setting in Canada. Hand 2007 Dec; 2(4) 2 Chatterjee A, McCarthy JE, Montagne SA, Leong K, Kerrigan CL. A cost, profit and efficiency analysis of performing carpal tunnel surgery in the operating room vs the clinic in the U.S. Ann Plas
Surg 2011; 66.
1/20/2014
3
Exemplary Care Cutting-edge Research World-class Education
Can Wide Awake Surgery Improve Efficiency?
• One group in the UK streamlined their entire
practice for both patients and surgeons.3
•Time from referral to surgery
18 weeks 4 weeks
•Specialist time with patient
2.5 hrs 45min
3 Bismil MSK, Bismil QMK, Harding D, Harris P, Lamyman E, Sansby L. Transition to total one-stop wide-awake hand surgery service-audit: a retrospective review. J R Soc Med Sh Rep 2012;3(23).
Exemplary Care Cutting-edge Research World-class Education
Will I Lose Patients?
• 100 consecutive patients were polled post-
operatively.4
• 91% found it was less painful or
comparable to procedures done under
local at the dentists office.
• 86% would prefer to be awake for further
hand surgery.
• 90% would recommend wide awake
surgery to a friend. 4 Teo I, Lam W, Muthayya P, Steele K, Alexander S, Miller G. Patients’ perspective on wide-awake hand surgery—100 consecutive cases. J Hand Surg Eur Vol. 2013 38(9).
Exemplary Care Cutting-edge Research World-class Education
Economic Effects of Wide Awake Surgery
• Reduces direct and indirect costs.
• Increased efficiency in the delivery of care in
the ambulatory setting.
• Net result is greater patients cared for, at a
lower cost, with a high patient satisfaction rate.
1/20/2014
4
Exemplary Care Cutting-edge Research World-class Education
So How is this a “Win” for my Practice?
• Efficiency
• Safety
• Satisfaction
• …and the insurers get this.
• Opportunity to improve re-imbursement
Exemplary Care Cutting-edge Research World-class Education
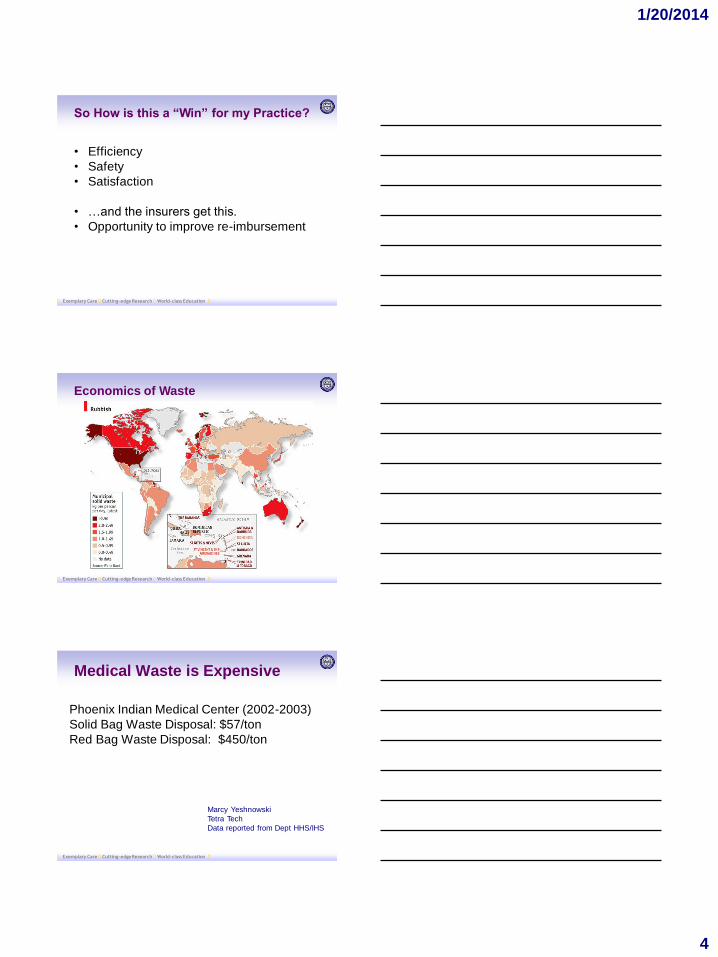
Economics of Waste
Exemplary Care Cutting-edge Research World-class Education
Medical Waste is Expensive
Phoenix Indian Medical Center (2002-2003)
Solid Bag Waste Disposal: $57/ton
Red Bag Waste Disposal: $450/ton
Marcy Yeshnowski
Tetra Tech
Data reported from Dept HHS/IHS
1/20/2014
5
Exemplary Care Cutting-edge Research World-class Education
The Costs Extend Beyond
Our Backyard
Exemplary Care Cutting-edge Research World-class Education
AAHS 2014
Exemplary Care Cutting-edge Research World-class Education
Kamilo: The Great Pacific Garbage Patch
• Hawaiian
Islands/Kamilo
Beach
• North Pacific Gyre
• Miles of trash: up
to10 feet deep
National Oceanic and Atmospheric
Administration
1/20/2014
6
Exemplary Care Cutting-edge Research World-class Education
• Trash from all over
the world
• 90% is plastic
• Takes 50-500 years
to degrade
Exemplary Care Cutting-edge Research World-class Education
Environment Cost = Economic Cost
Ian Jones / Wild Orchids for Trotsky
Exemplary Care Cutting-edge Research World-class Education
The Perfect Storm:
Decreased reimbursement
Pressure to improve safety and satisfaction
Strained global environment
1/20/2014
7
Exemplary Care Cutting-edge Research World-class Education
The Lean and Green Movement
Leadership of AAHS, ASSH, ASRM & ASPN
•Identify the Obstacles and Opportunities
• Reduce cost
• Reduce waste
• Improve safety
• Patient satisfaction
•Wide awake surgery can be part of the
solution
Hand surgeons doing their part…
Exemplary Care Cutting-edge Research World-class Education
Thank You
Julie E. Adams MD
Orthopaedic Surgery
University of Minnesota
Wide-awake hand surgery: strategies for
implementation
• Arthrex, Articulinx, Acumed: consulting
• Biomet: Royalties
• Elsevier: Honorarium
Disclosures
• Wide-awake hand surgery has many benefits
– Patient/surgeon satisfaction
– Cost benefit
– Safety
– Time
Introduction
Ulnar Neuropathy
Decompression vs. Transposition
• Safety concerns
• Charting concerns
• Patient/institutional acceptance
• Anesthesia care providers/nursing buy-in
• “that’s not how we do things here”
• “we don’t have the staffing/space/time to
do monitoring”
Barriers to implementation
Ulnar Neuropathy
Decompression vs. Transposition
• Local-alone, MAC, regional and general cases with
tourniquet in an academic multisite practice
– 2 ASC (hospital owned)
– ASC (in free standing multisubspecialty orthopedic
clinic)
– 3 clinics
– 2 hospitals
Background
Detection
• Ruth Jackson Orthopaedic Society traveling
fellowship: visit to Don Lalonde
• Prior to: dabbled
May 2013
Detection
• Enthusiastic about
WALANT and
implementation.
– Challenges: getting local “in”
with enough time for epi to
work (~ 20-30 minutes)
– Buy-in and logistical barriers
Returned….
Ulnar Neuropathy
Decompression vs. Transposition
• Already had buy-in from partners
– Other attendings in our fellowship program
– Procedure room + epi used by practice partners and me already
• Approached preop nurses and Anesthesiologists at my
highest volume facility (connected to the hospital with
slowest turnover) – Their concerns
– My concerns
– Plan to reconcile
– Avoid discounting concerns of any party (even if they make no sense)
Careful about how I implemented….
Ulnar Neuropathy
Decompression vs. Transposition
• Develop your 30 second narrative and present it in a
respectful way
• Figure out who the stakeholders are and involve them
from the start
• Presenting your plan and having an alternative
• Making it a “win-win”
• Being flexible
• Good pre-extant relationship with periop
– preop nurses, anesthesia.
Arguments that work—generating LEVERAGE
Ulnar Neuropathy
Decompression vs. Transposition
• Develop your 30 second narrative and present it in a
respectful way
– This is why I want to do this
– This is why I think it is safe/ better for our patients/ better for
our hospital or ASC/ environment
– Here is the evidence (Printouts/articles/references)
– “millions of people a day have lidocaine with epi in dental
offices without monitoring and no adverse effects”
– “not different than an injection in the office (which is
currently done without monitoring)”
Arguments that work—generating LEVERAGE
Ulnar Neuropathy
Decompression vs. Transposition
• Figure out who the
stakeholders are and
involve them from the
start
– Typically charge preop
nurse
– Surgery center/hospital
surgery manager
– Anesthesiology
– Surgical services lead
Arguments that work—generating LEVERAGE
Ulnar Neuropathy
Decompression vs. Transposition
• Presenting your dilemma and having an alternative
• Making it a “win-win”
– “I would love to give (our institution) more business but….I
suppose I will need to take the patient to (Y institution/do
case in my clinic). I really would prefer to operate at (X).”
– “I could do “n” number of cases per block time with wide
awake, vs “p” number of cases with local and MAC
Arguments that work—generating LEVERAGE
Ulnar Neuropathy
Decompression vs. Transposition
• Being flexible-accept baby steps from your institution
(or suggest them)
– “Would it be ok to try this on a few select patients and see
how things go?”
– “Let’s do all the monitoring you want initially, and then see
if we truly need it”
– “Let’s do a pilot study”
– “Ok, I understand you don’t feel comfortable with this. Can
you help me understand why? What parameters would you
feel comfortable with?”
Arguments that work—generating LEVERAGE
Ulnar Neuropathy
Decompression vs. Transposition
• Good pre-extant relationship with periop
– Head preop nurse, anesthesia.
– What do YOU think you need from ME to make this work?
• Preop order in computer for lido with epi
• List of items needed
• Patient supine with pulse ox and BP monitoring, RN at bedside,
consent and preinjection pause.
Arguments that work—generating LEVERAGE
Ulnar Neuropathy
Decompression vs. Transposition
• If your practice is at multiple sites- EACH ONE is likely
to be different.
• Even if in same hospital system.
• Even if one is the hospital and one is the ASC
• REMEMBER- their past experiences may shape how they
perceive your plans-it may have nothing to do with you!
– Did another surgeon demand MAC anesthesia mid way through a
local alone case?
– Did a patient have pain/bleeding during another local alone case
(maybe without epi?)
Outcomes
Ulnar Neuropathy
Decompression vs. Transposition • “I appreciate you looking at this issue and working to improve patient care and
efficiency and cost effectiveness. I'd like to understand the rationale behind
restricting the BMI at []. If the team requires more reassurance that this is
effective and safe and wants to see "how it goes", I'm ok with that, I’m just
curious.”
• “Thanks for your note and comments. I am and have been on board with you on
this matter. But here at [] we like to lead from behind, so we are ramping up a
little cautiously because at this current juncture a variety of stakeholders have to
be on board….I would actually like to see the studies if you wouldn't mind taking
the time to send me the citations.”
• “Thanks [], I understand, and as I said, I'm ok convincing people this is a good
idea by progressive experience. Thanks again for your support.”
Outcomes- my experience
Ulnar Neuropathy
Decompression vs. Transposition • “I appreciate you looking at this issue and working to improve patient care and
efficiency and cost effectiveness. I'd like to understand the rationale behind
restricting the BMI at []. If the team requires more reassurance that this is
effective and safe and wants to see "how it goes", I'm ok with that, I’m just
curious.”
• “Thanks for your note and comments. I am and have been on board with you on
this matter. But here at [] we like to lead from behind, so we are ramping up a
little cautiously because at this current juncture a variety of stakeholders have to
be on board….I would actually like to see the studies if you wouldn't mind taking
the time to send me the citations.”
• “Thanks [], I understand, and as I said, I'm ok convincing people this is a good
idea by progressive experience. Thanks again for your support.”
Outcomes- my experience
Ulnar Neuropathy
Decompression vs. Transposition • “I appreciate you looking at this issue and working to improve patient care and
efficiency and cost effectiveness. I'd like to understand the rationale behind
restricting the BMI at []. If the team requires more reassurance that this is
effective and safe and wants to see "how it goes", I'm ok with that, I’m just
curious.”
• “Thanks for your note and comments. I am and have been on board with you on
this matter. But here at [] we like to lead from behind, so we are ramping up a
little cautiously because at this current juncture a variety of stakeholders have to
be on board….I would actually like to see the studies if you wouldn't mind taking
the time to send me the citations.”
• “Thanks [], I understand, and as I said, I'm ok convincing people this is a good
idea by progressive experience. Thanks again for your support.”
Outcomes- my experience
Ulnar Neuropathy
Decompression vs. Transposition • “I appreciate you looking at this issue and working to improve patient care and
efficiency and cost effectiveness. I'd like to understand the rationale behind
restricting the BMI at []. If the team requires more reassurance that this is
effective and safe and wants to see "how it goes", I'm ok with that, I’m just
curious.”
• “Thanks for your note and comments. I am and have been on board with you on
this matter. But here at [] we like to lead from behind, so we are ramping up a
little cautiously because at this current juncture a variety of stakeholders have to
be on board….I would actually like to see the studies if you wouldn't mind taking
the time to send me the citations.”
• “Thanks [], I understand, and as I said, I'm ok convincing people this is a good
idea by progressive experience. Thanks again for your support.”
Outcomes- my experience
Ulnar Neuropathy
Decompression vs. Transposition
• ASC #1 (hospital owned/operated; busiest,
most of my practice)
– Wants preop order for lido with epi
– Patient supine/BP and pulse ox/ RN at
bedside/preinjection pause. RN does usual intake (what
are your meds/allergies/when did you eat last?).
– No preop H&P-just need a reason for patient
presentation entered into EMR.
Outcomes- my experience
Ulnar Neuropathy
Decompression vs. Transposition
• Hospital #1,2 (owned by same as ASC #1)
– Wants preop order for lido with epi
– Doesn’t yet care about BP/pulse ox
– RN does usual intake (what are your
meds/allergies/when did you eat last?).
– No preop H&P-just need a reason for them there
entered into EMR.
Outcomes- my experience
Ulnar Neuropathy
Decompression vs. Transposition
• ASC #2 (owned by same as ASC #1, hosp
1&2)
– Just delighted I am doing cases there.
– Doesn’t yet care about BP/pulse ox
– RN does abbreviated intake (“what are we doing for
you today”)
– No preop H&P-just need a reason for them there
entered into EMR.
– Draws up injection for me.
Outcomes- my experience
Ulnar Neuropathy
Decompression vs. Transposition
• Clinic #1, 2 (owned by hosp #1, operated by
physician’s group)
– Our rules
– Pre injection time out
– Pre procedure time out
– RNs or MAs take care of “orders”
Outcomes- my experience
Ulnar Neuropathy
Decompression vs. Transposition
• Clinic #3
– No monitoring
– RNs or MAs take care of “orders”
– Ok to do “trauma” cases/I&D’s
Outcomes- my experience
Ulnar Neuropathy
Decompression vs. Transposition
• ASC #3
– Still working on it….
Outcomes- my experience
Ulnar Neuropathy
Decompression vs. Transposition
• It’s a give and take
• They may require some reassurance and evidence
that it is safe and effective
• Its ok to start out in a limited fashion-that is still a
“win”- just keep asking questions and probing as
time goes on.
• There are some places that are going to have to be
on the trailing edge of change
Outcomes- my experience
For AACM Conference and registration details:
aacm.org.ar | [email protected]
On behalf of the American Associati on for Hand Surgery (AAHS) and the Asociaciόn
Argentina de Cirugía de la Mano (AACM), we invite you to participate in the AAHS Pre-Course:
Surgical Advances In Elbow, Wrist And Hand Surgery
October 15, 2014 | 11am – 7pm
Buenos Aires, Argentina
Program Chair: Julie Adams, MD
PROGRAM SCHEDULE
11:00–11:15am Introduction and remarks
Mark Baratz, MD Carlos Eugenio Martinez, MD
Scientific Session: Bony Trauma Symposia
11:15–11:35am Scaphoid Fractures/Non-Unions: Tips and Techniques
Thomas B. Hughes, MD, and Carlos Zaidemberg, MD
11:35–11:40am Questions & Answers
11:40am– PIP Fracture Dislocat ions – Treatment Options 12:10pm Jeffrey Greenberg, MD, Alejandro Badia, MD,
and Cherrie A. Heinrich, MD
12:10–12:15pm Questions & Answers
12:15–12:45pm Challenging Elbow Fractures Scott F. Duncan, MD, Scott Steinmann, MD, and Mark Baratz, MD
12:45–12:50pm Questions & Answer
12:50–1:20 pm Wrist Injuries and Complications of Wrist Injuries Michael S. Bednar, MD, Eduardo Rafael Zancolli, MD, and Miguel Capomassi, MD
1:20–1:25 pm Questions & Answers
1:25–1:45 pm Open Forum for Questions & Answers
1:45–3:00 pm LUNCH BREAK
Scientific Session: Reconstruction
3:00–3:30pm Advances in Wrist and Hand Arthroscopy and Endoscopy Mark Rekant, MD, John Lubahn, MD, and Martin Caloia, MD
3:30–3:35 pm Questions & Answers
3:35–4:05 pm Advances in Wrist and Hand Arthroplasty and Reconstruction Marco Rizzo, MD, Peter Murray, MD, and David Botzenka, MD
4:05–4:10 pm Questions & Answers
4:10–4:40 pm Surgical Management of Scapholunate Instability Julie Adams, MD, Mario Rodriguez Sanmartino, MD, and William Lanzinger, MD
4:40–4:45 pm Questions & Answers
4:45–5:00 PM BREAK
5:00–5:30 pm Reconstruction of Congenital Hand Lesions Steve Moran, MD, Alex Davit, MD, and Hilton Gottshalk, MD
5:30–5:35 pm Questions & Answers
5:35–6:05pm Management of Nerve Injuries: Strategies and Techniques Randip R. Bindra, MD, Michael Neumeister, MD, and Loree Kallianen, MD
6:05–6:10pm Questions & Answers
6:10–6:45pm Tendon Repair and Reconstruction Donald H. Lalonde, MD, Jerry I. Huang, MD, and Jose Maria Rotella, MD
6:45–6:50pm Questions & Answers
6:50–7:00pm Open Forum for Questions & Answers; Adjourn
AAHS Precourse
AACM meeting October 15, 2014
Buenos Aires,
Argentina
www.handsurgery.org
www.aacm.org.ar
Thank You!
1/16/2014
1
Don Lalonde MD
Saint John, Canada
Professor Surgery
Dalhousie University
Wide awake hand surgery
Office practice • Office operating room accredited by
CAAASF for pure local anesthesia (50k)
• All sedation cases go to the hospital
• A second room has a stretcher where I
inject local into patients
• I inject 2 or three patients before I do the
first one
• OR
• I inject a patient, then see a few consults
before operating
McKee D,. Optimal time delay between
epinephrine injection and incision to minimize
bleeding Surg Plast. Reconstr. Surg. 131: 811,
2013.)
• Level I evidence from humans 2013
• It takes a mean of 26 minutes for maximal
vasoconstriction after injection of
1:100,000 epinephrine with lidocaine
beneath human skin (NOT 7 minutes –
1987 pig study)
• Helpful to inject the local anesthesia
before bringing the patient into the
operating room.
1/16/2014
2
Office practice • Worst case scenario, I would abort
surgery, wrap up hand like a laceration,
and take patient to the hospital (this has
never happened)
How to “talk patients into”
• “You can test your repair during the
surgery to make sure you get a better
result”
• “Have you ever had a problem after an
operation?”
• Preop testing hassle factor
• Fear of needles
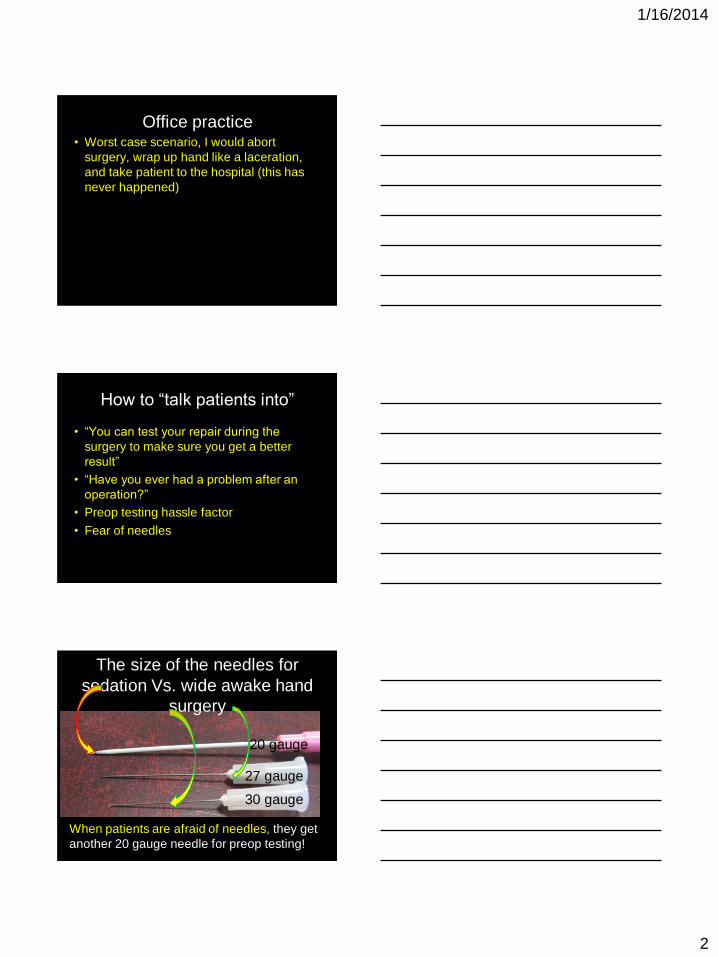
The size of the needles for
sedation Vs. wide awake hand
surgery
20 gauge
30 gauge
27 gauge
When patients are afraid of needles, they get
another 20 gauge needle for preop testing!
1/16/2014
3
How to inject local anesthesia
so that it hardly hurts at all
Sept 2013 PRS with movies
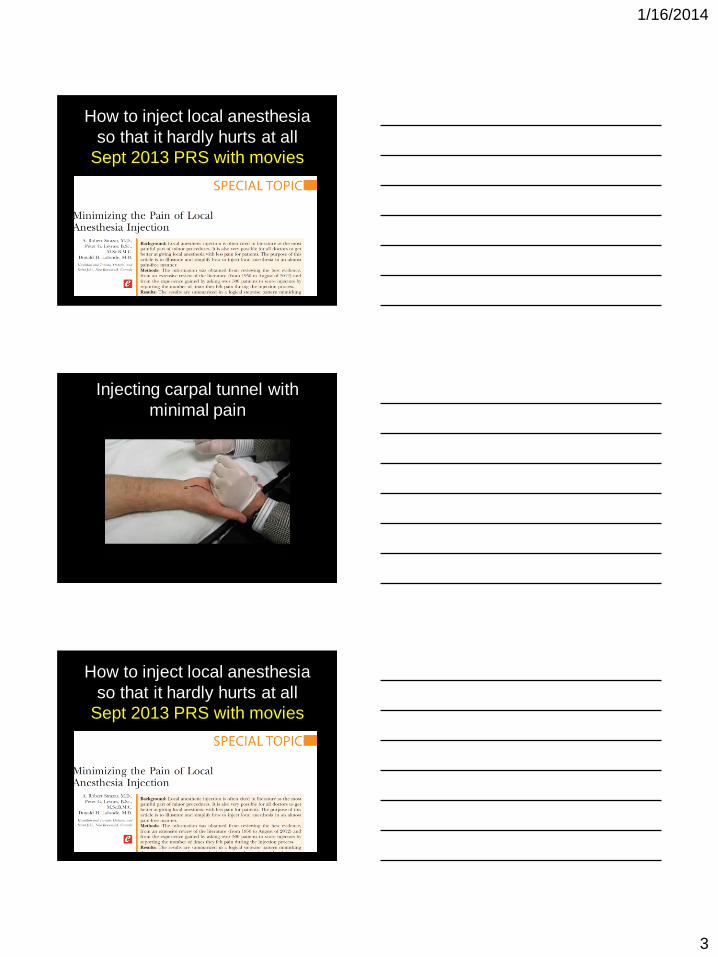
Injecting carpal tunnel with
minimal pain
How to inject local anesthesia
so that it hardly hurts at all
Sept 2013 PRS with movies
1/16/2014
4
Typical intraoperative patient education while
closing skin
(instead of talking about the weather with the
nurses or doctors in the room)
Epinephrine in the finger IS safe
4 of the main papers
• 1. A critical look at the evidence for and against
elective epinephrine use in the finger. Thomson
CJ, Lalonde DH, Denkler KA. Plast Reconstr
Surg.119(1): 260-266, January 2007.
• The cause of the myth was procaine
• procaine responsible for the finger deaths
blamed on adrenaline between 1920 and
1945.
adrenaline morphine
phentolamine naloxone
(α blocker) (Narcan)
=
1/16/2014
5
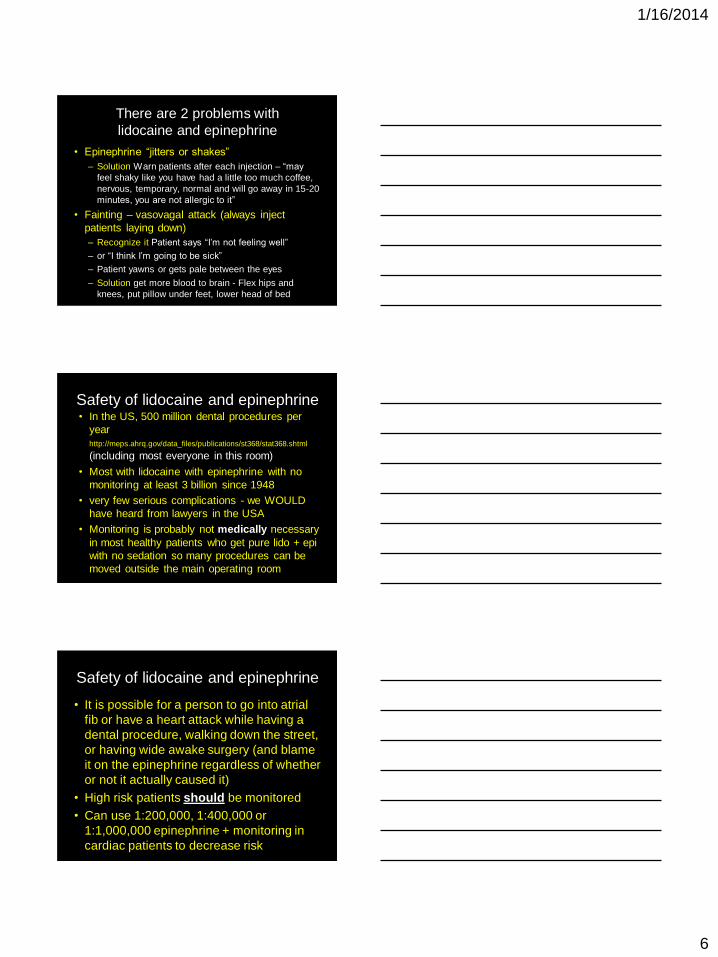
Phentolamine reversal of vasoconstriction
after lidocaine + adrenaline Injection
2cc Lidocaine +
Adrenaline only Lidocaine +Adrenaline
+phentolamine 1 hour
after (1mg in 1cc)
How to use phentolamine alpha blocker
to reverse epinephrine vasoconstriction
• I have never HAD to use phentolamine
rescue in over 2000 fingers, but you can
inject phentolamine if you are
uncomfortable sending them home with a
white finger tip (rare)
• 1mg phentolamine in 1-5cc of saline and
inject it everywhere epi has been injected
in small volumes
• 5mg phentolamine IV will drop your blood
pressure
August 2013
J Am Acad Orthop
Surg. 2013
Aug;21(8):443-7.
1/16/2014
6
There are 2 problems with
lidocaine and epinephrine
• Epinephrine “jitters or shakes”
– Solution Warn patients after each injection – “may
feel shaky like you have had a little too much coffee,
nervous, temporary, normal and will go away in 15-20
minutes, you are not allergic to it”
• Fainting – vasovagal attack (always inject
patients laying down)
– Recognize it Patient says “I’m not feeling well”
– or “I think I’m going to be sick”
– Patient yawns or gets pale between the eyes
– Solution get more blood to brain - Flex hips and
knees, put pillow under feet, lower head of bed
Safety of lidocaine and epinephrine • In the US, 500 million dental procedures per
year
http://meps.ahrq.gov/data_files/publications/st368/stat368.shtml
(including most everyone in this room)
• Most with lidocaine with epinephrine with no
monitoring at least 3 billion since 1948
• very few serious complications - we WOULD
have heard from lawyers in the USA
• Monitoring is probably not medically necessary
in most healthy patients who get pure lido + epi
with no sedation so many procedures can be
moved outside the main operating room
Safety of lidocaine and epinephrine
• It is possible for a person to go into atrial
fib or have a heart attack while having a
dental procedure, walking down the street,
or having wide awake surgery (and blame
it on the epinephrine regardless of whether
or not it actually caused it)
• High risk patients should be monitored
• Can use 1:200,000, 1:400,000 or
1:1,000,000 epinephrine + monitoring in
cardiac patients to decrease risk
1/16/2014
7
84 year old man told by cardiologist not fit
for general anesthesia for tendon transfer
(he said no problem with local)
• EI to EPL with 30cc of ½% lidocaine with
1:200:000 epinephrine
• 7mg / kg is more than safe; Dr Vasconez
and colleagues showed 35mg/kg is safe Plast Reconstr Surg.1996 Jun;97(7):1379-1384.
• 70 kg lady X 7 mg/kg = 490 mg of
lidocaine with 1: 100,000 epinephrine
• 490 mg of lidocaine is 49cc of 1%
lidocaine with epi is extremely safe
• I stay at 50cc of 1% lidocaine with epi to
always stay out of trouble without
monitoring
Calculation of safe dose of
lidocaine + epinephrine
Volume and dosage of local infiltration for
most hand operations Oct 2013 J Hand Surg
1/16/2014
8
Contraindications to epinephrine
in the finger
• If they have a nice pink finger before I
inject, they will have a nice pink finger
after I inject unless I hurt the blood supply
to the finger with my surgery
• Patients who don’t have good perfusion in
the finger before I inject such as Buerger's
disease Bad renal failure
WALANT flexor tendon repair
• Less rupture
• Less tenolysis
• Better patient assessment and education
during the surgery
• Know if superficialis should be repaired or
not
• Comfortable starting true active movement
after surgery as opposed to place and hold
WALANT tendon transfers
• Can adjust the tension of the transfer
before you close the skin so you get it not
too tight or too loose
• Patient can see transfer works with his
own eyes
1/16/2014
9
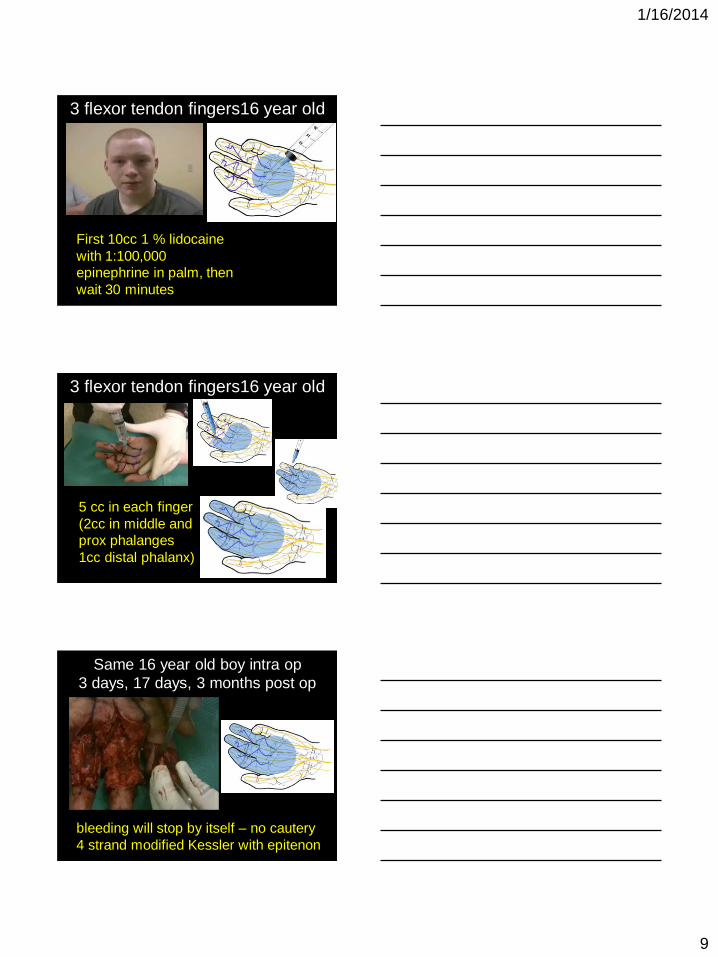
3 flexor tendon fingers16 year old
First 10cc 1 % lidocaine
with 1:100,000
epinephrine in palm, then
wait 30 minutes
3 flexor tendon fingers16 year old
5 cc in each finger
(2cc in middle and
prox phalanges
1cc distal phalanx)
Same 16 year old boy intra op
3 days, 17 days, 3 months post op
bleeding will stop by itself – no cautery
4 strand modified Kessler with epitenon
1/16/2014
10
Up to half a fist 45/45/45
post op protocol
start 3 days post op
• Up to half a fist of active flexion
• MP 45° active extension (half way
extended)
• PIP 45° active flexion (half way flexed)
• DIP 45° active flexion (half way flexed)
Consider submitting your surgery and
therapy papers to the journal Hand
AAHS meets in a warm place every January
1/16/2014
11
Thank you