Embed Size (px)
Citation preview

Use of GlideScope in Patients Undergoing NIM Thyroidectomy C. Ron Cannon1, M.D., Robert Michael Cannon2, Ralph Didlake, M.D2., William R. Replogle, Ph.D.2
1Head and Neck Surgical Group, 1038 River Oaks Drive Flowood, Mississippi 39236, 2University of Mississippi Medical Center, Jackson, MS 39216,
In performing thyroidectomy, the gold standard is that of visualization of the recurrent laryngeal nerve. The nerve integrity
monitor (NIM) is thought to serve as a valuable adjunct.1 In a study of 29,998 nerves by Dralle et al; the dissections were
divided into three groups, those with no recurrent laryngeal nerve identification, a second group with visualization recurrent
laryngeal nerve identification and visual ID use of recurrent laryngeal nerve monitoring. They found that visualization of the
recurrent laryngeal nerve is the gold standard in that there was no statistical difference in nerve visualization with or without
monitoring.2 There was evidence of improved results with use of the NIM but it did not reach statistical significance. In a meta-
analysis of 64,699 nerves, there was no statistical difference in the rate of true vocal cord paralysis using nerve integrity
monitoring versus recurrent laryngeal nerve identification without monitoring.3
Use of the nerve integrity monitor, however, is becoming more prevalent. It is commonly used in otologic and parotid
procedures and becoming more so in thyroidectomy. In a survey of 685 otolaryngologists, 29% use the NIM when performing
Thyroidectomy. The surgeons who used the NIM were three times more likely to use the nerve integrity monitor if they had
been exposed to it during training.4
In the last 5-7 years, a video laryngoscope has been developed that allows video visualization of placement of the endotracheal
tube and is commonly known as the “GlideScope” (Verathon Medical, Bothell, WA, USA). The use of the GlideScope has been
found to be effective in both primary intubation and in management of the difficult airway in both adults and children.5,6 Use of
the GlideScope has recently been reported in patients undergoing NIM thyroidectomy. In a brief clinical description, three
cases successful use of the GlideScope for NIM tube thyroidectomy were reported.7 In a more recent report of 250 patients
undergoing NIM thyroidectomy, the GlideScope allowed successful intubation in all of the patients.
The purpose of this study is to understand the value of using the GlideScope to assure proper NIM tube and electrode
placement within the larynx at the time of thyroidectomy.
A total of 33 patients undergoing thyroidectomy or parathyroidectomy using the NIM system are reported.
After direct laryngoscopy and intubation by the anesthesiologist the patient is positioned on the operating room table for
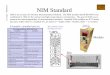
thyroidectomy or parathyroidectomy. The GlideScope is then used to visualize the endotracheal tube within the larynx. (Figure
1) If repositioning of the endotracheal tube proved necessary measurements were made as to proper vertical positioning of the
length of the tube and also rotational orientation of the tube within the larynx to assure maximal contact at the EMG electrodes
with the true vocal folds. Once the optimal tube position has been verified the patient is prepped and the procedure
commences.
RESULTS Of the 33 patients, there were 6 men and 27 women. The average age was 58.3 years with a range of 28-82 years. Of the
surgeries performed, there were 20 lobectomies, 8 total thyroidectomies, 5 parathyroid gland excisions, and 2 patients
underwent concomitant zone VI dissections. There were no instances of NIM system malfunction/nonfunction noted.
The pathology indicated a benign goiter in 16 patients; there were 8 benign follicular adenomas. Of the malignancies, there
were 3 papillary thyroid cancers and 1 squamous cell carcinoma. The squamous cell carcinoma within the thyroid gland
resulted as metastatic disease after previous chemoradiation for a T3N2bM0, clinical stage IV, supraglottic laryngeal cancer.
One patient underwent surgery for what was found to be thyroiditis and 5 patients underwent surgery with findings of a
parathyroid gland adenoma.
Some type of endotracheal tube adjustment was required frequently, in a total of 69.7% of the patients. In 33% of the patients,
tube retraction to a proper depth within the larynx was needed. There were no patients that required advancement of the tube
to properly align the electrodes. In 15% of patients, endotracheal tube depth was fine but tube rotation was required to properly
align the electrodes. Finally, in 21% of the patients, both adjustment of tube depth and also tube rotation for proper alignment
were required.
Of the 33 patients, all had successful visualization of the recurrent laryngeal nerve at surgery. All of the patients were found to
have recurrent laryngeal nerves in their proper anatomic position with the exception of one patient who had a non-recurrent
laryngeal nerve on the right side. The nerve was successfully identified and dissected with normal function postoperatively.
Another patient had a transient left true vocal cord paresis which subsequently resolved thought secondary to traction type
injury. A final patient underwent a right thyroid lobectomy, but developed a left-sided vocal cord paresis postoperatively. This
was thought to be pressure injury from the endotracheal tube cuff. This paresis resolved also. There were no permanent
instances of recurrent laryngeal nerve paresis.
Use of the GlideScope permits optimal placement of the NIM tube prior to initiation of thyroidectomy. It promotes a team approach to
optimal tube placement by both anesthesiologists and the otolaryngologist-head and neck surgery and eliminates tube location as a
possible reason for a non-functioning NIM system. It is non-invasive, inexpensive and usually requires less than 1-2 minutes to verify
tube placement and adjust the tube as needed. Use of the GlideScope in this situation is recommended.
1.RandolphGW,Dralle H, Abdullah H, et al. Electrophysiologic Recurrent Laryngeal Monitoring during Thyroid and Parathyroid Surgery: International Standards Guideline Statement.
Laryngoscope 2011; 121:S1-S16.
2. Dralle H,Sekula C,Haerting J, et al. Risk factors of paresis and functional outcome after recurrent laryngeal nerve monitoring. Surgery 2004; 136(6):1310-1322.
3. Higgins TS, Gupta R, Ketcham AS, et al. Recurrent laryngeal nerve monitoring versus identification alone on post thyroidectomy true vocal fold palsy: a Meta-Analysis. Laryngoscope
2011; 121(5):1009-10017.
4. Horne SK, Gal TK, Brennan KA. Prevalence and patterns of intraoperative monitoring for thyroidectomy. Otolaryngol Head Neck Surg 2007; 136:952-956.
5. Aziz MF,Healy D,Kleterpal S, et al. Routine Clinical practice effectiveness of the GlideScope in difficult airway management: an analysis of 2,004 GlideScope intubations.Complicationsand
failures from 2 institutions. Anesthesiology 2011; 114(1):34-41.
6. Armstrong J,John J,Karsli C. A comparison between GlideScope video laryngoscope and direct laryngoscope in paediatric patients with difficult airways- a pilot study. Anesthesia 2010;
65(4):353-357.
7.Berkow C,Dachiw A,Tufano R. Use of the Glidescope for placement of a recurrent laryngeal monitoring tube. Journ Clin Anes 2011; 23(1):81-83.
8. Kanotra SP,Kuriloff DB,Lesser J, et al. GlideScope assisted nerve integrity monitoring tube placement for intra-operative recurrent laryngeal nerve monitoring. 2012; 126(12):1271-1273.
9. Lu IC, Chu KS, Tsai CJ, et al Optimaldepth of NIM EMG endotracheal tube for IONM of the RLN during thyroidectomy. World J Surg 2008;32:1935-1939.
10. Cannon CR. Topographical analysis of the recurrent laryngeal nerve during thyroidectomy. Presented at sectional meeting of Triologic Society, 3-7 February 2010 at Orlando, Florida. 11. Cannon CR, Lee R,Didlake R.Management of the Substernal Goiter: a team approach. Journal MSMA 2010; 51(7):2010.
Objectives: Thyroidectomy using the nerve integrity monitor requires proper placement of the endotracheal tube with the
electrodes aligned correctly within the larynx. The purpose of this study is to ascertain the percentage of patients who require
endotracheal tube adjustment prior to beginning the thyroidectomy.
Study Design: A prospective study of 33 patients undergoing NIM thyroidectomy is reported.
Methods: The GlideScope (Verathon Medical) is a curved blade intubation device with attached video camera allowing
visualization on a monitor. After routine general orotracheal intubation, the GlideScope was utilized to check the position of the
tube in two planes: depth of tube placement and rotation of the tube within the larynx to properly align the electrodes prior to
initiation of surgery.
Results: Tube adjustment was required in a 69.7% of the patients. In 33% of the patients, tube retraction to a proper depth was
needed. Tube rotation was required in 15% of the patients. In 21% of the patients both adjustment of tube depth and tube
rotation for proper electrode alignment was required.
Conclusions: After the anesthesiologist places the NIM endotracheal tube, tube adjustment is frequent prior to initiation of
thyroidectomy. The GlideScope is readily available in the OR, its use adds little time to the procedure, and assures proper NIM
tube placement. Use of the GlideScope is recommended.
Figure 1: GlideScope view of endotracheal tube within the larynx. Note proper alignment of EMG electrodes contacting the vocal
folds.:
Use of the NIM system is fraught with several potential issues regarding the equipment and the monitoring system. Most of these
relate to the endotracheal tube. This type problem has been reported in 3.8% to 23% of patients undergoing NIM thyroidectomy.1 It is
also thought that a right-handed anesthesiologist tends to rotate the tube clockwise to approximately 30 degrees when intubating the
patient. This rotational error would require a counterclockwise rotation to properly align the NIM tube electrodes within the larynx.
However only 5 of the 12 patients in this series required counterclockwise tube rotation.
There seems to be no significant relationship between the endotracheal tube depth of insertion and the patient’s weight, age, body
mass index, or height. After initial tube positioning, tube readjustment during thyroidectomy is required in only 5.7%.9 In this series, of
patients requiring tube correction after intubation, about 50% required advancement of the tube and 50% required retraction of the
tube. In the current series, the tube always had to be retracted but not advanced.
The significance between adequate NIM tube placement and optimal NIM tube placement in terms of reliability of the NIM system is
not known. The NIM endotracheal tube has a long area wired for laryngeal contact and it may be that this “sweet spot” allows the NIM
system to function with tube placement that is not always optimal. In the senior author’s experience, use of the GlideScope has only
recently been utilized. However in several previous series of thyroidectomies without verifying tube position, there were few instances
of NIM system failure related to tube placement.,9,10
The real advantage of GlideScope verification of optimal NIM tube placement is that it eliminates tube placement issues from the paradigm of possible causes of a non-functioning nerve monitor which may encountered during thyroidectomy.
METHODS
INTRODUCTION
Abstract DISCUSSION
CONCLUSIONS
References