Embed Size (px)
Citation preview

Use
CAD
of a
on
Wei-Shao Lin, D
aAssistant Professor, Department ofbDirector, Advanced Education in Pr
Lin et al
For persona
of digital data acquisition and
/CAM technology for the fabrication
fixed complete dental prosthesis
dental implants
DS,a Bryan T. Harris, DMD,a
Amirali Zandinejad, DDS, MSc,a and Dean Morton, BDS, MSb
School of Dentistry, University of Louisville, Louisville, KY
The work flow in this report describes a metal-resin fixed complete dental prosthesis fabricated by using digital dataacquisition at the implant fixture level with a computer-aided design and computer-aided manufacturing (CAD/CAM)fabricated tissue-colored anodized titanium framework. (J Prosthet Dent 2014;111:1-5)
Two different traditional implantimpression techniques, pickup (opentray) and transfer (closed tray), are usedto obtain impression at the implantfixture level.1 Many studies have focusedon the factors affecting the accuracyof implant impressions and definitivecasts, including splinting or not splint-ing impression copings, modification ofimpression copings, time delay for stonepouring, dimensional stability of im-pression materials and stones, and thedesign and use of custom trays.2 Digitaldata acquisition at the implant fixturelevel has become available and may offersome advantages over conventional im-pression techniques such as improvedpatient comfort and acceptance (espe-cially from those with a strong gagreflex), reduced distortion of theresulting definitive cast, and potentialcost effectiveness for both clinicians anddental technicians.3-6 Digital data ac-quisition at the implant fixture levelcan be achieved by using a scannableimpression coping (Scan Body; Strau-mann) and an intraoral digital scan-ner (Cadent iTero; Cadent Ltd).7 Thescanned data can be interpreted bythe dental laboratory-based computer-aided design and computer-aided man-ufacturing (CAD/CAM) software(Straumann Cares 8.0; Straumann) forthe design of customized anatomicabutments and/or transmitted to the
Oral Healosthodon
Downloal use only. N
modeling center (Cadent iTero; CadentLtd) for the fabrication of milled defini-tive polyurethane casts.
The passive fit of fixed dental pros-theses on dental implants has beenconsidered critical in decreasing theincidence of mechanical complicationssuch as screw loosening, screw fracture,and occlusal inaccuracies.8 Differentapproaches have been proposed toenhance the passive fit of frameworks.CAD/CAM fabricated frameworks de-monstrate a more consistent and supe-rior passive fit than conventionally castframeworks.9 The CAD/CAM processallows the omission of several steps usedin the conventional casting technique,including waxing, investment, casting,and polishing. These procedures areconsidered to introduce inaccuraciesand the inaccuracies may become moreevident with more extensive frame-works.10 A verification device has beenproposed to confirm the accuracy of adefinitive cast.11 A retrospective study12
suggested that the fabrication of a veri-fication device and cast ensured theclinically passive fit ofmetal frameworks,which were verified using the 1-screwtechnique (Sheffield test).13
This article describes a work flowwith digital data acquisition at theimplant fixture level, a milled definitivepolyurethane cast, and CAD/CAM fabri-cated tissue-colored anodized titanium
th and Rehabilitation.tics; and Professor and Chair, Department of O
ded from ClinicalKey.com at University of Louisville July 25,o other uses without permission. Copyright ©2016. Elsevier In
framework for the fabrication of ametal-resin fixed complete dental pros-thesis on dental implants.
TECHNIQUE
First clinical appointment
1. Evaluate the existing dental im-plants (Fig. 1A), and secure scannableimpression copings (Scan Body RN;Straumann) to the implants with a 15Ncm preload (Fig. 1B).
2. Complete the digital data acqui-sition at the implant fixture level with anintraoral digital scanner (Cadent iTero;Cadent Ltd) following the manufac-turer’s instructions. Obtain the scans ofthe impression copings (Scan Body RN;Straumann) and surrounding periim-plant soft tissue areas (Fig. 1C). Sendthe approved scan data to the dentallaboratory (Roy Dental Laboratory).
First laboratory procedure
1. Import the scan data into thecorresponding CAD/CAM software(Straumann Cares 8.0; Straumann).Design, approve, and transmit the in-formation to the manufacturer (CadentiTero; Cadent Ltd) for fabrication of themilled polyurethane definitive cast.
2. Upon receipt of the milled poly-urethane definitive cast, use a drill press
ral Health and Rehabilitation.
2016.c. All rights reserved.

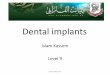
1 A, Occlusal view of existing implants. B, Scannable impression copings secured to implants. C, Digital dataacquisition obtained with intraoral scanner.
2 A, Four dowel pins attached to base of definitive cast. B, Milled polyurethane definitive cast with removable implantanalogs in place.
2 Volume 111 Issue 1
unit (Pindex; Coltene/Whaledent Inc)to place 4 parallel pin holes at thebase of milled polyurethane defin-itive cast. Lute the dowel pins andsleeves (Dual Pin and Sleeve; SelectDental Mfg) into the parallel pin holes
The Journal of Prosthetic Dentis
DownloaFor personal use only. N
at the base of definitive cast withcyanoacrylate resin (3M Scotch SuperGlue; 3M ESPE), and insert thecorresponding removable implant ana-logs (RN Reposition Analog; Strau-mann) into the milled polyurethane
try
ded from ClinicalKey.com at University of Louisville July 25,o other uses without permission. Copyright ©2016. Elsevier In
definitive cast from the occlusal surface(Fig. 2A, B).
3. Spray separating medium (SuperSep; Kerr Corp) onto the base of themilled polyurethane definitive cast. Poura stone base for the milled polyurethane
Lin et al
2016.c. All rights reserved.

3 Milled polyurethane definitive cast with stone base.
January 2014 3
definitive cast over dowel pins/sleeves assembly with Type IV dentalstone (Silky Rock; Whip Mix Corp)(Fig. 3).
4. Attach 1 temporary abutment (RNsynOcta post for temporary restoration,Bridge; Straumann) to all implant
4 A, Completed segmental verification ddefinitive cast.
5 A, Verification device luted as 1 piece
Lin et al
DownloaFor personal use only. N
analogs and connect them by using lightpolymerizing acrylic resin (Triad DentureBase; Dentsply Prosthetics) to fabricate averification device.11,12 Section the veri-fication device with a diamond disk(911.11.220 DS DIAM DISC; BrasselerUSA) (Fig. 4A).
evice on definitive cast. B, Completed imp
intraorally. B, Verification stone cast.
ded from ClinicalKey.com at University of Louisville July 25,o other uses without permission. Copyright ©2016. Elsevier In
5. Attach 1 temporary abutment(RN synOcta post for temporary resto-ration, crown; Straumann) on thedefinitive cast and block out theremaining implant analog areas withwax (Truwax Baseplate Wax Regular;Dentsply Prosthetics). Fabricate animplant-retained trial base with lightpolymerizing acrylic resin (Triad Den-ture Base; Dentsply Prosthetics) andwax (Truwax Baseplate Wax Regular;Dentsply Prosthetics) (Fig. 4B).
Second clinical appointment
1. Evaluate the verification deviceintraorally and connect all the segmentswith autopolymerizing acrylic resin(Pattern Resin LS; GC America)(Fig. 5A). Remove the verification deviceand connect the corresponding implantanalogs (RN synOcta Analog; Strau-mann) with the verification device. Place
lant-retained trial base and wax rim on
2016.c. All rights reserved.

6 A, Digital design of custom-milled titanium bar. B, Completed tissue-colored anodized titanium framework with milledpolyurethane definitive cast and facial matrix assembly.
7 Panoramic radiograph of definitive prosthesis.
4 Volume 111 Issue 1
the assembly into the Type IV dentalstone (Resin Rock; Whip Mix Corp) toobtain a verification cast (Fig. 5B).
2. Evaluate and adjust the implant-retained trial base for esthetics, func-tion, and occlusal vertical dimension.Select the prosthetic teeth (BlueLineDCL;Ivoclar Vivadent) and obtain the facebowtransfer and interocclusal recordwith trialbase and registration material (RegisilRigid; Dentsply Prosthetics). Articulatethe definitive cast and the opposing castin a semi-adjustable articulator (HanauModular Articulator System; Whip MixCorp).
Second laboratory procedure
1. Arrange the selected prostheticteeth (BlueLine DCL; Ivoclar Vivadent)on the implant-retained trial base withwax (Truwax Baseplate Wax Regular;Dentsply Prosthetics).
The Journal of Prosthetic Dentis
DownloaFor personal use only. N
Third clinical appointment
1. Evaluate the trial arrangement onthe implant-retained trial base for es-thetics, function, and occlusion intra-orally. Make necessary adjustments toachieve optimal clinical outcome.
Third laboratory procedure
1. Make a facial matrix with polyvi-nyl siloxane putty (Sil-Tech; IvoclarVivadent) around the facial surface ofthe trial arrangement and milled poly-urethane definitive cast assembly topreserve the spatial orientation of theprosthetic teeth as determined at thetrial insertion appointment.
2. Send the trial arrangement, milledpolyurethane definitive cast, and verifi-cation stone cast to a CAD/CAM facil-ity (Cagenix; Cagenix Inc). Have thedental laboratory technician fabricate
try
ded from ClinicalKey.com at University of Louisville July 25,o other uses without permission. Copyright ©2016. Elsevier In
a custom-milled CAD/CAM titaniumbar (AccuFrame Plus; Cagenix) using thetrial arrangement for the restorativespace assessment and the verificationstone cast to obtain accurate interim-plant spatial relationships during theprocess (Fig. 6).
3. Arrange the prosthetic teeth onthe custom-milled CAD/CAM titaniumbar as determined at the trial insertionappointment by using the facial matrix.
4. Process the definitive tooth ar-rangement with heat polymerizingacrylic resin (SR Ivocap High Impact;Ivoclar Vivadent). Finish and polishthe definitive prosthesis.
Fourth clinical appointment
1. Verify the fit of the definitivemetal-resin fixed complete dental pros-thesis intraorally with the 1-screw tech-nique (Sheffield test)13 and a radiograph(Fig. 7). Adjust the intaglio surface andocclusal contacts of the definitive pros-thesis with a laboratory tungsten carbidecutting instrument (Carbide Cutter;Brasseler USA) as necessary.
2. Secure the definitive metal-resinfixed complete dental prosthesis to theimplants with a 35 Ncm preload(Fig. 8). Instruct the patient as tothe home care regimen and scheduleperiodic maintenance appointments.
DISCUSSION
There are many advantages associ-ated with digital data acquisition at the
Lin et al
2016.c. All rights reserved.

8 Definitive prosthesis. A, Smile. B, Frontal view.
January 2014 5
implant fixture level,3-6 and patientswith strong gag reflexes may signifi-cantly benefit from this work flowbecause the intraoral scanner does nottouch the soft palate and allows thepatients to rest during data acquisitionif necessary.5 There are some disad-vantages of the digital data acquisitionat the implant fixture level, such ashigher initial investment of requiredintraoral digital scanner and CAD/CAM software; further, additionalsystem-specific training and experienceare required for both clinicians anddental technicians. Furthermore, thelarge size of the intraoral digital scan-ner tip may prevent the scanning in theposterior region for patients with smallopenings.6
The proposed laboratory pro-cedures included placing dowel pins/sleeves onto the base of the milledpolyurethane definitive cast andcreating a stone base for the milledcast. The dowel pins and sleeves canprovide flexibility for the laboratoryprocess when there is a need toremove and reposition the milledpolyurethane definitive cast from thestone base, as when replacingdamaged removable implant analogs.The stone base provides a stable sur-face for the articulation of milledpolyurethane definitive cast in a semi-adjustable articulator.
Lin et al
DownloaFor personal use only. N
Summary
This article presents a work flow forobtaining digital data acquisition at theimplant fixture level with an intraoralscanner for a metal-resin fixed completedental prosthesis on dental implants. Itprovides an alternative to obtain adefinitive cast. To ensure the passive fitof the definitive prosthesis, a verifica-tion device and cast were used in thework flow. With the further develop-ment of intraoral scanners and CAD/CAM systems, the verification deviceand cast may be omitted.
REFERENCES
1. Chee W, Jivraj S. Impression techniques forimplant dentistry. Br Dent J 2006;201:429-32.
2. Lee H, So JS, Hochstedler JL, Ercoli C. Theaccuracy of implant impressions: a systematicreview. J Prosthet Dent 2008;100:285-91.
3. Lee SJ, Gallucci GO. Digital vs conventionalimplant impressions: efficiency outcomes.Clin Oral Implants Res 2013;24:111-5.
4. Christensen GJ. Impressions are changing:deciding on conventional, digital or digitalplus in-office milling. J Am Dent Assoc2009;140:1301-4.
5. Ramsey CD, Ritter RG. Utilization of digitaltechnologies for fabrication of definitiveimplant-supported restorations. J EsthetRestor Dent 2012;24:299-308.
6. Nayyar N, Yilmaz B, McGlumphy E.Using digitally coded healing abutments andan intraoral scanner to fabricate implant-supported, cement-retained restorations.J Prosthet Dent 2013;109:210-5.
7. Galhano GÁ, Pellizzer EP, Mazaro JV. Opticalimpression systems for CAD-CAM restora-tions. J Craniofac Surg 2012;23:575-9.
ded from ClinicalKey.com at University of Louisville July 25,o other uses without permission. Copyright ©2016. Elsevier In
8. Abduo J, Bennani V, Waddell N, Lyons K,Swain M. Assessing the fit of implantfixed prostheses: a critical review. IntJ Oral Maxillofac Implants 2010;25:506-15.
9. Drago C, Howell K. Concepts for designingand fabricating metal implant frameworksfor hybrid implant prostheses. J Prosthodont2012;21:413-24.
10. Abduo J, Lyons K, Bennani V, Waddell N,Swain M. Fit of screw-retained fixed implantframeworks fabricated by different methods:a systematic review. Int J Prosthodont2011;24:207-20.
11. Knudson RC, Williams EO, Kemple KP.Implant transfer coping verification jig.J Prosthet Dent 1989;61:601-2.
12. Ercoli C, Geminiani A, Feng C, Lee H. Theinfluence of verification jig on framework fitfor nonsegmented fixed implant-supportedcomplete denture. Clin Implant Dent RelatRes 2012;14:188-95.
13. Kan JY, Rungcharassaeng K, Bohsali K,Goodacre CJ, Lang BR. Clinical methods forevaluating implant framework fit. J ProsthetDent 1999;81:7-13.
Corresponding author:Dr Wei-Shao LinDepartment of Oral Health and RehabilitationUniversity of LouisvilleSchool of Dentistry501 S Preston StLouisville, KY 40202E-mail: [email protected]
AcknowledgmentsThe authors thank Roy Dental Laboratory, NewAlbany, IN, and Cagenix, Memphis, TN for theirassistance in this study.
Copyright ª 2014 by the Editorial Council forThe Journal of Prosthetic Dentistry.
2016.c. All rights reserved.


























![[Dental Implants Cost]](https://img.pdfslide.us/doc/110x75/55638cefd8b42ad2128b4ef9/dental-implants-cost-55849922c2925.jpg)
