Embed Size (px)
Citation preview

ORIGINAL RESEARCH
Usability of Nasal Glucagon Device: PartiallyRandomized Caregiver and Third-Party UserExperience Trial with Simulated Administrationat a Japanese Site
Toshihiko Aranishi . Yukiko Nagai . Yasushi Takita .
Shuyu Zhang . Rimei Nishimura
Received: July 11, 2019 / Published online: November 4, 2019� Eli Lilly and Company 2019
ABSTRACT
Introduction: Glucagon is the only approvedmedicine for severe hypoglycemia available forcaregivers of people with diabetes. Nasal gluca-gon (NG) was recently approved in the USA as aneedle-free, ready-to-use alternative to
injectable glucagon. This simulated user expe-rience study in Japan compared NG and intra-muscular glucagon (IMG) administration bycaregivers, and NG administration by untrainedthird parties.Methods: This was an open-label, single-center,partially randomized crossover, simulated userexperience trial conducted in Japan (October2018 to December 2018). Caregivers who livewith and care for a relative with diabetes wererandomized (1:1, stratified by patient diabetestype 1 or 2) to one of two simulated adminis-tration sequences (group 1: NG then IMG;group 2: IMG then NG). Caregivers receivedtraining on each device 2 weeks before simu-lated administration of the device. Third partiesreceived no training and only conducted simu-lated NG administration. Outcome measuresincluded the percentage of successful adminis-trations (based on critical step completion anddose; primary outcome), time to completeadministration, and user satisfaction/preferences.Results: In caregivers (N = 19), the percentageof successful administrations was greater (89.5%vs 26.3%, P\ 0.001) and mean time to com-plete administration was shorter (23.9 vs207.3 s, P\ 0.001) with NG than with IMG. Inthird parties (N = 20), 95% of NG administra-tion attempts were successful (mean time tocomplete administration, 55.5 s). All caregiversand 80% of third parties reported that the NGdevice was easy to use. All caregivers and 70% of
Enhanced Digital Features To view enhanced digitalfeatures for this article go to https://doi.org/10.6084/m9.figshare.9784958.
Electronic supplementary material The onlineversion of this article (https://doi.org/10.1007/s13300-019-00711-1) contains supplementary material, which isavailable to authorized users.
T. Aranishi (&)Health Outcomes/Health Technology Assessment/Real World Evidence, Medicines Development Unit-Japan, Eli Lilly Japan K.K., Kobe, Japane-mail: [email protected]
Y. NagaiDiabetes Products, Medicines Development Unit-Japan, Eli Lilly Japan K.K., Kobe, Japan
Y. TakitaStatistical Science, Medicines Development Unit-Japan, Eli Lilly Japan K.K., Kobe, Japan
S. ZhangGlobal Statistics and Science, Eli Lilly and Company,Indianapolis, IN, USA
R. NishimuraDivision of Diabetes, Metabolism andEndocrinology, Department of Internal Medicine,The Jikei University Hospital, Tokyo, Japan
Diabetes Ther (2020) 11:197–211
https://doi.org/10.1007/s13300-019-00711-1

third parties were confident and willing to usethe device in a real emergency, and more than80% of caregivers preferred the NG device toIMG.Conclusion: This simulated user experiencestudy confirmed that glucagon administrationusing a nasal delivery device was quicker, easier,and had a higher success rate than intramus-cular administration in Japan, where the glu-cagon injection kit is not available.Funding: Eli Lilly.Plain Language Summary: Plain languagesummary available for this article.
Keywords: Administration; Caregivers; Diabetesmellitus; Glucagon; Hypoglycemia; Intranasal;Intranasal administration; Patient preference
Key Summary Points
Nasal glucagon (NG) is currently beingdeveloped as a needle-free, ready-to-usealternative to injectable glucagon for useby caregivers for the treatment of severehypoglycemia in patients with diabetes.
In this simulated user experience trialconducted in Japan, we hypothesized thatthe NG device would be faster and moreaccurate when used by caregivers,compared with intramuscular glucagon(IMG) administration.
We also hypothesized that the NG devicecould be used successfully by untrainedthird parties.
Both the speed and the rate of successfulglucagon administration weresignificantly greater with the NG devicethan with IMG injection, and caregiversstrongly preferred using the NG deviceover IMG.
The availability of a nasal glucagondelivery device would likely increase thewillingness of patients and their caregiversto keep glucagon with them andadminister it in the event of a severehypoglycemic episode.
PLAIN LANGUAGE SUMMARY
Glucagon is a drug used to treat people withdiabetes when they have very low blood sugarlevels (severe hypoglycemia), which can lead tounconsciousness. However, injection of gluca-gon into muscle (e.g., in the hip) using a needleand syringe takes multiple steps and can beconfusing and difficult for caregivers ofpatients, especially in an emergency. In thisstudy, we tested a new way to give glucagonusing a needle-free, ready-to-use device thatreleases drug into a patient’s nose. The studywas done in Japan and involved relatives ofpeople with diabetes (caregivers) who weretrained on injecting glucagon into muscle andon using the nasal device before trying it on amanikin 2 weeks later. The study also included‘‘third parties’’ who did not have a relative withdiabetes and who were tested on the nasaldevice without any training. In the caregivergroup, the nasal device was quicker, easier, andhad a higher success rate (delivering an effectivedose) than injection. Third parties could alsouse the nasal device successfully. In a ques-tionnaire, all caregivers and most third partiescommented that the nasal device was easy touse, and they were confident and willing to useit in an emergency. When asked to compare thetwo methods, caregivers strongly preferred thenasal device to injections. These results suggestthat a nasal device might make people withdiabetes more likely to keep glucagon withthem and their caregivers more likely to use itwhen needed.
INTRODUCTION
Severe hypoglycemia is a serious condition thatcan occur in patients with type 1 (T1D) or type 2diabetes (T2D). By definition, hypoglycemia isconsidered severe when the patient cannot self-treat through carbohydrate ingestion and mustrely on others to provide assistance [1]. If nottreated, severe hypoglycemia can result inreduced cognitive function, unconsciousness,seizures, and, if prolonged, coma and death[2, 3]. Moreover, fear of hypoglycemia adversely
198 Diabetes Ther (2020) 11:197–211

affects quality of life for the majority of patientsand their caregivers [4–6].
Glucagon is the only approved medicine forsevere hypoglycemia available for use [1, 7] bycaregivers in Japan. Currently available gluca-gon must be administered by intramuscularinjection for the treatment of hypoglycemia,which involves multiple steps that can be con-fusing, as well as daunting, to caregivers. In asimulation study, 69% of parents of children orteenagers with diabetes had difficulty handlingthe components required to prepare for gluca-gon injection, and often injected less than a fulldose [8]. Although training in intramuscularglucagon (IMG) administration is recom-mended [7], caregivers do not always receiveinstructions and few have hands-on training[8]. Glucagon for intramuscular injection isavailable in kit form in many countries; how-ever, this is not the case in Japan. Instead, glu-cagon powder, diluent, syringes, and needlesrequired for IMG administration are onlyavailable as separate components. This increasesthe complexity of preparing glucagon forintramuscular injection and may also increasethe chance of mistakenly administering otherdrugs such as insulin in an emergency. Thereluctance of caregivers to inject glucagon maycontribute to the low possession rate for gluca-gon in Japan [9].
Nasal glucagon (NG) has recently beenapproved in the USA, and is under considera-tion in other countries, for emergency treat-ment of severe hypoglycemia as a needle-free,ready-to-use alternative to IMG (Fig. 1; video inelectronic supplementary material). Nasal glu-cagon has been shown to have similar efficacyto IMG for the treatment of severe hypo-glycemia in adults, children, and adolescentswith T1D, both when delivered by health careprofessionals in controlled trials [10–12] andwhen delivered by caregivers in non-medicalsettings [10–12]. Further, users of the NG devicein real-world situations reported that it was easyto use [13, 14]. A previous study conducted inCanada, in which caregivers and third partiessimulated glucagon administration using amanikin, indicated that the full dose of gluca-gon was achieved more frequently with NGthan with IMG [15]. The time and skill required
to inject IMG, and the relative improvementsprovided by a nasal delivery alternative, may beeven greater in Japan, where the glucagon kit isnot available.
The aim of the current simulation studyconducted in Japan was to compare NG andIMG administration by caregivers, and to assessNG administration by untrained third parties.We hypothesized that, compared with IMGadministration, the NG device would be faster,have a higher rate of successful administration,and be preferred by users.
METHODS
Study Design
This was an open-label, single-center, partiallyrandomized crossover, simulated user experi-ence trial conducted between October and
Fig. 1 Nasal glucagon device. Image copyright of Eli Lillyand Company
Diabetes Ther (2020) 11:197–211 199

December 2018 (first participant enrolledOctober 27, 2018; last participant completedDecember 22, 2018). The protocol was approvedby the ethics review committee of the study site(PS Clinic), and the study was conducted inaccordance with the principles of the Declara-tion of Helsinki, Ethical Guidelines for Medicaland Health Research Involving Human Subjectsin Japan [16], and all applicable laws and regu-lations. As this was a non-interventional trial,submission to a clinical trial registry was notrequired. All participants provided informedconsent before the start of the study.
Study Population
The trial enrolled two types of participants:caregivers and third parties. Caregivers weredefined as people who live with and care for arelative with diabetes and were assumed to haveknowledge of the therapeutic effect of glucagonfor severe hypoglycemia. Third parties weredefined as people who do not live with or carefor a person with diabetes and who have notbeen trained to administer glucagon. Men orwomen aged 20 years or more were eligible forenrollment. Caregivers were eligible for inclu-sion if they were first- or second-degree relativeswho lived with and cared for a patient with T1Dor T2D (if T2D, the patient must be treated withinsulin) who agreed not to learn how toadminister glucagon during the study, except aspart of the trial. Third parties were eligible forinclusion if they did not live with and care for arelative with diabetes. For both caregiver andthird-party cohorts, people who were diagnosedwith T1D or T2D, had previous experienceinjecting glucagon, were a health care provideror pharmaceutical company employee, or whowere judged by an investigator as having beensufficiently trained or educated to enable themto perform the simulated administration withease were excluded.
Study Protocol
CaregiversAt visit 1, enrolled caregivers were randomized[1:1, using a randomization table and stratified
by patient diabetes type (T1D or T2D)] to one oftwo simulated administration sequences:group 1 simulated glucagon administrationusing the NG device first, followed by IMG, andgroup 2 simulated IMG administration first,followed by the NG device. Randomizing thesequence of glucagon administration methodsin the two groups was intended to minimizeany potential learning effects between eachadministration device simulation. After ran-domization, caregivers were individuallytrained on their first device (NG or IMG). Healthcare providers (e.g., nurse or pharmacist)explained the steps involved in using the deviceand demonstrated its use. The order of criticalsteps was also explained. Caregivers did notperform simulated administration during thetraining session but could ask questions aboutadministration. There was no time limit on thetraining session. At visit 2 (14 ± 2 days later),caregivers performed simulated administrationusing their first assigned device. On the sameday, caregivers were trained on their seconddevice, as above. At visit 3 (14 ± 2 days aftervisit 2), caregivers performed simulated admin-istration using their second assigned device.
Third PartiesThird parties received information about thetherapeutic effect of glucagon on hypo-glycemia, but did not receive training on use ofthe device before simulated administration. Atvisit 1, enrolled third parties performed simu-lated administration using the NG device.
Simulated AdministrationAt the start of the simulation session, individualparticipants entered a room containing a multi-purpose manikin (model MW25 11404-000,Kyoto Kagaku Co., Ltd) lying supine on thefloor, an investigator, three evaluators (physi-cian, nurse, and/or pharmacist), a timekeeper,and a table with glucagon administrationequipment. For NG administration by care-givers, the table contained an NG device iden-tical to the commercially representative productbut without drug powder, a Humalog� Mir-ioPen� (KwikPen�) (Eli Lilly Japan K.K.), anInsulin Glargine BS Injection [Lilly]� cartridge
200 Diabetes Ther (2020) 11:197–211

(Eli Lilly Japan K.K.), and a 32-gauge needle (BDMicro-FineTM Plus). For IMG administration bycaregivers, the table contained Glucagon GNovo� 1 mg (Novo Nordisk Pharma Ltd.), aHumalog� MirioPen� (KwikPen�), an InsulinGlargine BS Injection [Lilly] cartridge, a32-gauge needle, a 2.5-mL disposable syringewith 23-gauge needle (Terumo syringe 2.5 mLwith 23G), and alcohol swabs. For both care-giver scenarios, the insulin products were pro-vided as decoys. For NG administration by thirdparties, the table contained only an NG deviceidentical to the commercially representativeproduct but without drug powder.
At the start of the simulated administration, theparticipant was told that the patient (i.e., themanikin) was unconscious as a result of severehypoglycemia and required emergency glucagontreatment. Immediately after the simulation star-ted, the timekeeper initiated loud sounds (ambu-lance siren and phone ringtone of approx. 80 dB)to add stress to the participant, as in a real emer-gency. Participants could not ask for instructionson how to administer glucagon during the simu-lation nor were printed instructions available;however, the NG package illustration was avail-able. The simulation ended when the participantcompleted or abandoned glucagon administra-tion, or if a caregiver administered insulin insteadof glucagon, or if 15 min had elapsed.
Outcome MeasuresThe primary study end point was the percentageof participants with successful administration ofglucagon by caregivers using each method.Administration was considered successful if allcritical steps (see Table S1 in the electronicsupplementary material) were completed cor-rectly (as judged by the majority of evaluators)and a full dose (100% for NG device, at least90% for IMG) was administered. Administrationwas considered partial (IMG only) if all criticalsteps were completed correctly, but a partialdose (greater than 0% and less than 90%) wasadministered. Administration was consideredfailed if not all critical steps were completedcorrectly, or if the dose was 0%, or if insulin wasadministered instead of glucagon.
Participant demographics and background(including patient background for caregivers,
with permission from the patients) wereobtained by interview at visit 1. Outcome mea-sures included the time needed to completeadministration (time from being asked to startsimulated administration to the end of simula-tion) and administration status (successful,partial, failed). For NG administration, inaccordance with the device’s characteristics, theadministered dose was considered to be 100% ifthe plunger was pushed in until the green linewas no longer visible; otherwise, the dose wasconsidered to be 0%. For IMG administration,the relative dose (i.e., percentage reduction inweight from before administration to afteradministration, based on the sum of the fulldose of 1000 mg, glucagon vial, solution vial,and syringe with needle) was calculated; dosesgreater than 0% and less than 90% were con-sidered partial doses, and doses of at least 90%were considered full doses. The time needed tocomplete administration was measured as thetime from when the participant was told to startadministration to the time when the participantremoved the NG device or needle from themanikin. If the time exceeded 15 min, or if theparticipant administered insulin or abandonedglucagon administration, the administrationwas considered incomplete.
After each simulation session, participantswere given a satisfaction questionnaire consist-ing of six questions regarding the specific glu-cagon device just used (see Table S2 in theelectronic supplementary material). Each ques-tion included the options ‘‘strongly agree’’,‘‘agree’’, ‘‘disagree’’, or ‘‘strongly disagree’’ asanswers. In addition, at the end of the secondsimulation, caregivers were given a user-prefer-ence questionnaire consisting of eight questionsregarding their preferences between the NG andIMG administration methods (see Table S3 inthe electronic supplementary material).
Statistical AnalysisWe aimed to enroll 20 caregivers (10 with a rela-tive with T1D, 10 with a relative with T2D) toensure that at least 16 caregivers completed thestudy. Assuming successful administration in94% and 13% of attempts for NG and IMG,respectively [15], this sample size would providegreater than 99% power to detect a statistically
Diabetes Ther (2020) 11:197–211 201

significant difference between NG and IMG witha two-sided alpha of 0.05. For balance, we aimedto enroll 20 participants in the third-party cohort.
Analyses were conducted on all caregivers whowere randomized and completed simulatedadministrationswithboth theNGdeviceand IMG,and on all third parties who completed the simu-lated NG administration. Comparisons betweenadministration methods within the caregivercohort were analyzed using the McNemar test(exact method) for categorical outcomes and theWilcoxon signed-rank test for continuous out-comes. Comparisons between the caregiver andthird-party cohorts for the NG device were ana-lyzed using the Fisher’s exact test for categoricaloutcomes and the Wilcoxon rank sum test forcontinuous outcomes. Time-to-event analyseswere conducted using the Kaplan–Meier method;participants who could not administer a dose orfailed the simulated administrationwere censored.Time to complete administration is reported asmean, standard deviation (SD), median, mini-mum, and maximum in minutes and in secondsfor administration attempts considered successfulor partial. Participants who could not administer adose or failed the simulated administration weretreated as censored at the maximum allowabletime (15 min). The percentage of participantscompleting successful/partial administration inless than 1 min, 1 min to less than 2min, 2 min toless than 3 min, 3 min to less than 5 min, and5 min to less than 10 min is also reported for eachcohort anddevice. Satisfactionanduser-preferencequestionnaire data are reported as the percentageofparticipantsgivingeachpossible answer for eachcohort and device, as applicable.
RESULTS
Participant Disposition and Demographicand Baseline Clinical Characteristics
Twenty participants were enrolled in both thecaregiver and third-party cohorts (Fig. 2). Onecaregiver randomized to administer NG first(group 1) withdrew by participant decision aftervisit 1 but before the first simulation. All otherparticipants completed the study.
In the caregiver cohort, participant charac-teristics in the two randomized groups were wellbalanced (Table 1). Most caregivers were women(80%), were the spouse of a patient with dia-betes (60%), and had not had previous experi-ence with severe hypoglycemia in the patient(85%). In contrast, there were equal numbers ofmen and women in the third-party cohort(Table 1).
Percentage of Successful SimulatedGlucagon Administrations
Within the caregiver cohort, the percentage ofsuccessful glucagon administrations was signif-icantly greater with NG than with IMG (89.5%vs 26.3%, P\0.001; Table 2). In the third-partycohort, 95% of NG administrations were suc-cessful; this percentage did not differ from thatin the caregiver cohort. The percentage of failedadministrations with IMG (15.8%) was numer-ically greater compared with NG (10.5%) in thecaregiver cohort, and compared with NG in thethird-party cohort (5.0%).
The reasons that caregivers failed simulatedadministration were (1) for the NG device, noglucagon delivered (two caregivers who did notpush the plunger completely), and (2) for theIMG device, gave up (two caregivers), incom-pletion of critical steps (three caregivers), andno glucagon delivered (two caregivers). Threecaregivers started to prepare insulin for injec-tion instead of glucagon, but none of the care-givers administered insulin during thesimulation. No caregivers or third-party partic-ipants started to prepare insulin for adminis-tration with the NG device. No caregiversattempted to administer insulin to the manikinfor either method.
Time to Administer Glucagon
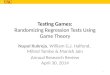
Within the caregiver cohort, the time requiredto complete successful or partial (IMG only)glucagon administration was significantlyshorter (P\0.001) with the NG device (mean23.9 s) than with IMG (mean 207.3 s; Table 3and Fig. 3a). Third parties required significantlylonger than caregivers for NG administration
202 Diabetes Ther (2020) 11:197–211

(mean 55.5 vs 23.9 s, respectively; Table 3 andFig. 3b). All caregivers and 63.2% of third par-ties completed NG administration within 1 min(Fig. 4). In contrast, no caregivers completedIMG administration within 1 min, and most(56.3%) required 3–5 min.
Device Preference
All caregivers and most third parties reported thatthe NG device was easy to use, they were confi-dent using the device during the simulation, andthey were confident and willing to use the devicein the event of a real emergency (Fig. 5). Allcaregivers and 70–100% of third parties answered‘‘agree’’ or ‘‘strongly agree’’ to the five positivelyworded questions with respect to the NG device.Note that all caregivers and 95% of third partiesanswered ‘‘disagree’’ or ‘‘strongly disagree’’ to theone negatively worded question (‘‘The glucagondelivery method is intimidating and difficult forcaregivers like me to use in case of an episode ofrescue of severe hypoglycemia’’). In contrast,caregivers were generally not as comfortable ad-ministering IMG, although there was some vari-ability in the responses (Fig. 5). Only 21% ofcaregivers said that they were confident they
could administer IMG during a real severe hypo-glycemic event. Most (70%) caregivers found theIMG administration method ‘‘intimidating anddifficult’’. However, 47% agreed that they wouldbe willing to use IMG in the event of an emer-gency, and 58% agreed that they would recom-mend their loved one have glucagon available.
When asked to directly compare the twomethods of glucagon administration, caregiversstrongly favored the NG device over IMG(Fig. 6). More than 80% of caregivers reportedthat they preferred the NG device in terms ofease, confidence, and willingness in using thedevice. In contrast, more than 70% of caregiversthought that IMG administration was unac-ceptable for successful rescue during a severehypoglycemic event.
DISCUSSION
This simulated user experience study confirmsand extends previous findings [15] that nasaladministration of glucagon is easier, quicker,and had a higher success rate than intramus-cular administration. This study is the first tocompare NG and IMG administration by
Fig. 2 Disposition of participants in the caregiver and third-party cohorts. NG nasal glucagon, IMG intramuscular glucagon
Diabetes Ther (2020) 11:197–211 203

Japanese caregivers and third parties. Mostcaregivers and third parties could use the NGdevice correctly and reported that they wereconfident in its use. These results suggest thatthe availability of a ready-to-use form of gluca-gon (i.e., NG device) in Japan may increase thenumber of patients with diabetes who keepglucagon on hand in case of emergency [9].
Both the speed and accuracy of glucagonadministration were significantly greater with
the NG device than with IMG. The high successrate with NG administration observed in thisstudy is consistent with the previous Canadiansimulation study, in which 15 of 16 (94%)caregivers and 14 of 15 (93%) third partiesdelivered a full dose of glucagon with the NGdevice [15]. In contrast, only a quarter of IMGadministration attempts by caregivers weresuccessful in our study, and many caregiversadministered only a partial dose by this route.
Table 1 Participant demographics and characteristics
Caregiver cohort Third-party cohort
Group 1a (N = 10) Group 2b (N = 10) Total (N = 20) (N = 20)
Both cohorts
Sex, n (%)
Female 8 (80.0) 8 (80.0) 16 (80.0) 10 (50.0)
Male 2 (20.0) 2 (20.0) 4 (20.0) 10 (50.0)
Age, years
Mean (SD) 49.5 (9.91) 47.3 (14.94) 48.4 (12.39) 44.3 (14.90)
Median (min, max) 50.0 (34, 66) 52.0 (23, 64) 50.0 (23, 66) 46.0 (21, 67)
Caregivers only
Relationship with the patient, n (%)
Spouse 6 (60.0) 6 (60.0) 12 (60.0) –
Child 4 (40.0) 3 (30.0) 7 (35.0) –
Mother 0 (0.0) 1 (10.0) 1 (5.0) –
Patient diabetes type, n (%)
Type 1 5 (50.0) 5 (50.0) 10 (50.0) –
Type 2 5 (50.0) 5 (50.0) 10 (50.0) –
Patient diabetes duration, years
Mean (SD) 15.5 (14.39) 12.2 (7.86) 13.9 (11.41) –
Median (min, max) 14.0 (1, 50) 11.5 (1, 22) 13.0 (1, 50) –
Experience with severe hypoglycemia in a cohabiting patient, n (%)
No 8 (80.0) 9 (90.0) 17 (85.0) –
Yes 2 (20.0) 1 (10.0) 3 (15.0) –
max maximum, min minimum, SD standard deviationa Group 1: nasal glucagon ? intramuscular glucagonb Group 2: intramuscular glucagon ? nasal glucagon
204 Diabetes Ther (2020) 11:197–211

Interestingly, the percentages of successful andpartial IM glucagon administrations in ourstudy (26.3% and 57.9%, respectively) werehigher than in the Canadian study (13% and38%, respectively). Possible reasons for this dif-ference include the potentially higher level ofcommitment of Japanese participants and thedirect training from health care professionalsthat caregivers received, as would normallyoccur in Japan, whereas the Canadian studytrained patients who then described the
method to their caregivers. The third-partycohort was intended to simulate acquaintancesor bystanders who would not typically have anytraining or experience administering glucagon.The training given to caregivers in our study,and the lack of training given to third parties,was intended to simulate these real-lifecircumstances.
In this study, all caregivers and most thirdparties could successfully complete NG admin-istration in less than a minute, whereas IMG
Table 2 Percentage of participants with successful, partial, or failed simulated administration
Caregiver cohort Third-party cohort
NG (N = 19) IMG (N = 19) NG (N = 20)
Administration outcome, n (%)
Successful 17 (89.5) 5 (26.3) 19 (95.0)
Partial NA 11 (57.9) NA
Failed 2 (10.5) 3 (15.8) 1 (5.0)
P value vs caregiver NG \ 0.001a 0.605b
IMG intramuscular glucagon, NA not applicable, NG nasal glucagona McNemar test (exact method)b Fisher’s exact test
Table 3 Time required to complete administration (successful or partial)
Caregiver cohort Third-party cohort
NG (N = 19) IMG (N = 19) NG (N = 20)
Time to administer glucagon (min)
n 17 16 19
Mean (SD) 0.399 (0.1015) 3.455 (1.2232) 0.925 (0.5259)
Median (min, max) 0.383 (0.23, 0.62) 3.350 (1.68, 6.02) 0.783 (0.33, 2.50)
Time to administer glucagon (s)
n 17 16 19
Mean (SD) 23.9 (6.09) 207.3 (73.39) 55.5 (31.56)
Median (min, max) 23.0 (14, 37) 201.0 (101, 361) 47.0 (20, 150)
P value vs caregiver NG \ 0.001a \ 0.001b
NG nasal glucagon, IMG intramuscular glucagon, SD standard deviation, max maximum, min minimuma Wilcoxon signed-rank testb Wilcoxon rank sum test
Diabetes Ther (2020) 11:197–211 205

administration by caregivers took an average ofabout 3.5 min. In the Canadian study, theaverage administration times required by care-givers for both NG (16 s) and IMG (1.89 min)were shorter than the times observed in ourstudy [15]. The longer administration timesobserved in our study for the NG device are
likely related to the shrink-wrap packaging and,for IMG, is likely related to the additional stepsrequired to assemble the separate componentsfor injection, as opposed to the glucagon kitused in the Canadian study [15]. Notably, dur-ing the IMG simulation, three caregivers startedto prepare insulin for injection, although none
Fig. 3 Time-to-event analyses for the time needed to complete successful and partial simulated administrations. NG nasalglucagon, IMG intramuscular glucagon
Fig. 4 Distribution of time required to administer glucagon (successful and partial administration only). NG nasalglucagon, IMG intramuscular glucagon
206 Diabetes Ther (2020) 11:197–211

Diabetes Ther (2020) 11:197–211 207

actually tried to administer insulin. In theCanadian study, 5 of 16 (31%) caregivers actu-ally attempted to inject insulin, either insteadof or in addition to glucagon [15]. Providingglucagon in a nasal delivery device wouldminimize the potential for confusion betweenglucagon and insulin during a real emergency.
Both caregivers and third parties found theNG device easy to use. Caregiver responses tothe questionnaires were strongly positive aboutthe NG device compared with the IMG admin-istration. These results are consistent with thoseof the Canadian simulation study [15], as well asthose of real-world studies of the NG device, inwhich participants indicated that the device
was easy to use [13, 14]. The possession rate forglucagon among patients with T1D in Japan isreportedly very low (15.9%), mostly becausepatients do not think they will need glucagon,but also because of reluctance by family mem-bers to inject [9]. Higher glucagon possessionrates have been reported in Australia (92%) [8],Israel (60%) [17], Croatia (45%) [18], and theUSA (49%) [19]; this difference may reflect thelack of a glucagon kit in Japan, the older age ofpatients in this study (most other studies wereof pediatric patients), or cultural factors.Because the NG device is ready to use and is lessintimidating than using a syringe and needlefor IMG injection, availability of the NG devicemay help increase the number of patients whokeep glucagon on hand.
Strengths of this study include the random-ized, crossover study design (caregiver cohort),sufficient statistical power to assess the primaryobjective, inclusion of a third-party cohort toexamine use of the NG device in the absence ofany training, and measurement of both objective
bFig. 5 User satisfaction with the NG and IMG admin-istration methods. Shown are the percentages of partici-pants who responded ‘‘strongly agree’’, ‘‘agree’’, ‘‘disagree’’,or ‘‘strongly disagree’’ to six questions for each cohort/device. Note that question 4 was a negatively wordedquestion. NG nasal glucagon, IMG intramuscular glucagon
Fig. 6 Caregiver preferences for the NG or IMG admin-istration methods. Shown are the percentages of caregiverswho responded ‘‘NG device’’, ‘‘IMG’’, or ‘‘same’’ for
questions a–g, and ‘‘NG device’’, ‘‘IM glucagon’’, ‘‘same’’,‘‘neither’’, or ‘‘both’’ for question h. NG nasal glucagon,IMG intramuscular glucagon
208 Diabetes Ther (2020) 11:197–211

(success rate, time to completion) and subjective(satisfaction and user-preference) outcomes.However, it should be acknowledged that thiswas a simulation study that could not exactlyreplicate a real-life emergency, including thestress and fear of the situation, and where thetime elapsed between training and administra-tion of glucagon in a real-life emergency is likelyto be longer. Further, as drug administration by athird party is prohibited by the Medical Practi-tioners’ Act in Japan, we did not test the use ofIMG by third parties. Under this condition, itwas not appropriate to conduct a simulatedadministration study using IMG in third partieswithout training, considering the risk of acci-dental needlestick injury. In contrast, becauseNG can be administered easily without apparentsafety risks to the user, we could evaluate thepercentage of successful NG administration bythird parties who had no training. The study wasalso open-label out of necessity. All participantswere adults, and most caregivers looked after anadult patient with diabetes; the results may bedifferent for caregivers who look after a child orfor adolescents who might administer glucagon.Finally, the results with Japanese participantsmay not be applicable to people from othercountries, particularly because the glucagoninjection kit available in most other countries isnot available in Japan.
CONCLUSION
This simulation study confirmed that adminis-tration of glucagon using a nasal delivery devicewas quicker, easier, and successful more fre-quently than administration by intramuscularinjection in Japan, where the glucagon injec-tion kit is not available. The availability of anNG delivery device would likely increase thewillingness of patients and their caregivers tokeep glucagon with them and administer it inthe event of severe hypoglycemia.
ACKNOWLEDGEMENTS
The authors would like to thank all study par-ticipants, and physicians and staff at each
investigational site for their contributions tothis study.
Funding. This study was sponsored by EliLilly Japan K.K. (Kobe, Japan), developer of anasal glucagon device. Eli Lilly Japan K.K. wasinvolved in the study design, data collection,data analysis, and preparation of the manu-script, and funded the costs of Open Access. Allauthors had full access to all of the data in thisstudy and take complete responsibility for theintegrity of the data and accuracy of the dataanalysis.
Medical Writing and/or Editorial Assis-tance. Medical writing assistance was providedby Rebecca Lew, PhD, CMPP, and Luke Carey,PhD, CMPP of ProScribe—Envision PharmaGroup, and was funded by Eli Lilly Japan K.K.ProScribe’s services complied with internationalguidelines for Good Publication Practice (GPP3).
Authorship. All named authors meet theInternational Committee of Medical JournalEditors (ICMJE) criteria for authorship for thisarticle, take responsibility for the integrity ofthe work as a whole, and have given theirapproval for this version to be published.
Authorship Contributions. Toshihiko Aran-ishi, Yasushi Takita and Shuyu Zhang wereinvolved in the study design; Yukiko Nagai andRimei Nishimura were involved in data collec-tion; Yasushi Takita and Shuyu Zhang con-ducted the statistical analysis; and all authorswere involved in data interpretation.
Disclosures. Toshihiko Aranishi is anemployee and shareholder of Eli Lilly Japan K.K.or Eli Lilly and Company. Yukiko Nagai is anemployee and shareholder of Eli Lilly Japan K.K.or Eli Lilly and Company. Yasushi Takita is anemployee and shareholder of Eli Lilly Japan K.K.or Eli Lilly and Company. Shuyu Zhang is anemployee and shareholder of Eli Lilly andCompany. Rimei Nishimura has receivedspeaker honoraria from Astellas Pharma, Nip-pon Boehringer Ingelheim, Eli Lilly Japan K.K.,Kissei Pharmaceutical, Medtronic Japan, MSD,Novartis Pharma K.K., Novo Nordisk Pharma,
Diabetes Ther (2020) 11:197–211 209

Sanofi K.K., and Takeda Pharmaceutical, andcontract research fees for collaborative researchwith the Japan Diabetes Foundation.
Compliance with Ethics Guidelines. Theprotocol was approved by the ethics reviewcommittee of the study site (PS Clinic), and thestudy was conducted in accordance with theprinciples of the Declaration of Helsinki, EthicalGuidelines for Medical and Health ResearchInvolving Human Subjects in Japan [16], and allapplicable laws and regulations. As this was anon-interventional trial, submission to a clini-cal trial registry was not required. All partici-pants provided informed consent to participatebefore the start of the study.
Data Availability. Lilly provides access to allindividual participant data collected during thetrial, after anonymization, with the exception ofpharmacokinetic or genetic data. Data are avail-able to request 6 months after the indicationstudied has been approved in the USA and EUand after primary publication acceptance,whichever is later. No expiration date of datarequests is currently set once data are madeavailable. Access is provided after a proposal hasbeen approved by an independent review com-mittee identified for this purpose and after receiptof a signed data sharing agreement. Data anddocuments, including the study protocol, statis-tical analysis plan, clinical study report, and blankor annotated case report forms, will be providedin a secure data sharing environment. For detailson submitting a request, see the instructionsprovided at www.vivli.org.
Open Access. This article is distributedunder the terms of the Creative CommonsAttribution-NonCommercial 4.0 InternationalLicense (http://creativecommons.org/licenses/by-nc/4.0/), which permits any non-commercial use, distribution, and reproductionin any medium, provided you give appropriatecredit to the original author(s) and the source,provide a link to the Creative Commons license,and indicate if changes were made.
REFERENCES
1. American Diabetes Association. 6. Glycemic targets:standards of medical care in diabetes—2019. Dia-betes Care. 2019;42:S61–70.
2. Kalra S, Mukherjee JJ, Venkataraman S, et al.Hypoglycemia: the neglected complication. IndianJ Endocrinol Metab. 2013;17:819–34.
3. Villani M, de Courten B, Zoungas S. Emergencytreatment of hypoglycaemia: a guideline and evi-dence review. Diabet Med. 2017;34:1205–11.
4. Fidler C, Elmelund Christensen T, Gillard S. Hypo-glycemia: an overview of fear of hypoglycemia,quality-of-life, and impact on costs. J Med Econ.2011;14:646–55.
5. Nefs G, Pouwer F, Holt RIG, et al. Correlates andoutcomes of worries about hypoglycemia in familymembers of adults with diabetes: the second Dia-betes Attitudes, Wishes and Needs (DAWN2) study.J Psychosom Res. 2016;89:69–77.
6. Polonsky WH, Fisher L, Hessler D, Johnson N.Emotional distress in the partners of type 1 diabetesadults: worries about hypoglycemia and other keyconcerns. Diabetes Technol Ther. 2016;18:292–7.
7. Kedia N. Treatment of severe diabetic hypoglycemiawith glucagon: an underutilized therapeuticapproach. Diabetes Metab Syndr Obes.2011;4:337–46.
8. Harris G, Diment A, Sulway M, Wilkinson M. Glu-cagon administration—underevaluated and under-taught. Pract Diabetes Int. 2001;18:22–5.
9. Murata T, Okazaki K, Yanagisawa K, et al. Glucagonunderutilized among type 1 diabetes mellituspatients in Japan. Diabetes Technol Ther.2013;15:748–50.
10. Boido A, Ceriani V, Pontiroli AE. Glucagon forhypoglycemic episodes in insulin-treated diabeticpatients: a systematic review and meta-analysiswith a comparison of glucagon with dextrose and ofdifferent glucagon formulations. Acta Diabetol.2015;52:405–12.
11. Rickels MR, Ruedy KJ, Foster NC, et al. Intranasalglucagon for treatment of insulin-induced hypo-glycemia in adults with type 1 diabetes: a random-ized crossover noninferiority study. Diabetes Care.2016;39:264–70.
12. Sherr JL, Ruedy KJ, Foster NC, et al. Glucagon nasalpowder: a promising alternative to intramuscularglucagon in youth with type 1 diabetes. DiabetesCare. 2016;39:555–62.
210 Diabetes Ther (2020) 11:197–211

13. Deeb LC, Dulude H, Guzman CB, et al. A phase 3multicenter, open-label, prospective study designedto evaluate the effectiveness and ease of use of nasalglucagon in the treatment of moderate and severehypoglycemia in children and adolescents withtype 1 diabetes in the home or school setting.Pediatr Diabetes. 2018;19:1007–13.
14. Seaquist ER, Dulude H, Zhang XM, et al. Prospectivestudy evaluating the use of nasal glucagon for thetreatment of moderate to severe hypoglycaemia inadults with type 1 diabetes in a real-world setting.Diabetes Obes Metab. 2018;20:1316–20.
15. Yale JF, Dulude H, Egeth M, et al. Faster use andfewer failures with needle-free nasal glucagon ver-sus injectable glucagon in severe hypoglycemiarescue: a simulation study. Diabetes Technol Ther.2017;19:423–32.
16. Ministry of Education, Culture, Sports, Science andTechnology, and Ministry of Health, Labour andWelfare. Ethical guidelines for medical and health
research involving human subjects [in Japanese].2014. http://www.mhlw.go.jp/file/06-Seisakujouhou-10600000-Daijinkanboukouseikagakuka/0000069410.pdf. Accessed 4 April 2019.
17. Yanai O, Phillip M, Harman I, Elitzur-Leiberman E,Pilpel D. IDDM patients’ opinions on the use ofglucagon emergency kit in severe episodes ofhypoglycaemia. Pract Diabetes Int. 1997;14:40–2.
18. Vilovic M, Kurir TT, Novak A, et al. Hypoglycemiaand glucagon utilization in insulin-treated diabeticpatients. Exp Clin Endocrinol Diabetes. 2018.https://doi.org/10.1055/a-0741-6763.
19. Mitchell BD, He X, Sturdy IM, Cagle AP, Settles JA.Glucagon prescription patterns in patients witheither type 1 or 2 diabetes with newly prescribedinsulin. Endocr Pract. 2015;22:123–35.
Diabetes Ther (2020) 11:197–211 211