Embed Size (px)
Citation preview
US Evaluation of Truncal VeinsGSV, AAGSV, SSV
What to look for, measure and report.
Linda Antonucci, RPhS, RVT, RDCS
Disclosure
Linda Antonucci, RPhS, RVT, RDCS
I disclose the following financial relationship: I am a paid consultant for AngioDynamics
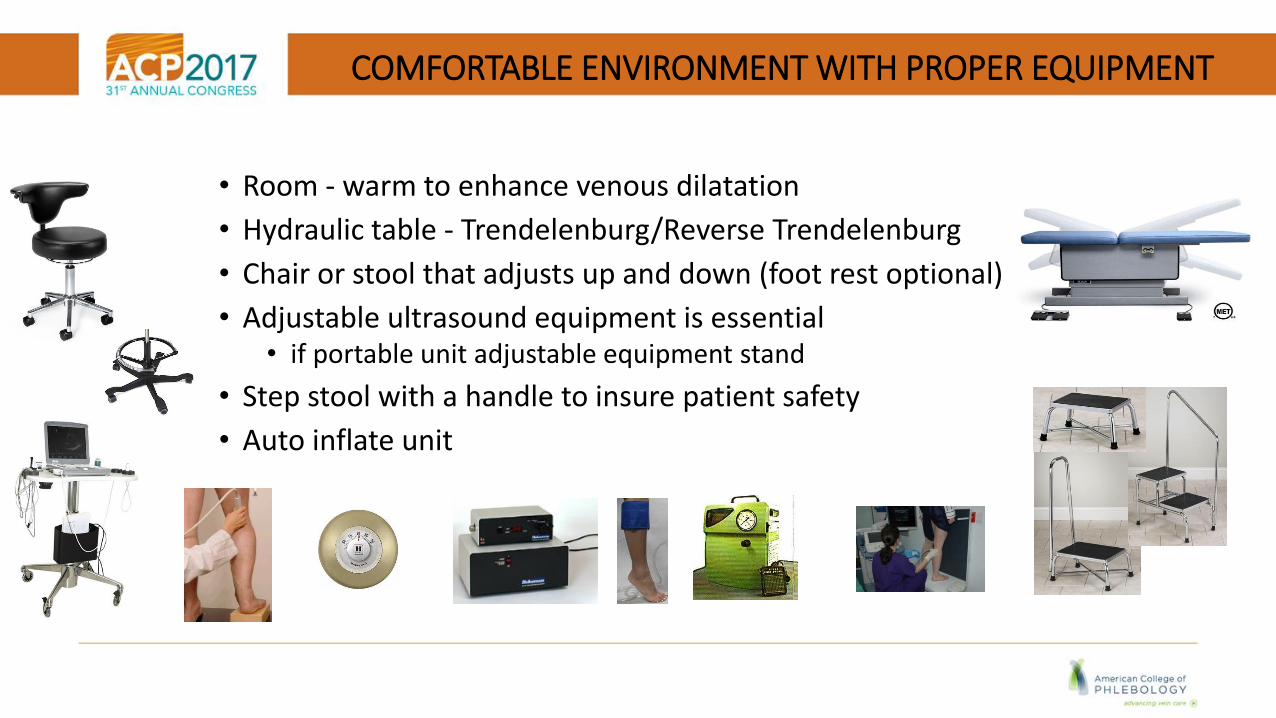
COMFORTABLE ENVIRONMENT WITH PROPER EQUIPMENT
• Room - warm to enhance venous dilatation
• Hydraulic table - Trendelenburg/Reverse Trendelenburg
• Chair or stool that adjusts up and down (foot rest optional)
• Adjustable ultrasound equipment is essential• if portable unit adjustable equipment stand
• Step stool with a handle to insure patient safety
• Auto inflate unit

BEFORE YOU BEGIN
• Do you have pain, aching, or heaviness in your legs?
• Does one leg bother you more than the other?
• Do your legs bother you more at the beginning or at the end of the day?
• Do you have swelling that worsens at the end of the day?
• Have you had any prior vein interventions?
• Have you ever had a DVT or SVT?
• Does anyone in your family have vein problems?
Photo courtesy of Daniella DePeri, PA
Ask a few Basic Questions Specific for SVI examDRAW visible varices while you CHAT
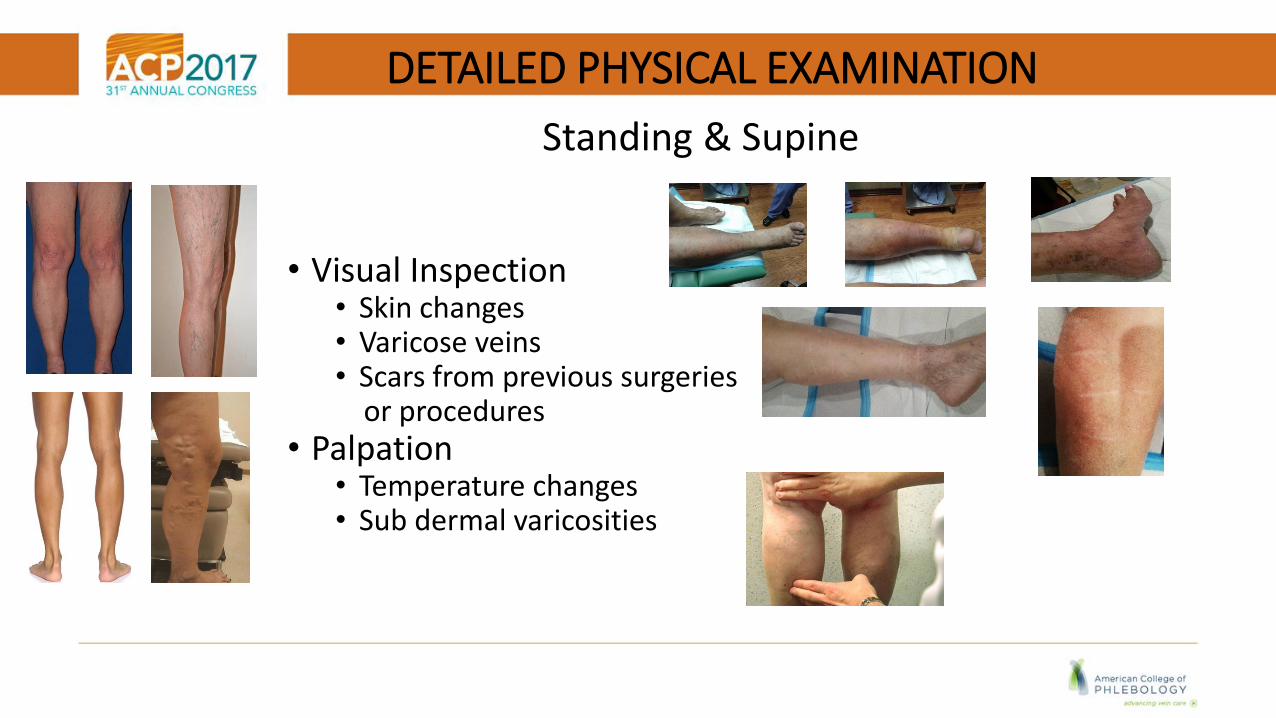
DETAILED PHYSICAL EXAMINATION
• Visual Inspection• Skin changes• Varicose veins• Scars from previous surgeries
or procedures• Palpation
• Temperature changes • Sub dermal varicosities
Standing & Supine

DEEP VEINS MATTER
• Perform a complete bilateral evaluation of the deep system
• Supine
• Reverse Trendelenburg >20 degrees
The calf veins, great saphenous vein and small saphenous are considered optional for a reflux evaluation, but should be included.
PATIENT POSITION FOR SUPERFICIAL VENOUS INSUFFICIENCY EVALUATION
STANDING
EXPERTS AGREESupine positionis unacceptable
Cartoon taken from www.cardstock.com
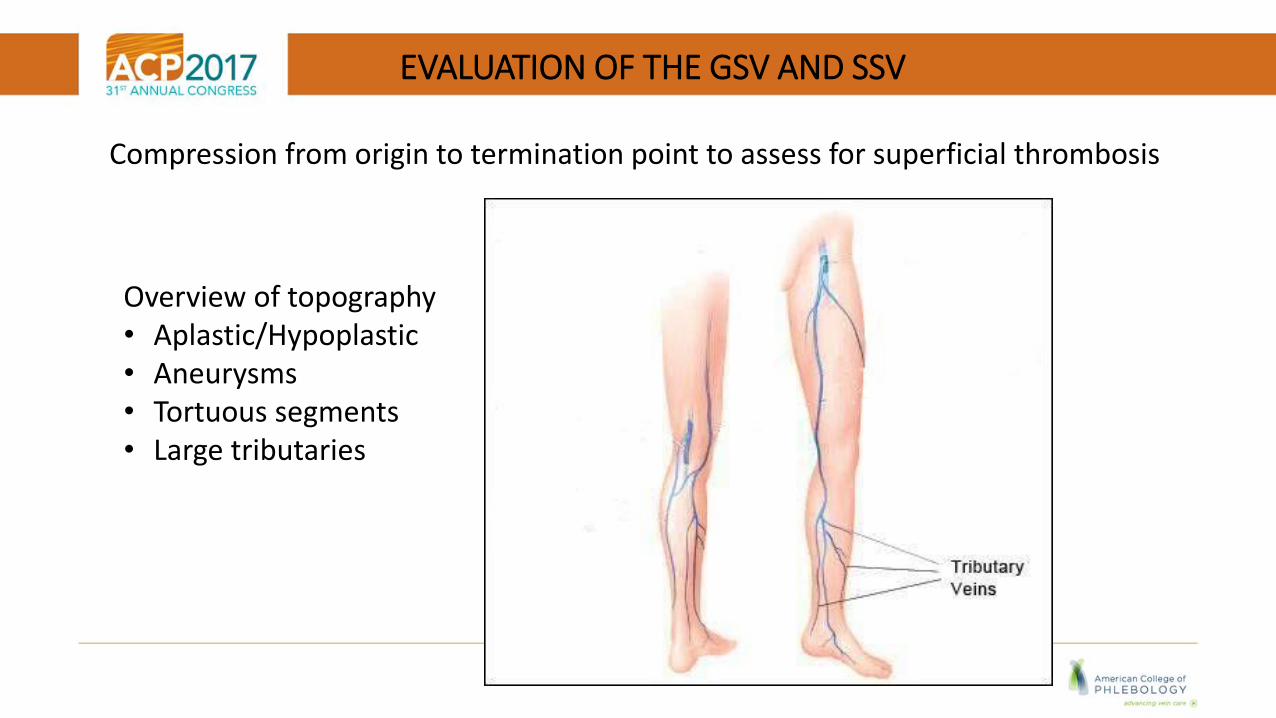
EVALUATION OF THE GSV AND SSV
Compression from origin to termination point to assess for superficial thrombosis
Overview of topography• Aplastic/Hypoplastic• Aneurysms• Tortuous segments• Large tributaries
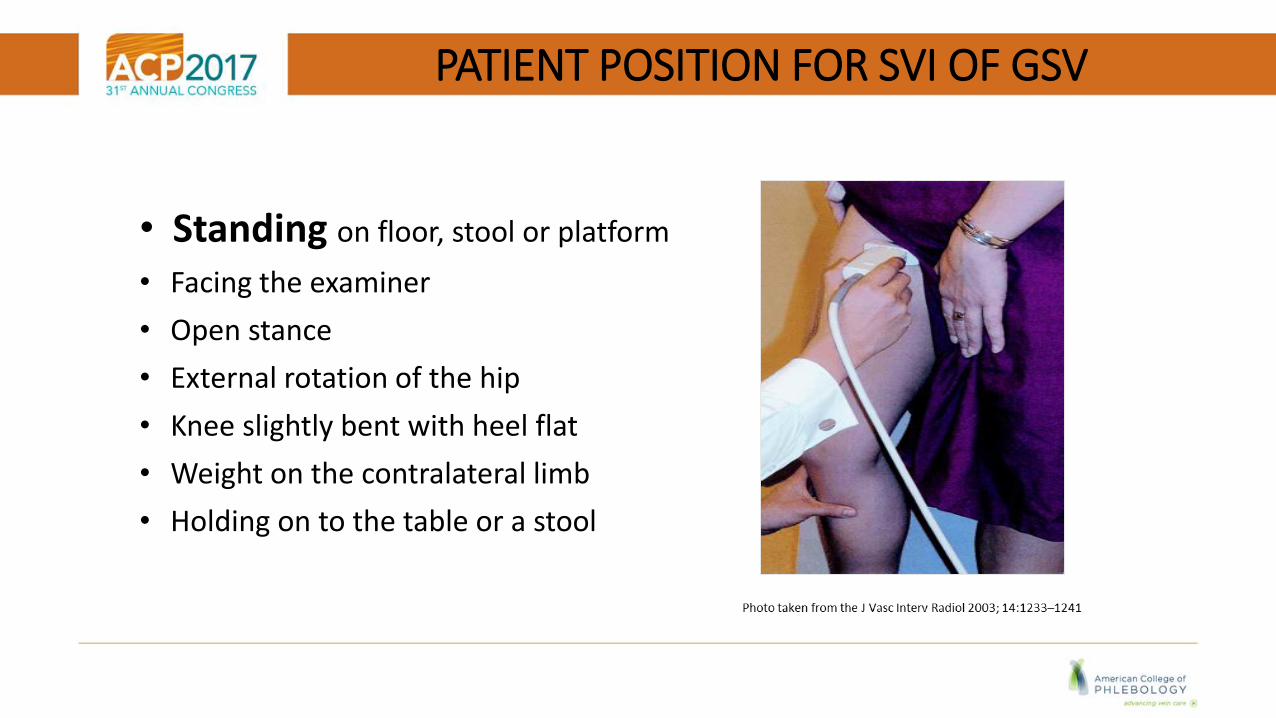
PATIENT POSITION FOR SVI OF GSV
• Standing on floor, stool or platform
• Facing the examiner
• Open stance
• External rotation of the hip
• Knee slightly bent with heel flat
• Weight on the contralateral limb
• Holding on to the table or a stool
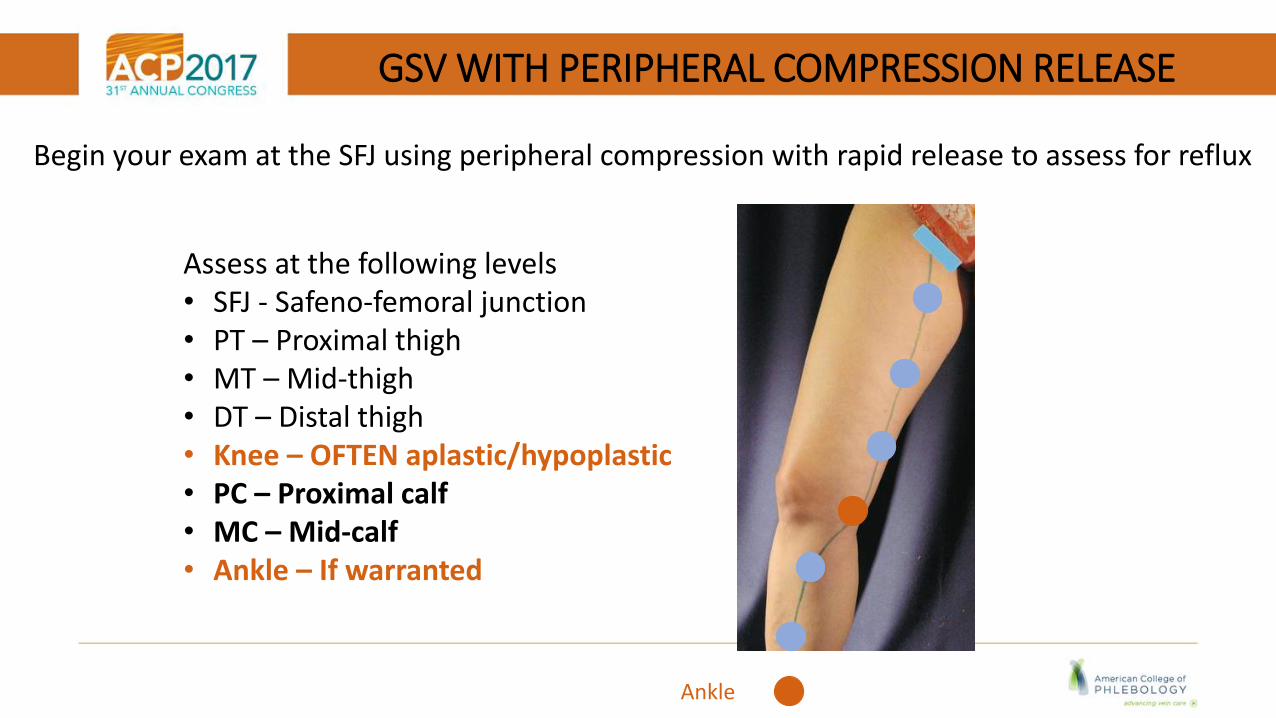
GSV WITH PERIPHERAL COMPRESSION RELEASE
Begin your exam at the SFJ using peripheral compression with rapid release to assess for reflux
Assess at the following levels• SFJ - Safeno-femoral junction• PT – Proximal thigh• MT – Mid-thigh• DT – Distal thigh• Knee – OFTEN aplastic/hypoplastic• PC – Proximal calf• MC – Mid-calf • Ankle – If warranted
Ankle
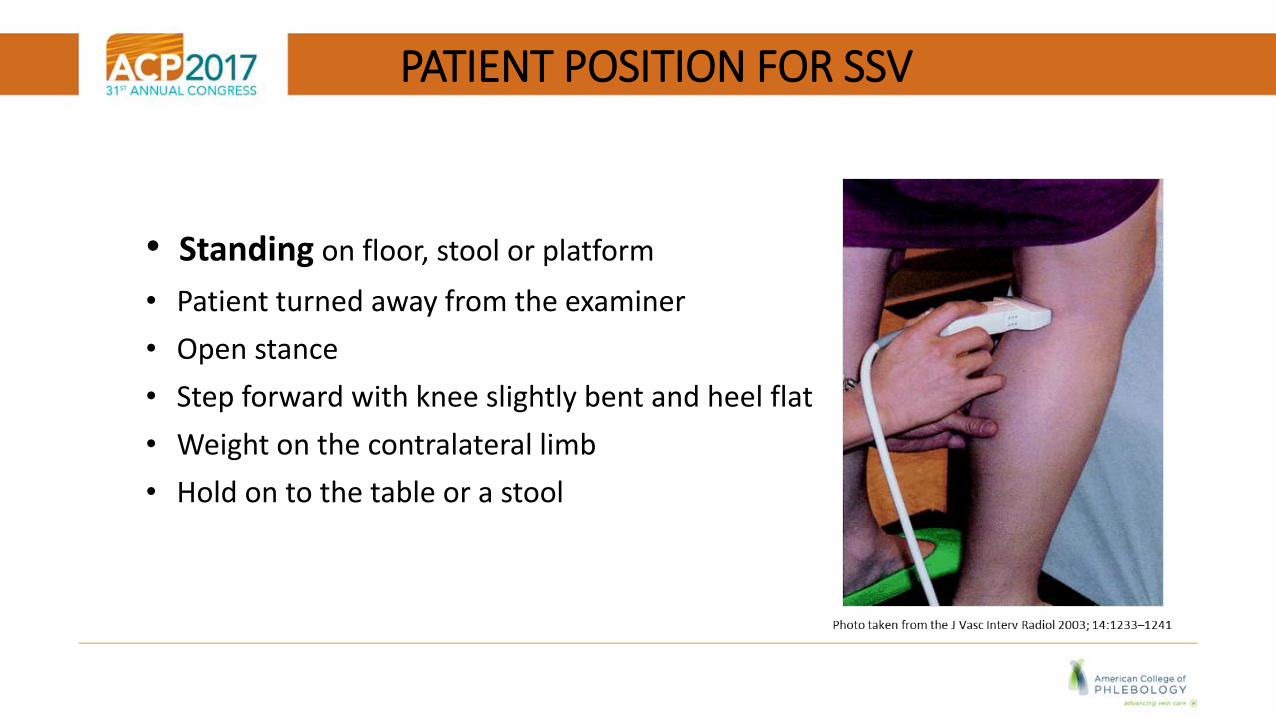
PATIENT POSITION FOR SSV
• Standing on floor, stool or platform
• Patient turned away from the examiner
• Open stance
• Step forward with knee slightly bent and heel flat
• Weight on the contralateral limb
• Hold on to the table or a stool
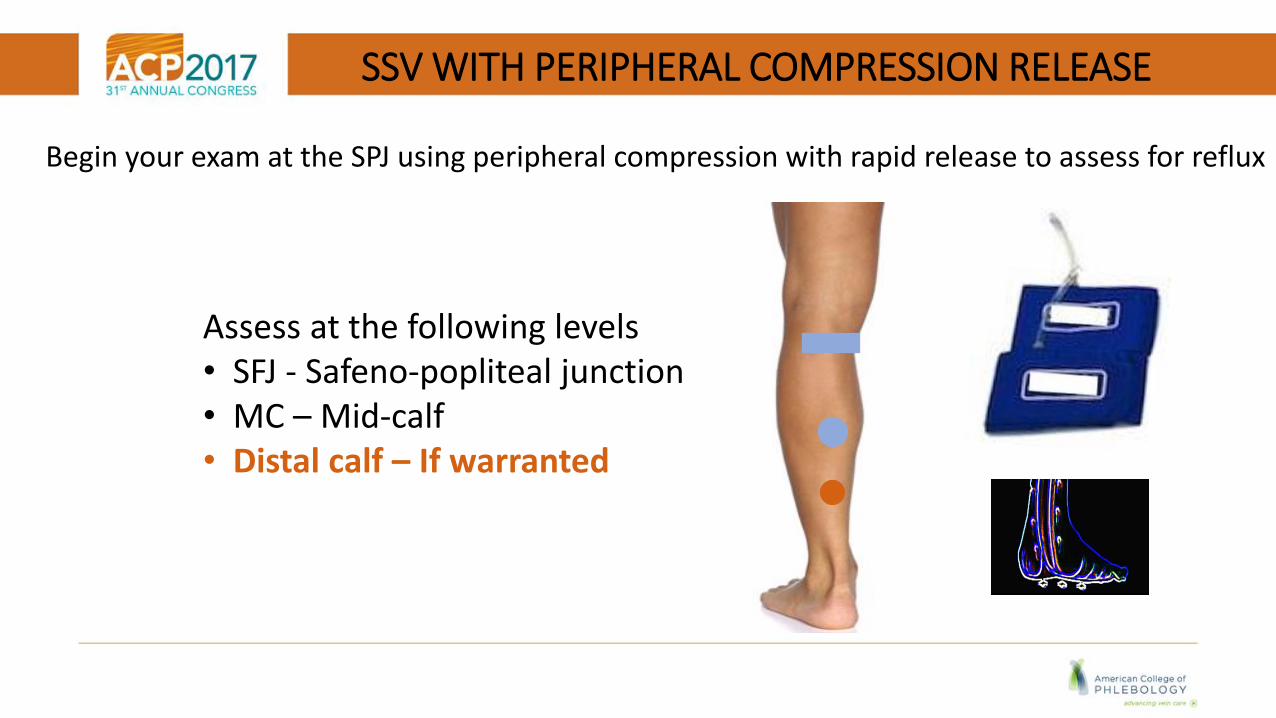
SSV WITH PERIPHERAL COMPRESSION RELEASE
Begin your exam at the SPJ using peripheral compression with rapid release to assess for reflux
Assess at the following levels• SFJ - Safeno-popliteal junction• MC – Mid-calf • Distal calf – If warranted

NORMAL GSV & SSV
Diameter• GSV 5.0 mm + 2.4mm• SSV 3 mm + 1.3mm
Competent Valve • GSV < 0.5 sec • SSV < 0.5 sec
J Korean Surg Soc. 2013 Oct; 85(4): 169–174. Published online 2013 Sep 30. doi: 10.4174/jkss.2013.85.4.169
Valve Closure
Use SAX view to obtain an anteroposterior
diameter measurement
A valve closure time of < 0.5 sec is considered
competent.

REFLUX DEFINED AND MEASURED IN THE SUPERFICIAL VEINS
PW Doppler
• GSV > 0.5 sec
• SSV > 0.5 sec REFLUX DURATION
Reflux is defined as retrograde flow of blood a vein
Color DopplerFlow reversal

REFLUX EVALUATION FOR GSV & AAGSV
• Identify the SFJ in SAX then turn to LAX
• PW Doppler examine the entire length of the vein using
peripheral compression rapid release to assess for reflux
• Measure diameter and depth and appropriately label each segment
• Measure and document the reflux duration
SFJDiam. _____Depth_____PTDiam. _____Depth_____MTDiam. _____Depth_____DTDiam. _____Depth_____KNEEDiam. _____Depth_____PCDiam. _____Depth_____MCDiam._____Depth_____DCDiam._____Depth_____
GSV reflux _______sec
AAGSV reflux _______sec
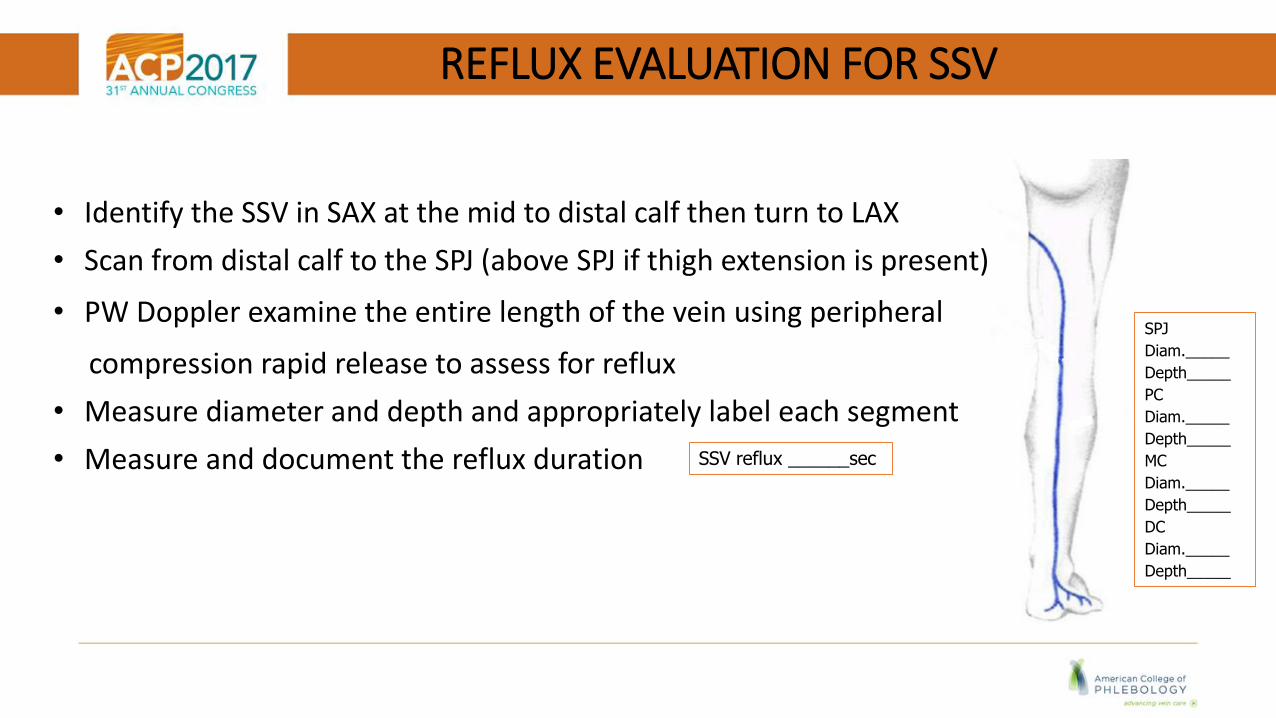
REFLUX EVALUATION FOR SSV
• Identify the SSV in SAX at the mid to distal calf then turn to LAX
• Scan from distal calf to the SPJ (above SPJ if thigh extension is present)
• PW Doppler examine the entire length of the vein using peripheral
compression rapid release to assess for reflux
• Measure diameter and depth and appropriately label each segment
• Measure and document the reflux duration SSV reflux ______sec
SPJ
Diam._____
Depth_____
PC
Diam._____
Depth_____
MC
Diam._____
Depth_____
DC
Diam._____
Depth_____
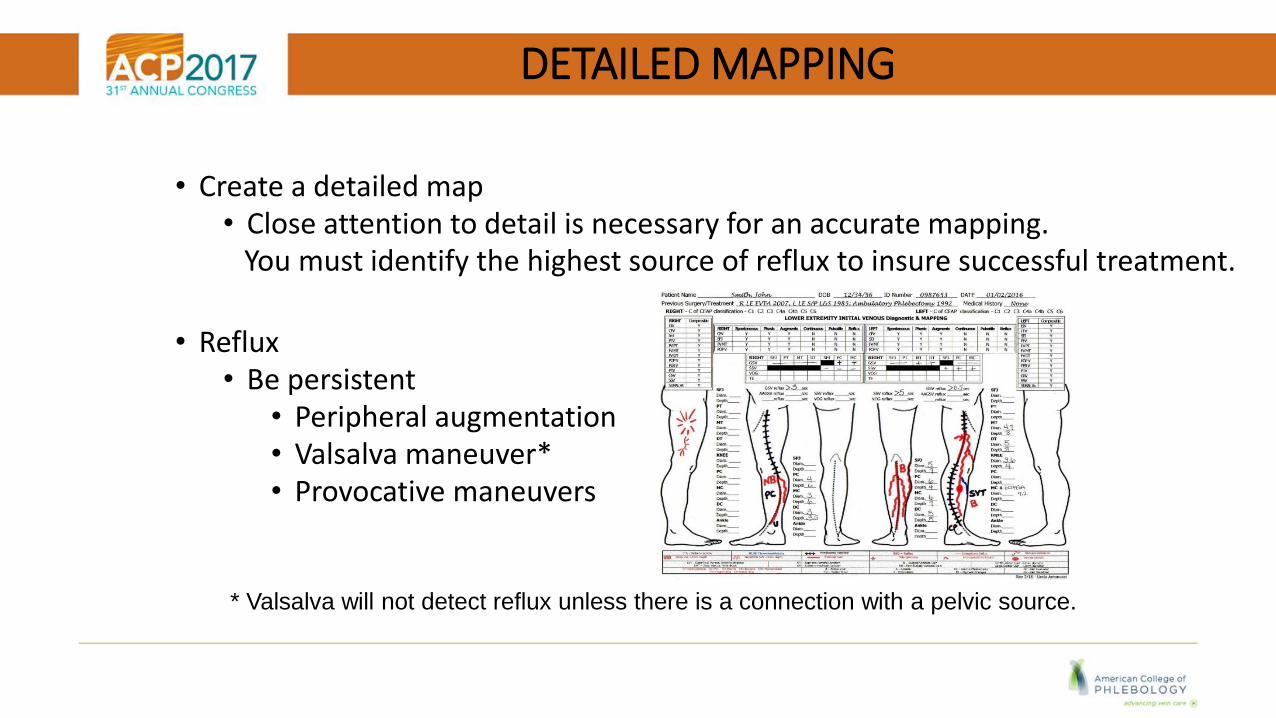
DETAILED MAPPING
• Create a detailed map• Close attention to detail is necessary for an accurate mapping.
You must identify the highest source of reflux to insure successful treatment.
• Reflux• Be persistent
• Peripheral augmentation• Valsalva maneuver*• Provocative maneuvers
* Valsalva will not detect reflux unless there is a connection with a pelvic source.

GSV ORIGIN AND TERMINATION
ORIGIN anterior to the medial
malleolus
TERMINATESatSFJ
Images taken from “Venous Ultrasound A Comprehensive Approach” used with permission from Dr. Miguel LoVuolo
The great saphenous vein dramatically changes direction at the white dot which is referred to as Boyd’s point and deviates toward the posterior aspect of the knee.
GSV
AASV __
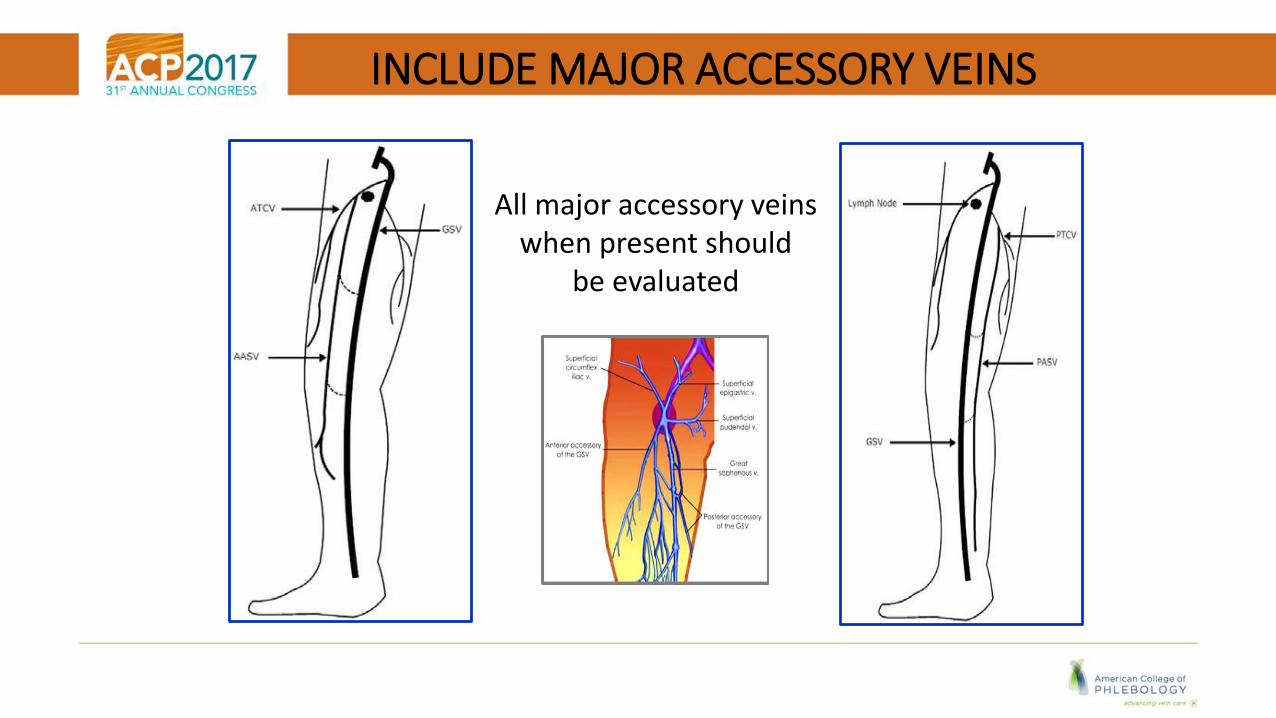
INCLUDE MAJOR ACCESSORY VEINS
All major accessory veinswhen present should
be evaluated
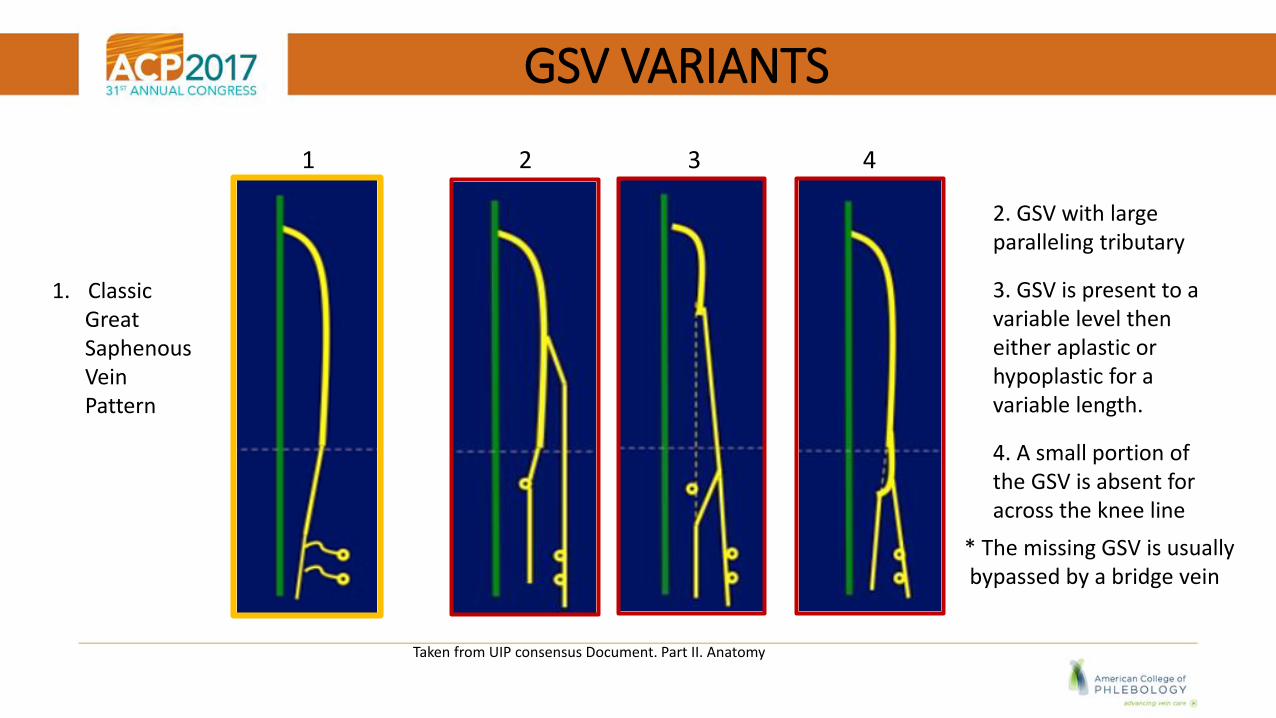
GSV VARIANTS
Taken from UIP consensus Document. Part II. Anatomy
1 2 3 4
1. ClassicGreatSaphenous Vein Pattern
2. GSV with large paralleling tributary
3. GSV is present to a variable level then either aplastic or hypoplastic for a variable length.
4. A small portion of the GSV is absent for across the knee line
* The missing GSV is usuallybypassed by a bridge vein
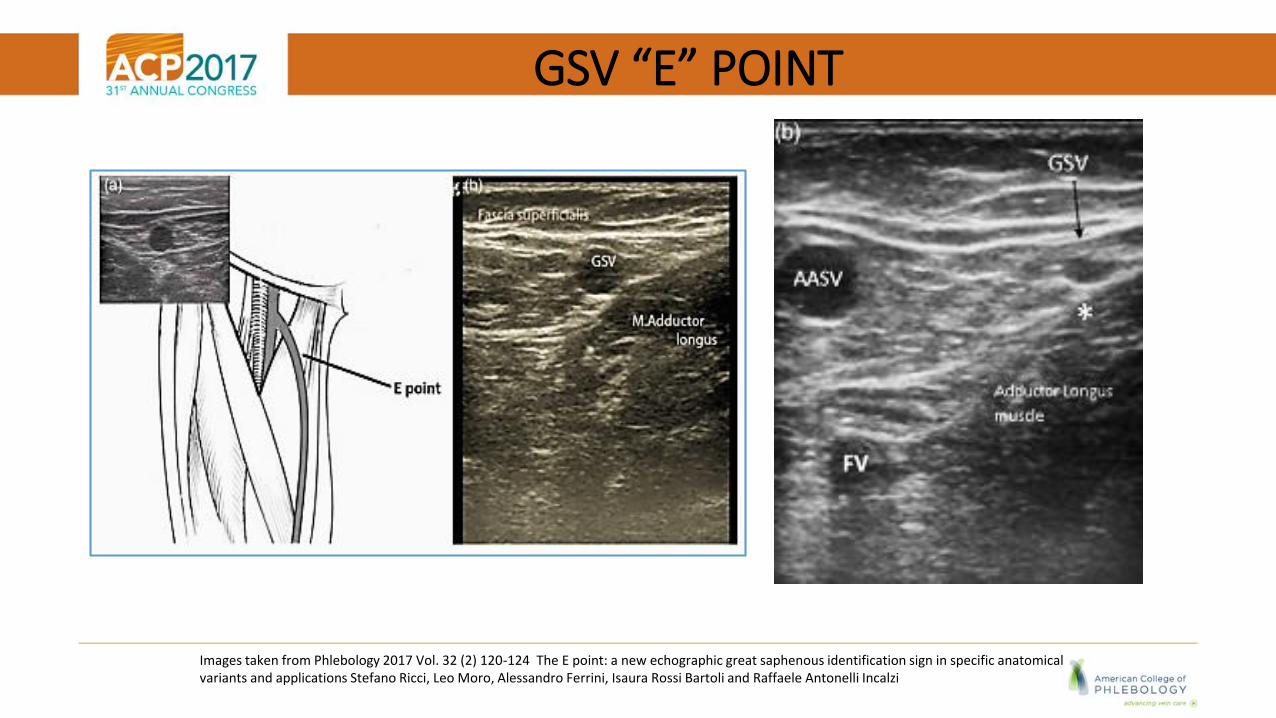
GSV “E” POINT
Images taken from Phlebology 2017 Vol. 32 (2) 120-124 The E point: a new echographic great saphenous identification sign in specific anatomical variants and applications Stefano Ricci, Leo Moro, Alessandro Ferrini, Isaura Rossi Bartoli and Raffaele Antonelli Incalzi
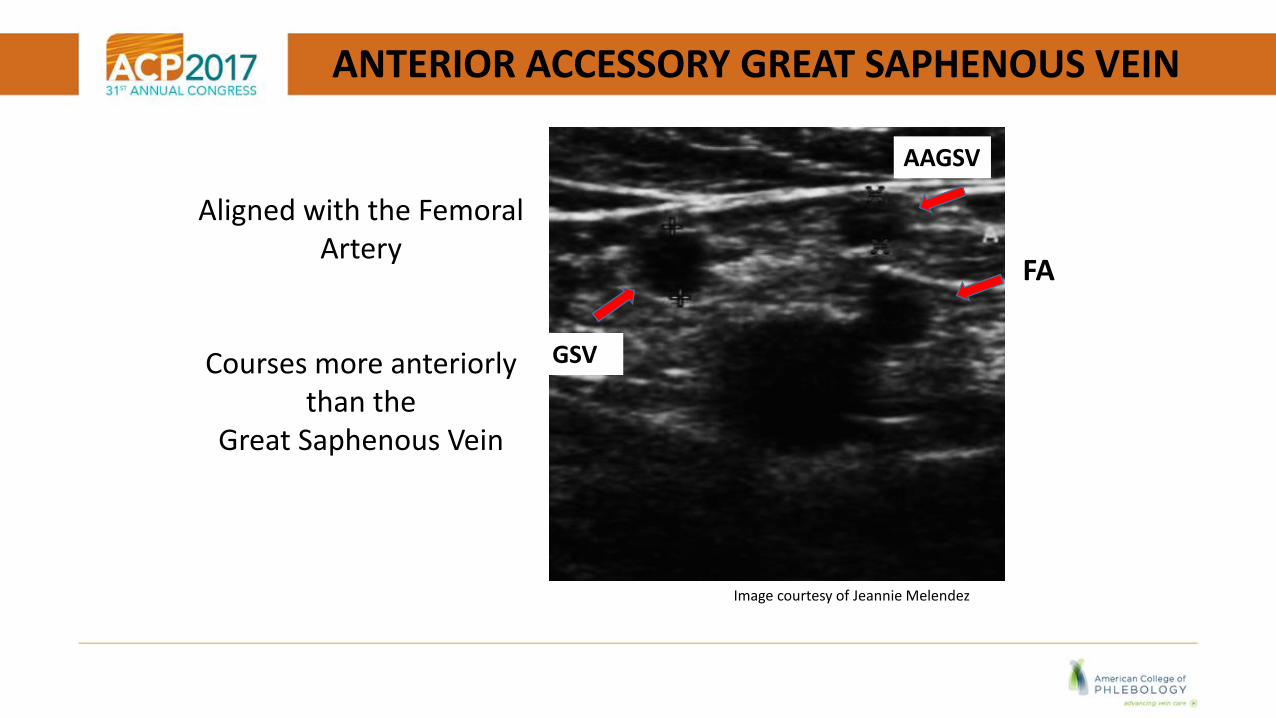
ANTERIOR ACCESSORY GREAT SAPHENOUS VEIN
Aligned with the Femoral Artery
Courses more anteriorly than the
Great Saphenous Vein
AAGSV
GSV
FA
Image courtesy of Jeannie Melendez
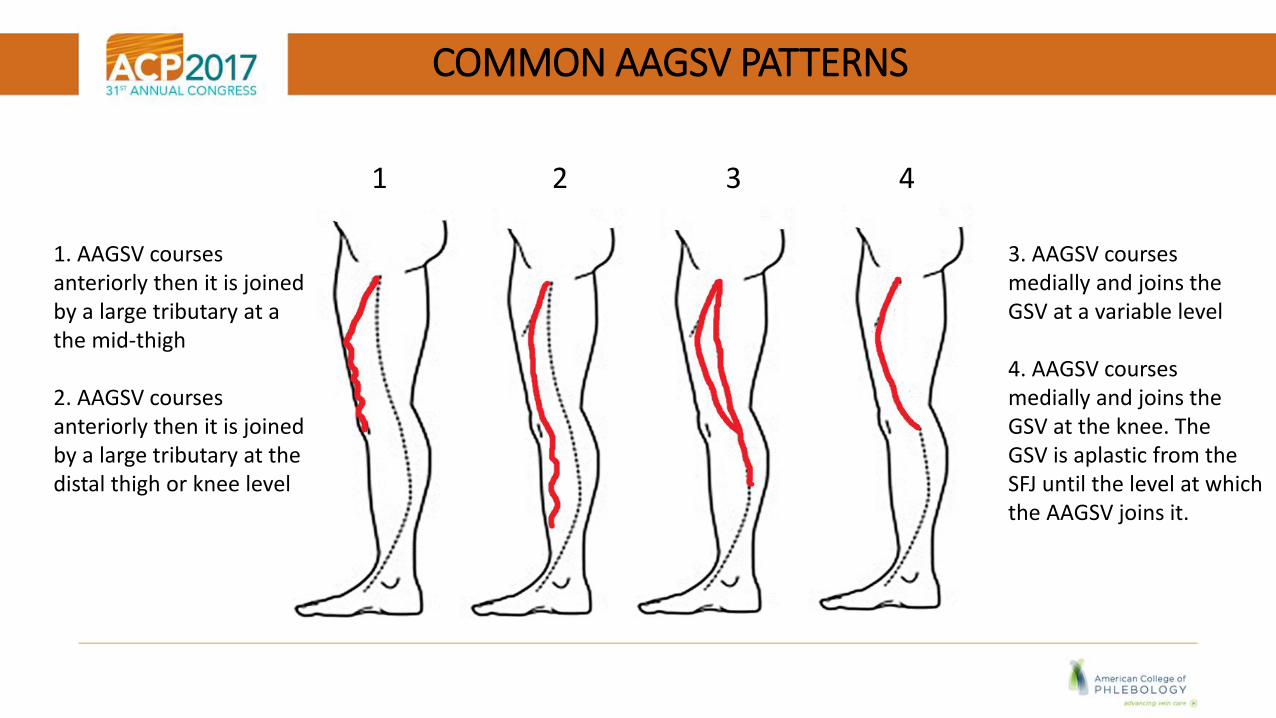
COMMON AAGSV PATTERNS
1 2 3 4
1. AAGSV coursesanteriorly then it is joined by a large tributary at a the mid-thigh
2. AAGSV coursesanteriorly then it is joined by a large tributary at the distal thigh or knee level
3. AAGSV coursesmedially and joins the GSV at a variable level
4. AAGSV coursesmedially and joins the GSV at the knee. The GSV is aplastic from theSFJ until the level at which the AAGSV joins it.
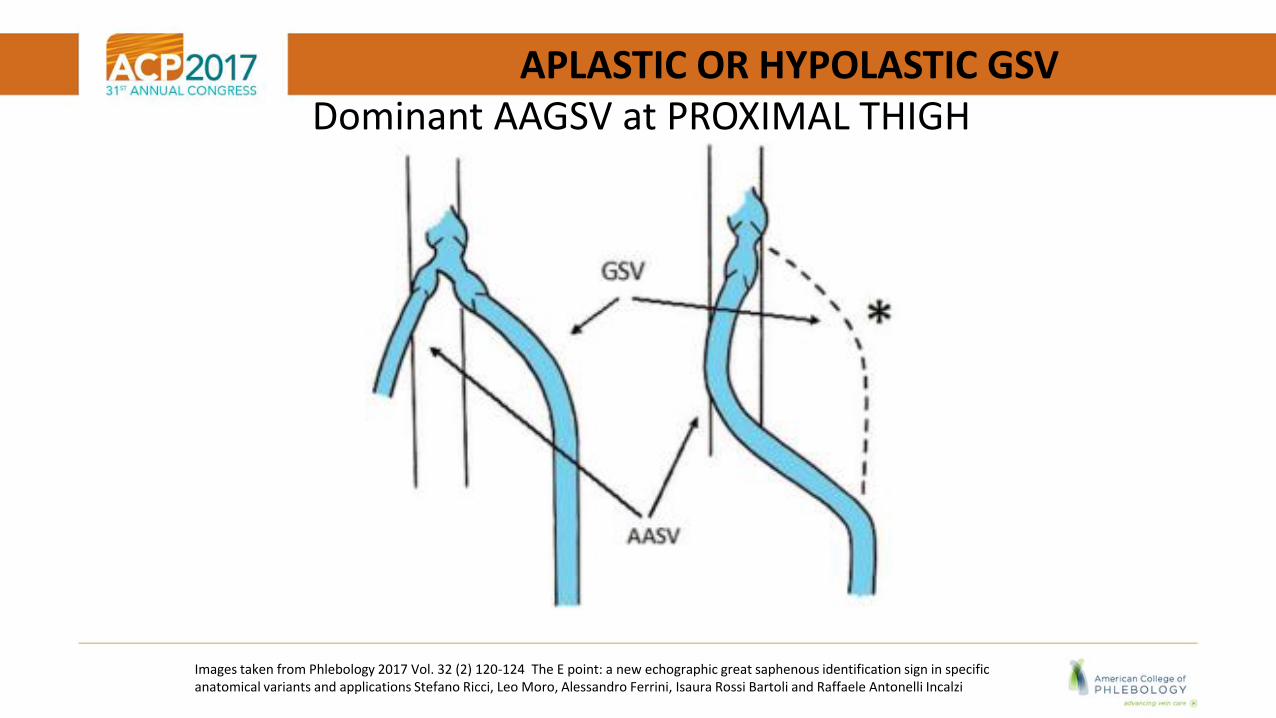
APLASTIC OR HYPOLASTIC GSV Dominant AAGSV at PROXIMAL THIGH
Images taken from Phlebology 2017 Vol. 32 (2) 120-124 The E point: a new echographic great saphenous identification sign in specific anatomical variants and applications Stefano Ricci, Leo Moro, Alessandro Ferrini, Isaura Rossi Bartoli and Raffaele Antonelli Incalzi
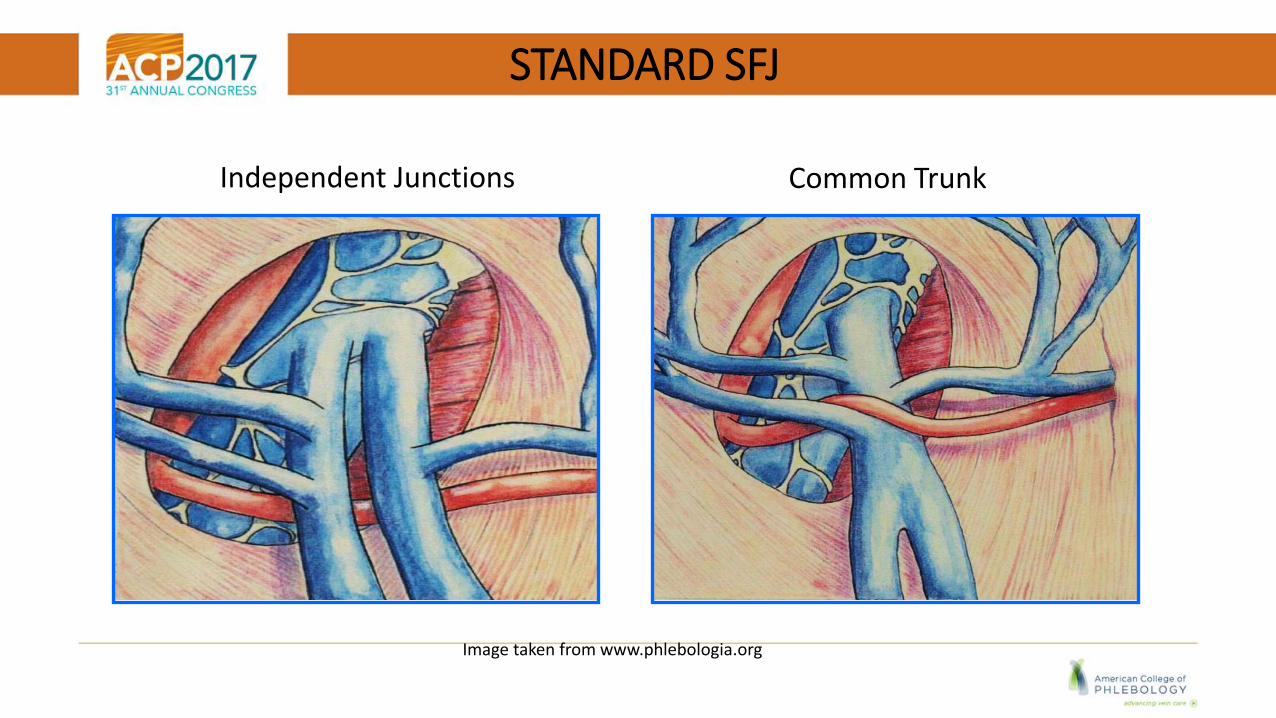
STANDARD SFJ
Image taken from www.phlebologia.org
Common TrunkIndependent Junctions

SFJ VARIANT - ECTASIA
Image taken from www.phlebologia.org
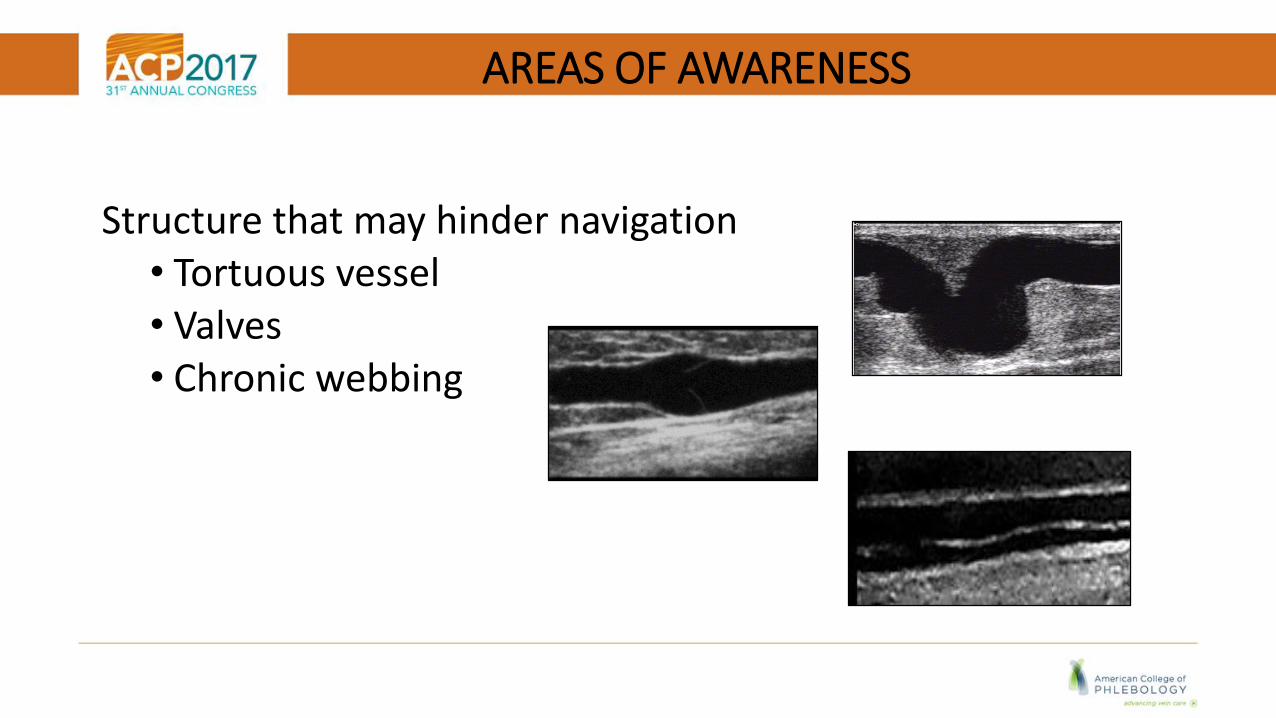
AREAS OF AWARENESS
Structure that may hinder navigation • Tortuous vessel• Valves• Chronic webbing
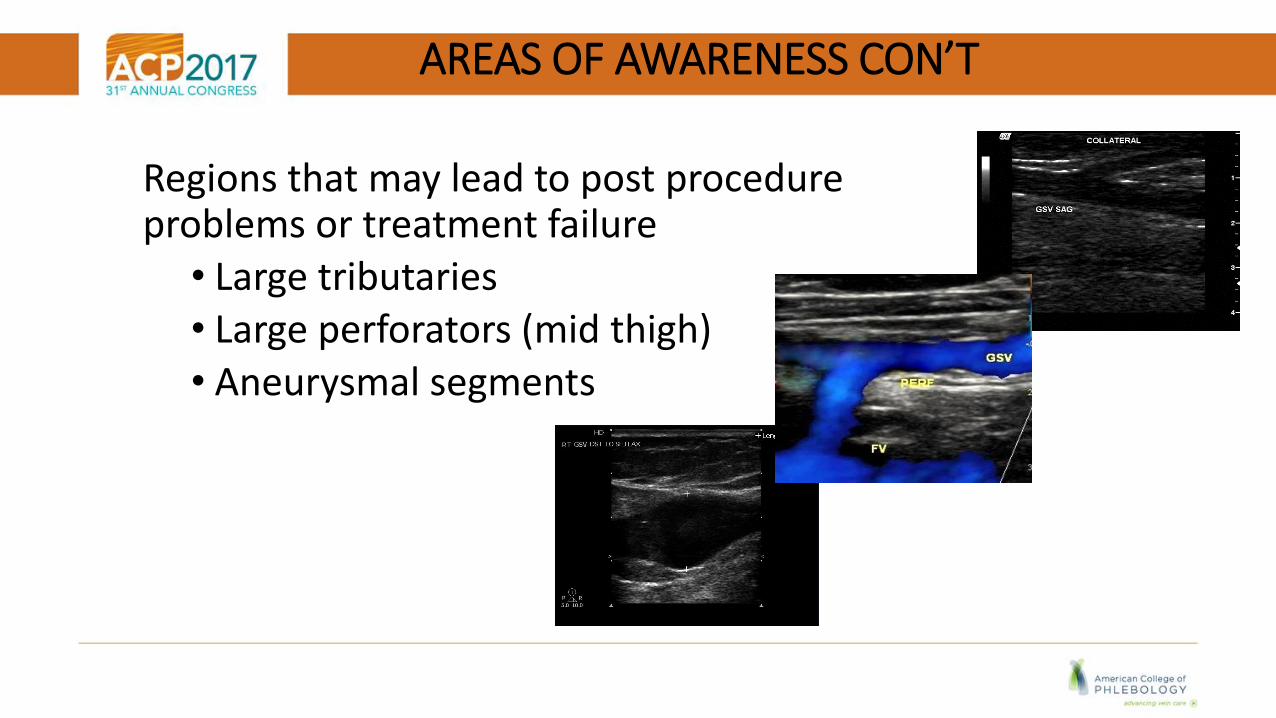
AREAS OF AWARENESS CON’T
Regions that may lead to post procedure problems or treatment failure
• Large tributaries • Large perforators (mid thigh)• Aneurysmal segments
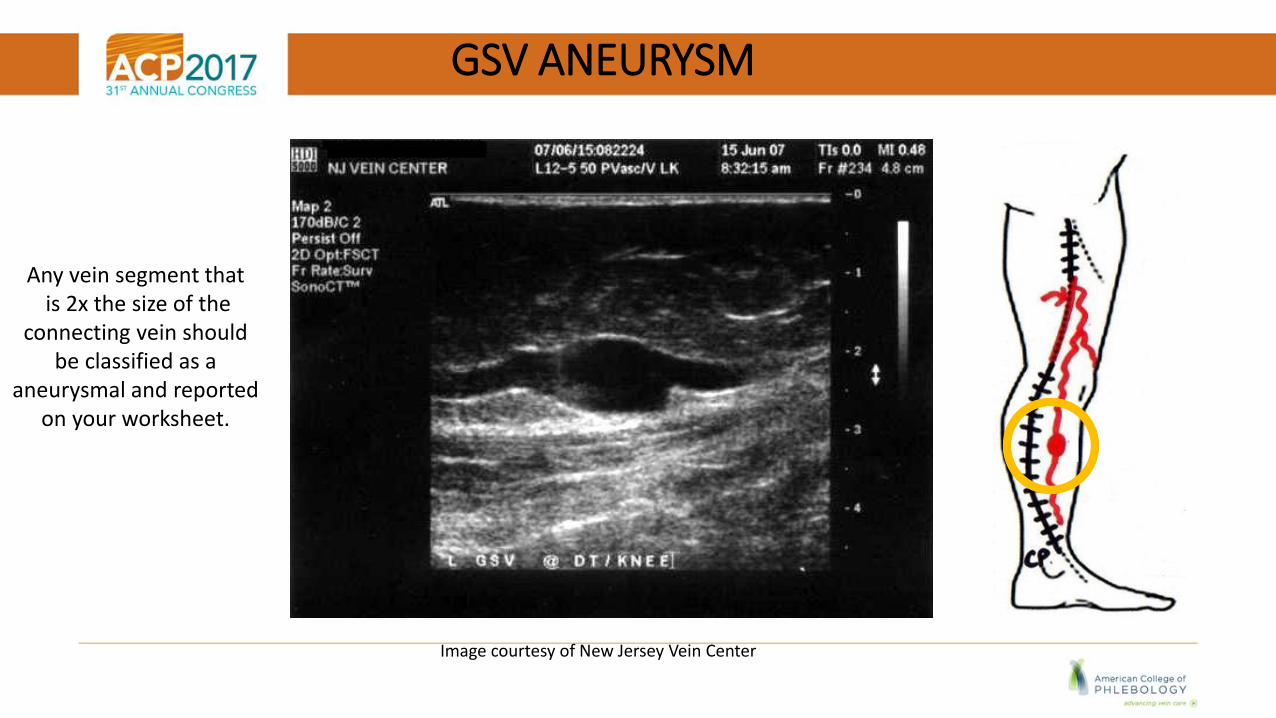
GSV ANEURYSM
Image courtesy of New Jersey Vein Center
Any vein segment thatis 2x the size of the
connecting vein should be classified as a
aneurysmal and reported on your worksheet.
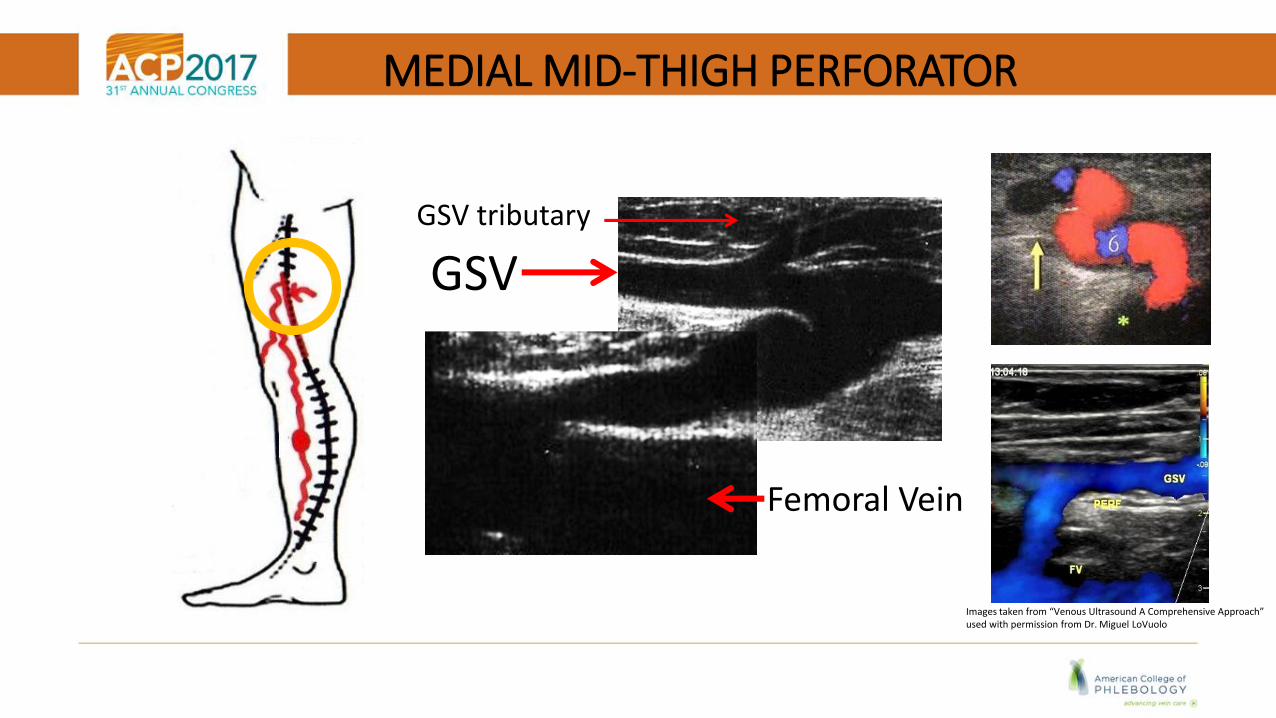
MEDIAL MID-THIGH PERFORATOR
GSV
Femoral Vein
GSV tributary
Images taken from “Venous Ultrasound A Comprehensive Approach” used with permission from Dr. Miguel LoVuolo
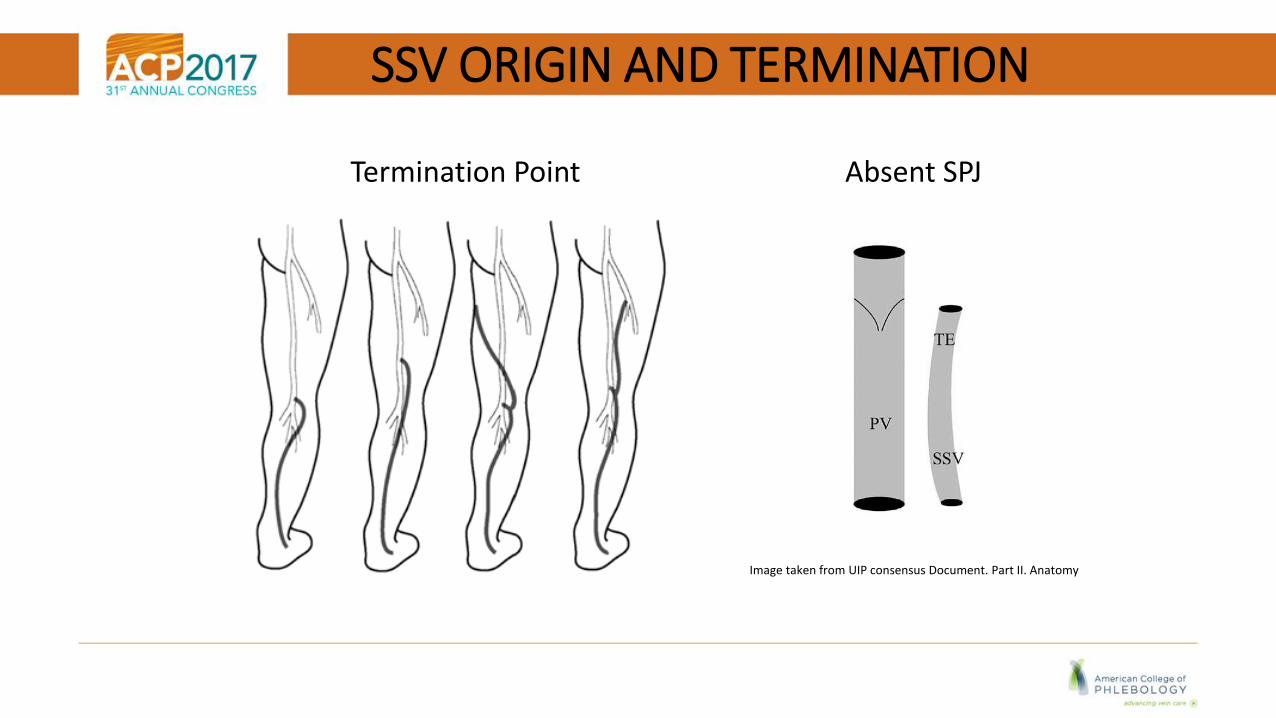
SSV ORIGIN AND TERMINATION
Termination Point Absent SPJ
Image taken from UIP consensus Document. Part II. Anatomy
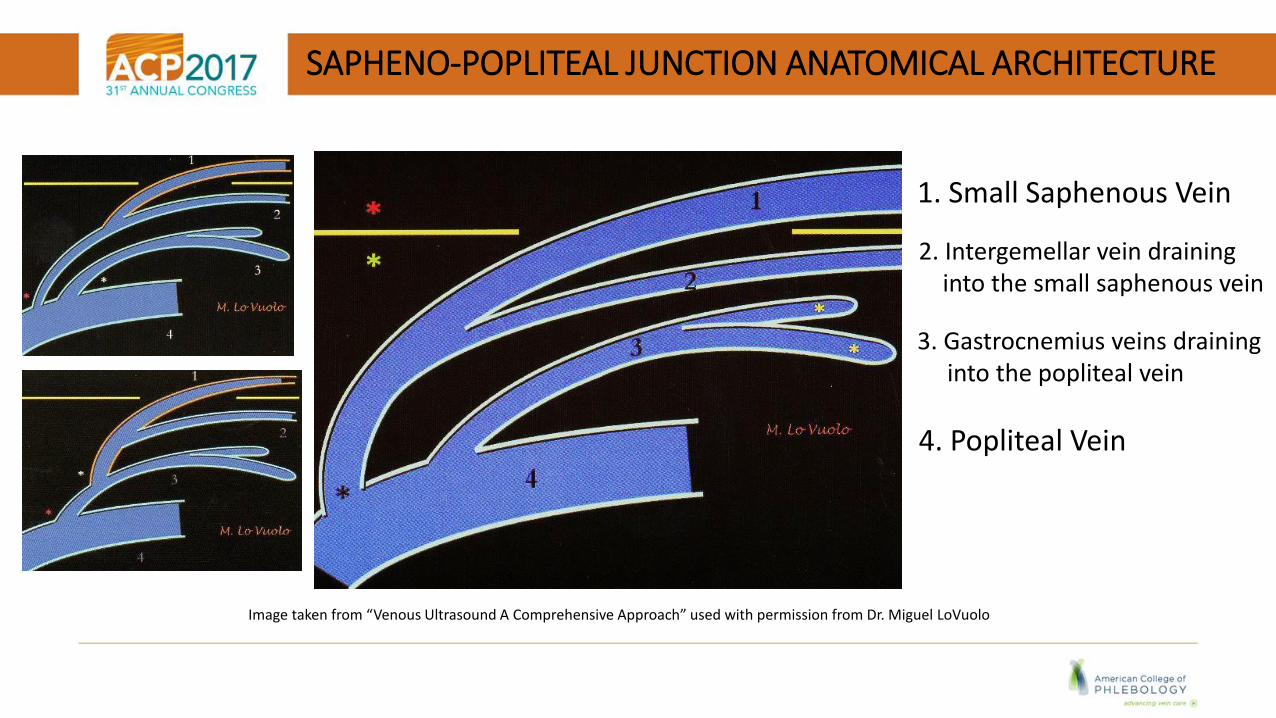
SAPHENO-POPLITEAL JUNCTION ANATOMICAL ARCHITECTURE
Image taken from “Venous Ultrasound A Comprehensive Approach” used with permission from Dr. Miguel LoVuolo
1. Small Saphenous Vein
2. Intergemellar vein draininginto the small saphenous vein
3. Gastrocnemius veins draining into the popliteal vein
4. Popliteal Vein

“BECAUSE OF” OR THE “CAUSE OF”
Image taken from researchgate.org

Linda Antonucci, RPhS, RVT, RDCS Email - [email protected]


![Malassezia Folliculitis versus Truncal Acne Vulgaris ... · 278 Malassezia Folliculitis versus Truncal Acne Vulgaris (Clinical and Histopathological Study) support the diagnosis [5,6,10]](https://img.pdfslide.us/doc/110x75/5cdf712988c99399558c9005/malassezia-folliculitis-versus-truncal-acne-vulgaris-278-malassezia-folliculitis.jpg)