Embed Size (px)
Citation preview
British Heart Journal, 1978, 40, 874-882
Use of 129caesium, 99Tcm stannous pyrophosphate,and a combination of the two in the assessment ofmyocardial infarctionS. WALTON, E. KAFETZAKIS, R. A. SHIELDS, H. J. TESTA, AND D. J.ROWLAND S
From the Departments of Cardiology, Medical Physics and Nuclear Medicine, Manchester Royal Infirmary
SUMMARY Acutely damaged myocardium was shown in 103 patients with suspected acute myocardialinfarction using 99Tcm PYP. A significant incidence of false positive and false negative results occurred,'true' results being defined by standard clinical, electrocardiographic, and enzyme criteria. Localisationof infarction compared reasonably well with standard electrocardiographic criteria but more frequentlysuggested true posterior involvement. Serial estimates of infarct size may be of value in the recognitionof infarct extension during the acute phase.
Viable perfused myocardium was shown in 63 patients with a variety of cardiac disorders using 129Cs.The technique gives a reliable indication of anterior infarction but tends to underestimate inferiorinfarction. There was good correlation with the electrocardiogram with regard to localisation and extentof infarction.
Nineteen patients received both isotopes and were included in each ofthe above groups. The combina-tion permits further assessment of equivocal results. Furthermore as 129Cs demonstrates both previousand recent infarction and 99Tcm PYP accumulates only in acutely damaged myocardium it was possibleto estimate the extent of previous and recent myocardial damage.
Myocardial infarction may be demonstrated usingradioisotopes in two distinct ways. Firstly, ionictracers, behaving like potassium, accumulate inviable perfused myocardium, while infarcted areasmay appear as regions of diminished or absentuptake. Secondly, recent myocardial damage can beshown using tracers which selectively concentratein acutely injured cells. Both techniques arepotentially useful to show and localise infarctionbut neither is entirely satisfactory. In ionic tracerstudies, perfusion defects may represent old orrecent infarction and such defects may be obscuredby tracer uptake in healthymyocardium. Backgroundradiation, movement of the heart associated withcardiac activity and with respiration, and the limitedresolution of nuclear imaging techniques mayresult in failure to detect small areas of abnormality.On the other hand, selective uptake into acutelydamaged tissue is often not apparent for up to 12hours after the onset of symptoms. Furthermoresuch uptake can be obscured by uptake in normaloverlying bone and it may not be specific to acute
Received for publication 2 September 1977
myocardial infarction. The purpose of this studywas to evaluate both types of tracer in the assessmentof myocardial infarction when used alone or as acombination in the same patient to assess equivocalresults. Furthermore, the additional informationprovided by the combination might provide anestimate of the extent of previous and recentmyocardial damage as well as an indication ofprognosis.
Patients and methods
'29Caesium (129Cs)l was used to demonstrate viableperfused myocardium and 99Tcm stannous pyro-phosphate2 (99Tcm PYP) to demonstrate acutelydamaged tissue. 129Cs has a half life of 32 hoursand decays by electron capture with principalgamma ray emissions at 372 and 411 keV. 99Tcmhas a half life of 6 hours and decays by isometrictransition emitting a single gamma ray of 140 keV.
'As Caesium chloride produced by the M.R.C. cyclotron atHammersmith Hospital.'Produced by kit from C.I.S., France.
874
on March 24, 2022 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.40.8.874 on 1 August 1978. D
ownloaded from
129Cs and 99Tcm PYP in myocardial infarction
Initially 129Cs imaging was carried out with arectilinear scanner (J & P Engineering Ltd). Thehigh energy collimator was used and the singlechannel analyser was set to accept pulses between350 and 480 keV. The scan speed was 12-5 mm s-Iat a line spacing of 4 mm giving a maximum countdensity of 8 mm-2. Later 129Cs and all 99Tcm PYPstudies were made using a standard gamma camera(Radicamera Mk II General Electric) fitted withthe low-energy, parallel hole collimator for the99Tcm studies and the mid-energy, parallel holecollimator for the 129Cs studies. A 20 per centwindow width was used for all the camera studiescentered on 140 keV for 99Tcm and 400 keV for129Cs. Each 129Cs image was integrated over 10minutes giving an average of 300 000 counts total.Each 99Tcm image was integrated until 600 000counts had been collected. Data were accumulatedon a 64 x 64 matrix and stored on magnetic diskusing the Med II Computer system.
Forty-four patients with a variety of cardiacdisorders including ischaemic heart disease, cardio-myopathy, and valvular disease were studied with'29Cs alone. Eighty-four patients with suspectedacute myocardial infarction were studied with99Tcm PYP alone. Nineteen patients with suspectedacute myocardial infarction were studied with both'29Cs and 99Tcm PYP. All imaging was reported bythe same experienced observer without knowledgeof clinical information.
In all 103 patients with suspected acute myo-cardial infarction received 99Tcm PYP. Their agesranged from 27 to 80 (mean 55) years. The male:female ratio was 6:1. These patients had dailyelectrocardiograms and estimation of the serumenzymes SGOT, SHBD, and CK over the first3 days after admission. In 21 of them the cardio-specific MB fraction of CK was also estimated.Samples were stored at 4°C. Mini-column chroma-tography was then performed to separate the CKisoenzymes and MBCK activity was estimatedspectophotometrically using Worthington Statzymereagent.
Imaging was performed 12 to 102 (mean 61)hours after the onset of symptoms. Ten patientshad repeat examinations on one or more occasions.10 mCi of 99Tcm PYP were administered intra-venously and imaging was performed 40 minuteslater in anteroposterior (AP), left anterior oblique(LAO), and left lateral (LL) views. 99Tcm PYPuptake was considered to be normal when confinedto sternum and ribs and abnormal when additionaluptake was detected in the region corresponding tothe heart.The area of myocardial tracer uptake was
outlined using a light pen on the computer display.
This area was measured as the number of elementsof matrix (pixels) thus enclosed. The largest areain any of the three views was taken to representinfarct size.
Standard clinical, electrocardiographic, andenzyme criteria (all patients) and MBCK elevation(21 patients) were used to assess the reliability of99Tcm PYP in the diagnosis of acute myocardialinfarction. 99Tcm PYP is taken up by bone andacutely damaged myocardium. Localisation ofinfarction was achieved by using the sternum as alandmark and recognising the different patterns ofuptake associated with involvement of particularwalls. Standard 12 lead electrocardiographic criteria(New York Heart Association, 1973) were used toassess the reliability of 99Tcm PYP in the localisationof acute myocardial infarction.
Sixty-three patients with a variety of cardiacdisorders received 129Cs. Their ages ranged from20 to 79 (mean 51) years. The male:female ratiowas 5:1. All had standard 12 lead electrocardio-grams. 2 mCi of 129Cs were administered intra-venously along with 5 mCi of 99Tcm bound tohuman serum albumin (99Tcm HSA), the latteracting as a blood pool marker. Blood pool imagestaken simultaneously with myocardial images wereused in a computer subtraction technique to allowfor residual 129Cs in the blood pool (Rothman et al.,1974). Each element in the 99Tcm image wasmultiplied by a factor and subtracted from thecorresponding element in the 129Cs image. Thefactor was chosen empirically so that the resultantintracavity count density was just reduced to zero.Such dual imaging was then performed 45 minutesafter injection in the AP, LAO, and LL views.129Cs imaging was compared with electrocardio-graphy in the diagnosis and localisation of infarction.In comparison with 99Tcm PYP, localisation with129Cs is considerably easier because the remainingviable myocardium can be identified.An attempt was made to assess infarct size by
classifying defects as large when they involved morethan one wall, medium if between half and one wall,and small if less than half of one wall. Infarct sizewas estimated from the electrocardiograms usingthe criteria of Selvester (Selvester et al., 1972).Of the 19 patients with suspected acute myo-
cardial infarction who received both 129Cs and99Tcm PYP, 18 were men. Their ages ranged from27 to 69 (mean 51) years. The time from onset ofsymptoms to imaging with 99Tcm PYP ranged from19 to 102 (mean 65) hours. It is not possible toperform the two examinations simultaneously sincethe high energy (372 and 411 keV) of the gammarays emitted by 129Cs produce scattered radiationwhich might give the spurious appearance of tracer
3
875
on March 24, 2022 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.40.8.874 on 1 August 1978. D
ownloaded from
S. Walton, E. Kafetzakis, R. A. Shields, H. J. Testa, and D. J'. Rowlands
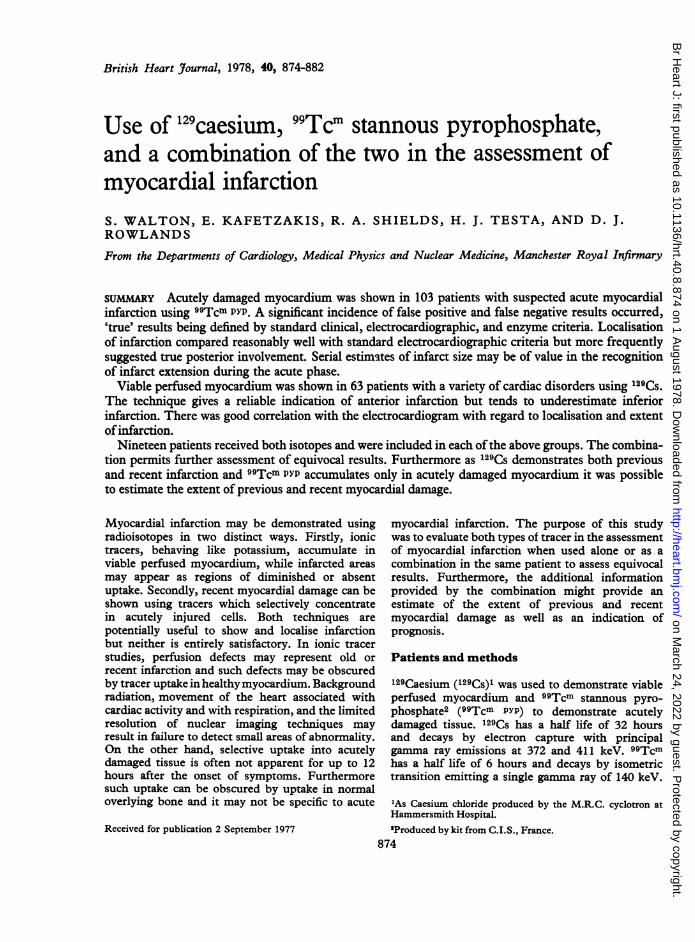
Fig. 1 Imaging with 99Tcm Py/ in a normal suject (left)and a patient with acute myocardial infarction (right).
uptake during 99Tcm PYP imaging. Also the use of99Tcm PYP simultaneously with 129Cs precludes theuse of subtraction as 99Tcm HSA could not be usedto provide blood pool images. Therefore, imagingwith 99Tcm PYP was performed the day before or2 days after imaging with 129Cs. Imaging wasotherwise performed as above. Estimates of infarctsize using 129Cs were compared with those obtainedusing 99Tcm PYP.
Results
Fig. 1, 2, and 3 show examples of normal andabnormal appearances by both techniques.Of the 103 patients admitted with a diagnosis of
suspected acute myocardial infarction, 72 werethought to have definite infarction as judged by atypical clinical story together with electrocardio-graphic and/or enzyme changes. Thirty-one patientswere judged to be dubious, that is to have a clinicalstory suggestive of infarction but with negative
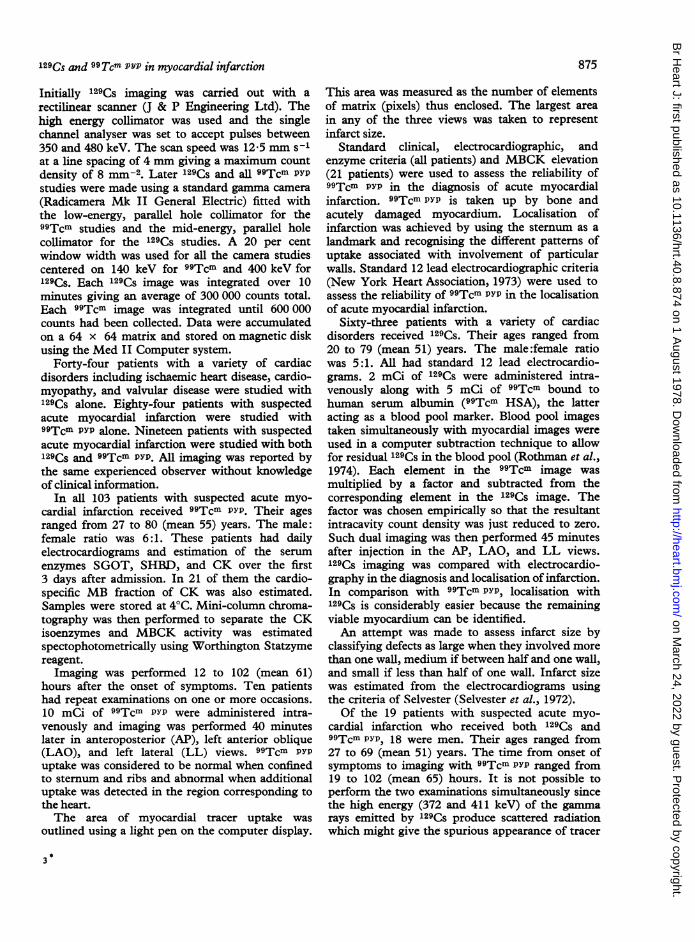
Fig. 2 Imaging with 129Cs in a normal subject (left) and apatient with a large infarction of the interventricularseptum (right).
electrocardiogram and enzyme findings. 99Tcm PYPresults in these 103 patients are shown in Table 1.Uptake of 99Tcm PYP was compared with an increasein serum levels of MBCK in the 21 patients inwhom this investigation was performed. The resultsare shown in Table 2. Localisation of infarctionusing 99Tcm PYP is compared with electrocardio-graphic localisation in the 56 patients with positivetracings and is shown in Table 3. There is goodgeneral agreement. Posterior extension of inferiorinfarction was found more frequently by 99Tcm Pypimaging than by the standard electrocardiographiccriteria. Posterior extension on imaging correlatedwell, however, with pronounced 'reciprocal changes'in the ST segment and T waves ofthe (R) praecordialleads (Table 4). Estimates of infarct size in thepatients with myocardial uptake of 99Tcm Pypranged from 65 to 420 (mean 194) pixels; 420 pixelsbeing the largest estimate of infarct size obtained,these were classified as small if less than 140,
876
on March 24, 2022 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.40.8.874 on 1 August 1978. D
ownloaded from
129Cs and 99T7cm PYP in myocardial infarction
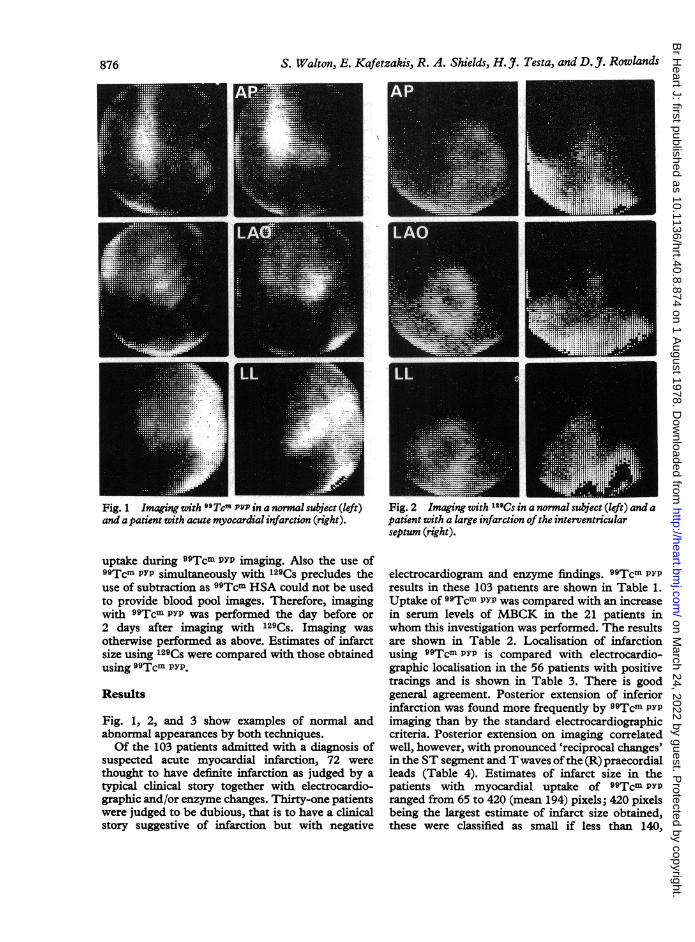
Fig. 3 Imaging with99Tcm Pyp and 129Cs in thesame patient. Left-99TcmPtP showing acute myo-
cardial infarction(29.12.76); centre99TcmP/P showingfurther myo-
cardial infarction (23.2.77);right-t29Cs showingremaining viable myocar-dium after both acuteepisodes (25.2.77).
medium if between 140 and 280, and large if morethan 280. Of the patients in whom imaging with99Tcm PYP was repeated, 6 patients showed eitherno change or a decrease in estimated infarct size.An increase in estimated infarct size was shown in
Table 1 Uptake of 99Tcm PyP in 103patients withsuspected acute myocardial infarction
99Tcm Pvp Definite Doubtfulinfarction* infarction*
Uptake 59 6No uptake 13 25
*Clinical, electrocardiographic, and enzyme criteria
Table 2 Uptake of 99Tcm PY/ and serum levels ofMBCKin 21 patients with suspected acute myocardial infarction
TCmT VVp MBCK isoenzymeRaised Normal
Uptake 16 1No uptake 3 1
4 and in 2 of these this was associated with furtherpain and a rise in serum enzymes. The results areset out in Table 5.Table 6 shows the relation between the 12 lead
electrocardiogram and 129Cs imaging in the diagnosisofmyocardial infarction and Table 7 the comparisonwith regard to the localisation of infarction in the23 patients with electrocardiographic evidence ofinfarction and defective 129Cs uptake. There is a
Table 3 Localisation of acute myocardial infarction in56patients with uptake of 9sTcm PYP and electrocardio-graphic evidence of acute infarction
O9Tcm DPy Electrodardiographic localisationlocalisation Anterior Inferior Anterior and Inferior and
AS A AL inferior posterior
Anterior 2 13 3 7 1 1Inferior 9 4Anterior and
inferior 4Inferior and
posterior 1 1 8 2
AS, anteroseptal; A, extensive anterior; AL, anterolateral.
877
on March 24, 2022 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.40.8.874 on 1 August 1978. D
ownloaded from
S. Walton, E. Kafetzakis, R. A. Shields, H. J7. Testa, and D. JI. Rowlands
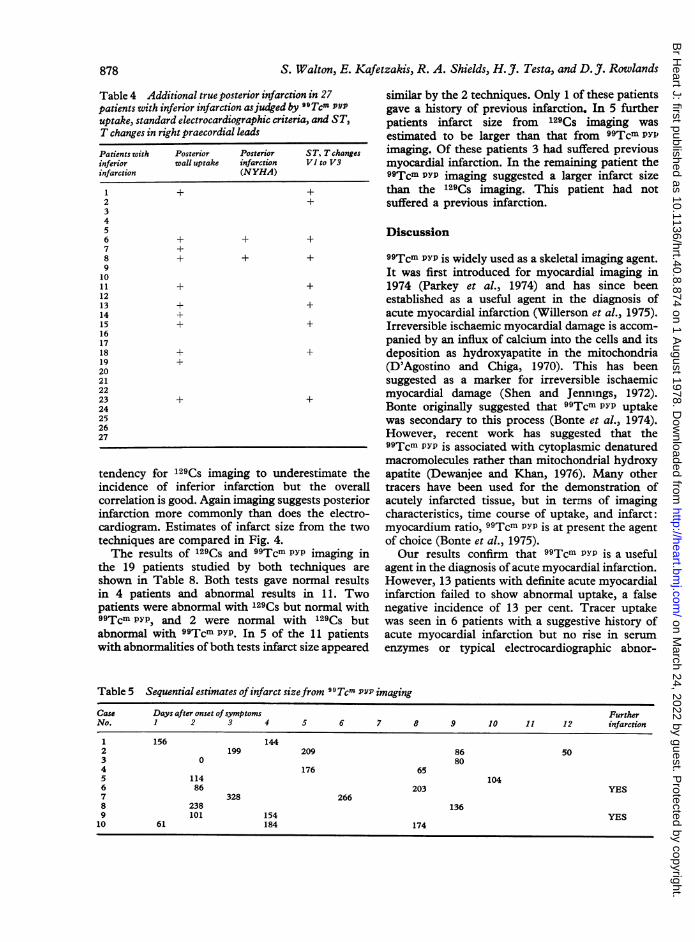
Table 4 Additional true posterior infarction in 27patients with inferior infarction asjudged by BOTcm pYPuptake, standard electrocardiographic criteria, and ST,T changes in right praecordial leads
Patients with Posterior Posterior ST, T changesinferior wall uptake infarction VI to V3infarction (NYHA)
1 + +2 +3456 + + +7 +8 + + +91011 + +1213 + +14 +15 + +161718 + +19 +20212223 + +24252627
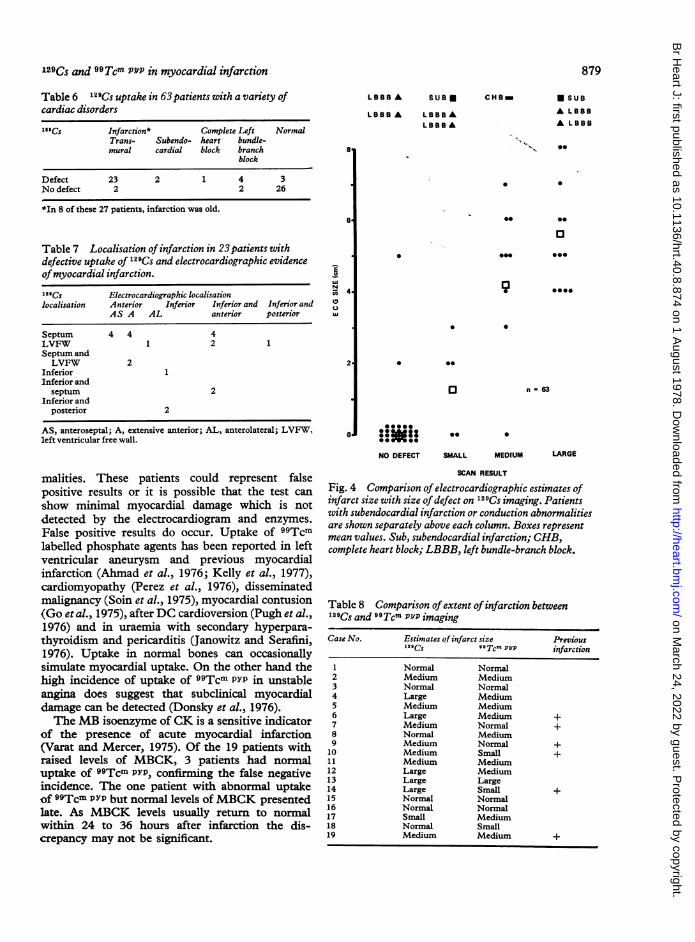
tendency for 129Cs imaging to underestimate theincidence of inferior infarction but the overallcorrelation is good. Again imaging suggests posteriorinfarction more commonly than does the electro-cardiogram. Estimates of infarct size from the twotechniques are compared in Fig. 4.The results of '29Cs and 99Tcm PYP imaging in
the 19 patients studied by both techniques areshown in Table 8. Both tests gave normal resultsin 4 patients and abnormal results in 11. Twopatients were abnormal with 129Cs but normal with99Tcm PYP, and 2 were normal with '29Cs butabnormal with 99Tcm PYP. In 5 of the 11 patientswith abnormalities of both tests infarct size appeared
similar by the 2 techniques. Only 1 of these patientsgave a history of previous infarction. In 5 furtherpatients infarct size from 129Cs imaging was
estimated to be larger than that from 99Tcm Pyxrimaging. Of these patients 3 had suffered previousmyocardial infarction. In the remaining patient the99Tcm PYP imaging suggested a larger infarct sizethan the 129Cs imaging. This patient had notsuffered a previous infarction.
Discussion
99Tcm PYP is widely used as a skeletal imaging agent.It was first introduced for myocardial imaging in1974 (Parkey et al., 1974) and has since beenestablished as a useful agent in the diagnosis ofacute myocardial infarction (Willerson et al., 1975).Irreversible ischaemic myocardial damage is accom-panied by an influx of calcium into the cells and itsdeposition as hydroxyapatite in the mitochondria(D'Agostino and Chiga, 1970). This has beensuggested as a marker for irreversible ischaemicmyocardial damage (Shen and Jennings, 1972).Bonte originally suggested that 99Tcm PYP uptakewas secondary to this process (Bonte et al., 1974).However, recent work has suggested that the99Tcm PYP is associated with cytoplasmic denaturedmacromolecules rather than mitochondrial hydroxyapatite (Dewanjee and Khan, 1976). Many othertracers have been used for the demonstration ofacutely infarcted tissue, but in terms of imagingcharacteristics, time course of uptake, and infarct:myocardium ratio, 99Tcm PYP is at present the agentof choice (Bonte et al., 1975).Our results confirm that 99Tcm PYP is a useful
agent in the diagnosis of acute myocardial infarction.However, 13 patients with definite acute myocardialinfarction failed to show abnormal uptake, a falsenegative incidence of 13 per cent. Tracer uptakewas seen in 6 patients with a suggestive history ofacute myocardial infarction but no rise in serum
enzymes or typical electrocardiographic abnor-
Table 5 Sequential estimates ofinfarct sizefrom 99Tcm PYP imaging
Case Days after onset ofsymptoms FurtherNo. 1 2 3 4 5 6 7 8 9 10 11 12 infarction
1 156 1442 199 209 86 503 0 804 176 655 114 1046 86 203 YES7 328 2668 238 1369 101 154 YES10 61 184 174
878
on March 24, 2022 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.40.8.874 on 1 August 1978. D
ownloaded from
129Cs and 99Tcm PYP in myocardial infarction
Table 6 129Cs uptake in 63patients with a variety ofcardiac disorders
29Cs Infarction* Complete Left NormalTrans- Subendo- heart bundle-mural cardial block branch
block
Defect 23 2 1 4 3No defect 2 2 26
*In 8 of these 27 patients, infarction was old.
LBBB A SUB * CHB_
LBBB A LBBBALBBB A
8
6
Table 7 Localisation of infarction in 23patients withdefective uptake of 12"Cs and electrocardiographic evidenceofmyocardial infarction."29CS Electrocardiographic localisationlocalisation Anterior Inferior Inferior and Inferior and
AS A AL anterior posterior
Septum 4 4 4LVFW 1 2 1Septum andLVFW 2
Inferior 1Inferior and
septum 2Inferior and
posterior 2
AS, anteroseptal; A, extensive anterior; AL, anterolateral; LVFW,left ventricular free wall.
IC,
UN
0
Q
NO DEFECT SMALL
malities. These patients could represent falsepositive results or it is possible that the test canshow minimal myocardial damage which is notdetected by the electrocardiogram and enzymes.False positive results do occur. Uptake of 99Tcmlabelled phosphate agents has been reported in leftventricular aneurysm and previous myocardialinfarction (Ahmad et al., 1976; Kelly et al., 1977),cardiomyopathy (Perez et al., 1976), disseminatedmalignancy (Soin et al., 1975), myocardial contusion(Go et al., 1975), after DC cardioversion (Pugh et al.,1976) and in uraemia with secondary hyperpara-thyroidism and pericarditis (Janowitz and Serafini,1976). Uptake in normal bones can occasionallysimulate myocardial uptake. On the other hand thehigh incidence of uptake of 99Tcm PYP in unstableangina does suggest that subclinical myocardialdamage can be detected (Donsky et al., 1976).The MB isoenzyme of CK is a sensitive indicator
of the presence of acute myocardial infarction(Varat and Mercer, 1975). Of the 19 patients withraised levels of MBCK, 3 patients had normaluptake of 99Tcm PYP, confirming the false negativeincidence. The one patient with abnormal uptakeof 99Tcm PYP but normal levels ofMBCK presentedlate. As MBCK levels usually return to normalwithin 24 to 36 hours after infarction the dis-crepancy may not be significant.
MEDIUM LARGE
SCAN RESULT
Fig. 4 Comparison of electrocardiographic estimates ofinfarct size with size of defect on 129Cs imaging. Patientswith subendocardial infarction or conduction abnormalitiesare shown separately above each column. Boxes representmean values. Sub, subendocardial infarction; CHB,complete heart block; LBBB, left bundle-branch block.
Table 8 Comparison of extent ofinfarction between"12 Cs and 9 Tcm PYP imaging
Case No. Estimates of infarct size Previous129Cs 99cmT P/p infarction
1 Normal Normal2 Medium Medium3 Normal Normal4 Large Medium5 Medium Medium6 Large Medium +7 Medium Normal +8 Normal Medium9 Medium Normal +10 Medium Small +11 Medium Medium12 Large Medium13 Large Large14 Large Small +15 Normal Normal16 Normal Normal17 Small Medium18 Normal Small19 Medium Medium +
879
* SUB
A LBBBA LBBB
0.*-
* 0
0
OSe @000
*000
* 0
0 @*
0
:000
* *00 0
on March 24, 2022 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.40.8.874 on 1 August 1978. D
ownloaded from
S. Walton, E. Kafetzakis, R. A. Shields, H. J. Testa, and D. 7. Rowlands
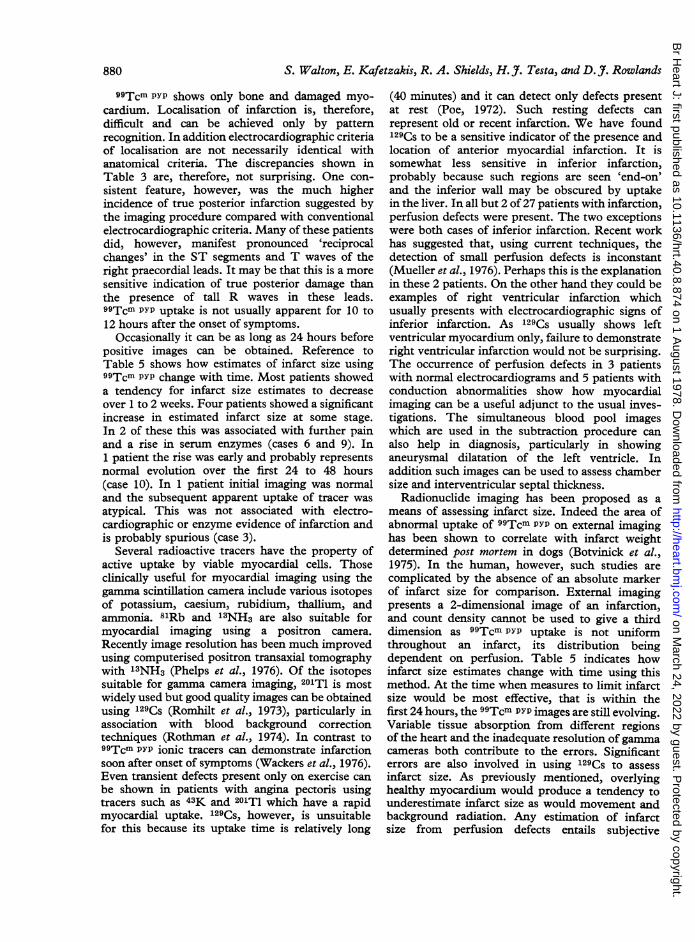
99Tcm PYP shows only bone and damaged myo-cardium. Localisation of infarction is, therefore,difficult and can be achieved only by patternrecognition. In addition electrocardiographic criteriaof localisation are not necessarily identical withanatomical criteria. The discrepancies shown inTable 3 are, therefore, not surprising. One con-sistent feature, however, was the much higherincidence of true posterior infarction suggested bythe imaging procedure compared with conventionalelectrocardiographic criteria. Many of these patientsdid, however, manifest pronounced 'reciprocalchanges' in the ST segments and T waves of theright praecordial leads. It may be that this is a moresensitive indication of true posterior damage thanthe presence of tall R waves in these leads.99Tcm PYP uptake is not usually apparent for 10 to12 hours after the onset of symptoms.
Occasionally it can be as long as 24 hours beforepositive images can be obtained. Reference toTable 5 shows how estimates of infarct size using99Tcm PYP change with time. Most patients showeda tendency for infarct size estimates to decreaseover 1 to 2 weeks. Four patients showed a significantincrease in estimated infarct size at some stage.In 2 of these this was associated with further painand a rise in serum enzymes (cases 6 and 9). In1 patient the rise was early and probably representsnormal evolution over the first 24 to 48 hours(case 10). In 1 patient initial imaging was normaland the subsequent apparent uptake of tracer wasatypical. This was not associated with electro-cardiographic or enzyme evidence of infarction andis probably spurious (case 3).
Several radioactive tracers have the property ofactive uptake by viable myocardial cells. Thoseclinically useful for myocardial imaging using thegamma scintillation camera include various isotopesof potassium, caesium, rubidium, thallium, andammonia. 81Rb and 13NH3 are also suitable formyocardial imaging using a positron camera.Recently image resolution has been much improvedusing computerised positron transaxial tomographywith 13NH3 (Phelps et al., 1976). Of the isotopessuitable for gamma camera imaging, 201T1 is mostwidely used but good quality images can be obtainedusing 129Cs (Romhilt et al., 1973), particularly inassociation with blood background correctiontechniques (Rothman et al., 1974). In contrast to99Tcm PYP ionic tracers can demonstrate infarctionsoon after onset of symptoms (Wackers et al., 1976).Even transient defects present only on exercise canbe shown in patients with angina pectoris usingtracers such as 43K and 201TI which have a rapidmyocardial uptake. 129Cs, however, is unsuitablefor this because its uptake time is relatively long
(40 minutes) and it can detect only defects presentat rest (Poe, 1972). Such resting defects canrepresent old or recent infarction. We have found129Cs to be a sensitive indicator of the presence andlocation of anterior myocardial infarction. It issomewhat less sensitive in inferior infarction,probably because such regions are seen 'end-on'and the inferior wall may be obscured by uptakein the liver. In all but 2 of27 patients with infarction,perfusion defects were present. The two exceptionswere both cases of inferior infarction. Recent workhas suggested that, using current teclmiques, thedetection of small perfusion defects is inconstant(Mueller et al., 1976). Perhaps this is the explanationin these 2 patients. On the other hand they could beexamples of right ventricular infarction whichusually presents with electrocardiographic signs ofinferior infarction. As 129Cs usually shows leftventricular myocardium only, failure to demonstrateright ventricular infarction would not be surprising.The occurrence of perfusion defects in 3 patientswith normal electrocardiograms and 5 patients withconduction abnormalities show how myocardialimaging can be a useful adjunct to the usual inves-tigations. The simultaneous blood pool imageswhich are used in the subtraction procedure canalso help in diagnosis, particularly in showinganeurysmal dilatation of the left ventricle. Inaddition such images can be used to assess chambersize and interventricular septal thickness.
Radionuclide imaging has been proposed as ameans of assessing infarct size. Indeed the area ofabnormal uptake of 99Tcm PYP on external imaginghas been shown to correlate with infarct weightdetermined post mortem in dogs (Botvinick et al.,1975). In the human, however, such studies arecomplicated by the absence of an absolute markerof infarct size for comparison. External imagingpresents a 2-dimensional image of an infarction,and count density cannot be used to give a thirddimension as 99Tcm PYP uptake is not uniformthroughout an infarct, its distribution beingdependent on perfusion. Table 5 indicates howinfarct size estimates change with time using thismethod. At the time when measures to limit infarctsize would be most effective, that is within thefirst 24 hours, the 99Tcm PYP images are still evolving.Variable tissue absorption from different regionsof the heart and the inadequate resolution ofgammacameras both contribute to the errors. Significanterrors are also involved in using 129Cs to assessinfarct size. As previously mentioned, overlyinghealthy myocardium would produce a tendency tounderestimate infarct size as would movement andbackground radiation. Any estimation of infarctsize from perfusion defects entails subjective
880
on March 24, 2022 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.40.8.874 on 1 August 1978. D
ownloaded from
129Cs and 99Tcm PYP in myocardial infarction
assessment of the original mass of myocardium.Such estimates necessarily include old as well asrecent infarction and it has been reported thatperfusion defects resulting from myocardial in-farction tend to diminish or disappear over thefirst 24 hours after infarction (Wackers et al., 1976).Whatever this process represents it makes inter-pretation of the effects of intervention difficult.These factors do not necessarily preclude theassessment of infarct size using radionuclidemethods. Indeed we showed a reasonable correlationbetween 129CS imaging and the electrocardiogramin such assessments. They do, however, limit theaccuracy with which these measurements can bemade.
Perhaps of more relevance to the individual thanthe size of any particular acute episode is theextent of remaining viable myocardium. Ionictracers are well suited for this as they show healthyperfused tissue and do not distinguish old fromrecent damage.The combination of 99Tcm PYP with agents that
show myocardial perfusion has been reported.Nishimura using 43K and 201Tl concluded that thedemonstration of myocardial perfusion helped toconfirm or exclude the presence of acute myocardialinfarction and to improve accuracy in localisinginfarction (Nishimura et al., 1975). He made nocomparison of infarct size. Parkey using 201Tlfound that the combination offered a clearer pictureof the extent of myocardial damage and possiblyprognosis (Parkey et al., 1974). Sizing was comparedafter subjective assessment. Any comparison ofinfarct size must be seen in the context of isotopedistribution. Zaret et al. (1976), using 43K, found agood correlation with regional myocardial bloodflow (RMBF) as assessed by 51Chromium micro-spheres. 99Tcm PYP uptake increased as RMBFdecreased down to a value of 40 per cent of normalRMBF. Below this value, however, uptake decreasedas RMBF decreased. Indeed, over the centre of theinfarcted zone uptake was mainly in the less severelyaffected subepicardium (Zaret et al., 1976). Thissuggests that 99Tcm PYP uptake occurs in ischaemicas well as necrotic tissue. Taken in conjunctionwith the fact that defects of 129CS uptake may beminimised by overlying healthy tissue and move-ment, we can understand the one patient in whomestimated infarct size using 99Tcm PYP appearedlarger than that from 129CS imaging, and the twopatients with normal 129Cs appearances but uptakeof 99Tcm PYP typical of acute myocardial infarction.However, these factors tend to underestimate anydifference resulting from previous infarction. Thismakes the group who had suffered previous infarc-tion particularly interesting. All these patients had
881
defective uptake of 129Cs. In 2 patients there wasnormal uptake of 99Tcm PYP and in 3 estimatedinfarct size using 99TcP PYP was smaller than thatusing 129Cs. The 2 estimates agreed in 1 patient.It is tempting to suppose that this discrepancy maybe reflecting the previous damage. Two patientswith no previous history of myocardial infarctionalso had larger estimates of infarct size using 129Csthan using 99Tcm PYP. Unfortunately the electro-cardiogram in one of these showed left bundle-branch block and was ofno help in deciding whetheror not previous damage had occurred. The otherpatient had extensive acute anterior and inferiorinfarction on the electrocardiogram. The resultsin the case of this patient might represent under-estimation of the extent of a large infarction using99Tcm PYP. This would be explained by poordelivery of tracer to regions with severely compro-mised perfusion.
Conclusion
The relatively high incidence of false positive andfalse negatives associated with the 99Tcm PYP testand the fact that it does not become positive forsome time after the actual infarction mean that it isnot demonstrably superior, in general, to currentinvestigative methods (electrocardiogram and en-zymes), though it is helpful in certain patients,particularly those with true posterior infarction.The ionic tracer technique has a lower incidence
of false positives and false negatives and is alsomore likely to show evidence of true posteriorinfarction than the electrocardiogram. It does not,however, distinguish between recent and old in-farction.The combination of the two techniques provides
more useful information than either alone. Inaddition to clarifying equivocal results, roughestimates of infarct size can be determined by eithertechnique. The ionic imaging may underestimatethe extent of non-viable myocardium, whereas the99Tcm PYP technique may exaggerate the apparentarea of recent infarction perhaps by includingischaemic but non-necrotic areas. Where there isno previous infarction, a combined assessment bythe two techniques may provide a more reliableindication of infarct size. In the presence ofpreviousinfarction the estimates of total infarct size using99Tcm PYP tend to be lower than those using 129Cs,the difference, in part at least, probably representingthe extent of earlier necrosis. While significantobjections still exist to the application of thesetechniques to the assessment of intervention in theacute phase of myocardial infarction, the extent of
on March 24, 2022 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.40.8.874 on 1 August 1978. D
ownloaded from
S. Walton, E. Kafetzakis, R. A. Shields, H. J. Testa, and D. J. Rozwlands
remaining viable myocardium as measured by 129Csmay be of prognostic significance.
It is important that the value of these new anduseful techniques should not be exaggerated.
References
Ahmad, M., Dubiel, J. P., Verdon, T. A., Jr., and Martin,R. H. (1976). Technetium 99m stannous pyrophosphatemyocardial imaging in patients with and without leftventricular aneurysm. Circulation, 53, 833-838.
Bonte, F. J., Parkey, R. W., Graham, K. D., and Moore, J. G.(1975). Distributions of several agents useful in imagingmyocardialinfarcts.journal of NuclearMedicine, 16,132-135.
Bonte, F. J., Parkey, R. W., Graham, K. D., Moore, J., andStokely, E. M. (1974). A new method for radionucideimaging of myocardial infarcts. Radiology, 110, 473-474.
Botvinick, E. H., Shames, D., Lappin, H., Tyberg, J. V.,Townsend, R., and Pormley, W. W. (1975). Noninvasivequantitation of myocardial infarction with technetium 99mpyrophosphate. Circulation, 52, 909-915.
D'Agostino, A. N., and Chiga, M. (1970). Mitochondrialmineralization in human myocardium. American Journal ofClinical Pathology, 53, 820-824.
Dewanjee, M. K., and Kahn, D. C. (1976). Mechanism oflocalisation of 9BmTc-labeled pyrophosphate and tetra-cycline in infarcted myocardium. Journal of NuclearMedicine, 17, 639-646.
Donsky, M. S., Curry, G. C., Parkey, R. W., Meyer, S. L.,Bonte, F. J., Platt, M. R., and Willerson, J. T. (1976).Unstable angina pectoris. Clinical angiographic and myo-cardial scintigraphic observations. British Heart Journal,38,257-263.
Go, R. T., Doty, D. B., Chiu, C. L., and Christie, H. (1975).A new method of diagnosing myocardial contusion in manby radionuclide imaging. Radiology, 116, 107-110.
Janowitz, W. R., and Serafini, A. N. (1976). Intense myo-cardial uptake of 99mTc diphosphonate in a uremic patientwith secondary hyperparathyroidism and pericarditis: casereport. Journal of Nuclear Medicine, 17, 896-898.
Kelly, R. J., Cowan, R. J., Maynard, C. D., Headley, R. N.,and Kahl, F. R. (1977). Localisation of onmTc stannouspyrophosphate in left ventricular aneurysms. Jrournal ofNuclear Medicine, 18, 342-345.
Mueller, T. M., Marcus, M. L., Ehrhardt, J. C., Chaudhuri,T., and Abboud, F. M. (1976). Limitations of thallium-201myocardial perfusion scintigrams. Circulation, 54, 640-646.
New York Heart Association (1973). Nomenclature andCriteria for the Diagnosis of Diseases of the Heart andGreat Vessels, 7th ed. Little, Brown, Boston.
Nishimura, A., Gortan, R. J., Kim, Y. A., and Williams, J. F.(1975). Dual radionuclide myocardial scanning for thediagnosis and location ofacute myocardial infarcts (abstract).Circulation, 51 and 52, Suppl. II, 223.
Parkey, R. W., Bonte, F. J., Meyer, S. L., Atkins, J. M.,Curry, G. L., Stokely, E. M., and Willerson, J. T. (1974).A new method for radionucide imaging of acute myocardialinfarction in humans. Circulation, 50, 540-546.
Parkey, R. W., Bonte, F. J., Stokely, E. M., Lewis, S. E.,Graham, K. D., Buja, L. M., and Willerson, J. T. (1976).Acute myocardial infarction imaged with n9mTc stannouspyrophosphate and 20'Tz: a clinical evaluation. Jrournal ofNuclear Medicine, 17, 771-779.
Perez, L. A., Hayt, D. B., and Freeman, L. M. (1976).Localization of myocardial disorders other than infarctionwith 99mTc-labeled phosphate agents. J7ournal of NuclearMedicine, 17,241-246.
Phelps, M. E., Hoffman, E. J., Coleman, R. E., Welch, M. J.,Raichle, M. E., Weiss, E. S., Sobel, B. E., and Ter-Pogossian,M. M. (1976). Tomographic images of blood pool andperfusion in brain and heart. Journal of Nuclear Medicine,17, 603-612.
Poe, N. D. (1972). Comparative myocardial uptake andclearance characteristics of potassium and cesium. J7ournalof Nuclear Medicine, 13, 557-560.
Pugh, B. R., Buja, L. M., Parkey, R. W., Poliner, L. R.,Stokely, E. M., Bonte, F. J., and Willerson, J. T. (1976).Cardioversion and 'false positive' technetium-99m stannouspyrophosphate scintigrams. Circulation, 54, 399-403.
Romhidt, D. W., Adolph, R. J., Sodd, V. J., Levenson, N. I.,August, L. S., Ni4Nyama, H., and Berke, R. A. (1973).Cesium-129 niyomia1 scintigraphy to detect myocardialinfarction. Circulation, 48, 1242-1251.
Rothman, M. T., Critchley, M., Shail, G., Shields, R. A.,Testa, H. J., and Rowlands, D. J. (1974). Myocardialscanning using 129Cs (abstract). British Heart_Journal, 36,1035.
Selvester, R. H., Wagner, J. O., and Rubin, H. B. (1972).Quantitation of myocardial infarct size and location byelectrocardiogram and vectorcardiogram. In Quantitationin Cardiology, pp. 31-44. Ed. by H. A. Snellen, H. C.Hemberg, P. G. Hugenholz, and J. H. Van Bemmel.Leiden University Press, Leiden.
Shen, A. C., and Jennings, R. B. (1972). Kinetics of calciumaccumulation in acute myocardial ischemic injury. AmericanJ7ournal of Pathology, 67, 441-452.
Soin, J. S., Burdine, J. A., and Beal, W. (1975). Myocardiallocalization of 99mTc-pyrophosphate without evidence ofacute myocardial infarction. J'ournal of Nuclear Medicine,16,944-946.
Varat, M. A., and Mercer, D. W. (1975). Cardiac specificcreatine phosphokinase isoenzyme in the diagnosis of acutemyocardial infarction. Circulation, 51, 855-859.
Wackers, F. J. T., Sokole, E. B., Samson, G., Schoat,J. B. van der, Lie, K. I., Liem, K. L., and Wellens, H. J. J.(1976). Value and limitations of Thallium-201 scintigraphyin the acute phase of myocardial infarction. New EnglandJ'ournal of Medicine, 295, 1-5.
Willerson, J. T., Parkey, R. W., Bonte, F. J., Meyer, S. L.,Atkins, J. M., and Stokely, E. M. (1975). Technetiumstannous pyrophosphate myocardial scintigrams in patientswith chest pain of varying etiology. Circulation, 51,1046-1052.
Zaret, B. L., DiCola, V. C., Donabedian, R. K., Puri, S.,Wolfson, S., Freedman, G. S., and Cohen, L. S. (1976).Dual radionucide study of myocardial infarction. Relation-ships between myocardial uptake of potassium-43, tech-netium-99m stannous pyrophosphate, regional myocardialblood flow and creatine phosphokinase depletion. Circula-tion, 53, 422-428.
Requests for reprints to S. Walton, Department ofCardiology, Manchester Royal Infirmary, OxfordRoad, Manchester M13 9WL.
882
on March 24, 2022 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.40.8.874 on 1 August 1978. D
ownloaded from

![Ceramics based on calcium pyrophosphate nanopowders 19 02.pdf · 9 Processing and Application of Ceramics 7 [1] (2013) 9–14 Ceramics based on calcium pyrophosphate nanopowders Tatiana](https://img.pdfslide.us/doc/110x75/5eda4b32b3745412b571196b/ceramics-based-on-calcium-pyrophosphate-19-02pdf-9-processing-and-application.jpg)



























